18F PET dengan florbetapir untuk diagnosis awal dementia penyakit Alzheimer dan dementia lain dalam kalangan orang yang mempunyai ketakmampuan kognitif ringan (MCI)
Información
- DOI:
- https://doi.org/10.1002/14651858.CD012216.pub2Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 22 noviembre 2017see what's new
- Tipo:
-
- Diagnostic
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Demencia y trastornos cognitivos
- Copyright:
-
- Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
-
Gabriel Martínez, Robin WM Vernooij, and Paulina Fuentes Padilla: contributed to the conception, design, and draft of the protocol; overall responsibility of study selection; data extraction; contact of the authors; draft of discussion; and authors’ conclusion sections.
-
Leon Flicker: contributed to the conception, and designed and reviewed the draft protocol and final manuscript.
-
Xavier Bonfill Cosp: reviewed the draft protocol and final manuscript.
-
Javier Zamora: designed and drafted the protocol, performed statistical analyses, updated the statistical methods section and final manuscript.
Sources of support
Internal sources
-
No sources of support supplied
External sources
-
National Institute for Health Research (NIHR), UK.
This review was supported by the NIHR, via Cochrane Infrastructure funding to the Cochrane Dementia and Cognitive Improvement group. The views and opinions expressed therein are those of the review authors and do not necessarily reflect those of the Systematic Reviews Programme, the NIHR, the NHS, or the Department of Health
Declarations of interest
Gabriel Martínez has no known conflicts of interest.
Leon Flicker has no known conflicts of interest.
Robin WM Vernooij has no known conflicts of interest.
Paulina Fuentes Padilla has no known conflicts of interest.
Javier Zamora has no known conflicts of interest.
Xavier Bonfill Cosp has no known conflicts of interest.
Acknowledgements
Gabriel Martínez is a PhD candidate in Methodology of Biomedical Research and Public Health at the Department of Paediatrics, Obstetrics and Gynaecology and Preventive Medicine, Universitat Autònoma de Barcelona, Barcelona, Spain.
We are grateful to the authors of included and excluded studies who responded to our requests for additional information.
We thank the Cochrane Dementia and Cognitive Improvement Group (CDCIG) for strong support, especially Sue Marcus in finalizing the review.
We thank Anna Noel‐Storr, Information Specialist of the CDCIG, for her assistance with the design of the search strategy.
We thank Gerard Urrútia and Marta Roqué i Figuls for their contribution in the preparation of the protocol for the review (Martínez 2016)
We thank the peer reviewers for their many helpful suggestions.
Version history
| Published | Title | Stage | Authors | Version |
| 2017 Nov 22 | 18F PET with florbetapir for the early diagnosis of Alzheimer’s disease dementia and other dementias in people with mild cognitive impairment (MCI) | Review | Gabriel Martínez, Robin WM Vernooij, Paulina Fuentes Padilla, Javier Zamora, Xavier Bonfill Cosp, Leon Flicker | |
| 2016 May 30 | <sup>18</sup>F PET ligands for the early diagnosis of Alzheimer’s disease dementia and other dementias in people with mild cognitive impairment (MCI) | Protocol | Gabriel Martínez, Leon Flicker, Robin WM Vernooij, Paulina Fuentes Padilla, Javier Zamora, Marta Roqué i Figuls, Gerard Urrútia, Xavier Bonfill Cosp | |
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
- *Aniline Compounds;
- *Ethylene Glycols;
- *Fluorine Radioisotopes;
- *Positron‐Emission Tomography;
- Alzheimer Disease [diagnostic imaging, etiology];
- Cognitive Dysfunction [*complications];
- Dementia [*diagnostic imaging, etiology];
- Diagnosis, Differential;
- Disease Progression;
- Early Diagnosis;
- Sensitivity and Specificity;
Medical Subject Headings Check Words
Humans;

Study flow diagram.
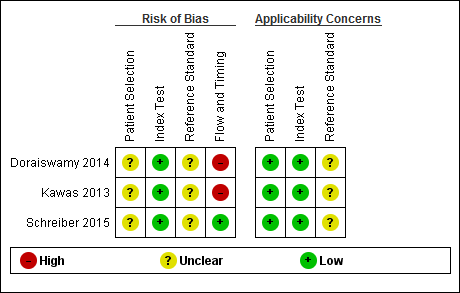
Risk of bias and applicability concerns summary: review authors' judgements about each domain for each included study
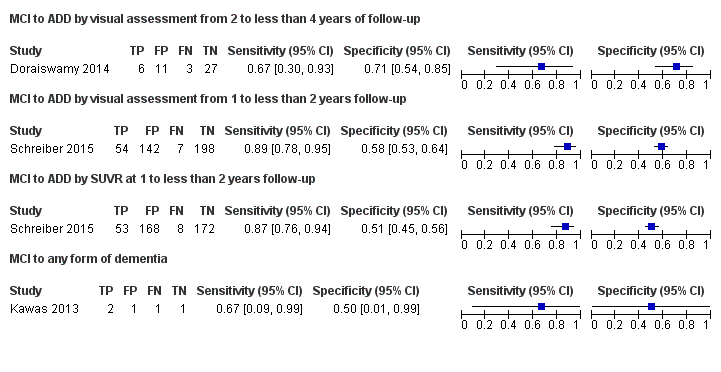
Forest plot of tests: 1 MCI to ADD by visual assessment from 2 to less than 4 years of follow‐up, 2 MCI to ADD by visual assessment from 1 to less than 2 years follow‐up, 3 MCI to ADD by SUVR at 1 to less than 2 years follow‐up, 4 MCI to any form of dementia.

MCI to ADD by visual assessment from 2 to less than 4 years of follow‐up.

MCI to ADD by visual assessment from 1 to less than 2 years follow‐up.

MCI to ADD by SUVR at 1 to less than 2 years follow‐up.

MCI to any form of dementia.
| What is the diagnostic accuracy of 18F‐florbetapir PET amyloid biomarker for predict progression to ADD, any other form of dementia (non‐ADD) or any form of dementia in people with MCI? | |||||||
| Descriptive | |||||||
| Patient population | Participants diagnosed with MCI at time of performing the test using any of the Petersen criteria or Winblad criteria or CDR = 0.5 or any 16 definitions included by Matthews (Matthews 2008). | ||||||
| Sources of referral | Not reported (n = 2) Mixed (memory clinics, newspaper ads, radio, and other public media campaigns) (n = 1) | ||||||
| MCI criteria | ADNI criteria, CDR 0.5 criterion was included (n = 2) CIND (cognitive impairment not dementia) (Matthews 2008) (n = 1) | ||||||
| Sampling procedure | Unclear (n = 3) | ||||||
| Prior testing | The only testing prior to performing the 18F‐florbetapir PET amyloid biomarker was the application of diagnostic criteria for identifying participants with MCI | ||||||
| Settings | Community and institutionalised (n = 1) Not reported (n = 2) | ||||||
| Index test | 18F‐florbetapir PET | ||||||
| Threshold prespecified at baseline | Yes (n = 3) | ||||||
| Threshold interpretation | Visual (n = 3) Quantitative (n = 1) | ||||||
| Threshold | Visual:
SUVR (Standardised Uptake Volume ratio):
| ||||||
| 18F‐florbetapir retention region | Global cortex (n = 1) | ||||||
| Reference Standard | Alzheimer’s disease dementia: NINCDS‐ADRDA (n = 1) Unclear (n = 1) Any form of dementia: DSM‐IV criteria for dementia (n = 1) | ||||||
| Target condition | Progression from MCI to Alzheimer’s disease dementia or any other forms of dementia (non‐ADD) or any form of dementia | ||||||
| Included studies | Prospectively well‐defined cohorts with any accepted definition of MCI (as above). Three studies (N = 458 participants) were included. Number of participants included in analysis: 453. | ||||||
| Quality concerns | The participant selection and reference standard QUADAS‐2 domain: unclear risk of bias. The index test domain: low risk of bias in all three included studies. The flow and timing domain: high risk of bias in the two included studies. Unclear concerns about applicability in the reference standard domain in all three included studies. | ||||||
| Limitations | Limited investigation of heterogeneity and sensitivity analysis due to insufficient number of studies. We were unable to evaluate progression from MCI to any other form of dementia (non‐ADD) due to lack of included studies. | ||||||
| Test | Studies | Cases/Participants | Sensitivity | Specificity | Consequences in a cohort of 100 | ||
| Proportion converting1 | Missed cases2 | Overdiagnosed2 | |||||
| Alzheimer's disease dementia | |||||||
| 18F‐florbetapir by visual assessment from one to less than two years of follow‐up | 1 | 61/401 | 89% (95% CI 78% to 95%) | 58% (95% CI 53% to 64%) | 15 | 2 | 36 |
| 18F‐florbetapir by quantitative assessment from one to less than two years of follow‐up | 1 | 61/401 | 87% (95% CI 76% to 94%) | 51% (95% CI 45% to 56%) | 15 | 2 | 42 |
| 18F‐florbetapir by visual assessment from two to less than four years of follow‐up | 1 | 9/47 | 67% (95% CI 30% to 93%) | 71% (95% CI 54% to 85%) | 19 | 6 | 23 |
| Any form of dementia | |||||||
| 18F‐florbetapir by visual assessment from one to less than two years of follow‐up | 1 | 3/5 | 67% (95% CI 9% to 99%) | 50% (95% CI 1% to 99%) | 60 | 20 | 20 |
| Investigation of heterogeneity and sensitivity analysis: The planned investigations were not possible due to the limited number of studies available for each analysis. | |||||||
| Conclusions:18F‐florbetapir PET scan is not an accurate test for detecting progression from MCI to Alzheimer’s disease dementia or any form of dementia. The strength of the evidence was weak because of considerable variation in study methods, unclear methodological quality due to poor reporting, and high risk of bias due to possible conflict of interest. There is a need for conducting studies using standardised 18F‐florbetapir PET scan methodology in larger populations. | |||||||
| 1. Proportion converting to ADD or any form of dementia in each included study. 2. Missed and overdiagnosed numbers were computed using the proportion converting to the target condition. | |||||||
| Test | No. of studies | No. of participants |
| 1 MCI to ADD by visual assessment from 2 to less than 4 years of follow‐up Show forest plot | 1 | 47 |
| 2 MCI to ADD by visual assessment from 1 to less than 2 years follow‐up Show forest plot | 1 | 401 |
| 3 MCI to ADD by SUVR at 1 to less than 2 years follow‐up Show forest plot | 1 | 401 |
| 4 MCI to any form of dementia Show forest plot | 1 | 5 |