Recordatorios por mensajes de telefonía celular para acudir a las citas de atención sanitaria
Referencias
References to studies included in this review
References to studies excluded from this review
Additional references
References to other published versions of this review
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Ir a:
| Methods | Study design: randomised controlled trial (from April to May 2007) | |
| Participants | China, Hospital Health Promotion Centre. 1891 adults (mean age 50.6 years, 57.6% male) who had scheduled appointments within 72 hours to 2 months from recruitment. 32 adults who failed to provide telephone numbers were excluded. | |
| Interventions | SMS group: Participants received text message reminders delivered through a mobile phone SMS, 72 hrs before appointment. The SMS was automatically sent through GSM model linked to the electronic health record system. The text message included participant's name and appointment details. Telephone group: Participants were called by the office medical assistants from the health promotion centre, 72 hrs before appointment. A maximum of three reminders were attempted in the telephone group. If the phone was unanswered, the participant would be called on their mobile phone number. Call content was the same as the SMS content. Control group: No reminders. | |
| Outcomes | Attendance rate at the healthcare appointment. Costs of reminders. | |
| Funding | Not specified | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated random numbers. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding (performance bias and detection bias) | Unclear risk | No information of blinding of researchers was provided. Blinding of participants was not possible due to the nature of the intervention, but this is unlikely to have influenced outcomes. |
| Incomplete outcome data (attrition bias) | Low risk | 11 participants could not be contacted by telephone or SMS as they changed their numbers or there was incorrect recording of the phone numbers by the medical assistant. The numbers of those lost‐to‐follow up are small in comparison to sample size. |
| Selective reporting (reporting bias) | Unclear risk | Protocol is not available, however, the number of possible outcomes seems restricted to those reported. |
| Other bias | Low risk | Control and intervention groups were similar at baseline for age and gender. No other apparent source of bias was identified. |
| Methods | Study design: randomised controlled trial (from August 2004 to February 2005). | |
| Participants | Scotland. Inner city general practice. 415 appointments made by 173 participants who had failed to attend two or more routine appointments in the preceding year. Same day appointments and participants with no mobile phones numbers were excluded. | |
| Interventions | SMS group: Participants received text message reminders delivered through a mobile phone SMS. The text message was sent between 8:00‐9:00 on the morning preceding afternoon appointments, and between 16:00‐17:00 on the afternoon preceding morning appointments. Texts were sent from a PC using www.vodafone.net. Control group: No reminders. | |
| Outcomes | Non‐attendance rate. | |
| Funding | This study was funded by the Lothian and Borders Primary Care Research Network. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A random sequence of labels. The randomisation sequence was based on a table of random numbers. |
| Allocation concealment (selection bias) | Low risk | "[S]ealed opaque numbered envelopes. One of two trained designated receptionists randomised each appointment by sequentially opening the sealed envelopes and allocating the appointment to the intervention group or the control group as indicated. |
| Blinding (performance bias and detection bias) | Unclear risk | No information of blinding of researchers was provided. Blinding of participants was not possible due to the nature of the intervention, but this is unlikely to have influenced outcomes. |
| Incomplete outcome data (attrition bias) | Low risk | Three appointments had to be excluded due to incorrect recording of the appointment date. 25 out of 191 text messages in the intervention group were not successfully delivered. |
| Selective reporting (reporting bias) | Low risk | Protocol is available and the study's pre‐specified outcomes have been reported. |
| Other bias | High risk | Groups were comparable at baseline for age and gender. However, as the unit of analysis is the appointment rather than the individual participant, who may have more than one appointment in the study period, there is potential clustering of data. |
