Maniobras para la reducción de la pronación dolorosa del codo en niños pequeños
Información
- DOI:
- https://doi.org/10.1002/14651858.CD007759.pub4Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 28 julio 2017see what's new
- Tipo:
-
- Intervention
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Lesiones óseas, articulares y musculares
- Copyright:
-
- Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
Marjolein Krul
Drafting the protocol; searching the literature; inclusion procedure; data extraction and assessing risk of bias; drafting the text of the first published version of the review.
Johannes C van der Wouden
Contact author: providing general advice on the protocol and review; methodological advice; inclusion procedure; data extraction and assessing risk of bias. Drafting the text of the 2017 update.
Emma J Kruithof
Inclusion, data extraction and risk of bias assessment for the 2017 update. Interpreted results and assisted in drafting text.
Lisette WA van Suijlekom‐Smit
Providing general advice on the protocol and review.
Bart W Koes
Providing general advice on the protocol and review.
Sources of support
Internal sources
-
Department of General Practice, Erasmus MC, Netherlands.
-
Department of General Practice and Elderly Care Medicine, Amsterdam Public Health research institute, VUmc University Medical Center Amsterdam, Netherlands.
External sources
-
No sources of support supplied
Declarations of interest
None known.
Acknowledgements
We are grateful to Meisam Abdar for his translation of Asadi 2011 and to Serafín García‐Mata for providing details of the design of their study (Garcia‐Mata 2014).
The authors would like to acknowledge valuable comments at protocol and review stages from: Karen Black, Lesley Gillespie, Helen Handoll, Brian Rowe, Cathie Sherrington, Sue Stephen, Ben Vandemeer and Janet Wale. We particularly thank Joanne Elliott for her help with the search strategy and Lindsey Elstub for her help during editorial processing. We thank Ella Curtis for providing her paper.
This project was supported by the National Institute for Health Research via Cochrane Infrastructure funding to the Cochrane Bone, Joint and Muscle Trauma Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
Version history
| Published | Title | Stage | Authors | Version |
| 2017 Jul 28 | Manipulative interventions for reducing pulled elbow in young children | Review | Marjolein Krul, Johannes C van der Wouden, Emma J Kruithof, Lisette WA van Suijlekom‐Smit, Bart W Koes | |
| 2012 Jan 18 | Manipulative interventions for reducing pulled elbow in young children | Review | Marjolein Krul, Johannes C van der Wouden, Lisette WA van Suijlekom‐Smit, Bart W Koes | |
| 2009 Oct 07 | Manipulative interventions for reducing pulled elbow in young children | Review | Marjolein Krul, Johannes C van der Wouden, Lisette WA van Suijlekom‐Smit, Bart W Koes | |
| 2009 Jul 08 | Manipulative interventions for reducing pulled elbow in young children | Protocol | Marjolein Krul, Johannes C van der Wouden, Lisette WA van Suijlekom‐Smit, Bart W Koes | |
Differences between protocol and review
We had not anticipated that attempts for reducing the pulled elbow could have been made before the child entered into the study. We found one study where this was reported to be the case in 15% of the participants, a study performed in a tertiary paediatric orthopaedic unit (Garcia‐Mata 2014). We decided to include all children in the analysis, and perform a sensitivity analysis without the inclusion of the data from the 15%.
We added continued failure after a second attempt using the same initial procedure as an additional secondary outcome.
We also used Google to search for studies (October 2016) and found one study from Iran which was included for this update (Asadi 2011).
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
- *Elbow Injuries;
- Joint Dislocations [etiology, *therapy];
- Manipulation, Orthopedic [adverse effects, *methods, statistics & numerical data];
- Pain Measurement;
- Pronation;
- Radius [*injuries];
- Randomized Controlled Trials as Topic;
- Sprains and Strains [etiology, *therapy];
- Supination;
- Treatment Failure;
Medical Subject Headings Check Words
Child, Preschool; Female; Humans; Infant; Male;
PICO
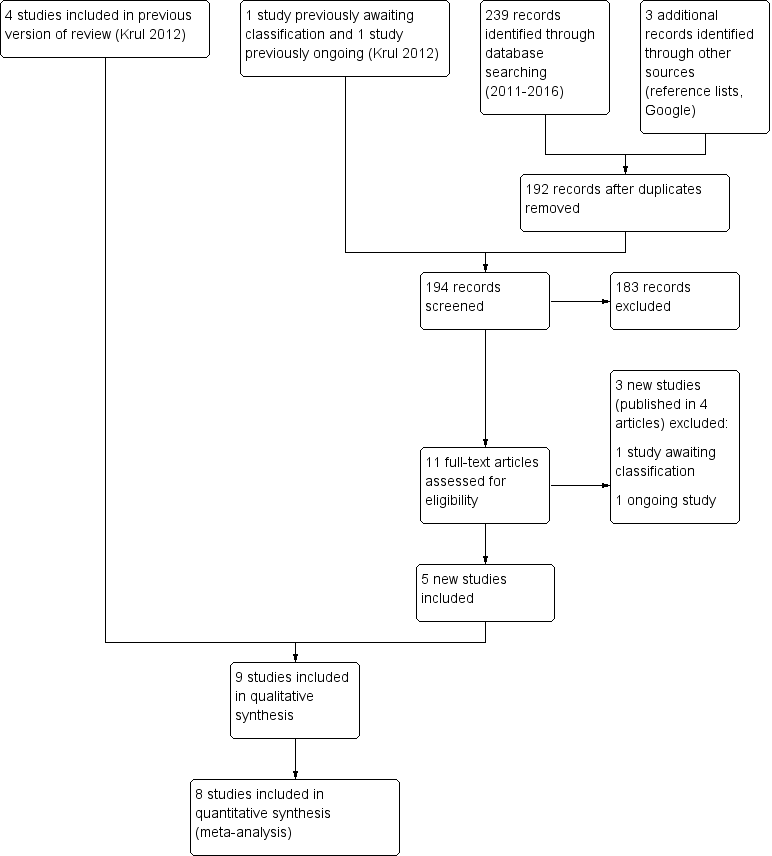
Study flow diagram
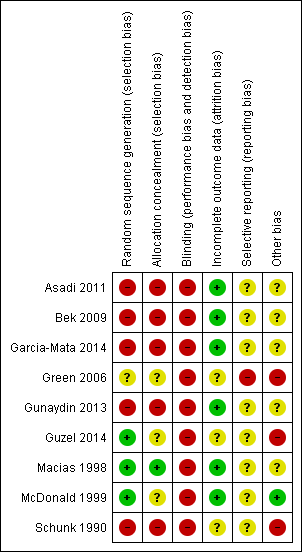
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
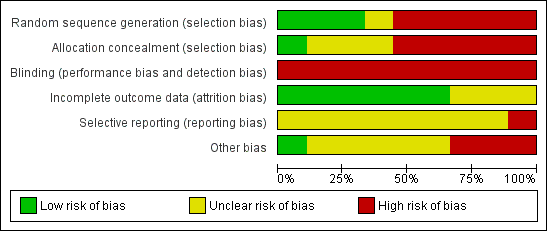
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.

Forest plot of comparison: 1 Pronation versus supination, outcome: 1.1 Failure: second attempt required.

Comparison 1 Pronation versus supination, Outcome 1 Failure: second attempt required.

Comparison 1 Pronation versus supination, Outcome 2 Failure: continued failure after second attempt with same procedure.

Comparison 2 Supination and extension versus supination then flexion, Outcome 1 Failure: second attempt required.
