Withdrawal of immunosuppressant or biologic therapy for patients with quiescent Crohn's disease
Abstract
Background
Crohn's disease (CD) is a chronic, relapsing and remitting disease of the gastrointestinal tract that can cause significant morbidity and disability. Current treatment guidelines recommend early intervention with immunosuppressant or biological therapy in high‐risk patients with a severe disease phenotype at presentation. The feasibility of therapeutic de‐escalation once remission is achieved is a commonly encountered question in clinical practice, driven by patient and clinician concerns regarding safety, adverse events, cost and national regulations. Withdrawal of immunosuppressant and biologic drugs in patients with quiescent CD may limit adverse events and reduce healthcare costs. Alternatively, stopping these drug therapies may result in negative outcomes such as disease relapse, drug desensitization, bowel damage and need for surgery.
Objectives
To assess the feasibility and safety of discontinuing immunosuppressant or biologic drugs, administered alone or in combination, in patients with quiescent CD.
Search methods
We searched CENTRAL, MEDLINE, Embase and the Cochrane IBD Group Specialized Register from inception to 19 December 2017. We also searched the reference lists of potentially relevant manuscripts and conference proceedings to identify additional studies.
Selection criteria
Randomized controlled trials (RCTs) and prospective cohort studies that followed patients for a minimum duration of six months after drug discontinuation were considered for inclusion. The patient population of interest was adults (> 18 years) with CD (as defined by conventional clinical, endoscopic or histologic criteria) who had achieved remission while receiving immunosuppressant or biologic drugs administered alone or in combination. Patients then discontinued the drug regimen following a period of maintenance therapy of at least six months. The comparison was usual care (i.e. continuation of the drug regimen).
Data collection and analysis
The primary outcome measure was the proportion of patients who relapsed following discontinuation of immunosuppressant or biologic drugs, administered alone or in combination. Secondary outcomes included: the proportion of patients who responded to the reintroduction of immunosuppressant or biologic drugs, given as monotherapy or combination therapy; the proportion of patients who required surgery following relapse; the proportion of patients who required hospitalization for CD following relapse; the proportion of patients who developed new CD‐related complications (e.g. fistula, abscesses, strictures) following relapse; the proportion of patients with elevated biomarkers of inflammation (CRP, fecal calprotectin) in those who stop and those who continue therapy; the proportion of patients with anti‐drug antibodies and low serum trough drug levels; time to relapse; and the proportion of patients with adverse events, serious adverse events and withdrawal due to adverse events. For dichotomous outcomes, we calculated the risk ratio (RR) and 95% confidence interval (95% CI). Data were analyzed on an intention‐to‐treat basis where patients with missing outcome data were assumed to have relapsed. The overall quality of the evidence supporting the primary and secondary outcomes was assessed using the GRADE criteria.
Main results
A total of six RCTs (326 patients) evaluating therapeutic discontinuation in patients with quiescent CD were eligible for inclusion. In four RCTs azathioprine monotherapy was discontinued, and in two RCTs azathioprine was discontinued from a combination therapy regimen consisting of azathioprine with infliximab. No studies of biologic monotherapy withdrawal were eligible for inclusion. The majority of studies received unclear or low risk of bias ratings, with the exception of three open‐label RCTs, which were rated as high risk of bias for blinding. Four RCTs (215 participants) compared discontinuation to continuation of azathioprine monotherapy, while two studies (125 participants) compared discontinuation of azathioprine from a combination regimen to continuation of combination therapy. Continuation of azathioprine monotherapy was shown to be superior to withdrawal for risk of clinical relapse. Thirty‐two per cent (36/111) of azathioprine withdrawal participants relapsed compared to 14% (14/104) of participants who continued with azathioprine therapy (RR 0.42, 95% CI 0.24 to 0.72, GRADE low quality evidence). However, it is uncertain if there are any between‐group differences in new CD‐related complications (RR 0.34, 95% CI 0.06 to 2.08, GRADE low quality evidence), adverse events (RR 0.88, 95% CI 0.67 to 1.17, GRADE low quality evidence), serious adverse events (RR 3.29, 95% CI 0.35 to 30.80, GRADE low quality evidence) or withdrawal due to adverse events (RR 2.59, 95% CI 0.35 to 19.04, GRADE low quality evidence). Common adverse events included infections, mild leukopenia, abdominal symptoms, arthralgias, headache and elevated liver enzymes. No differences between azathioprine withdrawal from combination therapy versus continuation of combination therapy were observed for clinical relapse. Among patients who continued combination therapy with azathioprine and infliximab, 48% (27/56) had a clinical relapse compared to 49% (27/55) of patients discontinued azathioprine but remained on infliximab (RR 1.02, 95% CI 0.68 to 1.52, P = 0.32; GRADE low quality evidence). The effects on adverse events (RR 1.11, 95% CI 0.44 to 2.81, GRADE low quality of evidence) or serious adverse events are uncertain (RR 1.00, 95% CI 0.21 to 4.66; GRADE very low quality of evidence). Common adverse events in the combination therapy studies included infections, liver test elevations, arthralgias and infusion reactions.
Authors' conclusions
The effects of withdrawal of immunosuppressant therapy in people with quiescent Crohn's disease are uncertain. Low quality evidence suggests that continuing azathioprine monotherapy may be superior to withdrawal for avoiding clinical relapse, while very low quality evidence suggests that there may be no difference in clinical relapse rates between discontinuing azathioprine from a combination therapy regimen, compared to continuing combination therapy. It is unclear whether withdrawal of azathioprine, initially administered alone or in combination, impacts on the development of CD‐related complications, adverse events, serious adverse events or withdrawal due to adverse events. Further high‐quality research is needed in this area, particularly double‐blind RCTs in which biologic therapy or an immunosuppressant other than azathioprine is withdrawn.
PICO
Plain language summary
Is withdrawal of drug therapy feasible in patients with CD who have achieved remission?
Background
Crohn's disease is a serious, chronic, inflammatory disease of the small and large intestine. Symptoms include abdominal pain, diarrhea, bleeding and weight loss. When people with Crohn's disease are experiencing symptoms the disease is 'active'. When the symptoms stop, it is called 'remission'. When people in remission experience symptoms it is called a 'relapse'. Immunosuppressant drugs (e.g. azathioprine, 6‐mercaptopurine and methotrexate) and biologic medications (e.g. infliximab, adalimumab, vedolizumab and ustekinumab) are commonly used alone or in combination to treat Crohn's disease. While effective for initially controlling disease (i.e. inducing remission), there are safety and cost concerns regarding the long‐term use of these drugs for the prevention of relapse in people with Crohn's disease in remission.
Study characteristics
We performed a comprehensive literature review and identified six randomized controlled trials (an experiment in which participants are randomly assigned to receive two or more interventions and the results are compared) that involved a total of 326 participants. Four of the six studies assigned patients who had been receiving azathioprine alone to either continue or discontinue therapy (215 participants). Two of the six studies assigned patients who had been receiving azathioprine in addition to infliximab to continue therapy or discontinue azathioprine (111 participants).
Key results
Clinical relapse occurred in 13% (14/104) of patients who continued azathioprine monotherapy compared to 32% (36/111) of patients who discontinued azathioprine monotherapy. No differences were observed for Crohn's disease‐related complications, side effects, serious side effects and withdrawal due to side effects. Common side effects included infections, mild decrease in the number of white blood cells, abdominal symptoms, joint pain, headache and elevated liver enzymes. Among patients who continued combination therapy with azathioprine and infliximab, 48% (27/56) had a clinical relapse compared to 49% (27/55) of patients discontinued azathioprine but remained on infliximab. No differences in side effects, serious side effects or withdrawal due to side effects were observed. Common side effects reported in the combination therapy studies included infections, liver test elevations, joint pain and infusion reactions (a hypersensitivity reaction to the biologic medication).
Quality of evidence
Overall, the quality of evidence for each outcome was low due to a high risk of study bias and small numbers of patients evaluated.
Conclusions
The effects of withdrawal of immunosuppressant therapy in people with Crohn's disease in remission are uncertain. Low quality evidence suggests that continuing azathioprine monotherapy may be superior to withdrawal of azathioprine for avoiding clinical relapse in people with Crohn's disease in remission. Low quality evidence suggests that stopping the immunosuppressive after combination therapy does not seem to impact on the risk of relapsing. It is unclear whether the withdrawal of azathioprine, initially administered alone or in combination, impacts on the development of Crohn's disease‐related complications, side effects, serious side effects, or withdrawal from the studies due to side effects. Additional research is needed in this area to better inform clinical practice, particularly high‐quality randomized controlled trials examining outcomes when biologic therapy is withdrawn.
Authors' conclusions
Summary of findings
| Usual care compared to immunosuppressive withdrawal after monotherapy for patients with quiescent Crohn's disease | ||||||
| Patient or population: Patients with quiescent Crohn's disease | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
| Risk with immunosuppressive withdrawal after monotherapy | Risk with usual care | |||||
| Relapse at 12, 18 or 24 months | Study population | RR 0.42 | 215 | ⊕⊕⊝⊝ | Sparse data (50 events) | |
| 324 per 1,000 | 136 per 1,000 | |||||
| New CD‐related complications | Study population | RR 0.34 | 135 | ⊕⊝⊝⊝ | Very sparse data (5 events) | |
| 58 per 1,000 | 20 per 1,000 | |||||
| Adverse events | Study population | RR 0.88 | 186 | ⊕⊕⊝⊝ | Sparse data (45 events) | |
| 240 per 1,000 | 211 per 1,000 | |||||
| Serious adverse events | Study population | RR 3.29 | 134 | ⊕⊝⊝⊝ | Very sparse data (2 events) | |
| 0 per 1,000 | 0 per 1,000 | |||||
| Withdrawal due to adverse events | Study population | RR 2.59 | 135 | ⊕⊝⊝⊝ | Very sparse data (5 events) | |
| 14 per 1,000 | 38 per 1,000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded one level due to high risk of bias for blinding in one study and unclear risk of bias in three studies in the pooled analysis 2 Downgraded one level due to sparse data 3 Downgraded one level due to unclear risk of bias in the two studies in the pooled analysis 4 Downgraded two levels due to very sparse data 5 Downgraded one level due to unclear risk of bias in the three studies in the pooled analysis | ||||||
| Usual care compared to immunosuppressive withdrawal after combination therapy for patients with quiescent Crohn's disease | ||||||
| Patient or population: Patients with quiescent Crohn's disease | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
| Risk with immunosuppressive withdrawal after combination therapy | Risk with usual care | |||||
| Relapse at 12 or 24 months | Study population | RR 1.02 | 111 | ⊕⊕⊝⊝ | Sparse data (54 events) | |
| 491 per 1,000 | 501 per 1,000 | |||||
| Adverse events | Study population | RR 1.11 | 111 | ⊕⊕⊝⊝ | Sparse data (51 events) | |
| 455 per 1,000 | 505 per 1,000 | |||||
| Serious adverse events | Study population | RR 1.00 | 80 | ⊕⊝⊝⊝ | Very sparse data (6 events) | |
| 75 per 1,000 | 75 per 1,000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded one level due to high risk of bias for blinding 2 Downgraded one level due to sparse data 3 Downgraded two levels due to very sparse data | ||||||
Background
Description of the condition
Crohn's disease (CD) is a chronic, relapsing and remitting, immune‐mediated disease of the gastrointestinal tract which can result in significant morbidity and disability through progressive bowel damage. Typical symptoms include abdominal pain, chronic diarrhoea, weight loss, fatigue and impaired quality of life. The exact etiology of CD remains unknown, however a complex interplay between environmental factors, genetic susceptibility and intestinal microbiota likely cause the abnormal immune response and compromised epithelial barrier function that characterize the condition (Haag 2015).
Young adults are primarily affected, with the highest incidence of diagnosis reported during the second or third decades of life (Molodecky 2012). Epidemiological studies show a steady increase in the worldwide incidence of CD (Molodecky 2012). The highest incidence rates are reported in Australia (29.3 per 100,000 person‐years; Wilson 2010), Canada (20 per 100,000 person‐years; Bernstein 2006), New Zealand (16 per 100,000 person‐years; Gearry 2006) and Northern Europe (10 per 100,000 person‐years; Thompson 1998).
CD most commonly affects the terminal ileum and colon, yet any segment of the gastrointestinal tract may be involved. Extra‐intestinal manifestations may occur in up to half of all patients (Harbord 2016). Inflammatory disease is the most frequent phenotype at diagnosis, however approximately 50% of patients eventually develop stricturing or penetrating disease which often necessitates surgery (Peyrin‐Biroulet 2012). Over 90% of CD patients develop endoscopic disease recurrence within 15 years of the first bowel resection (Buisson 2012).
Description of the intervention
Current treatment guidelines recommend a sequential 'step‐up' approach, with initial use of first‐line drugs such as oral corticosteroids and subsequent escalation to immunosuppressant and biologic agents as monotherapy or in combination if necessary (Colombel 2010a). Conversely, the 'step‐down' approach involves initially treating high‐risk patients and those with severe disease at diagnosis with immunosuppressant and biologic medications. Evidence in support of the step‐down strategy has accumulated over the last decade (Colombel 2010b; D'Haens 2010). For example, in the SONIC trial (The Study of Biologic and Immunomodulator Naive Patients in Crohn’s Disease), 56.8% of patients treated with combination therapy achieved steroid‐free remission at week 26, as compared with 44.4% of patients receiving biologic alone, or with 30% of patients receiving azathioprine alone (Colombel 2010b). Findings from D'Haens 2008 also suggest that early combination therapy may be more effective than conventional management for induction of remission in CD. At week 26, 60% of patients receiving combination infliximab and azathioprine achieved clinical remission compared to 23% of those who received corticosteroids followed in sequence by azathioprine and infliximab (D'Haens 2008). Consequently, in this era of early intervention, there is an increasing number of patients being exposed to immunosuppressants and biologics early in their disease course and for a longer time horizon.
The feasibility of de‐escalation of therapy once remission is achieved is a common question encountered in clinical practice, driven by patient and clinician concerns around safety, adverse events, cost, convenience and national regulations. Long‐term exposure to thiopurines has been associated with the development of lymphoproliferative disorders (Beaugerie 2009), and cancer of the skin and urinary tract (Bourrier 2016; Peyrin‐Biroulet 2011). Tumor necrosis factor‐alpha (TNF‐α) antagonist therapies may increase the risk of infections (Billioud 2013), and conflicting evidence about a potential increase in the risk of melanoma exists (Andersen 2014; Long 2012). Patients receiving combination therapy may have an increased risk of developing hepatosplenic T cell lymphoma (Subramaniam 2014), non‐Hodgkin’s lymphoma (Siegel 2009), and infections. The potential long‐term consequences of exposure to biologic agents remains unknown.
Biologic medications are relatively expensive. It is estimated that TNF‐α antagonists account for 64% of the direct costs of CD treatment (van der Valk 2014), although costs are likely to decrease with the approval of biosimilar drugs. Questions have been raised as to whether discontinuing immunosuppressant and biologic therapies in patients with quiescent CD may limit adverse events and reduce the high healthcare costs associated with these therapies while maintaining remission.
How the intervention might work
Withdrawal of immunosuppressant and biologic drugs in patients with quiescent CD may reduce the risk of adverse events and reduce healthcare costs without any impact upon the disease state. Alternatively, stopping these drug therapies may result in negative outcomes such as disease relapse, drug desensitization, bowel damage and need for surgery.
Why it is important to do this review
A systematic appraisal of the literature was required to highlight the potential benefits and risks of withdrawing immunosuppressant and biologic drug therapy in CD patients who have achieved remission.
Objectives
The primary objective of this review was to assess the feasibility and safety of discontinuing immunosuppressant or biologic drugs, administered alone or in combination, in patients with quiescent CD.
Methods
Criteria for considering studies for this review
Types of studies
Randomized controlled trials (RCTs), controlled clinical trials, and prospective cohort studies with a control group were considered for inclusion. Included studies followed patients for a minimum duration of six months after drug discontinuation.
Types of participants
Adults (> 18 years) with CD (as defined by conventional clinical, endoscopic or histologic criteria) who achieved remission (as defined by the original study) while receiving immunosuppressant or biologic drugs administered alone or in combination were considered for inclusion.