| Methods | Study design: randomised controlled trial (from November 2003 to June 2004). | |
| Participants | UK. Six randomly‐selected ear, nose and throat (ENT) clinics in one district general hospital. 441 participants who were scheduled to attend the selected clinics were eligible. Participants who could not be contacted by telephone, who were not familiar with SMS and those not wishing to participate in the study were excluded. 291 participants were included in the study. | |
| Interventions | SMS group: All participants received postal reminders two weeks before appointment. Intervention group also received text message reminders 24 hours before appointment. Texts were sent through a web‐based provider. Control group: Postal reminder two weeks before appointment only. | |
| Outcomes | Attendance rate; Proportion of participants willing to be contacted by SMS (before the intervention). | |
| Funding | Not specified. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information on the method of randomisation was provided. |
| Allocation concealment (selection bias) | Unclear risk | No information on allocation concealment was provided. |
| Blinding (performance bias and detection bias) | Unclear risk | No information of blinding of researchers was provided. Blinding of participants was not possible due to the nature of the intervention, but this is unlikely to have influenced outcomes. |
| Incomplete outcome data (attrition bias) | Low risk | There was no loss to follow up. |
| Selective reporting (reporting bias) | Unclear risk | Protocol was not available, however the number of possible outcomes seems restricted to those reported. |
| Other bias | Unclear risk | The authors state that the groups were comparable at baseline on age and gender, although no data are provided to support this. |
| Methods | Study design: randomised controlled trial (between April and October 2005). | |
| Participants | Malaysia. Seven primary care clinics. 993 participants whose follow‐up appointments fell between 48 hours to 3 months from recruitment date. Either the patients or their caregivers had to have a mobile phone with text messaging function. | |
| Interventions | SMS group: Participants received text message reminders delivered through a mobile phone SMS, 24 to 48 hrs before appointment. The text message included participant's name and appointment details. Mobile phone group: Participants were called 24 to 48 hrs before appointment. A maximum of three reminders was attempted in the intervention groups. Call content was the same as the SMS content. Control group: No reminders. | |
| Outcomes | Attendance rate at the healthcare appointment. Costs of reminders. | |
| Funding | This research was funded via an unrestricted grant from the International Medical University, Malaysia. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation method using software. |
| Allocation concealment (selection bias) | Low risk | The researcher who did the randomisation was said to be not involved in patient recruitment or delivery of the intervention. The method of allocation concealment is not stated. |
| Blinding (performance bias and detection bias) | Low risk | Research assistants were blinded to the intervention. Participants could not be blinded due to the nature of the intervention, but this is unlikely to have influenced outcomes. |
| Incomplete outcome data (attrition bias) | Low risk | Between 9 to 11 participants in each group did not receive the allocated intervention due to incorrect assignments by researchers. They were included in the intention‐to‐treat analysis. |
| Selective reporting (reporting bias) | Unclear risk | Protocol is not available, however, the number of possible outcomes seems restricted to those reported. |
| Other bias | High risk | The groups are comparable on age, gender, income, reason for follow‐up, and whether the participant is the patient or the caregiver. However, the definition of 'attendance' is strict, being attendance at the clinics on scheduled days, whereas participants in the study were not accustomed to healthcare appointments but rather walk‐in visits; Consequently, 48% of the participants actually visited the clinic on days other than the appointment dates. |
| Methods | Study design: randomised controlled trial (study dates not reported). | |
| Participants | Malaysia. Two primary care clinics. 931 participants with chronic diseases such as diabetes, asthma, hypertension, dyslipidaemia, and coronary artery disease with a scheduled return appointment between 1 and 6 months. Ownership of a mobile phone by the patient or an accompanying person who would be able to contact the patient was required. | |
| Interventions | SMS group: Participants received a standard text message reminder 24 to 48 hours before the scheduled appointment. Telephone reminder: Participants received a reminder call 24 to 48 hours before the scheduled appointment. If the contact was unsuccessful, up to three further attempts were made at 4‐hourly intervals. Control group: No reminders. | |
| Outcomes | Non‐attendance rate, defined as the rate of those who did not attend, attended early, or attended late without rescheduling their appointment. | |
| Funding | This study was made possible with research funding from University of Malaya (reference F0381/2005C) and University Kebangsaan Malaysia (reference FF‐225‐2005). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation by computer, using a block size of three units. |
| Allocation concealment (selection bias) | Low risk | Assignment of participants was done by computer using a list of anonymous identification codes. |
| Blinding (performance bias and detection bias) | Low risk | The recruiters who enrolled the research subjects were blinded to the intervention at the time of recruitment. Study subjects could not be blinded due to the nature of the intervention, but this is unlikely to have influenced outcomes. |
| Incomplete outcome data (attrition bias) | Low risk | Attendance rates were calculated based on intention‐to‐treat principle. |
| Selective reporting (reporting bias) | Unclear risk | Protocol is not available. However, the number of possible outcomes seems restricted to those reported. |
| Other bias | Low risk | Control and intervention groups were similar at baseline for age, gender, chronic disease, mobile phone ownership. However, in the control group more patients (78.0%) owned a mobile telephone than in the intervention groups (telephone 67.2%; text messaging 68.5%). No other apparent sources of bias were identified. |
| Methods | Study design: randomised controlled trial (from December 2010 until end of 2011). | |
| Participants | China. Zhongshan Ophthalmic Center, Guangzhou. 258 parent–child pairs involved in the Childhood Cataract Programme of the Chinese Ministry of Health. Parent–child pairs were eligible if: 1) the child was diagnosed as having congenital or development cataract, regardless of treatment status; and 2) the parents owned a mobile phone and could use the free mobile service used in this study. Children with as‐yet‐unoperated cataract and with previous cataract surgery with or without placement of intraocular lenses were all eligible to take part. Illiterate parents were eligible if assisted by a literate partner. Children were ineligible if they showed other ocular abnormalities. If intraocular pressure could not be controlled within 1 week after surgery, children were withdrawn from the study and referred to the Center's glaucoma department. | |
| Interventions | SMS group: Participants received 4 SMS reminders per appointment, i.e. at 10am and 4pm on 1 and 4 days before the date of the appointment. Appointments were once every month before surgery and at 1 week, 1 month, 2 months and 3 months post surgery (then every 3 months). The reminder read (in Chinese): "This is a reminder of the appointment for routine ophthalmic examination of your child at Zhongshan Ophthalmic Center at [time] on [date]. Rigorous and regular follow‐up is essential to timely and successful management of childhood cataract. Please make your preparations in advance and be on time." Control group: Participants in the control group received standard care, without any appointment reminders. | |
| Outcomes | Primary outcome: Attendance rate. Secondary outcomes: Additional procedures (surgeries, laser treatments, or changes in eyeglass prescription); occurrence of secondary ocular hypertension. | |
| Funding | Funded by the Key Projects for Hospital Clinical Disciplines of Ministry of Health of China in 2010‐2012 and partly by Fundamental Research Funds of State Key Laboratory of Ophthalmology. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers. |
| Allocation concealment (selection bias) | Low risk | Written allocation assignments were sealed in individual opaque envelopes marked only with study identification numbers. |
| Blinding (performance bias and detection bias) | Low risk | Regular ocular examinations and analyses were performed by investigators and clinical staff, both masked to group allocation. Study participants and the study personnel in charge of randomization and sending the SMS could not be masked, because the intervention required overt participation. However, this is unlikely to have influenced outcomes. |
| Incomplete outcome data (attrition bias) | High risk | The rate of non‐attendance at the visit at 3 months after surgery, and thus the percentage of patients lost to follow‐up, was high in both the intervention (17%) and control (67%) group. This percentage is particularly high in the control group, therefore it was not possible to state whether the intervention improved outcomes significantly. |
| Selective reporting (reporting bias) | Unclear risk | Protocol is not available. However, the number of possible primary outcomes seems restricted to those reported. Some secondary outcomes were reported, for which it could not be judged whether these were subject to undue selection. |
| Other bias | Low risk | Treatment and control groups were comparable at baseline for gender, residence status, parent's education, travel cost, number of children per household, and cataract history. No other sources of bias were identified. |
| Methods | Study design: randomised controlled trial (from September 2010 until April 2011). | |
| Participants | Kenya. 12 public health clinics. Participants were 1200 adult men who were in need of follow‐up care after circumcision. Included were men aged 18 or older who had undergone circumcision on the day of screening. Participants needed to be in possession of a mobile phone at the time of enrolment, and be able and willing to respond to a questionnaire administered by phone 42 days after circumcision. | |
| Interventions | SMS group: For the first seven days after circumcision, participants in the intervention group were sent daily text messages with post‐operative instructions and asking them to visit the clinic at seven days post‐procedure. Control group: Participants in the control group received standard care, but no text messages. | |
| Outcomes | Attendance at the seven‐day post‐operative clinic visit, that is: within 3 days before or after the scheduled 7‐day visit. | |
| Funding | Funded by the University of Washington International AIDS Research and Training Program, which is supported by the Fogarty International Center (NIH 5D43‐TW000007). Additional support for the trial was provided by the Department of Epidemiology and Biostatistics at the University of Illinois at Chicago; and the Biostatistics and International Cores of the University of Washington Center for AIDS Research, an NIH funded program (P30 AI027757) which is supported by the following NIH Institutes and Centers (NIAID, NCI, NIMH, NIDA, NICHD, NHLBI, NIA). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was done using a computer‐generated block randomisation scheme with variable blocks of size 4 to16. Randomisation was stratified by clinic. |
| Allocation concealment (selection bias) | Low risk | "A biostatistician in Seattle, who was not involved in any other aspect of study implementation, developed the randomization sequence [...] Investigators and study staff were blinded to the block number, block size, and sequence in the block. Individual participant randomization envelopes were shipped from Seattle to Kisumu, while the key to intervention assignments was retained in Seattle. Participants were assigned to intervention arms using pre‐prepared sequentially numbered, sealed, opaque envelopes containing group assignment. Study staff issued the next envelope in the series." |
| Blinding (performance bias and detection bias) | Low risk | "Because of the nature of the intervention, it was not possible to mask participants to group assignments. However, clinicians and nurses performing the circumcision procedure and follow‐up were not aware of study group assignment." It is unlikely that the lack of blinding of participants would have influenced outcomes. |
| Incomplete outcome data (attrition bias) | Low risk | The primary analysis followed the intention‐to‐treat principle and was unadjusted. 12 (1%) participants whose clinic records could not be located after an extensive search were considered lost to follow‐up. Sensitivity analyses were performed in which the 12 men with missing clinic records were considered as failures to return. |
| Selective reporting (reporting bias) | Unclear risk | Protocol is not available. However, the number of possible outcomes seems restricted to those reported. |
| Other bias | Low risk | There were minor differences in the proportions of men reporting zero versus one partner in the past month in the intervention versus control arms. However, the proportion reporting multiple partners was similar. Other baseline characteristics were similar in both study arms. |
| Methods | Study design: randomised controlled trial (study dates not reported). | |
| Participants | Australia. 2 physical therapy outpatient departments. 679 patients in need of physical therapy. Participants were included if they had an appointment in a physical therapy outpatient clinic at 1 of the participating clinics and provided a mobile telephone number on which they could be contacted. Participants were excluded if they had an appointment scheduled on the same day on which they made the appointment or if they already had participated in the project by being allocated for a previous appointment during the trial. | |
| Interventions | SMS group: Participants were sent an SMS reminder 2 days before their appointment if it was made more than 3 days in advance, or the day before the appointment if it was made within 2 days. The content of the SMS reminder was “Reminder: Physical therapy appointment at [site] on [day], [date] at [time]. Please call [number] ONLY if you cannot attend.” Control group: Participants received no appointment reminders. | |
| Outcomes | Non‐attendance rate, defined as the number of scheduled appointments not attended as a proportion of the total number of scheduled appointments. | |
| Funding | The trial was funded by the participating hospitals. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The randomisation sequence was prepared by an independent researcher using random number tables stratified for site in permuted blocks of 10. |
| Allocation concealment (selection bias) | Low risk | Group allocation was concealed in a computer file. An administration assistant opened the pre‐prepared computer file and selected the next participant in sequence, revealing their allocation by changing the text colour in the cell from white to black. |
| Blinding (performance bias and detection bias) | Low risk | "Data were retrieved in a blinded manner (i.e. without reference to group allocation) by a member of the research team by using the hospital’s data management system or were recorded manually by outpatient physical therapists at the time of the next scheduled appointment. Treating physical therapists were blinded to group allocation." Participants could not be blinded due to the nature of the intervention, but this is unlikely to have influenced outcomes. |
| Incomplete outcome data (attrition bias) | Low risk | Numbers of those lost to follow‐up or excluded from analysis were comparable across the different study arms. All data were analysed according to intention‐to‐treat principles. |
| Selective reporting (reporting bias) | Unclear risk | Protocol is not available. However, the list of reported outcomes seems comprehensive. |
| Other bias | Low risk | Intervention and control groups were comparable on all assessed demographic variables. No other sources of bias were identified. |
Characteristics of excluded studies [ordered by study ID]
Ir a:
| Study | Reason for exclusion |
| Study design: cohort study. | |
| Study design: no randomisation. | |
| Study design: cohort study. | |
| Study underpowered: intervention group of n = 2. | |
| Outcome data for visit adherence not presented. |
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Attendance rate at healthcare appointments Show forest plot | 7 | 5841 | Risk Ratio (M‐H, Random, 95% CI) | 1.14 [1.03, 1.26] |
| Analysis 1.1 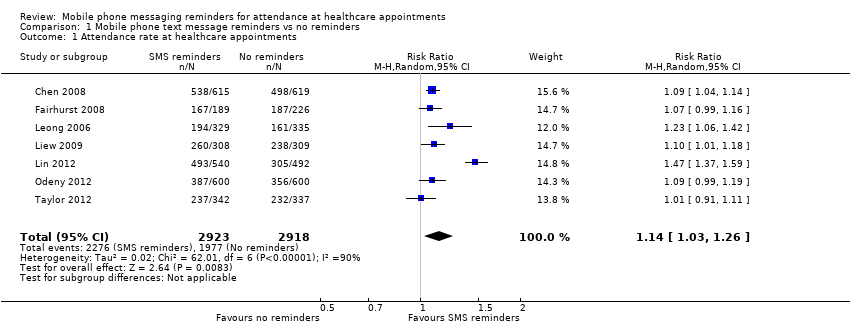 Comparison 1 Mobile phone text message reminders vs no reminders, Outcome 1 Attendance rate at healthcare appointments. | ||||
| 2 Attendance rate at healthcare appointments (sensitivity analysis) Show forest plot | 6 | 4809 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [1.05, 1.12] |
| Analysis 1.2  Comparison 1 Mobile phone text message reminders vs no reminders, Outcome 2 Attendance rate at healthcare appointments (sensitivity analysis). | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Attendance rate at healthcare appointments Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Analysis 2.1 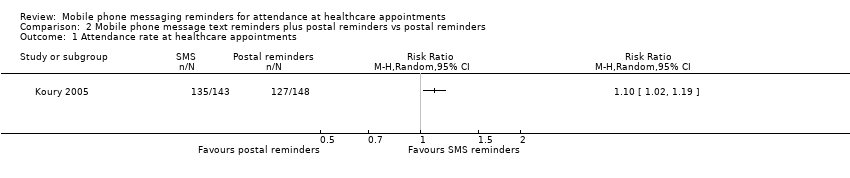 Comparison 2 Mobile phone message text reminders plus postal reminders vs postal reminders, Outcome 1 Attendance rate at healthcare appointments. | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Attendance rate at healthcare appointments Show forest plot | 3 | 2509 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.95, 1.02] |
| Analysis 3.1 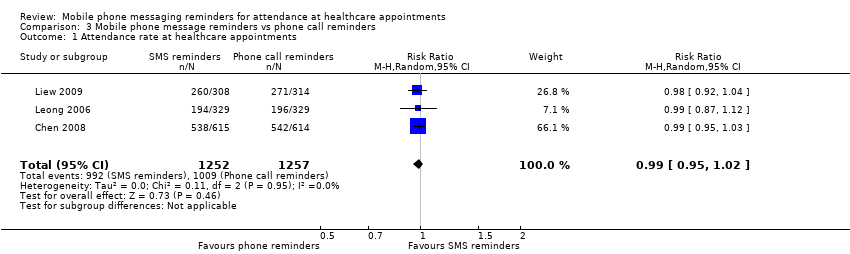 Comparison 3 Mobile phone message reminders vs phone call reminders, Outcome 1 Attendance rate at healthcare appointments. | ||||
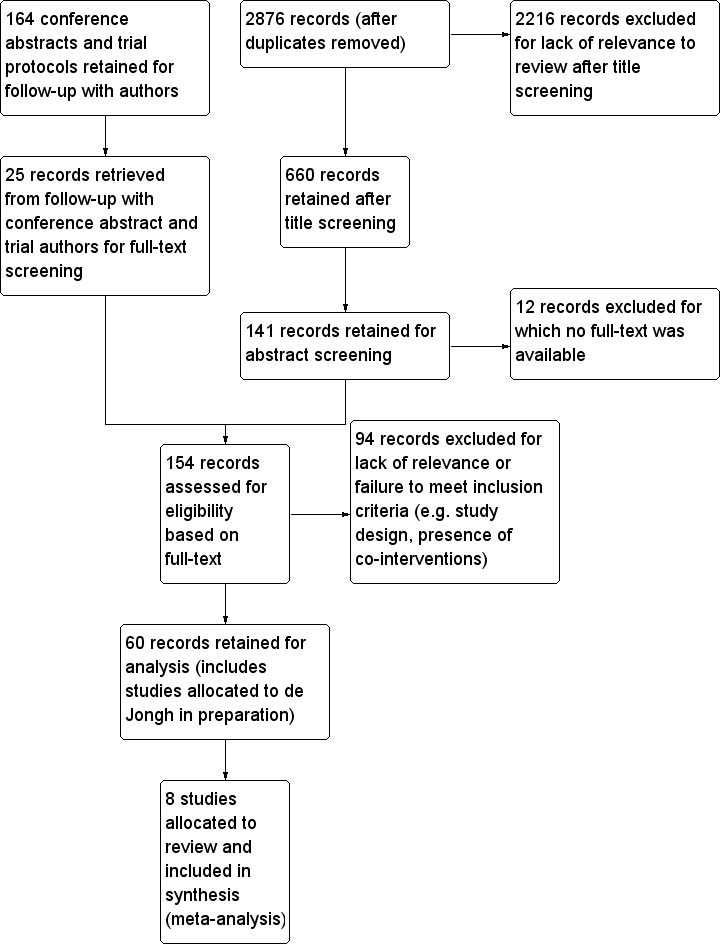
Study flow diagram. (Note: search strategy and screening selection is common for this review and for de Jongh in preparation until the final allocation stage).
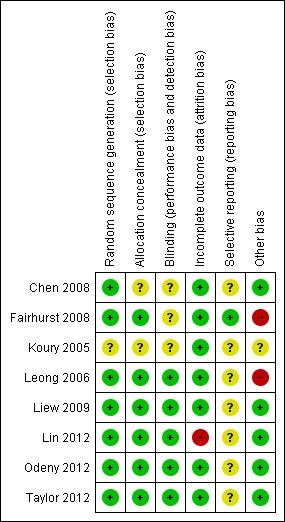
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
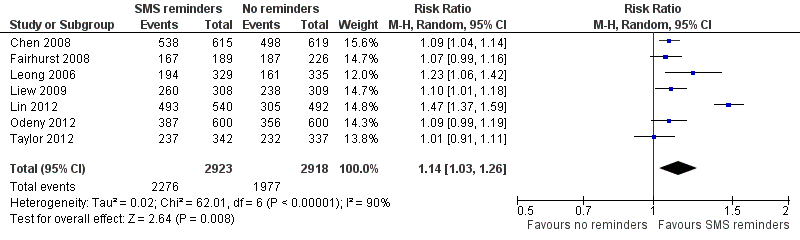
Forest plot of comparison: 1 Mobile phone text message reminders vs no reminders, outcome: 1.1 Attendance rate at healthcare appointments.

Forest plot of comparison: 2 Mobile phone message text reminders plus postal reminders vs postal reminders, outcome: 2.1 attendance rate of scheduled healthcare appointments.

Forest plot of comparison: 3 Mobile phone message reminders vs phone call reminders, outcome: 3.1 Attendance rate at healthcare appointments.

Comparison 1 Mobile phone text message reminders vs no reminders, Outcome 1 Attendance rate at healthcare appointments.

Comparison 1 Mobile phone text message reminders vs no reminders, Outcome 2 Attendance rate at healthcare appointments (sensitivity analysis).
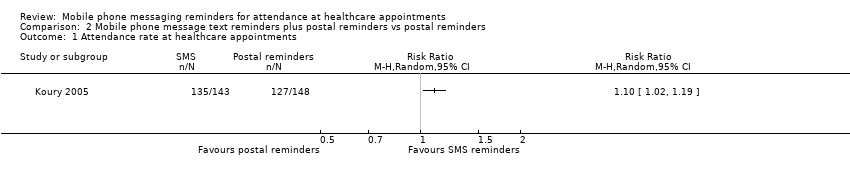
Comparison 2 Mobile phone message text reminders plus postal reminders vs postal reminders, Outcome 1 Attendance rate at healthcare appointments.
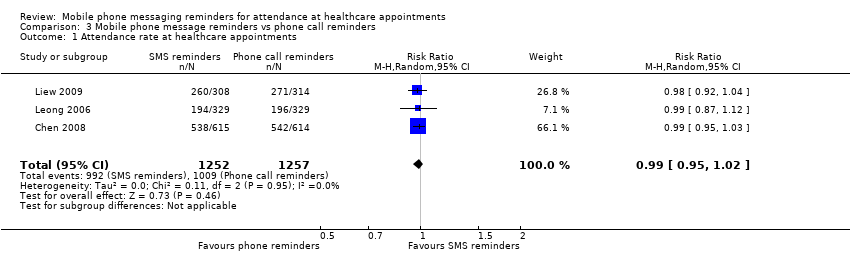
Comparison 3 Mobile phone message reminders vs phone call reminders, Outcome 1 Attendance rate at healthcare appointments.
| Patient or population: Patients with healthcare appointments | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| No reminders | Mobile phone text message reminders | ||||
| Attendance rate at healthcare appointments | 678 per 1000 | 773 per 1000 | RR 1.14 (1.03 to 1.26) | 5841 | ⊕⊕⊕⊝ |
| Other outcomes | None of the included studies reported on health outcomes, costs, user evaluation of the intervention, user perception of safety, potential harms or adverse effects of the intervention. | ||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| a Unclear risk of bias for several categories in the included studies. | |||||
| Patient or population: Patients with healthcare appointments | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Postal reminders | Mobile phone message text plus postal reminders | ||||
| Attendance rate at healthcare appointments | 858 per 1000 | 944 per 1000 | RR 1.10 | 291 | ⊕⊕⊝⊝ |
| Other outcomes | The included study did not report on health outcomes, costs, user evaluation of the intervention, user perception of safety, potential harms or adverse effects of the intervention. | ||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| aOnly one study included, with small number or participants. No information provided about the method of randomisation, allocation concealment, blinding and selective outcome reporting (unclear risk of bias). Low risk only for attrition bias. | |||||
| Mobile phone message reminders compared to phone call reminders for patients with healthcare appointments | |||||
| Patient or population: patients with healthcare appointments | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Phone call reminders | Mobile phone message reminders | ||||
| Attendance rate at healthcare appointments | 803 per 1000 | 795 per 1000 | RR 0.99 | 2509 | ⊕⊕⊕⊝ |
| Costs | While the attendance rates after text messages versus phone reminders were similar, the costs per text message per attendance were 55% and 65% lower than costs per phone call reminder in two included studies. | ||||
| Adverse outcomes | One study reported that there were no adverse events during the study period. Two studies did not report on adverse events. | ||||
| Other outcomes | None of the included studies reported on health outcomes, user evaluation of the intervention or user perception of safety. | ||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| a Unclear risk of bias for several categories in the included studies. | |||||
| Face‐to‐face | Postal Letter | Call to Landline | Call to Mobile | Web Based (Electronic Health Record) | | SMS / MMS | |
| Immediacy | Slow: Requires a visit to the provider | Slow: around 2 days | Immediate, if person is at home. Return call may be necessary. | Immediate, if person answers (more likely than landline). | Immediate | Immediate | Immediate |
| Privacy and Confidentiality | High: | High: | Low: Confidentiality prevents message being left as others may answer or retrieve it. | High: | Moderate: | Moderate: | High, if |
| Likelihood of misinterpretation | Low | Moderate | Low, as patient can request immediate clarification | Low, as patient can request immediate clarification | Moderate | Moderate | Moderate |
| Delivery confirmation possible | Not applicable | Yes, but only at significant expense | Unnecessary if call is answered. No, if message was left. | Unnecessary if call is answered. No, if message was left. | Not applicable | Yes | Yes |
| Cost | High | Moderate | Low | Moderate | Low | Low | Low |
| Study | Costs and cost effectiveness (monetary unit as specified in the study) | Participant evaluation of the intervention (as reported in the study) | Potential harms or adverse effects of the intervention (as reported in the study) |
| Cost per attendance: SMS group: 0.31 Yuan (4.7 GBP) Telephone group: 0.48 Yuan (7.3 GBP) Ratio of total cost per attendance: SMS group: 0.65 (relative to telephone group) | Not reported | Not reported | |
| Not reported | 98% willing to receive routine reminders of their appointments. Usefulness of the intervention:
| Not reported | |
| Cost per attendance: SMS group: 0.45 RM (0.67 GBP) Mobile phone group: 0.82 RM (0.123 GBP) Ratio of total cost per attendance: SMS group: 0.55 (relative to mobile phone group) | Not reported | No adverse events reported during the study period. | |
| Not reported | 132 out of 135 (97.8%) reported they would like the intervention to continue | Not reported |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Attendance rate at healthcare appointments Show forest plot | 7 | 5841 | Risk Ratio (M‐H, Random, 95% CI) | 1.14 [1.03, 1.26] |
| 2 Attendance rate at healthcare appointments (sensitivity analysis) Show forest plot | 6 | 4809 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [1.05, 1.12] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Attendance rate at healthcare appointments Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Attendance rate at healthcare appointments Show forest plot | 3 | 2509 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.95, 1.02] |