Haloperidol versus placebo for schizophrenia
Referencias
References to studies included in this review
References to studies excluded from this review
References to studies awaiting assessment
References to ongoing studies
Additional references
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: (DSM‐III‐R) schizophrenia. | |
| Interventions | 1. Haloperidol: fixed dose (FD) 12 mg/day, increased day 1‐14. N=52 | |
| Outcomes | Leaving the study early. Unable to use ‐ | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: (DSM‐III‐R) schizophrenia. | |
| Interventions | 1. Haloperidol: dose 10, 15 or 20 mg/day; initial dose 15 mg/day, adjusted accordingly thereafter. N=69. | |
| Outcomes | Leaving the study early. Unable to use ‐ | |
| Notes | data only taken from the initial 'acute phase' trial. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: (ICD‐9) schizophrenia. | |
| Interventions | 1. Haloperidol: dose 5 ‐ 20 mg/day. N=30. | |
| Outcomes | Adverse event: various observed effects. | |
| Notes | If, after entering the trial, participants showed improvement they could be discharged from hospital. If, however, they were readmitted due to relapse they could then re‐enter the study. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: (DSM‐III) schizophrenia. | |
| Interventions | 1. Haloperidol: dose 15 ‐ 75 mg/day. N=8. | |
| Outcomes | Adverse events: various observed effects, use of antiparkinson medication. Unable to use ‐ | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: (DSM‐III‐R) schizophrenia. | |
| Interventions | 1. Haloperidol: dose 4‐10 mg/day, dose adjusted as required days 1‐18. N=12. | |
| Outcomes | Adverse events: various observed effects. Unable to use ‐ | |
| Notes | participants already part of larger multicentre trial. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: (DSM‐III‐R) schizophrenia. | |
| Interventions | 1. Haloperidol: dose 20 mg/day, initial dose 2 mg/day increased in fixed increments day 2‐7. N=21. | |
| Outcomes | Leaving the study early. Unable to use ‐ | |
| Notes | Part of Nth American Trial. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: schizophrenia (40%), neurosis (60%).* | |
| Interventions | 1. Haloperidol: dose 2‐25 mg/day, mean 6 mg/day. N=19. | |
| Outcomes | Global effect: improved/not improved. Unable to use ‐ | |
| Notes | * use only data for those suffering from schizophrenia | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: schizophrenia. | |
| Interventions | 1. Haloperidol: dose 0.75 ‐ 4.5 mg/day, increased day 1 ‐ 42. N=26. | |
| Outcomes | Adverse events: various observed effects* | |
| Notes | * Adverse effects reported for haloperidol group only, reviewers assumed that placebo group had no adverse effects. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: schizophrenia (80%). | |
| Interventions | 1. Haloperidol: dose < 200 mg/day. N=17. | |
| Outcomes | Global effect: improved/not improved. Unable to use ‐ | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: (DSM‐III‐R) schizophrenia. | |
| Interventions | 1. Haloperidol: dose up to 75 mg/day, dose individually adjusted weekly. N=18. | |
| Outcomes | Adverse events: various observed effects. Unable to use ‐ | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random. | |
| Participants | Diagnosis: (DSM‐IV) schizophrenia or schizoaffective disorder. | |
| Interventions | 1. Aripiprazole: dose 15 mg/day. N=102. | |
| Outcomes | Leaving the study early. Unable to use: | |
| Notes | data taken from haloperidol and placebo groups only. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: schizophrenia (63%), major depressive disorder (37%). | |
| Interventions | 1. Haloperidol: dose 20 mg/day. N=20*. | |
| Outcomes | Leaving the study early | |
| Notes | * number of people with schizophrenia. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: (DSM‐III‐R) schizophrenia. | |
| Interventions | 1. Haloperidol: dose 20 mg/day. N=66. | |
| Outcomes | Leaving the study early Unable to use ‐ | |
| Notes | Part of 'Nth America 1997'. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: schizophrenia | |
| Interventions | 1. Haloperidol: dose 3 mg/day. N=10. | |
| Outcomes | Relapse: number remaining in remission < 1 year. Unable to use ‐ | |
| Notes | *Initial 'cross‐over' design of trial was disregarded after participant/clinician reluctance to switch neuroleptics. Data taken from first arm only. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: (DSM III) schizophrenia. | |
| Interventions | 1. Haloperidol: dose 1 mg/day. N=13. | |