Types of interventions
The intervention of interest was the discontinuation of immunosuppressant or biologic drugs, administered alone or in combination, following a period of maintenance therapy of at least six months. The comparison group was usual care.
Types of outcome measures
Primary outcomes
The primary outcome was the proportion of patients who relapsed (as defined by the included studies) following discontinuation of immunosuppressant or biologic drugs, administered alone or in combination.
Secondary outcomes
Secondary outcomes (where available) included: 1) the proportion of patients who responded to the reintroduction of immunosuppressant or biologic drugs, given as monotherapy or combination therapy; 2) the proportion of patients who required surgery following relapse; 3) the proportion of patients who required hospitalization for CD following relapse; 4) the proportion of patients who developed new CD‐related complications (e.g. fistula, abscesses, strictures) following relapse; 5) the proportion of patients with elevated biomarkers of inflammation (CRP, fecal calprotectin) in those who stop and those who continue therapy; 6) the proportion of patients with anti‐drug antibodies and low serum trough drug levels; 7) time to relapse and 8) the proportion of patients with adverse events, serious adverse events and withdrawal due to adverse events.
Search methods for identification of studies
Electronic searches
The following electronic databases were searched:
1. MEDLINE (Ovid, 1946 to 19 December 2017);
2. EMBASE (Ovid, 1984 to 19 December 2017);
3. CENTRAL; and
4. The Cochrane IBD Group Specialized Register.
The search strategies are listed in Appendix 1. The search was not limited by language, year of publication or type of publication.
Searching other resources
We also searched the reference lists of potentially relevant manuscripts to identify additional studies. Conference proceedings from Digestive Disease Week, the European Crohn's and Colitis Organisation annual meeting, and United European Gastroenterology Week published during the last five years were also searched to identify studies reported in abstract form only. ClinicalTrials.gov was searched to identify ongoing studies.
Data collection and analysis
Selection of studies
Two authors (JT and RB) independently screened titles and abstracts identified by the literature search to determine eligibility based on the inclusion criteria described above. Any disagreements between authors regarding study inclusion were resolved by discussion.
Data extraction and management
A data extraction form was used to collect information from the relevant studies. Two authors (JT and RB) independently extracted data. Consensus regarding data extraction was reached after discussion between authors. The following data were retrieved from the included studies:
1) general information: title, journal, year, publication type;
2) study information: study type, study design, setting, inclusion/exclusion criteria, methods of randomization, concealment of allocation and blinding, study duration, and definitions of remission and relapse;
3) population characteristics: number of participants recruited, total number of patients screened and randomized, total number of participants followed, baseline characteristics (e.g. age, sex, race, disease phenotype, disease duration, concurrent medications; prior medications);
4) intervention characteristics: type and dose of medication discontinued, duration of remission prior to discontinuation, duration of therapy prior to discontinuation;
5) follow‐up (length of follow‐up, withdrawals, number of patients lost to follow‐up); and
5) outcomes: primary and secondary outcomes, as described above.
Assessment of risk of bias in included studies
The methodological quality of each included RCT was independently assessed by two authors (JT and RB) using the Cochrane risk of bias tool (Higgins 2011a). Consensus was reached after discussion between authors on all studies. Factors assessed included:
1) sequence generation (i.e. was the allocation sequence adequately generated?);
2) allocation sequence concealment (i.e. was allocation adequately concealed?);
3) blinding (i.e. was knowledge of the allocated intervention adequately prevented during the study?);
4) incomplete outcome data (i.e. were incomplete outcome data adequately addressed?);
5) selective outcome reporting (i.e. are reports of the study free of suggestion of selective outcome reporting?); and
6) other potential sources of bias (i.e. was the study apparently free of other problems that could put it at high risk of bias?).
Studies will be assigned a low risk of bias, high risk of bias, or unclear risk of bias for each category.
We planned to assess the quality of non‐randomized, cohort studies was assessed using the Newcastle‐Ottawa scale (NOS) (Wells 2017). Factors assessed for cohort studies were:
1) Selection:
a) representativeness of the exposed cohort;
b) selection of the non‐exposed cohort; and
c) ascertainment of exposure.
2) Comparability:
a) comparability of cohorts on the basis of the design or analysis.
3) Outcome:
a) assessment of outcome;
b) appropriate length of follow‐up for outcomes to occur; and
c) adequacy of follow‐up of cohorts.
The quality of the total body of evidence for the primary and secondary outcomes of interest was assessed using the GRADE criteria (Schünemann 2011). Randomized trials are considered high quality and were downgraded due to:
1) risk of bias;
2) indirect evidence;
3) inconsistency (unexplained heterogeneity);
4) imprecision; and
5) publication bias.
The overall quality of evidence for each outcome was classified as high quality (i.e. further research is very unlikely to change our confidence in the estimate of effect); moderate quality (i.e. further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate); low quality (i.e. further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate); or very low quality (i.e. we are very uncertain about the estimate).
Measures of treatment effect
Review Manager (RevMan 5.3.5) was used to analyze data. All data were analyzed on an intention‐to‐treat (ITT) basis. The risk ratio (RR) and corresponding 95% confidence interval (CI) were calculated for dichotomous outcomes. We planned to calculate the mean difference (MD) and corresponding 95% CI for continuous outcomes and the hazard ratio (HR) and corresponding 95% CI using the generic inverse‐variance method for studies reporting the log hazard ratio and standard error for time‐to‐event outcomes.
Unit of analysis issues
When studies reported multiple observations for the same outcome, the outcomes were combined for fixed intervals of follow‐up (e.g. clinical remission at eight weeks). Cross‐over trials were included if data was available from the first phase of the study (i.e. before any cross‐over). Where studies allocated participants to more than one treatment arm, these arms were to be pooled for the primary analysis. Subgroup analyses were to be performed to compare efficacy and safety among different doses of drugs. The primary analysis considered the proportion of patients who experienced at least one efficacy or safety event.
Dealing with missing data
The original study authors were contacted in the case of unclear or missing data. Data that remained missing were considered to be a treatment failure, in accordance with the ITT principle. Where appropriate, sensitivity analyses were conducted to assess the impact of including unclear data on the effect estimate.
Assessment of heterogeneity
Heterogeneity was assessed using the Chi2 test (a P value of 0.10 was considered statistically significant) and the I2 statistic. An I2 value of 25% indicates low heterogeneity, 50% indicates moderate heterogeneity and 75% indicates high heterogeneity (Higgins 2003). We used sensitivity analyses to explore potential explanations for heterogeneity. If the I2 statistic showed a moderate to high degree of heterogeneity and the Chi2 test was statistically significant, forest plots were visually inspected for obvious outliers and sensitivity analysis were performed excluding the outlier to see if this explains the heterogeneity.
Assessment of reporting biases
Potential reporting bias was evaluated by comparing outcomes listed in protocols to published manuscripts. When protocols were not available, we compared outcomes listed in the methods section of published manuscripts to those described in the results section. If a sufficient number of studies are included (i.e. > 10) in the pooled analyses, we planned to investigate potential publication bias using funnel plots (Egger 1997).
Data synthesis
Data from individual trials were combined for meta‐analysis when the interventions, patient groups and outcomes were sufficiently similar (as determined by consensus). The pooled RR and 95% CI were calculated for dichotomous outcomes. For continuous outcomes, we planned to calculate the pooled MD and corresponding 95% CI. The standardized mean difference (SMD) and 95% CI were planned to be calculated when difference scales were used to measure the same outcome. Where studies reported estimates of log hazard ratios and standard errors obtained from Cox proportional hazards regression models, we planned to pool study results using the generic inverse‐variance method to obtain the pooled HR and corresponding 95% CI. Where a mixture of log‐rank and Cox model estimates are obtained from the studies, we planned to convert the log‐rank estimates into log hazard ratios and standard errors (Higgins 2011b). A fixed‐effect model was used to pool data unless heterogeneity exists between the studies. A random‐effects model was employed if heterogeneity existed (I2 50 to 75%). We did not pool data for meta‐analysis if a high degree of heterogeneity (I2 ≥ 75%) was detected.
Subgroup analysis and investigation of heterogeneity
Planned subgroup analyses included: different drug doses and routes of administration and different study designs (RCTs versus observational studies).
Sensitivity analysis
Sensitivity analyses were planned to examine the impact of the following variables on the pooled effect: random‐effects versus fixed‐effect modelling; low risk of bias only versus unclear or high risk of bias; and relevant loss to follow‐up (> 10% versus < 10%).
Results
Description of studies
Results of the search
A literature search conducted on 19 December 2017 identified 10,902 records. After excluding duplicate records, two authors (RB and JT) independently examined the abstracts of 6860 citations to identify eligible studies. Once the non‐applicable studies were excluded, 77 full‐text articles were assessed (Figure 1). A total of 67 of these records were excluded with reasons (see Characteristics of excluded studies). Eight reports of six studies that enrolled a total of 326 CD patients were determined to be eligible for inclusion in the review (Lémann 2005; O'Donoghue 1978; Roblin 2017; Van Assche 2008; Vilien 2004; Wenzl 2015; See Characteristics of included studies). Two ongoing studies were also identified (NCT01817426; NCT02177071). Four of the six included studies were RCTs in which immunosuppressant monotherapy (i.e. azathioprine) was discontinued (Lémann 2005; O'Donoghue 1978; Vilien 2004; Wenzl 2015). Two RCTs evaluated azathioprine withdrawal in patients who had achieved remission with azathioprine and infliximab combination therapy (Roblin 2017; Van Assche 2008). No studies of biologic monotherapy withdrawal were eligible for inclusion.

Study flow diagram.
Included studies
Roblin 2017 was an open‐label randomized trial that followed three cohorts of patients with inflammatory bowel disease (N = 81; 45 patients with CD) who had been treated with azathioprine and infliximab combination therapy for at least one year. These patients were in deep remission for at least six months. In cohort A patients continued to receive a stable dose of combination therapy; in cohort B, the initial azathioprine dose was reduced by half; and in cohort C, azathioprine therapy was completely withdrawn while the initial infliximab dose remained stable. The primary outcome was clinical relapse as defined by a Crohn's Disease Activity Index (CDAI) > 220 with an increase in CDAI of greater than 70 points from the previous assessment or need to change the original therapeutic regimen because of adverse events or drug intolerance.at 12 months. Patients with CD from cohorts A and C (n = 31) were included in this review.
Lémann 2005 was a non‐inferiority placebo‐controlled double‐blind RCT in which 83 patients with quiescent CD who had received azathioprine for at least 42 months were allocated to either continue azathioprine (n = 40) or switch to placebo (n = 43). The primary outcome was clinical relapse (as defined by a CDAI score between 150 and 250 for 3 consecutive weeks with an increase of at least 75 points above baseline value, or the need for CD‐related surgery except for limited perianal surgery) at 18 months.
O'Donoghue 1978 was a placebo‐controlled double‐blind trial in which 51 CD patients who achieved clinical remission after receiving at least 6 months of azathioprine monotherapy were randomized to continue azathioprine (n = 27) or switch to placebo (n = 24). The primary outcome was clinical relapse (defined as a significant deterioration in clinical state requiring a change in treatment as judged by two blinded physicians) at 12 months.
In Van Assche 2008, 80 patients who were in clinical remission and had received combination (azathioprine and infliximab) therapy for more than 6 months were randomized to either discontinue (n = 40) or continue (n = 40) azathioprine. The primary outcome was the proportion of patients who required a change in the infliximab dosing interval or stopped infliximab therapy. Patients were followed for 104 weeks.
Vilien 2004 was an open‐label RCT in which 29 CD patients were randomized to continue (n = 14) or stop (n = 15) azathioprine monotherapy. The patients had received azathioprine for at least two years and were in clinical remission at the time of withdrawal. The primary outcome was clinical relapse (as defined as a CDAI rise of greater or equal to 75 points and a total CDAI of at least 150, or, disease activity necessitating intervention) at month 12.
Wenzl 2015 was a placebo‐controlled double‐blind trial in which 52 CD patients in stable remission for at least 42 months and a minimum four‐year treatment history with azathioprine were randomized to continue azathioprine therapy (n = 26) or switch to placebo (n = 26). The primary outcome was clinical relapse at week 24, defined as either: a) a CDAI score greater than 150 with an increase of at least 60 points above the baseline CDAI score in the absence of infectious diarrhea; b) the development of at least one new fistula in patients who were fistula‐free prior to trial enrolment; c) an increase of four or more Perianal Disease Activity Index points compared to baseline; d) disease activity necessitating therapy with oral corticosteroids or anti‐TNF‐α drugs; e) the need for CD‐related abdominal or perianal surgery).
Excluded studies
Sixty‐seven reports were excluded during the screening process (See Characteristics of excluded studies). One study was excluded because it was a case report (Begun 2016). Helwig 2017 was excluded because it was a review article. Two letters were excluded (Benitez 2015; Chaparro 2015). Two of the reports described studies in which an immunosuppressant or biologic drug, or combination therapy, was reduced in dose rather than being completely withdrawn (Amiot 2016; Paul 2015). In three studies patients did not receive maintenance therapy for the minimum six‐month duration prior to therapy withdrawal (Feagan 2015a; Feagan 2015b; Rismo 2013). A total of nine reports exclusively enrolled pediatric patients (Crombe 2010a; Crombe 2010b; Crombe 2011; Grossi 2015b; Kang 2016; Kierkus 2015; Nuti 2010a; Nuti 2010b; Wynands 2008), and in one study CD specific data were not available (de Lima 2016). Sixteen studies were of a retrospective design and therefore did not met the inclusion criteria (Bouhnik 1996; Chauvin 2014; Domenech 2005; Fischer 2014; Gallego 2015; Hlavaty 2016b; Iborra 2016a; Iborra 2016b; Iimuro 2011; Kennedy 2016; Kim 1999; Monterubbianesi 2015; Monterubbianesi 2016a; Monterubbianesi 2016b; Waugh 2010a; Waugh 2010b). The most common reason for exclusion was the lack of a control group (i.e. a group of patients who continued to receive drug therapy), with 32 studies falling into this category (Bodini 2015; Bortlik 2015a; Bortlik 2015b; Bortlik 2016; Bots 2016a; Bots 2016b; Brooks 2017; Chen 2015a; Chen 2015b; Cortes 2016; Dai 2014; De Suray 2012a; De Suray 2012b; Duricová 2015; Echarri 2013; Farkas 2014; Grossi 2015a; Helwig 2016; Louis 2012; Molander 2014; Molander 2015; Molander 2016; Molnar 2013; Qiu 2015a; Qiu 2015b; Schnitzler 2009; Seirafi 2011a; Seirafi 2011b; Squires 2015; Thomsen 2015; Treton 2009; Zelinkova 2013).
Risk of bias in included studies
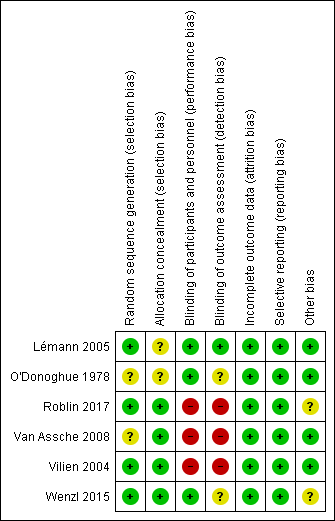
The Cochrane risk of bias analysis is summarized in Figure 2.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Four of the included RCTs were rated as low risk of bias (Lémann 2005; Roblin 2017; Vilien 2004; Wenzl 2015), and two were rated as unclear risk of bias with respect to random sequence generation (O'Donoghue 1978; Van Assche 2008). O'Donoghue 1978 reported that the treatment groups were randomly divided, but it is unclear how this was performed. Similarly, Van Assche 2008 does not clearly describe the randomization process.
Four of the included RCTs were rated as low risk of bias (Roblin 2017; Van Assche 2008; Vilien 2004; Wenzl 2015), and two were rated as unclear risk of bias (Lémann 2005; O'Donoghue 1978) with respect to allocation concealment (Lémann 2005; O'Donoghue 1978). Both Lémann 2005 and O'Donoghue 1978 fail to report sufficient detail regarding the method used to ensure that the individual performing the randomization was unaware of the next treatment assignment.
Blinding
Three of the included RCTs were rated as low risk of bias (Lémann 2005; O'Donoghue 1978; Wenzl 2015), and the remaining three studies were rated as high risk of bias with respect to blinding of participants and personnel (Roblin 2017; Van Assche 2008; Vilien 2004). Due to the open‐label design utilized in three studies no placebo was used and as such participants and personnel were aware of treatment assignment (Roblin 2017; Van Assche 2008; Vilien 2004).
With respect to blinding of outcome assessors, two of the RCTs were rated as unclear risk of bias (O'Donoghue 1978; Wenzl 2015), three were rated as high risk of bias (Roblin 2017; Van Assche 2008; Vilien 2004), and one was rated as low risk of bias (Lémann 2005). In Lémann 2005, biological tests results were reviewed by co‐investigators who were blinded to clinical information and the endoscopist was responsible for independently calculating the Crohn's Disease Endoscopic Index of Severity score. Blinded outcome assessment was not performed in three studies (Roblin 2017; Van Assche 2008; Vilien 2004).
Incomplete outcome data
All six RCTs were rated as low risk of bias for incomplete outcome data (Lémann 2005; O'Donoghue 1978; Roblin 2017; Van Assche 2008; Vilien 2004; Wenzl 2015).
Selective reporting
All six RCTs were rated as low risk of bias for selective reporting (Lémann 2005; O'Donoghue 1978; Roblin 2017; Van Assche 2008; Vilien 2004; Wenzl 2015).
Other potential sources of bias
Four of the five RCTs were rated as low risk of bias for other potential sources of bias (Lémann 2005; O'Donoghue 1978; Van Assche 2008; Vilien 2004). Wenzl 2015 and Roblin 2017 received an unclear rating for this factor since the trials were prematurely stopped due to slow enrolment.
Effects of interventions
See: Summary of findings for the main comparison Usual care compared to immunosuppressive withdrawal after monotherapy for patients with quiescent Crohn's disease; Summary of findings 2 Usual care compared to immunosuppressive withdrawal after combination therapy for patients with quiescent Crohn's disease
Withdrawal of immunosuppressant monotherapy
The proportion of patients who relapse following discontinuation
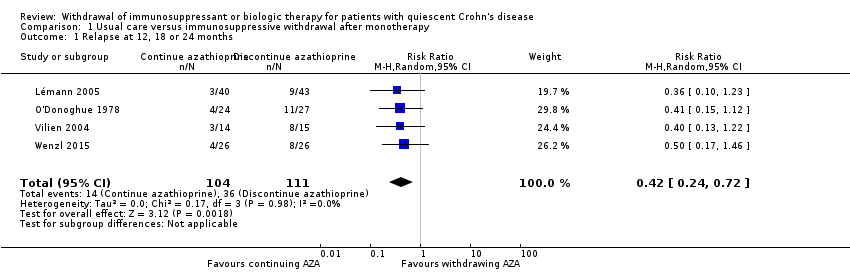
Four RCTs with a total of 215 participants provided data on the rate of clinical relapse following the discontinuation of azathioprine monotherapy (Lémann 2005; O'Donoghue 1978; Vilien 2004; Wenzl 2015). The follow‐up period was 12 months for two studies (O'Donoghue 1978, Vilien 2004), 18 months for one study (Lémann 2005) and 24 months for one study (Wenzl 2015). A total of 32.4% (36/111) participants assigned to azathioprine withdrawal experienced clinical relapse compared to 13.5% (14/104) patients assigned to therapeutic continuation. The pooled RR for the primary outcome was 0.42 (95% CI 0.24 to 0.72, P = 0.002, I² = 0%), indicating a statistically significant benefit in favour of continuing azathioprine monotherapy (Analysis 1.1). The GRADE analysis indicated that the overall quality of evidence for the primary outcome (clinical relapse) for placebo‐controlled studies was low due to high risk of bias for blinding in one study (Vilien 2004), unclear risk of bias in three studies (Lémann 2005; O'Donoghue 1978; Wenzl 2015) and sparse data (see summary of findings Table for the main comparison).
The proportion of patients with new CD‐related complications (e.g. fistula, abscesses, strictures) following discontinuation
Two RCTs with a total of 135 participants provided data on the proportion of patients with new CD‐related complications following the discontinuation of azathioprine monotherapy (Lémann 2005; Wenzl 2015). A total of 5.8% (4/69) patients in the monotherapy withdrawal group experienced a new CD‐related complication compared to 1.5% (1/66) participants in the monotherapy continuation group. The pooled RR demonstrated no statistically significant difference between the two groups (RR 0.34, 95% CI 0.06 to 2.08, P = 0.24; I² = 0%; Analysis 1.2). The GRADE analysis indicated that the overall quality of evidence for this outcome was very low due to unclear risk of bias and very sparse data (see summary of findings Table for the main comparison).
The proportion of patients with adverse events following discontinuation
Three trials with a total of 186 participants provided data on the proportion of patients who experienced an adverse event following discontinuation of azathioprine monotherapy (Lémann 2005; O'Donoghue 1978; Wenzl 2015). A total of 24.0% (23/96) of participants randomized to discontinue therapy versus 24.4% (22/90) participants randomized to continue therapy experienced an adverse event during the observation period. The pooled RR was 0.88 (95% CI 0.67 to 1.17, P = 0.39; I² = 0%) showing no statistically significant difference between the withdrawal and continuation groups (Analysis 1.3).The GRADE analysis indicated that the overall quality of evidence for this outcome was low due to sparse data and unclear risk of bias (see summary of findings Table for the main comparison). Common adverse events included infections, mild leukopenia, abdominal symptoms, arthralgias, headache and elevated liver enzymes.
The proportion of patients with serious adverse events following discontinuation
Two trials (N = 134) provided data on the proportion of patients with serious adverse events following discontinuation of azathioprine monotherapy (Lémann 2005; O'Donoghue 1978 ). A total of 0% (0/70) of participants who discontinued therapy versus 3.1% (2/64) of participants who continued therapy experienced a serious adverse event during the observation period. The pooled RR was 3.29 (95% CI 0.35 to 30.80, P = 0.30; I² = 0%) and demonstrated no statistically significant difference between treatment groups (Analysis 1.4). The GRADE analysis indicated that the quality of evidence for this outcome was very low due to unclear risk of bias and very sparse data (see summary of findings Table for the main comparison). The two serious adverse events included myelodysplastic syndrome (Lémann 2005), and pancytopenia (O'Donoghue 1978).
The proportion of patients who withdraw due to adverse events following discontinuation
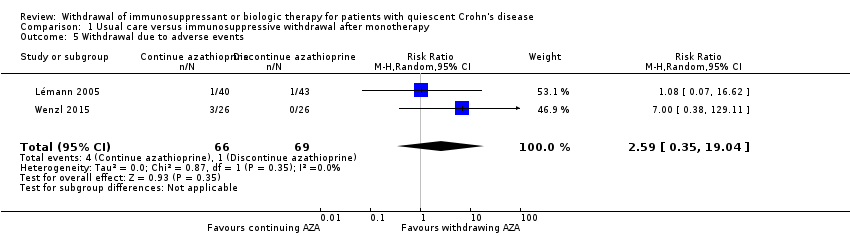
Two trials with a total of 135 participants provided data on the proportion of patients who withdrew due to adverse events following discontinuation of azathioprine monotherapy (Lémann 2005; Wenzl 2015). A total of 1.4% (1/69) of participants randomized to therapeutic discontinuation versus 6.0% (4/66) of participants randomized to therapeutic continuation withdrew from the study due to an adverse event. The pooled RR of 2.59 (95% CI 0.35 to 19.04, P = 0.35; I² = 0%) failed to demonstrate a statistically significant difference between azathioprine monotherapy discontinuation compared to continuation (Analysis 1.5). The GRADE analysis indicated that the quality of evidence for this outcome was very low due to unclear risk of bias and very sparse data (see summary of findings Table for the main comparison).
Other outcomes
There were no data available to assess between‐group differences in: time to relapse; the proportion of patients who responded to the reintroduction of immunosuppressant monotherapy; the proportion of patients with elevated biomarkers of inflammation; the proportion of patients with anti‐drug antibodies and low serum trough drug levels; the proportion of patients who required surgery following relapse; or the proportion of patients who required hospitalization following relapse.
Withdrawal of anti‐TNF‐α monotherapy or other biologics
None of the included studies examined withdrawal of anti‐TNF‐α monotherapy, or withdrawal of other biologics used in Crohn's disease.
Withdrawal of immunosuppressant from combination therapy
Proportion of patients who relapse following discontinuation of immunosuppressant from combination therapy
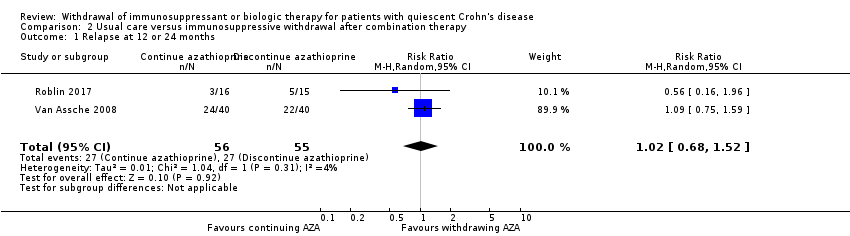
Two studies (Roblin 2017; Van Assche 2008), reported on the proportion of patients who relapsed following discontinuation of an immunosuppressant from combination therapy (N = 111). The follow‐up period was 12 months for one study (Roblin 2017), and 24 months for one study (Van Assche 2008). When data from these studies were combined, a total of 49% (27/55) of patients who were withdrawn from azathioprine (but continued to receive infliximab) experienced clinical relapse compared to 48% (27/56) of patients who continued combination therapy with both azathioprine and infliximab. The pooled RR revealed no statistically significant difference between groups (RR 1.02, 95% CI 0.68 to 1.52, P = 0.92, I2 = 4%; (Analysis 2.1). The GRADE analysis indicated that the quality of evidence for this outcome was low due to high risk of bias for blinding and sparse data (see summary of findings Table 2).
The proportion of patients with adverse events following discontinuation of immunosuppressant from combination therapy
Two RCTs (Roblin 2017; Van Assche 2008), reported on the proportion of patients who experienced an adverse event following discontinuation of an immunosuppressant from combination therapy (N = 111). When data were pooled, 45% (25/55) of patients who were withdrawn from azathioprine (but continued to receive infliximab) experienced an adverse event compared to 46% (26/56) of patients who continued combination therapy with both azathioprine and infliximab. The pooled RR revealed no statistically significant difference between groups (RR 1.11, 95% CI 0.44 to 2.81, P = 0.83, I2 = 16%; Analysis 2.2). Likewise, the RR in each type of study neither revealed no differences between groups (RR 1.09, 95% CI 0.75 to 1.59, in the RCT (Van Assche 2008); and RR of 0.56, 95% CI 0.16 to 1.96 in the observational study (Roblin 2017)). The GRADE analysis indicated that the quality of evidence for this outcome was low due to high risk of bias for blinding and sparse data (see summary of findings Table 2). Common adverse events included infections, liver test elevations, arthralgias and infusion reactions.
The proportion of patients with serious adverse events following discontinuation of immunosuppressant from combination therapy
One study (Van Assche 2008) reported on the proportion of patients who experienced a serious adverse event following discontinuation of an immunosuppressant from combination therapy (N = 80). In both the azathioprine discontinuation and continuation groups, 0.07% (3/40) of patients experienced a serious adverse event. Thus, there was no statistically significant between‐group difference (RR 1.00, 95% CI 0.21 to 4.66; Analysis 2.3). The GRADE analysis indicated that the quality of evidence for this outcome was very low due to high risk of bias for blinding and very sparse data (see summary of findings Table 2). Serious adverse events in the azathioprine discontinuation group include appendectomy (n = 1), skin carcinoma (n = 1), and ureterolithiasis (n = 1). Serious adverse events in group that continued combination therapy include pregnancy (n = 1), pneumonia (n = 1) and partial colectomy (n =1).
Other outcomes
There were no data available to assess between‐group differences in: time to relapse; the proportion of patients who experienced a CD‐related complication; the proportion of patients who responded to the reintroduction of immunosuppressant monotherapy; the proportion of patients with elevated biomarkers of inflammation; the proportion of patients with anti‐drug antibodies and low serum trough drug levels; the proportion of patients who required surgery following relapse; the proportion of patients who required hospitalization following relapse; or the proportion of patients who withdrew from the study due to adverse events.
Withdrawal of an anti‐TNF‐αagent from combination therapy
None of the included studies examined withdrawal of an anti‐TNF‐α agent from a combination therapy regimen.
Due to the small number of included studies and limited data, pre‐specified sensitivity analyses to assess the impact of risk of bias were not performed. Sensitivity analyses to examine the impact of using random effects versus fixed effect modelling were performed; the results are presented in Table 1. The application of fixed effect modelling had no or minimal change on the point estimates for all comparisons.
| Comparison 1: Usual care versus immunosuppressive withdrawal after monotherapy | |||
| Outcome | Random Effects RR (95% CI) | Fixed Effect RR (95% CI) | Impact |
| 1.1 Relapse at 12, 18 or 24 months | 0.42 (0.24‐0.72) | 0.42 (0.24‐0.72) | No change |
| 1.2 New CD‐related complications | 0.34 (0.06‐2.08) | 0.34 (0.06‐2.08) | No change |
| 1.3 Adverse events | 0.88 (0.67‐1.17) | 0.97 (0.71‐1.32) | Minimal |
| 1.4 Serious adverse events | 3.29 (0.35‐30.80) | 3.29 (0.35‐30.80) | No change |
| 1.5 Withdrawal due to adverse events | 2.59 (0.35‐19.04) | 3.10 (0.49‐19.41) | Minimal |
| Comparison 2: Usual care versus Immunosuppressive withdrawal after combination therapy | |||
| Outcome | Random Effects RR (95% CI) | Fixed Effect RR (95% CI) | |
| 2.1 Relapse at 12 or 24 months | 1.02 (0.68‐1.52) | 0.99 (0.69‐1.43) | Minimal |
| 2.2 Adverse events | 1.11 (0.44‐2.81) | 1.04 (0.73‐1.47) | Minimal |
| 2.3 Serious adverse events | No pooling | No pooling | No pooling |
Discussion
Summary of main results
Six RCTs enrolling a total of 326 patients were identified by the literature search and met the criteria for inclusion for this review (Lémann 2005; O'Donoghue 1978; Roblin 2017; Van Assche 2008; Vilien 2004; Wenzl 2015).
Immunosuppressant monotherapy withdrawal
Our primary results suggest that patients with quiescent CD who continue azathioprine monotherapy may be less likely to experience clinical relapse compared to those who discontinue azathioprine therapy (RR 0.42, 95% CI 0.24 to 0.72, P = 0.002). However, these results should be interpreted with caution, since GRADE analysis revealed that the quality of evidence was low due to high risk of bias for blinding and sparse data. Furthermore, it is important to note that none of the studies were performed specifically for patients in 'deep remission' (clinical, biochemical and endoscopic remission).
No statistically significant between‐group differences were observed regarding the secondary outcomes. However, the quality of evidence supporting these findings ranges from very low to low , indicating the further research may impact on our confidence in the estimate of effect, and may ultimately change the estimate.
Immunosuppressant withdrawal from combination therapy
Two RCTs evaluated the withdrawal of azathioprine from a combination therapy regimen in patients with inactive CD (Roblin 2017; Van Assche 2008). These studies reported on the proportion of patients who relapsed and the proportion of patients who experienced an adverse event. Pooled and separate analyses were conducted, revealing with no statistical significant differences between the discontinuation and continuation groups. The overall quality of evidence was low, indicating that further research may impact on the confidence in the estimate of effect, and may ultimately change the estimate.
Van Assche 2008 was the only study to both evaluate the withdrawal of azathioprine from a combination therapy regimen and report on the proportion of patients with serious adverse events. No statistically significant difference was observed between treatment groups. The overall quality of evidence supporting this outcome was rated as very low. Thus, our confidence in the estimate of effect is limited. It should be noted that Van Assche 2008 was designed as a superiority study, with continued azathioprine therapy assumed to be superior to discontinued azathioprine therapy. This study was not adequately powered to detect non‐inferiority between the withdrawal and control groups.
Overall completeness and applicability of evidence
An exhaustive literature search was performed to identify potential included studies, and handsearching was performed to ensure that no eligible reports were missed. Unfortunately, several of our pre‐specified secondary outcomes of interest were not addressed in the included studies. There were no data on time to relapse; the proportion of patients who responded to immunosuppressant reintroduction; the proportion of patients with elevated biomarkers of inflammation; the proportion of patients with anti‐drug antibodies and low serum trough levels; the proportion of patients requiring surgery due to relapse; and the proportion of patients requiring hospitalization due to relapse in any of the included studies. Furthermore, the literature search failed to identify any controlled data regarding the withdrawal of anti‐TNF‐α therapy (as part of either a monotherapy or combination therapy regimen) in CD patients with inactive disease.
All of the included studies evaluated azathioprine monotherapy, or a combination therapy administered using azathioprine and infliximab, which may limit the applicability of the results of this systematic review to these specific medications. The findings of this systematic review are confined to patients in remission at the time of drug withdrawal. It is worth emphasizing that there were variations between included studies in the definition of remission and length of remission prior to drug withdrawal (summarized in Table 2).
| Study | Length of remission prior to drug withdrawal | Definition of remission prior to drug withdrawal |
| Minimum 6 months | CDAI ≤ 150 and fecal calprotectin levels < 250 μg/g | |
| Mean 62 months (standard deviation 26 months); Minimum 42 months | Clinical remission (CDAI ≤ 150) and no need for medical/surgical therapy in the previous 42 months | |
| Minimum 6 months | Clinical remission not otherwise specified | |
| Minimum 6 months | Clinical response to infliximab and disease control | |
| Not specified | Clinical remission: physician's global assessment | |
| Minimum 12 months | Clinical remission, no need for new medical therapy in the previous 12 months |
Both studies evaluating the withdrawal of azathioprine from a combination therapy regimen (Roblin 2017; Van Assche 2008) are likely to have had patient groups comprised primarily of those who had previously failed immunosuppressant monotherapy. It could be argued that in this cohort, the subsequent withdrawal of this agent would not be expected to have a significant effect (compared to, for example, a patient cohort in which patients initially commenced combination therapy and then had their immunosuppressant withdrawn).
The literature search did not identify any controlled studies of anti‐TNF‐α withdrawal, however it should be noted that the STORI trial, a relatively large, uncontrolled, prospective cohort study (N = 115) examined infliximab withdrawal from a combination therapy regimen in patients with quiescent CD (Louis 2012). Details pertaining to this study are listed in the Characteristics of excluded studies.
Quality of the evidence
The Cochrane risk of bias tool was used to assess the risk of bias of the included RCTs. Three of the RCTs received an unclear risk of bias rating for items including random sequence generation (O'Donoghue 1978), allocation concealment (Lémann 2005; O'Donoghue 1978), blinding of outcome assessors (O'Donoghue 1978; Wenzl 2015), and other bias (Wenzl 2015). Three of the RCTs were open‐label trials, and therefore received a high risk of bias rating for blinding of study participants and personnel (Roblin 2017; Van Assche 2008; Vilien 2004), while the remaining three RCTs received a low risk of bias rating for this factor. With regard to blinding of outcome assessors, three RCTs received a high risk of bias rating (Roblin 2017; Van Assche 2008; Vilien 2004), and one RCT received a low risk of bias rating (Lémann 2005). All six RCTs received low risk of bias ratings for incomplete outcome data and selective reporting (see Figure 2).
The overall quality of evidence supporting each outcome was assessed using the GRADE approach. As described in the Summary of findings table 2, the GRADE assessments for immunosuppressive monotherapy withdrawal compared to continuation ranged from very low (i.e. we are very uncertain about the estimate) to low (i.e. the true effect may be substantially different from the estimate of effect).
The GRADE assessments for immunosuppressive withdrawal from combination therapy compared to uninterrupted combination therapy are described in the Summary of findings table 2. Quality assessments ranged from very low (i.e. we are very uncertain about the estimate) to low (i.e. the true effect may be substantially different from the estimate of effect).
Potential biases in the review process
The methods and reporting structure employed for this systematic review were based on recommendations provided by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011c). A comprehensive literature search was developed and conducted, and the protocol was published in advance to facilitate transparency. The literature screening and data extraction were independently performed by two authors, and the quality of included studies and evidence was rigorously assessed. However, there are some potential limitations of the current systematic review. First, few additional data were obtained from unpublished sources. While we planned to investigate the possibility of publication bias using funnel plots, this was prevented by the insufficient number of included studies (i.e. less than 10 studies). Second, definitions of clinical relapse varied across studies; however, it should be noted that high statistical heterogeneity was not detected. Third, during the review execution there were some deviations from the published protocol. These derivations are transparently reported, and we feel they are unlikely to change our conclusions (see Differences between protocol and review).
Agreements and disagreements with other studies or reviews
The available evidence on cessation of immunosuppressant and anti‐TNF‐α drug therapy in patients with inactive CD has been systematically reviewed in six other reviews (Doherty 2018; French 2011; Gisbert 2016; Kennedy 2016; Pariente 2014; Torres 2015).
Doherty 2018 is a topical review, on the withdrawal of treatment in inflammatory bowel disease. This review summarizes expert opinions and was published by the European Crohn's and Colitis Organisation. It is stated that a systematic review of the literature was conducted, however the search date and search strategy were not reported. No risk of bias or quality assessments were performed, nor were the data meta‐analyzed. The authors conclude that a) there is a strong rationale for ceasing or de‐escalating immunosuppressant and anti‐TNF‐α therapy, particularly when used together in a combination regimen; b) CD patients who are withdrawn from drug therapy should be in clinical, biochemical and endoscopic remission and at low risk for relapse; and c) the decision to stop therapy should be based on the individual patient. It is also noted that further evidence from RCTs on the withdrawal of drug therapy is needed.
French 2011 is a systematic review and meta‐analysis that evaluated the impact of azathioprine withdrawal on the rate of relapse in CD patients with inactive disease. The literature search was conducted in September 2010, and a total of five studies, three RCTs (Lémann 2005; O'Donoghue 1978; Vilien 2004), and two retrospective cohort studies were included (Kim 1999; Sokol 2010). The authors conclude that immunosuppressant (i.e. azathioprine and 6‐mercaptopurine) continuation is more effective than withdrawal for remission of Crohn's disease. The current study differs from French 2011 in that three additional RCTs (Roblin 2017; Van Assche 2008; Wenzl 2015), were identified and included, and no retrospective data were included (Kim 1999; Sokol 2010).
Torres 2015 is a systematic review focused on the withdrawal of immunosuppressants or biologics in patients with quiescent CD or ulcerative colitis. A total of 7 RCTs, 16 prospective cohort studies and 43 retrospective cohort studies were deemed eligible for inclusion. Two of the RCTs, and 15 of the prospective cohort studies and all retrospective cohort studies were not included in the current review because the study population was not of interest (i.e. ulcerative colitis, pregnant and pediatric patients) or there was no control group. No meta‐analyses were performed. The authors conclude that disease activity, prognostic factors and complicated disease were associated with future relapse, and that approximately 50% of inflammatory bowel disease patients who discontinue therapy relapse. They also state that the cessation of drug therapy is a decision that should be made based on the individual patient.
Pariente 2014 performed a systematic literature review to identify studies evaluating the cessation of immunosuppressants or anti‐TNF‐α agents in inflammatory bowel disease patients. Studies that employed a retrospective design, lacked a control group, and exclusively enrolled ulcerative colitis patients met the eligibility criteria. A total of 11 relevant studies were identified, including one of the five RCTs included in the current systematic review (Van Assche 2008). No risk of bias assessments or meta‐analyses were performed. The authors conclude that therapeutic de‐escalation should be initiated on a case‐by‐case basis.
Gisbert 2016 performed a systematic literature review and meta‐analysis of studies evaluating the risk of relapse after discontinuation of anti‐TNF‐α therapy in clinically quiescent CD or ulcerative colitis. In contrast to the current review, studies that employed a retrospective design or lacked a control group, and those enrolling patients with ulcerative colitis met the eligibility criteria. The authors conclude that approximately one‐third of patients with inflammatory bowel disease relapsed after one year of discontinuing anti‐TNF‐α therapy, and this proportion increased to about one‐half in the longer term.
Kennedy 2016 performed a systematic literature review and meta‐analysis of studies assessing outcomes following anti‐TNF‐α withdrawal in patients with inflammatory bowel disease in clinical remission. This review included studies that employed a retrospective design or lacked a control group. The authors conclude that approximately one‐third of patients with IBD flare within one year of withdrawal of anti‐TNF‐α therapy.

Study flow diagram.
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Comparison 1 Usual care versus immunosuppressive withdrawal after monotherapy, Outcome 1 Relapse at 12, 18 or 24 months.

Comparison 1 Usual care versus immunosuppressive withdrawal after monotherapy, Outcome 2 New CD‐related complications.

Comparison 1 Usual care versus immunosuppressive withdrawal after monotherapy, Outcome 3 Adverse events.

Comparison 1 Usual care versus immunosuppressive withdrawal after monotherapy, Outcome 4 Serious adverse events.
Comparison 1 Usual care versus immunosuppressive withdrawal after monotherapy, Outcome 5 Withdrawal due to adverse events.
Comparison 2 Usual care versus immunosuppressive withdrawal after combination therapy, Outcome 1 Relapse at 12 or 24 months.

Comparison 2 Usual care versus immunosuppressive withdrawal after combination therapy, Outcome 2 Adverse events.
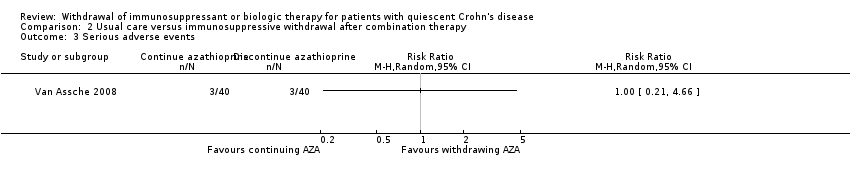
Comparison 2 Usual care versus immunosuppressive withdrawal after combination therapy, Outcome 3 Serious adverse events.
| Usual care compared to immunosuppressive withdrawal after monotherapy for patients with quiescent Crohn's disease | ||||||
| Patient or population: Patients with quiescent Crohn's disease | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
| Risk with immunosuppressive withdrawal after monotherapy | Risk with usual care | |||||
| Relapse at 12, 18 or 24 months | Study population | RR 0.42 | 215 | ⊕⊕⊝⊝ | Sparse data (50 events) | |
| 324 per 1,000 | 136 per 1,000 | |||||
| New CD‐related complications | Study population | RR 0.34 | 135 | ⊕⊝⊝⊝ | Very sparse data (5 events) | |
| 58 per 1,000 | 20 per 1,000 | |||||
| Adverse events | Study population | RR 0.88 | 186 | ⊕⊕⊝⊝ | Sparse data (45 events) | |
| 240 per 1,000 | 211 per 1,000 | |||||
| Serious adverse events | Study population | RR 3.29 | 134 | ⊕⊝⊝⊝ | Very sparse data (2 events) | |
| 0 per 1,000 | 0 per 1,000 | |||||
| Withdrawal due to adverse events | Study population | RR 2.59 | 135 | ⊕⊝⊝⊝ | Very sparse data (5 events) | |
| 14 per 1,000 | 38 per 1,000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded one level due to high risk of bias for blinding in one study and unclear risk of bias in three studies in the pooled analysis 2 Downgraded one level due to sparse data 3 Downgraded one level due to unclear risk of bias in the two studies in the pooled analysis 4 Downgraded two levels due to very sparse data 5 Downgraded one level due to unclear risk of bias in the three studies in the pooled analysis | ||||||
| Usual care compared to immunosuppressive withdrawal after combination therapy for patients with quiescent Crohn's disease | ||||||
| Patient or population: Patients with quiescent Crohn's disease | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
| Risk with immunosuppressive withdrawal after combination therapy | Risk with usual care | |||||
| Relapse at 12 or 24 months | Study population | RR 1.02 | 111 | ⊕⊕⊝⊝ | Sparse data (54 events) | |
| 491 per 1,000 | 501 per 1,000 | |||||
| Adverse events | Study population | RR 1.11 | 111 | ⊕⊕⊝⊝ | Sparse data (51 events) | |
| 455 per 1,000 | 505 per 1,000 | |||||
| Serious adverse events | Study population | RR 1.00 | 80 | ⊕⊝⊝⊝ | Very sparse data (6 events) | |
| 75 per 1,000 | 75 per 1,000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded one level due to high risk of bias for blinding 2 Downgraded one level due to sparse data 3 Downgraded two levels due to very sparse data | ||||||
| Comparison 1: Usual care versus immunosuppressive withdrawal after monotherapy | |||
| Outcome | Random Effects RR (95% CI) | Fixed Effect RR (95% CI) | Impact |
| 1.1 Relapse at 12, 18 or 24 months | 0.42 (0.24‐0.72) | 0.42 (0.24‐0.72) | No change |
| 1.2 New CD‐related complications | 0.34 (0.06‐2.08) | 0.34 (0.06‐2.08) | No change |
| 1.3 Adverse events | 0.88 (0.67‐1.17) | 0.97 (0.71‐1.32) | Minimal |
| 1.4 Serious adverse events | 3.29 (0.35‐30.80) | 3.29 (0.35‐30.80) | No change |
| 1.5 Withdrawal due to adverse events | 2.59 (0.35‐19.04) | 3.10 (0.49‐19.41) | Minimal |
| Comparison 2: Usual care versus Immunosuppressive withdrawal after combination therapy | |||
| Outcome | Random Effects RR (95% CI) | Fixed Effect RR (95% CI) | |
| 2.1 Relapse at 12 or 24 months | 1.02 (0.68‐1.52) | 0.99 (0.69‐1.43) | Minimal |
| 2.2 Adverse events | 1.11 (0.44‐2.81) | 1.04 (0.73‐1.47) | Minimal |
| 2.3 Serious adverse events | No pooling | No pooling | No pooling |
| Study | Length of remission prior to drug withdrawal | Definition of remission prior to drug withdrawal |
| Minimum 6 months | CDAI ≤ 150 and fecal calprotectin levels < 250 μg/g | |
| Mean 62 months (standard deviation 26 months); Minimum 42 months | Clinical remission (CDAI ≤ 150) and no need for medical/surgical therapy in the previous 42 months | |
| Minimum 6 months | Clinical remission not otherwise specified | |
| Minimum 6 months | Clinical response to infliximab and disease control | |
| Not specified | Clinical remission: physician's global assessment | |
| Minimum 12 months | Clinical remission, no need for new medical therapy in the previous 12 months |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Relapse at 12, 18 or 24 months Show forest plot | 4 | 215 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.24, 0.72] |
| 2 New CD‐related complications Show forest plot | 2 | 135 | Risk Ratio (M‐H, Random, 95% CI) | 0.34 [0.06, 2.08] |
| 3 Adverse events Show forest plot | 3 | 186 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.67, 1.17] |
| 4 Serious adverse events Show forest plot | 2 | 134 | Risk Ratio (M‐H, Random, 95% CI) | 3.29 [0.35, 30.80] |
| 5 Withdrawal due to adverse events Show forest plot | 2 | 135 | Risk Ratio (M‐H, Random, 95% CI) | 2.59 [0.35, 19.04] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Relapse at 12 or 24 months Show forest plot | 2 | 111 | Risk Ratio (M‐H, Random, 95% CI) | 1.02 [0.68, 1.52] |
| 2 Adverse events Show forest plot | 2 | 111 | Risk Ratio (M‐H, Random, 95% CI) | 1.11 [0.44, 2.81] |
| 3 Serious adverse events Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |