| Author (year) | n total | n TBI | % TBI | Intervention | Comparator | %TBI Intervention | %TBI comparator |
| Botulinum toxin A vs placebo |
| NCT00900666 | 19 | 7 | 37 | Botulinum toxin A | Placebo | NR | NR |
| Burbaud 1996 | 23 | 4 | 17 | Botulinum toxin A | Placebo | NR | NR |
| Fietzek 2014 | 52 | 6 | 12 | Botulinum toxin A | Placebo | 12 | 12 |
| Grazko 1995 | 20 | 1 | 5 | Botulinum toxin A | Placebo | Cross‐over trial | ‐ |
| Simpson 2009 | 60 | 11 | 18 | Botulinum toxin A | Tizanidine or placebo | 15 | 14 and 26 placebo |
| Smith 2000 | 21 | 2 | 10 | Botulinum toxin A | Placebo | 10 | 16 |
| Botulinum toxin A vs therapy |
| Guo 2006 | 60 | 17 | 28 | Botulinum toxin A with rehab | Rehab only | 26 | 30 |
| Botulinum toxin A vs botulinum toxin A (dosage) |
| Gracies 2009 | 21 | 6 | 29 | High dilution botulinum toxin A with endplate target | Low dilution botulinum toxin A with end plate target | NR | NR |
| Botulinum toxin A vs botulinum toxin A (volume) |
| Francisco 2002 | 13 | 3 | 23 | High volume botulinum toxin A | Low volume botulinum toxin A | 16 | 28 |
| Barnes 2010 | 192 | 11 | 6 | High volume botulinum toxin A | Low volume botulinum toxin A | 5 | 6 |
| Botulinum toxin A vs botulinum toxin A (location) |
| Childers 1996 | 17 | 2 | 12 | Botulinum toxin A injections towards mid belly | Botulinum toxin A injections away from mid belly | 0 | 25 |
| Gracies 2009 | 21 | 6 | 29 | High dilution botulinum toxin A with endplate target | Low dilution botulinum toxin A with end plate target | NR | NR |
| Baclofen vs placebo |
| Armstrong 1997 | 19 | 2 | 11 | Intrathecal dose of baclofen | Saline | 16 | 0 |
| Van Schaeybroeck 2000 | 11 | 1 | 9 | Intrathecal baclofen | Placebo | 16 | 0 |
| Cyclobenzaprine vs placebo |
| Ashby 1972 | 15 | 4 | 27 | Cyclobenzaprine | Placebo | Cross‐over trial | ‐ |
| Phenothiazine vs placebo |
| Burke 1975 | 9 | 2 | 22 | Phenothiazine | Placebo | Cross‐over trial | ‐ |
| Tizanidine vs placebo |
| Meythaler 2001b | 17 | 8 | 47 | Tizanidine | Placebo | Cross‐over trial | ‐ |
| Tizanidine vs botulinum toxin A |
| Simpson 2009 | 60 | 11 | 18 | Botulinum toxin A | Tizanidine or placebo | 15 | 14 and 26 placebo |
| Tizanidine vs diazepam |
| Bes 1988 | 105 | 16 | 15 | Tizanidine | Diazepam | 10 | 20 |
| Casting vs control |
| Harvey 2006 | 44 | 7 | 16 | Splint | No splint | 13 | 21 |
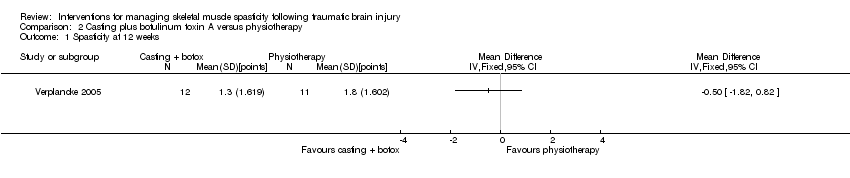
| Casting vs therapy |
| Harvey 2006 | 44 | 7 | 16 | Splint | No splint | 13 | 21 |
| Splinting vs control |
| Copley 2013 | 10 | 2 | 20 | Individualised hand splint | No splint | 33 | 0 |
| Lannin 2003 | 28 | 2 | 7 | Stretching and hand splint | Stretching only | NR | NR |
| Thibaut 2015 | 17 | 7 | 41 | Soft splints | No treatment | NR | NR |
| Splinting vs therapy |
| Lannin 2003 | 28 | 2 | 7 | Stretching and hand splint | Stretching only | NR | NR |
| Thibaut 2015 | 17 | 7 | 41 | Soft splints | Stretching | NR | NR |
| Functional electrical stimulation vs control |
| Chang 2009 | 14 | 3 | 21 | Upper limb botulinum toxin A injections for higher hand function | Upper limb botulinum toxin A injections for lower hand function | 33 | 0 |
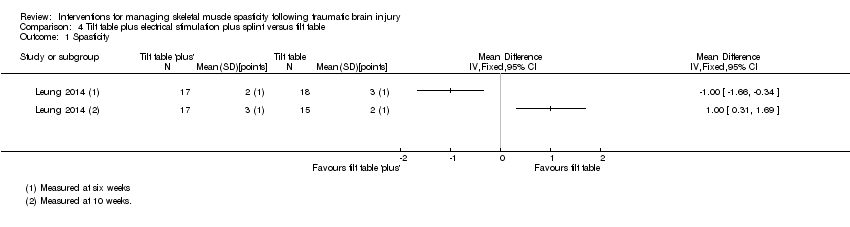
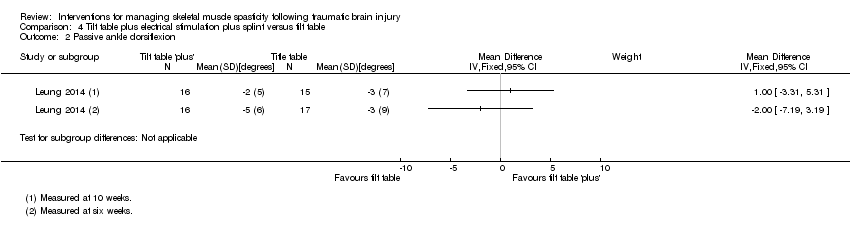
| Electrical stimulation + splinting vs splinting |
| Leung 2012 | 36 | 5 | 14 | Electrical stimulation to the wrist and finger extensor muscles for 1 hour a day + wrist splint for 12 hours a day, over 4 weeks | Wrist splint for 12 hours a day, over 4 weeks | 6 | 22 |
| Repetitive peripheral magnetic stimulation vs sham |
| Krewer 2014 | 66 | 3 | 5 | Repetitive peripheral magnetic stimulation | Sham stimulation | 10 | 0 |
| Transcutaneous electrical acupoint stimulation vs another dose |
| Zhao 2015 | 60 | 1 | 2 | Transcutaneous electrical acupoint stimulation (100 Hz) | Transcutaneous electrical acupoint stimulation (2 Hz) | 0 | 5 |
| Transcutaneous electrical acupoint stimulation vs sham |
| Zhao 2015 | 60 | 1 | 2 | Transcutaneous electrical acupoint stimulation (100 Hz) | Sham stimulation | 0 | 0 |
| Ultrasound vs infrared |
| Nakhostin 2009 | 21 | 1 | 5 | Infrared | Therapeutic ultrasound | NR | NR |
| Robot vs bobath |
| Fazekas 2007 | 30 | 8 | 27 | Robot‐mediated therapy with bobath therapy | Bobath therapy | 13 | 40 |