Latihan otot lantai pelvis untuk pencegahan dan rawatan inkontinens urinari dan fikal dalam kalangan wanita antenatal dan postnatal.
Abstract
Background
About one‐third of women have urinary incontinence and up to one‐tenth have faecal incontinence after childbirth. Pelvic floor muscle training (PFMT) is commonly recommended during pregnancy and after birth for both prevention and treatment of incontinence.
This is an update of a review previously published in 2012.
Objectives
To determine the effectiveness of pelvic floor muscle training (PFMT) in the prevention or treatment of urinary and faecal incontinence in pregnant or postnatal women.
Search methods
We searched the Cochrane Incontinence Specialised Register (16 February 2017) and reference lists of retrieved studies.
Selection criteria
Randomised or quasi‐randomised trials in pregnant or postnatal women. One arm of the trial included PFMT. Another arm was no PFMT, usual antenatal or postnatal care, another control condition, or an alternative PFMT intervention.
Data collection and analysis
Review authors independently assessed trials for inclusion and risk of bias. We extracted data and checked them for accuracy. Populations included: women who were continent (PFMT for prevention), women who were incontinent (PFMT for treatment) at randomisation and a mixed population of women who were one or the other (PFMT for prevention or treatment). We assessed quality of evidence using the GRADE approach.
Main results
The review included 38 trials (17 of which were new for this update) involving 9892 women from 20 countries. Overall, trials were small to moderate sized, and the PFMT programmes and control conditions varied considerably and were often poorly described. Many trials were at moderate to high risk of bias. Other than two reports of pelvic floor pain, trials reported no harmful effects of PFMT.
Prevention of urinary incontinence: compared with usual care, continent pregnant women performing antenatal PFMT may have had a lower risk of reporting urinary incontinence in late pregnancy (62% less; risk ratio (RR) for incontinence 0.38, 95% confidence interval (CI) 0.20 to 0.72; 6 trials, 624 women; low‐quality evidence). Similarly, antenatal PFMT decreased the risk of urinary incontinence in the mid‐postnatal period (more than three to six months' postpartum) (29% less; RR 0.71, 95% CI 0.54 to 0.95; 5 trials, 673 women; moderate‐quality evidence). There was insufficient information available for the late (more than six to 12 months') postnatal period to determine effects at this time point.
Treatment of urinary incontinence: it is uncertain whether antenatal PFMT in incontinent women decreases incontinence in late pregnancy compared to usual care (RR 0.70, 95% CI 0.44 to 1.13; 3 trials, 345 women; very low‐quality evidence). This uncertainty extends into the mid‐ (RR 0.94, 95% CI 0.70 to 1.24; 1 trial, 187 women; very low‐quality evidence) and late (RR 0.50, 95% CI 0.13 to 1.93; 2 trials, 869 women; very low‐quality evidence) postnatal periods. In postnatal women with persistent urinary incontinence, it was unclear whether PFMT reduced urinary incontinence at more than six to 12 months' postpartum (RR 0.55, 95% CI 0.29 to 1.07; 3 trials; 696 women; very low‐quality evidence).
Mixed prevention and treatment approach to urinary incontinence: antenatal PFMT in women with or without urinary incontinence (mixed population) may decrease urinary incontinence risk in late pregnancy (26% less; RR 0.74, 95% CI 0.61 to 0.90; 9 trials, 3164 women; low‐quality evidence) and the mid‐postnatal period (RR 0.73, 95% CI 0.55 to 0.97; 5 trials, 1921 women; very low‐quality evidence). It is uncertain if antenatal PFMT reduces urinary incontinence risk late postpartum (RR 0.85, 95% CI 0.63 to 1.14; 2 trials, 244 women; low‐quality evidence). For PFMT begun after delivery, there was considerable uncertainty about the effect on urinary incontinence risk in the late postnatal period (RR 0.88, 95% CI 0.71 to 1.09; 3 trials, 826 women; very low‐quality evidence).
Faecal incontinence: six trials reported faecal incontinence outcomes. In postnatal women with persistent faecal incontinence, it was uncertain whether PFMT reduced incontinence in the late postnatal period compared to usual care (RR 0.68, 95% CI 0.24 to 1.94; 2 trials; 620 women; very low‐quality evidence). In women with or without faecal incontinence (mixed population), antenatal PFMT led to little or no difference in the prevalence of faecal incontinence in late pregnancy (RR 0.61, 95% CI 0.30 to 1.25; 2 trials, 867 women; moderate‐quality evidence). For postnatal PFMT in a mixed population, there was considerable uncertainty about the effect on faecal incontinence in the late postnatal period (RR 0.73, 95% CI 0.13 to 4.21; 1 trial, 107 women, very low‐quality evidence).
There was little evidence about effects on urinary or faecal incontinence beyond 12 months' postpartum. There were few incontinence‐specific quality of life data and little consensus on how to measure it. We found no data on health economics outcomes.
Authors' conclusions
Targeting continent antenatal women early in pregnancy and offering a structured PFMT programme may prevent the onset of urinary incontinence in late pregnancy and postpartum. However, the cost‐effectiveness of this is unknown. Population approaches (recruiting antenatal women regardless of continence status) may have a smaller effect on urinary incontinence, although the reasons for this are unclear. It is uncertain whether a population‐based approach for delivering postnatal PFMT is effective in reducing urinary incontinence. Uncertainty surrounds the effects of PFMT as a treatment for urinary incontinence in antenatal and postnatal women, which contrasts with the more established effectiveness in mid‐life women.
It is possible that the effects of PFMT might be greater with targeted rather than mixed prevention and treatment approaches and in certain groups of women. Hypothetically, for instance, women with a high body mass index are at risk factor for urinary incontinence. Such uncertainties require further testing and data on duration of effect are also needed. The physiological and behavioural aspects of exercise programmes must be described for both PFMT and control groups and how much PFMT women in both groups do, to increase understanding of what works and for whom.
Few data exist on faecal incontinence or costs and it is important that both are included in any future trials. It is essential that future trials use valid measures of incontinence‐specific quality of life for both urinary and faecal incontinence.
PICO
Ringkasan bahasa mudah
Berkesankah senaman otot lantai pelvis yang dilakukan semasa hamil atau selepas bersalin untuk mencegah atau merawat inkontinens?
Soalan ulasan
Untuk menilai sama ada melakukan senaman otot pelvis (PFME) semasa hamil atau selepas bersalin mengurangkan inkontinens. Ini adalah kemas kini ulasan terbitan 2012.
Latar belakang
Lebih satu pertiga wanita mengalami masalah pengaliran keluar air kencing (inkontinens urinari) secara tidak sengaja (luar kawal) di trimester kedua dan ketiga kehamilan dan kira‐kira satu pertiga kebocoran air kencing berlaku dalam tempoh tiga bulan pertama selepas bersalin. Lebih kurang satu perempat wanita mengalami kentut (angin) atau najis (inkontinens anus) tak terkawal pada akhir kehamilan dan satu perlima mengalami kebocoran angin atau najis setahun selepas bersalin. PFME sering disyorkan oleh para profesional kesihatan ketika hamil dan selepas bersalin untuk mencegah dan merawat inkontinens. Otot‐otot yang terlibat akan diperkukuhkan dan sentiasa kuat dengan melakukan PFME secara berkala. Otot‐otot akan menguncup beberapa kali berturut‐turut, lebih daripada sekali sehari, beberapa hari seminggu dan berterusan selama‐lamanya.
Adakah ulasan ini terkini?
Bukti adalah terkini sehingga 16 Februari 2017.
Ciri‐ciri kajian
Kami memasukkan 38 kajian (17 adalah kajian baharu dalam kemas kini ini) yang melibatkan 9892 wanita dari 20 buah negara. Kajian‐kajian ini termasuklah wanita hamil atau wanita yang telah melahirkan bayi mereka dalam tempoh tiga bulan. Wanita melaporkan kebocoran air kencing, najis, kedua‐dua air kencing atau najis, atau tiada kebocoran. Mereka telah ditetapkan secara rawak untuk menerima PFME (untuk cuba elakkan inkontinens atau sebagai rawatan untuk inkontinens) atau tidak dan kesan‐kesannya dibandingkan.
Sumber‐sumber pembiayaan kajian
Sembilan belas kajian telah dibiaya awam. Satu kajian telah menerima geran daripada sumber‐sumber awam dan swasta. Tiga kajian tidak menerima sebarang pembiayaan dan 15 kajian tidak mengisytiharkan sumber‐sumber pembiayaan.
Keputusan utama
Wanita hamil tanpa kebocoran air kencing yang melakukan PFME untuk mengelakkan kebocoran: wanita mungkin melaporkan kurang kebocoran air kencing pada akhir kehamilan dan tiga hingga enam bulan selepas bersalin. Tiada cukup maklumat untuk menentukan sama ada kesan‐kesan ini berterusan sehingga melepasi tahun pertama selepas kelahiran bayi.
Wanita dengan kebocoran air kencing, hamil atau selepas bersalin, yang melakukan PFME sebagai rawatan: Adalah tidak pasti sama ada melakukan PFME semasa hamil mengurangkan kebocoran di akhir kehamilan atau dalam setahun selepas kelahiran bayi. Adalah tidak jelas sama ada melakukan PFME membantu wanita dengan kebocoran selepas bersalin.
Wanita dengan atau tanpa kebocoran air kencing (kumpulan yang bercampur), hamil atau selepas bersalin, yang melakukan PFME dengan tujuan sama ada untuk mencegah atau merawat kebocoran: wanita yang mula bersenam semasa hamil kurang berkemungkinan untuk melaporkan kebocoran pada akhir kehamilan dan sehingga enam bulan selepas bersalin, tetapi tidak pasti sama ada dapat kesannya bertahan selama satu tahun selepas bersalin. Bagi wanita yang memulakan PFME selepas bersalin, kesan ke atas kebocoran satu tahun selepas kelahiran adalah tidak pasti.
Kebocoran najis: beberapa kajian (hanya enam) mempunyai bukti mengenai kebocoran najis. Satu tahun selepas bersalin, adalah tidak pasti jika PFME boleh membantu mengurangkan kebocoran najis dlam kalangan wanita yang mula bersenam selepas bersalin. Adalah tidak pasti juga jika wanita dengan atau tanpa kebocoran najis (kumpulan bercampur) yang telah memulakan PFME ketika hamil kurang cenderung untuk kebocoran najis di akhir kehamilan atau sehingga satu tahun selepas bersalin.
Terdapat sedikit maklumat mengenai bagaimana PFME boleh mempengaruhi kebocoran yang berkaitan dengan kualiti kehidupan. Terdapat dua laporan kesakitan otot lantai pelvis tetapi tiada kesan‐kesan mudarat lain PFME direkodkan. Adalah tidak diketahui sama ada PFME menawarkan nilai untuk wang kerana tiada kajian yang menganalisis ekonomi kesihatan. Adalah tidak diketahui jika PFME menawarkan nilai untuk wang kerana tiada data ekonomi kesihatan dikenal pasti.
Kualiti bukti
Secara keseluruhan, kajian‐kajian yang dijalankan tidaklah besar dan kebanyakannya mempunyai masalah reka bentuk, termasuklah butiran terhad tentang bagaimana wanita dibahagikan secara rawak ke dalam beberapa kumpulan, dan laporan ukuran yang tidak tepat. Beberapa masalah telah dijangka kerana adalah mustahil untuk mengelakkan profesional kesihatan atau wanita dari mengetahui sama ada mereka (berada dalam kumpulan) bersenam atau tidak. PFME amat berbeza di antara kajian‐kajian dan sering sukar untuk dijelaskan. Kualiti bukti secara umumnya adalah rendah dan sangat rendah.
Authors' conclusions
Summary of findings
| Antenatal pelvic floor muscle training compared to control for prevention of urinary and faecal incontinence | ||||||
| Patient or population: pregnant women who were continent when randomised Setting: hospital or outpatient settings in Canada, Italy, Mexico, Norway, Spain, Thailand, Turkey, UK and USA Intervention: antenatal PFMT Comparison: control (no PFMT or usual care) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with antenatal PFMT | |||||
| Urinary incontinence in late pregnancy | Study population | RR 0.38 | 624 | ⊕⊕⊝⊝ | Upper and lower limits of the CI of summary statistic suggest clinical importance. | |
| 421 per 1000 | 160 per 1000 | |||||
| Urinary incontinence mid‐postnatal period (> 3‐6 months) | Study population | RR 0.71 | 673 | ⊕⊕⊕⊝ | Risk reduction is a clinically important effect but the upper limit of the CI is close to no effect. | |
| 251 per 1000 | 179 per 1000 | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 1.20 | 44 | ⊕⊕⊝⊝ | Wide CI including no effect. | |
| 440 per 1000 | 528 per 1000 | |||||
| Faecal incontinence in late pregnancy | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence mid‐postnatal period (> 3‐6 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Incontinence‐specific quality of life | Mean 2.66, SD 4.1 | Mean 0.24, SD 1.2 | MD 2.42 lower | 152 | ⊕⊕⊕⊝ | Measured in late postnatal period. Upper and lower limits of the CI of summary statistic suggest clinical importance in ICIQ‐SF (Nyström 2015). |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; ICIQ‐SF: International Consultation on Incontinence ‐ Short Form; MD: mean difference; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio; SD: standard deviation. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Downgraded two levels for serious inconsistency and imprecision (multiple small RCTs, fewer than 300 events, heterogeneous intervention and control groups). 2Downgraded one level for serious imprecision (multiple small RCTs, fewer than 300 events). 3Downgraded two levels for very serious imprecision (single, small trial with wide confidence interval). 4Downgraded one level for serious imprecision (single trial, fewer than 300 events). The outcome measures relate to the presence of incontinence symptoms rather than absence. Symptoms of urinary and faecal incontinence were measured based on self‐report. | ||||||
| Antenatal pelvic floor muscle training compared to control for treatment of urinary and faecal incontinence | ||||||
| Patient or population: pregnant women who were incontinent when randomised Setting: health services or obstetric clinics in Brazil, Canada, the Netherlands and Turkey Intervention: antenatal PFMT Comparison: control (usual care) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with antenatal PFMT | |||||
| Urinary incontinence in late pregnancy | Study population | RR 0.70 | 345 | ⊕⊝⊝⊝ | Wide CI including no effect. | |
| 776 per 1000 | 543 per 1000 | |||||
| Urinary incontinence mid‐postnatal period (> 3‐6 months) | Study population | RR 0.94 | 187 | ⊕⊝⊝⊝ | Wide CL including no effect. | |
| 528 per 1000 | 496 per 1000 | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.50 | 869 | ⊕⊝⊝⊝ | Wide CI including no effect. | |
| 232 per 1000 | 116 per 1000 | |||||
| Faecal incontinence in late pregnancy | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence mid‐postnatal period (> 3‐6 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Incontinence‐specific quality of life (ICIQ‐SF) | Mean 4.7, SD 5.6 | Mean 1.2, SD 2.5 | MD 3.5 lower | 41 | ⊕⊕⊝⊝ | MD suggests clinically important effect but the upper limit of the CI is close to no effect. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; ICIQ‐SF: International Consultation on Incontinence ‐ Short Form; MD: mean difference; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio; SD: standard deviation. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Downgraded three levels due to serious risk of selection bias (one trial with heavy weighting in the pooled estimate at high risk), inconsistency and indirectness, and very serious imprecision (fewer than 300 events, wide confidence interval, two trials without any details about PFMT interventions). 2Downgraded three levels due to serious risk of selection bias, indirectness and imprecision (singe trial, fewer than 300 events, wide confidence interval, no details about PFMT interventions). 3Downgraded three levels due to very serious risk of selection bias, inconsistency and imprecision (fewer than 300 events, wide confidence interval) and serious indirectness (no details about the PFMT intervention in one trial with about half the weighting in the pooled estimate). 4Downgraded two levels due to serious indirectness and imprecision (single trial, fewer than 300 participants, wide confidence interval). The outcome measures relate to the presence of incontinence symptoms rather than absence. As this comparison addresses the effect of PFMT for treatment of existing continence symptoms, the data are "negative," that is continuing incontinence rather than cure. Symptoms of urinary and faecal incontinence were measured based on self‐report. | ||||||
| Antenatal pelvic floor muscle training compared to control for mixed prevention and treatment of urinary and faecal incontinence | ||||||
| Patient or population: pregnant women some of who were incontinent symptoms and some who were not when randomised Setting: health services, obstetric clinics or hospitals in Brazil, China, France, Italy, Norway, UK or USA Intervention: antenatal PFMT Comparison: control (no PFMT, usual care or unspecified control) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with antenatal PFMT | |||||
| Urinary incontinence in late pregnancy | Study population | RR 0.74 | 3164 | ⊕⊕⊝⊝ | RR suggests clinically important effect but the upper limit of the CI suggests lack of clinical importance. | |
| 575 per 1000 | 425 per 1000 | |||||
| Urinary incontinence mid‐postnatal period (> 3‐6 months) | Study population | RR 0.73 | 1921 | ⊕⊝⊝⊝ | RR suggests clinically important effect but the upper limit of the CI suggests lack of clinical importance. | |
| 363 per 1000 | 265 per 1000 | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.85 | 244 | ⊕⊕⊝⊝ | RR suggests clinically important effect but the CI includes no effect. | |
| 448 per 1000 | 381 per 1000 | |||||
| Faecal incontinence in late pregnancy | Study population | RR 0.61 | 867 | ⊕⊕⊕⊝ | Wide CI including no effect. | |
| 43 per 1000 | 26 per 1000 | |||||
| Faecal incontinence mid‐postnatal period (> 3‐6 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Incontinence‐specific quality of life late postnatal period (> 6‐12 months) (ICIQ‐SF) | Mean 2.1, SD 3.3 | Mean 1.9, SD 3.7 | MD 0.2 lower | 190 | ⊕⊕⊝⊝ | MD and CI suggest lack of clinically important effect. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; ICIQ‐SF: International Consultation on Incontinence ‐ Short Form; MD: mean difference; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio; SD: standard deviation. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Downgraded two levels due to serious inconsistency (statistically significant heterogeneity) and indirectness (limited details about PFMT intervention in two trials with more than one‐quarter of the weighting in the pooled estimate). 2Downgraded three levels due to serious risk of selection bias (no information about random allocation concealment in three trials carrying more than 50% of weighting in the pooled estimate), serious imprecision (statistically significant heterogeneity) and serious indirectness (includes two trials carrying about 40% of the weighting in the pooled estimate with no information about PFMT intervention). 3Downgraded two levels due to serious indirectness (no information about PFMT in one trial with more than two‐thirds of the weighting in the pooled estimate) and serious imprecision (fewer than 300 event). 4Downgraded one level due to serious imprecision (single trial with fewer than 300 events). 5Downgraded two levels due to serious indirectness (single trial, no information about PFMT intervention) and serious imprecision (fewer than 300 events). The outcome measures relate to the presence of incontinence symptoms rather than absence. For those comparisons that addressed the effect of PFMT for treatment of existing continence symptoms, the data were "negative," that is continuing incontinence rather than cure. Symptoms of urinary and faecal incontinence were measured based on self‐report. | ||||||
| Postnatal pelvic floor muscle training compared to control for treatment of urinary and faecal incontinence | ||||||
| Patient or population: postnatal women who were incontinent when randomised Setting: health services or obstetric clinics in Canada, Republic of Korea, New Zealand and UK Intervention: postnatal PFMT Comparison: control (no PFMT or usual care) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with postnatal PFMT | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.55 | 696 | ⊕⊝⊝⊝ | RR suggests clinically important effect but the CI includes no effect. | |
| 724 per 1000 | 398 per 1000 | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.68 | 620 | ⊕⊝⊝⊝ | RR suggests clinically important effect but the CI includes no effect. | |
| 137 per 1000 | 93 per 1000 | |||||
| Incontinence‐specific quality of life | Mean 21.22, SD 2.11 | Mean 19.56, SD 1.88 | MD 1.66 lower | 18 | ⊕⊝⊝⊝ | Wide CI including no effect. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). BFLUTS: British Female Lower Urinary Tract Symptoms questionnaire; CI: confidence interval; MD: mean difference; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio; SD: standard deviation. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Downgraded three levels due to very serious risk of selection bias (two trials with 90% of weighting in pooled estimate at high risk) and inconsistency (statistically significant heterogeneity), and serious indirectness (two trials with 90% of weighting in pooled estimate provide insufficient information about the intervention). 2Downgraded three levels due to very serious risk of selection bias (two trials with 100% of weighting in pooled estimate at high risk), inconsistency (statistically significant heterogeneity) and imprecision (fewer than 300 events, wide confidence interval) and serious indirectness (neither trial provides sufficient information about the intervention). 3Downgraded three levels due to very serious risk of selection bias and imprecision (fewer than 300 events, wide confidence interval). The outcome measures relate to the presence of incontinence symptoms rather than absence. As this comparison addresses the effect of PFMT for treatment of existing continence symptoms, the data are "negative," that is continuing incontinence rather than cure. Symptoms of urinary and faecal incontinence were measured based on self‐report. | ||||||
| Postnatal pelvic floor muscle training compared to control for mixed prevention and treatment of urinary and faecal incontinence | ||||||
| Patient or population: postnatal women some of whom had incontinent symptoms and some of whom had not when randomised Setting: health services or hospitals in Australia, China and Switzerland Intervention: postnatal PFMT Comparison: control (no PFMT or usual care) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with postnatal PFMT | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.88 | 826 | ⊕⊝⊝⊝ | Wide CI including no effect. | |
| 294 per 1000 | 212 per 1000 | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.73 | 107 | ⊕⊝⊝⊝ | Wide CI including no effect. | |
| 54 per 1000 | 39 per 1000 | |||||
| Incontinence‐specific quality of life | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Downgraded three levels due to serious inconsistency (statistically significant heterogeneity) and imprecision (fewer than 300 events, wide confidence interval). 2Downgraded three levels due to very serious risk of selection bias and imprecision (fewer than 300 events, wide confidence interval) and serious indirectness (no information about the PFMT intervention). The outcome measures relate to the presence of incontinence symptoms rather than absence. For those comparisons that address the effect of PFMT for treatment of existing continence symptoms, the data are "negative," that is continuing incontinence rather than cure. Symptoms of urinary and faecal incontinence were measured based on self‐report. | ||||||
Background
Accumulating epidemiological evidence suggests that women who have had a baby are at increased risk of developing urinary incontinence. It seems that both pregnancy and delivery are risk factors (Foldspang 1999; Milsom 2017; Rortveit 2003a; Rortveit 2003b; Viktrup 2006). Similarly, these women seem to be at greater risk of faecal incontinence, particularly those who have had vaginal deliveries (Eason 2002; MacArthur 2001; Pollack 2004; Sultan 1999).
Description of the condition
Urinary incontinence
Urinary incontinence (involuntary leakage of urine) is a common problem amongst adults living in the community (Milsom 2017). It is more frequent in women and pregnancy or the postnatal period may be the first time many women experience urinary incontinence. Stress urinary incontinence (involuntary urine leakage with physical exertion) and urgency urinary incontinence (involuntary leakage associated with, or immediately following, a sudden compelling need to void) are the two most common types of urine leakage in women. Many women have symptoms of both stress and urgency urinary incontinence. This is called mixed urinary incontinence. Of these types, stress urinary incontinence is most commonly associated with pregnancy and the postnatal period, although there is a small but significant increase in risk of urgency urinary incontinence (Milsom 2017).
It seems that the prevalence of urinary incontinence increases during pregnancy (particularly in the second trimester) and then gradually decreases during the first postpartum year (Milsom 2017). Variation is evident in prevalence estimates of all types of urinary incontinence during pregnancy but this may be as high as 58%, with stress urinary incontinence affecting about 31% of nulliparous women and 42% of parous women (Wesnes 2007). The prevalence of persistent urinary incontinence in the first three months following delivery is approximately 30% (Thom 2010).
Findings from moderate‐ to large‐sized cohorts of women suggest that factors associated with a greater risk of postpartum urinary incontinence are:
-
parity (Milsom 2017);
-
higher maternal body mass index (BMI) (Durnea 2017; Gyhagen 2013; Pizzoferrato 2014; Quiboeuf 2016; Svare 2014);
-
age (Quiboeuf 2016);
-
urinary incontinence before or during pregnancy (Durnea 2017; Gartland 2016; Pizzoferrato 2014; Svare 2014);
-
vaginal delivery (Gartland 2016; Gyhagen 2013);
-
operative vaginal deliveries or perineal or anal sphincter trauma (Durnea 2017; Gartland 2012; Svare 2014);
-
high birthweight of the baby (Gyhagen 2013; Pizzoferrato 2014; Wesnes 2017).
These associations have been observed anywhere between four to six months' postpartum through to 12 to 20 years following first delivery (Gartland 2012; Gyhagen 2013; Pizzoferrato 2014; Wesnes 2017).
Faecal incontinence
Faecal incontinence (involuntary loss of solid or liquid stool) is less common than urinary incontinence but is particularly distressing both psychologically and physically (Johanson 1996). Women may also experience involuntary loss of flatus (wind). The term anal incontinence is used to encompass involuntary loss of faeces or flatus.
The prevalence of faecal incontinence is difficult to estimate as the definition of this condition varies between studies, different assessment tools are used and because women may be reluctant to admit to faecal incontinence (MacArthur 2013). In addition, variation is also apparent in the time points at which faecal incontinence is measured during pregnancy and following delivery and in which groups of women (e.g. primiparous versus multiparous). For the purpose of this review, faecal incontinence was considered a generic term that encompassed involuntary loss of solid stool, liquid stool, flatus, or a combination of these.
Some form of faecal incontinence may be present during pregnancy in first‐time mothers, with a prevalence anywhere up to 12% to 35% for flatal incontinence and 2.0% to 9.5% for loss of formed stool (Johannessen 2016; Svare 2016). Persistent symptoms at three months' postpartum may be 19% to 46% for flatus and 2.4% to 8.0% for the involuntary loss of formed stool (Brown 2012; Signorello 2000). In the longer term, these rates seem to persist, with about 31% of primiparous women reporting involuntary loss of flatus at six and 12 years after delivery and 9% to 12% reporting loss of formed stool (MacArthur 2013). One systematic review by Bols 2010 suggested that the aetiological factor most strongly associated with postpartum faecal incontinence is a third‐ or fourth‐degree rupture of the external anal sphincter.
Description of the intervention
Pelvic floor muscle training
Pelvic floor muscle training (PFMT) refers to the performance of repeated voluntary contractions of the pelvic floor muscles (PFM), according to a protocol that outlines the frequency, intensity and progression of exercises, as well as the duration of the training period. A PFMT programme typically includes one or more sets of exercises per day, performed on at least several days of the week, for at least eight weeks. It is recommended that initial training be followed by maintenance PFM exercises to ensure duration of effect in the longer term (Bø 2004; Mørkved 2014).
In many countries, it is common for women to receive information about, and encouragement to perform, some PFM exercises during pregnancy and after delivery. During pregnancy, information on PFMT may be received from a health professional or obtained from other sources (e.g. leaflets and websites) but this advice may not lead to effective training if the exercise parameters and behaviour are insufficient. Nevertheless, we continued to use the term PFMT to make the review easier to read.
For women who are continent during pregnancy, PFMT is undertaken to prevent leakage. Women who develop symptoms of incontinence during pregnancy or postpartum may be referred to a health professional specifically for treatment and supervision of exercise.
Prevention of urinary and faecal incontinence with PFMT
Prevention is primary, secondary or tertiary prevention (Hensrud 2000). Primary prevention aims to remove the causes of a disease. As an example, a trial that compares two obstetric practices (e.g. liberal versus restrictive episiotomy policies) and the effect on the prevalence of postnatal incontinence amongst previously continent women is a primary prevention trial. Secondary prevention aims to detect asymptomatic dysfunction and treat it early to stop progression. A trial that compares a treatment to improve the muscular supports of the bladder with no treatment in postnatal women who had weak PFM but no urinary incontinence symptoms is classified as a secondary prevention trial. Tertiary prevention is the treatment of existing symptoms to prevent progression of disease.
Clinically, it may be difficult to screen all potential trial participants to see if a disease process is either absent altogether or present but asymptomatic. In addition, with a condition such as incontinence there might be more than one factor that could contribute to development of the problem, for example denervation, fascial deficits and poor muscle function. It is impractical to screen for all possible factors and, in many cases, there are no reliable or valid clinical tests available. Consequently, prevention trials may enrol people purely on the basis of the absence of symptoms. This is commonly the case in incontinence studies and the findings of these studies are probably a combination of primary and secondary prevention effects. This review makes no attempt to distinguish between primary and secondary effects and considers them together.
Treatment of urinary and faecal incontinence with PFMT
PFMT for the treatment of urinary incontinence was popularised by Arnold Kegel (Kegel 1948). However, in one review of the literature prior to 1949, Bø 2004 identified several records of the use of PFM exercise. PFMT was principally recommended in the treatment of stress and mixed urinary incontinence but was increasingly part of treatment offered to women with urgency urinary incontinence. The use of PFMT in the treatment of urinary incontinence is based on two functions of the PFM: support of the pelvic organs and a contribution to the sphincteric closure mechanism of the urethra. More detail about how PFMT might work to treat urinary incontinence can be found in the background to a previous Cochrane review of PFMT (Dumoulin 2014).
PFMT is used in the treatment of faecal incontinence, although there are fewer studies of its effectiveness than for urinary incontinence. Theoretically, the external anal sphincter muscle (which is continuous with the puborectalis muscle component of the PFM) could be trained in a similar way and it is unclear whether it is possible for people to know the difference between a voluntary external anal sphincter contraction and a voluntary PFM contraction (Norton 2012).
PFMT is recommended as a first‐line therapy for urinary incontinence (Abrams 2017; Dumoulin 2014). However, a wide range of options is available to treat urinary and faecal incontinence, including conservative interventions (PFM rehabilitation including use of electrical stimulation and biofeedback), lifestyle interventions, bladder training, anti‐incontinence devices, pharmaceutical interventions and surgery.
How the intervention might work
There are a variety of plausible reasons why PFMT might help prevent urinary incontinence. For example, trained muscle might be less prone to injury and previously trained muscle might be easier to retrain after damage as the appropriate motor patterns are already learned. It may be that previously trained muscle has a greater reserve of strength so that injury to the muscle itself, or its nerve supply, does not cause sufficient loss of muscle function to reach the threshold where reduced urethral closure pressure results in leakage. During pregnancy, training the PFM might help to counteract the increased intra‐abdominal pressure caused by the growing fetus, the hormonally mediated reduction in urethral closure pressure, and the increased laxity of fascia and ligaments in the pelvic area. A similar rationale might be used to support the use of PFMT to improve the function of the external anal sphincter and thus prevent faecal incontinence.
Essentially, a PFMT programme may be prescribed for women to:
-
increase strength (the maximum force generated by a muscle in a single contraction);
-
increase endurance (ability to contract repetitively, or to sustain a single contraction over time);
-
co‐ordinate muscle activity (such as the precontraction of PFM prior to a rise in intra‐abdominal pressure, or to suppress urgency);
-
address a combination of these (Bø 2014).
However, based on the plausible reasons above, strength training tends to be emphasised for pregnant and postnatal women. Characteristic features of strength training include low numbers of repetitions with high loads and one way to increase load is to increase the amount of voluntary effort with each near maximal voluntary contraction (Bø 2014).
There is a subgroup of women where there are particular uncertainties about whether the intervention might work and how it might work (Hilde 2013). These are women with avulsion (separation) of the PFM from the pelvic wall or other major defects in the PFM that are palpated or seen on imaging (e.g. ultrasound, magnetic resonance imaging). It is possible that these women might benefit from PFMT after the birth, helping the injury 'heal' (Hilde 2013). However, it is also possible that PFMT does not assist the return of function if the muscle no longer has the attachments that anatomically enable it to compress and lift the urethra with a muscle contraction.
Why it is important to do this review
Urinary and faecal incontinence are experienced by many women during pregnancy and following childbirth and can have a significant impact on quality of life (Handa 2007; Rogers 2017). With the high prevalence of incontinence in pregnant and postnatal women, this is potentially a 'costly' condition. There are direct costs borne by women, such as buying continence products, laundry costs and visits to a general practitioner or continence service. Less direct but no less important costs for women may include the social or physical activity limits they adopt to prevent embarrassment of leakage in public. Preventing or treating the condition with PFMT is likely to incur considerable cost to health services because supervised (e.g. several one‐to‐one contacts with a health professional) conservative therapies such as PFMT are more expensive than usual care (Wagner 2017). However, cost‐effectiveness modelling of non‐surgical treatments for stress urinary incontinence in women found more intensive forms of PFMT were likely to be worthwhile (Imamura 2010). It is unclear if it would offer greater value for money to prevent the condition than treat it.
Although PFMT is recommended as the first choice of conservative management for incontinence, uncertainties about its effectiveness in antenatal and postnatal women remain (Dumoulin 2017), such as whether PFMT might be more effective if targeted to specific groups, or more effective as a prevention or treatment intervention. Also, with increasing pressure on constrained healthcare budgets worldwide, it is important to clarify whether the intervention offers value for money to ensure efficient allocation of resources.
This review is a major update of Boyle 2012, which examined the effectiveness of PFMT for the prevention, treatment or mixed prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women. Uncertainties identified in previous iterations of the review appear to have contributed to completion of some moderate‐ to large‐sized randomised controlled trials in this population (e.g. Fritel 2015). As several new trials have now been published with findings that could change the review outcomes, an update that was rigorous in terms of methods and analyses was required.
Since the last update of this review in 2012, other authors have published systematic reviews that address the effects of PFMT during pregnancy and after delivery for the prevention and treatment of urinary incontinence and the effects of antenatal PFMT on labour and delivery outcomes (Du 2015; Mørkved 2014).
Objectives
To determine the effectiveness of pelvic floor muscle training (PFMT) in the prevention or treatment of urinary and faecal incontinence in pregnant or postnatal women.
We wished to test the following comparisons.
-
Antenatal PFMT versus no PFMT, usual care or other control condition for the:
-
primary or secondary prevention of incontinence;
-
treatment of incontinence;
-
mixed prevention or treatment of incontinence (i.e. treating a mixed population with PFMT).
-
-
Postnatal PFMT versus no PFMT, usual care, or other control condition for the:
-
treatment of incontinence;
-
mixed prevention or treatment of incontinence.
-
Methods
Criteria for considering studies for this review
Types of studies
Randomised (including cluster and cross‐over) controlled trials and quasi‐randomised studies (e.g. allocation by alternation) were eligible for inclusion. We excluded other forms of controlled clinical trials.
Types of participants
Trials that recruited antenatal (i.e. pregnant) or postnatal women (i.e. women immediately following delivery or women with persistent urinary or faecal incontinence symptoms up to three months after their most recent delivery). Women could be with or without urinary, faecal, or both urinary and faecal incontinence symptoms at recruitment.
We compared three populations of women.
-
Prevention trials in antenatal women who were continent when randomised.
-
Treatment trials in antenatal or postnatal women who were incontinent when randomised.
-
Mixed prevention and treatment trials in antenatal or postnatal women where some women had incontinence symptoms and some did not when randomised.
Close attention was given to the distinction between treatment and prevention trials because the effect of PFMT might differ for these two purposes. For the trials that recruited antenatal or postnatal women, whether they had symptoms of incontinence or not, the PFMT intervention was a prevention strategy for the non‐symptomatic women and treatment for symptomatic women. The two effects could not be distinguished in these trials.
Types of interventions
One arm of all eligible trials included a PFMT programme to improve the function of the PFM, the external anal sphincter or both. PFMT was a programme of repeated voluntary PFM contractions, although this was a limited definition compared with the fuller ideal (Dumoulin 2014). All types of PFMT were considered, including variations in the purpose and timing of PFMT (e.g. PFMT for strengthening, PFMT for urgency suppression), ways of teaching PFMT, types of contractions (fast or sustained) and number of contractions.
Acceptable control interventions were usual antenatal and postnatal care, placebo treatment or no treatment. Usual antenatal or postnatal care in many countries included advice about PFMT. We included studies in which the control group had, or might have, received PFMT advice providing the PFMT arm was more intensive in some way than the control arm. For example, in the PFMT arm, women were taught the exercises by a health professional, whereas usual care involved distribution of a leaflet about PFMT on the postnatal wards.
Trials in which PFMT was combined with other physical therapy modalities such as biofeedback, electrical stimulation or multi‐modal exercise programmes were included. Studies where advice on strategies for symptoms of urgency and frequency (but without a scheduled voiding regimen characteristic of bladder training) were also eligible for inclusion. Trials in which PFMT was combined with another stand‐alone therapy such as bladder training or drug therapy (e.g. anticholinergic drug) were excluded. Trials of electrical stimulation (without PFMT) were excluded.
Types of outcome measures
With regards to prevention, it seemed that the most appropriate measure of outcome was the self‐reported absence of urinary or faecal incontinence symptoms. For treatment, a wider range of outcomes was considered important, although the self‐reporting of cure or improvement in urinary or faecal incontinence symptoms was thought to be most important. These outcomes are the opposite of each other, being either the presence or absence of incontinence symptoms. For consistency throughout the review, we chose to report presence of incontinence symptoms rather than absence. For the comparisons that addressed the effect of PFMT for treatment of existing continence symptoms, readers should be aware that the data were 'negative,' that is continuing incontinence rather than cure.
Primary outcomes
-
Self‐reported urinary or faecal incontinence.
-
Incontinence‐specific quality of life (e.g. International Consultation on Incontinence Questionnaire (ICIQ; 4 items, higher score worse), Incontinence Impact Questionnaire (IIQ; 30 items, higher score worse), Urogenital Distress Inventory (UDI; 19 items, higher score worse ) (Avery 2004; Avery 2007; Shumaker 1994).
Secondary outcomes
-
Women's observations:
-
severity of incontinence (e.g. Incontinence Index score, slight, moderate or severe (Sandvik 1993)).
-
-
Quantification of symptoms:
-
number of urinary or faecal incontinence episodes.
-
-
Clinician's measures:
-
loss of urine under stress test (e.g. cough or pad test).
-
-
Other quality of life and health status measures:
-
psychological measures (e.g. Hospital Anxiety and Depression Score (Zigmond 1983));
-
general health status (e.g. 36‐item Short Form (SF‐36) (Ware 1993)).
-
-
Health economics:
-
costs of intervention(s);
-
resource implications of differences in outcomes (e.g. differences in number of doctor visits, or referrals);
-
formal economic analysis (cost effectiveness, cost utility).
-
-
Adverse effects:
-
discomfort or pain associated with PFMT.
-
-
Other outcomes:
-
labour and delivery outcome (e.g. type of delivery, perineal trauma, episiotomy, length of second stage) for women who did antenatal PFMT;
-
sexual function;
-
pelvic organ prolapse;
-
non‐prespecified outcomes that were judged important when performing the review.
-
While not outcomes per se, we also extracted data on two particular variables that might help explain variations in PFMT effect:
-
PFM function (e.g. electromyography, vaginal or anal squeeze pressures);
-
Treatment adherence (e.g. surrogates such as class attendance, and more direct measures such as home exercise frequency).
Search methods for identification of studies
We imposed no restrictions on language of publication, publication status (i.e. full publication, grey literature, etc.) or any other restrictions on the searches described below.
Electronic searches
We drew on the search strategy developed for Cochrane Incontinence. We identified relevant trials from the Cochrane Incontinence Specialised Register, which is also described under the Cochrane Incontinence module in the Cochrane Library. The register contains trials identified from the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, MEDLINE In‐Process, MEDLINE Epub Ahead of Print, CINAHL, ClinicalTrials.gov, World Health Organization International Clinical Trials Registry Platform (WHO ICTRP), UK Clinical Research Network Portfolio and handsearching of journals and conference proceedings. Some of the trials in the Cochrane Incontinence Specialised Register are also contained in CENTRAL. The date of the last search was 16 February 2017.
The terms used to search the Cochrane Incontinence Specialised Register are given in Appendix 1.
Searching other resources
We searched for other possible relevant trials in the reference lists of relevant articles. We performed no tailored search for health economics studies.
Data collection and analysis
Selection of studies
Two review authors assessed all potentially eligible studies without prior consideration of the results. We resolved any disagreements by discussion and, where these were not resolved, a third review author had final responsibility. We included only randomised or quasi‐randomised controlled trials, and excluded trials that made comparisons other than those prespecified. Excluded studies are listed, with reasons for their exclusion, in the Characteristics of excluded studies.
Data extraction and management
Two review authors independently undertook data extraction onto a proforma and cross‐checked them. We resolved any differences by discussion. Where trial data were possibly collected but not reported, or data were reported in a form that could not be used in the formal comparisons, we sought further clarification from the trialists. We processed all included trial data as described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Assessment of risk of bias in included studies
Two review authors independently evaluated the methodological quality of the included trials using the 'Risk of bias' tool developed for Cochrane. We considered random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data and other bias and deemed each category at low, high or unclear risk of bias. Where there was insufficient information to make a clear decision, trials were rated at 'unclear risk.' Any disagreements were resolved by discussion.
Allocation (selection bias)
When considering random sequence bias, we assessed whether the method used to generate the allocation sequence in each study would allow an assessment of whether it produced comparable groups. We assessed the method as:
-
low risk of bias: any truly random process such as computer‐generated random number sequences;
-
high risk of bias: any non‐random process such as allocation by birth date or bed number;
-
unclear risk of bias.
For assessing allocation concealment, we determined the methods to conceal allocation to interventions prior to assignment and whether intervention allocation could have been foreseen in advance or during recruitment, or changed after assignment. We assessed the methods as:
-
low risk of bias: all forms of remote or web‐based allocation and sequentially numbered, sealed and opaque envelopes;
-
high risk of bias: open random allocation, envelopes where not all the above criteria were met (not sequentially numbered, unsealed, non‐opaque), all methods of alternation;
-
unclear risk of bias.
Blinding (performance bias and detection bias)
We did not have any criteria for performance bias as it was not considered feasible due to the nature of the intervention to blind the personnel or participants to group allocation. It is likely that this lack of blinding would unfortunately influence the results of the review.
We did not have any criteria for detection bias as it was not considered feasible to blind participants to the assessment of the two a priori outcomes of this review (prevalence of incontinence and incontinence quality of life) as both were self‐reported. We assessed blinding separately for other outcomes, such as the pad test and PFM function measures.
Incomplete outcome data (attrition bias)
For each outcome, we described the completeness of data, including attrition and exclusions from the analysis. In making a judgement about attrition bias, we considered the:
-
proportion of the total sample lost to follow‐up and the adequacy of any imputation methods used for missing data;
-
similarity in proportion of losses by group;
-
whether reasons were provided for losses and whether these differed by group;
-
if participants were analysed in the group to which they were assigned.
We assessed the methods as:
-
low risk of bias: trials with 10% or less loss to follow‐up and without a differential loss to follow‐up;
-
high risk of bias: trials with more than 20% loss to follow‐up without appropriate imputation methods or trials in which participants were not analysed in the group to which they were randomised;
-
unclear risk of bias: when the proportion of dropouts was between 10% and 20% without appropriate imputation methods (with no major differential or lack of similar reasons between groups) or when there was no reporting of losses to follow‐up.
Selective reporting (reporting bias)
For each included trial, we determined the possibility of selective outcome reporting bias and described what we found based on the following criteria:
-
low risk of bias: it was clear that all of the trial's prespecified outcomes were reported;
-
high risk of bias: not all of the trial's prespecified outcomes were reported, a primary outcome was not prespecified, outcomes of interest to the review and for which data were collected, were reported incompletely and so could not be used;
-
unclear risk of bias: a lack of detail in reporting made it difficult to assess whether all prespecified outcomes were presented.
Other bias
For each included study, we described any important concerns we had about other possible sources of bias that had not previously been considered in the categories above. In particular, we looked for a declaration of conflict of interest and the funding source. Other sources of bias were reported in the Characteristics of included studies.
Measures of treatment effect
For categorical outcomes, we related the numbers reporting an outcome to the numbers at risk in each group to derive a risk ratio (RR) and its 95% confidence interval (CI). For continuous variables, we used means and standard deviations (SD) to derive mean differences (MD). Where possible, data from different studies were pooled using a fixed‐effect model.
Some trials measured outcomes at more than one time point, usually in trials where PFMT began antenatally. There were some differences in the timing of outcome measures but, for the meta‐analysis, timing seemed to fall into the following clinical categories:
-
late pregnancy (from 20 weeks' gestation up to delivery);
-
early postnatal (zero to three months after delivery);
-
mid‐postnatal (more than three to six months after delivery);
-
late postnatal (more than six to 12 months after delivery);
-
medium term (more than one to five years after index delivery);
-
long‐term (more than five to 10 years after index delivery);
-
very long‐term (more than 10 years after index delivery).
Where a trial took measures at two time points within a single category (e.g. at eight and 12 months after delivery), we used the data from the longer time period. Few medium‐, long‐ and very long‐term data were available. Accordingly, these data were reported in text and not forest plots.
Unit of analysis issues
The primary unit of analysis was per women randomised.
For the meta‐analysis of multi‐arm studies, the data from the PFMT intervention arms were combined for comparison with the control arm. The mean and standard deviation for the combined data were calculated according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Dealing with missing data
Where possible, the trial data were analysed according to the intention‐to‐treat principle, that is by the randomised groups, and irrespective of whether women received treatment according to their randomised allocation. We did not impute missing outcome data.
Assessment of heterogeneity
The extent of heterogeneity was assessed in three ways: visual inspection of data plots, Chi² test for heterogeneity and the I² statistic (Higgins 2011). Possible explanations for the heterogeneity were sought and discussed.
Assessment of reporting biases
To minimise reporting bias, the review authors undertook a comprehensive search for eligible trials and were vigilant for duplication of data.
Data synthesis
We used the Mantel‐Haenszel methods with a fixed‐effect model approach in the meta‐analyses in this review, unless statistically significant heterogeneity (Chi² test, P < 0.10) in the comparison suggested a more conservative random‐effect model was indicated.
GRADE and 'Summary of findings' tables
We created 'Summary of findings' tables using the following outcomes:
-
urinary incontinence in late pregnancy (antenatal PFMT trials only);
-
urinary incontinence mid‐postnatal period (antenatal PFMT trials only);
-
urinary incontinence late postnatal period;
-
faecal incontinence in late pregnancy (antenatal PFMT trials only);
-
faecal incontinence mid‐postnatal period (antenatal PFMT trials only);
-
faecal incontinence late postnatal period;
-
incontinence‐specific quality of life.
For antenatal PFMT trials, we assessed the evidence in late pregnancy (postintervention effect) and the mid‐postnatal period (durability of effect postdelivery). In postnatal training trials, we assessed the evidence in the late postnatal period (sustained postintervention effect). We used the five GRADE considerations (study limitations, inconsistency of effect, imprecision, indirectness and publication bias) to assess the quality of the body of evidence as it related to the studies that contributed data to the meta‐analyses for the prespecified outcomes (Atkins 2004). We used methods and recommendations described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions using GRADEpro GDT software (GRADEpro GDT; Higgins 2011). We justified all decisions to downgrade or upgrade the quality of studies using footnotes and made comments to aid the reader's understanding of the review where necessary.
Subgroup analysis and investigation of heterogeneity
In each comparison, trials were subgrouped according to the control comparison because, a priori, we thought it plausible that the size or direction of effect would be influenced by the control condition. The four subgroups were:
-
PFMT versus no PFMT;
-
PFMT versus unspecified control (i.e. the trialist gave insufficient information about the control condition to classify it as one of the others);
-
PFMT versus usual care;
-
PFMT (more intensive, e.g. addition of biofeedback) versus PFMT (less intensive).
Sensitivity analysis
Sensitivity analysis with respect to trial quality was planned, as there is some evidence that the adequacy of randomisation (sequence generation and allocation concealment) may have an impact on the findings of a meta‐analysis (Moher 1998). However, there were insufficient trials and too many other potential causes of heterogeneity to make this useful.
Results
Description of studies
Results of the search
The flow of literature through the assessment process is shown in the PRISMA flowchart (Figure 1).
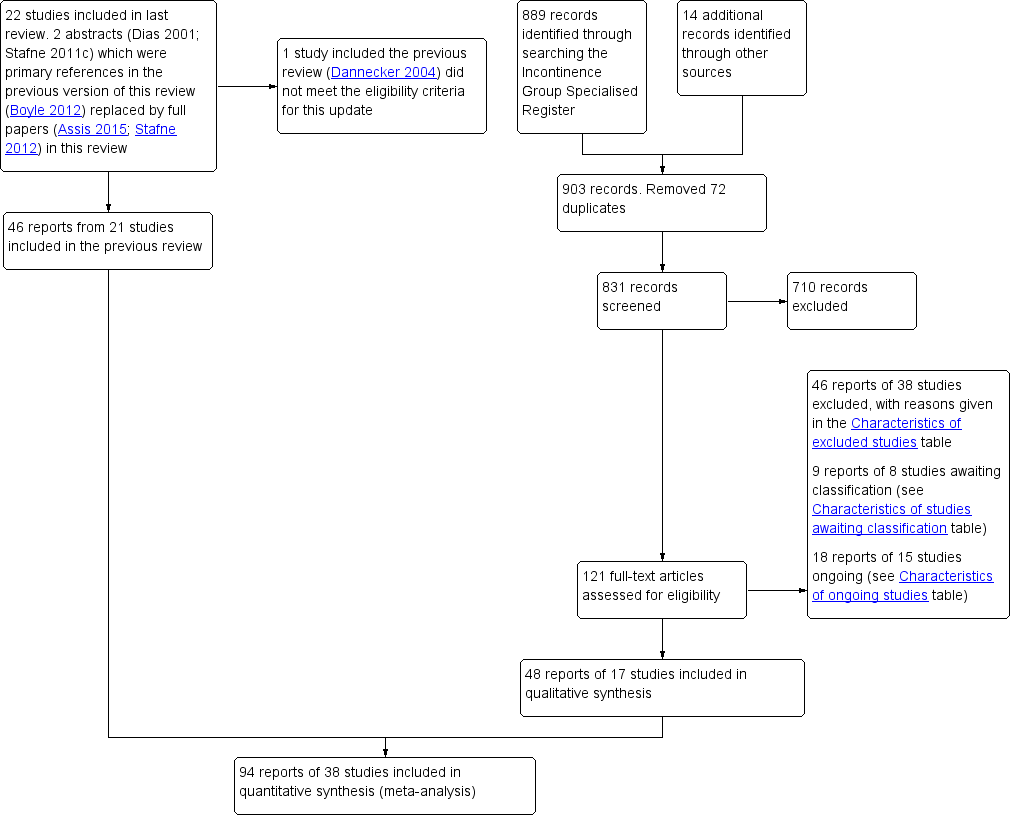
PRISMA study flow diagram.
The previous version of the review included 49 reports of 22 studies (Boyle 2012). The search update yielded 831 titles and abstracts and 121 records were obtained for further assessment. We included 48 reports from 17 new studies. The updated review now synthesises data from 94 reports of 38 studies that randomised 9892 women (4939 PFMT, 4953 controls) from 20 countries.
One trial included in the previous review did not meet the eligibility criteria for the intervention and was excluded from the update (Dannecker 2004; see Excluded studies). Forty‐six reports of 38 studies were excluded from the update and reasons are given in the Characteristics of excluded studies. In addition, 15 studies were classified as ongoing (see the Characteristics of ongoing studies) and eight require further assessment to determine eligibility (see the Characteristics of studies awaiting classification).
Three papers were published in Chinese and the data were extracted by translators for screening and further analysis (Kou 2013; Liu 2011; Wen 2010).
Included studies
The review includes 38 trials and further details are provided in the Characteristics of included studies.
-
Seven were primary or secondary prevention trials (i.e. none of the women had incontinence symptoms at the start of training) (Barakat 2011; Gaier 2010; Gorbea 2004; Kocaoz 2013; Pelaez 2014; Reilly 2002; Stothers 2002). Two trials provided subgroup data for women continent at randomisation (Mørkved 2003; Sampselle 1998). All nine investigated the effect of beginning PFMT antenatally.
-
Ten were treatment trials (i.e. all women had incontinence symptoms at the start of training). These investigated the effects of beginning PFMT antenatally and postnatally (Ahlund 2013; Cruz 2014; Dinc 2009; Dumoulin 2004; Glazener 2001; Kim 2012; Sangsawang 2016; Skelly 2004; Wilson 1998; Woldringh 2007).
-
Twenty‐one were mixed prevention or treatment trials as some women did, and others did not, have incontinence symptoms at the start of training. These trials investigated the effects of starting PFMT antenatally or postnatally (Assis 2015; Bø 2011; Chiarelli 2002; Dokmeci 2008; Ewings 2005; Fritel 2015; Frost 2014; Frumenzio 2012; Hilde 2013; Hughes 2001; Ko 2011; Kou 2013; Liu 2011; Meyer 2001; Miquelutti 2013; Mørkved 2003; Peirce 2013; Sampselle 1998; Sleep 1987; Stafne 2012; Wen 2010).
Twenty of the 38 studies were included in the previous version of this review (Assis 2015; Bø 2011; Chiarelli 2002; Dinc 2009; Dumoulin 2004; Ewings 2005; Glazener 2001; Gorbea 2004; Hughes 2001; Ko 2011; Meyer 2001; Mørkved 2003; Reilly 2002; Sampselle 1998; Skelly 2004; Sleep 1987; Stafne 2012; Stothers 2002; Wilson 1998; Woldringh 2007). Two trials were previously included in abstract form (Assis 2015; Stafne 2012).
The primary reference for eight trials was a conference abstract (Cruz 2014; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010; Hughes 2001; Skelly 2004; Stothers 2002). No further published reports were found for seven of these eight trials and one trialist kindly provided additional data from a thesis (Hughes 2001). One‐to‐one randomisation was assumed (the numbers in the intervention (139 women) and control (129 women) groups suggested this was likely) for one trial so that data could be used in the meta‐analysis (Skelly 2004).
Nineteen of the 38 included studies were publicly funded (university or national research funds or charitable trust) and one received grants from both public and private sources (Glazener 2001). Three studies did not receive any specific funding (Ahlund 2013; Barakat 2011; Kim 2012). Sixteen studies did not declare funding sources (Assis 2015; Bø 2011; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010; Gorbea 2004; Hughes 2001; Kim 2012; Kocaoz 2013; Kou 2013; Liu 2011; Pelaez 2014; Skelly 2004; Stothers 2002; Wen 2010). Fourteen trials declared no conflicts of interest (Ahlund 2013; Bø 2011; Chiarelli 2002; Dinc 2009; Dokmeci 2008; Fritel 2015; Glazener 2001; Hilde 2013; Ko 2011; Miquelutti 2013; Peirce 2013; Pelaez 2014; Sangsawang 2016; Stafne 2012). The remaining 14 trials did not report funding.
In all, 34 of the 38 trials contributed data to one or more meta‐analysis.
Settings
Women were recruited from various health services including antenatal and urology clinics, outpatient physiotherapy clinics, gynaecology and obstetric departments, and hospital settings in the following 20 countries: Australia (Chiarelli 2002), Brazil (Assis 2015; Cruz 2014; Miquelutti 2013), Canada (Dumoulin 2004; Skelly 2004; Stothers 2002), China (Ko 2011; Kou 2013; Liu 2011; Wen 2010), England (Ewings 2005; Glazener 2001; Reilly 2002; Sleep 1987), France (Fritel 2015), Ireland (Peirce 2013), Italy (Frumenzio 2012; Gaier 2010), Mexico (Gorbea 2004), Netherlands (Woldringh 2007), New Zealand (Glazener 2001; Wilson 1998), Norway (Bø 2011; Hilde 2013; Mørkved 2003; Stafne 2012), Republic of Korea (Kim 2012), Scotland (Glazener 2001), Spain (Barakat 2011; Pelaez 2014), Sweden (Ahlund 2013), Switzerland (Meyer 2001), Thailand (Sangsawang 2016), Turkey (Dinc 2009; Dokmeci 2008; Kocaoz 2013), and the US (Frost 2014; Sampselle 1998).
Sample characteristics
Parity (number of births)
Seven studies did not report parity or gravidity (Cruz 2014; Frost 2014; Frumenzio 2012; Kocaoz 2013; Skelly 2004; Stothers 2002; Wen 2010). Five of these were conference abstracts (Cruz 2014; Frost 2014; Frumenzio 2012; Skelly 2004; Stothers 2002). Trials that investigated the effects of antenatal PFMT for prevention of urinary incontinence recruited only continent women in their first pregnancy or having their first baby (or both), which trialists variously called nulliparous or primiparous women, or continent women regardless of parity (Barakat 2011; Gaier 2010; Gorbea 2004; Pelaez 2014; Reilly 2002). Trials testing antenatally for treatment of incontinence included women in their first pregnancy or nulliparae or multiparae women (Dinc 2009; Sangsawang 2016; Woldringh 2007). In trials of postnatal PFMT for treatment of urinary incontinence, all but one (Ahlund 2013, primiparous) recruited nulliparae or multiparae women (Dumoulin 2004; Glazener 2001; Kim 2012; Wilson 1998). In the mixed prevention and treatment studies investigating antenatal PFMT, most recruited women in their first pregnancy or who were having their first baby (Assis 2015; Bø 2011; Dokmeci 2008; Fritel 2015; Hughes 2001; Ko 2011; Miquelutti 2013; Mørkved 2003; Sampselle 1998). One included both nulliparae and multiparae (Stafne 2012). In the mixed prevention and treatment trials of postnatal PFMT, four included women who had just had their first baby (Hilde 2013; Liu 2011; Meyer 2001; Peirce 2013). The other three recruited mixed nulliparae and multiparae (Chiarelli 2002; Ewings 2005; Sleep 1987). In the trials with mixed parity samples, it is unknown if parity was comparable in six trials (Cruz 2014; Frumenzio 2012; Kocaoz 2013; Kou 2013; Skelly 2004; Stothers 2002). It was not comparable in one trial (Barakat 2011).
Age
Participant age was variously described, although five trials did not report this (Cruz 2014; Dokmeci 2008; Frost 2014; Peirce 2013; Skelly 2004). Three trials reported an age range, with women aged between their early 20s to early 40s (Kou 2013; Stothers 2002; Wen 2010). In two trials, about 50% to 60% of the women were aged 20 to 29 years (Chiarelli 2002; Ewings 2005). Median age was about 28 years in two trials (Hughes 2001; Reilly 2002) and 36 years in another trial (Dumoulin 2004). In the remaining 24 studies, the mean age was in the early 20s (Miquelutti 2013), mid to late 20s for 14 trials (Assis 2015; Dinc 2009; Fritel 2015; Gaier 2010; Gorbea 2004; Kocaoz 2013; Liu 2011; Meyer 2001; Mørkved 2003; Pelaez 2014; Sampselle 1998; Sangsawang 2016; Sleep 1987; Wilson 1998), and early 30s for 10 trials (Ahlund 2013; Barakat 2011; Bø 2011; Frumenzio 2012; Glazener 2001; Hilde 2013; Kim 2012; Ko 2011; Stafne 2012; Woldringh 2007). Age was comparable at baseline between groups in 29 trials but was unclear in the other nine (Cruz 2014; Dokmeci 2008; Frumenzio 2012; Kou 2013; Meyer 2001; Peirce 2013; Skelly 2004; Stothers 2002; Wen 2010).
Weight
Twenty‐two of the 38 trials reported bodyweight or BMI. For the women recruited antenatally, mean or median BMI was in the low to mid 20s (Barakat 2011; Bø 2011; Fritel 2015; Gaier 2010; Hughes 2001; Ko 2011; Miquelutti 2013; Mørkved 2003; Pelaez 2014; Reilly 2002; Sangsawang 2016; Stafne 2012; Woldringh 2007). Two trials reported that mean bodyweight in kilograms was in the mid 60s on average (Assis 2015, 67 kg; Gorbea 2004, 66 kg). About 30% of women had a BMI in the overweight or obese range in one trial that recruited women antenatally and in two that recruited women on postnatal wards (Chiarelli 2002; Ewings 2005; Kocaoz 2013). In three trials that recruited postnatal women with persistent incontinence symptoms, the mean or median BMI was in the normal range (Ahlund 2013; Dumoulin 2004; Kim 2012). BMI was about 26 kg/m² in one mixed treatment and prevention study which recruited women postnatally (Hilde 2013). BMI or bodyweight was comparable at baseline between groups for all of these trials, although two trials noted that weight gain in pregnancy differed significantly between the groups, being greater in either the PFMT group or in the control group (Barakat 2011; Gorbea 2004).
Type of delivery
Some details on delivery were given by 11 of 15 trials that began PFMT after delivery. In eight of these trials, all women delivered vaginally (Chiarelli 2002; Frost 2014; Hilde 2013; Kim 2012; Liu 2011; Peirce 2013; Sleep 1987; Wen 2010). In the study by Chiarelli 2002, all women had a forceps or ventouse delivery, while Peirce 2013 reported that about 39% of women had an instrumental delivery. The types of delivery appeared comparable across the PFMT and control groups in both trials. In the trials by Glazener 2001 and Wilson 1998, some women had a caesarean section (about 8% in Glazener 2001 and 18% in Wilson 1998) with the proportion of caesarean sections being similar in both the PFMT and control groups for both trials. Glazener 2001 also reported that about 14% of women in both the PFMT and control groups had assisted vaginal deliveries. In the remaining small trial by Meyer 2001, it was unclear if all 107 women delivered vaginally but it was reported that 30% of PFMT group and 16% of control group women had forceps delivery; this difference was not "statistically significant" (P = 0.10).
For the trials in which PFMT began antenatally, it is possible that the type of delivery was affected by PFMT. For these trials, the type of delivery was a possible confounder of the postnatal incontinence outcome but may itself be an outcome of importance. A short summary of the data is given here. The data are also reported in more detail in the analysis. Some details on the type of delivery, by group, were given by only 13 of the 23 trials in which PFMT began antenatally. In 11 trials, the delivery type was similar across both comparison groups (Barakat 2011; Fritel 2015; Frost 2014; Hughes 2001; Ko 2011; Miquelutti 2013; Mørkved 2003; Reilly 2002; Sampselle 1998; Stothers 2002; Woldringh 2007). However, in two trials, there seemed to be fewer vaginal deliveries in the PFMT group (Dinc 2009; Gorbea 2004). Miquelutti 2013 reported a "statistically significantly" longer duration of delivery in the PFMT group (MD 9.48, 95% CI 0.32 to 18.64; P < 0.05).
Exclusion criteria
The most common exclusion criterion (in 27 trials) was a comorbidity that contraindicated exercise in pregnancy or made PFMT difficult (or both), or might have altered the outcome of training, such as serious medical or neuromuscular conditions. Ten trials excluded women with high‐risk pregnancies (Bø 2011; Dokmeci 2008; Fritel 2015; Gorbea 2004; Ko 2011; Meyer 2001; Miquelutti 2013; Mørkved 2003; Sangsawang 2016; Stafne 2012). Sixteen trials included women with singleton pregnancies or excluded women with twins, or other multiple pregnancies or births (Ahlund 2013; Barakat 2011; Bø 2011; Cruz 2014; Fritel 2015; Gorbea 2004; Hilde 2013; Liu 2011; Meyer 2001; Miquelutti 2013; Mørkved 2003; Pelaez 2014; Sangsawang 2016; Stafne 2012; Stothers 2002; Wen 2010). Eight excluded women if the baby was stillborn or was very ill or died after birth (Chiarelli 2002; Ewings 2005; Glazener 2001; Hilde 2013; Mørkved 2003; Peirce 2013; Sleep 1987; Stafne 2012). Five excluded women if language difficulties meant it was difficult to seek informed consent (Chiarelli 2002; Dumoulin 2004; Ewings 2005; Peirce 2013; Woldringh 2007). An additional six outlined language requirements as part of their inclusion criteria (Bø 2011; Cruz 2014; Fritel 2015; Hilde 2013; Peirce 2013; Pelaez 2014). Four trials specifically excluded women who experienced pain with a PFM contraction (Dinc 2009; Ko 2011; Mørkved 2003; Sangsawang 2016).
Pelvic floor muscle training regimens and control interventions
The PFMT and control interventions are described in the Characteristics of included studies (overview) and in Table 1 (details of exercise parameters and adherence).
| Study ID | Voluntary pelvic floor muscle contraction confirmed? | PFMT parameters | PFMT supervision | Control comparison | Adherence | Notes |
| (treatment trial) | Vaginal palpation performed by study midwife: after randomisation and at each of the 3 visits to midwife (PFMT and control groups). | PFMT started with 3 fast contractions, followed by 3 sets of 8‐12 slow velocity, near maximal contractions, 6‐sec hold; 7 days per week for 6 months. Received written instructions on PFMT, but no information provided on PFMT progression. | Visit to the study midwife every 6th week (3 times during study period). | Usual care: written information describing PFM anatomy and PFMT. Received instructions on how to correctly perform PFM contraction (vaginal palpation) from midwife. | Women in the PFMT group were asked at each midwife visit how often they did PFMT; results not reported. | PFMT in lying or sitting positions. |
| (prevention trial) | Perineometry (at 1st meeting), but unclear by whom (PFMT group). | 5‐10 slow PFM contractions with 6‐sec hold, rest 6 sec between contractions with 3 rapid contractions at the end (as per Mørkved 2003). Daily PFMT in 4 positions, and 1 group (27 women) had 5 supervised sessions with a physiotherapist. Received manual of home PFMT exercises and asked to complete an exercise diary. | Supervised PFMT (27 women): received up to 5 monthly supervised exercise sessions with physiotherapist (22, 26, 30, 34, 38 weeks' gestation). Unsupervised PFMT (27 women): trained to perform PFMT by physiotherapist (1 session). | Did not receive intervention and did not exercise. | Not reported, although it stated that no dropouts occurred throughout the duration of the study due to all women in the PFMT group complying with the exercise protocol. | PFMT in a variety of positions including left side lying, sitting, reclined sitting, sitting with legs crossed, standing. Translation (Portuguese). |
| (prevention trial) | Not reported. | PFMT included in the 7‐ to 8‐min cool‐down period as part of a 35‐ to 45‐min exercise session, 3 days per week for duration of pregnancy (potential mean of 85 sessions in total). No specific details provided about PFMT programme. | Group exercise classes, supervised by a qualified fitness specialist, with the assistance of an obstetrician. | Not reported. | Adherence to PFMT was 90%. | General exercises targeted major muscles of arms and abdomen to promote good posture and prevent low back pain, and in the 3rd trimester strengthen the muscles of labour and PF. 1 session of aerobic dance per week. Accompanied by music. |
| (mixed prevention and treatment trial) | Participants did not have individual assessment of correct voluntary PFM contraction (due to pragmatic nature of study). Instructors were trained in how to explain a correct PFM contraction. | PFMT included as part of 15‐min strength training session within a 60‐min group exercise class. PFMT: 3 sets of 8‐12 maximal contractions, 6‐ to 8‐sec hold; strong verbal motivation to perform close to maximum PFM contractions. Women encouraged to participate in at least 2 out of 3 fitness classes per week for 12 weeks. Daily PFMT at home: 3 sets of 8‐12 close to maximum PFM contractions. Also encouraged to be physically active for at least 30 min per day. Received a specific PFMT brochure. | Group exercise classes, 2 or 3 per week for 12 weeks, led by certified aerobic instructors. Instructors were taught by a physiotherapist with > 20 years of experience in assessing, treating and researching women with PF dysfunction. | Usual antenatal care. | Mean adherence to exercise classes was 17.2 out of a possible 24 sessions. 40% (21/52) of women attended at least 80% of sessions. | PFMT integrated into aerobic dance class (accompanied by music): 5‐min warm‐up; 30‐min low‐impact aerobics; 15‐min strength training (including PFMT); 5‐min stretching and relaxation. PFMT in a variety of position including sitting, kneeling and standing. Informed of deep abdominal muscle co‐contraction during maximal PFM contraction. |
| (mixed prevention and treatment trial) | Visual inspection of perineum (PFMT group). | Maximum of 6 voluntary PFM contractions per set; 3‐6 sec hold; 3 sets per day; for 8 weeks. | PFMT taught 1‐to‐1 with physiotherapist. 1 (20 min) contact in hospital, and another (30 min) 8 weeks later at home or hospital. | Routine postnatal care; usual postnatal leaflet given; invitation to join postnatal class on ward; no restriction on PFMT if recommended by other health professional. | 84% (292/348) of women in the PFMT group and 58% (189/328) of controls were performing PFMT at "adequate" level at 3 months' postpartum. | Women were "asked if they were performing their PF exercises." |
| (treatment trial) | Not reported. | 5‐6 biweekly sessions. No specific details provided about PFMT. | Supervised by a physiotherapist. | Similar unsupervised PFMT at home. | Not reported. | Conference abstract. |
| (treatment trial) | Vaginal digital palpation (both PFMT and control groups). | Progressive PFMT programme. Level 1: 3 sets of 10 near maximal contractions; 3‐sec hold, 3‐sec rest; quick contraction, 1‐sec hold, 1‐sec rest; twice daily. Level 2: 3 sets of 10 near maximal contractions; 5‐sec hold, 5‐sec rest; quick contraction, 2‐sec hold, 2‐sec rest; twice daily. Level 3: 3 sets of 15 near maximal contractions; 10‐sec hold, 10‐sec rest; quick contraction, 2‐sec hold, 2‐sec rest; 3 per day. | Trained by a researcher on how to do PFMT in accordance with booklet of PFM exercises. | Usual care: instructed on how to perform a correct PFM contraction, but did not receive training about exercises. | Not reported. | In 2nd stage of study, 68% of women in study group were contracting the proper muscle group. The rest were given more training and reassessed 1 week later. |
| (mixed prevention and treatment trial) | Not reported. | Not reported. | Not reported. | Not reported. | Not reported. | Conference abstract. |
| (treatment trial) | Not reported. | 8‐12 close to maximal voluntary PFM contraction per set; 6‐ to 8‐sec hold each with 3‐4 fast contractions at the end of each contraction; 6‐sec rest between contractions; 3 sets per day; 5 days per week; for 8 weeks. Also taught 'the knack' (voluntary PFM contraction prior to hard cough and maintained through cough until abdominal wall relaxed). | PFMT taught 1‐to‐1 with physiotherapist. | Same number of physiotherapy contacts for relaxation massage of back and extremities; asked not to do PFMT at home. | Not reported. | In addition to PFMT 15 min of electrical stimulation (biphasic rectangular form, 50 Hz, pulse width 250 msec, duty cycle 6 sec on and 18 sec off for 1st 4 weeks, then 8 sec on and 24 sec off for next 4 weeks, at maximal tolerated current intensity) and 25 min of electromyographic biofeedback per appointment. |
| (mixed prevention and treatment trial) | Not reported. | 6 months. | PFMT taught 1‐to‐1 with physiotherapist in hospital. | Standard care including verbal promotion of PFMT and leaflet on PFMT. | Of 117 women in the PFMT group, 114 were visited by the physiotherapist in hospital, 21 attended the 2‐month PFMT group, and 5 attended the 4‐month group. | ‐ |
| (mixed prevention and treatment trial) | Vaginal digital palpation at each session (possibly by physiotherapist, but not stated; PFMT group). | 1 session per week (20‐30 min), total of 8 sessions between 6th and 8th month of pregnancy. Also 'the knack' (voluntary PFM contraction prior to increasing intra‐abdominal pressure). Provided with written information on PF anatomy and PFMT, and encouraged to perform daily PFMT at home, 10‐20 contractions. | Individually supervised by a physiotherapist or midwife at each session. In total, 37 different therapists (all trained by the same specialist physiotherapist) were involved in delivering the exercises. | Usual care, including written information on PF anatomy and PFMT (encouraged to perform daily at home, 10‐20 PFM contractions). | 69.3% (97/140) of women in the PFMT group completed all planned sessions, and 82.8% (116/140) completed at least 1 session (4‐8, median 8). At the end of pregnancy, women in both groups reported a similar frequency and duration of PFMT (including number of contractions). PFMT was performed daily at home by 4.3% (6/140) of PFMT women and 10.6% (15/142) of controls, at the end of pregnancy. | PFMT performed in standing (5 min) and lying (10 min). |
| (mixed prevention and treatment trial) | Not reported. | Standard postpartum discharge instructions plus written and verbal instructions for PFMT. | Not reported. | Standard postpartum discharge instructions. | Not reported. | Conference abstract. |
| (mixed prevention and treatment trial) | Not reported. | 2 weekly session of Kegel exercises; 8 weeks. Daily home exercises (20 min) and stretching. | Not reported. | Did not receive any PFMT, no other details provided. | Not reported. | Conference abstract. |
| (prevention trial) | Not reported. | 12‐week PFMT programme. | PFMT supervised by a physiotherapist and midwife. | Routine care and PFM exercises, customary instruction at intake visit. | Not reported. | Conference abstract. |
| (treatment trial) | Not reported. | 8‐10 sessions of fast and slow voluntary PFM contraction per day with aim of 80‐100 per day; for up to 8 months. | PFMT taught 1‐to‐1 with nurse, health visitor or continence advisor. | Usual antenatal and postnatal care that may have included advice on PFMT. | 78% (218/278) of women in the PFMT group and 48% (118/244) of controls had done some PFMT in the 11th postnatal month. Mean (SD) number of voluntary PFM contractions per day at 12 months' postnatal: PFMT group 20 (29) and controls 5 (15). | Frequency and urgency strategies added if needed at 7 or 9 months postnatally. 52.7% (394/747) of women at 6 years' follow‐up and 70.1% (471/672) of women at 12 years' follow‐up completed a questionnaire. About 50% of women in PFMT and control groups were performing any PFMT at both time points. Daily PFMT was undertaken by 6% (17/263) of PFMT women compared to 12% (29/253) of control women at 6 years; and 7% (15/227) of PFMT group compared to 8% (20/241) of control women at 12 years. |
| (prevention trial) | Surface electromyography (electrodes either side of anus; PFMT group). | 10 voluntary PFM contraction; 8‐sec hold followed by 3 fast, 1‐sec contractions; 6‐sec rest between contractions; for up to 20 weeks. Asked to complete an exercise diary. | PFMT taught 1‐to‐1 with physiotherapist. | Requested not to do PFMT during pregnancy or postnatally. | 63% attended all 8 physiotherapy appointments, 21% attended 7 appointments. | Electromyographic biofeedback at each appointment. |
| (mixed prevention and treatment trial) | Vaginal digital palpation (PFMT and control groups). | Progressive supervised PFM training programme (as per Mørkved 1997) for 16 weeks. Daily PFMT at home, 3 sets of 8‐12 close to maximal contractions. Customary written information on discharge from postnatal ward. Asked to complete an exercise diary. | Supervised exercise class from 6 weeks' postpartum, led by an experienced physiotherapist, once per week for 16 weeks. Class attendance was documented. | Usual care. Received customary written information on discharge from postnatal ward. At 6 weeks were instructed on how to perform a correct PFM contraction (verified with vaginal digital palpation). | 96% (72/75) of women in the PFMT group who completed the trial adhered to 80% of the class and daily home training. In the control group (retrospective questioning), 16.5% reported performing daily PFMT at home ≥ 3 times per week. | 4% (7/175) of women were unable to perform a voluntary PFM contraction at baseline. At baseline (6 weeks' postpartum) more women in the control group were performing PFMT ≥ 3 times or more per week. |
| (mixed prevention and treatment trial) | Vaginal digital palpation (PFMT and control groups). | Daily; for up to 11 months. | 1 individual session with physiotherapist, and 1 group PFMT session led by physiotherapist at 22‐25 weeks' gestation with maximum of 6 women per group. | Usual antenatal and postnatal care that may have included advice on PFMT (personal communication). | 79% (461/586) of women in PFMT group attended group PFMT session (personal communication). | 3.5% (16/460) of women who attended group PFMT session could not perform a voluntary PFM contraction after teaching, and 2.8% (13/460) of women could contract but not sustain a contraction (personal communication). Conference abstract. |
| (treatment trial) | Perineometer (vaginal probe) used to ensure PFM contraction and assess control of contraction in both PFMT and control groups. Unclear if this was performed every session with the PFMT women. | 20 maximal voluntary PFM contractions, 10‐sec hold, 3 times per week; for 8 weeks (as part of a class), and daily at home. Progressed by changing position (prone, sitting and standing). Initial session included information on PFM anatomy and function. Also provided with a booklet which included a training programme and an exercise diary. | Supervised training sessions (1‐hour duration) with a specialist physiotherapist (23 in total, unclear if individual contacts or group classes). | Usual care. Received the same information and demonstration session as PFMT group and instructions on how to correctly perform PFM contraction (perineometer). Unsupervised, daily PFMT for 8 weeks. | Not reported. | PFMT integrated with trunk stabilisation exercises (progressive abdominal strengthening, bridging, and side‐bridge). |
| (mixed prevention and treatment trial) | Observation of inward movement of perineum during contraction (PFMT group). | 3 repetitions of 8 PFM contractions, 6‐sec hold each, 2‐min rest between repetitions; repeated twice daily at home with additional training in groups once per week for 45 min for 12 weeks. Asked to complete an exercise diary. | Group training sessions (10 women) supervised by a physiotherapist once per week for 12 weeks. | Regular antenatal care and the customary written postpartum instructions that did not include PFMT from the hospital. Not discouraged from performing PFMT on their own. | > 80% attended every training session and 0 were absent more than twice. At 35 gestational weeks, 87% of PFMT group reported practice of PFMT ≥ 75% of the time. | Group training was performed in sitting and standing positions with legs apart to emphasise specific strength training of the PFM and relaxation of other muscles. |
| (prevention trial) | Observation of inward movement of perineum or digital vaginal palpation, or both (PFMT group). Vaginal digital palpation used to teach PFM contraction in 23.5% (16/68) of women. | 3 sets of 10 maximal voluntary PFM contractions at level 3 (2‐sec hold, 2‐sec rest for strength; 10‐sec hold, 10‐sec rest for endurance); 3 sessions per day during pregnancy and postpartum. Women received education about the anatomy and functions of the PFM and PFMT (unclear from whom) and were asked to complete an exercise diary (including progressions). | Exercise compliance was checked at every hospital visit (9‐10 visits on average, over a minimum of 12 weeks), and pregnant women were called once per month to encourage regular exercise. | Not instructed to do PFMT. Once data collection complete, controls received PFMT and a brochure with the relevant information during the 12th week home visit. | Women asked to record the number of times they did their exercises. No data reported. | Digital vaginal palpation was refused by 52/68 women due to concerns about pregnancy, cultural/religious reasons. Unclear if women progressed through levels 1‐3 or started at level 3, whether they did 3 sets of 10 exercises per day or 3 sets of 10 exercises 3 times per day, or how the sets were divided between endurance and strength training. |
| (mixed prevention and treatment trial) | Not reported. | PFM (Kegel) exercises undertaken 2‐3 times per day for 20‐30 min or 150‐200 contractions (3‐sec hold then relax), performed until 12 months' postpartum. Biofeedback used twice per week (no further details available). | Not reported who supervised the programme, or the number and type of contacts with health professional(s). | Usual care: received standard postpartum information. | Not reported. | Translation (Chinese). |
| (mixed prevention and treatment trial) | Not reported. | PFMT 2‐3 times per day, 15‐30 min each set (4‐ to 6‐sec hold, 10‐sec relaxation), started after birth and continued for ≥ 10 weeks. | Exercises taught by experienced midwives who also supervised the programme (number and type of contacts/visits unclear). | Usual care: standard postpartum information. Unclear if this included PFMT. | Not reported. | Translation (Chinese). Positions of exercises included supine, sitting or any other position, with legs slightly separated, with instructions to contract anus, vaginal and urinary tract while breathing in, and to relax with expiration. |
| (mixed prevention and treatment trial) | Not reported. | Up to 8 months; no details of PFMT provided. Each clinic session was followed by 20 min of biofeedback and 15 min of electrical stimulation. | 12 sessions (6 weeks) with a physiotherapist between 2 and 10 months postnatally. | No intervention. Women received PFMT education after 3rd assessment at 10 months' postpartum. | Not reported. | In addition to PFMT, 20 min of biofeedback and 15 min of electrical stimulation (vaginal electrode, biphasic rectangular waveform, pulse width 200‐400 msec, frequency 50 Hz, intensity 15‐15 mA, contraction time 6 sec, rest time 12 sec) per appointment. |
| (mixed prevention and treatment trial) | Instructed on correct contraction, but not verified (due to pragmatic nature of study). | PFMT (maximal rapid and sustained PFM contractions) performed as part of a class (50 min) for a median of 5 (range 2‐10) sessions between 18‐24 weeks' to 36‐38 weeks' gestation. Provided with an exercise guide and asked to do daily PFMT at home (30 rapid, 20 sustained (10‐sec hold) contractions), as well as 30‐min daily aerobic exercise (no specific examples provided). Received standard antenatal education and asked to complete an exercise diary. | Supervised by a trained study physiotherapists on a monthly basis. Either group or individual training sessions, depending on the number of women present. | Usual care: received standard antenatal and postnatal education (on labour, breastfeeding and pain relief) by trained physiotherapy, nursing and medial staff. | Analysis of adherence in intervention group was not possible as women failed to complete or return their exercise diaries. | PFMT performed in standing and sitting position. PFMT integrated into non‐aerobic exercise programme designed to reduce back pain. Included abdominal, stretching and relaxation exercises and exercises designed to promote venous return. |
| (mixed prevention and treatment) | Vaginal digital palpation and observation of perineum (both PFMT and control groups). | 8‐12 near maximal voluntary PFM contractions; 6‐ to 8‐sec hold each, 3‐4 fast contractions at the end of each contraction; 6‐sec rest between contractions; twice daily at home; for ≤ 8 months. Also asked to attend weekly 60‐min PFMT class for 12 weeks. Women asked to complete an exercise diary. | Group training session (10‐15 women), once per week for 12 weeks, supervised by physiotherapists (5 in total). | Usual antenatal and postnatal care that may have included advice on PFMT. Correct PFM contraction verified. Not discouraged from doing PFMT on their own. | 19% (28/148) of PFMT women attended less than half the 12 weekly PFMT classes and did not return training diaries. | During exercise class voluntary PFM contraction undertaken in a range of body positions (lying, sitting, kneeling and standing with legs apart). PFMT interspersed with abdominal, back and thigh muscle exercises (accompanied by music). 62% (188/280) of women completed a questionnaire at 6‐year follow‐up, and 45% of women in both the former PFMT and control groups were doing PFMT at least weekly. |
| (mixed prevention and treatment trial) | Contraction assessed with anal biofeedback as part of training session (by obstetrician or specialist nurse); PFMT group. | Sets of 10 PFM contractions (Kegel exercises), 5‐sec hold; 10‐sec rest between contractions; twice daily for 5 min with biofeedback; for 3 months. Standard postpartum education by midwives or physiotherapists, including written information. Women asked to complete an exercise diary. | Biofeedback (electromyographic) training provided at initial session, but no further contact with health professionals. | Usual care: "conventional PFM training," but no details provided. Women asked to complete an exercise diary. | Poor adherence defined as performing < 70% of the intended home exercise sessions. 7/30 women in the PFMT group reported poor adherence. | The portable biofeedback machines were programmed to the electromyography setting with the work period set to 10 contractions (5‐sec duration) with a 10‐sec rest between each contraction. PFMT for treatment of FI. |
| (prevention trial) | Instructed on correct contraction, but not formally verified. Women were asked to test themselves at home by stopping the flow of urine, digital palpation or using a mirror to observe the perineum (PFMT group). | PFMT programme, 3 times per week; for ≥ 22 weeks. Started with 1 set of 8 contractions increasing to 100; divided into different sets of slow (6 sec) and fast (5 as fast as possible) contractions. Unclear if this progression related to class or home exercises. Daily PFMT at home, 100 contractions in different sets. Received standard antenatal education about PFM. | Group training sessions (8‐12 women) designed and supervised by a physical activity and sport sciences graduate; 55‐ to 60‐min duration (10 min of PFMT); 70‐78 sessions in total. | Usual care: follow‐up by midwives, standard information about PFMT. Women were not asked not to do PFMT. | All women included in analysis attended ≥ 80% of exercise sessions. | PFMT integrated into supervised exercise programme; 30 min low‐impact aerobics including general strength training, PFMT and cool down (stretching, relaxation or massage); sometimes accompanied by music. PFMT in a variety of positions. Women wore heart rate monitors to control exercise intensity. |
| (prevention trial) | Unclear, but seems likely as physiotherapists gave individualised programmes to those unable to follow exercise regimen due to inability to do voluntary PFM contraction (PFMT group). | 8‐12 voluntary PFM contractions; 6‐sec hold each; 2‐min rest between each set of contractions; 3 sets of 8‐12 contractions twice daily; for about 20 weeks (as described by Bø 1995). | About 5 (monthly) contacts with physiotherapist between 20 weeks' gestation and delivery. | Usual antenatal and postnatal care that may have included advice on PFMT. Women appeared to have had same number of clinic visits as the PFMT group, and were asked if doing PFMT at each of these visits. | 43% (52/120) of women in the PFMT group did not return an exercise diary; 11% (13/120) completed < 28 days of PFMT; and 46% (55/120) completed ≥ 28 days. When asked postnatally, 28% (33/120) of PFMT women and 34% (37/110) of controls were doing occasional or no PFMT. | If unable to follow PFMT regimen then individualised programme until able to do so. 71% (164/230) of women completed a telephone questionnaire at 8‐year follow‐up, and 68.4% of women were doing PFMT, with 38% stating they were doing PFMT twice or more per week. |
| (mixed prevention and treatment trial) | Yes, but unclear how or by whom (PFMT group). | PFMT tailored to individual ability. 30 maximal or near maximal voluntary PFM contraction per day; for ≤ 17 months. | Not reported. | Usual antenatal and postnatal care; no systematic PFMT programme. | At 35 weeks' gestation, 85% of women in the PFMT group reported to be doing PFMT 75% of the time. At 1 year, PFMT adherence reported to vary between 62% and 90%. | ‐ |
| (treatment trial) | Assessed by ability to stop or slow the flow of urine for 1‐2 sec (PFMT group). | 20 sets of PFM exercises, twice daily, at least 5 days per week, for 6 weeks. 1 set of PFM exercises was 1 slow contraction (10‐sec hold), followed by 10 fast contractions; no progression in number of contractions per set. Also received a handbook with information on stress UI, PFM function, instructions on PFMT and a urinary diary. | Supervised group sessions (4‐5 women) with a midwife; 45 min; once every 2 weeks for 6 weeks (3 sessions in total). | Usual care: from health professionals, obstetricians or midwives. Did not receive information about UI and received no training support about performing correct PFM exercises. | No women were excluded for failing to perform the PFMT for < 28 (of approximately 42) days. | PFMT performed in various positions including lying down, sitting and standing. |
| (treatment trial) | Not reported. | Not reported. | "One to one teaching about pelvic floor exercises." | "Conventional care (hand‐out information about pelvic muscle exercises)." | Not reported. | Conference abstract. |
| (mixed prevention and treatment trial) | Not reported. | As for controls with additional section in leaflet recommending a specific exercise each week that integrated voluntary PFM contraction with usual activities of daily living; up to 3 months. Asked to complete a daily exercise diary for 4 weeks. | 1‐to‐1 session with midwife co‐ordinator each postnatal day in hospital. | Usual antenatal and postnatal care including PFMT leaflet; might include PFMT at antenatal class or postnatal class on ward (or both); instructed to do voluntary PFM contraction as often as remembered and mid‐stream urine stop. | At 10 days postnatally, 78% of PFMT group and 68% of controls were doing some PFMT; with 58% of PFMT group and 42% of controls doing some PFMT at 3 months. | ‐ |
| (mixed prevention and treatment trial) | Vaginal digital palpation (PFMT group). | 8‐12 near maximal voluntary PFM contractions; 6‐ to 8‐sec hold each with 3 fast contractions at the end of each contraction. Asked to perform PFM exercises as part of a 45‐min home programme at least twice per week or a weekly 60‐min exercise class (or both). Received written information including brochure with an evidence‐based PFMT programme, and asked to complete an exercise diary. | Group training sessions (8‐15 women) supervised by physiotherapist, 60 min, once per week for 12 weeks | Usual care: received customary information from midwife or GP. Also given a detailed information brochure including evidence‐based PFMT programme. Women were not discouraged from exercising. | Adherence to the general exercise protocol (exercising ≥ 3 days per week, moderate to high intensity) was 55% (217/397) in the PFMT group and 10% (36/365) in the control group. 67% of the PFMT group performed PFMT ≥ 3 times per week compared to 40% in the control group | PFMT integrated into standardised exercise programme: 30‐ to 35‐min low‐impact aerobics; 20‐ to 25‐min strengthening exercises (including PFMT, 3 sets of 10 reps); 5‐ to 10‐min stretching and relaxation. PFMT performed in a variety of positions, with legs apart to emphasise specific strengthening of the PFM. |
| (prevention trial) | Not reported. | 12 contractions, 3 times daily. | Seen twice monthly throughout pregnancy, and every 3 months postnatally for 1 year. | "Other (placebo) including no pelvic floor exercises." | Not reported. | Conference abstract. |
| (mixed prevention and treatment trial) | Assessment of PFM strength and contraction by an obstetrician (PFMT group; no further details) | Anal contraction; 3‐sec hold (while inhaling) followed by relaxation with 3‐5 faster contractions at the end of each contraction; 15‐30 min each set; twice daily; 6‐8 weeks. | Exercises taught by experienced midwives but unclear who supervised the programme of the number and type of contacts/visits. | Usual care: no other details provided other than "conventional guidance." | Not reported. | PFMT performed in a variety of positions including lying down, sitting or standing. Translation (Chinese). |
| (treatment trial) | Not reported. | Mix of fast and slow voluntary PFM contractions 8‐10 times per day with aim of 80‐100 voluntary PFM contraction daily; up to 9 months. | 1‐to‐1 sessions with physiotherapist at 3, 4, 6 and 9 months postnatally. | Usual PFMT as taught in antenatal and postnatal classes. | Mean (95% CI) number of daily voluntary PFM contraction at 12 months' postnatally was 86 (69‐104) in the PFMT group and 35 (30 to 40) in the control group. | Perineometry for biofeedback at each appointment. Mean time to teach PFMT to the PFMT group was 32 (95% CI 30 to 34) min. |
| Observation and palpation of perineal body by physiotherapists. Women also encouraged to practice self‐palpation (PFMT group). | Not reported. At each visit, women were asked about the frequency and duration of PFMT. | 1‐to‐1 30‐min sessions with physiotherapist. 4 in total: 3 antenatally and 1 at 6 weeks postnatally. In total, 25 physiotherapists (specialised in PFMT) were involved in delivering the exercises. | Usual antenatal and postnatal care including advice on PFMT; nearly two‐thirds received some instruction on PFMT. | At 35 weeks' gestation, 6% reported no PFMT, 17% reported some PFMT, 40% were doing PFMT at low intensity and 37% were exercising intensively in the PFMT group vs 36% reported no PFMT, 25% reported some PFMT, 26% were doing PFMT at low intensity and 14% were exercising intensively in the control group. | ‐ |
CI: confidence interval; FI: faecal incontinence; min: minute; PF: pelvic floor; PFM: pelvic floor muscle; PFMT: pelvic floor muscle training; SD: standard deviation; sec: second; UI: urinary incontinence.
First, the PFMT programmes were classified by their possible physiological effect(s) (strength, endurance, co‐ordination or a combination), based on the described exercise parameters. Second, the amount of contact or supervision from health professionals (low fewer than five contacts; moderate six to 12 contacts; high more than 12 contacts), confirmation of a correct PFM contraction and nature of the control interventions were examined. Third, adherence data were considered to assess whether exercise behaviour was likely to support a physiological effect. Trials were classified according to whether they provided data for both the intervention and control groups, the intervention group only or neither group. The likely impact of the exercise programmes on PFM function and the clinical difference between the intervention and control conditions are considered in the Discussion.
We categorised 11 trials as providing strength training and six as probably strength training trials, 17 in all.
-
Eleven trials clearly provided exercise parameters that favoured strength training; short duration contractions of maximal or near maximal effort and a relatively small number of repetitions (Ahlund 2013; Bø 2011; Dinc 2009; Dumoulin 2004; Hilde 2013; Kim 2012; Kocaoz 2013; Miquelutti 2013; Mørkved 2003; Sampselle 1998; Stafne 2012). The exercise protocol described by Bø 1995 was the PFM strength training protocol on which the trials by Bø 2011, Mørkved 2003, and Dumoulin 2004 were based. Supervised treatment duration was only eight weeks in the trials by Dumoulin 2004 and Kim 2012 and this might have been insufficient for muscle hypertrophy to be established. In addition to strength training, Dumoulin 2004 included some co‐ordination type training. Women were encouraged to perform voluntary PFM contraction in conjunction with rises in intra‐abdominal pressure, such as with coughing or sneezing, also known as 'the Knack' (Miller 2008). Kim 2012 included trunk stabilisation exercises. With regard to contact with health professionals, this was low in two trials (fewer than five contacts) (Ahlund 2013; Miquelutti 2013), moderate (six to 12 contacts) in four (Dumoulin 2004; Kocaoz 2013; Mørkved 2003; Stafne 2012) and high (more than 12 contacts) in three (Bø 2011; Hilde 2013; Kim 2012). Four trials stated that PFMT was supervised in an exercise class (Bø 2011; Hilde 2013; Mørkved 2003; Stafne 2012). Eight trials confirmed a correct voluntary PFM contraction prior to training (Ahlund 2013; Dinc 2009; Hilde 2013; Kim 2012; Kocaoz 2013; Mørkved 2003; Sampselle 1998; Stafne 2012). Five of these also confirmed a correct contraction in the control group along with provision of usual antenatal and postnatal care (Ahlund 2013; Dinc 2009; Hilde 2013; Kim 2012; Mørkved 2003). In the remaining six trials, the control conditions were usual care, which may or may not have included PFMT or no PFMT as controls were asked not to train (Bø 2011; Dumoulin 2004; Kocaoz 2013; Miquelutti 2013; Sampselle 1998; Stafne 2012). With regard to adherence, five trials reported some information about exercise behaviour and four of these compared group exercise classes and home PFMT versus usual care (Bø 2011; Hilde 2013; Mørkved 2003; Stafne 2012). The fifth trial with adherence data compared standardised instruction and home PFMT with usual care (Sampselle 1998). In Stafne 2012, 67% of the PFMT group performed home PFMT at least three times per week compared to 40% of controls in late pregnancy. At six months' postpartum, Hilde 2013 found that 96% of the PFMT group who completed the trial adhered to 80% of the class and daily home training, whereas 16.5% of controls reported daily PFMT at home, three or more times per week. The other three trials reported data only for the intervention group, with adherence to PFMT of about 70% (Bø 2011) and 80% (Mørkved 2003), or 85% of PFMT women doing PFMT 75% of the time (Sampselle 1998).
-
Six trials described PFMT programmes that were characteristic of strength training but did not mention loading (effort) (Assis 2015; Chiarelli 2002; Gorbea 2004; Ko 2011; Peirce 2013; Reilly 2002). Two trials referenced the exercise protocols of other authors. Reilly 2002 cited Bø 1995 (strength and load training) and Ko 2011 cited Reilly 2002. The supervised treatment duration was only eight weeks in the trial by Chiarelli 2002 and this may have been insufficient for muscle hypertrophy to be established. In addition to strength training, women undertook some co‐ordination type training, daily biofeedback or participated in a weekly exercise class supervised by a physiotherapist (Ko 2011; Peirce 2013; Reilly 2002). In two trials, the control groups did not exercise (Assis 2015; Gorbea 2004). In the other four trials, controls were randomised to usual care which may or may not have included PFMT (Chiarelli 2002; Ko 2011; Peirce 2013; Reilly 2002). A correct PFM contraction for women in the exercise group was confirmed in five of the six trials (Assis 2015; Chiarelli 2002; Gorbea 2004; Ko 2011; Peirce 2013). However, none of the control groups appeared to have confirmation of a correct contraction. With regard to adherence, five of the six trials reported some information about exercise behaviour (Chiarelli 2002; Gorbea 2004; Ko 2011; Peirce 2013; Reilly 2002). Five trials offered individual supervision (Assis 2015; Chiarelli 2002; Gorbea 2004; Peirce 2013; Reilly 2002). One offered group sessions (Ko 2011). At three months' postpartum, Chiarelli 2002 reported that more women in the PFMT group (84%) compared to controls (58%) were doing "adequate" PFMT. Similarly, in Reilly 2002, about 75% of the PFMT group and 66% of the control group were doing more than occasional or no PFMT (27.5% in the PFMT group and 34% in the control group reported occasional or no PFMT). During the antenatal intervention period, nearly half the women in the PFMT group exercised for 28 days or more (which is approximately once per week over 20 weeks). The other three trials reported data only for the intervention group, with two reporting that over 80% of women attended most or all supervised visits (Gorbea 2004; Ko 2011). Ko 2011 and Peirce 2013 reported that more than three‐quarters of women in the PFMT group completed 70% or more of the prescribed exercise.
There was insufficient detail in the other 21 trials to classify them as providing strength or endurance training.
-
Seven trials provided some information about PFMT but could not be categorised (Glazener 2001; Kou 2013; Liu 2011; Pelaez 2014; Sangsawang 2016; Wen 2010; Wilson 1998). None had any description of effort (i.e. load). Supervised treatment was only six to eight weeks in two trials and this might have been insufficient for muscle hypertrophy to be established if strengthening was intended (Sangsawang 2016; Wen 2010). Five of the seven trials included variously described mixes of fast and slow contractions with relatively large numbers of sets (eight to 10 per day) and few repetitions per set (about 10) or exercise sets of 15‐ to 30‐minute duration (Glazener 2001; Pelaez 2014; Sangsawang 2016; Wen 2010; Wilson 1998). Overall, all appeared to recommend a large number of contractions per day (more than 100) or a minimum of 30 minutes of PFMT per day. The programmes might have affected strength or endurance, or both, depending on the number of contractions performed daily and the amount of voluntary effort with each contraction. The amount of contact with healthcare providers varied. In two trials, women participated in group exercise sessions, either three groups over a period of six weeks or a total of 70 to 80 groups over 22 weeks (Pelaez 2014; Sangsawang 2016). In another two trials, women had one‐to‐one sessions with health professionals, with three or four visits spread over eight to nine months (Glazener 2001; Wilson 1998). In three trials, the number and duration of contacts with healthcare providers was unknown (Kou 2013; Liu 2011; Wen 2010), although it is possible this was twice per week in the trial that included biofeedback (Kou 2013). Only three trials mention confirmation of correct PFM contraction, being verified by an obstetrician or by the women themselves using self‐palpation, mirror observation of the perineum or mid‐stream urine stoppage (Pelaez 2014; Sangsawang 2016; Wen 2010). In all trials, the control group received usual care that may have included advice or opportunities to do PFMT (e.g. in an antenatal class), with the exception of Sangsawang 2016 where women received usual care but no information on urinary incontinence or PFMT. Four trials provided some adherence data. The women in the trials by Glazener 2001 and Wilson 1998 were supervised individually and performed significantly more voluntary PFM contractions per day at 12 months' postpartum in the PFMT groups. The mean number of contractions was 20 (SD 29) and 86 (95% CI 69 to 104) per day in PFMT women, and 5 (SD 15) and 35 (95% CI 30 to 40) per day in control women. Glazener 2001 followed up women for six years after the index delivery. Similar proportions of women in both groups were doing some PFMT, 50% (132/263) in the intervention group and 50% (127/253) in the control group. The other two trials offered group supervision and reported adherence data for the training groups only. Pelaez 2014 reported that all PFMT women attended at least 80% of the exercise sessions (approximately 70 to 78 in total). In the trial by Sangsawang 2016, it appeared that all women had done PFMT for 28 days (of 42 in total).
-
Fourteen trials did not specify any details of the PFMT received by intervention group (Barakat 2011; Cruz 2014; Dokmeci 2008; Ewings 2005; Fritel 2015; Frost 2014; Frumenzio 2012; Gaier 2010; Hughes 2001; Meyer 2001; Skelly 2004; Sleep 1987; Stothers 2002; Woldringh 2007). Eight of these were conference abstracts (Cruz 2014; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010; Hughes 2001; Skelly 2004; Stothers 2002). Four trials mentioned that women were asked to do daily PFMT at home (Fritel 2015; Frumenzio 2012; Hughes 2001; Stothers 2002). One asked women to complete a daily exercise diary (Sleep 1987). Most trials provided one or more one‐to‐one supervisory sessions with a health professional, two invited women to one or two additional group sessions (Ewings 2005; Hughes 2001). Barakat 2011 provided PFMT within approximately 85 exercise classes over the course of pregnancy. Three trials confirmed a correct PFM contraction either by digital palpation or observation and palpation of the perineal body (Fritel 2015; Hughes 2001; Woldringh 2007). The control conditions were: no PFMT (Frumenzio 2012; Meyer 2001; Stothers 2002), usual care (which may or may not have included advice on PFMT) (Frost 2014; Gaier 2010; Hughes 2001; Skelly 2004), usual care that included advice about PFMT (Ewings 2005; Sleep 1987; Woldringh 2007), and PFMT at home (Cruz 2014; Fritel 2015). In two trials, the control condition was unclear (Barakat 2011; Dokmeci 2008). In five of the 14 trials, no information was provided about adherence, or the number of contacts with health professionals in either the intervention or control groups (Cruz 2014; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010). All were abstracts. Six of the 14 trials provided some information about exercise behaviour (Barakat 2011; Ewings 2005; Fritel 2015; Hughes 2001; Sleep 1987; Woldringh 2007). Three trials reported adherence data for both the intervention and control groups (Fritel 2015; Sleep 1987; Woldringh 2007). In the trial by Fritel 2015, 69% of women in the PFMT group completed all eight supervised weekly exercise sessions and 83% completed at least one. Fewer women in the PFMT group (4.3%) compared to controls (10.6%) were doing daily exercise at home at the end of pregnancy. Woldringh 2007 reported that 37% of the PFMT women were exercising intensively, compared to 14% of controls, at 36 weeks' gestation. Similarly, at three months' postpartum, Sleep 1987 reported that more women in the PFMT group (58%) compared to controls (42%) were doing some PFMT. The other three trials provided data only for the intervention group (Barakat 2011; Ewings 2005; Hughes 2001). Barakat 2011 reported "adherence to training in the experimental group was 90%" (a mean of 85 sessions in total) and Hughes 2001 (personal communication) observed that 79% of women assigned to PFMT attended the single group training session. In contrast, Ewings 2005 invited PFMT women to attend a class at two and four months postnatally and, of the 117 women, only 18% attended at two months and 4% attended at four months.
Outcome measures
Twenty‐five of the 38 trials clearly stated the primary outcome(s) of interest in the trial.
-
In 17 trials, it was self‐reported urinary incontinence (Assis 2015; Bø 2011; Chiarelli 2002; Cruz 2014; Ewings 2005; Fritel 2015; Glazener 2001; Gorbea 2004; Hilde 2013; Ko 2011; Kou 2013; Mørkved 2003; Pelaez 2014; Reilly 2002; Sangsawang 2016; Skelly 2004; Stafne 2012). Three used the International Consultation on Incontinence Questionnaire‐Short Form (ICIQ‐SF) (Cruz 2014; Fritel 2015; Pelaez 2014).
-
Three trials used loss of urine under stress test (Dumoulin 2004; Kocaoz 2013; Stothers 2002).
-
One trial used the Bristol Female Lower Urinary Tract Symptoms (BFLUTS; 34 question tool, higher score worse) questionnaire, quality of life domain (Kim 2012).
-
One trial combined data from a urinary diary and questionnaire to give an incontinence severity score (Woldringh 2007).
-
One trial used the unspecified "urinary condition score" (Liu 2011).
-
One trial used PFM strength (perineometry) (Ahlund 2013).
-
One trial used the occurrence of traumatic tears and use of episiotomy (Gaier 2010).
While there was some consistency in the choice of outcome measures by trialists, the differences in the measures or the way the data were reported limited the possibilities for combining results from individual trials.
Only three trials reported long‐term results after the first year (Glazener 2001; Mørkved 2003; Reilly 2002).
Excluded studies
Thirty‐eight trials were excluded for the following reasons.
-
Twenty‐eight studies did not collect any urinary or faecal incontinence outcome data (Agur 2005; Assis 2013; Barakat 2014; Barakat 2016; Dias 2011; Domingues 2015; Dougherty 1989; Golmakani 2015; Hou 2010; Huang 2014; Lekskulchai 2014; Li 2010; Liu 2013; Mahmoodi 2014; Morin 2015; NCT01696201; NCT01723293; NCT01753622; Nielsen 1988; Norton 1990; Oblasser 2016; Okido 2015; Perales 2016; Ruiz 2013; Siva 2014; Thorp 1994; Wang 2014; Zhu 2012).
-
Three trials compared the Epi‐No device versus control (Dannecker 2004; Dietz 2014; Kamisan Atan 2016). The women were recruited in very late pregnancy (33 to 37 weeks' gestation) and the primary purpose of the intervention was prevention of perineal trauma. In one trial, it seemed women did PFM contractions with the Epi‐No device in the vagina (Dannecker 2004). However, this was unclear in the other two (Dietz 2014; Kamisan Atan 2016).
-
Four trials included PFMT as part of an intervention but the actual comparisons were: active versus sham magnetic stimulation (Culligan 2005), one type of feedback versus another (Fynes 1999; Mahony 2004), and PFMT plus episiotomy versus caesarean section (Taskin 1996). Another trial compared abdominal exercise with no abdominal exercise (Gouldthorpe 2003).
-
One study was excluded because of internal inconsistencies and data discrepancies (Mason 2010).
-
One trial was listed in a trials register but there was no report of this trial available. There was no response to a letter sent to the principal investigator (Mason 1999).
Risk of bias in included studies
We have provided details for each trial in the Characteristics of included studies. A summary of the risk of bias for each individual trial is presented in Figure 2, while Figure 3 summarises the risk of bias across all trials included in the review.
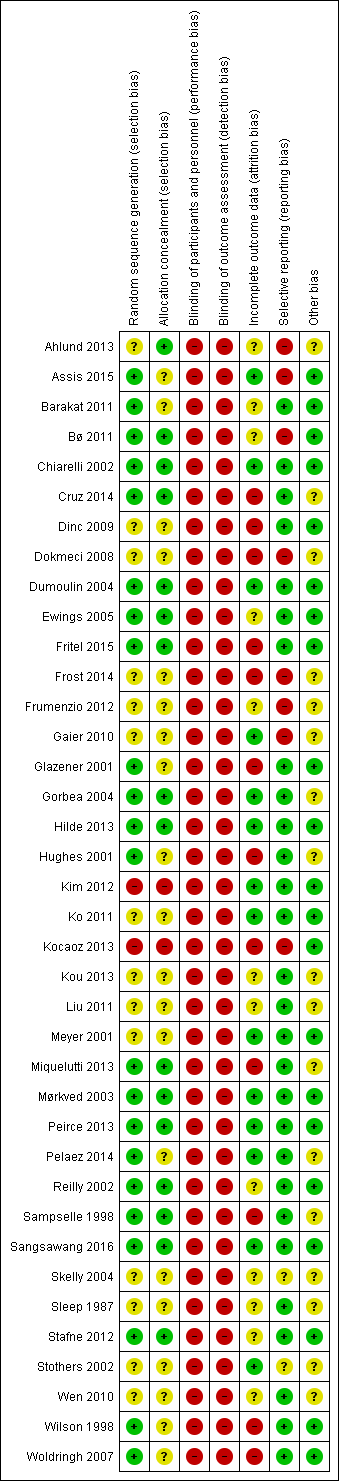
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
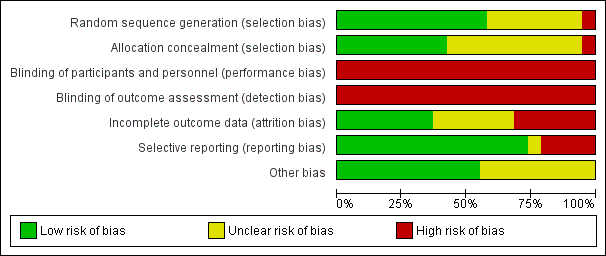
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Due to the brevity of reporting, it was difficult to assess the eight trials that were published as conference abstracts (Cruz 2014; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010; Hughes 2001; Skelly 2004; Stothers 2002). In addition, one of these abstracts did not report sample size (Skelly 2004). However, one‐to‐one randomisation was assumed. Three trials were small, with fewer than 25 women per comparison group (Dokmeci 2008; Dumoulin 2004; Kim 2012). Ten were of moderate size, with between 25 and 50 women per group (Ahlund 2013; Assis 2015; Barakat 2011; Cruz 2014; Dinc 2009; Frumenzio 2012; Gorbea 2004; Sampselle 1998; Sangsawang 2016; Stothers 2002). Twenty‐one trials allocated more than 50 women per group (Bø 2011; Chiarelli 2002; Ewings 2005; Fritel 2015; Frost 2014; Gaier 2010; Glazener 2001; Hilde 2013; Hughes 2001; Ko 2011; Kocaoz 2013; Kou 2013; Liu 2011; Meyer 2001; Miquelutti 2013; Mørkved 2003; Pelaez 2014; Reilly 2002; Stafne 2012; Wen 2010; Woldringh 2007). Three of these were large, that is, with more than 300 women per comparison group (Chiarelli 2002; Glazener 2001; Stafne 2012). Two were very large trials of more than 500 women per group (Hughes 2001; Sleep 1987). Peirce 2013 used block randomisation, meaning 30 women were allocated to PFMT and biofeedback and 90 women were included in the PFMT‐only group. Wilson and colleagues randomised just over 100 women to the control and individual treatment groups, with the individual treatment group being further randomised into three groups: PFMT only, PFMT with vaginal cones and vaginal cones only (Wilson 1998).
Twenty‐two of the 38 trials reported an a priori power calculation (Ahlund 2013; Assis 2015; Barakat 2011; Chiarelli 2002; Dinc 2009; Dumoulin 2004; Fritel 2015; Glazener 2001; Gorbea 2004; Hilde 2013; Kim 2012; Ko 2011; Meyer 2001; Miquelutti 2013; Mørkved 2003; Peirce 2013; Pelaez 2014; Reilly 2002; Sangsawang 2016; Sleep 1987; Stafne 2012; Woldringh 2007). One of the trials without a power calculation was a pilot trial (Ewings 2005).
Allocation
Random allocation generation
Twenty‐two trials provided enough information on random allocation generation for us to be reasonably sure that they had a low risk of bias (Assis 2015; Barakat 2011; Bø 2011; Chiarelli 2002; Cruz 2014; Dumoulin 2004; Ewings 2005; Fritel 2015; Glazener 2001; Gorbea 2004; Hilde 2013; Hughes 2001; Miquelutti 2013; Mørkved 2003; Peirce 2013; Pelaez 2014; Reilly 2002; Sampselle 1998; Sangsawang 2016; Stafne 2012; Wilson 1998; Woldringh 2007). Fourteen trials provided insufficient information for a judgement to be made, therefore these trials were at unclear risk of bias (Ahlund 2013; Dinc 2009; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010; Ko 2011; Kou 2013; Liu 2011; Meyer 2001; Skelly 2004; Sleep 1987; Stothers 2002; Wen 2010). Two trials were categorised as high risk of bias (Kim 2012; Kocaoz 2013). Kocaoz 2013 used methods suggestive of alternation and Kim 2012 provided participants with an envelope from which they drew one of two cards.
Random allocation concealment
Sixteen studies reported adequate allocation concealment and were at low risk of bias (Ahlund 2013; Bø 2011; Chiarelli 2002; Cruz 2014; Dumoulin 2004; Ewings 2005; Fritel 2015; Gorbea 2004; Hilde 2013; Miquelutti 2013; Mørkved 2003; Peirce 2013; Reilly 2002; Sampselle 1998; Sangsawang 2016; Stafne 2012). Two trials were at high risk of bias, being unable to adequately conceal randomisation (Kim 2012; Kocaoz 2013). The 22 remaining trials were at unclear risk of bias as insufficient information (e.g. not described or stated "randomised") was provided.
Blinding
Blinding of participants and therapists
Given the nature of the intervention, it was not feasible for the included trials to blind the treatment provider or participants to group allocation and so all 38 trials were at high risk of performance bias. The difficulty of blinding exercise‐based interventions is a common problem.
Blinding of outcome assessment
Because the two main outcomes of interest in this review, urinary incontinence and incontinence‐specific quality of life, are self‐reported, these are unblinded measures. As a result, all 38 trials were deemed to be at high risk of detection bias. Blinded outcome assessment should be possible for some secondary outcomes, such as pad testing, and 12 trials attempted this (Bø 2011; Chiarelli 2002; Cruz 2014; Dumoulin 2004; Fritel 2015; Glazener 2001; Hilde 2013; Kim 2012; Mørkved 2003; Reilly 2002; Sampselle 1998; Stothers 2002).
Incomplete outcome data
Reporting of dropout and withdrawal and analysis by intention to treat
Based on the criteria for assessment of attrition bias reported in the methods (see 'Assessment of risk of bias' in Included studies), 10 trials were at low risk of attrition bias (Assis 2015; Chiarelli 2002; Dumoulin 2004; Hilde 2013; Kim 2012; Ko 2011; Meyer 2001; Pelaez 2014; Sangsawang 2016; Stothers 2002). Another 10 were at unclear risk (Ahlund 2013; Barakat 2011; Frumenzio 2012; Kou 2013; Liu 2011; Reilly 2002; Skelly 2004; Sleep 1987; Stafne 2012; Wen 2010). Some trials did not report on losses to follow‐up and were at unclear risk of bias (Bø 2011; Frumenzio 2012; Kou 2013; Liu 2011; Skelly 2004; Wen 2010). Two of these were abstracts (Frumenzio 2012; Skelly 2004). The remaining 12 trials were at high risk. All trials appeared to analyse participants in the groups to which they were assigned.
Selective reporting
All outcomes appeared to have been reported in the majority of trials, with 28 of 38 trials assessed at low risk of bias in this domain. Eight trials were at high risk of bias. Six of these did not report all of the prespecified outcome measures (Ahlund 2013; Assis 2015; Bø 2011; Dokmeci 2008; Frumenzio 2012; Gaier 2010), and, of these, two also did not state the a priori primary outcome measure (Dokmeci 2008; Frumenzio 2012). A further two were at high risk due to not presenting data that related to a key outcome of the review (i.e. self‐reported urinary incontinence) (Frost 2014; Kocaoz 2013). Three of these were conference abstracts (Dokmeci 2008; Frost 2014; Frumenzio 2012). Two trials were at unclear risk of bias as it was uncertain if selective reporting had taken place (Skelly 2004; Stothers 2002).
Other potential sources of bias
From the 38 trials in this review, we considered 21 to be free of problems (such as conflict of interest) that could put them at risk of other bias. We considered the risk of other bias as unclear for 17 trials (Ahlund 2013; Cruz 2014; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010; Gorbea 2004; Hughes 2001; Kou 2013; Liu 2011; Miquelutti 2013; Pelaez 2014; Sampselle 1998; Skelly 2004; Sleep 1987; Stothers 2002; Wen 2010).
Effects of interventions
See: Summary of findings for the main comparison Antenatal pelvic floor muscle training compared to control for prevention of urinary and faecal incontinence; Summary of findings 2 Antenatal pelvic floor muscle training compared to control for treatment of urinary and faecal incontinence; Summary of findings 3 Antenatal pelvic floor muscle training compared to control for mixed prevention and treatment of urinary and faecal incontinence; Summary of findings 4 Postnatal pelvic floor muscle training compared to control for treatment of urinary and faecal incontinence; Summary of findings 5 Postnatal pelvic floor muscle training compared to control for mixed prevention and treatment of urinary and faecal incontinence
There were some data available to explore the hypothesis that PFMT is better than usual antenatal and postnatal care, or no treatment, for the prevention or treatment of urinary and faecal incontinence. The primary analysis investigated the prevalence of urinary and faecal incontinence. Data for outcomes of secondary interest (in 'Other data' tables) are only briefly discussed to give an indication of whether the findings were broadly consistent with the pooled data, or not. Thirty‐four trials contributed data to one or more forest plots. The four trials that did not were by Ahlund 2013, Dokmeci 2008, Frost 2014, and Liu 2011.
The 'Summary of findings' tables present the selected outcomes for each of the five main comparisons.
-
Antenatal PFMT compared to control for prevention of urinary and faecal incontinence: summary of findings Table for the main comparison.
-
Antenatal PFMT compared to control for treatment of urinary and faecal incontinence: summary of findings Table 2.
-
Antenatal PFMT compared to control for mixed prevention and treatment of urinary and faecal incontinence: summary of findings Table 3.
-
Postnatal PFMT compared to control for treatment of urinary and faecal incontinence: summary of findings Table 4.
-
Postnatal PFMT compared to control for mixed prevention and treatment of urinary and faecal incontinence: summary of findings Table 5.
Comparison 1: antenatal pelvic floor muscle training for prevention of incontinence
Ten trials reported antenatal PFMT for prevention of incontinence (Barakat 2011; Gaier 2010; Gorbea 2004; Kocaoz 2013; Mørkved 2003; Pelaez 2014; Reilly 2002; Sampselle 1998; Sangsawang 2016; Stothers 2002). Seven recruited nulliparous or primiparous or primigravid women during pregnancy (Gaier 2010; Gorbea 2004; Mørkved 2003; Pelaez 2014; Reilly 2002; Sampselle 1998; Sangsawang 2016). The other three recruited "pregnant women" or both primiparous and multiparous women (Barakat 2011; Kocaoz 2013; Stothers 2002). All women were continent at recruitment.
In all 10 trials, PFMT began during pregnancy. Controls were asked not to do PFMT, did not receive instruction on PFMT, received usual care that might have included information on PFMT, or the control condition was not specified (Barakat 2011; Gaier 2010; Gorbea 2004; Kocaoz 2013; Mørkved 2003; Pelaez 2014; Reilly 2002; Sampselle 1998; Sangsawang 2016; Stothers 2002).
Two of these trials were mixed prevention and treatment trials but published or unpublished data were available for women who were continent at recruitment (Mørkved 2003; Sampselle 1998). In Sampselle 1998, 54/72 women were continent based on a standing stress test at 20 weeks' gestation. After dropouts, there were unpublished data from 37 previously continent women (16 PFMT and 21 controls). Mørkved 2003 published data for 207/301 women who were continent before pregnancy and at 20 weeks' gestation. After dropouts, there were data from 193 previously continent women (94 PFMT and 99 controls). Neither trial was powered to find differences in the previously continent subgroup, as the subgroup sizes were small.
Primary outcome
Self‐reported urinary or faecal incontinence
-
Women randomised to PFMT were about 62% less likely to report urinary incontinence in late pregnancy compared to controls (RR 0.38, 95% CI 0.20 to 0.72; 6 trials, 624 women, random‐effects, I² = 78%, T² = 0.44; low‐quality evidence) (Analysis 1.1).
There was statistically significant heterogeneity in this comparison and in both subgroups (PFMT versus no PFMT, PFMT versus usual care). A random‐effects model was used because of the heterogeneity. Two trials appeared to contribute most to the heterogeneity (Gorbea 2004; Pelaez 2014), and both found many fewer cases of urinary incontinence in the intervention than control groups. Gorbea 2004 was the only trial that specifically asked controls not to do PFMT during pregnancy. In addition, as none of the PFMT women reported urinary incontinence in late pregnancy, the point estimate and CIs were perhaps less stable given there were no events in one of the two comparison groups. In Pelaez 2014, the PFMT was very intensive and of longer duration than other trials in the same subgroup. The intervention included three supervised exercise classes per week for at least 22 weeks and 80% of women attended the maximum number of classes.
-
PFMT women were about 62% less likely to report urinary incontinence, compared to controls, in the early postpartum period (RR 0.38, 95% CI 0.17 to 0.83; 5 trials, 439 women, random‐effects, I² = 74%, T² = 0.55) (Analysis 1.2). There was statistically significant heterogeneity in this comparison, as well as in one subgroup (PFMT versus usual care), which included the trial by Pelaez 2014 (see above).
-
PFMT women were still less likely than controls to have urinary incontinence in the mid‐postnatal period (three to six months), although the difference in risk had reduced to 29% (RR 0.71, 95% CI 0.54 to 0.95; 5 trials, 673 women, fixed‐effect, I² = 0%; moderate‐quality evidence) (Analysis 1.3). Overall, the pooled estimate favoured PFMT.
-
There were not enough participants (44 women; low‐quality evidence) in the trial by Sampselle 1998 to identify whether there was a difference in prevalence of urinary incontinence between PFMT women and women in the control group at 12 months' postpartum (RR 1.20, 95% CI 0.65 to 2.21) (Analysis 1.4).
Two trials measured incontinence at greater than five years (Mørkved 2003; Reilly 2002; seeTable 1 ). The pooled data suggested that the earlier effectiveness of PFMT did not persist in the long term (RR 1.07, 95% CI 0.77 to 1.48; 2 trials, 352 women, fixed‐effect, I² = 25%) (Analysis 1.6). Reilly 2002 found that 68.4% of women randomised to the intervention group were still performing PFMT, with 38% doing PFMT at least twice per week after eight years. Mørkved 2003 reported that the same number of women in the PFMT and control groups (45%) were exercising at least weekly, six years after the primary study. The lack of a difference in prevalence rates of incontinence in these three trials suggests that perhaps PFMT is not effective in the long term. There could be three immediately plausible explanations for this. The women may have stopped exercising, they may have had subsequent pregnancies or, as shown by Mørkved 2003, women were performing similar PFMT regimens regardless of which group they had initially been randomised.
None of the 10 trials reported data on the prevalence of either antenatal or postpartum faecal incontinence.
Incontinence‐specific quality of life
Reilly 2002 (King's Health Questionnaire) and Pelaez 2014 (ICIQ‐SF) were the only two trials to mention incontinence‐specific quality of life. Pelaez 2014 found a difference between the two groups in favour of PFMT (MD ‐2.42, 95% CI ‐3.32 to ‐1.52; 2 trials, 152 women; moderate‐quality evidence) (Analysis 1.13; lower score indicates better incontinence‐specific quality of life). Reilly 2002 did not report their data but stated there was no difference between the groups on any of the eight subscales (Analysis 1.14).
Secondary outcomes
Severity of incontinence
Seven of the 10 trials reported some data on symptom severity, such as frequency or amount of urine leakage (Analysis 1.14) (Barakat 2011; Gorbea 2004; Pelaez 2014; Reilly 2002; Sampselle 1998; Sangsawang 2016; Stothers 2002). The choice of measures (many of these of unknown validity) or the ways of reporting these were highly variable and data reporting was often incomplete. Two of the most recent trials used individual item scores from the ICIQ‐SF; frequency (item 3) and amount of leakage (item 4) (Barakat 2011; Pelaez 2014). There was a consistent pattern of effect in favour of PFMT, when compared to usual care, for frequency, amount and other urinary incontinence severity indices in two trials (Pelaez 2014; Sangsawang 2016).
Number of urinary or faecal incontinence episodes
None of the trials reported number of urinary or faecal incontinence episodes.
Loss of urine under stress test
Three trials reported whether women were continent or not based on a stress test (positive cough or one‐hour pad test) (Gorbea 2004; Kocaoz 2013; Reilly 2002). Women in the PFMT group were less likely to be incontinent in late pregnancy (RR 0.36, 95% CI 0.19 to 0.70; 1 trial, 102 women) or in the early postnatal period (RR 0.09, 95% CI 0.02 to 0.47; 2 trials, 174 women, fixed‐effect, I² = 0%) when compared with no treatment controls (Analysis 1.15; Analysis 1.16) (Gorbea 2004; Kocaoz 2013). There was no difference between PFMT versus usual care groups in the early postnatal period (RR 0.88, 95% CI 0.33 to 2.29; 1 trial, 148 women) (Analysis 1.16) (Reilly 2002). Two trials used the SF‐36 (Barakat 2011; Reilly 2002). In the general health domain, Reilly 2002 reported that the PFMT group scored significantly higher than the control group at three months' postpartum (MD 7.2, 95% CI 2.36 to 12.04), while Barakat 2011 found that women in the PFMT group were more likely to rate their health as very good (18/34 women in the PFMT group versus 9/33 women in the control group) (Analysis 1.17).
Other quality of life and health status measures
None of the trials reported other quality of life and health status measures.
Health economics
None of the trials reported health economic data.
Adverse effects
Only one trial noted any adverse events: two of 43 PFMT women withdrew due to pelvic floor pain (Stothers 2002). Barakat 2011 stated "there were no exercise‐related injuries experienced during pregnancy." No other trial reported whether there were adverse effects or not.
Other outcomes
Pelvic floor muscle function
Three trials measured PFM function (Gaier 2010; Gorbea 2004; Reilly 2002). However, Gaier 2010 reported no data. Measures were electromyography and vaginal squeeze pressure (Gorbea 2004; Reilly 2002). The lack of explanation of the type of electromyography and unusual presentation of the data in Gorbea 2004 made it difficult to interpret the findings. In Reilly 2002, mean vaginal squeeze pressure was not greater in the PFMT group than the control group (MD 1.00, 95% CI ‐1.31 to 3.31) (Analysis 1.18). Gaier 2010 reported significantly higher PFM strength in women doing PFMT. However, it was unclear how this was measured and the data were not given in the conference abstract.
Delivery outcome
Five trials reported delivery outcome (Barakat 2011; Gaier 2010; Gorbea 2004; Reilly 2002; Stothers 2002). However, the data by Stothers 2002 were not reported by group. Three trials reported the number of caesarean sections (Barakat 2011; Gorbea 2004; Reilly 2002). There was no difference between PFMT and control groups in any of these trials (RR 1.28, 95% CI 0.89 to 1.85; 3 trials, 373 women, fixed‐effect, I² = 49%) (Analysis 1.19). Two trials reported type of vaginal delivery (normal or instrumental) (Barakat 2011; Reilly 2002). Two trials reported perineal trauma (Barakat 2011; Gaier 2010). There were no apparent differences between groups for either outcome (Analysis 1.20).
Any other outcome not prespecified but of interest
None of the trials reported any other outcomes not prespecified but of interest.
Comparison 2: antenatal pelvic floor muscle training for treatment of incontinence
Four trials reported antenatal PFMT for treatment of incontinence (Cruz 2014; Dinc 2009; Skelly 2004; Woldringh 2007). Two trials recruited primiparous and multiparous women (Dinc 2009; Woldringh 2007). Two trials reported as abstracts did not state parity (Cruz 2014; Skelly 2004). In all four trials, the control group received usual care.
Primary outcome
Self‐reported urinary or faecal incontinence
-
There was no difference in prevalence of urinary incontinence in late pregnancy (RR 0.70, 95% CI 0.44 to 1.13; 3 trials, 345 women, random‐effects, I² = 71%, T² = 0.11; very low‐quality evidence) (Analysis 2.1).
This comparison showed statistically significant heterogeneity; a random‐effects model was used to provide a more conservative estimate (Analysis 2.1).
-
There were no differences in the early postnatal period (RR 0.75, 95% CI 0.37 to 1.53; 2 trials, 292 women, random‐effects, I² = 65%, T² = 0.19) or mid‐postnatal period (RR 0.94, 95% CI 0.70 to 1.24; 1 trial, 187 women; very low‐quality evidence) (Analysis 2.2; Analysis 2.3).
-
Two trials measured urinary incontinence in the late postnatal period. A random‐effects model was used because of statistically significant heterogeneity in this comparison and there was no difference between groups (RR 0.50, 95% CI 0.13 to 1.93; 2 trials, 869 women, random‐effects, I² = 94%, T² = 0.89; very low‐quality evidence) (Analysis 2.4) (Skelly 2004; Woldringh 2007). Skelly 2004 was available only as a conference abstract with limited data on which to base a risk of bias assessment and about half of the women randomised appeared to have urinary incontinence symptoms pre‐pregnancy. In Woldringh 2007, at 35 weeks' gestation, about two‐thirds of women in the control group were doing some form of PFMT, compared to 94% in the PFMT group. These, or other unknown reasons, could have contributed to the observed heterogeneity.
None of the four trials reported data on the prevalence of either antenatal or postpartum faecal incontinence.
Incontinence‐specific quality of life
Two trials used a validated incontinence‐specific quality of life measure (Cruz 2014, ICIQ‐SF; Woldringh 2007, IIQ). Cruz 2014 found a better quality of life in PFMT women in late pregnancy (MD ‐3.50, 95% CI ‐6.13 to ‐0.87; 1 trial, 41 women, low‐quality evidence) (Analysis 2.14; lower score better). Woldringh 2007 categorised IIQ scores, which meant that it was not possible to interpret these data (Analysis 2.15).
Secondary outcomes
Severity of incontinence
Woldringh 2007 reported on leakage severity, but the validity of this measure is unknown (Analysis 2.16).
Number of urinary or faecal incontinence episodes
None of the trials reported number of urinary or faecal incontinence episodes.
Loss of urine under stress test
None of the trials reported loss of urine under stress test.
Other quality of life and health status measures
None of the trials reported other quality of life and health status measures.
Health economics
None of the trials reported health economic data.
Adverse effects
None of the trials reported on adverse effects.
Other outcomes
Pelvic floor muscle function
Cruz 2014 found no difference between the groups in maximal vaginal squeeze pressure in the third trimester (Analysis 2.17).
Comparison 3: antenatal pelvic floor muscle training for mixed prevention and treatment of incontinence
Eleven trials reported antenatal PFMT for mixed prevention and treatment of incontinence (Assis 2015; Bø 2011; Dokmeci 2008; Fritel 2015; Frumenzio 2012; Hughes 2001; Ko 2011; Miquelutti 2013; Mørkved 2003; Sampselle 1998; Stafne 2012). The control group consisted of usual care in seven trials (Bø 2011; Fritel 2015; Hughes 2001; Miquelutti 2013; Mørkved 2003; Sampselle 1998; Stafne 2012). There was no PFMT in two trials (Assis 2015; Ko 2011). Two did not specify the control group (Dokmeci 2008; Frumenzio 2012).
Nine trials were in women who were delivering their first baby (Assis 2015; Bø 2011; Dokmeci 2008; Fritel 2015; Hughes 2001; Ko 2011; Miquelutti 2013; Mørkved 2003; Sampselle 1998). One recruited both primiparous and multiparous women (Stafne 2012). Parity was not stated in Frumenzio 2012, which was an abstract.
Primary outcome
Self‐reported urinary or faecal incontinence
-
Women randomised to PFMT had about 26% less risk of urinary incontinence in late pregnancy (RR 0.74, 95% CI 0.61 to 0.90; 9 trials, 3164 women, random‐effects, I² = 82%, T² = 0.06; low‐quality evidence) (Analysis 3.1).
There was statistically significant heterogeneity in both subgroups (PFMT versus no exercise and PFMT versus usual care) in this comparison (Analysis 3.1). The point estimates favoured PFMT in all but two trials (Bø 2011; Fritel 2015). In the seven trials where the point estimates favoured PFMT, there was considerable variation with RR ranging from 0.07 to 0.93 (Assis 2015; Hughes 2001; Ko 2011; Miquelutti 2013; Mørkved 2003; Sampselle 1998; Stafne 2012). The data that appeared notably different, being markedly in favour of PFMT, were those from Assis 2015 for reasons unknown, although this was one of two trials in which controls were asked not to do PFMT. In the two trials where the point estimates did not favour PFMT, there were plausible explanations for no differences between the two groups. Participants in Bø 2011 were encouraged to attend at least two out of three possible exercise classes every week. These exercise classes were led by general fitness instructors who were taught by a physiotherapist how to deliver PFMT to women. It may be that the women in this trial considered the classes solely as general fitness and did not concentrate on the PFMT component. In Fritel 2015, the authors reported that at the end of pregnancy there was no difference in the frequency and duration of PFMT between groups, suggesting no difference in exercise adherence between the PFMT and usual care groups.
-
There was a difference in the prevalence of urinary incontinence between antenatal PFMT and control groups in the early postnatal (RR 0.80, 95% CI 0.67 to 0.95; 5 trials, 760 women, fixed‐effect, I² = 0%, T² = 0.00) (Analysis 3.2) and mid‐postnatal periods (RR 0.73, 95% CI 0.55 to 0.97; 5 trials, 1921 women, random‐effects, I² = 65%, T² = 0.06; very low‐quality evidence) (Analysis 3.3), but not in the late postnatal period (RR 0.85, 95% CI 0.63 to 1.14; 2 trials, 244 women, fixed‐effect, I² = 0%; low‐quality evidence) (Analysis 3.4).
In the mid‐postnatal period, while all the point estimates favoured PFMT, these varied considerably between the trials (RRs of 0.42 to 0.97). In the one trial with long‐term data (six years), Mørkved 2003, there was no difference between groups (RR 1.38, 95% CI 0.77 to 2.45; 1 trial, 188 women) (Analysis 3.6). Women in the control group were offered a description of the PFMT programme after the post‐treatment comparison and this and other events (such as subsequent births) may have contributed to a lack of difference.
Two trials collected data on faecal incontinence in late pregnancy (Bø 2011; Stafne 2012). Bø 2011 also reported on faecal incontinence in the early postnatal period. There were no differences between PFMT and usual care groups at either time‐point (late pregnancy: RR 0.61, 95% CI 0.30 to 1.25; 2 trials, 867 women, fixed‐effect; moderate‐quality evidence; early postnatal: RR 0.36, 95% CI 0.04 to 3.37; 1 trial, 90 women) (Analysis 3.7; Analysis 3.8).
Incontinence‐specific quality of life
Four trials used a validated incontinence‐specific quality of life measure (Fritel 2015, ICIQ‐SF and Contilife (higher score better); Dokmeci 2008; Ko 2011, IIQ‐7; Hughes 2001, BFLUTS questionnaire). Fritel 2015 (ICIQ‐SF) found no difference in incontinence‐specific quality of life between PFMT and usual care groups at any of three time points (late pregnancy, early and late (late: MD ‐0.20, 95% CI ‐1 to 0.81; 190 women, low‐quality evidence) postnatal periods) (Analysis 3.13; Analysis 3.14; Analysis 3.15). However, all point estimates were in favour of the PFMT group. The two trials that reported IIQ‐7 scores had contrasting findings. Ko 2011 found better quality of life in the PFMT group at each of three time points (late pregnancy, early and mid‐postnatal) compared to no PFMT, whereas Dokmeci 2008 stated there were no "statistically significant" differences in late pregnancy or early postpartum (no data provided) between PFMT and unspecified controls (Analysis 3.18). The overall score in the trial by Hughes 2001 was not reported.
Secondary outcomes
Severity of incontinence
Two trials reported some data on symptom severity, such as frequency or amount of urine leakage. None of the data suggested that PFMT was superior to control, or vice versa, at the primary endpoint of either three months' postpartum (Hughes 2001) or 12 months' postpartum (Sampselle 1998).
Number of urinary or faecal incontinence episodes
None of the trials reported number of urinary or faecal incontinence episodes.
Loss of urine under stress test
The single trial reporting pad test data (24 hour) found no difference between PFMT and usual care groups (Analysis 3.17) (Fritel 2015).
Other quality of life and health status measures
Other quality of life and health status measures included:
-
Urogenital Distress Index‐Short Form (UDI‐6) (Dokmeci 2008; Ko 2011);
-
Female Pelvic Floor questionnaire (bladder, bowel, prolapse and sex scores; Fritel 2015);
-
Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ; higher score better) (Dokmeci 2008);
-
State Trait Anxiety Inventory (Miquelutti 2013);
-
Psychological General Wellbeing Index (Stafne 2012);
-
Euro‐QoL‐5D (Fritel 2015; higher score better).
There were no differences between groups for these other measures of well‐being (Analysis 3.18).
Three trials measured some aspect of sexual function in pregnancy, immediately postpartum and up to six years post‐index delivery (Dokmeci 2008; Fritel 2015; Mørkved 2003). Overall, there was no difference in sexual function or the proportion of women who were sexually active in late pregnancy and up to 12 months' postpartum (Dokmeci 2008; Fritel 2015). At six years, Mørkved 2003 found that PFMT women were twice as likely to report sexual satisfaction compared to controls (Analysis 3.18).
Health economics
None of the trials reported health economic data.
Adverse effects
Two trials reported no adverse effects (Fritel 2015; Miquelutti 2013).
Other outcomes
Pelvic floor muscle function
PFM function was measured using perineometry, electromyography and digital palpation (Assis 2015; Dokmeci 2008; Fritel 2015; Mørkved 2003). In the three trials that reported data, point estimates favoured PFMT women over controls (Assis 2015; Fritel 2015; Mørkved 2003). There were differences in favour of PFMT in both trials that measured vaginal squeeze pressures (Analysis 3.19) (Assis 2015; Mørkved 2003).
Delivery outcome
Six trials reported the number of caesarean sections, with no difference between groups (RR 0.95, 95% CI 0.79 to 1.14; 6 trials, 1899 women, fixed‐effect, I² = 25%, T² = 0.00) between PFMT and control groups (Analysis 3.20) (Bø 2011; Fritel 2015; Ko 2011; Miquelutti 2013; Mørkved 2003; Stafne 2012). Mørkved 2003 found no difference in the type of delivery, although women in the supervised antenatal PFMT group had a shorter second stage of labour. However, it is worth noting that fetal head circumference was also smaller in the PFMT group. Ko 2011 also reported rates of episiotomy among women and there was no difference between the groups (RR 0.86, 95% CI 0.53 to 1.39).
Participant satisfaction and further treatment
Fritel 2015 reported no difference between the groups in the proportion of women who wanted further supervised training at 12 months' postpartum, or in the number of medical visits since delivery between the PFMT and usual care groups (Analysis 3.22).
Comparison 4: postnatal pelvic floor muscle training for treatment of incontinence
Five trials reported postnatal PFMT for treatment of incontinence and provided supervised PFMT beginning at three or more months' postpartum as treatment for women with persistent urinary incontinence symptoms after delivery (Ahlund 2013; Dumoulin 2004; Glazener 2001; Kim 2012; Wilson 1998). The control group received usual care or were asked not to do PFMT (Ahlund 2013; Dumoulin 2004; Glazener 2001; Kim 2012; Wilson 1998).
Primary outcome
Self‐reported urinary or faecal incontinence
-
Women randomised to PFMT were about 22% less likely to have urinary incontinence after treatment compared to controls more than six and up to 12 months postdelivery (RR 0.78, 95% CI 0.69 to 0.87; 3 trials, 696 women, fixed‐effect). However, there was statistical heterogeneity in this comparison (I² = 90%) and when the more conservative random‐effects model was used there was no difference (RR 0.55, 95% CI 0.29 to 1.07; 696 women, I² = 90%, T² = 0.30; very low‐quality evidence) (Analysis 4.3).
Women in all three studies were recruited at three months or more postpartum. In the case of Dumoulin 2004, women were recruited after completing an incontinence questionnaire at their annual gynaecological visit, so it seems likely many were much more than three months' postpartum at trial entry. Therefore, after a further two months' intervention, it seemed likely the postintervention outcome was between six and 12 months' postdelivery for most. For this reason, a decision was made to present the data from the trial in the late postnatal category (greater than six to 12 months) along with that from Glazener 2001 and Wilson 1998, who both measured outcome 12 months postdelivery.
In addition to possible differences in timing of outcome measurement, there were other obvious dissimilarities between the three studies. In Dumoulin 2004, women randomised to the control group were specifically asked not to do any PFMT, while women in the control group in Glazener 2001 and Wilson 1998 received usual postnatal care and some did PFMT. Glazener 2001 reported a mean of 20 PFM contractions every day in the PFMT group versus five PFM contractions every day in the control group. A total of 86 (PFMT) versus 35 (control) were performed in the trial by Wilson 1998. The second difference was that Dumoulin 2004 employed a strengthening PFMT regimen which incorporated electrical stimulation and biofeedback, while participants also had weekly contact with a physiotherapist for eight weeks. In contrast, Glazener 2001 and Wilson 1998 did not clearly aim their PFMT regimens at either strength or endurance and in both studies the intervention group had three or four contacts with health professionals over a six‐month period.
Glazener 2001 reported urinary incontinence prevalence at six years (RR 0.96, 95% CI 0.88 to 1.05; 1 trial, 516 women) and 12 years after the index delivery (RR 1.03, 95% CI 0.94 to 1.12; 1 trial, 471 women), with no difference between PFMT and control group at either time‐point (Analysis 4.5; Analysis 4.6).
Two trials reported data on the prevalence of faecal incontinence one year after delivery (Glazener 2001; Wilson 1998). There was statistically significant heterogeneity, therefore a random‐effects model was used to give a more conservative estimate of effect (RR 0.68, 95% CI 0.24 to 1.94, random‐effects, I² = 74%, T² = 0.42; 2 trials, 620 women; very low‐quality evidence) (Analysis 4.9).
Glazener 2001 reported no difference in the prevalence of faecal incontinence at six years (RR 0.95, 95% CI 0.60 to 1.50; 509 women) and 12 years (RR 1.36, 95% CI 0.84 to 2.22; 1 trial, 468 women) post‐index delivery (Analysis 4.11; Analysis 4.12). At both these time points, Glazener 2001 reported that about 50% of women in both the intervention and control groups were doing "any" PFMT. When questioned about performing daily PFMT, it was interesting to note that only 6% of the PFMT group were exercising daily, compared to 12% of the control group at six years' follow‐up. After 12 years, 7% of the intervention group and 8% of the control group were performing daily PFMT (Table 1).
Incontinence‐specific quality of life
Two trials used incontinence‐specific quality of life measures (Dumoulin 2004: IIQ and UDI; Kim 2012: BFLUTS). Kim 2012 found no difference between PFMT and usual care groups post‐treatment (MD ‐1.66, 95% CI ‐3.51 to 0.19; 18 women) (Analysis 4.13). Dumoulin 2004 reported an improvement in IIQ and UDI score in women who were doing PFMT compared with women who were randomised to the control (no PFMT) group (Analysis 4.15).
Secondary outcomes
Severity of incontinence
All five treatment trials reported some data on incontinence severity, for instance frequency or amount of urine leakage. None of the measures, or the methods of reporting these, were common to the five trials. The data suggest that women randomised to PFMT with symptoms of urinary incontinence might have had less severe symptoms than women in the control groups but this was not a consistent or clear‐cut finding (Analysis 4.14).
Number of urinary or faecal incontinence episodes
None of the trials reported number of urinary or faecal incontinence episodes.
Loss of urine under stress test
None of the trials reported loss of urine under stress test.
Other quality of life and health status measures
Glazener 2001 used the Hospital Anxiety and Depression Scale to measure quality of life and found reduced anxiety in the PFMT group (Analysis 4.15).
Health economics
None of the trials reported health economic data.
Adverse effects
Dumoulin 2004 stated that none of the women in the PFMT group reported any adverse events (with PFMT or electrical stimulation).
Other outcomes
Pelvic floor muscle function
One trial measured PFM function using a dynamometer and three trials reported vaginal squeeze pressure (Ahlund 2013; Dumoulin 2004; Kim 2012; Wilson 1998). Dynamometer findings favoured the PFMT group, as did the vaginal squeeze pressure readings in two trials (Analysis 4.16) (Ahlund 2013; Dumoulin 2004; Kim 2012).
Any other outcome not prespecified but of interest
Wilson 1998 noted that the mean time to teach PFMT to the intervention group was 32 minutes (95% CI 30 to 34) but no further economic analysis was reported (Table 1).
Comparison 5: postnatal pelvic floor muscle training for mixed prevention and treatment of incontinence
Ten trials reported postnatal PFMT for mixed prevention and treatment of incontinence (Chiarelli 2002; Ewings 2005; Frost 2014; Hilde 2013; Kou 2013; Liu 2011; Meyer 2001; Peirce 2013; Sleep 1987; Wen 2010). These randomised women to postnatal PFMT versus usual care with the exception of one, in which the controls were asked to do no exercise (Meyer 2001). The trials recruited previously nulliparous women during their first pregnancy (Meyer 2001), women having their first baby (Hilde 2013; Liu 2011; Peirce 2013), or postnatal women of mixed parity (Chiarelli 2002; Ewings 2005; Sleep 1987). Three trials did not report this information (Frost 2014; Kou 2013; Wen 2010).
Primary outcome
Self‐reported urinary or faecal incontinence
The only information from the early postnatal period was from Frost 2014, a conference abstract. This trial did not contribute any data to the review but the authors stated that there were no significant differences in "urinary symptoms" at six to eight weeks' postpartum between the PFMT and control (usual care) groups.
There was no difference in the prevalence of urinary incontinence in women randomised to postnatal PFMT or control group in the:
-
mid‐postnatal period, up to six months (RR 0.95, 95% CI 0.75 to 1.19, random‐effects, I² = 65%, T² = 0.04; 5 trials, 2800 women) (Analysis 5.2) or
-
late postnatal period, more than six to 12 months (RR 0.88, 95% CI 0.71 to 1.09, fixed‐effect, I² = 50%, T² = 0.00; 3 trials, 826 women; very low‐quality evidence) (Analysis 5.3).
There was statistically significant heterogeneity in both comparisons. There was no detail of the PFMT programmes in three of the five trials contributing data to the mid‐postnatal comparison (Ewings 2005; Meyer 2001; Sleep 1987). In addition, there were other notable dissimilarities, including the risk profile of the recruited population (e.g. Chiarelli 2002) and the degree of contrast between PFMT and control groups in exercise supervision and prescription (e.g. Sleep 1987, low contrast; Kou 2013, high contrast). In the two trials with findings in favour of PFMT, the control groups were offered usual care, while the PFMT interventions were intensively supervised or enhanced with application of health behaviour theory (Chiarelli 2002; Kou 2013). In addition, Chiarelli 2002 recruited women who were at potentially increased risk of postnatal incontinence, such as those who had a large baby or a forceps delivery.
There was considerably less difference in PFMT and control groups in the other three trials for various reasons and none found a difference between the groups. All control groups received usual postnatal care that may have or did include information about PFMT. Ewings 2005 reported that 114/117 women randomised to PFMT received one‐to‐one instruction on PFMT but only 21 attended one group class, with five attending both available classes. There was no difference between groups. Hilde 2013 randomised women to PFMT delivered in a weekly exercise class plus home exercise, versus a home exercise control condition. Both groups had a correct PFM contraction confirmed prior to training. Sleep 1987 randomised women within 24 hours of delivery to an individual daily session with a midwife co‐ordinator while in hospital and home exercise, versus usual care that included postnatal classes taken by an obstetric physiotherapist. At three months' postpartum, the proportion of women doing PFMT was reasonably similar (58% with PFMT and 42% with control).
Chiarelli 2002 and Kou 2013 also contributed data to the late postpartum comparison with the addition of that from Meyer 2001. Women in the study by Meyer 2001 were randomised to either eight months of supervised PFM rehabilitation with a physiotherapist or no PFMT. Like Kou 2013, there was a high degree of contrast between the PFMT and control groups. However, unlike Kou 2013, Meyer 2001 found no difference between groups in the prevalence of urinary incontinence. Neither of these trials reported details of their randomisation procedures.
Two trials reported the prevalence of postnatal faecal incontinence (Meyer 2001; Sleep 1987). Neither demonstrated a difference between PFMT and control groups (at more than six to 12 months: RR 0.73, 95% CI 0.13 to 4.21; 1 trial, 107 women; very low‐quality evidence) (Analysis 5.6; Analysis 5.7; Analysis 5.8).
Incontinence‐specific quality of life
One of the 10 trials reported incontinence‐specific quality of life data, with no differences between PFMT and controls for faecal incontinence (Analysis 5.10; Analysis 5.13; Peirce 2013).
Secondary outcomes
Severity of incontinence
Four trials reported some data on symptom severity (Hilde 2013; Liu 2011; Sleep 1987; Wen 2010).
At three months' postpartum, Sleep 1987 found no difference between the groups in frequency of leakage or the number of women using absorbent pads (often or always), whereas Liu 2011 reported less severe urinary incontinence (unspecified measure) in the PFMT group (Analysis 5.11).
Number of urinary or faecal incontinence episodes
None of the trials reported number of urinary or faecal incontinence episodes.
Loss of urine under stress test
At six months' postpartum, Hilde 2013 found no difference between the groups for amount of leakage on pad test and the results for unspecified urinary incontinence severity were inconsistent (Liu 2011; Wen 2010). Pooled data from two studies found no difference in the risk of positive pad test between PFMT compared to usual care (RR 0.96, 95% CI 0.58 to 1.57; 2 trials, 85 women, fixed‐effect, I² = 0%) (Analysis 5.12) (Hilde 2013; Wen 2010). At 12 months, unspecified urinary incontinence severity was less in the PFMT group compared to usual care and fewer women in the PFMT groups had a positive pad test (Wen 2010).
Other quality of life and health status measures
Two trials measured some aspect of sexual function (Meyer 2001; Sleep 1987). Meyer 2001 noted fewer women in the PFMT group reported a diminished vaginal sexual response at 10 months' postpartum, while Sleep 1987 found no difference between groups in the proportion of women who had attempted or had pain with sexual intercourse at three months' postpartum (Analysis 5.13).
Health economics
None of the trials reported health economic data.
Adverse effects
Two trials collected data on adverse events, with none reported in either group or in those using biofeedback as an adjunct to PFMT (Hilde 2013; Peirce 2013).
Other outcomes
Pelvic floor muscle function
Two studies measured PFM function using the Oxford scale (Liu 2011; Wen 2010). The outcomes at three, six and 12 months' postpartum were in favour of the PFMT group compared to usual care. Three trials assessed vaginal squeeze pressure at six, 10 and 12 months' postpartum and found no difference between the groups (Hilde 2013; Kou 2013; Meyer 2001). Two trials measured anal pressure, in cm of water (Meyer 2001) or mmHg (Peirce 2013), and neither found a difference between PFMT and control groups (Analysis 5.14).
Any other outcome not prespecified but of interest
One trial measured pelvic organ prolapse symptoms at six months' postpartum and found no difference between the groups (Analysis 5.15) (Hilde 2013).
Discussion
This review considers whether PFMT (as defined by the trialists) is better than usual antenatal or postnatal care for the prevention and treatment of urinary and faecal incontinence in childbearing women. Another Cochrane Review addressed a similar question (whether PFMT was better than no treatment, placebo or inactive control treatments) in women with urinary incontinence (Dumoulin 2014). This review specifically excluded trials that recruited antenatal or postnatal women.
Summary of main results
Is pelvic floor muscle training better than usual antenatal or postnatal care for the prevention and treatment of urinary and faecal incontinence?
There are three possible ways of delivering PFMT interventions to women during pregnancy and in the postpartum period. The first way is to provide PFMT for women who have no symptoms when PFMT begins (i.e. prevention). The second is to prescribe PFMT for women who have already developed symptoms of incontinence (i.e. treatment). The third is to provide PFMT for all women regardless of whether they have urinary incontinence symptoms or not when PFMT begins (i.e. mixed prevention and treatment approach). Comparisons were drawn within the following three populations of women.
-
Women who were continent when randomised to intervention groups, that is, prevention studies.
-
Women who were incontinent at randomisation, that is, treatment studies.
-
Trials including a mixed population, that is, some women were continent and some women were incontinent at randomisation.
Primary or secondary prevention of incontinence
Summary data from six trials suggested that PFMT during pregnancy decreased urinary incontinence in late pregnancy compared to usual care (RR 0.38, 95% CI 0.20 to 0.72; 624 women; low‐quality evidence). At between three months and up to six months following delivery (mid‐postpartum), summary data from five trials suggested that PFMT decreased the prevalence of urinary incontinence compared to usual care (RR 0.71, 95% CI 0.54 to 0.95; 673 women; moderate‐quality evidence). With only subgroup data from one small trial of 72 women, there were too few data from six months to one year after delivery (late postpartum) to comment meaningfully (Sampselle 1998). A single trial of 152 women suggested PFMT probably improved incontinence‐specific quality of life in late pregnancy compared to usual care (ICIQ‐SF: MD ‐2.42 , 95% CI ‐3.32 to ‐1.52 ; moderate‐quality evidence) (Pelaez 2014). None of the trials reported data on faecal incontinence in late pregnancy, or in the mid‐ and late postpartum periods (summary of findings Table for the main comparison).
Two trials conducted a long‐term follow‐up of participants at eight and six years with no difference between PFMT and control groups (Analysis 1.6) (Mørkved 2003; Reilly 2002).
Treatment of incontinence
We expressed uncertainty about the effects of PFMT for treatment of urinary incontinence in antenatal and postnatal women below. The uncertainty arose from the lack of precision in the pooled estimate of effect; the CIs for the summary statistic were generally wide, and included a null effect.
Antenatal women
Based on summary data from three trials, we are uncertain whether PFMT decreased existing urinary incontinence in late pregnancy compared to usual care (RR 0.70, 95% CI 0.44 to 1.13; 345 women; very low‐quality evidence). We are equally uncertain whether PFMT to treat antenatal urinary incontinence reduced urinary incontinence in the mid‐ (RR 0.94, 95% CI 0.70 to 1.24; 1 trial, 187 women; very low‐quality evidence) or late (RR 0.50, 95% CI 0.13 to 1.93; 2 trials, 869 women; very low‐quality evidence) postnatal periods. Data from a single trial of 41 women suggested that PFMT may have improved incontinence‐specific quality of life in late pregnancy compared to usual care (ICIQ‐SF: MD ‐3.50, 95% CI ‐6.13 to ‐0.87; low‐quality evidence) (Cruz 2014). None of the trials reported data on faecal incontinence in late pregnancy, or in the mid‐ and late postpartum periods in this comparison (summary of findings Table 2). Evidence in this comparison was particularly weak, with all trials limited by incomplete reporting of intervention and control conditions and trial methods. Two trials in this comparison were reported only as conference abstracts.
Postnatal women
Based on summary data from three trials, we were uncertain whether PFMT to treat postnatal urinary incontinence reduced urinary incontinence in the late postnatal period (RR 0.55, 95% CI 0.29 to 1.07; 696 women; very low‐quality evidence). We noted that two of the three trials that carried the greatest weighting in the pooled estimate compared PFMT (with limited supervision by a healthcare professional) with usual care and some women in the control groups were doing PFMT (Glazener 2001; Wilson 1998). There was no difference between groups in Wilson 1998 and close to no difference in Glazener 2001. In the third trial, Dumoulin 2004 compared a shorter and more intensively supervised PFMT intervention with no treatment and found a reduction in the risk of urinary incontinence in favour of PFMT. Based on the data from a single very small trial, we were uncertain whether urinary incontinence‐specific quality of life after treatment was improved with PFMT (BFLUTS: MD ‐1.66 , 95% CI ‐3.51 to 0.19; 18 women; very low‐quality evidence) (Kim 2012). Likewise, based on summary data from two trials, we are uncertain whether PFMT reduces faecal incontinence in the late postnatal period compared to usual care (RR 0.68, 95% CI 0.24 to 1.94; 620 women; very low‐quality evidence) (Glazener 2001; Wilson 1998) (summary of findings Table 4).
Glazener 2001 carried out long‐term follow‐up of women at six and 12 years after the initial study. There was no difference in the prevalence of urinary incontinence between the PFMT and control groups at either of these time points suggesting that the possible benefits of PFMT were not upheld in the long term. Glazener and colleagues also measured faecal incontinence atsix and 12 years after delivery. These results did not show a difference but the CIs were wide, highlighting the need for more evidence in this area.
Trials with a mixed prevention and treatment approach
Antenatal women
Summary data from nine trials suggested that antenatal PFMT, delivered to a population of women with or without existing urinary incontinence symptoms, may have decreased the prevalence of urinary incontinence in late pregnancy (RR 0.74, 95% CI 0.61 to 0.90; 3164 women; low‐quality evidence). The two trials that compared PFMT to no training seemed to show a greater effect than the other seven trials that compared PFMT and usual care (Assis 2015; Ko 2011). Summary data from the mid‐postnatal period also favoured PFMT over control, although there was uncertainty about this effect (RR 0.73, 95% CI 0.55 to 0.97; 5 trials, 1921 women; very low‐quality evidence). Two trials reported data on urinary incontinence in the late postpartum period and there may have been no difference in urinary incontinence prevalence between PFMT and usual care, although there was uncertainty about this effect (RR 0.85, 95% CI 0.63 to 1.14; 244 women; low‐quality evidence).
Similarly, antenatal PFMT may have led to little or no difference in the prevalence of faecal incontinence in late pregnancy (RR 0.61, 95% CI 0.30 to 1.25; moderate‐quality evidence). There were no data for the prevalence of faecal incontinence in the mid‐ or late postnatal periods in this comparison. A single trial (ICIQ‐SF: MD ‐0.20, 95% CI ‐1.21 to 0.80; 190 women; low‐quality evidence) found that antenatal PFMT may have led to little or no difference in incontinence‐specific quality of life in the late postnatal period compared to usual care (Fritel 2015). However, it is important to note that in Fritel 2015, women in both groups reported a similar frequency and duration of PFMT (including the number of contractions) at the end of pregnancy. This suggested that the lack of difference between groups was because the control group was routinely doing adequate PFMT, which was encouraging in terms of delivering PFMT to the general population (summary of findings Table 3).
Postnatal women
Based on summary data from three trials, we were uncertain whether postnatal PFMT, delivered to a population of women with or without existing urinary incontinence symptoms, reduced urinary incontinence in the late postnatal period (RR 0.88, 95% CI 0.71 to 1.09; 826 women; very low‐quality evidence). We were equally uncertain whether PFMT reduced faecal incontinence in the late postnatal period compared to no PFMT (RR 0.73, 95% CI 0.13 to 4.21; 1 trial, 107 women; very low‐quality evidence) (Meyer 2001). There were no incontinence‐specific quality of life data in this comparison (summary of findings Table 5).
Delivery outcomes
Few adverse events were reported with PFMT. However, it was possible that PFMT during pregnancy might influence labour and delivery outcomes. This did not seem to be the case based on data from nine antenatal PFMT trials included in this review.
Three of the antenatal PFMT trials for the prevention of incontinence reported on delivery outcome (Barakat 2011; Gaier 2010; Gorbea 2004). The risk of caesarean section was not different (RR 1.28, 95% CI 0.89 to 1.85; 373 women) (Analysis 1.19). Gaier 2010 reported data on rates of episiotomy, with the control group receiving more episiotomies than the PFMT group, while Barakat 2011 reported rates of perineal trauma with no apparent difference in grades of perineal tear between the groups (Analysis 1.20).
Six of the antenatal PFMT trials for mixed prevention and treatment of incontinence reported on delivery outcome (Bø 2011; Fritel 2015; Ko 2011; Miquelutti 2013; Mørkved 2003; Stafne 2012). The risk of caesarean section was not different (RR 0.95, 95% CI 0.79 to 1.14; 1899 women) (Analysis 3.20). None of the three trials that reported data for the risk of assisted vaginal deliveries found a difference between the PFMT and control groups (Analysis 3.21) (Fritel 2015; Mørkved 2003; Stafne 2012). Two trials reported data on rates of episiotomy, with the control group receiving more episiotomies than the PFMT group (Analysis 3.21) (Ko 2011; Mørkved 2003). Du 2015 published a non‐Cochrane systematic review of antenatal PFMT and delivery outcomes where their findings appeared consistent with the above. Their review included more studies, as it contained trials that did not collect urinary incontinence or faecal incontinence data.
There were no data on labour or delivery outcomes reported in any of the trials of antenatal PFMT for treatment of incontinence.
Overall completeness and applicability of evidence
The self‐report measures of urinary and faecal incontinence were considered the most important outcomes in this review. However, there was variability in the way urinary and faecal incontinence were defined, how the questions were asked and how the data were presented. There were few incontinence‐specific quality of life data and little agreement about a standard measure. Further, some trials only partially reported a score (e.g. one domain of several included in the total score) or a statement about difference or lack of it, sometimes with a P value, as these data were collected but not reported or only partially reported this is a form of reporting bias.
Unfortunately, faecal incontinence data were rarely collected in the prevention or mixed prevention and treatment trials; only six studies presented data. Being a less common event than urinary incontinence, larger trials are needed to accurately document the effect of PFMT on this outcome and more trials must collect these data to enable a more precise effect estimate based on pooled data.
The usefulness of evidence was somewhat reduced by the short durations of follow‐up after intervention. This was particularly problematic in the antenatal PFMT trials, where the outcome was either measured at the end of pregnancy or in the three months postbirth. At three months' postpartum, there may not have been full resolution of many of the physiological changes associated with pregnancy and childbirth. A minimum follow‐up of six months postnatally is probably more useful to be sure how many cases of urinary or faecal incontinence are persistent. For treatment studies, while a postintervention measure is useful, data on the duration of effect (e.g. one year or longer) are needed. With regard to longer‐term follow‐up, only three studies provided data after five years (Glazener 2001; Mørkved 2003; Reilly 2002). Longer‐term data are difficult to interpret, as control groups may be offered a structured PFMT after the postintervention outcome is measured, women may have more children and so on. However, in the absence of longer‐term data about urinary and faecal incontinence and other variables (parity, bodyweight, etc.), there is an insufficient evidence base to begin to analyse and interpret.
Pregnancy and birth appear to be the most consistent and important factors associated with the development of urinary and faecal incontinence in women. Therefore, all women who have a child, or children, might be considered at risk of later incontinence. In addition, some women (such as those who have a connective tissue disorder, high BMI or an assisted delivery) might be at even greater risk (Durnea 2017; Svare 2014). The bulk of trials reviewed were undertaken in samples of antenatal women, principally those in their first pregnancy and most data were for urinary incontinence. The findings suggested that continent antenatal women benefited more from "structured" PFMT programmes (in terms of content and delivery) than women in usual care groups that may have incorporated some (or ad hoc) PFMT advice or teaching.
Trials of antenatal PFMT for mixed prevention and treatment also mostly recruited women having their first baby and showed a similar pattern of benefit of structured PFMT versus control conditions. However, the pooled data suggested less reduction in risk of urinary incontinence, upper CIs closer to one (i.e. no reduction in risk of urinary incontinence) and overall there was also more uncertainty about the effect.
Efforts to determine what value women, healthcare professionals and their professional organisations, provider and funding bodies give to this body of evidence about urinary incontinence prevention through structured and supervised antenatal PFMT (at least for first‐time mothers) are warranted. If the findings are considered sufficiently certain and of value, then changes to the current ad hoc delivery of PFMT advice in pregnancy within 'usual care' are needed. Alongside this, and to inform any decisions about the 'value' of antenatal PFMT for prevention of incontinence, investigations into health economics are needed. In the absence of such studies, there is no evidence about value for money. It is encouraging that one ongoing study identified in the search planned to collect and report economic data (Berghmans 2016).
We summarised data from all the trials. There were a few that we considered informed us enough about what was done in both PFMT and control groups that we were more confident in the estimate of differences in outcome. These were trials where sufficient information was provided about the intervention and control conditions such that it was possible to reach a judgement about:
-
the soundness of the physiology of the PFMT (i.e. whether the structured PFMT intervention was likely to strengthen muscle);
-
exercise behaviour in both groups (i.e. were both groups doing similar or quite different amounts of PFMT);
-
the degree of contrast between the two groups (e.g. did the PFMT group attend many exercise classes while the control group had none (high contrast), or did the PFMT group have one instruction session and the controls had none (low contrast)) (see Table 1 and Potential biases in the review process (heterogeneity)).
Four trials contained the necessary amount of information (Chiarelli 2002; Hilde 2013; Reilly 2002; Stafne 2012). All were at low risk of selection bias and had moderate to large sample sizes. Two examined the effect of antenatal PFMT for prevention of urinary and faecal incontinence (Reilly 2002; primiparous women with bladder neck hypermobility) and mixed prevention and treatment (Stafne 2012; healthy pregnant women, mixed parity) and two the effect of postnatal PFMT for mixed prevention and treatment of urinary and faecal incontinence (Chiarelli 2002, mixed parity, after ventouse or forceps delivery or baby weighing 4000 g or greater; Hilde 2013, primiparous women after vaginal delivery). Looking at the GRADE rated outcomes, data from these individual trials were consistent with the pooled estimates of effect. Antenatal training appeared to have clinically important reductions in urinary incontinence in late pregnancy and between more than three to six months postnatally (Reilly 2002; Stafne 2012). The effect of postnatal training for mixed prevention and treatment may not be clinically important at more than three to six months after delivery for urinary incontinence (Chiarelli 2002; Hilde 2013). However, it is possible that women at higher risk of postnatal incontinence benefited more (Chiarelli 2002).
Quality of the evidence
Overall, the evidence was moderate, low or even very low quality (see summary of findings Table for the main comparison; summary of findings Table 2; summary of findings Table 3; summary of findings Table 4; summary of findings Table 5). The most common reasons for downgrading the evidence were:
-
imprecision, with few overall events contributing to the pooled analysis and wide CIs around the estimates of effect;
-
inconsistency, because many of the meta‐analyses demonstrated statistically significant heterogeneity (Chi² test P < 0.10) or had an I² > 50%;
-
indirectness, due to lack of clear reporting of the PFMT intervention or the control condition or both.
Some comparisons were downgraded for selection bias, arising from inadequate reporting of random sequence generation and random allocation. Most comparisons in the 'Summary of findings' tables were affected by more than one of the above and were downgraded twice or three times.
Trial quality and reporting
We evaluated methodological quality from the trial reports, which was limited when the only source of publication was from an abstract (see Included studies). In addition, abstracts reported few data.
The adequacy of reporting randomisation remains disappointing as fewer than half of the included trials reported both random sequence generation and allocation concealment and 13/38 studies described neither. The nature of the intervention means it was not feasible to blind the treatment provider or participants to group allocation (performance bias) in any of the included trials. The difficulty of blinding exercise‐based interventions is unavoidable. Furthermore, it is impossible to blind either of the primary outcomes in the review because both were self‐reported (prevalence of urinary incontinence or faecal incontinence and incontinence‐specific quality of life). Approximately three‐quarters of the trials (28/38) had a low risk of reporting bias but only just over half (21/38) were deemed to be low risk in terms of potential sources of other biases (Figure 2; Figure 3).
Based on the reported adequacy of randomisation, proportion and management of participant dropouts and withdrawals, and low risk of selective reporting or other biases, six trials appeared to be at low risk of bias (Chiarelli 2002; Dumoulin 2004; Hilde 2013; Mørkved 2003; Peirce 2013; Sangsawang 2016). However, this assessment did not take into account the quality of descriptions of the PFMT interventions or control conditions. If this was taken into account, the trial by Sangsawang 2016 would be downgraded in quality, as the intervention was of short duration and insufficient information was provided to determine the likely physiological effect of the PFMT. Sensitivity analysis on the basis of trial quality was not considered appropriate in view of the small number of trials contributing to each comparison.
Potential biases in the review process
We combined data from a diverse set of studies. This may inevitably impact on the applicability of our findings to practice. We summarise below the issues related to the heterogeneity of the studies we used.
Sources of heterogeneity
There were three notable sources of clinical heterogeneity. These were the variation in baseline characteristics (e.g. parity, type of delivery, type and duration of incontinence, if women were symptomatic when recruited), the PFMT programmes and the control care. To investigate the effects of baseline characteristics on treatment outcome would require an individual participant data meta‐analysis, which was beyond the scope of this review.
Variability of pelvic floor muscle training regimens
The content of PFMT programmes was often poorly described. Downgrading the evidence on the basis of inconsistency and indirectness was therefore inevitable in view of lack of information about PFMT and control conditions, PFMT content, and supervision of exercise programmes (see 'Summary of findings' tables).
More than half the trials provided insufficient information to be sure of the likely physiological effect of the exercise and only half reported confirmation of a correct PFM contraction prior to training (see PFMT regimens and control interventions, Included studies and Table 1). Consequently, it was difficult to evaluate the potential physiological efficacy of the exercise programmes. Including trials with a suboptimal exercise regimen alongside those with a sufficient regimen could adversely influence the pooled estimate of PFMT effect.
Alongside the physiological efficacy of the exercise, support for the behavioural aspects of exercise is also required. Behavioural support is commonly provided through supervision of exercise, and the extent of this varied markedly between trials. The least supervision was either one group or individual session to introduce the PFMT and the most was a mean of 85 classes between the sixth to 39th week of pregnancy (Table 1). Attendance was sometimes used as a surrogate for measuring adherence. It may be a good measure of adherence if the number of required attendances was sufficient to strengthen the PFM (Haskell 2007). However, if clinic attendance was less than twice per week, then it was likely that additional training needed to be completed at home to achieve a sufficient exercise regimen. Measurement of home exercise adherence then becomes a critical component of assessing the likely efficacy of the training. Half of the included trials reported some type of adherence data for women in the intervention or control groups but only nine studies asked women in both PFMT and control groups about their exercise behaviour (see Included studies). Adherence data should be collected in both study groups, although it is acknowledged that measuring it may change exercise behaviour. In turn, this may lead to an overestimate of the likely effect in 'real' life and may diminish the difference in effect between structured PFMT and control conditions.
Assessment of the interaction between quality and the effect of the intervention has been recommended but there were too few trials to conduct a formal sensitivity analysis by intervention quality (Herbert 2005). Rather than excluding or including trials on the basis of sufficiency of PFMT, or the likelihood that a clear‐cut comparison between PFMT and the control condition had been made, the preferred approach would be a sensitivity analysis on the basis of PFMT programme characteristics or amount of clinical difference between the PFMT and control interventions. However, more trials would be needed in each of the comparisons in the review before this was possible. We tried to distil information about the physiological and behavioural quality of the PFMT interventions, alongside the degree of contrast between the PFMT and control groups (see 'Sample characteristics' in Included studies and Summary of main results).
Variability of control conditions
The control conditions were also highly variable and usually poorly described, with many including a blanket statement about women in control groups receiving usual or standard care. However, it often it was unclear whether usual care encompassed advice about PFMT (i.e. written or verbal instructions) or a more ad hoc arrangement (see 'Sample characteristics' in Included studies, and Table 1).
Agreements and disagreements with other studies or reviews
The overall findings and conclusions in this updated review are generally the same as the previous version, despite this update containing more trials and substantially more data than the previous review and integrating the GRADE scores for assessing the quality of evidence (Boyle 2012). Since the last update of this review in 2012, one non‐Cochrane systematic review on the effects of PFMT during pregnancy and postpartum for the prevention and treatment of urinary incontinence has been published (Mørkved 2014). Although Mørkved 2014 considered the data in slightly different categories, they reported that PFMT during pregnancy and after delivery was effective in treating and preventing urinary incontinence, particularly when women adhered to a strength‐training protocol and were closely supervised. The findings of this review agreed with those of Mørkved 2014 relating to methodological factors such as the heterogeneity of the populations in the included trials, differences in reported outcome measures, and considerable variation in the PFMT and control conditions between trials.

PRISMA study flow diagram.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 1 Urinary incontinence in late pregnancy.

Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 2 Urinary incontinence early postnatal period (0‐3 months).

Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 3 Urinary incontinence mid‐postnatal period (> 3‐6 months).

Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 4 Urinary incontinence late postnatal period (> 6‐12 months).

Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 6 Urinary incontinence long term (> 5 years).

Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 13 Incontinence‐specific quality of life.
| Study | Measure of | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus no PFMT | |||||
| Stothers 2002 | Frequency of leakage | Leakage episodes in 5 days | Mean 3.4, SD not reported, n=7 at 6 months postpartum | Mean 6.0, SD not reported, n=8 at 6 months postpartum | Not calculable |
| Stothers 2002 | Amount of leakage | Volume of urine loss (g) on stress test with standardised bladder volume | Mean 18, SD not reported, n=? at 6 months postpartum | Mean 38, SD not reported, n=? at 6 months postpartum | Not calculable |
| Stothers 2002 | Other leakage severity | Not measured | |||
| PFMT versus usual care | |||||
| Gorbea 2004 | Frequency of leakage | Less than weekly, weekly or daily urinary incontinence (not clear if self‐reported or from urinary diary) | 4 less than weekly, 2 weekly and none with daily leakage, n=38 at 6 weeks postpartum | 6 less than weekly, 8 weekly and 2 with daily leakage, n=34 at 6 weeks postpartum | Not calculated as validity/reliability of this measure not known |
| Gorbea 2004 | |||||
| Gorbea 2004 | Other leakage severity | Grade I, II or III leakage, where I=loss of urine with coughing or lifting, II=urine leakage when walking, and III=urine leakage when upright | 6 grade I, and none with grade II or III leakage, n=38 at 6 weeks postpartum | 10 grade I, 6 grade II, and none grade III leakage, n=34 at 6 weeks postpartum | Not calculated as validity/reliability of this measure not known |
| Pelaez 2014 | Frequency of leakage | Self‐reported leakage frequency categorised as never, once a week, 2‐3 times a week, once a day, several times a day, all the time (item 3, ICIQ‐SF) | 60 never, 3 once a week, n=63 at 36‐40 weeks gestation | 54 never, 18 once a week, 9 2‐3 times a week, 7 once a day, 1 several times a day, n=89 | Author reported p‐value 0.0001 |
| Pelaez 2014 | Amount of leakage | Self‐reported amount of leakage categorised as none, small, moderate, large (item 4, ICIQ‐SF) | 60 none, 3 small, n=63 at 36‐40 weeks gestation | 54 report none, 27 a small, 5 moderate, 3 large, n=89 | Author reported p‐value 0.0001 |
| Pelaez 2014 | Symptom bother | Symptom impact, numbered VAS 0‐10 (10 worse) (item 5, ICIQ‐SF) | Mean 0.10, SD 0.64, n=63 | Mean 0.97, SD 1.8, n=89 | Mean difference ‐0.87 (95% CI ‐1.28 to ‐0.46) |
| Reilly 2002 | Incontinence‐specific quality of life | King's Health Questionnaire | Not reported | Not reported | "No difference between the study groups on any of the 8 scales, and all mean scores were low" |
| Reilly 2002 | |||||
| Reilly 2002 | Other leakage severity | Mild, moderate or severe urinary incontinence (not clear how categorised) | 19 mild, 3 moderate and 1 severe, n=74 at 3 months postpartum | 30 mild, 5 moderate and 1 severe, n=74 at 3 months post partum | Not calculated as validity/reliability of this measure not known |
| Sampselle 1998 | Frequency of leakage | Not measured | |||
| Sampselle 1998 | Amount of leakage | Not measured | |||
| Sampselle 1998 | Other leakage severity | Average score from questionnaire re urine leakage with gentle cough, hard cough, sneeze and laugh scored 0 for none, 1 for dampness, 2 for wetness and 3 for soaked | Mean 0.30, standard deviation 0.44, n=16 at 12 months postpartum | Mean 0.32, standard deviation 0.41, n=21 at 12 months postpartum | Not calculated as validity/reliability of this measure not known |
| Sangsawang 2016 | Frequency of leakage | Bladder diary, number of leakages per week | Mean 12.4, SD 5.3, n=9 of 33 at 38 weeks gestation | Mean 23.1, SD 5.7, n=16 of 30 at 38 weeks gestation | Mean difference ‐8.9 (95% CI ‐13.7 to ‐4.0) |
| Sangsawang 2016 | Amount of leakage | Self‐reported: none, small (drops), moderate (wetting underwear), large (wetting outer clothing) | None 24, small 2, moderate 4, large 3 | None 14, small 2, moderate 8, large 6 | Author reported p‐value 0.03 |
| Sangsawang 2016 | Other leakage severity | Perceived severity on VAS (0‐10) | Mean 5.0, SD 0.9, n=9 of 33 | Mean 6.3, SD 1.2, n=16 of 30 | Mean difference ‐2.0 (95% CI ‐3.4 to ‐0.6) |
| PFMT versus unspecified control | |||||
| Barakat 2011 | Frequency of leakage | Self‐reported leakage frequency categorised as never, once a week, 2‐3 times a week, once a day, several times a day, all the time (item 3, ICIQ‐SF) | 24 never, 5 once a week, 2 2‐3 times a week, 2 once a day, 1 several times a day, n=34 | 22 never, 5 once a week, 1 2‐3 times a week, 2 once a day, 3 several times a day, n=33 | Author reported p‐value >0.05 |
| Barakat 2011 | Amount of leakage | Self‐reported amount of leakage categorised as none, small, moderate, large (item 4, ICIQ‐SF) | Not reported | Not reported | |
| Barakat 2011 | Other leakage severity | ||||
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 14 Severity of incontinence.
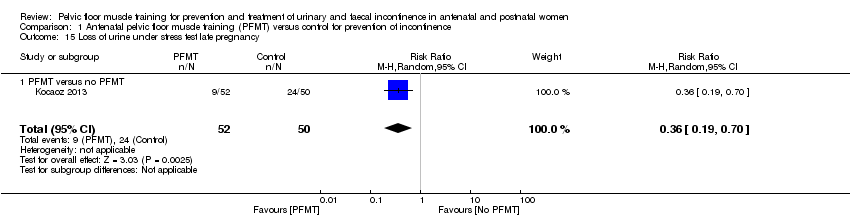
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 15 Loss of urine under stress test late pregnancy.

Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 16 Loss of urine under stress test early postnatal period (0‐3 months).
| Study | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus usual care | ||||
| Reilly 2002 | SF‐36, general health scale (0=worst, 100=best) | Mean 84.4, SD 13.5, n=76 | Mean 77.2, SD 16.3, n=72 | Mean difference 7.2 (95% CI 12.04, 2.36) |
| PFMT versus unspecified control | ||||
| Barakat 2011 | Maternal perception of health status (presume an item derived from SF‐36). Rated as very bad, somewhat bad, good or very good | 1 very bad, 14 good, 18 very good, n=34 | 1 very bad, 5 somewhat bad, 18 good, 9 very good, n=33 | |
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 17 Quality of life and health status measures.
| Study | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus no PFMT | ||||
| Gorbea 2004 | No or minimal contraction on electromyography. Not clear what type of electromyography or how categorised | 14 of 14 at 6 weeks postpartum | 10 of 12 at 6 weeks postpartum | Not calculated as validity/reliability of this measure not known |
| PFMT versus usual care | ||||
| Gaier 2010 | PF muscle strength (measure not reported) | Significantly higher in the training group at 12 | ||
| Reilly 2002 | Vaginal squeeze pressure (need unit of measurement), early post‐natal | Mean 11.5, SD 7.8, n=68 | Mean 10.5, SD 5.5, n=64 | Mean difference 1.0 (95% CI ‐1.31 to 3.31) |
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 18 Pelvic floor muscle function.

Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 19 Delivery outcome: caesarean section.
| Study | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus no control | ||||
| Stothers 2002 | Type of delivery | 73.3% vaginal, 26.7% caesarean; not reported per group | ||
| Stothers 2002 | ||||
| PFMT versus usual care | ||||
| Gaier 2010 | Number with episiotomy | 2 of 65 | 6 of 62 | Relative risk 0.32 (95% CI 0.07 to 1.52) |
| Gaier 2010 | Perineal trauma | 0.5% | 4.2% | Unable to calculate |
| Reilly 2002 | Type of delivery | 78 normal vaginal, 13 ventouse, 8 forceps, n=120 | 72 normal vaginal, 22 ventouse, 2 forceps, n=110 | Relative risk for normal vaginal delivery 0.99 (95% CI 0.82 to 1.20) Relative risk for assisted vaginal delivery 0.80 (95% CI 0.47 to 1.36) |
| Reilly 2002 | ||||
| PFMT versus unspecified control | ||||
| Barakat 2011 | Type of delivery | 20 normal vaginal, 7 assisted vaginal, n=34 | 18 normal vaginal, 5 assisted vaginal, n=33 | Relative risk for normal vaginal delivery 1.08 (95% CI 0.71 to 1.64) Relative risk for assisted vaginal delivery 1.36 (95% CI 0.48 to 3.86) |
| Barakat 2011 | Perineal trauma | 22 intact perineum, 6 grade 1 tear, 5 grade 2 tear, 1 grade 3 tear, n=34 | 19 intact perineum, 6 grade 1 tear, 8 grade 2 tear, 0 grade 3 tear, n=33 | Relative risk for perineal tear 0.83 (95% CI 0.45 to 1.52) |
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 20 Delivery outcome: other.

Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 1 Urinary incontinence late pregnancy.

Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 2 Urinary incontinence early postnatal period (0‐3 months).
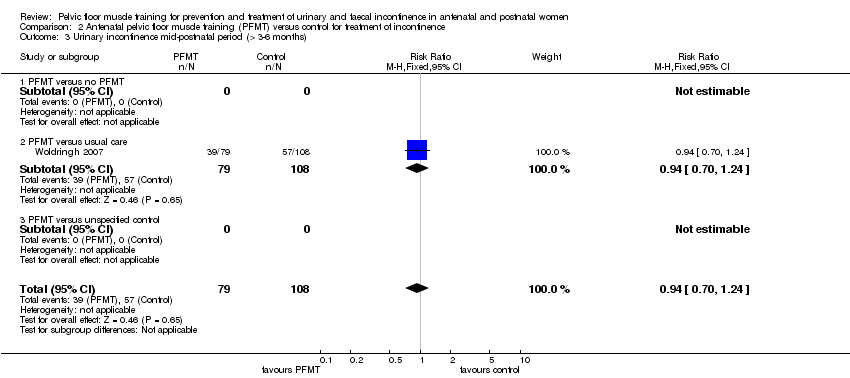
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 3 Urinary incontinence mid‐postnatal period (> 3‐6 months).
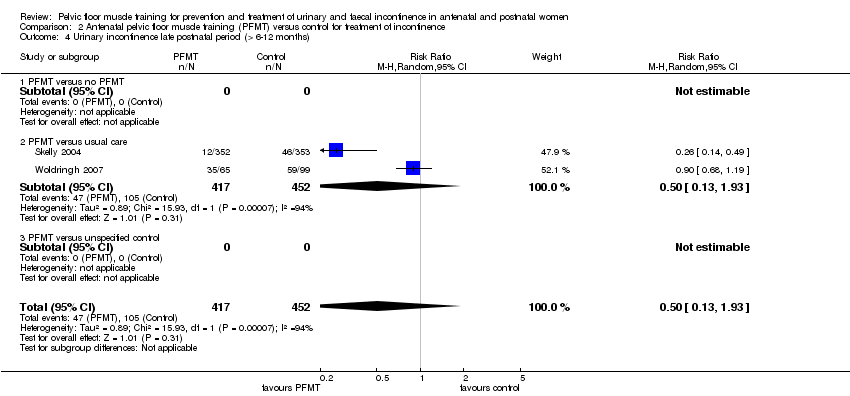
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 4 Urinary incontinence late postnatal period (> 6‐12 months).

Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 14 Incontinence‐specific quality of life.
| Study | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus usual care | ||||
| Woldringh 2007 | Incontinence Impact Questionnaire (IIQ), and data then dichotomised into impact versus no impact in four subscales ‐ impact on social relations, impact on emotional health, impact on recreational activities, and impact on physical activities (not clear how this was done) | Impact on social relations 2, on emotional health 11, on recreational activities 10, and on physical activities 4, n=65 at 12 months postpartum | Impact on social relations 5, on emotional health 14, on recreational activities 10, and on physical activities 7, n=99 at 12 months postpartum | Not calculated as validity/reliability of this measure not known |
| Woldringh 2007 | ||||
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 15 Quality of life and health status measures.
| Study | Measure of | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus usual care | |||||
| Woldringh 2007 | Frequency of leakage | 7 day urinary diary | Not reported | Not reported | |
| Woldringh 2007 | Amount of leakage | Not measured | |||
| Woldringh 2007 | Other leakage severity | A combination of data from a 7 day bladder diary and a questionnaire (PRAFAB, Vierhout 1990), ending with a score between 0 and 10. Mild urinary incontinence 0 to 4, and moderate to severe incontinence 5 to 10 | 9 with moderate to severe leakage, n=65 at 12 months postpartum | 8 with moderate to severe leakage, n=99 at 12 months postpartum | Not calculated as validity/reliability of this measure not known |
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 16 Severity of incontinence.
| Study | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus usual care | ||||
| Cruz 2014 | Maximal vaginal squeeze pressure, in cm water (Peritron) | Mean 29.8, SD 18.8, n=20 in third trimester | Mean 24.2, SD 12.9, n=21 in third trimester | Mean difference 5.6 (95% CI ‐4.32 to 15.52) |
| Cruz 2014 | ||||
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 17 Pelvic floor muscle function.
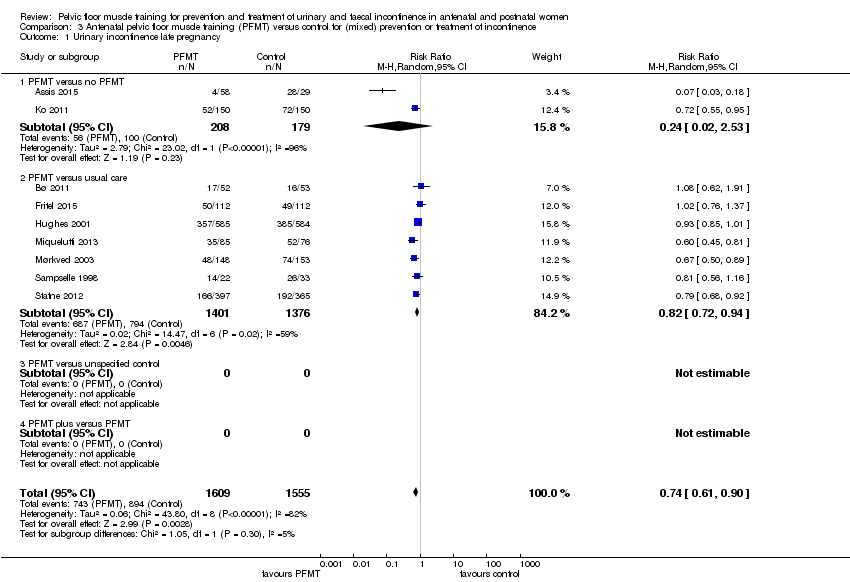
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 1 Urinary incontinence late pregnancy.

Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 2 Urinary incontinence early postnatal period (0‐3 months).

Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 3 Urinary incontinence mid‐postnatal period (> 3‐6 months).

Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 4 Urinary incontinence late postnatal period (> 6‐12 months).

Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 6 Urinary incontinence long term (> 5 years).
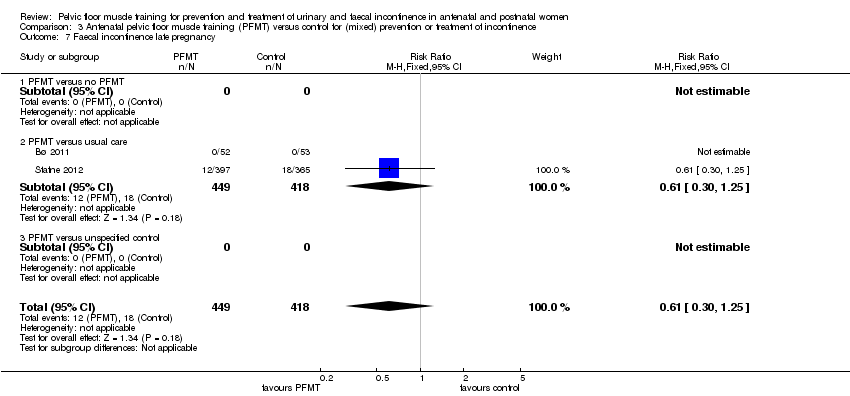
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 7 Faecal incontinence late pregnancy.

Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 8 Faecal incontinence early postnatal period (0‐3 months).
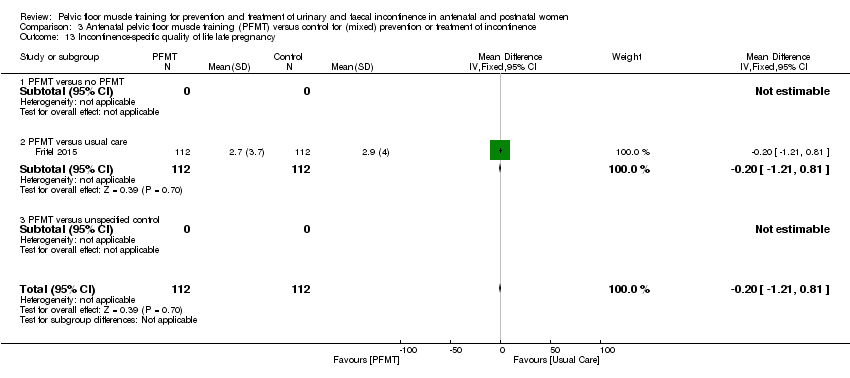
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 13 Incontinence‐specific quality of life late pregnancy.

Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 14 Incontinence‐specific quality of life early postnatal period (0‐3 months).

Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 15 Incontinence‐specific quality of life late postnatal period (> 6‐12 months).
| Study | Measure of | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus usual care | |||||
| Hughes 2001 | Frequency of leakage | Experiencing occasional or more than occasional urine leakage (not clear how measured) | 217 of 585 at 3 months postpartum | 210 of 584 at 3 months postpartum | Relative risk 1.03 (95% CI 0.89 to 1.20) |
| Hughes 2001 | Amount of leakage | Experiencing a drop or more than a drop of urine leakage (not clear how measured) | 228 of 585 at 3 months postpartum | 234 of 584 at 3 months postpartum | Relative risk 0.97 (95% CI 0.84 to 1.12) |
| Hughes 2001 | Other leakage severity | Not measured | |||
| Sampselle 1998 | Frequency of leakage | Not measured | |||
| Sampselle 1998 | Amount of leakage | Not measured | |||
| Sampselle 1998 | Other leakage severity | Average score from questionnaire re urine leakage with gentle cough, hard cough, sneeze and laugh scored 0 for none, 1 for dampness, 2 for wetness and 3 for soaked | Mean 0.38, SD 0.56, n=22 at 12 months postpartum | Mean 0.42, SD 0.49, n=24 at 12 months postpartum | Not calculated as validity/reliability of this measure not known |
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 16 Severity of incontinence.
| Study | Measure | PFMT | Control | Difference |
| PFMT versus usual care | ||||
| Fritel 2015 | 24 hour pad test (g) | Mean 0.9, SD 1.6, n=78 at 2 months postpartum | Mean 1.3, SD 3.3, n=85 at 2 months postpartum | Mean difference ‐0.40 (95% CI ‐1.19 to 0.39) |
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 17 Loss of urine under stress test early postnatal period (0‐3 months).
| Study | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus no PFMT | ||||
| Ko 2011 | UDI‐6 (0‐100) | Mean 3.44, SD 3.26, n=150 in late pregnancy; Mean 0.81, SD 1.36, n=150 at 0‐3 months postpartum; Mean 0.35, SD 0.84, n=150 at > 3‐6 months postpartum | Mean 4.66, SD 3.32, n=150 in late pregnancy; Mean 1.54, SD 1.59, n=150 at 0‐3 months postpartum; Mean 0.86, SD 1.14, n=150 at > 3‐6 months postpartum | Late pregnancy, mean difference ‐1.22 (95% CI ‐1.96 to ‐0.48); 0‐3 months postpartum, mean difference ‐0.73 (95% CI ‐1.06 to ‐0.40); > 3‐6 months postpartum, mean difference ‐0.51 (95% CI ‐0.74 to ‐0.28) |
| Ko 2011 | IIQ7 (0‐100) | Mean 3.77, SD 6.01, n=150 in late pregnancy; Mean 1.73, SD 3.57, n=150 at 0‐3 months postpartum; Mean 0.77, SD 2.07, n=150 at > 3‐6 months postpartum | Mean 5.28, SD 5.16, n=150 in late pregnancy; Mean 5.28, SD 5.61, n=150 at 0‐3 months postpartum; Mean 1.56, SD 2.20, n=150 at > 3‐6 months postpartum | Late pregnancy, mean difference ‐1.51 (95% CI ‐2.78 to ‐0.24); 0‐3 months postpartum, mean difference ‐3.55 (95% CI ‐4.61 to ‐2.49); > 3‐6 months postpartum, mean difference ‐0.79 (95% CI ‐1.27 to ‐0.31) |
| Ko 2011 | ||||
| Ko 2011 | ||||
| Ko 2011 | ||||
| Ko 2011 | ||||
| Ko 2011 | ||||
| Ko 2011 | ||||
| PFMT versus usual care | ||||
| Fritel 2015 | Female Pelvic Floor Questionnaire (FPFQ) bladder score (0‐10; 10 worse) | Mean 1.7, SD 1.3, n=112 in late pregnancy; Mean 0.8, SD 0.9, n=105 at 0‐3 months postpartum; Mean 0.9, SD 1.1, n=94 at > 6‐12 months postpartum | Mean 2.0, SD 1.4, n=111 in late pregnancy; Mean 0.9, SD 1.0, n=107 at 0‐3 months postpartum; Mean 1.0, SD 1.1, n=97 at > 6‐12 months postpartum | Late pregnancy, mean difference ‐0.30 (95% CI ‐0.65 to 0.05); 0‐3 months postpartum, mean difference ‐0.10 (95% CI ‐0.36 to 0.16); >6‐12 months postpartum, mean difference ‐0.10 (95% CI ‐0.41 to ‐0.12) |
| Fritel 2015 | FPFQ bowel score (0‐10) | Mean 1.3, SD 1.1, n=112 in late pregnancy; Mean 1.2, SD 1.2, n=104 at 0‐3 months postpartum; Mean 1.0, SD 1.0, n=94 at > 6‐12 months postpartum | Mean 1.4, SD 1.1, n=112 in late pregnancy; Mean 1.4, SD 1.2, n=107 at 0‐3 months postpartum; Mean 1.1, SD 1.0, n=97 > 6‐12 months postpartum | Late pregnancy, mean difference ‐0.10 (95% CI ‐0.39 to ‐0.19); 0‐3 months postpartum, mean difference ‐0.20 (95% CI ‐0.52 to 0.12); >6‐12 months postpartum, mean difference ‐0.10 (95% CI ‐0.38 to 0.18) |
| Fritel 2015 | FPFQ prolapse score (0‐10) | Mean 0.7, SD 1.2, n=112 in late pregnancy; Mean 0.3, SD 1.1, n=104 at 0‐3 months postpartum; Mean 0.4, SD 1.2, n=95 at > 6‐12 months postpartum | Mean 0.7, SD 1.4, n=112 in late pregnancy; Mean 0.5, SD 1.3, n=107 at 0‐3 months postpartum; Mean 0.4, SD 1.0, n=97 at > 6‐12 months postpartum | Late pregnancy, mean difference 0.00 (95% CI ‐0.34 to 0.34); 0‐3 months postpartum, mean difference ‐0.20 (95% CI ‐0.52 to 0.12); >6‐12 months postpartum, mean difference 0.00 (95% CI ‐0.31 to 0.31) |
| Fritel 2015 | Female Pelvic Floor Questionnaire sex score (0‐10; 10 worse) | Mean 2.7, SD 1.8, n=79 in late pregnancy; Mean 3.1, SD 2.1, n=73 at 0‐3 months postpartum; Mean 2.4, SD 1.8, n=86 at > 6‐12 months postpartum | Mean 3.1, SD 2.1, n=68 in late pregnancy; Mean 3.5, SD 2.2, n=77 at 0‐3 months postpartum; Mean 2.7, SD 2.0, n=83 at > 6‐12 months postpartum | Late pregnancy, mean difference ‐0.90 (95% CI ‐1.54 to ‐0.26); 0‐3 months postpartum, mean difference ‐0.40 (95% CI ‐1.09 to 0.29); >6‐12 months postpartum, mean difference ‐0.30 (95% CI ‐0.87 to 0.27) |
| Fritel 2015 | Contilife score (0‐10; 10 better) | Mean 9.3, SD 1.1, n=108 in late pregancy; Mean 9.6, SD 0.8, n=102 at 0‐3 months postpartum; Mean 9.5, SD 1.2, n=91 at > 6‐12 months postpartum | Mean 9.2, SD 1.3, n=109 in late pregancy; Mean 9.5, SD 0.8, n=101 at 0‐3 months postpartum; Mean 9.5, SD 1.0, n=89 at > 6‐12 months postpartum | Late pregnancy, mean difference 0.10 (95% CI ‐0.22 to 0.42); 0‐3 months postpartum, mean difference 0.10 (95% CI ‐0.12 to 0.32); >6‐12 months postpartum, mean difference 0.00 (95% CI ‐0.32 to 0.32) |
| Fritel 2015 | Sexually active | 83 of 112 at end of pregnancy; 74 of 104 at 0‐3 months postpartum; 89 of 95 at > 6‐12 months postpartum | 70 of 112 at end of pregnancy; 79 of 106 at 0‐3 months postpartum; 91 of 97 at > 6‐12 months postpartum | Late pregnancy, relative risk 1.19 (95% CI 0.99 to 1.42); 0‐3 months postpartum, relative risk 0.95 (95% CI 0.81 to 1.13); >6‐12 months postpartum, relative risk 1.0 (95% CI 0.93 to 1.07) |
| Fritel 2015 | EuroQoL‐5D (0‐100; 100 better) | Mean 76.4, SD 20.4, n=111 at end of pregnancy; Mean 82.8, SD 18.2, n=105 at 0‐3 months postpartum; Mean 86.8, SD 13.1, n=94 at > 6‐12 months postpartum | Mean 77.9, SD 16.3, n=112 at end of pregnancy; Mean 80.4, SD 17.0, n=107 at 0‐3 months postpartum; Mean 82.9, SD 14.8, n=97 at > 6‐12 months postpartum | Late pregnancy, mean difference ‐1.50 (95% CI ‐6.35 to 3.35); 0‐3 months postpartum, mean difference 2.40 (95% CI ‐2.34 to 7.14); >6‐12 months postpartum, mean difference 3.90 (95% CI ‐0.06 to 7.86) |
| Fritel 2015 | ||||
| Hughes 2001 | ||||
| Hughes 2001 | BFLUTs questionnaire: a negative effect on exercise in response to question "does incontinence affect physical activity?" | 47 of 585 at 6 months postpartum | 41 of 584 at 6 months postpartum | Relative risk 1.14 (95% CI 0.76 to 1.71) |
| Hughes 2001 | ||||
| Hughes 2001 | ||||
| Hughes 2001 | ||||
| Hughes 2001 | ||||
| Hughes 2001 | ||||
| Hughes 2001 | ||||
| Miquelutti 2013 | State Trait Anxiety Inventory (STAI) (20‐80; 50‐64 high; 65‐80 very high) | Trait anxiety 18 of 85 State anxiety 16 of 85 | Trait anxiety 20 of 76 State anxiety 14 of 76 | Trait anxiety, relative risk 0.80 (95% CI 0.46 to 1.40) State anxiety, relative risk 1.02 (95% CI 0.53 to 1.95) |
| Miquelutti 2013 | ||||
| Miquelutti 2013 | ||||
| Miquelutti 2013 | ||||
| Miquelutti 2013 | ||||
| Miquelutti 2013 | ||||
| Miquelutti 2013 | ||||
| Miquelutti 2013 | ||||
| Mørkved 2003 | Sexual satisfaction at 6 years post‐delivery | 34 of 94 | 17 of 94 | Relative risk 2.00 (95% CI 1.20 to 3.32) |
| Mørkved 2003 | ||||
| Mørkved 2003 | ||||
| Mørkved 2003 | ||||
| Mørkved 2003 | ||||
| Mørkved 2003 | ||||
| Mørkved 2003 | ||||
| Mørkved 2003 | ||||
| Stafne 2012 | Psychological General Well‐being Index (PGWBI) (0‐110; 110 better) | Total score at end of pregnancy: Mean 79.5 (95% CI 78.5 to 80.6), n=389 | Total score at end of pregnancy: Mean 78.5 (95% CI 77.5 to 79.6), n=361 | Mean difference 0.71 (95% CI ‐0.60 to 2.01) |
| Stafne 2012 | ||||
| Stafne 2012 | ||||
| Stafne 2012 | ||||
| Stafne 2012 | ||||
| Stafne 2012 | ||||
| Stafne 2012 | ||||
| Stafne 2012 | ||||
| PFMT versus unspecified control | ||||
| Dokmeci 2008 | UDI‐6 | No data | No data | Authors stated that there was a significant decrease in scores between first trimester and third trimester and between third trimester and 6 weeks postpartum |
| Dokmeci 2008 | IIQ‐7 | No data | No data | Authors stated that there were no significant differences observed during pregnancy or postpartum |
| Dokmeci 2008 | PISQ‐12 | No data | No data | Authors stated that there were no significant differences observed during pregnancy or postpartum |
| Dokmeci 2008 | ||||
| Dokmeci 2008 | ||||
| Dokmeci 2008 | ||||
| Dokmeci 2008 | ||||
| Dokmeci 2008 | ||||
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 18 Quality of life and health status measures.
| Study | Measure | PFMT | Control | Difference |
| PFMT versus no PFMT | ||||
| Assis 2015 | Perinometry, vaginal squeeze pressure (cm water), late pregnancy | Mean 9.45, SD 1.05, n=58 | Mean 4.7, SD 1.7, n=29 | Mean difference 4.75 (95% CI 4.07 to 5.43) |
| Assis 2015 | ||||
| PFMT versus usual care | ||||
| Fritel 2015 | Pelvic floor muscle strength, modified Oxford scale (0‐5; 5 better) | Mean 3.5, SD 1.5, n=105 at 2 months postpartum | Mean 3.3, SD 1.3, n=107 at 2 months postpartum | Mean difference 0.12 (95% CI ‐0.18 to 0.58) |
| Fritel 2015 | Change in pelvic floor muscle strength, baseline to 2 months postpartum | Mean 0.08, SD 1.32, n=101 | Mean ‐0.25, SD 1.11, n=103 | Mean difference 0.33 (95% CI ‐0.00 to 0.66) |
| Mørkved 2003 | Vaginal squeeze pressure (cm water) | Mean 29.5, 95% CI 26.8 to 32.2, n=143 at 3 months postpartum | Mean 25.6, 95% CI 23.2 to 27.9, n=146 at 3 months postpartum | Mean difference 3.90 (95% CI 0.35 to 7.45) |
| Mørkved 2003 | ||||
| PFMT versus unspecified control | ||||
| Dokmeci 2008 | Electromyography with vaginal electrode | No data | No data | Authors stated that "Maximum pelvic floor strength was increased significantly between first and third visits in PFMT group, p=0.03 and between first and post‐partum visits in control group, p=0.03." |
| Dokmeci 2008 | ||||
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 19 Pelvic floor muscle function.

Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 20 Delivery outcome: caesarean section.
| Study | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus no PFMT | ||||
| Ko 2011 | Episiotomy | 99 of 150 | 104 of 150 | Relative risk 0.95 (95% CI 0.81 to 1.11) |
| Ko 2011 | Severe perineal lacerations | 10 of 150 | 10 of 150 | |
| Ko 2011 | ||||
| PFMT versus usual care | ||||
| Fritel 2015 | Spontaneous vaginal delivery | 72 of 137 | 72 of 135 | Relative risk 0.99 (95% CI 0.79 to 1.23) |
| Fritel 2015 | Assisted delivery | 29 of 137 | 35 of 135 | Relative risk 0.82 (95% CI 0.53 to 1.26) |
| Fritel 2015 | ||||
| Miquelutti 2013 | Vaginal delivery | 44 of 76 | 38 of 71 | Relative risk 1.08 (95% CI 0.81 to 1.44) |
| Miquelutti 2013 | Duration active phase labour (min) | Mean 284.5, SD 175, n=78 | Mean 254.2, SD 139.4, n=71 | Mean difference 30.3 (95% CI ‐40.9 to 101.4) |
| Miquelutti 2013 | Duration 2nd stage labour (min) | Mean 29.2, SD 23.3, n=78 | Mean 19.7, SD 13.0, n=71 | Mean difference 9.48 (95% CI 0.32 to 18.64) |
| Mørkved 2003 | Type of delivery (excluding twin pregnancy, preterm delivery, planned caesarean section and induced labour) | 91 normal vaginal deliveries, 15 asssisted vaginal deliveries, 5 emergency caesarean section, n=111 | 91 normal vaginal deliveries, 19 assisted vaginal deliveries, 3 emergency caesarean section, n=113 | Relative risk for normal vaginal delivery 1.02 (95% CI 0.90 to 1.15) Relative risk for assisted vaginal delivery 0.80 (95% CI 0.43 to 1.50) |
| Mørkved 2003 | Perineal trauma | 56 with episiotomy, and 7 with third or fourth degree tears, n=111 | 72 with episiotomy, and 9 with third or fourth degree tears, n=113 | Relative risk for episiotomy 0.79 (95% CI 0.63 to 1.00) |
| Mørkved 2003 | Duration 2nd stage labour (min) | Mean 40, 95% CI 33 to 47, n=111 | Mean 45, 95% CI 38 to 52, n=113 | Mean difference ‐5.00 (95% CI ‐14.79 to 4.79) |
| Stafne 2012 | Assisted vaginal delivery | 62 of 426 | 50 of 425 | Relative risk 1.24 (95% CI 0.87 to 1.75) |
| Stafne 2012 | Mean duration labour (min) | Mean 289, n=426? | Mean 281, n=425? | Unable to estimate |
| Stafne 2012 | Mean duration active 2nd stage labor (min) | Mean 32, n=426? | Mean 29, n=425? | Unable to estimate |
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 21 Delivery outcome: other.
| Study | Measure | PFMT | Control | Difference |
| PFMT versus usual care | ||||
| Fritel 2015 | Additional postnatal pelvic floor muscle training | 50 of 92 at 12 months postpartum | 61 of 97 at 12 months postpartum | Relative risk 0.86 (95% CI 0.68 to 1.10) |
| Fritel 2015 | Medical visits since delivery | Mean 3.0, SD 2.5, n=84 at 12 months postpartum | Mean 3.0, SD 2.2, n=83 at 12 months postpartum | Mean difference 0.00 (95% CI ‐0.71 to 0.71) |
| PFMT versus unspecified control | ||||
| Frumenzio 2012 | Visual analogue scale patient satisfaction (0‐10) | Mean 7.6 | No data | Not able to calculate |
| Frumenzio 2012 | ||||
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 22 Patient satisfaction and further treatment.

Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 3 Urinary incontinence late‐postnatal period (> 6‐12 months).

Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 5 Urinary incontinence long term (> 5‐10 years).

Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 6 Urinary incontinence very long term (> 10 years).

Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 9 Faecal incontinence late‐postnatal period (> 6‐12 months).

Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 11 Faecal incontinence long term (> 5‐10 years).

Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 12 Faecal incontinence very long term (> 10 years).

Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 13 Incontinence‐specific quality of life.
| Study | Measure of | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus no PFMT | |||||
| Dumoulin 2004 | Frequency of leakage | Not measured | |||
| Dumoulin 2004 | Amount of leakage | Change, in grams, in 20 min pad test with standardised bladder volume | A: Median change 19.0, interquartile range 6.0 to 25.0, n=23 after 9 weeks of PFMT B: Median change 8, interquartile range 4.0 to 2.35, n=20 after 9 weeks of PFMT | Median change 0, interquartile range ‐3.0 to 9.8, n=19 after 9 weeks of control condition | Not calculable |
| Dumoulin 2004 | Other leakage | Change in visual analogue scale for perceived burden of incontinence (Stach‐Lempinen et al 2001) | A: Median change 3.0, interquartile range 2.0 to 4.0, n=23 after 9 weeks of PFMT B: Median change 2.5, interquartile range 0.8 to 5.0, n=20 after 9 weeks of PFMT | Median change 0, interquartile range ‐0.1 to 0.02, n=19 after 9 weeks of control condition | Not calculable |
| PFMT versus usual care | |||||
| Ahlund 2013 | Incontinence score (0‐20, 20 worse) | ICIQ‐FLUTS | Median 4.0, range 0 to 15, n=40 at 9 months postpartum | Median 4, range 0 to 12, n=42 at 9 months postpartum | Not calculable |
| Ahlund 2013 | Voiding score (0‐12, 12 worse) | ICIQ‐FLUTS | Median 1.0, range 0 to 5, n=40 at 9 months postpartum | Median 0.0, range 0 to 8, n=42 at 9 months postpartum | Not calculable |
| Ahlund 2013 | Incontinence score (0‐20, 20 worse) | ICIQ‐FLUTS | Median 4.0, range 0 to 15, n=40 at 9 months postpartum | Median 4, range 0 to 12, n=42 at 9 months postpartum | Not calculable |
| Glazener 2001 | Frequency of leakage | Not measured | |||
| Glazener 2001 | Amount of leakage | Using absorbent pads | 41 of 276 at 12 months postpartum | 55 of 245 at 12 months postpartum | Relative risk 0.66 (95% CI 0.46, 0.95) |
| Glazener 2001 | Other leakage severity | Visual analogue scale for severity of urine leakage | Mean 2.8, 95% CI 2.4 to 3.1, n=142 at 12 months postpartum | Mean 3.6, 95% CI 3.1 to 4.0, n=142 at 12 months postpartum | Mean difference ‐0.80 (95% CI ‐1.37 to ‐0.23) |
| Kim 2012 | Urinary symptoms (? range) | BFLUTS | Mean 40.56, SD 5.36, n=9 at between 8‐14 weeks postpartum | Mean 46.89, SD 3.62, n=9 at between 8‐14 weeks postpartum | |
| Kim 2012 | |||||
| Kim 2012 | |||||
| Wilson 1998 | Frequency of leakage | Not measured | |||
| Wilson 1998 | Amount of leakage | Urine loss on home pad test (Wilson et al 1989), in grams | Mean 2.1, 95% CI ‐0.3 to 4.5, n=18 at 12 months postpartum | Mean 2.6, 95% CI 0.1 to 5.1, n=82 at 12 months postpartum | Mean difference ‐0.50 (95% CI ‐3.81 to 2.81) |
| Wilson 1998 | Other leakage severity | Not measured | |||
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 14 Severity of incontinence.
| Study | Outcome measure | PFMT data | Control data | Difference |
| Dumoulin 2004 | Change in Urogenital Distress Inventory Score (maximum score 57) | A: Median change 4, interquartile range 1 to 10, n=23 after 9 weeks PFMT B: Median change 7, interquartile range 3 to 8, n=20 after 9 weeks PFMT | Median change 0, interquartile range ‐2.3 to 6.5, n=19 after 9 weeks of control condition | Not calculable |
| Dumoulin 2004 | Change in Incontinence Impact Questionnaire (maximum score 90) | A: Median change 10, interquartile range 2 to 16, n=23 after 9 weeks PFMT B: Median change 13, interquartile range 6 to 25, n=20 after 9 weeks PFMT | Median change 0.5, interquartile range ‐6.5 to 5.0, n=19 after 9 weeks of control condition | Not calculable |
| Glazener 2001 | Hospital Anxiety and Depression Score ‐ anxiety score | Mean 6.1, 95% CI 5.6 to 6.5, n=238 at 12 months | Mean 6.8, 95% CI 6.3 to 7.3, n=219 at 12 months postpartum | Mean difference ‐0.79 (95% CI ‐1.43 to ‐0.05) |
| Glazener 2001 | ||||
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 15 Quality of life and health status measures.
| Study | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus no PFMT | ||||
| Dumoulin 2004 | Maximal strength (Newtons, pelvic floor dynamometer, Dumoulin et al 2003) | A: Median change 0.7, range ‐0.2 to 2.3, n=23 after 9 weeks PFMT B: Median change 0.5, range ‐0.6 to 2.5, n=20 after 9 weeks PFMT | Median change ‐0.5, range ‐1.7 to 1.0, n=19 after 9 weeks PFMT | Not calculable |
| Dumoulin 2004 | ||||
| Dumoulin 2004 | ||||
| PFMT versus usual care | ||||
| Ahlund 2013 | Maximal voluntary contraction (cm mercury, perineometer) | Median 26.0, estimated range 7 to 49, n=40 at 9 months postpartum | Median 18.2, estimated range 6 to 54, n=42 at 9 months postpartum | Not calculable |
| Ahlund 2013 | Endurance (secs, continuous contraction until pressure=0) | Median 26.7, estimated range 1 to 65, n =40 at 9 months postpartum | Median 23.4, estimated range 3 to 60, n=42 at 9 months postpartum | Not calculable |
| Ahlund 2013 | Oxford scale (0‐5, 0=no activity; 5, strong) | Median 4, estimated range 2 to 5, n=40 at 9 months postpartum | Median 3, estimated range 2 to 5, n=42 at 9 months postpartum | Not calculable |
| Kim 2012 | Maximal squeeze pressure (mm mercury, perineometer) | Mean 25.78, SD 10.74, n= 9 at between 8‐14 weeks postpartum | Mean 8.11, SD 2.57, n=9 at between 8‐14 weeks postpartum | Mean difference 17.67 (95% CI 10.46 to 24.88) |
| Kim 2012 | Holding time (sec, perineometer) | Mean 14.34, SD 3.08, n=9 at between 8‐14 weeks postpartum | Mean 8.89, SD 2.10, n=9 at between 8‐14 weeks postpartum | Mean difference 5.45 (95% CI 3.01 to 7.89) |
| Kim 2012 | ||||
| Wilson 1998 | Maximal vaginal squeeze pressure (cm water) | Mean 13.6, 95% CI 9.8 to 17.4, n=19 at 12 months postpartum | Mean 13.1, 95% CI 11.3 to 14.9, n=79 at 12 months postpartum | Mean difference 0.50 (95%CI ‐3.46 to 4.46) |
| Wilson 1998 | ||||
| Wilson 1998 | ||||
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 16 Pelvic floor muscle function.

Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 2 Urinary incontinence mid‐postnatal period (> 3‐6 months).

Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 3 Urinary incontinence late postnatal period (> 6‐12 months).

Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 6 Faecal incontinence early postnatal period (0‐3 months).

Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 8 Faecal incontinence late‐postnatal period (> 6‐12 months).
| Study | Measure of | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus usual care | |||||
| Hilde 2013 | Amount of leakage | Pad test, 1 min with standardised bladder volume (positive test 2g or more) | Median 4.0, range 2.0 to 80.0, n=87 at 6 months postpartum | Median 6.0, range 2.0 to 114.0, n=88 at 6 months postpartum | Mann Whitney‐U 213.5, z‐value ‐0.13, p‐value 0.90 |
| Hilde 2013 | |||||
| Hilde 2013 | |||||
| Liu 2011 | Urinary condition score, not specified (lower score better; 3 months postpartum) | Mean 2.2, SD 0.2, n=106 | Mean 2.8, SD 0.4, n=86 | Mean difference ‐0.60 (95% CI ‐0.69 to ‐0.51) | |
| Liu 2011 | Urinary condition score, not specified (lower score better; 6 months postpartum) | Mean 2.0, SD 0.4, n=106 | Mean 2.5, SD 0.4, n =86 | Mean difference ‐0.50 (95% CI ‐0.61 to ‐0.39) | |
| Liu 2011 | |||||
| Sleep 1987 | Frequency of leakage | Urine leakage once or more per week | 64 of 816 at 3 months postpartum | 57 of 793 at 3 months postpartum | Relative risk 1.09 (95% CI 0.77 to 1.54) |
| Sleep 1987 | Amount of leakage | Using absorbent pads sometimes or always | 38 of 815 at 3 months postpartum | 43 of 793 at 3 months postpartum | Relative risk 0.86 (95% CI 0.56 to 1.32) |
| Sleep 1987 | Other leakage severity | Not measured | |||
| Wen 2010 | Stress UI | Criteria from International Continence Society, 0‐5 (lower score better; 6 months postpartum) | Mean 2.84, SD 0.43, n=75 | Mean 2.50, SD 0.41, n=73 | Mean difference 0.34 (95% CI 0.20 to 0.48) |
| Wen 2010 | Stress UI | Criteria from International Continence Society, 0‐5 (lower score better; 12 months postpartum) | Mean 1.16, SD 0.38, n=75 | Mean 2.20, SD 0.39, n=73 | Mean difference ‐1.04 (95% CI ‐1.16 to ‐0.92) |
| Wen 2010 | Amount of leakage | Pad test (postive test more than 2g) | 7 of 75 at 12 months postpartum | 19 of 73 at 6 months postpartum | Relative risk 0.29 (95% CI 0.11 to 0.75) |
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 11 Severity of incontinence.
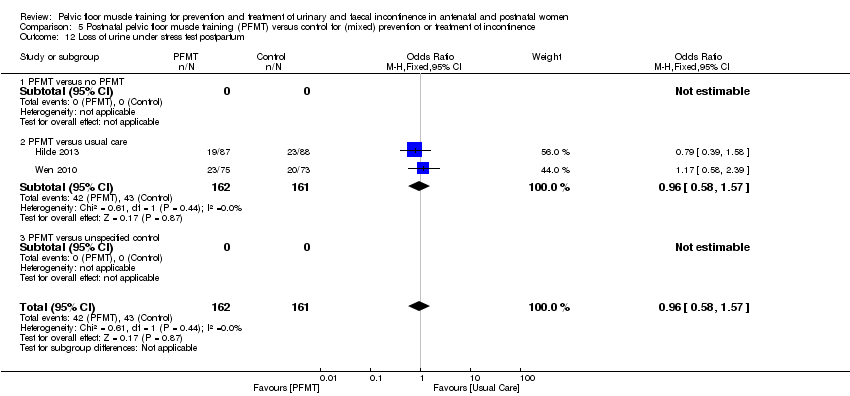
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 12 Loss of urine under stress test postpartum.
| Study | Measure of | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus no PFMT | |||||
| Meyer 2001 | Sexual function | Reduced vaginal response at 10 months postpartum | 5 of 51 | 13 of 56 | Relative risk 0.42 (95% CI 0.16 to 1.10) |
| Meyer 2001 | |||||
| Meyer 2001 | |||||
| PFMT versus usual care | |||||
| Peirce 2013 | Faecal Incontinence Specific Quality of Life | Rockwood Faecal Incontinence Quality of Life Scale (low better, no total score, 4 domain scores) | Lifestyle: no data; coping/behaviour: no data, depression/self perception: no data, embarrassment: no data, n=30 | Lifestyle: no data, coping/behaviour: no data, depression/self perception: no data, embarrassment: no data, n=90 | Lifestyle p =0.29, coping/behaviour p=0.27, depression/self perception p=089, embarrassment p=0.51 |
| Peirce 2013 | |||||
| Peirce 2013 | |||||
| Sleep 1987 | General wellbeing | 5 point Likhert scale in response to question "how are you feeling generally?" | 11 feeling not very well or not at all well, n=816 at 3 months postpartum | 18 feeling not very well or not at all well, n=793 at 3 months postpartum | Not calculated as validity/reliability of this measure not known |
| Sleep 1987 | Sexual function | Attempted sexual intercourse within 3 months of delivery | 714 of 819 | 681 of 792 | Relative risk 1.01 (95% CI 0.98 to 1.05) |
| Sleep 1987 | Sexual function | Dyspareunia at 3 months postpartum | 167 of 819 | 154 of 792 | Relative risk 1.05 (95% CI 0.86 to 1.28) |
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 13 Quality of life and health status measures.
| Study | Outcome measure | PFMT data | Control data | Difference |
| PFMT versus no PFMT | ||||
| Meyer 2001 | Strength, vaginal squeeze pressure, in cm water (manometer, 10 months postpartum) | Mean 33, SD 22, n=51 | Mean 41, SD 27, n=56 | Mean difference ‐8.0 (95%CI ‐17.3 to 1.3) |
| Meyer 2001 | Mean anal squeeze pressure, in cm water (anorectal manometer, 10 months postpartum) | Mean 36, SD 20, n=51 | Mean 43, SD 24, n=56 | Mean difference ‐7.0 (95%CI ‐15.4 to 1.4) |
| Meyer 2001 | ||||
| PFMT versus usual care | ||||
| Hilde 2013 | Resting pressure, vaginal squeeze pressure (cm water, manometer) | n=87 at 6 months postpartum | n=88 at 6 months postpartum | Mean difference 1.3 (95% CI ‐1.0 to 3.6, p=0.257), reported by authors |
| Hilde 2013 | Strength, vaginal squeeze pressure (cm water, manometer) | n=87 at 6 months postpartum | n=88 at 6 months postpartum | Mean difference 3.3 (95% CI ‐1.4 to 8.0, p=0.172), reported by authors |
| Hilde 2013 | Endurance, vaginal squeeze pressure (cm sec, manometer) | n=87 at 6 months postpartum | n=88 at 6 months postpartum | Mean difference 29.8 (95% CI ‐10.6 to 70.2, p=0.148), reported by authors |
| Kou 2013 | Resting pressure, vaginal squeeze pressure (cm water) | Mean 33.7, SD 15.8, n=80 at 12 months postpartum | Mean 30.1, SD 15.3, n=70 at 12 months postpartum | Mean difference 3.60 (95% CI ‐1.38 to 8.58) |
| Kou 2013 | Vaginal squeeze pressure (cm water) | Mean 86.5, SD 14.8, n=80 at 12 months postpartum | Mean 60.4, SD 14.1, n=70 at 12 months postpartum | Mean difference 26.10 (95% CI 21.47 to 30.73) |
| Kou 2013 | Contraction time (sec) | Mean 5.9, SD 2.9, n=80 at 12 months postpartum | Mean 4.1, SD 2.6, n=70 at 12 months postpartum | Mean difference 1.80 (95% CI 0.92 to 2.68) |
| Liu 2011 | PF muscle tension (Oxford scale) | Mean 3.95, SD 0.32, n=106 at 3 months postpartum | Mean 3.02, SD 0.28, n=86 at 3 months postpartum | Mean difference 0.93 (95% CI 0.34 to 1.52) |
| Liu 2011 | PF muscle tension (Oxford scale) | Mean 4.73, SD 0.35, n=106 at 6 months postpartum | Mean 3.25, SD 0.41, n=86 at 6 months postpartum | Mean difference 1.48 (95% CI 1.37 to 1.59) |
| Liu 2011 | PF muscle tension (Oxford scale) | Mean 4.82, SD 0.38, n=106 at 12 months postpartum | Mean 3.43, SD 0.39, n=86 at 12 months postpartum | Mean difference 1.40 (95% CI 1.29 to 1.51) |
| Peirce 2013 | Mean anal resting pressure (mm Hg, anorectal manometer) | Mean 39, SD 13, n=30 at 3 months postpartum | Mean 43, SD 17, n=90 at 3 months postpartum | Mean difference ‐4.00 (95% CI ‐9.83 to 1.83) |
| Peirce 2013 | Mean anal squeeze pressure (mm Hg, anorectal manometer) | Mean 64, SD 17, n=30 at 3 months postpartum | Mean 62, SD 23, n=90 at 3 months postpartum | Mean difference 2.00 (95% CI ‐5.72 to 9.72) |
| Peirce 2013 | ||||
| Wen 2010 | PFMS (Oxford scale) | Mean 3.34, SD 0.35, n=75 at 6 months postpartum | Mean 3.25, SD 0.41, n=73 at 6 months postpartum | Mean difference 0.09 (95% CI ‐0.03 to 0.21) |
| Wen 2010 | PFMS (Oxford scale) | Mean 4.56, SD 0.38, n=75 at 12 months postpartum | Mean 3.46, SD 0.39, n=73 at 12 months postpartum | Mean difference 1.10 (95% CI 0.98 to 1.22) |
| Wen 2010 | ||||
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 14 Pelvic floor muscle function.
| Study | Measure | PFMT | Control | Difference |
| PFMT versus usual care | ||||
| Hilde 2013 | ICIQ‐Vag, bulging inside vagina (yes, no) | 8 of 87 at 6 months postpartum | 22 of 88 at 6 months postpartum | Mean difference 0.37 (95% CI 0.17 to 0.78) |
| Hilde 2013 | ICIQ‐Vag, bulging outside vagina (yes, no) | 5 of 87 at 6 months postpartum | 6 of 88 at 6 months postpartum | Mean difference 0.84 (95% CI 0.27 to 2.66) |
| Hilde 2013 | POP‐Q, stage 1 or 2 | 61 of 87 at 6 months postpartum | 64 of 88 at 6 months postpartum | Mean difference 0.88 (95% CI 0.46 to 1.70) |
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 15 Pelvic organ prolapse symptoms.
| Antenatal pelvic floor muscle training compared to control for prevention of urinary and faecal incontinence | ||||||
| Patient or population: pregnant women who were continent when randomised Setting: hospital or outpatient settings in Canada, Italy, Mexico, Norway, Spain, Thailand, Turkey, UK and USA Intervention: antenatal PFMT Comparison: control (no PFMT or usual care) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with antenatal PFMT | |||||
| Urinary incontinence in late pregnancy | Study population | RR 0.38 | 624 | ⊕⊕⊝⊝ | Upper and lower limits of the CI of summary statistic suggest clinical importance. | |
| 421 per 1000 | 160 per 1000 | |||||
| Urinary incontinence mid‐postnatal period (> 3‐6 months) | Study population | RR 0.71 | 673 | ⊕⊕⊕⊝ | Risk reduction is a clinically important effect but the upper limit of the CI is close to no effect. | |
| 251 per 1000 | 179 per 1000 | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 1.20 | 44 | ⊕⊕⊝⊝ | Wide CI including no effect. | |
| 440 per 1000 | 528 per 1000 | |||||
| Faecal incontinence in late pregnancy | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence mid‐postnatal period (> 3‐6 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Incontinence‐specific quality of life | Mean 2.66, SD 4.1 | Mean 0.24, SD 1.2 | MD 2.42 lower | 152 | ⊕⊕⊕⊝ | Measured in late postnatal period. Upper and lower limits of the CI of summary statistic suggest clinical importance in ICIQ‐SF (Nyström 2015). |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; ICIQ‐SF: International Consultation on Incontinence ‐ Short Form; MD: mean difference; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio; SD: standard deviation. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Downgraded two levels for serious inconsistency and imprecision (multiple small RCTs, fewer than 300 events, heterogeneous intervention and control groups). 2Downgraded one level for serious imprecision (multiple small RCTs, fewer than 300 events). 3Downgraded two levels for very serious imprecision (single, small trial with wide confidence interval). 4Downgraded one level for serious imprecision (single trial, fewer than 300 events). The outcome measures relate to the presence of incontinence symptoms rather than absence. Symptoms of urinary and faecal incontinence were measured based on self‐report. | ||||||
| Antenatal pelvic floor muscle training compared to control for treatment of urinary and faecal incontinence | ||||||
| Patient or population: pregnant women who were incontinent when randomised Setting: health services or obstetric clinics in Brazil, Canada, the Netherlands and Turkey Intervention: antenatal PFMT Comparison: control (usual care) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with antenatal PFMT | |||||
| Urinary incontinence in late pregnancy | Study population | RR 0.70 | 345 | ⊕⊝⊝⊝ | Wide CI including no effect. | |
| 776 per 1000 | 543 per 1000 | |||||
| Urinary incontinence mid‐postnatal period (> 3‐6 months) | Study population | RR 0.94 | 187 | ⊕⊝⊝⊝ | Wide CL including no effect. | |
| 528 per 1000 | 496 per 1000 | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.50 | 869 | ⊕⊝⊝⊝ | Wide CI including no effect. | |
| 232 per 1000 | 116 per 1000 | |||||
| Faecal incontinence in late pregnancy | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence mid‐postnatal period (> 3‐6 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Incontinence‐specific quality of life (ICIQ‐SF) | Mean 4.7, SD 5.6 | Mean 1.2, SD 2.5 | MD 3.5 lower | 41 | ⊕⊕⊝⊝ | MD suggests clinically important effect but the upper limit of the CI is close to no effect. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; ICIQ‐SF: International Consultation on Incontinence ‐ Short Form; MD: mean difference; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio; SD: standard deviation. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Downgraded three levels due to serious risk of selection bias (one trial with heavy weighting in the pooled estimate at high risk), inconsistency and indirectness, and very serious imprecision (fewer than 300 events, wide confidence interval, two trials without any details about PFMT interventions). 2Downgraded three levels due to serious risk of selection bias, indirectness and imprecision (singe trial, fewer than 300 events, wide confidence interval, no details about PFMT interventions). 3Downgraded three levels due to very serious risk of selection bias, inconsistency and imprecision (fewer than 300 events, wide confidence interval) and serious indirectness (no details about the PFMT intervention in one trial with about half the weighting in the pooled estimate). 4Downgraded two levels due to serious indirectness and imprecision (single trial, fewer than 300 participants, wide confidence interval). The outcome measures relate to the presence of incontinence symptoms rather than absence. As this comparison addresses the effect of PFMT for treatment of existing continence symptoms, the data are "negative," that is continuing incontinence rather than cure. Symptoms of urinary and faecal incontinence were measured based on self‐report. | ||||||
| Antenatal pelvic floor muscle training compared to control for mixed prevention and treatment of urinary and faecal incontinence | ||||||
| Patient or population: pregnant women some of who were incontinent symptoms and some who were not when randomised Setting: health services, obstetric clinics or hospitals in Brazil, China, France, Italy, Norway, UK or USA Intervention: antenatal PFMT Comparison: control (no PFMT, usual care or unspecified control) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with antenatal PFMT | |||||
| Urinary incontinence in late pregnancy | Study population | RR 0.74 | 3164 | ⊕⊕⊝⊝ | RR suggests clinically important effect but the upper limit of the CI suggests lack of clinical importance. | |
| 575 per 1000 | 425 per 1000 | |||||
| Urinary incontinence mid‐postnatal period (> 3‐6 months) | Study population | RR 0.73 | 1921 | ⊕⊝⊝⊝ | RR suggests clinically important effect but the upper limit of the CI suggests lack of clinical importance. | |
| 363 per 1000 | 265 per 1000 | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.85 | 244 | ⊕⊕⊝⊝ | RR suggests clinically important effect but the CI includes no effect. | |
| 448 per 1000 | 381 per 1000 | |||||
| Faecal incontinence in late pregnancy | Study population | RR 0.61 | 867 | ⊕⊕⊕⊝ | Wide CI including no effect. | |
| 43 per 1000 | 26 per 1000 | |||||
| Faecal incontinence mid‐postnatal period (> 3‐6 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Incontinence‐specific quality of life late postnatal period (> 6‐12 months) (ICIQ‐SF) | Mean 2.1, SD 3.3 | Mean 1.9, SD 3.7 | MD 0.2 lower | 190 | ⊕⊕⊝⊝ | MD and CI suggest lack of clinically important effect. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; ICIQ‐SF: International Consultation on Incontinence ‐ Short Form; MD: mean difference; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio; SD: standard deviation. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Downgraded two levels due to serious inconsistency (statistically significant heterogeneity) and indirectness (limited details about PFMT intervention in two trials with more than one‐quarter of the weighting in the pooled estimate). 2Downgraded three levels due to serious risk of selection bias (no information about random allocation concealment in three trials carrying more than 50% of weighting in the pooled estimate), serious imprecision (statistically significant heterogeneity) and serious indirectness (includes two trials carrying about 40% of the weighting in the pooled estimate with no information about PFMT intervention). 3Downgraded two levels due to serious indirectness (no information about PFMT in one trial with more than two‐thirds of the weighting in the pooled estimate) and serious imprecision (fewer than 300 event). 4Downgraded one level due to serious imprecision (single trial with fewer than 300 events). 5Downgraded two levels due to serious indirectness (single trial, no information about PFMT intervention) and serious imprecision (fewer than 300 events). The outcome measures relate to the presence of incontinence symptoms rather than absence. For those comparisons that addressed the effect of PFMT for treatment of existing continence symptoms, the data were "negative," that is continuing incontinence rather than cure. Symptoms of urinary and faecal incontinence were measured based on self‐report. | ||||||
| Postnatal pelvic floor muscle training compared to control for treatment of urinary and faecal incontinence | ||||||
| Patient or population: postnatal women who were incontinent when randomised Setting: health services or obstetric clinics in Canada, Republic of Korea, New Zealand and UK Intervention: postnatal PFMT Comparison: control (no PFMT or usual care) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with postnatal PFMT | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.55 | 696 | ⊕⊝⊝⊝ | RR suggests clinically important effect but the CI includes no effect. | |
| 724 per 1000 | 398 per 1000 | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.68 | 620 | ⊕⊝⊝⊝ | RR suggests clinically important effect but the CI includes no effect. | |
| 137 per 1000 | 93 per 1000 | |||||
| Incontinence‐specific quality of life | Mean 21.22, SD 2.11 | Mean 19.56, SD 1.88 | MD 1.66 lower | 18 | ⊕⊝⊝⊝ | Wide CI including no effect. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). BFLUTS: British Female Lower Urinary Tract Symptoms questionnaire; CI: confidence interval; MD: mean difference; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio; SD: standard deviation. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Downgraded three levels due to very serious risk of selection bias (two trials with 90% of weighting in pooled estimate at high risk) and inconsistency (statistically significant heterogeneity), and serious indirectness (two trials with 90% of weighting in pooled estimate provide insufficient information about the intervention). 2Downgraded three levels due to very serious risk of selection bias (two trials with 100% of weighting in pooled estimate at high risk), inconsistency (statistically significant heterogeneity) and imprecision (fewer than 300 events, wide confidence interval) and serious indirectness (neither trial provides sufficient information about the intervention). 3Downgraded three levels due to very serious risk of selection bias and imprecision (fewer than 300 events, wide confidence interval). The outcome measures relate to the presence of incontinence symptoms rather than absence. As this comparison addresses the effect of PFMT for treatment of existing continence symptoms, the data are "negative," that is continuing incontinence rather than cure. Symptoms of urinary and faecal incontinence were measured based on self‐report. | ||||||
| Postnatal pelvic floor muscle training compared to control for mixed prevention and treatment of urinary and faecal incontinence | ||||||
| Patient or population: postnatal women some of whom had incontinent symptoms and some of whom had not when randomised Setting: health services or hospitals in Australia, China and Switzerland Intervention: postnatal PFMT Comparison: control (no PFMT or usual care) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with postnatal PFMT | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.88 | 826 | ⊕⊝⊝⊝ | Wide CI including no effect. | |
| 294 per 1000 | 212 per 1000 | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.73 | 107 | ⊕⊝⊝⊝ | Wide CI including no effect. | |
| 54 per 1000 | 39 per 1000 | |||||
| Incontinence‐specific quality of life | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Downgraded three levels due to serious inconsistency (statistically significant heterogeneity) and imprecision (fewer than 300 events, wide confidence interval). 2Downgraded three levels due to very serious risk of selection bias and imprecision (fewer than 300 events, wide confidence interval) and serious indirectness (no information about the PFMT intervention). The outcome measures relate to the presence of incontinence symptoms rather than absence. For those comparisons that address the effect of PFMT for treatment of existing continence symptoms, the data are "negative," that is continuing incontinence rather than cure. Symptoms of urinary and faecal incontinence were measured based on self‐report. | ||||||
| Study ID | Voluntary pelvic floor muscle contraction confirmed? | PFMT parameters | PFMT supervision | Control comparison | Adherence | Notes |
| (treatment trial) | Vaginal palpation performed by study midwife: after randomisation and at each of the 3 visits to midwife (PFMT and control groups). | PFMT started with 3 fast contractions, followed by 3 sets of 8‐12 slow velocity, near maximal contractions, 6‐sec hold; 7 days per week for 6 months. Received written instructions on PFMT, but no information provided on PFMT progression. | Visit to the study midwife every 6th week (3 times during study period). | Usual care: written information describing PFM anatomy and PFMT. Received instructions on how to correctly perform PFM contraction (vaginal palpation) from midwife. | Women in the PFMT group were asked at each midwife visit how often they did PFMT; results not reported. | PFMT in lying or sitting positions. |
| (prevention trial) | Perineometry (at 1st meeting), but unclear by whom (PFMT group). | 5‐10 slow PFM contractions with 6‐sec hold, rest 6 sec between contractions with 3 rapid contractions at the end (as per Mørkved 2003). Daily PFMT in 4 positions, and 1 group (27 women) had 5 supervised sessions with a physiotherapist. Received manual of home PFMT exercises and asked to complete an exercise diary. | Supervised PFMT (27 women): received up to 5 monthly supervised exercise sessions with physiotherapist (22, 26, 30, 34, 38 weeks' gestation). Unsupervised PFMT (27 women): trained to perform PFMT by physiotherapist (1 session). | Did not receive intervention and did not exercise. | Not reported, although it stated that no dropouts occurred throughout the duration of the study due to all women in the PFMT group complying with the exercise protocol. | PFMT in a variety of positions including left side lying, sitting, reclined sitting, sitting with legs crossed, standing. Translation (Portuguese). |
| (prevention trial) | Not reported. | PFMT included in the 7‐ to 8‐min cool‐down period as part of a 35‐ to 45‐min exercise session, 3 days per week for duration of pregnancy (potential mean of 85 sessions in total). No specific details provided about PFMT programme. | Group exercise classes, supervised by a qualified fitness specialist, with the assistance of an obstetrician. | Not reported. | Adherence to PFMT was 90%. | General exercises targeted major muscles of arms and abdomen to promote good posture and prevent low back pain, and in the 3rd trimester strengthen the muscles of labour and PF. 1 session of aerobic dance per week. Accompanied by music. |
| (mixed prevention and treatment trial) | Participants did not have individual assessment of correct voluntary PFM contraction (due to pragmatic nature of study). Instructors were trained in how to explain a correct PFM contraction. | PFMT included as part of 15‐min strength training session within a 60‐min group exercise class. PFMT: 3 sets of 8‐12 maximal contractions, 6‐ to 8‐sec hold; strong verbal motivation to perform close to maximum PFM contractions. Women encouraged to participate in at least 2 out of 3 fitness classes per week for 12 weeks. Daily PFMT at home: 3 sets of 8‐12 close to maximum PFM contractions. Also encouraged to be physically active for at least 30 min per day. Received a specific PFMT brochure. | Group exercise classes, 2 or 3 per week for 12 weeks, led by certified aerobic instructors. Instructors were taught by a physiotherapist with > 20 years of experience in assessing, treating and researching women with PF dysfunction. | Usual antenatal care. | Mean adherence to exercise classes was 17.2 out of a possible 24 sessions. 40% (21/52) of women attended at least 80% of sessions. | PFMT integrated into aerobic dance class (accompanied by music): 5‐min warm‐up; 30‐min low‐impact aerobics; 15‐min strength training (including PFMT); 5‐min stretching and relaxation. PFMT in a variety of position including sitting, kneeling and standing. Informed of deep abdominal muscle co‐contraction during maximal PFM contraction. |
| (mixed prevention and treatment trial) | Visual inspection of perineum (PFMT group). | Maximum of 6 voluntary PFM contractions per set; 3‐6 sec hold; 3 sets per day; for 8 weeks. | PFMT taught 1‐to‐1 with physiotherapist. 1 (20 min) contact in hospital, and another (30 min) 8 weeks later at home or hospital. | Routine postnatal care; usual postnatal leaflet given; invitation to join postnatal class on ward; no restriction on PFMT if recommended by other health professional. | 84% (292/348) of women in the PFMT group and 58% (189/328) of controls were performing PFMT at "adequate" level at 3 months' postpartum. | Women were "asked if they were performing their PF exercises." |
| (treatment trial) | Not reported. | 5‐6 biweekly sessions. No specific details provided about PFMT. | Supervised by a physiotherapist. | Similar unsupervised PFMT at home. | Not reported. | Conference abstract. |
| (treatment trial) | Vaginal digital palpation (both PFMT and control groups). | Progressive PFMT programme. Level 1: 3 sets of 10 near maximal contractions; 3‐sec hold, 3‐sec rest; quick contraction, 1‐sec hold, 1‐sec rest; twice daily. Level 2: 3 sets of 10 near maximal contractions; 5‐sec hold, 5‐sec rest; quick contraction, 2‐sec hold, 2‐sec rest; twice daily. Level 3: 3 sets of 15 near maximal contractions; 10‐sec hold, 10‐sec rest; quick contraction, 2‐sec hold, 2‐sec rest; 3 per day. | Trained by a researcher on how to do PFMT in accordance with booklet of PFM exercises. | Usual care: instructed on how to perform a correct PFM contraction, but did not receive training about exercises. | Not reported. | In 2nd stage of study, 68% of women in study group were contracting the proper muscle group. The rest were given more training and reassessed 1 week later. |
| (mixed prevention and treatment trial) | Not reported. | Not reported. | Not reported. | Not reported. | Not reported. | Conference abstract. |
| (treatment trial) | Not reported. | 8‐12 close to maximal voluntary PFM contraction per set; 6‐ to 8‐sec hold each with 3‐4 fast contractions at the end of each contraction; 6‐sec rest between contractions; 3 sets per day; 5 days per week; for 8 weeks. Also taught 'the knack' (voluntary PFM contraction prior to hard cough and maintained through cough until abdominal wall relaxed). | PFMT taught 1‐to‐1 with physiotherapist. | Same number of physiotherapy contacts for relaxation massage of back and extremities; asked not to do PFMT at home. | Not reported. | In addition to PFMT 15 min of electrical stimulation (biphasic rectangular form, 50 Hz, pulse width 250 msec, duty cycle 6 sec on and 18 sec off for 1st 4 weeks, then 8 sec on and 24 sec off for next 4 weeks, at maximal tolerated current intensity) and 25 min of electromyographic biofeedback per appointment. |
| (mixed prevention and treatment trial) | Not reported. | 6 months. | PFMT taught 1‐to‐1 with physiotherapist in hospital. | Standard care including verbal promotion of PFMT and leaflet on PFMT. | Of 117 women in the PFMT group, 114 were visited by the physiotherapist in hospital, 21 attended the 2‐month PFMT group, and 5 attended the 4‐month group. | ‐ |
| (mixed prevention and treatment trial) | Vaginal digital palpation at each session (possibly by physiotherapist, but not stated; PFMT group). | 1 session per week (20‐30 min), total of 8 sessions between 6th and 8th month of pregnancy. Also 'the knack' (voluntary PFM contraction prior to increasing intra‐abdominal pressure). Provided with written information on PF anatomy and PFMT, and encouraged to perform daily PFMT at home, 10‐20 contractions. | Individually supervised by a physiotherapist or midwife at each session. In total, 37 different therapists (all trained by the same specialist physiotherapist) were involved in delivering the exercises. | Usual care, including written information on PF anatomy and PFMT (encouraged to perform daily at home, 10‐20 PFM contractions). | 69.3% (97/140) of women in the PFMT group completed all planned sessions, and 82.8% (116/140) completed at least 1 session (4‐8, median 8). At the end of pregnancy, women in both groups reported a similar frequency and duration of PFMT (including number of contractions). PFMT was performed daily at home by 4.3% (6/140) of PFMT women and 10.6% (15/142) of controls, at the end of pregnancy. | PFMT performed in standing (5 min) and lying (10 min). |
| (mixed prevention and treatment trial) | Not reported. | Standard postpartum discharge instructions plus written and verbal instructions for PFMT. | Not reported. | Standard postpartum discharge instructions. | Not reported. | Conference abstract. |
| (mixed prevention and treatment trial) | Not reported. | 2 weekly session of Kegel exercises; 8 weeks. Daily home exercises (20 min) and stretching. | Not reported. | Did not receive any PFMT, no other details provided. | Not reported. | Conference abstract. |
| (prevention trial) | Not reported. | 12‐week PFMT programme. | PFMT supervised by a physiotherapist and midwife. | Routine care and PFM exercises, customary instruction at intake visit. | Not reported. | Conference abstract. |
| (treatment trial) | Not reported. | 8‐10 sessions of fast and slow voluntary PFM contraction per day with aim of 80‐100 per day; for up to 8 months. | PFMT taught 1‐to‐1 with nurse, health visitor or continence advisor. | Usual antenatal and postnatal care that may have included advice on PFMT. | 78% (218/278) of women in the PFMT group and 48% (118/244) of controls had done some PFMT in the 11th postnatal month. Mean (SD) number of voluntary PFM contractions per day at 12 months' postnatal: PFMT group 20 (29) and controls 5 (15). | Frequency and urgency strategies added if needed at 7 or 9 months postnatally. 52.7% (394/747) of women at 6 years' follow‐up and 70.1% (471/672) of women at 12 years' follow‐up completed a questionnaire. About 50% of women in PFMT and control groups were performing any PFMT at both time points. Daily PFMT was undertaken by 6% (17/263) of PFMT women compared to 12% (29/253) of control women at 6 years; and 7% (15/227) of PFMT group compared to 8% (20/241) of control women at 12 years. |
| (prevention trial) | Surface electromyography (electrodes either side of anus; PFMT group). | 10 voluntary PFM contraction; 8‐sec hold followed by 3 fast, 1‐sec contractions; 6‐sec rest between contractions; for up to 20 weeks. Asked to complete an exercise diary. | PFMT taught 1‐to‐1 with physiotherapist. | Requested not to do PFMT during pregnancy or postnatally. | 63% attended all 8 physiotherapy appointments, 21% attended 7 appointments. | Electromyographic biofeedback at each appointment. |
| (mixed prevention and treatment trial) | Vaginal digital palpation (PFMT and control groups). | Progressive supervised PFM training programme (as per Mørkved 1997) for 16 weeks. Daily PFMT at home, 3 sets of 8‐12 close to maximal contractions. Customary written information on discharge from postnatal ward. Asked to complete an exercise diary. | Supervised exercise class from 6 weeks' postpartum, led by an experienced physiotherapist, once per week for 16 weeks. Class attendance was documented. | Usual care. Received customary written information on discharge from postnatal ward. At 6 weeks were instructed on how to perform a correct PFM contraction (verified with vaginal digital palpation). | 96% (72/75) of women in the PFMT group who completed the trial adhered to 80% of the class and daily home training. In the control group (retrospective questioning), 16.5% reported performing daily PFMT at home ≥ 3 times per week. | 4% (7/175) of women were unable to perform a voluntary PFM contraction at baseline. At baseline (6 weeks' postpartum) more women in the control group were performing PFMT ≥ 3 times or more per week. |
| (mixed prevention and treatment trial) | Vaginal digital palpation (PFMT and control groups). | Daily; for up to 11 months. | 1 individual session with physiotherapist, and 1 group PFMT session led by physiotherapist at 22‐25 weeks' gestation with maximum of 6 women per group. | Usual antenatal and postnatal care that may have included advice on PFMT (personal communication). | 79% (461/586) of women in PFMT group attended group PFMT session (personal communication). | 3.5% (16/460) of women who attended group PFMT session could not perform a voluntary PFM contraction after teaching, and 2.8% (13/460) of women could contract but not sustain a contraction (personal communication). Conference abstract. |
| (treatment trial) | Perineometer (vaginal probe) used to ensure PFM contraction and assess control of contraction in both PFMT and control groups. Unclear if this was performed every session with the PFMT women. | 20 maximal voluntary PFM contractions, 10‐sec hold, 3 times per week; for 8 weeks (as part of a class), and daily at home. Progressed by changing position (prone, sitting and standing). Initial session included information on PFM anatomy and function. Also provided with a booklet which included a training programme and an exercise diary. | Supervised training sessions (1‐hour duration) with a specialist physiotherapist (23 in total, unclear if individual contacts or group classes). | Usual care. Received the same information and demonstration session as PFMT group and instructions on how to correctly perform PFM contraction (perineometer). Unsupervised, daily PFMT for 8 weeks. | Not reported. | PFMT integrated with trunk stabilisation exercises (progressive abdominal strengthening, bridging, and side‐bridge). |
| (mixed prevention and treatment trial) | Observation of inward movement of perineum during contraction (PFMT group). | 3 repetitions of 8 PFM contractions, 6‐sec hold each, 2‐min rest between repetitions; repeated twice daily at home with additional training in groups once per week for 45 min for 12 weeks. Asked to complete an exercise diary. | Group training sessions (10 women) supervised by a physiotherapist once per week for 12 weeks. | Regular antenatal care and the customary written postpartum instructions that did not include PFMT from the hospital. Not discouraged from performing PFMT on their own. | > 80% attended every training session and 0 were absent more than twice. At 35 gestational weeks, 87% of PFMT group reported practice of PFMT ≥ 75% of the time. | Group training was performed in sitting and standing positions with legs apart to emphasise specific strength training of the PFM and relaxation of other muscles. |
| (prevention trial) | Observation of inward movement of perineum or digital vaginal palpation, or both (PFMT group). Vaginal digital palpation used to teach PFM contraction in 23.5% (16/68) of women. | 3 sets of 10 maximal voluntary PFM contractions at level 3 (2‐sec hold, 2‐sec rest for strength; 10‐sec hold, 10‐sec rest for endurance); 3 sessions per day during pregnancy and postpartum. Women received education about the anatomy and functions of the PFM and PFMT (unclear from whom) and were asked to complete an exercise diary (including progressions). | Exercise compliance was checked at every hospital visit (9‐10 visits on average, over a minimum of 12 weeks), and pregnant women were called once per month to encourage regular exercise. | Not instructed to do PFMT. Once data collection complete, controls received PFMT and a brochure with the relevant information during the 12th week home visit. | Women asked to record the number of times they did their exercises. No data reported. | Digital vaginal palpation was refused by 52/68 women due to concerns about pregnancy, cultural/religious reasons. Unclear if women progressed through levels 1‐3 or started at level 3, whether they did 3 sets of 10 exercises per day or 3 sets of 10 exercises 3 times per day, or how the sets were divided between endurance and strength training. |
| (mixed prevention and treatment trial) | Not reported. | PFM (Kegel) exercises undertaken 2‐3 times per day for 20‐30 min or 150‐200 contractions (3‐sec hold then relax), performed until 12 months' postpartum. Biofeedback used twice per week (no further details available). | Not reported who supervised the programme, or the number and type of contacts with health professional(s). | Usual care: received standard postpartum information. | Not reported. | Translation (Chinese). |
| (mixed prevention and treatment trial) | Not reported. | PFMT 2‐3 times per day, 15‐30 min each set (4‐ to 6‐sec hold, 10‐sec relaxation), started after birth and continued for ≥ 10 weeks. | Exercises taught by experienced midwives who also supervised the programme (number and type of contacts/visits unclear). | Usual care: standard postpartum information. Unclear if this included PFMT. | Not reported. | Translation (Chinese). Positions of exercises included supine, sitting or any other position, with legs slightly separated, with instructions to contract anus, vaginal and urinary tract while breathing in, and to relax with expiration. |
| (mixed prevention and treatment trial) | Not reported. | Up to 8 months; no details of PFMT provided. Each clinic session was followed by 20 min of biofeedback and 15 min of electrical stimulation. | 12 sessions (6 weeks) with a physiotherapist between 2 and 10 months postnatally. | No intervention. Women received PFMT education after 3rd assessment at 10 months' postpartum. | Not reported. | In addition to PFMT, 20 min of biofeedback and 15 min of electrical stimulation (vaginal electrode, biphasic rectangular waveform, pulse width 200‐400 msec, frequency 50 Hz, intensity 15‐15 mA, contraction time 6 sec, rest time 12 sec) per appointment. |
| (mixed prevention and treatment trial) | Instructed on correct contraction, but not verified (due to pragmatic nature of study). | PFMT (maximal rapid and sustained PFM contractions) performed as part of a class (50 min) for a median of 5 (range 2‐10) sessions between 18‐24 weeks' to 36‐38 weeks' gestation. Provided with an exercise guide and asked to do daily PFMT at home (30 rapid, 20 sustained (10‐sec hold) contractions), as well as 30‐min daily aerobic exercise (no specific examples provided). Received standard antenatal education and asked to complete an exercise diary. | Supervised by a trained study physiotherapists on a monthly basis. Either group or individual training sessions, depending on the number of women present. | Usual care: received standard antenatal and postnatal education (on labour, breastfeeding and pain relief) by trained physiotherapy, nursing and medial staff. | Analysis of adherence in intervention group was not possible as women failed to complete or return their exercise diaries. | PFMT performed in standing and sitting position. PFMT integrated into non‐aerobic exercise programme designed to reduce back pain. Included abdominal, stretching and relaxation exercises and exercises designed to promote venous return. |
| (mixed prevention and treatment) | Vaginal digital palpation and observation of perineum (both PFMT and control groups). | 8‐12 near maximal voluntary PFM contractions; 6‐ to 8‐sec hold each, 3‐4 fast contractions at the end of each contraction; 6‐sec rest between contractions; twice daily at home; for ≤ 8 months. Also asked to attend weekly 60‐min PFMT class for 12 weeks. Women asked to complete an exercise diary. | Group training session (10‐15 women), once per week for 12 weeks, supervised by physiotherapists (5 in total). | Usual antenatal and postnatal care that may have included advice on PFMT. Correct PFM contraction verified. Not discouraged from doing PFMT on their own. | 19% (28/148) of PFMT women attended less than half the 12 weekly PFMT classes and did not return training diaries. | During exercise class voluntary PFM contraction undertaken in a range of body positions (lying, sitting, kneeling and standing with legs apart). PFMT interspersed with abdominal, back and thigh muscle exercises (accompanied by music). 62% (188/280) of women completed a questionnaire at 6‐year follow‐up, and 45% of women in both the former PFMT and control groups were doing PFMT at least weekly. |
| (mixed prevention and treatment trial) | Contraction assessed with anal biofeedback as part of training session (by obstetrician or specialist nurse); PFMT group. | Sets of 10 PFM contractions (Kegel exercises), 5‐sec hold; 10‐sec rest between contractions; twice daily for 5 min with biofeedback; for 3 months. Standard postpartum education by midwives or physiotherapists, including written information. Women asked to complete an exercise diary. | Biofeedback (electromyographic) training provided at initial session, but no further contact with health professionals. | Usual care: "conventional PFM training," but no details provided. Women asked to complete an exercise diary. | Poor adherence defined as performing < 70% of the intended home exercise sessions. 7/30 women in the PFMT group reported poor adherence. | The portable biofeedback machines were programmed to the electromyography setting with the work period set to 10 contractions (5‐sec duration) with a 10‐sec rest between each contraction. PFMT for treatment of FI. |
| (prevention trial) | Instructed on correct contraction, but not formally verified. Women were asked to test themselves at home by stopping the flow of urine, digital palpation or using a mirror to observe the perineum (PFMT group). | PFMT programme, 3 times per week; for ≥ 22 weeks. Started with 1 set of 8 contractions increasing to 100; divided into different sets of slow (6 sec) and fast (5 as fast as possible) contractions. Unclear if this progression related to class or home exercises. Daily PFMT at home, 100 contractions in different sets. Received standard antenatal education about PFM. | Group training sessions (8‐12 women) designed and supervised by a physical activity and sport sciences graduate; 55‐ to 60‐min duration (10 min of PFMT); 70‐78 sessions in total. | Usual care: follow‐up by midwives, standard information about PFMT. Women were not asked not to do PFMT. | All women included in analysis attended ≥ 80% of exercise sessions. | PFMT integrated into supervised exercise programme; 30 min low‐impact aerobics including general strength training, PFMT and cool down (stretching, relaxation or massage); sometimes accompanied by music. PFMT in a variety of positions. Women wore heart rate monitors to control exercise intensity. |
| (prevention trial) | Unclear, but seems likely as physiotherapists gave individualised programmes to those unable to follow exercise regimen due to inability to do voluntary PFM contraction (PFMT group). | 8‐12 voluntary PFM contractions; 6‐sec hold each; 2‐min rest between each set of contractions; 3 sets of 8‐12 contractions twice daily; for about 20 weeks (as described by Bø 1995). | About 5 (monthly) contacts with physiotherapist between 20 weeks' gestation and delivery. | Usual antenatal and postnatal care that may have included advice on PFMT. Women appeared to have had same number of clinic visits as the PFMT group, and were asked if doing PFMT at each of these visits. | 43% (52/120) of women in the PFMT group did not return an exercise diary; 11% (13/120) completed < 28 days of PFMT; and 46% (55/120) completed ≥ 28 days. When asked postnatally, 28% (33/120) of PFMT women and 34% (37/110) of controls were doing occasional or no PFMT. | If unable to follow PFMT regimen then individualised programme until able to do so. 71% (164/230) of women completed a telephone questionnaire at 8‐year follow‐up, and 68.4% of women were doing PFMT, with 38% stating they were doing PFMT twice or more per week. |
| (mixed prevention and treatment trial) | Yes, but unclear how or by whom (PFMT group). | PFMT tailored to individual ability. 30 maximal or near maximal voluntary PFM contraction per day; for ≤ 17 months. | Not reported. | Usual antenatal and postnatal care; no systematic PFMT programme. | At 35 weeks' gestation, 85% of women in the PFMT group reported to be doing PFMT 75% of the time. At 1 year, PFMT adherence reported to vary between 62% and 90%. | ‐ |
| (treatment trial) | Assessed by ability to stop or slow the flow of urine for 1‐2 sec (PFMT group). | 20 sets of PFM exercises, twice daily, at least 5 days per week, for 6 weeks. 1 set of PFM exercises was 1 slow contraction (10‐sec hold), followed by 10 fast contractions; no progression in number of contractions per set. Also received a handbook with information on stress UI, PFM function, instructions on PFMT and a urinary diary. | Supervised group sessions (4‐5 women) with a midwife; 45 min; once every 2 weeks for 6 weeks (3 sessions in total). | Usual care: from health professionals, obstetricians or midwives. Did not receive information about UI and received no training support about performing correct PFM exercises. | No women were excluded for failing to perform the PFMT for < 28 (of approximately 42) days. | PFMT performed in various positions including lying down, sitting and standing. |
| (treatment trial) | Not reported. | Not reported. | "One to one teaching about pelvic floor exercises." | "Conventional care (hand‐out information about pelvic muscle exercises)." | Not reported. | Conference abstract. |
| (mixed prevention and treatment trial) | Not reported. | As for controls with additional section in leaflet recommending a specific exercise each week that integrated voluntary PFM contraction with usual activities of daily living; up to 3 months. Asked to complete a daily exercise diary for 4 weeks. | 1‐to‐1 session with midwife co‐ordinator each postnatal day in hospital. | Usual antenatal and postnatal care including PFMT leaflet; might include PFMT at antenatal class or postnatal class on ward (or both); instructed to do voluntary PFM contraction as often as remembered and mid‐stream urine stop. | At 10 days postnatally, 78% of PFMT group and 68% of controls were doing some PFMT; with 58% of PFMT group and 42% of controls doing some PFMT at 3 months. | ‐ |
| (mixed prevention and treatment trial) | Vaginal digital palpation (PFMT group). | 8‐12 near maximal voluntary PFM contractions; 6‐ to 8‐sec hold each with 3 fast contractions at the end of each contraction. Asked to perform PFM exercises as part of a 45‐min home programme at least twice per week or a weekly 60‐min exercise class (or both). Received written information including brochure with an evidence‐based PFMT programme, and asked to complete an exercise diary. | Group training sessions (8‐15 women) supervised by physiotherapist, 60 min, once per week for 12 weeks | Usual care: received customary information from midwife or GP. Also given a detailed information brochure including evidence‐based PFMT programme. Women were not discouraged from exercising. | Adherence to the general exercise protocol (exercising ≥ 3 days per week, moderate to high intensity) was 55% (217/397) in the PFMT group and 10% (36/365) in the control group. 67% of the PFMT group performed PFMT ≥ 3 times per week compared to 40% in the control group | PFMT integrated into standardised exercise programme: 30‐ to 35‐min low‐impact aerobics; 20‐ to 25‐min strengthening exercises (including PFMT, 3 sets of 10 reps); 5‐ to 10‐min stretching and relaxation. PFMT performed in a variety of positions, with legs apart to emphasise specific strengthening of the PFM. |
| (prevention trial) | Not reported. | 12 contractions, 3 times daily. | Seen twice monthly throughout pregnancy, and every 3 months postnatally for 1 year. | "Other (placebo) including no pelvic floor exercises." | Not reported. | Conference abstract. |
| (mixed prevention and treatment trial) | Assessment of PFM strength and contraction by an obstetrician (PFMT group; no further details) | Anal contraction; 3‐sec hold (while inhaling) followed by relaxation with 3‐5 faster contractions at the end of each contraction; 15‐30 min each set; twice daily; 6‐8 weeks. | Exercises taught by experienced midwives but unclear who supervised the programme of the number and type of contacts/visits. | Usual care: no other details provided other than "conventional guidance." | Not reported. | PFMT performed in a variety of positions including lying down, sitting or standing. Translation (Chinese). |
| (treatment trial) | Not reported. | Mix of fast and slow voluntary PFM contractions 8‐10 times per day with aim of 80‐100 voluntary PFM contraction daily; up to 9 months. | 1‐to‐1 sessions with physiotherapist at 3, 4, 6 and 9 months postnatally. | Usual PFMT as taught in antenatal and postnatal classes. | Mean (95% CI) number of daily voluntary PFM contraction at 12 months' postnatally was 86 (69‐104) in the PFMT group and 35 (30 to 40) in the control group. | Perineometry for biofeedback at each appointment. Mean time to teach PFMT to the PFMT group was 32 (95% CI 30 to 34) min. |
| Observation and palpation of perineal body by physiotherapists. Women also encouraged to practice self‐palpation (PFMT group). | Not reported. At each visit, women were asked about the frequency and duration of PFMT. | 1‐to‐1 30‐min sessions with physiotherapist. 4 in total: 3 antenatally and 1 at 6 weeks postnatally. In total, 25 physiotherapists (specialised in PFMT) were involved in delivering the exercises. | Usual antenatal and postnatal care including advice on PFMT; nearly two‐thirds received some instruction on PFMT. | At 35 weeks' gestation, 6% reported no PFMT, 17% reported some PFMT, 40% were doing PFMT at low intensity and 37% were exercising intensively in the PFMT group vs 36% reported no PFMT, 25% reported some PFMT, 26% were doing PFMT at low intensity and 14% were exercising intensively in the control group. | ‐ | |
| CI: confidence interval; FI: faecal incontinence; min: minute; PF: pelvic floor; PFM: pelvic floor muscle; PFMT: pelvic floor muscle training; SD: standard deviation; sec: second; UI: urinary incontinence. | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Urinary incontinence in late pregnancy Show forest plot | 6 | 624 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.20, 0.72] |
| 1.1 PFMT versus no PFMT | 2 | 174 | Risk Ratio (M‐H, Random, 95% CI) | 0.14 [0.01, 2.04] |
| 1.2 PFMT versus usual care | 4 | 450 | Risk Ratio (M‐H, Random, 95% CI) | 0.44 [0.22, 0.91] |
| 2 Urinary incontinence early postnatal period (0‐3 months) Show forest plot | 5 | 439 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.17, 0.83] |
| 2.1 PFMT versus no PFMT | 2 | 174 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.11, 0.67] |
| 2.2 PFMT versus usual care | 2 | 198 | Risk Ratio (M‐H, Random, 95% CI) | 0.30 [0.04, 2.31] |
| 2.3 PFMT versus unspecified control | 1 | 67 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.43, 1.79] |
| 3 Urinary incontinence mid‐postnatal period (> 3‐6 months) Show forest plot | 5 | 673 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.54, 0.95] |
| 3.1 PFMT versus no PFMT | 1 | 86 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.35, 2.20] |
| 3.2 PFMT versus usual care | 4 | 587 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.70 [0.52, 0.94] |
| 4 Urinary incontinence late postnatal period (> 6‐12 months) Show forest plot | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.20 [0.65, 2.21] |
| 4.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.2 PFMT versus usual care | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.20 [0.65, 2.21] |
| 4.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5 Urinary incontinence medium term (> 1‐5 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 5.1 PFMT versus no PFMT | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 PFMT versus usual care | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.3 PFMT versus unspecified control | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 Urinary incontinence long term (> 5 years) Show forest plot | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 6.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6.2 PFMT versus usual care | 2 | 352 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [0.77, 1.48] |
| 6.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 7 Faecal incontinence late pregnancy | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 7.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 7.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 7.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 8 Faecal incontinence early postnatal period (0‐3 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 9 Faecal incontinence mid‐postnatal period (> 3‐6 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 10 Faecal incontinence late postnatal period (> 6‐12 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11 Faecal incontinence medium term (> 1‐5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12 Faecal incontinence long term (> 5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13 Incontinence‐specific quality of life Show forest plot | 1 | 152 | Mean Difference (IV, Fixed, 95% CI) | ‐2.42 [‐3.32, ‐1.52] |
| 13.1 PFMT versus no PFMT | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13.2 PFMT versus usual care | 1 | 152 | Mean Difference (IV, Fixed, 95% CI) | ‐2.42 [‐3.32, ‐1.52] |
| 13.3 PFMT versus unspecified control | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 14 Severity of incontinence Show forest plot | Other data | No numeric data | ||
| 14.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 14.2 PFMT versus usual care | Other data | No numeric data | ||
| 14.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 15 Loss of urine under stress test late pregnancy Show forest plot | 1 | 102 | Risk Ratio (M‐H, Random, 95% CI) | 0.36 [0.19, 0.70] |
| 15.1 PFMT versus no PFMT | 1 | 102 | Risk Ratio (M‐H, Random, 95% CI) | 0.36 [0.19, 0.70] |
| 16 Loss of urine under stress test early postnatal period (0‐3 months) Show forest plot | 3 | 322 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.35 [0.17, 0.75] |
| 16.1 PFMT versus no PFMT | 2 | 174 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.09 [0.02, 0.47] |
| 16.2 PFMT versus usual care | 1 | 148 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.33, 2.29] |
| 16.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 17 Quality of life and health status measures Show forest plot | Other data | No numeric data | ||
| 17.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 17.2 PFMT versus usual care | Other data | No numeric data | ||
| 17.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 18 Pelvic floor muscle function Show forest plot | Other data | No numeric data | ||
| 18.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 18.2 PFMT versus usual care | Other data | No numeric data | ||
| 18.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 18.4 PFMT plus vs PFMT | Other data | No numeric data | ||
| 19 Delivery outcome: caesarean section Show forest plot | 3 | 373 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.28 [0.89, 1.85] |
| 19.1 PFMT versus no PFMT | 1 | 76 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.83 [1.07, 3.15] |
| 19.2 PFMT versus usual care | 1 | 230 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.24 [0.66, 2.36] |
| 19.3 PFMT versus unspecified control | 1 | 67 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.29, 1.57] |
| 20 Delivery outcome: other Show forest plot | Other data | No numeric data | ||
| 20.1 PFMT versus no control | Other data | No numeric data | ||
| 20.2 PFMT versus usual care | Other data | No numeric data | ||
| 20.3 PFMT versus unspecified control | Other data | No numeric data | ||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Urinary incontinence late pregnancy Show forest plot | 3 | 345 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.44, 1.13] |
| 1.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 1.2 PFMT vs usual care | 3 | 345 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.44, 1.13] |
| 1.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 2 Urinary incontinence early postnatal period (0‐3 months) Show forest plot | 2 | 292 | Risk Ratio (M‐H, Random, 95% CI) | 0.75 [0.37, 1.53] |
| 2.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 2.2 PFMT versus usual care | 2 | 292 | Risk Ratio (M‐H, Random, 95% CI) | 0.75 [0.37, 1.53] |
| 2.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 3 Urinary incontinence mid‐postnatal period (> 3‐6 months) Show forest plot | 1 | 187 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.70, 1.24] |
| 3.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 3.2 PFMT versus usual care | 1 | 187 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.70, 1.24] |
| 3.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4 Urinary incontinence late postnatal period (> 6‐12 months) Show forest plot | 2 | 869 | Risk Ratio (M‐H, Random, 95% CI) | 0.50 [0.13, 1.93] |
| 4.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 4.2 PFMT versus usual care | 2 | 869 | Risk Ratio (M‐H, Random, 95% CI) | 0.50 [0.13, 1.93] |
| 4.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 5 Urinary incontinence medium term (> 1‐5 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Urinary incontinence long term (> 5 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 6.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 7 Faecal incontinence late pregnancy | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 8 Faecal incontinence early postnatal period (0‐3 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 9 Faecal incontinence mid‐postnatal period (> 3‐6 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 10 Faecal incontinence late postnatal period (> 6‐12 months) | 0 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 10.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 10.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 10.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 11 Faecal incontinence medium term (> 1‐5 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 11.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12 Faecal incontinence long term (> 5 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 12.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13 Faecal incontinence very long term (> 10 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 13.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 14 Incontinence‐specific quality of life Show forest plot | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | ‐3.5 [‐6.13, ‐0.87] |
| 14.1 PFMT versus no PFMT | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 14.2 PFMT versus usual care | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | ‐3.5 [‐6.13, ‐0.87] |
| 14.3 PFMT versus unspecified control | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 15 Quality of life and health status measures Show forest plot | Other data | No numeric data | ||
| 15.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 15.2 PFMT versus usual care | Other data | No numeric data | ||
| 15.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 16 Severity of incontinence Show forest plot | Other data | No numeric data | ||
| 16.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 16.2 PFMT versus usual care | Other data | No numeric data | ||
| 16.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 17 Pelvic floor muscle function Show forest plot | Other data | No numeric data | ||
| 17.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 17.2 PFMT versus usual care | Other data | No numeric data | ||
| 17.3 PFMT versus unspecified control | Other data | No numeric data | ||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Urinary incontinence late pregnancy Show forest plot | 9 | 3164 | Risk Ratio (M‐H, Random, 95% CI) | 0.74 [0.61, 0.90] |
| 1.1 PFMT versus no PFMT | 2 | 387 | Risk Ratio (M‐H, Random, 95% CI) | 0.24 [0.02, 2.53] |
| 1.2 PFMT versus usual care | 7 | 2777 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.72, 0.94] |
| 1.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 1.4 PFMT plus versus PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 2 Urinary incontinence early postnatal period (0‐3 months) Show forest plot | 5 | 760 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.67, 0.95] |
| 2.1 PFMT versus no PFMT | 1 | 300 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.51, 1.02] |
| 2.2 PFMT versus usual care | 3 | 367 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.67, 1.16] |
| 2.3 PFMT versus unspecified control | 1 | 93 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.77 [0.61, 0.97] |
| 3 Urinary incontinence mid‐postnatal period (> 3‐6 months) Show forest plot | 5 | 1921 | Risk Ratio (M‐H, Random, 95% CI) | 0.73 [0.55, 0.97] |
| 3.1 PFMT versus no PFMT | 1 | 300 | Risk Ratio (M‐H, Random, 95% CI) | 0.60 [0.38, 0.92] |
| 3.2 PFMT versus usual care | 3 | 1528 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.65, 1.11] |
| 3.3 PFMT versus unspecified control | 1 | 93 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.20, 0.86] |
| 4 Urinary incontinence late postnatal period (> 6‐12 months) Show forest plot | 2 | 244 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.85 [0.63, 1.14] |
| 4.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.2 PFMT versus usual care | 2 | 244 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.85 [0.63, 1.14] |
| 4.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5 Urinary incontinence medium term (> 1‐5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Urinary incontinence long term (> 5 years) Show forest plot | 1 | 188 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.38 [0.77, 2.45] |
| 6.1 PFMT versus usual care | 1 | 188 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.38 [0.77, 2.45] |
| 7 Faecal incontinence late pregnancy Show forest plot | 2 | 867 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.30, 1.25] |
| 7.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 7.2 PFMT versus usual care | 2 | 867 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.30, 1.25] |
| 7.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 8 Faecal incontinence early postnatal period (0‐3 months) Show forest plot | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.36 [0.04, 3.37] |
| 8.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 8.2 PFMT versus usual care | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.36 [0.04, 3.37] |
| 8.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 9 Faecal incontinence mid‐postnatal period (> 3‐6 months) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 9.1 PFMT versus no PFMT | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.2 PFMT versus usual care | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.3 PFMT versus unspecified control | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 Faecal incontinence late‐postnatal period (> 6‐12 months) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 10.1 PFMT versus no PFMT | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 PFMT versus usual care | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 PFMT versus unspecified control | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 Faecal incontinence medium term (> 1‐5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12 Faecal incontinence long term (> 5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13 Incontinence‐specific quality of life late pregnancy Show forest plot | 1 | 224 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐1.21, 0.81] |
| 13.1 PFMT versus no PFMT | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13.2 PFMT versus usual care | 1 | 224 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐1.21, 0.81] |
| 13.3 PFMT versus unspecified control | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 14 Incontinence‐specific quality of life early postnatal period (0‐3 months) Show forest plot | 1 | 211 | Mean Difference (IV, Fixed, 95% CI) | ‐0.60 [‐1.45, 0.25] |
| 14.1 PFMT versus no PFMT | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 14.2 PFMT versus usual care | 1 | 211 | Mean Difference (IV, Fixed, 95% CI) | ‐0.60 [‐1.45, 0.25] |
| 14.3 PFMT versus unspecified control | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 15 Incontinence‐specific quality of life late postnatal period (> 6‐12 months) Show forest plot | 1 | 190 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐1.20, 0.80] |
| 15.1 PFMT versus no PFMT | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 15.2 PFMT versus usual care | 1 | 190 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐1.20, 0.80] |
| 15.3 PFMT versus unspecified control | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 16 Severity of incontinence Show forest plot | Other data | No numeric data | ||
| 16.3 PFMT versus no PFMT | Other data | No numeric data | ||
| 16.4 PFMT versus usual care | Other data | No numeric data | ||
| 16.5 PFMT versus unspecified control | Other data | No numeric data | ||
| 17 Loss of urine under stress test early postnatal period (0‐3 months) Show forest plot | Other data | No numeric data | ||
| 17.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 17.2 PFMT versus usual care | Other data | No numeric data | ||
| 17.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 18 Quality of life and health status measures Show forest plot | Other data | No numeric data | ||
| 18.3 PFMT versus no PFMT | Other data | No numeric data | ||
| 18.4 PFMT versus usual care | Other data | No numeric data | ||
| 18.5 PFMT versus unspecified control | Other data | No numeric data | ||
| 19 Pelvic floor muscle function Show forest plot | Other data | No numeric data | ||
| 19.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 19.2 PFMT versus usual care | Other data | No numeric data | ||
| 19.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 19.4 PFMT plus vs PFMT | Other data | No numeric data | ||
| 20 Delivery outcome: caesarean section Show forest plot | 6 | 1899 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.79, 1.14] |
| 20.1 PFMT versus no PFMT | 1 | 300 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.12 [0.79, 1.57] |
| 20.2 PFMT versus usual care | 5 | 1599 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.73, 1.12] |
| 20.3 PFMT versus unspecified | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 21 Delivery outcome: other Show forest plot | Other data | No numeric data | ||
| 21.3 PFMT versus no PFMT | Other data | No numeric data | ||
| 21.4 PFMT versus usual care | Other data | No numeric data | ||
| 21.5 PFMT versus unspecified control | Other data | No numeric data | ||
| 22 Patient satisfaction and further treatment Show forest plot | Other data | No numeric data | ||
| 22.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 22.2 PFMT versus usual care | Other data | No numeric data | ||
| 22.3 PFMT versus unspecified control | Other data | No numeric data | ||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Urinary incontinence early postnatal period (0‐3 months) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 1.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 1.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2 Urinary incontinence mid‐postnatal period (> 3‐6 months) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 PFMT plus versus PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2.2 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2.3 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2.4 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 3 Urinary incontinence late‐postnatal period (> 6‐12 months) Show forest plot | 3 | 696 | Risk Ratio (M‐H, Random, 95% CI) | 0.55 [0.29, 1.07] |
| 3.1 PFMT versus no PFMT | 1 | 62 | Risk Ratio (M‐H, Random, 95% CI) | 0.29 [0.18, 0.47] |
| 3.2 PFMT versus usual care | 2 | 634 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.61, 1.06] |
| 3.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 4 Urinary incontinence medium term (> 1‐5 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.1 PFMT versus no PFMT | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 PFMT versus usual care | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 PFMT versus unspecified control | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Urinary incontinence long term (> 5‐10 years) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.2 PFMT versus usual care | 1 | 516 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.88, 1.05] |
| 5.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Urinary incontinence very long term (> 10 years) Show forest plot | 1 | 471 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.94, 1.12] |
| 6.1 PFMT versus usual care | 1 | 471 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.94, 1.12] |
| 7 Faecal incontinence early postnatal period (0‐3 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 8 Faecal incontinence mid‐postnatal period (> 3‐6 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 9 Faecal incontinence late‐postnatal period (> 6‐12 months) Show forest plot | 2 | 620 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.24, 1.94] |
| 9.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 9.2 PFMT versus usual care | 2 | 620 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.24, 1.94] |
| 9.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 10 Faecal incontinence medium term (> 1‐5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11 Faecal incontinence long term (> 5‐10 years) Show forest plot | 1 | 509 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.60, 1.50] |
| 11.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11.2 PFMT versus usual care | 1 | 509 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.60, 1.50] |
| 11.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12 Faecal incontinence very long term (> 10 years) Show forest plot | 1 | 468 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.36 [0.84, 2.22] |
| 12.1 PFMT versus no PFMT | 0 | 0 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.2 PFMT versus usual care | 1 | 468 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.36 [0.84, 2.22] |
| 12.3 PFMT versus unspecified control | 0 | 0 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13 Incontinence‐specific quality of life Show forest plot | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | ‐1.66 [‐3.51, 0.19] |
| 13.1 PFMT versus usual care | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | ‐1.66 [‐3.51, 0.19] |
| 14 Severity of incontinence Show forest plot | Other data | No numeric data | ||
| 14.2 PFMT versus no PFMT | Other data | No numeric data | ||
| 14.3 PFMT versus usual care | Other data | No numeric data | ||
| 14.4 PFMT versus unspecified control | Other data | No numeric data | ||
| 15 Quality of life and health status measures Show forest plot | Other data | No numeric data | ||
| 16 Pelvic floor muscle function Show forest plot | Other data | No numeric data | ||
| 16.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 16.2 PFMT versus usual care | Other data | No numeric data | ||
| 16.3 PFMT versus unspecified control | Other data | No numeric data | ||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Urinary incontinence early postnatal period (0‐3 months) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2 Urinary incontinence mid‐postnatal period (> 3‐6 months) Show forest plot | 5 | 2800 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.75, 1.19] |
| 2.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 2.2 PFMT versus usual care | 5 | 2800 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.75, 1.19] |
| 2.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 3 Urinary incontinence late postnatal period (> 6‐12 months) Show forest plot | 3 | 826 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.71, 1.09] |
| 3.1 PFMT versus no PFMT | 1 | 107 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.31, 2.21] |
| 3.2 PFMT versus usual care | 2 | 719 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.71, 1.10] |
| 3.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4 Urinary incontinence medium term (> 1‐5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5 Urinary incontinence long term (> 5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Faecal incontinence early postnatal period (0‐3 months) Show forest plot | 1 | 1609 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.51, 1.67] |
| 6.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6.2 PFMT versus usual care | 1 | 1609 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.51, 1.67] |
| 6.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 7 Faecal incontinence mid‐postnatal period (> 3‐6 months) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.1 PFMT versus no PFMT | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 PFMT versus usual care | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.3 PFMT versus unspecified control | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 Faecal incontinence late‐postnatal period (> 6‐12 months) Show forest plot | 1 | 107 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.73 [0.13, 4.21] |
| 8.1 PFMT versus no PFMT | 1 | 107 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.73 [0.13, 4.21] |
| 8.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 8.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 9 Faecal incontinence medium term (> 1‐5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 10 Incontinence‐specific quality of life | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 10.1 PFMT versus no PFMT | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 PFMT versus usual care | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 PFMT versus unspecified control | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 Severity of incontinence Show forest plot | Other data | No numeric data | ||
| 11.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 11.2 PFMT versus usual care | Other data | No numeric data | ||
| 11.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 12 Loss of urine under stress test postpartum Show forest plot | 2 | 323 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.58, 1.57] |
| 12.1 PFMT versus no PFMT | 0 | 0 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.2 PFMT versus usual care | 2 | 323 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.58, 1.57] |
| 12.3 PFMT versus unspecified control | 0 | 0 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13 Quality of life and health status measures Show forest plot | Other data | No numeric data | ||
| 13.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 13.2 PFMT versus usual care | Other data | No numeric data | ||
| 13.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 14 Pelvic floor muscle function Show forest plot | Other data | No numeric data | ||
| 14.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 14.2 PFMT versus usual care | Other data | No numeric data | ||
| 14.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 14.4 PFMT plus versus PFMT | Other data | No numeric data | ||
| 15 Pelvic organ prolapse symptoms Show forest plot | Other data | No numeric data | ||
| 15.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 15.2 PFMT versus usual care | Other data | No numeric data | ||
| 15.3 PFMT versus unspecified control | Other data | No numeric data | ||