Hybrid repair versus conventional open repair for aortic arch dissection
Información
- DOI:
- https://doi.org/10.1002/14651858.CD012920.pub2Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 25 julio 2021see what's new
- Tipo:
-
- Intervention
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Vascular
- Copyright:
-
- Copyright © 2021 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
EPK: acquiring trial reports, trial selection, data extraction, data analysis, data interpretation, and review drafting,
SS: review drafting
FJ: data interpretation
AE: acquiring trial reports, trial selection, and data extraction
DD: data interpretation
DV: review drafting
NH: trial selection, data interpretation, review drafting, future review updates, and guarantor of the review
Sources of support
Internal sources
-
No sources of support provided
External sources
-
Chief Scientist Office, Scottish Government Health Directorates, The Scottish Government, UK
The Cochrane Vascular editorial base is supported by the Chief Scientist Office.
Declarations of interest
EPK: none known.
SS: SS and his institution have received payment from Gore Medical for training physicians on endovascular aortic repair. SS is the Principal Investigator in the INSIGHT post Market Surveillance trial of the INCRAFT abdominal aortic endograft (Cordis/Cardinal health). He reports he has no conflict of interest which will affect this review.
FJ: Institution received funding from the Health Research Board (Ireland) for a Cochrane Training Fellowship to enable me to undertake a Cochrane Systematic Review over 24 months. This training grant provides me with funding to attend Cochrane Training Programmes/conferences over the two year period of my fellowship.
AE: has received funding from Health Research Board (Ireland) under the HRB Cochrane Ireland Fellowship Scheme to undertake a Cochrane Systematic Review (Elhelali 2021) (Grant number CTF‐2016‐1863).
DD: none known.
DV: none known.
NH: has received payment for consultation on Regulatory Documents (Versono Ltd and Integer) and for working on medical device design at Boston Scientific (Enterprise Ireland Bioinnovate Fellow). Her institution has received payment for provision of training on endovascular aortic repair from Gore Medical. She is investigator in the INSIGHT Post Market Surveillance Trial of the Incraft AAA device (Cordis/Cardinal Health). Her Institution has received payment for an Aortic Fellowship grant (Jotec/Cryolife), and Research fellowship grants (Gore Medical and Medtronic). She declares no competing interests, relationships, conditions or circumstances, which will conflict with this review.
Acknowledgements
We are very grateful to Cochrane Vascular for their support and guidance in the preparation of this review.
The review authors and the Cochrane Vascular editorial base are grateful to the following peer reviewers for their time and comments: Piergiorgio Cao FRCS, Senior Professor of Vascular Surgery, University of Perugia; Consultant Vascular Surgeon, Ospedale Bel Colle Viterbo, Clinica Mater Dei Roma, Rome, Italy; Mr Stephen Badger, Belfast Health & Social Care Trust, Belfast, UK.
Version history
| Published | Title | Stage | Authors | Version |
| 2021 Jul 25 | Hybrid repair versus conventional open repair for aortic arch dissection | Review | Edel P Kavanagh, Sherif Sultan, Fionnuala Jordan, Ala Elhelali, Declan Devane, Dave Veerasingam, Niamh Hynes | |
| 2018 Jan 19 | Hybrid repair versus conventional open repair for aortic arch dissection | Protocol | Edel P Kavanagh, Fionnuala Jordan, Niamh Hynes, Ala Elhelali, Declan Devane, Dave Veerasingam, Sherif Sultan | |
Differences between protocol and review
There are no differences between the protocol and review.
Notes
Parts of the Methods section of this review are based on a standard template established by Cochrane Vascular.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
Medical Subject Headings Check Words
Humans;
PICO
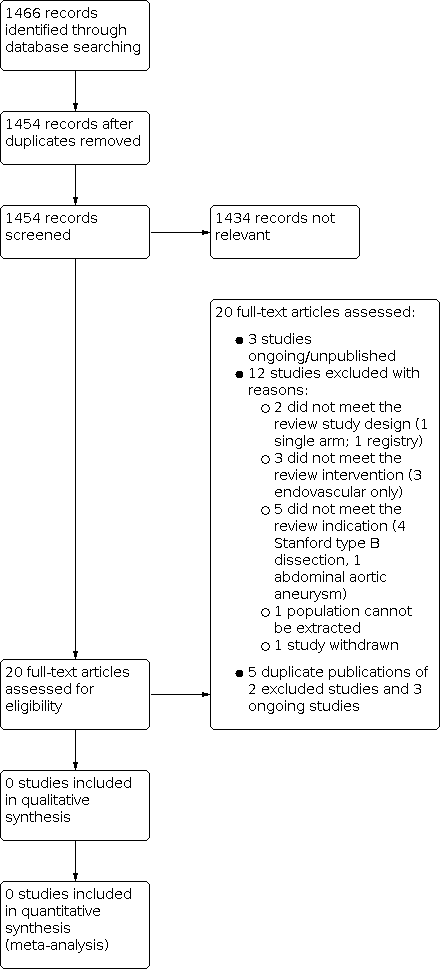
Study flow diagram.
| Types of outcome measures | Defined by | Including |
|---|---|---|
| Primary outcomes | ||
| Mortality | Dissection related and all causes | (Grade V) All deaths at 30 days and 12 months |
| Neurological deficit | Global events | (Grade I ‐ IV) Postoperative agitation, delirium, obtundation, or myoclonic movements, without localised cerebral neurological signs |
| Focal events | (Grade I ‐ IV) Lateralising sensory or motor deficit or focal seizure activity | |
| Spinal neurological events | (Grade I ‐ IV) Paraplegia, paraparesis | |
| Cardiac injury | Myocardial ischaemia | (Grade I ‐ IV) |
| Low cardiac output syndrome | (Grade I ‐ IV) | |
| Arrhythmia | (Grade I ‐ IV) | |
| Pericardial effusion | (Grade I ‐ IV) | |
| Respiratory compromise | Parenchymal complications | (Grade I ‐ IV) Atelectasis, pneumonia, pulmonary oedema, and acute respiratory distress syndrome |
| Pleural complications | (Grade I ‐ IV) Pneumothorax, pleural effusion | |
| Renal ischaemia | Modified RIFLE classification (Bellomo 2004): Risk (I), Injury (II), Failure (III), Loss/End‐Stage Kidney Dysfunction (IV) | (Grade I ‐ IV) Serum creatinine increase, glomerular filtration rate (GFR) decrease, anuria, haemodialysis |
| Secondary outcomes | ||
| False lumen thrombosis | Partial or complete thrombosis | ‐ |
| Mesenteric ischaemia | Gut complications | (Grade I ‐ IV) Ileus or gastric paresis, gut ischaemia manifested as metabolic acidosis or increased lactate |
| Grades as defined by Yan 2014: Grade I: any deviation from the normal postoperative course but self‐limiting or requiring simple therapeutic regimens (including antiemetics, antipyretics, analgesics, electrolytes, and physiotherapy); Grade II: complications requiring pharmacological treatment for resolution; Grade III: complications requiring surgical, endoscopic, or radiological intervention but not requiring regional or general anaesthesia or requiring interdisciplinary intervention; Grade IV: complications requiring surgical, endoscopic, or radiological intervention under regional or general anaesthesia, or requiring new intensive care unit (ICU) admission or ongoing ICU management for > 7 days or hospitalisation for > 30 days, or causing secondary organ failure; Grade V: death caused by a complication. | ||
| Summary of findings for the main comparison: Hybrid repair versus conventional open repair for aortic arch dissection | ||||||
| Patient or population: patients with a diagnosis of aortic arch dissection Settings: hospital Intervention: hybrid repair Comparison: open repair | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | Number of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Risk with open repair | Risk with hybrid repair | |||||
| Mortality, Follow‐up: median N (months) | Study population | HR N (N to N) | N | ⊕⊝⊝⊝ ⊕⊕⊝⊝ ⊕⊕⊕⊝ ⊕⊕⊕⊕ | ||
| N per 1000 | N per 1000 | |||||
| Neurological deficit, Follow‐up: median N (months) | Study population | RR N (N to N) | N | ⊕⊝⊝⊝ ⊕⊕⊝⊝ ⊕⊕⊕⊝ ⊕⊕⊕⊕ | ||
| N per 1000 | N per 1000 | |||||
| Cardiac injury, Follow‐up: median N (months) | Study population | RR N (N to N) | N | ⊕⊝⊝⊝ ⊕⊕⊝⊝ ⊕⊕⊕⊝ ⊕⊕⊕⊕ | ||
| N per 1000 | N per 1000 | |||||
| Respiratory compromise, Follow‐up: median N (months) | Study population | RR N (N to N) | N | ⊕⊝⊝⊝ ⊕⊕⊝⊝ ⊕⊕⊕⊝ ⊕⊕⊕⊕ | ||
| N per 1000 | N per 1000 | |||||
| Renal ischaemia, Follow‐up: median N (months) | Study population | RR N (N to N) | N | ⊕⊝⊝⊝ ⊕⊕⊝⊝ ⊕⊕⊕⊝ ⊕⊕⊕⊕ | ||
| N per 1000 | N per 1000 | |||||
| False lumen thrombosis, Follow‐up: median N (months) | Study population | RR N (N to N) | N | ⊕⊝⊝⊝ ⊕⊕⊝⊝ ⊕⊕⊕⊝ ⊕⊕⊕⊕ | ||
| N per 1000 | N per 1000 | |||||
| Mesenteric ischaemia, Follow‐up: median N (months) | Study population | RR N (N to N) | N | ⊕⊝⊝⊝ ⊕⊕⊝⊝ ⊕⊕⊕⊝ ⊕⊕⊕⊕ | ||
| N per 1000 | N per 1000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||