Recordatorios por mensajes de telefonía celular para acudir a las citas de atención sanitaria
Información
- DOI:
- https://doi.org/10.1002/14651858.CD007458.pub3Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 05 diciembre 2013see what's new
- Tipo:
-
- Intervention
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Consumidores y comunicación
- Copyright:
-
- Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
Ipek Gurol‐Urganci developed the protocols and was involved in both the original version of this review and the 2013 update. She has led the updated search process and participated in screening the papers. She collected, analysed, interpreted the data and participated in writing the review.
Thyra de Jongh was involved in the original version of this review and has led the 2013 update. This includes the screening and quality appraisal processes for the studies, as well as the data extraction and management. She has collected, analysed and interpreted the data and participated in writing the review.
Vlasta Vodopivec Jamsek helped develop the protocols. For the 2013 update of this review she has been involved in data extraction and has contributed to writing the review.
Rifat Atun provided strategic guidance in all stages of the study and contributed to writing of the review.
Josip Car conceived the review together with Rifat Atun and has played a coordinating role in all stages of the study. He contributed to writing the review.
Sources of support
Internal sources
-
eHealth Unit, Department of Primary Care and Social Medicine, Imperial College, UK.
salaries, office space
-
Centre for Health Management, Tanaka Business School, Imperial College, UK.
salaries, office space
-
Department of Family Medicine, Faculty of Medicine, University of Ljubljana, Slovenia.
salaries, office space
-
London School of Hygiene and Tropical Medicine, UK.
salaries, office space
External sources
-
No sources of support supplied
Declarations of interest
None known.
Acknowledgements
We acknowledge the very helpful support of the Cochrane Consumers and Communication Review Group editorial base in different stages of this review.
Version history
| Published | Title | Stage | Authors | Version |
| 2013 Dec 05 | Mobile phone messaging reminders for attendance at healthcare appointments | Review | Ipek Gurol‐Urganci, Thyra de Jongh, Vlasta Vodopivec‐Jamsek, Rifat Atun, Josip Car | |
| 2012 Jul 11 | Mobile phone messaging reminders for attendance at healthcare appointments | Review | Josip Car, Ipek Gurol‐Urganci, Thyra de Jongh, Vlasta Vodopivec‐Jamsek, Rifat Atun | |
| 2008 Oct 08 | Mobile phone messaging reminders for attendance at scheduled healthcare appointments | Protocol | Josip Car, Ipek Gurol‐Urganci, Thyra de Jongh, Vlasta Vodopivec‐Jamsek, Rifat Atun | |
Differences between protocol and review
Changes between the protocol (Car 2008b) and the original review (Car 2012):
We were not able to search the following databases we had listed in the protocol (Car 2008b):
-
Proceedings from the MEDNET Congresses: We could not access the proceedings.
-
TrialsCentralTM (www.trialscentral.org): The website for the database was not functional and did not allow for the search of clinical trials.
-
African Trials Register: The trials in the African Trials Register are collected with a search strategy using the Cochrane Controlled Trials Register and the African Health Anthology (AHA). As we searched both original sources, it was not necessary to access the African Trials Register separately.
-
Health Star: The database ceased to exist as of December 2000, with all peer‐reviewed journal articles transferred to PubMed.
Changes between the original (Car 2012) and the updated review:
Compared to the first version of this review (Car 2012) several changes have been made to the methodology. These changes were approved by the editors of the Cochrane Consumers and Communication Review Group before the update was conducted. Specifically, we have made the following changes:
-
We excluded the LILACS and African Health Anthology databases from our search, as these proved very difficult to search and produced no studies of interest to the initial review that were not also retrieved from other, included databases;
-
We no longer included the following study designs: quasi‐randomised controlled trials (QRCTs), controlled before and after studies (CBAs), and interrupted time series (ITS) with at least three time points before and after the intervention, because the original review found no such studies that met the criteria for inclusion;
-
We reorganised the data extraction sheet to group specific data under different headings, but maintaining all relevant fields, to enable a better overview;
-
We no longer aimed to conduct subgroup analysis for different age categories as the original review indicated that very few studies stratified outcomes by age;
-
We no longer aimed to conduct sensitivity analysis to check for the effects of publication language or source of funding as the original review found only a few studies published in languages other than English and source of funding did not appear to be relevant factor;
-
In the original review, study results were not combined in a meta‐analysis if there was substantial clinical, methodological or statistical heterogeneity. In the updated review, however, we have conducted a meta‐analysis of all combined results, despite significant statistical heterogeneity. Instead, we have addressed the issue of heterogeneity by also performing a sensitivity analysis of the results, with exclusion of the outlying study.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
Medical Subject Headings Check Words
Humans;
PICO
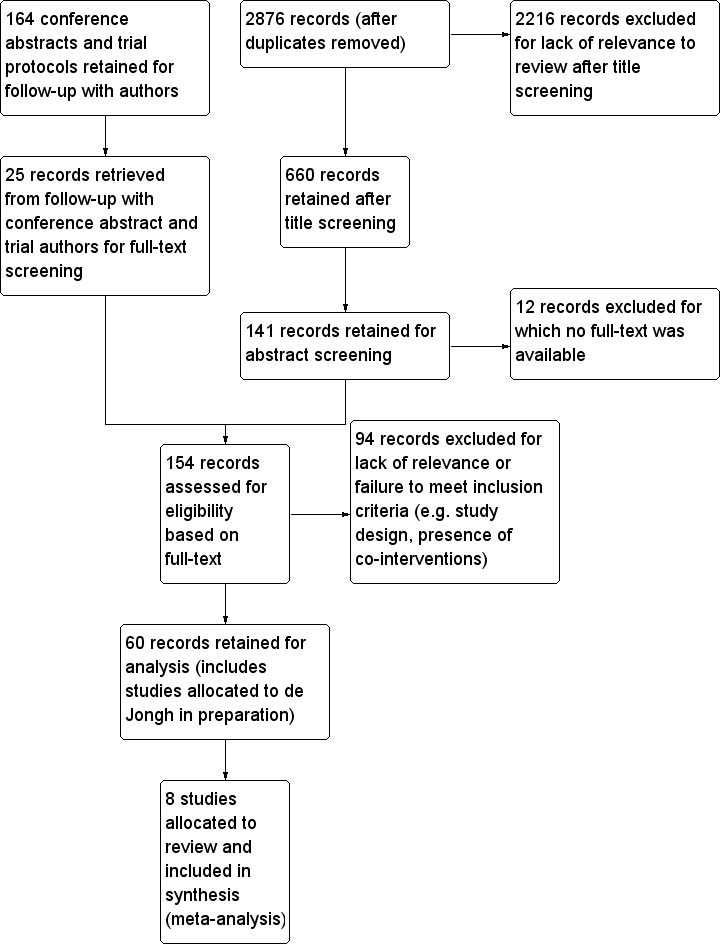
Study flow diagram. (Note: search strategy and screening selection is common for this review and for de Jongh in preparation until the final allocation stage).
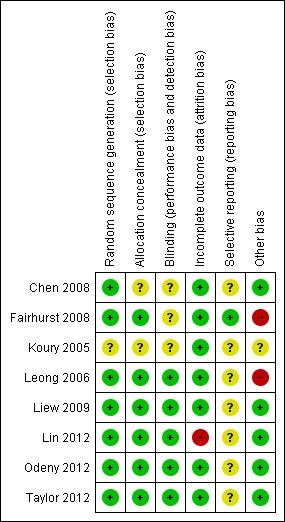
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
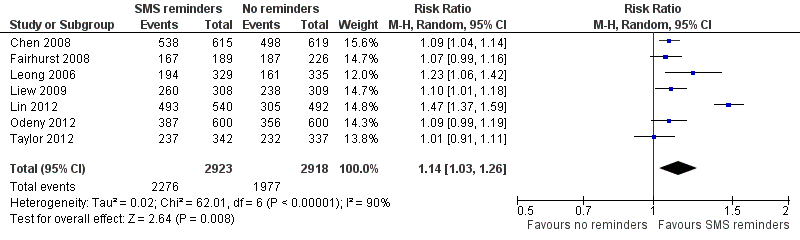
Forest plot of comparison: 1 Mobile phone text message reminders vs no reminders, outcome: 1.1 Attendance rate at healthcare appointments.

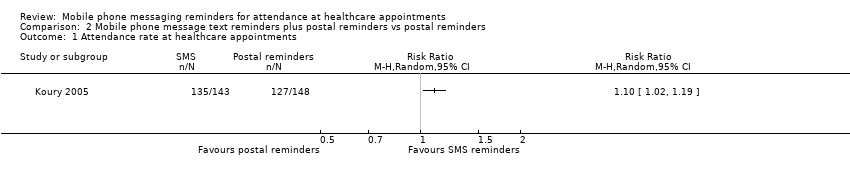
Forest plot of comparison: 2 Mobile phone message text reminders plus postal reminders vs postal reminders, outcome: 2.1 attendance rate of scheduled healthcare appointments.

Forest plot of comparison: 3 Mobile phone message reminders vs phone call reminders, outcome: 3.1 Attendance rate at healthcare appointments.

Comparison 1 Mobile phone text message reminders vs no reminders, Outcome 1 Attendance rate at healthcare appointments.

Comparison 1 Mobile phone text message reminders vs no reminders, Outcome 2 Attendance rate at healthcare appointments (sensitivity analysis).
Comparison 2 Mobile phone message text reminders plus postal reminders vs postal reminders, Outcome 1 Attendance rate at healthcare appointments.
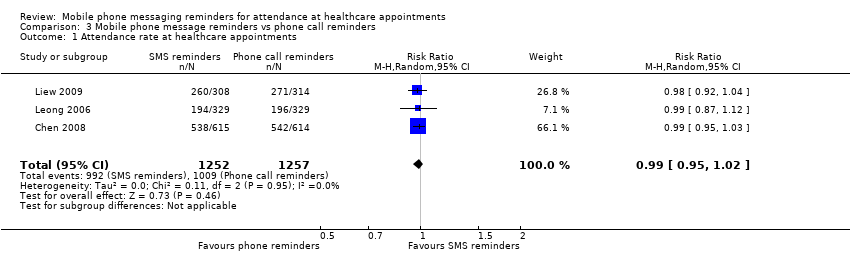
Comparison 3 Mobile phone message reminders vs phone call reminders, Outcome 1 Attendance rate at healthcare appointments.
| Patient or population: Patients with healthcare appointments | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| No reminders | Mobile phone text message reminders | ||||
| Attendance rate at healthcare appointments | 678 per 1000 | 773 per 1000 | RR 1.14 (1.03 to 1.26) | 5841 | ⊕⊕⊕⊝ |
| Other outcomes | None of the included studies reported on health outcomes, costs, user evaluation of the intervention, user perception of safety, potential harms or adverse effects of the intervention. | ||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| a Unclear risk of bias for several categories in the included studies. | |||||
| Patient or population: Patients with healthcare appointments | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Postal reminders | Mobile phone message text plus postal reminders | ||||
| Attendance rate at healthcare appointments | 858 per 1000 | 944 per 1000 | RR 1.10 | 291 | ⊕⊕⊝⊝ |
| Other outcomes | The included study did not report on health outcomes, costs, user evaluation of the intervention, user perception of safety, potential harms or adverse effects of the intervention. | ||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| aOnly one study included, with small number or participants. No information provided about the method of randomisation, allocation concealment, blinding and selective outcome reporting (unclear risk of bias). Low risk only for attrition bias. | |||||
| Mobile phone message reminders compared to phone call reminders for patients with healthcare appointments | |||||
| Patient or population: patients with healthcare appointments | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Phone call reminders | Mobile phone message reminders | ||||
| Attendance rate at healthcare appointments | 803 per 1000 | 795 per 1000 | RR 0.99 | 2509 | ⊕⊕⊕⊝ |
| Costs | While the attendance rates after text messages versus phone reminders were similar, the costs per text message per attendance were 55% and 65% lower than costs per phone call reminder in two included studies. | ||||
| Adverse outcomes | One study reported that there were no adverse events during the study period. Two studies did not report on adverse events. | ||||
| Other outcomes | None of the included studies reported on health outcomes, user evaluation of the intervention or user perception of safety. | ||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| a Unclear risk of bias for several categories in the included studies. | |||||
| Face‐to‐face | Postal Letter | Call to Landline | Call to Mobile | Web Based (Electronic Health Record) | | SMS / MMS | |
| Immediacy | Slow: Requires a visit to the provider | Slow: around 2 days | Immediate, if person is at home. Return call may be necessary. | Immediate, if person answers (more likely than landline). | Immediate | Immediate | Immediate |
| Privacy and Confidentiality | High: | High: | Low: Confidentiality prevents message being left as others may answer or retrieve it. | High: | Moderate: | Moderate: | High, if |
| Likelihood of misinterpretation | Low | Moderate | Low, as patient can request immediate clarification | Low, as patient can request immediate clarification | Moderate | Moderate | Moderate |
| Delivery confirmation possible | Not applicable | Yes, but only at significant expense | Unnecessary if call is answered. No, if message was left. | Unnecessary if call is answered. No, if message was left. | Not applicable | Yes | Yes |
| Cost | High | Moderate | Low | Moderate | Low | Low | Low |
| Study | Costs and cost effectiveness (monetary unit as specified in the study) | Participant evaluation of the intervention (as reported in the study) | Potential harms or adverse effects of the intervention (as reported in the study) |
| Cost per attendance: SMS group: 0.31 Yuan (4.7 GBP) Telephone group: 0.48 Yuan (7.3 GBP) Ratio of total cost per attendance: SMS group: 0.65 (relative to telephone group) | Not reported | Not reported | |
| Not reported | 98% willing to receive routine reminders of their appointments. Usefulness of the intervention:
| Not reported | |
| Cost per attendance: SMS group: 0.45 RM (0.67 GBP) Mobile phone group: 0.82 RM (0.123 GBP) Ratio of total cost per attendance: SMS group: 0.55 (relative to mobile phone group) | Not reported | No adverse events reported during the study period. | |
| Not reported | 132 out of 135 (97.8%) reported they would like the intervention to continue | Not reported |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Attendance rate at healthcare appointments Show forest plot | 7 | 5841 | Risk Ratio (M‐H, Random, 95% CI) | 1.14 [1.03, 1.26] |
| 2 Attendance rate at healthcare appointments (sensitivity analysis) Show forest plot | 6 | 4809 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [1.05, 1.12] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Attendance rate at healthcare appointments Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Attendance rate at healthcare appointments Show forest plot | 3 | 2509 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.95, 1.02] |