Yoga versus atención no habitual para la esquizofrenia
Información
- DOI:
- https://doi.org/10.1002/14651858.CD012052.pub2Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 28 septiembre 2017see what's new
- Tipo:
-
- Intervention
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Esquizofrenia
- Copyright:
-
- Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
Julie Broderick: writing the protocol and writing the review.
Niall Crumlish: development of the protocol and contributing to writing the review.
Alice Waugh: development of the protocol and contributing to writing the review.
Davy Vancampfort: development of the protocol contributing to writing the review.
Sources of support
Internal sources
-
Trinity Centre for Health Sciences, Dublin, Ireland.
Employs lead author Julie Broderick.
-
St. James Hospital, Dublin, Ireland.
Employs review authors Niall Crumlish and Alice Waugh.
-
Katholieke Universiteit Leuven, Leuven, Belgium.
Employs review author Davy Vancampfort.
External sources
-
Health Research Board, Ireland.
This review was conducted as part of a series of reviews which were funded by a Cochrane Fellowship Grant (CFT‐2014‐880).
Declarations of interest
Julie Broderick: "This work was supported by a Cochrane Training Fellowship funded by the Health Research Board, Ireland. This consisted of protected time to write this review and support for relevant training".
Niall Crumlish: none known.
Alice Waugh: none known.
Davy Vancampfort: none known.
Acknowledgements
The review authors would like to thank Professor Clive E Adams for the opportunity to perform this series of reviews and for his advice throughout, as well as the staff of the Cochrane Schizophrenia Group Editorial Base, particularly Claire Irving, for their support in the writing of the protocol and review. The Cochrane Schizophrenia Group Editorial Base in Nottingham, UK, produces and maintains standard text for use in the Methods section of their reviews, and the review authors have used this text as the basis for what appears here, adapting it as required. The review authors have also used and adapted their previous description of yoga, first published in 'Yoga versus standard care for schizophrenia' (Broderick 2015). This review is part of a series of reviews (Table 1) to populate an overview. As such, there is some consistency between reviews to streamline content for the forthcoming overview.
The review authors would also like to thank the Information Scientist of the Cochrane Schizophrenia Group, Farhad Shokraneh, who developed the search strategy.
We would also like to thank and acknowledge Genevieve Gariepy for peer reviewing this version of the review.
Parts of this review were drafted using RevMan HAL v 4.2. You can find more information about RevMan HAL here.
Version history
| Published | Title | Stage | Authors | Version |
| 2017 Sep 28 | Yoga versus non‐standard care for schizophrenia | Review | Julie Broderick, Niall Crumlish, Alice Waugh, Davy Vancampfort | |
| 2016 Jan 21 | Yoga versus non‐standard care for schizophrenia | Protocol | Julie Broderick, Niall Crumlish, Alice Waugh, Davy Vancampfort | |
Differences between protocol and review
Renaming of non‐standard care intervention from Non‐standard care or approaches (in addition to standard care) to Non‐standard care: We have removed the 'in addition to standard care' to clarify that both interventions would be 'in addition to standard care', and to keep the interventions the same as the published title.
Some updating of the text in the methods section to reflect changes in Schizophrenia Group's methods template.
Changing of wording of outcomes from 'clinically significant response' to 'clinically important change' in line with current Schizophrenia Group template. Specified outcomes in the 'Summary of findings' table should be 'clinically important'.
As no relapse data were available, we presented 'relapse' as a blank row in the 'Summary of findings' table but added 'leaving the study early' data. This was not prespecified in our protocol.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
Medical Subject Headings Check Words
Humans;
PICO

37Study flow diagram for 2015 searches

'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.

Comparison 1 YOGA versus NON‐STANDARD CARE, Outcome 1 Mental state: 1. Clinically important change (PANSS ‐ not improved) short term.

Comparison 1 YOGA versus NON‐STANDARD CARE, Outcome 2 Mental state: 2. Average endpoint score (various scales) short term.
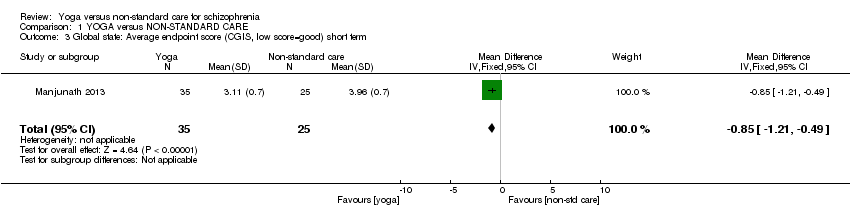
Comparison 1 YOGA versus NON‐STANDARD CARE, Outcome 3 Global state: Average endpoint score (CGIS, low score=good) short term.

Comparison 1 YOGA versus NON‐STANDARD CARE, Outcome 4 Social functioning: 1. Clinically important change (SOFS ‐ not improved) short term.

Comparison 1 YOGA versus NON‐STANDARD CARE, Outcome 5 Social functioning: 2. Average score at endpoint (two scales).
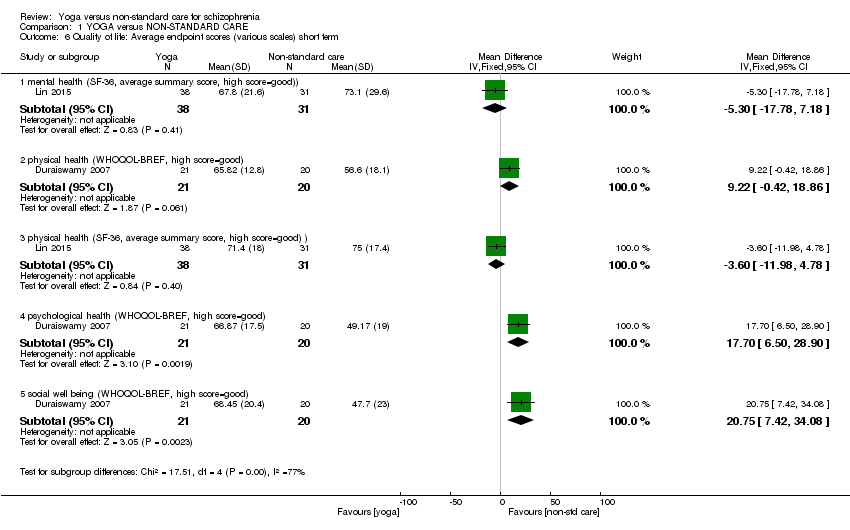
Comparison 1 YOGA versus NON‐STANDARD CARE, Outcome 6 Quality of life: Average endpoint scores (various scales) short term.

Comparison 1 YOGA versus NON‐STANDARD CARE, Outcome 7 Adverse effects.

Comparison 1 YOGA versus NON‐STANDARD CARE, Outcome 8 Leaving the study early ‐ short term.
| Intervention | plus | Control | Participants | Reference tag | Relevant Cochrane review |
| Yoga | nil | standard care | people with schizophrenia | Behere 2011; Ikai 2013; Ikai 2014; Jayaram 2013; Lin 2006;Lin 2015;Varambally 2012a; Visceglia 2011 | Yoga versus standard care for schizophrenia |
| counselling | standard care | ||||
| motivational and feedback session | |||||
| nil | caregivers of people with schizophrenia | ||||
| Yoga | non‐standard care | people with schizophrenia | Yoga as part of a package of care versus non‐standard care | ||
| Chlorpromazine | nil | placebo | Chlorpromazine versus placebo for schizophrenia | ||
| 'Tagara' (local drug with anti‐psychotic properties) and 'Brahmyadiyoga' (a herbal compound) | nil | Chlorpromazine versus herbal compounds for schizophrenia | |||
| chlorpromazine | |||||
| * This particular study used yoga combined with relaxation exercises, breathing exercises, body movement exercises, basic acting exercises, the Alexander technique, theatre games, exercise ''to build self confidence'', creative work using props, use of music to enhance creativity and moods. | |||||
| Methods | Allocation: randomised (clearly described). |
| Participants | Diagnosis: people with a clinical diagnosis of schizophrenia. |
| Interventions | 1. Yoga: the yoga intervention should be clearly described and consist of the following components; (i) shithileekarana vyayama (loosening exercises) for approximately 10 minutes (ii) yoga postures (asanas) for approximately 20 minutes (iii) breathing exercises and relaxation techniques for approximately 20 minutes using a manualised protocol, yoga programme for 12 weeks, 3 times weekly, follow‐up at 6 months and 1 year, yoga delivered by a trained yoga instructor, meditation not included. 2. Standard care control*. All groups stable pharmacotherapy. |
| Outcomes | Mental state (binary outcomes). Relapses (binary outcomes). QOL (binary outcomes). Disability (binary outcomes). Activities of daily living (binary outcomes). Costs: cost of services, cost of care. Adverse events related to yoga (number and type of injuries). Service outcomes: days in hospital, time attending outpatient psychiatric clinic. |
| Notes | Adherence should be logged with patients expected to adhere to 70% to 75% of scheduled sessions. * Regarding design of a future study, readers are directed to the first yoga review in this series (Broderick 2015) ‐ as a comprehensive yoga versus standard care study has not yet been published, this would be the initial priority. When this is conducted, many legitimate active comparators to yoga could be suggested; such as, but not limited to the following; yoga versus talking therapy, yoga versus expressive therapies, yoga versus other forms of exercise such as Tai'chi. |
| Intervention | plus | Active Comparator Broad Group | Specific interventions* |
| Yoga | nil | expressive therapy | art therapy |
| drama therapy | |||
| music therapy | |||
| dance therapy | |||
| writing therapy | |||
| talking therapies | cognitive behavioural therapy | ||
| dialectic behaviour therapy | |||
| humanistic therapies | |||
| exercise | aerobic‐based interventions | ||
| combined aerobic and resistance programme | |||
| resistance‐based interventions | |||
| Tai'chi | |||
| qi'gong | |||
| *This list of specific interventions is not exhaustive and merely provides some examples of legitimate active comparators to yoga which are not currently available. These interventions could also be considered alternatively. For instance, exercise consists of heterogeneous interventions, it is accepted there could be other equally justifiable intervention titles such as 'supervised' exercise, 'non‐supervised exercise', or 'group‐based exercise', 'individual exercise', or exercise could be considered in terms of intensity such as 'high intensity', 'moderate intensity' and 'low intensity'. Note the specific intervention should be delivered by suitably qualified personnel. | |||
| YOGA versus NON‐STANDARD CARE for schizophrenia | ||||||
| Patient or population: people with schizophrenia | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | YOGA versus NON‐STANDARD CARE | |||||
| Mental state: clinically important change Follow‐up: 4 months | Low1 | RR 0.81 | 84 | ⊕⊕⊝⊝ | ||
| 800 per 1000 | 648 per 1000 | |||||
| Moderate1 | ||||||
| 900 per 1000 | 729 per 1000 | |||||
| High1 | ||||||
| 1000 per 1000 | 810 per 1000 | |||||
| Global state: relapse | No trial reported this outcome. | |||||
| Social functioning: clinically important change | Low1 | RR 0.90 | 84 | ⊕⊕⊝⊝ | ||
| 700 per 1000 | 630 per 1000 | |||||
| Moderate1 | ||||||
| 900 per 1000 | 810 per 1000 | |||||
| Adverse effects ‐ any | See comment | See comment | Not estimable | 85 | ⊕⊕⊕⊝ | Risks were calculated from pooled risk differences. The study reported no adverse effects. |
| Quality of life: clinically important change SF‐36 average change score mental health * | The mean quality of life: average change ‐ mental health in the intervention (yoga) groups was | 69 | ⊕⊕⊝⊝ | * no trial reported binary data; we chose 1 of 2 QOL measures as proxy measure | ||
| Physical health: clinically important change WHQOL‐BREF ‐ average change score * | The mean physical health: average change in the intervention (yoga) groups was | 41 | ⊕⊕⊝⊝ | * no trial reported binary data; we chose physical health dimension of QOL measure as proxy measure. | ||
| Costs: direct and indirect costs of care | No trial reported this outcome. | |||||
| Leaving the study early: short term | Low1 | RR 0.64 | 586 | ⊕⊕⊕⊝ | ||
| 200 per 1000 | 120 per 1000 | |||||
| Moderate1 | ||||||
| 400 per 1000 | 240 per 1000 | |||||
| High1 | ||||||
| 600 per 1000 | 360 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence CI: confidence interval; RR: risk ratio | ||||||
| 1 Moderate risk approximates to that of non‐standard care in trial(s). 3 Imprecision: Downgraded one level due to small sample size 7 Imprecision: Downgraded one level as based on one study with no reported adverse events. 8 Risk of bias: Downgraded one level as a number of participants withdrew from one trial and it was not clear to which group they were randomised. | ||||||
| Review title | Status |
| Yoga versus standard care for schizophrenia | Full review: Broderick 2015 |
| Yoga versus non‐standard care for schizophrenia | This review. |
| Yoga as part of a package of care versus standard care | Protocol: Broderick 2016b |
| Yoga as part of a package of care versus non‐standard care |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Mental state: 1. Clinically important change (PANSS ‐ not improved) short term Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 overall | 1 | 84 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.81 [0.62, 1.07] |
| 1.2 specific ‐ negative symptoms | 1 | 84 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.57, 0.90] |
| 1.3 specific ‐ positive symptoms | 1 | 84 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.84, 1.38] |
| 2 Mental state: 2. Average endpoint score (various scales) short term Show forest plot | 4 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1 overall (PANSS) | 3 | 170 | Mean Difference (IV, Fixed, 95% CI) | ‐4.69 [‐8.35, ‐1.03] |
| 2.2 specific ‐ depressive symptoms (CDS) | 1 | 69 | Mean Difference (IV, Fixed, 95% CI) | 0.10 [‐1.01, 1.21] |
| 2.3 specific ‐ depressive symptoms (HDRS) | 1 | 60 | Mean Difference (IV, Fixed, 95% CI) | ‐1.41 [‐2.40, ‐0.42] |
| 2.4 specific ‐ negative symptoms (PANSS) | 4 | 214 | Mean Difference (IV, Fixed, 95% CI) | ‐1.15 [‐2.30, 0.01] |
| 2.5 specific ‐ positive symptoms (PANSS) | 4 | 214 | Mean Difference (IV, Fixed, 95% CI) | ‐0.36 [‐1.35, 0.63] |
| 3 Global state: Average endpoint score (CGIS, low score=good) short term Show forest plot | 1 | 60 | Mean Difference (IV, Fixed, 95% CI) | ‐0.85 [‐1.21, ‐0.49] |
| 4 Social functioning: 1. Clinically important change (SOFS ‐ not improved) short term Show forest plot | 1 | 84 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.78, 1.04] |
| 5 Social functioning: 2. Average score at endpoint (two scales) Show forest plot | 1 | 88 | Mean Difference (IV, Fixed, 95% CI) | 3.20 [‐0.57, 6.97] |
| 5.1 SOFS, high score=good | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 3.70 [‐0.70, 8.10] |
| 5.2 Emotional recognition, TRACS, high score=good | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 1.80 [‐5.54, 9.14] |
| 6 Quality of life: Average endpoint scores (various scales) short term Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 6.1 mental health (SF‐36, average summary score, high score=good)) | 1 | 69 | Mean Difference (IV, Fixed, 95% CI) | ‐5.30 [‐17.78, 7.18] |
| 6.2 physical health (WHOQOL‐BREF, high score=good) | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | 9.22 [‐0.42, 18.86] |
| 6.3 physical health (SF‐36, average summary score, high score=good) ) | 1 | 69 | Mean Difference (IV, Fixed, 95% CI) | ‐3.60 [‐11.98, 4.78] |
| 6.4 psychological health (WHOQOL‐BREF, high score=good) | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | 17.70 [6.50, 28.90] |
| 6.5 social well being (WHOQOL‐BREF, high score=good) | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | 20.75 [7.42, 34.08] |
| 7 Adverse effects Show forest plot | 1 | Risk Difference (M‐H, Fixed, 95% CI) | Subtotals only | |
| 7.1 any serious | 1 | 85 | Risk Difference (M‐H, Fixed, 95% CI) | 0.0 [‐0.05, 0.05] |
| 7.2 others | 1 | 85 | Risk Difference (M‐H, Fixed, 95% CI) | 0.0 [‐0.05, 0.05] |
| 8 Leaving the study early ‐ short term Show forest plot | 6 | 586 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.51, 0.86] |