Intermittent versus continuous systemic therapy as treatment for unresectable metastatic colorectal cancer
Abstract
This is a protocol for a Cochrane Review (Intervention). The objectives are as follows:
To assess the effect of intermittent systemic therapy versus continuous systemic therapy in terms of survival, toxicity and quality of life in patients with unresectable metastatic colorectal cancer (CRC).
Background
Colorectal cancer (CRC), defined as cancer that develops in the colon or rectum, is one of the most prevalent malignancies and has a high mortality rate (American Cancer Society 2014). In 2012 there were nearly 1.4 million new cases and a mortality of 694,000 deaths worldwide (Ferlay 2015). In Western countries CRC is the second most common cancer in women and the third most common cancer in men (Ferlay 2015). A high proportion of these patients are elderly (≥65 years), and thus are more susceptible to the harm caused by treatment, such as chemotherapy‐related toxicity and death (Hurria 2011). When there is no prospect of cure, both comfort and quality of life are important to consider for all people with CRC.
Survival of patients with metastatic CRC has improved significantly in the past years (Khattak 2012; Tournigand 2004). As a result, treatment exposure has also improved. Therefore, it is important to develop or modify current treatment strategies to reduce toxicities and other adverse events, and, consequently, improve quality of life in the palliative setting.
Description of the condition
The proportion of patients with CRC diagnosed with synchronous metastasis (metastasis at diagnosis) is approximately 20% to 34%; almost 50% will develop metachronous metastasis (metastasis developing after diagnosis), with the liver being the most common site involved (NCCN 2014; Van Cutsem 2010). Resectability of metastatic CRC is generally decided by a multidisciplinary team. The criteria used for resection of metastatic disease indicates the likelihood of achieving complete resection of all evident disease (negative surgical margins) whilst maintaining adequate liver reserve (NCCN 2014). More recently, there have been significant improvements in the palliative systemic treatment of patients with unresectable metastatic CRC. Decades ago, median survival with best supportive care was five to six months (Scheithauer 1993). With the introduction of the fluoropyrimidines, median survival has increased to 11 to 12 months, and has increased further to about two years with the administration of combination chemotherapy and the incorporation of multidisciplinary approaches, such as resection of liver metastasis (Hochster 2014; Khattak 2012; Tournigand 2004). For patients with metastatic CRC diagnosed between 2003 and 2009, the five‐year survival rate was 13% (American Cancer Society 2014).
Description of the intervention
Palliative systemic treatment for patients with unresectable metastatic CRC includes chemotherapy and targeted therapy with a palliative intent, with the aim to prolong life, postpone progression and preserve quality of life (Cunningham 2010). Systemic therapy has been shown to improve median survival in these patients (Best 2000; NGTATG 1992; Renouf 2011; Sanoff 2008; Scheithauer 1993).
Nonetheless, an evaluation of intermittent systemic therapy in a prospective setting has been initiated because of non‐compliance of patients with intensive therapy, and a treatment‐related decrease in quality of life (Chibaudel 2012). In the past decade, several trials have been published on this subject, with discordant results (Alexopoulos 2006; Chibaudel 2012; Maughan 2003). A recent publication, Kay 2015, evaluated the current use of intermittent chemotherapy in daily practice, and concluded that there was no statistically significant difference in overall survival for patients who had a chemotherapy‐free interval who were receiving first‐line chemotherapy monotherapy with irinotecan or oxaliplatin. Kay 2015 reported that patients who had a chemotherapy‐free interval and were receiving combination therapy of irinotecan and bevacizumab actually had poorer overall survival.
Two previous systematic reviews concluded that there was no clinically significant reduction in overall survival with intermittent treatment compared with continuous therapy (Berry 2015; Pereira 2015). Neither review pooled trials that reported quality of life. Pereira 2015 concluded that continuous treatment was associated with increased toxicity. As described above, quality of life is a very important issue in the consideration of intermittent therapy and the benefit in quality of life needs to be assessed.
How the intervention might work
In current practice, systemic therapy is often administered until treatment failure or resistance to therapy occurs. A patient is considered resistant when the disease fails to respond to a given therapy (primary resistance), or there is progression of the disease though initially responding to therapy (secondary resistance). As a result, treating a patient with proven resistance does not seem to be advisable within six months (Tonini 2013).
However, several theories could justify the reintroduction of the same therapy. Firstly, by discontinuing therapy, previously suppressed tumour suppressor genes might be expressed again and the same therapy might therefore become effective; resistance to therapy could be delayed by intermittent therapy.
Secondly, tumours are a heterogenous mass that consist of multiple genetic and epigenetic clones. It could be possible that treatment‐sensitive and treatment‐resistant clones are both present in one tumour. When treatment regimens are alternated, tumour cells that were sensitive to previous treatment have the ability to progress and therefore regain sensitivity to that previous treatment. Thirdly, when the initial therapy is discontinued, the tumour might be allowed to reverse into a previous epigenetic profile in the meantime, and the tumour can become re‐susceptible for the same therapy (Santini 2012; Tonini 2013). Biological evidence for this strategy and the improvement in quality of life should be taken into account when the effect of intermittent versus continuous systemic therapy is studied. If survival is unimpaired, toxicities reduced and quality of life is improved in patients receiving intermittent systemic therapy, this will be beneficial for patients in a palliative setting.
Why it is important to do this review
Although eligible treatment options are available for patients with unresectable metastatic CRC, it remains an incurable disease. Therefore, the focus of treatment in this terminal phase of life should be on comfort and maintenance of quality of life. The choice of systemic therapy has expanded over recent years, with multiple lines of therapy and efficacy of systemic therapy improved in patients with unresectable metastatic CRC. As a result, life expectancy has also improved and therefore treatment exposure has increased.
As current guidelines prescribe, patients with unresectable metastatic CRC currently receive continuous systemic therapy for their remaining lifetime, with the focus on the associated toxic effects, periodic clinical visits and their impact on quality of life (NCCN 2014). Continuous chemotherapy frequently increases fatigue, hand‐foot syndrome and oxaliplatin‐related neuropathy, and subsequently deteriorates quality of life (Braun 2011).
Thus, if intermittent administration can decrease toxicities and improve quality of life without decreasing survival or tumour control, this will be a great improvement in the palliative care for patients with unresectable metastatic CRC. In addition, fewer periodic clinical visits and oral therapy could also reduce the impact of the disease on patients' quality of life.
Objectives
To assess the effect of intermittent systemic therapy versus continuous systemic therapy in terms of survival, toxicity and quality of life in patients with unresectable metastatic colorectal cancer (CRC).
Methods
Criteria for considering studies for this review
Types of studies
We will consider randomised controlled trials (RCTs) that assess the effect of intermittent systemic therapy versus continuous systemic therapy for inclusion. We will include cluster‐RCTs and crossover randomised designs: however, it is unlikely that these designs are used in trials that assess this clinical question. There will be no minimum follow‐up period. We will consider abstracts if sufficient information and data will be available to analyse any of the outlined outcomes of this review.
Types of participants
Male and female adults (≥ 18 years) with unresectable metastatic colorectal cancer (CRC) (TNM stage1 IV) T1‐4, N0‐3, M1 (NCCN 2014).
1The TNM staging system for solid tumours uses the size and extension of the primary tumour (T), its lymphatic involvement (N) and the presence of metastases to classify the progression of cancer (M).
Types of interventions
Every intermittent treatment schedule starts with induction chemotherapy. Intermittent therapy in this study is defined as stopping or changing maintenance therapy after initial cycles of chemotherapy and then restarting with any kind of therapy at any point in time. There will be no restrictions regarding type of systemic therapy, as long as the regimes are compliant with this definition. We will consider the comparison between intermittent and continuous chemotherapy independently of the line of therapy.
We will include studies that use any of the four following basic strategies of intermittent therapy:
-
intermittent chemotherapy with Fluorouracil (5FU) maintenance therapy;
-
intermittent chemotherapy with no maintenance therapy (chemotherapy‐free interval);
-
intermittent chemotherapy with biologicals as maintenance therapy;
-
intermittent chemotherapy plus intermittent targeted therapy.
Apart from different options in treatment strategies, there are also differences in the length of the interval depriving the patient of therapy. Intermittent therapy can be restarted at progression of disease or at a set point in time. Progression of disease is defined as when the cancer continues to grow or spreads, preferably defined according to the Response Evaluation Criteria In Solid Tumours (RECIST) criteria (Eisenhauer 2009). We will include trials regardless of the duration of the interval.
Continuous systemic therapy can be chemotherapy, targeted therapy or other novel agents. We will select studies for inclusion regardless of the treatment dose, delivery, duration or intensity. We will allow therapy at initial diagnosis or concomitant therapy in the included studies provided that this is equally distributed across all arms of the included trial. Examples of therapy schemes can be found in Table 1. Additional treatments can be of any kind, e.g. best supportive care, radiotherapy or interventional radiological techniques.
| Table 1. Examples of intermittent versus continuous treatment schemes | |
| 1. | Intermittent: FOLFOX17, 12 weeks; sLV5‐FU22, 24 weeks; FOLFOX7, 12 weeks |
| Continuous: FOLFOX4 every 2 weeks until progression of disease (PD) (Tournigand 2004) | |
| 2. | Intermittent: FOLFIRI3, 12 weeks; chemotherapy‐Free‐Interval (CFI); restart FOLFIRI at PD |
| Continuous: FOLFIRI, 24 weeks (Alexopoulos 2006) | |
| 3. | Intermittent: Bevacizumab + capecitabine/oxaliplatin, 18 weeks; CFI; restart Bevacizumab+ capecitabine/oxaliplatin at PD |
| Continuous: Bevacizumab + capecitabine/oxaliplatin, 18 weeks; bevacizumab+capecitabine, restart bevacizumab+capecitabine/oxaliplatin at PD (Simkens 2015) | |
1 FOLFOX: FOL: folinic acid; F: fluorouracil (5‐FU); OX: oxaliplatin.
2 sLV5‐FU2: simplified leucovorin plus bolus and infusional fluorouracil.
3 FOLFIRI: FOL: folinic acid; F: fluorouracil (5‐FU); IRI: irinotecan.
We will not use any restrictions regarding RECIST criteria use or grading of toxicity/adverse events. We will use this as described by the trial authors.
Types of outcome measures
For patients with unresectable metastatic CRC, we will compare intermittent systemic therapy with continuous systemic therapy in terms of survival (using a non‐inferiority approach) and side effects (using a superiority approach).
Primary outcomes
-
Overall survival, measured from date of randomisation until date of death;
-
Toxicity: we will assess the incidence of grade 3 and 4 toxicity, preferably as defined by the National Cancer Institute (NCI 2010):
Grade 3 toxicity is considered as "severe or medically significant but not immediately life‐threatening; hospitalisation or prolongation of hospitalisation indicated; disabling; limiting self care activities of daily living (ADL)" (NCI 2010). Grade 4 toxicity is considered as "life‐threatening consequences; urgent intervention indicated" (NCI 2010). If possible we will also compare distinct toxicities (e.g. hand‐foot syndrome or fatigue). We will report the toxicities that were reported by the trial authors at any given time point.
Secondary outcomes
-
Quality of life: we will take this into account at multiple time points, depending on how the included studies have measured it. We will take into account all types of quality of life scales, both validated (preferable) and non‐validated questionnaires;
-
progression‐free survival: this is defined as the time from the start of treatment until progression, and progression is preferably measured by the RECIST criteria (which is not required for a study to be included).
Search methods for identification of studies
Electronic searches
We will search the following databases to identify studies that meet the inclusion criteria:
-
CENTRAL (the Cochrane Central Register of Controlled Trials, the Cochrane Library) (Appendix 1);
-
MEDLINE (via Ovid SP) (Appendix 2);
-
Embase (via Ovid SP) (Appendix 3);
-
PsychInfo.
The CCCG Information Specialist will design the literature search strategy, which the review authors (MF, YC, EB and EK) will provide input on. We will not apply any date or language restrictions. We will not exclude studies based on publication status. We will examine relevant errata or retraction statements for information.
We will search the ClinicalTrials Website (https://clinicaltrials.gov/) and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/en/) for ongoing trials.
We will search for additional studies by screening the bibliographies of all retrieved and relevant publications identified by the above search strategies. Also we will search for additional trials through the Cochrane specialist register. We will search the grey literature, including conference abstracts and guidelines.
The literature search will be rerun within 12 months of publication of the Cochrane Review.
Searching other resources
We will screen all references of retrieved eligible studies for relevant studies. We will also scan previous reviews on this topic for relevant studies.
Data collection and analysis
Selection of studies
Two review authors (MF and YC) will independently screen the titles and abstracts of all articles we identify in the literature searches, and will code them as either 'retrieve' or 'do not retrieve'. The two review authors will resolve any discrepancies by discussion. In the case of disagreement, we will consult a third review author (EK) in order to reach a consensus on titles and abstracts. We will retrieve the full‐text papers of articles where we consider the titles and abstracts to be relevant or where eligibility is unclear. Two review authors (MF and YC) will independently assess these articles for inclusion and will resolve any discrepancies by discussion. In case of disagreement, we will consult a third review author (EK).
We will contact the study authors in case the information we require for meta‐analysis is not sufficiently reported. We will collate multiple reports of one study and we will indicate a primary data source. In the case of a multiple‐arm study, of which not all arms assess the treatment of interest, we will only consider study arms that compare continuous versus intermittent systemic therapy. As the included trials must be randomised, this will not disturb the baseline characteristics of the study population.
We will present the study selection process in a PRISMA flow chart (Figure 1). We will list the excluded studies and their reasons for exclusion in a 'Characteristics of excluded studies' table. We will include studies irrespective of whether the study presents outcome data. We will use Covidence software for reference handling (Covidence 2013).

Study flow diagram.
Data extraction and management
Two review authors (MF and YC) will independently extract data from the included studies. We will pilot test the data extraction form first.
The data collection form will contain the following items.
-
General information: study title, study author(s), source, publication date, contact address, language, funding sources and author declaration(s) of interest;
-
Study characteristics: number, age, gender, site of metastatic disease, whether or not participants received previous adjuvant systemic therapy (in curative setting), site of primary tumour (colon or rectum), performance status (if available), how resectability was measured, method of chemotherapy administration, dosage and duration of the intervention, moment of restart of intermittent therapy, how progression was measured, type of quality of life measurement scale, type of toxicity measurement scales, toxicities, details of comparison regimen, number of participants that dropped out or that were lost to follow‐up;
-
Outcomes: overall survival, toxicities, progression‐free survival and quality of life.
We will check both the magnitude and the direction of the effect size reported by the included studies to ensure that we do not include any incorrect values in the pooled analysis. We will resolve any disagreements regarding data collection by consulting a third review author (EK). We will use Covidence software for data extraction (Covidence 2013).
Assessment of risk of bias in included studies
Two review authors (MF and YC) will assess and discuss the following methodological 'Risk of bias' domains according to the Cochrane 'Risk of bias' assessment tool (Higgins 2011, chapter 8.5.d), using Covidence software (Covidence 2013).
-
sequence generation;
-
concealment of treatment allocation;
-
blinding of participants and personnel;
-
blinding of outcome assessment (in this case partly only secondary objectives, primary objective cannot be blinded);
-
incomplete outcome data;
-
selective outcome reporting;
-
other potential threats to validity (considering external validity, e.g. relevant use of co‐interventions in both study arms, or selection of specific patient groups).
We will judge each domain as either at low risk, high risk or unclear risk of bias according to criteria used in the Cochrane ‘Risk of bias’ assessment tool (see Appendix 4) (Higgins 2011a, chapter 8.5.d).
We will obtain support for our judgements from reports, personal correspondence and previous comparable trials from the same research team.
Measures of treatment effect
For time‐to‐event data (e.g. progression‐free survival and overall survival), we will calculate the hazard ratios (HR) and their 95% confidence intervals (CI) for each trial. If no HRs are reported, we will extrapolate them from the reported Kaplan‐Meier curves (Parmar 1998).
For dichotomous variables (e.g. toxicity rates), we will calculate relative ratios (RR) and their 95% Cl.
For continuous outcomes (e.g. quality of life measurements), we will use mean differences (or standardised mean differences if results are expressed on different scales) along with their 95% CI as summary statistic in meta‐analyses.
We will check the magnitude and direction of the effect size reported to ensure we avoid errors.
When possible, we will pool summary data for dichotomous, continuous and time‐to‐event outcomes obtained by means of meta‐analysis using a random‐effects model (DerSimonian 1986).The estimation of between study heterogeneity might be inaccurate when we identify a small number of trials for inclusion and the random‐effects model might be biased. If the number of included trials is lower than 10, we will also perform a meta‐analysis using a fixed‐effect model. We will use the inverse variance method to run both the fixed‐effect and random‐effects model.
Unit of analysis issues
For parallel group individually randomised trials, the unit of analysis will be the individual patient.
We do not expect to find either cross‐over RCTs or cluster‐RCTs. However, in case we identify cluster RCTs or crossover trials that meet the inclusion criteria of this review, we will handle unit of analysis issues.
Cluster‐RCTs
Cluster‐RCTs are unlikely for this procedure. However, if we identify any cluster‐RCTs that meet the inclusion criteria of this review, we will include them in the analyses along with individually RCTs. We will adjust their sample sizes using the methods described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011b, chapter 16.3.4 or 16.3.6) using an estimate of the intra‐cluster correlation co‐efficient (ICC) derived from the trial (if possible), from a similar trial or from a study of a similar population. If we use ICCs from other sources, we will report this and conduct sensitivity analyses to investigate the effect of variation in the ICC. If we identify both cluster‐RCTs and individually RCTs, we plan to synthesise the relevant information. We will consider it reasonable to combine the results from both if there is little heterogeneity between the study designs and we consider the interaction between the effect of intervention and the choice of randomisation unit to be unlikely.
Cross‐over trials
Should we find cross‐over trials that meet the inclusion criteria of this review, we will perform sensitivity analysis by excluding those trials to assess whether this type of trial significantly affects the pooled estimates. We will use preferably the data from the first period, if reported.
Multiple‐arm trials
If multiple‐arm trials meet the inclusion criteria, we will include pair‐wise comparison of appropriate arms in the analyses. In the event of one trial arm appearing twice in a single meta‐analysis, we will halve the numbers in the control arm to avoid double counting.
Dealing with missing data
We will contact the study authors by e‐mail or telephone to retrieve any missing information concerning missing or dropout data. If we do not receive a reply from the study authors, we will consider both the best‐case and worst‐case scenarios for dropouts.
Assessment of heterogeneity
We will assess the level of heterogeneity between the included studies using the Chi2 test (P < 0.05). We will quantify the level of heterogeneity between studies using the I2 statistic. We will present data in a qualitative analysis if there is heterogeneity. We will interpret the I2 statistic value according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011c, chapter 9.5.2).
We will not pool data if heterogeneity is high (i.e. if the I2 statistic value is greater than 75%). We will investigate potential sources of between‐study heterogeneity by means of subgroup analysis (see Subgroup analysis and investigation of heterogeneity).
Assessment of reporting biases
We will present a funnel plot for the detection of potential reporting bias if we analyse more than 10 studies. We will check these against the protocols, if available, and compare the outcomes reported with those planned.
Data synthesis
Regarding the toxicity endpoint, the interpretation of the results will follow the usual superiority (or inferiority) approach: that is, in the intermittent versus continuous schedule comparison, a summary relative risk of less than one with the CI not crossing the null value (i.e. one) will mean that the intermittent schedule is associated with a significantly lower toxicity rate. We will use an alpha level of 5% as a level of significance.
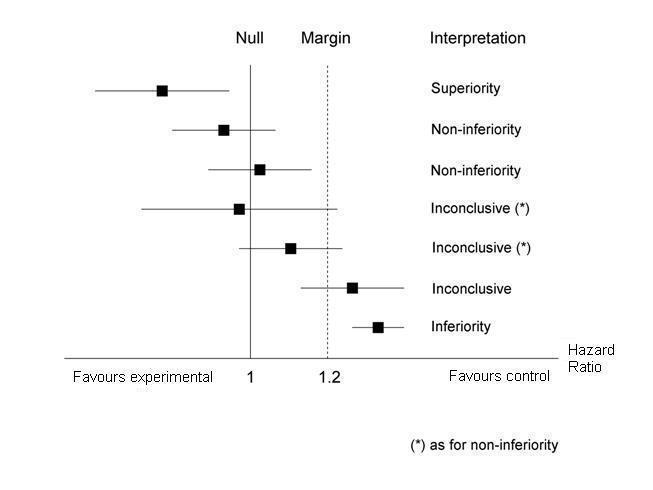
In contrast, when we will interpret the survival findings, we will use a non‐inferiority analysis (D'Agostino 2003). In the intermittent versus continuous schedule comparison we do not need the former to be better in terms of efficacy, but we do need to assess whether the former can be considered equivalent to the latter in terms of expected patient survival. This can be done by setting a margin, that is, the maximum acceptable impairment/reduction in efficacy observed in patients undergoing the experimental treatment as compared to those undergoing the reference treatment. In other words, the margin is the maximum value of the effect difference between experimental and control treatment that can be acceptable to still consider the former non‐inferior to the latter. For the present study, we will consider a margin of 20%: in other words the CI of the summary HR (resulting from the intermittent versus continuous schedule comparison) should not cross the value of 1.2 for the experimental schedule to be considered non‐inferior to the reference schedule.
We chose the 20% margin based on the clinical (and ethical) consideration that an experimental treatment could be of clinical value if it is less toxic than the comparator treatment and if its efficacy is not worse than the comparator by more than 20%, a margin often used in the oncology field (especially in the metastatic setting, where even larger margins are often accepted) (Hong 2012; Hu 2015; Muro 2010; Tsuburaya 2014; Yamada 2013). Moreover, the conclusion of a recent meta‐analysis on the same subject further justifies the use of this margin as the difference between the two treatments was lower than the margin we chose (Berry 2015). The constancy assumption for non‐inferiority approach is likely to be met because, to the best of our knowledge, we have no reason to believe that over time changes have occurred in disease or outcome which could negatively have affected the choice of the margin.
We have presented a schematic on how to interpret all possible results of the meta‐analysis in the non‐inferiority perspective in Figure 2.

Non‐inferiority interpretation of meta‐analysis findings
Intention‐to‐treat (ITT) analysis is usually considered as an unbiased approach for superiority trials. However, ITT analysis may not be conservative in the case of non‐inferiority trials (inclusion of dropouts tends to bias the findings toward equivalence). Accordingly, we will retrieve data from both ITT and per‐protocol analysis; then we will assess the impact of the type of analysis (or the lack of such a type of information) by means of sensitivity analysis. Regarding the ITT analysis, for dropouts we will consider the best‐case and worst‐case scenarios. We will retrieve data from both the ITT and per‐protocol analysis, and then we will assess the impact of the type of analysis by means of sensitivity/subgroup analysis. We will determine the impact of the type of analysis by means of sensitivity/subgroup analysis. Regarding toxicity, we will consider best‐case and worst‐case scenarios in the analyses.
We will enter survival data (HRs and corresponding CI) directly in RevMan when reported (RevMan 2014); when unavailable, we will extrapolate them from Kaplan‐Meier survival curves using dedicated methods (Parmar 1998; Tierney 2007).
If the included studies report continuous outcomes using different scales, we will ensure that higher scores have the same meaning for any particular outcome; furthermore, we will report in which cases the effect direction will be reversed to guarantee consistency across results and thus to correctly pool the data.
Subgroup analysis and investigation of heterogeneity
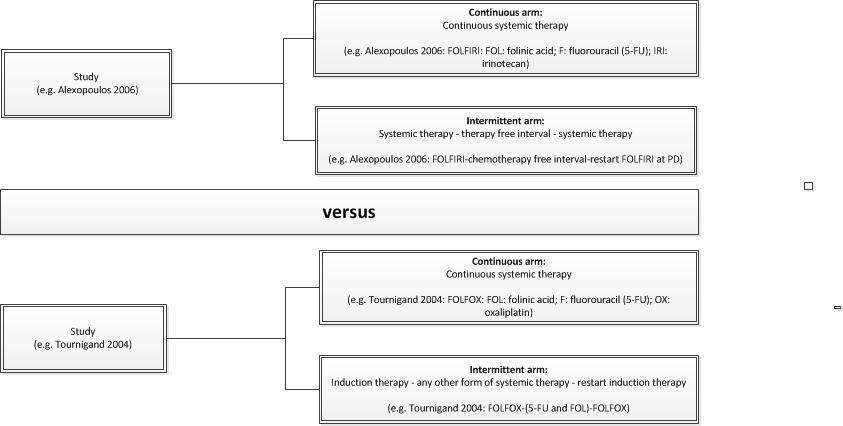
In order to investigate the potential sources of heterogeneity, we will consider the following pre‐specified subgroups (also see Figure 3): a subgroup of studies where the arm of intermittent chemotherapy has:

Planned subgroup analysis
-
no maintenance therapy (therapy‐free interval); versus
-
has any (simplified) form of systemic therapy (after induction chemotherapy)
Within these subgroups, our interpretation of the results in terms of survival will follow the non‐inferiority design described in the above paragraph.
Sensitivity analysis
We will use sensitivity analysis to assess the robustness of the meta‐analysis findings. To achieve this we will investigate whether exclusion of lower quality trials or exclusion of trials reporting per‐protocol analysis results (or not reporting the type of analysis) changes the results of our meta‐analysis. Moreover, we will use sensitivity analysis by excluding trials with specific trial characteristics (e.g. cluster‐RCTs, crossover trials and differences in between studies regarding the moment of randomisation) to assess whether specific trial features (e.g. design) might affect heterogeneity. If this is the case, the interpretation of results in terms of survival will follow the non‐inferiority design described in the above paragraph.
Quality of the evidence
We will use the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) system to assess the quality of evidence for the listed outcomes as at one of four levels (Guyatt 2011).
| Grade | Definition |
| High | Further research is very unlikely to change our confidence in the estimate of effect |
| Moderate | Further research is likely to have an impact on our confidence in the estimate of effect and may change the estimate |
| Low | Further research is very likely to have an important impact on our confidence on the estimate of effect and is likely to change the estimate |
| Very low | Any estimate of effect is very uncertain |
The quality of evidence can be downgraded by one (serious concern) or two levels (very serious concern) for the following reasons: risk of bias (see Assessment of risk of bias in included studies), inconsistency (unexplained heterogeneity, inconsistency of results), indirectness (indirect population, intervention, control, outcomes) and imprecision (wide CI, single trial).
We will create the ‘Summary of findings' table using the GRADEpro software (GRADEpro 2014). We will use the general template and other requirements as stated by the Cochrane Handbook for Systematic Reviews of Interventions chapter 11 (Higgins 2011c).
For the primary outcomes (overall survival and toxicity), we will report the main results of the meta‐analysis in ‘Summary of findings' table(s), as recommended by Higgins 2011. We will use the GRADEpro Guideline Development Tool (GDT) to create the 'Summary of findings' table(s) (GRADEpro 2014).
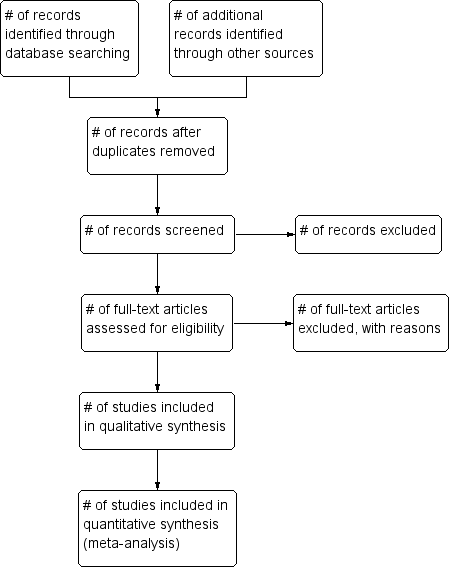
Study flow diagram.
Non‐inferiority interpretation of meta‐analysis findings
Planned subgroup analysis
| Table 1. Examples of intermittent versus continuous treatment schemes | |
| 1. | Intermittent: FOLFOX17, 12 weeks; sLV5‐FU22, 24 weeks; FOLFOX7, 12 weeks |
| Continuous: FOLFOX4 every 2 weeks until progression of disease (PD) (Tournigand 2004) | |
| 2. | Intermittent: FOLFIRI3, 12 weeks; chemotherapy‐Free‐Interval (CFI); restart FOLFIRI at PD |
| Continuous: FOLFIRI, 24 weeks (Alexopoulos 2006) | |
| 3. | Intermittent: Bevacizumab + capecitabine/oxaliplatin, 18 weeks; CFI; restart Bevacizumab+ capecitabine/oxaliplatin at PD |
| Continuous: Bevacizumab + capecitabine/oxaliplatin, 18 weeks; bevacizumab+capecitabine, restart bevacizumab+capecitabine/oxaliplatin at PD (Simkens 2015) | |
| 1 FOLFOX: FOL: folinic acid; F: fluorouracil (5‐FU); OX: oxaliplatin. | |