Rehabilitación después de la cirugía por lesiones del tendón flexor de la mano
Resumen
Antecedentes
Se pueden ofrecer varios tratamientos de rehabilitación después de una cirugía para las lesiones del tendón flexor de la mano. La rehabilitación suele incluir una combinación de un régimen de ejercicios y una ortesis, además de otros tratamientos de rehabilitación, que se suelen administrar juntos. La efectividad de esas intervenciones sigue sin estar clara.
Objetivos
Evaluar los efectos (beneficiosos y perjudiciales) de diferentes intervenciones de rehabilitación después de la cirugía para las lesiones del tendón flexor de la mano.
Métodos de búsqueda
Se realizaron búsquedas en el Registro Cochrane Central de ensayos controlados (Cochrane Central Register of Controlled Trials), en el Registro especializado del Grupo Cochrane de Lesiones óseas, articulares y musculares (Cochrane Bone, Joint and Muscle Trauma Group), en MEDLINE, en Embase, en dos bases de datos adicionales y en dos registros de ensayos internacionales, sin restricciones de idioma. La última fecha de búsqueda fue el 11 de agosto de 2020. También se buscó en las listas de referencias de los estudios incluidos y en las revisiones sistemáticas relevantes.
Criterios de selección
Se incluyeron los ensayos controlados aleatorizados (ECA) y cuasialeatorizados que compararon cualquier intervención de rehabilitación posoperatoria con ninguna intervención, control, placebo u otra intervención de rehabilitación posoperatoria en individuos que se han sometido a una cirugía por lesiones del tendón flexor de la mano. Las principales comparaciones de interés fueron los ensayos que compararon diferentes regímenes de movilización con otro régimen de movilización o con un control. Los principales desenlaces de interés fueron la funcionalidad comunicada por el paciente, la amplitud de movimiento activo de los dedos y el número de participantes que presentaron un evento adverso.
Obtención y análisis de los datos
Dos autores de la revisión seleccionaron de forma independiente los ensayos para inclusión, extrajeron los datos, evaluaron el riesgo de sesgo y evaluaron la calidad del conjunto de evidencia para los desenlaces principales mediante el enfoque GRADE, según la metodología estándar de Cochrane.
Resultados principales
Se incluyeron 16 ECA y un ensayo cuasialeatorizado, con un total de 1108 participantes, principalmente adultos. En general, los participantes tenían entre siete y 72 años, y el 74% eran hombres. Los estudios se centraron principalmente en las lesiones del tendón flexor en la zona II.
Los 17 estudios fueron heterogéneos en cuanto a los tipos de tratamientos de rehabilitación proporcionados, la intensidad, la duración del tratamiento y el ámbito del mismo. Cada ensayo analizó una de las 14 comparaciones, ocho de las cuales eran de diferentes regímenes de ejercicios. Los otros ensayos examinaron el momento de regreso a las actividades funcionales sin restricciones después de la cirugía (un estudio); el uso de dispositivos externos aplicados al participante para facilitar la movilización, como un exoesqueleto (un estudio) o un dispositivo de movimiento pasivo continuo (un estudio); modalidades como la terapia con láser (dos estudios) o la terapia con ultrasonido (un estudio); y un tratamiento de imágenes motoras (un estudio). En ningún ensayo se analizaron diferentes tipos de ortesis; diferentes regímenes de uso de ortesis, incluida la duración; diferentes tiempos de inicio de la movilización; diferentes tipos de tratamiento de las cicatrices; ni diferentes tiempos de comienzo del fortalecimiento.
En general, los ensayos tuvieron alto riesgo de sesgo en uno o más dominios, incluida la falta de cegamiento, los datos de desenlace incompletos y el informe selectivo de los desenlaces. El agrupamiento de los datos se limitó a los datos de la rotura de los tendones en una comparación de tres ensayos. La evidencia disponible para todos los desenlaces informados de todas las comparaciones se consideró de certeza muy baja, lo que significa que se tiene muy poca confianza en las estimaciones del efecto.
Se presentaron los resultados de tres comparaciones de regímenes de ejercicios, ya que estos se utilizan habitualmente en la práctica clínica actual.
El régimen temprano de flexión activa más ejercicios pasivos controlados versus el régimen temprano de ejercicios pasivos controlados (protocolo Kleinert modificado) se comparó en un ensayo de 53 participantes con reparaciones del tendón flexor de la zona II principalmente. Hay evidencia certeza de muy baja de que no hay diferencias clínicamente importantes entre los dos grupos en cuanto a la funcionalidad calificada por el paciente o la amplitud de movimiento activo de los dedos a los seis ó 12 meses de seguimiento. Hay evidencia de certeza muy baja de que hay poca diferencia entre los grupos en cuanto a los eventos adversos: hubo 15 en total. Las tres roturas de tendones fueron sometidas a una cirugía secundaria.
Un régimen de ejercicios activos versus un régimen de inmovilización durante tres semanas se comparó en un ensayo que informó datos de 84 participantes con reparaciones del tendón flexor de la zona II. El ensayo no informó sobre la funcionalidad autocalificada, sobre el rango de movimiento durante tres a seis meses ni sobre el número de participantes que presentaron eventos adversos. La evidencia de certeza muy baja de un rango de movimiento deficiente (menos de un cuarto de lo normal) de los dedos en un seguimiento de uno a tres años hace que no se tenga confianza en el hallazgo de cero casos en el grupo activo versus siete casos en grupo de régimen de inmovilización. La misma falta de confianza se aplica al hallazgo de poca diferencia entre los dos grupos en los eventos adversos (cinco roturas de tendones en el grupo activo versus diez probables adherencias de las cicatrices en el grupo de inmovilización) indicados con la cirugía.
El régimen de ejercicios de colocar y mantener realizado dentro de una ortesis versus un régimen pasivo controlado que utiliza la tracción de una banda elástica se comparó en tres ensayos heterogéneos, que informaron datos de un máximo de 194 participantes, con reparaciones del tendón flexor de la zona II principalmente. Los ensayos no informaron sobre la amplitud de movimiento durante tres a seis meses, ni sobre el número de participantes que presentaron eventos adversos. Hubo evidencia de certeza muy baja de que no hubo diferencias en la funcionalidad autocalificada mediante la evaluación funcional con la Disability of the Arm, Shoulder and Hand (DASH) entre los dos grupos a los seis meses (un ensayo) o a los 12 meses (un ensayo). Hay evidencia de certeza muy baja de un ensayo de mayor amplitud de movimiento activo de los dedos a los 12 meses después de colocarlos y mantenerlos. No se dispuso de datos sobre la cirugía secundaria; sin embargo, las siete roturas de tendones registradas habrían requerido cirugía.
Toda la evidencia de las otras cinco comparaciones de ejercicios, así como la de las otras seis comparaciones realizadas por los estudios incluidos, fueron incompletas y, cuando estaban disponibles, de certeza muy baja.
Conclusiones de los autores
Falta evidencia de ECA sobre la mayoría de las intervenciones de rehabilitación utilizadas después de la cirugía por lesiones del tendón flexor de la mano. La evidencia limitada y de certeza muy baja de las 14 comparaciones examinadas en los 17 estudios incluidos significa que se tiene muy poca confianza en las estimaciones del efecto de todos los desenlaces para los que se disponía de datos en estas comparaciones.
La escasez de evidencia identificada en esta revisión apunta a la necesidad urgente de ECA con suficiente potencia estadística que examinen temas clave relacionados con la rehabilitación de estas lesiones. Será valioso un enfoque consensuado para identificarlos y establecer criterios mínimos de realización de los estudios y de presentación de los informes. Las sugerencias realizadas para futuros estudios de investigación se detallan en la revisión.
PICO
Resumen en términos sencillos
¿Cuáles son las mejores formas de recuperar el movimiento de la mano después de una cirugía para reparar los tendones flexores (tendones de la mano que permiten que los dedos se doblen)?
¿Por qué es importante esta pregunta?
Los tendones flexores son fuertes cuerdas lisas que conectan los músculos del antebrazo (entre la mano y el codo) con los huesos de los dedos. Estos tendones permiten doblar los dedos. (Otros tendones, conocidos como tendones extensores, permiten enderezarlos.)
Si los tendones flexores se dañan (por ejemplo, debido a un corte profundo con un vidrio roto) suele ser necesaria una cirugía. El objetivo de la cirugía es reparar los tendones para que se pueda restablecer el movimiento de los dedos afectados.
Después de la cirugía, los tendones necesitan un largo período de rehabilitación para recuperarse de la lesión, de la cirugía y para restablecer el movimiento. Este período suele durar 12 semanas, aunque puede ser más largo en el caso de las personas con lesiones complejas o con complicaciones como deformidades articulares. La rehabilitación suele implicar varios pasos diferentes. Después de la cirugía, las personas a menudo deben usar una férula u otro dispositivo para estabilizar o inmovilizar la mano y la muñeca. También deben hacer a menudo ejercicios de la mano para evitar que los tendones reparados se peguen al tejido circundante y limiten el movimiento de la mano.
Hay muchos tipos de programas de rehabilitación diferentes, pero no está claro si algunos son mejores que otros. Se planificó revisar la evidencia de los estudios de investigación para determinar:
‐ qué enfoques son más eficaces para restaurar el movimiento y la función de los dedos; y
‐ que enfoque reduce el riesgo de eventos adversos (no deseados), como roturas de tendones, tejido cicatrizante que se adhiere a otros tejidos y rigidez de las articulaciones.
¿Cómo se identificó y evaluó la evidencia?
Primero, se buscó en la literatura médica los estudios que compararan cualquier enfoque de rehabilitación después de una cirugía del tendón flexor contra:
‐ ningún tratamiento;
‐ un tratamiento con placebo (falso) (en el que, por ejemplo, la persona piensa que puede estar recibiendo terapia con láser pero la máquina está apagada); u
‐ otro enfoque de rehabilitación.
Luego se compararon los resultados y se resumió la evidencia de todos los estudios. Finalmente, la confianza en la evidencia se calificó sobre la base de factores como los métodos y los tamaños de los estudios, así como la consistencia de los hallazgos entre los estudios que evaluaron la misma comparación.
¿Qué se encontró?
Se encontraron 17 estudios con un total de 1108 personas que habían sido operadas para reparar los tendones flexores desgarrados. Las personas tenían entre siete y 72 años, y tres cuartos de ellos eran varones.
Diez estudios evaluaron uno de los ocho programas diferentes de ejercicios de mano. Los otros siete estudios evaluaron una variedad de otros enfoques de rehabilitación, tales como:
‐ la terapia con láser, en la que la luz se dirige a los tendones para estimular la cicatrización;
‐ ultrasonido, en el que las ondas de sonido se dirigen a los tendones para estimular la cicatrización; y
‐ una máquina portátil (exoesqueleto), diseñada para ayudar a las personas en sus movimientos.
Se encontró muy poca evidencia sobre los efectos beneficiosos y los riesgos de los diferentes enfoques de rehabilitación. La evidencia encontrada no era sólida. Por ejemplo, sólo se identificaron las tres comparaciones de ejercicios más relevantes:
‐ un estudio (84 personas) que comparó los ejercicios de los dedos con la inmovilización;
‐ un estudio (53 personas) que evaluó los efectos de agregar ejercicios regulares para los dedos (20 a 30 veces durante las horas en que se está despierto por cuatro semanas a partir del primer día después de la cirugía) a los ejercicios "pasivos" (en los que las personas doblaban regularmente los dedos de la mano lesionada utilizando la mano no lesionada); y
‐ tres estudios (190 personas) que evaluaron los efectos de agregar ejercicios de "colocar y mantener" (durante los cuales las personas utilizan su mano no lesionada para doblar los dedos de la mano lesionada, y luego tienen que mantener los dedos doblados en su lugar durante unos segundos sin ningún tipo de apoyo) con los ejercicios pasivos.
Los estudios fueron demasiado pequeños, o proporcionaron muy poca información sólida o utilizable, para que se pueda determinar qué enfoque es el mejor.
¿Qué significa esto?
No se sabe qué método funciona mejor para que las personas recuperen el movimiento de la mano después de una cirugía para reparar los tendones flexores. Esto se debe a que no hay suficientes evidencia sólida sobre los efectos beneficiosos y los riesgos de los diferentes métodos.
Se necesitan más estudios de investigación para ayudar a informar a los médicos y a los pacientes sobre la elección con respecto a la rehabilitación después de la cirugía de las lesiones del tendón flexor.
¿Cuál es el grado de actualización de esta revisión?
La evidencia de esta revisión Cochrane está actualizada hasta agosto de 2020.
Authors' conclusions
Summary of findings
| Addition of active flexion exercises to controlled passive exercise regimen for rehabilitation following surgery for flexor tendon injuries of the hand | ||||||
| Patient or population: participants undergoing rehabilitation following surgery for flexor tendon injuries of the handa | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Early controlled passive exercise regimen (modified Kleinert protocol) | Early active flexion plus early controlled passive exercise regimen | |||||
| Functional assessment using a patient reported outcome measure: Follow‐up: 6 months | Study population | ‐ | 62 fingers (1 RCT) | ⊕⊝⊝⊝ | The study reporting this outcome reported median and interquartile ranges. It found no evidence of a difference between the two groups (reported P = 0.942). It is very unlikely that a difference of 0.3 on an 11 point scale is clinically important. | |
| See comment. Median 8.5, IQR 3.5 | See comment. | |||||
| Functional assessment using a patient reported outcome measure: Follow‐up: 12 months | Study population | ‐ | 63 fingers | ⊕⊝⊝⊝ | The study reporting this outcome reported median and interquartile ranges. It found no evidence of a difference between the two groups (reported P = 0.113). It is very unlikely that a difference of 0.5 on an 11 point scale is clinically important | |
| See comment. Median 8.8, IQR 2.9 | See comment. | |||||
| Active finger range of motion | Study population | ‐ | 63 fingers | ⊕⊝⊝⊝ | This difference is not meaningful and could have been due to error in measurement: for goniometric measurement, the minimal detectable difference is between 12 and 30 degrees with a standard error of measurement ranging from 4 to 11 degrees per joint (Reissner 2019). | |
| Mean AROM in the control group was 134 degrees | MD 3 degrees higher | |||||
| Active finger range of motion | Study population | ‐ | 63 fingers | ⊕⊝⊝⊝ | This difference is not meaningful and could have been due to error in measurement: for goniometric measurement, the minimal detectable difference is between 12 and 30 degrees with a standard error of measurement ranging from 4 to 11 degrees per joint (Reissner 2019). | |
| Mean AROM in the control group was 140 degrees | MD 9 degrees higher | |||||
| Adverse events: participants incurring one or more adverse events Follow‐up: 12 months | Study population | RR 0.58 (0.23 to 1.44) | 69 fingers (1 RCT) | ⊕⊝⊝⊝ | The 15 adverse events comprised 3 tendon ruptures, 6 wound dehiscence, 1 complex regional pain syndrome and 5 transitory swelling and tenderness of the tendon sheaf. | |
| 282 per 1000 | 164 per 1000 (65 lower to 406 higher) | |||||
| Adverse event (tendon rupture) | Study population | RR 1.73 | 69 fingers | ⊕⊝⊝⊝ | All three tendon ruptures (4.3%) underwent secondary surgery. | |
| 31 per 1000 | 54 per 1000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aThe majority (68%) were zone II flexor tendon repairs; the rest being zone I and III. dDowngraded one level due to serious indirectness reflecting the reflecting the uncertain nature of the outcome. eDowngraded two levels due to very serious imprecision reflecting the small number of events. | ||||||
| Active exercise regimen compared with an immobilisation regimen following surgery for flexor tendon injuries of the hand | ||||||
| Patient or population: participants undergoing rehabilitation following surgery for flexor tendon injuries of the handa | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Immobilisation regimen for three weeks | Active exercise regimen commenced within one day post‐surgery | |||||
| Functional assessment using a patient reported outcome measure | See comment. | See comment. | Not estimable | ‐ | See comment. | Outcome was not reported |
| Functional assessment using a patient reported outcome measure | See comment. | See comment. | Not estimable | ‐ | See comment. | Outcome was not reported |
| Range of movement | See comment. | See comment. | Not estimable | ‐ | See comment. | Outcome was not reported |
| Range of movement | Study population | RR 0.08 | 84 | ⊕⊝⊝⊝ | Poor outcome is < 25% of normal. The 7 (15%) cases of poor range of finger movement were all in the immobilisation group | |
| 149 per 1000 | 12 per 1000 | |||||
| Adverse events: participants incurring one or more adverse events | See comment. | See comment. | Not estimable | 84 | See comment | Outcome was not reported. Only tendon rupture and indication for tenolysis data provided; see below. |
| Adverse events requiring (or indicated for) surgery | Study population | RR 0.64 | 84 | ⊕⊝⊝⊝ | All five cases of tendon rupture (13.5% of 37) needing surgical repair occurred after 2 weeks in the active mobilisation group and all 10 cases of range of motion deficiency (21.3% of 47) indicating scar adhesion and need for tenolysis occurred in the immobilisation group. | |
| 213 per 1000 | 137 per 1000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group (in this table, this is directly based on the study population) and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aAll were zone II flexor tendon repairs. bDowngraded two levels for very serious risk of bias reflecting detection bias (no blinding of outcome assessors), potential selection bias and attrition bias. cDowngraded one level for serious indirectness reflecting the unsatisfactory nature of the outcome. dDowngraded one level because of low number of events and wide confidence intervals for this outcome. eThese complications reflect the anticipated complications of early active mobilisation (early re‐rupture) and immobilisation (scar adhesions and contractures). It is uncertain whether tenolysis was actually done for those participants with range of motion deficit in the immobilisation group. | ||||||
| Place and hold exercise versus controlled passive exercise following surgery for flexor tendon injuries of the hand | ||||||
| Patient or population: participants undergoing rehabilitation following surgery for flexor tendon injuries of the handa | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Controlled passive exercise regimen | Place and hold exercise regimen | |||||
| Functional assessment using a patient reported outcome measure: assessed with DASH questionnaire (0 to 100; higher scores = worse disability) | Study population | Not estimable | 26 | ⊕⊝⊝⊝ | The study reporting this outcome reported median and interquartile ranges, finding no evidence of a difference between the two groups (reported P = 0.62). | |
| See comment. Median 15, IQR 10 to 30 | See comment. Median 23, IQR 2 to 26 | |||||
| Functional assessment using a patient reported outcome measure: | Study population | ‐ | 89 | ⊕⊝⊝⊝ | These differences are not clinically important. The recommended minimal clinically important difference for DASH is 15 (DASH/QuickDASH). | |
| Mean DASH score was 3.1 | Mean DASH score was 1.1 lower (2.77 lower to 0.57 higher) | |||||
| Range of movement | See comment. | See comment. | Not estimable | ‐ | See comment. | Outcome was not reported |
| Range of movement | Study population | ‐ | 89 (102 digits) | ⊕⊝⊝⊝ | ||
| Mean ROM was 128 degrees | Mean ROM was 28 degrees higher | |||||
| Adverse events: participants incurring one or more adverse events | See comment. | See comment. | Not estimable | 84 | See comment. | This outcome was not reported by the three trials testing this comparison. Only tendon rupture (see next) was commonly reported. One trial (26 participants), reporting by tendon or digit (36 digits), also reported on scar adherence (reported only in the controlled passive group), flexion contracture at the DIP and PIP joints and tendon lag; very low certainty evidence for all individual complications. |
| Adverse events requiring (or indicated for) surgery | Study populationsh | RR 0.81 | 196 tendons | ⊕⊝⊝⊝ | These data were limited to tendon rupture. We considered that all 7 tendon ruptures (3.6% of 196 tendons) would have required surgery.j | |
| 40 per 1000 | 33 per 1000 (8 to 140) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group (in this table, this is directly based on the study population) and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aThe majority were zone II flexor tendon repairs; one of the three studies making this comparison also included 7 zone I injuries and 7 zone III injuries. bAll exercises started at 3 days from surgery. The place and hold exercise regimens varied among the three studies. In two studies, the exercises were carried out with a dorsal orthosis and in one study, the dorsal orthosis was removal when doing the exercises cAll exercises started at 3 days from surgery. The controlled passive exercise regimens varied among the three studies. However, rubber band traction was common to all three. dDowngraded two levels for very serious risk of bias reflecting lack of blinding (performance and detection bias) eDowngraded one level for serious imprecision. fDowngraded one level for serious imprecision, also reflecting the potential 'ceiling' effect as the mean values were very low and thus cannot discriminate between the two groups. gDowngraded one level for serious imprecision as the data are presented for tendons not participants. hControl group risk was devised from the summed data from the three studies. These results were not available for participants rather than tendons. iDowngraded two levels for very serious imprecision reflecting a very low number of events and wide confidence interval for this outcome. jWe did not include the 14 cases of scar adherence (70% of 20 tendons) reported in the controlled passive group of one trial because the outcome was not defined and no details of the extent or consequences were provided. | ||||||
Background
Description of the condition
Tendons connect muscles to bones and enable motion at joints. The flexor tendons of the hand, which connect various flexor muscles in the forearm and hand to the bones (phalanges) in the fingers and thumb, act to bend (i.e. flex) the fingers or thumb. They are essential for complex hand function, including pinch, grip and motor dexterity. There are two flexor tendons in each finger; these connect with the flexor digitorum profundus (FDP) and the flexor digitorum superficialis (FDS) muscles in the forearm. The two flexor tendons in the thumb connect with the flexor pollicis longus (FPL) and flexor pollicis brevis (FPB) muscles. For much of the finger, flexor tendons move within tunnels called flexor sheaths. These are synovium‐lined tunnels that hold the tendons close to the bones, ensuring mechanical efficiency and preventing the tendons from 'bowstringing' across the joints. Sections of the sheaths are thickened into five fibrous bands called annular pulleys (A1 to A5) and three flexible compressible sections called cruciate pulleys (C1 to C3).
Flexor tendon injuries can be caused by open cuts (such as by broken glass) to the hand and crush injuries. They can also be caused by sudden forced extension of the fingers or thumb resulting in an avulsion injury where the tendon is, or tendons are, pulled away from the bone. Flexor tendon injuries of the hand are relatively common with 33 injuries per 100,000 person‐years (De Jong 2014). The incidence of tendon injuries is higher in males and in people aged 20 to 29 years (De Jong 2014). The FDP tendon of the fifth (little) finger is the most commonly injured tendon in isolation (Rosberg 2003).
Five anatomical zones (zones I to V) are commonly used to categorise the level of tendon injury in the fingers, hand and forearm (Verdan 1960). Zone I includes the FDP tendons from the insertion of the FDP on the distal phalanx bone to the insertions of the FDS tendons on the middle phalanx. Zone II extends between the FDS insertions to the proximal edges of the A1 pulleys. Zone III is the area in the palm of the hand between the A1 pulleys and the distal edge of the transverse carpal ligament in the wrist. Zone IV includes the tendons passing in the carpal tunnel. Zone V is the section proximal to the carpal tunnel at the wrist to the origin of the tendons at their respective muscle bellies. Injuries in zone II, where the tendons are contained within the flexor sheaths, are the most common (De Jong 2014). Often, the associated pulleys are damaged during the flexor tendon injury in this zone. The clinical issues related to an inefficient pulley system can include bowstringing, reduced composite finger flexion, stiffness and reduced grip strength (Lilly 2006).
Laceration or avulsion injury to the flexor tendons is generally managed with surgery. Acute injuries tend to be managed with primary surgical repair of the tendon. This is done by direct end‐to‐end tendon repair with multi‐strand sutures (2, 4, 6 or 8 strand) of the core of the tendon and with additional peripheral sutures around the sides of the tendon. The pattern and strength of the suture repairs prevent gapping and contribute to the strength of the repair. When primary repair of the tendon has failed (that is, a tendon ruptures) or when primary repair is not feasible due to concurrent injuries (e.g. nerve, blood vessel, bony injury or infection) or loss of tendon length, secondary surgical intervention may be advised. Secondary surgery involves either secondary repair of the failed primary tendon repair or a two‐stage reconstructive surgical process. Zone II injury is typically considered to be more difficult both to repair surgically and to rehabilitate. Repair of zone II tendons often requires more additional procedures (e.g. excising one slip of the FDS tendon or part of the A2 or A4 pulleys) than other zones, often resulting in poorer mobility and functional outcomes (Tang 2013).
Description of the intervention
This review examines the rehabilitation interventions that are prescribed after the surgical repair of both open and closed flexor tendon injuries. Rehabilitation interventions are usually provided by a physical therapist or an occupational therapist who specialises in providing hand therapy interventions. Therapists often prescribe a combination of interventions to protect the tendon repair, promote tendon healing, remedy any effects of scarring and swelling, and to regain mobility and function of the hand. Early rehabilitation in the first six to eight weeks following surgery is focused on protecting the tendon repair (Evans 2012; Strickland 2005). Intervention in this early postoperative period can include patient education, fabrication of a type of orthosis, an exercise regimen, wound care (application of dressings or topical applications), swelling management (e.g. compression therapy, elevation or cryotherapy), scar management (e.g. massage treatments, topical applications, desensitisation programmes) and electrotherapy modalities (e.g. neuromuscular electrical stimulation) (Pettengill 2005; Villecio 2010).
A therapist will fabricate an orthosis in order to protect the tendon repair. Orthoses restrict hand use and usually allow joints to move within a safe range of motion (ROM). Orthoses can be made from a variety of materials. They can also have different designs including hand‐based designs (crossing only the finger and/or thumb and wrist joints) (Peck 2014), forearm‐based designs (extending from finger and/or thumb to the proximal forearm), or they can have a dynamic component (often using an elastic traction system to mimic the action of the tendons, thus preventing strain on the repairs when moving the joints) (Evans 2012; Strickland 2005). Variations also exist with respect to the specific position of the wrist and digits within the orthosis.
Historically, post‐operative management consisted of immobilisation for three weeks post surgery based on the early animal studies by Mason and Allen in the 1940s (Mason 1941). This was based on the principle that tendons required extrinsic healing from surrounding tissues before they could be subject to gliding stresses (Peacock 1965). However, by the 1970s, surgeons such as Kleinert and Duran (Kleinert 1975; Duran 1975) proposed passive flexion either using rubber band traction systems or passive exercises based on the concepts that tendons could heal intrinsically and thus minimise adhesions. As surgical techniques and strength of repairs have continued to improve, place and hold exercises, synergistic wrist gliding exercises and active gliding exercises have been incorporated in the rehabilitation regimens. Active flexion exercises are recommended; this is where fingers are bent through a progressive arc of motion from one third to full bending, typically over a period of four weeks (Tang 2018a).There has also been a simultaneous shift of orthotic positioning of the wrist and finger/thumb joints from significant flexion to keeping the wrist in extension to allow for reduced work of flexion and mechanical efficiency (Evans 2012). Different exercise regimens are in use, often defined in terms of the types of exercise entailed. These include: immobilisation regimens, passive motion exercise regimens, place and hold exercise regimens, or active motion exercise regimens (Clancy 2013; Gelberman 1991; Hagberg 2000; Pettengill 2005). Regimens are typically named after the type of exercises that are initiated in the early postoperative period.
-
Immobilisation regimens: During immobilisation, therapists prescribe no exercise during a defined postoperative time period. The patient is usually placed in a dorsal extension blocking plaster cast or an orthosis including the affected wrist, fingers and thumb.
-
Passive motion exercise regimens: These refer to bending the finger manually with assistance from either the patient's other hand, from another person (e.g. a physical therapist) or by means of a dynamic component (e.g. elastic component such as rubber bands). The patient then actively straightens the finger into the orthosis using the muscle power of the uninjured extensor tendon. For the purpose of this review controlled passive exercise regimens imply the use of rubber band traction to hold the fingers in passive flexion.
-
Place and hold exercise regimens: These are exercise programmes where the injured digit is manually flexed using either the patient's uninjured hand or by another person (e.g. a physical therapist); the patient then tries to hold the flexed position by actively using the muscle strength of the injured flexor tendon.
-
Active motion exercise regimens: These refer to bending and straightening the fingers and thumb through an arc of motion using the patient's own muscle strength with no assistance.
Exercise regimens may comprise combinations of these regimens (for example, passive motion exercises followed by place and hold and/or active exercises) or variations of these regimens (for example, active motion through a 'mid‐range' or 'full‐range', or synergistic motion of the wrist and hand using the tenodesis effect). The timing of the commencement of the exercise programme (for example, delaying the commencement of certain types of exercises following surgery), as well as duration and frequency of exercises may also vary (Evans 2012).
Rehabilitation generally progresses over time. Interventions recommended later in the rehabilitation process include grip and pinch strengthening, functional rehabilitation (that is, prescription of graduated hand function by introducing more strenuous self‐care, domestic and work duties) and return‐to‐work interventions (for example, work hardening and job modifications). There is variability in these exercise regimens with regards to frequency and repetitions of the performed exercises as well as the intervals of progression from one to a different type of exercise. During the later stages of rehabilitation, additional orthosis can also be fabricated to prevent and manage joint deformities or tightness of soft tissue components.
Work hardening programmes are graded exercises and activities to improve strength, endurance and co‐ordination to facilitate a person's return to employment (Pettengill 2010).
The mode of delivery of the intervention is also an important consideration. People may receive early rehabilitation in a hospital or clinic setting. Later programmes may take place in the clinic setting, or alternatively the individual might perform them in the home or workplace. In each setting, the level of patient supervision differs. For example, a therapist may supervise rehabilitation in a clinic setting. Whereas, there may be limited supervisions for a tele‐rehabilitation programme, or none or limited supervision for a home exercise programme.
How the intervention might work
Over the last few decades, knowledge of tendon biology and biomechanics has improved considerably (Osei 2014; Wu 2013). This includes tendon response to injury, repair and stress as well as the mechanical characteristics of the current surgical techniques (to improve the strength of the repair whilst allowing smooth excursion of the tendons through the tunnels of the flexor tendon sheaths) (Lutsky 2015). This knowledge has, in turn, influenced rehabilitation protocols and the types of treatments offered (Groth 2004).
Advances in flexor tendon surgery such as surgical repair techniques, suture types, tendon grafting, use of antiseptic and other wound and scar limiting agents, wide‐awake surgery, have also influenced the advancement of hand rehabilitation (Bindra 2005; Tang 2018a). Various surgical repair techniques are currently used around the world and contribute to the choice of orthosis and exercise protocol prescribed, with different types of repairs being thought to withstand greater forces and therefore being able to tolerate earlier active mobilisation.
Rehabilitation aims to protect the repaired tendons, promote intrinsic tendon healing, minimise extrinsic scar tissue formation, optimise tendon gliding and restore motion and functional use (Elliot 2007Strickland 2005). The types of rehabilitation interventions recommended by healthcare providers are generally based on a number of factors that may include: the nature of the injury (e.g. traumatic open injury or closed avulsion injury), stage of the rehabilitation (e.g. immediately following the surgery versus longer term rehabilitation at three months or beyond), the strength of the repair (e.g. number of suture strands in the repair), associated injuries (e.g. concomitant nerve, bone, blood vessel or ligament damage), pre‐injury medical history or ability to comply with rehabilitation (Evans 2012).
Various rehabilitation treatments are frequently used in the early to late post‐operative stages. Education is considered very important for patient adherence to rehabilitation following surgery (Evans 2012). Advice often focuses on the importance of adhering to treatment recommendations, the level of functional activity permitted and general care of the repaired tendon and wound (Pettengill 2010). Orthoses are applied in the early post‐surgical stage. The purpose of providing orthoses is to position the wrist and fingers so that the tendon repairs are not under any tension, but still allow motion within a safe range (Pettengill 2010). Careful positioning of the hand within the orthosis is necessary. Therefore, the joint angles within the orthosis have great significance. For example, it is thought that dynamic traction designs with the metacarpal joints in 70 degrees of flexion increases the risk of proximal interphalangeal (PIP) joint flexion contracture (Burge 1990). Early designs of exercise regimens assumed that 3 mm to 5 mm of tendon excursion (i.e. the distance a tendon travels upon motion of a joint) decreased tendon adhesions that limit finger mobility (Duran 1975). Therapists often recommend protocol‐based exercise regimens to improve the tendons' gliding function by minimising adhesions (Khanna 2009), preventing joint stiffness and improving range of motion. Practitioners believe these exercises to be essential in regaining long‐term finger dexterity and hand function (Pettengill 2010). Moreover, research suggests that controlled stress on the tendons, created by either passive or active motion, facilitates healing, controls early collagen deposition and facilitates biochemical events that increase tensile strength (Buckwalter 1999; Evans 2012). However, excessive stress during motion may also pose a risk of gapping or rupture of the repaired tendon ends (Evans 2005). The timing of the interventions, especially the commencement of an exercise regimen, may influence how an intervention works (Adolfsson 1996; Evans 2012). Various studies have found that periods of immobilisation immediately following repair can result in loss of tensile strength and glide (Evans 2012). However, other authors advocate delayed mobilisation for up to three to five days to allow inflammation and oedema to subside and minimise the strain on the flexor tendon (Halikis 1997; Zhao 2004). Wound care treatments are essential in preventing infection and facilitating wound healing (Von der Heyde 2010). As therapists often prescribe early exercise, the dressings should not impede motion or place extra stress on the tendon repairs when the finger is moved. Oedema management helps to reduce the amount of swelling in the digit and hand. Oedema in the subcutaneous tissue adds significantly to the gliding resistance, whereas pulleys may add to the resistance of the swollen repaired tendon (Wu 2013). Scar management treatments may be advisable to promote optimal scar formation and prevent skin and tendon adhesions or reduce scar hypersensitivity (Jones 2005). Electrotherapy modalities, such as neuromuscular electrical stimulation, are thought to provoke stronger muscle contractions. Practice guidelines have recommended therapeutic ultrasound for promoting healing while minimising the formation of soft‐tissue and skin adhesions (Pettengill 2010). Therapists may also utilise strengthening and work hardening treatments to facilitate early return‐to‐work, leisure and sporting activities in the later stages following surgery (Pettengill 2010).
Why it is important to do this review
Flexor tendon injuries create significant impairment in terms of the functional use of the hand. They create an economic burden on our health care systems and an indirect costs related to missed workdays. A recent study in the United States estimated the cost of flexor tendon lacerations to society using a validated prevalence‐based cost of illness model (Mehrzad 2019). They reported that flexor tendon lacerations incur an estimated cost of up to USD 409.1 million annually. The estimated total direct costs per injury are USD 13,725, whereas indirect costs up to USD 112,888. Therefore, it is important to focus our efforts to improve treatments and rehabilitation protocols which decrease not only the physical and psychological burden to the individual but also financial costs that impact not only the person, but also society as a whole.
Flexor tendon injuries of the hand can result in loss of finger and thumb motion, reduced functional hand use and quality of life. The management of these injuries has evolved over several decades. At present, there is no gold standard rehabilitation programme used for rehabilitation following surgery for flexor tendon injuries. As a result, centres across the globe use a wide range of rehabilitation treatments. Clinical practice is often influenced by the results of biomechanical and biological studies (Osei 2014; Wu 2013). Instead we need to examine the high‐quality clinical evidence to establish the effectiveness and safety of rehabilitation interventions for managing flexor tendon injuries of the hand and thus identify those interventions that are most effective at restoring digital motion and function whilst minimising the risk of complications and adverse events.
Objectives
To assess the effects (benefits and harms) of different rehabilitation interventions after surgery for flexor tendon injuries of the hand.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised and quasi‐randomised (i.e. with treatment allocation method that is not strictly random, such as allocation by patient hospital identification number) controlled trials evaluating rehabilitation interventions after surgery for flexor tendon injuries of the hand.
Types of participants
We included trials of individuals who had undergone post‐surgical rehabilitation following primary and secondary repair, or reconstruction of partial or total lacerations or rupture of one or more flexor tendons in any of the flexor tendon zones of injuries. We excluded studies examining the effectiveness of tendon transfers for people with neurological conditions.
Types of interventions
We included all types of rehabilitation following surgery for flexor tendon injury of the hand. Primary interventions included orthoses to protect the repair/reconstruction, exercise regimens, scar management and hand strengthening. We also considered interventions for reducing or controlling oedema, for work hardening and desensitisation programmes. We also considered the timing of the interventions' commencement (e.g. early active motion regimens). We excluded wound care, oral pharmacological interventions and topical pain relief ointments.
The main comparisons we considered were:
-
different types of orthoses; e.g. dynamic orthosis versus static orthosis; comparisons of different finger and wrist positioning within the orthosis;
-
different orthosis wearing regimens, including duration; e.g. six weeks or shorter versus longer than six weeks;
-
different exercise regimens; e.g. controlled active mobilisation versus controlled passive mobilisation;
-
different timings for commencing mobilisation; e.g. started within the first three days versus after three days;
-
different types of scar management; e.g. massage versus topical applications such as silicone gel sheets;
-
different timings for commencing strengthening; e.g. six to 10 weeks versus after 10 weeks;
-
different doses for interventions, other than orthosis wearing regimen; e.g. ultrasound dose, frequency or amount of interventions.
For interventions in which a control or sham group was appropriate (such as scar management, or strengthening and work hardening), we compared the active intervention versus the control or sham group. For the exercise protocols, we selected the least aggressive protocol as the control group.
Types of outcome measures
We included studies if the protocol included the measurement of at least one clinical outcome related to function, range of motion or adverse event reporting. We assessed all outcomes as short‐term (defined as three months or less), medium term (over three months to six months) and long‐term (over six months).
Primary outcomes
-
Functional assessment using a patient reported outcome measure, such as Patient Rated Wrist and Hand Evaluation (PRWHE); Michigan Hand Questionnaire (MHQ); or Disability of the Arm, Shoulder and Hand (DASH)
-
Active finger ROM using goniometric measurement. Different classification systems have been designed that incorporate ROM and are used to describe outcomes following tendon surgery (such as, Stickland‐Glogovac classification; Strickland classification; Tang classification)
-
Adverse events including tendon rupture, revision surgery, scar adhesion, delayed wound healing, loss of mobility or function, joint contracture, triggering of the digit, pulley failure, persistent pain and sensory deficits. We will report the total number of participants with adverse events and for each of these events
Secondary outcomes
-
Passive finger ROM using goniometric measurement
-
Hand strength (including grip strength, pinch strength)
-
Return to previous activity (including return to work, education, musical instrument or sport). Return to work will be reported separately if available (including same, modified or alternate duties) for individuals working at the time of injury
-
Functional assessment using an objective measure (including Jebsen Hand Function Test)
-
Quality of life using a self‐report measure (such as Euro‐QOL, SF‐36)
-
Satisfaction with the result of the surgery at three months or longer
Where available, we collected resource and cost data such as health care utilisation, and insurance data related to work absence, and reported these data in the Characteristics of included studies. However, these data were not a focus of this review.
Search methods for identification of studies
Electronic searches
We conducted a comprehensive search of the following databases:
-
Cochrane Bone, Joint and Muscle Trauma Group Specialised Register (18 June 2019);
-
Cochrane Central Register of Controlled Trials (CENTRAL) (11 August 2020 Issue 8);
-
MEDLINE (including Epub Ahead of Print, In‐Process and Other Non‐Indexed Citations, Daily and Versions(R) (1946 to 10 August 2020);
-
Embase (1980 to 11 August 2020);
-
AMED (1985 to 18 June 2019);
-
CINAHL Plus (1937 to 18 June 2019).
We also searched the following clinical trials registries for ongoing or recently completed trials:
-
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (18 June 2019);
-
US National Institutes of Health Clinical Trials search portal (ClinicalTrials.gov) (11 August 2020).
In MEDLINE, we combined subject‐specific terms with the sensitivity‐maximising version of the Cochrane Highly Sensitive Search Strategy for identifying randomised trials (Lefebvre 2011). Search strategies for all major databases are reported in Appendix 1. We did not apply any language or date restrictions.
Searching other resources
We searched the reference lists of included studies, relevant articles on flexor tendon rehabilitation and any known systematic reviews on the topic for information on additional trials, including unpublished or ongoing studies. Where necessary, we contacted authors of key papers and abstracts to request further information about their trials.
Data collection and analysis
Review authors followed recommended strategies for data collection and analysis documented in Chapters 7 and 9 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Selection of studies
Two review authors (BJ and SP) independently screened the titles and abstracts of all retrieved references. We retrieved full‐text articles of all studies that appeared to meet the eligibility criteria. The same two review authors independently screened the full‐text articles against the eligibility criteria and documented their decisions. Review authors compared their lists; a third review author (MR) was available to resolve any disagreement, which was not required. Where identification was possible, we collated multiple reports of the same study and placed these under the same study ID. We have included a PRISMA flow chart to illustrate the study selection process (Moher 2009). We attempted to contact trial authors for clarification of study methods and characteristics, where necessary, to establish trial eligibility.
Data extraction and management
Two review authors (BJ and SP) independently extracted data using a standard pre‐defined data extraction forms specifically developed for this review.
We extracted the following study characteristics.
-
Methods: study design, date of study, duration of study, study setting, randomisation procedure, allocation, blinding and unit of analysis.
-
Participants: number of participants, number of involved digits, number of injured flexor tendons, age (mean, standard deviation, range), sex, type of flexor tendon injury, baseline characteristics, time between injury and surgery, inclusion criteria, exclusion criteria, type of surgery, diabetes and smoking status.
-
Interventions: intervention, comparison (e.g. control or sham), co‐interventions, and care programmes provided to all participants.
-
Outcomes: primary outcomes, secondary outcomes specific and collected, time points of evaluation, and resource use.
-
Notes: funding for trial, relevant conflicts of interest related to the study of trial authors, and any unit of analysis issues.
Two review authors (SP and BJ) independently extracted outcome data from included studies. We noted in the Characteristics of included studies tables if trial authors did not report outcome data in a usable way. We resolved disagreements by discussion. Two review authors (SP or BJ) transferred data into Cochrane's statistical software, Review Manager 5 (RevMan 2014), and a third review author (MR) cross‐checked the entries.
Assessment of risk of bias in included studies
Two review authors (BJ and SP) used Cochrane's tool for assessing risk of bias to independently evaluate the risk of bias for each trial in the following eight domains (Higgins 2011):
-
sequence generation (selection bias);
-
allocation concealment (selection bias);
-
blinding of participants and personnel (performance bias);
-
blinding of outcome assessment (detection bias) for participant self reported outcomes;
-
blinding of outcome assessment (detection bias) for objective assessments;
-
incomplete outcome data, rated separately for data measured at less than three months, three months to six months; and grater than six months follow‐up (attrition bias);
-
selective outcome reporting (reporting bias);
-
other risk of bias (whether the unit of analysis was appropriate, checking for premature stopping of the trial and the basis for this; and for extreme baseline differences between comparison groups).
We assessed risk of bias of self‐reported and objective outcome measurements separately for the two blinding and incomplete outcome data domains. For each domain, we assigned a judgement of high, low or unclear risk of bias based on the criteria in Table 8.5.d of the Cochrane Handbook (Higgins 2011). The review authors resolved disagreement by discussion and consensus. When criteria were unclear, one review author attempted to obtain further information from the authors of the trial. Where information on risk of bias related to unpublished data or correspondence with trial authors was received, we noted this in the 'Risk of bias' tables.
Measures of treatment effect
For dichotomous data we used risk ratios (RRs) with 95% confidence intervals (CIs).
For continuous data measured with the same scale, we used mean differences (MDs) and 95% CIs. If trials used different scoring systems to measure the same underlying concept (for example, different measures of function), we planned to use the standardized mean differences (SMDs) and 95% CIs. We used final scores in preference to change scores.
Where reported in trial reports, we presented non‐parametric data, such as medians (Med) and interquartile ranges (IQR) in the text, tables or both.
Unit of analysis issues
We clarified the unit of analysis; thus, whether the number reported represents participants, hands, digits or flexor tendons. Potential unit of analysis issues arise when multiple fingers on the same hand have had separate flexor tendon injuries. Bilateral involvement may be possible. We sought information about the unit of randomisation (that is, participants, hands, involved digits or involved tendons) for studies that included participants with multiple‐digit involvement in the same hand or had bilateral injury. We examined the study reports to see whether analyses were conducted using methods that take into account the dependency of observations. If trials did not report appropriate analyses, we contacted the authors for further information and data. If such data were not available and where possible, we planned to conduct sensitivity analyses that considered the number of randomised participants with bilateral or multiple digit involvement. We also avoided unit of analysis issues related to repeated observations of the same outcome, such as by presenting separate data for different periods of follow‐up (section 9.3.1; Higgins 2011). Where a single trial reported on multiple trial arms, we included only the relevant groups of the trial. If the same meta‐analysis combined two comparisons from the trial, we planned to split the control group to avoid double‐counting. However, this was not the case in any of the included studies.
Dealing with missing data
Intention‐to‐treat (ITT) analysis was our first choice when data were available. If data for key study characteristics or primary outcomes were missing or incomplete, we contacted the trial authors to obtain these. We considered conducting sensitivity analyses when missing data were not obtainable and their absence was considered likely to introduce bias. We also planned to conduct sensitivity analyses to explore the effects of excluding best‐case and worst‐case studies from the analyses. However, we did not have sufficient studies to complete this. We also planned to calculate missing data where possible; for example, calculating standard deviations from other available data such as standard errors (Section 16.1.3.1; Higgins 2011), or from data that was presented graphically. Again, we were not able to do this for any of the included studies.
Assessment of heterogeneity
Review authors assessed clinical heterogeneity (i.e. study populations, interventions and outcomes) between studies qualitatively. We assessed statistical heterogeneity by visual inspection of the overlap of CIs on the forest plots, along with consideration of the Chi2 tests for heterogeneity and I2 statistic (Higgins 2011). We based our interpretation of the I2 value in Higgins 2011:
-
0% to 40% might not be important;
-
30% to 60% may represent moderate heterogeneity;
-
50% to 90% may represent substantial heterogeneity;
-
75% to 100% may represent very substantial heterogeneity.
Assessment of reporting biases
To reduce outcome reporting bias, we searched for published and unpublished studies without language restrictions. We sought trial registration documents for all trials by searching ClinicalTrials.gov and the ICTRP. We compared these with the corresponding published RCTs (Dwan 2008). We contacted the authors of unpublished trials to ask for unpublished results. Selective outcome reporting biases were appraised as part of the risk of bias assessment of each trial. We planned to investigate the likelihood of publication bias by generating funnel plots if we had pooled data from 10 trials or more. However, we did not have a sufficient number of studies to conduct this analysis.
Data synthesis
When considered appropriate, we aimed to pool results of comparable groups of trials with similar characteristics (participants, interventions, outcome measures and timing of outcome measurements) to obtain estimates of the efficacy of specific rehabilitation interventions following flexor tendon surgery. We planned to pool results in a meta‐analysis using either a fixed‐effect or a random‐effects model (depending on the level of clinical and methodological heterogeneity). Our choice of the model to report would be guided by careful consideration of the extent of heterogeneity and whether it can be explained, in addition to other factors, such as the number and size of included studies. We used 95% CIs throughout. We considered not pooling data where there is considerable heterogeneity (I2 > 75%) that cannot be explained by the diversity of methodological or clinical features among trials. Where it was inappropriate to pool data, we presented trial data in the analyses or tables for illustrative purposes and reported these in the text as a narrative synthesis.
Subgroup analysis and investigation of heterogeneity
If sufficient studies were available, we had planned to perform subgroup analyses including:
-
zone of the tendon repair (zone I, II, III, IV and V);
-
type of suture technique for surgical repair (two‐strand, four‐strand, six‐strand repairs);
-
primary repair, secondary repair (i.e. repair following rupture of a primary repaired tendon) versus secondary tendon reconstruction;
-
timing of the start of the intervention (e.g. immediate (within the first three days), three days to six weeks, six to 10 weeks, after 10 weeks);
-
thumb versus fingers injuries;
-
partial lacerations, complete lacerations and avulsion injuries (ruptures);
-
workers' compensation insurance versus private insurance.
We selected these subgroups because the nature of each group may influence the intervention outcome. Repair of flexor tendons in different zones are thought to have different outcomes because of the biomechanics of the flexor tendons (Rigo 2016; Stone 1989). The strength of the repair is thought to increase together with the number of strands, which in turn may influence outcomes (Lee 2015; Myer 2016). Primary and secondary repair and secondary reconstruction may have different outcomes due to the length of time after the initial injury and different method used (Freilich 2007).
Where subgroup analysis was possible and appropriate, we planned to investigate whether the results of subgroups were significantly different by inspecting the overlap of confidence intervals and performing the test for subgroup differences available in RevMan 5 (RevMan 2014).
Sensitivity analysis
If sufficient studies had been available, we planned to conduct sensitivity analyses on various aspects of trial and review methodology and the robustness of the results.These included sensitivity analyses to explore the effects of the following:
-
exclusion of trials at high or unclear risk of selection bias from inadequate concealment of allocation;
-
exclusion of trials at high or unclear risk of attrition bias from incomplete outcome data;
-
exclusion of trials reported only in conference proceedings and other short reports;
-
the choice of statistical model for pooling (fixed‐effect versus random‐effects);
-
exclusion of trials at risk of unit of analysis issues, relating either to body parts or outcome reporting (e.g. total complications where it is unclear whether participants had more than one reported complication).
We did not conduct any sensitivity analyses in the current version of this review.
Summary of findings and assessment of the certainty of the evidence
We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to assess the certainty of evidence (Schünemann 2011). We used GRADEPro software (www.gradepro.org) to create 'Summary of findings' tables. We presented the results of the most important comparisons of the review in these 'Summary of findings' tables, which summarise the certainty of the evidence, the magnitude of effect of the interventions examined and the sum of available data for each outcome (Schünemann 2011). The 'Summary of findings' tables include an overall grading of evidence certainty related to each of the main outcomes.
According to GRADE, an initial judgement of 'high‐certainty evidence' is reserved for a body of evidence based on RCTs. We downgraded the certainty of evidence to 'moderate certainty', 'low certainty' or 'very low certainty', depending on the presence and extent of five factors: study limitations, inconsistency of effect, imprecision, indirectness or publication bias. We prepared 'Summary of findings' tables for those comparisons that tested interventions commonly used in clinical current practice. We selected the following primary outcomes for presentation in 'Summary of findings' tables: functional assessment using a patient‐reported outcome measure at medium‐term follow‐up (more than three to six months) and long‐term follow‐up (greater than six months); active range of motion at medium‐ and long term follow‐ups (we used total active range of movement in preference to poor outcome categories of classification systems); and total of participants with adverse events and total of participants with adverse events requiring (or indicated for) surgery.
Results
Description of studies
Results of the search
We conducted searches up to August 2020. We screened a total of 1278 records from the following databases: Cochrane Bone, Joint and Muscle Trauma Group Specialised Register (26 records), CENTRAL (208 records), MEDLINE (462 records), Embase (227 records), CINAHL Plus (63 records), AMED (75 records), WHO ICTRP (138 records), and ClinicalTrials.gov (79 records) (Table 1).
| Database | Period Searched | Date Searched | Number of hits |
|---|---|---|---|
| Cochrane Bone, Joint and Musculoskeletal Trials (BJMT) Specialised Register | 18 June 2019 | 18 June 2019 | 26 |
| CENTRAL | August 2020, Issue 8 | 11 August 2020 | 208 |
| MEDLINE | January 1946 to August 2020 | 10 August 2020 | 462 |
| Embase | January 1980 to June 2019 | 18 June 2019 | 227 |
| CINAHL PLUS | January 1937 to June 2019 | 18 June 2019 | 63 |
| AMED | January 1985 to August 2020 | 10 January 2017 | 75 |
| ClinicalTrials.gov | 11 August 2020 | 79 | |
| WHO International Clinical Trials Registry Platform (ICTRP) | 18 June 2019 | 138 |
Among all searches, we identified a total of 47 articles for potential inclusion, for which we obtained full reports where possible. After linking any references pertaining to the same study under a single study ID, we identified 40 studies. Upon further analysis, we included 17 studies (Abdel Sabour 2018; Adolfsson 1996; Farzad 2014; Geetha 2014; Gelberman 1991; Gulke 2018; Hagberg 2000; Kneafsey 1994; Ozkan 2004; Poorpezeshk 2018; Rigo 2017; Scavenius 2000; Silva 2003; Stenekes 2009; Trumble 2010; Uday Raj 2018; Vialaneix 2003). We excluded 12 studies (Bainbridge 1994; Baktir 1996; Horsfall 2016; ISRCTN80184286; Kingston 2014; NCT01939808; Peck 1998; Peck 2014; Percival 1989; Stegink Jansen 1990; Xiao 2018; Yildirim 2010). Four studies are awaiting classification (Kitis 2009; Liu 2004; Naude 2019; Yavari 2009). We found seven ongoing studies from searching the WHO ICTRP (CTRI/2019/01/016821; IRCT201310138177N8; IRCT20150721023277N7; NCT03812978; NCT03850210; NCT04237415; NCT04385485). A flow diagram summarising the study selection process is shown in Figure 1.
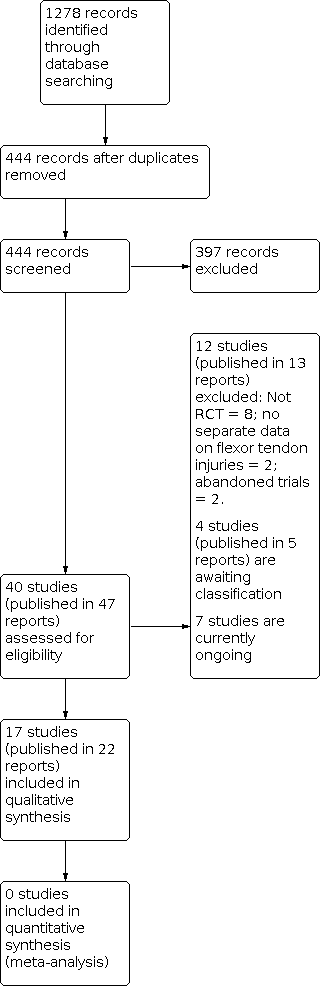
Diagram showing the flow of studies through the study selection process
Translation from German to English was obtained for one included study (Gulke 2018).
Included studies
Full descriptions of each of 17 included trials is provided in the Characteristics of included studies table. A summary of the each study's characteristics and participant details is included in Table 2.
| Study | Country | Setting | Recruited Participants; Digits; Tendons | Final follow‐up Participants; Digits; Tendons | Zones | Age (years) Mean (Range) | Male | Female |
|---|---|---|---|---|---|---|---|---|
| Egypt | Rehabilitation Department | 33; NR; 45 | 26; NR; 36 | I‐III | 26.8 (15‐60)a | 21a | 5a | |
| Sweden | NR | 96; 106; NR | 82; 91; 118 | II | 37a | 54a | 28a | |
| Iran | Hand therapy clinic | 54; 64; 108 | 54; 64; 108 | II | 28.5 (13‐50) | 37 | 17 | |
| India | Hospital | 106; 139; NR | 100; 131; NR | II | G1: NR (10‐45)a G2: 35 (22‐50)a | 89a | 11a | |
| USA | Multi‐centre hospital | 51; 60; 102b | 51; 60; 102 | II | 29.4a | NR | NR | |
| Germany | Physiotherapy clinic | 62; NR;NR | 59; NR; NR | II | 29.5 (18‐60) | 44 | 18 | |
| Sweden | NR | 100; 108; NR | NR; NR; NR | II | NR | NR | NR | |
| UK | Plastic surgery centre | 112; NR; NR | 80; NR; NR | I‐III | NR | NR | NR | |
| Turkey | Hand surgery centre | 25; 41; NR | 23; 39; NR | I‐V | 24 (7‐43) | 15 | 10 | |
| Iran | Plastic surgery centre | 97; 114; 114 | 77; 92; 92 | I‐III | 27a | 60a | 17a | |
| Norway | Orthopaedic surgery centre | 53; 73; 73 | 45; 63; 63 | I‐III | 38.7 (18‐72)c | 36c | 14c | |
| Denmark | Hand surgery centre | 39; 39; 39 | 33; 33; 33 | I‐II | NR | NR | NR | |
| Brazil | Hand surgery centre | 84; NR; 152 | NR; NR; NR | II | 34 (18‐66) | NR | NR | |
| Netherlands | Plastic surgery centre | 28; NR; NR | 25; NR; NR | All | 33.5a | 18a | 7a | |
| USA | Multi‐centre hand surgery centre | 103; 119; 238 | 89; 102; 204 | II | 29 (15‐51)a | 63a | 30a | |
| India | Plastic surgery centre | 30; NR; NR | 30; NR; NR | V | NR | NR | NR | |
| France | NR | 35; NR; NR | NR; NR NR | II | 35 | NR | NR |
NR: Not reported; G1: Group 1; G2: Group 2
aOnly reported at follow‐up (not at baseline)
bParticipants were only eligible if they were available for the 6 month follow‐up. Thus, this number is likely to have been much higher than reported here.
cExcludes 3 participants who experienced tendon ruptures after randomisation.
Design
Sixteen trials were described as randomised, although six did not describe the randomisation process used (Hagberg 2000, Kneafsey 1994, Scavenius 2000; Silva 2003; Stenekes 2009; Vialaneix 2003). Gelberman 1991 was quasi‐randomised. All trials used a parallel‐group design and allocated participants into one of two intervention arms. All studies appeared to randomise at the level of the participant. Of note is that the composition of the ultrasound intervention in Geetha 2014 was changed twice during study recruitment; this was not randomised.
Setting
The 17 included trials were conducted in 13 countries: two each in India (Geetha 2014; Uday Raj 2018), Iran (Farzad 2014; Poorpezeshk 2018), Sweden (Adolfsson 1996; Hagberg 2000) and USA (Gelberman 1991; Trumble 2010); and one each in Brazil (Silva 2003), Denmark (Scavenius 2000), Egypt (Abdel Sabour 2018), France (Vialaneix 2003), Germany (Gulke 2018), Netherlands (Stenekes 2009), Norway (Rigo 2017), Turkey (Ozkan 2004) and UK (Kneafsey 1994).
There were two multicentre studies (Gelberman 1991.Trumble 2010). Three studies did not state clearly how many centres were involved (Abdel Sabour 2018; Hagberg 2000; Vialaneix 2003). The remainder were all single‐centre studies.
Studies were conducted in various clinical settings. This included rehabilitation, physiotherapy or hand therapy clinics (Abdel Sabour 2018; Farzad 2014; Gulke 2018) or hospital departments or centres such as plastic surgery, hand surgery and orthopaedic surgery (Geetha 2014; Gelberman 1991; Kneafsey 1994; Ozkan 2004; Poorpezeshk 2018; Rigo 2017; Scavenius 2000; Silva 2003; Stenekes 2009; Trumble 2010; Uday Raj 2018). Three studies did not report where the study was conducted (Abdel Sabour 2018; Hagberg 2000; Vialaneix 2003).
The earliest study was published in 1991 (Gelberman 1991).
Funding sources and potential conflicts of interest
Ten studies did not disclose funding sources or potential conflicts of interest (Adolfsson 1996; Farzad 2014; Gelberman 1991; Hagberg 2000; Kneafsey 1994; Ozkan 2004; Scavenius 2000; Silva 2003; Stenekes 2009; Vialaneix 2003). Three studies reported receiving no financial support (Abdel Sabour 2018; Rigo 2017; Uday Raj 2018). Three studies received funding to support their research (Geetha 2014; Poorpezeshk 2018; Trumble 2010). Additionally, Abdel Sabour 2018 and Trumble 2010 reported conflicts of interest but did not state what these were. Five studies stated that they had no conflicts of interest to declare (Geetha 2014; Gulke 2018; Poorpezeshk 2018; Rigo 2017; Uday Raj 2018).
Participants
A total of 1108 participants were recruited into the 17 trials. The number of participants in each trial ranged from 25 (Ozkan 2004) to 112 (Kneafsey 1994). Only 10 studies reported the sex distribution of participants (Abdel Sabour 2018; Adolfsson 1996; Farzad 2014; Geetha 2014; Gulke 2018; Ozkan 2004; Poorpezeshk 2018; Rigo 2017; Stenekes 2009; Trumble 2010). Further, while some studies reported the sex distribution at baseline, others reported those available at follow‐up or analysis. From the 608 participants for which data were available, 74% were male. Age data were reported in 13 studies (Abdel Sabour 2018; Adolfsson 1996; Farzad 2014; Geetha 2014; Gelberman 1991; Gulke 2018; Ozkan 2004; Poorpezeshk 2018; Rigo 2017; Silva 2003; Stenekes 2009; Trumble 2010; Vialaneix 2003); see Table 2. The distribution of ages for those studies in which it was reported ranged from 7 years (Ozkan 2004) to 72 years (Rigo 2017). Five studies reported including children (Abdel Sabour 2018; Farzad 2014; Geetha 2014; Ozkan 2004; Trumble 2010). However, no studies focused specifically on rehabilitation interventions for children.
Nine studies focused on flexor tendon injuries in flexor tendon zone II (Adolfsson 1996; Farzad 2014; Geetha 2014; Gelberman 1991; Gulke 2018; Hagberg 2000; Silva 2003; Trumble 2010; Vialaneix 2003). One study included injuries in zone I or II (Scavenius 2000); three studies included zones I to III (Kneafsey 1994; Poorpezeshk 2018; Rigo 2017); one study included zone I to V injuries (Ozkan 2004); one study included only zone V injuries (Uday Raj 2018) and two studies included injuries in all flexor tendon zones (Abdel Sabour 2018; Stenekes 2009).
In two studies, participants contributed one digit each with one or two tendon lacerations; participants with multiple digit lacerations were not included (Scavenius 2000; Silva 2003). In nine studies, participants contributed one or more than one digit to the study (Adolfsson 1996; Farzad 2014; Geetha 2014; Gelberman 1991; Hagberg 2000; Ozkan 2004; Poorpezeshk 2018; Rigo 2017; Trumble 2010). In the remaining six studies, it was unclear if participants with more than one digit or tendon lacerations were included in the study (Abdel Sabour 2018; Gulke 2018; Kneafsey 1994; Stenekes 2009; Uday Raj 2018; Vialaneix 2003).
Intervention and comparisons
The trials presented findings across different treatment interventions. Ten studies focused on our main comparison examining exercise regimens with the same or different orthosis designs (Abdel Sabour 2018; Farzad 2014; Hagberg 2000; Kneafsey 1994; Rigo 2017; Scavenius 2000; Silva 2003; Trumble 2010; Uday Raj 2018; Vialaneix 2003). Mobilisation regimens tested included:
-
early active flexion plus controlled passive exercise regimen versus early controlled passive exercise regimen (modified Kleinert protocol) (Rigo 2017);
-
early active flexion plus passive exercise regimen (Strickland and Small protocol) versus controlled passive exercise regimen (Kleinert protocol) (Vialaneix 2003);
-
active flexion plus active extension exercise regimen versus passive flexion plus active extension exercise regimen (Scavenius 2000);
-
active flexion exercise regimen versus controlled passive exercise regimen (Hagberg 2000);
-
active exercise regimen versus immobilisation regimen (Silva 2003);
-
early place and hold progress to tendon gliding exercise regimen (multiple treatments) versus early passive progressed to active exercise regimen (multiple treatments) (Uday Raj 2018);
-
place and hold exercise regimen versus controlled passive exercise regimen (Abdel Sabour 2018; Farzad 2014; Trumble 2010);
-
early passive flexion exercise regimen (modified Duran protocol) versus early controlled passive exercise regimen (modified Kleinert protocol) (Kneafsey 1994).
Other interventions included duration of rehabilitation programme and return to unrestricted activities (Adolfsson 1996); devices such as an exoskeleton (Gulke 2018) and a continuous passive motion device (Gelberman 1991); ultrasound therapy (Geetha 2014); laser therapy (Ozkan 2004; Poorpezeshk 2018) and motor imagery (Stenekes 2009). Rehabilitation interventions varied in intensity, duration and setting.
Outcomes
The outcomes measured in each trial are summarised in an outcome matrix in Table 3.
| Study ID | Function: patient‐reported | Active ROM | Adverse event | Passive ROM | Strength | Return to work | Function: objective measure | Quality of life | Satisfaction |
|---|---|---|---|---|---|---|---|---|---|
| X | X | X | X | ||||||
| X | X | X | X | X | |||||
| X | X | ||||||||
| X | X | X | |||||||
| X | X | ||||||||
| X | X | X | X | X | |||||
| X | X | ||||||||
| X | X | ||||||||
| X | X | X | |||||||
| X | X | X | |||||||
| X | X | X | X | ||||||
| X | X | X | |||||||
| X | X | ||||||||
| X | X | X | |||||||
| X | X | X | X | X | X | ||||
| X | X | X | |||||||
| X | X | X |
Primary outcome measures
Six of the 17 studies reported our primary outcome of interest, functional status using a patient‐reported outcome measure. Three studies used a subjective assessment of overall function using a visual analogue scale (VAS) (Adolfsson 1996; Rigo 2017; Stenekes 2009). One study used the MHQ (Stenekes 2009) and three studies used the DASH outcome measure (Abdel Sabour 2018; Gulke 2018; Trumble 2010).
All studies but one (Poorpezeshk 2018) measured our primary outcome of interest, active ROM. However, ROM was reported using several different classification systems that are based on goniometric ROM measurements used to calculate categories, from a poor to an excellent overall outcome. These include the Strickland‐Glogovac (Strickland 1980), Strickland or Modified Strickland (Strickland 1985), Tang (Tang 2007), International Federation of Societies for Surgery of the Hand (IFSSHP) (Silva 2003); Lousville (Lister 1977), Tsuge (Tsuge 1977) and Buck‐Gramcko (Buck‐Gramcko 1976) classifications. Total active motion (TAM) (Kleinert 1983; ASSH 1976) calculates the total active range of motion of the digits including the metacarpophalangeal (MCP), proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints. Three classification systems (Strickland‐Glogovac, Strickland, Tang) categorise outcomes as excellent, good, fair/satisfactory, poor or failure for zone II injuries (Table 4). They calculate the sum of active ranges of motion of the PIP and DIP joints (total flexion minus extension deficits). Motion is reported as a percentage of the contralateral side. If the contralateral PIP and DIP joint is not measured, the total is assumed to be 175 degrees. The IFSSH classification is similar but instead of the contralateral ROM the total active movement is calculated as a percentage of total passive movement. Classification systems (Lousville, Tsuge, Buck‐Gramcko) that are based on measurement of movement using fingertip to palm distance were not included as an outcome of interest in our review due to the lack of standardisation of this outcome measure and inherent subjectivity in its measurement. The Lousville classification system (Lister 1977) incorporates the extension deficit as well as movement measured in cm of the distance from the fingertip to the distal palmar crease. The Tsuge classification (Tsuge 1977) measures the distance between finger pulp and distal palmar crease and the angle of each joint with the fingers in maximum flexion. The Buck‐Gramcko system (Buck‐Gramcko 1976) incorporates range of motion, total extension lag and fingertip to nail distance; and has separate grading systems for digits and thumb. Where a classification system is based purely on goniometric measurement (e.g. Strickland classification systems), we report on the number of participants who had a 'poor' outcome. This is due to the inconsistency in cut‐off measurements used to classify 'good' to 'excellent' outcomes. Flexion contractures, extension deficits and joint / tendon lags are also evaluated using ROM measured with a goniometer and have been reported as adverse events for the purpose of this review.
| Classification system | Outcome (% motion achieved) | Excellent | Good | Fair or satisfactory | Poor | Failure |
| Strickland‐Glogovac | % active PIP + DIP ROM (active flexion ‐ extension deficit) compared to contralateral side or 175 degrees* | 85% to 100% | 70% to 84% | 50% to 69% | 0% to 49% | Not applicable |
| ROM (in degrees) | > 150 | 125 to 149 | 90 to 124 | < 90 | Not applicable | |
| Strickland or Modified Strickland | % active PIP + DIP ROM (active flexion ‐ extension deficit) compared to contralateral side or 175 degrees* | 75% to 100% | 50% to 74% | 24% to 49% | 0% to 24% | Not applicable |
| ROM (in degrees) | > 132 | 88 to 131 | 45 to 87 | < 44 | Not applicable | |
| Tang*** | % active PIP + DIP ROM compared to contralateral side or 175 degrees* | 90% to 100% | 70% to 89% | 50% to 69% | 30% to 49% | < 30% |
| IFSSH | % Total active motion compared to total passive motion** | 75% to 100% | 50% to 74% | 24% to 49% | 0% to 24% | Not applicable |
| Total Active Motion | % active MCP + PIP + DIP ROM (active flexion ‐ extension deficit) compared to contralateral side | Normal | > 75% | 50% to 75% | < 50% | < pre‐surgery |
DIP: distal interphalangeal; IFFSH: International Federation of Societies for Surgery of the Hand; MCP: metacarpophalangeal; ROM: range of movement; PIP: proximal interphalangeal
*The sum of active ROM of the PIP and DIP joints is calculated in degrees. This is done by adding the flexion achieved at the PIP and DIP joints and subtracting any extension deficits from the total. Motion is reported as a % of the contralateral side. It is assumed that 175 degrees is the sum of motion of the normal PIP and DIP joints of the unaffected side. % motion achieved = ((PIP + DIP flexion) ‐ (PIP + DIP extension deficit)) X 100 divided by 175.
** % motion achieved = (Total active motion X 100) divided by Total passive motion.
***According to Tang, the excellent and good scores are further divided into plus and minus sub‐grades based on their grip strength and quality of motion (investigator’s subjective judgement of the coordination, visual arc and speed of motion).
The studies that reported ROM using the different classification systems include: TAM (Farzad 2014; Gelberman 1991; Hagberg 2000; Scavenius 2000; Stenekes 2009; Uday Raj 2018), Strickland‐Glogovac classification (Gelberman 1991; Rigo 2017 ), Strickland classification (Farzad 2014; Geetha 2014; Gulke 2018; Ozkan 2004; Scavenius 2000; Silva 2003; Vialaneix 2003), Lousville classification(Adolfsson 1996; Vialaneix 2003; Uday Raj 2018), Tang classification (Rigo 2017), Tsuge classification (Adolfsson 1996) and Buck‐Gramcko classification (Adolfsson 1996; Ozkan 2004). The mean values for active ROM for individual joints was provided by two studies (Gulke 2018; Hagberg 2000). Individual joint active ROM for the affected digit's interphalangeal joints for each participant was provided by only one study (Gelberman 1991). One study used another non‐validated, non‐standardised classification system that was not clearly described in the paper (Kneafsey 1994). While Silva and colleagues (Silva 2003) stated they used the IFSSH system, the classification system reported was not referenced in the paper.
Fifteen of the studies reported our primary outcome of interest, adverse events (Abdel Sabour 2018; Adolfsson 1996; Farzad 2014; Geetha 2014; Gelberman 1991; Gulke 2018; Hagberg 2000; Ozkan 2004; Poorpezeshk 2018; Rigo 2017; Scavenius 2000; Silva 2003Trumble 2010; Uday Raj 2018; Vialaneix 2003). Adverse events were not reported in two studies (Kneafsey 1994, Stenekes 2009). Tendon rupture was the only adverse event consistently reported in all of the studies that reported adverse events. One study reported the timing of the ruptures (Rigo 2017) and two studies reported the intra‐operative findings of the cause of the ruptured tendon (Rigo 2017; Silva 2003). In the fifteen studies that clearly reported the presence or absence of tendon ruptures, there were a total of 41 tendon ruptures reported ranging between zero ruptures in three studies (Farzad 2014; Poorpezeshk 2018; Uday Raj 2018) to a maximum of 13 ruptures (Hagberg 2000). It was difficult for the review authors to determine how many secondary surgeries were performed in total, as several papers reported rupture as an adverse event, but did not clearly state whether these patients went on to have secondary repairs or reconstructions of the tendon ruptures. Secondary surgeries for ruptured tendons were reported by three studies (Rigo 2017; Trumble 2010; Vialaneix 2003). One study reported that one patient underwent a DIP fusion (Vialaneix 2003). Another common secondary surgery performed after a flexor tendon repair is a tenolysis, in which scar tissue is removed to allow the tendon to move freely. Only three studies reported the number of participants undergoing tenolysis (Silva 2003; Scavenius 2000; Vialaneix 2003). In these three studies, a total of 21 patients required a tenolysis. Few studies reported other adverse events including rates of infections (Gelberman 1991), delays in post‐operative wound healing (Rigo 2017; Geetha 2014 ), or diagnosis of chronic regional pain syndrome / Sudeck's disease (Rigo 2017; Gulke 2018). Flexion contracture or extension deficit was reported in five studies (Abdel Sabour 2018; Geetha 2014; Gulke 2018; Hagberg 2000; Trumble 2010).
Secondary outcome measures
-
Passive finger ROM using goniometric measurement was reported in one study (Poorpezeshk 2018).
-
Hand grip strength was reported in nine studies (Adolfsson 1996; Geetha 2014; Gulke 2018; Kneafsey 1994; Ozkan 2004; Rigo 2017; Scavenius 2000; Stenekes 2009; Uday Raj 2018).
-
Return to activity (including return to work) was addressed in three studies. Absence from work was recorded and compared between the two groups in one study (Adolfsson 1996). Mean and range for number of days to return to full duties without restriction was reported for each group in one study (Trumble 2010). Mean and range of days to return to work for all participants regardless of group was reported in one study (Vialaneix 2003).
-
Functional assessment using an objective measure was reported in one study, which used both the Jebsen‐Taylor hand function score and the Purdue Pegboard dexterity test (Trumble 2010).
-
Quality of life using a self‐report measure was not reported by any study.
-
Satisfaction with the intervention provided and whether the patients would recommend the treatment was investigated in one study (Gulke 2018). Another study measured patient satisfaction with Laser/placebo intervention using an analogue scale from 1 (dissatisfied) to 7 (completely satisfied) (Poorpezeshk 2018). Two studies reported a similar construct, satisfaction with hand function after the surgery using an analogue scale (Abdel Sabour 2018; Trumble 2010).
We obtained additional data not reported in study publications from trial authors of the following studies: Adolfsson 1996; Geetha 2014; Ozkan 2004; Rigo 2017. A number of attempts to contact authors of the other 13 trials for clarification were unsuccessful.
Excluded studies
We excluded 12 studies after review of the full‐text publication (Bainbridge 1994; Baktir 1996; Horsfall 2016; ISRCTN80184286; Kingston 2014; NCT01939808; Peck 1998; Peck 2014; Percival 1989; Stegink Jansen 1990; Xiao 2018; Yildirim 2010). Two studies (Kingston 2014; Xiao 2018) were excluded as they included participants who may have had a flexor tendon injury; however, separate data were not available for only the participants with flexor tendon injuries. Two studies found through a trial registry were abandoned before recruitment started (ISRCTN80184286; NCT01939808). The main reason for excluding the other eight studies was because a non‐randomised study design was used.
Studies awaiting classification
Four studies are awaiting classification pending either clarification from the authors or translation to English (Kitis 2009; Liu 2004; Naude 2019; Yavari 2009). Kitis 2009 compared early active mobilisation versus passive mobilisation but it is unclear whether it is a randomised trial. Liu 2004 appears to have randomised 62 children to a multi‐component intervention group consisting exercises with an occupational therapist‐play or to a control group that received general rehabilitation. This article, which was identified after editorial review, requires translation from Chinese. Naude 2019 was a pilot feasibility study that compared graded active digital flexion with a modified Duran protocol focusing on passive digital flexion in 31 participants with zone II, later extended to include zone I, II and IV flexor tendon injuries of the hand. There was a substantial loss to follow‐up, leaving only 14 participants at eight weeks follow‐up. We retained this recently identified trial in this section given its currently minimal contribution to the evidence base. Yavari 2009 examined active mobilisation commenced at 14 days versus four weeks of immobilisation in 240 people, but requires multiple clarifications, including whether this study is a randomised trial (no evidence in support of this description); an imbalance in the numbers allocated; and incorrect data and percentages that do not compute to whole numbers (indicating that these data may be incorrect).
Ongoing studies
Details of seven ongoing studies are given below:
1. CTRI/2019/01/016821: trial registered in January 2019 comparing conventional hand therapy versus an assistive device for a three month period (2 sessions per day for 60 minutes) in 120 participants in India. The main outcomes are active flexion and total active movement measured at 3 and 6 weeks, and 3, 6 and 12 months. The listed secondary outcomes include grip and pinch strength, and function using the Quick‐DASH at the same time points. This study has not yet been completed.
2. IRCT201310138177N8: trial registered in November 2013 in Iran randomising 20 participants between the ages of 15 and 60 years to either an active or passive mobilisation regimen. Although this study is reported as being completed, we have not found a published report. Outcomes include adverse events, range of motion, grip and pinch strength.
3. IRCT20150721023277N7: trial registered in August 2018 comparing early active to passive exercise regimen for zone I and II flexor tendon repairs in participants over the age of 12 years. This is randomised parallel intervention trial aiming to recruit 30 participants is being conducted in Iran and will have the following primary outcomes: satisfaction with ADL tasks and hand function. The listed secondary outcomes include: DASH, fine motor dexterity, range of motion, grip strength, and pinch strength.
4. NCT03812978: trial registered in February 2019 randomised 101 participants following FDP tendon repair in Sweden to either a smart phone application programme to improve exercise adherence or a control group. Both groups receive a standard hand therapy programme. According to the trials register, this study has completed recruitment but no data have yet been reported. The primary outcomes are related to adherence. The listed secondary outcomes include self‐efficacy and range of motion.
5. NCT03850210: trial registered in June 2015 and is now completed, but no data are yet available. This UK‐based trial randomised 60 participants over age 16 years with zone II flexor tendon repair to either a traditional long forearm based splint or a Manchester short splint that allows wrist movement. Primary outcome includes range of motion, and secondary outcome includes adverse events.
6. NCT04237415: trial registered retrospectively in January 2020, which states that recruitment for the trial has been completed. This trial, undertaken at UMUT ERASLAN, Pamukkale University, Turkey, randomised 22 participants to either EMG biofeedback or a control group. Primary outcome includes finger joint range of motion (measured at 6, 12, and 24 weeks), electrical muscle activity (at 5, 12, and 24 weeks), grip strength (12 and 24 weeks), and the Michigan Hand Questionnaire (at 5, 12 and 24 weeks).
7. NCT04385485: trial registered retrospectively in May 2020, for which trial recruitment has been completed. This Swedish trial randomised 64 participants aged 16 years and older who have had either zone I or II tendon injuries to either active rehabilitation or passive rehabilitation groups. Primary outcome includes range of motion (measured at 4, 8 and 12 weeks, and 6 and 12 months). Secondary outcomes include grip strength and pinch strength (at 6 and 12 months), adverse events including tendon rupture, need for secondary operation (within the first 12 months), function measured using the DASH (at 3, 6 and 12 months).
Risk of bias in included studies
Full details of the 'Risk of bias' assessments are presented in the Characteristics of included studies. Summaries are presented in Figure 2and Figure 3. For studies in which we rated a risk of bias as unclear, we attempted to contact the trial authors to request clarification or additional data. Where authors provided additional information or data, this has been recorded in the Characteristics of included studies. Additional information on study methods and data used in the risk of bias assessment was obtained from (Adolfsson 1996; Geetha 2014; Ozkan 2004; Rigo 2017).

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
We rated generation of the randomisation sequence to be at low risk of bias in 10 trials (Abdel Sabour 2018; Adolfsson 1996; Farzad 2014; Geetha 2014; Gulke 2018; Ozkan 2004; Poorpezeshk 2018; Rigo 2017; Trumble 2010; Uday Raj 2018). Three of these trials used a random envelope draw of cards created for the study (Adolfsson 1996; Rigo 2017; Trumble 2010). One trial used a computerised random number generator (Farzad 2014); two studies used stratified block randomisation (Gulke 2018; Poorpezeshk 2018); one used random card selection (Geetha 2014); one used a random number table (Ozkan 2004); and one study used a lottery system (Uday Raj 2018). One study used a quasi‐randomisation sequence by allocating participants to groups based on whether they were born in an even or odd number month (Gelberman 1991). Six studies did not clearly report the randomisation process used (Hagberg 2000, Kneafsey 1994, Scavenius 2000; Silva 2003; Stenekes 2009; Vialaneix 2003), and attempts to obtain this information from trial authors were unsuccessful.
Allocation concealment was rated to be at low risk of bias in five trials (Abdel Sabour 2018; Adolfsson 1996; Geetha 2014; Rigo 2017; Trumble 2010). Allocation concealment was rated to be at high risk of bias in Gelberman 1991, where participants were placed in one of two study groups depending upon the month in which they were born. The remaining 11 studies were rated as having unclear risk of bias, as they did not report a clear method for concealing the allocation sequence (Farzad 2014; Gulke 2018; Hagberg 2000; Kneafsey 1994; Ozkan 2004; Poorpezeshk 2018; Scavenius 2000; Silva 2003; Stenekes 2009; Uday Raj 2018; Vialaneix 2003). Attempts to clarify this with trial authors were unsuccessful.
Blinding
Five studies were rated as having low risk of performance bias (Farzad 2014; Geetha 2014; Gelberman 1991; Ozkan 2004; Scavenius 2000). Three studies achieved blinding of both participants and study personnel for self reported outcomes and were rated as having low risk of bias as these studies did not include any patient self reported outcomes (Farzad 2014; Geetha 2014; Gelberman 1991). One study (Ozkan 2004) achieved blinding of the participants, but it is unlikely that the personnel were blinded due to the nature of the intervention. Scavenius 2000 was rated as having low risk of bias as none of the outcomes were self‐reported or measured by the treatment provider. Eight included studies were not able to achieve participant blinding due to the nature of interventions and were rated as having a high risk of bias (Abdel Sabour 2018; Adolfsson 1996; Gulke 2018; Rigo 2017; Silva 2003; Stenekes 2009; Trumble 2010; Vialaneix 2003). Four studies (Hagberg 2000; Kneafsey 1994; Poorpezeshk 2018; Uday Raj 2018) were classified as having an unclear risk of bias regarding blinding of participants and personnel. One study (Uday Raj 2018) reported that participants were blinded from which group they were in, but were aware they were receiving one of the interventions. Due to the nature of the intervention, care providers could not be blinded to the intervention. It is not known how successful the blinding of the participants was considering the care providers could not be blinded. It was classified as unclear risk as attempts to clarify this with trial authors were unsuccessful. Another study with an unclear rating was Poorpezeshk 2018, which stated in the clinical trials registry that the study was "double‐blinded". However it is unclear where this blinding occurred. Due to the nature of the interventions, it is possible that the participants could have been blinded to the interventions, but this was not explicitly stated.
Blinding of outcome assessment (detection bias) was assessed in two categories, for self‐reported measures and measurements recorded by observers. For self‐reported measures, where these were available, blinding was considered to be low risk for Ozkan 2004 only. It was unclear whether blinding was achieved in two studies that did have self‐reported outcomes (Abdel Sabour 2018; Poorpezeshk 2018). In these instances, an explicit statement regarding assessor blinding was not included in the trial description, and attempts to clarify this issue with trial authors were unsuccessful. The risk was considered to be high for five studies (Adolfsson 1996; Gulke 2018; Rigo 2017; Stenekes 2009; Trumble 2010). The other nine studies did not include any self‐reported outcomes.
Blinding of outcome assessment (detection bias) for objective outcomes was deemed to be low risk of bias in four included studies (Farzad 2014; Geetha 2014; Ozkan 2004; Poorpezeshk 2018). It was unclear whether blinding of outcome assessors was achieved in nine studies (Abdel Sabour 2018; Gulke 2018; Hagberg 2000; Kneafsey 1994; Scavenius 2000; Silva 2003; Stenekes 2009; Uday Raj 2018; Vialaneix 2003). In these instances, an explicit statement regarding assessor blinding was not included in the trial description, and attempts to clarify this issue with trial authors were unsuccessful. The risk of bias from unblinded outcome assessors was considered to be high for four studies (Adolfsson 1996; Gelberman 1991; Rigo 2017; Trumble 2010). Adolfsson 1996 only blinded the assessors for the final outcome assessment at 24 weeks, but not at the earlier time points of assessment. Blinding of outcome assessors was not undertaken in the other three studies, which clearly reported that measurement of outcomes was performed by the treating therapists (Gelberman 1991; Rigo 2017; Trumble 2010).
Incomplete outcome data
Seven studies did not clearly report if any of the participants were lost to follow‐up (Gelberman 1991; Hagberg 2000; Kneafsey 1994; Ozkan 2004; Scavenius 2000; Silva 2003; Vialaneix 2003). Of the 10 studies that reported the loss to follow‐up of the participants, three included trials achieved complete follow‐up of the data set (Farzad 2014; Stenekes 2009; Uday Raj 2018). Only five studies reported number of participants lost to follow‐up for each group (Abdel Sabour 2018; Geetha 2014; Poorpezeshk 2018; Rigo 2017; Trumble 2010). Two studies (Adolfsson 1996; Gulke 2018) reported the total number of participants in the study lost to follow‐up (i.e. no specific reporting of the number lost in each group). The time interval when the loss to follow‐up occurred was not clearly reported. The biggest loss to follow‐up was noted by Poorpezeshk 2018, in which 20 participants were lost to follow‐up, all from the control group. Studies were examined for attrition bias at three time intervals: less than three months, three to six months, and greater than six months.
For outcomes measures under three months, we rated five studies as having low risk of bias (Abdel Sabour 2018; Farzad 2014; Geetha 2014; Rigo 2017; Uday Raj 2018). Seven studies were rated as unclear risk either due to insufficient data being provided in the study publications and no further data being received from the trial authors upon request (Gulke 2018; Hagberg 2000; Kneafsey 1994; Ozkan 2004; Stenekes 2009; Trumble 2010; Vialaneix 2003). Two studies did not collect data at this time point (Gelberman 1991; Silva 2003). We rated two studies at high risk of bias (Adolfsson 1996; Poorpezeshk 2018). In Adolfsson 1996, the number of participants and digits contributed to the study was provided via correspondence from the study authors. The 82 participants who were included in the analysis did not include 14 drop‐outs, eight of whom were lost to follow‐up. It is unclear from which group the 14 drop‐outs were excluded from or the reasons for lost to follow‐up. In Poorpezeshk 2018, the loss to follow‐up was 34% in the control group (with no dropouts in the intervention group), which may have influenced the effect size.
For outcomes measured between three and six months, we rated two studies as having low risk of bias (Geetha 2014; Rigo 2017). We rated six as having unclear risk of bias due to insufficient data being provided in the study publications and no further data being received from the trial authors upon request (Abdel Sabour 2018; Gulke 2018; Hagberg 2000; Kneafsey 1994; Trumble 2010; Vialaneix 2003). One study, Adolfsson 1996, was rated as having high risk of bias, as it is not clear how the dropouts were accounted for in the analysis or which groups they were in.
Only six studies measured outcomes beyond six months (Gelberman 1991; Hagberg 2000; Rigo 2017; Scavenius 2000; Silva 2003; Trumble 2010). Of these, two were rated to be at low risk of bias for completeness of outcome data (Rigo 2017; Trumble 2010). Three studies rated as having an unclear risk of bias did not provide sufficient information in their publications and attempts to obtain this were unsuccessful (Hagberg 2000; Scavenius 2000; Silva 2003). Gelberman 1991 was rated to be at high risk of bias as it was not clear how many participants dropped out of the study, and only those who were a minimum of six months following surgery were included.
Selective reporting
We rated two studies as having a low risk of bias for selective reporting (Abdel Sabour 2018; Poorpezeshk 2018). We rated seven studies as having an unclear risk of bias for selective reporting due to insufficient information being provided in the publications for the studies, and attempts to obtain this information from the trial authors were unsuccessful (Farzad 2014; Gelberman 1991; Gulke 2018; Ozkan 2004; Rigo 2017; Scavenius 2000; Trumble 2010). We assessed eight studies as having a high risk of bias for selective outcome reporting, as they did not specify results for some of the outcomes listed in the methods section of the publication, or in a published protocol (Adolfsson 1996; Geetha 2014; Hagberg 2000; Kneafsey 1994; Silva 2003; Stenekes 2009; Uday Raj 2018; Vialaneix 2003).
We compared the outcomes reported to their study design as reported on the clinical trial register where available. We were only able to retrieve trial registration documents for three studies (Abdel Sabour 2018; Geetha 2014; Poorpezeshk 2018).
Other potential sources of bias
We rated six studies to be at high risk of other bias (Abdel Sabour 2018; Geetha 2014; Rigo 2017; Scavenius 2000; Stenekes 2009; Uday Raj 2018), mainly because of unit of analysis errors. However, the unit of analysis was not always clearly stated when reporting outcomes in some of the included studies. Some measurements like grip and pinch strength are recorded per hand, whereas other outcomes may be reported per digit or per tendon repair (that is, one or more tendons can be repaired in the same digit). This means that it is very easy for a unit of analysis error to occur and can lead to errors in analysis and misleading interpretation of the study's findings. Five studies clearly reported the unit of analysis for their outcome measures and four were assessed as being at low risk of bias (Adolfsson 1996; Farzad 2014; Gelberman 1991; Trumble 2010). The other study, Rigo 2017, was rated at high risk of other bias, as strength was analysed as a finger level outcome, rather than hand/participant level outcome; hence, a unit of analysis error occurred. Eight studies were rated as having an unclear risk of bias, due to insufficient information being provided to make a judgement (Gulke 2018; Hagberg 2000; Kneafsey 1994; Ozkan 2004; Poorpezeshk 2018; Silva 2003; Uday Raj 2018; Vialaneix 2003). Four other studies were identified as being at high risk of bias and it appears as if an unit of analysis error was likely (Abdel Sabour 2018; Geetha 2014; Hagberg 2000; Stenekes 2009). Like Rigo 2017, Geetha 2014 analysed grip strength for each of the digits included in the study; however, grip strength is calculated per hand/participant and this likely to have resulted in an unit of analysis error. Similarly, it is unclear whether the number of ruptures that occurred were per person, digit or tendon in Hagberg 2000. In Stenekes 2009, pinch strength was measured for each affected digit; however, the unit of analysis appears to be affected tendons. In Abdel Sabour 2018, the unit of analysis is tendons not fingers; however, measurements such as range of motion, scar adhesion and DASH are measured at the finger or person level. A unit of analysis error appears to have occurred for these outcomes as analyses appear to have been conducted per tendon.
Geetha 2014 additionally reported outcomes of movement and strength in non‐standardised categories. These ranges for movement and strength were not uniform between the groups and not recorded at the same time interval. This made it difficult to compare the outcomes between the groups. Further, Rigo 2017 recorded grip and pinch strength as a percentage of the contralateral side, with no consideration made in the analysis for hand dominance.
Scavenius 2000 was rated as high risk as the intervention groups also received different surgical treatments which may have influenced the results.
Effects of interventions
See: Summary of findings 1 Early active flexion plus controlled passive exercise regimen versus early controlled passive exercise regimen for rehabilitation following surgery for flexor tendon injuries of the hand; Summary of findings 2 Active exercise regimen compared with an immobilisation regimen following surgery for flexor tendon injuries of the hand; Summary of findings 3 Place and hold exercise regimen versus controlled passive exercise regimen following surgery for flexor tendon injuries of the hand
We were able to perform very limited meta‐analyses because of clinical heterogeneity or incomplete outcome reporting of the included trials. Summary data and effect estimates (with 95% CIs) for all trials are presented where available. If an outcome is not referred to in a subsection or table, then no data for that outcome were available in the trials. If there is no analysis reported for a particular outcome for a comparison, trialists reported insufficient data (e.g. no standard deviations for continuous outcomes) to perform the required analysis. Our attempts to obtain missing data were generally unsuccessful. Where possible, we have provided as much detail as possible from the original source, for transparency and to enhance interpretation of the findings.
There were no trials testing the following comparison categories that were prespecified as 'main comparisons' in the protocol.
-
different types of orthoses;
-
different orthosis wearing regimens, including duration;
-
different timings for commencing mobilisation;
-
different types of scar management;
-
different timings for commencing strengthening.
We created 'Summary of findings' tables for the following three exercise regimen comparisons, which were selected as they are commonly used in current clinical practice (Bigorre 2018; Tang 2018b).
-
Early active flexion plus controlled passive exercise regimen versus early controlled passive exercise regimen (modified Kleinert protocol) (summary of findings Table 1).
-
Active exercise regimen versus immobilisation regimen (summary of findings Table 2).
-
Place and hold exercise regimen versus controlled passive exercise regimen (summary of findings Table 3).
Suitability of trials for meta‐analysis
Most comparisons were tested by single trials only. Of the two comparisons tested by two and three trials respectively, we considered it appropriate to pool only one outcome (tendon rupture).
In addition, 11 (of 17) trials reported data that could not be included in the statistical analysis, for several reasons:
-
omission of measures (or errors) of variability (e.g. SDs) in reports of continuous outcomes (Adolfsson 1996; Hagberg 2000; Poorpezeshk 2018; Scavenius 2000; Trumble 2010; Vialaneix 2003);
-
conclusions stated without support for point estimates, or frequency counts of outcomes (Hagberg 2000; Stenekes 2009);
-
lack of reporting of the time point of measurement (Stenekes 2009);
-
conclusion stated with no point estimate, or data for either group (Adolfsson 1996; Hagberg 2000; Kneafsey 1994; Scavenius 2000; Trumble 2010; Uday Raj 2018; Vialaneix 2003); and,
-
data were skewed and reported in a format not able to be entered into RevMan 5 (Abdel Sabour 2018); and,
-
comparison of data between groups were measured at different time points or used different outcome definitions (Geetha 2014).
Early active flexion plus controlled passive exercise regimen versus early controlled passive exercise regimen alone
One trial (Rigo 2017), which randomised 53 participants with 73 zone I to III FDP tendon repairs, evaluated the addition of active flexion exercises to a controlled passive exercise regimen comprising a modified Kleinert regimen, which was used in both intervention groups. Both active and passive only groups commenced the exercise regiments at one day post‐surgery.
Outcomes were assessed post‐surgically at one and two months (for ROM only) and at 3, 6 and 12 months (for all outcome measures). The outcomes assessed included functional assessment using a patient reported outcome measure (injured finger use in activities of daily living (ADL) using a visual analogue scale); active finger range of motion (Strickland‐Glogovac and Tang classifications); adverse events (number of participants with tendon ruptures, complex regional pain syndrome, wound dehiscence, finger oedema) and strength (grip and pinch strength).
The main outcomes for this comparison, for which there is only very low‐certainty evidence, are presented in summary of findings Table 1. For all outcomes, the evidence was downgraded two levels due to very serious risk of bias and one level due to serious imprecision, reflecting wide confidence intervals, confidence intervals crossing the line of no effect, or both. The evidence was also downgraded one level for serious indirectness for the functional assessment outcome used in this trial; there is also no information on the minimally important difference for this outcome. Unit of analysis problems resulting from the reporting by digit instead of participant means that the confidence intervals are narrower than they should be. Additionally, although the trial authors provided us with mean and SD data for continuous outcomes, it should be noted these were reported as median (Med) and interquartile range (IQR) data in the trial report. We also present the latter for the ADL results because there were greater disparities between these and the mean and SD data for this outcome.
Primary outcomes
-
Functional assessment using a patient reported outcome measure
-
The use of the injured finger(s) in ADL at 2, 3, 6 and 12 month follow‐ups was evaluated using a visual analogue scale (0 to 10; higher scores = better ADL). The Med and IQR results presented in the trial report are shown in Analysis 1.1, and the mean and SD results provided by the trial authors to us are shown, is in Analysis 1.2.
-
There were no significant between‐group differences at any time point reported by the authors. All differences between the two groups were under 1.0 point and thus unlikely to be clinically important.
-
The exploratory analyses in Analysis 1.2 indicated higher scores in the active group at two months, but not subsequently.
-
-
-
Active finger range of motion
-
Active range of motion was measured using a goniometer as a continuous outcome. Using the individual PIP and DIP joint measurements of the finger, these were summed to calculate TAM. From these data, Strickland‐Glogovac (Strickland 1980) and Tang (Tang 2007) classifications were calculated (refer to Table 4 for a definition for each of the classifications categories).
-
TAM of PIP and DIP joints (in degrees).
-
No evidence of between‐group differences were found between the two groups at any of the follow‐ups (Analysis 1.3).
-
-
Strickland classification (number of fingers that were classified as a "poor" category)
-
There were no significant differences between groups at any time interval (Analysis 1.4). Rigo 2017 also found no statistically significant differences in the distribution of participants in the four categories (excellent, good, fair and poor) for active range of motion for the finger digits at 2, 3, 6 or 12 months. The data at 12 months were excellent (20), good (8), fair (5) and poor (1) for the active group and excellent (14), good (6), fair (5) and poor (4) for the control group; reported P = 0.247.
-
-
Tang classification (number of fingers that were classified as a "failure" or "poor" result (Analysis 1.4).
-
There were no significant differences between groups at any time interval.
-
-
-
Adverse events
-
Overall, there were six adverse events reported in the active group versus nine adverse events in the control group (RR 0.58, 95% CI 0.23 to 1.44; Analysis 1.5).
-
Tendon rupture
-
Two FDP tendon ruptures occurred in the active group at weeks 5 and 6 respectively, whereas one FDP rupture was reported at week 12 in the control group. All ruptures underwent secondary surgery.
-
-
Complex regional pain syndrome
-
The only participant developing this adverse outcome was in the control group.
-
-
Wound dehiscence
-
Delayed wound healing or superficial infection was seen in six fingers in the control group versus none in the active group.
-
-
Swelling and tenderness of the tendon sheaf (all transitory)
-
This was seen in four fingers in the active group versus one in the control group.
-
-
Secondary outcomes
One secondary outcome, strength, was reported for Rigo 2017 (Table 3).
-
Strength
-
Grip strength (percentage of the contralateral hand)
-
There was no evidence of important differences between two groups at 3, 6 or 12 months follow‐ups in grip strength (Analysis 1.6).
-
-
Pinch strength (percentage of the contralateral hand)
-
Pinch strength was better at three and six months in the active group; however, this advantage did not persist at 12 months (Analysis 1.6).
-
-
Early active flexion plus passive exercise regimen (Strickland and Small protocol) versus controlled passive exercise regimen (Kleinert protocol)
One trial, Vialaneix 2003, randomised 35 participants who had a primary flexor tendon repair in zone II into two intervention groups listed in the heading. At the third post‐operative day, 16 participants randomised to the active group commenced early passive flexion, active flexion and active extension within the orthosis using the Strickland exercise regimen (Strickland 2000; Small 1989) and 19 participants commenced early controlled passive mobilisation using rubber band traction, according to the Kleinert regimen (Kleinert 1967).
Outcomes were measured at an average of 18 months following the surgery, but also reported at 8, 12 and 24 weeks. Outcomes measured included active finger range of motion (Strickland classification); fingertip to palm distance (not an outcome of interest for this review); adverse events (subsequent surgical procedures) and return to previous activity (total duration of time off work after the surgery for a subgroup of 15 manual workers).
This trial was reported as a conference abstract only and provided very limited and incomplete data. The certainly of the available evidence for this comparison is very low, reflecting downgrading two levels for very serious risk of bias and two levels for very serious imprecision.
Primary outcomes
-
Functional assessment using a patient reported outcome measure
-
Not reported
-
-
Active finger range of motion
-
Using the Strickland classification, the total percentages of participants achieving "good‐excellent" results in the two groups were reported at 8, 12 and 24 weeks. These are shown below. Some of the percentages do not correspond to whole numbers if the numbers randomised (16 versus 19) are used. The authors reported that the study did not show any significant difference in "functional outcome" between the two groups.
-
At 8 weeks (percentage of participants with good or excellent outcomes): 75% active group versus 95% controlled passive group (probably corresponds to 18/19 versus 12/16)
-
At 12 weeks (percentage of participants with good or excellent outcomes): 81% active group versus 94% controlled passive group
-
At 24 weeks (percentage of participants with good or excellent outcomes): 92% active group versus 100% controlled passive group
-
-
-
Adverse events
-
These were not reported. However, subsequent surgery required in eight participants comprised five tenolysis, one DIP fusion and two flexor tendon grafts due to late rupture. No breakdown was provided by treatment group.
-
Secondary outcomes
No secondary outcomes were reported for individual groups for Vialaneix 2003 (Table 3).
Active flexion plus active extension exercise regimen (plus modified Kessler suture surgical technique) versus passive flexion plus active extension exercise regimen (plus grasping suture and external pull‐out know surgical technique)
Scavenius 2000 randomised 39 participants with zone I and II flexor tendon repairs into either an active flexion plus active extension exercise regimen group (active group) or passive flexion plus active extension exercise regimen group (passive group). Each group also received a different surgical technique with the active group having a Modified Kessler suture (Ti‐cron 4.0) repair, and the passive group receiving a grasping suture (Prolene 2.0) and external pull‐out knot technique. Participants had flexor tendon repairs to the thumb (n = 6) or digits (n = 33) in flexor tendon zone I or II. The active group (n = 20) also performed active extension exercises but performed active flexion exercises (instead of passive) which was described as a Mantero protocol. The passive group (n = 19) performed active extension and controlled passive flexion exercises (using a protocol reported by study authors to have been developed "by May E. et al").
The outcomes assessed at one year following surgery included active finger range of motion (TAM and Strickland classification for the FDP repairs of the digits only; that is, this outcome was not calculated for the thumb tendon repairs) and adverse events (tendon ruptures, scar adhesions requiring tenolysis surgery).
This trial was reported as a conference abstract only and provided very limited and incomplete data. Data were missing for the number of participants in each group in the analyses and no measures of variability were provided for range of motion. The certainly of the available evidence for this comparison is very low, reflecting downgrading two levels for very serious risk of bias, two levels for very serious imprecision and one level for serious indirectness (as the groups received different surgical techniques).
Primary outcomes
-
Functional assessment using a patient reported outcome measure
-
Not reported.
-
-
Active finger range of motion
-
TAM for the digits (numbers in each group not reported)
-
Scavenius 2000 reported that there was no significant difference between the two groups in mean TAM as a percentage of normal values: active group was 70.1% compared with the passive group at 75.7%.
-
-
Strickland classification
-
Scavenius 2000 reported the differences in the percentages of participants in the four categories (excellent, good, fair and poor) for active range of motion for the finger digits was not significant. Data for the two groups were for excellent (25%), good (8%), fair (67%) and poor (0%) for the active group and excellent (27%), good (33%), fair (40%) and poor (0%) for the passive group.
-
-
-
-
Active thumb IP joint motion (numbers in each group not reported)
-
Scavenius 2000 reported the mean range of motion for the repaired thumb tendons was 51.7 degrees in the active group and 66.7 degrees in the passive group (between group difference reported as not significant: reported P = 0.7).
-
-
-
Adverse events.
-
-
Adverse events were recorded for each group were the number of participants who experienced a tendon rupture and the number of participants with scar adhesions that required surgery (tenolysis surgical procedure). Data for these are presented Analysis 2.1.
-
Tendon ruptures. All three tendon ruptures occurred in the active group.
-
Tenolysis surgery was required for four participants in the active group and two participants in the passive group.
-
-
Secondary outcomes
No secondary outcomes were reported for Scavenius 2000 (Table 3).
Active flexion exercise regimen versus controlled passive exercise regimen
One trial, Hagberg 2000, which was reported in a published abstract only, randomised 100 participants who had direct tendon repair for zone II lacerations in 108 digits. They compared an early active mobilisation group (active group) with an early controlled passive mobilisation using rubber band traction group (controlled passive group). The exercise regimen and orthosis were continued for three weeks following the tendon repair, after which participants were allowed to commence active mobilisation. No further details on the trial participants, including the numbers in each group, were provided.
The outcomes reported in the abstract were limited to active finger range of motion (TAM and DIP joint flexion) and adverse events (tendon ruptures; extension deficit) at one year. The data were incomplete and unusable and it is unclear whether the results applied to participants or digits. The certainly of the available evidence for this comparison is very low, reflecting downgrading two levels for very serious risk of bias and two levels for very serious imprecision.
Primary outcomes
-
Functional assessment using a patient reported outcome measure
-
Not reported.
-
-
Active finger range of motion
-
TAM
-
The median range of motion was 245 degrees in the early active group versus 250 degrees in the controlled passive group. The authors stated there was no statistically significant difference between the groups.
-
-
DIP active motion
-
The median active motion was 65 degrees in the active group and 58 degrees in the controlled passive group. The authors stated there was no statistically significant difference between the groups.
-
-
-
Adverse events
-
Tendon ruptures
-
There were 13 tendon ruptures overall, five of which occurred in the active group and eight in the controlled passive group.
-
-
Extension deficit of the DIP joint.
-
The median extension deficit was 5 degrees in both groups.
-
-
Secondary outcomes
No secondary outcomes were reported for Hagberg 2000 (Table 3).
Active exercise regimen versus immobilisation regimen
One study, Silva 2003, compared an early active exercise regimen (active group) with an immobilisation regimen (immobilisation group) following a zone II flexor tendon repairs in 84 people (152 tendons). Both groups received a dorsal blocking orthosis to protect the flexor tendon repair for three weeks following surgery. The active group commenced an exercise programme 12 hours after surgery. The program consisted of 10 hourly motions of active flexion‐extension during a 16 hour waking day. The immobilisation group did not perform any exercises in the orthosis. After three weeks, the orthosis was discarded by both groups.
Outcomes were evaluated at a mean of 22 months post surgery (range 12 to 36 months). Outcomes assessed included finger range of motion (to calculate outcomes as per the IFSSH and Strickland classifications (described in Table 4) and adverse events (indication for tenolysis surgery; tendon ruptures and repair of these).
The main outcomes for this comparison, for which only very low certainty evidence is available, are presented in summary of findings Table 2.
Primary outcomes
-
Functional assessment using a patient reported outcome measure
-
Not reported.
-
-
Active finger range of motion
-
Only the number of participants for each of the IFSSH or Strickland classification groups were reported. For the analysis, we present the numbers in the poor categories of the two outcomes. At 12 months or more post‐surgery, the active exercise group had fewer poor outcomes than the immobilisation group when rated using either the IFSSH (1/37 versus 15/47; RR 0.08, 95% CI 0.01 to 0.61) or Strickland's classification (0/37 versus 7/47; RR 0.08, 95% CI 0.00 to 1.43; very low‐certainty evidence); seeAnalysis 3.1.
-
Trial authors reported that according to the IFSSH classification (% of participants in this category(number of digits)):
-
Active exercise group: excellent 0% (n = 0); good 65% (n = 24); satisfactory 32% (n = 12); poor 3% (n = 1).
-
Immobilisation group: excellent 0% (n = 0); good 43% (n = 20); satisfactory 25% (n = 12); poor 32% (n = 15).
-
-
Trial authors reported the following according to the Strickland's classification (% of participants in this category(number of digits)):
-
Active exercise group: excellent 62% (n = 23); good 35% (n = 13); satisfactory 3% (n = 1); poor 0% (n = 0).
-
Immobilisation group: excellent 47% (n = 22); good 23% (n = 11); satisfactory 15% (n = 7); poor 15% (n = 7).
-
-
-
Adverse events
-
The overall number of participants experiencing one or more adverse events was not reported.
-
Tendon ruptures was reported in 13.5% of the participants in the active group (5 of 37 participants), all of which occurred in the second week after commencing active mobilisation (Analysis 3.2). All participants underwent immediate surgical rerepair performed in the same way as the primary tendon suture and were returned to the early active exercise regimen. No participants in the Immobilisation group experienced a tendon rupture.
-
-
-
Tenolysis surgery was not required by participants in the active group compared with 21% participants (10 of 47 participants) of the immobilisation group, whose range of motion deficit fulfilled the indication criterion for tenolysis (Analysis 3.2). However, it is not clear whether these went on to have tenolysis.
-
Actual or indicated secondary surgery for tendon rupture or a range of motion deficit indicating scar adhesions
-
Secondary surgery was either tendon repair in the active group or indication for tenolysis in the immobilisation group (5/37 versus 10/47; RR 0.64, 95% CI 0.24 to 1.70; very low‐certainty evidence; Analysis 3.2).
-
-
Secondary outcomes
One secondary outcome was reported for Silva 2003 (Table 3).
-
Passive finger range of motion
-
Although measured to calculate the IFFSH classification, these data were not reported separately in the publication.
-
Early place and hold progressed to tendon gliding exercise regimen versus early passive progressed to active exercise regimen
One randomised study of 30 participants with zone V flexor tendon repairs evaluated the benefits between two types of multiple treatment exercise regimens (Uday Raj 2018). One group received of early mobilisation with place and hold exercises commenced in the first week which progressed to a graduated tendon gliding exercise program at four weeks (place and hold group). The second intervention group received a passive exercise regimen which was progressed to full active exercises of all finger joints at four weeks (passive group). Both groups received the same standard hand therapy treatments and both were placed in dorsal blocking splints (although at different positions for the wrist‐ place and hold at 20 to 30 degrees and passive at 45 to 50 degrees).
Outcomes were evaluated at 4 and 12 weeks for range of motion; and at 12 weeks for grip strength. Outcomes included active finger range of motion (TAM); active finger tip to distal palmar crease distance (not an outcome of interest for this review); wrist active range of motion (not an outcome of interest for this review); adverse events (tendon ruptures) and strength (grip strength measured using a Jamar Dynamometer). The certainly of the available evidence for this comparison is very low, reflecting downgrading by two levels for very serious risk of bias, two levels for very serious imprecision for tendon rupture and one level for serious indirectness, reflecting the inadequate description of outcome assessment.
Primary outcomes
-
Functional assessment using a patient‐reported outcome measure
-
Not reported.
-
-
Active finger range of motion
-
Data for active ROM was reported as a percentage difference in mean values of TAM between the 12 week and initial measurement at four weeks, and reported for individual digits (i.e. index, middle, ring and small digit data were reported separately). Requests to the trial authors for more information, including final ROM data, were unsuccessful.
-
-
Adverse events
-
Only tendon rupture was reported; there were none in either group.
-
Secondary outcomes
One secondary outcome was reported for Uday Raj 2018 (Table 3).
-
Strength
-
Grip strength was measured at 12 weeks post surgery using a Jamar hand‐held dynamometer, and reported as the percentage difference in strength between the participant's affected hand and their unaffected hand. The place and hold group had significantly greater difference between their affected and non affected sides than the passive group (MD 6.90%, 95% CI 4.86 to 8.94; Analysis 4.1).
-
Place and hold exercise regimen versus controlled passive exercise regimen
Three heterogeneous trials compared place and hold exercise (place and hold group) versus controlled passive exercise (controlled passive group) (Abdel Sabour 2018; Farzad 2014; Trumble 2010).
Abdel Sabour 2018 recruited 33 participants (45 tendons) following a 2‐strand flexor tendon repair; this study included zones I, II and II flexor tendon injuries. Both groups were placed in a dorsal blocking orthosis with the wrist positioned in 20 degrees flexion and MCP joints in 70 degrees flexion. Exercises commenced three days following the repair. The place and hold exercise regimen consisted of passive flexion of the affected finger and then the participant tried to maintain the flexed posture through contraction of the involved muscle for five seconds. Controlled passive exercise regimen consisted of passive finger flexion achieved by the modified Kleinert rubber band traction system. Both groups performed additional active extension plus passive range of motion of each digit. The place and hold group were allowed to progress to active wrist tenodesis glides but the time interval has not been specified. They performed 25 repetitions of each exercise every waking hour for the first six weeks post‐surgery. At six weeks, the orthosis was discarded. Outcomes, which were assessed from six weeks up to six months, included functional assessment using a patient reported outcome measure (DASH score); adverse events (tendon rupture; scar adherence; flexion contracture; extension lag) and satisfaction with the result of the surgery.
Farzad 2014 randomised 54 participants (64 digits; 108 tendons) with zone II flexor tendon injuries into the two exercise regimen groups. Participants in both groups were placed in a dorsal blocking orthosis with their wrist positioned at 0 to 30 degrees of flexion and their MCP joints in 70 to 90 degrees flexion. Exercises were commenced three days following a 2‐strand flexor tendon repair. Participants of the place and hold group were advised to passively flex their fingers using the other hand with their wrist in 30 degrees of extension (out of the orthosis), and then hold the finger position actively for 3 to 5 seconds, performing 10 repetitions four times a day. In the controlled passive group, flexion was caused by rubber band traction within the dorsal blocking orthosis. Patients performed active finger extension within the dorsal blocking orthosis, performing 10 repetitions every waking hour. At three weeks, both groups progressed to active exercises. Outcomes, which were assessed at eight weeks by an independent blinded assessor, included active finger range of motion (TAM) of PIP and DIP joints combined, Strickland classification (described in Table 4) and adverse events (tendon ruptures).
Trumble 2010 randomised 103 participants (119 digits) who had undergone 4‐strand zone II flexor tendon repair to a place and hold regimen using a tenodesis orthosis or to a passive exercise regimen using an orthosis with rubber band traction. Participants of the place and hold group were placed in a dorsal blocking orthosis for six weeks and were also provided with a tenodesis orthosis (using a wrist hinge) to perform exercises during the first four weeks post‐operation. Place and hold finger exercises were initiated on day three, active flexor tendon gliding exercises at week four, and composite wrist and finger flexion exercises were introduced at week five post‐surgery. Participants of the controlled passive group performed a combination of Kleinert and Duran protocols. This included being placed in a rubber band traction orthosis and coming out of the orthosis to perform passive flexion‐extension and active interphalangeal extension during the first three weeks post‐operation. Place and hold exercises were introduced at three weeks post‐operation and active finger flexion commenced at six weeks. Range of motion and flexion contracture were evaluated at 6, 12, 26 and 52 weeks. All other outcomes were assessed at one year post‐surgery. These included functional assessment using a patient‐reported outcome measure (DASH score); active finger range of motion (PIP and DIP joints); adverse events (tendon ruptures, flexion contracture); return to previous activity (total days from injury to return to work on full duties); functional assessment using an objective measure (Jebsen‐Taylor hand function score, Perdue Pegboard test); satisfaction with the result of the surgery (numerical analogue scale from 1 (dissatisfied) to 10 (completely satisfied).
The main outcomes for this comparison, for which only very low certainty evidence is available, are presented in summary of findings Table 3.
Primary outcomes
-
Functional assessment using a patient reported outcome measure (DASH score, 0 to 100 with a higher score indicating more disability); see Analysis 5.1.
-
This was reported in two trials but at different times (6 months and 12 months).
-
Reflecting the non‐normal distribution of the results, Abdel Sabour 2018 reported Med and IQR and found no evidence of a difference between the two groups at six months: place and hold group Med 23, IQR 2 to 26; passive group Med 15, IQR 10 to 30; reported P = 0.62. They also reported mean and standard deviations in their discussion, which are shown in an exploratory analysis, again showing no evidence of a difference between the two groups (MD ‐1.10, 95% CI ‐14.44 to 12.24; 26 participants; very low‐certainty evidence; downgraded one level for serious risk of bias and two levels for very serious imprecision).
-
Trumble 2010 found no important difference in function between the two groups at one year (MD ‐1.10, 95% CI ‐2.77 to 0.57; 89 participants; very low‐certainty evidence; downgraded two levels for very serious risk of bias and one level for imprecision, reflecting potential ceiling effects given the very low DASH scores indicating minimal upper limb disability).
-
-
-
Active finger range of motion; see Analysis 5.2
-
Active finger range of motion was reported using a continuous range of motion outcome (TAM) in Abdel Sabour 2018 and Trumble 2010, and also as a dichotomous outcome by categorising the continuous outcome into four categories (Poor; Good; Satisfactory; Excellent) using the Strickland Classification System in Abdel Sabour 2018. Active range of motion was not directly reported in Abdel Sabour 2018 but goniometry data would have been used to assess contracture and deformity (see adverse events).
-
Farzad 2014 found the TAM at PIP and DIP joint was significantly better in the place and hold group compared with the controlled passive group at eight weeks (MD 32.00 degrees, 95% CI 15.5 to 48.5; 64 digits; very low certainty evidence).
-
Trumble 2010 found greater active range of motion in the place and hold group at 6, 12, 26 weeks and, as shown in Analysis 5.2, at 52 weeks: MD 28.00 degrees, 95% CI 18.87 to 37.13; 102 digits; very low certainty evidence). The number of participants or digits included in the analyses for the 6, 12 and 26 week time points were not reported.
-
In Farzad 2014, no digits in the place and hold group had a "poor" outcome according to the Stickland classification system compared with nine in the controlled passive group at eight weeks (0/31 versus 9/33; RR 0.06, 95% CI 0.00 to 0.92; Analysis 5.3). The numbers of digits in each category were as follows: place and hold group: excellent: 45% (n = 14); good 32% (n = 10); satisfactory 23% (n = 7); poor 0% (n = 0); controlled passive group: excellent: 24% (n = 8); good 18% (n = 6); satisfactory 30% (n = 10); poor 27% (n = 9).
-
-
-
Adverse events
-
-
The available data for these, reported by tendons (digits) rather than participants, are presented in Analysis 5.4. There were no data for overall numbers of participants incurring one or more adverse events. Only Abdel Sabour 2018 reported on adverse events other than tendon rupture.
-
-
Three tendon ruptures were reported for Abdel Sabour 2018, none in Farzad 2014 and four in Trumble 2010. There was no evidence of a difference between groups (3/96 participants or tendons versus 4/100; RR 0.81, 95% CI 0.19 to 3.50; 196 participants). All four participants in Trumble 2010 underwent surgery to re‐repair the tendons using a two‐stage surgical reconstruction; they were all excluded from final analysis.
-
Abdel Sabour 2018 reported no tendons had scar adherence in the place and hold group compared with 14 in the controlled passive group (0/16 versus 14/20; RR 0.04, 95% CI 0.00 to 0.66). Specific criteria for assessing scar adherence were not provided in this study and it is unclear whether further intervention was undertaken.
-
Abdel Sabour 2018 measured flexion contracture at DIP joint and PIP joint and then as a combined DIP + PIP joint measure. The results probably applied to follow‐up at six weeks.There were fewer DIP joint contractures in the place and hold group: 1/16 versus 10 of 20 tendons (RR 0.13, 95% CI 0.02 to 0.88); as well as fewer PIP joint contractures in the place and hold group (3/16 versus 8/20; RR 0.47, 95% CI 0.15 to 1.48). Abdel Sabour 2018 reported significantly lower combined DIP and PIP flexion deformity, measured in degrees, at six weeks in the place and hold group but we are unsure of these data and have not reported these here. Although assessed in Trumble 2010, data for flexion contractures were not reported.
-
Tendon lag was calculated in Abdel Sabour 2018 by measuring the difference between the passive and active range of motion at the PIP joint and DIP joint to calculate the FDS and FDP tendon lag respectively. Presence of a lag was reported (number of patients with lag as a percentage of participants in that group). Tendon lag is generally reported as an arc of motion (in degrees).There were fewer digits with FDP tendon lag in the place and hold group (2/16 versus 15/20; RR 0.25, 95% CI 0.06 to 0.98) as well as there were fewer digits with FDS tendon lag (2/16 versus 10/20; RR 0.17, 95% CI 0.04 to 0.62).
-
-
Secondary outcomes
Two secondary outcomes were reported for Abdel Sabour 2018, three for Trumble 2010 but none for Farzad 2014 (Table 3). The evidence was of very low certainty, downgraded at least one level for serious risk of bias and two levels for very serious imprecision, for all secondary outcomes.
-
Passive finger range of motion
-
This was measured and used to calculate the tendon lag for Abdel Sabour 2018, as reported in adverse events above, but separate data were not provided.
-
-
Return to previous activity
-
Excluding the four participants with tendon ruptures, Trumble 2010 reported that the participants in the place and hold group returned to full‐duty work without restriction significantly earlier (P < 0.05) with an average of 82 days (range 68 to 94 days) compared with an average of 103 days (range 76 to126 days) in the controlled passive group.
-
-
Functional assessment using objective measures
-
At one year, Trumble 2010 found little difference between the groups in the results of the Jebsen‐Taylor test (MD ‐3.00 seconds, 95% CI ‐9.38 to 3.38; Analysis 5.5) or Purdue pegboard scores (MD 1.00 pegs, 95% CI ‐2.54 to 4.54, Analysis 5.6).
-
-
Satisfaction with the result of the surgery
-
Patients’ satisfaction with their hand function after surgery at three months or longer was evaluated by Abdel Sabour 2018 using a numerical analogue scale ranging from 0 (completely dissatisfied) to 10 (completely satisfied). Reflecting the non‐normal distribution of the data, Abdel Sabour 2018 reported the following findings for 26 participants: place and hold group Med 6, IQR 4 to 8.5; passive group Med 4, IQR 2 to 7; reported P = 0.049.
-
Trumble 2010 found little difference between the two groups in satisfaction scores, rated using a numerical rating scale from 1 (dissatisfied) to 10 (completely satisfied), at one year (MD 1.20, 95% CI ‐0.50 to 2.90; Analysis 5.7).
-
Early passive flexion exercise regimen (modified Duran protocol) versus early controlled passive exercise regimen (modified Kleinert protocol)
Kneafsey 1994 compared controlled passive flexion exercise regimen using a modified Duran, Strickland and Glogovac protocol (passive group) with a controlled passive flexion plus active extension using a modified Kleinert protocol exercise regimen (controlled passive group) in 112 participants with either zones I, II or III tendon lacerations. Participants in the passive group performed isolated and composite flexion in the orthosis without the rubber band traction, and both active and passive extension within the orthosis. Participants in the controlled passive group performed active extension exercises, and fingers were maintained in passive flexion using rubber band traction orthosis between exercises. The sole report of this trial was a published conference abstract reporting an interim analysis of the first 80 participants.
Outcomes measured, up to a possible six months, included active finger range of motion and strength (power grip, pinch grip and maximum finger pressure) measured using a Jamar dynamometer. No data were provided and the timing of the follow‐up to which statistical significance testing applied is unclear.
Primary outcomes
-
Functional assessment using a patient reported outcome measure
-
Not reported.
-
-
Active finger range of motion
-
The authors reported that there was no statistical significance difference in outcome between the two groups (P > 0.05).
-
-
Adverse events
-
Not reported.
-
Secondary outcomes
One secondary outcome was reported for Kneafsey 1994 (Table 3).
-
Strength
-
The authors reported that there was no statistical significance difference in outcome between the two groups (P > 0.05).
-
Unrestricted activity at 8 weeks post‐surgery versus unrestricted activity at 10 weeks post‐surgery
Adolfsson 1996 randomised 96 participants (106 digits) with zone II flexor tendon lacerations to either unrestricted hand activity commenced at eight versus ten weeks following surgery. Results were reported for 82 participants (91 digits). All participants received standardised interventions for the first six weeks, which included a forearm based orthosis extending to the PIP joint; initial four weeks of passive flexion with rubber band traction and active extension exercises within the orthosis; followed by two weeks of active exercises within the orthosis. The participants were then randomised at six weeks into the two different programmes that advised a gradual increase in loading to unrestricted activities to be commenced at either eight weeks (8‐week group) or ten weeks (10‐week group).
In Adolfsson 1996, active range of motion data and distance from the fingertip and middle of the pulp to the distal palmar crease data were used to calculate the Buck‐Gramcko (Buck‐Gramcko 1976), Louisville (Lister 1977) and Tsuge (Tsuge 1977) classification systems for the fingers; and the Buck‐Gramcko score for FPL repairs (Buck‐Gramcko 1976). None of these results were relevant to this review. Other outcome measures recorded at 16 weeks included subjectively rated functional assessment of hand function using a visual analogue scale; strength (grip strength using a Jamar dynamometer) and return to previous activity (whether they were absent from work or not). The authors did not provide measures of variability for continuous outcomes.
The certainty of the available evidence for this comparison is very low, reflecting downgrading by two levels for very serious risk of bias and two levels for very serious imprecision.
Primary outcomes
-
Functional assessment using a patient‐reported outcome measure
-
Subjective assessment of function, which was measured using a participant's subjective assessment of their own hand function using a visual analogue scale, was equivalent in both groups with a mean value of 88%.
-
-
Active finger range of motion
-
Comparison between the two groups of active ROM was recorded by the trial authors using three different classification scales, none of which are relevant to our review, as they do not rely solely on goniometric measurement. However, Adolfsson 1996 found no significant differences between the groups at any time interval.
-
-
Adverse events
-
Tendon rupture
-
One FDP tendon in the 8‐week group ruptured at seven weeks after the repair; no tendons ruptured in the 10‐week group (Analysis 6.1).
-
-
Secondary outcomes
Two secondary outcomes were reported for Adolfsson 1996 (Table 3).
-
Strength (percentage of the strength of the contralateral hand)
-
Adolfsson 1996 reported the mean grip strength at 16 weeks post surgery was 72% of the uninjured hand in the 8‐week group compared with 76% in the 10‐week group.
-
-
Return to previous activity
-
Of those participants working at the time of injury, 31 participants in the 8‐week group returned to work on average 2.1 weeks earlier than the 29 participants in the 10‐week group.
-
Exoskeleton versus physiotherapy
One randomised study (Gulke 2018) evaluated the benefit of applying an exoskeleton (exoskeleton group) compared with physiotherapy (physiotherapy group) following zone II flexor tendon repairs of both the FDP and FDS tendons in the index, middle or ring fingers in 62 participants. All participants were placed in a modified Kleinert orthosis with rubber band traction on the second day post surgery and commenced active and passive (as required) extension of the fingers within the orthosis (10 repetitions/hour). From the second week post‐surgery, patients were randomised to the exoskeleton group or the physiotherapy group. The exoskeleton group had the device applied by the physiotherapist for 30 minutes three times a week. No other treatments were provided. The physiotherapy group received physiotherapy treatment but the type of treatment and dose was not specified. It is assumed that the physiotherapy intervention was likely to be multi‐modal, consisting of various treatments. Both groups received treatment three times a week until function was deemed by the doctor to be satisfactory.
Outcomes were evaluated at 6, 12 and 18 weeks post‐surgery. Outcomes evaluated included functional assessment using a patient reported outcome measure (DASH score); active finger range of motion (isolated PIP and DIP joint ROM; TAM of the MCP, PIP and DIP joint; Strickland classification); adverse events (extension deficit; tendon ruptures; complex regional pain syndrome); strength (grip and pinch strength); satisfaction with the rehabilitation intervention (not an outcome of interest for this review). Please refer to Table 4 for a description of how the categories for the Strickland Classification (Strickland 2005) were defined in this study.
This article was published in German, and a translation of the article was obtained.
The certainty of the evidence is very low, being downgraded by two levels for very serious risk of bias and one or two levels for serious or very serious imprecision.
Primary outcomes
-
Functional assessment using a patient reported outcome measure
-
The DASH score was used to measure function and disability. This score ranges from 0 to 100 with a higher score indicating more disability.
-
Whilst both groups improved over time, there is very low‐certainty evidence of no clinically important between‐group differences at either 12 weeks (MD ‐2.80, 95% CI ‐7.63 to 2.03; 59 participants) or 18 weeks (MD ‐0.70, 95% CI ‐4.53 to 3.13); see Analysis 7.1.
-
-
-
Active finger range of motion
-
Isolated PIP joints and the DIP joints (as well as MCP joints, which are not the focus of this review) of the affected finger were measured and reported. These measurements were summed to calculate TAM of the affected finger.These measurements were also used to categorise the participants into four outcome groups (Poor; Fair; Good; Excellent) according to the Strickland classification (Strickland 2005).
-
PIP joint active finger range of motion: there is very low‐certainty evidence of little or no between‐group difference in this outcome at any time interval (Analysis 7.2).
-
DIP joint active finger range of motion: there is very low‐certainty evidence of little or no between‐group difference in this outcome at any time interval (Analysis 7.3).
-
TAM of the affected finger: there is very low‐certainty evidence of little or no between‐group difference in this outcome at any time interval (Analysis 7.4).
-
None of the participants in either group had a poor rating according to the Strickland classification at 18 weeks post‐surgery. In the exoskeleton group, the results were: excellent 80% (n = 24); good 18% (n = 5); satisfactory 3% (n = 1); poor 0% (n = 0). In the physiotherapy group, the results were: excellent 62% (n = 18); good 17% (n = 5); satisfactory 20% (n = 6); poor 0% (n = 0).
-
-
-
Adverse events
-
Three types of adverse events were recorded: tendon ruptures, diagnosis of complex regional pain syndrome (CRPS) and extension deficit. Data for the first two outcomes are shown in Analysis 7.5.
-
One participant of the physiotherapy group suffered a tendon rupture.
-
One participant of the exoskeleton group was diagnosed with CRPS at six weeks.
-
The number of participants with extension deficit at the PIP joint was not stated. This outcome was reported only as a continuous outcome (degrees of deficit).
-
-
Secondary outcomes
One secondary outcome was reported for Gulke 2018 (Table 3).
-
Strength
-
Grip strength (kg)
-
At 18 weeks, there were no significant differences between groups (Analysis 7.6).
-
-
Pinch strength between thumb and injured finger (kg)
-
At 18 weeks, there were no significant differences between groups (Analysis 7.6).
-
-
Continuous passive motion device versus controlled passive progressed to active exercise regimen (Modified Kleinert)
Gelberman 1991, a quasi‐randomised trial of 51 participants (60 digits) with zone II flexor tendon repairs, compared continuous passive motion (CPM) device (CPM group) with controlled passive exercise regimen using rubber band traction (controlled passive group). Participants began therapy on the first postoperative day. Digits were protected in dorsal‐blocking orthosis for a minimum of six weeks. The CPM group had the device attached to the protective orthosis on the first day following surgery to allow 60 degrees arc of PIP joint and a 30 to 40 degree arc of DIP joint motion. The CPM group used the device in isolation for 8 to 12 hours a day in the first four weeks. Active movements were introduced at four weeks to be performed in addition to the motion provided by the CPM device. The controlled passive group was placed in a similar dorsal blocking orthosis but with rubber band traction was applied. Patients performed active extension and passive flexion to the palmar crease for the first four weeks, when active flexion was introduced. Gelberman 1991 noted frequent problems with power failures and mechanical breakages of the CPM devices early on as well as issues with adherence; these were alleviated by increased time in patient education, both initially and at intervals throughout the rehabilitation period.
Outcomes were assessed by treating therapists at a minimum of six months post surgery (mean 10.8 months, range: 6 to 38 months). Outcomes included active finger range of motion (TAM and Strickland‐Glogovac classification (Strickland 1980)) and adverse events (infection; tendon rupture).
The evidence for all reported outcomes was of very low certainty, downgraded by two levels for very serious risk of bias and two levels for very serious imprecision.
Primary outcomes
-
Functional assessment using a patient‐reported outcome measure
-
Not reported.
-
-
Active finger range of motion
-
TAM was calculated by summing the total active motion of the MCP, PIP and DIP joints at six months post‐surgery. This was then used to categorise participants into groups according to the Strickland‐Glogovac classification (see below).
-
There is very low certainty evidence of higher TAM values in the CPM group (MD 20.48 degrees, 95% CI 0.89 to 40.07; 59 digits; Analysis 8.1).
-
-
Fewer digits in the CPM group had a poor outcome according to the Strickland‐Glogovac classification (1/29 versus 8/30; RR 0.13, 95% CI 0.02 to 0.97; Analysis 8.2). The data for each of the categories are detailed below:
-
CPM group (% of the entire group in this category(number of digits)): excellent 35% (n = 10); good 31% (n = 9); fair 31% (n = 9); poor 3% (n = 1).
-
Controlled passive group (% of the entire group in this category(number of digits)): excellent 27% (n = 8); good 23% (n = 7); fair 23% (n = 7); poor 27% (n = 8).
-
-
-
Adverse events
-
Gelberman 1991 reported on tendon rupture and infections for each group (Analysis 8.3).
-
One participant in the controlled passive group ruptured both FDP and FDS tendons at four weeks post‐surgery and underwent immediate secondary surgery. His data were not included in the final analysis.
-
No infections occurred in either group.
-
-
Secondary outcomes
No secondary outcomes were reported for Gelberman 1991 (Table 3).
Ultrasound therapy versus control
One study of 106 participants (139 digits with zone II flexor tendon injuries), Geetha 2014, compared the effect of daily ultrasound therapy lasting five minutes on the repair site in the initial three weeks of rehabilitation versus a control group. Both groups were immobilised a dorsal plaster of Paris cast for three weeks with wrist in neutral and MCP joints in 70 degrees flexion and commenced the same mobilisation from three weeks. Over the five‐year duration of the trial, three different ultrasound regimens with different frequencies, intensities and timing were tested in turn. Details of these are provided in Characteristics of included studies. These three groups were neither randomised nor concurrent and we have pooled the data from the three ultrasound groups in the analyses.
Outcomes assessed included change in active finger ROM (combined measurement summing PIP and DIP joint ROM between 3 to 12 weeks, measured in degrees; Strickland Classification (Strickland 1980) at 3 months); grip strength (measured at 12 weeks); and adverse events (wound dehiscence, tendon ruptures, extension lag). Grip strength was inappropriately reported for digits, not participants. The results for ROM were reported for involved fingers instead of participants and thus resulted in unit of analysis errors.
The evidence for all outcomes reported for this comparison was of very low certainty, reflecting downgrading by two levels for very serious risk of bias, one level for serious indirectness and at least one level for serious imprecision, given the low numbers of events and participants.
Primary outcomes
-
Functional assessment using a patient reported outcome measure
-
Not reported.
-
-
Active finger range of motion
-
Change in active ROM between three weeks and three months (PIP and DIP ROM combined), which was reported separately for the three ultrasound groups and control group, was presented as the summed mean totals of combined PIP and DIP joint flexion range or motion (TAM). These are entered into RevMan 5 as three subgroups. We split the numbers of the control group into three in order to provide a pooled estimate for this outcome, which favours ultrasound: MD 26.47 degrees, 95% CI 19.70 to 33.24; 131 digits; Analysis 9.1
-
-
-
Trial authors reported that according to the Strickland's classification (% of participants in this category(number of digits)):
-
Ultrasound (91 digits): excellent 20% (n = 18); good 57% (n = 52); fair (satisfactory) 5% (n = 5); poor 18% (n = 16).
-
Immobilisation group (40 digits): excellent 5% (n = 2); good 20% (n = 8); fair (satisfactory) 10% (n = 4); poor 65% (n = 26).
-
Based on the above data, and adding the two cases with rupture as a poor outcome in the ultrasound group, there were fewer digits with a poor ROM outcome in the ultrasound group: 16/93 versus 26/40; RR 0.26, 95% CI 0.16 to 0.44; 133 digits; Analysis 9.2).
-
-
-
Adverse events
-
Adverse events included tendon ruptures and wound dehiscence which were reported as the number of participants with this adverse event in each group (Analysis 9.3). Data for extension lag deficits were not usable and hence the overall numbers of participants with adverse events were not calculated.
-
Wound dehiscence
-
Wound dehiscence was observed in four participants allocated to ultrasound. Ultrasound therapy was stopped and the four participants were excluded from the study. No control group participants experienced wound dehiscence.
-
-
Tendon rupture
-
Two participants allocated ultrasound experienced tendon rupture after three weeks.
-
-
Extension lag deficits were also measured by the trial investigators. However, the available data were not usable for the following reasons. The method for calculating extension lag was not defined and was used interchangeably with flexion deformities in the publication. Extension lag was also expressed in a non‐standardised format as ranges of extension deficit (measured goniometrically) and these ranges differed between the groups. The time intervals for when this motion was achieved also differed between the groups; some data were reported at eight weeks and some at 12 weeks.
-
Secondary outcomes
One secondary outcome was reported for Geetha 2014 (Table 3).
-
Grip strength
-
Grip strength was inappropriately reported as number of digits rather than participants achieving a certain percentage of contralateral grip strength. This percentage threshold also varied between groups. Thus the reported data are unusable.
-
Low level laser therapy versus control (placebo)
Two heterogeneous trials compared low level laser therapy with a placebo control (Ozkan 2004; Poorpezeshk 2018).
Ozkan 2004 randomised 25 participants (41 digits) with flexor tendon injuries in zones I to V to either GaAs laser therapy (laser group) or a placebo control group. All participants received the Washington rehabilitation program for 12 weeks after surgery. In the laser group, whirlpool and infrared GaAs diode laser of 100 Hz frequency was applied from day 8 to 21 post surgery in 21 digits (13 participants). The control group, 20 digits (12 participants) received the same intervention with the machine switched off (i.e. placebo). Review‐relevant outcomes, which were measured at 12 weeks post surgery, include: active finger range of motion (total active motion, Strickland classification (Strickland 1980)); adverse events (tendon ruptures); and grip strength.
Poorpezeshk 2018, which included 97 participants (114 fingers) with flexor tendon injuries in zones I to III, randomised between red and infrared low level laser therapy (laser group) and a placebo control group, to examine the adjuvant effect of low‐level laser therapy on recovery of tendon injury in patients. Post‐operative care appeared to have consisted of four weeks of immobilisation in a plaster brace. Ten sessions of laser or sham therapy were provided from the second post‐operative day, two to three times a week. The probe was placed over the repair site using contact method. Outcomes were assessed by two independent blinded assessors. Review‐relevant outcomes include adverse events (infection; tendon rupture) and weekly measurement of passive range of motion of the PIP and DIP joints. Final assessments were recorded at four weeks post‐surgery.
We rated the available evidence as very low certainty, downgraded one level for serious risk of bias and two levels for very serious imprecision.
Primary outcomes
-
Functional assessment using a patient reported outcome measure
-
Not reported in either trial.
-
-
Active range of motion
-
Total active motion was reported in Ozkan 2004 only. Ozkan 2004, which did not state how this outcome was derived, did not find evidence of a between‐group difference (MD ‐14.17 degrees, 95% CI ‐36.48 to 8.14; 41 digits; Analysis 10.1).
-
Strickland's classification (number of digits (% of total digits)): One digit in each group was rated as a "poor" outcome based on the Strickland classification (Analysis 10.2). Data for all groups Strickland categories for the laser group were: excellent 60% (n = 12); good 25% (n = 5); fair 10% (n = 2); poor 5% (n = 1); and for the placebo group: excellent 58% (n = 11); good 16% (n = 3); fair 21% (n = 4); poor 5% (n = 1).
-
-
Adverse events
-
Between the two trials, two adverse effects, both tendon rupture, were observed in Ozkan 2004 and one, a wound infection, in Poorpezeshk 2018 (Analysis 10.3).
-
One participant of the laser group of Poorpezeshk 2018 experienced a wound infection, which was managed with conservative treatment.
-
One tendon rupture was reported in each group of Ozkan 2004; both were excluded from the analysis for other outcome measures. No tendon rupture was reported in either group of Poorpezeshk 2018.
-
-
Secondary outcomes
Two secondary outcomes were reported. These were passive finger range of motion reported in Poorpezeshk 2018 and strength in Ozkan 2004 (Table 3).
-
Passive finger range of motion
-
In Poorpezeshk 2018, total passive range of motion at the PIP and DIP joints were measured by a goniometer and recorded after the first session of laser therapy, and at weekly intervals until four weeks.
-
The trial investigators reported that at four weeks, total passive range of motion was greater in the laser group with a mean (SD) of 235 degrees (0.0) compared with 110 degrees(10) for the control group (P < 0.001). Given that an SD 0.0 is unlikely to be correct, these data should be considered unreliable.
-
-
-
Strength
-
In Ozkan 2004, grip strength was calculated as a percentage loss in the affected hand compared with the unaffected side at 12 weeks post surgery. There was very low certainty evidence of little difference between the two groups (MD ‐4.55, 95% CI ‐9.29 to 0.19; Analysis 10.4).
-
Motor imagery intervention versus control
Stenekes 2009, which included any zone of flexor tendon injury, compared kinaesthetic motor imagery of finger flexion movements (motor imagery group) with a control group in 25 participants. Standard care provided to both groups included six weeks using a Kleinert dorsal blocking orthosis; with only passive finger flexion allowed for the first four weeks and then 'place and hold' flexion exercises from four to six weeks. During these six weeks, the motor imagery intervention comprised eight sessions of motor imagery (10 repetitions of mental active flexion, held for three seconds followed by imagined finger extension and stretch) on a daily basis.
Outcomes included functional assessment using a patient‐reported outcome measure (MHQ; a single item question on hand skills using VAS); active finger range of motion (TAM); and strength (grip and pinch strength). Stenekes 2009 also measured preparation time of finger flexion and kinematic analysis including drawing accuracy and speed (which were not outcomes of interest of this review). Final follow‐up was at 12 weeks. The authors did not provide data for functional assessment or ROM outcomes.
The evidence for all outcomes reported for this comparison was of very low certainty, reflecting downgrading by two levels for very serious risk of bias, and at least one level for serious imprecision, given the low numbers of participants.
Primary outcomes
-
Functional assessment using a patient‐reported outcome measure
-
Function was measured using two different questionnaires including the MHQ and a one‐item question on hand skills using a VAS. These were completed for each hand for each participant. Stenekes 2009 reported that there was no significant between group difference for either outcome.
-
-
Active finger range of motion
-
TAM was calculated per hand and recorded as a percentage of the other side. Stenekes 2009 reported that there was no significant difference between groups in TAM.
-
-
Adverse events
-
Not reported.
-
Secondary outcomes
One secondary outcome was reported for Stenekes 2009 (Table 3).
-
Strength
-
Grip strength
-
At 12 weeks, no significant difference in grip strength was found between the two groups (Analysis 11.1).
-
-
Pinch strength
-
At 12 weeks, no significant difference in pinch strength was found between the two groups (Analysis 11.1).
-
-
Subgroup and sensitivity analyses, and assessment of publication bias
We could not perform any subgroup analyses in this review. Clinical heterogeneity of interventions and outcomes, or paucity of specified subgroups, meant that these analyses were not possible. Furthermore, sensitivity analyses were not performed as no meta‐analyses were conducted. Also, we were unable to generate funnel plots to assess small study effects. We consider the risk of publication bias to be low as many of the published studies reported statistically non‐significant results. However, whilst it is possible that some unpublished studies with non‐significant results exist, their inclusion in the review would be unlikely to change our conclusions.
Discussion
Summary of main results
The objective of this systematic review was to determine the effectiveness and safety of various rehabilitation treatments to optimise outcomes following surgery for flexor tendon injuries of the hand compared with no treatment, a control or another rehabilitation treatment. We have considered the results of 17 studies investigating different rehabilitation interventions following flexor tendon surgeries of the hand in a total of 1108 mainly adult participants. Most studies focused on zone II flexor tendon repairs. Only four studies included participants with zones IV and V. Five studies included children as well as adult participants. Most of the participants (74% overall where reported) were male.
The 17 studies were heterogeneous with respect to the types of rehabilitation treatments provided, intensity, duration of treatment and the treatment setting. The comparisons were confined to two comparison categories listed in our protocol. Ten studies focused on our main comparison examining exercise regimens with the same or different orthosis designs. These studies mainly focused on the type of exercises and orthoses prescribed at commencement of the rehabilitation phase. The comparisons of the other seven studies fitted loosely in our final category testing 'different doses for interventions, other than orthosis wearing regimen' that we expanded to include comparisons of a non‐exercise rehabilitation intervention versus control (no or placebo intervention). We found no studies examining the effectiveness of other adjunctive treatments in the early phase of rehabilitation, such as scar management, early oedema management, wound care, orthosis types (especially wrist and finger joint positions and inclusion of the wrist were found.
We rated the evidence available for all reported outcomes of all comparisons as very low certainty, which means that we have very little certainty in the estimates of effect.
Different exercise regimens
The 10 studies testing mobilisation strategies were heterogeneous with respect to the types of rehabilitation treatments provided, intensity, duration of treatment and the treatment setting. Three of these studies, however, tested a similar comparison. We presented the findings of the following three exercise regimen comparisons in 'Summary of findings' tables, as they are commonly used in current clinical practice.
Early active flexion plus controlled passive exercise regimen versus early controlled passive exercise regimen (modified Kleinert protocol)
The evidence for the single trial making this comparison is presented in summary of findings Table 1. The trial recruited 53 participants with mainly zone II flexor tendon repairs but reported data for a maximum of 69 fingers,Standard care was provided to all participants. There is very low‐certainty evidence of no clinically important difference between the two groups in patient‐rated function at 6 or 12 months follow‐up. The same applies to active finger range of motion at the two follow‐up times. There is very low‐certainty evidence of little difference in adverse events: the 15 adverse events comprised three tendon ruptures, six wound dehiscence, one complex regional pain syndrome and five transitory swelling and tenderness of the tendon sheaf. All three tendon ruptures (4.3%) underwent secondary surgery.
Active exercise regimen versus immobilisation regimen for three weeks
The evidence for the single trial making this comparison is presented in summary of findings Table 2. The trial reports data for 84 participants with zone II flexor tendon repairs, The trial did not report on self‐rated function, on range of movement in the medium term (three to six months) or on numbers of participants experiencing one or more adverse events. The very low‐certainty evidence for poor (under one‐quarter of normal) range of finger movement at one to three years follow‐up reflects the trial's very few events, which means we are uncertain of the finding of zero cases in the active group versus seven cases in the immobilisation regimen. The same uncertainty applies to the finding of little difference between the two groups in adverse events or indicated for surgery. All five cases of tendon rupture (13.5% of 37) needing surgical repair occurred after two weeks in the active mobilisation group and all 10 cases of range of motion deficiency (21.3% of 47) indicating scar adhesion and need for tenolysis occurred in the immobilisation group.
Place and hold exercise regimen versus controlled passive exercise regimen
The evidence for the three heterogeneous trials making this comparison is presented in summary of findings Table 3. The trials reported data for a maximum of 194 participants with mainly zone II flexor tendon repairs. The place and hold regimens using orthoses differed among the three trials as did the passive exercise regimens, although all used rubber band traction. The trials did not report on range of movement in the medium term (three to six months) or on numbers of participants experiencing one or more adverse events. The very low‐certainty evidence means we are uncertain of the findings of no difference in self‐rated function using the DASH between the two groups at six months (data from one trial) or at 12 months (data from one trial). There is very low‐certainty evidence from one trial of greater active finger range of motion at 12 months after place and hold. Secondary surgery data were not available; however, we considered that all seven recorded tendon ruptures would have required surgery.
Other exercise comparisons
There was limited and very low‐certainty evidence available for the following five comparisons, each of which was tested by small single trials. In the following, we focus on the outcomes for which data for primary outcomes were presented in an analysis.
-
One trial of 35 participants with zone II flexor tendon repairs compared early active flexion plus passive exercise regimen (Strickland and Small protocol) versus controlled passive exercise regimen (Kleinert protocol). No usable data were available for this comparison, which was published only as a conference abstract.
-
One trial of 39 participants with zone I and II flexor tendon repairs compared active flexion plus active extension exercise regimen versus passive flexion plus active extension exercise regimen. Although presented in an analysis, the number of adverse events of tendon rupture (3) and need for tenolysis surgery (4) are too few to draw any conclusions. This trial was published only as a conference abstract.One trial of 100 participants with zone II flexor tendon repairs compared active flexion exercise regimen versus controlled passive exercise regimen. No usable data were available for this comparison, which was published only as a conference abstract,
-
One trial of 30 participants with zone V flexor tendon repairs compared early place and hold progress to tendon gliding exercise regimen (multiple treatments) versus early passive progressed to active exercise regimen (multiple treatments). No usable data for primary outcomes were available for this comparison.
-
One trial reporting an interim analysis of 80 participants with zones I, II or III tendon lacerations compared early passive flexion exercise regimen (modified Duran protocol) versus early controlled passive exercise regimen (modified Kleinert protocol). No usable data were available for this comparison.
Other comparisons tested in the included trials
The other interventions tested were the duration of rehabilitation programme and return to unrestricted activities (one trial); devices such as an exoskeleton (one trial) and a continuous passive motion device (one trial); ultrasound therapy (one trial); laser therapy (two trials) and motor imagery (one trial). Rehabilitation interventions varied in intensity, duration and setting. All the evidence for the limited outcome results available for these comparisons was rated as very low‐certainty evidence. In the following, we focus on the outcomes for which data for primary outcomes were presented in an analysis.
-
One trial reporting results for 96 participants with zone II flexor tendon repairs compared unrestricted activity at 8 weeks post‐surgery versus unrestricted activity at 10 weeks post‐surgery. The only results presented in an analysis was one tendon rupture.
-
One trial of 62 participants with zone II flexor tendon repairs compared applying an exoskeleton versus physiotherapy reported results at 12 and 18 weeks; thus short‐ and medium term follow‐up. For both follow‐up times, there is very low‐certainty evidence of no clinically important between‐group differences in function assessed using DASH or in active finger range of motion. There was one case of tendon rupture and one of complex regional pain syndrome.
-
One quasi‐randomised trial of 51 participants with zone II flexor tendon repairs compared a continuous passive motion device (CPM) versus controlled passive progressed to active exercise regimen. There is very low‐certainty evidence of marginally higher total active range of motion values in the CPM group at six months. There was one tendon rupture and no infections reported.
-
One trial of 106 participants with zone II flexor tendon repairs compared ultrasound (there were three different ultrasound regimens applied without prior specification in a protocol during the study) versus no ultrasound. Standard care was provided to all participants. There is very low‐certainty evidence of a greater improvement in total active finger motion after ultrasound at three months. Although the two cases of tendon rupture and four cases of wound dehiscence all occurred in the ultrasound group, these events were too few to draw any conclusions.
-
Two heterogeneous trials, including 25 participants with zones I to V repairs and 97 participants with zones I to III repairs, compared low level laser therapy with a placebo control. Standard care was provided to all participants. There is very low‐certainty evidence from the smaller trial of no between group difference in active finger range of motion at 12 weeks. There were two tendon ruptures and one wound infection reported.
-
One trial, published only as a conference abstract, of 25 participants with any zone of flexor tendon injury, compared motor imagery of finger flexion movements with a control group. Standard care was provided to all participants. No usable data were available for our primary outcomes.
Overall completeness and applicability of evidence
Completeness of the evidence
The data available for this review are very limited. The 17 heterogeneous and often poorly reported studies investigated different rehabilitation interventions following flexor tendon surgeries of the hand in a total of 1108 mainly adult participants. The trials tested one of 14 comparisons, 10 of which tested different exercise regimens. Of note, we identified no trials testing several of the 'main comparisons' listed in our protocol: namely, different types of orthoses; different orthosis‐wearing regimens, including duration; different timings for commencing mobilisation; different types of scar management; or different timings for commencing strengthening. Data pooling was undertaken for one outcome (7 cases of tendon rupture in a total of 196 participants or digits) in one comparison tested by three trials (place and hold exercise regimen versus controlled passive exercise regimen). We did not pool data for laser therapy, the only other multi‐trial comparison of tested by more than one trial. Although, with one exception, studies reported on finger range of motion, only six of the 17 studies reported on functional status using a patient‐reported outcome measure. Data were absent or incomplete for most other outcome measures.
Applicability of the evidence
The evidence in this review is limited also in its applicability. In terms of the study populations, it should be noted that most studies focused on zone II tendon repairs. Several studies did not report demographic data, such as gender and age, details of the type of surgery, and sufficiently detailed participant eligibility criteria. Where the populations were described, these were generally young adults and mostly male (Table 2).
Partly reflecting the limited reports, such as conference abstracts only, of several studies, the limited information on the interventions hinders applicability. While the interventions in most of the exercise trials were prescribed at commencement of the rehabilitation phase, the details of the exercise regimens with regard to specific exercises provided, their frequency and repetitions were not generally adequately described. Details of how these programmes were progressed after the first six weeks, through exercise regimens, splinting for contractures, strengthening programmes and return to restricted and or unrestricted activity were lacking.
Many of the studies also reported using concomitant treatments at the same time as the study intervention, possibly confounding the effects of the study intervention. Of particular note is Scavenius 2000, where a different surgical repair technique, which is not a rehabilitation modality, was used in the two groups. When assessing applicability of such trials, it is important to consider that such co‐interventions, whether applied to all participants or differently between the two groups, may have affected the trial findings.
Longer‐term outcomes (greater than six months) were often not collected and thus we are uncertain about the harms and benefits of these treatments at these later time points. Outcomes were not reported in a consistent way. Range of motion was reported using several different classification systems. Different classification systems used within the same studies often achieved different outcomes which makes interpretation of the data challenging. While it is attractive to be able to state how many participants received an excellent versus a poor outcome, these systems use different thresholds, so comparison across classification systems is not possible. Therefore use of goniometric measurement for affected digits (individual joint flexion/extension measurements and TAM) is easier to compare and to interpret the clinical significance across groups within a study and across studies comparing the same interventions. This also allows for interpretation of other important adverse events such as flexion contractures and active lag of the gliding tendons from adhesion formation using an objective goniometric cut‐off, rather than subjective impressions.
In particular, while studies reported on the number of tendon ruptures, it would be useful for clinicians to know details about these ruptures, including information on what stage of rehabilitation that the rupture occurred; if there was a cause identified; how many of these ruptures proceeded to have secondary surgeries; whether they were directly repaired or proceeded to have two stage tendon reconstructions; and the final outcomes that they achieved.
Many studies did not report their trial protocols a priori, or conform to the CONSORT statement for reporting their trial's findings.
Quality of the evidence
We presented ’Summary of findings’ tables only for trials addressing the primary questions of the review using the GRADE approach to assess the quality of all the evidence examined (Schünemann 2011). The certainty of the evidence was very low for the three selected comparisons (summary of findings Table 1; summary of findings Table 2; summary of findings Table 3). Most of the evidence was downgraded for a combination of two out of three reasons. Evidence was based on small, single trials, leading to concerns about imprecise effect estimates. Even with the ability to pool three studies to examine the effectiveness of place and hold exercises versus controlled passive exercise regimens, in most outcomes we were only able to derive meaningful data from one of the studies (summary of findings Table 3). Methodological quality varied across studies, but in general was of low to very low quality. All studies were small, ranging from 25 participants (Stenekes 2009) to a maximum of 100 participants (Geetha 2014; Hagberg 2000). According to the GRADE approach (Schünemann 2011), the overall certainty of the evidence for all outcomes for all intervention comparisons was very low.
Trials were downgraded due to serious risk of bias. Lack of reporting of randomisation sequence generation and allocation concealment, lack of blinding of assessors (performance and detection bias), and attrition bias seriously impacted the quality of the included trials. One of the largest issues was the inadequacy of reporting of study design and methods employed in the trials, leading to unclear risk of bias assessments. Attempts to obtain this information from the authors was unsuccessful in most cases. Inconsistency and publication bias were not rated, given the very limited pooling of data from the few trials making the same comparisons. Trials were largely downgraded further due to serious imprecision and indirectness. Serious imprecision reflecting wide confidence intervals, including those crossing the line of no effect, as well as unit of analysis errors reduced our confidence in the effect estimates. Further downgrading for serious indirectness reflected the inadequacy and unsatisfactory nature (including low reliability and validity) of some of the outcome measures.
Among other quality issues, unit of analysis errors are especially important to identify. Randomisation usually occurs at the patient level. However the unit of analysis in flexor tendon surgery rehabilitation outcomes can be patients, digits or tendons (i.e. two tendons can be injured in the same digit). Frequently reported outcomes such as grip strength are measured per patient, whereas active ROM is reported per digit. Seven studies were clear in their unit of analysis and accounted for these differences, three committed unit of analysis errors, and in seven studies it was unclear if a unit of analysis error may have occurred.
Potential biases in the review process
Although review authors attempted to minimise bias in the selection of studies for this review, collection of published data and analysis, our searches were limited to electronic databases and clinical trials registries. Therefore, we may have missed any unpublished studies. Furthermore, it was difficult to obtain all relevant data required for a systematic review from the authors of the included studies, often because of the length of time that had passed since some of the studies were completed, or no contact information was available for the authors. It was also difficult to assess selective outcome reporting for studies for which study protocols or trial registry was not available or accessible, and for which study authors did not adequately report the methods used.
In addition, unit of analysis errors or concerns (tendon/digit/participant) were identified in some studies. For studies that included participants with multiple tendon or digit repairs but did not account for this in the analysis, bias may have been introduced.
Changes were made to the protocol published a priori. These have been reported explicitly in Differences between protocol and review.
Agreements and disagreements with other studies or reviews
To our knowledge, five other systematic reviews have been published on this topic (Chesney 2011; Neiduski 2018; Starr 2013; Thien 2004; Woythal 2019). Thien 2004 is a previous Cochrane Review published in 2004 and thus out of date; we excluded one paper (Percival 1989) previously included in Thien 2004 as it was not a randomised trial.
The other four systematic reviews included outcomes from both randomised and non‐randomised studies.
-
Chesney 2011 reviewed flexor tendon rehabilitation protocols for zone II flexor tendon injuries of the hand. The reviewers concluded that there was weak evidence to support both early active motion regimens and regimens that combined passive mobilisation and active extension. These exercise regimens provided superior results with regard to ROM while maintaining an acceptable low rate of tendon rupture. The review included 15 studies comprising of three RCTs, two quasi experimental studies and 10 case series. One of the RCTs, Su 2005, investigated the effects of a stainless steel tendon repair device which is not considered a rehabilitation treatment using our inclusion criteria.
-
Neiduski 2018 reported that place and hold exercise regimens appear to provide better outcomes than passive flexion regimens for patients with two to six‐strand repairs of flexor tendon injuries, as examined by nine studies. However, they also included non‐randomised study designs, and hence are likely to have serious risk of bias impacting our certainty of this evidence.
-
Starr 2013 included flexor tendon injuries in all zones with the focus on comparing rehabilitation protocols between early passive and early active range of motion. They included four RCTs, eight quasi‐experimental comparative studies and 22 prospective and retrospective case series. They too included Su 2005. They found that early passive range of motion protocols had a statistically significantly decreased risk for tendon rupture but an increased risk for postoperative decreased ROM compared with early active motion protocols.
-
Woythal 2019 conducted a systematic review that aimed to examine the effectiveness of splints, with or without wrist immobilisation, following surgery for flexor tendon injury. They found no studies that met their inclusion criteria (randomised trials0 and hence qualitatively summarised the most relevant studies. They concluded that it is impossible to currently provide evidence‐based recommendations for or against immobilising the wrist following flexor tendon repairs.
Findings of our review are consistent with the other systematic reviews in concluding that evidence is insufficient and inconclusive to determine which rehabilitation regimens are safe and most effective in restoring function and motion following flexor tendon surgeries of the hand. All of these reviews have a narrower scope than ours in that they restricted their study eligibility criteria according to the type of exercise regimens used, whereas our review has focused on all types of interventions used by therapists for rehabilitation following flexor tendon surgery. Therefore, to our knowledge, ours is the most comprehensive review of rehabilitation interventions following flexor tendon surgery, and includes several trials not included in the other reviews (Abdel Sabour 2018; Geetha 2014; Gulke 2018; Ozkan 2004; Poorpezeshk 2018; Rigo 2017; Silva 2003; Stenekes 2009; Uday Raj 2018; Vialaneix 2003).
One study in Persian language (Yavari 2009) is awaiting classification while we are seeking further clarification from the authors on participant numbers and method of randomisation. Another study is awaiting classification (Kitis 2009) as we await further clarification from the author whether the trial was randomised or not. Five trials are currently ongoing (CTRI/2019/01/016821; NCT03812978; IRCT201310138177N8; IRCT20150721023277N7; NCT03850210) and will likely be included in future updates of this review. These studies are examining interventions of interest and are sufficiently large enough to change the findings of future updates of this review.
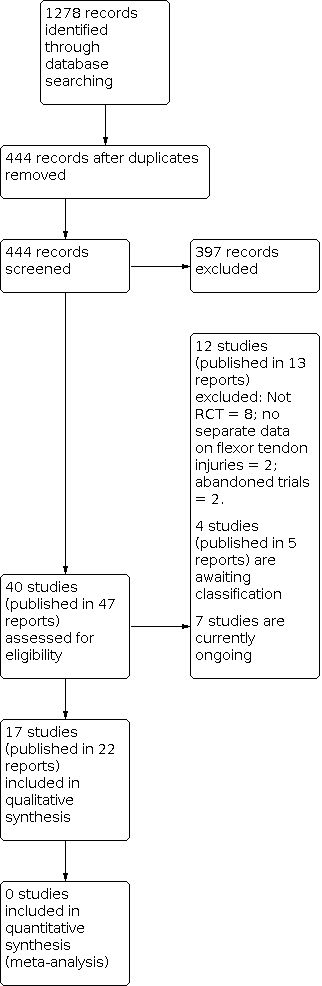
Diagram showing the flow of studies through the study selection process

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
| Self‐reported function for ADL using a VAS (0 to 10; higher = better) | ||||||
| Study | Follow‐up | Active Median (IQR) | Active N (digits) | Control Median; IQR | Control N (digits) | Reported P value |
|---|---|---|---|---|---|---|
| Rigo 2017 | At 2 months | 7.2 (3.0) | 36 | 6.5 (3.1) | 32 | P = 0.204 |
| At 3 months | 7.3 (3.6) | 36 | 7.7 (3.0) | 31 | P = 0.850 | |
| At 6 months | 8.8 (1.5) | 32 | 8.5 (3.5) | 30 | P = 0.942 | |
| At 12 months | 9.3 (1.2) | 34 | 8.8 (2.0) | 29 | P = 0.113 | |
Comparison 1: Early active flexion plus controlled passive exercise regimen versus early controlled passive exercise regimen (modified Kleinert protocol), Outcome 1: Self‐reported function for ADL using a VAS (0 to 10; higher = better)

Comparison 1: Early active flexion plus controlled passive exercise regimen versus early controlled passive exercise regimen (modified Kleinert protocol), Outcome 2: Self‐reported function using VAS for ADLs (0 to 10; higher scores = better); secondary analyses

Comparison 1: Early active flexion plus controlled passive exercise regimen versus early controlled passive exercise regimen (modified Kleinert protocol), Outcome 3: Active finger range of motion (degrees)

Comparison 1: Early active flexion plus controlled passive exercise regimen versus early controlled passive exercise regimen (modified Kleinert protocol), Outcome 4: Finger range of movement ‐ Poor outcome

Comparison 1: Early active flexion plus controlled passive exercise regimen versus early controlled passive exercise regimen (modified Kleinert protocol), Outcome 5: Adverse events

Comparison 1: Early active flexion plus controlled passive exercise regimen versus early controlled passive exercise regimen (modified Kleinert protocol), Outcome 6: Strength (% of the contralateral hand or digit)

Comparison 2: Early active flexion + active extension exercise regimen (+ modified Kessler suture surgical technique) versus passive flexion + active extension exercise regimen (+ grasping suture and external pull‐out knot surgical technique), Outcome 1: Adverse events

Comparison 3: Active exercise regimen versus immobilisation regimen, Outcome 1: Range of movement at 12+ months: poor outcome

Comparison 3: Active exercise regimen versus immobilisation regimen, Outcome 2: Adverse events

Comparison 4: Early place and hold progressed to tendon gliding exercise regimen versus early passive progressed to active exercise regimen, Outcome 1: Grip strength at 12 weeks (% difference between normal and affected hands)

Comparison 5: Place and hold exercise regimen versus Controlled passive exercise regimen, Outcome 1: Function (self‐reported): DASH scores (0 to 100; higher score = more disability)

Comparison 5: Place and hold exercise regimen versus Controlled passive exercise regimen, Outcome 2: Range of movement (Total Active Movement) (degrees)

Comparison 5: Place and hold exercise regimen versus Controlled passive exercise regimen, Outcome 3: Range of movement (Strickland Criteria) at 8 weeks: Poor outcome

Comparison 5: Place and hold exercise regimen versus Controlled passive exercise regimen, Outcome 4: Adverse events

Comparison 5: Place and hold exercise regimen versus Controlled passive exercise regimen, Outcome 5: Function (observed): Jebsen Taylor at 52 weeks (seconds)

Comparison 5: Place and hold exercise regimen versus Controlled passive exercise regimen, Outcome 6: Function (observed): Purdue pegboard at 52 weeks (pegs)

Comparison 5: Place and hold exercise regimen versus Controlled passive exercise regimen, Outcome 7: Satisfaction with hand function (0 to 10: complete satisfaction) at 6 months

Comparison 6: Unrestricted activity at 8 weeks post‐surgery versus unrestricted activity at 10 weeks, Outcome 1: Adverse event (tendon rupture)

Comparison 7: Exoskeleton versus physiotherapy, Outcome 1: Function (self‐reported): DASH scores (0 to 100; higher score = more disability)

Comparison 7: Exoskeleton versus physiotherapy, Outcome 2: Active finger range of motion of PIP joint (degrees)

Comparison 7: Exoskeleton versus physiotherapy, Outcome 3: Active finger range of motion of DIP joint (degrees)

Comparison 7: Exoskeleton versus physiotherapy, Outcome 4: Active finger range of motion (Total Active Movement) (degrees)

Comparison 7: Exoskeleton versus physiotherapy, Outcome 5: Adverse events

Comparison 7: Exoskeleton versus physiotherapy, Outcome 6: Strength at 18 weeks

Comparison 8: Continuous passive motion device versus controlled passive progressed to active exercise regimen (Modified Kleinert), Outcome 1: Active finger range of motion (degrees)

Comparison 8: Continuous passive motion device versus controlled passive progressed to active exercise regimen (Modified Kleinert), Outcome 2: Range of movement at > 6 months (Strickland criteria) ‐ poor outcome

Comparison 8: Continuous passive motion device versus controlled passive progressed to active exercise regimen (Modified Kleinert), Outcome 3: Adverse event

Comparison 9: Ultrasound versus control, Outcome 1: Improvement in active range of movement (Difference between 3 and 12 weeks; Total Active Motion measured in degrees)

Comparison 9: Ultrasound versus control, Outcome 2: Active finger range of motion (Strickland classification) at 3 months ‐ Poor outcome

Comparison 9: Ultrasound versus control, Outcome 3: Adverse events

Comparison 10: Low‐level laser therapy versus placebo control, Outcome 1: Active finger range of motion (Total active motion (degrees)) at 12 weeks

Comparison 10: Low‐level laser therapy versus placebo control, Outcome 2: Range of movement at 12 weeks: poor outcome

Comparison 10: Low‐level laser therapy versus placebo control, Outcome 3: Adverse events

Comparison 10: Low‐level laser therapy versus placebo control, Outcome 4: Grip strength at 12 weeks (% lost using uninjured hand as comparison)

Comparison 11: Motor imagery versus control, Outcome 1: Strength (kg)
| Addition of active flexion exercises to controlled passive exercise regimen for rehabilitation following surgery for flexor tendon injuries of the hand | ||||||
| Patient or population: participants undergoing rehabilitation following surgery for flexor tendon injuries of the handa | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Early controlled passive exercise regimen (modified Kleinert protocol) | Early active flexion plus early controlled passive exercise regimen | |||||
| Functional assessment using a patient reported outcome measure: Follow‐up: 6 months | Study population | ‐ | 62 fingers (1 RCT) | ⊕⊝⊝⊝ | The study reporting this outcome reported median and interquartile ranges. It found no evidence of a difference between the two groups (reported P = 0.942). It is very unlikely that a difference of 0.3 on an 11 point scale is clinically important. | |
| See comment. Median 8.5, IQR 3.5 | See comment. | |||||
| Functional assessment using a patient reported outcome measure: Follow‐up: 12 months | Study population | ‐ | 63 fingers | ⊕⊝⊝⊝ | The study reporting this outcome reported median and interquartile ranges. It found no evidence of a difference between the two groups (reported P = 0.113). It is very unlikely that a difference of 0.5 on an 11 point scale is clinically important | |
| See comment. Median 8.8, IQR 2.9 | See comment. | |||||
| Active finger range of motion | Study population | ‐ | 63 fingers | ⊕⊝⊝⊝ | This difference is not meaningful and could have been due to error in measurement: for goniometric measurement, the minimal detectable difference is between 12 and 30 degrees with a standard error of measurement ranging from 4 to 11 degrees per joint (Reissner 2019). | |
| Mean AROM in the control group was 134 degrees | MD 3 degrees higher | |||||
| Active finger range of motion | Study population | ‐ | 63 fingers | ⊕⊝⊝⊝ | This difference is not meaningful and could have been due to error in measurement: for goniometric measurement, the minimal detectable difference is between 12 and 30 degrees with a standard error of measurement ranging from 4 to 11 degrees per joint (Reissner 2019). | |
| Mean AROM in the control group was 140 degrees | MD 9 degrees higher | |||||
| Adverse events: participants incurring one or more adverse events Follow‐up: 12 months | Study population | RR 0.58 (0.23 to 1.44) | 69 fingers (1 RCT) | ⊕⊝⊝⊝ | The 15 adverse events comprised 3 tendon ruptures, 6 wound dehiscence, 1 complex regional pain syndrome and 5 transitory swelling and tenderness of the tendon sheaf. | |
| 282 per 1000 | 164 per 1000 (65 lower to 406 higher) | |||||
| Adverse event (tendon rupture) | Study population | RR 1.73 | 69 fingers | ⊕⊝⊝⊝ | All three tendon ruptures (4.3%) underwent secondary surgery. | |
| 31 per 1000 | 54 per 1000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aThe majority (68%) were zone II flexor tendon repairs; the rest being zone I and III. dDowngraded one level due to serious indirectness reflecting the reflecting the uncertain nature of the outcome. eDowngraded two levels due to very serious imprecision reflecting the small number of events. | ||||||
| Active exercise regimen compared with an immobilisation regimen following surgery for flexor tendon injuries of the hand | ||||||
| Patient or population: participants undergoing rehabilitation following surgery for flexor tendon injuries of the handa | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Immobilisation regimen for three weeks | Active exercise regimen commenced within one day post‐surgery | |||||
| Functional assessment using a patient reported outcome measure | See comment. | See comment. | Not estimable | ‐ | See comment. | Outcome was not reported |
| Functional assessment using a patient reported outcome measure | See comment. | See comment. | Not estimable | ‐ | See comment. | Outcome was not reported |
| Range of movement | See comment. | See comment. | Not estimable | ‐ | See comment. | Outcome was not reported |
| Range of movement | Study population | RR 0.08 | 84 | ⊕⊝⊝⊝ | Poor outcome is < 25% of normal. The 7 (15%) cases of poor range of finger movement were all in the immobilisation group | |
| 149 per 1000 | 12 per 1000 | |||||
| Adverse events: participants incurring one or more adverse events | See comment. | See comment. | Not estimable | 84 | See comment | Outcome was not reported. Only tendon rupture and indication for tenolysis data provided; see below. |
| Adverse events requiring (or indicated for) surgery | Study population | RR 0.64 | 84 | ⊕⊝⊝⊝ | All five cases of tendon rupture (13.5% of 37) needing surgical repair occurred after 2 weeks in the active mobilisation group and all 10 cases of range of motion deficiency (21.3% of 47) indicating scar adhesion and need for tenolysis occurred in the immobilisation group. | |
| 213 per 1000 | 137 per 1000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group (in this table, this is directly based on the study population) and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aAll were zone II flexor tendon repairs. bDowngraded two levels for very serious risk of bias reflecting detection bias (no blinding of outcome assessors), potential selection bias and attrition bias. cDowngraded one level for serious indirectness reflecting the unsatisfactory nature of the outcome. dDowngraded one level because of low number of events and wide confidence intervals for this outcome. eThese complications reflect the anticipated complications of early active mobilisation (early re‐rupture) and immobilisation (scar adhesions and contractures). It is uncertain whether tenolysis was actually done for those participants with range of motion deficit in the immobilisation group. | ||||||
| Place and hold exercise versus controlled passive exercise following surgery for flexor tendon injuries of the hand | ||||||
| Patient or population: participants undergoing rehabilitation following surgery for flexor tendon injuries of the handa | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Controlled passive exercise regimen | Place and hold exercise regimen | |||||
| Functional assessment using a patient reported outcome measure: assessed with DASH questionnaire (0 to 100; higher scores = worse disability) | Study population | Not estimable | 26 | ⊕⊝⊝⊝ | The study reporting this outcome reported median and interquartile ranges, finding no evidence of a difference between the two groups (reported P = 0.62). | |
| See comment. Median 15, IQR 10 to 30 | See comment. Median 23, IQR 2 to 26 | |||||
| Functional assessment using a patient reported outcome measure: | Study population | ‐ | 89 | ⊕⊝⊝⊝ | These differences are not clinically important. The recommended minimal clinically important difference for DASH is 15 (DASH/QuickDASH). | |
| Mean DASH score was 3.1 | Mean DASH score was 1.1 lower (2.77 lower to 0.57 higher) | |||||
| Range of movement | See comment. | See comment. | Not estimable | ‐ | See comment. | Outcome was not reported |
| Range of movement | Study population | ‐ | 89 (102 digits) | ⊕⊝⊝⊝ | ||
| Mean ROM was 128 degrees | Mean ROM was 28 degrees higher | |||||
| Adverse events: participants incurring one or more adverse events | See comment. | See comment. | Not estimable | 84 | See comment. | This outcome was not reported by the three trials testing this comparison. Only tendon rupture (see next) was commonly reported. One trial (26 participants), reporting by tendon or digit (36 digits), also reported on scar adherence (reported only in the controlled passive group), flexion contracture at the DIP and PIP joints and tendon lag; very low certainty evidence for all individual complications. |
| Adverse events requiring (or indicated for) surgery | Study populationsh | RR 0.81 | 196 tendons | ⊕⊝⊝⊝ | These data were limited to tendon rupture. We considered that all 7 tendon ruptures (3.6% of 196 tendons) would have required surgery.j | |
| 40 per 1000 | 33 per 1000 (8 to 140) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group (in this table, this is directly based on the study population) and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aThe majority were zone II flexor tendon repairs; one of the three studies making this comparison also included 7 zone I injuries and 7 zone III injuries. bAll exercises started at 3 days from surgery. The place and hold exercise regimens varied among the three studies. In two studies, the exercises were carried out with a dorsal orthosis and in one study, the dorsal orthosis was removal when doing the exercises cAll exercises started at 3 days from surgery. The controlled passive exercise regimens varied among the three studies. However, rubber band traction was common to all three. dDowngraded two levels for very serious risk of bias reflecting lack of blinding (performance and detection bias) eDowngraded one level for serious imprecision. fDowngraded one level for serious imprecision, also reflecting the potential 'ceiling' effect as the mean values were very low and thus cannot discriminate between the two groups. gDowngraded one level for serious imprecision as the data are presented for tendons not participants. hControl group risk was devised from the summed data from the three studies. These results were not available for participants rather than tendons. iDowngraded two levels for very serious imprecision reflecting a very low number of events and wide confidence interval for this outcome. jWe did not include the 14 cases of scar adherence (70% of 20 tendons) reported in the controlled passive group of one trial because the outcome was not defined and no details of the extent or consequences were provided. | ||||||
| Database | Period Searched | Date Searched | Number of hits |
|---|---|---|---|
| Cochrane Bone, Joint and Musculoskeletal Trials (BJMT) Specialised Register | 18 June 2019 | 18 June 2019 | 26 |
| CENTRAL | August 2020, Issue 8 | 11 August 2020 | 208 |
| MEDLINE | January 1946 to August 2020 | 10 August 2020 | 462 |
| Embase | January 1980 to June 2019 | 18 June 2019 | 227 |
| CINAHL PLUS | January 1937 to June 2019 | 18 June 2019 | 63 |
| AMED | January 1985 to August 2020 | 10 January 2017 | 75 |
| ClinicalTrials.gov | 11 August 2020 | 79 | |
| WHO International Clinical Trials Registry Platform (ICTRP) | 18 June 2019 | 138 |
| Study | Country | Setting | Recruited Participants; Digits; Tendons | Final follow‐up Participants; Digits; Tendons | Zones | Age (years) Mean (Range) | Male | Female |
|---|---|---|---|---|---|---|---|---|
| Egypt | Rehabilitation Department | 33; NR; 45 | 26; NR; 36 | I‐III | 26.8 (15‐60)a | 21a | 5a | |
| Sweden | NR | 96; 106; NR | 82; 91; 118 | II | 37a | 54a | 28a | |
| Iran | Hand therapy clinic | 54; 64; 108 | 54; 64; 108 | II | 28.5 (13‐50) | 37 | 17 | |
| India | Hospital | 106; 139; NR | 100; 131; NR | II | G1: NR (10‐45)a G2: 35 (22‐50)a | 89a | 11a | |
| USA | Multi‐centre hospital | 51; 60; 102b | 51; 60; 102 | II | 29.4a | NR | NR | |
| Germany | Physiotherapy clinic | 62; NR;NR | 59; NR; NR | II | 29.5 (18‐60) | 44 | 18 | |
| Sweden | NR | 100; 108; NR | NR; NR; NR | II | NR | NR | NR | |
| UK | Plastic surgery centre | 112; NR; NR | 80; NR; NR | I‐III | NR | NR | NR | |
| Turkey | Hand surgery centre | 25; 41; NR | 23; 39; NR | I‐V | 24 (7‐43) | 15 | 10 | |
| Iran | Plastic surgery centre | 97; 114; 114 | 77; 92; 92 | I‐III | 27a | 60a | 17a | |
| Norway | Orthopaedic surgery centre | 53; 73; 73 | 45; 63; 63 | I‐III | 38.7 (18‐72)c | 36c | 14c | |
| Denmark | Hand surgery centre | 39; 39; 39 | 33; 33; 33 | I‐II | NR | NR | NR | |
| Brazil | Hand surgery centre | 84; NR; 152 | NR; NR; NR | II | 34 (18‐66) | NR | NR | |
| Netherlands | Plastic surgery centre | 28; NR; NR | 25; NR; NR | All | 33.5a | 18a | 7a | |
| USA | Multi‐centre hand surgery centre | 103; 119; 238 | 89; 102; 204 | II | 29 (15‐51)a | 63a | 30a | |
| India | Plastic surgery centre | 30; NR; NR | 30; NR; NR | V | NR | NR | NR | |
| France | NR | 35; NR; NR | NR; NR NR | II | 35 | NR | NR | |
| NR: Not reported; G1: Group 1; G2: Group 2 aOnly reported at follow‐up (not at baseline) bParticipants were only eligible if they were available for the 6 month follow‐up. Thus, this number is likely to have been much higher than reported here. cExcludes 3 participants who experienced tendon ruptures after randomisation. | ||||||||
| Study ID | Function: patient‐reported | Active ROM | Adverse event | Passive ROM | Strength | Return to work | Function: objective measure | Quality of life | Satisfaction |
|---|---|---|---|---|---|---|---|---|---|
| X | X | X | X | ||||||
| X | X | X | X | X | |||||
| X | X | ||||||||
| X | X | X | |||||||
| X | X | ||||||||
| X | X | X | X | X | |||||
| X | X | ||||||||
| X | X | ||||||||
| X | X | X | |||||||
| X | X | X | |||||||
| X | X | X | X | ||||||
| X | X | X | |||||||
| X | X | ||||||||
| X | X | X | |||||||
| X | X | X | X | X | X | ||||
| X | X | X | |||||||
| X | X | X |
| Classification system | Outcome (% motion achieved) | Excellent | Good | Fair or satisfactory | Poor | Failure |
| Strickland‐Glogovac | % active PIP + DIP ROM (active flexion ‐ extension deficit) compared to contralateral side or 175 degrees* | 85% to 100% | 70% to 84% | 50% to 69% | 0% to 49% | Not applicable |
| ROM (in degrees) | > 150 | 125 to 149 | 90 to 124 | < 90 | Not applicable | |
| Strickland or Modified Strickland | % active PIP + DIP ROM (active flexion ‐ extension deficit) compared to contralateral side or 175 degrees* | 75% to 100% | 50% to 74% | 24% to 49% | 0% to 24% | Not applicable |
| ROM (in degrees) | > 132 | 88 to 131 | 45 to 87 | < 44 | Not applicable | |
| Tang*** | % active PIP + DIP ROM compared to contralateral side or 175 degrees* | 90% to 100% | 70% to 89% | 50% to 69% | 30% to 49% | < 30% |
| IFSSH | % Total active motion compared to total passive motion** | 75% to 100% | 50% to 74% | 24% to 49% | 0% to 24% | Not applicable |
| Total Active Motion | % active MCP + PIP + DIP ROM (active flexion ‐ extension deficit) compared to contralateral side | Normal | > 75% | 50% to 75% | < 50% | < pre‐surgery |
| DIP: distal interphalangeal; IFFSH: International Federation of Societies for Surgery of the Hand; MCP: metacarpophalangeal; ROM: range of movement; PIP: proximal interphalangeal *The sum of active ROM of the PIP and DIP joints is calculated in degrees. This is done by adding the flexion achieved at the PIP and DIP joints and subtracting any extension deficits from the total. Motion is reported as a % of the contralateral side. It is assumed that 175 degrees is the sum of motion of the normal PIP and DIP joints of the unaffected side. % motion achieved = ((PIP + DIP flexion) ‐ (PIP + DIP extension deficit)) X 100 divided by 175. ** % motion achieved = (Total active motion X 100) divided by Total passive motion. ***According to Tang, the excellent and good scores are further divided into plus and minus sub‐grades based on their grip strength and quality of motion (investigator’s subjective judgement of the coordination, visual arc and speed of motion). | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1.1 Self‐reported function for ADL using a VAS (0 to 10; higher = better) Show forest plot | 1 | Other data | No numeric data | |
| 1.2 Self‐reported function using VAS for ADLs (0 to 10; higher scores = better); secondary analyses Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.2.1 ADL VAS at 2 months (0=worst; 10=best) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.2.2 ADL VAS at 3 months (0=worst; 10=best) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.2.3 ADL VAS at 6 months (0=worst; 10=best) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.2.4 ADL VAS at 12 months (0=worst; 10=best) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.3 Active finger range of motion (degrees) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.3.1 Total Active Movement at 1 month (degrees) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.3.2 Total Active Movement at 2 months (degrees) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.3.3 Total Active Movement at 3 months (degrees) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.3.4 Total Active Movement at 6 months (degrees) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.3.5 Total Active Movement at 12 months (degrees) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.4 Finger range of movement ‐ Poor outcome Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.4.1 Strickland classification at 1 month | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.4.2 Strickland classification at 2 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.4.3 Strickland classification at 3 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.4.4 Strickland classification at 6 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.4.5 Strickland classification at 12 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.4.6 Tang classification at 1 month | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.4.7 Tang classification at 2 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.4.8 Tang classification at 3 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.4.9 Tang classification at 6 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.4.10 Tang classification at 12 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.5 Adverse events Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.5.1 Tendon rupture | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.5.2 Complex Regional Pain Syndrome | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.5.3 Wound dehiscence | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.5.4 Transitory swelling + tenderness | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.5.5 Any adverse event | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.6 Strength (% of the contralateral hand or digit) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.6.1 Grip Strength at 3 months (% of the contralateral hand) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.6.2 Grip Strength at 6 months (% of the contralateral hand) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.6.3 Grip Strength at 12 months (% of the contralateral hand) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.6.4 Pinch Strength at 3 months (% of the contralateral digit) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.6.5 Pinch Strength at 6 months (% of the contralateral digit) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.6.6 Pinch Strength at 12 months (% of the contralateral digit) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 2.1 Adverse events Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.1.1 Tendon ruptures | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.1.2 Scar adhesions requiring surgery (Tenolysis) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 3.1 Range of movement at 12+ months: poor outcome Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.1.1 IFSSH criteria | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.1.2 Strickland criteria | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.2 Adverse events Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.2.1 Tendon ruptures | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.2.2 Movement restrictions indicating need for tenolysis | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.2.3 Secondary surgery (actual or indicated) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 4.1 Grip strength at 12 weeks (% difference between normal and affected hands) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 5.1 Function (self‐reported): DASH scores (0 to 100; higher score = more disability) Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.1.1 DASH at 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.1.2 DASH at 52 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.2 Range of movement (Total Active Movement) (degrees) Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.2.1 At 8 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.2.2 At 52 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.3 Range of movement (Strickland Criteria) at 8 weeks: Poor outcome Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 5.4 Adverse events Show forest plot | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.4.1 Tendon rupture | 3 | 196 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.81 [0.19, 3.50] |
| 5.4.2 Scar adherence | 1 | 36 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.04 [0.00, 0.66] |
| 5.4.3 Flexion contracture of the DIP joint | 1 | 36 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.12 [0.02, 0.88] |
| 5.4.4 Flexion contracture of the PIP joint | 1 | 36 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.47 [0.15, 1.48] |
| 5.4.5 FDS tendon lag | 1 | 36 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.25 [0.06, 0.98] |
| 5.4.6 FDP tendon lag | 1 | 36 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.17 [0.04, 0.62] |
| 5.5 Function (observed): Jebsen Taylor at 52 weeks (seconds) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.6 Function (observed): Purdue pegboard at 52 weeks (pegs) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.7 Satisfaction with hand function (0 to 10: complete satisfaction) at 6 months Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 6.1 Adverse event (tendon rupture) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 7.1 Function (self‐reported): DASH scores (0 to 100; higher score = more disability) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.1.1 DASH at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.1.2 DASH at 18 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.2 Active finger range of motion of PIP joint (degrees) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.2.1 PIP joint range of motion at 6 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.2.2 PIP joint range of motion at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.2.3 PIP joint range of motion at 18 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.3 Active finger range of motion of DIP joint (degrees) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.3.1 DIP joint range of motion at 6 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.3.2 DIP joint range of motion at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.3.3 DIP joint range of motion at 18 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.4 Active finger range of motion (Total Active Movement) (degrees) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.4.1 TAM at 6 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.4.2 TAM at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.4.3 TAM at 18 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.5 Adverse events Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.5.1 Tendon rupture | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.5.2 CRPS (complex regional pain syndrome) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.6 Strength at 18 weeks Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.6.1 Grip strength (kg) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.6.2 Pinch strength (kg) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 8.1 Active finger range of motion (degrees) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8.1.1 TAM at > 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8.2 Range of movement at > 6 months (Strickland criteria) ‐ poor outcome Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 8.3 Adverse event Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 8.3.1 Tendon rupture at >6 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 8.3.2 Infection at >6 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 9.1 Improvement in active range of movement (Difference between 3 and 12 weeks; Total Active Motion measured in degrees) Show forest plot | 1 | 131 | Mean Difference (IV, Fixed, 95% CI) | 26.47 [19.70, 33.24] |
| 9.1.1 1MHz; 0.7W/cm2 increased to 1w/cm2 | 1 | 50 | Mean Difference (IV, Fixed, 95% CI) | 31.50 [19.94, 43.06] |
| 9.1.2 1 MHz; 0.3w/cm2 increased to 1.0w/cm2 | 1 | 40 | Mean Difference (IV, Fixed, 95% CI) | 23.80 [11.89, 35.71] |
| 9.1.3 3Mhz; 0.5w/cm2 increased to 0.7w/cm2 | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | 23.90 [12.20, 35.60] |
| 9.2 Active finger range of motion (Strickland classification) at 3 months ‐ Poor outcome Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 9.3 Adverse events Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 9.3.1 Tendon rupture at 3 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 9.3.2 Wound dehiscence <3 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 10.1 Active finger range of motion (Total active motion (degrees)) at 12 weeks Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 10.2 Range of movement at 12 weeks: poor outcome Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 10.2.1 Strickland scoring system at 12 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 10.3 Adverse events Show forest plot | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 10.3.1 Tendon rupture | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 10.3.2 Wound infection | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 10.4 Grip strength at 12 weeks (% lost using uninjured hand as comparison) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 11.1 Strength (kg) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 11.1.1 Grip strength (kg) at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 11.1.2 Pinch strength (kg) at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |