Inmunoterapia oral y sublingual para la alergia al huevo
Resumen
Antecedentes
La alergia clínica al huevo es una alergia alimentaria común. El tratamiento actual se basa en evitar estrictamente los alérgenos. La inmunoterapia oral podría ser un tratamiento opcional mediante la desensibilización al alérgeno del huevo.
Objetivos
Determinar la eficacia y la seguridad de la inmunoterapia oral y sublingual en niños y adultos con alergia al huevo mediada por inmunoglobulina E (IgE) en comparación con un tratamiento de placebo o una estrategia de evitación.
Métodos de búsqueda
Se hicieron búsquedas de artículos de revistas en 13 bases de datos, actas de congresos, tesis y registros de ensayos, utilizando una combinación de encabezados temáticos y palabras de texto ( última búsqueda el 31 marzo de 2017).
Criterios de selección
Se incluyeron ensayos controlados aleatorizados (ECA) que compararon la inmunoterapia oral o sublingual administrada mediante cualquier protocolo con placebo o una dieta de eliminación. Los participantes fueron niños o adultos con alergia clínica al huevo.
Obtención y análisis de los datos
Se recuperaron 97 estudios a partir de las búsquedas electrónicas. Se seleccionaron los estudios, se extrajeron los datos y evaluó la calidad metodológica. Se intentó establecer contacto con los investigadores de los estudios para obtener los datos no publicados, cuando fue posible. Se utilizó la estadística I² para evaluar la heterogeneidad estadística. Se calculó un riesgo relativo (RR) agrupado con intervalos de confianza (IC) del 95% para cada resultado mediante un modelo de efectos fijos de Mantel‐Haenzel cuando la heterogeneidad estadística era baja (valor I² menor que 50%). La calidad de la evidencia de todos los resultados se calificó mediante el método GRADE.
Resultados principales
Se incluyeron 10 ECA que cumplieron con los criterios de inclusión, que involucraban a un total de 439 niños (inmunoterapia oral 249; intervención de control 190), de 1 a 18 años de edad. Cada estudio utilizó un protocolo diferente de inmunoterapia oral; en ninguno se utilizó la inmunoterapia sublingual. Tres estudios usaron un placebo y siete estudios usaron una dieta de evitación del huevo como control. Los resultados primarios fueron: una mayor cantidad de huevo que puede ser ingerido y tolerado sin eventos adversos mientras se recibe la inmunoterapia oral o sublingual específica del alérgeno, en comparación con el control; y una recuperación completa de la alergia al huevo después de la finalización de la inmunoterapia oral o sublingual, en comparación con el control. La mayoría de los niños (82%) del grupo de inmunoterapia oral pudieron ingerir una porción parcial de huevo (1 g a 7,5 g) en comparación con el 10% de los niños del grupo de control (RR 7,48; IC del 95%: 4,91 a 11,38; DR 0,73; IC del 95%: 0,67 a 0,80). Menos de la mitad (45%) de los niños que recibieron inmunoterapia oral pudieron tolerar una ración completa de huevo en comparación con el 10% del grupo control (RR 4,25; IC del 95%: 2,77 a 6,53; DR 0,35, IC del 95%: 0,28 a 0,43). Los 10 ensayos informaron sobre el número de niños con eventos adversos graves (EAG) y el número de niños con eventos adversos de leves a graves. Un total de 21/249 niños (8,4%) del grupo de inmunoterapia oral presentaron EAG que requirieron epinefrina/adrenalina y ninguno en el grupo control. Los eventos adversos leves a graves fueron frecuentes; el 75% de los niños presentaron eventos adversos leves a graves durante el tratamiento de inmunoterapia oral versus el 6,8% del grupo de control (RR 8,35; IC del 95%: 5,31 a 13,12). Cabe destacar que siete estudios usaron una dieta de evitación del huevo como control. Los eventos adversos se produjeron en el 4,2% de los niños, que pueden estar relacionados con la ingesta accidental de alimentos que contienen huevo. Tres estudios usaron un control de placebo y un 2,6% de los niños presentaron eventos adversos. En general, hubo un rigor metodológico inconsistente en los ensayos. Todos los estudios reclutaron un escaso número de niños y utilizaron diferentes métodos para proporcionar la inmunoterapia oral. Ocho estudios incluidos se consideraron con alto riesgo de sesgo en al menos un dominio. Además, la calidad de la evidencia se consideró baja debido al pequeño número de participantes y de eventos y posibles sesgos.
Conclusiones de los autores
La exposición frecuente y creciente al huevo durante uno a dos años en las personas alérgicas al huevo aumenta la tolerancia, ya que casi todos se vuelven más tolerantes en comparación con una minoría del grupo de control y casi la mitad de las personas son totalmente tolerantes al huevo al final del tratamiento en comparación con 1 de cada 10 personas que evitan el huevo. Sin embargo, casi todos los que recibieron tratamiento experimentaron eventos adversos, principalmente relacionados con la alergia. Se halló que 1 de cada 12 niños tuvieron reacciones alérgicas graves que requirieron epinefrina, y algunas personas renunciaron a la inmunoterapia oral. La inmunoterapia oral para la alergia al huevo parece ser eficaz, pero la confianza en la compensación entre los efectos beneficiosos y perjudiciales es baja, porque hubo un pequeño número de ensayos con pocos participantes, y problemas metodológicos en algunos ensayos.
PICO
Resumen en términos sencillos
¿Ayuda a las personas con alergia al huevo el hecho de aumentar diariamente cantidades pequeñas de proteína de huevo?
Antecedentes
Hasta hace poco, la única opción práctica para las personas con alergias alimentarias era la evitación estricta de los alimentos a los que eran alérgicas. Es difícil evitar el huevo, ya que se encuentra en muchos alimentos. Incluso evitándolos, el temor a una ingesta accidental de alimentos con huevo por estar rotulados de forma errónea o por la contaminación cruzada es constante incluso para los pacientes más cuidadosos con alergias alimentarias. El consumo accidental de alimentos que contienen huevo puede causar eventos potencialmente mortal.
La inmunoterapia oral es un nuevo tipo de tratamiento para la alergia al huevo, que también se conoce como desensibilización oral o vacunación. El tratamiento consiste en consumir diariamente una cantidad pequeña de proteína de huevo, que se aumenta gradualmente con el transcurso del tiempo hasta lograr una ración completa. Este método podría alterar la respuesta alérgica a la proteína del huevo por parte del sistema inmunológico del cuerpo, aumentando la cantidad de huevo que se puede ingerir sin inducir reacciones adversas.
Fecha de la búsqueda
Para esta actualización, se realizaron búsquedas hasta marzo de 2017.
Características de los estudios
Se incluyeron 10 ensayos controlados aleatorizados (estudios que asignan a las personas al azar a recibir tratamiento) que compararon la inmunoterapia oral con el placebo (un tratamiento falso que no contiene huevo) o una dieta sin huevo en personas con alergia al huevo. Los 10 estudios incluyeron un total de 439 niños (249 en el grupo de inmunoterapia oral [tratamiento con huevo] y 190 en el grupo de control [sin huevo]) de 1 a 18 años de edad.
Resultados clave
La evidencia mostró que tratar la alergia al huevo con cantidades pequeñas y crecientes de huevo ayuda a la mayoría de niños con alérgicos al huevo a tolerar una ración parcial de huevo, siempre que continuaran consumiendo una cantidad diaria de proteína de huevo. Los efectos secundarios fueron frecuentes durante el tratamiento de inmunoterapia oral aunque generalmente fueron leves a moderados. No obstante, 21 de 249 niños tratados con inmunoterapia oral para la alergia al huevo requirieron fármacos debido a una reacción grave. En los estudios no se informó sobre la calidad de vida de los niños y sus familias durante el tratamiento de inmunoterapia oral.
Calidad de la evidencia
Los ensayos incluían números pequeños y hubo problemas en la forma de realizarlos, por lo tanto, se necesita más investigación.
Authors' conclusions
Summary of findings
| Oral and sublingual immunotherapy versus no therapy for egg allergy | ||||||
| Population: children with egg allergy Setting: hospitals Comparison: placebo or egg‐free diet. (Three studies used placebo and seven studies used an egg avoidance diet as controls) | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Oral immunotherapy versus no therapy for egg allergy | |||||
| Increase in the amount of egg that could be tolerated | Study population | RR 7.48 | 410 | ⊕⊕⊝⊝ | 82% of children in the oral immunotherapy group could ingest a partial serving of egg (1 g to 7.5 g) compared to 10% of the control group. | |
| 102 per 1000 | 763 per 1000 | |||||
| Complete recovery | Study population | RR 4.25 | 439 | ⊕⊕⊝⊝ | 45% of children receiving oral immunotherapy were able to tolerate a full serving of egg compared to 10% of the control group. | |
| 100 per 1000 | 425 per 1000 | |||||
| Numbers of children with serious adverse events | See comment | See comment | Not estimable | 439 | ⊕⊕⊝⊝ | All 10 trials reported numbers of children with serious adverse events (SAEs): SAEs requiring epinephrine/adrenaline occurred in 21/249 (8.4%) of children in the oral immunotherapy group and none in the control group. Because adverse events were classified differently among the studies, it is difficult to comment on whether they were under‐ or over‐estimated. Surprisingly, only one study showed a high level of SAEs (Vazquez‐Ortiz 2014): 13 children required epinephrine/adrenaline administration 18 times, and one grade 5 reaction occurred. |
| Number of children with mild‐to‐severe adverse events | Study population | RR 8.35 | 439 | ⊕⊕⊝⊝ | Mild‐to‐severe adverse events were frequent; 75% of children presented mild‐to‐severe adverse events during oral immunotherapy treatment versus 6.8% of children in the control group. | |
| 68 per 1000 | 568 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| The assumed risk is the risk of the control arm 1 Downgraded one level because of risk of bias: all studies were assessed at high or unclear risk of bias in at least one domain. | ||||||
Background
This is an update of the 2014 version of this review. Please see the 'Differences between protocol and review' section for changes in the review since the protocol or the last version of the review.
Description of the condition
Clinical egg allergy is one of the most common food allergies in western countries, affecting up to approximately 2% of young children (Savage 2007). Osborne 2011 showed an 8.9% prevalence of challenge‐proven egg allergy in 12‐month old infants in Australia. Natural tolerance, that is, developing tolerance to egg over time, is common but some children will remain allergic until adulthood. Egg‐allergic reactions may persist throughout adulthood although symptoms may be milder. It has been shown that 75% to 85% of young children with egg allergy could tolerate heat‐denatured (baked) egg products, showing mild or no symptoms (Leonard 2012; Osborne 2011); most outgrow the allergy.
Despite this trend, recent data have shown that milk and egg allergies are becoming more persistent and that children may not be outgrowing these allergies until adolescence rather than during the first five to six years of life as previously thought (Savage 2007). It appears that the longer the egg allergy persists the less likely it is that tolerance will develop (Wood 2003b). Thus, it has become imperative to understand individualized prognoses of egg allergy and to develop clinical management that may improve the quality of life of egg‐allergic children and, ideally, promote earlier development of tolerance. It is likely that most children who tolerate baked‐egg products will develop tolerance after undergoing oral immunotherapy, and perhaps, this is achieved more rapidly if treated with oral immunotherapy (Leonard 2012). Those children who do not tolerate heat‐denatured egg are likely to be more difficult to treat (Leonard 2012). Consequently, an adequate placebo group is needed to investigate the ability of oral immunotherapy to induce long‐term tolerance.
An immunoglobulin E (IgE)‐antibody mediated allergic reaction to egg is based on circulating levels of soluble IgE, which is produced by B cells and binds to the surface of mast cells and basophils. Mast cells are found in the skin, gut, and respiratory tract and are situated adjacent to nerves and blood vessels. Among the most important of their immune functions is the propensity to bind IgE, utilizing the high‐affinity IgE receptor FcåR1. When egg allergen is re‐encountered and recognized by cell‐bound IgE, adjacent FcåR1‐IgE complexes move closer together and bring their signalling machinery into close proximity, which sets off a cascade of phosphorylation ultimately resulting in calcium influx. When calcium enters the cell, the activated mast cell undergoes degranulation and the contents of these granules are released into the extracellular space. The immediate liberation of preformed powerful vaso‐active compounds such as histamine, platelet activating factor, tryptase, carboxypeptidase, chymase, and heparin, elicit the acute symptoms of type 1 hypersensitivity reactions in the skin, gut, respiratory, and cardiovascular systems (Galli 2010). These symptoms include urticaria, angioedema, flushing, nausea, vomiting, abdominal pain, diarrhoea, wheezing, coughing and bronchospasm, rhinorrhoea, and hypotension or syncope, which can occur alone or in combination and typically begin within minutes and up to two hours after food ingestion (Burks 2008; Simons 2011).
There is no interventional therapy for egg allergy currently approved by the USA Food and Drug Administration (FDA), nor by the European Medicines Agency (EMA). Current management relies upon strict allergen avoidance, including the small quantities present in a variety of foods, and obvious sources such as desserts (Muraro 2014). In the USA, European Union, Australia, Japan, and Singapore, food‐labelling laws require food manufacturers to label packaging in plain language, listing the presence of common allergens and products (Burks 2012a). However, similar laws are not in place in many other countries, and in these settings, care is required to identify hidden forms of egg allergens, such as ovalbumin or ovomucoid (Burks 2012a). Studies that evaluated growth measurements against dietary records have suggested that food allergy puts children at risk of inadequate nutrition (Christie 2002). Specifically, where children's food allergy is concerned, it is advisable to involve a dietitian in formulating a nutritionally adequate, allergen‐free diet. The quality of life of people with food allergies and their caregivers is reduced due to the fear of incorrect labelling or accidentally ingesting egg‐containing food, and the ever‐present threat of anaphylaxis (Cummings 2010). The management of clinical egg allergy consists of teaching people with allergy and their carers to recognize the symptoms and signs of severe reaction, prompt use of epinephrine auto‐injection, and activation of emergency medicine assistance (Simons 2009). Therapeutic interventions that provide lifelong protection against potential egg ingestion are therefore required.
Description of the intervention
Traditional subcutaneous immunotherapy (also known as allergy shots) was studied since the early twentieth century and was able to induce desensitization (Ring 2011). However, subcutaneous immunotherapy treatment is not feasible due to the high rate of systemic reactions (Nelson 1997; Oppenheimer 1992). Given the safety issues associated with subcutaneous immunotherapy, oral immunotherapy and sublingual immunotherapy have been studied as optional treatments.
Although there have been reports in the literature over the last 100 years on the use of oral immunotherapy for food allergy, most research on this topic began with Patriarca 1984, who demonstrated the successful treatment of allergies to cow’s milk, egg, fish, and fruits with standardized oral immunotherapy protocols. In a pilot study of oral immunotherapy for egg allergy in children, Buchanan demonstrated the safety of a 24‐month egg oral immunotherapy protocol involving modified rush desensitization, build‐up, and maintenance phases (Buchanan 2007).
The initial aim of oral immunotherapy is to provide clinical desensitization, that is, to achieve a state in which effector cells involved in a specific immune response develop reduced reactivity or become non‐reactive upon increased introduction of an allergen. In a desensitized state, a person may be non‐reactive while regularly receiving the allergen. However, when regular administration ends the previous level of reactivity returns. The aim of treatment is initially to desensitize people to egg allergen by increasing the threshold dose of exposure, and therefore, reduce the risk of anaphylaxis. The longer‐term goal is to induce a state of tolerance to an allergen where the non‐reactive state remains present permanently through down‐regulation of the TH2 response to egg, and which will endure irrespective of whether a previously clinically reactive person continues to consume egg products or not following the completion of the treatment (Land 2011).
There are different types of oral immunotherapy protocols. Oral immunotherapy involves the regular administration of small amounts of allergen by the oral route to rapidly induce desensitization, then over time, induce tolerance to the allergen.
Studies have considered immunotherapy that is ingested and immunotherapy administered sublingually. In this review, oral immunotherapy specifically refers to ingested immunotherapy and sublingual immunotherapy refers to immunotherapy administered under the tongue.
People undergoing oral immunotherapy generally ingest a mixture of protein powder in a vehicle food (e.g. apple sauce). People undergoing sublingual immunotherapy generally receive a small amount of liquid extract under the tongue. Both treatments are typically initiated in a controlled setting where gradually increased doses of allergen are given up to a targeted dose. In standard protocols most dosing is subsequently done at home.
How the intervention might work
Oral immunotherapy involves the administration of initially very small doses (usually micrograms or milligrams) of food allergen to food‐allergic people in a controlled clinical setting. The dose of the administered food allergen is then systematically increased until a maximum tolerated dose is achieved (Jones 2009). Regular dosing with this maximal dose is then maintained at home by the person with the allergy (or their carer). Of note, it has been demonstrated that underlying the clinical benefits of oral immunotherapy were changes to multiple aspects of the immune system, leading to a dampened allergic response (Jones 2009). Changes included decrease in allergen‐specific IgE and increase in allergen‐specific IgG4 (Buchanan 2007; Itoh 2010; Patriarca 2003; Staden 2007), as well as suppression of mast cells and basophils, an increase in T regulatory cells (TRegs), and a change in cytokine profile. Additionally, micro‐array analysis of T cells has revealed changes in several apoptotic pathways, although the significance of this result remains unknown (Jones 2009). Cytokine analysis demonstrated a clear decrease in TH2 cytokines without a concomitant increase in TH1 cytokines, causing a shift in TH1 and TH2 skewing and arguing against oral immunotherapy. Rather, a decrease in IL‐2 was noted, possibly suggesting clonal anergy or deletion as a possible mechanism of oral immunotherapy (Land 2011). However, caution needs to be applied when interpreting these results; both studies had small cohorts of participants and the selection criteria for the immunological studies were not sufficiently clear (Jones 2009; Land 2011).
Successful desensitization is thought to induce immunological tolerance by generating allergen specific IL‐10 secreting Tr1 or TGF‐secreting TH3 regulatory T cells, or both (Sicherer 2010).
Why it is important to do this review
Food allergy is an IgE‐mediated immediate‐type hypersensitivity that is thought to be the result of a breakdown in the normal process of oral tolerance. Although the prevalence of food allergy continues to rise, avoidance remains the standard of care because no disease‐modifying treatments are readily available. Although questions regarding the safety of treatments, and the potential for development of long‐term immunological tolerance remain, oral immunotherapy and sublingual immunotherapy offer potential hope for the future treatment of egg allergy.
There is a need to systematically identify, critically appraise, and summarize the available evidence on the benefits and risks associated with oral immunotherapy and sublingual immunotherapy for the management of people with egg allergy.
Objectives
To determine the efficacy and safety of oral and sublingual immunotherapy in children and adults with immunoglobulin E (IgE)‐mediated egg allergy as compared to a placebo treatment or an avoidance strategy.
Methods
Criteria for considering studies for this review
Types of studies
Randomized controlled trials (RCTs), quasi‐RCTs, and controlled clinical trials (CCTs) were eligible for inclusion.
Types of participants
Children and adults diagnosed with an immediate‐type egg allergy were included. Egg allergy was defined as a history of systemic clinical reaction within minutes to hours after the ingestion of egg in people with objective evidence of sensitization to egg. Objective evidence was:
-
a positive skin prick test (SPT) or the presence of specific IgE; and
-
a positive open or double‐blind, placebo‐controlled food challenge. The positive reaction to the challenge should be the immediate onset of symptoms suggestive of IgE‐mediated mechanisms such as urticaria, angioedema, vomiting, diarrhoea, abdominal pain, and any alteration in the level of consciousness.
Types of interventions
Egg oral immunotherapy or sublingual immunotherapy administered by any protocol compared with a placebo group, or treatment with a continued avoidance diet.
Types of outcome measures
Primary outcomes
Successful desensitization or achieved tolerance defined as:
-
an increase in the amount of egg that can be ingested and tolerated without adverse reaction (i.e. evidence of desensitization);
-
a complete recovery from egg allergy whether or not egg is eaten (i.e. induction of immunologic tolerance);
-
numbers of participants with serious adverse events; and
-
numbers of participants with mild‐to‐severe adverse events.
Secondary outcomes
-
Medication used due to adverse events.
-
Immunological changes suggestive of the induction of tolerance (e.g. decreased wheal diameter on SPT testing with egg, decreased egg‐specific IgE levels, increased egg‐specific IgG4 levels.
-
Change in quality of life.
-
Cost‐effectiveness of treatment.
Search methods for identification of studies
We conducted systematic searches for RCTs, quasi‐RCTs, and CCTs regardless of language, geographical area, or publication status to 31 March 2017.
Electronic searches
We searched: the Cochrane Library, MEDLINE, Embase, PubMed, ISI Web of Science, Google Scholar, AMED, BIOSIS, CAB, CINAHL, Global Health, TRIP, and WHO Global Health Library. The MEDLINE search strategies are detailed in Appendix 1 and the search strategies used for other databases are presented in Appendix 2. We combined subject search strategies with adaptations of the highly sensitive search strategy designed by Cochrane for identifying RCTs and CCTs as described in the Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0, Box 6.4.b (Higgins 2011).
Searching other resources
We identified unpublished studies, ongoing work and research in progress by searching key trials registers ( ISRCTN registry (www.isrctn.com/).; clinicaltrials.gov). We also searched the proceedings of conferences important to allergy and immunology and not included in the electronic databases. We used key articles retrieved from the electronic database searches (including seminal research studies and review articles) to conduct citation searches in Web of Science and Scopus. We searched for grey literature via Google Scholar (scholar.google.com) and contacted experts in the field.
Data collection and analysis
Selection of studies
Two review authors (OR, MAT) independently screened the retrieved titles and abstracts of records and excluded irrelevant ones. We retrieved the full text of reports of potentially relevant studies. Multiple reports from the same study were identified and grouped under a single study identifier. Two review authors (OR, MGC) independently undertook the examination of studies and selection based on the eligibility criteria. If required, study investigators were contacted to clarify eligibility. If the two review authors did not agree on including a study, even after discussion, a third author acted as an arbiter (SZ).
Data extraction and management
We created a data extraction form that included the following items: trial characteristics (setting, oral immunotherapy regimen, eligibility criteria); methodological quality (randomization, blinding, selective reporting); participant characteristics; results and outcomes. The form was piloted using two sample studies. Two review authors (OR, MGC) working independently, extracted data. We contacted study investigators when information was not available from study reports. Disagreements between review authors were resolved by discussion and, if required, arbitration by a third review author (SZ).
Assessment of risk of bias in included studies
Two review authors (SZ, MGC) worked independently using Cochrane’s risk of bias tool to evaluate each included study. We considered the following types of potential bias: selection bias (adequacy of randomization and allocation concealment); performance bias (blinding of participants and personnel); detection bias (blinding of outcome assessors); and attrition bias (loss to follow‐up). Any disagreements were discussed and a third review author acted as arbiter if necessary. Assessment results were summarized in 'Risk of bias' tables. We performed sensitivity analyses to determine the influence of studies with high risk of bias on meta‐analysis results.
Measures of treatment effect
Categorical data were extracted for each intervention group, and risk ratios (RRs) and absolute risk differences (RDs) calculated. Mean and standard deviation were obtained for continuous data and analyses performed using the mean differences (MDs). For each measure of effect the 95% confidence intervals (CI) were given. The number needed to treat for an additional beneficial outcome (NNTB) and the number needed to treat for an additional harmful outcome (NNTH) were presented when RDs were statistically significant.
Unit of analysis issues
We did not anticipate any unit of analysis issues for this intervention. For example, cross‐over trials would not be a rational approach to assess immunotherapy because the goal of treatment is to induce tolerance, and a participant would not be able to serve as their own control if their immune response had been altered. We did not expect large numbers of egg‐allergic people from various cohorts, so cluster‐randomization was unlikely to be encountered.
Dealing with missing data
We attempted to contact study investigators to request missing data. Data were analysed on an intention‐to‐treat (ITT) basis whenever possible.
Assessment of heterogeneity
We anticipated clinical heterogeneity in the studies that were reviewed, including the ages of the study population and differences in the immunotherapy protocol. However, despite these potential differences we believe that we were able to analyse the studies together to assess the efficacy of oral immunotherapy. We assessed statistical heterogeneity using the I² statistic (Higgins 2011); an I² value greater than 50% implies substantial heterogeneity.
Assessment of reporting biases
We planned to assess reporting and publication bias by examining the degree of asymmetry of a funnel plot in RevMan 5.3 provided that a sufficient number of studies (n > 10) were available (RevMan 2014). However, this was not feasible.
Data synthesis
We used a Mantel‐Haenszel fixed‐effect model for meta‐analysis, and summarized evidence in a 'Summary of findings' table. All analyses were conducted using Review Manager (RevMan 2014).
Subgroup analysis and investigation of heterogeneity
Depending on the data available, we planned to undertake subgroup analyses for: presence of asthma, other food allergies, history of previous anaphylaxis, the oral immunotherapy or sublingual immunotherapy regimen, duration of treatment, time since completion of treatment, and RCT versus non‐RCT. However, there were insufficient data for subgroup analysis to be performed.
Sensitivity analysis
A sensitivity analysis was performed for reviewed studies that were deemed at high risk of bias mainly in two domains: detection and performance biases.
'Summary of findings' table
Following standard Cochrane methodology, we created a 'Summary of findings' table for all of our outcomes. Also following standard Cochrane methodology, we assessed the quality of evidence for each outcome using the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias (GRADEpro GDT)).
Results
Description of studies
Results of the search
The electronic searches from the previous version of the review and this update retrieved 96 records, of which 85 remained after removing duplicates. Two review authors screened the records based on title and abstract and excluded 59 records. We obtained the full‐text articles for 26 records. Of these, we excluded 11 trials that did not meet our inclusion criteria. Five studies are awaiting classification, and two were ongoing studies. We included 10 studies from 11 records in this review update (Figure 1).
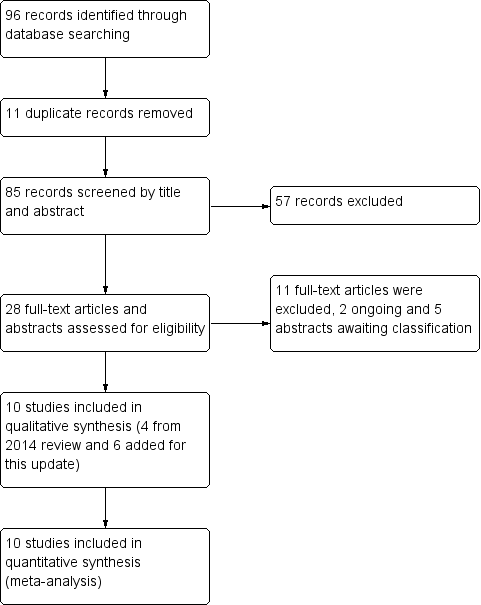
Study flow diagram.
Included studies
We included 10 published studies that met our inclusion criteria; of these, six studies (including 272 children) were added for this update (see Characteristics of included studies). The studies recruited a total of 439 children (249 intervention/190 control) who were aged from 1 to 18 years.
Three studies used placebo control (Burks 2012; Caminiti 2015; Giavi 2016), and seven studies used an avoidance diet as the control (Akashi 2017; Dello Iacono 2013; Escudero 2015; Fuentes‐Aparicio 2013; Meglio 2013; Pérez‐Rangel 2017; Vazquez‐Ortiz 2014).
Five studies excluded children with history of anaphylaxis (Akashi 2017; Burks 2012; Escudero 2015;Giavi 2016; Pérez‐Rangel 2017), but two studies included children with history of anaphylaxis (Dello Iacono 2013; Fuentes‐Aparicio 2013). Anaphylaxis history was not clearly defined in the inclusion criteria of three studies (Caminiti 2015;Meglio 2013;Vazquez‐Ortiz 2014).
Four studies excluded children with severe or uncontrolled asthma (Dello Iacono 2013; Meglio 2013; Pérez‐Rangel 2017; Vazquez‐Ortiz 2014). One study excluded children with severe atopic dermatitis (Vazquez‐Ortiz 2014). Two studies excluded children with egg non IgE mediated adverse events, eosinophilic oesophagitis, immune system diseases or malignant diseases, any baseline disease contra‐indicating the use of epinephrine and/or allergy to any component of the placebo (Escudero 2015;Pérez‐Rangel 2017). Children were excluded based on: diagnosis of cardiovascular disease (Vazquez‐Ortiz 2014), neuropsychiatric impairment (Vazquez‐Ortiz 2014), receiving any other immunotherapy (Meglio 2013), significant pre‐ and post‐natal diseases (although significance was not defined) (Giavi 2016), use of systemic drugs (such as antihistamines, beta‐agonists, ACE‐inhibitors) (Giavi 2016), congenital illness or malformation that may affect normal growth (Giavi 2016), and participation in another clinical trial (Giavi 2016). Two studies excluded children with parental history of unreliable management of complications and treatment (Dello Iacono 2013; Giavi 2016).
Two studies administered antihistamine treatment as a co‐intervention (Meglio 2013; Pérez‐Rangel 2017). Oral immunotherapy was used in combination with antihistamines if recurrent allergic symptoms developed in Akashi 2017. Children with asthma on preventive treatment continued therapy during oral immunotherapy in Vazquez‐Ortiz 2014. Two studies did not report exclusion criteria (Caminiti 2015; Fuentes‐Aparicio 2013).
Oral immunotherapy protocols
Egg oral immunotherapy protocols differed. Nine studies included a build‐up phase in a hospital, day treatment centre, or research centre followed by gradual up‐dosing in hospital or at home, and a maintenance phase at home (Burks 2012; Caminiti 2015; Dello Iacono 2013; Escudero 2015; Fuentes‐Aparicio 2013; Giavi 2016; Meglio 2013; Pérez‐Rangel 2017; Vazquez‐Ortiz 2014). Akashi 2017 reported that the oral immunotherapy protocol was carried out at home only. Burks 2012 was characterized by an increasing dose in research settings followed by an approximate doubling every 30 minutes, up to 50 mg. The maximum tolerated single dose of egg was given in the clinic on the following day and provided the starting dose for the build‐up phase. Attainment of a minimum dose of 3 mg of egg white powder was required to continue dosing. The children then continued a build‐up dosing at home. For children who did not achieve a dose of 50 mg on the first day, doses were doubled every two weeks up to 50 mg. Therefore, the dose was increased to 75 mg with following increases by 25% up to 2 g. The maximum time allowed for the build‐up phase was 10 months; the dose achieved at 10 months was considered to be the maintenance dose. After reaching their highest build‐up dose (maximum 2 g), children continued this dose daily for at least two months before the month 10 oral food challenge; children in the egg oral immunotherapy group continued maintenance dosing through to 22 months. The Fuentes‐Aparicio 2013 protocol included in‐hospital administration of 1 mg egg and was continued by tripling the dose every 30 minutes, up to 30 mg. On the second day, 30 mg was administered in one single dose, with treatment continuing at home at the same dose. Subsequently, weekly increases were made in the clinic until 10 g of powdered egg, the equivalent of one egg, was reached. In Dello Iacono 2013 children started with one drop of undiluted raw hen's egg emulsion (0.015 mL) in a day hospital then continued at home with gradually increasing doses. The doses were increased at six further day hospital visits (on days 8, 29, 64, 92, 134, 176). Dose increases were customized based on the frequency and severity of side effects and in cases of intercurrent illness or worsening asthma. The oral immunotherapy protocol in Meglio 2013 started with 0.27 mg of hen's egg protein in hospital and thereafter children doubled the dose at home every eight days until day 80. Subsequently, the doses were doubled every 16 days to achieve a total daily intake of 25 mL at six months. In the Vazquez‐Ortiz 2014 oral immunotherapy protocol, pasteurized liquid egg white containing 8.3 g of protein per 100 mL was used, in which allergenicity was equivalent to raw egg white. The induction phase involved 16 weeks and started with a 2‐day in‐hospital rush phase, in which doses were increased hourly, starting with 0.083 mg egg white protein. Children were then discharged home and continued receiving the last tolerated dose once daily throughout the week. Weekly increases were given at the outpatient clinic until the equivalent of one raw egg (60 g of fresh product) could be given. The Caminiti 2015 oral immunotherapy procedure consisted of weekly administration, at the hospital clinic, of increasing doses of dehydrated egg white, diluted with sterile saline, starting with 0.1 mg. The dose was doubled every week until week 16, to achieve a cumulative dose of 4 g in approximately four months. When the dose of 4 g was tolerated, the oral immunotherapy protocol was continued with cooked or boiled egg at home. The Escudero 2015 protocol followed the procedure described in Staden 2007, which consisted of an initial dose escalation phase in hospital starting with 0.08 mg of egg white and subsequently increasing every 20 minutes up to 140 mg of egg white protein (cumulative dose was 280 mg). This was followed by a build‐up phase with a weekly increase of the last maximum tolerated dose in hospital up to 2.8 g of egg white protein and a maintenance phase, which consisted in consumption of at least one undercooked egg (defined by the authors as fried egg, scrambled or undercooked omelet) every 48 hours. Children were permitted to freely consume any other egg‐containing food. The Giavi 2016 oral immunotherapy protocol was characterized by an escalation phase in hospital increasing the dose of hydrolysed egg every 20 to 30 minutes to reach 9 ± 1 g of hydrolysed egg. In the absence of adverse events the child received the full dose of 9 ± 1 g of hydrolysed egg, and in the absence of adverse events occurring, the child received the full dose of hydrolysed egg daily for six months. The Pérez‐Rangel 2017 oral immunotherapy protocol involved a consecutive five day build‐up phase starting with a highest tolerated single dose at the baseline egg double‐blinded placebo‐controlled food challenge test (DBPCFC). This consisted in an escalation dose of egg white starting from 4 mg and finishing with 1.8 g of egg white every 20 minutes until objective IgE‐mediated manifestations or subjective mild‐to‐moderate symptoms occurred. The regimen was conducted in an outpatient clinic. The build‐up target was 3.6 g of dehydrated egg white with a cumulative dose of 5.4 g administered on the last day. The maintenance phase consisted in eating one undercooked egg every 48 hours. Moreover, children were permitted to freely consume any other egg‐containing food. In Akashi 2017, oral immunotherapy was carried out at home with a starting dose of 0.1 mg of dried powdered egg and this was increased up to 4 g with three to four days interval. The escalation protocol was based on the method used in Patriarca 2003. Children were permitted to continue oral immunotherapy in combination with antihistamines in case of recurrent allergic symptoms.
Each study used a different egg preparation: Burks 2012 used raw white egg powder. Fuentes‐Aparicio 2013 used powdered pasteurized egg. Dello Iacono 2013 and Meglio 2013 used raw egg emulsion. Vazquez‐Ortiz 2014 used pasteurized liquid egg white. Caminiti 2015, Escudero 2015 and Pérez‐Rangel 2017 used dehydrated egg white. Giavi 2016 used hydrolysed egg. Akashi 2017 used dried powdered egg.
There were also differences among included studies regarding the duration of oral immunotherapy to achieve full desensitization, defined as the ability to digest a small egg serving without adverse events. Burks 2012 reported desensitization in 75% of children after 22 months of oral immunotherapy; the target maintenance dose was 10 g egg white powder. Desensitization was evaluated by oral food challenge test. The duration of oral immunotherapy in Fuentes‐Aparicio 2013 varied between four and 28 weeks (average 10 weeks) targeted to achieve a tolerance of 10 g of whole egg. The Dello Iacono 2013 oral immunotherapy protocol duration, to achieve "maximum tolerance" by digesting 40 mL or raw egg emulsion without adverse events, was six months. Desensitization was evaluated by a DBPCFC test. The planned duration of oral immunotherapy for children to be able to tolerate 25 mL of raw egg in Meglio 2013 was 181 days. The actual duration of the oral immunotherapy was longer, with a mean duration of 215 days (range 178 to 287 days). None of the oral food challenge tests were performed for the intervention group at the end of the study; only children in the control group underwent DBPCFC at six months after enrolment. The duration of oral immunotherapy in Vazquez‐Ortiz 2014 was 12 months and desensitization was evaluated by oral food challenge to one raw egg, meaning 3.8 g of raw egg white or if not reached, the highest tolerated dose. The oral immunotherapy protocol in Caminiti 2015 aimed to achieve a tolerance a 4 g of dehydrated egg white in approximately four months and DBPCFC performed by the end of the study. Desensitized children received an egg‐containing diet with two to three eggs per week for six months, following a three‐month egg avoidance diet, after which a repeat DBPCFC was performed (Caminiti 2015). In Escudero 2015, the primary study outcome was to assess the induction of sustained unresponsiveness after three months of egg oral immunotherapy and an egg avoidance diet for one month, defined as the ability to consume 2808 mg of egg white protein without symptoms in a DBPCFC at four months. The oral immunotherapy duration in Giavi 2016 was six months with the target to tolerate 43.2 g of boiled egg on oral food challenge. The Pérez‐Rangel 2017 study was randomized for the first five months, during which an intervention group of children received egg oral immunotherapy shortly after randomization and control group children were on an egg avoidance diet; thereafter the control group was stopped and control group children who failed DBPCFC at five months began an oral immunotherapy treatment. The results reported here were extracted from the first five months of the randomized study period. No food challenge test was performed on children in the oral immunotherapy group at five months. Akashi 2017 used an oral immunotherapy protocol that lasted on average 6.5 months (range 5 to 8) aiming to achieve tolerance of 4 g dry egg powder on oral food challenge by the end of the oral immunotherapy protocol.
Clinical history of allergic reactions after egg digestion was an inclusion criterion for all studies. In two studies, positive clinical history was defined as development of symptoms within two hours after ingestion of egg (Burks 2012;Escudero 2015), and in one study the definition was as an immediate (< 1 h) reaction following egg ingestion (Giavi 2016).
Nine studies reported as one of the inclusion criteria a positive skin prick test (SPT) (Burks 2012; Caminiti 2015; Dello Iacono 2013; Escudero 2015; Fuentes‐Aparicio 2013; Giavi 2016; Meglio 2013; Pérez‐Rangel 2017; Vazquez‐Ortiz 2014). Positive egg‐specific IgE (sIgE) levels was an inclusion criteria in all ten studies although the definition, if it was specified, varied among the studies. In Burks 2012 more than 5 kU/L for participants six years of age or older, or 12 kU/L or more for those five years old; in Giavi 2016 and in Giavi 2016 it was considered positive level of 0.35 kU/L or higher; Akashi 2017, Escudero 2015, Pérez‐Rangel 2017 defined IgE positivity if the levels were of 0.7 kU/L or higher. In seven studies DBPCFC was performed at baseline (Akashi 2017Caminiti 2015;Dello Iacono 2013;Escudero 2015;Meglio 2013;Pérez‐Rangel 2017Vazquez‐Ortiz 2014). Two studies required oral food challenge at baseline (Giavi 2016 and Fuentes‐Aparicio 2013); oral food challenge was not performed at baseline in Burks 2012.
In seven studies a DBPCFC test was performed on all children in the control group at the end of the study (Akashi 2017; Caminiti 2015; Dello Iacono 2013; Escudero 2015; Meglio 2013; Pérez‐Rangel 2017; Vazquez‐Ortiz 2014). In three of these seven studies, DBPCFC was also performed for oral immunotherapy group participants (Akashi 2017; Dello Iacono 2013; Escudero 2015). An open oral food challenge was performed in oral immunotherapy group participants at the end of the study in five trials (Burks 2012; Caminiti 2015; Fuentes‐Aparicio 2013; Giavi 2016; Vazquez‐Ortiz 2014) and in two trials it was performed in control group participants (Burks 2012; Giavi 2016).
The follow‐up period varied for each study, and included: 36 months (Escudero 2015), 24 months (Burks 2012), 13 months (Caminiti 2015), 12 months (Vazquez‐Ortiz 2014), six months (Akashi 2017; Dello Iacono 2013; Fuentes‐Aparicio 2013, Giavi 2016; Meglio 2013) and five months (Pérez‐Rangel 2017). All children were receiving daily maintenance at the time of follow‐up.
Study funding sources
Two included RCTs did not receive financial support (Caminiti 2015; Dello Iacono 2013). Two studies were supported by national research grants (Burks 2012; Vazquez‐Ortiz 2014). Pérez‐Rangel 2017 was supported by a Merck Sereno grant and by a grant from the ALK‐Abelló pharmaceutical company. Escudero 2015 was not funded, but the English language publication was financially supported by Stallergenes pharmaceutical company. Some authors of the Giavi 2016 study are or were employees for Nestec Ltd. Akashi 2017 declared that the study was partially supported by a grant from the Ministry of Health, Labour and Welfare Japan, and funds from a Research Center of Taiho Pharmaceutical Company. Study funding sources were not reported for two studies (Fuentes‐Aparicio 2013; Meglio 2013).
Withdrawal rate
We calculated the withdrawal rate for each study. The main reason for withdrawal was the occurrence of adverse events. Interestingly, Giavi 2016 reported one dropout due to anxiety. In Burks 2012 the dropout rate was 15% for children in the oral immunotherapy group and 13% for placebo group children; the overall withdrawal rate for both study groups was 14.5%. Fuentes‐Aparicio 2013 reported a 4% overall dropout rate (7.5% for the oral immunotherapy group and 0% for the placebo group). Meglio 2013 reported an overall 5% dropout rate, with 10% in the oral immunotherapy group and 0% in the control group. There were no dropouts in Dello Iacono 2013. Vazquez‐Ortiz 2014 reported 18% withdrawal in the oral immunotherapy group and none in the control group, resulting in an overall withdrawal of 11%. Caminiti 2015 reported an overall dropout rate of 13% (6% for the oral immunotherapy group and 21% for the placebo group). Escudero 2015 had a 7% dropout rate in the oral immunotherapy group and none in the control group, the overall withdrawal rate being 3%. Giavi 2016 reported a 27% withdrawal rate in the oral immunotherapy group and none in the control group; overall withdrawal: 14%. In Pérez‐Rangel 2017, the overall withdrawal rate was 9%: 10.5% in the oral immunotherapy group and 7% in the placebo group. Akashi 2017 had an overall withdrawal rate of 17%: 22% in the oral immunotherapy group and 11% in the placebo group.
Excluded studies
We excluded 11 studies that did not meet our inclusion criteria. The reasons for exclusion were: no previous history of exposure to egg (one study); comparison group not placebo or a continued avoidance diet (seven studies); results were for combined egg and milk‐allergic participants (three studies). See Characteristics of excluded studies.
Studies awaiting classification
Our rsearch revealed abstracts for five studies with insufficient information to assess eligibility. See Characteristics of studies awaiting classification.
Ongoing studies
Searches of clinical trials registers identified two potentially relevant trials (NCT02083471; NCT01846208; Characteristics of ongoing studies). These will be assessed for inclusion in a future review update following completion of the studies.
Risk of bias in included studies
We analysed seven domains of potential risk of bias for the included studies. The risk of bias decisions are shown in Characteristics of included studies, and summarized in Figure 2 and Figure 3.
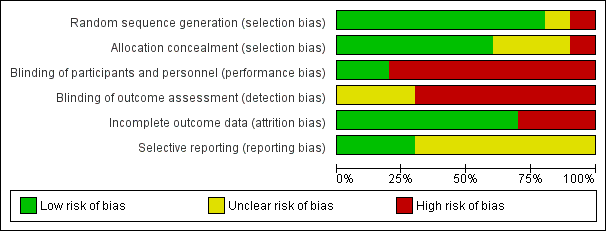
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
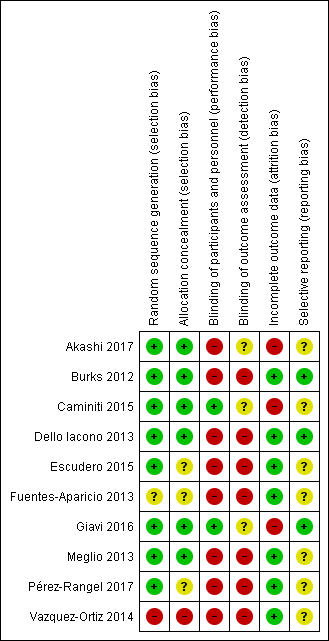
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Eight included studies (Akashi 2017; Burks 2012; Caminiti 2015; Dello Iacono 2013; Escudero 2015; Giavi 2016; Meglio 2013; Pérez‐Rangel 2017) provided a description of an adequately generated random sequence and were judged to be at low risk of bias. We judged one study (Fuentes‐Aparicio 2013) to be at unclear risk of bias due to insufficient information. One study was assessed at high risk of bias because participants were divided into two groups (active or control group) based on parent's choice (Vazquez‐Ortiz 2014).
Six included studies provided a description of an adequately concealed allocation and were judged to be at low risk of bias (Akashi 2017; Burks 2012; Caminiti 2015; Dello Iacono 2013; Giavi 2016; Meglio 2013). We judged three studies to be at an unclear risk of bias due to insufficient information (Escudero 2015; Fuentes‐Aparicio 2013; Pérez‐Rangel 2017). One study was assessed at high risk of bias because participants were divided into two groups (active or control group) based on parent's choice (Vazquez‐Ortiz 2014).
Blinding
No studies were assessed at low risk of detection bias. Two studies were at low risk of bias for participant and personnel blinding (Caminiti 2015; Giavi 2016). Eight studies were assessed at high risk of bias for this domain (Akashi 2017; Burks 2012; Dello Iacono 2013; Escudero 2015; Fuentes‐Aparicio 2013; Meglio 2013; Pérez‐Rangel 2017; Vazquez‐Ortiz 2014), but seven used egg avoidance as a control, making blinding impossible. No studies were assessed at low risk of bias for blinding outcome assessment (detection bias), but was at high risk in seven studies (Burks 2012; Dello Iacono 2013; Escudero 2015; Fuentes‐Aparicio 2013; Meglio 2013; Pérez‐Rangel 2017; Vazquez‐Ortiz 2014). Three studies were assessed at unclear risk of bias for this domain (Akashi 2017; Caminiti 2015; Giavi 2016).
Incomplete outcome data
Three studies were assessed at high risk of attrition bias because there was an imbalance in numbers for missing data across intervention groups (Akashi 2017; Caminiti 2015; Giavi 2016). Seven studies were assessed at low risk of attrition bias because of low levels of attrition or because attrition was equal between groups (Burks 2012; Dello Iacono 2013; Escudero 2015; Fuentes‐Aparicio 2013; Meglio 2013; Pérez‐Rangel 2017; Vazquez‐Ortiz 2014) .
Selective reporting
Protocols were available for three studies and were assessed at low risk of bias (Burks 2012; Dello Iacono 2013; Giavi 2016). Seven studies did not provide clear pre‐specified outcomes and were assessed at unclear risk of bias (Akashi 2017; Caminiti 2015; Fuentes‐Aparicio 2013; Escudero 2015; Meglio 2013; Pérez‐Rangel 2017; Vazquez‐Ortiz 2014).
Other potential sources of bias
The included studies appeared free of other sources of bias.
Effects of interventions
Increase in the amount of egg that could be tolerated (Analysis 1.1)
We pooled nine studies (410 children: 234 intervention/176 control). Most children (82%) in the oral immunotherapy group could ingest a partial serving of egg (1 g to 7.5 g) compared to 10% of the control group (RR 7.48, 95% CI 4.91 to 11.38; RD 0.73, 95% CI 0.67 to 0.80; children = 410; studies = 9; I² = 27% for RR and I² = 73% for RD). Children who did not reach complete desensitization at the end of oral immunotherapy tolerated a higher quantity of egg powder compared to baseline: 4000 mg versus 600 mg (Akashi 2017); 100.8 mg versus 481.3 mg (Escudero 2015). Four children (8%) in Vazquez‐Ortiz 2014 achieved partial desensitization, defined as the ability to digest 0.8 g to1.7 g of raw egg white protein. Partial tolerance (< 40 mL but > 10 mL raw egg emulsion) was achieved in 90% of children in the oral immunotherapy group in Dello Iacono 2013. Although 80% of children in Meglio 2013 achieved intake of 25 mL of raw egg, only 30% who reached the full target dose of 25 mL raw egg without any symptoms and 50% of children presented some symptoms with duration < 2 h and spontaneous resolution. The tolerated egg quantity was not reported in four studies (Burks 2012; Caminiti 2015, Fuentes‐Aparicio 2013; Pérez‐Rangel 2017). Our GRADE assessment judged the quality of evidence to be low.
Complete recovery (Analysis 1.2)
All 10 included trials (N = 439; 249 intervention/190 control) reported this outcome. Burks 2012 reported desensitization in 75% of children after 22 months of oral immunotherapy; the target maintenance dose was 10 g egg white powder. Of note, the data from long‐term follow‐up of the Burks 2012 RCT participants who continued to receive oral immunotherapy daily demonstrated that 45% (18/40 oral immunotherapy‐treated participants) achieved sustained unresponsiveness by year 3, and 50% (20/40 oral immunotherapy‐treated participants) by year 4 (Jones 2016). Fuentes‐Aparicio 2013 reported that 92.5% of children achieved the desired tolerance of 10 g of whole egg. However, only 54% of children who completed the protocol had a good tolerance on the oral food challenge test with raw egg six months after finishing oral immunotherapy, and were allowed a diet containing egg without any restrictions. Dello Iacono 2013 used a six month oral immunotherapy protocol duration to achieve "maximum tolerance" by digesting 40 mL or raw egg emulsion without adverse events. None of the children could tolerate 40 mL of raw egg emulsion by the end of the oral immunotherapy protocol. In Meglio 2013 at the end of the oral immunotherapy protocol 80% of children were able to tolerate 25 mL of raw egg. Of note, just 30% of children (N = 3) tolerated a full raw egg dose without symptoms; 50% of children continued to have some symptoms shortly after digesting the target amount of raw egg. Complete desensitization in Vazquez‐Ortiz 2014 (which was evaluated by oral food challenge to one raw egg, meaning 3.8 g raw egg white) was achieved in 54% of children (N = 28). The oral immunotherapy protocol in Caminiti 2015 aimed to achieve a tolerance a 4 g of dehydrated egg white and 95% of children were successfully desensitized. Desensitized children were placed on an egg‐containing diet with two to three eggs per week for six months, following a three‐month egg avoidance diet. DBPCFC after this time period showed that only 31% of children (5/16 children) maintained the achieved tolerance; the remaining 69% (11/16) lost their desensitization and reacted to egg (Caminiti 2015).
In Escudero 2015, sustained unresponsiveness, defined as the ability to consume 2808 mg of egg white protein without symptoms in a DBPCFC by the end of the oral immunotherapy protocol was achieved in 37% of oral immunotherapy children. These children were allowed to regularly consume food containing egg and at least two undercooked eggs per week. Giavi 2016 aimed to tolerate 43.2 g of boiled egg by the end of the oral immunotherapy protocol and 36% of the children had a negative egg oral food challenge test.
The Pérez‐Rangel 2017 study reported complete desensitization, defined as ability to consume one undercooked egg (fried, scrambled, or omelet) without or with only mild adverse events every 48 hours, was achieved in 89.5% of oral immunotherapy group children by the end of the oral immunotherapy. Akashi 2017 used an oral immunotherapy protocol that was aiming to achieve tolerance of 4 g dry egg powder on oral food challenge: 57% of oral immunotherapy children reached complete desensitization.
A total of 439 children were analyzed (249 intervention/190 control). Fewer than half (45%) of children receiving oral immunotherapy were able to tolerate a full serving of egg compared to 10% of the control group (RR 4.25, 95% CI 2.77 to 6.53; RD 0.35, 95% CI 0.28 to 0.43; children = 439; studies = 10; I² = 22% for RR and I² = 86% for RD). Spontaneous tolerance, defined as the spontaneous resolution of egg allergy without applying specific treatments, was achieved in a total of 19 children: in Fuentes‐Aparicio 2013 (7 children); Vazquez‐Ortiz 2014 (5 children); Giavi 2016 (3 children); Meglio 2013 (2 children); Caminiti 2015 (1 child) and Escudero 2015 (1 child). Our GRADE assessment judged the quality of evidence to be low.
Adverse effects
Number of participants with serious adverse events (SAEs) (Analysis 1.3)
All 10 included trials (N = 439) reported occurrence of serious adverse events. A total of 21 children required epinephrine/adrenaline treatment (Vazquez‐Ortiz 2014, N = 13; Fuentes‐Aparicio 2013, N = 5; 1 each in Caminiti 2015; Escudero 2015 and Akashi 2017). In total, 21 (8.4%) of the 249 children receiving oral immunotherapy required epinephrine. No children in the control group required epinephrine. Our GRADE assessment judged the quality of evidence to be low.
Number of participants with mild‐to‐severe adverse events (Analysis 1.4)
All included trials (N = 439) reported occurrence of mild‐to‐severe adverse events (RR 8.35, 95% CI 5.31 to 13.12; RD 0.67, 95% CI 0.61 to 0.73; children = 439; studies = 10; I² = 29% for RR and I² = 82% for RD). Although all studies provided detailed reports of adverse events, there was significant heterogeneity in methods of reporting. Adverse events occurred most frequently either in the oral immunotherapy escalation phase or in association with oral immunotherapy dosing. Seventy‐five per cent of children presented with mild‐to‐severe adverse events during oral immunotherapy treatment versus 6.8% of control group children. Based on available data, we could not comment on whether over‐ or under‐reporting of adverse events is a concern, although this is a possibility. Our GRADE assessment judged the quality of evidence to be low.
In Burks 2012 (N = 55) adverse events rates were highest during the first 10 months of oral immunotherapy. However, no serious adverse events or need for epinephrine were reported. Adverse events, most of which were oral or pharyngeal, were associated with 25% of 11,860 doses of oral immunotherapy with egg and 3.9% of 4018 doses of placebo. In the oral immunotherapy group 78% of children had oral or pharyngeal adverse events compared with 20% in the placebo group (P < 0.001). After 10 months, the rate of symptoms in the oral immunotherapy group decreased to 8.3% (15,815 doses). In addition to dosing‐related symptoms, 437 other adverse events were reported; 96% were considered to be unrelated to dosing on the basis of the timing and types of symptoms.
Fuentes‐Aparicio 2013 (N = 72) described 21 children (52.5%) who had symptoms at some stage of oral immunotherapy treatment. In eight children (20%) symptoms were very mild, and moderate‐to‐severe in 13 children. Eight children required treatment with antihistamines and corticosteroids and five children required epinephrine treatment.
Dello Iacono 2013 (N = 20) reported that all children who received oral immunotherapy experienced adverse events (n = 53 events) although none resulted from accidental exposure to egg. According to Sampson’s classification, where grade 1 is the mildest anaphylactic reaction and grade 5 is severe anaphylactic reaction with loss of consciousness (Sampson 2003), three (5.6%) were grade 1, 10 (18.9%) were grade 2, 35 (66%) were grade 3, and five (9%) were grade 4. No children in the oral immunotherapy group had a grade 5 reaction, needed oral or intramuscular steroids or epinephrine, or required access emergency services. Eighty‐one per cent of adverse events occurred during administration of the first 6 mL, and 100% occurred with first administration of 20 mL hen's egg, which means that all children experienced some adverse events while increasing the oral immunotherapy dosage. The children in the oral immunotherapy group had relative risk of 4.96 (95% CI 3.30 to 7.45) for incurring an adverse event, but there were no significant differences in severity of reactions. No children discontinued treatment because of adverse events. Three children (30%) in the control group had a total of five adverse events because of accidental ingestion of trace amounts of egg. The severity grade was 3 or 4; no children required intramuscular epinephrine.
In Meglio 2013 (N = 20) 70% of children presented with mild‐to‐severe adverse events. No serious adverse events were reported.
In Vazquez‐Ortiz 2014 (N = 82), 45 children (90%) had dose‐related events including 13 who required epinephrine treatment. There were 1024 adverse events detected, corresponding to 7.6% of oral immunotherapy doses. The highest incidence of events occurred during the induction phase. The symptom distribution of adverse events were: vomiting (19.7%); lower respiratory tract involvement (18.8%); abdominal pain (15.7%); mouth itchiness (13.7%); urticaria (13.1%); rhinoconjunctivitis (7.7%); angioedema (6.7%); hoarseness (2.1%); diarrhoea (1.5%) atopic dermatitis flare (0.7%); and dysphagia (0.5%). Delayed adverse events represented a total of 4.3% of all reactions (3.8% gastro‐ intestinal plus 0.5% skin symptoms). The severity distribution of adverse events (as classified by Sampson's anaphylaxis grading, Sampson 2003) was: grade 1 = 30%; grade 2 = 31.2%; grade 3 = 15.9%; and grade 4 = 22.9%. Grade 4 was experienced by 58% of children receiving oral immunotherapy, consisting of a mild cough/wheeze in 78% of occasions. One child experienced a grade 5 reaction during the induction phase, leading to discontinuation. Multisystem involvement represented a total of 11.5% of all dose‐related adverse events. Accidental adverse events occurred in five children (15.6%) in the control group, nevertheless no epinephrine or adrenaline was needed. There was a total of 1024 adverse events in the oral immunotherapy group and seven in the control group.
Caminiti 2015 (N = 31) reported that adverse events occurred in three children during the desensitization procedure, one of whom discontinued oral immunotherapy. In the egg‐containing diet arm, one child had abdominal pain with urticaria after exercise, and another had rhinitis and/or asthma during a respiratory tract infection. One participant (5.9%) required epinephrine treatment. No adverse events were observed in the control group.
Escudero 2015 (N = 61) reported 145 allergic reactions as adverse events during oral immunotherapy in 70% (N = 21) of children, presented mainly in the escalation phase (70%, N = 21), followed by the build‐up phase (53%, N = 16) and reducing to 33% (N = 10) in the maintenance phase. Ninty‐eight per cent (98%) of children experienced mild symptoms and 2% had a moderate allergic reaction. In one child (0.04%) epinephrine treatment was needed due to a systemic reaction (rhinitis, urticaria, and mild respiratory distress). The protocol was modified for this child by reducing the oral immunotherapy dose by 50%. The most common adverse events were gastro‐intestinal (82%), oropharyngeal symptoms (21.5%), rhinitis (11.4%), respiratory distress (6.3%), and generalized urticaria (3.8%). Moreover, 7% of children (N = 2) withdrew from the study for non‐severe repeated allergic reactions (abdominal pain and vomiting).
Giavi 2016 (N = 29) reported that all children, except one in the oral immunotherapy group, experienced at least one adverse event during the course of treatment. There was no significant difference between the hydrolysed egg and placebo groups with respect to type of adverse events.
In Pérez‐Rangel 2017 (N = 33), safety data during the first control randomized oral immunotherapy period, which was included in our analysis, was received from the authors following personal communication (Ibanez Sandin MD 2017 [pers comm]). Fifteen of 18 children presented with adverse events in the escalation phase (n = 40 adverse events). These included: oropharyngeal symptoms (n = 29); gastro‐intestinal symptoms (n = 17); cutaneous symptoms (n = 4); and rhinitis (n = 4). All adverse events were reported to be mild. At the beginning of the build‐up phase nine of 17 children presented with adverse events (n = 45 adverse events). All adverse events were mild, and the distribution among organ systems were similar to the build‐up phase: oropharyngeal symptoms (n = 37); gastro‐intestinal symptoms (n = 20); cutaneous symptoms (n = 10); rhinitis (n = 1); and asthma (n = 1). Five months after baseline in the maintenance phase, 45 mild adverse events were reported: oropharyngeal symptoms (n = 39); gastro‐intestinal symptoms (n = 10); cutaneous symptoms (n = 18); rhinitis (n = 4); and asthma (n = 2). Participants could present multiple symptoms in the same adverse event.
Akashi 2017 (N = 36) reported that 17 of 18 children in the oral immunotherapy group experienced adverse events: vomiting (N = 4), diarrhoea (N = 5), urticaria or angioedema (N = 6), and respiratory symptoms including coughing and wheezing (N = 3). Of the three children with respiratory symptoms, one developed persistent asthma. Eight children had oral cavity itchiness and six children had mild abdominal pain, but no children required an epinephrine injection. A total of 32 mild‐to‐severe adverse events were reported.
Medication used due to adverse events
Burks 2012 mentioned that only one child received prednisone but without specifying the route, dose, or duration of treatment. In Fuentes‐Aparicio 2013 antihistamine therapy was administrated for 10 cases, steroids in nine cases, B2‐agonists in five cases, and epinephrine treatment in five cases. The administration route, dose, and duration of these medications were not reported. As mentioned previously, all children in Meglio 2013 received cetirizine treatment orally (0.25 mg/kg/day) for the duration of the study, but no other medication was reported (Meglio 2013). In Dello Iacono 2013, information on medication used was reported for both groups, in association with oral immunotherapy dose for the experimental group and for traces of egg in the control group. Unfortunately, the number of cases in which antihistamine treatment was used was not clearly reported in the oral immunotherapy group. In the control group there were three cases requiring treatment. Nebulized epinephrine was used in two cases in the oral immunotherapy group and in two cases in the control group. There were three children in the oral immunotherapy group who needed B2‐agonists, and no cases were documented for steroid administration in the oral immunotherapy group. Additionally, there were two children in the control group who required oral steroid therapy. No information was provided for dose or duration. In Vazquez‐Ortiz 2014 children with asthma on preventive treatment continued therapy during oral immunotherapy. Furthermore, according to the study protocol, antihistamines were indicated for adverse events during oral immunotherapy: rhinoconjunctivitis or skin symptoms, inhaled salbutamol for mild cough or wheeze, and epinephrine for moderate or severe anaphylaxis. There were 18 epinephrine injections in 13 cases, salbutamol was given on 159 occasions and antihistamines in 475, but without specifying the route, dose, or duration of the treatment. Caminiti 2015 reported three cases that required treatment: in one case intramuscular adrenaline, steroid, cetirizine, and inhaled salbutamol was used and oral immunotherapy was discontinued. In the second case oral antihistamine was used, and in the other case inhaled bronchodilators and steroids were used. There were no data available regarding dose or duration of treatment. Escudero 2015 reported only one event where medication was needed ‐ the child required epinephrine treatment; subsequently, the oral immunotherapy protocol was reduced by 50%. No other treatments were reported. Giavi 2016 did not report requirement for medication during oral immunotherapy treatment, despite the presence of adverse events. In Pérez‐Rangel 2017 all children received 10 mg of cetirizine daily during the build‐up phase and for half of the maintenance phase. The study authors did not report whether any medications were used to treat adverse events during the blinded phase of oral immunotherapy, but did report the use of antihistamines, corticosteroids, inhaled short‐acting B2‐broncodilatator and intramuscular adrenaline/epinephrine during the second, open phase of the study. Akashi 2017 reported use of antihistamines for recurrent adverse events, however there were no data available on how many times such a treatment was used during oral immunotherapy. The administration route, dose, and duration of these medications were not reported.
Immunological changes
Skin prick test (SPT)
Nine studies (403 children; 231 oral immunotherapy; 172 control/placebo) reported performing SPT at baseline (Burks 2012;Caminiti 2015;Dello Iacono 2013;Escudero 2015;Fuentes‐Aparicio 2013; Giavi 2016;Meglio 2013;Pérez‐Rangel 2017; Vazquez‐Ortiz 2014) and it was performed at the end of oral immunotherapy in seven studies (total number of children = 292; oral immunotherapy = 166; control/placebo = 126) (Burks 2012;Caminiti 2015;Dello Iacono 2013;Escudero 2015; Fuentes‐Aparicio 2013Meglio 2013;Pérez‐Rangel 2017). There were non‐significant differences between children in the oral immunotherapy and control groups before starting immunotherapy. A significant difference in SPT wheal size was found at the end of oral immunotherapy in all seven studies that performed the test (Table 1). Moreover, Burks 2012 showed that a decrease in wheal size from baseline to 22 months (P = 0.009) was correlated with sustained unresponsiveness at 24 months (P = 0.005).
| Study name | Oral immunotherapy | Control/placebo | Oral immunotherapy versus control/placebo | |||||
| Pre‐treatment | Post‐treatment | P value | Pre‐treatment | Post‐treatment | P value | P value pre‐treatment | P value post‐treatment | |
| 10.5 (2.5 to 26.0) | not available | not available | 13.0 (7.5 to 20.0) | not available | not available | not significant | P = 0.02 | |
| 11.0 (6.5 to 18) | 9.2 | P = 0.05 | 9.0 (6.0 to 16.0) | 10.0 | not available | not significant | P = 0.88 | |
| 10.0 (7.0 to 15.0) | 5.0 (4.0 to 13.0) | not available | 9.25 (5.5 to 15.0) | 10.0 (5.5 to 15.0) | not available | P = 0.976 | P = 0.007 | |
| 6.0 (3.0 to 11.0) | 5.0 (3.0 to 8.0) | P = 0.001 | 6.0 (3.0 to 12.0) | 5.5 (0 to 13.0) | P = 0.45 | P = 0.2 | P = 0.16 | |
| 8.74 (4 to 16) | not available | P < 0.001 | 9.68 (3.0 to 16.0) | not available | not available | not available | not available | |
| 5.5 (2.5 to 7.0) | 3.5 (1.0 to 5.0) | P < 0.01 | 4.0 (1.0 to 7.0) | 6.0 (1.0 to 8.0) | P = NS | not available | not available | |
| 7.0 (5.0 to 10.0) | not available | not available | 7.0 (4.0 to 12.0) | not available | not available | not available | P < 0.05 | |
Serologic testing
Specific IgE (sIgE) levels at baseline and at the end of the oral immunotherapy protocol were investigated by using different laboratory methods in each study. However, there were no data available for sIgE levels at the end of the oral immunotherapy protocol in Vazquez‐Ortiz 2014. For sIgE determination Burks 2012, Caminiti 2015, Escudero 2015, Giavi 2016, Pérez‐Rangel 2017, Vazquez‐Ortiz 2014 used the Thermo Immuno‐CAP system (Fisher Scientific); Dello Iacono 2013 and Fuentes‐Aparicio 2013 used the Phadia CAP System fluorescence enzyme immunoassay (FEIA) (Phadia Diagnostics); Meglio 2013 used the Realtest Reverse Enzyme Allergo Sorbent Test (REAST) (Lofarma) and an allergen micro array assay (Immuno Solid‐phase Allergen Chip ISAC; VBC Genomics Bioscience Research, Vienna, Austria) in accordance with the manufacturer’s recommendations. A panel of 104 allergens (inhalants and foods), that also contained the following five purified natural hen's egg allergens: ovomucoid (Gal d 1), ovalbumin (Gal d 2), ovotransferrin (Gal d 3), lysozyme (Gal d 4), and serum albumin (Gal d 5), was used. Akashi 2017 used CAP system for sIgE determination. Because of the differences in the upper limit of measurement it was impossible to combine data.
Nevertheless, two studies reported a statistically significantly decreased levels of egg sIgE antibody after oral immunotherapy compared to control (Burks 2012; Dello Iacono 2013). In Dello Iacono 2013 (N = 20) the difference in the reduction of IgE between pre‐ and post‐oral immunotherapy was ‐14.4 kUA/L (range ‐27.6 to 0.1) in the oral immunotherapy group and 2 kUA/L (range ‐8.9 to ‐13.8) in the control group (P < 0.001). Futhermore, the median reduction in sIgE levels from baseline to the end of oral immunotherapy protocol for egg oral immunotherapy group was not statistically significantly greater than that for control group (Akashi 2017; Burks 2012; Caminiti 2015; Escudero 2015; Fuentes‐Aparicio 2013; Giavi 2016; Pérez‐Rangel 2017). Meglio 2013 (N = 20) reported statistically significant reduction for sIgE before and after oral immunotherapy protocol for oral immunotherapy group: for ovomucoid (Gald1) by REAST (20.9 ± 45.6 versus 14.8 ± 30.7; P = 0.02), and for both ovomucoid (Gald1) (6.67 ± 8.36 versus 1.78 ± 1.74; P < 0.01) and ovalbumin (Gald2) measured by ISAC method (2.92 ± 5.05 versus 0.74 ± 1.22; P < 0.02), respectively. There were no differences in reduction of sIgE measured by REAST technique from baseline compared with the final point of the study in the control group. Interestingly, there was a statistically significant increase in ovomucoid (Gald1) measured using the ISAC method in the control group at the end of the study (5.32 ± 6.89 versus 7.81 ± 10.53; P < 0.05). In Caminiti 2015 (N = 31), the egg‐specific IgE level after oral immunotherapy was 34.2 kUA/L in the intervention group and 38.9 kUA/L in the placebo group. Of note, follow‐up of these children showed that at 10 months, formerly active oral immunotherapy children who continued with an egg‐containing diet for the following six months had significantly lower sIgE levels compared to baseline (37.6 versus 12.2 kUA/L, P = 0.02). Escudero 2015 (N = 61) reported a statistically significant decrease from baseline to the end of oral immunotherapy in both groups only for ovalbumin IgE (6.3 kUA/L (0.7 to 185) versus 2.2 kUA/L (0.3 to 192), P < 0.001) and 2.2 kUA/L (0.7 to 43.5) versus 1.3 kUA/L (0.3 to 32.3), P = 0.01); no differences were seen for ovomucoid or egg white IgE. Akashi 2017 (N = 36) reported a statistically significant decrease in sIgE levels from baseline to the end of the study in the control group (median 36.4 versus 30.6 kUA/mL; P < 0.05). It was not possible to extrapolate data for sIgE antibodies in Burks 2012, Fuentes‐Aparicio 2013, or Pérez‐Rangel 2017. In Giavi 2016 (N = 29) no statistically significant difference was observed regarding sIgE levels (change over time expressed as median (min‐max) ‐3.230 kUA/L (‐8.90 to 0.42); P = 0.29).
Eight studies (total number of children = 337; oral immunotherapy = 189; control/placebo = 148) evaluated changes in egg‐specific IgG4 antibodies and all eight showed a statistically significant increase in the level of these antibodies after oral immunotherapy (Akashi 2017; Burks 2012; Caminiti 2015; Escudero 2015; Fuentes‐Aparicio 2013; Giavi 2016; Meglio 2013; Pérez‐Rangel 2017). Akashi 2017 (N = 36) demonstrated a statistically significant increase of egg white‐specific IgG4 in the oral immunotherapy group after completing the oral immunotherapy protocol (median, 13 U/mL at baseline to 94 U/mL at the end of oral immunotherapy; P < 0.01), whereas such a change was absent in the control group (median, 13 U/mL at baseline to 13 U/mL; P = 1.00). In Burks 2012 (N = 55) the median reduction of egg‐specific IgG4 by the end of oral immunotherapy for the oral immunotherapy group was significantly higher (median, 48.5 kU/L range ‐0.1 to 162.1; P < 0.01) compared to the placebo group (there were no numerical data available for the placebo group). Caminiti 2015 (N = 31) reported a significant increase of the mean egg‐specific IgG4 levels by the end of oral immunotherapy in intervention group children (29.2 µg/mL versus 0.9 µg/mL, P = 0.001). In Escudero 2015 (N = 61) there was an increase in median egg‐specific IgG4 observed from baseline to the end of oral immunotherapy in the oral immunotherapy group (0.4 mg/L (0.1 to 6.2) versus 4.4 mg/L (0.1 to 30), P = 0.0001). Giavi 2016 (N = 29) reported a significant increase over time from baseline to the end of oral immunotherapy in specific IgG4 in the active group (expressed as change over time, median (range): for egg yolk IgG4 (0.10 mg/L, 0.00 to 1.71, P = 0.01) and for ovalbumin IgG4 (0.11 mg/L, ‐0.00 to 3.59, P = 0.04); there were no differences observed in the median change of IgG4 levels for egg white (0.07 mg/L, ‐0.31 to 2.54, P = 0.07) and for ovomucoid (0.00 mg/L, ‐0.56 to 1.04, P = 0.14). Meglio 2013 (N = 20) found a statistically significant increase in the level of IgG4 only for ovalbumin (Gald2) at the end of oral immunotherapy (average, ± SD 2.6 mg/L (± 0.4) versus 2.95 mg/L (± 0.4); P = 0.02), but not for ovomucoid (Gald1) (average, ± SD 0.9 mg/L (± 0.7) versus q.8 mg/L (± 1.5). Data for the egg‐specific IgG4 levels were presented graphically in two studies and could not be extracted for analysis (Fuentes‐Aparicio 2013; Pérez‐Rangel 2017).
In addition, six studies (281 children; oral immunotherapy = 161; control/placebo = 120) showed a statistically significant increase in IgG4 compared to the control group (Burks 2012; Caminiti 2015; Escudero 2015; Fuentes‐Aparicio 2013; Giavi 2016; Pérez‐Rangel 2017). In Caminiti 2015 (N = 31) egg‐specific IgG4 levels after oral immunotherapy were statistically significantly higher in the intervention group (29.2 µg/mL) than in the placebo group (1.5 µg/mL, P = 0.001). Follow‐up of these children showed that at 10 months, formerly active oral immunotherapy children who continued with egg‐containing diet for the following six months had significantly higher sIgG4 levels compared to baseline (32.4 versus 0.9 µg/mL, P = 0.001). Median sIgG4 levels in Escudero 2015 (N = 61) were higher in the oral immunotherapy group by the end of oral immunotherapy than in the control group (4.4 mg/L (0.1 to 30) versus 0.4 mg/L (0.1 to 7.5); P = 0.001). Giavi 2016 (N = 29) reported that a greater increase of egg‐specific IgG4 occurred in the oral immunotherapy group compared to placebo by the end of oral immunotherapy, however these data were not reported. It was not possible to extrapolate precise data for sIgG4 from Burks 2012, Fuentes‐Aparicio 2013 and Pérez‐Rangel 2017 because data were reported graphically.
Two studies reported a significant reduction in basophil activation test in the oral immunotherapy group compared to placebo at the end of treatment (Burks 2012; Giavi 2016) (84 children; oral immunotherapy group = 55; placebo group = 29): in Burks 2012 the differences in CD63 activation were statistically significant (0.01 μg/mL, P = 0.002; 0.1 μg/mL, P = 0.001). In Giavi 2016 a significant decrease in percentage of CD203c+ cells (P = 0.04) occurred and there was a trend for a lower percentage of CD63+ cells (P = 0.07).
Meglio 2013 (N = 20) performed cytokines (IL‐4, IL‐5, IL‐6, IL‐10, IL‐12, IL‐13), interferon‐gamma and tumour necrosis factor‐alfa analysis and found a statistically significant increase of IL‐5 levels in the oral immunotherapy group at the end of treatment (mean, 19.00 ± 9.4 pg/mL; range = 5.00 to 32.00 versus 28.13 ± 14.7 pg/mL; range, 12.00 to 56.00; P = 0.03).
Quality of life and cost‐effectiveness
There were no data available regarding quality of life or cost‐effectiveness.
Discussion
Summary of main results
Egg oral immunotherapy appears to be an effective treatment option to induce desensitization in children with immunoglobulin E (IgE)‐mediated egg allergy, despite a difference in immunotherapy protocols. Nevertheless, oral immunotherapy is an alternative to the current therapeutic mainstay of an avoidance diet. Oral immunotherapy may have a positive effect on overall quality of life, including positive nutritional consequences and the potential avoidance of allergy related emergencies.
Nearly half (45%) of children receiving oral immunotherapy were able to tolerate a full serving of egg compared to 10% of the control group (RR 4.25, 95% CI 2.77 to 6.53; RD 0.35, 95% CI 0.28 to 0.43; children = 439; studies = 10; I² = 22% for RR and I² = 86% for RD). Our GRADE assessment judged the quality of evidence to be low (summary of findings Table for the main comparison). We found that 82% of children receiving oral immunotherapy increased the amount of egg they could tolerate during the treatment period (RR 7.48, 95% CI 4.91 to 11.38; RD 0.73, 95% CI 0.67 to 0.80; children = 410; studies = 9; I² = 27% for RR and I² = 73% for RD). Our GRADE assessment judged the quality of evidence to be low (summary of findings Table for the main comparison). There were differences in the levels required for partial desensitization (defined as an increase in the threshold dose, not reaching one complete raw egg) achieved. Such differences may be due to different egg oral immunotherapy protocols used in the included trials. Moreover, it seems that regular consumption of uncooked egg and other egg‐containing food after stopping oral immunotherapy may be helpful to achieve sustained unresponsiveness to egg allergy. It was reported that 16 children who received oral immunotherapy achieved desensitization after six months of an egg‐containing diet, but after three months of an egg‐avoidance diet, only five children maintained tolerance to re‐introduction of eggs to their diet (Caminiti 2015). Of note, long‐term follow up of Burks 2012 reported that 50% of the children who were treated with egg oral immunotherapy in the original cohort achieved a sustained unresponsiveness by the fourth year of oral immunotherapy.
There is a possibility that oral immunotherapy may modulate immunological response (Jones 2016; Wright 2016). Seven studies reported a significant reduction in wheal diameter on skin prick test after completion of oral immunotherapy (Burks 2012;Caminiti 2015;Dello Iacono 2013;Escudero 2015;Fuentes‐Aparicio 2013; Meglio 2013;Pérez‐Rangel 2017). Moreover, two studies showed a reduction in egg‐specific immunoglobulin E (sIgE) levels versus control (Burks 2012; Dello Iacono 2013). Two further studies showed a reduction in egg sIgE levels versus baseline in children who received oral immunotherapy (Escudero 2015; Meglio 2013). Of note, all eight studies that evaluated egg sIgG4 levels showed an increase in egg sIgG4 levels after oral immunotherapy (Akashi 2017; Burks 2012;Caminiti 2015;Escudero 2015;Fuentes‐Aparicio 2013; Giavi 2016;Meglio 2013;Pérez‐Rangel 2017). Furthermore, two studies demonstrated a significant reduction in basophil activation in the oral immunotherapy group compared to placebo at the end of treatment (Burks 2012;Giavi 2016). However, none of the immune parameters tested in the included studies were consistently predictive of the oral immunotherapy treatment outcomes (Akashi 2017; Burks 2012;Caminiti 2015;Dello Iacono 2013;Escudero 2015;Fuentes‐Aparicio 2013; Giavi 2016;Meglio 2013;Pérez‐Rangel 2017; Vazquez‐Ortiz 2014). More data are needed to better understand the underlying mechanism that might be induced by oral immunotherapy.
It is important to note that 75% of children in the intervention groups experienced at least one adverse event during oral immunotherapy (RR 8.35, 95% CI 5.31 to 13.12; RD 0.67, 95% CI 0.61 to 0.73; children = 439; studies = 10; I² = 29% for RR and I² = 82% for RD). Our GRADE assessment judged the quality of evidence to be low (summary of findings Table for the main comparison). Most symptoms were related to the build‐up phase in association with oral immunotherapy dosing. However, most symptoms were mild and self‐limiting. We found that 8.4% of children had a serious adverse event, requiring epinephrine/adrenaline administration (effect not estimable, our GRADE assessment judged the quality of evidence to be low, summary of findings Table for the main comparison). Because adverse events were defined differently among the included studies, it is difficult to comment on whether these were under‐ or over‐estimated. Caminiti 2015 reported 10 adverse events, but Vazquez‐Ortiz 2014 reported 1024 adverse events. Surprisingly, only one study showed a high level of serious adverse events (Vazquez‐Ortiz 2014): 13 children required epinephrine/adrenaline administration 18 times, and one grade 5 reaction occurred (according to the Sampson 2003 classification scheme). Vazquez‐Ortiz 2014 reported that available treatments were insufficiently effective. The risks associated with administering oral immunotherapy need to be evaluated against the 'real life' risks of standard care, namely an avoidance diet, although it is difficult to accurately estimate the true rate of accidental allergic reactions.
We found that reporting on different potential medications was poor. Although four included studies provided detailed information about antihistamine, steroid, epinephrine/adrenaline, and B2‐agonists administration in association with oral immunotherapy dose, and symptoms that occurred on those specific occasions, information on administration route, dose and duration of use was absent (Caminiti 2015; Dello Iacono 2013; Fuentes‐Aparicio 2013; Vazquez‐Ortiz 2014). Only Meglio 2013 and Pérez‐Rangel 2017 administrated antihistamine treatment as a co‐intervention with oral immunotherapy. It was therefore difficult to assess whether oral immunotherapy‐induced adverse allergic reactions could be avoided. Likewise, because Akashi 2017, Burks 2012 and Giavi 2016 did not provide specific information regarding medications used for adverse events (antihistamines, steroids, epinephrine/adrenaline, B2‐agonists), it was difficult to assess the extent of oral immunotherapy‐induced adverse events. No study reported on drug administration route, dose and duration of such therapy.
Sclar 2014 reported that anaphylaxis is often underestimated. In a study of food‐related allergic reactions in children, the most common reason given for lack of epinephrine/adrenaline administration to children experiencing a severe adverse event was that the event was not recognized as severe (47.7% of cases in which epinephrine/adrenaline was not used) (Fleischer 2012).
Overall, the dropout rate, mainly due to adverse events, has been reported at 15% to 20% in oral immunotherapy trials (Khoriaty 2013).The dropout rate data from Akashi 2017, Burks 2012, Caminiti 2015, Giavi 2016, Vazquez‐Ortiz 2014 agrees with the information reported previously in Khoriaty 2013. However, the withdrawal rate in the other five studies (Dello Iacono 2013; Escudero 2015; Fuentes‐Aparicio 2013; Meglio 2013; Pérez‐Rangel 2017) was surprisingly low, with Dello Iacono 2013 having no dropouts: it may be that participant collaboration is easier in a smaller study, perhaps because there is more medical attention. Dello Iacono 2013 did not discuss their high adherence rate within the study. Meglio 2013 discussed the high adherence rate in their study, giving as the possible explanation a longer intervention period; the protocol took longer than the expected period (planned 181 days) with a mean of 219 days (range 178 to 287 days). The very gradual protocol that was adopted may encourage more safety and more parental collaboration as the percentage increment between doses was the same and there were no dose 'jumps' in the daily egg administrations for the entire period of desensitization. Moreover, co‐intervention with antihistamine was used in their study. More studies are needed to confirm or to disprove such a hypothesis.
Overall completeness and applicability of evidence
All included studies addressed the primary outcome of complete tolerance of one egg serving. The 10 included studies included only children and recruitment selection bias was possible. No included studies reported on adults. The study population characteristics suggest that the included studies may be generalizable to a larger population group. Oral immunotherapy appears to be effective both in young children and in later childhood. However, children aged less than three years were included in only Giavi 2016, but the sample size was too small to draw any conclusions. More studies are needed in this age group. Nevertheless, one randomized controlled trial is registered in clinical.trials.gov that will also include adults (NCT02083471). Another factor that may influence the development of desensitization is the presence of anaphylaxis. Of the 10 included studies, two included children with a history of anaphylaxis (Dello Iacono 2013; Fuentes‐Aparicio 2013). Oral immunotherapy appeared to be effective regardless of anaphylaxis history.
Oral immunotherapy both with and without an antihistamine co‐intervention was included in the review; this did not seem to affect the treatment effect.
Of note, 45% of children achieved full tolerance after oral immunotherapy and could ingest a full serving of egg without adverse effect; these children were able to continue diets that included egg. However, concerns about compliance and interruption due to sickness should be addressed.
We found that 82% of children could tolerate a partial serving of egg, reducing dietary limitations, and risk of serious adverse event. Adverse events are likely to be the most important factors to be considered when applying evidence to practice. The difference in reporting methods for symptoms during oral immunotherapy makes those symptoms complicated to quantify. As previously mentioned, there is a risk of both under‐ or over‐estimation. The need for parenteral epinephrine treatment could be a reflection of serious adverse events. Five studies reported the data of children in the oral immunotherapy group who needed epinephrine/adrenaline treatment (Akashi 2017; Caminiti 2015; Escudero 2015; Fuentes‐Aparicio 2013; Vazquez‐Ortiz 2014). Requirement was as high as 26% of the oral immunotherapy group population (Vazquez‐Ortiz 2014). On the other hand, frequent, milder symptoms during oral immunotherapy might influence participants’ quality of life and compliance. Inquiring about the study participants' acceptance of this therapy would be insightful. If applied to practice, physicians would have to cautiously consider, and discuss with the participant at length, whether the risks are acceptable; and to ensure good compliance of the children's parents or guardians.
With one exception, all children in the included studies started oral immunotherapy during hospital admission, as day patients, or in a research centre. Akashi 2017 started oral immunotherapy treatment at the child's home, but with medical personnel available to intervene if allergic reactions occurred. During the build‐up phase children were closely monitored during visits to the clinic or research centre, where close follow‐up and individualized guidance was provided. Whether these time and personnel commitments are feasible in practice could be a factor, and are dependent on the institution providing the oral immunotherapy.
There was no information available regarding children's and their families quality of life during oral immunotherapy. It could be speculated that a high rate of even mild adverse events may negatively influence the everyday life of participants, and in the case of children, their caregivers.
Quality of the evidence
According to the GRADE approach described in Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), the overall judgement of the quality of the body of evidence contributing to the results of the review is low. The reasons for downgrading evidence was the high likelihood of bias and imprecision of results (few events and a small number of participants). High likelihood of bias is suspected because of the methodological limitations in the studies, resulting in possible selection, performance, and detection bias. The confidence intervals were wide because of small sample sizes and variability in the estimated treatment effect. Four studies did not perform a sample size calculation and this could be a source of random error risk (Akashi 2017; Fuentes‐Aparicio 2013; Meglio 2013; Pérez‐Rangel 2017). The random error is closely related to imprecision. The results of smaller studies are subject to greater sampling variation and hence are less precise. Imprecision is reflected in the confidence interval around the intervention effect estimate from each study and in the weight given to the results of each study in the meta‐analysis (Higgins 2011). However, there was a consistently positive treatment effect of oral immunotherapy despite clinical heterogeneity, although a low I² value reflects non‐substantial statistical heterogeneity, and differences in oral immunotherapy protocols among studies.
We did not include a sufficient number of studies to create a funnel plot to assess publication bias. Given few included studies, most of which detected statistically significant results, we could not rule out the presence of reporting bias. The strength of the evidence was that there was a consistently positive treatment effect, despite clinical heterogeneity in participant characteristics and oral immunotherapy protocols. Furthermore, we could not rule out the possibility of under‐or over‐reporting of adverse events during oral immunotherapy.
Potential biases in the review process
A strength of this review was the thorough search strategy, including several databases, conference papers, and trial registries, to minimize the possibility of missing studies. A possible source of bias relates to the exclusion of potentially relevant studies when requests to the authors for additional information went unanswered. These studies are listed in the Characteristics of studies awaiting classification tables. Moreover, some studies that fulfilled our criteria were excluded because they combined results for immunotherapy for two or more foods. For example, Staden 2007, fulfilled the eligibility criteria but results for both egg and milk immunotherapy were combined in the published article and we were unable to split the data to focus only on egg allergy. It is possible that the inclusion of such data could have altered the results of the meta‐analysis. The ongoing studies (NCT02083471; NCT01846208) emphasize the need for frequent updates of this review as oral immunotherapy for egg allergy continues to be a topic of active research. Ongoing and future studies could potentially affect our conclusions.
Agreements and disagreements with other studies or reviews
To our knowledge, this is the only systematic review on immunotherapy specifically for egg allergy. The findings of our review are in agreement with a systematic review and meta‐analysis on food allergies that included evaluation of egg oral immunotherapy as a subgroup (Nurmatov 2017).
Nurmatov 2017 included nine studies in the egg oral immunotherapy subgroup (Burks 2012;Caminiti 2015;Dello Iacono 2013;Escudero 2015;Fuentes‐Aparicio 2013Meglio 2013;Morisset 2007;Patriarca 1998;Staden 2007). Nurmatov 2017 excluded Vazquez‐Ortiz 2014, and did not include three studies included in this review (Akashi 2017; Giavi 2016;Pérez‐Rangel 2017). This was probably due to the last search date in Nurmatov 2017, which was 31 March 2016. We did not include Morisset 2007, Patriarca 1998 and Staden 2007 because these studies combined results for egg and milk allergy.
Nurmatov 2017 found that oral immunotherapy substantially reduced the risk for egg allergy (RR hen's egg = 0.22, 95% CI 0.11 to 0.45). Of note, safety data remain a challenge. Nurmatov 2017 pooled safety data for three food allergies (cow's milk, egg, and peanut allergies), making comparisons difficult.
We included 10 studies that reported significant numbers of adverse events during oral immunotherapy (Vazquez‐Ortiz 2014), which was not included in Nurmatov 2017. Another difference regarding safety between our review and Nurmatov 2017 was documentation of serious adverse events of oral immunotherapy treatment, requiring epinephrine/adrenaline administration. This was not reported in Nurmatov 2017. Moreover, medication used for the treatment of adverse events was not reported in Nurmatov 2017.
An outcome in both our review and in Nurmatov 2017 was assessment of changes in disease‐specific quality of life using a validated instrument. Results were similar in both reviews: both reported lack of quality of life data.
We agree with conclusions made by the authors of Nurmatov 2017 that oral immunotherapy may be effective in increasing desensitization in participants with IgE‐mediated egg allergy, and that oral immunotherapy is associated with a modest increased risk in serious systemic adverse events and a substantial increase in mild‐to‐severe adverse events.
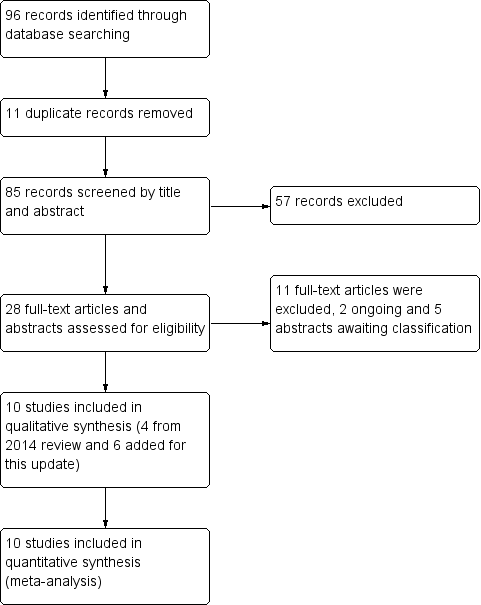
Study flow diagram.
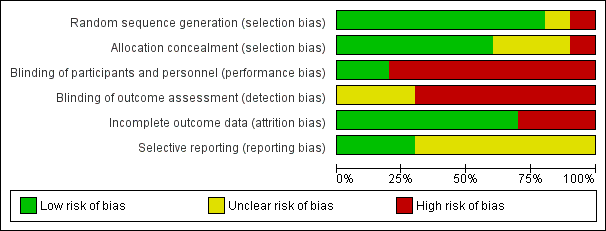
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Comparison 1 Oral and sublingual immunotherapy versus no therapy for egg allergy, Outcome 1 Increase in the amount of egg that can be tolerated.

Comparison 1 Oral and sublingual immunotherapy versus no therapy for egg allergy, Outcome 2 Complete recovery.

Comparison 1 Oral and sublingual immunotherapy versus no therapy for egg allergy, Outcome 3 Number of participants with serious adverse events.

Comparison 1 Oral and sublingual immunotherapy versus no therapy for egg allergy, Outcome 4 Number of participants with mild‐to‐severe adverse events.
| Oral and sublingual immunotherapy versus no therapy for egg allergy | ||||||
| Population: children with egg allergy Setting: hospitals Comparison: placebo or egg‐free diet. (Three studies used placebo and seven studies used an egg avoidance diet as controls) | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Oral immunotherapy versus no therapy for egg allergy | |||||
| Increase in the amount of egg that could be tolerated | Study population | RR 7.48 | 410 | ⊕⊕⊝⊝ | 82% of children in the oral immunotherapy group could ingest a partial serving of egg (1 g to 7.5 g) compared to 10% of the control group. | |
| 102 per 1000 | 763 per 1000 | |||||
| Complete recovery | Study population | RR 4.25 | 439 | ⊕⊕⊝⊝ | 45% of children receiving oral immunotherapy were able to tolerate a full serving of egg compared to 10% of the control group. | |
| 100 per 1000 | 425 per 1000 | |||||
| Numbers of children with serious adverse events | See comment | See comment | Not estimable | 439 | ⊕⊕⊝⊝ | All 10 trials reported numbers of children with serious adverse events (SAEs): SAEs requiring epinephrine/adrenaline occurred in 21/249 (8.4%) of children in the oral immunotherapy group and none in the control group. Because adverse events were classified differently among the studies, it is difficult to comment on whether they were under‐ or over‐estimated. Surprisingly, only one study showed a high level of SAEs (Vazquez‐Ortiz 2014): 13 children required epinephrine/adrenaline administration 18 times, and one grade 5 reaction occurred. |
| Number of children with mild‐to‐severe adverse events | Study population | RR 8.35 | 439 | ⊕⊕⊝⊝ | Mild‐to‐severe adverse events were frequent; 75% of children presented mild‐to‐severe adverse events during oral immunotherapy treatment versus 6.8% of children in the control group. | |
| 68 per 1000 | 568 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| The assumed risk is the risk of the control arm 1 Downgraded one level because of risk of bias: all studies were assessed at high or unclear risk of bias in at least one domain. | ||||||
| Study name | Oral immunotherapy | Control/placebo | Oral immunotherapy versus control/placebo | |||||
| Pre‐treatment | Post‐treatment | P value | Pre‐treatment | Post‐treatment | P value | P value pre‐treatment | P value post‐treatment | |
| 10.5 (2.5 to 26.0) | not available | not available | 13.0 (7.5 to 20.0) | not available | not available | not significant | P = 0.02 | |
| 11.0 (6.5 to 18) | 9.2 | P = 0.05 | 9.0 (6.0 to 16.0) | 10.0 | not available | not significant | P = 0.88 | |
| 10.0 (7.0 to 15.0) | 5.0 (4.0 to 13.0) | not available | 9.25 (5.5 to 15.0) | 10.0 (5.5 to 15.0) | not available | P = 0.976 | P = 0.007 | |
| 6.0 (3.0 to 11.0) | 5.0 (3.0 to 8.0) | P = 0.001 | 6.0 (3.0 to 12.0) | 5.5 (0 to 13.0) | P = 0.45 | P = 0.2 | P = 0.16 | |
| 8.74 (4 to 16) | not available | P < 0.001 | 9.68 (3.0 to 16.0) | not available | not available | not available | not available | |
| 5.5 (2.5 to 7.0) | 3.5 (1.0 to 5.0) | P < 0.01 | 4.0 (1.0 to 7.0) | 6.0 (1.0 to 8.0) | P = NS | not available | not available | |
| 7.0 (5.0 to 10.0) | not available | not available | 7.0 (4.0 to 12.0) | not available | not available | not available | P < 0.05 | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Increase in the amount of egg that can be tolerated Show forest plot | 9 | 410 | Risk Ratio (M‐H, Fixed, 95% CI) | 7.48 [4.91, 11.38] |
| 2 Complete recovery Show forest plot | 10 | 439 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.25 [2.77, 6.53] |
| 3 Number of participants with serious adverse events Show forest plot | 10 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4 Number of participants with mild‐to‐severe adverse events Show forest plot | 10 | 439 | Risk Ratio (M‐H, Fixed, 95% CI) | 8.35 [5.31, 13.12] |