L’extrait de Cyclamen europaeum contre la sinusite aiguë
Résumé scientifique
Contexte
La sinusite aiguë est une cause fréquente de consultation en soins primaires. Elle est à l’origine de symptômes importants, dont des douleurs faciales, un nez congestionné, des maux de tête, un mucus nasal épais, de la fièvre et de la toux, et entraîne souvent des absences au travail ou à l'école. Le traitement de la sinusite se concentre sur l'élimination des facteurs en cause et sur le contrôle des composantes inflammatoires et infectieuses. L'extrait liquide naturel, congelé, et séché de la plante Cyclamen europaeum administré par voie intranasale est considéré comme ayant des effets bénéfiques pour soulager la congestion en facilitant le drainage nasal. Il a également un effet anti‐inflammatoire.
Objectifs
Évaluer l'efficacité de l'extrait intranasal topique de Cyclamen europaeum sur la réponse clinique chez l’adulte et l’enfant atteint de sinusite aiguë.
Stratégie de recherche documentaire
Nous avons effectué des recherches dans CENTRAL, qui comprend le registre spécialisé du groupe Cochrane sur les infections respiratoires aiguës, MEDLINE, Embase et des registres d’essais cliniques (ClinicalTrials.gov ; OMS ICTRP) en janvier 2018. Nous avons également cherché d'autres études pertinentes dans les listes de références des études incluses et dans la documentation examinée, et nous avons communiqué avec les auteurs des essais pour obtenir de plus amples renseignements.
Critères de sélection
Essais contrôlés randomisés comparant l'extrait de Cyclamen europaeum administré par voie intranasale à un placebo, des antibiotiques, des corticostéroïdes intranasaux, ou à l'absence de traitement chez l'adulte ou l'enfant atteint de sinusite aiguë, ou chez les deux. La sinusite aiguë a été définie par diagnostic clinique et confirmée par endoscopie nasale ou par examen radiologique.
Recueil et analyse des données
Deux auteurs de la revue ont indépendamment extrait les données et évalué la qualité des essais. Nous avons utilisé les procédures méthodologiques standard prévues par Cochrane.
Résultats principaux
Nous avons inclus deux essais contrôlés randomisés portant sur un total de 147 patients adultes externes atteints d'une sinusite aiguë confirmée par radiologie ou endoscopie nasale, qui ont été assignés aux groupes d'étude sur le Cyclamen europaeum en spray nasal ou placebo pendant 15 jours maximum. Les risques de biais de sélection et de détection n'étaient pas clairement établis, car l’assignation secrète et l'aveugle des évaluateurs de résultats n'étaient rapportés dans aucune des études. L'abandon était élevée (60 %) dans une étude, bien que les abandons aient été équilibrés entre les groupes d'étude.
Aucune des deux études n'a fait état des deux principaux critères de jugement : la proportion de participants dont les symptômes ont disparu ou se sont améliorés après 14 jours et après 30 jours. Aucun effet indésirable grave ni aucune complication liée au traitement n'ont été signalés ; toutefois, davantage d’effets indésirables bénins, tels qu’une irritation nasale et de la gorge, une épistaxis légère et des éternuements ont été observés chez les participants du groupe prenant duCyclamen europaeum (50 %) comparativement aux participants du groupe prenant le placebo (24 %) (risque relatif de 2,11, intervalle de confiance à 95 % 1,35 à 3,29) ; preuves de qualité moyenne.
Conclusions des auteurs
L'efficacité de Cyclamen europaeum chez les personnes atteintes de sinusite aiguë est inconnue. Bien qu'aucun effet secondaire grave n'ait été observé, 50 % des participants ayant reçu Cyclamen europaeum ont signalé des effets indésirables contre 24 % de ceux ayant reçu le placebo.
PICO
Résumé simplifié
L'extrait de Cyclamen europaeum est‐il efficace pour les personnes atteintes de sinusite aiguë ?
Problématique de la revue
Nous avons évalué l'efficacité de l’extrait liquide naturel séché et congelé deCyclamen europaeum par rapport à un traitement sans substance active (placebo) pour soigner ou soulager la sinusite aiguë chez l’adulte et chez l’enfant. Il s’agit d’un médicament à base de plantes tiré de tubercules deCyclamen europaeum et administré avec vaporisateur nasal.
Contexte
La sinusite aiguë est une affection courante qui survient lorsque les cavités osseuses à proximité du nez sont enflammées à la suite d'une infection. Les symptômes peuvent comprendre un mucus nasal épais, un nez congestionné, des douleurs faciales, des maux de tête, de la fièvre et de la toux. Les symptômes durent jusqu'à huit semaines chez les adultes et jusqu'à 12 semaines chez les enfants. La sinusite aiguë est le plus souvent causée par des virus. Des complications peuvent survenir si l'infection se propage. La sinusite aiguë est une affection courante qui entraîne des coûts importants.
Il existe toute une gamme de traitements conservateurs pour traiter la sinusite aiguë. Les antibiotiques sont couramment prescrits, mais les recommandations cliniques diffèrent sur le moment où les antibiotiques devraient être administrés pour traiter la sinusite aiguë. Les rares études sur l'extrait de Cyclamen europaeum administré en spray nasal suggèrent qu'il peut aider à soulager la congestion nasale.
Date de recherche
Les données sont à jour au 18 janvier 2018.
Caractéristiques des études
Nous avons inclus dans la revue deux études portant sur 147 adultes atteints de sinusite aiguë. Les participants ont été répartis au hasard pour recevoir Cyclamen europaeum sous forme de spray intranasal ou une substance non active pendant 15 jours au maximum.
Sources de financement des études
Des sociétés pharmaceutiques ont financé les deux études.
Résultats principaux
Nous voulions déterminer quelle était la proportion de participants dont les symptômes ont disparu ou se sont améliorés dans les 14 et 30 jours, mais nous n'avons trouvé aucun élément probant. Les études incluses ont fourni des données sur l'évolution des scores des symptômes de la sinusite aiguë avec le traitement. Une des études a fait état d'une amélioration de la douleur faciale dans les sept jours. Les complications ou les jours d'absence à l'école ou au travail n’étaient pas rapportés dans ces études.
Les personnes qui ont reçu du Cyclamen europaeum au lieu d'une substance non active ont rapporté davantage d'effets secondaires tels qu’une irritation nasale, des éternuements et un saignement nasal léger. Aucun effet secondaire majeur n'est survenu.
Nous n'avons trouvé aucune preuve de l'efficacité de Cyclamen europaeum.
Qualité des données
Nous avons évalué la qualité des deux études et nous avons jugé que les données n’étaient que modérément fiables pour le seul résultat qui pouvait être évalué, en l’occurrence les effets secondaires. Dans l’une des études, le taux d'abandon était élevé (60 %), mais ces abandons étaient décrits et répartis similairement entre les groupes d'étude. Nous avons constaté des résultats cohérents d'une étude à l'autre en ce qui concerne les effets indésirables. Aucune des deux études n'a indiqué si les évaluateurs des résultats savaient quels traitements les participants recevaient. En raison du petit nombre de participants et des faiblesses dans la conception de l'étude, nous ne pouvons pas être certains du résultat.
Authors' conclusions
Summary of findings
| Cyclamen europaeum compared to placebo for acute sinusitis | ||||||
| Patient or population: adults with acute sinusitis | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | Comments | |
| Risk with placebo | Risk with Cyclamen europaeum | |||||
| Proportion of participants with resolution or improvement of symptoms up to 30 days | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported this outcome. |
| Proportion of participants with any adverse event | Study population | RR 2.11 | 147 | ⊕⊕⊕⊝ Moderate | We downgraded the quality of the evidence as concealment of allocation to treatment and blinding of outcome assessors were not reported in the studies. Also, 1 study had a small sample size with a high attrition rate. | |
| 240 per 1000 | 506 per 1000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) CI: confidence interval; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence | ||||||
Background
Description of the condition
Sinusitis is a common condition that carries a large healthcare economic burden (Feldt 2013). Acute sinusitis is inflammation of one or more of the paranasal sinuses, with symptoms lasting less than eight weeks in adults and less than 12 weeks in children (Georgy 2012; Kaliner 1997). Sinusitis is one of the 10 most common reasons for visits to primary care physicians, and it is the fifth most common diagnosis for which antibiotics are prescribed. Primary care physicians tend to consider acute sinusitis to be of bacterial origin and prescribe antibiotics in 85% to 98% of cases. However, most sinusitis cases are caused by viruses. According to epidemiological estimates, only 0.2% to 2% of viral upper respiratory tract infections in adults progress to bacterial rhinosinusitis (Snow 2001). A recent systematic review and meta‐analysis reported that the prevalence of bacterial infection in acute sinusitis is likely to be greater than 2%, but this remains poorly defined (Shintani Smith 2015). Bacterial infections often resolve without antibiotic treatment. A multicentre prospective cohort study reported that antibiotics were prescribed in 71.2% of people with acute sinusitis (Dallas 2017).
Clinical signs and symptoms are not reliable indicators to effectively identify which cases of sinusitis should be treated with antibiotics. No accurate practice‐based test exists to diagnose acute bacterial sinusitis; clinicians rely mostly on clinical findings for diagnosis. Signs and symptoms of acute bacterial sinusitis and prolonged viral upper respiratory tract infection are similar, resulting in frequent misclassification of viral infections. There is no evidence to effectively distinguish bacterial from viral acute rhinosinusitis using fever and facial, dental, or both facial and dental pain (Hauer 2014). Watchful waiting is supported by current guidelines within the first seven to 10 days after symptoms of upper respiratory tract infection symptoms appear (Aring 2016). Antibiotics and intranasal steroids have been recommended for acute bacterial rhinosinusitis, although most international guidelines do not recommend the use of antibiotics to treat mild, moderate, or uncomplicated acute rhinosinusitis (Dass 2016). There is no consensus as to when to use antibiotics; furthermore, overuse of antibiotics is an alarming problem among both patients and practitioners. Antibiotics should be prescribed for people with acute rhinosinusitis whose symptoms persist for more than 10 days, in the case of onset of severe signs or symptoms of high fever (> 39 °C) and purulent nasal discharge or facial pain lasting for at least three consecutive days, or worsening symptoms following a typical viral illness lasting for five days that was initially improving (Harris 2016; Kaplan 2014).
The common cold frequently involves the upper airways, including occlusion in the sinus cavities (Gwaltney 1994). In a retrospective analysis, rhinorrhoea, purulent secretions, sinus tenderness, and a history of sinusitis were significant predictors for diagnosing sinusitis (Little 2000; Zalmanovici Trestioreanu 2013).
Diagnosis is often confirmed by sinus imaging, and computed tomography of the sinuses is helpful for people whose symptoms do not improve with treatment. Radiography is not recommended for evaluating acute uncomplicated sinusitis (Aring 2016).
Sinusitis is accompanied by inflammation of the contiguous nasal mucosa; hence, rhinosinusitis has become the preferred term (Snow 2001). Inflammation of nasal mucosa and blockage of the sinus ostium play an essential role in the development of sinusitis (Tutkun 1996). The characteristic signs and symptoms of rhinosinusitis are sinus obstruction, mucus retention, and infection. Complications can occur through intracranial extension of the infection.
Description of the intervention
The term Cyclamen europaeum has been applied to several related species of Cyclamen, but strictly applies to Cyclamen purpurascens. The tuber of Cyclamen europaeum (Cyclamen purpurascens), a member of the Primulaceae family, has been used in herbal medicine for a range of indications; it is reported to be a drastic purgative. An extract of the tuber has been used for sinusitis in the form of nasal spray known as Nasodren and Sinuforte (Micromedex 2.0).
How the intervention might work
Sinusitis treatment focuses on eliminating causative factors and controlling the inflammatory and infectious components (Becker 2003; Passali 2016). The frozen, dried, natural fluid extract of the Cyclamen europaeum plant delivered intranasally is thought to have beneficial effects in relieving congestion by facilitating nasal drainage, and has an anti‐inflammatory effect (Mashkova 2010). Beneficial effects were observed when used either as a monotherapy for mild or moderately severe disease or in combination with other agents for the treatment of acute or exacerbated chronic rhinosinusitis (Savvateeva 2010). Including Cyclamen europaeum in combined therapy for mild and moderately severe acute rhinosinusitis and exudative otitis media may make it possible to avoid drainage procedures and shorten the duration of antibacterial treatment. Simultaneous acceleration of the recovery of functional activity of the endonasal mucosa suggests a pronounced antirecurrence action of this therapy (Bogomil'skii 2010). When Cyclamen europaeum extract was used in comparison to saline for patients with chronic sinusitis and nasal polyps undergoing endoscopic sinus surgery, a significant improvement in patients' symptoms, nasal endoscopic signs, and patient satisfaction was reported. These results are thought to be connected to activities of the extract in facilitating nasal drainage and clearing the paranasal sinuses (Mullol 2009).
Why it is important to do this review
Key points of agreement in clinical guidelines regarding therapy for acute rhinosinusitis include efficacy of symptomatic treatment and the importance of reducing unnecessary antibiotic use. However, there is no consensus in guidelines regarding when antibiotics should be considered as a reasonable treatment strategy (Meltzer 2011). The management of rhinosinusitis depends on the duration and severity of symptoms. A variety of conservative and pharmacological interventions are available, although physicians can find it difficult to develop a cohesive and logical approach to sinusitis treatment (Benninger 1997; Libman 2017; Rosenfeld 2015; Sharp 2015). Antibiotics are not needed for mild to moderate sinusitis within the first week of illness. A greater likelihood of bacterial rhinosinusitis after 10 days makes antibiotic therapy a reasonable option (Van den Broek 2014). Around 80% of participants with acute sinusitis treated without antibiotics improved within two weeks (Ahovuo‐Saloranta 2014). In a Cochrane Review, a small clinical benefit was observed in participants treated with antibiotics (Ahovuo‐Saloranta 2014). A recent systematic review found that antibiotic treatment provided more symptomatic relief within the first days of treatment compared to placebo, but after 10 days both groups had similar improvement rates (Burgstaller 2016). Avoiding antibiotics for acute sinusitis could reduce antibiotic adverse effects, antibiotic resistance, and healthcare costs (Smith 2012). Another Cochrane Review did not find clear evidence for efficacy of nasal irrigations, decongestants, and antihistamines for acute sinusitis in children (Shaikh 2014). The use of adjunctive medications for acute sinusitis, such as antihistamines, decongestants, and systemic and nasal corticosteroids, also remains controversial (Shrum 2001; Venekamp 2014; Zalmanovici Trestioreanu 2013). Recent studies have tested Cyclamen europaeum extract, a novel phytotherapeutic product marketed in Europe and delivered intranasally, for its effectiveness in relieving symptoms in acute sinusitis, and found the treatment to be effective (Mullol 2009; Pfaar 2012). A recent prospective observational study reported that Cyclamen europaeum given as a monotherapy appears to be more effective than other monotherapies and combination therapies and at a lower cost per cured patient (Mullol 2013). However, a systematic review addressing the effectiveness of this therapy has not been conducted.
Objectives
To assess the effectiveness of topical intranasal Cyclamen europaeum extract on clinical response in adults and children with acute sinusitis.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials.
Types of participants
Children and adults with acute sinusitis. Acute sinusitis was defined by a clinical diagnosis (including purulent nasal discharge and congestion, cough beyond seven days, facial pain, and fever) and radiological evidence or nasal endoscopy. We included trials in mixed populations with acute and non‐acute sinusitis if outcomes were reported separately for these subgroups.
Types of interventions
Intranasal Cyclamen europaeum extract (any preparation, dose, or duration of treatment) compared to placebo, antibiotics, intranasal corticosteroids, or no treatment. We included studies reporting combined interventions only if both treatment arms received the same co‐interventions, except for Cyclamen europaeum extract.
Types of outcome measures
Primary outcomes
-
Proportion of participants with resolution or improvement of symptoms up to 14 days.
-
Proportion of participants with resolution or improvement of symptoms up to 30 days.
Secondary outcomes
-
Proportion of participants with any adverse event.
-
Proportion of participants who developed complications.
-
Days off school or work.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Trials (CENTRAL; 2018, Issue 1), part of the Cochrane Library (www.cochranelibrary.com) (accessed 18 January 2018), which includes the Cochrane Acute Respiratory Infections Group's Specialised Register, MEDLINE Ovid (1946 to 18 January 2018), and Embase.com (1974 to 18 January 2018). We searched CENTRAL and MEDLINE with the search strategy detailed in Appendix 1. We combined the MEDLINE search with the Cochrane Highly Sensitive Search Strategy for identifying randomised trials in MEDLINE; sensitivity‐maximising version (2008 revision): Ovid format (Lefebvre 2011). We adapted the search strategy for Embase (see Appendix 2). There were no language or publication restrictions.
Searching other resources
We searched the WHO International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/en; search strategy in Appendix 3), and ClinicalTrials.gov (www.clinicaltrials.gov; search strategy in Appendix 4) on 1 February 2018. We inspected the reference lists of all identified studies and review literature for further relevant studies. We contacted trial authors for additional information (see Characteristics of excluded studies).
Data collection and analysis
Selection of studies
Two review authors (AZT, AB) independently screened titles and abstracts of all studies identified as a result of the search for potential inclusion in the review. We retrieved the full‐text study reports or publications of studies deemed potentially relevant, and two review authors (AZT, AB) independently screened the full‐text studies for inclusion, and identified and recorded reasons for exclusion of ineligible studies. Any disagreements were resolved through discussion or by consulting a third review author (BP) when necessary. We identified and excluded duplicates and collated multiple reports of the same study so that each study, rather than each report, was the unit of interest in the review. We recorded the selection process in sufficient detail to complete a PRISMA flow diagram and Characteristics of excluded studies table (Moher 2009). We did not impose any language restrictions.
Data extraction and management
We used a data collection form for study characteristics and outcome data that had been piloted on at least one study in the review. Two review authors (AZT, AB) extracted study characteristics from the included studies. We planned to extract the following study characteristics.
-
Methods: study design, total duration of study, details of any 'run in' period, number of study centres and location, study setting, withdrawals, and date of study.
-
Participants: N, mean age, age range, gender, severity of condition, diagnostic criteria, smoking history, inclusion criteria, and exclusion criteria.
-
Interventions: intervention, comparison, concomitant medications, and excluded medications.
-
Outcomes: primary and secondary outcomes specified and collected, and time points reported.
-
Notes: funding for trial, and notable conflicts of interest of trial authors.
Two review authors (AZT, AB) independently extracted outcome data from the included studies. We noted in the Characteristics of included studies table if outcome data were not reported in a usable way. Any disagreements were resolved by consensus or by involving a third review author (BP). One review author (AZT) transferred data into the Review Manager 5 file (Review Manager 2014). We double‐checked that data were entered correctly by comparing the data presented in the systematic review with the study reports. A second review author (AB) spot‐checked study characteristics for accuracy against the trial report.
Assessment of risk of bias in included studies
Two review authors (AZT, AB) independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Any disagreements were resolved by discussion or by involving a third review author (BP). We assessed risk of bias according to the following domains.
-
Random sequence generation.
-
Allocation concealment.
-
Blinding of participants and personnel.
-
Blinding of outcome assessment.
-
Incomplete outcome data.
-
Selective outcome reporting.
-
Other bias.
We graded each potential source of bias as high, low, or unclear and provided a justification for our judgement in the 'Risk of bias' table. We summarised the 'Risk of bias' judgements across different studies for each of the domains listed. Where necessary, we considered blinding separately for different key outcomes. Where information on risk of bias related to unpublished data or correspondence with a trialist, we noted this in the 'Risk of bias' table.
When considering treatment effects, we took into account the risk of bias for the studies that contributed to that outcome.
We included trials if they met the following criteria:
-
a randomisation method is described that would not allow the investigator or participant to know or influence the intervention group before the eligible participant entered into the study (low risk of bias); and
-
randomisation is stated but no information on the method used is available (unclear risk of bias).
Assessment of bias in conducting the systematic review
We conducted the review according to this published protocol and planned to report any deviations in the Differences between protocol and review section.
Measures of treatment effect
We analysed dichotomous data by calculating the risk ratio (RR) and risk difference (RD) for each trial with the uncertainty in each result expressed as a 95% confidence interval (CI). We analysed continuous outcomes when normally distributed by using the mean and standard deviation from each study and calculating the mean difference (MD) and the 95% CI. We expressed the results according to the recommendations in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We performed all analyses on the basis of intention‐to‐treat.
Unit of analysis issues
We included randomised controlled trials with standard designs and parallel groups in the review. Participants were included only once in the analyses.
Dealing with missing data
We tried to contact study authors to obtain missing data.
Assessment of heterogeneity
We assessed heterogeneity by inspection of the graphical presentations and I² statistic for heterogeneity. Values of 25%, 50%, and 75% corresponded to low, medium, and high levels of heterogeneity.
Assessment of reporting biases
We planned a funnel plot analysis to assess possible publication bias.
Data synthesis
We used the fixed‐effect model for combining study data.
GRADE and ‘Summary of findings’ table
We created summary of findings Table for the main comparison table using the outcome proportion of participants with any adverse event. We used the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness, and publication bias) to assess the quality of a body of evidence as it relates to the studies which contribute data to the meta‐analyses for the prespecified outcomes (Atkins 2004). We used methods and recommendations described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), employing GRADEpro GDT software (GRADEpro GDT 2014).
Subgroup analysis and investigation of heterogeneity
We planned subgroup analyses according to the treatment in the control group to assess the impact of this possible source of heterogeneity. We included only two studies in the review, and both used placebo in the control group.
Sensitivity analysis
We planned to use the random‐effects model to test the robustness of results when heterogeneity was present. We detected no heterogeneity between the studies. We performed a sensitivity analysis to check the robustness of the result by imputing data, considering best‐case scenario (assuming none of the dropouts in the intervention group had an adverse event and all dropouts in the control group had an adverse event) and worst‐case scenario (assuming all dropouts in the intervention group had an adverse event and none of the dropouts in the control group had an adverse event), as Ponikau 2012 had a high dropout rate.
Results
Description of studies
Results of the search
We identified 87 references from the electronic searches. After removing 21 duplicates, two review authors (AZT, AB) inspected 66 abstracts. We excluded 56 abstracts for the following reasons: not acute sinusitis, not randomised, observational study, intervention of interest not used, no relevant outcomes, review articles. We considered 10 studies for inclusion after inspecting the abstracts and obtaining full‐text reports (Figure 1). We excluded eight studies which did not meet the inclusion criteria for this review.
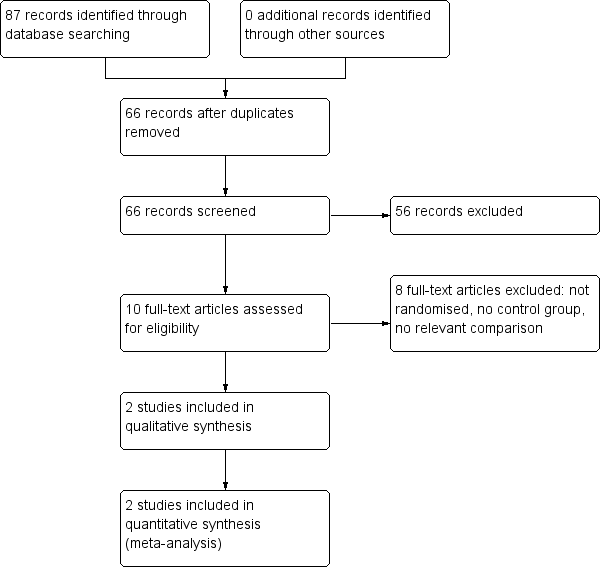
Study flow diagram.
Included studies
See Characteristics of included studies table.
Two studies (147 participants) met the inclusion criteria and were included in the review. Participants were assigned to nasal Cyclamen europaeum spray or placebo. The studies were multicentre trials: one was conducted in 13 centres in Germany (Pfaar 2012), and one study involved outpatients in 25 centres in the USA (Ponikau 2012).
Participants were adults with a documented episode of acute sinusitis confirmed by radiology or nasal endoscopy. The entry criteria and participants in the trials were similar.
Both studies used a placebo in the control group and the same dose of Cyclamen europaeum lyophilised extract, 1.3 mg once daily in each nostril, in the treatment group. Pfaar 2012 used concomitant amoxycillin in both arms or an alternative for participants who were allergic to penicillin. Treatment duration in the studies was 15 days in Pfaar 2012 and seven days in Ponikau 2012.
The outcomes in the included studies reported change from baseline in mean total symptom score, individual symptom scores, endoscopic changes, treatment failure or need for additional treatment, complications, sleep quality, and overall treatment satisfaction in Pfaar 2012; and change from baseline in sinus opacification on computed tomography (CT) scans, reduction in total symptom score, other symptom scores changes from baseline, and endoscopic inflammation in Ponikau 2012.
Information on adverse events that occurred during the trials is presented in Table 1. The studies described participants who dropped out before the end of the study, and their reasons for leaving.
| Study ID | Cyclamen europaeum | Placebo |
| 67% total 50% nasal irritation mild/moderate 27% mild epistaxis 4% sneezing 3 discontinued treatment | 29% total 4% nasal irritation 14% mild epistaxis 4% vertigo 2 discontinued treatment | |
| 15.4% total Influenza, throat irritation, migraine, sneezing No serious adverse events Did not discontinue treatment | 12.5% total Headache, ear pain, gastritis, back pain, conjunctival haemorrhage No serious adverse events Did not discontinue treatment |
Excluded studies
See Characteristics of excluded studies table.
We excluded eight studies for the following reasons: not randomised, control group not used, intervention of interest not used (Bogomil'skii 2010; Ianov 2007; Kriukov 2007; Mashkova 2010; Ovchinnikov 2009; Rybak 2008; Semenov 2011; Svistushkin 2013). We contacted one author to ask if the study was randomised; we subsequently excluded this study because quasi‐randomisation was used (Ovchinnikov 2009). All excluded studies were published in the same journal between 2007 and 2013.
Risk of bias in included studies

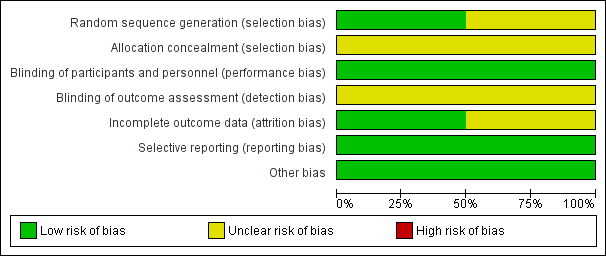
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
The studies were randomised, double‐blind, placebo‐controlled trials.
Allocation
Pfaar 2012 did not report randomisation methods (unclear risk of bias). Ponikau 2012 adequately reported generation of the allocation sequence (low risk of bias). Neither study reported concealment of allocation to treatment (unclear risk of bias).
Blinding
The trials were double‐blinded, and the method of blinding was described (low risk of bias). Blinding of outcome assessors was not reported in the studies (unclear risk of bias).
Incomplete outcome data
Both studies described dropouts before the end of the study and provided reasons (low risk of bias). Total losses to follow‐up were 17% in Pfaar 2012 and 60% in Ponikau 2012. Dropouts were balanced between study arms.
Selective reporting
The studies reported outcomes and results as prespecified in their protocols (low risk of bias).
Other potential sources of bias
We did not identify possible sources of bias. The studies were small and were assessed as moderate quality for the only outcome assessed (adverse events), with similar direction of results for the outcome included in our meta‐analysis. Both studies were supported by pharmaceutical companies, but funding sources did not seem to influence results.
Effects of interventions
We included two studies (147 participants) (Pfaar 2012; Ponikau 2012). See summary of findings Table for the main comparison.
Primary outcomes
1. Proportion of participants with resolution or improvement of symptoms up to 14 days
No studies reported this outcome. One study reported changes in mean total symptom score up to seven days and a trend toward greater symptomatic relief in the Cyclamen europaeum group, although this was not clear (P = 0.64) (Pfaar 2012). Uncertainty in results was observed for improvement of nasal obstruction and oedema. Improvement in facial pain up to seven days was observed, and this was obvious (mean difference ‐1.20, 95% confidence interval (CI) ‐2.32 to ‐0.08; P = 0.04) (Pfaar 2012). There was no clear difference between treatment and control groups for total or individual symptom scores in Ponikau 2012.
2. Proportion of participants with resolution or improvement of symptoms up to 30 days
No studies reported this outcome.
Secondary outcomes
1. Proportion of participants with any adverse event
Both studies reported data for this outcome (Table 1). More adverse events were reported in the Cyclamen europaeum group than in the placebo group during the treatment period, and we are confident in the result (risk ratio (RR) 2.11, 95% CI 1.35 to 3.29; risk difference 0.26, 95% CI 0.13 to 0.40; Analysis 1.1). We assessed the quality of the evidence as moderate (summary of findings Table for the main comparison).
We performed sensitivity analysis by imputing data to check the robustness of the result, considering best‐case scenario (assuming none of the dropouts in the intervention group had an adverse event and all dropouts in the control group had an adverse event) (RR 0.94, 95% CI 0.68 to 1.30; Analysis 1.2), and worst‐case scenario (assuming all dropouts in the intervention group had an adverse event and none of the dropouts in the control group had an adverse event) (RR 3.49, 95% CI 2.30 to 5.30; Analysis 1.3).
2. Proportion of participants who developed complications
Only one study reported this outcome; no complications were reported (Pfaar 2012).
3. Days off school or work
No studies reported this outcome.
We did not perform planned funnel plots and subgroup analyses due to the small number of included studies and because both used a placebo in the control group.
Discussion
Rhinosinusitis is one of the most common upper respiratory diseases treated in general practice (Marple 2006; Schappert 2006). The condition is associated with significant economic burden, which includes reduced productivity and absenteeism, as well as medical costs (Fokkens 2007; Padia 2016; Rudmik 2017). Sinusitis is a common disorder that can cause further morbidity and mortality through progression of inflammation and extension of infection. It is associated with significant patient symptomatology that adversely affects quality of life (Carr 2016). Management of uncomplicated acute rhinosinusitis includes analgesics, saline irrigations and intranasal steroids. The use of antibiotics for people with acute rhinosinusitis is widespread, and there seems to be only a slight added benefit over placebo (Sng 2015). There is a need for improved antibiotic stewardship across all settings (Sharp 2015). Alternative treatments should be considered according to severity of symptoms. We aimed to investigate whether Cyclamen europaeum extract, a novel phytotherapeutic treatment, is an effective topical treatment for acute sinusitis.
Summary of main results
We included two small studies that involved a total of 147 adult participants who received Cyclamen europaeum extract as an intranasal spray versus placebo and provided moderate‐quality evidence for the only outcome assessed (adverse events). We could not assess whether Cyclamen europaeum is effective or not for treating sinusitis. We were able to meta‐analyse results for adverse events only; data for other review outcomes were not available from the included studies. Neither study showed clear differences for total symptom scores changes between people who received Cyclamen europaeum and those who received placebo, although Pfaar 2012 reported a trend toward improvement in total symptom score and obvious difference for improvement of facial pain up to seven days. More adverse events during the treatment period were found in participants in the Cyclamen europaeum group compared to those in the placebo group, although no serious adverse events were reported in either study (Table 1).
Overall completeness and applicability of evidence
The study population included in this review was diagnosed both clinically and by radiology or endoscopy and is not identical to people diagnosed in clinical practice, among whom diagnosis is usually based on clinical symptoms and signs alone.
Cyclamen europaeum extract has been available for the treatment of acute rhinosinusitis in over 20 European countries as an intranasal product. Clinical trials in people with acute rhinosinusitis suggest that Cyclamen europaeum reduces symptoms (Semenov 2011); improves mucociliary transport time (Lopatin 2007); and increases cure rate (Mullol 2009). The saponin fraction of Cyclamen europaeum immediately stimulates nasal secretions. These actions are attributable to irritation of the trigeminal nerve endings in the nasal mucous membranes through cholinergic pathways, leading to reflex discharge of inflammatory sinus exudates through the nose and subsequent decongestion (Gedevanishvili 2007; Jurkiewicz 2016). One study found this treatment was as effective as traditional treatment, and when used as initial monotherapy, reduced drug loading (Svistushkin 2013). We could not assess in our review whether Cyclamen europaeum is effective or not.
Quality of the evidence
We included two small studies (147 participants) in this review. The studies were randomised, but neither reported concealment of allocation to treatment (Pfaar 2012; Ponikau 2012). Both studies found the same direction of effect for the outcome included in the meta‐analysis, that is more adverse events in the groups receiving Cyclamen europaeum. Ponikau 2012 had a high dropout rate (60%), but dropouts were described and balanced between study arms, and absolute numbers of dropouts were small as sample size was small in this study; we performed a sensitivity analysis considering both extreme scenarios to test the robustness of the result and this did not change the conclusion. Both studies were funded by pharmaceutical companies, among them Hartington Pharmaceutical; Cyclamen europaeum nasal spray known as Sinuforte or Nasodren is a trademark and brand of Hartington Pharmaceutical. This did not seem to influence the results, as more adverse events were reported in participants who received Cyclamen europaeum compared to the placebo group. Using GRADE principles we assessed the evidence for the only outcome meta‐analysed, that is proportion of participants with any adverse event, as of moderate quality (summary of findings Table for the main comparison), downgrading quality due to lack of reporting of concealment of allocation to treatment and blinding of outcome assessors in the studies, and a small sample size with high dropouts in Ponikau 2012.
Potential biases in the review process
We conducted searches according to Cochrane Acute Respiratory Infections Group recommendations. Two review authors (AZT, AB) independently selected studies for inclusion and extracted data. Two review authors (AZT, BP) analysed data and interpreted results to prevent possible bias in the review process. We conducted this review according to the published protocol. Participants received concomitant antibiotics in Pfaar 2012; as both groups received antibiotics, the only intervention that differed between groups was Cyclamen europaeum or placebo, and the effect could only be attributed to Cyclamen europaeum. We assessed both studies as at unclear risk of bias for blinding of outcome assessors and at low risk of bias for blinding of participants and personnel.
Agreements and disagreements with other studies or reviews
The limited existing evidence for Cyclamen europaeum treatment, which is controversial, has not been systematically reviewed, and we found the methodology of many studies to be questionable (see Characteristics of excluded studies). One study found that monotherapy with Cyclamen europaeum for participants with moderately severe acute sinusitis was associated with recovery in 73% of people (Semenov 2011). Jurkiewicz 2016 reported that Cyclamen europaeum efficiently reduced symptoms of acute sinusitis. We could not assess the effectiveness of Cyclamen europaeum for acute sinusitis in our review.
The included studies reported no serious adverse events linked to Cyclamen europaeum treatment. This was consistent with findings reported by Kriukov 2007, Ovchinnikov 2009, and Svistushkin 2013.

Study flow diagram.
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Comparison 1 Cyclamen europaeum versus placebo, Outcome 1 Proportion of participants with any adverse event ‐ intention‐to‐treat.

Comparison 1 Cyclamen europaeum versus placebo, Outcome 2 Proportion of participants with any adverse events ‐ best‐case sensitivity analysis.

Comparison 1 Cyclamen europaeum versus placebo, Outcome 3 Proportion of participants with any adverse event ‐ worst‐case sensitivity analysis.
| Cyclamen europaeum compared to placebo for acute sinusitis | ||||||
| Patient or population: adults with acute sinusitis | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | Comments | |
| Risk with placebo | Risk with Cyclamen europaeum | |||||
| Proportion of participants with resolution or improvement of symptoms up to 30 days | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported this outcome. |
| Proportion of participants with any adverse event | Study population | RR 2.11 | 147 | ⊕⊕⊕⊝ Moderate | We downgraded the quality of the evidence as concealment of allocation to treatment and blinding of outcome assessors were not reported in the studies. Also, 1 study had a small sample size with a high attrition rate. | |
| 240 per 1000 | 506 per 1000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) CI: confidence interval; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence | ||||||
| Study ID | Cyclamen europaeum | Placebo |
| 67% total 50% nasal irritation mild/moderate 27% mild epistaxis 4% sneezing 3 discontinued treatment | 29% total 4% nasal irritation 14% mild epistaxis 4% vertigo 2 discontinued treatment | |
| 15.4% total Influenza, throat irritation, migraine, sneezing No serious adverse events Did not discontinue treatment | 12.5% total Headache, ear pain, gastritis, back pain, conjunctival haemorrhage No serious adverse events Did not discontinue treatment |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Proportion of participants with any adverse event ‐ intention‐to‐treat Show forest plot | 2 | 147 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.11 [1.35, 3.29] |
| 2 Proportion of participants with any adverse events ‐ best‐case sensitivity analysis Show forest plot | 2 | 147 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.68, 1.30] |
| 3 Proportion of participants with any adverse event ‐ worst‐case sensitivity analysis Show forest plot | 2 | 147 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.49 [2.30, 5.30] |