Pharmacological interventions for drug‐using offenders
Abstract
Background
The review represents one in a family of four reviews focusing on a range of different interventions for drug‐using offenders. This specific review considers pharmacological interventions aimed at reducing drug use and/or criminal activity for illicit drug‐using offenders.
Objectives
To assess the effectiveness of pharmacological interventions for drug‐using offenders in reducing criminal activity and/or drug use.
Search methods
Fourteen electronic bibliographic databases (searched between 2004 and 21 March 2013) and five additional Web resources (searched between 2004 and 11 November 2011) were searched. Experts in the field were contacted for further information.
Selection criteria
Randomised controlled trials assessing the efficacy of any pharmacological interventions for reducing, eliminating or preventing relapse in drug‐using offenders were included. Data on the cost and cost‐effectiveness of interventions were reported.
Data collection and analysis
We used standard methodological procedures as expected by The Cochrane Collaboration.
Main results
A total of 76 trials across the four reviews were identified. After a process of prescreening had been completed, 17 trials were judged to meet the inclusion criteria for this specific review (six of the 17 trials are awaiting classification for the review). The remaining 11 trials contained a total of 2,678 participants. Nine of the eleven studies used samples with a majority of men. The interventions (buprenorphine, methadone and naltrexone) were compared to non pharmacological treatments (e.g., counselling) and other pharmacological drugs. The methodological trial quality was poorly described, and most studies were rated as 'unclear' by the reviewers. The biggest threats to risk of bias were generated through blinding (performance and detection bias) and incomplete outcome data (attrition bias). When combined, the results suggest that pharmacological interventions do significantly reduce subsequent drug use using biological measures, (three studies, 300 participants, RR 0.71 (95% CI 0.52 to 0.97)), self report dichotomous data (three studies, 317 participants, RR 0.42, (95% CI 0.22 to 0.81)) and continuous measures (one study, MD ‐59.66 (95% CI ‐120.60 to 1.28)) . In the subgroups analysis for community setting, (two studies, 99 participants: RR 0.62 (95% CI 0.35 to 1.09)) and for secure establishment setting, (one study, 201 participants: RR 0.76 (95% CI 0.52 to 1.10)), the results are no longer statistically significant. Criminal activity was significantly reduced favouring the dichotomous measures of re arrest, (one study, 62 participants, RR 0.60 (95% CI 0.32 to 1.14)), re‐incarceration, (three studies, 142 participants, RR 0.33 (95% CI 0.19 to 0.56)) and continuous measures (one study, 51 participants, MD ‐74.21 (95% CI ‐133.53 to ‐14.89)). Findings on the effects of individual pharmacological interventions on drug use and criminal activity show mixed results. Buprenorphine in comparison to a non pharmacological treatment seemed to favour buprenorphine but not significantly with self report drug use, (one study, 36 participants, RR 0.58 (95% CI 0.25 to 1.35)). Methadone and cognitive behavioural skills in comparison to standard psychiatric services, did show a significant reduction for self report dichotomous drug use (one study, 253 participants, RR 0.43 (95% CI 0.33 to 0.56)) but not for self report continuous data (one study 51 participants) MD ‐0.52 (95% CI ‐1.09 to 0.05)), or re incarceration RR 1.23 (95% CI 0.53 to 2.87)). Naltrexone was favoured significantly over routine parole and probation for re incarceration (two studies 114 participants, RR 0.36 (95% CI 0.19 to 0.69)) but no data was available on drug use. Finally, we compared each pharmacological treatment to another. In each case we compared methadone to: buprenorphine, diamorphine and naltrexone. No significant differences were displayed for either treatment for self report dichotomous drug use (one study, 193 participants RR 1.23 (95% CI 0.86 to 1.76)), continuous measures of drug use MD 0.70 (95% CI ‐5.33 to 6.73) or criminal activity RR 1.25 (95% CI 0.83 to 1.88)) between methadone and buprenorphine. Similiar results were found for comparisons with Diamorphine with no significant differences between the drugs for self report dichotomous drug use for arrest (one study, 825 participants RR 1.25 (95% CI 1.03‐1.51)) or Naltrexone for dichotomous measures of re incarceration (one study, 44 participants, RR 1.10 (95% CI 0.37 to 3.26)), and continuous outcome measure of crime MD ‐0.50 (95% CI ‐8.04 to 7.04)) or self report drug use MD 4.60 (95% CI ‐3.54 to 12.74)).
Authors' conclusions
Pharmacological interventions for drug‐using offenders do appear to reduce overall subsequent drug use and criminal activity (but to a lesser extent). No statistically significant differences were displayed by treatment setting. Individual differences are displayed between the three pharmacological interventions (buprenorphine, methadone and naltrexone) when compared to a non pharmacological intervention, but not when compared to each other. Caution should be taken when interpreting these findings, as the conclusions are based on a small number of trials, and generalisation of these study findings should be limited mainly to male adult offenders. Additionally, many studies were rated at high risk of bias because trial information was inadequately described.
PICO
Plain language summary
Pharmacological interventions for drug‐using offenders
Drug‐using offenders by their nature represent a socially excluded group in which drug use is more prevalent than in the rest of the population. Pharmacological interventions play an important role in the rehabilitation of drug‐using offenders. For this reason, it is important to investigate what we know works when pharmacological interventions are provided for offenders. The review identified 17 trials (six of which are awaiting classification) containing 2,678 offenders. Interventions included evaluations of (1) naltrexone in comparison with routine parole, social psychological treatment or both, (2) methadone maintenance in comparison with different counselling options and (3) naltrexone, diamorphine and buprenorphine in comparison with a non pharmacological alternative and in combination with another pharmacological treatment. Overall, the findings suggest that such interventions have an impact on reducing drug use and criminal activity to a variable extent. Methadone does not seem to perform better than control intervention in different settings. However, because the number of studies is small, this finding should be taken with caution. Findings on the effects of individual pharmacological interventions on drug use and criminal activity show mixed results. Buprenorphine and methadone, were shown to reduce subsequent drug use but results were statistically significant only for methadone. We could not evaluate the impact of buprenorphine on criminal activity because we did not have the relevant study data. Methadone was not found to have a significant impact on reduction of re‐incarceration whereas naltrexone, significantly reduced re incarceration. We also investigated whether one treatment was better than another. We found no significant differences between any of the drug comparisons (methadone vs buprenorphine, diamorphine and naltrexone) on any of the outcome measures. Aside from any practical implications relating to administration or the cost of the drug this suggests that one drug does not perform better than another. The results were based on the findings of single trials and should be interpreted with caution until further trial evidence is available to confirm or refute these findings. One study provided some cost comparisons between buprenorphine and methadone, but data were not sufficient to generate a cost‐effectiveness analysis. In conclusion, we found that pharmacological interventions do reduce subsequent drug use and criminal activity (to a lesser extent). Additionally, we found individual differences and variation between the degree to which successful interventions were implemented and were able to sustain reduction of drug use and criminal activity.
Authors' conclusions
Background
This review represents part of a family of four reviews undertaken to closely examine what works in reducing drug use and criminal activity among drug‐using offenders. Overall, the four reviews contain 76 trials, generating 99 publications and 58 different comparisons (Perry 2013a; Perry 2013b; Perry 2013c). The four reviews represent specific interests in pharmacological interventions, non‐pharmacological interventions, female offenders and offenders with co‐occurring mental illness. All four reviews stem from an updated previous Cochrane systematic review (Perry 2006). In this set of four reviews, we consider the effectiveness of interventions based on two key outcomes and analyse the impact of setting and intervention type. Presented here is the revised methodology for this individual review, focusing on the impact of pharmacological interventions provided for drug‐using offenders.
Description of the condition
Offenders as a socially excluded group of people demonstrate significant drug use and subsequent health problems. Studies investigating the prevalence of drug dependence in UK prisons report variable results of 10% (Gunn 1991), 39% (Brooke 1996) and 33% (Mason 1997). Similar trends have been reported elsewhere. In France, 30% of prison inmates are heroin addicted, and in Australia, 59% of prison inmates report injecting (primarily heroin) drug use histories. In the US, it is recognised that many offenders are in need of treatment to tackle their drug use (Lo 2000).The link between drug use, subsequent health and social and criminological consequences is well documented in the literature (e.g., Michel 2005), and offenders have a high risk of death from opioid overdose within two weeks of release from incarceration (Bird 2003; Binswanger 2007).
Description of the intervention
Internationally, methadone maintenance has been the primary choice for chronic opioid dependence in prisons and jails, including those in the Netherlands, Australia, Spain and Canada, and it is being increasingly implemented in the criminal justice setting (Moller 2007; Stallwitz 2007). The US has not generally endorsed the use of methadone treatment, and only 12% of correctional settings offer this option for incarcerated inmates (Fiscella 2004). Reasons for this lack of expansion suggest that methadone amongst the public and criminal justice system providers has been considered a substitute for another addiction. In contrast, buprenorphine appears not to carry the same social stigma associated with methadone treatment and has been used in France, Austria and Puerto Rico (Catania 2003; Reynaud‐Maurupt 2005; Garcia 2007). Naltrexone treatment has shown some promising findings, but associated problems surrounding high attrition and low medication compliance in the community and high mortality rates (e.g. Gibson 2007; Minozzi 2011) pose concerns. Trials conducted in the criminal justice setting are still lacking, and continuity of care is considered crucial in the treatment of drug‐involved offenders who transition between prison and the community.
How the intervention might work
A growing body of evidence shows the effects of pharmacological interventions for drug use among the general population. Existing reviews have focused on naltrexone maintenance treatment for opioid dependence (Amato 2005; Lobmaier 2008; Minozzi 2011) and the efficacy of methadone (Marsch 1998; Faggiano 2003; Mattick 2009) and buprenorphine maintenance (Mattick 2009). Recent guidance has been provided from the National Institute for Health and Clinical Excellence on evidence‐based use of naltrexone, methadone and buprenorphine for the management of opioid dependence (NICE 2007a; NICE 2007b). Five Cochrane reviews (including 52 studies) reported on the effectiveness of opiate methadone therapies (Amato 2005). Findings showed that methadone maintenance therapies at appropriate doses were most effective in retaining participants in treatment and in suppressing heroin use, but evidence of effectiveness for other relevant outcome measures such as criminal activity was weak and was not systematically evaluated.
Systematic reviews evaluating treatment programs more generally for offender populations have focused on evaluating treatment in one setting such as community‐based programmes, (e.g.,Mitchell, 2012a; Mitchell, 2012b); or have based their evidence on literature from one country (e.g. Germany or the US) (Chanhatasilpa 2000; Egg 2000) or a number of specific treatments (Mitchell 2006). Pharmacological systematic reviews of offender treatment appear to be sparse. We identified two previous reviews, one focusing on specific drug‐ and property‐related criminal behaviours in methadone maintenance treatment (Marsch 1998) and an evaluation of the effectiveness of opioid maintenance treatment (OMT) in prison and post‐release. The later of these two reviews identified six experimental studies up until January 2011 (Hedrich 2011). The review authors found that OMT in prison was significantly associated with reduced heroin use, injecting and syringe sharing. Use of pre‐release OMT was also found to have important implications for associated treatment uptake after release, but the impact on criminal activity was equivocal.
Why it is important to do this review
The current review will provide a systematic examination of trial evidence relating to the effectiveness of pharmacological interventions for drug‐using offenders. We believe it is important to conduct this review because the link between drug use and subsequent criminological consequences and a high risk of death suggests that a systematic review evaluating the effectiveness of routinely used pharmacological treatments is required. In order to address this broad topic a series of questions will consider the effectiveness of different interventions, in relation to criminal activity, drug misuse treatment setting and type of treatment. The review will additionally, report descriptively on the costs and cost effectiveness of such treatment programs.
Objectives
To assess the effectiveness of pharmacological interventions for drug‐using offenders in reducing criminal activity and/or drug misuse. The review addressed the following questions:
-
Do pharmacological treatments for drug‐using offenders reduce drug use?
-
Do pharmacological treatments for drug‐using offenders reduce criminal activity?
-
Does the treatment setting (e.g. court, community, prison/secure establishment) affect outcome(s) of pharmacological treatments?
-
Does the type of pharmacological treatment (e.g. medication type) affect treatment outcome(s)?
-
Does one type of pharmacological treatment perform better than one other?
Additionally, this review aimed to report on the cost and cost‐effectiveness of interventions.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) evaluating pharmacological interventions to reduce, eliminate or prevent relapse and/or criminal activity among drug‐using offenders were included. Relapse was used to refer to individuals who may have returned to an incarcerated setting or been subsequently arrested, who relapsed back into drug misuse or who did both.
Types of participants
Illicit drug‐misusing offenders were included in the review regardless of gender, age, ethnicity or psychiatric illness. Drug use was deemed relevant to any studies that referred to individuals using occasional drugs, being dependent on drugs or known to abuse drugs. We excluded studies that referred to tobacco or alcohol use. Offenders were defined as individuals who were involved in the criminal justice system. Offenders were those in police custody, being processed by the court system, residing in secure establishments (e.g. special hospitals, prisons or jails) or based in the community (i.e. under the care of probation or parole services).
Types of interventions
Included interventions were designed wholly or in part to eliminate or prevent relapse to drug use, criminal activity or both among participants. Different types of interventions were included in the review:
Experimental interventions included in the review:
-
Methadone.
-
Naltrexone.
-
Buprenorphine.
-
Diamorphine.
-
Combined pharmacological and counselling interventions.
-
Pharmacological treatments for cocaine and amphetamine dependence.
Control interventions included in the review.
-
No treatment.
-
Minimal treatment.
-
Waiting list.
-
Treatment as usual.
-
Other treatment (e.g., pharmacological or psychosocial)
Types of outcome measures
Primary outcomes
For the purpose of our review, we categorised primary outcomes into those related to dichotomous and continuous drug use, criminal activity or both. When papers reported several different follow‐up periods, the longest time period was included in the review. Given that reporting of criminal convictions can take time to be recorded and logged within the criminal justice system, we believe that such measures provide the most conservative estimate of effectiveness. For specific meta‐analyses of sub groupings, all reported follow‐up periods were reviewed so that the most appropriate time period for combining comparable studies would be selected.
-
Drug use measures were reported as:
-
-
self‐report drug use (unspecified drug, specific drug use not including alcohol/tobacco, Addiction Severity Index drug composite scores); and
-
biological drug use (measured by drugs tested by urine or hair analysis).
-
-
Criminal activity as measured by:
-
-
self‐report or official report of criminal activity (including arrest for any offence, drug offences, re‐incarceration, convictions, charges and recidivism).
-
Secondary outcomes
Our secondary outcome reported on cost or cost‐effectiveness information. These findings were presented in a descriptive narrative. A full critical appraisal based on the Drummond 1997 checklist was undertaken for those studies for which sufficient information was presented.
Search methods for identification of studies
Electronic searches
Electronic searches
The update searches identified records from 2004 to March 2013.
-
MEDLINE (1966 to March 2013).
-
EMBASE (1980 to March 2013).
-
CENTRAL (1980 to March 2013).
-
PsycINFO (1978 to March 2013).
-
Pascal (1973 to November 2004)a.
-
SciSearch (Science Citation Index) (1974 to March 2013).
-
Social SciSearch (Social Science Citation Index) (1972 to March 2013).
-
ASSIA (1987 to March 2013).
-
Wilson Applied Science and Technology Abstracts (1983 to October 2004)a.
-
Inside Conferences (1993 to November 2004)a.
-
Dissertation Abstracts (1961 to October 2004)a.
-
NTIS (1964 to March 2013).
-
Sociological Abstracts (1963 to March 2013).
-
HMIC (to March 2013).
-
PAIS (1972 to March 2013).
-
SIGLE (1980 to June 2004)b.
-
Criminal Justice Abstracts (1968 to March 2013).
-
LILACS (2004 to March 2013).
-
National Research Register (March 2004)c.
-
Current Controlled Trials (December 2009).
-
Drugscope (February 2004)-unable to access.
-
SPECTR (March 2004)d.
aUnable to access further to 2004 search.
bDatabase not updated since original 2004 search.
cNo longer exists.
dNow Campbell Collaboration searched on line.
To update the original review (Perry et al, 2006), the search strategy was restricted to studies that were published or unpublished from 2004 onwards. A number of original databases were not searched for this update (indicated by the key at the end of the database list). Pascal, ASSIA, Wilson Applied Science and Technology Abstracts, Inside Conferences and Dissertation Abstracts were not searched. These databases are available only via the fee‐charging DIALOG online host service. We did not have the resources to undertake these searches. The National Research Register no longer exists, and SIGLE has not been updated since 2005. Drugscope is available only to subscribing members. The original searches were undertaken by Drugscope staff.
Search strategies were developed for each database to exploit the search engine most effectively and to make use of any controlled vocabulary. Search strategies were designed to restrict the results to RCTs. No language restriction was placed on the search results. We included methodological search filters designed to identify trials. Whenever possible, filters retrieved from the InterTASC Information Specialists' Sub‐Group (ISSG) Search Filter Resource site (http://www.york.ac.uk/inst/crd/intertasc/) were used. If filters were unavailable from this site, search terms based on existing filters were used instead.
In addition to the electronic databases, a range of relevant Internet sites (Home Office, National Institute of Drug Abuse (NIDA) and European Association of Libraries and Information Services on Alcohol and Other Drugs (ELISAD)) were searched. Directory web sites, including OMNI (http://www.omni.ac.uk), were searched up until November 2011. The review did not place any language restrictions on identification and inclusion of studies in the review.
Details of the update search strategies and results and of the Internet sites searched are listed in Appendix 1; Appendix 2; Appendix 3; Appendix 4; Appendix 5; Appendix 6; Appendix 7; Appendix 8; Appendix 9; Appendix 10; Appendix 11; Appendix 12; Appendix 13.
Searching other resources
Reference checking
The reference lists of all retrieved articles were scrutinised for further references. Searches of the catalogues of relevant organisations and research founders were also undertaken.
Personal communication
Experts were contacted and were asked about their knowledge of other studies, published or unpublished, relevant to the review.
Data collection and analysis
Selection of studies
Two independent review authors inspected the search hits by reading the titles and abstracts. Each potentially relevant study located in the search was obtained as a full article and was independently assessed for inclusion by two review authors. In the case of discordance, a third independent review author arbitrated. Translation of articles not written in the English language was undertaken by a single review author.
The screening process was divided into two key phases. Phase one used the initial eight key questions reported in the original review (Perry 2006). These included the following.
Prescreening criteria: phase one
-
Is the document written in 2004 or later? [If "no," exclude document.]
-
Is the document an empirical study? [If "no," exclude document.]
-
Does the study evaluate an intervention, a component of which is designed to reduce, eliminate or prevent relapse among drug‐using offenders?
-
Are the participants referred by the criminal justice system at baseline?
-
Does the study report pre programme and post programme measures of drug use?
-
Does the study report pre programme and post programme measures of criminal behaviour?
-
Does the study include a comparison group?
-
Do the outcome measures refer to the same length of follow‐up for two groups?
After relevant papers from phase one had been identified, phase two screening was performed to identify papers reporting on pharmacological interventions. Criteria included the following.
Prescreening: phase two
-
Is the intervention a pharmacological intervention? [if "yes" include document]
Pharmacological interventions (excluding those focused only on alcohol outcomes, only on tobacco outcomes or on both) were implied if the programme was targeted at reducing drug use in a group of individuals or if their use could be ascertained from the background characteristics of the group.
Offenders included individuals residing in special hospitals, prisons or the community (i.e. under the care of the probation service) and offenders who were diverted from court or placed on arrest referral schemes for treatment.
The study setting could change throughout the process of the study. For example, offenders could begin the study in prison but then progress through a work release project into a community setting.
Finally, studies need not report both drug and criminal activity outcomes. If either one of these was reported, the study was included in the review.
Data extraction and management
Data extraction forms were used to standardise the reporting of data from all included studies as potentially relevant. Data were extracted by two independent review authors.
Assessment of risk of bias in included studies
Four independent review authors (AEP, JMG, MM‐SJ, MN) assessed risk of bias in all included studies using risk of bias assessment criteria recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
The risk of bias assessment for RCTs in this review was performed using the criteria recommended by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). The recommended approach for assessing risk of bias in studies included in a Cochrane Review involves the use of a two‐part tool that addresses six specific domains, namely, sequence generation and allocation concealment (selection bias), blinding of participants and providers (performance bias), blinding of outcome assessor (detection bias), incomplete outcome data (attrition bias), selective outcome reporting (reporting bias) and other sources of bias. The first part of the tool involves describing what was reported to have happened in the study. The second part of the tool involves assigning a judgement related to the risk of bias for that entry in terms of low, high or unclear risk. To make these judgements, we used the criteria indicated by the Cochrane Handbook for Systematic Reviews of Interventions as adapted for the addiction field.
The domains of sequence generation and allocation concealment (avoidance of selection bias) were addressed in the tool by a single entry for each study.
Blinding of participants, personnel and outcome assessor (avoidance of performance bias and detection bias) was considered separately for objective outcomes (e.g. dropping out, using substance of abuse as measured by urinalysis, relapsing of participants at the end of follow=up, engaging of participants in further treatments) and subjective outcomes (e.g. duration and severity of signs and symptoms of withdrawal, participant self‐reported use of substance, side effects, social functioning as integration at school or at work, family relationships).
Incomplete outcome data (avoidance of attrition bias) were considered for all outcomes except dropping out of treatment, which very often is the primary outcome measure in trials on addiction. See Appendix 14 for details
For studies identified in the most recent search, the review authors attempted to contact study authors to establish whether a study protocol was available.
Measures of treatment effect
For continuous outcome measures a mean difference (MD) with 95% confidence intervals (CI) was used. Higher scores for continuous measures are representative of greater harm. Dichotomous outcomes were presented as risk ratios (RRs) with 95% CIs.
Dealing with missing data
When data were missing from the original publication, review authors attempted to contact the study author via email to obtain missing data.
Assessment of heterogeneity
Heterogenity was assessed using I2 and Q statistics.
Data synthesis
The RevMan software package was used to perform a series of meta‐analyses for continuous and dichotomous outcome measures. A random‐effects model was used to account for the fact that participants did not come from a single underlying population. A narrative review were performed to address each of the key questions outlined in the objectives. The narrative tables included a presentation of study details (e.g. author, year of publication, and country of study origin), study methods (e.g. random assignment), participants (e.g. number in sample, age, gender, ethnicity, age, mental health status), interventions (e.g. description, duration, intensity, setting), outcomes (e.g. description, follow‐up period, reporting mechanism), resource and cost information and resource savings (e.g. number of staff, intervention delivery, estimated costs, estimated savings) and notes (e.g. methodological and quality assessment information). For outcomes of criminal activity, data were sufficient to allow the review authors to divide this activity into re‐arrest and re‐incarceration categories.
