La Neonatal Behavioral Assessment Scale (Neonatal Behavioral Assessment Scale, NBAS por su sigla en inglés) y el sistema Newborn Behavioral Observations (Observaciones Conductuales del Recién Nacido, NBO por su sigla en inglés) para apoyar a los cuidadores y mejorar los resultados en los cuidadores y los lactantes
Información
- DOI:
- https://doi.org/10.1002/14651858.CD011754.pub2Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 14 marzo 2018see what's new
- Tipo:
-
- Intervention
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Problemas de desarrollo, psicosociales y de aprendizaje
- Copyright:
-
- Copyright © 2018 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
Contact author and guarantor of the review: JB.
Drafting of protocol: JB and CBT.
Study selection: JB, CBT and NH.
Data extraction: JB, NH and CB.
Assessment of study quality, including risk of bias: JB, NH and CBT.
Data entry into RevMan 5: NH.
Analyses: JB, NH and YW.
Interpretation of analyses: JB and CBT.
Drafting of final review: JB NH and CBT.
Disagreement resolution: CBT.
Updating of review: JB and CBT.
Sources of support
Internal sources
-
None, Other.
External sources
-
None, Other.
Declarations of interest
Jane Barlow is an Editor with Cochrane Developmental, Psychosocial and Learning Problems and was Co‐Chair of the Campbell Social Welfare Group until May 2015.
Nadeeja INS Herath ‐ none known.
Christine Bartram Torrance (CBT) is certified in the Neonatal Behavioral Assessment Scale (NBAS) and Newborn Behavioral Observations (NBO) system. CBT is facilitating the NBAS as part of her collaboration with an observational study in West Africa and will train colleagues in its delivery, for which she will receive payment. In this study, CBT is responsible for conducting NBAS sessions and ensuring handover of her role to local staff members, including ensuring they are trained and certified in the NBAS. Both this review and the observational study are being conducted as part of her PhD. CBT delivers NBAS occasionally on a voluntary basis. CBT is not currently being paid for conducting the NBAS or NBO in her study and has not been paid for conducting them previously in voluntary roles. CBT expects to continue offering these sessions in a voluntary capacity in the future. In terms of support in training others in the NBAS, CBT has not been paid previously, but as CBT is certified, it is possible that she could be paid in the future for training or support in training, or for delivering the sessions in research or support capacities.
Cathy Bennett is the proprietor of Systematic Research Ltd. The company received a consultancy fee to enable CB to work as a co‐author of this review. CB has business relationships with other clients, who may provide consultancy fees for evidence‐based medicine reviews, projects and reports.
Yinghui Wei ‐ none known.
Acknowledgements
We thank the editorial team of Cochrane Developmental, Psychosocial and Learning Problems (Margaret Anderson, Joanne Wilson, and Geraldine Macdonald) for their support and advice. We also thank Jo Abbott, who undertook the searches, and the editor, external referees and statistician, who reviewed and commented on the protocol and earlier drafts of the review.
Version history
| Published | Title | Stage | Authors | Version |
| 2018 Mar 14 | The Neonatal Behavioral Assessment Scale (NBAS) and Newborn Behavioral Observations (NBO) system for supporting caregivers and improving outcomes in caregivers and their infants | Review | Jane Barlow, Nadeeja INS Herath, Christine Bartram Torrance, Cathy Bennett, Yinghui Wei | |
| 2015 Jun 21 | The Neonatal Behavioral Assessment Scale (NBAS) and Newborn Behavioral Observations system (NBO) for supporting caregivers and improving outcomes in caregivers and their infants | Protocol | Samantha Christine Bartram, Jane Barlow, Dieter Wolke | |
Differences between protocol and review
-
Review authors
-
Dieter Wolke left the review team, and Nadeeja Herath, who undertook a significant amount of the work on the review as part of her visiting fellowship to the UK, along with Cathy Bennett joined the review team.
-
-
Methods > Types of outcome measures
-
We refined our list of primary outcomes. We deleted 'infant attachment security' because the studies do not measure this outcome, and 'caregiver sensitivity and responsiveness', which duplicates 'caregiver interaction'. We moved 'caregiver reflective functioning' from our list of primary outcomes to our list of secondary outcomes because we felt it is not a primary outcome for change in studies of the NBAS/NBO.
-
We also refined our list of secondary outcomes by removing the outcome of 'caregiver involvement in caregiving activities and interaction' because it duplicated 'caregiver interaction'.
-
-
Methods > Searching other resources
-
We did not contact authors and experts in the field to identify unpublished studies because these studies are all registered with the National Brazelton Institute, who provided us with the necessary information.
-
-
Methods > Data extraction and management
-
Nadeeja Herath extracted the data, with Jane Barlow conducting a check of all extracted data due to time limitations.
-
-
Methods > Assessment of risk of bias in included studies
-
Nadeeja Herath assessed the risk of bias in included studies, with Jane Barlow conducting checks of all assessments due to time limitations.
-
-
summary of findings Table for the main comparison
-
It was not possible to populate summary of findings Table for the main comparison with data on 'infant attachment security' or 'caregiver reflective functioning' because these were not measured in the included studies. We did, however, provide information about 'quality of caregiver‐infant interaction', 'caregiver mental health', 'infant social, emotional, cognitive and motor development', 'caregiver perception of infant', and 'caregiver knowledge' because these were key outcomes of interest, all of which were measured in the included studies.
-
-
In addition, we were unable to use some of our methods, as specified in our protocol (Bartram 2016). These are reported in Table 1.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
Medical Subject Headings Check Words
Humans; Infant, Newborn;
PICO
Study flow diagram.

Risk of bias summary: review authors' judgments about each risk of bias item for each included study.

Risk of bias graph: review authors' judgments about each risk of bias item presented as percentages across all included studies.

Comparison 1 NBAS or NBO versus control, Outcome 1 Quality of caregiver‐infant interaction: postintervention.

Comparison 1 NBAS or NBO versus control, Outcome 2 Caregiver mental health (maternal depression): EPDS postintervention score.
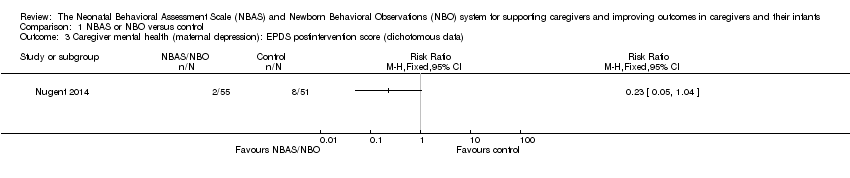
Comparison 1 NBAS or NBO versus control, Outcome 3 Caregiver mental health (maternal depression): EPDS postintervention score (dichotomous data).

Comparison 1 NBAS or NBO versus control, Outcome 4 Infant social, emotional, cognitive and motor development.

Comparison 1 NBAS or NBO versus control, Outcome 5 Caregiver perception of infant.
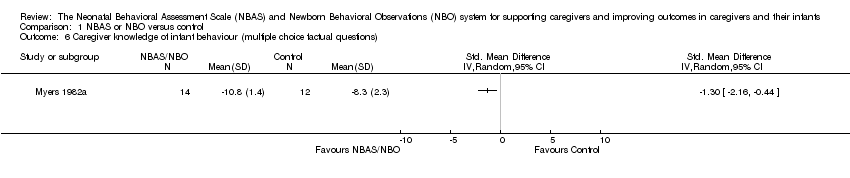
Comparison 1 NBAS or NBO versus control, Outcome 6 Caregiver knowledge of infant behaviour (multiple choice factual questions).

Comparison 1 NBAS or NBO versus control, Outcome 7 Caregiver stress.

Comparison 2 NBAS or NBO versus control: subgroup analysis, Outcome 1 Quality of caregiver‐infant interaction.
| NBAS or NBO versus control for caregiver‐infant interaction, caregiver mental health, and caregiver functioning | |||||
| Patient or population: caregiver‐infant dyads Settings: hospitals, clinics, home Intervention: NBAS or NBO Comparison: NBAS or NBO administered with no interaction | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | Number of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Control group | NBAS or NBO | ||||
| Quality of caregiver‐infant interaction (parental sensitivity, attunement, etc.); continuous data Assessed at postintervention using validated assessment scales for caregiver‐infant interaction: higher scores indicate better outcome | The mean score for quality of caregiver‐infant interaction ranged across control groups from 3.72 to 51.90 | The mean caregiver‐infant interaction score in the intervention groups was 0.53 lower (0.90 lower to 0.17 lower) | — | 304 | ⊕⊕⊝⊝ |
| Caregiver mental health (depression), dichotomous data Assessed at postintervention using the EPDS; lower scores indicate less depression | Low‐risk population | RR 0.23 (0.05 to 1.04) | 106 (1 study) | ⊕⊕⊝⊝ | |
| 157 per 1000 | 36 per 1000 (8 to 163) | ||||
| Medium‐risk population | |||||
| NA | NA | ||||
| High‐risk population | |||||
| NA | NA | ||||
| Infant social, emotional, cognitive and motor development Assessed when infant aged 4 months, using the BSID; higher scores indicate better development | The mean score for infant mental development in the control group was 107.83 | The mean score for infant mental development in the intervention groups was0.13 lower (0.48 lower to 0.22 higher) | — | 125 (1 study) | ⊕⊕⊝⊝ |
| Caregiver perception of infant (parents' perception of the degree of difficult temperament of the infant) Assessed at postintervention, 8 weeks after delivery; higher score indicates better outcome | The mean score for caregiver perception of infant in the control group was 18.90 | The mean score for caregiver perception of the infant in the intervention group was 0.36 lower (0.95 lower to 0.24 higher) | — | 44 (1 study) | ⊕⊕⊝⊝ |
| Caregiver stress (maternal perceptions of her adjustment to the parenting role) Assessed when infant aged 4 months, using the PSI | The mean score for parent‐related caregiver stress in the control group was 2.19 | The mean score for parent‐related caregiver stress in the intervention groups was0.00 (0.35 lower to 0.35 higher) | — | 125 (1 study) | ⊕⊕⊝⊝ |
| Caregiver knowledge (related to infants' physical capacities, including reflexes and senses) Assessed at postintervention, using multiple choice factual questions; higher scores indicate better outcome | The mean score for caregiver knowledge in the control groups was8.30 | The mean score for caregiver knowledge in the intervention groups was 1.30 higher (0.44 to 2.16 higher) | — | 26 (1 study) | ⊕⊕⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| 1Downgraded due to risk of bias due to poor quality research (e.g. limitations in design, including inadequate randomisation or allocation procedures, together with attrition, which ranged from 4% to 20% in seven studies – none of which conducted an intention‐to‐treat analysis), inconsistency for the main outcome due to high levels of heterogeneity for the NBAS; and indirectness in terms of the low levels of generalisability to wider risk groups within the population. 2Downgraded due to risk of bias due to poor quality research (e.g. limitations in design, including inadequate randomisation or allocation procedures, together with attrition, which ranged from 4% to 20% in seven studies – none of which conducted an intention‐to‐treat analysis), and indirectness in terms of the low levels of generalisability to wider risk groups within the population. | |||||
| Unit of analysis issues | Cluster‐randomised trials The randomisation of clusters can result in an overestimate of the precision of the results (with a higher risk of a type I error) when their use has not been compensated for in the analysis. Had we included a cluster‐RCT, we planned to explore whether the authors had adequately controlled for the effects of clustering in the study. When they had, and when there was little difference between the study designs, and when there was unlikely to be an interaction between the effect of the intervention and the choice of randomisation method, we planned to combine the data from the cluster‐RCT with data from individual RCTs. When the effects of clustering had not been controlled for properly, we planned to derive an estimate of the intracluster correlation coefficient (ICC) from the study or that of a similar population, and to report whether an ICC had been used and conduct sensitivity analyses to determine the effect of using an ICC. We also planned to assess the impact of including data from a cluster‐RCT on the inclusion of the study in the meta‐analyses using a sensitivity analysis to explore the effects of the randomisation method. However, no cluster RCTs were identified or included. |
| Trials with multiple treatments groups In the event that we had identified a multi‐arm study in which the NBAS and NBO had been compared with an alternative treatment and a control group, we planned to only extract data from two arms (e.g. NBAS and control group). In the event that we had identified a multi‐arm study in which the NBAS had been compared with the NBO and involved only one control group, we planned to combine the data from the NBAS and NBO arms for primary analyses and to conduct secondary, subgroup analyses and split the control group data. However, we identified no multiple treatment groups. | |
| Cross‐over trials Cross‐over trials are not possible with this type of intervention, and none were identified. | |
| Assessment of reporting bias | We planned to draw funnel plots (estimated differences in treatment effects against their standard error) if there was a sufficient number of included studies (e.g. more than 10), to identify asymmetry due to publication bias and other small study effects. We also planned to assess whether there had been selective reporting of outcomes and to assess the impact of this using a sensitivity analysis. However, there were insufficient studies to undertake this analysis. |
| Subgroup analysis and investigation of heterogeneity | We planned to explore possible reasons for heterogeneity by undertaking the following, additional subgroup analyses, scrutinising studies to determine the extent of between‐trial differences.
However, it was only possible to undertake subgroup analysis for NBAS versus NBO, due to the small number of studies. |
| Sensitivity analysis | We planned to conduct sensitivity analyses on the basis of method of sequence generation only, to assess the robustness of the results, but this was not possible due to the small number of studies. |
| NBAS: Neonatal Behavioral Assessment Scale; NBO: Newborn Behavioral Observations system; RCT: randomised controlled trial. | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Quality of caregiver‐infant interaction: postintervention Show forest plot | 7 | 304 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.53 [‐0.90, ‐0.17] |
| 2 Caregiver mental health (maternal depression): EPDS postintervention score Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3 Caregiver mental health (maternal depression): EPDS postintervention score (dichotomous data) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4 Infant social, emotional, cognitive and motor development Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 BSID: mental development | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 BSID: psychomotor development | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Caregiver perception of infant Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 6 Caregiver knowledge of infant behaviour (multiple choice factual questions) Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7 Caregiver stress Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 PSI: parent‐related sources of stress | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 PSI: child‐related sources of stress | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Quality of caregiver‐infant interaction Show forest plot | 7 | 304 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.53 [‐0.90, ‐0.17] |
| 1.1 NBAS | 5 | 231 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.49 [‐0.99, ‐0.00] |
| 1.2 NBO | 2 | 73 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.69 [‐1.18, ‐0.20] |