Intervenciones para la promoción del ejercicio habitual en pacientes con cáncer o que han presentado la enfermedad
Información
- DOI:
- https://doi.org/10.1002/14651858.CD010192.pub2Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 24 septiembre 2013see what's new
- Tipo:
-
- Intervention
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Cáncer ginecológico, neurooncología y otros cánceres
- Copyright:
-
- Copyright © 2015 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
All authors contributed to the design, development and drafting of the protocol for this review. LB and KEH conducted screening and data extraction, with assistance from DJR and SJCT. LS conducted analysis of the trials according to the CALO‐RE taxonomy. MAT, LS, DJR, KAR, SJCT and JMS assisted with interpretation of results and drafting of the final report. LB led the final report.
Sources of support
Internal sources
-
None, Not specified.
External sources
-
None, Not specified.
Declarations of interest
The authors have no conflicts of interest to report.
Acknowledgements
We thank Jane Hayes for designing the search strategy and Clare Jess, Gail Quinn and Dr Chris Williams for their contributions to the editorial process. We thank Mr David Salisbury for assisting with the organisation of the screening process. We thank Dr Dawn Carnes for independently reviewing the risk of bias in the lead authors' published trials. We would like to thank Mr John Batchelor for assistance in drafting the plain language summary of findings.
The National Institute for Health Research (NIHR) is the largest single funder of the Cochrane Gynaecological Cancer Group. The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the NIHR, the NHS or the Department of Health.
Version history
| Published | Title | Stage | Authors | Version |
| 2018 Sep 19 | Interventions for promoting habitual exercise in people living with and beyond cancer | Review | Rebecca R Turner, Liz Steed, Helen Quirk, Rosa U Greasley, John M Saxton, Stephanie JC Taylor, Derek J Rosario, Mohamed A Thaha, Liam Bourke | |
| 2013 Sep 24 | Interventions for promoting habitual exercise in people living with and beyond cancer | Review | Liam Bourke, Kate E Homer, Mohamed A Thaha, Liz Steed, Derek J Rosario, Karen A Robb, John M Saxton, Stephanie JC Taylor | |
| 2012 Nov 14 | Interventions for promoting habitual exercise in people living with and beyond cancer. | Protocol | Liam Bourke, Kate E Homer, Mohamed A Thaha, Liz Steed, Derek Rosario, Karen A Robb, John Saxton, Stephanie JC Taylor | |
Differences between protocol and review
-
We have highlighted reasons why we contacted corresponding authors and have quantified how many times we attempted to do this by email (please see Selection of studies; Excluded studies).
-
We have provided a justification for exclusion of cross‐over trials and for when during the screening process they were screened out (please see Unit of analysis issues).
-
We did not examine funnel plots because too few studies were identified (please see Assessment of risk of bias in included studies).
-
We reported only a subset of excluded trials because of the large number of manuscripts that needed to be full text screened and the large proportion of these that were excluded (please see Excluded studies).
-
We highlighted when a manuscript reported insufficient information to allow judgement of an aspect of bias (please see Other potential sources of bias).
-
We were not able to find any trials describing "pattern" of resistance exercise (i.e. the period of rest in between sets) and hence did not discount any studies for not reporting this. We judged that it would be more informative to include the studies that we found than to not report on resistance exercise interventions at all.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
- Breast Neoplasms [rehabilitation];
- *Cancer Survivors;
- Colorectal Neoplasms [rehabilitation];
- *Exercise;
- Exercise Tolerance [physiology];
- *Habits;
- Health Promotion;
- Muscle Strength;
- Neoplasms [*rehabilitation];
- Patient Compliance [statistics & numerical data];
- Prostatic Neoplasms [rehabilitation];
- Randomized Controlled Trials as Topic;
- *Sedentary Behavior;
- Time Factors;
Medical Subject Headings Check Words
Female; Humans; Male;
PICO

PRISMA flow diagram.
