Clorpromazina versus penfluridol para la esquizofrenia
Información
- DOI:
- https://doi.org/10.1002/14651858.CD011831.pub2Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 23 septiembre 2017see what's new
- Tipo:
-
- Intervention
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Esquizofrenia
- Copyright:
-
- Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
Navid Khalili: Wrote the protocol, discussed allocation of responsibility for the tasks, selection of studies, data extraction, edited the Cochrane Schizophrenia Group template for the methods section, contributed in entering data in the Review Manager (RevMan) software, substantially contributed in writing and completing the primary draft of the manuscript and read and approved the final version of the review.
Mostafa Vahedian: Discussed allocation of responsibility for the tasks, selection of studies, data extraction, edited the Cochrane Schizophrenia Group template for the methods section, contributed in entering data in RevMan substantially contributed in writing and completing the primary draft of the manuscript and read and approved the final version of the review.
Naemeh Nikvarz: Discussed allocation of responsibility for the tasks, selection of studies, data extraction, contributed in entering data in RevMan and Grade profiler software, substantially contributed in writing and completing the primary draft of the manuscript and critically revised it and read and approved the final version of the review.
Sources of support
Internal sources
-
Kerman University of Medical Sciences, Kerman, Iran.
Employs lead author Naemeh Nikvarz and review author Navid Khalili. Review author Mostafa Vahedian is a student at this university.
External sources
-
No sources of support supplied
Declarations of interest
NK: No conflict of interest.
MV: No conflict of interest.
NN: No conflict of interest.
Acknowledgements
The Cochrane Schizophrenia Group Editorial Base in Nottingham produces and maintains standard text for use in the Methods section of their reviews. We have used this text as the basis of what appears here and adapted it as required.
The search term was developed by the Information Specialist of the Cochrane Schizophrenia Group and the contact author of this protocol. Jun Xia from Systematic Review Solutions extracted data of Chinese studies. We would like to thank Jamie Majdi and Pippa Shaw for peer reviewing this version of the review.
Parts of this review were generated using RevMan HAL v 4.0. You can find more information about RevMan here.
Version history
| Published | Title | Stage | Authors | Version |
| 2017 Sep 23 | Chlorpromazine versus penfluridol for schizophrenia | Review | Naemeh Nikvarz, Mostafa Vahedian, Navid Khalili | |
| 2015 Aug 15 | Chlorpromazine versus penfluridol for schizophrenia | Protocol | Navid Khalili, Mostafa Vahedian, Naemeh Nikvarz, Mojtaba Piri | |
Differences between protocol and review
We have reworded and regrouped the outcomes to more closely reflect the latest Cochrane Schizophrenia Group's methods template. Originally, the outcome of the adverse event/effect of death was the first outcome on our preferred 'Summary of fIndings' list. This seemed to strike an unfortunate, unwanted and inaccurate emphasis and for the full review we reordered outcomes.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
Medical Subject Headings Check Words
Adult; Humans;
PICO

Chlorpromazine structure
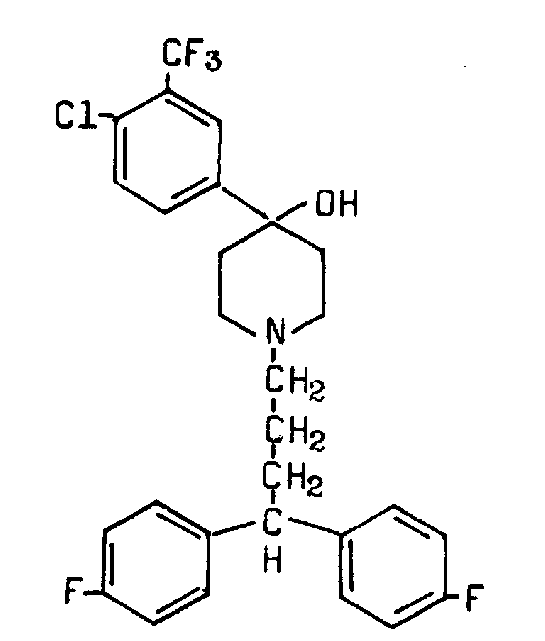
Penfluridol structure

Study flow diagram.
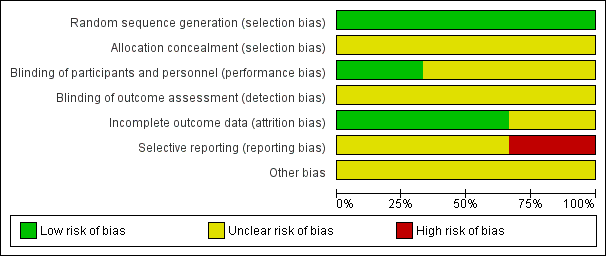
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
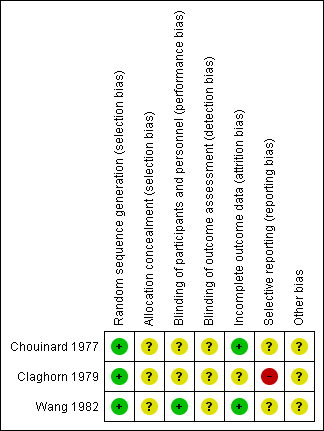
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.

Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 1 Service utilisation: 1. Hospital readmission.

Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 2 Adverse effects: 1a. General ‐ needing antiparkinsonian medication.

Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 3 Adverse effects: 1b. General ‐ need to reduce antipsychotic dose due to side effects.

Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 4 Adverse effects: 2a. Specific ‐ extrapyramidal events (moderate or severe) ‐ short term.

Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 5 Adverse effects: 2b. Specific ‐ extrapyramidal events (moderate or severe) ‐ medium term.

Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 6 Adverse effects: 2c. Specific ‐ anticholinergic (moderate or severe) ‐ short term.
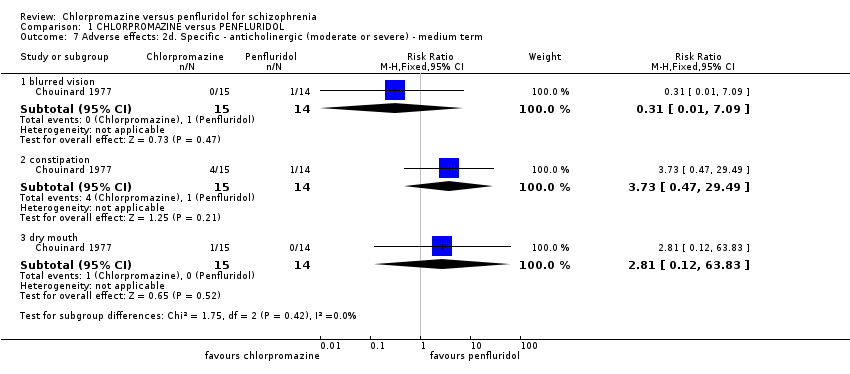
Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 7 Adverse effects: 2d. Specific ‐ anticholinergic (moderate or severe) ‐ medium term.

Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 8 Adverse effects: 2e. Specific ‐ central nervous system (moderate or severe) ‐ short term.

Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 9 Adverse effects: 2f. Specific ‐ central nervous system (moderate or severe) ‐ medium term.
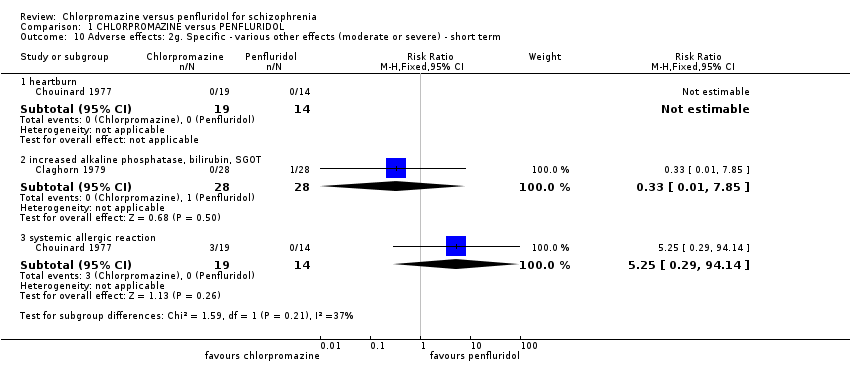
Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 10 Adverse effects: 2g. Specific ‐ various other effects (moderate or severe) ‐ short term.

Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 11 Adverse effects: 2h. Specific ‐ various other effects (moderate or severe) ‐ medium term.

Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 12 Leaving the study early: 1a. Any reason.

Comparison 1 CHLORPROMAZINE versus PENFLURIDOL, Outcome 13 Leaving the study early: 1b. Due to adverse events.
| Methods | Allocation: randomised, fully explicit description of methods of randomisation and allocation concealment. |
| Participants | Diagnosis: schizophrenia. |
| Interventions | 1. Chlorpromazine: oral‐maximum around 400 mg/day. N = 150. 2. Penfluridol: oral‐maximum around 80 mg/week. N = 150. Both groups could receive antiparkinsonian medication as required. |
| Outcomes | Service utilisation: Hospital admission, time to admission. Global state: Clinically significant response in global state, relapse. Mental state: Clinically significant response in mental state. Adverse effects: Clinically significant extrapyramidal side effects, death. Leaving the study early. Functioning: Employed, days working, in supportive relationship, healthy days. Economic outcomes. |
| Notes | * Powered to be able to identify a difference of ˜ 20% between groups for primary outcome with adequate degree of certainty. |
| Chlorpromazine versus Penfluridol for schizophrenia | ||||||
| Patient or population: patients with schizophrenia | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk3 | Corresponding risk | |||||
| Penfluridol | Chlorpromazine | |||||
| Service utilisation: hospital admission (short term) | 150 per 1000 | 28 per 1000 | RR 0.19 (0.01 to 3.60) | 29 | ⊕⊕⊝⊝ low 1,2 | |
| Global state: clinically important change in global state | See comment | Not estimable | 0 | See comment | No studies reported 'clinically important change in global state'. Change in global state was measure using global state scales but all data were presented without SD. | |
| Global state: relapse | See comment | Not estimable | 0 | See comment | No studies reported this outcome. | |
| Mental state: clinically important change in mental state | See comment | Not estimable | 0 | See comment | No studies reported 'clinically important change in mental state'. Change in mental state was measure using mental state scales but all data were presented without SD. | |
| Adverse effect/event: clinically important extrapyramidal adverse events ‐ akathisia (medium term) | 200 per 1000 | 38 per 1000 | RR 0.19 (0.04 to 1.06) | 85 | ⊕⊕⊝⊝ low 1,2 | The same studies reported data for other extrapyramidal adverse events such as rigidity, tremor, dystonia and dyskinesia. There was no observable difference between chlorpromazine and penfluridol regarding any of these adverse effects. |
| Adverse effect/event: death | See comment | Not estimated | 2 RCTs (0) | See comment | No deaths reported. | |
| Leaving the study early: any reason (medium term) | 400 per 1000 | 484 per 1000 | RR 1.21 (0.83 to 1.77) | 130 | ⊕⊕⊝⊝ low 1,2 | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Serious risk of bias: downgraded by one level ‐ study had an unclear risk of bias for random sequence generation and blinding of assessors. | ||||||
| Review title | Reference |
| Acetophenazine versus chlorpromazine | |
| Chlorpromazine dose for people with schizophrenia | |
| Cessation of medication for people with schizophrenia already stable on chlorpromazine | |
| Chlorpromazine versus atypical antipsychotic drugs for schizophrenia | |
| Chlorpromazine versus clotiapine for schizophrenia | Developing protocol |
| Chlorpromazine versus haloperidol for schizophrenia | |
| Chlorpromazine versus metiapine | |
| Chlorpromazine versus penfluridol for schizophrenia | Current review |
| Chlorpromazine versus piperacetazine | |
| Chlorpromazine versus placebo for schizophrenia | |
| Chlorpromazine for psychosis induced aggression or agitation |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Service utilisation: 1. Hospital readmission Show forest plot | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.19 [0.01, 3.60] |
| 1.1 short term | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.19 [0.01, 3.60] |
| 2 Adverse effects: 1a. General ‐ needing antiparkinsonian medication Show forest plot | 2 | 74 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.70 [0.51, 0.95] |
| 2.1 short term | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.46, 1.46] |
| 2.2 medium term | 1 | 41 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.63 [0.43, 0.91] |
| 3 Adverse effects: 1b. General ‐ need to reduce antipsychotic dose due to side effects Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 medium term | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.74 [0.26, 2.06] |
| 4 Adverse effects: 2a. Specific ‐ extrapyramidal events (moderate or severe) ‐ short term Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4.1 akatisia | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.2 dyskinesia | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.3 dystonia | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.4 rigidity | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.15 [0.01, 2.90] |
| 4.5 tremor | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5 Adverse effects: 2b. Specific ‐ extrapyramidal events (moderate or severe) ‐ medium term Show forest plot | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.1 akathisia | 2 | 85 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.19 [0.04, 1.06] |
| 5.2 dyskinesia | 2 | 85 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.14, 6.52] |
| 5.3 dystonia | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.06, 13.54] |
| 5.4 muscle spasm | 1 | 56 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.0 [0.13, 70.64] |
| 5.5 rigidity | 2 | 70 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.22 [0.04, 1.20] |
| 5.6 tremor | 2 | 85 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.70 [0.14, 3.43] |
| 6 Adverse effects: 2c. Specific ‐ anticholinergic (moderate or severe) ‐ short term Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 6.1 constipation | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.42 [0.60, 32.71] |
| 6.2 dry mouth | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.25 [0.10, 51.46] |
| 6.3 increased salivation | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.25 [0.01, 5.72] |
| 7 Adverse effects: 2d. Specific ‐ anticholinergic (moderate or severe) ‐ medium term Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 7.1 blurred vision | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.31 [0.01, 7.09] |
| 7.2 constipation | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.73 [0.47, 29.49] |
| 7.3 dry mouth | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.81 [0.12, 63.83] |
| 8 Adverse effects: 2e. Specific ‐ central nervous system (moderate or severe) ‐ short term Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 8.1 agitation | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.25 [0.10, 51.46] |
| 8.2 drowsiness | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 8.25 [0.49, 137.94] |
| 8.3 dizziness | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.25 [0.03, 2.12] |
| 8.4 insomnia | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.25 [0.10, 51.46] |
| 9 Adverse effects: 2f. Specific ‐ central nervous system (moderate or severe) ‐ medium term Show forest plot | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 9.1 drowsiness | 2 | 85 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.54, 2.05] |
| 9.2 dizziness | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.47 [0.05, 4.60] |
| 9.3 excitement | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.81 [0.12, 63.83] |
| 9.4 faintness | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.15, 5.76] |
| 9.5 insomnia | 2 | 85 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.17 [0.03, 0.93] |
| 10 Adverse effects: 2g. Specific ‐ various other effects (moderate or severe) ‐ short term Show forest plot | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 10.1 heartburn | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 10.2 increased alkaline phosphatase, bilirubin, SGOT | 1 | 56 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.01, 7.85] |
| 10.3 systemic allergic reaction | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 5.25 [0.29, 94.14] |
| 11 Adverse effects: 2h. Specific ‐ various other effects (moderate or severe) ‐ medium term Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 11.1 depression | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.19 [0.01, 3.60] |
| 11.2 decreased sexual drive | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.47 [0.05, 4.60] |
| 11.3 impotence | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.81 [0.12, 63.83] |
| 11.4 photosensitivity | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.81 [0.12, 63.83] |
| 11.5 poor appetite | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.06, 13.54] |
| 12 Leaving the study early: 1a. Any reason Show forest plot | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 12.1 medium term | 3 | 130 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.21 [0.83, 1.77] |
| 13 Leaving the study early: 1b. Due to adverse events Show forest plot | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 13.1 short term | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 6.75 [0.39, 116.00] |
| 13.2 medium term | 2 | 74 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.53 [0.72, 3.28] |