| Outcomes | Relapse: number remaining in remission < 1 year. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: psychiatric symptoms. | |
| Interventions | 1. Haloperidol: dose 1 mg/ml. N=8 | |
| Outcomes | Adverse events: various observed effects. Unable to use ‐ | |
| Notes | Data only taken from intial double blind phase. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: schizophrenia. | |
| Interventions | 1. Haloperidol: dose 4‐12 mg/day. N=29. | |
| Outcomes | Adverse effects: various observed effects. Unable to use ‐ | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: schizophrenia. | |
| Interventions | 1. Haloperidol: dose up to 15 mg/day. N=14. | |
| Outcomes | Adverse events: various observed effects. Unable to use ‐ | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: schizophrenia. | |
| Interventions | 1. Haloperidol: dose 6 mg/day. N=8. | |
| Outcomes | Adverse events: use of antiparkinson medication. Unable to use ‐ | |
| Notes | Group numbers not stated in text, reviewers have assumed that they were divided into three sets of 8 (see table 1). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: (DSM‐III‐R) schizophrenia. | |
| Interventions | 1. Haloperidol: dose 4 wks 0.5‐10 mg/day followed by 4 wks placebo. N=12. | |
| Outcomes | Global effect: improved/not improved. Unable to use ‐ | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | Allocation: random assignment. | |
| Participants | Diagnosis: schizophrenia. | |
| Interventions | 1. Haloperidol: dose 6 weeks 4.5 mg/day followed by 6 weeks placebo. N=30. | |
| Outcomes | Global effect: FFS, improved/not improved. Unable to use ‐ | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
AIMS ‐ Assessment of Involuntary Movement Scale.
BAS ‐ Barnes Akathisa Scale.
BHGRS ‐ Bunney‐Hamburg Global Rating Scale.
BPRS ‐ Brief Pyschiatric Rating Scale.
BPRS‐C ‐ Brief Psychiatric Rating Scale for Children.
CCS ‐ Clinical Change Scale.
CGI ‐ Clinical Global Impression.
CPRS ‐ Comprehensive Psychophathological Rating Scale.
CPRS ‐ Childrens Psychiatric Rating Scale.
DICA‐R ‐ Diagnostic Interview for Children & Adolescents (Revised).
DSM‐III‐R ‐ Diagnositic and statistical manual of mental disorders: 3rd edition ‐ revised.
EPS ‐ Extrapyramidal Sypmtoms.
ESRS ‐ Extrapyramidal Symptom Rating Scale.
FC ‐ Feighners Criteria.
FFS ‐ Fergus Falls Scale.
GPS ‐ General Psychopathology Subscale.
ICD‐9 ‐ 9th International Classification of Diseases.
IMPS ‐ Inpatient Multidimensional Psychiatric Scale.
KRS ‐ Krawiecka Rating Scale.
MSC ‐ Mental Status Checklist.
PGI ‐ Patient Global Impression.
PRP ‐ Psychotic Reaction Profile.
RDC ‐ Research Diagnostic Criteria.
SANS ‐ Scale for the Assessment of Negative Symptoms.
SAS ‐ Simpson Angus Scale.
UKU ‐ side effect rating scale.
WBRS ‐ Ward Behaviour Rating Scale.
WISC‐R ‐ Wechsler Intelligence Scale for Children (Revised).
WPPSI ‐ Wechsler Preschool & Primary Scale of Intelligence.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
| Allocation: unclear. | |
| Allocation: unclear. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: unclear. | |
| Allocation: unclear. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: unclear. | |
| Allocation: random, crossover study . | |
| Allocation: random. | |
| Allocation: unclear, no recording of random allocation. | |
| Allocation: not random, ABA design. | |
| Allocation: random. | |
| Allocation: not random, ABA design. | |
| Allocation: unclear. | |
| Allocation: random. | |
| Allocation: not random, ABA design. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: not random, ABA design. | |
| Allocation: random. | |
| Allocation: not random, ABA design. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: not random, ABA design. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: not random, ABA design. | |
| Allocation: unclear. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: not random, meta‐analysis. | |
| Allocation: random, crossover. | |
| Allocation: random. | |
| Allocation: not random. | |
| Allocation: random. | |
| Allocation: unclear. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: unclear . | |
| Allocation: random. | |
| Allocation: random but with non‐random additions. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: not random, ABA design. | |
| Allocation: random. | |
| Allocation: random, cross‐over. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: unclear. | |
| Allocation: not random, ABA design. | |
| Allocation: random. | |
| Allocation: unclear if randomised. | |
| Allocation: quasi‐randomised. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: random. | |
| Allocation: random. |
ABA: Before and after trial.
EPS: Extrapyramidal Symptoms.
HAM‐D: Hamilton Depression Scale.
Characteristics of studies awaiting assessment [ordered by study ID]
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | To be assessed. |
Characteristics of ongoing studies [ordered by study ID]
| Trial name or title | A double‐blind randomised comparison of the efficacacy and safety of short acting intramuscular olanzapine, short acting intramuscular haloperidol and intramuscular placebo in patients with schizophrenia |
| Methods | |
| Participants | people with schizophrenia, schizophreniform disorder or schizoaffective disorder, aged over 18 years |
| Interventions | intramuscular and oral olanzapine versus haloperidol or placebo |
| Outcomes | efficacy and safety |
| Starting date | 2000 |
| Contact information | National Research Register |
| Notes |
| Trial name or title | Prophylaxis of puerperal psychosis |
| Methods | |
| Participants | people who have already had peurperal psychosis and about to have another baby |
| Interventions | within 72hrs of delivery participants started on lithiun, haloperidol or placebo, followed by regular visits as outpatients every two weeks for two months |
| Outcomes | prevention of further attacks |
| Starting date | 2000 |
| Contact information | National Research Register |
| Notes |
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size | |||||||||||||||||||||
| 1 Global effect: 1. No marked global improvement Show forest plot | 10 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | ||||||||||||||||||||||
| Analysis 1.1  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 1 Global effect: 1. No marked global improvement. | |||||||||||||||||||||||||
| 1.1 0‐6 weeks (clinician rated). | 3 | 159 | Risk Ratio (M‐H, Random, 95% CI) | 0.44 [0.31, 0.62] | |||||||||||||||||||||
| 1.2 >6‐24 weeks (clinician rated) | 8 | 308 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.59, 0.81] | |||||||||||||||||||||
| 1.3 >6‐24 weeks (nurse rated) | 1 | 28 | Risk Ratio (M‐H, Random, 95% CI) | 0.59 [0.37, 0.92] | |||||||||||||||||||||
| 2 Global effect: 2. Not discharged from hospital (>6‐24 weeks) Show forest plot | 1 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.47, 1.52] | |||||||||||||||||||||
| Analysis 1.2  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 2 Global effect: 2. Not discharged from hospital (>6‐24 weeks). | |||||||||||||||||||||||||
| 3 Global effect: 3. Relapse or not remaining in remission (<52 weeks) Show forest plot | 2 | 70 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.57, 0.87] | |||||||||||||||||||||
| Analysis 1.3  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 3 Global effect: 3. Relapse or not remaining in remission (<52 weeks). | |||||||||||||||||||||||||
| 4 Mental state: 1. No clinical improvement (<20% reduction in BPRS score, 0‐6 weeks) Show forest plot | 1 | 24 | Risk Ratio (M‐H, Random, 95% CI) | 0.76 [0.54, 1.08] | |||||||||||||||||||||
| Analysis 1.4  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 4 Mental state: 1. No clinical improvement (<20% reduction in BPRS score, 0‐6 weeks). | |||||||||||||||||||||||||
| 5 Mental state: 2. Average end point BPRS score by 6 weeks (high = poor) Show forest plot | 2 | 72 | Mean Difference (IV, Fixed, 95% CI) | ‐11.89 [‐17.04, ‐6.74] | |||||||||||||||||||||
| Analysis 1.5  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 5 Mental state: 2. Average end point BPRS score by 6 weeks (high = poor). | |||||||||||||||||||||||||
| 6 Mental state: 3. Change in BPRS total score by 3 weeks (high = good, data likely to be skewed) Show forest plot | Other data | No numeric data | |||||||||||||||||||||||
| Analysis 1.6
Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 6 Mental state: 3. Change in BPRS total score by 3 weeks (high = good, data likely to be skewed). | |||||||||||||||||||||||||
| 7 Leaving the study early Show forest plot | 20 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | ||||||||||||||||||||||
| Analysis 1.7  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 7 Leaving the study early. | |||||||||||||||||||||||||
| 7.1 0‐6 weeks | 12 | 898 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.73, 0.95] | |||||||||||||||||||||
| 7.2 >6‐24 weeks | 8 | 304 | Risk Ratio (M‐H, Random, 95% CI) | 0.56 [0.30, 1.04] | |||||||||||||||||||||
| 7.3 < 52 weeks | 1 | 50 | Risk Ratio (M‐H, Random, 95% CI) | 2.58 [0.14, 46.83] | |||||||||||||||||||||
| 8 Adverse events: 1. Anticholinergic effects Show forest plot | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | ||||||||||||||||||||||
| Analysis 1.8  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 8 Adverse events: 1. Anticholinergic effects. | |||||||||||||||||||||||||
| 8.1 blurred vision | 2 | 240 | Risk Ratio (M‐H, Random, 95% CI) | 3.42 [0.91, 12.91] | |||||||||||||||||||||
| 8.3 dry mouth | 2 | 73 | Risk Ratio (M‐H, Random, 95% CI) | 1.81 [0.71, 4.59] | |||||||||||||||||||||
| 9 Adverse events: 2. Cardiovascular effects Show forest plot | 5 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | ||||||||||||||||||||||
| Analysis 1.9  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 9 Adverse events: 2. Cardiovascular effects. | |||||||||||||||||||||||||
| 9.1 blood pressure ‐ dizziness / low BP | 4 | 285 | Risk Ratio (M‐H, Random, 95% CI) | 1.13 [0.43, 2.95] | |||||||||||||||||||||
| 9.2 blood pressure ‐ high BP | 1 | 16 | Risk Ratio (M‐H, Random, 95% CI) | 3.0 [0.14, 64.26] | |||||||||||||||||||||
| 10 Adverse events: 3a. Movement disorders ‐ acute Show forest plot | 5 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | ||||||||||||||||||||||
| Analysis 1.10  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 10 Adverse events: 3a. Movement disorders ‐ acute. | |||||||||||||||||||||||||
| 10.1 dystonia | 3 | 109 | Risk Ratio (M‐H, Random, 95% CI) | 8.52 [1.66, 43.85] | |||||||||||||||||||||
| 10.2 oculogyric crises | 2 | 83 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.10, 8.89] | |||||||||||||||||||||
| 11 Adverse events: 3b. Movement disorders ‐ non‐acute Show forest plot | 10 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | ||||||||||||||||||||||
| Analysis 1.11  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 11 Adverse events: 3b. Movement disorders ‐ non‐acute. | |||||||||||||||||||||||||
| 11.1 akathisia | 4 | 333 | Risk Ratio (M‐H, Random, 95% CI) | 2.57 [1.39, 4.75] | |||||||||||||||||||||
| 11.2 needing antiparkinson medication | 3 | 246 | Risk Ratio (M‐H, Random, 95% CI) | 2.69 [1.53, 4.72] | |||||||||||||||||||||
| 11.3 parkinsonism (including EPS) | 4 | 163 | Risk Ratio (M‐H, Random, 95% CI) | 11.65 [2.88, 47.11] | |||||||||||||||||||||
| 11.4 rigidity | 3 | 99 | Risk Ratio (M‐H, Random, 95% CI) | 4.30 [0.94, 19.74] | |||||||||||||||||||||
| 11.5 tremor | 4 | 323 | Risk Ratio (M‐H, Random, 95% CI) | 2.49 [0.59, 10.49] | |||||||||||||||||||||
| 12 Adverse events: 3c. Movement disorders ‐ chronic Show forest plot | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | ||||||||||||||||||||||
| Analysis 1.12  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 12 Adverse events: 3c. Movement disorders ‐ chronic. | |||||||||||||||||||||||||
| 12.1 dyskinesia and tardive dyskinesia | 1 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 2.83 [0.12, 64.89] | |||||||||||||||||||||
| 12.2 teeth grinding | 1 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 2.53 [0.11, 57.83] | |||||||||||||||||||||
| 12.3 'thick' speech | 1 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 5.89 [0.33, 105.81] | |||||||||||||||||||||
| 13 Adverse events: 4. Sleep related effects Show forest plot | 7 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | ||||||||||||||||||||||
| Analysis 1.13  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 13 Adverse events: 4. Sleep related effects. | |||||||||||||||||||||||||
| 13.1 insomnia | 3 | 307 | Risk Ratio (M‐H, Random, 95% CI) | 1.68 [0.79, 3.55] | |||||||||||||||||||||
| 13.2 sleepiness | 6 | 364 | Risk Ratio (M‐H, Random, 95% CI) | 3.43 [1.53, 7.73] | |||||||||||||||||||||
| 14 Adverse events: 5. Other adverse effects Show forest plot | 7 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | ||||||||||||||||||||||
| Analysis 1.14  Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 14 Adverse events: 5. Other adverse effects. | |||||||||||||||||||||||||
| 14.1 confusion | 1 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 2.53 [0.11, 57.83] | |||||||||||||||||||||
| 14.2 drooling | 2 | 83 | Risk Ratio (M‐H, Random, 95% CI) | 2.75 [0.30, 25.38] | |||||||||||||||||||||
| 14.3 facial edema | 1 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 2.83 [0.12, 64.89] | |||||||||||||||||||||
| 14.4 headache | 2 | 231 | Risk Ratio (M‐H, Random, 95% CI) | 1.06 [0.66, 1.70] | |||||||||||||||||||||
| 14.5 infection | 1 | 24 | Risk Ratio (M‐H, Random, 95% CI) | 7.0 [0.40, 122.44] | |||||||||||||||||||||
| 14.6 nausea / vomiting | 2 | 231 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.50, 1.66] | |||||||||||||||||||||
| 14.7 perspiration | 2 | 93 | Risk Ratio (M‐H, Random, 95% CI) | 4.73 [0.58, 38.89] | |||||||||||||||||||||
| 14.8 weight loss | 1 | 27 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.36, 1.75] | |||||||||||||||||||||
| 14.9 weight gain | 1 | 207 | Risk Ratio (M‐H, Random, 95% CI) | 10.10 [1.32, 77.46] | |||||||||||||||||||||

Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 1 Global effect: 1. No marked global improvement.

Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 2 Global effect: 2. Not discharged from hospital (>6‐24 weeks).
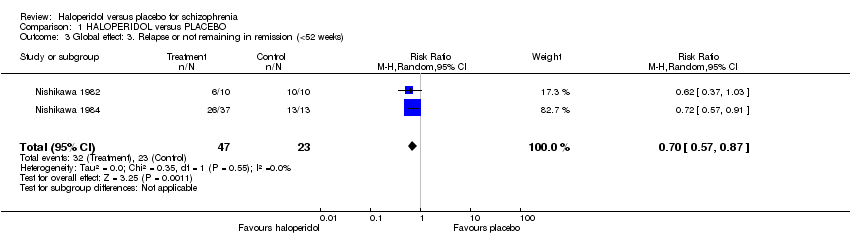
Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 3 Global effect: 3. Relapse or not remaining in remission (<52 weeks).

Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 4 Mental state: 1. No clinical improvement (<20% reduction in BPRS score, 0‐6 weeks).

Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 5 Mental state: 2. Average end point BPRS score by 6 weeks (high = poor).
| Study | Haloperidol ‐ number | Haloperidol ‐ mean | Haloperidol ‐ SD | Placebo ‐ number | Placebo ‐ mean | Placebo ‐ SD |
| Klieser 1989 | 20 | 2.0 | 22.6 | 16 | ‐4.1 | 20.4 |
Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 6 Mental state: 3. Change in BPRS total score by 3 weeks (high = good, data likely to be skewed).

Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 7 Leaving the study early.

Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 8 Adverse events: 1. Anticholinergic effects.
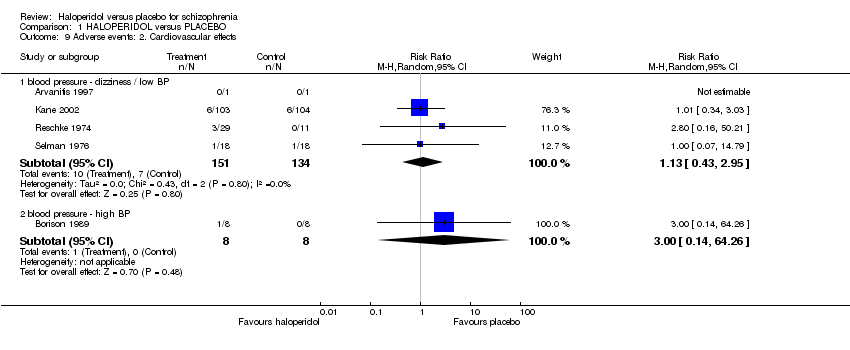
Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 9 Adverse events: 2. Cardiovascular effects.

Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 10 Adverse events: 3a. Movement disorders ‐ acute.
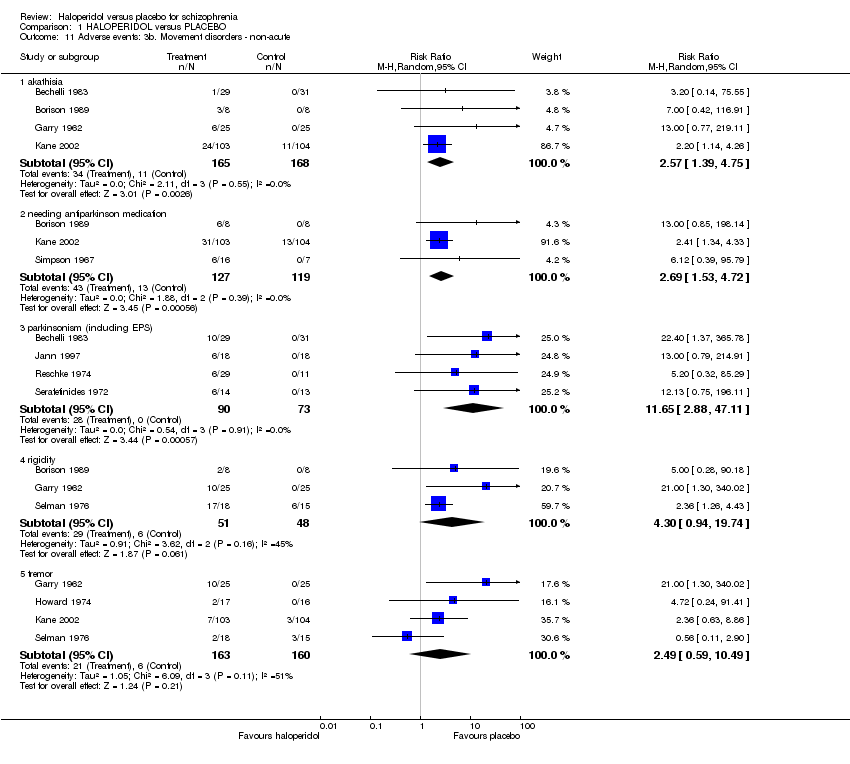
Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 11 Adverse events: 3b. Movement disorders ‐ non‐acute.

Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 12 Adverse events: 3c. Movement disorders ‐ chronic.
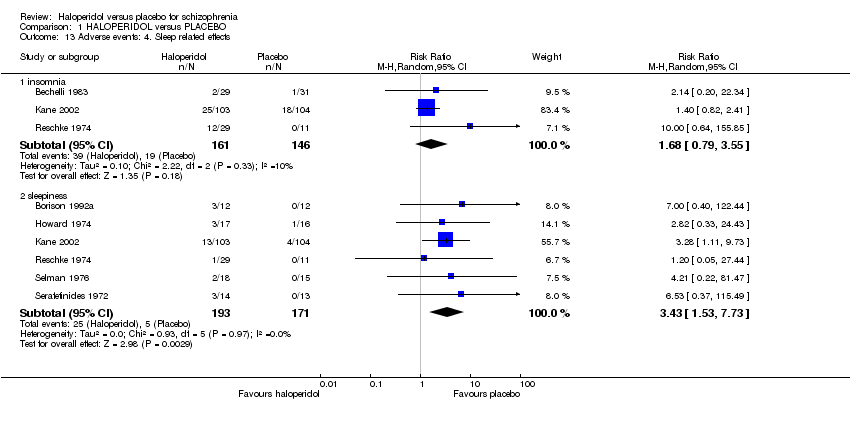
Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 13 Adverse events: 4. Sleep related effects.
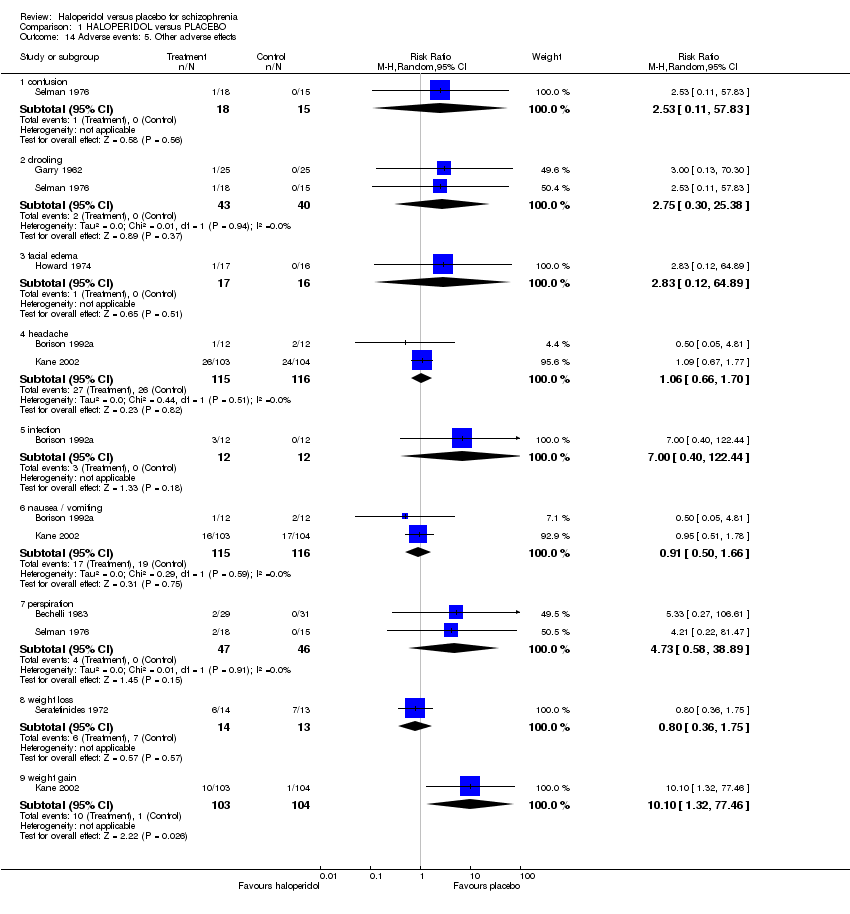
Comparison 1 HALOPERIDOL versus PLACEBO, Outcome 14 Adverse events: 5. Other adverse effects.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Global effect: 1. No marked global improvement Show forest plot | 10 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1 0‐6 weeks (clinician rated). | 3 | 159 | Risk Ratio (M‐H, Random, 95% CI) | 0.44 [0.31, 0.62] |
| 1.2 >6‐24 weeks (clinician rated) | 8 | 308 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.59, 0.81] |
| 1.3 >6‐24 weeks (nurse rated) | 1 | 28 | Risk Ratio (M‐H, Random, 95% CI) | 0.59 [0.37, 0.92] |
| 2 Global effect: 2. Not discharged from hospital (>6‐24 weeks) Show forest plot | 1 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.47, 1.52] |
| 3 Global effect: 3. Relapse or not remaining in remission (<52 weeks) Show forest plot | 2 | 70 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.57, 0.87] |
| 4 Mental state: 1. No clinical improvement (<20% reduction in BPRS score, 0‐6 weeks) Show forest plot | 1 | 24 | Risk Ratio (M‐H, Random, 95% CI) | 0.76 [0.54, 1.08] |
| 5 Mental state: 2. Average end point BPRS score by 6 weeks (high = poor) Show forest plot | 2 | 72 | Mean Difference (IV, Fixed, 95% CI) | ‐11.89 [‐17.04, ‐6.74] |
| 6 Mental state: 3. Change in BPRS total score by 3 weeks (high = good, data likely to be skewed) Show forest plot | Other data | No numeric data | ||
| 7 Leaving the study early Show forest plot | 20 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 7.1 0‐6 weeks | 12 | 898 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.73, 0.95] |
| 7.2 >6‐24 weeks | 8 | 304 | Risk Ratio (M‐H, Random, 95% CI) | 0.56 [0.30, 1.04] |
| 7.3 < 52 weeks | 1 | 50 | Risk Ratio (M‐H, Random, 95% CI) | 2.58 [0.14, 46.83] |
| 8 Adverse events: 1. Anticholinergic effects Show forest plot | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 8.1 blurred vision | 2 | 240 | Risk Ratio (M‐H, Random, 95% CI) | 3.42 [0.91, 12.91] |
| 8.3 dry mouth | 2 | 73 | Risk Ratio (M‐H, Random, 95% CI) | 1.81 [0.71, 4.59] |
| 9 Adverse events: 2. Cardiovascular effects Show forest plot | 5 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 9.1 blood pressure ‐ dizziness / low BP | 4 | 285 | Risk Ratio (M‐H, Random, 95% CI) | 1.13 [0.43, 2.95] |
| 9.2 blood pressure ‐ high BP | 1 | 16 | Risk Ratio (M‐H, Random, 95% CI) | 3.0 [0.14, 64.26] |
| 10 Adverse events: 3a. Movement disorders ‐ acute Show forest plot | 5 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 10.1 dystonia | 3 | 109 | Risk Ratio (M‐H, Random, 95% CI) | 8.52 [1.66, 43.85] |
| 10.2 oculogyric crises | 2 | 83 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.10, 8.89] |
| 11 Adverse events: 3b. Movement disorders ‐ non‐acute Show forest plot | 10 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 11.1 akathisia | 4 | 333 | Risk Ratio (M‐H, Random, 95% CI) | 2.57 [1.39, 4.75] |
| 11.2 needing antiparkinson medication | 3 | 246 | Risk Ratio (M‐H, Random, 95% CI) | 2.69 [1.53, 4.72] |
| 11.3 parkinsonism (including EPS) | 4 | 163 | Risk Ratio (M‐H, Random, 95% CI) | 11.65 [2.88, 47.11] |
| 11.4 rigidity | 3 | 99 | Risk Ratio (M‐H, Random, 95% CI) | 4.30 [0.94, 19.74] |
| 11.5 tremor | 4 | 323 | Risk Ratio (M‐H, Random, 95% CI) | 2.49 [0.59, 10.49] |
| 12 Adverse events: 3c. Movement disorders ‐ chronic Show forest plot | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 12.1 dyskinesia and tardive dyskinesia | 1 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 2.83 [0.12, 64.89] |
| 12.2 teeth grinding | 1 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 2.53 [0.11, 57.83] |
| 12.3 'thick' speech | 1 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 5.89 [0.33, 105.81] |
| 13 Adverse events: 4. Sleep related effects Show forest plot | 7 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 13.1 insomnia | 3 | 307 | Risk Ratio (M‐H, Random, 95% CI) | 1.68 [0.79, 3.55] |
| 13.2 sleepiness | 6 | 364 | Risk Ratio (M‐H, Random, 95% CI) | 3.43 [1.53, 7.73] |
| 14 Adverse events: 5. Other adverse effects Show forest plot | 7 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 14.1 confusion | 1 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 2.53 [0.11, 57.83] |
| 14.2 drooling | 2 | 83 | Risk Ratio (M‐H, Random, 95% CI) | 2.75 [0.30, 25.38] |
| 14.3 facial edema | 1 | 33 | Risk Ratio (M‐H, Random, 95% CI) | 2.83 [0.12, 64.89] |
| 14.4 headache | 2 | 231 | Risk Ratio (M‐H, Random, 95% CI) | 1.06 [0.66, 1.70] |
| 14.5 infection | 1 | 24 | Risk Ratio (M‐H, Random, 95% CI) | 7.0 [0.40, 122.44] |
| 14.6 nausea / vomiting | 2 | 231 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.50, 1.66] |
| 14.7 perspiration | 2 | 93 | Risk Ratio (M‐H, Random, 95% CI) | 4.73 [0.58, 38.89] |
| 14.8 weight loss | 1 | 27 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.36, 1.75] |
| 14.9 weight gain | 1 | 207 | Risk Ratio (M‐H, Random, 95% CI) | 10.10 [1.32, 77.46] |