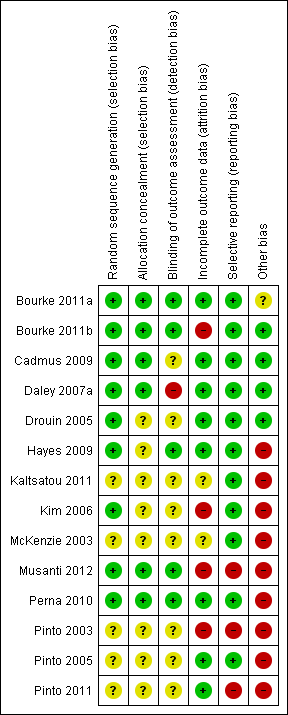
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
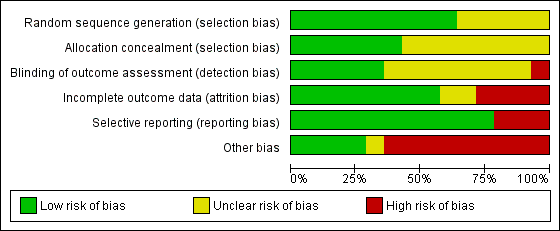
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Comparison 1 Aerobic exercise tolerance, Outcome 1 Aerobic exercise tolerance (all cancers: 8 to 12 weeks of follow‐up).

Comparison 1 Aerobic exercise tolerance, Outcome 2 Aerobic exercise tolerance (all cancers: 8 to 12 weeks of follow‐up sensitivity analysis).
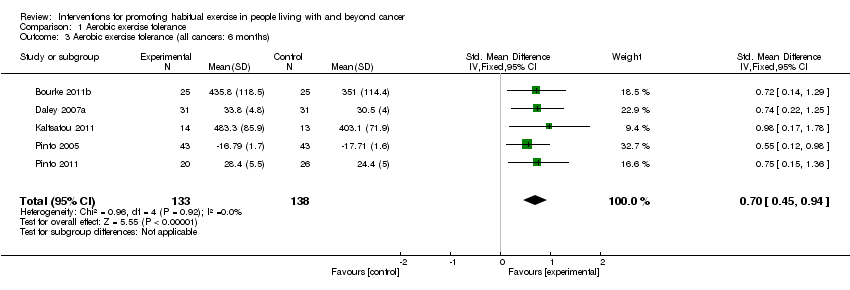
Comparison 1 Aerobic exercise tolerance, Outcome 3 Aerobic exercise tolerance (all cancers: 6 months).
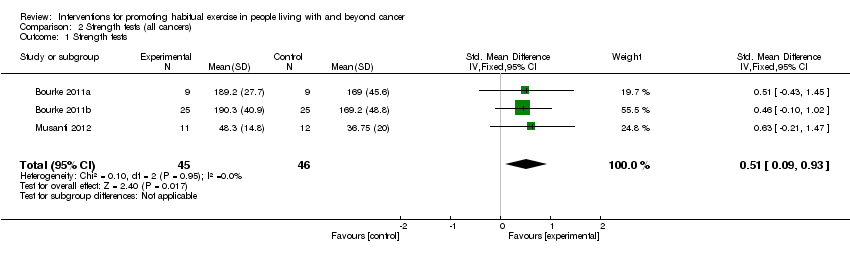
Comparison 2 Strength tests (all cancers), Outcome 1 Strength tests.

Comparison 2 Strength tests (all cancers), Outcome 2 Strength tests (all cancers: sensitivity analysis).
| Study | Exercise components | n | Meets Rock et al guidelines? | Adherence summary | At least 75% adherence? | High risk of bias? | Change in AET reported? | Adverse effects |
| Aerobic | 37, 38 (intervention vs control) | 33% reported 150 minutes/wk of moderate intensity aerobic exercise at an average of 76% HR, for six months | 75% of women were doing between 90 and 119 minutes of moderate intensity aerobic activity per week at six months | Yes; for up to 119 minutes per week | No | No | Five of the 37 women randomly assigned to exercise experienced an adverse effect; two were related to the study (plantar fasciitis) | |
| Aerobic | 34, 36, 38 (intervention, sham, control, respectively) | No | 77% of the exercise therapy; attended 70% (at least 17 of 24 sessions) or more of sessions | Unclear | Yes; outcome assessors were not blinded to participants’ group allocation | Yes | Three withdrawals in the intervention group: unclear as to why this occurred. Some withdrawals because of medical complications in placebo and control arms but unclear whether study related | |
| Aerobic | 13 intervention, 8 placebo stretching controls | Unclear | Participants in the intervention group averaged 3.6 days per week of aerobic exercise over an 8‐week period | Unclear | No | Yes | None reported | |
| Aerobic | 14, 13 (intervention vs control) | Unclear | Not reported | Not reported | Yes; method of measuring exercise and adherence not reported | No | None reported | |
| Aerobic | 22,19 (intervention vs control). | No | Average weekly frequency of exercise was 2.4 ± 0.6 sessions, and average duration of exercise within prescribed target HR was 27.8 ± 8.1 minutes per session. Overall adherence was 78.3% ± 20.1% | Yes | Yes; data missing for 45% of the cohort | Yes | Reasons for withdrawal included personal problems (n = 2), problems at home (n = 2), problems related to chemotherapy (n = 3), thrombophlebitis in the lower leg (n = 2), non-exercise‐related injuries (n = 1), and death (n = 1). Unclear to which arm of the trial these date relate | |
| Aerobic | 12, 12 (intervention vs control) | Unclear | Participants attended a mean of 88% of the 36‐session supervised exercise programme | Yes | Yes; 38% lost to follow‐up. Exercise tolerance test was performed but no control group comparison data were reported | Yes | None reported; however, it is unclear why the six controls dropped out | |
| Aerobic | 43, 43 (intervention vs control) | Unclear | At week 12, intervention participants reported a mean of 128.53 minutes/wk of moderate intensity exercise. However, no changes were reported in the accelerometer data in the intervention group (change score = ‐0.33 kcal/h) | Less than 75% of the intervention group was meeting the prescribed goal after week 4 | Yes; significantly more control group participants were receiving hormone treatment. Accelerometer data do not support the self‐reported physical activity behaviour | Yes | Not clear whether chest pain was related to exercise in dropout whose participation was terminated | |
| Aerobic | 20, 26 (intervention vs control) | Three‐day PAR questionnaire indicates that 64.7% of the intervention group and 40.9% of the control group were achieving the guidelines at three months | Correlation between self‐reported moderate intensity exercise and accelerometer data at three‐month follow‐up, when the only significant between‐group change is reported: r = 0.32 | No | Yes; accelerometer data were not reported; also, cited correlation is weak (0.32). Further, substantial contamination was noted in the control group | Yes | One cancer recurrence in the control group at three months | |
| Aerobic and resistance | 9, 9 (intervention vs control) | Six weeks of resistance exercise twice a week | 90% attendance at the supervised sessions. 94% of independent exercise sessions were completed | Yes | No | Yes | One stroke in the intervention group, unrelated to the exercise programme | |
| Aerobic and resistance | 25, 25 (intervention vs control) | Six weeks of resistance exercise twice a week | 95% attendance at supervised exercise sessions. Compliance with self‐directed exercise aspect of the lifestyle intervention was 87% | Yes | Yes; high dropout rate at postintervention six‐month follow‐up assessment | Yes | Two men in the intervention arm were discontinued because of cardiac complications before the 12‐week assessments. Two more reported musculoskeletal complaints before the six‐month assessment. Five men reported various health problems in the control group that prohibited them from attending the six‐month assessment | |
| Aerobic and resistance | 16, 16 (intervention vs control) | Unclear | Most women (88%) allocated to the intervention group participated in 70% or more of scheduled supervised exercise sessions | Unclear | Yes; adherence data on unsupervised aspect of the intervention are not clear | No | None reported | |
| Aerobic and resistance | 7,7 (intervention vs control) | No | Unclear | Unclear | Yes; adherence to exercise not reported | No | None reported | |
| Aerobic and resistance | Flexibility group (n = 13), aerobic group (n = 12), resistance group (n = 17), aerobic and resistance group (n = 13) | 12 weeks of resistance exercise two or three times per week | Mean percentages of adherence were as follows: flexibility = 85%, aerobic = 81%, resistance = 91% and aerobic plus resistance = 86% | Unclear | Yes; a significant number of dropouts belonged to the resistance exercise group (n = 8/13). Only 50% of activity logs were returned | Yes | Adverse effects were reported in two women during the study. In both cases, the women developed tendonitis: one in the shoulder and the other in the foot. Both had a history of tendonitis, and both received standard treatment | |
| Aerobic and resistance | 51 participants in total. Numbers randomly assigned to each arm are unclear | Three months of resistance exercise three times per week | Women assigned to the structured intervention completed an average of 83% of their scheduled hospital‐based exercise sessions (only 4 weeks in duration), and 76.9% completed all 12 sessions. Home‐based component (8 weeks in duration) | Unclear | Yes; numbers randomly assigned to intervention and control groups are unclear, as are numbers completing in each arm | No | Unclear | |
| AET = aerobic exercise tolerance. | ||||||||
| Behaviour change technique | YALE | |||||||||||||
| Theory | TTM | EXSEM | TTM | TTM | TTM SCT | |||||||||
| 1. Provide Info on consequences of behaviour in general | X | X | X | X | ||||||||||
| 2. Provide Info on consequences of behaviour to the individual | ||||||||||||||
| 3. Provide Info about others' approval | ||||||||||||||
| 4. Provide normative info about others' behaviour | ||||||||||||||
| Programme set goal | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| 5. Goal setting (behaviour) | X | X | X | X | X | X | ||||||||
| 6. Goal setting (outcome) | ||||||||||||||
| 7. Action planning | ||||||||||||||
| 8. Barrier identification/Problem solving | X | X | X | X | X | X | ||||||||
| 9. Setting of graded tasks | X | X | X | X | X | X | X | X | X | |||||
| 10. Prompt review of behavioural goals | X | X | ||||||||||||
| 11. Prompt review of outcome goals | ||||||||||||||
| 12. Prompt rewards contingent on effort or progress towards goal | X | X | X | |||||||||||
| 13. Provide rewards contingent on successful behaviour | X | |||||||||||||
| 14. Shaping | ||||||||||||||
| 15. Prompt generalisation of a target behaviour | X | X | X | X | X | |||||||||
| 16. Prompt self‐monitoring of behaviour | X | X | X | X | X | X | X | X | X | X | ||||
| 17. Prompt self‐monitoring of behavioural outcome | X | X | X | X | X | X | ||||||||
| 18. Prompt focus on past success | X | |||||||||||||
| 19. Feedback on performance provided | X | X | X | X | ||||||||||
| 20. Information provided on where and when to perform behaviour | X | X | ||||||||||||
| 21. Instruction provided on how to perform the behaviour | X | X | X | X | X | X | X | X | X | X | ||||
| 22. Modelling/Demonstration of behaviour | X | X | X | |||||||||||
| 23. Teaching to use prompts/cues | X | X | X | |||||||||||
| 24. Environmental restructuring | X | X | ||||||||||||
| 25. Agreement on behavioural contract | X | |||||||||||||
| 26. Prompt practise | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| 27. Use of follow‐up prompts | X | X | ||||||||||||
| 28. Facilitating social comparison | ||||||||||||||
| 29. Planning social support/social change | X | X | X | |||||||||||
| 30. Prompt identification as role model/position advocate | ||||||||||||||
| 31. Prompt anticipated regret | ||||||||||||||
| 32. Fear arousal | ||||||||||||||
| 33. Prompt self‐talk | ||||||||||||||
| 34. Prompt use of imagery | ||||||||||||||
| 35. Relapse prevention/coping planning | X | X | ||||||||||||
| 36. Stress management/emotional control training | X | |||||||||||||
| 37. Motivational interviewing | ||||||||||||||
| 38. Time management | ||||||||||||||
| 39. General communication skills training | ||||||||||||||
| 40. Stimulation of anticipation of future rewards | ||||||||||||||
| EXSEM = exercise self‐esteem model; SCT = social cognitive theory; TTM = transtheroretical model. | ||||||||||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Aerobic exercise tolerance (all cancers: 8 to 12 weeks of follow‐up) Show forest plot | 7 | 330 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.73 [0.51, 0.95] |
| 2 Aerobic exercise tolerance (all cancers: 8 to 12 weeks of follow‐up sensitivity analysis) Show forest plot | 3 | 154 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.84 [0.51, 1.17] |
| 3 Aerobic exercise tolerance (all cancers: 6 months) Show forest plot | 5 | 271 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.70 [0.45, 0.94] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Strength tests Show forest plot | 3 | 91 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.51 [0.09, 0.93] |
| 2 Strength tests (all cancers: sensitivity analysis) Show forest plot | 2 | 68 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.47 [‐0.01, 0.96] |