Subgroup analysis and investigation of heterogeneity
A subgroup analysis of setting (secure versus community) and pharmacological drug type (buprenorphine, methadone and naltrexone) was conducted.
Sensitivity analysis
When appropriate, sensitivity analyses were planned to assess the impact of studies with high risk of bias. Because of the overall high risk of bias of the included studies, this analysis was not conducted.
Results
Description of studies
Results of the search
The updated searches to March 2013 produced a total of 3885 new records. Submissions from expert authors provided a further 15 records. Assessment of titles and abstracts excluded a total of 3765 records, leaving 135 potentially relevant RCT publications. In phase two, a further 118 study comparisons were excluded, leaving 17 studies for review of pharmacological interventions for drug‐using offenders with four different comparisons. Six of the 17 trials are awaiting classification, and data from the remaining eleven trials (n = 2678 participants) are presented (Figure 1).
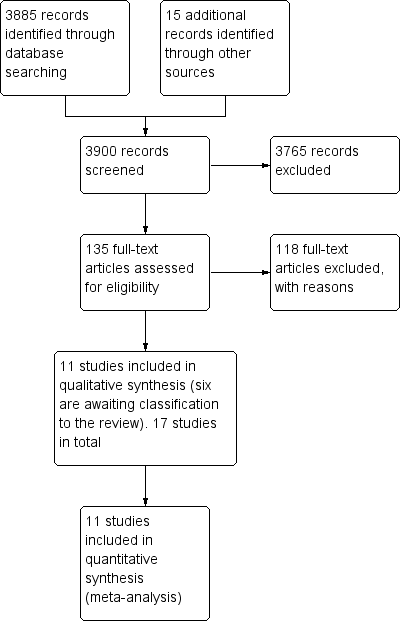
Study flow diagram of papers within the review.
Included studies
-
The fourteen publications were published between 1969 and 2011 and represented eleven trials, including 2678 participants. The eleven trials consisted of eleven singular trial publications on different interventions (Bayanzadeh, 2004; Cornish 1997; Cropsey 2011; Coviello 2010; Dolan 2003; Dole 1969; Kinlock 2005; Kinlock 2007; Lobmaier 2010; Lobmann 2007; Magura 2009). See Table 1 for a summary of study information and outcomes.
Open in table viewer
Table 1. Table 1 summary of outcomes and comparisonsStudy
Setting
Intervention
Comparison group
Follow‐up period
Outcome type
Outcome description
Prison
Methadone treatment in combination with CBT and widely focused on coping and problem‐solving skills.
Non‐methadone drugs plus standard psychiatric services and therapeutic medications
6 months
Biological drug use
Self‐report drug use
Drug use yes/no
Frequency of drug injections (percentage)
Syringe sharing
Morphine urine analysis
Community
Naltrexone
Routine parole/probation
6 months and during 6 months of treatment
Criminal activity dichotomous
% re‐incarcerated during 6 months of follow‐up
Community
Naltrexone
Psychosocial treatment only
6 months
Biological drug use dichotomous
Criminal activity dichotomous
% positive urine drug screen opioids
% positive urine drug screen cocaine
% violating parole/probation
Community
Buprenorphine
Placebo
End of treatment
3 months
Biological drug use dichotomous
Self‐report drug use dichotomous
% positive urine opiates
% self‐report injection drug use
Prison
Pharmacological (methadone)
Waiting list control
4 months
2 months
3 months
Biological drug use continuous
Biological drug use dichotomous
Self‐report drug use dichotomous
% hair positive for morphine
% self‐reported any injection
% self‐reported heroin injection
Prison
Methadone
Waiting list control.
At between 7 and 10 months
At 50 weeks
Biological drug use continuous
Biological drug use dichotomous
Self‐report drug use dichotomous
Heroin use
Re‐incarceration
Treatment retention
Employment
Prison
Counselling + methadone initiation pre‐release(a) and post‐release (b)
Counselling only
1 month
3 months
6 months
12 months
Biological drug use dichotomous
Self‐report drug use dichotomous
Criminal activity dichotomous
% positive for urine opioids
% positive for urine cocaine
% self‐reported 1 or more days heroin
n used heroin for entire 180‐day follow‐up period
Re‐incarcerated
Self‐reported criminal activity
Prison
Prison based levo alpha acetyl methanol and transfer to methadone after release
untreated controls
During 9 months
Biological drug use dichotomous
Self‐report drug use dichotomous
Criminal activity dichotomous
Heroin use
Arrest
Re incarceration
Frequency of illegal activity
Admission drug use
Average weekly income
Prison
Naltrexone
Methadone
6 months
Criminal activity continuous
Criminal activity dichotomous
Self‐report drug use continuous
Mean days of criminal activity
% re‐incarcerated
Mean days of heroin use
Mean days of benzodiazepine use
Mean days of amphetamine use
Community
Pharmacological (diamorphine)
Methadone
12 months
Criminal activity dichotomous
% self‐reported criminal activity
% police‐recorded offences
Prison
Buprenorphine
Methadone
3 months
Criminal activity dichotomous
Self‐report drug use continuous
Self‐report drug use dichotomous
% re‐incarcerated
% arrested for property crime
% arrested for drug possession
Mean days of heroin use
% any heroin/opioid use
-
A number of studies produced different comparisons and were combined appropriately according to time point of measurement (e.g. 1 month, 3 months, 6 months, 12 months) and type of outcome.
Treatment regimens and settings
-
Seven studies used methadone as the intervention or for comparison (Dole 1969; Dolan 2003; Bayanzadeh, 2004; Kinlock 2005; Kinlock 2007; Lobmann 2007;Magura 2009). Lobmann 2007 compared methadone with diamorphine and Magura 2009 compared methadone with buprenorphine. All other studies compared methadone maintenance with interventions where there was no drugs administration (waiting list or counselling alone).
-
Three studies used naltrexone in oral and implantation formats in comparison with probation or parole (Cornish 1997), psychosocial therapy (Coviello 2010) and methadone (Lobmaier 2010), and the final study compared the use of buprenorphine with a placebo (Cropsey 2011).
-
The studies were categorised by setting; four studies were conducted in the community (Cornish 1997; Lobmann 2007; Coviello 2010; Cropsey 2011) and the remainder in secure settings (Dole 1969; Dolan 2003; Bayanzadeh, 2004; Kinlock 2005; Kinlock 2007; Magura 2009; Lobmaier 2010).
-
No identified studies were conducted in a court setting.
-
Different outcome measures were presented for each study, and just under half of all studies reported four or more outcome measures (see Table 1). Criminal justice and drug outcomes were measured by all studies except four. Two studies (Cornish 1997; Coviello 2010) reported on criminal activity outcomes only, and two studies (Dolan 2003; Cropsey 2011) reported on drug use only.
Countries in which the studies were conducted
-
Seven studies were published in the US, one in Iran, one in Australia, one in Norway and another in Germany.
Duration of trials
-
Most studies (n = 7) reported outcomes of six months or less, and the longest follow‐up period was 12 months.
Participants
-
The eleven studies included adult drug‐using offenders, nine of the eleven studies used samples with a majority of men and one study used female offenders only (Cropsey 2011); in one study, gender was not reported (Lobmann 2007).
-
The average age of study participants ranged from a mean of 27 years to 40.9 years.
Excluded studies
A total of 118 study comparisons were excluded. Reasons for exclusion included lack of criminal justice involvement in referral to the intervention (29 studies). Twenty excluded studies did not report relevant drug and/or crime outcome measures at both pre intervention and postintervention periods. Eleven studies reported allocation of participants to study groups that were not strictly randomly assigned or did not contain original trial data. One study was excluded in which follow‐up periods were not equivalent across study groups (Di Nitto 2002), and another (Berman 2004) was excluded because the intervention (acupuncture) was not included for evaluation in the present review. A total of 59 study comparisons were excluded because the study population did not include a pharmacological intervention or did not consist of offenders. One study reported the protocol of a trial only (Baldus 2011). We were unable to obtain the data for one paper (Cogswell 2011).
Risk of bias in included studies
See Figure 2 and Figure 3 for further information.
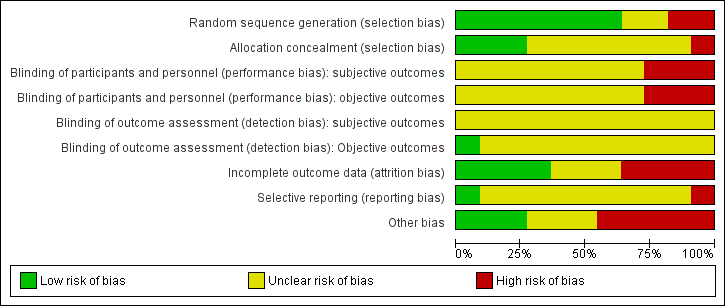
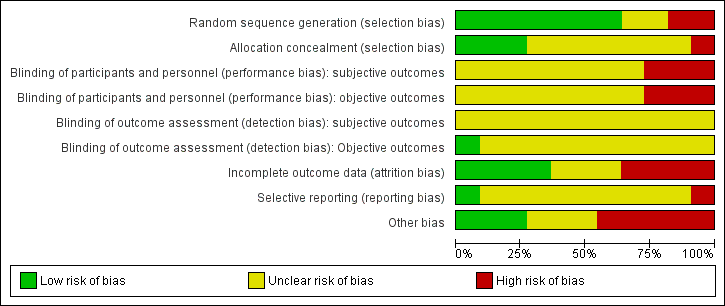
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Randomisation: All of the 11 included studies were described as randomised. In two studies, the reporting of this information was not noted as unclear, as it was difficult to find an accurate description of the methodology used. Two studies were reported at high risk of bias and six studies at low risk of bias .
Allocation concealment: Of the 11 included studies, only three reported that the allocation process was concealed and were rated at low risk of bias. One study was rated at high risk of bias. All of the remaining seven studies were rated as unclear, and the review author was not able to decide whether allocation concealment had occurred within the studies.
Blinding
Blinding was assessed across four dimensions considering performance and detection bias across subjective and objective measures see Appendix 14. Eight studies were rated as unclear risk of bias providing no information on blinding across all four domains (Bayanzadeh, 2004; Cropsey 2011; Dolan 2003; Dole 1969; Kinlock 2005; Kinlock 2007; Lobmann 2007; Magura 2009). Three studies were rated at high risk of bias for participant and personnel blinding (Cornish 1997; Coviello 2010; Lobmaier 2010). One study (Cornish 1997) was rated at low risk of outcome assessors on objective measures.
Incomplete outcome data
Four studies and four comparisons were noted at low risk of bias, four studies were noted at high risk of bias and the final three studies were rated as unclear.
Selective reporting
Unclear reporting was allocated to most of the studies within this category. Of the 11 studies, nine were rated as unclear, and one study was rated at low risk. The final study was reported at high risk of bias.
Other potential sources of bias
Threats to other bias within the study designs generally yielded mixed results. In total, five studies were rated at high risk. Low risk was noted in three further studies, and three studies were rated as unclear.
Effects of interventions
The 11 studies were included in a series of meta‐analyses. We group our studies by drug and criminal activity outcomes (re arrest and re incarceration), setting (community and secure establishment) and intervention type (buprenorphine, methadone and naltrexone). Tests for heterogeneity at the 0.01 level revealed that across all meta‐analyses, the studies were found to be homogeneous. Relative Risk (RR) was used to investigate the results of combining dichotomous outcome measures, and Mean Difference were calculated for continuous data comparisons. Higher scores on continuous measures represented greater harm.
Comparison 1 Pharmacological treatment vs no pharmacological treatment
Do pharmacological interventions for drug‐using offenders reduce drug use?
For dichotomous measure, results show an overall statistically significant reduction in drug use for objective results (biological), three studies, 300 participants: RR 0.71 (95% CI 0.52 to 0.97) and for subjective (self ‐report), three studies, 317 participants: RR 0.42 (95% CI 0.22 to 0.81). Whereas for continuous measures, self‐report drug use did not show statistically significant differences, one study, 51participants: MD ‐59.66 (95% CI ‐120.60 to 1.28), see Analysis 1.1; Analysis 1.4; and Analysis 1.5.
Does setting of intervention (community, prison/secure establishment) affect outcomes of pharmacological interventions?
In the subgroups analysis for community setting, (two studies, 99 participants: RR 0.62 (95% CI 0.35 to 1.09)) and for secure establishment settings, (one study, 201 participants: RR 0.76 (95% CI 0.52 to 1.10)), the results are no longer statistically significant, see Analysis 1.2 and Analysis 1.3.
Do pharmacological interventions for drug‐using offenders reduce criminal activity?
Analysis 1.6; and Analysis 1.7 shows the impact of dichotomous and continuous criminal activity outcome measures. The results support an overall reduction in criminal activity but favour a greater reduction in re‐incarceration, three studies, 142 participants: RR 0.36 (95% CI 0.21 to 0.60) than in re‐arrests, one study, 62 participants: RR 0.60 (95%CI 0.32 to 1.14). The impact on criminal activities was evaluated also utilizing continuous measures in one study, 51 participants: MD of ‐74.21 (95% CI ‐133.53, to 14.89) the result is statistically significant in favour of pharmacological interventions.
Does the type of pharmacological intervention (medication type) affect treatment outcomes?
Buprenorphine impact on drug use
The impact of buprenorphine vs no pharmacological treatment in reduction of self‐report drug use, was evaluated in one study, 36 participants: RR 0.58 (95% CI 0.25 to 1.35). The result is not statistically significant see Analysis 2.1
Methadone impact on drug use
The impact of methadone vs no pharmacological treatment in reduction of self‐report drug use was evaluated using dichotomous measure in one study, 253 participants: RR 0.43 (95% CI 0.33 to 0.56) and using continuous measure in one study, 51 participants: MD ‐0.52 (95% CI ‐1.09 to 0.05). The results are statistically significant in favour of methadone for dichotomous outcome see Analysis 3.1; Analysis 3.2.
Methadone impact on criminal activity
One study, 62 participants suggest that, methadone interventions do not reduce subsequent criminal activity for re‐incarceration, (RR of 1.23 (95% CI 0.53 to 2.87) see Analysis 3.3.
Naltrexone impact on criminal activity
Two studies, 114 participants focusing on the use of naltrexone vs no pharmacological treatment and subsequent criminal activity. The results indicate that naltrexone does appear to reduce subsequent re incarceration, with an RR of 0.36 (95% CI 0.19, 0.69), see Analysis 4.1.
Comparison 2. Different pharmacological treatments
Do one type of pharmacological treatment perform better than one other?
1.Methadone vs buprenorphine
Impact on drug use
One study (Magura 2009), showed a non statistically significant reduction in self report drug use for 193 participants using a dichotomous outcome RR 1.23 (95% CI 0.86‐1.76) and continuous outcomes MD 0.70 (95% CI ‐5.33 ‐ 6.73) see Analysis 5.1 and Analysis 5.2 .
Criminal activity
One study (Magura 2009) showed a non statistically significant reduction in criminal activity for 193 participants RR 1.25 (95% CI 0.83 ‐1.88) see Analysis 5.3.
2. Methadone vs diamorphine
Criminal activity
Rearrest: One study, (Lobmann 2007) 825 participants shows a non statistically significant reduction in criminal activity for re‐arrests: RR 1.25 (95% CI 1.03 to 1.51) see Analysis 6.1.
3. Methadone vs Naltrexone
Impact on drug use
One study (Lobmaier 2010) showed a non statistically significant reduction in self reported drug use continuous MD 4.60 (95% CI ‐3.54 ‐ 12.74) see Analysis 7.1.
Criminal activity
one study (Lobmaier 2010) showed a non statistically significant reduction in dichotomous re incarceration, outcomes RR 1.10 (95% CI 0.37 ‐ 3.26) and continuous outcomes MD ‐0.50 (95% CI ‐8.04 ‐ 7.04) see Analysis 7.2; Analysis 7.3.
Cost and cost‐effectiveness
The Magura study noted differences in the costs of administering buprenorphine and methadone, but were not sufficient for us to conduct a full cost effectiveness appraisal (Magura 2009). The investigators estimated that about ten times as many inmates can be served with methadone as with buprenorphine with the same staff resources. This cost implication is also endorsed in the community, where physicians have difficulty in obtaining reimbursement for buprenorphine treatment for released inmates, making the continued use of buprenorphine problematic after release.
Discussion
Summary of main results
This systematic review provides evidence from 11 trials producing several meta‐analyses. When combined, the results suggest that pharmacological interventions do reduce subsequent drug use and criminal activity (but to a lesser extent). No significant difference was found between treatment settings. We did not find any studies evaluating the impact of pharmacological interventions in court settings. Currently, we cannot comment on the effectiveness of such interventions in this setting. Findings of the effects of individual interventions on drug use and criminal activity show mixed results.
When compared to a non pharmacological intervention both buprenorphine and methadone were shown to reduce subsequent drug use. We could not determine the impact of buprenorphine on criminal activity because we did not have the relevant study data. As a result, we cannot comment on the success of this intervention in reducing criminal activity. For methadone and naltrexone the impact on criminal activity outcomes showed conflicting results: Methadone was not found to have a significant impact on reduction of re‐incarceration whereas naltrexone significantly reduced re incarceration. When comparing the drugs to one another we found no significant differences between the drug comparisons (methadone vs buprenorphine, diamorphine and naltrexone) on any of the outcome measures suggesting that one pharmacological drug does not preside over another. One study provided some cost comparisons between buprenorphine and methadone, but data were not sufficient to generate a cost‐effectiveness analysis. In conclusion, we found that pharmacological interventions do reduce subsequent drug use and criminal activity (to a lesser extent). Additionally, we found individual differences and variation on different outcome measures when pharmacological interventions were compared to a non pharmacological treatment but no significant differences when compared to another pharmacological treatment.
Buprenorphine
The Cropsey study specifically evaluated buprenorphine for opioid‐dependent women with HIV risk and found that buprenorphine given to participants in prison (followed by its use upon release into the community) was beneficial in preventing or delaying relapse to opioid use (Cropsey 2011). The findings of this study add to the growing body of evidence (which primarily includes men) suggesting that outcomes with buprenorphine are comparable with what others have found with both methadone and methadone maintenance (Lobmaier 2010). The findings however were not sustained post treatment, and most women had relapsed to active opioid treatment at the three‐month follow‐up point. Support for this conclusion is provided by the meta‐analysis suggests no long‐term significant effect. Future studies on the use of buprenorphine in women should evaluate its impact on long‐term effects with the goal of assessing its effect on opioid abstinence and prevention of associated criminal activity (Cropsey 2011). Overall, the dosage of buprenorphine varied between studies; in one study, instances of 30 mg rising to 130 mg were reported (Lobmaier 2010). A meta‐analysis of buprenorphine dose and treatment outcome found that a higher dosage (16 to 32 mg per day) predicted better retention in treatment when compared with a lower dosage (Fareed, 2012).
Methadone
The Dole study found that 3 of 12 prisoners who started using methadone before release were convicted of new crimes during an 11.5‐month follow‐up compared with 15 of 16 prisoners randomly assigned to a control condition (Dole 1969). In contrast, another study reported on opioid agonist maintenance by examining levo‐alpha‐acetylmethadol (LAAM) before prison release and found no significant differences with regard to subsequent arrest of participants who received LAAM and a control group at nine months post‐release (Kinlock 2005). Subsequent Kinlock studies involving evaluations of counselling only and counselling with transfer in comparison with counselling and methadone support the findings of Dole 1969 and Dolan 2003 suggesting that methadone programmes can provide effective opioid agonist therapy for prisoners with a history of heroin addiction (Kinlock 2007). In support of methadone treatment, the World Health Organisation has listed methadone as an essential medication and has strongly recommended that treatment should be made available in prison and supported subsequently within the community to significantly reduce the likelihood of adverse health and criminogenic consequences (Hergert 2005).
Dosage of methadone treatment varied across studies. For example, Magura 2009 reported problems with the use of sub optimal doses of methadone when higher doses were available. Investigators argue that higher doses appear to reflect participant preference because most did not intend to continue treatment after release. The Dolan study reported moderate doses of methadone (61 mg) and noted that outcomes may have improved if higher doses had been given (Dolan 2003). Significantly lower doses of methadone were noted in the Dole study, in which 10 mg of methadone per day was increased to a dosage of 35 mg per day (Dole 1969). Participants in the Kinlock 2005 study were medicated three times per week, starting at 10 mg and increasing by 5 mg every third medication day during incarceration to a target dose of 50 mg. Evidence from the Amato 2005 review suggests that low dosages of methadone maintenance lead to compromise in the effectiveness of treatment and that recommendations for dosage should be monitored at around 60 mg. Additional systematic review evidence considering the use of methadone and a tapered dose for the management of opioid withdrawal show a wide range of programmes with differing outcome measures, making the application of meta‐analysis difficult (Amato 2013). The authors conclude that slow tapering with temporary substitution of long‐acting opioids can reduce withdrawal severity; however, most participants still relapsed to heroin use (Amato 2013).
Naltrexone
For evaluation of naltrexone, two studies (one pilot: Cornish 1997) and a subsequent larger replication trial (Coviello 2010) show that use of a larger sample size consisting of a diverse group of offenders resulted in no differences in criminal behaviour between naltrexone and treatment as usual groups. The authors note that one of the major differences between the two studies remains the extent and quality of supervision provided by parole officers. The authors suggest that for treatment to be successful, use of oral naltrexone by probationers and parolees requires more supervision than is typically available within the criminal justice system. Study authors reported instances of 35 mg of naltrexone rising to 300 mg (Coviello 2010). Other research evidence related to naltrexone use and mortality rates highlights possible concerns about the high risk of death after treatment. Gibson 2007 compared mortality rates associated with naltrexone and methadone by using retrospective data analysis of coronial participants between 2000 and 2003. Findings show that participants receiving naltrexone were up to 7.4 times more likely to die after receiving treatment when compared with those using methadone over the same time period. Although this study was not conducted in a population of prisoners, it is likely that such risks are comparable; therefore generalised use of naltrexone and associated subsequent supervision of those taking naltrexone in its oral form require careful consideration.
Overall completeness and applicability of evidence
Overall, the findings of this review suggest that pharmacological interventions have an impact on reducing self‐report drug use. Individual pharmacological drugs had differing effects, particularly in relation to subsequent drug use. Promising results highlight the use of methadone within a prison environment but may be limited to shorter‐term outcomes when prisoners are released into the community. For naltrexone, the evidence is sparse and presents problems associated with different mechanisms of drug administration (e.g. oral vs implants). We can say little about the cost and cost‐effectiveness of these studies. One study reported some descriptive cost information, but the information was insufficient to generate a cost analysis Magura 2009. In conclusion, high‐quality research is required to evaluate the processes involved in the engagement of offenders mandated to substance abuse programmes to enable us to understand better why a programme works and why it does not.
Quality of the evidence
A number of limitations within each of the studies are highlighted by the authors. High dropout rates were noted in the methadone group after prison release in the Lobmaier study and appear to be more difficult to maintain in offender populations (Lobmaier 2010). Major limitations of the Coviello 2010 study included low treatment retention and low six‐month follow‐up rates. Most offenders did not return for the follow‐up evaluation because they could not be located (63%). Only two‐thirds of treated participants remained in treatment in the Dolan study (Dolan 2003). As a consequence, the study does not provide conclusive evidence regarding the efficacy of oral naltrexone in this offender sample. Attrition was also a problem in the Kinlock 2005 study; this was due in part to the fact that individuals were being transferred to other prisons or were having their sentences extended because of preexisting charges (Kinlock 2005). Similiar problems of segregation and impact of sentence releases affected the sample size in the Bayanzadeh, 2004 study. Such attrition within studies threatens the comparability of experimental and control groups, thereby ensuring that any conclusions should be taken with considerable caution. In particular, the Bayanzadeh study noted some of the practical difficulties associated with contamination between experimental and control groups, given that the ideal would be to keep the groups apart.
Sample sizes were considered modest in a number of studies, with attrition presenting difficulties in interpretation of study findings. For example, 30% attrition at follow‐up producing possible threats to the internal validity of the study design (Magura 2009) and similar small sample sizes in the Lobmaier trial may have been too small to reveal any differences between the two treatment conditions (Lobmaier 2010). Larger trials are therefore required to assess the possible advantages of one treatment over the other. The Cropsey 2011 study identified a sample of 36 women and randomly allocated 15 to the intervention and 12 to the placebo group. Investigators note that although the potency of buprenorphine for control of opioid use is clearly demonstrated, a larger sample size may be needed to detect significant differences between groups on other variables of interest. The study was limited to three months of treatment, and further studies should explore the provision of buprenorphine for longer periods of time to prolong opioid abstinence and prevent associated criminal activity. Similiar short follow‐up periods were noted in other trials, including Dolan 2003.
Potential biases in the review process
Despite limitations associated with the literature, two limitations in review methodology were achieved. Specifically, the original review included an additional five fee paying databases and one search using DrugScope. In this current review resources did not allow such extensive searching. Whislt the electronic databases searches have been updated to March 2013. the web site search has been updated to November 2011. As a result some literature may have been missed from this current review

Study flow diagram of papers within the review.
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
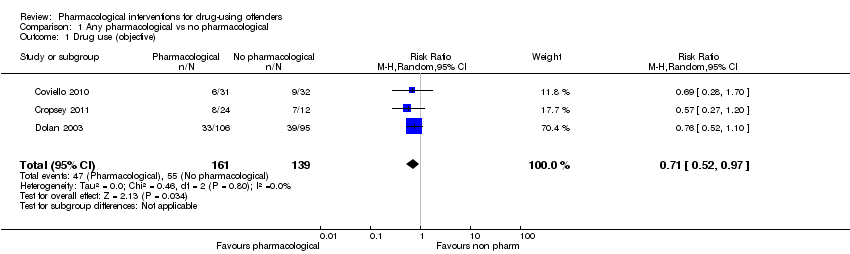
Comparison 1 Any pharmacological vs no pharmacological, Outcome 1 Drug use (objective).

Comparison 1 Any pharmacological vs no pharmacological, Outcome 2 Drug use community setting.
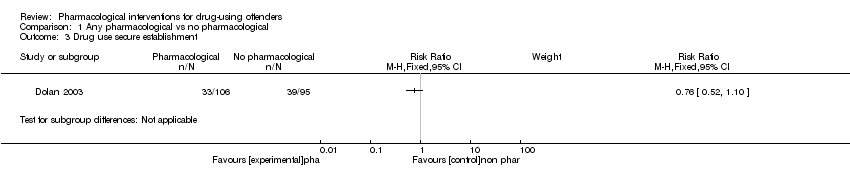
Comparison 1 Any pharmacological vs no pharmacological, Outcome 3 Drug use secure establishment.
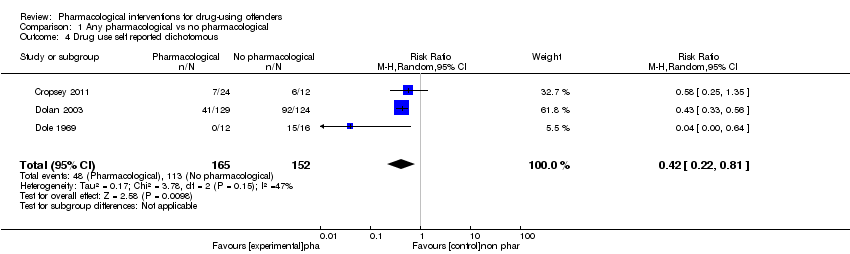
Comparison 1 Any pharmacological vs no pharmacological, Outcome 4 Drug use self reported dichotomous.
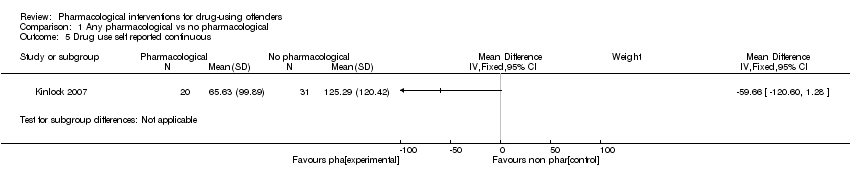
Comparison 1 Any pharmacological vs no pharmacological, Outcome 5 Drug use self reported continuous.
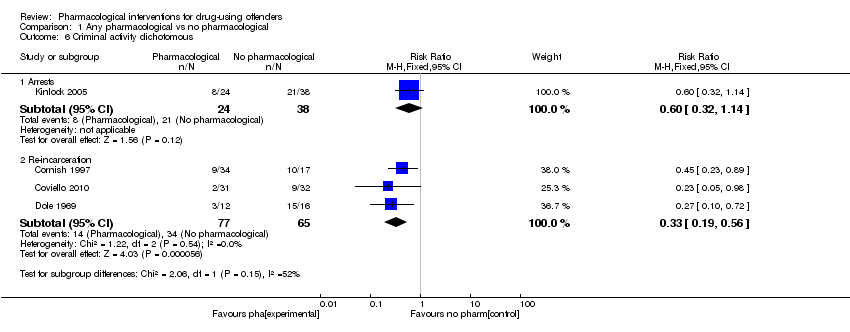
Comparison 1 Any pharmacological vs no pharmacological, Outcome 6 Criminal activity dichotomous.

Comparison 1 Any pharmacological vs no pharmacological, Outcome 7 Criminal activity continuous.

Comparison 2 Buprenorphine vs no pharmacological, Outcome 1 Self report drug use dichotomous.

Comparison 3 Methadone vs no pharmacological, Outcome 1 Self‐report drug use dichotomous.
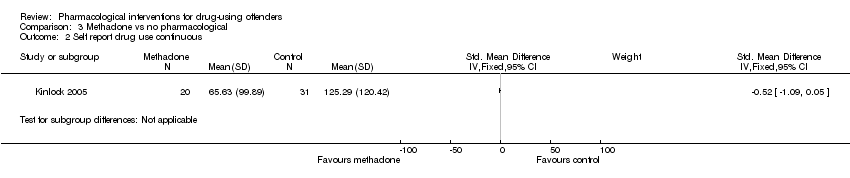
Comparison 3 Methadone vs no pharmacological, Outcome 2 Self report drug use continuous.
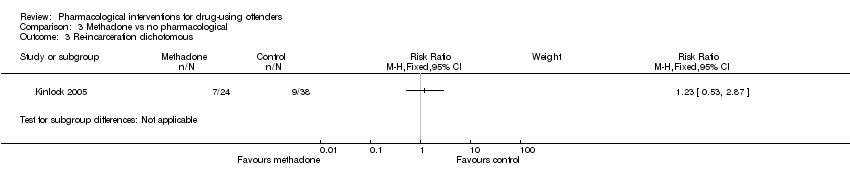
Comparison 3 Methadone vs no pharmacological, Outcome 3 Re‐incarceration dichotomous.
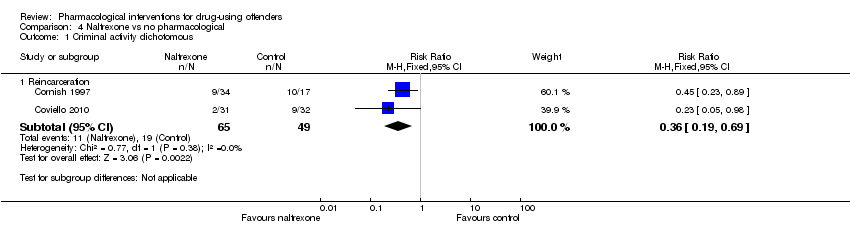
Comparison 4 Naltrexone vs no pharmacological, Outcome 1 Criminal activity dichotomous.

Comparison 5 Methadone vs buprenorphine, Outcome 1 Self reported drug use dichotomous.
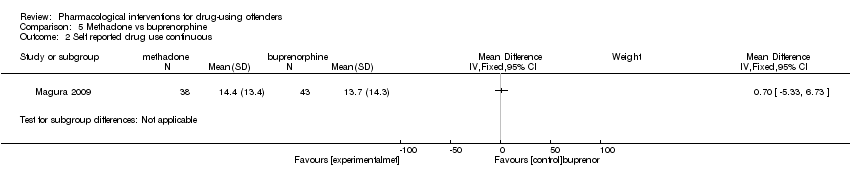
Comparison 5 Methadone vs buprenorphine, Outcome 2 Self reported drug use continuous.

Comparison 5 Methadone vs buprenorphine, Outcome 3 Criminal activity dichotomous.

Comparison 6 Methadone vs diamorphine, Outcome 1 criminal activity dichotomous.

Comparison 7 Methadone vs naltrexone, Outcome 1 self reported drug use continuous.

Comparison 7 Methadone vs naltrexone, Outcome 2 criminal activity dichotomous.

Comparison 7 Methadone vs naltrexone, Outcome 3 criminal activity continuous.
| Study | Setting | Intervention | Comparison group | Follow‐up period | Outcome type | Outcome description |
| Prison | Methadone treatment in combination with CBT and widely focused on coping and problem‐solving skills. | Non‐methadone drugs plus standard psychiatric services and therapeutic medications | 6 months | Biological drug use Self‐report drug use | Drug use yes/no Frequency of drug injections (percentage) Syringe sharing Morphine urine analysis | |
| Community | Naltrexone | Routine parole/probation | 6 months and during 6 months of treatment | Criminal activity dichotomous | % re‐incarcerated during 6 months of follow‐up | |
| Community | Naltrexone | Psychosocial treatment only | 6 months | Biological drug use dichotomous Criminal activity dichotomous | % positive urine drug screen opioids % positive urine drug screen cocaine % violating parole/probation | |
| Community | Buprenorphine | Placebo | End of treatment 3 months | Biological drug use dichotomous Self‐report drug use dichotomous | % positive urine opiates % self‐report injection drug use | |
| Prison | Pharmacological (methadone) | Waiting list control | 4 months 2 months 3 months | Biological drug use continuous Biological drug use dichotomous Self‐report drug use dichotomous | % hair positive for morphine % self‐reported any injection % self‐reported heroin injection | |
| Prison | Methadone | Waiting list control. | At between 7 and 10 months At 50 weeks | Biological drug use continuous Biological drug use dichotomous Self‐report drug use dichotomous | Heroin use Re‐incarceration Treatment retention Employment | |
|
| Prison | Counselling + methadone initiation pre‐release(a) and post‐release (b) | Counselling only | 1 month 3 months 6 months 12 months | Biological drug use dichotomous Self‐report drug use dichotomous Criminal activity dichotomous | % positive for urine opioids % positive for urine cocaine % self‐reported 1 or more days heroin n used heroin for entire 180‐day follow‐up period Re‐incarcerated Self‐reported criminal activity |
| Prison | Prison based levo alpha acetyl methanol and transfer to methadone after release | untreated controls | During 9 months | Biological drug use dichotomous Self‐report drug use dichotomous Criminal activity dichotomous | Heroin use Arrest Re incarceration Frequency of illegal activity Admission drug use Average weekly income | |
| Prison | Naltrexone | Methadone | 6 months | Criminal activity continuous Criminal activity dichotomous Self‐report drug use continuous | Mean days of criminal activity % re‐incarcerated Mean days of heroin use Mean days of benzodiazepine use Mean days of amphetamine use | |
| Community | Pharmacological (diamorphine) | Methadone | 12 months | Criminal activity dichotomous | % self‐reported criminal activity % police‐recorded offences | |
| Prison | Buprenorphine | Methadone | 3 months | Criminal activity dichotomous Self‐report drug use continuous Self‐report drug use dichotomous | % re‐incarcerated % arrested for property crime % arrested for drug possession Mean days of heroin use % any heroin/opioid use |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Drug use (objective) Show forest plot | 3 | 300 | Risk Ratio (M‐H, Random, 95% CI) | 0.71 [0.52, 0.97] |
| 2 Drug use community setting Show forest plot | 2 | 99 | Risk Ratio (M‐H, Random, 95% CI) | 0.62 [0.35, 1.09] |
| 3 Drug use secure establishment Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4 Drug use self reported dichotomous Show forest plot | 3 | 317 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.22, 0.81] |
| 5 Drug use self reported continuous Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 6 Criminal activity dichotomous Show forest plot | 4 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 6.1 Arrests | 1 | 62 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.60 [0.32, 1.14] |
| 6.2 Re‐incarceration | 3 | 142 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.19, 0.56] |
| 7 Criminal activity continuous Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Self report drug use dichotomous Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Self‐report drug use dichotomous Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2 Self report drug use continuous Show forest plot | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 3 Re‐incarceration dichotomous Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Criminal activity dichotomous Show forest plot | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 Reincarceration | 2 | 114 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.36 [0.19, 0.69] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Self reported drug use dichotomous Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2 Self reported drug use continuous Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 3 Criminal activity dichotomous Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 re incarceration | 1 | 116 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.25 [0.83, 1.88] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 criminal activity dichotomous Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 arrest | 1 | 825 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.25 [1.03, 1.51] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 self reported drug use continuous Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 2 criminal activity dichotomous Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 re incarceration | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.37, 3.26] |
| 3 criminal activity continuous Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |