Bisfosfonati za osteoporozu kod osoba s cističnom fibrozom
Abstract
Background
Osteoporosis is a disorder of bone mineralisation occurring in about one third of adults with cystic fibrosis. Bisphosphonates can increase bone mineral density and decrease the risk of new fractures in post‐menopausal women and people receiving long‐term oral corticosteroids. This is an updated version of a previous review.
Objectives
To assess the effects of bisphosphonates on the frequency of fractures, bone mineral density, quality of life, adverse events, trial withdrawals, and survival in people with cystic fibrosis.
Search methods
We searched the Cystic Fibrosis and Genetic Disorders Group's Trials Register of references (identified from electronic database searches and hand searches of journals and abstract books) on 5 May 2022.
We performed additional searches of PubMed, clinicaltrials.gov and the WHO ICTRP (International Clinical Trials Registry Platform) on 5 May 2022.
Selection criteria
Randomised controlled trials of at least six months duration studying bisphosphonates in people with cystic fibrosis.
Data collection and analysis
Authors independently selected trials, extracted data and assessed risk of bias in included studies. Trial investigators were contacted to obtain missing data. We judged the certainty of the evidence using GRADE.
Main results
We included nine trials with a total of 385 participants (272 adults and 113 children (aged five to 18 years)). Trial durations ranged from six months to two years. Only two of the studies were considered to have a low risk of bias for all the domains.
Bisphosphonates compared to control in people with cystic fibrosis who have not had a lung transplant
Seven trials included only adult participants without lung transplants, one trial included both adults and children without lung transplantation (total of 238 adults and 113 children). We analysed adults (n = 238) and children (n = 113) separately.
Adults
Three trials assessed intravenous bisphosphonates (one assessed pamidronate and two assessed zoledronate) and five trials assessed oral bisphosphonates (one assessed risedronate and four assessed alendronate). Bisphosphonates were compared to either placebo or calcium (with or without additional vitamin D). Data showed no difference between treatment or control groups in new vertebral fractures at 12 months (odds ratio (OR) 0.22, 95% confidence interval (CI) 0.02 to 2.09; 5 trials, 142 participants; very low‐certainty evidence) and two trials (44 participants) reported no vertebral fractures at 24 months. There was no difference in non‐vertebral fractures at 12 months (OR 2.11, 95% CI 0.18 to 25.35; 4 trials, 95 participants; very low‐certainty evidence) and again two trials (44 participants) reported no non‐vertebral fractures at 24 months. There was no difference in total fractures between groups at 12 months (OR 0.57, 95% CI 0.13 to 2.50; 5 trials, 142 participants) and no fractures were reported in two trials (44 participants) at 24 months. At 12 months, bisphosphonates may increase bone mineral density at the lumbar spine (mean difference (MD) 6.31, 95% CI 5.39 to 7.22; 6 trials, 171 participants; low‐certainty evidence) and at the hip or femur (MD 4.41, 95% 3.44 to 5.37; 5 trials, 155 participants; low‐certainty evidence). There was no clear difference in quality of life scores at 12 months (1 trial, 47 participants; low‐certainty evidence), but bisphosphonates probably led to more adverse events (bone pain) at 12 months (OR 8.49, 95% CI 3.20 to 22.56; 7 trials, 206 participants; moderate‐certainty evidence).
Children
The single trial in 113 children compared oral alendronate to placebo. We graded all evidence as low certainty. At 12 months we found no difference between treatment and placebo in new vertebral fractures (OR 0.32, 95% CI 0.03 to 3.13; 1 trial, 113 participants) and non‐vertebral fractures (OR 0.19, 95% CI 0.01 to 4.04; 1 trial, 113 participants). There was also no difference in total fractures (OR 0.18, 95% CI 0.02 to 1.61; 1 trial, 113 participants). Bisphosphonates may increase bone mineral density at the lumbar spine at 12 months (MD 14.50, 95% CI 12.91 to 16.09). There was no difference in bone or muscle pain (MD 3.00, 95% CI 0.12 to 75.22), fever (MD 3.00, 95% CI 0.12 to 75.22) or gastrointestinal adverse events (OR 0.67, 95% CI 0.20 to 2.26). The trial did not measure bone mineral density at the hip/femur or report on quality of life.
Bisphosphonates compared to control in people with cystic fibrosis who have had a lung transplant
One trial of 34 adults who had undergone lung transplantation compared intravenous pamidronate to no bisphosphonate treatment. It did not report at 12 months and we report the 24‐month data (not assessed by GRADE). There was no difference in the number of fractures, either vertebral or non‐vertebral. However, bone mineral density increased with treatment at the lumbar spine (MD 6.20, 95% CI 4.28 to 8.12) and femur (MD 7.90, 95% CI 5.78 to 10.02). No participants in either group reported either bone pain or fever. The trial did not measure quality of life.
Authors' conclusions
Oral and intravenous bisphosphonates may increase bone mineral density in people with cystic fibrosis, but there are insufficient data to determine whether treatment reduces fractures. Severe bone pain and flu‐like symptoms may occur with intravenous bisphosphonates.
Before any firm conclusions can be drawn, trials in larger populations, including children, and of longer duration are needed to determine effects on fracture rate and survival. Additional trials are needed to determine if bone pain is more common or severe (or both) with the more potent zoledronate and if corticosteroids can ameliorate or prevent these adverse events. Future trials should also assess gastrointestinal adverse effects associated with oral bisphosphonates.
PICO
Laički sažetak
Bisfosfonati za osteoporozu kod osoba s cističnom fibrozom
Istraživačko pitanje
Kakvi su učinci bisfosfonata (lijekova koji sprječavaju gubitak koštane mase), bilo danih oralnim putem (na usta) ili intravenski (izravno u venu), na osteoporozu kod osoba s cističnom fibrozom (CF)?
Dosadašnje spoznaje
Cistična fibroza je teški genetski poremećaj koji pogađa mnoge organe (npr. pluća i gušteraču). Oko 23,5% oboljelih ima smanjenu gustoću kostiju, poznatiju kao osteoporoza, koja povećava vjerojatnost prijeloma. Kratkoročni i dugoročni učinci prijeloma (npr . rebara i kralježnice) mogu pogoršati bolest pluća i dovesti do češće hospitalizacije. Bisfosfonati su lijekovi koji povećavaju mineralnu gustoću kostiju tako što usporavaju resorpciju kosti. Koriste se za liječenje osteoporoze uzrokovane menopauzom ili kortikosteroidnim lijekovima. Zanimalo nas je utječu li bisfosfonati na učestalost prijeloma kostiju, gustoću kostiju i kvalitetu života te izazivaju li ikakve nuspojave kod osoba s cističnom fibrozom. Ovo je obnovljeni Cochraneov sustavni pregled.
Datum pretraživanja dokaza
U ovaj sustavni pregled uključeni su dokazi objavljeni do 5. svibnja 2022. godine.
Značajke istraživanja
U ovaj je sustavni pregled uključeno devet ispitivanja s 272 odrasle osobe i 113 djece (u dobi od 5 do 18 godina) u trajanju od šest mjeseci do dvije godine. Osam ispitivanja uključivalo je 238 odraslih osoba bez presađenih pluća; u tri od njih osam korišteni su intravenski bisfosfonati (u jednom je korišten pamidronat, a u ostala dva zoledronat), a u pet ispitivanja korišteni su oralni bisfosfonati (u jednom risedronat, a u ostala četiri alendronat). Ispitivanja su uspoređivala bisfosfonate ili s placebom (lijek bez aktivne tvari) ili s kalcijem (sa ili bez dodatnog vitamina D). Jedno od ovih osam ispitivanja, koje je uspoređivalo oralni alendronat s placebom, također je uključivalo 113 djece i njihove smo rezultate zasebno analizirali. Posljednje ispitivanje na 34 odrasle osobe koje su bile podvrgnute transplantaciji pluća uspoređivalo je intravenski pamidronat s liječenjem bez bisfosfonata.
Ključni rezultati
Bisfosfonati su dosljedno povećavali gustoću kostiju u lumbalnom dijelu kralježnice i kukova. Također su povećali gustoću kostiju kod djece u lumbalnoj kralježnici. Čini se da liječenje bisfosfonatima nije smanjilo stopu prijeloma (bilo na kralježnici ili negdje drugdje) ili smrti u odraslih ili djece. Međutim, to može biti povezano s malim brojem sudionika i kratkim trajanjem ispitivanja. Jaka bol u kostima i simptomi slični gripi su često bili povezani s intravenskim bisfosfonatima, posebice u pacijenata koji nisu bili na terapiji kortikosteroidima. Potrebno je više istraživanja da se procijeni učinak premedikacije kortikosteroidima. Potrebno je više istraživanja i da se procijeni je li bol u kostima češća ili jača (ili oboje) s jačim lijekom, zoledronatom, te mogu li kortikosteroidi smanjiti ili spriječiti ove nuspojave. Dodatna istraživanja također bi trebala procijeniti gastrointestinalne nuspojave u želucu i probavnom sustavu koji su povezani s oralnim bisfosfonatima. Potrebna su istraživanja s većim brojem sudionika i s dužim praćenjem kako bi se pokazalo kako bisfosfonati utječu na stopu prijeloma i preživljenje. Trebalo bi provesti više istraživanja koja uključuju djecu s cističnom fibrozom kako bi se bolje razumjeli učinci, dobrobiti i štete koje ti lijekovi mogu imati na njih.
Bisfosfonati u usporedbi s kontrolom kod osoba s CF‐om koje nisu imale transplantaciju pluća
Odrasle osobe
Pet ispitivanja (142 sudionika) prijavilo je da nema razlike između liječenih ili kontrolnih skupina u novim kralježničnim ili prijelomima van kralježnice nakon 12 mjeseci, a dva ispitivanja (44 sudionika) su prijavila kako nije bilo prijeloma nakon 24 mjeseca. Nakon 12 mjeseci, rezultati iz šest ispitivanja (171 sudionik) pokazala su da bisfosfonati mogu povećati gustoću kostiju u lumbalnoj kralježnici, a pet ispitivanja (155 sudionika) prijavilo je isti učinak na gustoću kostiju kukova ili femura. Nije bilo jasne razlike u rezultatima kvalitete života (QoL) nakon 12 mjeseci, ali bisfosfonati su vjerojatno doveli do više bolova u kostima nakon 12 mjeseci, kako je objavljeno u sedam ispitivanja (206 sudionika).
Djeca
Nakon 12 mjeseci nije bilo razlike između liječenja i placeba u novim kralježničnim ili prijelomima van kralježnice. Bisfosfonati mogu povećati gustoću kostiju u lumbalnoj kralježnici nakon 12 mjeseci. Nije bilo razlike u bolovima u kostima ili mišićima, u pojavi vrućice ili gastrointestinalnim nuspojavama. Ispitivanje nije mjerilo mineralnu gustoću kosti kukova/femura niti kvalitetu života.
Bisfosfonati u usporedbi s kontrolom kod osoba s CF‐om koje su imale transplantaciju pluća
Ovo ispitivanje opisalo je rezultate nakon 24 mjeseca. Nije bilo razlike u broju prijeloma, bilo u kralježnici ili u drugim kostima, ali mineralna gustoća kostiju lumbalne kralježnice i femura se povećala s liječenjem. Nije bilo prijavljenih bolova u kostima niti povišene temperature. Ispitivanje nije mjerilo kvalitetu života.
Pouzdanost dokaza
Pouzdanost dokaza se razlikovala, a posebice su zabrinjavajući bili rizici od pristranosti u svim ispitivanjima. Najmanje tri ispitivanja djelomično su financirale farmaceutske tvrtke. U jednom je ispitivanju osoblje koje je analiziralo snimke kostiju moglo znati koji su sudionici bili liječeni bisfosfonatima; to je moglo utjecati na njihovu objektivnost. Dva ispitivanja nisu izvijestila o prijelomima, ali mislimo da oni vjerojatno ne bi značajno promijenili rezultate ovog sustavnog pregleda.
Authors' conclusions
Summary of findings
| Patient or population: adults with cystic fibrosis who have not had a lung transplant Settings: outpatients Comparison: placebo or no bisphosphonatesb | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Bisphosphonates | |||||
| New vertebral fractures
Follow‐up: 12 months | 42 per 1000 | 9 per 1000 (1 to 88) | OR 0.22 (0.02 to 2.09) | 142 (5) | ⊕⊝⊝⊝ very lowc,d |
|
| New non‐vertebral fractures
Follow‐up: 12 months | 21 per 1000 | 44 per 1000 (4 to 532) | OR 2.11 (0.18 to 25.35) | 95 (4) | ⊕⊝⊝⊝ very lowd,e |
|
| BMD: % change in BMD at the lumbar spine
Follow‐up: 12 months | The mean % change in BMD (lumbar spine) ranged across control groups from ‐1.8% to 0.7% | The mean % change in BMD in the intervention groups was 6.31% higher (5.39% higher to 7.22% higher) | NA | 171 (6) | ⊕⊕⊝⊝ lowf |
|
| BMD: % change in BMD at the hip or femur
Follow‐up: 12 months | The mean % change in BMD (hip or femur) ranged across control groups from ‐2.8% to ‐0.7% | The mean % change in BMD in the intervention groups was 4.41% higher (3.44% higher to 5.37% higher) | NA | 155 (5) | ⊕⊕⊝⊝ lowf |
|
| QoL: change in physical and mental component scores (SF36v2)
Follow‐up: 12 months | The change in mean (SD) SF36 physical score was ‐3.69 (8.33) in the control group | The mean change in SF36 physical score in the intervention group was 2.51 higher (1.38 lower to 6.40 higher) than in the control group | NA | 47 (1) | ⊕⊕⊝⊝ lowd,g | The results for the physical and mental components are heterogeneous
|
| The change in mean (SD) SF36 mental score was 3.26 (12.27) in the control group | The mean change in SF36 mental score in the intervention group was 5.93 lower (11.73 lower to 0.13 higher) than in the control group | |||||
| Adverse events: bone pain (all routes of bisphosphonate administration)
Follow‐up: 12 months | 38 per 1000 | 323 per 1000 (122 to 857) | OR 8.49 (3.20 to 22.56) | 206 (7) | ⊕⊕⊕⊝ moderateh | Bone pain Separating by route of administration did not change the results; both routes favoured control. Oral bisphosphonates: MD 4.98 (1.24 to 20.09) and IV bisphosphonates: MD 14.17 (3.64 to 55.17)
Fever Oral route: 2 trials of oral alendronate reported that none of the participants in either group experienced fever IV route: 3 trials showed that bisphosphonates were associated with a higher occurrence of fever OR 12.64 (2.31 to 69.11)
GI adverse effects Only measured in the oral bisphosphonates trials. At 12 months, 1 trial reported 3 occurrences of diarrhoea (1 in the bisphosphonate group and 2 in the placebo group) (Aris 2004) 1 trial reported no GI adverse effects in either group (Bianchi 2013) 1 trial reported 10 GI adverse events in the bisphosphonates group compared to 7 in the control group (Papaioannou 2008) |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). BMD: bone mineral density; CI: confidence interval; GI: gastrointestinal; IV: intravenous; MD: mean difference; NA: not applicable; OR: odds ratio; QoL: quality of life; SD: standard deviation; SF36v2: medical outcomes study 36‐item short form. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
| aTrials used different types and formulations of bisphosphonates: IV zoledronate (Boyle 2005; Chapman 2009); IV pamidronate (Haworth 2001); oral alendronate (Aris 2004; Bianchi 2013; Krasovsky 2010; Papaioannou 2008); oral risedronate (Haworth 2011). | ||||||
| Patient or population: children with cystic fibrosis who have not had a lung transplant Settings: outpatients Intervention: oral alendronate plus oral calcifediol and RDA dietary calcium Comparison: oral placebo plus oral calcifediol and RDA dietary calcium | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Bisphosphonates | |||||
| New vertebral fractures
Follow‐up: 12 months | 54 per 1000 | 17 per 1000 (2 to 169) | OR 0.32 (0.03 to 3.13) | 113 (1) | ⊕⊕⊝⊝ lowa |
|
| New non‐vertebral fractures
Follow‐up: 12 months | 36 per 1000 | 7 per 1000 (1 to 145) | OR 0.19 (0.01 to 4.04) | 113 (1) | ⊕⊕⊝⊝ lowa |
|
| BMD: % change in BMD at the lumbar spine
Follow‐up: 12 months | The % change in BMD at the lumbar spine was higher in the treatment group than the control group, MD 14.50 (95% CI 12.91 to 16.09) | NA | 113 (1) | ⊕⊕⊝⊝ lowa |
| |
| BMD: % change in BMD at the hip or femur | This outcome was not reported |
| ||||
| QoL | This outcome was not reported |
| ||||
| Adverse events
Follow‐up: 12 months | There was no difference in bone or muscle pain, OR 3.00 (95% CI 0.12 to 75.22); fever, OR 3.00 (95% CI 0.12 to 75.22); or GI adverse events OR 0.67 (95% CI 0.20 to 2.26) | NA | 113 (1) | ⊕⊕⊝⊝ lowa |
| |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). BMD: bone mineral density; CI: confidence interval; GI: gastrointestinal; MD: mean difference; NA: not applicable; OR: odds ratio; QoL: quality of life; RDA: recommended daily allowance. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
| aDowngraded twice due to imprecision cause by small participant numbers and low event rates. | ||||||
| Patient or population: adults with cystic fibrosis who have had a lung transplant Settings: outpatients Intervention: bisphosphonates (IV pamidronate plus oral vitamin D and oral calcium) Comparison: oral vitamin D and oral calcium | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Bisphosphonates | |||||
| New vertebral fractures
Follow‐up: 12 months | This outcome was not reported at 12 months ‐ see comments | 1 study reported results at 24 months (Aris 2000) and found no difference in the number of participants with a vertebral fracture, OR 3.92 (95% CI 0.36 to 42.20) | ||||
| New non‐vertebral fractures
Follow‐up: 12 months | This outcome was not reported at 12 months ‐ see comments | 1 study reported results at 24 months (Aris 2000) and found no difference in the number of participants with a non‐vertebral fracture, OR 0.46 (95% CI 0.09 to 2.27) | ||||
| BMD: % change in BMD at the lumbar spine
Follow‐up: 12 months | This outcome was not reported at 12 months ‐ see comments | 1 study reported results at 24 months (Aris 2000) and found the % change in BMD was higher in the treatment group than the control group MD 6.20 (95% CI 4.28 to 8.12) | ||||
| BMD: % change in BMD at the hip or femur
Follow‐up: 12 months | This outcome was not reported at 12 months ‐ see comments | 1 study reported results at 24 months (Aris 2000) and found the % change in BMD was higher in the treatment group than the control group, MD 7.90 (95% CI 5.78 to 10.02). | ||||
| QoL | This outcome was not reported at any time point |
| ||||
| Adverse events
Follow‐up: 12 months | This outcome was not reported at 12 months ‐ see comment | 1 study reported results at 24 months (Aris 2000) and found none of the participants in either group experienced bone pain or fever | ||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). BMD: bone mineral density; CI: confidence interval; IV: intravenous; MD: mean difference; OR: odds ratio; QoL: quality of life. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
Background
Description of the condition
Cystic fibrosis (CF) is a serious autosomal recessive genetic disorder with an incidence of 1 in 3000 to 6000 births (Scotet 2020). It is caused by mutations in the cystic fibrosis transmembrane regulator (CFTR) gene (Rafeeq 2017) with a carrier rate of 1 in 28 to 40 (Scotet 2020). The incidence of CF varies between racial and ethnic groups, being more common in white populations (Cystic Fibrosis Foundation 2019). The major components of CF are lung disease and exocrine pancreatic insufficiency. In the past, only one third of people with CF lived to the age of 18 (Yankaskas 1999); however, recent advances in medical science and technology have increased the life expectancy of people with CF into the fifth decade of life (Cystic Fibrosis Foundation 2019; De Boeck 2020). As survival improves, long‐term sequelae of the disease, including osteoporosis (Paccou 2013; Putman 2019; Stalvey 2013b), diabetes mellitus (Kelsey 2019), and liver disease (Sakiani 2019) have been of increasing significance.
Osteoporosis decreases bone mineral density (BMD), making bones more susceptible to fracture. Osteopenia refers to a milder degree of bone demineralisation. Bone density is assessed using dual‐energy X‐ray absorptiometry (DXA), which measures absolute bone density in grams per square centimetre (g/cm2) and can be compared to a population mean. BMD is usually expressed as standard deviations (SDs) from the population mean, either as a Z‐score (compared to age‐ and sex‐matched data) or a T‐score (compared to the healthy young adult mean for the participant's sex). The World Health Organization (WHO) classifies osteopenia as a T‐score of between ‐1 and ‐2.5, and osteoporosis as a T‐score of ‐2.5 or less (Cosman 2014). Osteoporotic fractures account for the morbidity and mortality associated with osteoporosis (Curtis 2017).
Decreased BMD has been observed in children, adolescents, and adults with CF (Bianchi 2006; Buntain 2004; Cairoli 2019; Caldeira 2008; Gupta 2017; Nishiyama 2018; Sermet‐Gaudelus 2007). A retrospective cohort study of 102 adults aged 25 to 30 years with CF and end‐stage lung disease found a mean T‐score of ‐2.3 and ‐1.9 at the lumbar spine and femoral neck respectively, with 52% of individuals with a T‐score of less than ‐2.5 at either site (Robinson 2019). Inadequate bone mass accrual during childhood and adolescence has been reported (Buntain 2006). A study of 52 children aged 6 to 18 years showed significantly lower mean (SD) BMD in both prepubertal (P < 0.001) and peri‐ or postpubertal groups (P < 0.001) when compared to 62 healthy controls of similar age and sex. It was noted in this cohort that 37 of the 52 children were vitamin D deficient (Gupta 2017). A further study compared 153 people with CF (aged 5 to 48 years) to 149 controls; while no differences in BMD were identified in well‐nourished children (aged 5 to 10 years), a deficit during adolescence that increased throughout adulthood was noted (Buntain 2004).
The aetiology of CF‐related bone disease is thought to be multifactorial. An imbalance of increased bone resorption and decreased bone formation has been observed (Boyle 2006; Gore 2010), even in young prepubertal children (Ambroszkiewicz 2013). Proposed contributing factors to bone disease include CFTR dysfunction, malnutrition and exocrine pancreatic insufficiency; vitamin D, vitamin K or calcium deficiency; poor nutrition and growth resulting in low body weight; respiratory infections and systemic inflammation with increased systemic inflammatory cytokines; use of exogenous glucocorticoids; delayed puberty and hypogonadism; diabetes mellitus; physical inactivity resulting in decreased weight‐bearing activity and organ transplantation with associated immunosuppressive therapy and potential renal osteodystrophy (Anabtawi 2019; Aris 2005; Boyle 2006; Dumortier 2021; Gore 2010; Hall 2010; Haworth 2010; Javier 2011; Paccou 2013; Sidhaye 2019). Furthermore, BMD has been positively associated with pulmonary function, physical function, nutritional status and negatively associated with chronological age and recurrent pulmonary exacerbations (Alicandro 2014; Donadio 2013; Legroux‐Gerot 2012; Smith 2017). Studies have indicated that the loss of CFTR activity in osteoblasts results in accentuated inflammation‐driven bone resorption (Le Heron 2010; Stalvey 2013a).
The clinical consequence of CF‐related bone disease is potential fractures, including rib and vertebral fractures, which may be precipitated by coughing. Acutely, vertebral and rib fractures cause pain and debilitation, reducing lung function, ineffective cough and airway clearance, limitations in respiratory physiotherapy, and reduced physical activity. Chronic consequences may include kyphosis and chest wall deformities which may worsen lung function. Hence, a vicious cycle of further impairment in lung function and deterioration in bone health may result (Aris 2005; Boyle 2006; Hayes 2011).
Bone disease is also a consideration in lung transplantation (Mitchell 2019), as the high‐dose corticosteroids and other immunosuppression required post‐transplantation can be expected to worsen bone disease further (Aris 1996; Kovvuru 2020).
Description of the intervention
Bisphosphonates are a class of drugs that inhibit bone resorption (Cremers 2019; Giger 2013; Russell 2007). Considerations in using bisphosphonate therapy include different formulations (oral, intravenous (IV)), dosage, frequency of administration, intermittent versus continuous dosing, and duration of therapy (Russell 2006).
Potential side effects include an acute‐phase response leading to fever and 'flu‐like' symptoms (myalgia, arthralgia malaise). Osteonecrosis of the jaw has been associated with high‐dose IV bisphosphonate therapy in people with malignancy, and less commonly in osteoporosis (Pendrys 2008; Reyes 2016). Prolonged bisphosphonate use has also been associated with atypical femoral fractures, a rare subset of subtrochanteric or diaphyseal fractures (Saleh 2013; Starr 2018), and incidence increases with length of use. Upper gastrointestinal side effects including oesophagitis and oesophageal ulcers have been associated with oral agents (Cryer 2002). Studies estimating the incidence of these side effects vary, but are generally between 9% and 11%. A recent study evaluating gastrointestinal side effects in a hospital setting between 2017 and 2019 found an incidence of 10.7% with administration of oral bisphosphonates (Nguyen 2021). There have been links to increased incidence of gastrointestinal cancers; however, a recent retrospective study over nine years found no association of oral bisphosphonates with cancer risk (Choi 2020). Increased risk of atrial fibrillation has been reported with bisphosphonate use, however the evidence is mixed and unconfirmed (Reyes 2016).
How the intervention might work
Bisphosphonates have proven effective treatments for disorders of excessive bone resorption (Giger 2013). These disorders include Paget's disease of bone, myeloma, bone metastases (Russell 2006); postmenopausal osteoporosis (Black 1996; Gui‐Feng 2018); other forms of osteoporosis (e.g. associated with glucocorticoid administration (Allen 2016; Saag 1998)); and osteogenesis imperfecta (Dwan 2016; Glorieux 1998; Shi 2016). Positive outcomes have included increased bone mass, increased BMD, and a reduction in fracture frequency.
Bone resorption has been observed to increase during CF pulmonary exacerbations due to the stimulatory effect of pro‐inflammatory cytokines on osteoclast activity (Shead 2010). Loss of the CFTR in osteoblasts may exacerbate the effect of inflammation to stimulate osteoclastogenesis (Le Heron 2010; Stalvey 2013a; Weitzmann 2013). Since bisphosphonates inhibit osteoclastic bone resorption, these agents may minimise bone loss in this context.
A double‐blind randomised controlled trial (RCT) observed women with osteopenia over a six‐year period who received four infusions of either 5 mg of zoledronate or normal saline at 18‐month intervals. The risk of vertebral and non‐vertebral fragility fractures was significantly lower (P < 0.001) when compared to the placebo group (Reid 2018).
A Cochrane Review comparing bisphosphonates for glucocorticoid‐induced osteoporosis (GIOP) to control groups found a statistically significant reduction in vertebral fractures with a relative improvement of 43% (95% confidence interval (CI) 9% to 65%); a non‐statistically significant reduction in non‐vertebral fractures with a relative improvement of 21% (95% CI ‐33% to 53%); and significant improvement in BMD of both lumbar vertebrae and femoral neck, with absolute increases of 3.5% (95% CI 2.9% to 4.1%) and 2.06% (95% CI 1.45% to 2.68%) respectively (Allen 2016). This evidence is particularly promising since corticosteroid use is associated with osteoporosis among people with CF.
Why it is important to do this review
This is an update of a previous Cochrane Review (Brenckmann 2001; Conwell 2009; Conwell 2012; Conwell 2014).
A multifaceted approach to the prevention and treatment of low BMD has been recommended including optimising vitamin, calcium, and nutritional status, encouraging weight‐bearing exercise, endocrinological assessment and management of delayed puberty or hypogonadism, aggressive treatment of pulmonary infections, minimising exposure to corticosteroids, and treatment of CF‐related diabetes (Aris 2005). A 2005 consensus statement addressing the issue of bone health and disease in CF recommended consideration of oral or IV bisphosphonates in individuals with DXA T‐ or Z‐scores of 2.0 or less, awaiting transplant or with a BMD loss more than 3% to 5% per year (Aris 2005).
The 2011 European Cystic Fibrosis Bone Mineralisation guidelines outline recommended assessment, prevention and treatment strategies in detail (Sermet‐Gaudelus 2011). In terms of screening for CF‐related bone disease in children, the guidelines recommend starting DXA screening between 8 and 10 years of age (or earlier if there are significant risk factors for low BMD). They further recommend consideration of bisphosphonate treatment in adults who:
-
are taking continuous systemic oral glucocorticoids for at least three months with a BMD Z‐score or T‐score of ‐1.5 or less;
-
sustain a low trauma fracture while taking systemic glucocorticoids;
-
have had a low trauma fracture or in whom the lumbar spine or total hip or femoral neck Z‐score or T‐score is ‐2.0 or less and there is evidence of significant bone loss (more than 4% per year) on serial DXA measurements despite optimisation of clinical care;
-
are awaiting or have undergone solid organ transplantation and have a BMD Z‐score or T‐score of ‐1.5 or less;
-
are starting a prolonged course of oral glucocorticoids (over three months) and have a BMD Z‐score or T‐score of ‐1.5 or less (Sermet‐Gaudelus 2011).
These guidelines also recommend the consideration of bisphosphonate treatment after failure of optimal conservative treatment in children who:
-
are taking continuous systemic glucocorticoids for at least three months and have a history of low trauma fracture or have a BMD Z‐score of ‐2.0 or less (or both);
-
have a BMD Z‐score of ‐2.0 or less in the total body or lumbar spine and a history of low‐trauma extremity fractures or vertebral compression fractures;
-
are awaiting or have undergone solid organ transplantation and have a BMD Z‐score of ‐2.0 or less;
-
are prescribed continuous systemic glucocorticoids and have a BMD Z‐score of ‐2.0 or less (Sermet‐Gaudelus 2011).
In transplant recipients, the recommendations are that:
-
low BMD and a history of low trauma fractures are not an absolute contraindication for lung transplant listing in people with CF;
-
bone loss after solid organ transplantation can be lessened by the prescription of bisphosphonates in people with CF (Sermet‐Gaudelus 2011).
In 2020, an expert panel comprising paediatricians and rheumatologists provided evidence‐based recommendations on the diagnosis and treatment of secondary osteoporosis in children. Regarding screening for CF‐related bone disease, they recommend specifically following the above 2011 guidelines (Galindo‐Zavala 2020). Regarding bisphosphonate use, the recommendations are:
-
clinicians should consider the use of bisphosphonates prior to established osteoporosis, in children with
-
low BMD in early puberty;
-
low Z‐scores and decreasing trajectory; and
-
pathological fracture or vertebral fracture regardless of Z‐score;
-
-
IV bisphosphonates are preferred in paediatric osteoporosis, particularly in children with vertebral fractures;
-
oral bisphosphonates are only to be used in children with mild osteoporosis, no vertebral fractures and no contraindications with oesophagitis risk factors (e.g. gastroesophageal reflux or hiatus hernia); and
-
bisphosphonate dosing should be ceased or weaned for children with no fractures for the previous year and with a Z‐score greater than ‐2.0 (Galindo‐Zavala 2020).
Given that the most recent guidelines recommend considering bisphosphate therapy, a review of the available evidence assessing bisphosphonates for osteoporosis in people with CF is important.
Objectives
To assess the effects of bisphosphonates in improving clinical outcomes in people with cystic fibrosis (CF) including bone health (fractures and bone mineral density (BMD)), quality of life (QoL), adverse effects and survival.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs).
Types of participants
People of all ages and of both sexes with cystic fibrosis (CF) diagnosed clinically or by sweat and genetic testing, including all degrees of disease severity and bone mineral density (BMD).
Types of interventions
The review authors considered for inclusion all RCTs which compared bisphosphonates to controls (other bisphosphonates, placebo or usual treatment) for treating or preventing osteoporosis in people with CF. All doses and routes of administration were eligible. Trials had to have a minimum duration of six months to allow time to observe an effect of treatment.
Types of outcome measures
The review authors planned to assess the following outcomes for each comparison in the review.
Primary outcomes
-
Fractures:
-
number of participants with any fracture;
-
number of participants with fractures by site:
-
non‐vertebral;
-
vertebral.
-
-
Secondary outcomes
-
BMD as measured by dual‐energy X‐ray absorptiometry (DXA), reported as percentage (%) change from baselinea:
-
lumbar spine;
-
hip or femur;
-
radius;
-
total body.
-
-
Quality of life (QoL) (CF‐related, osteoporosis‐related or general QoL measures).
-
Adverse events such as bone pain, fever and gastrointestinal (GI) adverse events (number of participants, number of adverse events).
-
Withdrawals:
-
withdrawals due to adverse events;
-
total withdrawals.
-
-
Survival.
aThe review authors will also consider data reported using other methods of measuring bone density such as single‐energy X‐ray absorptiometry (SXA) and quantitative tomography (QCT), but will report separately if these are available.
Search methods for identification of studies
The review authors did not limit searches by date, language or publication status.
Electronic searches
The Group's Information Specialist identified relevant trials from the Group's Cystic Fibrosis Trials Register using the terms: CF‐related bone disease AND bisphosphonates.
The Cystic Fibrosis Trials Register is compiled from electronic searches of the Cochrane Central Register of Controlled Trials (CENTRAL) (updated each new issue), weekly searches of MEDLINE, a search of Embase to 1995 and the prospective hand searching of two journals ‐ Pediatric Pulmonology and the Journal of Cystic Fibrosis. Unpublished work is identified by searching the abstract books of three major cystic fibrosis conferences: the International Cystic Fibrosis Conference; the European Cystic Fibrosis Conference and the North American Cystic Fibrosis Conference. For full details of all searching activities for the register, please see the relevant sections of the Cystic Fibrosis and Genetic Disorders Group website.
Date of the most recent search of the Group's Cystic Fibrosis Trials Register: 5 May 2022.
We also searched the following databases and trial registries:
-
PubMed (www.ncbi.nlm.nih.gov/pubmed/; 1946 to 5 May 2022);
-
US National Institutes of Health Ongoing Trials Register Clinicaltrials.gov (www.clinicaltrials.gov; searched 5 May 2022);
-
World Health Organization International Clinical Trials Registry Platform (WHO ICTRP) (trialsearch.who.int; searched 5 May 2022).
For details of our search strategies, please see Appendix 1.
Searching other resources
We checked the bibliographies of included studies and any relevant systematic reviews identified for further references to relevant trials.
For the original review, the review authors searched abstracts from major osteoporosis conferences (The American Society for Bone and Mineral Research and The Institute of Biomedical Science (ASBMR‐IBM) 2nd Joint Meeting 1998; ASBMR 21st Annual Meeting 1999) and also the reference lists from the retrieved articles.
Data collection and analysis
Selection of studies
In the original review, two authors (Christine Brenckmann (CB) and Alexandra Papaioannou (AP)) independently reviewed the trials in order to assess which trials should be included. For the updated reviews from 2009 to 2014, two authors (Louise Conwell (LC) and Anne Chang (AC)) independently reviewed the trials included in the original review in addition to trials identified by the updated searches. In the current review from 2022, a third author (Tomas Jeffery (TJ)) also reviewed the data. If there was disagreement about whether a trial should be included, the authors planned to ask an independent author from a third centre to review the paper(s) in question. The review authors documented the reasons for excluding any trial.
Data extraction and management
In the original review, each author independently extracted trial information (see below) and data for the outcome measures listed above. The review authors contacted the first authors of the included trials to verify their data and obtain unpublished data where necessary. The authors used the Cochrane Review Manager software to compile and analyse the data (RevMan Web 2022). The authors compared their data and resolved differences by referring to the original article; they planned to resolve any remaining differences with a third individual.
From 2009 to 2014 the authors (LC, AC) reviewed trials that satisfied the inclusion criteria. In the 2022 review a third author (TJ) also reviewed the data. We recorded the following information when available: trial setting; year of trial; source of funding; participant recruitment details (including number of eligible participants); inclusion and exclusion criteria; randomisation and allocation concealment method; numbers of participants randomised; blinding (masking) of participants, care providers and outcome assessors; dose and type of intervention; duration of therapy; co‐interventions; numbers of participants not followed up; reasons for withdrawals from trial protocol (clinical, side effects, refusal and other); side effects of therapy; and whether intention‐to‐treat analyses were possible.
The review authors reported data at six months, 12 months, and annually thereafter, which are appropriate time points to assess treatment effects on fracture frequency and duration. For percentage change in BMD, the review authors combined and reported data for the end of trial as it is unknown what length of trial is needed for effect of treatment to be evident. The review authors used the Cochrane Review Manager software to compile and analyse the data (RevMan Web 2022). Similarly, the authors compared their data and resolved differences by referring to the original article.
The review authors conducted separate analyses for participants who had received a lung transplant and for those who had not. At this stage, the number of people with CF who have received other organ transplants is small. Therefore, the authors planned to include individuals with other organ transplants in the analysis of participants with a lung transplant, since they share a common risk factor for osteoporosis, that is the long‐term use of immunosuppressive agents which lower BMD.
For the current version of the review (2022), the authors have analysed children (aged 18 years or younger) and adults (over 18 years) separately. Originally, they planned this division as a subgroup analysis if they had been able to combine at least 10 trials, but for the current update the authors decided to present adult data separately to paediatric data.
Assessment of risk of bias in included studies
The two authors who performed the original review independently assessed the quality of the trials using the system as described by Jadad (Jadad 1996). If there was disagreement about whether a trial should be included, or about the quality score it should receive, the authors asked an independent author from a third centre to review the paper(s) in question.
In this review update, the authors (TJ, LC, AC) independently assessed the risk of bias in the trials using the criteria described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2017):
-
randomisation process i.e. the generation of allocation sequence;
-
allocation process i.e. quality of allocation blinding;
-
degree of blinding (of clinician or person delivering treatment, of participant or of outcome assessor);
-
is attrition bias present i.e. use of intention‐to‐treat analysis?
-
is selective reporting present?
For each of the criteria, the authors gave a judgement of a high, low, or unclear risk of bias based on guidance from Cochrane (Higgins 2017) and gave the reasons for these judgements in the risk of bias tables (Characteristics of included studies).
Measures of treatment effect
For the dichotomous outcome variables (adverse events, fractures, survival) of each individual study, the authors calculated the odds ratio (OR) using a modified intention‐to‐treat analysis (where incomplete data assumes failure of treatment). They also calculated the summary ORs and 95% confidence intervals (CIs) using Cochrane's statistical package, RevMan Web (RevMan Web 2022). They planned to calculate the numbers needed to treat (NNT) from the pooled OR and its 95% CIs applied to a specified baseline risk, which is the sum of all the events in the control groups (in all trials) divided by the total participant numbers in control groups in all trials using an online calculator (Cates 2003).
For continuous outcomes (changes in BMD and laboratory values), the authors recorded the mean relative change from baseline for each group or mean post‐treatment or post‐intervention values and standard deviation (SD). They planned to calculate the SDs if standard errors were reported. They would then calculate a pooled estimate of treatment effect by the mean difference (MD) and 95% CIs, again using Cochrane's statistical package (RevMan Web 2022). If trials reported outcomes using different measurement scales, the authors planned to estimate the standardised MD.
Unit of analysis issues
There were no cross‐over trials, but if there had been, the authors planned only to use data from the first arm of the trial for any analysis due to the potential for a carry‐over effect. They would have analysed count data of rare events as rates (number of counts to the amount of time during which they could have happened). They planned to use the summary statistic rate ratio in meta‐analysis. For rate ratios of common events, whereby one participant may have more than one event, they planned to use the generic inverse variance (GIV) method of analysis.
Dealing with missing data
The review authors contacted primary authors of trials to obtain missing data or clarify data. Bianchi was contacted and provided data, demographic and methodology clarification (Bianchi 2013). The review authors attempted to contact Krasovsky and Boyle for data and demographic clarification, however to date have received no response (Boyle 2005; Krasovsky 2010).
Assessment of heterogeneity
The authors planned to describe any heterogeneity between the trial results and test it to see if it reached statistical significance using the I2 statistic (Higgins 2003). This measure describes the percentage of total variation across trials that are due to heterogeneity rather than by chance (Higgins 2003).
The values of I2 lie between 0% and 100%, and a simplified categorisation of heterogeneity that the authors planned to use is of low (I2 value of 0% to 40%), moderate (I2 value 30% to 60%), substantial (I2 value 50% to 90%), and considerable (75% to 100%) (Higgins 2017). The P value from the Chi2 test also indicates the strength of evidence for heterogeneity, considered to be statistically significant when the P value was less than 0.10 (Higgins 2017).
Assessment of reporting biases
In order to identify selective reporting, the review authors compared outcome measures reported within the published papers to the measures described in the methodology sections or with the trial protocols if they were available.
Data synthesis
The review authors included the results from trials that met the inclusion criteria and reported any of the outcomes of interest in the subsequent meta‐analyses using a fixed‐effect model. They would have used a random‐effects model, if there was at least moderate heterogeneity (I2 over 30%).
Subgroup analysis and investigation of heterogeneity
The authors analysed the trials in subgroups of drug route of administration (intravenous (IV) versus oral administration) when assessing outcomes. Whilst not relevant in this update, in future updates, the authors plan a subgroup analysis of participants taking cystic fibrosis transmembrane regulator (CFTR) modulating drugs.
Sensitivity analysis
The authors had also planned to conduct sensitivity analyses to assess the impact of the potentially important factors on the overall outcomes:
-
differences in the medications used in the intervention and comparison groups;
-
analysis using a random‐effects model;
-
analysis by 'treatment received'; and
-
analysis by 'intention‐to‐treat'.
The authors report oral and IV administration separately within the Effects of interventions section, but there were not enough data to perform a meaningful sensitivity analysis by further breaking down into individual medications used. They present the findings of the sensitivity analysis undertaken using a random‐effects model at the end of the section Effects of interventions. There were not sufficient data available to undertake sensitivity analyses by 'treatment received' or by 'intention‐to‐treat'.
Summary of findings and assessment of the certainty of the evidence
The authors have presented a summary of findings table for each separate comparison included in the review. Within each table they have reported the following outcomes which they selected based on their clinical relevance and importance to the CF community.
-
New vertebral fractures at 12 months.
-
New non‐vertebral fractures at 12 months.
-
BMD (% change) at lumbar spine at 12 months.
-
BMD (% change) at hip/femur at 12 months.
-
QoL at 12 months.
-
Adverse events.
The authors determined the certainty of the evidence using the GRADE approach and starting from a judgement of high certainty, downgraded evidence in the presence of a high risk of bias in at least one trial, indirectness of the evidence, unexplained heterogeneity or inconsistency, imprecision of results, and high probability of publication bias (Schünemann 2017a; Schünemann 2017b). They downgraded evidence by one level if they considered the limitation to be serious and by two levels if very serious.
Results
Description of studies
Results of the search
The original review identified two trials. The 2014 version of this review included seven trials. In the 2022 version of the review, searches identified 55 new records, 25 of which the authors excluded on the basis of title and abstract and are not described further. The authors assessed 30 references to 17 trials for eligibility with full‐text review. They excluded eight references to eight trials and describe these in Characteristics of excluded studies
In total, nine clinical trials with 385 participants met the inclusion criteria for this review (Aris 2000; Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010; Papaioannou 2008).
Details of the selection process are presented in Figure 1.

Selection process for this update.
Included studies
Nine clinical trials met the inclusion criteria for this review (Aris 2000; Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010; Papaioannou 2008) and the authors described the trial details in Characteristics of included studies.
Two trials were published only as abstracts; the review authors contacted the lead investigator of one for details of the full publication, and the supervising author for another, but to date have not received a reply (Boyle 2005; Krasovsky 2010). Four trials were published both as abstracts and full review papers (Aris 2000; Aris 2004; Haworth 2001; Haworth 2011). Three trials were published as full review papers (Bianchi 2013; Chapman 2009; Papaioannou 2008).
Funding for one trial was provided by grants from the Cystic Fibrosis Foundation and the Verne S Caviness General Center for Clinical Research (Aris 2000). Another trial was funded by the US Food and Drug Administration, Merck and Co. Inc., the Clinical Nutrition Research Unit, the Verne S Caviness General Center for Clinical Research at University of North Carolina, the Cystic Fibrosis Foundation, and the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) (Aris 2004). Novartis Pharmaceuticals Pty Ltd (Australia) partly funded one trial (Chapman 2009). Study funding was also provided by Merck Frosst Canada (Papaioannou 2008). Haworth and colleagues received funding from the Cystic Fibrosis Trust in the UK (Haworth 2001; Haworth 2011). The later Haworth study was funded by unrestricted educational grants from Proctor & Gamble (Norwich, USA) and the Cystic Fibrosis Trust, with support to investigators from the UK National Institute for Health and Care Research (NIHR) (Haworth 2011). The Telethon Foundation (Italy) funded one study that included children (Bianchi 2013). It is unclear whom provided funding for the two trials published as abstracts, Boyle and Krasovsky (Boyle 2005; Krasovsky 2010).
Factors that will contribute to the heterogeneity in the results of the review include differences in trial populations and concomitant general health, activity levels, and medications (prednisone, cyclosporin A, azathioprine in the transplant group).
Trial design
All the trials had similar designs, duration of planned intervention (12 to 24 months), and outcome measures. All trials were a parallel design, none had a cross‐over design. There were four single‐centre trials (Aris 2000; Aris 2004; Boyle 2005; Haworth 2001), four multicentre trials (Bianchi 2013; Chapman 2009; Haworth 2011; Papaioannou 2008), and one did not state if it was single or multicentre (Krasovsky 2010). Only one trial reported sample size and power calculations (Bianchi 2013). In the Boyle trial, enrolment ceased after five participants were randomised and follow‐up duration was decreased from 12 months to six months due to adverse events (i.e. musculoskeletal pain) (Boyle 2005). The follow‐up duration of another trial was also shortened from 12 months to six months due to adverse events (i.e. bone pain) (Haworth 2001).
Participants
There were a total of 385 included participants across the nine included trials. Eight trials recruited adults only (Aris 2000; Aris 2004; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010; Papaioannou 2008) and one trial recruited both adults and children (aged 18 years or younger, recruiting down to an age of five years) where children comprised 88% (113 out of 128) participants in the intervention phase (Bianchi 2013). The numbers of participants in each trial ranged from five participants (Boyle 2005) to 128 participants (Bianchi 2013).
Participants in all trials were required to have a confirmed diagnosis of cystic fibrosis (CF) and low bone mineral density (BMD); the inclusion criteria and degree of BMD was variable across trials. Five trials used low T‐scores as a marker of low BMD (Aris 2000; Aris 2004; Boyle 2005; Chapman 2009; Papaioannou 2008) and four trials used low Z‐scores (Bianchi 2013; Haworth 2001; Haworth 2011; Krasovsky 2010). Most trials using oral bisphosphonate therapy stated they excluded individuals with existing gastrointestinal (GI) disease that could be exacerbated by the drugs (Aris 2004; Haworth 2011; Papaioannou 2008) or otherwise stated any contraindications, which would likely include existing GI disease (Bianchi 2013).
Boyle enroled five participants but did not clarify which sex participants were. All other trials gave such details, which when combined included 156 females, 219 males. Three trials had roughly equal numbers of males and females (Aris 2000; Aris 2004; Bianchi 2013) and five trials had more males than females (Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010; Papaioannou 2008). No trials had more females than males.
One trial assessed 34 adults post lung transplantation (Aris 2000). The participants in the other seven trials had CF but had not undergone a lung transplant.
Interventions
Two trials assessed intravenous (IV) pamidronate (Aris 2000; Haworth 2001) and two trials assessed IV zoledronate (Boyle 2005; Chapman 2009); oral alendronate was used in four trials (Aris 2004; Bianchi 2013; Krasovsky 2010; Papaioannou 2008) and oral risedronate in one trial (Haworth 2011).
All participants in eight of the trials received supplemental calcium and vitamin D (Aris 2000; Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2011; Krasovsky 2010; Papaioannou 2008). In the 2001 study by Haworth, participants with pancreatic insufficiency were prescribed long‐term oral vitamin D supplements (all participants except one participant in the control group) (Haworth 2001). Oral prednisolone was administered to all participants of one study for three days starting on the morning of the first infusion (Chapman 2009). This was repeated with subsequent infusions if a reaction to the first infusion was thought likely.
Outcomes measured
Seven trials reported fractures, vertebral and non‐vertebral (Aris 2000; Aris 2004; Bianchi 2013; Chapman 2009; Krasovsky 2010; Haworth 2011; Papaioannou 2008).
All trials assessed change in BMD post intervention. BMD at the lumbar spine was reported by all studies (Aris 2000; Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010; Papaioannou 2008). BMD at the femoral neck was reported by six studies (Aris 2000; Aris 2004; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010). BMD at the distal forearm was reported by two studies (Chapman 2009; Haworth 2001).
Seven trials reported withdrawals (Aris 2000; Aris 2004; Bianchi 2013; Chapman 2009; Haworth 2001; Haworth 2011; Papaioannou 2008).
Eight trials all reported both survival and adverse events (Aris 2000; Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Papaioannou 2008). Only one trial reported on quality of life (QoL) (Papaioannou 2008).
Excluded studies
Eight clinical trials were excluded (Cawood 2005; Conway 2004; Hardin 2005; Haworth 1998; NCT01702415; NCT01882400; Ringuier 2004; Rudge 2005).
Four trials were not randomised control trials (RCTs) (Cawood 2005; Conway 2004; NCT01882400; Ringuier 2004). One trial assessed the effect of growth hormone on bone mineral content in children with CF, but did not assess the use of bisphosphonates and hence did not meet the inclusion criteria for this review (Hardin 2005). A further trial only examined the adverse event profile of bisphosphonates and was not a treatment trial (Haworth 1998). Of the remaining excluded trials, one assessed the effects of once‐weekly oral alendronate for 12 months on bone in children on glucocorticoid treatment; however, only one of the 22 included children had CF and this participant was in the placebo group (Rudge 2005) and the final excluded trial had its funding withdrawn and it was stopped before recruiting its first participant (NCT01702415).
Risk of bias in included studies
For detailed information on the risk of bias of each included trial, please refer to the risk of bias tables attached to the Characteristics of included studies section of this review. The summary and risk of bias items are presented in the figures (Figure 2; Figure 3).

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Generation of sequence
All trials stated that allocation was randomised.
We judged three trials to have a low risk of bias (Bianchi 2013; Haworth 2011; Papaioannou 2008). In the first trial, centralised randomisation was undertaken by a statistician using a computer‐generated list of random numbers (Bianchi 2013). A further trial reported the use of a computer‐generated randomisation code, stratified according to institution (prepared by an independent randomisation centre) with use of block allocation to ensure equitable distribution to each treatment group (Papaioannou 2008). In the third trial, participants were allocated to treatment or placebo using a computer program to minimise differences between groups in treatment centre, sex and baseline lumbar spine BMD (Haworth 2011). Two trials described a "blocks of four" design, but the actual method of randomisation was not discussed and we judged the risk of bias due to the generation of the randomisation sequence as unclear (Aris 2000; Aris 2004). The remaining four trials also did not discuss the method of randomisation and hence the risk of bias was unclear (Boyle 2005; Chapman 2009; Haworth 2001; Krasovsky 2010).
Concealment of allocation sequence
Due to the computer‐generated schedules of random numbers, the concealment of allocation and hence risk of bias was low in three trials (Bianchi 2013; Haworth 2011; Papaioannou 2008). However, concealment of the allocation schedule was judged to be unclear in the remaining six trials (Aris 2000; Aris 2004; Boyle 2005; Chapman 2009; Haworth 2001; Krasovsky 2010).
Blinding
Participants
In two trials, participants were not blinded to the treatment group and we judge this to have a high risk of bias (Aris 2000; Krasovsky 2010). In another trial, blinding of participants was not discussed, however the intervention group received an infusion and the control group did not, meaning the participants likely knew which group they were in, and thus we judged the risk of bias to be high (Haworth 2001). Participants were blinded to the intervention group in the remaining six trials, which we therefore judged to have a low risk of bias (Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2011; Papaioannou 2008).
Clinician or person delivering treatment
In two trials, clinicians giving the interventions were not blinded and thus risk of bias was high (Aris 2000; Krasovsky 2010). Three trials were described as "double‐blind", but the blinding of those delivering treatment was not specifically discussed (Aris 2004; Boyle 2005; Chapman 2009); in a further trial, blinding was not reported, however the intervention group received an infusion and the control group did not, meaning those delivering the treatment likely knew which participants fell into which group, thus the risk of bias was high (Haworth 2001). Hence, these four trials were judged to have an unclear risk of bias. Clinicians delivering treatment were blinded in three trials, leading us to judge them to have a low risk of bias (Bianchi 2013; Haworth 2011; Papaioannou 2008).
Outcome assessors
In one trial, only the radiologist who interpreted the dual‐energy X‐ray absorptiometry (DXA) scans was blinded (Aris 2000). In the Chapman trial, it was stated that the personnel who performed and analysed the DXA scans were blinded to the treatment group, but it was not clear whether all the outcome assessors were blinded (Chapman 2009). In two trials, blinding was not reported (Haworth 2001; Krasovsky 2010) and two other trials were described as "double‐blind" although it was not specifically discussed whether all the outcome assessors were blinded (Aris 2004; Boyle 2005). Hence, considering these different types of participants and personnel together, there was some risk of bias in six of the trials (Aris 2000; Aris 2004; Boyle 2005; Chapman 2009; Haworth 2001; Krasovsky 2010).
Person(s) responsible for participants care, participants and outcome assessors were blinded to treatment group allocation in two trials (Bianchi 2013; Papaioannou 2008). In the later Haworth trial, only the study pharmacist had access to the treatment allocation (Haworth 2011). Hence, there was a low risk of bias in these three trials (Bianchi 2013; Haworth 2011; Papaioannou 2008).
Incomplete outcome data
Six trials described withdrawals from treatment but withdrawal rates and hence risk of attrition bias varied; for example, from protocol commencement to BMD (lumbar spine) measurement at end of the trial, total withdrawals were 13/53 (25%) (Aris 2004), 3/5 (60%) (Boyle 2005), 3/22 (14%) (Chapman 2009), 3/31 (10%) (Haworth 2001), 12/36 (33.3%) (Haworth 2011), and 8/56 (14.2%) (Papaioannou 2008).
We judged four trials to have a low risk of bias (Bianchi 2013; Haworth 2001; Haworth 2011; Papaioannou 2008). One trial reported no withdrawals (Bianchi 2013). Haworth provided details of withdrawals from both trials. In the earlier trial, one participant in each group died of respiratory failure and one participant in the treatment group underwent a double lung transplant (Haworth 2001); and in the later trial, reasons for withdrawals were provided by the author and these were fairly equally spread across groups (Haworth 2011). In the remaining trial, all analyses were performed as intention‐to‐treat (included all available data) and withdrawals were described (Papaioannou 2008).
We judged three trials to have an unclear risk of bias (Aris 2000; Chapman 2009, Krasovsky 2010). In the Aris trial, three participants died during the course of the trial before the first primary end‐point measurement (causes of death were one each from sepsis, acute respiratory distress syndrome, and obliterative bronchiolitis) and these participants were excluded from the final analysis of baseline characteristics and outcome data. However, it was not reported which treatment group they were in (Aris 2000). In the Chapman trial, it was unclear which specific participants had BMD measurements available at each time point, particularly for forearm measures (fewer measurements compared with lumbar spine and femoral neck) (Chapman 2009). In the Krasovsky trial, it was not addressed whether or not there were any withdrawals from the study; the review authors reached out for clarification however there was no reply (Krasovsky 2010).
We judged two trials to have a high risk of bias (Aris 2004; Boyle 2005). In the 2004 Aris trial there were five withdrawals between commencement of protocol and outcomes measured at six months, but it was not stated whether they were in the treatment or the control group (Aris 2004). Also, between six months and one year there were a further four withdrawals from each group described with reasons and between one and two years (follow‐up period) there were nine withdrawals from the treatment group and seven from the placebo group. Only 75% of participants provided data for analysis for the primary endpoint of the trial at one year (Aris 2004). In the trial by Boyle, 40 participants were planned for enrolment but only five enroled (three in treatment group) before the trial was stopped by the Data and Safety Monitoring Board after three participants experienced adverse effects. It was assumed that the three participants with bone pain were in the treatment group, although this was not stated, meaning 60% of participants dropped out before the planned completion of the trial (Boyle 2005).
Selective reporting
Outcome measures described in the methodology were reported for most trials, hence we judged them to have a low risk of bias (Aris 2004; Bianchi 2013; Chapman 2009; Haworth 2011; Papaioannou 2008). The exception was the serum and urine biochemical measurements at the two‐day time point (only after first pamidronate infusion in intervention group) which were not reported in one trial (Aris 2000), bias was therefore judged as high. Two trials did not report fractures as an outcome (Boyle 2005; Haworth 2001). Whilst neither of these outcomes were detailed in the methodology, the absence is curious as fractures are an outcome measured in most other trials of their kind, and arguably the primary reason to initiate bisphosphonate therapy. We judged these to have an unclear risk of bias. Additionally, Boyle was published only as an abstract, making judgement of bias difficult. The remaining trial was also published as an abstract only, with insufficient detail to allow judgement on this domain (unclear risk of bias) (Krasovsky 2010).
Other potential sources of bias
There were other potential sources of bias in four trials (Haworth 2001; Aris 2004; Boyle 2005; Bianchi 2013).
Three trials were stopped early (Aris 2004; Boyle 2005; Haworth 2001). The first trial was designed to be two years in length, but few participants were willing to consent to such a lengthy study, so the protocol was revised to measure the primary endpoint at 12 months (Aris 2004). The second trial was stopped by the Data and Safety Monitoring Board after three participants experienced dramatic musculoskeletal pain, two requiring emergency room assessment. Symptoms began six to eight hours after infusion, peaked at 12 to 18 hours, and were characterised by severe chest and back pain. Along with musculoskeletal pain, one participant also experienced a fever of 104° F lasting for several hours and a rise in tumour necrosis factor‐α. Although the most severe symptoms resolved within 48 to 72 hours, participants reported continued arthralgias for up to a week (Boyle 2005). The third trial was planned to run for one year, but was shortened to six months because of adverse events (Haworth 2001).
In the Bianchi trial of oral alendronate there was a 12‐month observation phase in which all participants received counselling to adjust their dietary calcium intake to the recommended daily allowance, they were prescribed oral calcifediol (15 micrograms (ug)/day if bodyweight was under 20 kg; 25 ug/day if bodyweight was between 20 kg and 30 kg; and 35 ug/day if bodyweight was over 30 kg) and previous vitamin D supplementation (cholecalciferol 400 international units (IU)/day) was withdrawn (Bianchi 2013). The trial only included those participants in the intervention phase who did not have an increase in bone mineral apparent density by 5% or more after 12 months in the observational phase. If these participants were also included, it is possible the results of the antiresorptive intervention would have shown an even greater positive effect.
Effects of interventions
See: Summary of findings 1 Bisphosphonates compared with control for osteoporosis in people with cystic fibrosis who have not had a lung transplant; Summary of findings 2 Bisphosphonates compared with placebo for osteoporosis in children with cystic fibrosis who have not had a lung transplant; Summary of findings 3 Bisphosphonates compared with no bisphosphonates for osteoporosis in people with cystic fibrosis who have had a lung transplant
Nine trials were included, eight examined participants who had not undergone lung transplantation (Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010; Papaioannou 2008). Seven of the trials of non‐lung transplant participants were in adults only, but in one trial 88% of participants in the intervention phase were aged between five and 18 years (Bianchi 2013). We present the adult and the paediatric data separately. The remaining trial studied adults who had received lung transplants (Aris 2000).
Please see the summary of findings tables for details on certainty of evidence and rationale for quality grading:
-
bisphosphonates compared with control for osteoporosis in adults with CF who have not had a lung transplant (summary of findings Table 1);
-
bisphosphonates compared with placebo for osteoporosis in children with CF who have not had a lung transplant (summary of findings Table 2); and
-
bisphosphonates compared with no bisphosphonates for osteoporosis in people with CF who have had a lung transplant (summary of findings Table 3).
Bisphosphonates versus control for osteoporosis in adults with CF who have not had a lung transplant
Primary outcome
1. Fractures
Two trials did not report on fractures as an outcome measure. We contacted the authors to clarify if these had been measured in the trials, but have not received a reply to date (Boyle 2005; Haworth 2001).
a. Number of participants with any fracture
Combining data for both vertebral and non‐vertebral fractures from the available trials, there was no difference between groups at 12 months (odds ratio (OR) 0.57, 95% confidence interval (CI) 0.13 to 2.50; I2 = 0; 5 trials, 142 participants; Analysis 1.1) and no fractures reported at 24 months (2 trials, 44 participants; Analysis 1.1). There were no reported fractures in three trials (Bianchi 2013; Krasovsky 2010; Chapman 2009). See Figure 4.

Forest plot of comparison between bisphosphonates versus control (without lung transplantation), Outcome 1a Number of participants with any fracture.
b. Number of participants experiencing fractures by site
i. Non‐vertebral
Four trials (n = 95) reported data for non‐vertebral fractures at 12 months (Aris 2004; Bianchi 2013; Chapman 2009; Krasovsky 2010). In the 2004 Aris trial, two out of 20 participants in the alendronate group reported fractures (arm and rib) compared to one out of 20 participants in the control group (toe fracture) (Aris 2004). When data were combined, there was no statistically significant difference in the number of participants with new non‐vertebral fractures in the treatment group compared to controls (OR 2.11, 95% CI 0.18 to 25.35; 4 trials, 95 participants; very low‐certainty evidence; Analysis 1.2).
Two trials (n = 44) reported data for non‐vertebral fractures at 24 months (Chapman 2009; Haworth 2011). Chapman did not report any fractures in either group of 10 participants (Chapman 2009). Similarly, there were no non‐vertebral fractures in either group of 12 participants with the intervention of 35 mg weekly of oral risedronate for 24 months (Haworth 2011). See Figure 5.

Forest plot of comparison between bisphosphonates versus control (without lung transplantation), Outcome 1b i. Number of participants with non‐vertebral fractures.
ii. Vertebral
Five trials (n = 142) provided data for vertebral fractures at the 12‐month time point (Bianchi 2013; Chapman 2009; Haworth 2011; Krasovsky 2010; Papaioannou 2008). There were no vertebral fractures reported for either group (20 participants in each) in the trial assessing 10 mg daily of oral alendronate (Aris 2004) or for either group (10 participants in each) in the trial assessing IV zoledronate every three months (Chapman 2009). There were two new vertebral fractures in the control group (24 participants) compared to none in the 23 participants in the group receiving 70 mg weekly of oral alendronate (Papaioannou 2008). There were no new vertebral fractures reported for either group (10 participants in each) in the second trial assessing 70 mg of oral alendronate (Krasovsky 2010). There was one new vertebral fracture in the control group of seven participants compared to no fractures in the eight participants in the group receiving oral alendronate (5 mg/day for a bodyweight 25 kg or under; 10 mg/day for a bodyweight over 25 kg) (Bianchi 2013). Combining these data, there was no difference in the number of participants with new vertebral fractures in the treatment group compared to controls after 12 months of intervention (OR 0.22, 95% CI 0.02 to 2.09; I2 = 0; 5 trials, 142 participants; very low‐certainty evidence; Analysis 1.3).
At the 24‐month time point, data from two trials (n = 44) did not show any vertebral fractures in either treatment or control group (Chapman 2009; Haworth 2011) (Analysis 1.3). See Figure 6.

Forest plot of comparison between bisphosphonates versus control (without lung transplantation), Outcome 1b ii. Number of participants with vertebral fractures.
Secondary outcomes
1. BMD (% change)
a. Lumbar spine
Eight trials reported on this outcome (Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010; Papaioannou 2008). We have presented individual time points (Analysis 1.4) and summary end of trial data (Analysis 1.5). We then analysed by the different routes of administration.
Four trials (n = 101) reported data at the six‐month time point (Aris 2004; Boyle 2005; Chapman 2009; Haworth 2001). Results showed an increase in BMD measured at the lumbar spine in the treatment group with moderate statistical heterogeneity (mean difference (MD) 4.61, 95% CI 3.90 to 5.32; I2 = 39%; 4 trials, 101 participants; Analysis 1.4). In the Aris trial, lumbar spine BMD increased in participants receiving oral alendronate after six months of the intervention, while lumbar spine BMD decreased in control group participants at this time point; the relative change in BMD at the lumbar spine after six months was MD 5.50%, 95% CI 4.11 to 6.89; Aris 2004). The Boyle trial was stopped after only five participants were enroled (three in the treatment group); the mean (standard deviation (SD)) lumbar spine BMD increased by 4.7 (0.6)% six months after the single dose of IV zoledronate compared to no change in the two participants in the placebo group (Boyle 2005). In the Chapman trial, IV zoledronate was associated with a statistically significant positive effect on BMD at the lumbar spine after six months of treatment (MD 4.16, 95% CI 3.30 to 5.02; Chapman 2009). In the Haworth trial, after six months lumbar spine BMD had decreased in participants in the control group, while participants in the IV pamidronate group had gained BMD in this region; % change at six months (MD 5.80%, 95% CI 2.91 to 8.69; Haworth 2001).
The % change in BMD at the lumbar spine still increased at six months for both oral (Aris 2004) and IV bisphosphonates (Boyle 2005; Chapman 2009; Haworth 2001) when the different routes were analysed separately; oral bisphosphonates (MD 5.50, 95% CI 4.11 to 6.89; 1 trial, 48 participants; Analysis 1.4) and IV bisphosphonates (MD 4.29, 95% CI 3.47 to 5.12; I2 = 12%; 3 trials, 54 participants; Analysis 1.4).
Six trials (n = 171) reported data at the 12‐month time point (Aris 2004; Bianchi 2013; Chapman 2009; Haworth 2011; Krasovsky 2010; Papaioannou 2008). These combined data showed a significant increase in BMD in favour of bisphosphonates with zero statistical heterogeneity (MD 6.31, 95% CI 5.39 to 7.22; I2 = 0%; 6 trials, 171 participants; low‐certainty evidence; Analysis 1.4). In the Aris trial, after 12 months participants in the treatment group had increased lumbar spine BMD, but this was decreased in control group participants (MD 6.70, 95% CI 4.51 to 8.89; Aris 2004). Chapman reported that the intervention showed a positive effect on BMD at the lumbar spine after 12 months of treatment (MD 6.25, 95% CI 4.88 to 7.62; Chapman 2009). The remaining trials of oral bisphosphonates also showed an increase in BMD at the lumbar spine; for the oral risedronate trial (MD 5.50, 95% CI 0.61 to 10.39; Haworth 2011) and for the oral alendronate trials (MD 5.28, 95% CI 3.13 to 7.43; Papaioannou 2008), (MD 7.80, 95% CI 3.04 to 12.56; Krasovsky 2010) and (MD 7.20, 95% CI 4.64 to 9.76; Bianchi 2013).
When routes of administration were analysed separately, the % change in BMD still increased at 12 months for both oral bisphosphonates (MD 6.35, 95% CI 5.12 to 7.58; I2 = 0%; Aris 2004; Bianchi 2013; Haworth 2011; Krasovsky 2010; Papaioannou 2008) and IV bisphosphonates (MD 6.25, 95% CI 4.88 to 7.62; Chapman 2009).
Data for lumbar spine BMD were reported at 24 months by two trials (n = 43) and the overall result, too, favoured the treatment group although with moderate heterogeneity (MD 5.49, 95% CI 4.38 to 6.60; I2 = 40%; 2 trials, 43 participants; Analysis 1.4). Individually, only one trial, using IV zoledronic acid, showed a positive effect (MD 5.70, 95% CI 4.55 to 6.85; Chapman 2009) compared with the second trial of oral risedronate which did not (MD 3.00, 95% CI ‐0.95 to 6.95; Haworth 2011).
Pooled end‐of‐trial data from eight trials (n = 199) (Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010; Papaioannou 2008) shows positive effects on BMD at the lumbar spine with no statistical heterogeneity (MD 5.95, 95% CI 5.17 to 6.73; I2 = 0%; 8 trials, 199 participants; Analysis 1.5). Looking at the different routes of administration with the pooled end‐of‐trial data, there were positive effects for both oral bisphosphonates (MD 6.22, 95% CI 5.08 to 7.35; I2 = 16%; Aris 2004; Bianchi 2013; Haworth 2011; Krasovsky 2010; Papaioannou 2008) and IV bisphosphonates (MD 5.71, 95% CI 4.64 to 6.79; I2 = 0%; Boyle 2005; Chapman 2009; Haworth 2001).
b. Total hip or femur
Six trials reported on this outcome (Aris 2004; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010; Papaioannou 2008). We have presented individual time points (Analysis 1.6) and summary end‐of‐trial data (Analysis 1.7). We have also analysed the effects of the different routes of administration.
Data from three trials (n = 96) were combined at six months (Aris 2004; Chapman 2009; Haworth 2001); results favoured bisphosphonates for total hip or femur BMD, but with substantial heterogeneity (MD 3.58, 95% CI 2.75 to 4.40; I2 = 73%; 3 trials, 96 participants; Analysis 1.6). Chapman is responsible for the high level of statistical heterogeneity here; when removed from analysis the heterogeneity becomes zero. It is unclear the precise cause of this from a methodological perspective, however Chapman's high statistical weight in the analysis due to its comparatively narrow CIs and greatest MD is the cause of the statistical heterogeneity. Chapman is the only trial using IV zoledronate in this analysis, which may also be a contributing factor. Future versions of this review, with more included studies, aim to run subgroup analyses of the drugs used in order to clarify if this is a significant moderator of outcome. In the Aris trial, participants receiving oral alendronate showed increased total hip or femur BMD, but results were unchanged in the control group (MD 2.20, 95% CI 0.81 to 3.59; Aris 2004). Chapman reported that IV zoledronate was associated with a positive effect on BMD at the total hip or femur regions (MD 4.63, 95% CI 3.49 to 5.77; Chapman 2009). In the earlier Haworth trial, after the IV pamidronate intervention, participants in the control group had decreased total hip or femur BMD; participants in the treatment group had gained BMD in this region (MD 3.00, 95% CI 0.60 to 5.40; Haworth 2001).
At six months, when analysed by route of administration, both oral bisphosphonates (MD 2.20, 95% CI 0.81 to 3.59; Aris 2004) and IV bisphosphonates (MD 4.33, 95% CI 3.31 to 5.36; (Chapman 2009; Haworth 2001) had a positive effects on BMD at the total hip or femur regions, with moderate heterogeneity (I2 = 31%).
Data from five trials (n = 155) were combined at the 12‐month time point (Aris 2004; Chapman 2009; Haworth 2011; Krasovsky 2010; Papaioannou 2008); results showed a significant increase in total hip or femur BMD with low statistical heterogeneity (MD 4.41, 95% 3.44 to 5.37; I2 = 28%; 5 trials, 155 participants; low‐certainty evidence; Analysis 1.6). At 12 months, participants in the Aris trial receiving oral alendronate showed increased total hip or femur BMD, but this was decreased compared to baseline in the control group (MD 3.50, 95% CI 1.01 to 5.99; Aris 2004). Papaioannou showed an increase in BMD at the total hip or femoral neck (MD 3.44, 95% CI 1.72 to 5.16; Papaioannou 2008). Chapman reported a positive effect on BMD at the total hip or femur regions in the zoledronate group after 12 months of treatment (MD 5.71, 95% CI 4.25 to 7.17; Chapman 2009). Two trials, however, did not show an increase in BMD at this site at 12 months; the oral alendronate trial (MD 2.60, 95% CI ‐1.56 to 6.76; Krasovsky 2010) and the oral risedronate trial (MD 3.80, 95% CI ‐0.43 to 8.03; Haworth 2011).
At 12 months, when analysed by route of administration, both oral (MD 3.41, 95% CI 2.13 to 4.69; I2 = 0%; Aris 2004; Papaioannou 2008; Haworth 2011; Krasovsky 2010) and IV bisphosphonates (MD 5.71, 95% 4.25 to 7.17; Chapman 2009) showed positive effects on BMD.
At the 24‐month time point, the two trials (n = 42), Chapman using IV zoledronate (MD 6.73, 95% 5.51 to 7.95) and Haworth using oral risedronate (MD 4.00, 95% CI 0.01 to 7.99), favoured the intervention both individually and when combined (Chapman 2009; Haworth 2011). Combined data showed moderate heterogeneity (MD 6.49, 95% CI 5.32 to 7.66; I2 = 39%; Analysis 1.6).
Pooling end‐of‐trial results for all bisphosphonate trials (Aris 2004; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010; Papaioannou 2008), there were positive BMD effects at the total hip or femur but with substantial heterogeneity (MD 4.89, 95% CI 4.06 to 5.72; I2 = 69%; 6 trials, 178 participants; Analysis 1.7). Chapman is again the cause of the substantial heterogeneity, possibly for the reasons detailed above. When comparing routes of administration, both oral bisphosphonates (Aris 2004; Haworth 2011; Krasovsky 2010; Papaioannou 2008) and IV treatment (Chapman 2009; Haworth 2001) had positive BMD effects at the total hip or femur (MD 3.43, 95% 2.16 to 4.70; I2 = 0%) and (MD 5.96, 95% CI 4.87 to 7.05; I2 = 86%) respectively. The heterogeneity is explained by the relatively large gap in MD between the two IV trials, and the significant weight of Chapman in analysis due to its much narrower CIs. The trials also used different medications; Chapman used IV zoledronate, and Haworth used IV pamidronate.
c. Radius
Two trials reported data for distal radius (Chapman 2009; Haworth 2001) and one reported data for ultra distal radius (Haworth 2001). Both used IV bisphosphonates.
Combined data for distal radius at six months showed no difference between treatment and control with substantial heterogeneity (MD 0.02, 95% CI ‐0.73 to 0.78; I2 = 71%; 2 trials, 48 participants; Analysis 1.8). This was also true for individual trial results; Chapman reports no difference in distal radial BMD between the intervention and the control group at six months (MD 0.32, 95% CI ‐0.50 to 1.14; Analysis 1.8), while Haworth reports no difference in BMD as measured by single‐energy X‐ray absorptiometry (SXA) of the distal forearm (MD ‐1.70, 95% CI ‐3.66 to 0.26; Analysis 1.8). The substantial heterogeneity is explained by the reasons detailed above.
Only Chapman reported data at 12 and 24 months (Chapman 2009). At 12 months, distal radial BMD in the intervention group was not different from the control group (MD 0.32, 95% CI ‐0.30 to 0.94). However, at 24 months, the result favoured bisphosphonates (MD 1.50, 95% CI 0.41 to 2.59; Analysis 1.8).
When end‐of‐trial results were pooled for both trials (Chapman 2009; Haworth 2001), there was no difference in BMD at the distal forearm but with considerable heterogeneity (MD 0.74, 95% CI ‐0.21 to 1.70; I2 = 87%; 2 trials, 42 participants; Analysis 1.9).
In the Haworth trial, measurements of appendicular sites showed opposite trends (Haworth 2001). There was a decrease in BMD as measured by SXA of the ultra distal forearm in participants receiving pamidronate at six months (MD ‐2.70, 95% CI ‐5.59 to 0.19; Analysis 1.10).
d. Total body
No trial reported data for the change in BMD for the total body.
2. QoL
Eight trials did not report on QoL (Aris 2000; Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010). Only one trial of oral alendronate assessed mean changes in QoL over 12 months using the physical component score and mental component score of the Medical Outcomes Study 36‐item short form, version 2 (SF‐36v2) (Papaioannou 2008). There was no difference in the changes for the physical component score (MD 2.51, 95% CI ‐1.38 to 6.40; 1 study, 47 participants; low‐certainty evidence; Analysis 1.11), but the mental component score favoured control (MD ‐5.93, 95% CI ‐11.73 to ‐0.13; 1 study, 47 participants; low‐certainty evidence; Analysis 1.11).
3. Adverse events
Seven trials reported on adverse events (Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Papaioannou 2008).
We were able to present combined data in a meta‐analysis for bone pain (Analysis 1.12), fever (Analysis 1.13) and narrative information on GI adverse effects (for this outcome information was not available per participant for all trials, so has been presented narratively). If the required information from the trial investigators becomes available, we will perform a meta‐analysis for a future update of the review. We have initially analysed all routes of administration together and then presented separate analyses for oral or IV routes (moderate‐certainty evidence).
a. Bone pain
Combining results for all routes of administration and using end‐of‐trial data from seven trials (Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Papaioannou 2008), bisphosphonates were associated with a higher occurrence of bone pain with substantial heterogeneity (OR 8.49, 95% CI 3.20 to 22.56; I2 = 61%; 7 trials, 206 participants; Analysis 1.12). The substantial heterogeneity here is likely due to the different routes of administration and drugs used.
Investigating this further we split the trials by route of administration.
Three 12‐month trials of oral alendronate compared to placebo reported on this outcome (Aris 2004; Bianchi 2013; Papaioannou 2008). In the Aris trial, none of the participants in either the intervention or the control group experienced bone pain (Aris 2004). Bianchi stated that muscle or bone pain was reported in only one of the eight participants in the intervention group compared to two out of seven participants in the placebo group (Bianchi 2013). In this trial, a proportion of participants were taking systemic glucocorticoids in each group (30.8% and 30.2% for the alendronate and placebo groups respectively) (Bianchi 2013). The third trial oral alendronate also did not report bone pain in any participants; three of the participants in the treatment group (a similar proportion to the Bianchi trial) used oral corticosteroids with the mean yearly cumulative dose 49.32 mg (Papaioannou 2008).
In the 24‐month trial of oral risedronate, four participants withdrew completely due to bone pain (three in the first 12 months) and one participant discontinued the study medication due to bone pain (Haworth 2011). The trial further reported that bone pain was recorded 19 times by nine different risedronate participants in the first year after randomisation, while there were no episodes of bone pain in the placebo group (OR 43.59, 95% CI 2.27 to 837.56; Analysis 1.12); 14 of the 19 episodes (74%) occurred within the first 56 days after randomisation. Five events (26%) were classified as severe and led to the discontinuation of the trial medication. Of the other events, 10 were classified as moderate and four as mild. Only two events (11%) were considered to be unrelated to the trial medication. Bone pain usually started within 24 hours of the first dose of risedronate and lasted for approximately 72 hours (Haworth 2011).
Pooling results for bone pain from the four trials of oral bisphosphonates (Aris 2004; Bianchi 2013; Haworth 2011; Papaioannou 2008), the occurrence of bone pain was significantly higher in the intervention group (10 out of 72) compared to the placebo group (2 out of 74), but with considerable heterogeneity (OR 4.98, 95% CI 1.24 to 20.09; I2 = 83%; 4 trials, 143 participants; Analysis 1.12). The heterogeneity in this analysis comes from the fact that only two trials reported any adverse events, and they showed quite a difference in ORs; this could be attributed to the different medications used (Bianchi 2013; Haworth 2011).
Three trials reported on IV bisphosphonates (Boyle 2005; Chapman 2009; Haworth 2001). Boyle reported that three participants experienced dramatic musculoskeletal pain (characterised by severe chest and back pain), two requiring emergency room assessment with symptoms beginning six to eight hours after infusion and peaking at 12 to 18 hours (Boyle 2005). Although the most severe symptoms resolved within 48 to 72 hours, participants reported continued arthralgias for up to a week. It was presumed that these three participants were those in the treatment group (no reply was received to an attempt to contact the author) (Boyle 2005). Chapman reported that there was no difference between treatment and control groups with respect to musculoskeletal pain (four out of 10 in the zoledronate group, two out of 12 in the control group) (Chapman 2009) (OR 3.33, 95% CI 0.46 to 24.05; Analysis 1.12). Haworth reported that no participants in the control group experienced bone pain; but 11 out of 15 participants in the treatment group experienced moderate to severe pain following the first dose of medication (OR 94.56, 95% CI 4.65 to 1924.08). Nine participants reported severe bone pain and the pain was reported to be excruciating in seven participants rendering them bed bound and making sputum expectoration and physiotherapy difficult. None of the participants experiencing bone pain were taking corticosteroids, while three of the four participants without bone pain in the treatment group were taking this medication (Haworth 2001).
Pooling the results for IV bisphosphonates (Boyle 2005; Chapman 2009; Haworth 2001), including the trial in which participants received oral prednisone daily for three days on the morning of the first infusion (repeated with subsequent infusions if a reaction to the first infusion was thought likely) (Chapman 2009), the occurrence of bone pain was higher in participants in the treatment groups (18 out of 28) compared to control groups (2 out of 32) with moderate heterogeneity (OR 14.17, 95% CI 3.64 to 55.17; I2 = 47%; 3 trials, 60 participants; Analysis 1.12).
b. Fever
Combining results for all routes of administration and using end‐of‐trial data from five trials (Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001), bisphosphonates were associated with higher occurrence of fever with no heterogeneity (OR 12.64, 95% CI 2.31 to 69.11; I2 = 0%; 5 trials, 118 participants; Analysis 1.13).
In the two 12‐month trials of oral alendronate reporting this outcome, none of the participants in either the intervention or the control group experienced fever (Aris 2004; Bianchi 2013). Neither of the remaining trials of oral bisphosphonates stated that fever was one of the adverse events that were reported (Haworth 2011; Papaioannou 2008).
Combined data from the trials of IV bisphosphonates (Boyle 2005; Chapman 2009; Haworth 2001) show participants in the treatment groups were more likely to experience fever with no heterogeneity (OR 12.64, 95% CI 2.31 to 69.11; I2 = 0%; 3 trials, 55 participants; Analysis 1.13). Boyle reported that one participant experienced a fever of 104° F lasting for several hours and a rise in tumour necrosis factor‐α (OR 3.00, 95% CI 0.08 to 115.34; Boyle 2005). In the Chapman trial the number of participants experiencing fever was higher in the treatment group (eight out of 10 in the zoledronate group, one out of 12 in the control group) (OR 44.00, 95% CI 3.38 to 573.41; Chapman 2009). Haworth reported that two of the nine participants in the treatment group had febrile reactions (OR 6.74, 95% CI 0.29 to 154.26; Haworth 2001).
c. GI adverse effects
GI adverse effects were only assessed in the trials comparing oral bisphosphonates to placebo (Aris 2004; Bianchi 2013; Haworth 2011; Papaioannou 2008).
Three trials of oral alendronate reported at 12 months (Aris 2004; Bianchi 2013; Papaioannou 2008). In the Aris trial, three cases of diarrhoea were reported; one participant was receiving alendronate and two were receiving placebo. This was accompanied by abdominal cramping and loss of appetite. These participants continued to experience diarrhoea after discontinuing the trial medication. One participant reported dysphagia, but it was not clear which group they were in (Aris 2004). Bianchi reported no adverse effects in either group (Bianchi 2013). Papaioannou's trial of oral alendronate reported 10 GI‐related adverse events in the treatment group (three events of nausea or vomiting or both and one event of each of reflux, difficulty swallowing, oesophagitis, constipation, gastrointestinal upset, intestinal obstruction and stomach pain or burn) and seven gastrointestinal‐related adverse events in the control group (four events of nausea or vomiting or both and one event of each of constipation, intestinal obstruction and stomach pain or burn) (Papaioannou 2008).
GI symptoms were also reported in the 24‐month oral risedronate trial (26 in the treatment group and 16 in the placebo group). These events corresponded to the same number of participants in each study group (nine in risedronate, nine in placebo) (Haworth 2011).
d. Other adverse effects
Two 12‐month trials of oral bisphosphonates reported information on other adverse events. Bianchi stated that no participants reported headaches in the oral alendronate trial (Bianchi 2013). Papaionnou reported serious adverse events in the alendronate group as an exacerbation of CF (n = 3), bronchial superinfection (n = 1), hypoglycaemic seizure (n = 1), GI obstruction (n = 1) and intestinal obstruction (n = 1). Serious adverse events reported for the control group included an exacerbation of CF (n = 3), with two of these participants experiencing additional gastrointestinal complaints (Papaioannou 2008). In the 24‐month trial of oral risedronate, two participants discontinued the study medication in the first 12 months due to muscle aches or generalised pain. Within two years of randomisation 346 adverse events were recorded; most events were classed as respiratory exacerbations (n = 230) and it was stated that there was no difference in incidence between the two groups (Haworth 2011).
In regard to the trials of IV bisphosphonates, none of the trials assessed calcium levels post‐infusion (Boyle 2005; Chapman 2009; Haworth 2001). However, Chapman reported that musculoskeletal side effects were experienced following 27 of 63 zoledronate infusions, but after only four of 73 placebo infusions. This was despite administering prednisolone to all participants with at least the first infusion, and these side effects were more common after the first than the subsequent infusions. In six participants, the reactions were described as severe, in two cases resulting in withdrawal (Chapman 2009). In the earlier Haworth trial, it was reported that one participant developed phlebitis around the infusion site (Haworth 2001).
4. Withdrawals
We have presented data for total withdrawals (Analysis 1.15) and withdrawals due to adverse events (Analysis 1.14). We then examine withdrawals when separated by route of administration.
Six trials provide information on withdrawals; one trial states that there were no withdrawals (Bianchi 2013) and five trials describe withdrawals (Aris 2004; Chapman 2009; Haworth 2001; Haworth 2011; Papaioannou 2008).
Six months
At six months two trials reported no difference in total withdrawals (OR 1.77, 95% CI 0.27 to 11.60; I2 = 0%; 2 trials, 53 participants; Analysis 1.15) with no heterogeneity (Haworth 2001; Chapman 2009). Only Chapman reported one withdrawal due to adverse events, with no difference between treatment and control groups (OR 3.95, 95% CI 0.14 to 108.09; 2 trials, 53 participants; Analysis 1.14). The Aris trial of oral alendronate reported five of the 53 participants who started the protocol dropped out in the first six months, however it was unclear to which group these participants were allocated, so we did not include these data in the analysis at six months (Aris 2004).
In Haworth 2001, one participant from each group died, while a second participant in the pamidronate group withdrew in order to receive a double lung transplant. No participant withdrew due to other adverse events (Haworth 2001).
In Chapman 2009, there were two withdrawals at six months. One participant in the control group was lost to follow‐up, and one participant withdrew after only one infusion due to adverse events (Chapman 2009).
The Aris oral alendronate trial reported five of the 53 participants who started the protocol dropped out in the first six months; however, it was unclear to which group these participants were allocated, so we did not include these data in the analysis at six months. The reasons included pregnancy (n = 1, experienced a spontaneous abortion in her first trimester), dysphagia (n = 1, experienced difficulty swallowing the first tablet and had similar difficulties swallowing other medications), and diarrhoea (n = 3). For the first two participants, it was unclear which group they were allocated to. One of the participants experiencing diarrhoea was receiving alendronate and two were receiving placebo. No participants withdrew due to GI reflux symptoms.
12 months
At 12 months, five trials reported no difference in total withdrawals with no heterogeneity (OR 1.02, 95% CI 0.45 to 2.28; I2 = 0%; 5 trials, 177 participants; Analysis 1.15) (Aris 2004; Bianchi 2013; Chapman 2009; Haworth 2011; Papaioannou 2008). Regarding withdrawals due to adverse events; there were more withdrawals due to adverse events in the treatment group compared to the control group with moderate heterogeneity (OR 4.07, 95% CI 1.11 to 14.90; I2 = 51%; 5 trials, 177 participants; Analysis 1.14) (Aris 2004; Bianchi 2013; Chapman 2009; Haworth 2011; Papaioannou 2008). The moderate heterogeneity at 12 months is due to the Papaioannou trial; when removed from the analysis, heterogeneity is zero. This is due to its much lower OR and narrow CIs with a large number of participants, lending it a much higher weight in the analysis (Papaioannou 2008). It is unclear from a methodology standpoint why its results are so different; as multiple studies used oral alendronate in similar populations.
In Aris 2004, of the 48 participants who completed DXA assessment at six months, four out of 24 in each group withdrew before the DXA assessment at 12 months. In the treatment group, one withdrew due to lung transplantation, two moved away and one withdrew due to non‐compliance; in the control group two withdrew due to lung transplantation, one died and one moved away (Aris 2004).
In the 2008 Papaioannou trial, four of 27 participants in the treatment group withdrew; one due to an adverse event, one withdrew consent and two due to non‐compliance. In the placebo group, five out of 29 participants withdrew; two due to non‐compliance, two due to an adverse event and one was lost to follow‐up (Papaioannou 2008).
In Chapman 2009, six of the 22 participants withdrew by 12 months. In the treatment group, reaction at the infusion site led to two withdrawals. One of these participants required admission to hospital with severe pain and fever restricting movement, with onset 12 hours after the first infusion; this resolved after four days, but led to subsequent withdrawal from the trial. The second withdrawal experienced fever, rigor, bone pain and headache 24 hours after the first infusion with resolution in five days. Similar effects were experienced after the second infusion followed by withdrawal from the trial. The withdrawal that was unrelated to adverse events in the treatment group was due to loss to follow‐up. In the control group, one participant was lost to follow‐up, one participant decreased their BMD to withdrawal threshold, and one participant had poor compliance to protocol as well as BMD decreasing to the withdrawal threshold (Chapman 2009).
In the 2011 Haworth trial, six of the 36 participants withdrew by 12 months (Haworth 2011). One participant in the placebo group withdrew consent immediately after randomisation and before taking the medication; therefore, only 18 participants were commenced on placebo. By 12 months, two participants in the placebo group withdrew consent and one participant had died. Three out of 17 participants in the treatment group withdrew completely due to bone pain and three participants discontinued the trial medication (one citing bone pain and the other two participants citing muscle aches or generalised pain), but remained in the trial for follow‐up (Haworth 2011).
Bianchi 2013 reported no withdrawals.
24 months
Two trials reported no difference in total withdrawals with low heterogeneity (OR 0.95, 95% CI 0.34 to 2.69; I2 = 21%; 2 trials, 58 participants; Analysis 1.15) (Chapman 2009; Haworth 2011). There was however, a difference in withdrawals due to adverse events between the control and intervention groups with no heterogeneity (OR 16.34, 95% CI 1.98 to 134.89; I2 = 0%; 2 trials, 58 participants; Analysis 1.14) (Chapman 2009; Haworth 2011).
In the Chapman trial, nine of the 22 participants withdrew by 24 months (Chapman 2009). There were no further withdrawals from the treatment group between 12 and 24 months. Three additional participants withdrew between 12 and 24 months; two participants reached the BMD threshold for withdrawal, and one participant was withdrawn due to poor compliance (Chapman 2009).
In the 2011 Haworth trial, by 24 months 15 of the 36 participants had withdrawn (Haworth 2011). Three participants in the placebo group had withdrawn consent and four participants had died. Between 12 and 24 months one further participant withdrew from the intervention group (citing bone pain), leaving 12 participants (with nine still taking the trial drug) in this group at 24 months (Haworth 2011).
Withdrawals by route of administration
There were no trials of oral bisphosphonates with withdrawal data at six months. Combined data of four trials using oral bisphosphonates at 12 months showed no difference in total withdrawals with no heterogeneity (OR 0.96, 95% CI 0.39 to 2.36; I2 = 0%; 4 trials, 150 participants; Analysis 1.15) and no difference in withdrawals between groups due to adverse events, but with high statistical heterogeneity (OR 3.54, 95% CI 0.85 to 14.77; I2 = 74%; 4 trials, 150 participants; Analysis 1.14) (Aris 2004; Bianchi 2013; Haworth 2011; Papaioannou 2008). At 24 months there was just one trial of oral bisphosphonates, which showed no difference between groups for total withdrawals (OR 1.52, 95% CI 0.40 to 5.78; 1 trial, 36 participants; Analysis 1.15), but did show a difference in withdrawals due to adverse events (OR 27.86, 95% CI 1.44 to 537.26; 1 trial, 36 participants; Analysis 1.14) (Haworth 2011).
At six months there were two trials using IV bisphosphonates. As reported above there was no significant difference in the number of total withdrawals (OR 1.77, 95% CI 0.27 to 11.60) or withdrawals due to adverse events (OR 3.95, 95% CI 0.14 to 108.09), both with zero heterogeneity (Chapman 2009; Haworth 2001). At 12 months and 24 months only one trial was using IV bisphosphonates (Chapman 2009); at 12 months there was no difference between treatment group and control with respect to total withdrawals (OR 1.25, 95% CI 0.14 to 10.94) or withdrawals due to adverse events (OR 7.35, 95% CI 0.31 to 173.13). The same was true at 24 months for total withdrawals (OR 0.43, 95% CI 0.07 to 2.50) and withdrawals due to adverse events (OR 7.35, 95% CI 0.31 to 173.13) (Chapman 2009).
5. Survival
Four of the trials reported there were no deaths in either the treatment or control group (Bianchi 2013; Boyle 2005; Chapman 2009; Papaioannou 2008).
At six months, Haworth reported that IV pamidronate treatment did not significantly affect survival compared with the control group (14 out of 15 survivors in the pamidronate group, 15 out of 16 in the control group) (OR 0.93, 95% CI 0.05 to 16.39; 1 trial, 31 participants; Analysis 1.16) (Haworth 2001).
Of the 48 participants in the oral alendronate trial who completed DXA assessment at six months beyond baseline, one participant out of 24 in the control group died during the latter six months of the trial compared to none in the treatment group (Aris 2004). When the data were analysed, there was no difference between groups (OR 3.13, 95% CI 0.12 to 80.68; Analysis 1.16). Combining the survival data with the 12‐month outcome data of the oral risedronate trial (Haworth 2011), there was no difference between groups with no heterogeneity (OR 2.98, 95% CI 0.30 to 29.84; I2 = 0%; Analysis 1.16).
At 24 months, Haworth reported that oral risedronate treatment did not affect survival compared with the control group (16 out of 17 survivors in the risedronate group, 15 out of 19 in the control group) (OR 4.27, 95% CI 0.43 to 42.63) (Haworth 2011).
Bisphosphonates compared with control for osteoporosis in children with CF who have not had a lung transplant
Only one 12‐month trial of oral alendronate (n = 113) reported on this comparison (Bianchi 2013).
Primary outcome
1. Fractures
a. Number of participants with any fracture
There were five fractures in the 56 control participants compared to only one in the alendronate group, but when analysed the data showed no difference between groups (OR 0.18, 95% CI 0.02 to 1.61; Analysis 2.1).
b. Number of participants with fractures by site
i. Vertebral
Only one participant had vertebral fractures in the intervention group compared to three in the control group, but analysis of the data did not show a difference between groups (OR 0.32, 95% CI 0.03 to 3.13; 1 study, 113 participants; low‐certainty evidence; Analysis 2.3).
ii. Non‐vertebral
There were no non‐vertebral fractures in the intervention group compared to two non‐vertebral fractures in the control group; however, again the data did not show a difference between groups (OR 0.19, 95% CI 0.01 to 4.04; 1 study, 113 participants; low‐certainty evidence; Analysis 2.2). The trial did not specifically report hip or wrist fractures.
Secondary outcomes
1. BMD (% change)
a. Lumbar spine
At the end of 12 months, the % change in BMD was higher in the treatment group than in the control group at the lumbar spine (MD 14.50, 95% CI 12.91 to 16.09; 1 study, 113 participants; low‐certainty evidence; Analysis 2.4).
2. QoL
The trial did not report any QoL measurements.
3. Adverse events
a. Bone pain
Bianchi reported this outcome as bone or muscle pain (Bianchi 2013). There was no difference in bone or muscle pain experienced between the groups (one participant in the treatment group compared to none in the control group) (MD 3.00, 95% CI 0.12 to 75.22; 1 study, 113 participants; low‐certainty evidence; Analysis 2.5).
b. Fever
There was no difference in fever experienced between the groups (one participant in the treatment group compared to none in the control group) (MD 3.00, 95% CI 0.12 to 75.22; 1 study, 113 participants; low‐certainty evidence; Analysis 2.6).
c. GI adverse events
There was no difference in GI adverse events reported by the groups (five participants in the treatment group compared to seven in the control group) (OR 0.67, 95% CI 0.20 to 2.26; 1 study, 113 participants; low‐certainty evidence; Analysis 2.7).
d. Headache
There was no difference in headache reported by the groups (one participant in each group) (OR 0.98, 95% CI 0.06 to 16.10; Analysis 2.8).
e. Any adverse events
Eight participants in each reported any of the above adverse events, hence no difference between the group (OR 0.98, 95% CI 0.34 to 2.82; Analysis 2.9).
4. Withdrawals
There were no withdrawals in this trial.
5. Survival
There were no deaths reported during this trial.
Bisphosphonates versus control for osteoporosis in adults with CF who have had a lung transplant
Only one trial of IV pamidronate (n = 34) reported on this comparison (Aris 2000). The trial only reported at 24 months and we have not generated any GRADE judgements as we had specified the outcomes would be graded at the 12‐month time point.
Primary outcome
1. Fractures
a. Number of participants with any fracture
Combining the vertebral and non‐vertebral results, there was no difference in the total number of fractures (OR 0.94, 95% CI 0.24 to 3.77; Analysis 3.1).
b. Number of participants with fractures by site
i. Vertebral
There was no difference in the number of participants with new vertebral fractures in the bisphosphonate group (three out of 16 participants) versus the control group (one out of 18 participants) (OR 3.92, 95% CI 0.36 to 42.20; Analysis 3.3).
ii. Non‐vertebral
There was no difference in the number of participants with new non‐vertebral fractures in the treated (three out of 16 participants) versus the control group (six out of 18 participants) (OR 0.46, 95% CI 0.09 to 2.27; Analysis 3.2). The trial did not specifically report hip or wrist fractures.
Secondary outcomes
1. BMD (% change)
a. Lumbar spine
At the end of two years, the % change in BMD was higher in the treatment group than in the control group at the lumbar spine (MD 6.20, 95% CI 4.28 to 8.12; Analysis 3.4).
b. Total hip or femur
Likewise, at the end of two years, the % change in BMD was higher in the treatment group than in the control group at the femur (MD 7.90, 95% CI 5.78 to 10.02; Analysis 3.5).
2. QoL
The trial did not report any measure of QoL.
3. Adverse events
None of the 34 participants, all of whom were receiving corticosteroids, experienced any bone pain (Analysis 3.6). Participants were assessed at 24 hours post‐infusion for cellulitis, thrombophlebitis, or fever; but no cases were detected. Investigators analysed serum calcium, phosphorus, and magnesium and a complete blood count at 48 hours post‐infusion and reported that there were no significant differences compared with pre‐infusion data, with no episodes of hypocalcaemia and three episodes of mild hypervitaminosis D that resolved spontaneously. The trial in post‐transplant participants also reported that there was no difference in the degree of immunosuppression between the treatment and control groups (Aris 2000).
4. Withdrawals
There were no withdrawals other than those due to death in either treatment group (Analysis 3.7; Analysis 3.8).
5. Survival
Three participants died before the first BMD data could be collected at six months; these participants were excluded from further analysis and thus cannot be included as data in this review. The authors stated that the exclusion of these three participants did not significantly affect the subsequent analysis (Aris 2000). No other participants died during the course of the trial (Analysis 3.9).
Sensitivity analysis
a. Differences in the medications used in the intervention and comparison groups
We have reported on differences between oral and IV administration in the sections above; there were not enough data to perform a meaningful sensitivity analysis by further breaking down into individual medications used.
b. Analysis using random‐effects model
Adults who have not received a lung transplant
This section assesses for any difference in statistical significance using the random‐effects model in only those analyses where statistical heterogeneity measured using the I2 statistic was greater than 30%. Other analyses with lower statistical heterogeneity were not assessed using the random‐effects model.
Using the random‐effects model, the increase in BMD at the lumbar spine was still statistically significant at the six‐month time point (MD 4.81, 95% CI 3.75 to 5.88; I2 = 39%; 4 trials, 101 participants; Analysis 1.4), and the 24‐month time point (MD 5.04, 95% CI 2.76 to 7.31; I2 = 40%; 2 trials, 43 participants; Analysis 1.4).
The increase in BMD at the total hip or femur were also still statistically significant using the random‐effects model at the six‐month time point (MD 3.35, 95% CI 1.63 to 5.07; I2 = 73%; 3 trials, 96 participants; Analysis 1.6), the 24‐month time point (MD 6.05, 95% CI 3.74 to 8.36; I2 = 39%; 2 trials, 42 participants; Analysis 1.6), end of trial (MD 4.12, 95% CI 2.41 to 5.83; I2 = 69%; 6 trials, 178 participants; Analysis 1.7), and end of trial when looking at IV route of administration (MD 5.01, 95% CI 1.37 to 8.66; I2 = 86%; 2 trials, 47 participants; Analysis 1.7).
There remained no difference in BMD at the radius at six months (MD ‐0.49, 95% CI ‐2.42 to 1.45; I2 = 71%; 2 trials, 47 participants; Analysis 1.8) or end of trial (MD 0.01, 95% CI ‐3.12 to 3.14; I2 = 87%; 2 trials, 42 participants; Analysis 1.9).
Using the random‐effects model to analyse data for bone pain, participants in the intervention group were still more likely to experience bone pain when combining routes of administration (OR 9.09, 95% CI 1.17 to 70.57; I2 = 61%; 7 trials, 206 participants; Analysis 1.12) and when using IV bisphosphonates (OR 16.08, 95% CI 1.58 to 164.00; I2 = 47%; 3 trials, 60 participants; Analysis 1.12). Looking at oral bisphosphonates however, using a random‐effects model did not show a difference between groups (OR 3.78, 95% CI 0.03 to 460.84; I2 = 83%; 4 trials, 146 participants; Analysis 1.12), in contrast to analysis using the fixed‐effect model which showed that the intervention group were more likely to experience bone pain (OR 4.98, 95% CI 1.24 to 20.09; I2 = 83%; 4 trials, 146 participants; Analysis 1.12).
At 12 months, there was no difference in withdrawals due to adverse effects using the random‐effects model (OR 3.81, 95% CI 0.36 to 39.77; I2 = 61%; 5 trials, 177 participants; Analysis 1.14), whereas there was a difference using the fixed‐effect model (OR 4.07, 95% CI 1.11 to 14.90; I2 = 61%; 5 trials, 177 participants; Analysis 1.14). There remained no difference in withdrawals due to adverse events at 12 months when using a at the oral route of administration (OR 3.09, 95% CI 0.07 to 131.40; I2 = 74%; 4 trials, 150 participants; Analysis 1.14).
Adults who have received a lung transplant and non‐transplanted children
There was only one study including adults with lung transplants, and one study including children. As such, different effect models cannot be applied.
c. Analysis by 'treatment received'
Due to the lack of data, this was not possible.
d. Analysis by 'intention‐to‐treat'
Due to the lack of data, this was not possible.
Discussion
Summary of main results
We included a total of nine trials in the review. Eight trials investigated the effect of bisphosphonates (both oral and intravenous (IV) routes) in participants with cystic fibrosis (CF) who had not undergone lung transplantation; seven were in adults (Aris 2004; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010; Papaioannou 2008) and one was in adults and children (Bianchi 2013). We analysed adults (n = 238) and children (n = 113) separately. One trial assessed IV bisphosphonates in adults with CF who had undergone lung transplantation (Aris 2000). There was clinical heterogeneity between trials and not all trials reported all outcomes. For all comparisons, the lack of statistical differences in the rate of fractures, gastrointestinal (GI) adverse effects, withdrawals or survival may relate to the small numbers of participants involved and the short duration of the trials.
Bisphosphonates compared to control in adults with CF who have not had a lung transplant
Three trials assessed IV bisphosphonates (one assessed pamidronate and two assessed zoledronate) and five trials assessed oral bisphosphonates (one assessed risedronate and four assessed alendronate). Bisphosphonates were compared to either placebo or calcium (with or without additional vitamin D). There was very low‐certainty evidence which showed no effect of treatment on fractures (total, vertebral or non‐vertebral) in adults without lung transplantation (Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Krasovsky 2010; Papaioannou 2008).
Oral and IV bisphosphonates may increase bone mineral density (BMD) in adults with CF in trials of six, 12, and 24 months in some but not all regions (low certainty‐evidence). Oral bisphosphonates (alendronate and risedronate) were associated with increased BMD at the lumbar spine and hip or femur regions in adults with CF who had not undergone lung transplantation in the meta‐analysis from four studies (Aris 2004; Haworth 2011; Krasovsky 2010; Papaioannou 2008). Three trials assessing different IV bisphosphonate regimens (agent, duration and frequency) in this population group also showed improved lumbar spine BMD (Boyle 2005; Chapman 2009; Haworth 2001). Both IV bisphosphonate trials measuring hip or femur BMD showed positive effects on this outcome (Chapman 2009; Haworth 2001). The two trials that assessed radial BMD had conflicting results; it was significantly improved in the 24‐month zoledronate trial (Chapman 2009), but not in the pamidronate trial with six‐months follow‐up (Haworth 2001).
Only one trial assessed quality of life (QoL), with no difference in the effect of intervention on the physical component of the scoring system, but favouring the control group for the mental component of the score (Papaioannou 2008; low‐certainty evidence).
Regarding adverse events, moderate‐certainty evidence indicated that bone pain was probably associated with bisphosphonate therapy (all routes of administration) when compared to control (Aris 2004; Bianchi 2013; Boyle 2005; Chapman 2009; Haworth 2001; Haworth 2011; Papaioannou 2008). Bone pain was reported in two of the four trials of oral bisphosphonates (Bianchi 2013; Haworth 2011); however, it is unclear whether oral bisphosphonates were truly associated with increased bone pain as there were differences in statistical significance when using a fixed‐effect versus a random‐effects model in the analysis. Conversely, IV bisphosphonates were associated with bone pain (Boyle 2005; Chapman 2009; Haworth 2001) and severe bone pain and flu‐like symptoms were common with IV agents, especially in participants not taking glucocorticoids. Participants who did not receive corticosteroids during the clinical trial of IV pamidronate were more likely to experience bone pain (Haworth 2001). The observed relationship between the regular use of glucocorticoid therapy and lack of bone pain may be explained by evidence that corticosteroids suppress the release of tumour necrosis factor‐α (Steer 1997), an inflammatory cytokine known to increase bone resorption. Haworth suggests that bone pain may be avoided by prescribing a short course of oral corticosteroids before and at the time of pamidronate infusion (Haworth 2001). Zoledronate, a more potent bisphosphonate than pamidronate was associated with severe musculoskeletal pain resulting in discontinuation of one trial early in enrolment (Boyle 2005). In a subsequent trial of IV zoledronate, participants were prescribed daily prednisolone for three days commencing on the day of the first infusion (and repeated if thought necessary with subsequent infusions) (Chapman 2009). Musculoskeletal pain was not significantly increased in the treatment group; however, fever and other flu‐like effects were more commonly reported, severe in some participants, although the majority continued treatment. The authors proposed that a longer period of treatment with corticosteroids, including pre‐treatment dosing may diminish such adverse effects (Chapman 2009). A consensus statement has recommended pre‐treatment with oral corticosteroids for three to five days prior to bisphosphonate infusion, but this has not been studied in a randomised controlled trial (RCT) (Aris 2005).
The trials of oral bisphosphonates reported gastro‐oesophageal symptoms, but there were no differences between treatment and control groups (Aris 2004; Haworth 2011; Papaioannou 2008). Fever was not reported in association with oral bisphosphonates (Aris 2004).
There was no difference in withdrawals due to adverse events at six months when comparing bisphosphonate and control groups. However, there were more withdrawals from the bisphosphonates groups due to adverse events than in those in the control groups at both 12 months (Aris 2004; Bianchi 2013; Chapman 2009; Haworth 2011; Papaioannou 2008) and 24 months (Chapman 2009; Haworth 2011). When all withdrawals (for any reason) were considered, there was no difference between groups at any time point.
There was no effect on survival. Four trials reported there were no deaths in either the treatment or control group (Bianchi 2013; Boyle 2005; Chapman 2009; Papaioannou 2008). At six months, one trial reported one death in each group (Haworth 2001) and a second trial reported a single death in the control group only (Aris 2004).
Bisphosphonates compared to control in children with CF who have not had a lung transplant
The single trial in 113 children compared oral alendronate to placebo (Bianchi 2013). There was no effect of treatment on fractures (total, vertebral or non‐vertebral) in children without lung transplantation (low‐certainty evidence). At 12 months bisphosphonates may increase the % change in BMD at the lumbar spine (low‐certainty evidence), but this outcome was not measured at other sites (Bianchi 2013). This trial did not report any measure of QoL. Bisphosphonates may not make any difference to measures of bone or muscle pain, fever or GI adverse events (low‐certainty evidence). There were no deaths of any children in this trial.
Bisphosphonates compared to control in people with cystic fibrosis who have had a lung transplant
One trial of 34 adults who had undergone lung transplantation compared intravenous pamidronate to no bisphosphonate treatment. It did not report at 12 months and we report the 24‐month data (not assessed by GRADE). There was no effect of treatment on fractures (total, vertebral or non‐vertebral) in people with lung transplantation (Aris 2000). Lumbar spine and hip BMD showed greater improvements with IV pamidronate than with no bisphosphonate treatment (Aris 2000). This trial did not report any measure of QoL. None of the participants in this trial, all of whom were receiving corticosteroids, experienced any bone pain and there were no differences in any of the other adverse events measured and reported (Aris 2000). Three participants died before the first BMD data could be collected at six months and these participants are not included as data in this review; no other participants died during the course of the trial.
Sensitivity analysis
Analyses were assessed for any difference in statistical significance using the random‐effects model where statistical heterogeneity (I2) was greater than 30%. There were only two analyses which demonstrated differences using different statistical models. There was no difference in bone pain between the treatment and control groups in adults without lung transplant when looking at oral route of administration using the random‐effects model, whereas with the fixed‐effect model there was a significant difference (Aris 2004; Bianchi 2013; Haworth 2011; Papaioannou 2008). At 12 months, looking at total withdrawals due to adverse effects in adults without lung transplant, there was no difference using the random‐effects models, compared to a significant difference using the fixed‐effect model (Aris 2004; Bianchi 2013; Chapman 2009; Haworth 2011; Papaioannou 2008). The difference in outcomes between models at these two points mean the data here should be interpreted with caution. All other analyses with heterogeneity greater than 30% had no change in significance between models, which indicates the data are robust and supports the outcomes and conclusions drawn.
Overall completeness and applicability of evidence
There was significant clinical heterogeneity between the trials, but in the majority there was only low statistical heterogeneity.
There were potentially missing outcome data in several of the trials. In the 2000 Aris trial, three participants died over the course of the trial, but investigators did not report which group they belonged to (Aris 2000); it was unclear in the Chapman trial which specific participants had BMD measurements available at each time point (Chapman 2009); Krasovsky did not specify if there were withdrawals from the trial (Krasovsky 2010); in the 2004 Aris trial, not all withdrawals were explained, and only 75% of participants provided data for analysis at the end of one year (Aris 2004); in the Boyle trial 60% of participants dropped out before completion, and it was not specified to which group they belonged (Boyle 2005). While these missing data may have slightly altered the outcomes or quality of individual trials, the authors do not believe the missing data are sufficiently significant to meaningfully alter the results of the meta‐analyses performed in this review.
These trials provide valuable data on three different populations: adults with CF who have received a transplant, adults with CF who have not, and children with CF who have not. Although the inclusion criteria, duration of follow‐up and the magnitude of effect were different for the trials, similar trends for BMD effect were seen, suggesting that the beneficial effects of oral and IV bisphosphonates might be generalisable to a fairly broad population of people living with CF.
Certainty of the evidence
The certainty of evidence provided in this review ranges from moderate to very low (summary of findings Table 1; summary of findings Table 2). The main issues affecting the certainty of the evidence were the process of randomisation, allocation concealment, lack of blinding, level of heterogeneity and sample size. We did not use GRADE to assess the certainty of the evidence in the single trial of adults who had undergone lung transplantation as the trial did not report at 12 months, which was the time point we had specified in our methods; however we still present the 24‐month data in the third summary of findings table (summary of findings Table 3).
The certainty of the evidence for the primary outcome, number of fractures (both vertebral and non‐vertebral) was judged as very low for adults without lung transplant (summary of findings Table 1). Therefore, the true effect of bisphosphonate use on fracture incidence in people with CF is likely to differ substantially from our result. The certainty of evidence for fracture rate in children without lung transplant was judged as low. The certainty of the evidence for secondary outcomes in both adults and children without lung transplant was judged as low across all domains, except bone pain in adults, which was judged as moderate (summary of findings Table 1; summary of findings Table 2). Therefore, the conclusions drawn for secondary outcomes from this analysis may differ from the true effects, apart from the effect of bisphosphonates on bone pain in adults, which is likely close to the true effect.
All trials stated that allocation was randomised and the risk of bias due to generation of sequence was judged as unclear (Aris 2000; Aris 2004; Boyle 2005; Chapman 2009; Haworth 2001; Krasovsky 2010) or low (Bianchi 2013; Haworth 2011; Papaioannou 2008). Concealment of allocation of sequence was judged as low (Bianchi 2013; Haworth 2011; Papaioannou 2008) or unclear (Aris 2000; Aris 2004; Boyle 2005; Chapman 2009; Haworth 2001; Krasovsky 2010). If allocation is not appropriately randomised or concealed, there is a risk of clinicians consciously or unconsciously selecting participants for the different groups, which may affect results.
The risk of bias in the trials due to blinding was judged as high (Aris 2000; Haworth 2001; Krasovsky 2010), unclear (Aris 2004; Boyle 2005; Chapman 2009) or low (Bianchi 2013; Haworth 2011; Papaioannou 2008). When participants are aware of the treatment they are receiving, they may be more or less likely to report adverse events. The judgement of individuals who collect and interpret participant data may be affected when the assessor is aware of the treatment a participant is receiving. Lack of blinding may result in biased results.
The bias due to incomplete data (attrition) was judged as low (Bianchi 2013; Haworth 2001; Haworth 2011; Papaioannou 2008), unclear (Aris 2000; Chapman 2009, Krasovsky 2010), or high (Aris 2004; Boyle 2005). Incomplete data can reduce statistical power or misrepresent true outcomes; however in this case we do not believe the addition of any missing data would meaningfully alter the results of this review.
Bias due to selective reporting was judged as low (Aris 2004; Bianchi 2013; Chapman 2009; Haworth 2011; Papaioannou 2008), unclear (Boyle 2005; Haworth 2001; Krasovsky 2010) or high (Aris 2000). Selective reporting can distort the results of trials and falsely represent outcomes. However, the only evidence of selective reporting was regarding serum and urine biochemical measurements (Aris 2000), which were not outcomes assessed by this review; it may however bring the integrity of this trial's data into question.
There were other potential sources of bias in four trials (Aris 2004; Bianchi 2013; Boyle 2005; Haworth 2001). Three were stopped early (Aris 2004; Boyle 2005; Haworth 2001); the data from these trials may have shown more pronounced effects if they reached their planned conclusion and changed the outcome of this review's analysis. The Bianchi trial only included participants in their intervention who did not have an increase in bone mineral apparent density by 5% or more after 12 months in the observational phase (Bianchi 2013). If included, the anti‐resorptive intervention may have shown an even greater positive effect.
Potential biases in the review process
The review authors adhered to the Cochrane recommended search and review methods. As such the authors believe they have captured all relevant data for this review at the time searches were made.
This review found no significant reduction in fracture incidence in the intervention groups compared against controls. It is likely that there was not enough power to detect a treatment effect in the relatively small number of participants and short follow‐up times in included trials. This review sought to examine the effects of bisphosphonate in people with CF with osteoporosis over a number of time points. Unfortunately, there were very few trials that included data from longer than a 12‐month follow‐up period (Chapman 2009; Haworth 2011) so the conclusions drawn from this review may not be representative of the longer‐term effects in this population. This review also sought to examine the effects in both children and adults. There was only one trial that included data from children (Bianchi 2013), so again the conclusions drawn may not necessarily be representative of this population on a larger scale.
Agreements and disagreements with other studies or reviews
The authors are aware of no other published systematic review on the use of bisphosphonates for osteoporosis in people with CF, besides previous versions of this review (Brenckmann 2001; Conwell 2009; Conwell 2012; Conwell 2014).
The results of this review support the current guidelines recommending the use of bisphosphonate treatment in adults and children with CF with diagnosed CF‐related bone disease or osteoporosis; including those by the European Cystic Fibrosis Mineralisation guidelines (Sermet‐Gaudelus 2011) and the expert panel consensus recommendations for secondary osteoporosis in children published in Pediatric Rheumatology (Galindo‐Zavala 2020).
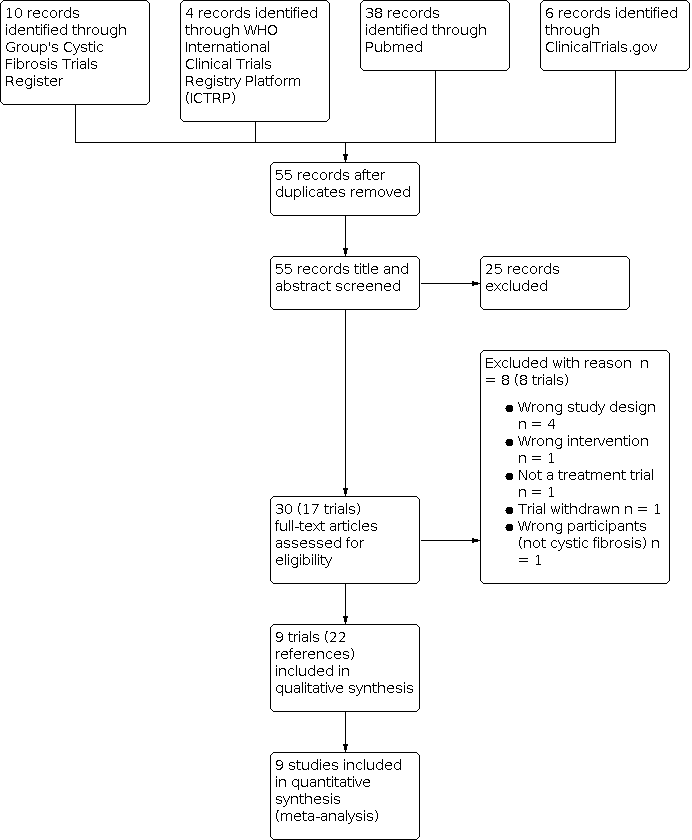
Selection process for this update.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Forest plot of comparison between bisphosphonates versus control (without lung transplantation), Outcome 1a Number of participants with any fracture.

Forest plot of comparison between bisphosphonates versus control (without lung transplantation), Outcome 1b i. Number of participants with non‐vertebral fractures.

Forest plot of comparison between bisphosphonates versus control (without lung transplantation), Outcome 1b ii. Number of participants with vertebral fractures.

Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 1: Total fractures

Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 2: Non‐vertebral fractures

Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 3: Vertebral fractures
![Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 4: % change in BMD, lumbar spine [DXA]](/es/cdsr/doi/10.1002/14651858.CD002010.pub5/media/CDSR/CD002010/image_n/nCD002010-CMP-001.04.svg)
Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 4: % change in BMD, lumbar spine [DXA]
![Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 5: % change in BMD, lumbar spine [DXA] (end of trial data only)](/es/cdsr/doi/10.1002/14651858.CD002010.pub5/media/CDSR/CD002010/image_n/nCD002010-CMP-001.05.svg)
Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 5: % change in BMD, lumbar spine [DXA] (end of trial data only)
![Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 6: % change in BMD, total hip/femur [DXA]](/es/cdsr/doi/10.1002/14651858.CD002010.pub5/media/CDSR/CD002010/image_n/nCD002010-CMP-001.06.svg)
Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 6: % change in BMD, total hip/femur [DXA]
![Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 7: % change in BMD, total hip/femur [DXA] (end of trial data only)](/es/cdsr/doi/10.1002/14651858.CD002010.pub5/media/CDSR/CD002010/image_n/nCD002010-CMP-001.07.svg)
Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 7: % change in BMD, total hip/femur [DXA] (end of trial data only)
![Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 8: % change in BMD, distal radius [SXA]](/es/cdsr/doi/10.1002/14651858.CD002010.pub5/media/CDSR/CD002010/image_n/nCD002010-CMP-001.08.svg)
Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 8: % change in BMD, distal radius [SXA]
![Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 9: % change in BMD, distal radius [SXA] (end of trial data only)](/es/cdsr/doi/10.1002/14651858.CD002010.pub5/media/CDSR/CD002010/image_n/nCD002010-CMP-001.09.svg)
Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 9: % change in BMD, distal radius [SXA] (end of trial data only)
![Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 10: % change in BMD, ultra distal radius [SXA]](/es/cdsr/doi/10.1002/14651858.CD002010.pub5/media/CDSR/CD002010/image_n/nCD002010-CMP-001.10.svg)
Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 10: % change in BMD, ultra distal radius [SXA]

Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 11: QoL

Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 12: Bone pain

Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 13: Fever

Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 14: Withdrawals due to adverse events

Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 15: Withdrawals (total)

Comparison 1: Bisphosphonates versus control (without lung transplantation) ‐ adults (18 years and over), Outcome 16: Survival

Comparison 2: Bisphosphonates versus control (without lung transplantation) ‐ children up to 18 years of age, Outcome 1: Total fractures

Comparison 2: Bisphosphonates versus control (without lung transplantation) ‐ children up to 18 years of age, Outcome 2: Non‐vertebral fractures

Comparison 2: Bisphosphonates versus control (without lung transplantation) ‐ children up to 18 years of age, Outcome 3: Vertebral fractures

Comparison 2: Bisphosphonates versus control (without lung transplantation) ‐ children up to 18 years of age, Outcome 4: % change in BMD, lumbar spine, DXA

Comparison 2: Bisphosphonates versus control (without lung transplantation) ‐ children up to 18 years of age, Outcome 5: Bone or muscle pain

Comparison 2: Bisphosphonates versus control (without lung transplantation) ‐ children up to 18 years of age, Outcome 6: Fever

Comparison 2: Bisphosphonates versus control (without lung transplantation) ‐ children up to 18 years of age, Outcome 7: Gastrointestinal adverse events

Comparison 2: Bisphosphonates versus control (without lung transplantation) ‐ children up to 18 years of age, Outcome 8: Headache

Comparison 2: Bisphosphonates versus control (without lung transplantation) ‐ children up to 18 years of age, Outcome 9: Any adverse event

Comparison 2: Bisphosphonates versus control (without lung transplantation) ‐ children up to 18 years of age, Outcome 10: Withdrawals, due to adverse events

Comparison 2: Bisphosphonates versus control (without lung transplantation) ‐ children up to 18 years of age, Outcome 11: Withdrawals, total

Comparison 2: Bisphosphonates versus control (without lung transplantation) ‐ children up to 18 years of age, Outcome 12: Survival

Comparison 3: Bisphosphonates versus control (with lung transplantation) ‐ adults (18 years and over), Outcome 1: Total Fractures

Comparison 3: Bisphosphonates versus control (with lung transplantation) ‐ adults (18 years and over), Outcome 2: Non‐vertebral fractures

Comparison 3: Bisphosphonates versus control (with lung transplantation) ‐ adults (18 years and over), Outcome 3: Vertebral fractures

Comparison 3: Bisphosphonates versus control (with lung transplantation) ‐ adults (18 years and over), Outcome 4: % change in BMD, lumbar spine, DXA

Comparison 3: Bisphosphonates versus control (with lung transplantation) ‐ adults (18 years and over), Outcome 5: % change in BMD, femur, DXA

Comparison 3: Bisphosphonates versus control (with lung transplantation) ‐ adults (18 years and over), Outcome 6: Bone pain

Comparison 3: Bisphosphonates versus control (with lung transplantation) ‐ adults (18 years and over), Outcome 7: Withdrawals, due to adverse events

Comparison 3: Bisphosphonates versus control (with lung transplantation) ‐ adults (18 years and over), Outcome 8: Withdrawals, total

Comparison 3: Bisphosphonates versus control (with lung transplantation) ‐ adults (18 years and over), Outcome 9: Survival
| Patient or population: adults with cystic fibrosis who have not had a lung transplant Settings: outpatients Comparison: placebo or no bisphosphonatesb | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Bisphosphonates | |||||
| New vertebral fractures
Follow‐up: 12 months | 42 per 1000 | 9 per 1000 (1 to 88) | OR 0.22 (0.02 to 2.09) | 142 (5) | ⊕⊝⊝⊝ very lowc,d |
|
| New non‐vertebral fractures
Follow‐up: 12 months | 21 per 1000 | 44 per 1000 (4 to 532) | OR 2.11 (0.18 to 25.35) | 95 (4) | ⊕⊝⊝⊝ very lowd,e |
|
| BMD: % change in BMD at the lumbar spine
Follow‐up: 12 months | The mean % change in BMD (lumbar spine) ranged across control groups from ‐1.8% to 0.7% | The mean % change in BMD in the intervention groups was 6.31% higher (5.39% higher to 7.22% higher) | NA | 171 (6) | ⊕⊕⊝⊝ lowf |
|
| BMD: % change in BMD at the hip or femur
Follow‐up: 12 months | The mean % change in BMD (hip or femur) ranged across control groups from ‐2.8% to ‐0.7% | The mean % change in BMD in the intervention groups was 4.41% higher (3.44% higher to 5.37% higher) | NA | 155 (5) | ⊕⊕⊝⊝ lowf |
|
| QoL: change in physical and mental component scores (SF36v2)
Follow‐up: 12 months | The change in mean (SD) SF36 physical score was ‐3.69 (8.33) in the control group | The mean change in SF36 physical score in the intervention group was 2.51 higher (1.38 lower to 6.40 higher) than in the control group | NA | 47 (1) | ⊕⊕⊝⊝ lowd,g | The results for the physical and mental components are heterogeneous
|
| The change in mean (SD) SF36 mental score was 3.26 (12.27) in the control group | The mean change in SF36 mental score in the intervention group was 5.93 lower (11.73 lower to 0.13 higher) than in the control group | |||||
| Adverse events: bone pain (all routes of bisphosphonate administration)
Follow‐up: 12 months | 38 per 1000 | 323 per 1000 (122 to 857) | OR 8.49 (3.20 to 22.56) | 206 (7) | ⊕⊕⊕⊝ moderateh | Bone pain Separating by route of administration did not change the results; both routes favoured control. Oral bisphosphonates: MD 4.98 (1.24 to 20.09) and IV bisphosphonates: MD 14.17 (3.64 to 55.17)
Fever Oral route: 2 trials of oral alendronate reported that none of the participants in either group experienced fever IV route: 3 trials showed that bisphosphonates were associated with a higher occurrence of fever OR 12.64 (2.31 to 69.11)
GI adverse effects Only measured in the oral bisphosphonates trials. At 12 months, 1 trial reported 3 occurrences of diarrhoea (1 in the bisphosphonate group and 2 in the placebo group) (Aris 2004) 1 trial reported no GI adverse effects in either group (Bianchi 2013) 1 trial reported 10 GI adverse events in the bisphosphonates group compared to 7 in the control group (Papaioannou 2008) |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). BMD: bone mineral density; CI: confidence interval; GI: gastrointestinal; IV: intravenous; MD: mean difference; NA: not applicable; OR: odds ratio; QoL: quality of life; SD: standard deviation; SF36v2: medical outcomes study 36‐item short form. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
| aTrials used different types and formulations of bisphosphonates: IV zoledronate (Boyle 2005; Chapman 2009); IV pamidronate (Haworth 2001); oral alendronate (Aris 2004; Bianchi 2013; Krasovsky 2010; Papaioannou 2008); oral risedronate (Haworth 2011). | ||||||
| Patient or population: children with cystic fibrosis who have not had a lung transplant Settings: outpatients Intervention: oral alendronate plus oral calcifediol and RDA dietary calcium Comparison: oral placebo plus oral calcifediol and RDA dietary calcium | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Bisphosphonates | |||||
| New vertebral fractures
Follow‐up: 12 months | 54 per 1000 | 17 per 1000 (2 to 169) | OR 0.32 (0.03 to 3.13) | 113 (1) | ⊕⊕⊝⊝ lowa |
|
| New non‐vertebral fractures
Follow‐up: 12 months | 36 per 1000 | 7 per 1000 (1 to 145) | OR 0.19 (0.01 to 4.04) | 113 (1) | ⊕⊕⊝⊝ lowa |
|
| BMD: % change in BMD at the lumbar spine
Follow‐up: 12 months | The % change in BMD at the lumbar spine was higher in the treatment group than the control group, MD 14.50 (95% CI 12.91 to 16.09) | NA | 113 (1) | ⊕⊕⊝⊝ lowa |
| |
| BMD: % change in BMD at the hip or femur | This outcome was not reported |
| ||||
| QoL | This outcome was not reported |
| ||||
| Adverse events
Follow‐up: 12 months | There was no difference in bone or muscle pain, OR 3.00 (95% CI 0.12 to 75.22); fever, OR 3.00 (95% CI 0.12 to 75.22); or GI adverse events OR 0.67 (95% CI 0.20 to 2.26) | NA | 113 (1) | ⊕⊕⊝⊝ lowa |
| |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). BMD: bone mineral density; CI: confidence interval; GI: gastrointestinal; MD: mean difference; NA: not applicable; OR: odds ratio; QoL: quality of life; RDA: recommended daily allowance. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
| aDowngraded twice due to imprecision cause by small participant numbers and low event rates. | ||||||
| Patient or population: adults with cystic fibrosis who have had a lung transplant Settings: outpatients Intervention: bisphosphonates (IV pamidronate plus oral vitamin D and oral calcium) Comparison: oral vitamin D and oral calcium | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Bisphosphonates | |||||
| New vertebral fractures
Follow‐up: 12 months | This outcome was not reported at 12 months ‐ see comments | 1 study reported results at 24 months (Aris 2000) and found no difference in the number of participants with a vertebral fracture, OR 3.92 (95% CI 0.36 to 42.20) | ||||
| New non‐vertebral fractures
Follow‐up: 12 months | This outcome was not reported at 12 months ‐ see comments | 1 study reported results at 24 months (Aris 2000) and found no difference in the number of participants with a non‐vertebral fracture, OR 0.46 (95% CI 0.09 to 2.27) | ||||
| BMD: % change in BMD at the lumbar spine
Follow‐up: 12 months | This outcome was not reported at 12 months ‐ see comments | 1 study reported results at 24 months (Aris 2000) and found the % change in BMD was higher in the treatment group than the control group MD 6.20 (95% CI 4.28 to 8.12) | ||||
| BMD: % change in BMD at the hip or femur
Follow‐up: 12 months | This outcome was not reported at 12 months ‐ see comments | 1 study reported results at 24 months (Aris 2000) and found the % change in BMD was higher in the treatment group than the control group, MD 7.90 (95% CI 5.78 to 10.02). | ||||
| QoL | This outcome was not reported at any time point |
| ||||
| Adverse events
Follow‐up: 12 months | This outcome was not reported at 12 months ‐ see comment | 1 study reported results at 24 months (Aris 2000) and found none of the participants in either group experienced bone pain or fever | ||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). BMD: bone mineral density; CI: confidence interval; IV: intravenous; MD: mean difference; OR: odds ratio; QoL: quality of life. | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1.1 Total fractures Show forest plot | 6 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1.1 12 months | 5 | 142 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.57 [0.13, 2.50] |
| 1.1.2 24 months | 2 | 44 | Odds Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 1.2 Non‐vertebral fractures Show forest plot | 5 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.2.1 12 months | 4 | 95 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.11 [0.18, 25.35] |
| 1.2.2 24 months | 2 | 44 | Odds Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 1.3 Vertebral fractures Show forest plot | 6 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.3.1 12 months | 5 | 142 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.22 [0.02, 2.09] |
| 1.3.2 24 months | 2 | 44 | Odds Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 1.4 % change in BMD, lumbar spine [DXA] Show forest plot | 8 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.4.1 6 months | 4 | 101 | Mean Difference (IV, Fixed, 95% CI) | 4.61 [3.90, 5.32] |
| 1.4.2 12 months | 6 | 171 | Mean Difference (IV, Fixed, 95% CI) | 6.31 [5.39, 7.22] |
| 1.4.3 24 months | 2 | 43 | Mean Difference (IV, Fixed, 95% CI) | 5.49 [4.38, 6.60] |
| 1.5 % change in BMD, lumbar spine [DXA] (end of trial data only) Show forest plot | 8 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.5.1 End of trial | 8 | 199 | Mean Difference (IV, Fixed, 95% CI) | 5.95 [5.17, 6.73] |
| 1.6 % change in BMD, total hip/femur [DXA] Show forest plot | 6 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.6.1 6 months | 3 | 96 | Mean Difference (IV, Fixed, 95% CI) | 3.58 [2.75, 4.40] |
| 1.6.2 12 months | 5 | 155 | Mean Difference (IV, Fixed, 95% CI) | 4.41 [3.44, 5.37] |
| 1.6.3 24 months | 2 | 42 | Mean Difference (IV, Fixed, 95% CI) | 6.49 [5.32, 7.66] |
| 1.7 % change in BMD, total hip/femur [DXA] (end of trial data only) Show forest plot | 6 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.7.1 End of trial | 6 | 178 | Mean Difference (IV, Fixed, 95% CI) | 4.89 [4.06, 5.72] |
| 1.8 % change in BMD, distal radius [SXA] Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.8.1 6 months | 2 | 48 | Mean Difference (IV, Fixed, 95% CI) | 0.02 [‐0.73, 0.78] |
| 1.8.2 12 months | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | 0.32 [‐0.30, 0.94] |
| 1.8.3 24 months | 1 | 14 | Mean Difference (IV, Fixed, 95% CI) | 1.50 [0.41, 2.59] |
| 1.9 % change in BMD, distal radius [SXA] (end of trial data only) Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.9.1 End of study | 2 | 42 | Mean Difference (IV, Fixed, 95% CI) | 0.74 [‐0.21, 1.70] |
| 1.10 % change in BMD, ultra distal radius [SXA] Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.10.1 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.11 QoL Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.11.1 Physical component | 1 | 47 | Mean Difference (IV, Fixed, 95% CI) | 2.51 [‐1.38, 6.40] |
| 1.11.2 Mental component | 1 | 47 | Mean Difference (IV, Fixed, 95% CI) | ‐5.93 [‐11.73, ‐0.13] |
| 1.12 Bone pain Show forest plot | 7 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.12.1 All routes of bisphosphonate administration | 7 | 206 | Odds Ratio (M‐H, Fixed, 95% CI) | 8.49 [3.20, 22.56] |
| 1.12.2 Oral bisphosphonates | 4 | 146 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.98 [1.24, 20.09] |
| 1.12.3 Intravenous bisphosphonates | 3 | 60 | Odds Ratio (M‐H, Fixed, 95% CI) | 14.17 [3.64, 55.17] |
| 1.13 Fever Show forest plot | 5 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.13.1 All routes of bisphosphonate administration | 5 | 118 | Odds Ratio (M‐H, Fixed, 95% CI) | 12.64 [2.31, 69.11] |
| 1.13.2 Oral bisphosphonates | 2 | 63 | Odds Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 1.13.3 Intravenous bisphosphonates | 3 | 55 | Odds Ratio (M‐H, Fixed, 95% CI) | 12.64 [2.31, 69.11] |
| 1.14 Withdrawals due to adverse events Show forest plot | 6 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.14.1 6 months | 2 | 53 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.95 [0.14, 108.09] |
| 1.14.2 12 months | 5 | 177 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.07 [1.11, 14.90] |
| 1.14.3 24 months | 2 | 58 | Odds Ratio (M‐H, Fixed, 95% CI) | 16.34 [1.98, 134.89] |
| 1.15 Withdrawals (total) Show forest plot | 6 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.15.1 6 months | 2 | 53 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.77 [0.27, 11.60] |
| 1.15.2 12 months | 5 | 177 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.45, 2.28] |
| 1.15.3 24 months | 2 | 58 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.34, 2.69] |
| 1.16 Survival Show forest plot | 7 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.16.1 6 months | 2 | 36 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.05, 16.39] |
| 1.16.2 12 months | 4 | 155 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.98 [0.30, 29.84] |
| 1.16.3 24 months | 2 | 58 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.27 [0.43, 42.63] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 2.1 Total fractures Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.1.1 12 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.2 Non‐vertebral fractures Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.2.1 12 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.3 Vertebral fractures Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.3.1 12 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.4 % change in BMD, lumbar spine, DXA Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2.4.1 12 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2.5 Bone or muscle pain Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.5.1 12 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.6 Fever Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.6.1 12 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.7 Gastrointestinal adverse events Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.7.1 12 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.8 Headache Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.8.1 12 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.9 Any adverse event Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.9.1 12 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.10 Withdrawals, due to adverse events Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.10.1 12 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.11 Withdrawals, total Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.11.1 12 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.12 Survival Show forest plot | 1 | 113 | Odds Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 2.12.1 12 months | 1 | 113 | Odds Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 3.1 Total Fractures Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.1.1 24 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.2 Non‐vertebral fractures Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.2.1 24 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.3 Vertebral fractures Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.3.1 24 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.4 % change in BMD, lumbar spine, DXA Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.4.1 24 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.5 % change in BMD, femur, DXA Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.5.1 24 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.6 Bone pain Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.6.1 24 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.7 Withdrawals, due to adverse events Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.8 Withdrawals, total Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.8.1 24 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.9 Survival Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.9.1 24 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |