Exposición quirúrgica abierta versus cerrada de dientes caninos desplazados hacia el techo de la boca
Información
- DOI:
- https://doi.org/10.1002/14651858.CD006966.pub3Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 21 agosto 2017see what's new
- Tipo:
-
- Intervention
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Salud oral
- Copyright:
-
- Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
Conceiving, designing and co‐ordinating the review (Nicola Parkin (NP)).
Developing search strategy and undertaking searches (NP, Philip Benson (PB)).
Screening search results and retrieved papers against inclusion criteria (NP, PB, Anwar Shah (AS), Bikram Thind (BT), Ismail Khalil (IK), Saiba Ghafoor (SG)).
Appraising risk of bias and quality of evidence (NP, PB).
Extracting data from papers (NP, PB, IK, SG).
Writing to authors for additional information (NP, IK, SG).
Data management for the review and entering data into RevMan 5 (NP).
Analysis and interpretation of data (NP, PB).
Writing the review (NP, PB).
Providing general advice on the review (PB).
Sources of support
Internal sources
-
No sources of support supplied
External sources
-
National Institute for Health Research (NIHR), UK.
This project was supported by the NIHR, via Cochrane Infrastructure funding to Cochrane Oral Health. The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
-
Cochrane Oral Health Global Alliance, Other.
The production of Cochrane Oral Health reviews has been supported financially by our Global Alliance since 2011 (http://oralhealth.cochrane.org/partnerships‐alliances). Contributors over the past year have been the American Association of Public Health Dentistry, USA; British Association for the Study of Community Dentistry, UK; the British Society of Paediatric Dentistry, UK; the Canadian Dental Hygienists Association, Canada; the Centre for Dental Education and Research at All India Institute of Medical Sciences, India; the National Center for Dental Hygiene Research & Practice, USA; New York University College of Dentistry, USA; NHS Education for Scotland, UK; and Swiss Society for Endodontology.
Declarations of interest
Nicola Parkin: none known. NP is an author on one of the included trials.
Philip E Benson: none known. PB is an author on one of the included trials.
Bikram Thind: none known.
Anwar Shah: none known.
Ismail Khalil: none known.
Saiba Ghafoor: none known.
Acknowledgements
We would like to thank Helen Worthington at Cochrane Oral Health in Manchester, UK, for her support and supervision of undergraduate students Ismail Khalil and Saiba Ghafoor. We also acknowledge Laura MacDonald, Anne Littlewood and Helen Wakeford from the Cochrane Oral Health editorial base; Jayne Harrison (editor with Cochrane Oral Health), Helen J Grady, Oswaldo Jesus Mejias Rotundo and Aman Ulhaq for comments on drafts of the review; and Jason Elliot‐Smith for final copy editing.
Version history
| Published | Title | Stage | Authors | Version |
| 2017 Aug 21 | Open versus closed surgical exposure of canine teeth that are displaced in the roof of the mouth | Review | Nicola Parkin, Philip E Benson, Bikram Thind, Anwar Shah, Ismail Khalil, Saiba Ghafoor | |
| 2008 Oct 08 | Open versus closed surgical exposure of canine teeth that are displaced in the roof of the mouth | Review | Nicola Parkin, Philip E Benson, Bikram Thind, Anwar Shah | |
| 2008 Jan 23 | Open versus closed surgical exposure of eye (canine) teeth that are displaced in the roof of the mouth | Protocol | Nicola Parkin, Philip E Benson, Bikram S Thind, Anwar Shah | |
Differences between protocol and review
The primary outcomes are now success of surgery, complications and aesthetics at the end of treatment. Periodontal (gum) health, duration of treatment and patient‐reported outcomes are secondary outcomes.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
Medical Subject Headings Check Words
Humans;
PICO


Closed technique

Risk of bias summary: review authors' judgements about each risk of bias item for each included study

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies

Study flow diagram of searches conducted for this update (2008 to 2017)

Comparison 1 Open surgical technique versus closed surgical technique, Outcome 1 Success of surgery.

Comparison 1 Open surgical technique versus closed surgical technique, Outcome 2 Aesthetics.
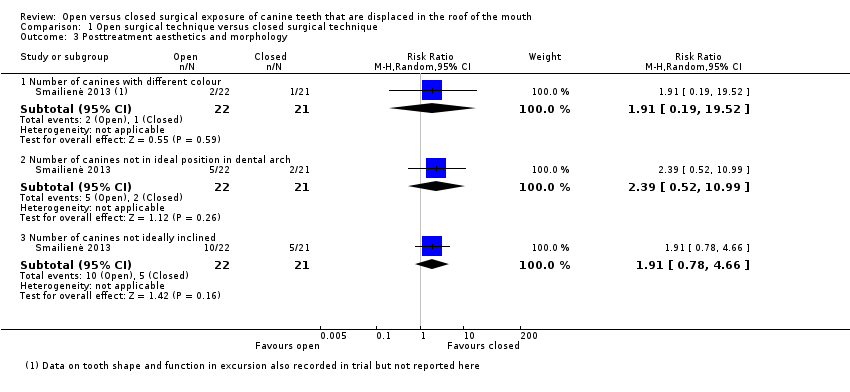
Comparison 1 Open surgical technique versus closed surgical technique, Outcome 3 Posttreatment aesthetics and morphology.
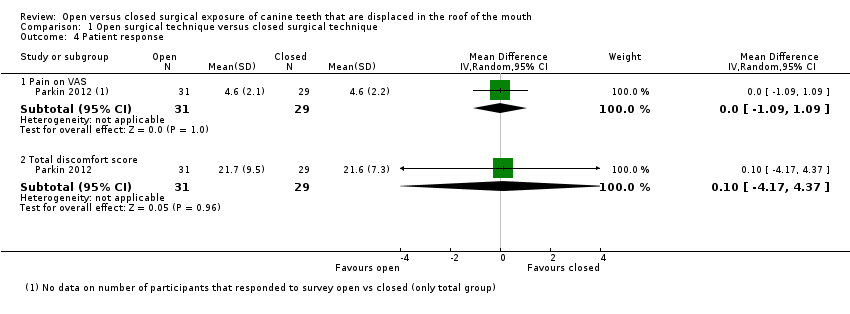
Comparison 1 Open surgical technique versus closed surgical technique, Outcome 4 Patient response.

Comparison 1 Open surgical technique versus closed surgical technique, Outcome 5 Pain (dichotomous).

Comparison 1 Open surgical technique versus closed surgical technique, Outcome 6 Gum health.

Comparison 1 Open surgical technique versus closed surgical technique, Outcome 7 Gingival recession (dichotomous).

Comparison 1 Open surgical technique versus closed surgical technique, Outcome 8 Treatment time.

Comparison 1 Open surgical technique versus closed surgical technique, Outcome 9 Patient response (satisfaction).
| Open surgical technique compared with closed surgical technique for palatally impacted canines | ||||||
| Patient or population: people with maxillary palatally impacted canines Settings: oral surgery departments Intervention: open surgical technique Comparison: closed surgical technique | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Closed surgery | Open surgery | |||||
| Success of surgery | 943 per 1000 | 934 per 1000 | RR 0.99 (0.93 to 1.06) | 141 | ⊕⊕⊝⊝ | The available evidence suggests that there is no difference in the success of surgery between the techniques and that both techniques have a high success rate. |
| Complications | One surgical failure was due to detachment of the gold chain (closed group). One study reported two complications following surgery, both in the closed group: a post‐operative infection requiring antibiotics and pain during alignment of the canine as the gold chain penetrated through the gum tissue of the palate. | |||||
| Aesthetics (reported in various manners at different time points) | This outcome was measured in a variety of ways in the studies that cannot be pooled. | ⊕⊝⊝⊝ | This outcome is subjective and can be measured and reported in many different ways. The current evidence suggests that there is no difference in aesthetic outcomes between the groups. | |||
| Patient response (pain and discomfort reported in different ways between 1 to 10 days postoperatively) | This outcome was measured in a variety of ways in the studies that cannot be pooled. | ⊕⊝⊝⊝ | This outcome is subjective and was measured and reported in different ways. The current evidence suggests that there is no difference in patient response outcomes between the groups. | |||
| Gum health (clinical attachment level (CAL); 3 months post‐debond) | Mean CAL in the closed group | Mean CAL in the intervention groups was 0.1 mm lower | 62 | ⊕⊕⊝⊝ | This outcome was measured and reported in different ways in different studies. The current evidence suggests that there is no difference in periodontal outcomes between the groups. | |
| Treatment time (length of time in operating theatre from first incision to final suture) | Mean of the closed group was 34.3 minutes in Parkin 2012; and 37.7 minutes in Gharaibeh 2008. | Mean of the open group was 3.18 minutes less (7.59 minutes less to 1.22 minutes more) | 89 (2 studies) | ⊕⊝⊝⊝ | The current evidence suggests that there is no difference in length of time in surgery between the groups. | |
| *The basis for the assumed risk is the Parkin 2012 closed group. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded one level due to high risk of bias in two studies. Downgraded one level as two studies had no failures. 2 Downgraded one level due to high risk of bias in one study. Downgraded one level as each outcome only reported by single studies. Downgraded one level as studies with few participants and large confidence intervals for some outcomes. 3 Downgraded two levels due to high risk of bias in two studies and subjective participant‐reported outcome with no blinding. Downgraded one level as each outcome only reported by single studies. 4 Downgraded two levels as single small study at high risk of bias. 5 Downgraded one level due to high risk of bias in one study. Downgraded one level as substantial heterogeneity between results. Downgraded one level as studies with few participants and large confidence intervals for some outcomes. | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Success of surgery Show forest plot | 3 | 141 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.93, 1.06] |
| 2 Aesthetics Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 Correctly identified treated tooth ‐ orthodontists | 1 | 67 | Mean Difference (IV, Random, 95% CI) | 2.70 [‐11.22, 16.62] |
| 2.2 Correctly identified treated tooth ‐ laypeople | 1 | 67 | Mean Difference (IV, Random, 95% CI) | 0.10 [‐8.42, 8.62] |
| 2.3 Unoperated canine looks best ‐ orthodontists | 1 | 67 | Mean Difference (IV, Random, 95% CI) | ‐0.30 [‐14.88, 14.28] |
| 2.4 Unoperated canine looks best ‐ lay people | 1 | 67 | Mean Difference (IV, Random, 95% CI) | ‐1.70 [‐15.69, 12.29] |
| 3 Posttreatment aesthetics and morphology Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 3.1 Number of canines with different colour | 1 | 43 | Risk Ratio (M‐H, Random, 95% CI) | 1.91 [0.19, 19.52] |
| 3.2 Number of canines not in ideal position in dental arch | 1 | 43 | Risk Ratio (M‐H, Random, 95% CI) | 2.39 [0.52, 10.99] |
| 3.3 Number of canines not ideally inclined | 1 | 43 | Risk Ratio (M‐H, Random, 95% CI) | 1.91 [0.78, 4.66] |
| 4 Patient response Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 Pain on VAS | 1 | 60 | Mean Difference (IV, Random, 95% CI) | 0.0 [‐1.09, 1.09] |
| 4.2 Total discomfort score | 1 | 60 | Mean Difference (IV, Random, 95% CI) | 0.10 [‐4.17, 4.37] |
| 5 Pain (dichotomous) Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 5.1 Pain day 1 | 1 | 32 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.61, 1.20] |
| 5.2 Pain day 7 | 1 | 32 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Gum health Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 6.1 Probing depths (mm) | 1 | 43 | Mean Difference (IV, Fixed, 95% CI) | ‐0.14 [‐0.48, 0.20] |
| 6.2 Bleeding on probing (PBI index) | 1 | 43 | Mean Difference (IV, Fixed, 95% CI) | 0.21 [‐0.14, 0.56] |
| 6.3 Clinical attachment loss (mm) | 1 | 62 | Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐0.45, 0.25] |
| 6.4 Crestal bone levels mesial (%) | 1 | 43 | Mean Difference (IV, Fixed, 95% CI) | 3.21 [‐0.33, 6.75] |
| 6.5 Crestal bone levels distal (%) | 1 | 43 | Mean Difference (IV, Fixed, 95% CI) | ‐0.18 [‐3.09, 2.73] |
| 6.6 Gingival recession ‐ midbuccal | 2 | 105 | Mean Difference (IV, Fixed, 95% CI) | ‐0.02 [‐0.21, 0.16] |
| 6.7 Gingival recession ‐ midpalatal | 1 | 43 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 7 Gingival recession (dichotomous) Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 7.1 Midpalatal recession | 1 | 62 | Risk Ratio (M‐H, Random, 95% CI) | 1.32 [0.63, 2.77] |
| 8 Treatment time Show forest plot | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 8.1 Length of time in surgery | 2 | 89 | Mean Difference (IV, Random, 95% CI) | ‐3.30 [‐9.97, 3.36] |
| 8.2 Time taken for eruption | 1 | 43 | Mean Difference (IV, Random, 95% CI) | ‐3.81 [‐5.80, ‐1.82] |
| 8.3 Length of fixed appliance phase | 1 | 43 | Mean Difference (IV, Random, 95% CI) | ‐3.77 [‐9.20, 1.66] |
| 9 Patient response (satisfaction) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |