Traitement hormonal substitutif après une chirurgie pour un cancer épithélial des ovaires
Résumé scientifique
Contexte
Les femmes ayant subi un traitement chirurgical pour un cancer épithélial de l'ovaire (CEO) peuvent développer des symptômes de ménopause, en raison de la perte immédiate de la fonction ovarienne suite à la chirurgie et la chimiothérapie. Les femmes peuvent présenter des symptômes vasomoteurs, des troubles du sommeil, des difficultés de concentration, des dysfonctionnements sexuels, des symptômes vaginaux et une accélération de l'ostéoporose. Bien que le traitement hormonal substitutif (THS) soit le traitement le plus efficace pour soulager ces symptômes, son innocuité a été mise en doute pour les femmes atteintes d’un CEO.
Objectifs
Évaluer l’innocuité et l'efficacité du THS pour les symptômes de la ménopause chez les femmes traitées chirurgicalement pour un CEO.
Stratégie de recherche documentaire
Nous avons effectué des recherches dans le Cochrane Central Register of Controlled Trials (CENTRAL ; 2019, numéro 6), MEDLINE via Ovid (1946 au 12 juin 2019) et Embase via Ovid (1980 à 2019, semaine 23). Nous avons également effectué des recherches dans des rapports de conférence et des registres d’essais. Il n'y avait aucune restriction concernant la langue.
Critères de sélection
Nous avons inclus des essais contrôlés randomisés (ECR) avec des participantes de tout âge et de tout statut ménopausique, ayant subi une intervention chirurgicale pour un CEO et, après diagnostic et traitement, ayant utilisé n'importe quel régime de THS pendant n’importe quelle durée, par rapport à un placebo ou à l'absence d'hormonothérapie. Nous avons également inclus des essais comparant différents régimes ou durées d'administration du THS.
Recueil et analyse des données
Deux auteurs de la revue ont indépendamment identifié les études répondant aux critères d'inclusion. Ils ont utilisé Covidence pour extraire les caractéristiques des études, les données sur les critères de jugement et pour évaluer la qualité méthodologique des études incluses.
Résultats principaux
Notre stratégie de recherche a permis d'identifier 2617 titres, desquels 2614 titres ont été exclus. Trois études, impliquant 350 femmes, ont répondu à nos critères d'inclusion. Deux de ces études portaient sur des femmes pré‐ et post‐ménopausées, et la troisième ne portait que sur des femmes pré‐ménopausées. La tranche d'âge globale des femmes incluses dans les études allait de 20 à 89,6 ans, avec un suivi médian allant de 31,4 mois à 19,1 ans. La répartition géographique des participants comprenait l'Europe, l'Afrique du Sud et la Chine. Tous les stades et sous‐types histologiques ont été inclus dans deux des études, mais le stade IV de la maladie a été exclu dans la troisième. Les trois études incluses ont utilisé une variété de régimes de THS (oestrogènes conjugués avec ou sans médroxyprogestérone et avec ou sans nylestriol) et de méthodes d'administration de THS (voie orale, patch et implant), Dans toutes les études, les comparaisons ont été faites par rapport à des femmes n’ayant pas reçu de THS.
Les études présentaient un risque faible ou peu clair de biais de sélection et de déclaration, et un risque élevé de biais de performance, de détection et d'attrition. La certitude des données probantes était faible pour la survie globale et la survie sans progression, et très faible pour l'évaluation de la qualité de vie, l'incidence du cancer du sein, l'accident ischémique transitoire (AIT), l'accident vasculaire cérébral (AVC) et l'infarctus du myocarde (IM).
La méta‐analyse de ces études a montré que le THS pourrait améliorer la survie globale (hazard ratio (HR) 0,71, intervalle de confiance (IC) à 95% 0,54 à 0,93 ; 350 participants, 3 études ; données probantes de faible certitude). L'évaluation de la qualité de vie à l'aide du questionnaire EORTC‐C30 n'a été réalisée que dans une seule étude. Nous ne savons pas si le THS améliore ou réduit la qualité de vie, la certitude des données probantes ayant été évaluée comme très faible (différence moyenne (DM) 13,67 points de plus, IC à 95 % 9,26 de plus à 18,08 de plus ; 1 étude ; 75 participants ; données probantes de très faible certitude). De même, le THS pourrait ne faire que peu ou pas de différence dans la survie sans progression (HR 0,76, IC à 95 % 0,57 à 1,01 ; 275 participants, 2 études ; données probantes de faible certitude).
Nous ne savons pas si le THS améliore ou réduit l'incidence du cancer du sein (rapport de risque (RR) 2,00, IC à 95 % 0,19 à 21,59 ; 225 participants, 2 études ; données probantes de très faible certitude) ; de l’AIT (RR 5,00, IC à 95 % 0,24 à 102.42 ; 150 participants, 1 étude ; données probantes de très faible certitude) ; de l’AVC (RR 0,67, IC à 95% 0,11 à 3,88 ; 150 participants, 1 étude ; données probantes de très faible certitude) ; et de l’IM (RR 0,20, IC à 95% 0,01 à 4,10 ; 150 participants, 1 étude ; données probantes de très faible certitude). L'incidence des calculs biliaires n'a pas été rapportée dans les études incluses.
Conclusions des auteurs
Le traitement hormonal substitutif pourrait légèrement améliorer la survie globale chez les femmes ayant subi un traitement chirurgical de CEO, mais la certitude des données probantes est faible. Le THS pourrait ne faire que peu ou pas de différence dans la qualité de vie, l'incidence du cancer du sein, de l'AIT, de l’ASC et de l'IM, la certitude des données probantes ayant été jugée très faible. L'utilisation du THS pourrait n’avoir que peu ou pas d'effet sur la survie sans progression. Les données probantes dans cette revue sont limitées par l'imprécision et le caractère incomplet des critères de jugement pertinents rapportés, et les résultats doivent donc être interprétés avec prudence. De futurs ECR bien conçus sont nécessaires car il s'agit d'un domaine important pour les femmes présentant des symptômes de ménopause après un traitement chirurgical pour un cancer des ovaires, d'autant plus que les médecins sont souvent réticents à prescrire un THS dans ce scénario. Les données probantes de cette revue sont trop limitées pour soutenir ou réfuter le fait que le THS soit très nocif pour cette population.
PICOs
Résumé simplifié
Traitement hormonal substitutif pour les symptômes de la ménopause chez des femmes ayant subi un traitement chirurgical pour un cancer épithélial des ovaires
Problématique
Le cancer épithélial de l'ovaire (CEO) se développe à partir de la couche superficielle de l'ovaire. Il s'agit du huitième cancer le plus fréquent et de la septième cause de décès par cancer chez les femmes dans le monde. Le traitement chirurgical des CEO comprend l'ablation de tous les dépôts tumoraux visibles dans l'abdomen ; cela inclut généralement les ovaires, l'utérus, l'épiploon (rideau de graisse qui pend de l'estomac et du côlon transverse) et le péritoine, avec ou sans ablation des ganglions lymphatiques ou d'autres organes. Les femmes qui étaient pré‐ménopausées avant l'intervention subissent ensuite la ménopause à la suite de l'opération. Leur qualité de vie peut s'en trouver affectée en raison de symptômes tels que les bouffées de chaleur, les sautes d'humeur, les changements de l’activité sexuelle, la sécheresse vaginale et la perte de densité osseuse. Environ un quart des femmes, en particulier les femmes jeunes, présenteront une maladie à un stade précoce et subiront les effets néfastes à long terme d'une ménopause provoquée par une intervention chirurgicale. Chez les femmes dont la maladie est avancée au moment du diagnostic, la qualité de vie est un facteur important à prendre en compte, leur maladie limitant leur espérance de vie.
Le traitement hormonal substitutif (THS) pourrait être efficace pour les symptômes de la ménopause, mais l’innocuité de ce traitement suscite de sérieuses inquiétudes. Ces préoccupations ne sont pas seulement liées au cancer, mais aussi au cœur, et doivent être mises en balance avec les effets positifs sur la santé du THS, pour les femmes en ménopause précoce. Ces dernières années, l’innocuité des THS a été remise en question et il se peut que les médecins se montrent prudents envers la prescription de THS aux femmes connaissant une ménopause d'origine chirurgicale après un traitement de CEO.
Objectif de la revue
Évaluer l’innocuité et l'efficacité du traitement hormonal substitutif (THS) pour les symptômes de la ménopause chez les femmes traitées chirurgicalement pour un CEO.
Quels sont les principaux résultats ?
Nous avons cherché des données probantes sur les avantages et des inconvénients du THS chez les patientes atteintes de CEO, jusqu'en juin 2019. Nous avons identifié trois études impliquant un total de 350 femmes. Nous avons constaté que le THS pourrait améliorer la survie globale et pourraient ne faire que peu ou pas de différence dans la survie sans progression. Nous ne sommes pas sûrs des effets sur la qualité de vie, l'incidence du cancer du sein, l'accident ischémique transitoire (également connu sous le nom de "mini accident vasculaire cérébral"), l'accident vasculaire cérébral (AVC) et l'infarctus du myocarde (crise cardiaque), la certitude des données probantes étant très faible. Il n'y a pas eu de rapports sur l'incidence des calculs biliaires.
Valeur probante des données
La certitude des données probantes était faible à très faible pour tous les critères de jugement, principalement en raison du petit nombre de participants et du faible nombre d'événements indésirables rapportés. La certitude des données probantes est également limitée en raison du risque élevé de biais des études incluses, ce qui signifie que leurs résultats pourraient surestimer ou sous‐estimer l'effet réel du traitement.
Quelles étaient les conclusions ?
Le traitement hormonal substitutif pourrait améliorer la survie globale des femmes connaissant une ménopause chirurgicale après un traitement pour un CEO, mais il pourrait ne faire que peu ou pas de différence dans la survie sans progression. La certitude globale de ces résultats est faible à très faible, principalement en raison d'un manque d'informations. Il s'agit d'un domaine de recherche très important, qui pourrait avoir un impact important sur de nombreuses femmes.
Authors' conclusions
Summary of findings
| Hormone replacement therapy (HRT) compared to no HRT for epithelial ovarian cancer (EOC) | ||||||
| Patients: women of any age diagnosed with any stage of EOC who had surgical treatment, regardless of chemotherapy treatment | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
| Risk with no HRT | Risk with HRT | |||||
| Overall survival | Study population | HR 0.71 | 350 | ⊕⊕⊝⊝ | The median follow‐up time in the three included studies was 31.4 months, 90 months and 19.1 years. | |
| 795 per 1,000 | 675 per 1,000 | |||||
| Quality of life, general condition | The mean quality of life (general condition) in the no HRT group was 13.84 points. | The mean quality of life (general condition) in the HRT group was 13.67 points higher | ‐ | 75 | ⊕⊝⊝⊝ | The EORTC‐C30 questionnaire was used to evaluate this outcome; higher values correspond with improvement. |
| Progression‐free survival | Study population | HR 0.76 | 275 | ⊕⊕⊝⊝ | The median follow‐up time in the two studies was 90 months and 19.1 years. | |
| 773 per 1,000 | 676 per 1,000 | |||||
| Incidence of breast cancer | Study population | RR 2.00 | 225 | ⊕⊝⊝⊝ | The median follow‐up time in the two studies was 31.41 months and 19.1 years. | |
| 8 per 1,000 | 17 per 1,000 | |||||
| Incidence of transient ischaemic attack | Study population | RR 5.00 | 150 | ⊕⊝⊝⊝ | The median follow‐up time in the study was 19.1 years. | |
| 7 per 1,000 | 33 per 1,000 | |||||
| Incidence of cerebrovascular accident | Study population | RR 0.67 | 150 | ⊕⊝⊝⊝ | The median follow‐up time in the study was 19.1 years. | |
| 40 per 1,000 | 27 per 1,000 | |||||
| Incidence of myocardial infarction | Study population | RR 0.20 | 150 | ⊕⊝⊝⊝ | The median follow‐up time in the study was 19.1 years. | |
| 27 per 1,000 | 5 per 1,000 | |||||
| Incidence of gallstones | ‐ | ‐ | ‐ | ‐ | ‐ | The incidence of gallstones was not reported in the included studies. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded by one level due to limitations in study design | ||||||
Background
Description of the condition
One in 70 women will develop ovarian cancer (Fleming 2013) and its age‐standardized incidence rate (ASR) is 6.6 per 100,000 women (GLOBOCAN 2018). This is lower in Western Africa and higher in Northern Europe, varying from 3 to 13 per 100,000) (Fleming 2013). One in 100 women will die of the disease (Fleming 2013) and the ASR of mortality is 3.9 per 100,000 (GLOBOCAN 2018). The median age at diagnosis of epithelial ovarian cancer (EOC) is 60 years (Michaelson‐Cohen 2009). However, 40% of women affected are 30 to 60 years old and 3% to 17% are less than 40 years old (Ibeanu 2011; Michaelson‐Cohen 2009; Wen 2013). The majority of women with EOC (60% to 75%) have advanced stage disease at presentation and the overall five‐year survival for all stages is 45% (Ibeanu 2011; Singh 2010).
Debulking (removal) of any visible tumour (also known as cytoreductive surgery) is standard surgery for disease staging and treatment; it includes hysterectomy, bilateral salpingo‐oophorectomy and omentectomy with or without pelvic and para‐aortic lymphadenectomy (i.e. the removal of all visible lesions in the abdomen and pelvic cavity including the ovaries, uterus (womb) and omentum (fatty curtain that hangs from the stomach/transverse colon), with or without lymph nodes) (Fleming 2013). In young women with early‐stage disease or disease present in only in one ovary, fertility‐sparing surgery (where only the affected ovary is removed) may be appropriate. Removal of the remaining ovary is recommended once the woman has completed her family. Bilateral oophorectomy (the surgical removal of both ovaries), and the consequent the loss of ovarian function in premenopausal women, induces an immediate surgical menopause and may result in a range of symptoms including vasomotor symptoms, sleep depravation, difficulty with concentration, sexual dysfunction, vaginal symptoms and accelerated osteoporosis (Biliatis 2012; Hopkins 2004). Symptoms following a surgical menopause in younger women may be more intense than in the natural menopause because of sudden onset (Li 2012; Singh 2010; Wen 2013).
Studies have demonstrated that the origin of many high‐grade (HG) serous EOCs (and primary peritoneal cancer), the most common histological sub‐type of EOC, may be the fimbrial end of the fallopian tube (Leeper 2002). In this review, we use the terms 'EOC' and 'ovarian cancer' as umbrella terms to include primary peritoneal and fallopian tube HG serous cancers.
Description of the intervention
Hormone replacement therapy is the delivery of hormones, usually oestrogen with or without progesterone, to replace the normal ovarian production of hormones either due to ovarian failure (chemotherapy‐induced menopause) or after surgical removal of both ovaries (surgically induced menopause). HRT can be administrated in a variety of formulations and doses. It can be taken orally, vaginally, intranasally, as an implant, skin patch, cream or gel. The administration of HRT can be continuous (every day), sequential (for part of each month) or less frequently (Marjoribanks 2012). HRT can relieve menopausal symptoms and prevent heart disease and osteoporosis (Ibeanu 2011). However, HRT may have an effect on blood lipids levels and cause headaches, bloationg and breast tenderness (Marjoribanks 2012).
For women with a uterus, progesterone is required to prevent endometrial hyperplasia and malignancy. Women without a uterus can be given oestrogen‐only HRT. Combined continuous HRT — consisting of an oestrogen and a progestogen, taken daily without a break — can increase the risk of coronary events, venous thromboembolism, stroke, breast cancer, gallstones and death from lung cancer (Marjoribanks 2012). However, oestrogen‐only HRT following hysterectomy has not been shown to increase the incidence of breast cancer (Chlebowski 2015; Marjoribanks 2012).
How the intervention might work
Hormone replacement therapy (HRT) is a very effective treatment for the management of menopausal symptoms and the prevention of heart disease and osteoporosis (Ibeanu 2011). However, the effect of hormones is also dependent on the availability of oestrogen and progesterone receptors. Oestrogen and progesterone are mainly included in the regimen given to women experiencing menopausal symptoms. Oestrogens have an important role in reproductive development, bone homeostasis, cardiovascular remodelling and brain function (Hua 2018). Oestrogen has a role in cancer through binding with two types of oestrogen receptors (ER), namely ERα (an oncogene) and ERβ (a tumour suppressor gene which can be expressed in 40% to 60% of ovarian tumours) (Hua 2018). However, a meta‐analysis did not show any prognostic effect of ER levels on survival in women with ovarian cancer (Zhao 2013). It has been shown that progesterone and progesterone receptors (PRs) interact with oestrogen in order to promote a proliferative and pro‐survival response in breast cells. Conversley, progesterone inhibits the oestrogen‐driven growth in the uterus and ovary and protects the ovary from neoplastic transformation (Diep 2015); it has also been shown to have a significant association with survival (Luo 2017; Zhao 2013). BRCA1 and BRCA2 are oncosuppressor genes which, when mutated, increase the lifetime risk of developing breast cancer to between 45% and 80% and ovarian and fallopian tubal cancers to between 15% and 56%. This compares with a general population lifetime risk of developing ovarian cancer of 2% to 3% (Marchetti 2013), although those with BRCA germline mutations have a significantly improved overall survival compared to non‐BRCA mutation carriers (Zhong 2015). However, women with breast cancer who are BRCA1 (but not BRCA2) mutation carriers have significantly poorer survival (Zhong 2015).
Hormone replacement therapy has been associated with angiogenesis (Hopkins 2004) that may stimulate residual ovarian cancer cells of either microscopic or visible disease in women treated for EOC or induce new hormone‐dependent diseases, such as breast cancer (Hopkins 2004; Singh 2010). For these reasons, clinicians may be cautious in prescribing HRT for menopausal symptoms in women after surgery for EOC. Benefits in quality of life for each individual therefore have to be weighed against any theoretical risks. However, the prognosis of early‐stage EOC is good, with a low incidence of recurrence and mortality (less than 10% of women with recurrent disease in stage I EOC) (Lowe 2013) and prolonged survival. Due to these reasons, the risks of premature menopause, including osteoporosis, cardiovascular disease, venous thromboembolic disease and stroke, may outweigh the risk of HRT use. Advanced stage EOC has a poor prognosis with a higher incidence of recurrence and mortality (rate greater than 90% for stage IV) (Lowe 2013) and five‐year overall survival of less than 25% to 30% (Biglia 2015; Ibeanu 2011). Quality‐of‐life outcomes are therefore important for both those with early‐ and late‐stage disease.
Hormone replacement therapy can relieve menopausal symptoms among women with early‐stage ovarian cancer and improve the quality of life of those with advanced‐stage disease (Ursic‐Vrscaj 2001). Three retrospective studies have shown that HRT use was not associated with an increase in overall survival and tumour recurrence or a trend to decreased mortality (Eeles 1991; Ursic‐Vrscaj 2001; Wen 2013). In one study, women with serous type ovarian cancer who received HRT achieved better overall survival (Mascarenhas 2006). In addition, two small randomized controlled trials (RCTs) showed no adverse effects of HRT on survival (Guidozzi 1999; Li 2012). Conversely, studies of HRT use in women with no type of cancer have shown an increased risk of developing ovarian cancer (Zhou 2008). Therefore, the effectiveness of HRT on overall survival of women with ovarian cancer remains unclear.
Why it is important to do this review
In recent years the safety of HRT has been questioned. This has led to fewer women taking HRT, with the consequence that more women experience menopausal symptoms and the long‐term effects of menopause. Premenopausal women affected by ovarian cancer who have both ovaries removed experience an acute surgically or chemotherapy‐induced menopause, which can lead to more prominent menopausal symptoms. Disease‐specific survival is better for younger women compared to older women (age at diagnosis 30 years or younger, versus 30 to 60 years and 60 years or older) (Fleming 2013). Therefore a younger population of women are longer‐term survivors of EOC and are more likely to experience an early and possibly more symptomatic menopause (Li 2012; Singh 2010; Wen 2013).
Hormone replacement therapy may be helpful for treatment of menopausal symptoms, but a meta‐analysis of cohort and case‐control studies showed increase risk of developing ovarian cancer in women not previously diagnosed with ovarian cancer who were on HRT for more than 10 years (Zhou 2008). There have been three systematic reviews looking into the use of HRT in ovarian cancer after surgery (Hopkins 2004; Li 2015; Pergialiotis 2015). The first systematic review included one RCT (Guidozzi 1999) and two observational studies (Eeles 1991; Ursic‐Vrscaj 2001) and suggested that HRT was acceptable as supportive and symptomatic therapy and did not affect overall survival and disease‐free survival (Hopkins 2004). The second and third systematic reviews (in which the last search was conducted in March 2015) included four cohort studies (Eeles 1991; Mascarenhas 2006; Ursic‐Vrscaj 2001; Wen 2013) and two RCTs (Guidozzi 1999; Li 2012), and showed a favourable impact of HRT on overall survival, without increasing the risk of recurrence (Li 2015; Pergialiotis 2015).
The aim of this Cochrane review is to investigate the safety of HRT in women experiencing surgically induced menopause, both from the oncological perspective (recurrence and survival) and also in terms of quality of life. We hope that this review will facilitate counselling and informed decision making by women who seek advice and management following their cancer treatment and early and acute menopause. Currently, there is no clear evidence and opinions are conflicting.
Objectives
To assess the safety and efficacy of hormone replacement therapy (HRT) for menopausal symptoms in women surgically treated for epithelial ovarian cancer (EOC).
Methods
Criteria for considering studies for this review
Types of studies
We included randomized controlled trials (RCTs) (excluding cluster‐randomized or cross‐over trials) comparing HRT of any regimen and duration of administration versus placebo or no hormone therapy, or trials comparing different regimens or duration of administration of HRT.
Types of participants
We included women of any age who were diagnosed with any stage of EOC and had surgical treatment, regardless of chemotherapy treatment.
Types of interventions
We included studies of HRT used after treatment for EOC. We did not study the aetiological effect of HRT used before diagnosis. We included any HRT (oestrogen alone or combined with progestin, oestrogen agonist/antagonist, progestin, or testosterone, and tibolone), of any regimen or duration of administration, compared with placebo or no hormone therapy. Due to pharmacokinetic differences between different regimens and durations of administration, we investigated the following three comparisons.
-
HRT versus placebo or no HRT
-
Different regimens of HRT
-
Different durations of HRT administration
Types of outcome measures
Primary outcomes
-
Overall survival: survival until death from all causes; survival was assessed from time of enrolment in the study.
-
Quality of life: defined as an individual's perception of life in the context of the culture and value systems (which also includes specific menopausal symptoms like hot flushes, night sweats, vaginal dryness, etc.) measured by any validated scale or questionnaire for quality of life.
Secondary outcomes
-
Progression‐free survival: survival until progression of disease. Survival was assessed from the time of enrolment in the study.
-
Adverse events
-
Incidence of breast cancer
-
Thromboembolic events (pulmonary embolism (PE), deep vein thrombosis (DVT), coronary event, myocardial infarction (MI), stroke, transient ischaemic accident (TIA), cerebrovascular accident (CVA)
-
Gallstones
-
Search methods for identification of studies
In consultation with the Cochrane Gynaecological, Neuro‐oncology and Orphan Cancers Information Specialists, we searched for papers published in any language. When necessary, papers would have been translated.
Electronic searches
We searched the following electronic databases on 12 June 2019:
-
the Cochrane Central Register of Controlled Trials (CENTRAL; 2019, Issue 6), in the Cochrane library (Appendix 1)
-
MEDLINE via Ovid (1946 to 12 June 2019) (Appendix 2)
-
Embase via Ovid (1980 to 2019 week 23) (Appendix 3)
Searching other resources
All relevant articles were identified on PubMed and using the 'related articles' feature; a further search was carried out for newly published articles. We searched the following registries for ongoing trials.
-
Metaregister (www.controlled‐trials.com/rct)
-
Physicians Data Query (www.cancer.gov/publications/pdq)
-
World Health Organization International Clinical Trials Registry Platform (WHO ICTRP) (www.who.int/ictrp/en/)
-
ClinicalTrails.gov (www.clinicaltrials.gov)
-
National Cancer Institute (www.cancer.gov/about‐cancer/treatment/clinical‐trials)
If we had identified any ongoing trials that had not been published, we would have approached the principal investigators and major co‐operative groups active in this area, to ask for relevant data.
We handsearched the citation lists of included studies, key textbooks, and previous systematic reviews, and contacted experts in the field to identify further reports of trials. We also handsearched conferences abstracts from the following sources.
-
Gynecologic Oncology (Annual Meeting of the American Society of Gynecologic Oncology)
-
International Journal of Gynecological Cancer (Annual Meeting of the International Gynecologic Cancer Society)
-
British Gynaecological Cancer Society (BGCS)
-
Annual Meeting of European Society of Gynaecological Oncology (ESGO)
Data collection and analysis
Selection of studies
We downloaded all titles and abstracts retrieved by electronic searching to a reference management database (Endnote). After duplicates were removed, we transferred these data to Covidence for study selection. Two review authors (NS and RB) examined the remaining references independently. We excluded those studies which clearly did not meet the inclusion criteria. We obtained copies of the full text of potentially relevant references. Two review authors (NS and RB) independently assessed the eligibility of the retrieved reports/publications. We resolved any disagreement through discussion and we consulted a third person (TL) for a final decision. We identified and excluded duplicates and collated multiple reports of the same study so that each study rather than each report was the unit of interest in the review. We recorded the selection process in sufficient detail to complete a PRISMA flow diagram and 'Characteristics of excluded studies' table (Liberati 2009).
Data extraction and management
Two review authors (NS and KP) independently extracted study characteristics and outcome data from included studies to a piloted data collection form, using Covidence. We noted in the Characteristics of included studies table if outcome data were not reported in a usable way. We resolved disagreements by consensus or by involving a third person (RB). One review author (NS) transferred data into the Review Manager 5 (RevMan 2014) file. We double‐checked that data were entered correctly by comparing the data presented in the systematic review with the study reports. A second review author (KP) spot‐checked study characteristics for accuracy against the trial report.
For included studies, we extracted the following details.
-
Author, year of publication and journal citation (including language)
-
Country
-
Setting
-
Inclusion and exclusion criteria
-
Study design, methodology
-
Study population
-
Total number enrolled
-
Participant characteristics: age, menopausal status at diagnosis, performance status
-
Treatment: type of surgery and chemotherapy
-
Tumour stage, grade and types
-
-
Intervention details
-
All types of HRT: oestrogen alone or combined with progestin, oestrogen agonist/antagonist, progestin, or testosterone, and tibolone
-
Duration of administration of HRT in years
-
Route and doses of HRT
-
-
Comparison
-
Placebo or no treatment
-
-
Risk of bias in study (see Assessment of risk of bias in included studies)
-
Duration of follow‐up
-
Outcomes: for each outcome, we extracted the outcome definition. For adjusted estimates, we recorded variables adjusted for in analyses.
-
Results: we extracted the number of participants allocated to each intervention group, the total number analyzed for each outcome and number of dropouts, including reason for leaving the study.
-
Notes: funding for trial and notable conflicts of interest of trial authors.
Outcome data were extracted as follows.
-
For time‐to‐event data (survival and disease progression), we extracted the log of the hazard ratio (log(HR)) and its standard error from trial reports. For those studies that they did not report the HR, we attempted to estimate HR, the observed minus expected events (O‐E) and the variance (V) using formula according to Tierney 2007.
-
For dichotomous outcomes (e.g. adverse events or deaths) we extracted the number of participants in each treatment arm who experienced the outcome of interest and the number of participants assessed at endpoint, in order to estimate a risk ratio.
-
For continuous outcomes (e.g. quality‐of‐life measures), we extracted the final value and standard deviation of the outcome of interest and the number of participants assessed at endpoint in each treatment arm at the end of follow‐up, in order to estimate the mean difference between treatment arms and its standard error.
Where possible, all data extracted would be those relevant to an intention‐to‐treat analysis, in which participants would be analyzed in groups to which they were assigned. We noted the time points at which outcomes were collected and reported.
Assessment of risk of bias in included studies
Two review authors (NS and KP) applied the Cochrane 'Risk of bias' tool independently and resolved differences by discussion or by appeal to a third review author (EM). We judged each item as being at high, low or unclear risk of bias, as set out in the criteria provided by Higgins 2011 (and shown below), and provided a quote from the study report and/or a statement as justification for the judgement for each item in the 'Risk of bias' table. We summarized results in both a 'Risk of bias' graph and a 'Risk of bias' summary. When interpreting treatment effects and meta‐analyses, we took into account the risk of bias for the studies that contributed to that outcome. Where information on risk of bias related to unpublished data or correspondence with a trialist, we noted this in the 'Risk of bias' table.
-
Random sequence generation
-
Low risk of bias: e.g. participants were assigned to treatments on basis of a computer‐generated random sequence or a table of random numbers
-
High risk of bias: e.g. participants were assigned to treatments on basis of date of birth, clinic ID number or surname, or there was no attempt to randomize participants
-
Unclear risk of bias: e.g. sequence generation not reported or the information was not available
-
-
Allocation concealment
-
Low risk of bias: e.g. where the allocation sequence could not be foretold
-
High risk of bias: e.g. the allocation sequence could be foretold by participants, investigators or treatment providers
-
Unclear risk of bias: e.g. allocation concealment was not reported
-
-
Blinding of participants and personnel
-
Low risk of bias if participants and personnel were adequately blinded
-
High risk of bias if participants were not blinded to the intervention that the participant received
-
Unclear risk of bias if this was not reported or unclear
-
-
Blinding of outcomes assessors
-
Low risk of bias if outcome assessors were adequately blinded
-
High risk of bias if outcome assessors were not blinded to the intervention that the participant received
-
Unclear risk of bias if this was not reported or unclear
-
-
Incomplete outcome data: we recorded the proportion of participants whose outcomes were not reported at the end of the study. We coded a satisfactory level of loss to follow‐up for each outcome as follows.
-
Low risk of bias if fewer than 20% of participants were lost to follow‐up and reasons for loss to follow‐up were similar in both treatment arms
-
High risk of bias if more than 20% of participants were lost to follow‐up or reasons for loss to follow‐up differed between treatment arms
-
Unclear risk of bias if loss to follow‐up was not reported
-
-
Selective reporting of outcomes
-
Low risk of bias: e.g. the study reported all outcomes specified in the protocol
-
High risk of bias: e.g. it was suspected that outcomes had been selectively reported
-
Unclear risk of bias: e.g. it was unclear whether outcomes had been selectively reported
-
-
Other biases
-
Low risk of bias: if we did not suspect any other source of bias and the trial appeared to be methodologically sound
-
High risk of bias: if we suspected that the trial had been prone to an additional bias
-
Unclear risk of bias: if we are uncertain whether an additional bias might had been present
-
Measures of treatment effect
We used the following measures of the effect of treatment.
-
For time‐to‐event data, we used the hazard ratio.
-
For dichotomous outcomes, we analyzed data based on the number of events and the number of people assessed in the intervention and comparison groups. We used these to calculate the risk ratio and 95% confidence interval (CI).
-
For continuous outcomes, we analyzed data based on the mean, standard deviation and number of people assessed for both the intervention and comparison groups to calculate mean difference between treatment arms, with a 95% CI. If the mean difference was reported without individual group data, we planned to use this to report the study results. If more than one study measured the same outcome using different tools, we planned to calculate the standardized mean difference and 95% CI using the inverse variance method in RevMan 2014.
Unit of analysis issues
If any trials with multiple treatment groups had been identified, we would have divided the ‘shared’ comparison group into the number of treatment groups and comparisons between each treatment group and treated the split comparison group as independent comparisons.
Dealing with missing data
We did not contact study authors to obtain missing data (participant, outcome or summary data). We reported on the levels of loss to follow‐up and assessed this as a source of potential bias. We explored the impact of including studies with high levels of missing data in the overall assessment of treatment effect by using sensitivity analysis. We did not impute missing outcome data for the primary outcome.
Assessment of heterogeneity
We assessed the degree of heterogeneity among trials using I2 (Higgins 2003) and Chi2 statistics (Deeks 2001). We regarded heterogeneity to be substantial if I² was greater than 50% and either Tau² was greater than zero, or there was a low P value (less than 0.10) in the Chi2 test for heterogeneity. If substantial heterogeneity was found, we would have used subgroup and sensitivity analyses to explore the causes of heterogeneity.
Assessment of reporting biases
If we identify more than ten studies in future updates of this review, we will examine funnel plots corresponding to meta‐analysis of the primary outcome to assess the potential for small‐study effects such as publication bias. We plan to assess funnel plot asymmetry visually, and if asymmetry is suggested by a visual assessment, we will perform exploratory analyses to investigate it.
Data synthesis
We carried out statistical analysis using Review Manager 5 (RevMan 2014). We used a fixed‐effect model for combining data if there was no substantial heterogeneity. If substantial statistical heterogeneity was detected, we used a random‐effects meta‐analysis to produce an overall summary and the results were presented as the average treatment effect with 95% CIs (DerSimonian 1986).
-
For time‐to‐event data, we pooled hazard ratios using the generic inverse variance facility of RevMan 2014.
-
For dichotomous outcomes, we calculated the risk ratio for each study and then pooled them.
-
For continuous outcomes, we pooled the mean differences between the treatment arms at the end of follow‐up, where all trials measured the outcome on the same scale; otherwise we planned to pool standardized mean differences.
When we were unable to pool the data statistically using meta‐analysis we conducted a narrative synthesis of results. We presented the major outcomes and results, organised by intervention categories according to the major types or aims (or both) of the identified interventions. Depending on the assembled research, we may also in future explore the possibility of organising the data by population. Within the data categories we will explore the main comparisons of the review.
We presented the overall quality of the evidence for each outcome listed below, using the GRADE approach, which took into account issues not only related to internal validity (risk of bias, inconsistency, imprecision, publication bias) but also to external validity, such as directness of results (Langendam 2013). We created a 'Summary of findings' table based on the methods described Chapter 12.2 of the Cochrane Handbook for Systematic Reviews of Interventions (Schunemann 2011), using GRADEpro GDT. We used the checklist to maximize consistent GRADE decisions and the GRADE Working Group quality of evidence definitions (Meader 2014). We downgraded the evidence from 'high' quality by one level for serious limitations (or two levels for very serious limitations) for each outcome, and outlined our rationale in the footnotes.
-
High quality: further research is very unlikely to change our confidence in the estimate of effect.
-
Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
-
Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
-
Very low quality: we were very uncertain about the estimate.
We included the following outcomes included in the 'Summary of findings' table.
-
Overall survival
-
Quality of life assessment
-
Progression‐free survival
-
Adverse events
-
Incidence of breast cancer
-
Incidence of thromboembolic events (DVT/ PE, stroke, MI)
-
Incidence of gallstones
-
Subgroup analysis and investigation of heterogeneity
We did not identify any substantial heterogeneity; therefore subgroup analysis were not conducted. In future updates, if more studies are included and substantial heterogeneity is identified, it will be of clinical interest to investigate the safety (risk and benefits) for the prespecified outcomes in this protocol for the following factors.
-
Menopausal status at diagnosis: premenopausal versus postmenopausal. If menopausal status is not extractable from studies, we will instead analyze by age (under 50 years versus 50 years or older).
-
Hysterectomy versus no hysterectomy.
-
Stage of cancer: stage I to II versus stage III to IV
-
Tumour types: endometrioid versus non‐endometrioid
-
Positive or negative oestrogen receptor, progesterone receptor or BRCA mutation status.
Sensitivity analysis
If necessary in any future update, we will use sensitivity analyses to assess the cause of substantial heterogeneity by omitting the studies with at a high risk of bias.
Results
Description of studies
Results of the search
We searched for references up to June 2019. We found 2617 references which met our search criteria, of which 29 were duplicates. Two review authors (NS and RB) independently screened titles and abstracts; the majority of references identified were not RCTs or the objective of study was to investigate the efficacy of hormones on therapeutic outcomes of ovarian cancer and not the effect of HRT. We reviewed 11 full‐text references and excluded eight as they did not meet the inclusion criteria. We identified three studies for inclusion (Eeles 2015; Guidozzi 1999; Li 2012) (see PRISMA flow diagram; Figure 1).
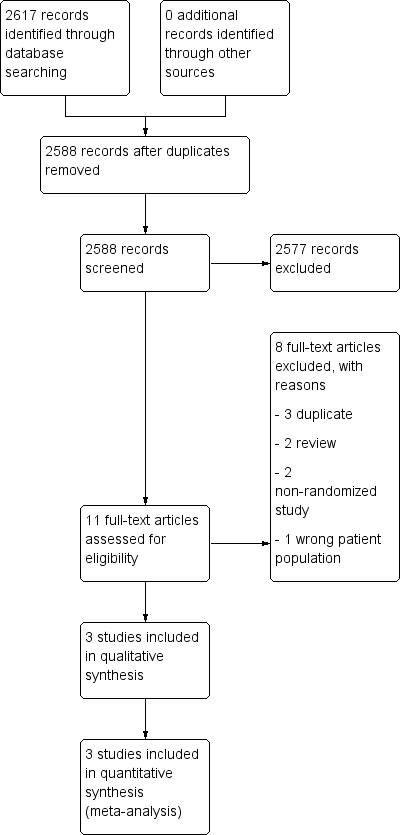
Study flow diagram.
Included studies
See Characteristics of included studies.
Study location and setting
One study (Eeles 2015) included women from multiple centres in the United Kingdom, Spain and Hungary, whereas Guidozzi 1999 and Li 2012 included single institutes in South Africa and China, respectively.
Participants
All women with a diagnosis of EOC had received cytoreductive surgery, chemotherapy, or both, and were well balanced across the two arms of the studies for demographic data. Eeles 2015 included 150 women with a median age of 58.7 years (and an age range of 29.3 to 89.6 years) and both pre and postmenopausal women were eligible for inclusion. Guidozzi 1999 included 130 women aged 59 years or younger, 44% of whom were between 56 and 59 years of age. Li 2012 included 90 women aged 45 years or younger (age range: 20 to 45 years).
The number of women that were lost to follow‐up were 0, 5 and 15 participants in Eeles 2015, Guidozzi 1999 and Li 2012, respectively. Two studies included all stages and histological types (Eeles 2015; Guidozzi 1999), whereas Li 2012 included only International Federation of Gynecology and Obstetrics (FIGO) stage I to III and serous and mucinous type. The majority of tumours were grade 3 in Eeles 2015 and grade 1 in Guidozzi 1999. There were no data on tumour grade in Li 2012. Participants were randomized to HRT versus no HRT arms using computer‐generated (Eeles 2015) or sealed‐envelope randomization (Guidozzi 1999; Li 2012).
The women that were excluded from studies were those who had conservative surgery to preserve their ovarian function, had history of hormone‐dependent malignancy with contraindications to hormone therapy (Eeles 2015), or had low malignant potential and had never taken hormone therapy (Guidozzi 1999).
None of the studies looked into the effect of BRCA status and HRT effects on survival in women with ovarian cancer. Oestrogen and progesterone receptors were investigated only in one study (Li 2012).
Interventions
The three included studies used a variety of HRT. Guidozzi 1999 used only conjugated oestrogen (0.625 mg/day). Li 2012 used combined HRT: conjugated oestrogen (0.625 mg/day) with medroxyprogesterone (4 mg/day) and nylestriol (2.5 mg/15 day) with medroxyprogesterone (4 mg/day). Eeles 2015 used oestrogen only: conjugated oestrogen, estradiol patch and estradiol implant, and combined with progesterone; conjugate oestrogen and norgestrel.
Outcomes
The median follow‐up time was 31.4 months, 90 months and 19.1 years for Li 2012, Guidozzi 1999 and Eeles 2015, respectively. There were participants who were lost to follow‐up: 3.8% in Guidozzi 1999 and 16.7% in Li 2012. These participants were excluded from the analysis and results. In Eeles 2015, where the median follow‐up was 19.1 years, 63.9% of participants discontinued hormone therapy; the most common being the presence of adverse effects or unknown reason.
There were participants who were assigned to HRT, but did not receive or discontinued HRT (65.5% in Eeles 2015 and 13.6 % in Guidozzi 1999). There were also participants who were assigned to no HRT, but who received HRT (10.7% in Eeles 2015 and 8.5% in Guidozzi 1999). However, all analyses were performed on an intention‐to‐treat basis for these studies.
Overall survival was the primary outcome in all three studies. The incidence of breast cancer was studied in two studies (Eeles 2015; Li 2012). Treatment adverse effects and quality of life (using the EORTC‐C30 questionnaire and GMU‐Gynae Index), were only studied in Li 2012. The EORTC‐C30 was used to assess five function domains (physical, emotional, social, role and cognitive), eight symptoms (fatigue, pain, nausea/vomiting, constipation, diarrhoea, insomnia, dyspnoea and loss of appetite) and global health/quality of life. The GMU‐Gynae Index assessed quality of sexual life (sexual difficulties, emotional exchange between the couple, regression of sexual life and sexual desire), symptoms of lower urinary tract infection (urethral burning and frequent urination), autonomic dysfunction (itchy skin, dry skin and formication). The incidence of gallstones was not reported in any study.
Dates of study, funding sources and declarations of interest
For Guidozzi 1999 the study period was four to seven years and included participants between January 1987 and June 1994. Eeles 2015 included participants between February 1990 and November 1995; and Li 2012 included participants between August 1999 and June 2003.
Funding was provided by their own institute in two studies(Guidozzi 1999; Li 2012); these studies did not provided details of any conflict of interest. Funding for Eeles 2015 was provided from multiple sources as this was a multicentre study; they declared conflicts of interest among the various authors.
Excluded studies
We excluded eight references from the full‐text review, of which three were duplicate reports (Guidozzi 1998; Guidozzi 1999a; Li 2008), two were non‐randomized studies (Bebar 2000; Ursic‐Vrscaj 2001), two were literature reviews (Guidozzi 2013; Lipkowitz 2015), and one was a study which included healthy postmenopausal women (Anderson 2003). See Characteristics of excluded studies.
Risk of bias in included studies
The details of risk of bias for the three included studies are shown in Figure 2 and Figure 3.
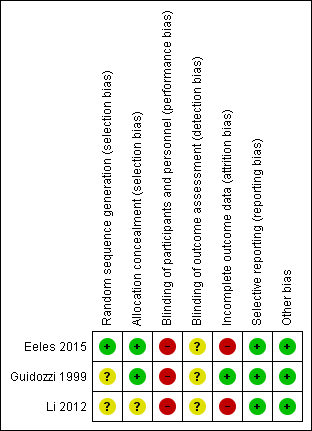
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
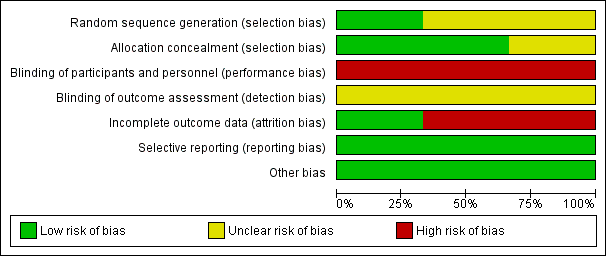
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
Three studies used randomization for allocation; one study clearly described using computer‐generated random permuted blocks (Eeles 2015) and the other two did not mention the method used (Guidozzi 1999; Li 2012).
Two studies showed adequate allocation concealment using central randomization (Eeles 2015) or sealed opaque envelopes (Guidozzi 1999); and one study had insufficient information to justify a judgement of low or high risk of bias (Li 2012).
Blinding
All studies had a high risk of performance bias because the participants knew the HRT they were receiving and there was no placebo used. There was no information about the assessors and whether they knew the treatment group in all three studies; therefore we classified the risk of detection bias as unclear.
Incomplete outcome data
All three studies reported data on losses to follow‐up and non‐compliance (0% and 65.3%, respectively in Eeles 2015; and 3.8% and 31.1%, respectively in Guidozzi 1999); however, they analyzed their results on an intention‐to‐treat basis. Li 2012 excluded from analysis participants who were lost to follow‐up or non‐compliance to HRT within six months (16.7%).
Selective reporting
The study protocols were not available, however, the studies reported the results as detailed in their objectives.
Other potential sources of bias
The studies appeared to be free of other sources of bias.
Effects of interventions
See summary of findings Table for the main comparison: HRT versus no HRT for women who have undergone surgical treatment for EOC.
Primary outcomes
Overall survival
All three studies reported overall survival. The pooled result showed that HRT may improve overall survival in women who have had surgery for EOC (HR 0.71, 95% CI 0.54 to 0.93; three studies, 350 participants; low‐certainty evidence; Analysis 1.1).
Quality of life
We are uncertain whether HRT improves or reduces the overall quality of life women who have had surgery for EOC (MD 13.67 points higher; 95% CI 9.26 higher to 18.08 higher; very low‐certainty evidence; one study, 75 participants; very low‐certainty evidence; Analysis 1.2).
Secondary outcome
Progression‐free survival
The effect of HRT on progression‐free survival in women who have had surgery for EOC was assessed in two studies (Eeles 2015; Guidozzi 1999); the range where the actual effect may be (the "margin of error") indicated that it may make little or no difference (HR 0.76, 95% CI 0.57 to 1.01; two studies, 275 participants; low‐certainty evidence; Analysis 1.3).
Incidence of breast cancer
It is uncertain whether HRT increased the incidence of breast cancer. There were only three participants who developed breast cancer: two participants in the HRT arm, and one participant in the no HRT arm, in one study (Eeles 2015); and none in another study (Li 2012). The effect of HRT varied and it was possible that HRT made little or no difference as we are very uncertain of the results (RR 2.00, 95% CI 0.19 to 21.59; two studies, 225 participants; very low‐certainty evidence; Analysis 1.4).
Transient ischaemic attack (TIA)
It was very uncertain whether HRT increases the incidence of TIA. There were only two participants who developed TIA in Eeles 2015, both in the HRT arm (RR 5.00, 95% CI 0.24 to 102.42; one study, 150 participants; very low‐certainty evidence; Analysis 1.5).
Cerebrovascular accident (CVA)
It was uncertain whether HRT decreases the incidence of CVA. There were five participants who developed CVA in one study (Eeles 2015): two participants in the HRT arm and three participants in the no HRT arm (RR 0.67; 95% CI 0.11 to 3.88; one study, 150 participants; very low‐certainty evidence; Analysis 1.6).
Myocardial infarction (MI)
It was uncertain whether HRT decreases the incidence of MI. There were two participants in Eeles 2015 who developed MI, both in the no HRT arm (RR 0.20, 95% CI 0.01 to 4.10; one study, 150 participants; very low‐certainty evidence; Analysis 1.7).
Incidence of gallstone
The incidence of gallstone was not reported in any of the included studies.
Subgroup and sensitivity analyses
We did not perform subgroup or sensitivity analyses for any outcomes due to there only being a small number of trials and no substantial heterogeneity identified.
Discussion
Summary of main results
The evidence on the efficacy and safety of HRT versus no HRT in women who have undergone surgical treatment for EOC is limited; only three small studies met the inclusion criteria for our review and they provided low‐ to very low‐certainty evidence. Quality of life, measured using EORTC‐C30 scale, was presented only in one study (Li 2012). HRT may slightly improve overall survival in women who have had surgical treatment for EOC, but may make little or no difference to quality of life, progression‐free survival, incidence of breast cancer, transient ischaemic accident, cerebrovascular accident and myocardial infarction events.
Overall completeness and applicability of evidence
All published RCTs that were included in this meta‐analysis reported outcomes for all the outcomes of this review, except the incidence of gallstones. We found that HRT may slightly improve overall survival and quality of life in women after oncological treatment for EOC.
One of the included trials was conducted across European centres including the United Kingdom, Spain and Hungary (Eeles 2015), while the other two were single‐centre trials in South Africa (Guidozzi 1999) and Asia (Li 2012). All three studies reported on overall survival; two reported progression‐free survival (Eeles 2015; Guidozzi 1999) and incidence of breast cancer (Eeles 2015; Li 2012). Adverse effects were only reported in one study, the results for which had wide confidence intervals influenced by the small sample size (Eeles 2015).
The EORTC‐C30 questionnaire was used for quality‐of‐life assessments in Li 2012, and we selected only the domain of general condition in this questionnaire for analysis. EORTC‐C30 is a standardized questionnaire commonly used for people with cancer (Snyder 2013), not a menopause‐specific assessment. The Menopause Specific Quality of Life Questionnaire (MENQOL), World Health Organization Quality of Life (WHO QOL‐BREF), Greene Climacteric Scale, Utian Quality of Life (UQOL) Scale, Women's Health Questionnaire (WHQ), 36‐Item Short Form (SF‐36), MENCAV, Cervantes Scale, Cervantes Short‐Form Scale, and Menopause Rating Scale (MRS) are the questionnaires that can be used to specifically assess menopausal symptoms (Jenabi 2015).
Hormone replacement therapy may increase the risk of developing other diseases such as breast cancer, when combined hormonal therapy is used (Benkhadra 2015; Chlebowski 2015; Manson 2013), coronary heart disease (Rossouw 2002; Rossouw 2007), stroke (Manson 2013; Rossouw 2002), pulmonary embolism (Manson 2013; Rossouw 2002), deep vein thrombosis (Manson 2013), dementia (Manson 2013) and gallbladder disease (Manson 2013). Prolonged use of HRT and the use of combined HRT for women older than 60 years of age has been associated with higher risk of developing pulmonary embolism and lower risk of colorectal cancer. Women who have undergone hysterectomy who use oestrogen‐only HRT may have an increased risk of stroke and colorectal cancer, when older than 60 and 70 years of age, respectively (Manson 2013). The use of HRT in healthy postmenopausal women has been associated with increased risk of developing ovarian cancer (Rodrigguez 2001; Zhou 2008), of both serous (Cancer Epidemiology 2015; Mørch 2012; Shi 2015) and endometrioid types (Cancer Epidemiology 2015; Mørch 2012). Using HRT for more than five years is linked to increased risk of ovarian cancer (Zhou 2008) and this correlation is stronger for the serous type (Mørch 2012).
Hormone receptors, oestrogen receptors or progesterone receptors and BRCA mutation status are known prognostic factors in ovarian cancer ( Luo 2017; Shen 2017; Zhong 2015). The presence of oestrogen receptors has been associated with favourable overall survival in women with unclassified EOC in Europe, South America and Oceania. However, oestrogen receptors have not been associated with a longer progression‐free survival (Shen 2017). The presence of progesterone receptors has also been associated with favourable overall survival and progression‐free survival in European women with unclassified EOC (Luo 2017). Likewise, BRCA mutation has been correlated to better overall and progression‐free survival (Zhong 2015). However, no studies were identified that looked at the effect of HRT in women who have undergone surgical treatment for EOC with hormone receptors or BRCA mutation.
We did not identified heterogeneity of outcomes among the various studies. There was no studies comparing the different regimens and duration of HRT, although there were variations in the age and race of participants, stage and histological type of disease, regimen, dose and route of administration for HRT. This may indicate the generalisability of the application in clinical practice. However, the information on duration of HRT use, hormone receptor status and BRCA mutation was limited.
Quality of the evidence
Using the GRADE system, we estimated the certainty of the evidence to be low because of limitations in the design of the included studies design and inconsistency of results. Not all studies had used placebo in the control group; participants knew what hormone therapy they received and in some studies, there was loss to follow‐up greater than 20% (Li 2012). There were also differences in the outcomes; one study showed an effect of HRT use (Eeles 2015), whereas the others did not show the same effect (or only partly in one study (Guidozzi 1999)). The GRADE rating was further downgraded to very low‐certainty evidence due to imprecision of results, small sample sizes and wide 95% CIs.
Potential biases in the review process
We conducted a comprehensive search of the available evidence. Two review authors independently searched for studies following clear inclusion and exclusion criteria and identified eligible studies. Two review authors independently extracted data and evaluated risk of bias. It remains possible that studies may have not been reported or were missed and not included. Analysis of publication bias could not be performed in this review as the number of included studies is lower than ten.
Agreements and disagreements with other studies or reviews
A recent meta‐analysis on the effect of HRT in the general population showed that HRT did not affect the risk of death from cardiac events, stroke and cancer (breast, lung, colorectal or ovarian) (Benkhadra 2015). However, combined HRT use, but not oestrogen‐only HRT, was associated with an increased risk of mortality from breast cancer (Benkhadra 2015). This meta‐analysis examined younger women (who started HRT aged under 60 or within 10 years of menopause) separately and found that HRT use was associated with lower all‐cause mortality. The evidence on HRT in women experiencing natural menopause remains unclear. The findings of a systematic review and meta‐analysis (which included 310,329 women) showed that women experiencing early menopause (at less than 45 years of age) had overall higher incidence of coronary heart disease and mortality from coronary heart disease, cardiovascular disease and all‐cause mortality (Muka 2016). A large epidemiological study, the Black Women’s Health Study, investigated all‐cause mortality in 11,212 women with natural menopause and found that women aged less than 45 years who never used HRT had a higher mortality rate; this was not significant for those who ever used HRT (Li 2013). In another USA‐based epidemiological study of 11,287 women, all‐cause mortality was higher in women experiencing menopause under 45 years of age (Malek 2019). Over a 7.1 year follow‐up, those experiencing menopause under 45 years who had ever used HRT had a higher all‐cause mortality rate than those who experienced menopause over 45 years of age who had ever used HRT, although limitations include association of smoking with an early age of menopause. In addition, women who used HRT for more than five years, from around the age of 50, were found to have a higher risk of ovarian cancer, especially for serous and endometrioid types (Cancer Epidemiology 2015).
There have been three previous systematic reviews of the use of HRT in EOC after treatment. The first systematic review, Hopkins 2004, included one RCT (Guidozzi 1999) and two observational studies. The second and third systematic reviews (Li 2015; Pergialiotis 2015) included two RCTs (Guidozzi 1999; Li 2012) and four cohort studies. The result of all these systematic reviews showed that HRT may make little or no difference to overall and progression‐free survival. Our review included three RCTs (Eeles 2015; Guidozzi 1999; Li 2012) and the results suggest that HRT may be associated with a slight improvement in overall survival and quality of life (especially for general condition), but may make little or no difference to progression‐free survival. The results of adverse events of HRT were not reported in any of the three previous systematic reviews (Hopkins 2004; Li 2015; Pergialiotis 2015).
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Comparison 1 Hormone replacement therapy versus no hormone replacement therapy, Outcome 1 Overall survival.

Comparison 1 Hormone replacement therapy versus no hormone replacement therapy, Outcome 2 Quality of life, general condition.

Comparison 1 Hormone replacement therapy versus no hormone replacement therapy, Outcome 3 Progression‐free survival.

Comparison 1 Hormone replacement therapy versus no hormone replacement therapy, Outcome 4 Incidence of breast cancer.

Comparison 1 Hormone replacement therapy versus no hormone replacement therapy, Outcome 5 Transient ischaemic attack.

Comparison 1 Hormone replacement therapy versus no hormone replacement therapy, Outcome 6 Cerebrovascular accident.

Comparison 1 Hormone replacement therapy versus no hormone replacement therapy, Outcome 7 Myocardial infarction.
| Hormone replacement therapy (HRT) compared to no HRT for epithelial ovarian cancer (EOC) | ||||||
| Patients: women of any age diagnosed with any stage of EOC who had surgical treatment, regardless of chemotherapy treatment | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
| Risk with no HRT | Risk with HRT | |||||
| Overall survival | Study population | HR 0.71 | 350 | ⊕⊕⊝⊝ | The median follow‐up time in the three included studies was 31.4 months, 90 months and 19.1 years. | |
| 795 per 1,000 | 675 per 1,000 | |||||
| Quality of life, general condition | The mean quality of life (general condition) in the no HRT group was 13.84 points. | The mean quality of life (general condition) in the HRT group was 13.67 points higher | ‐ | 75 | ⊕⊝⊝⊝ | The EORTC‐C30 questionnaire was used to evaluate this outcome; higher values correspond with improvement. |
| Progression‐free survival | Study population | HR 0.76 | 275 | ⊕⊕⊝⊝ | The median follow‐up time in the two studies was 90 months and 19.1 years. | |
| 773 per 1,000 | 676 per 1,000 | |||||
| Incidence of breast cancer | Study population | RR 2.00 | 225 | ⊕⊝⊝⊝ | The median follow‐up time in the two studies was 31.41 months and 19.1 years. | |
| 8 per 1,000 | 17 per 1,000 | |||||
| Incidence of transient ischaemic attack | Study population | RR 5.00 | 150 | ⊕⊝⊝⊝ | The median follow‐up time in the study was 19.1 years. | |
| 7 per 1,000 | 33 per 1,000 | |||||
| Incidence of cerebrovascular accident | Study population | RR 0.67 | 150 | ⊕⊝⊝⊝ | The median follow‐up time in the study was 19.1 years. | |
| 40 per 1,000 | 27 per 1,000 | |||||
| Incidence of myocardial infarction | Study population | RR 0.20 | 150 | ⊕⊝⊝⊝ | The median follow‐up time in the study was 19.1 years. | |
| 27 per 1,000 | 5 per 1,000 | |||||
| Incidence of gallstones | ‐ | ‐ | ‐ | ‐ | ‐ | The incidence of gallstones was not reported in the included studies. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded by one level due to limitations in study design | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Overall survival Show forest plot | 3 | 350 | Hazard Ratio (95% CI) | 0.71 [0.54, 0.93] |
| 2 Quality of life, general condition Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 Progression‐free survival Show forest plot | 2 | 275 | Hazard Ratio (95% CI) | 0.76 [0.57, 1.01] |
| 4 Incidence of breast cancer Show forest plot | 2 | 225 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.0 [0.19, 21.59] |
| 5 Transient ischaemic attack Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 6 Cerebrovascular accident Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7 Myocardial infarction Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |