Servicios de telerrehabilitación para el accidente cerebrovascular
Información
- DOI:
- https://doi.org/10.1002/14651858.CD010255.pub2Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 16 diciembre 2013see what's new
- Tipo:
-
- Intervention
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Accidentes cerebrovasculares
- Copyright:
-
- Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
Kate E Laver is the guarantor of the review. Contributions included co‐ordinating the review, drafting the protocol, developing the search strategy, searching for trials, obtaining copies of the trials, selecting which trials to include, extracting data from the trials, entering data, carrying out the analysis, interpreting the analysis and drafting the final review.
Daniel Schoene was involved in drafting the protocol, searching for trials, selecting which trials to include, extracting data from trials, interpreting the analysis and drafting the final review.
Maria Crotty was involved in drafting the protocol, selecting which trials to include (arbiter), interpreting the analysis and drafting the final review.
Stacey George was involved in drafting the protocol, selecting which trials to include (arbiter), interpreting the analysis and drafting the final review.
Natasha A Lannin was involved in drafting the protocol, carrying out the analysis, interpreting the analysis and drafting the final review.
Catherine Sherrington was involved in drafting the protocol, guiding and interpreting the analysis and drafting the final review.
All authors will be responsible for updating the review.
Declarations of interest
None known.
Acknowledgements
The authors wish to thank Brenda Thomas for her assistance in designing the search strategy. We would also like to thank Cochrane editors Peter Langhorne and Alex Pollock and external peer reviewer Paul Davies.
We wish to thank Andrea Turolla, Nancy Mayo, Greg Smith and Han Boter, who generously provided additional details and analyses from their trials to assist us with preparation of the review.
Version history
| Published | Title | Stage | Authors | Version |
| 2020 Jan 31 | Telerehabilitation services for stroke | Review | Kate E Laver, Zoe Adey‐Wakeling, Maria Crotty, Natasha A Lannin, Stacey George, Catherine Sherrington | |
| 2013 Dec 16 | Telerehabilitation services for stroke | Review | Kate E Laver, Daniel Schoene, Maria Crotty, Stacey George, Natasha A Lannin, Catherine Sherrington | |
| 2012 Dec 12 | Telerehabilitation services for stroke | Protocol | Kate E Laver, Daniel Schoene, Maria Crotty, Stacey George, Natasha A Lannin, Catherine Sherrington | |
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
Medical Subject Headings Check Words
Humans;
PICO
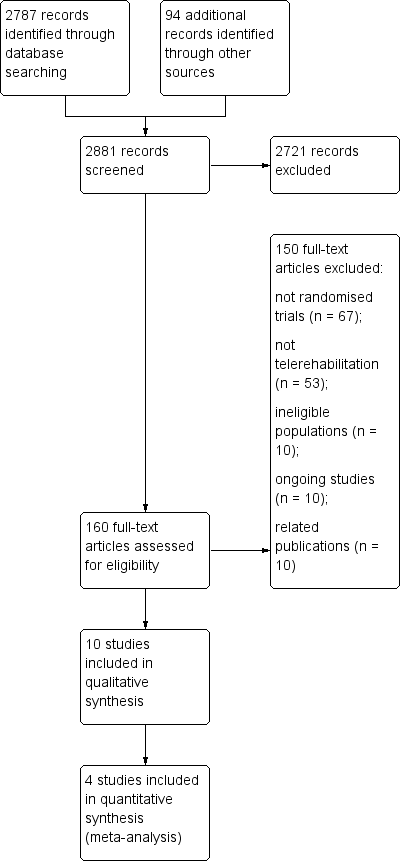
Study flow diagram.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
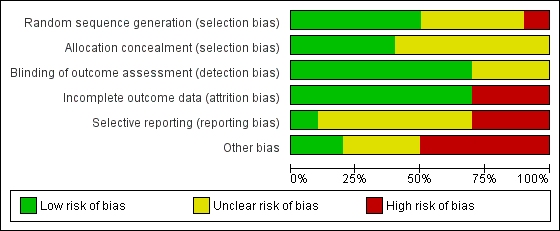
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
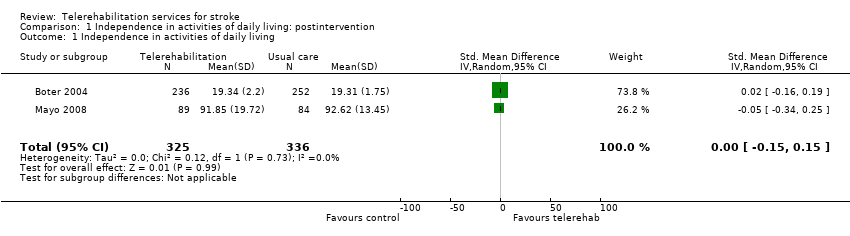
Comparison 1 Independence in activities of daily living: postintervention, Outcome 1 Independence in activities of daily living.
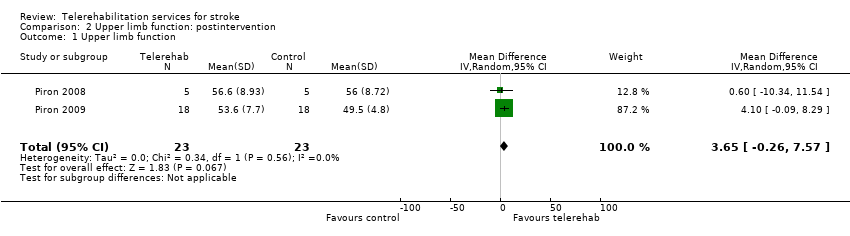
Comparison 2 Upper limb function: postintervention, Outcome 1 Upper limb function.
| Study | Screened | Randomised | Allocated to intervention group | Allocated to control group | Assessed at follow‐up |
| 691 | 536 | 263 | 273 | 486 | |
| 167 | 25 | 13 | 12 | 20 | |
| 52 | 52 | 27 | 25 | 44 | |
| 62 | 19 | 9 | 10 | 16 | |
| Not reported | 11 | Not reported | Not reported | 9 | |
| Not reported | 16 | Not reported | Not reported | Not reported | |
| 294 | 190 | 96 | 94 | 157 | |
| Not reported | 10 | 5 | 5 | 10 | |
| Not reported | 36 | 18 | 18 | 36 | |
| 161 | 38 | 19 | 19 | 32 |
| Study | Intervention | Comparison | Time after stroke | Country of study |
| Case management via 3 telephone calls and a home visit up to 24 weeks after discharge from an acute hospital following stroke | Usual care | Not reported; however, intervention was provided on discharge from acute facility | The Netherlands | |
| Upper limb therapy targeting finger and wrist movements provided via a computerised programme in which explicit feedback on performance was provided. Regular teleconferencing occurred between participant and therapist | Upper limb therapy targeting finger and wrist movements provided via a computerised programme whereby explicit feedback on performance was not provided. Regular teleconferencing occurred between participant and therapist | Chronic phase | USA | |
| A programme designed to improve the person's functional mobility administered via televisits, use of an in‐home messaging device and 5 telephone calls over a 3‐month period | Usual care | Subacute phase | USA | |
| Lower limb therapy targeting ankle movements provided via a computerised programme in which explicit feedback on performance was provided. Teleconferencing was used regularly, and performance data were emailed to the therapist | Lower limb therapy targeting ankle movements provided via a computerised programme whereby explicit feedback on performance was not provided. Teleconferencing was used regularly, and performance data were emailed to the therapist | Chronic phase | USA | |
| A total of 12 therapy sessions (occupational therapy and physiotherapy) were conducted via a desktop videophone. Interventions included education, retraining of self care, functional mobility and posture, home modifications and therapy to improve function in impaired limbs | The same intervention programme was delivered face‐to‐face | Not reported | USA | |
| Upper limb therapy using the Home Care Activity Device (computer‐based programme) for 1 month | Usual care and generic exercises were provided by a physician | Chronic phase | The Netherlands | |
| Case management intervention provided via home visits and telephone calls for 6 weeks following discharge from acute care | Participants were instructed to make an appointment with their general practitioner | Acute phase | Canada | |
| Upper limb therapy that was delivered using a virtual reality programme at home and supplemented by videoconferencing | Upper limb therapy that was delivered using a virtual reality programme and conducted in the clinic setting | Chronic phase | Italy | |
| Upper limb therapy that was delivered using a virtual reality telerehabilitation programme and that took place in the home | A programme of conventional upper limb exercises | Chronic phase | Italy | |
| An intervention to support the caregivers of stroke survivors by enhancing knowledge, skills and coping. Delivered via email, online chat sessions and online resources | Participants had access to some of the online resources | Not reported | USA |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Independence in activities of daily living Show forest plot | 2 | 661 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.00 [‐0.15, 0.15] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Upper limb function Show forest plot | 2 | 46 | Mean Difference (IV, Random, 95% CI) | 3.65 [‐0.26, 7.57] |