| Pronation compared with supination reduction techniques for pulled elbow in young children | ||||||
| Patient or population: Children with pulled elbow1 Settings: Emergency departments, ambulatory care centres or orthopaedic units Intervention: Pronation (all were hyperpronation) for first manipulation Comparison: Supination (all included flexion) for first manipulation | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Supination‐flexion | Hyperpronation | |||||
| Failure: second attempt required | 268 per 10002 | 94 per 1000 (67 to 134) | RR 0.35 (0.25 to 0.50) | 811 | ⊕⊕⊝⊝ | |
| Pain (preferably during the procedure) | see Comments | see Comments | see Comments | ⊕⊝⊝⊝ | Data for this outcome are incomplete and were measured in very different ways in four studies. | |
| Adverse effects (e.g. bruising) | see Comments | see Comments | None of the trials reported this outcome. | |||
| Failure: continued failure after second attempt using same procedure as before | 147 per 10002 | 24 per 1000 | RR 0.16 (0.09 to 0.32) | 624 | ⊕⊝⊝⊝ | This outcome represented the cumulative effect of two manipulations using hyperpronation versus cumulative effect of two manipulations using supination‐flexion. Reassuringly, both procedures when used again resulted in further successful reductions; these were proportionally greater with hyperpronation (64% versus 28%). However, the second attempt should not be considered independently of the first attempt and the characteristics of the children requiring a second attempt may have differed in important ways between the two groups. |
| Ultimate failure | see Comments | see Comments | Although potentially influenced by the initial (allocated) method of manipulation, this outcome reflected various manipulation protocols that stipulated the choice of method used for subsequent attempts. Overall failure at the end of the protocol ranged from 0 to 6 (4.1% of 148 episodes). | |||
| Recurrence (within one month) | see Comments | see Comments | None of the trials reported this outcome. | |||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1. Young children: typically aged under 7 years; mean age around 2 years. 2. Median control group (supination‐flexion) risk across studies 3. Evidence downgraded two levels for very serious risk of bias (selection and detection biases). 4. Evidence downgraded two levels for very serious risk of bias (selection, detection and incomplete outcome biases) and one level for inconsistency (two of the studies reported in favour of pronation, whereas two studies reported no difference between the procedures) 5. Evidence downgraded two levels for very serious risk of bias (and one level for imprecision (there were just 9 events in the hyperpronation group) | ||||||
| Radial head subluxation |
| Partial dislocation of the radial head peculiar to children |
| Dislocation of the head of the radius by elongation |
| Annular ligament displacement |
| Partial epiphyseal separation of the radial head |
| Anterior isolated subluxation of the radial head |
| Internal derangement of the elbow |
| Slipped elbow of young children |
| Painful elongation of young children |
| Painful paralysis in young children |
| Rotation syndrome |
| Painful pronation |
| Tamper tantrum elbow |
| Elbow sprain |
| Goyrands’s injury |
| Malaigne’s luxation |
| Gromeyer’s injury |
| Pronatio dolorosa infantum (Chassaignac) |
| Curbstone fracture |
| Supermarket elbow |
| Sunday (afternoon) arm |
| Housemaid’s elbow |
| Nursemaid’s elbow |
| Babysitter’s elbow |
| Sensitivity analysis | Results | NNT |
| Removal of quasi‐RCTs | RR 0.47, 95% CI 0.30 to 0.73; 370 participants; I2 = 13% | 8, 95% CI 5 to 17 |
| Removal of Green 2006 (baseline imbalance) | RR 0.34, 95% CI 0.24 to 0.49; 739 participants; I2 = 35% | 6, 95% CI 5 to 8 |
| Removal of 17 participants with prior manipulation in Garcia‐Mata 2014) | RR 0.35, 95% CI 0.24 to 0.50; 794 participants; I2 = 28% | 7, 95% CI 5 to 10 |
| Study | Outcome definition | Overall no. of failures / no. episodes | Protocol |
| Failure after 4 attempts | Not reported | 4 attempts, cross‐over on 3rd attempt | |
| Failure after 3 attempts | 0 / 66 (0%) | 3 attempts, cross‐over on 3rd attempt | |
| Failure after 3 attempts | 3 / 115 (2.6%) | 3 attempts, cross‐over on 2rd attempt original method for 3rd attempt | |
| Failure after 2 attempts | 2 / 75 (2.7%) | 2 attempts, cross‐over on 2nd attempt | |
| Failure after 3 attempts | 0 / 150 (0%) | 3 attempts, cross‐over on 3rd attempt | |
| Failure after 3 attempts | Not reported | 3 attempts, cross‐over on 3rd attempt | |
| Failure after 4 attempts | 1 / 90 (1.1%) | 4 attempts, cross‐over on 3rd attempt order same for 4th attempt | |
| Failure after 3 attempts | 6 / 148 (4.1%) | 3 attempts, cross‐over on 3rd attempt |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Failure: second attempt required Show forest plot | 8 | 811 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.35 [0.25, 0.50] |
| 2 Failure: continued failure after second attempt with same procedure Show forest plot | 6 | 624 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.16 [0.09, 0.32] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Failure: second attempt required Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |