Actaea racemosa (Cimicifuga spp.) para los síntomas menopáusicos
Referencias
References to studies included in this review
References to studies excluded from this review
References to studies awaiting assessment
References to ongoing studies
Additional references
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | Design: randomised, double‐blind, placebo‐controlled, parallel group trial Randomisation ratio: not stated Study duration: 3.5 years (from January 2006 to June 2008) | |
| Participants | Participant characteristics: 34 women enrolled, 28 were randomised (black cohosh = 15, placebo = 13) and 7 (25%) dropped out. Mean age (black cohosh = 56.7 ± 6.5 years, placebo = 50.8 ± 3.2 years). Duration of menopause not stated Inclusion criteria: female, aged ≥ 40 years, postmenopausal for ≥ 12 months or perimenopausal (amenorrhoea lasting 2 to 11 months in the preceding year). Onset of anxiety symptoms occurred within 3 years of onset of menopause or perimenopause or < 5 years after cessation of menstruation. Women with prior hysterectomy and uncertain menopausal status required a serum FSH ≥ 40 mIU/mL Exclusion criteria: major depressive disorder, bipolar disorder, panic disorder, phobic disorder, obsessive‐compulsive disorder, post‐traumatic stress disorder, acute stress disorder, substance‐induced anxiety disorder, schizophrenia, dementia, substance abuse or dependence disorder within the past 3 months; unstable medical condition, hepatic or renal disease, malignancy, serum thyrotropin level ≥ 5 μIU/mL, abnormal breast examination or mammogram result, history of endometrial hyperplasia or endometrial cancer, rapidly growing uterine leiomyomata, undiagnosed abnormal uterine bleeding, abnormal gynaecological examination result precluding use of black cohosh, known sensitivity to black cohosh; and concurrent use of prescribed anxiolytics, antidepressants, mood stabilisers, sedatives, complementary medicines (e.g. St. John's Wort), oral oestrogen, oestrogen cream, and phyto‐oestrogen preparations Diagnostic criteria: DSM‐IV Axis I diagnosis of anxiety disorder owing to menopause Co‐morbidities: not stated Co‐medications: not stated | |
| Interventions | Number of study centres: not stated Country/location: Philadelphia, Pennsylvania, US Setting: not stated Intervention (route, total, dose/day, frequency): oral ethanolic extract of Cimicifuga racemosa 32 to 128 mg (32 mg, standardised to 5.6% triterpene glycosides), 1 to 4 capsules daily Control (route, total, dose/day, frequency): oral rice flour, 1 to 4 capsules daily Duration of intervention: 12 weeks Duration of follow‐up: not applicable Run‐in period: not applicable Treatment before study: not stated Titration period: treatment began at 2 capsules daily for 2 weeks. Dose was increased to 4 capsules daily by study week 4 in women with ≤ 50% reduction in total Hamilton Anxiety Rating Scale Score | |
| Outcomes | Primary outcomes: total Hamilton Anxiety Rating Scale Score Secondary outcomes: Beck Anxiety Inventory Score, total GCS score, GCS subscale scores, Psychological General Well Being Index Rating Additional outcomes: adverse events, blood pressure, pulse rate and weight | |
| Notes | This study reported final value scores | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomisation was performed using blocked randomisation with varying block sizes" Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Unclear risk | Quote: "All study subjects and outcome raters were blinded as to treatment condition, and all results were analysed under blinded conditions..."; though there was no assurance that interventions matched in appearance, taste or odour Comment: probably done |
| Incomplete outcome data (attrition bias) | Low risk | "Intention‐to‐treat" (which assumed that those who withdrew were non‐responders) |
| Selective reporting (reporting bias) | Unclear risk | All primary and secondary outcomes listed were reported, though no study protocol was published or lodged |
| Other bias | Unclear risk | Baseline differences in age and duration of illness were evident |
| Methods | Design: randomised, double‐blind, active‐controlled, double‐dummy, multicentre, parallel group trial Randomisation ratio: 1:1 Study duration: 9 months (from September 2004 to May 2005) | |
| Participants | Participant characteristics: 244 women enrolled, 244 were randomised (black cohosh = 122, tibolone = 122) and 26 (10.7%) dropped out. Mean age (black cohosh = 51.8 ± 3.7 years, tibolone = 51.5 ± 3.5 years). Duration of amenorrhoea (black cohosh = 32.2 ± 24.6 months, tibolone = 35.4 ± 25.3 months) Inclusion criteria: female, aged between 40 and 60 years, history of menopausal complaints for at least 4 weeks, spontaneous amenorrhoeic interval ≥ 5 months since last regular menstruation, baseline E2 ≤ 30 pg/mL if amenorrhoeic < 12 months, KI ≥ 15 Exclusion criteria: HT within the last 4 weeks, psychoactive drugs, BMI > 28 kg/m2, endometrial thickness ≥ 5 mm if amenorrhoea ≥ 12 months or ≥ 15 mm if < 12 months, irregular gynaecological bleeding within the last 4 weeks, hysterectomy, amenorrhoea > 8 years, abnormal cervical smear examination, contraindication of tibolone, cancer, severe or current disease that could interfere with climacteric manifestations or treatment, drug abuse, alcohol addiction, participation in a Phase I or II trial in the last 180 days or a Phase III or IV trial within the last 90 days, and any drug, food, traditional Chinese medicine or nutritional supplement used for climacteric symptoms Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: not stated | |
| Interventions | Number of study centres: 5 Country/location: China Setting: hospital research centres Intervention (route, total, dose/day, frequency): oral isopropanolic extract of Cimicifuga racemosa (Remifemin, equivalent to 2.5 mg dry extract or 20 mg C. racemosa root) 2 tablet twice a day, and 2 tibolone‐matching placebo tablet daily Control (route, total, dose/day, frequency): oral tibolone 2.5 mg tablet daily, and 2 C. racemosa‐matching placebo tablets daily Duration of intervention: 12 weeks Duration of follow‐up: not applicable Run‐in period: not applicable Treatment before study: not stated Titration period: not applicable | |
| Outcomes | Primary outcomes: benefit (i.e. change in KI) to risk (i.e. number of adverse events) balance Secondary outcomes: total KI score, KI subscale scores, KI responder rate, Clinical Global Impression items, subject's global efficacy of effectiveness Additional outcomes: vital signs, body weight, concomitant disease, adverse events, endometrial thickness, liver function test, complete blood picture | |
| Notes | This study reported final value scores | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "All eligible subjects were randomly allocated to the two treatment groups" (method not described) Comment: probably not done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Low risk | Quote: "double‐blind"; "double dummy"; "patients received two Remifemin® tablets (1‐0‐1) and one tibolone‐matching placebo...the tibolone‐group applied two Remifemin®‐ matching placebos and one tibolone tablet" Comment: probably done. |
| Incomplete outcome data (attrition bias) | High risk | ITT was not mentioned, but the term 'full analysis set' was used; however, "six subjects were excluded from the full analysis set...for discontinuing the trial for any reason" A similar proportion of women withdrew from each group, though the reasons differed |
| Selective reporting (reporting bias) | Unclear risk | All primary and secondary outcomes listed were reported, although no study protocol was published or lodged |
| Other bias | Low risk | There were no significant differences in participant characteristics between groups at baseline |
| Methods | Design: randomised, double‐blind, placebo‐controlled, parallel group trial Randomisation ratio: not stated Study duration: not stated | |
| Participants | Participant characteristics: 128 women were randomised (exercise + black cohosh = 43, exercise only = 43, wellness control = 42), and 25 (19.5%) dropped out. Mean age (exercise + black cohosh = 51.8 ± 2.7 years, exercise only = 52.3 ± 2.3 years, wellness control = 52.4 ± 2.7 years). Duration of menopause not stated Inclusion criteria: female, aged between 48 and 55 years, living in Erlangen‐Nuremberg (Germany), 1 to 3 years postmenopausal, Caucasian Exclusion criteria: thrombosis, embolism, history of profound CHD, lumbar spine or hip fracture, secondary osteoporosis, hyperparathyroidism, medication or diseases that impact on muscle or bone, inflammatory disease, athletic history in the past decade, weight reduction > 5 kg in the last 6 months Diagnostic criteria: menopause was defined as self‐reported lack of a menstrual cycle for more than 12 months or a LH:FSH ratio < 1.0 Co‐morbidities: not stated Co‐medications: calcium (1.5 g/day) and cholecalciferol supplementation (500 IE/day) was provided to all women | |
| Interventions | Number of study centres: not stated Country/location: Erlangen, Germany Setting: not stated Intervention (route, total, dose/day, frequency): exercise (60 minutes, weekly; comprising 6 weeks of high‐intensity‐resistance/high‐impact exercise dedicated to bone parameters, interspersed by blocks of 10 weeks of moderate intensity exercise focusing on parameters related to CHD) + Cimicifuga racemosa (40 mg daily; 3 months on then 3 months off); exercise (60 minutes, weekly; comprising 6 weeks of high‐intensity‐resistance/high‐impact exercise dedicated to bone parameters, interspersed by blocks of 10 weeks of moderate‐intensity exercise focusing on parameters related to CHD) + placebo (daily; 3 months on then 3 months off) Control (route, total, dose/day, frequency): wellness control (60 minutes, weekly; comprising a low‐intensity exercise programme for a period of 10 weeks, interspersed with 10‐week blocks without exercise) + placebo (daily; 3 months on then 3 months off) Duration of intervention: 12 months (52 weeks) Duration of follow‐up: not stated Run‐in period: not stated Treatment before study: not stated Titration period: not stated | |
| Outcomes | Primary outcomes: bone mineral density (lumbar spine, proximal hip), 10‐year CHD risk Secondary outcomes: body composition (total and regional), MRS, aerobic capacity Additional outcomes: not stated | |
| Notes | This study reported both final value scores and change‐from‐baseline scores | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "women were finally assigned by computer‐generated block randomisation stratified for menopause age to three subgroups" Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Low risk | Quote: "the study was blinded for research assistants and participants"; "Blinding of the participants was successful in view of the fact that 77% of the participants in the CG [control group] considered that they were in the primary intervention group" Comment: probably done |
| Incomplete outcome data (attrition bias) | High risk | "intention‐to‐treat" was quoted, but the final analysis excluded women (n = 25) lost to follow‐up A greater number of women were lost to follow‐up in the wellness group when compared to the 2 exercise groups, primarily because women lost interest in the intervention. Other reasons for withdrawal were similar across treatment groups |
| Selective reporting (reporting bias) | Unclear risk | All primary and secondary outcomes listed were reported, although no study protocol was published or lodged |
| Other bias | Low risk | There were no significant differences in participant characteristics between groups at baseline |
| Methods | Design: randomised, double‐blind, placebo‐controlled, parallel group trial Randomisation ratio: not stated Study duration: not stated | |
| Participants | Participant characteristics: 48 women were randomised (black cohosh = 24, placebo = 24), and 2 (4.2%) dropped out. Mean age (black cohosh = 54.1 ± 5.0 years, placebo = 52.8 ± 4.4 years). Time postmenopausal (black cohosh = 3.7 ± 1.5 months, placebo = 2.8 ± 1.7 months) Inclusion criteria: female, Caucasian, aged between 35 and 60 years, had natural or surgical menopausal for at least 1 year but not more than 6 years, able to give voluntary consent, not taking any hormone replacement therapy or SERMs for the past 3 months, had not been diagnosed with osteoporosis or an osteoporosis‐related bone fracture, were sedentary and not involved in a regular exercise programme, and had not taken black cohosh for the past 3 months Exclusion criteria: smoker, lactose intolerant, history of taking bisphosphonates at any time in their life, history of kidney or liver disease, diabetes, parathyroid disease or documented osteoporosis with DEXA scan, failed to take study medication as directed, became ill or were diagnosed with osteoporosis or fracture during the study, changed their mind about being included in the study Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: not stated | |
| Interventions | Number of study centres: not stated Country/location: North Central Florida, US Setting: not stated Intervention (route, total, dose/day, frequency): oral Cimicifuga racemosa (40 mg, standardised to 2.5% triterpene glycosides) 1 capsule daily; plus calcium carbonate and vitamin D supplement, 1 caplet twice daily (dosage not described) Control (route, total, dose/day, frequency): oral placebo (lactose), 1 capsule daily; plus calcium carbonate and vitamin D supplement, 1 caplet twice daily (dosage not described) Duration of intervention: 12 weeks Duration of follow‐up: not applicable Run‐in period: not applicable Treatment before study: not stated Titration period: not stated | |
| Outcomes | Primary outcomes: serum C‐terminal telopeptide, serum osteocalcin Secondary outcomes: weight, height, BMI, blood pressure Additional outcomes: not stated | |
| Notes | The type of data reported was not clear | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "the participant was...randomized into either the experimental or the control group using a computer generated randomization table" Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Low risk | Quote: "double‐blind"; "the placebo group took an identical appearing placebo capsule" Comment: probably done |
| Incomplete outcome data (attrition bias) | High risk | ITT was not mentioned 2 women withdrew from the study (1 in each arm) ‐ the reasons for withdrawal differed between groups. Both women were excluded from the analysis by researchers |
| Selective reporting (reporting bias) | Unclear risk | All primary and secondary outcomes listed were reported, although no study protocol was published or lodged |
| Other bias | Unclear risk | Baseline differences in years postmenopausal was observed |
| Methods | Design: randomised, double‐blind, placebo‐controlled, multicentre, parallel group trial Randomisation ratio: 2:1 (active:placebo) Study duration: not stated | |
| Participants | Participant characteristics: 129 women were randomised (black cohosh = 84, placebo = 45), and 20 (15.5%) dropped out. Mean age (black cohosh = 52.5 ± 3.7 years, placebo = 52.2 ± 3.5 years). Duration of amenorrhoea (black cohosh = 38.7 ± 50.5 months, placebo = 37.3 ± 51.4 months) Inclusion criteria: female, early or perimenopause with climacteric disorders, aged between 45 and 60 years, ≥ 3 hot flushes daily (corresponding to ≥ 42 hot flushes during the run‐in period), ≥ 1 functioning ovary, normal gynaecological examination Exclusion criteria: history of breast or endometrial carcinoma, medication affecting menopausal complaints, hormone replacement therapy within the last month, alcohol abuse, drug abuse, serious conditions interfering with study objectives Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: not stated | |
| Interventions | Number of study centres: 14 Country/location: Switzerland Setting: private gynaecological practices (n = 12) and university menopause centres (n = 2) Intervention (route, total, dose/day, frequency): oral ethanolic extract of Cimicifuga racemosa (6.5 mg dry extract or 42 mg crude drug), 1 capsule daily Control (route, total, dose/day, frequency): oral placebo (excipients only), 1 capsule daily Duration of intervention: 12 weeks Duration of follow‐up: not applicable Run‐in period: 2 weeks Treatment before study: not stated Titration period: not applicable | |
| Outcomes | Primary outcomes: hot flushes (weekly weighted score), KI Secondary outcomes: MRS, urogenital symptoms, ophthalmic symptoms, serum FSH, karyopyknotic index Additional outcomes: clinical global impression of efficacy | |
| Notes | This study reported final value scores | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "patients were randomized in the ratio of 2:1" (method not described) Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Low risk | Quote: "double‐blind"; "one group received capsules of Cimicifuga racemosa extract...and the other group identically appearing placebo capsules" Comment: probably done |
| Incomplete outcome data (attrition bias) | High risk | Used the expression ITT, but "five patients were excluded from the intention‐to‐treat population because of serious protocol violations or a posteriori detected exclusion criteria" 15 women discontinued the study; however, the number and reasons for withdrawal were not given for each group separately |
| Selective reporting (reporting bias) | High risk | While no study protocol was published or lodged, there was limited discussion of many secondary outcome measures |
| Other bias | Unclear risk | Baseline differences in menopausal status and level of FSH were observed |
| Methods | Design: randomised, double‐blind, placebo‐controlled, multicentre, parallel group trial Randomisation ratio: not stated Study duration: 50 months (from February 2003 to December 2007) | |
| Participants | Participant characteristics: 89 women were randomised (black cohosh = 22, red clover = 22, CEO/MPA = 23, placebo = 22), and 9 (10.1%) dropped out. Mean age (black cohosh = 54.4 ± 3.9 years, red clover = 52.4 ± 4.6 years, CEO/MPA = 53.3 ± 4.0 years, placebo = 52.0 ± 4.2 years). Duration of amenorrhoea (black cohosh = 3.4 ± 2.6 years, red clover = 4.1 ± 2.8 years, CEO/MPA = 3.6 ± 2.9 years, placebo = 2.8 ± 2.9 years) Inclusion criteria: female, perimenopausal or postmenopausal with intact uterus, experiencing ≥ 35 vasomotor symptoms (hot flushes and night sweats) per week, amenorrhoea > 6 months and < 10 years' duration, FSH > 40 mIU/mL, HT not contraindicated Exclusion criteria: hysterectomy, abnormal vaginal bleeding of undetermined aetiology, abnormal transvaginal ultrasound (> 7 mm thickness), abnormal endometrial biopsy or mammogram, diabetes, positive pregnancy test, breastfeeding, history of endometrial hyperplasia/neoplasia, breast cancer or cancer of the reproductive tract, history of myocardial infarction, stroke, severe varicose veins, sickle cell anaemia, deep vein thrombosis, thrombophlebitis or thromboembolic disorder, untreated or uncontrolled hypertension (systolic blood pressure > 165 mmHg or diastolic blood pressure > 95 mmHg), history of severe recurrent depression, severe psychiatric disturbance, alcohol abuse or drug abuse, concurrent use of medication containing oestrogen, progestin, SERM, St. John's Wort, biphosphonates or dietary phyto‐oestrogens, history of migraine associated with hormone use, smoker, vegan diet, participation in another clinical trial within 30 days of enrolment, Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: not stated | |
| Interventions | Number of study centres: 2 Country/location: Chicago, Illinois, US Setting: University of Illinois Medical Centre outpatient facility, and University Feinberg School of Medicine Intervention (route, total, dose/day, frequency): oral ethanolic extract of Cimicifuga racemosa below‐ground parts (64 mg, standardised to 5.68% triterpene glycosides) 2 capsules daily; oral ethanolic extract of Trifolium pratense above‐ground parts (189 mg) 2 capsules daily Control (route, total, dose/day, frequency): oral CEO (0.625 mg) 1 capsule daily and oral MDP (2.5 mg) 1 capsule daily; oral placebo (not described) 2 capsules daily Duration of intervention: 12 months (52 weeks) Duration of follow‐up: not applicable Run‐in period: not applicable Treatment before study: 1‐month washout period for women using transdermal hormone preparations or oral botanical supplements, and 2‐month washout period for women using oral HT Titration period: not applicable | |
| Outcomes | Primary outcomes: vasomotor symptoms (e.g. hot flushes and night sweats) Secondary outcomes: relief of somatic symptoms (e.g. insomnia, joint pain, sleep, fatigue), mood changes (e.g. depression, anxiety), sexual dysfunction (e.g. vaginal dryness, dyspareunia, libido, difficulty achieving orgasm), HRQoL, KI, GCS, Pittsburgh Sleep Quality Index, Positive and Negative Affect Schedule Additional outcomes: complete blood count, urinalysis, serum chemistry, lipid analysis, serum oestradiol, serum FSH, serum LH, serum oestrone, serum testosterone, serum thyroid‐stimulating hormone, serum sex hormone binding globulin, liver function test, prothrombin time, body weight, height, bone density, adverse events | |
| Notes | This study reported change‐from‐baseline scores; final value scores were provided on request | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "a random, computer‐ generated code assigned two women in each cluster to each of the four treatment arms. There were 11 clusters with eight women in each cluster" Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Low risk | Quote: "Double blinded"; "the study capsules were identical in appearance, and there was no detectable odor for any of the preparations" Comment: probably done |
| Incomplete outcome data (attrition bias) | High risk | "intention‐to‐treat" was quoted, but the analysis consisted only of "randomised women who had been in the study for at least 3 months" 9 women withdrew from the study ‐ the number and reasons for withdrawal differed between groups |
| Selective reporting (reporting bias) | Unclear risk | All primary and secondary outcomes listed were reported, although no study protocol was published or lodged |
| Other bias | Unclear risk | Baseline differences in race and BMI were evident, although all analyses controlled for these variables |
| Methods | Design: randomised, double‐blind, placebo‐controlled, parallel group trial Randomisation ratio: not stated Study duration: not stated | |
| Participants | Participant characteristics: 85 women enrolled, 85 were randomised (black cohosh = 42, placebo = 43) and 16 (18.8%) dropped out. Mean age (black cohosh = 52% were aged between 50 to 59 years, placebo = 51% were aged between 50 to 59 years). Duration of menopause not stated Inclusion criteria: female, aged > 18 years, previously treated for breast cancer at the Columbia‐Presbyterian Medical Centre or 1 of its affiliates, experienced hot flushes daily, had completed primary therapy (including chemotherapy and radiotherapy) for breast cancer at least 2 months prior to study enrolment Exclusion criteria: using hormone replacement therapy for hot flushes, pregnant, history of major psychiatric illness, known to have recurrent or metastatic breast cancer Diagnostic criteria: not stated Co‐morbidities: history of breast cancer Co‐medications: tamoxifen | |
| Interventions | Number of study centres: not stated Country/location: New York, New York, US Setting: not stated Intervention (route, total, dose/day, frequency): oral isopropanolic extract of Cimicifuga racemosa (Remifemin, 10 mg) 2 capsules daily with meals Control (route, total, dose/day, frequency): oral placebo (not described) 2 capsules daily with meals Duration of intervention: 60 days (8.6 weeks) Duration of follow‐up: not applicable Run‐in period: not applicable Treatment before study: not stated Titration period: not applicable | |
| Outcomes | Primary outcomes: hot flushes (number and intensity) Secondary outcomes: menopausal symptom index, global rating of health and well‐being Additional outcomes: serum FSH, serum LH | |
| Notes | This study reported final value scores. Data had to be extrapolated from figures to be suitable for the pooling of results | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "We used one randomization list developed using the RanCode Plus program...Study participants [had] 50% probability of assignment to either group" Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Unclear risk | Quote: "double‐masked", though there was no mention of who was blinded, or any assurance that interventions matched in appearance, taste or odour Comment: probably done |
| Incomplete outcome data (attrition bias) | Low risk | "Intention‐to‐treat"; "missing data were handled by including all available data in the primary analyses" Number and reasons for withdrawal were similar between groups |
| Selective reporting (reporting bias) | Unclear risk | All primary and secondary outcomes listed were reported, although no study protocol was published or lodged |
| Other bias | Unclear risk | Baseline differences in age, race, years of education, employment status and marital status were observed |
| Methods | Design: randomised, double‐blind, placebo‐controlled, parallel group trial Randomisation ratio: not stated Study duration: 4 years (from May 2001 to May 2005) | |
| Participants | Participant characteristics: 74 were randomised (black cohosh = 37, placebo = 37) and 9 (12.2%) dropped out. Mean age (black cohosh = 55.12 ± 4.08 years, placebo = 54.18± 3.58 years). Duration of menopause not stated Inclusion criteria: female, postmenopausal, aged between 45 and 70 years, resident of New York Metro area, BMI < 33 kg/m2, amenorrhoea ≥ 12 months, serum oestradiol < 30 pg/mL, ≥ 5 hot flushes per day Exclusion criteria: hormone replacement therapy within the past 60 days, abnormal mammogram or transvaginal ultrasound Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: women were advised to stop taking phyto‐oestrogen‐containing supplements (such as soy isoflavones genestein or daidzein) or any herb, dietary supplement or over‐the‐counter product targeted at menopausal women (such as evening primrose, Rejuvex, Promensil, progesterone creams, etc.) and to not take any nutritional supplements other than multivitamins (not megadoses) throughout the study | |
| Interventions | Number of study centres: 1 Country/location: New York, US Setting: Columbia University College of Physicians and Surgeons Center for Menopause, Hormonal Disorders and Women's Health Intervention (route, total, dose/day, frequency): oral ethanolic extract of Cimicifuga racemosa rhizome (CimiPure, 40 mg, standardised to 2.5% triterpene glycosides) 1 capsule, twice daily Control (route, total, dose/day, frequency): oral placebo (dosage and formulation not described) Duration of intervention: 12 months (52 weeks) Duration of follow‐up: not stated Run‐in period: not stated Treatment before study: not stated Titration period: not stated | |
| Outcomes | Primary outcomes: hot flushes (intensity and frequency) Secondary outcomes: menopausal symptoms (GCS), quality of life, serum oestradiol, serum oestrone, serum LH, serum FSH, bone density Additional outcomes: physical/gynaecological examination, Papanicolaou smear, blood chemistry, coagulation profile, liver function test, vaginal maturation index, mammogram, electrocardiogram, endometrial thickness | |
| Notes | This study reported final value scores | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" (method not described) Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Unclear risk | Quote: "double‐blind"; though there was no mention of who was blinded, or any assurance that interventions matched in appearance, taste or odour Comment: probably done |
| Incomplete outcome data (attrition bias) | Low risk | "All [women] were included in the Intention‐to‐treat analysis" 9 women withdrew from the study; however, the number and reasons for withdrawal were not given for each group separately |
| Selective reporting (reporting bias) | High risk | No study protocol was published or lodged. Data were reported for the primary outcomes, but not for all secondary outcomes |
| Other bias | Low risk | There were no significant differences in participant characteristics between groups at baseline |
| Methods | Design: randomised, controlled, single‐centre trial Randomisation ratio: not stated Study duration: not stated | |
| Participants | Participant characteristics: 60 women were randomised (oestriol = 15, oestrogen = 15, oestradiol/norethisterone = 15, black cohosh = 15), and 5 (8.3%) dropped out. Mean age not stated. Duration of menopause not stated Inclusion criteria: female, hysterectomised, aged under 40 years, has at least 1 intact ovary, complaining of climacteric symptoms Exclusion criteria: type I diabetes mellitus, chronic hepatitis, deep vein thrombosis, breast cancer, contraindication to HT Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: not stated | |
| Interventions | Number of study centres: 1 Country/location: Kiel, Germany Setting: university gynaecological hospital Intervention (route, total, dose/day, frequency): oral isopropanolic extract of Cimicifuga racemosa (Remifemin, 2 mg) 2 tablets, twice daily Control (route, total, dose/day, frequency): oral oestriol (Ovestin, 1 mg) 1 tablet daily; oral conjugated oestrogen (Presomen, 1.25 mg) 1 tablet daily; oral oestradiol/norethisterone acetate (Trisequens) 1 tablet, daily Duration of intervention: not stated Duration of follow‐up: 24 weeks Run‐in period: not stated Treatment before study: not stated Titration period: not applicable | |
| Outcomes | Primary outcomes: KI, serum FSH, serum LH Secondary outcomes: not stated Additional outcomes: not stated | |
| Notes | This study reported final value scores | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" (method not described) Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Unclear risk | There is no mention of blinding Comment: probably not done |
| Incomplete outcome data (attrition bias) | High risk | ITT was not mentioned 5 women withdrew from the study; however, the number and reasons for withdrawal were not given for each group separately |
| Selective reporting (reporting bias) | Unclear risk | Data for all primary outcomes were reported, although no study protocol was published or lodged |
| Other bias | Unclear risk | Participant characteristics at baseline were not reported |
| Methods | Design: randomised, controlled, multicentre, parallel group trial Randomisation ratio: not stated Study duration: not stated | |
| Participants | Participant characteristics: 64 women enrolled, 64 were randomised (black cohosh = 32, oestradiol = 32), and 1 (1.6%) dropped out. Mean age (black cohosh = 50.5 ± 2.1 years, oestradiol = 50.9 ± 1.8 years). Duration of menopause (black cohosh = 9.0 ± 2.9 months, oestradiol = 9.1 ± 3.0 months) Inclusion criteria: spontaneous menopause of at least 6 months' duration, FSH > 30 mIU/L, presence of at least 5 hot flushes daily, endometrial thickness < 5 mm Exclusion criteria: previous HT, contraindications to HT Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: not stated | |
| Interventions | Number of study centres: 2 Country/location: Modena and Pavia, Italy Setting: university departments of obstetrics and gynaecology Intervention (route, total, dose/day, frequency): oral isopropanolic extract of Cimicifuga racemosa (Remifemin, 40 mg) 1 tablet daily Control (route, total, dose/day, frequency): transdermal oestradiol (Estraderm, 25 uG) every 7 days, plus dihydrogesterone (Dufaston, 10 mg) 1 tablet daily for the last 12 days of the 3‐month oestradiol treatment Duration of intervention: 3 months (12 weeks) Duration of follow‐up: not applicable Run‐in period: not applicable Treatment before study: not stated Titration period: not applicable | |
| Outcomes | Primary outcomes: hot flushes (number) Secondary outcomes: vasomotor and urogenital symptoms (GCS), anxiety and depression (Symptom Rating Test) Additional outcomes: endometrial thickness, serum FSH, serum LH, serum 17β‐oestradiol, serum prolactin, serum cortisol, lipid profile, liver function test | |
| Notes | This study reported final value scores | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "patients were randomly allocated on the basis of a computer‐generated number list" Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | High risk | Women were not blinded to treatment as the 2 interventions used different routes of administration and different dosage regimens. It is not clear if observers were blinded to treatment Comment: probably not done |
| Incomplete outcome data (attrition bias) | High risk | ITT was not mentioned 1 woman withdrew from the intervention group owing to nausea. A similar number of women in each group "refused to provide a blood sample at follow‐up" |
| Selective reporting (reporting bias) | Unclear risk | All primary and secondary outcomes listed were reported, although no study protocol was published or lodged |
| Other bias | Low risk | There were no significant differences in participant characteristics between groups at baseline |
| Methods | Design: randomised, double‐blind, placebo‐controlled, multicentre, parallel group trial Randomisation ratio: not stated Study duration: 25 months (from May 2001 to August 2003) | |
| Participants | Participant characteristics: 351 women were randomised (black cohosh = 80, multi‐botanical = 76, multi‐botanical plus dietary soy = 79, CEO and MPA = 32, placebo = 84), and 45 (12.8%) dropped out. Mean age (black cohosh = 52.0 ± 2.2 years, multi‐botanical = 52.2 ± 2.5 years, multi‐botanical plus dietary soy = 52.5 ± 2.5 years, CEO and MPA = 52.3 ± 2.6 years, placebo = 52.0 ± 2.5 years). Duration of menopause not stated Inclusion criteria: female, late menopausal transition (≥ 1 skipped menses in the last 12 months) or postmenopausal (no bleeding in the last 12 months) or FSH > 20 IU/mL (if participant had undergone hysterectomy without bilateral oophorectomy), aged between 45 and 55 years, and ≥ 2 vasomotor symptoms daily over the past 2 weeks (with ≥ 6 moderate to severe symptoms), negative mammogram in the last 2 years, normal thyroid stimulating hormone level Exclusion criteria: contraindications to HT, use of HT or oral contraceptives within the last 3 months, use of herbal medicines for menopausal symptoms within the last month, allergy to soy, bilateral oophorectomy, history of breast cancer, non‐adherence (< 80% of capsules administered) during the run‐in period Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: not stated | |
| Interventions | Number of study centres: not stated Country/location: Washington state, US Setting: group health (an integrated health plan) Intervention (route, total, dose/day, frequency): oral ethanolic extract of Cimicifuga racemosa rhizome and root (CimiPure, 80 mg, standardised to 2.5% triterpene glycosides) 2 capsules daily; oral multi‐botanical (ProGyne, incorporating 50 mg C. racemosa extract) 4 capsules daily; multi‐botanical (ProGyne, incorporating 50 mg C. racemosa extract) 4 capsules daily plus soy diet counselling; oral CEO (0.625 mg) 1 tablet daily, with (for women with a uterus) or without (for women with a uterus) MDP (2.5 mg) 1 tablet daily Control (route, total, dose/day, frequency): oral placebo (dose and constitution is not described) Duration of intervention: 12 months (52 weeks) Duration of follow‐up: not applicable Run‐in period: 2 weeks Treatment before study: not applicable Titration period: not applicable | |
| Outcomes | Primary outcomes: mean Wiklund Vasomotor Symptom subscale score, hot flushes and night sweats (frequency and intensity), vaginal bleeding Secondary outcomes: daytime hot flush rate, night‐time sweat rate, total Wiklund Menopause Symptom Scale Score, vaginal dryness, menstrual cyclicly, vaginal cytology, serum FSH, serum LH, serum oestradiol, serum sex hormone binding globulin Additional outcomes: adverse events | |
| Notes | Newton 2006 and Reed 2008 report the same study, but different outcomes. This study reported change‐from‐baseline scores; final value scores were provided on request. Standard errors had to be converted to standard deviations to be suitable for the pooling of results | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "participants were randomly assigned by using SAS software, stratified by previous HT and hysterectomy; block sizes within strata ranged from 5 to 25" Comment: probably done |
| Allocation concealment (selection bias) | Low risk | Quote: "the study nurse determined the appropriate stratum, assigned the participant the next study number in that stratum without knowledge of group assignment, and distributed study medications" Comment: probably done |
| Blinding (performance bias and detection bias) | Low risk | Quote: "double‐blind"; "to facilitate blinding, medications and lactose placebo were encapsulated to provide 2 white and 2 blue capsules to each woman" Comment: probably done |
| Incomplete outcome data (attrition bias) | Low risk | "mixed‐model analysis allowed us to use a true intention‐to‐treat approach" Numbers of withdrawals were similar between groups, though reasons for withdrawal differed. 16 women were unblinded; however, numbers were not given for each group separately |
| Selective reporting (reporting bias) | Unclear risk | All primary and secondary outcomes listed were reported, although no study protocol was published or lodged |
| Other bias | Unclear risk | Baseline differences in BMI were observed |
| Methods | Design: randomised, controlled, single centre, parallel group trial Randomisation ratio: not stated Study duration: not stated | |
| Participants | Participant characteristics: 120 women were randomised (black cohosh = 60, fluoxetine = 60) and 40 (33.3%) dropped out. Mean age (black cohosh = 53.1 ± 5.6 years, fluoxetine = 52.7 ± 6.4 years). Duration of menopause not stated Inclusion criteria: female, amenorrhoea for at least 1 year and serum FSH > 40 mIU/mL, had sought relief of menopausal symptoms Exclusion criteria: HT, herbal products or health food in the last 3 months, mental illness, psychiatric drug use, malignant disease, uncontrolled thyroid disease Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: not stated | |
| Interventions | Number of study centres: 1 Country/location: Ankara, Turkey Setting: university menopause clinic Intervention (route, total, dose/day, frequency): oral black cohosh extract (Remixin, 40 mg) 1 tablet daily Control (route, total, dose/day, frequency): oral fluoxetine (Prozac HCl, 20 mg) 1 tablet daily Duration of intervention: 6 months (24 weeks) Duration of follow‐up: not applicable Run‐in period: not applicable Treatment before study: not stated Titration period: not applicable | |
| Outcomes | Primary outcomes: monthly hot flush and night sweat score, modified KI Secondary outcomes: Beck's Depression Scale Score, RAND‐36 quality of life score Additional outcomes: adverse effects | |
| Notes | This study reported final value scores | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "The study population...was randomly assigned to 2 groups" Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Unclear risk | There is no mention of blinding Comment: probably not done |
| Incomplete outcome data (attrition bias) | High risk | ITT was not mentioned Number of withdrawals were similar between groups, though reasons for withdrawals were not provided |
| Selective reporting (reporting bias) | Unclear risk | All primary and secondary outcomes listed were reported, although no study protocol was published or lodged |
| Other bias | Low risk | There were no significant differences in participant characteristics between groups at baseline |
| Methods | Design: randomised, placebo‐controlled, double‐blind, multicentre, parallel group trial Randomisation ratio: 1:1 Study duration: not stated | |
| Participants | Participant characteristics: 309 women enrolled, 304 were randomised (black cohosh = 153, placebo = 151), and 36 dropped out (11.8%). Mean age (black cohosh = 54.0 ± 6.0 years, placebo = 55.0 ± 6.0 years). Median duration of climacteric complaints (black cohosh = 4.4 years, placebo = 5.1 years) Inclusion criteria: female, postmenopausal (≥ 12 months since last regular menstruation or ≥ 6 months since last regular menstruation plus FSH ≥ 50 U/L), ≥ 45 years of age, MRS ≥ 0.4 in at least 3 items Exclusion criteria: BMI > 35 kg/m2, cancer, drug abuse, diseases interfering with the assessment of climacteric symptoms, participation in another clinical trial within the last 180 days Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: not stated | |
| Interventions | Number of study centres: 24 Country/location: Germany Setting: Gynaecological and gynaecologically experienced private practices Intervention (route, total, dose/day, frequency): oral isopropanolic extract of Cimicifuga racemosa (Remifemin, equivalent to 2.5 mg extract or 20 mg root stock) 1 tablet, twice a day Control (route, total, dose/day, frequency): oral placebo (excipients only) 1 tablet, twice a day Duration of intervention: 12 weeks Duration of follow‐up: not applicable Run‐in period: not applicable Treatment before study: 1‐week washout period for those taking non‐hormonal climacteric drugs, supplements, antiepileptics, psycholeptics or psychoanaleptics. 4‐week washout period for those taking hormone replacement therapy Titration period: not applicable | |
| Outcomes | Primary outcomes: intensity of climacteric symptoms (MRS) Secondary outcomes: MRS subscales (hot flushes, atrophy, psyche and soma) Additional outcomes: adverse events, liver enzymes, BMI | |
| Notes | This study reported change‐from‐baseline scores; final value scores were not made available on request | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "each patient was randomly assigned to receive one blinded Remifemin tablet or matching placebo...medication was prenumbered using a 1:1 ‐ randomization block size of 4" (method of sequence generation not described) Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Unclear risk | Quote: "double‐blind", though there was no mention of who was blinded, or any assurance that interventions matched in appearance, taste or odour Comment: probably done |
| Incomplete outcome data (attrition bias) | Low risk | "The primary efficacy analysis used the Intention‐to‐treat population" Number and reasons for withdrawal were similar between groups |
| Selective reporting (reporting bias) | Unclear risk | All primary and secondary outcomes listed were reported, although no study protocol was published or lodged |
| Other bias | Low risk | There were no significant differences in participant characteristics between groups at baseline |
| Methods | Design: randomised, placebo‐controlled, double‐blind, multicentre, cross‐over trial Randomisation ratio: not stated Study duration: 4 months (from 31st October 2003 to 4th March 2004) | |
| Participants | Participant characteristics: 132 women were enrolled, 131 were randomised (black cohosh = 66, placebo = 65) and 32 (24.4%) dropped out. Mean age (black cohosh = 56.0 ± 8.3 years, placebo = 56.7 ± 8.9 years). Duration of menopause not stated Inclusion criteria: female, history of breast cancer or a perceived increased risk of breast cancer or did not wish to take oestrogen owing to the increased risk of breast cancer, ≥ 14 hot flushes per week for a period of at least 1 month for which therapeutic intervention was desired Exclusion criteria: malignant disease, concomitant use of anti‐neoplastic chemotherapy, androgens, oestrogens, oral herbal therapies, therapeutic herbal teas or tinctures, any prior use of black cohosh, use of antidepressants within the last 2 weeks (or planned use in the next 9 weeks), and current or planned use of other agents for treating hot flushes. Concomitant use of tamoxifen, raloxifene, aromatase inhibitors, vitamin E or soy were permitted if the participant had been on therapy for at least 1 month and were not anticipating a change in therapy/dosage during the study Diagnostic criteria: not stated Co‐morbidities: history of breast cancer (black cohosh = 59%, placebo = 69%) Co‐medications: tamoxifen (black cohosh = 40%, placebo = 48%), raloxifene (black cohosh = 2%, placebo = 0%), aromatase inhibitor (black cohosh = 12%, placebo = 10%), not receiving HT (black cohosh = 40%, placebo = 33%) | |
| Interventions | Number of study centres: not stated Country/location: US Setting: community clinics, hospitals and medical centres affiliated with the NCCTG Intervention (route, total, dose/day, frequency): oral extract of Cimicifuga racemosa rhizome (20 mg, standardised to 5% triterpene glycosides) 1 tablet, twice a day Control (route, total, dose/day, frequency): oral placebo (dosage and constitution not described) 1 tablet, twice a day Duration of intervention: 8 weeks (4 weeks' active treatment and 4 weeks' placebo treatment) Duration of follow‐up: not applicable Run‐in period: 1 week Treatment before study: 1 week run‐in period consisting of no treatment Titration period: not applicable | |
| Outcomes | Primary outcomes: hot flushes (severity and frequency) Secondary outcomes: GCS, quality of life, toxicity/adverse events Additional outcomes: treatment preference | |
| Notes | This study reported change‐from‐baseline scores; final value scores were provided on request | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "patients were randomly assigned" (method of sequence generation not described) Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Low risk | Quote: "all treatments were double‐blinded"; "participants received...black cohosh or an identical appearing placebo" Comment: probably done |
| Incomplete outcome data (attrition bias) | High risk | ITT was not mentioned. 16 women failed to provide hot flush data after baseline; however, the number and reasons for refusal were not given for each group separately |
| Selective reporting (reporting bias) | High risk | Excluding adverse events, data were reported for most primary and secondary outcomes, although no study protocol was published or lodged |
| Other bias | Low risk | There were no significant differences in participant characteristics between groups at baseline |
| Methods | Design: randomised, double‐blind, placebo‐controlled trial Randomisation ratio: not stated Study duration: not stated | |
| Participants | Participant characteristics: 80 women randomised (black cohosh = 30, CEO = 30, placebo = 20) and 16 (20%) dropped out. Mean age (black cohosh = 51.3 ± 3.1 years, CEO = 50.3 ± 2.8 years, placebo = 49.8 ± 3.1 years). Duration of menopause not stated Inclusion criteria: female, aged 46 to 58 years, ≥ 3 hot flushes a day, ≥ 1 other climacteric symptom Exclusion criteria: contraindications to HT, use of antihypertensive drugs, use of exogenous sexual hormones in the last 4 weeks, metabolic menopausal syndrome in the form of osteoporosis, menopause secondary to ovariectomy or radiation castration Diagnostic criteria: not stated Co‐morbidities: hysterectomy, uterine or vaginal prolapse, mycosis, biliary troubles, hypotension and varicosis were reported in 33 women (black cohosh = 11, CEO = 13, placebo = 9) Co‐medications: not stated | |
| Interventions | Number of study centres: not stated Country/location: not stated, possibly Germany Setting: not stated Intervention (route, total, dose/day, frequency): oral isopropanolic extract of Cimicifuga racemosa (Remifemin, 2 mg) 2 tablets twice a day; oral CEO (0.625 mg, plus 3 oral placebo tablets) daily for 21 days, then oral placebo (not described) 2 tablets, twice a day Control (route, total, dose/day, frequency): oral placebo (not described) 2 tablets, twice a day Duration of intervention: 12 weeks Duration of follow‐up: not applicable Run‐in period: not applicable Treatment before study: not stated Titration period: not applicable | |
| Outcomes | Primary outcomes: KI Secondary outcomes: Hamilton Anxiety Scale, vaginal epithelial proliferation, hot flushes, pruritus vulvae, genital inflammation, cohabitation/sexual complaints Additional outcomes: not stated | |
| Notes | Article in German. This study reported final value scores. Data had to be extrapolated from figures to be suitable for the pooling of results | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomised" (method not described) Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not don |
| Blinding (performance bias and detection bias) | Low risk | Quote: "double blind"; interventions were identical in taste and appearance (translated) Comment: probably done |
| Incomplete outcome data (attrition bias) | High risk | ITT was not mentioned The number and reasons for withdrawal differed between groups |
| Selective reporting (reporting bias) | Unclear risk | All primary and secondary outcomes listed were reported, although no study protocol was published or lodged |
| Other bias | Unclear risk | Baseline differences in mean parturition rate were observed |
| Methods | Design: randomised, double‐blind, placebo‐controlled, multicentre, parallel group trial Randomisation ratio: not stated Study duration: 23 months (from November 1998 to September 2000) | |
| Participants | Participant characteristics: 97 women were randomised, 2 (2.1%) dropped out and 33 (34%) violated the study protocol. This left 62 women for analysis (black cohosh = 20, CEO = 22, placebo = 20). Mean age (black cohosh = 52.25 ± 3.19, CEO = 52.32 ± 3.03, placebo = 54.05 ± 4.36). Mean duration of menopause not stated Inclusion criteria: female, postmenopausal, aged 40 to 60 years, BMI ≤ 30 kg/m2, last menstrual bleed ≥ 6 months ago, 17β‐oestradiol ≤ 40 pg/mL and FSH ≥ 25 mIU/mL, ≥ 3 hot flushes a day during the run‐in period, MRS (MRS, sum of items 1 to 6) ≥ 1.7 at visits 1 and 2, MRS item 1 ≥ 0.3 at visits 1 and 2 Exclusion criteria: signs of ovulatory or anovulatory cycles during the run‐in period, hysterectomy, non‐response to pretreatment with oestrogens, contraindications to HT, unresolved genital bleeding, suspicion or existence of an oestrogen‐dependent breast or endometrial carcinoma, endometrial thickness > 5 mm, endometriosis, past or present thromboembolism, phlebitis, acute or chronic hepatic lesion, metabolic disorders of bile pigments, diabetes mellitus, sickle cell anaemia, clinically relevant hypertriglyceridaemia or hypercholesterolaemia, history of myocardial infarction, genital neoplasms, known sensitivity to investigational drugs or ingredients, concomitant treatment with oestrogenic substances, psychotropics, antidepressants, hypnotics or sedatives, alcohol or drug abuse, poor general condition Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: not stated | |
| Interventions | Number of study centres: 13 Country/location: Czech Republic Setting: private gynaecological practices and outpatient clinics Intervention (route, total, dose/day, frequency): oral dried/ethanolic extract of Cimicifuga racemosa rhizome (Klimadynon or Menofem, 20 mg) 2 capsules daily; oral CEO (Oestrofeminal, 0.3 mg) 2 capsules daily Control (route, total, dose/day, frequency): oral placebo (constitution not described) 2 capsules daily Duration of intervention: 12 weeks Duration of follow‐up: not applicable Run‐in period: 2 weeks Treatment before study: not stated Titration period: not applicable | |
| Outcomes | Primary outcomes: CrossLaps (bone degradation marker), bone‐specific ALP (bone formation marker), LH, FSH, sex hormone binding globulin, total cholesterol, high‐density lipoprotein cholesterol, low‐density lipoprotein cholesterol, triglycerides, 17β‐oestradiol, vaginal cytology, MRS Secondary outcomes: hot flushes, vaginal bleeding, endometrial thickness, MRS subscores (major climacteric complaints, somatic complaints, mental score), sweating episodes, sleep disturbances Additional outcomes: blood chemistry, liver function test, complete blood count, activated thromboplastin time, international normalised ratio, blood pressure, heart rate, body weight, adverse events | |
| Notes | Intervention may be a combination formula, although this is not clear. This study reported change‐from‐baseline scores; final value scores were not provided on request. To extract data suitable for the pooling of results, standard errors had to be converted to standard deviations, some data extrapolated from figures, and postintervention means extrapolated from baseline and change from baseline data | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "patients were randomized to treatments using a randomly permuted block design" (method of sequence generation not described) Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not described Comment: probably not done |
| Blinding (performance bias and detection bias) | Low risk | Quote: "double‐blind"; "All three preparations were identical in appearance" Comment: probably done |
| Incomplete outcome data (attrition bias) | High risk | "The remaining...women were included in the per‐protocol (PP) analysis" Participant withdrawals were not reported |
| Selective reporting (reporting bias) | High risk | Data is reported for the primary outcome, and for most secondary outcomes (excluding hot flushes, vaginal bleeding and sleep disturbances). No study protocol was published or lodged |
| Other bias | Unclear risk | Baseline differences in MRS scores and oestradiol and FSH levels were observed |
ALP: alkaline phosphatase; BMI: body mass index; CEO: conjugated equine oestrogen; CHD: coronary heart disease; DEXA, dual‐energy X‐ray absorptiometry; DSM‐IV: Diagnostic and Statistical Manual of Mental Disorders, 4th Edition; FSH: follicle stimulation hormone; GCS: Greene Climacteric Scale; HRQoL: health‐related quality of life; HT: hormone therapy; ITT: intention to treat; KI: Kupperman Index; LH: luteinising hormone; MDP: medroxyprogesterone; MRS: Menopause Rating Scale; NCCTG: North Central Cancer Treatment Group; SERM: selective oestrogen receptor modulator.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
| The active intervention was a combination formulation (black cohosh and St. John's Wort) | |
| The active intervention was a combination formulation (black cohosh and St. John's Wort) | |
| The trial was a dose comparison study; hence, the comparator group was inappropriate | |
| The active intervention was a combination formulation (black cohosh and St. John's Wort) | |
| The active intervention was a combination formulation (black cohosh and St. John's Wort) | |
| The active intervention was a combination formulation (black cohosh, dong quai, milk thistle, red clover, American ginseng and chaste‐tree berry) | |
| The active intervention was a combination formulation (black cohosh, isoflavones and lignans) | |
| The active intervention was a combination formulation (black cohosh and St. John's Wort) | |
| The active intervention was a combination formulation (black cohosh and Soy isoflavones) |
Characteristics of studies awaiting assessment [ordered by study ID]
| Methods | Design: randomised, placebo‐controlled trial Randomisation ratio: not stated Study duration: not stated |
| Participants | Participant characteristics: 80 healthy symptomatic postmenopausal women Inclusion criteria: female and postmenopausal Exclusion criteria: not stated Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: not stated |
| Interventions | Number of study centres: 1 Country/location: not stated Setting: university affiliated tertiary centre Intervention (route, total, dose/day, frequency): dried extract of Cimicifuga racemosa rhizome (Klimadynon), 40 mg daily Control (route, total, dose/day, frequency): placebo (description and dosage not reported) Duration of intervention: 12 months Duration of follow‐up: not stated Run‐in period: not stated Treatment before study: not stated Titration period: not stated |
| Outcomes | Primary outcomes: not stated Secondary outcomes: not stated Additional outcomes: MRS, endometrial thickness, breast changes |
| Notes | Conference abstract only. Unable to locate author or full‐text article |
| Methods | Design: randomised controlled trial Randomisation ratio: not stated Study duration: not stated |
| Participants | Participant characteristics: 90 postmenopausal women Inclusion criteria: female and postmenopausal Exclusion criteria: not stated Diagnostic criteria: not stated Co‐morbidities: not stated Co‐medications: not stated |
| Interventions | Number of study centres: not stated Country/location: not stated Setting: not stated Intervention (route, total, dose/day, frequency): black cohosh root extract (description and dosage not reported) Control (route, total, dose/day, frequency): CEO 0.625 mg (frequency not reported) Duration of intervention: 6 months Duration of follow‐up: not stated Run‐in period: not stated Treatment before study: not stated Titration period: not stated |
| Outcomes | Primary outcomes: not stated Secondary outcomes: not stated Additional outcomes: KI, bone mineral density, urinary deoxypyridinolin |
| Notes | Conference abstract only. Unable to locate author or full‐text article |
CEO: conjugated equine oestrogen; KI: Kupperman Index; MRS: Menopause Rating Scale.
Characteristics of ongoing studies [ordered by study ID]
| Trial name or title | Black Cohosh Extract for the Management of Moderate to Severe Menopausal Symptoms in Thai Women |
| Methods | Randomised, double‐blind, placebo‐controlled trial with 2 parallel arms |
| Participants | Thai women; perimenopausal or postmenopausal; ≥ 40 years of age; Kupperman Index score ≥ 20 |
| Interventions | Cimicifuga racemosa rhizome and root extract or placebo, for 12 weeks |
| Outcomes | Kupperman Index score, frequency of menopausal symptoms, adverse events, liver function, quality of life |
| Starting date | December 2011 |
| Contact information | Dr Patsama Vichinsartvichai. Email: [email protected] |
| Notes | ‐ |
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Vasomotor symptoms: daily hot flush frequency Show forest plot | 3 | 393 | Mean Difference (IV, Fixed, 95% CI) | 0.07 [‐0.43, 0.56] |
| Analysis 1.1  Comparison 1 Black cohosh versus placebo, Outcome 1 Vasomotor symptoms: daily hot flush frequency. | ||||
| 2 Vasomotor symptoms: weekly hot flush frequency Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Analysis 1.2  Comparison 1 Black cohosh versus placebo, Outcome 2 Vasomotor symptoms: weekly hot flush frequency. | ||||
| 3 Vasomotor symptoms: hot flush intensity Show forest plot | 3 | 214 | Mean Difference (IV, Fixed, 95% CI) | 0.12 [‐0.06, 0.30] |
| Analysis 1.3  Comparison 1 Black cohosh versus placebo, Outcome 3 Vasomotor symptoms: hot flush intensity. | ||||
| 4 Vasomotor symptoms: night sweats Show forest plot | 1 | 164 | Mean Difference (IV, Fixed, 95% CI) | 0.27 [‐0.16, 0.70] |
| Analysis 1.4  Comparison 1 Black cohosh versus placebo, Outcome 4 Vasomotor symptoms: night sweats. | ||||
| 4.1 Night sweat frequency per day | 1 | 164 | Mean Difference (IV, Fixed, 95% CI) | 0.27 [‐0.16, 0.70] |
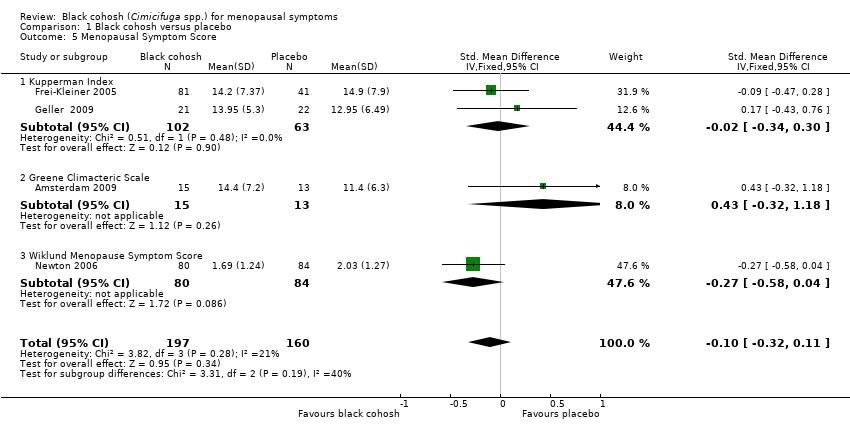
| 5 Menopausal Symptom Score Show forest plot | 4 | 357 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐0.32, 0.11] |
| Analysis 1.5  Comparison 1 Black cohosh versus placebo, Outcome 5 Menopausal Symptom Score. | ||||
| 5.1 Kupperman Index | 2 | 165 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.02 [‐0.34, 0.30] |
| 5.2 Greene Climacteric Scale | 1 | 28 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.43 [‐0.32, 1.18] |
| 5.3 Wiklund Menopause Symptom Score | 1 | 164 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.27 [‐0.58, 0.04] |
| 6 Adverse events Show forest plot | 2 | 344 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.82, 1.32] |
| Analysis 1.6  Comparison 1 Black cohosh versus placebo, Outcome 6 Adverse events. | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Vasomotor symptoms: daily hot flush frequency Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Analysis 2.1  Comparison 2 Black cohosh versus hormone therapy, Outcome 1 Vasomotor symptoms: daily hot flush frequency. | ||||
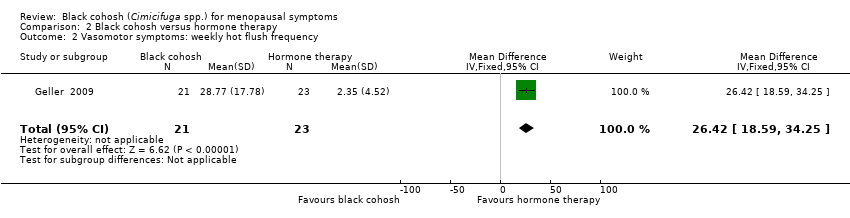
| 2 Vasomotor symptoms: weekly hot flush frequency Show forest plot | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 26.42 [18.59, 34.25] |
| Analysis 2.2  Comparison 2 Black cohosh versus hormone therapy, Outcome 2 Vasomotor symptoms: weekly hot flush frequency. | ||||
| 3 Vasomotor symptoms: hot flush intensity Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Analysis 2.3  Comparison 2 Black cohosh versus hormone therapy, Outcome 3 Vasomotor symptoms: hot flush intensity. | ||||
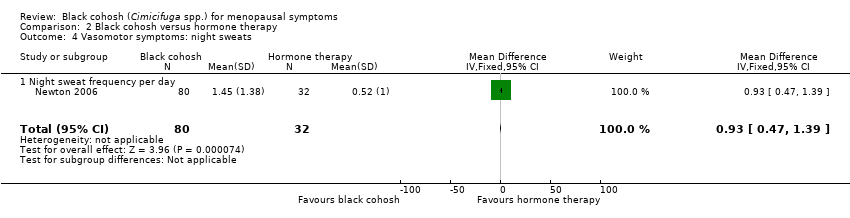
| 4 Vasomotor symptoms: night sweats Show forest plot | 1 | 112 | Mean Difference (IV, Fixed, 95% CI) | 0.93 [0.47, 1.39] |
| Analysis 2.4  Comparison 2 Black cohosh versus hormone therapy, Outcome 4 Vasomotor symptoms: night sweats. | ||||
| 4.1 Night sweat frequency per day | 1 | 112 | Mean Difference (IV, Fixed, 95% CI) | 0.93 [0.47, 1.39] |
| 5 Menopausal Symptom Score Show forest plot | 5 | 468 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.32 [0.13, 0.51] |
| Analysis 2.5  Comparison 2 Black cohosh versus hormone therapy, Outcome 5 Menopausal Symptom Score. | ||||
| 5.1 Kupperman Index | 3 | 312 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.20 [‐0.02, 0.43] |
| 5.2 Greene Climacteric Scale | 1 | 44 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.25 [‐0.37, 0.87] |
| 5.3 Wiklund Menopause Symptom Score | 1 | 112 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.77 [0.35, 1.19] |
| 6 Adverse events Show forest plot | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.21, 3.24] |
| Analysis 2.6  Comparison 2 Black cohosh versus hormone therapy, Outcome 6 Adverse events. | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
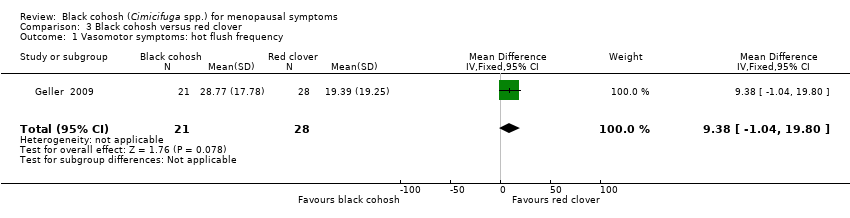
| 1 Vasomotor symptoms: hot flush frequency Show forest plot | 1 | 49 | Mean Difference (IV, Fixed, 95% CI) | 9.38 [‐1.04, 19.80] |
| Analysis 3.1  Comparison 3 Black cohosh versus red clover, Outcome 1 Vasomotor symptoms: hot flush frequency. | ||||
| 2 Vasomotor symptoms: hot flush intensity Show forest plot | 1 | 50 | Mean Difference (IV, Fixed, 95% CI) | 0.42 [‐0.08, 0.92] |
| Analysis 3.2  Comparison 3 Black cohosh versus red clover, Outcome 2 Vasomotor symptoms: hot flush intensity. | ||||
| 3 Menopausal score Show forest plot | 1 | 51 | Mean Difference (IV, Fixed, 95% CI) | ‐1.28 [‐5.48, 2.92] |
| Analysis 3.3  Comparison 3 Black cohosh versus red clover, Outcome 3 Menopausal score. | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Vasomotor symptoms: night sweats Show forest plot | 1 | 80 | Mean Difference (IV, Fixed, 95% CI) | ‐85.0 [‐132.50, ‐37.50] |
| Analysis 4.1  Comparison 4 Black cohosh versus fluoxetine, Outcome 1 Vasomotor symptoms: night sweats. | ||||
| 1.1 Night sweat score per month | 1 | 80 | Mean Difference (IV, Fixed, 95% CI) | ‐85.0 [‐132.50, ‐37.50] |
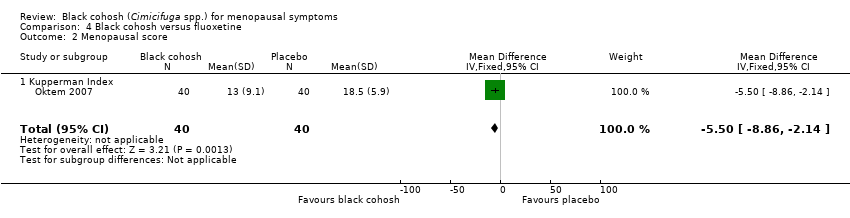
| 2 Menopausal score Show forest plot | 1 | 80 | Mean Difference (IV, Fixed, 95% CI) | ‐5.5 [‐8.86, ‐2.14] |
| Analysis 4.2  Comparison 4 Black cohosh versus fluoxetine, Outcome 2 Menopausal score. | ||||
| 2.1 Kupperman Index | 1 | 80 | Mean Difference (IV, Fixed, 95% CI) | ‐5.5 [‐8.86, ‐2.14] |
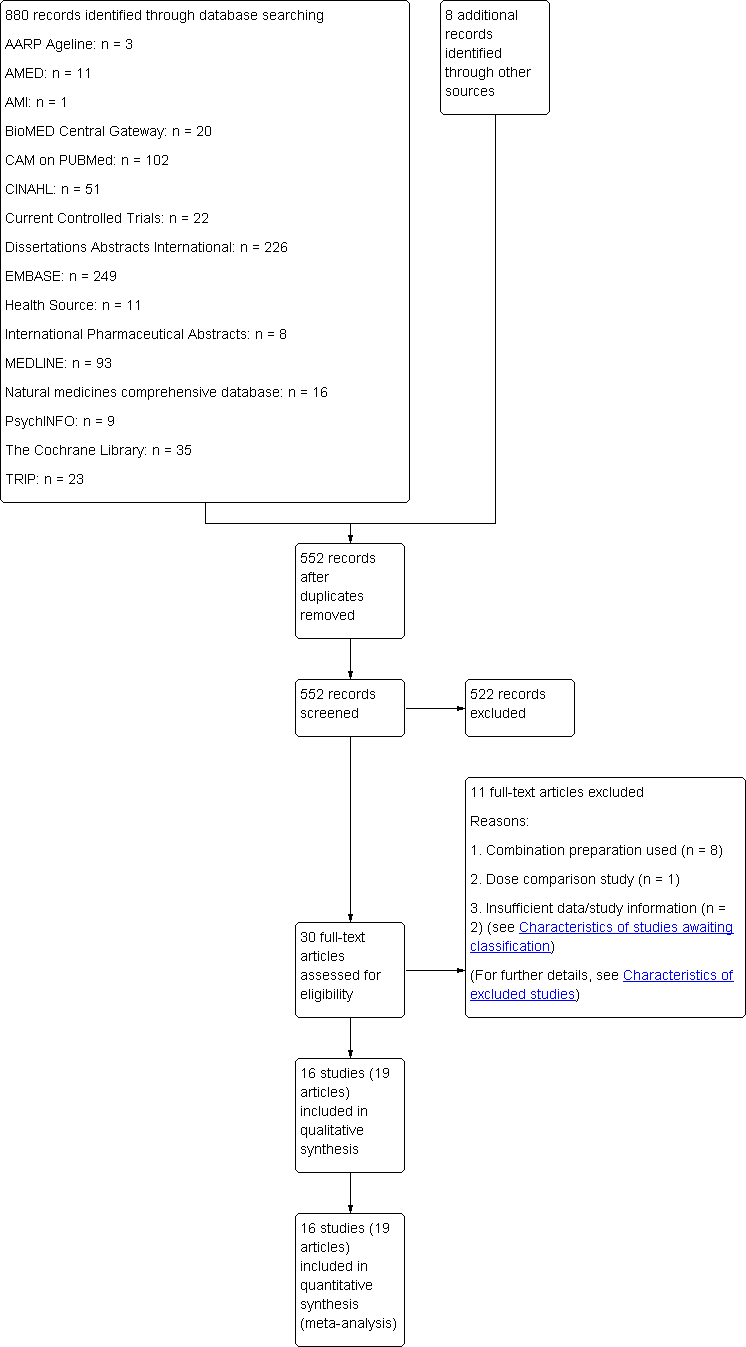
Study flow diagram.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Risk of bias graph: review authors' judgements about each 'Risk of bias' item presented as percentages across all included studies.

Forest plot of comparison: 1 Black cohosh versus placebo, outcome: 1.1 Vasomotor symptoms: daily hot flush frequency.

Forest plot of comparison: 1 Black cohosh versus placebo, outcome: 1.5 Menopausal Symptom Score.
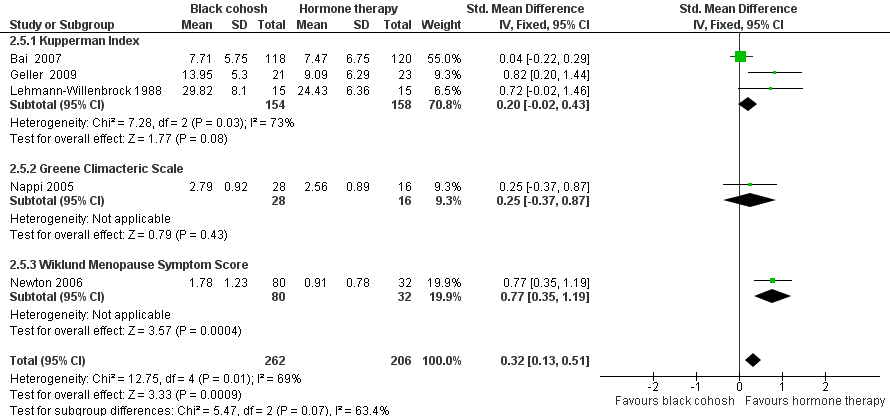
Forest plot of comparison: 2 Black cohosh versus hormone therapy, outcome: 2.5 Menopausal Symptom Score.

Comparison 1 Black cohosh versus placebo, Outcome 1 Vasomotor symptoms: daily hot flush frequency.
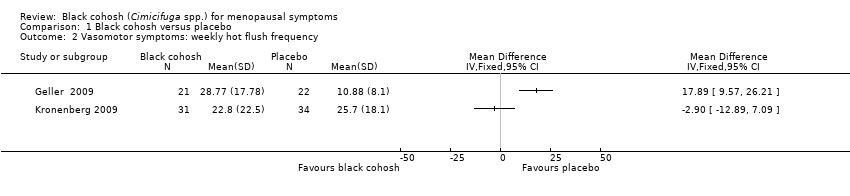
Comparison 1 Black cohosh versus placebo, Outcome 2 Vasomotor symptoms: weekly hot flush frequency.
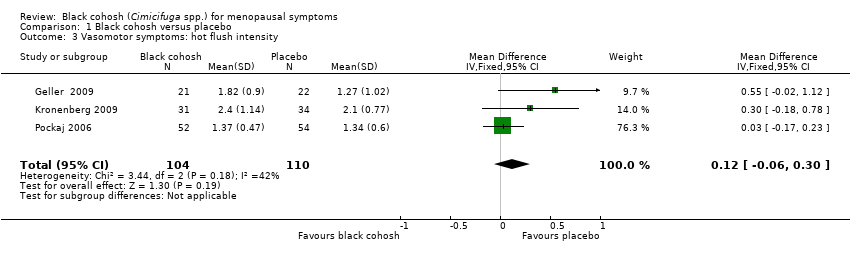
Comparison 1 Black cohosh versus placebo, Outcome 3 Vasomotor symptoms: hot flush intensity.

Comparison 1 Black cohosh versus placebo, Outcome 4 Vasomotor symptoms: night sweats.
Comparison 1 Black cohosh versus placebo, Outcome 5 Menopausal Symptom Score.

Comparison 1 Black cohosh versus placebo, Outcome 6 Adverse events.

Comparison 2 Black cohosh versus hormone therapy, Outcome 1 Vasomotor symptoms: daily hot flush frequency.
Comparison 2 Black cohosh versus hormone therapy, Outcome 2 Vasomotor symptoms: weekly hot flush frequency.

Comparison 2 Black cohosh versus hormone therapy, Outcome 3 Vasomotor symptoms: hot flush intensity.
Comparison 2 Black cohosh versus hormone therapy, Outcome 4 Vasomotor symptoms: night sweats.

Comparison 2 Black cohosh versus hormone therapy, Outcome 5 Menopausal Symptom Score.

Comparison 2 Black cohosh versus hormone therapy, Outcome 6 Adverse events.
Comparison 3 Black cohosh versus red clover, Outcome 1 Vasomotor symptoms: hot flush frequency.

Comparison 3 Black cohosh versus red clover, Outcome 2 Vasomotor symptoms: hot flush intensity.

Comparison 3 Black cohosh versus red clover, Outcome 3 Menopausal score.

Comparison 4 Black cohosh versus fluoxetine, Outcome 1 Vasomotor symptoms: night sweats.
Comparison 4 Black cohosh versus fluoxetine, Outcome 2 Menopausal score.
| Black cohosh versus placebo for menopausal symptoms | ||||||
| Patient or population: patients with menopausal symptoms | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Black cohosh versus placebo | |||||
| Vasomotor symptoms: daily hot flush frequency | The mean vasomotor symptoms: daily hot flush frequency in the intervention groups was | 393 | ⊕⊕⊕⊝ | |||
| Vasomotor symptoms: hot flush intensity | The mean vasomotor symptoms: hot flush intensity in the intervention groups was | 214 | ⊕⊕⊕⊝ | |||
| Vasomotor symptoms: night sweats | The mean vasomotor symptoms: night sweats in the intervention groups was | 164 | ⊕⊕⊕⊝ | |||
| Menopausal Symptom Score | The mean menopausal symptom score in the intervention groups was | 357 | ⊕⊕⊕⊝ | SMD ‐0.1 (‐0.32 to 0.11) | ||
| Adverse events | 427 per 1000 | 444 events per 1000 women | RR 1.04 | 344 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Two of the three trials did not provide sufficient details for randomisation and allocation concealment and two trials did not provide details for reasons for losses to follow up in each group | ||||||
| Domain | Support for judgement | Review authors’ judgement |
| Selection bias |
|
|
| Random sequence generation | Describe the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups | Selection bias (biased allocation to interventions) owing to inadequate generation of a randomised sequence |
| Allocation concealment | Describe the method used to conceal the allocation sequence in sufficient detail to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment | Selection bias (biased allocation to interventions) owing to inadequate concealment of allocations prior to assignment |
| Performance bias |
|
|
| Blinding of participants and personnel Assessments should be made for each main outcome (or class of outcomes) | Describe all measures used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. Provide any information relating to whether the intended blinding was effective | Performance bias owing to knowledge of the allocated interventions by participants and personnel during the study |
| Detection bias |
|
|
| Blinding of outcome assessmentAssessments should be made for each main outcome (or class of outcomes) | Describe all measures used, if any, to blind outcome assessors from knowledge of which intervention a participant received. Provide any information relating to whether the intended blinding was effective | Detection bias owing to knowledge of the allocated interventions by outcome assessors |
| Attrition bias |
|
|
| Incomplete outcome dataAssessments should be made for each main outcome (or class of outcomes) | Describe the completeness of outcome data for each main outcome, including attrition and exclusions from the analysis. State whether attrition and exclusions were reported, the numbers in each intervention group (compared with total randomised participants), reasons for attrition/exclusions where reported, and any re‐inclusions in analyses performed by the review authors | Attrition bias owing to amount, nature or handling of incomplete outcome data |
| Reporting bias |
|
|
| Selective reporting | State how the possibility of selective outcome reporting was examined by the review authors, and what was found | Reporting bias owing to selective outcome reporting |
| Other bias |
|
|
| Other sources of bias | State any important concerns about bias not addressed in the other domains in the tool. If particular questions/entries were pre‐specified in the review’s protocol, responses should be provided for each question/entry | Bias owing to problems not covered elsewhere in the table |
| Study | Interventions | Age (years), mean (SD) | Ethnic groups (%) | Duration of amenorrhoea (years), mean (SD) | Body mass index (kg/m2), mean (SD) |
| Amsterdam 2009 | I1: black cohosh | I1: 56.7 (6.5) | I1: White (71.4) | I1: NR | I1: NR |
| C1: placebo | C1: 50.8 (3.2) | C1: White (61.5) | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | ||
| Bai 2007 | I1: black cohosh | I1: 51.8 (3.7) | I1: NR | I1: 2.68 (2.05) | I1: 23.2 (2.3) |
| C1: tibolone | C1: 51.5 (3.5) | C1: NR | C1: 2.95 (2.11) | C1: 23.5 (2.4) | |
| Total: NR | Total: NR | Total: NR | Total: NR | ||
| Bebenek 2010 | I1: exercise + black cohosh | I1: 51.8 (2.7) | I1: NR | I1: NR | I1: NR |
| I2: exercise only | I2: 52.3 (2.3) | I2: NR | I2: NR | I2: NR | |
| C1: wellness control | C1: 52.4 (2.7) | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | ||
| Carlisle 2008 | I1: black cohosh + calcium and vitamin D supplement | I1: 54.1 (5.0) | I1: NR | I1: NR | I1: 29.0 (5.4) |
| C1: placebo + calcium and vitamin D supplement | C1: 52.8 (4.4) | C1: NR | C1: NR | C1: 29.8 (6.1) | |
| Total: 53.4 (4.7) | Total: NR | Total: NR | Total: 29.4 (5.7) | ||
| Frei‐Kleiner 2005 | I1: black cohosh | I1: 52.5 (3.7) | I1: NR | I1: 3.23 (4.21) | I1: NR |
| C1: placebo | C1: 52.2 (3.5) | C1: NR | C1: 3.11 (4.28) | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | ||
| Geller 2009 | I1: black cohosh | I1: 54.4 (3.9) | I1: White (61.9), African‐American (38.1), Hispanic (0) | I1: 3.4 (2.6) | I1: 28.3 (4.5) |
| I2: red clover | I2: 52.4 (4.6) | I2: White (22.7), African‐American (59.1), Hispanic (13.6) | I2: 4.1 (2.8) | I2: 30.5 (4.3) | |
| I3: conjugated oestrogen + MDP | I3: 53.3 (4.0) | I3: White (69.9), African‐American (30.4), Hispanic (0) | I3: 3.6 (2.9) | I3: 26.0 (3.9) | |
| C1: placebo | C1: 52.0 (4.2) | C1: White (22.7), African‐American (72.7), Hispanic (4.6) | C1: 2.8 (2.9) | C1: 30.1 (4.9) | |
| Total: 53.0 (4.2) | Total: White (44.3), African‐American (50.0), Hispanic (4.5) | Total: 3.5 (2.8) | Total: 28.7 (4.7) | ||
| Jacobson 2001 | I1: black cohosh | I1: NR | I1: European‐American (71.4), Hispanic (16.7), African‐American (9.5) | I1: NR | I1: NR |
| C1: placebo | C1: NR | C1: NR | C1: NR | ||
| Total: NR | Total: NR | Total: NR | Total: NR | ||
| Kronenberg 2009 | I1: black cohosh | I1: 55.1 (4.1) | I1: White (86.5), African (10.8) | I1: NR | I1: 25.7 (3.9) |
| C1: placebo | C1: 54.2 (3.6) | C1: White (86.5), African (5.4) | C1: 24.8 (4.0) | ||
| Total: 54.7 (3.8) | Total: White (86.5), African (8.1) | Total: NR | Total: 25.2 (3.9) | ||
| Lehmann‐Willenbrock 1988 | I1: black cohosh | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: oestriol | C1: NR | C1: NR | C1: NR | C1: NR | |
| C2: conjugated oestrogen | C2: NR | C2: NR | C2: NR | C2: NR | |
| C3: oestradiol/ norethisterone acetate | C3: NR | C3: NR | C3: NR | C3: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | ||
| Nappi 2005 | I1: black cohosh | I1: 50.5 (2.1) | I1: NR | I1: NR | I1: 22.9 (2.2) |
| C1: oestradiol + dihydrogesterone | C1: 50.9 (1.8) | C1: NR | C1: NR | C1: 22.0 (2.1) | |
| Total: NR | Total: NR | Total: NR | Total: NR | ||
| Newton 2006 / Reed 2008 | I1: black cohosh | I1: 52.0 (2.2) | I1: White (91), African‐American (4) | I1: NR | I1: 27.3 (5.0) |
| I2: multi‐botanical | I2: 52.2 (2.5) | I2: White (99), African‐American (1) | I2: NR | I2: 28.4 (6.3) | |
| I3: mult‐ibotanical + dietary soy | I3: 52.5 (2.5) | I3: White (95), African‐American (4) | I3: NR | I3: 28.4 (5.7) | |
| I4: conjugated oestrogen + MDP | I4: 52.3 (2.6) | I4: White (94), African‐American (0) | I4: NR | I4: 31.5 (7.9) | |
| C1: placebo | C1: 52.0 (2.5) | C1: White (88), African‐American (2) | C1: NR | C1: 29.2 (6.4) | |
| Total: 52.2 (2.4) | Total: White (93), African‐American (3) | Total: NR | Total: 28.6 (6.2) | ||
| Oktem 2007 | I1: black cohosh | I1: 53.1 (5.6) | I1: NR | I1: NR | I1: 26.5 (3.8) |
| C1: fluoxetine | C1: 52.7 (6.4) | C1: NR | C1: NR | C1: 27.8 (3.8) | |
| Total: NR | Total: NR | Total: NR | Total: NR | ||
| Osmers 2005 | I1: black cohosh | I1: 54.6 (6.0) | I1: NR | I1: NR | I1: 25.5 (3.0) |
| C1: placebo | C1: 55.0 (6.0) | C1: NR | C1: NR | C1: 24.9 (2.7) | |
| Total: NR | Total: NR | Total: NR | Total: NR | ||
| Pockaj 2006 | I1: black cohosh | I1: 56.0 (8.3) | I1: NR | I1: NR | I1: NR |
| C1: placebo | C1: 56.7 (8.9) | C1: NR | C1: NR | C1: NR | |
| Total: 56.4 (8.5) | Total: NR | Total: NR | Total: NR | ||
| Stoll 1987 | I1: black cohosh | I1: 51.3 (3.1) | I1: NR | I1: NR | I1: NR |
| C1: oestrogen | C1: 50.3 (2.8) | C1: NR | C1: NR | C1: NR | |
| C2: placebo | C2: 49.8 (3.1) | C2: NR | C2: NR | C2: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | ||
| Wuttke 2003/2006a/2006b | I1: black cohosh | I1: 52.3 (3.2) | I1: NR | I1: NR | I1: NR |
| C1: conjugated oestrogens | C1: 52.3 (3.0) | C1: NR | C1: NR | C1: NR | |
| C2: placebo | C2: 54.1 (4.4) | C2: NR | C2: NR | C2: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | ||
| C: control; I: intervention; NR: not recorded. | |||||
| Frequency of hot flushes per week, mean (SD) | Frequency of hot flushes per day, mean (SD) | Intensity of hot flushes, mean (SD) (define index/scale) | Frequency of night sweats per week, mean (SD) | Intensity of night sweats, mean (SD) (define index/scale) | Frequency of urogenital symptoms per week, mean (SD) (define symptoms) | Intensity of urogenital symptoms, mean (SD) (define symptoms and index/scale) | |
| Amsterdam 2009 | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Bai 2007 | I1: 30.0 (26.1) | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: 30.1 (20.1) | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Bebenek 2010 | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| I2: NR | I2: NR | I2: NR | I2: NR | I2: NR | I2: NR | I2: NR | |
| C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Carlisle 2008 | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Frei‐Kleiner 2005 | I1: NR | I1: 2.3 (1.9) | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: 3.5 (3.7) | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Geller 2009 | I1: 44.8 (16.7) | I1: NR | I1: 2.4 (0.6) (3‐point severity scale) | I1: NR | I1: NR | I1: NR | I1: 0.8 (1.0) |
| I2: 40.3 (15.4) | I2: NR | I2: 2.2 (0.7) (3‐point severity scale) | I2: NR | I2: NR | I2: NR | I2: 1.1 (1.0) | |
| I3: 52.1 (34.5) | I3: NR | I3: 2.0 (0.7) (3‐point severity scale) | I3: NR | I3: NR | I3: NR | I3: 0.7 (0.9) | |
| C1: 33.7 (14.1) | C1: NR | C1: 2.3 (0.7) (3‐point severity scale) | C1: NR | C1: NR | C1: NR | C1: 1.1 (0.9) | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| (Vaginal dryness, 3‐point scale) | |||||||
| Jacobson 2001 | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Kronenberg 2009 | I1: 37.6 (18.7) | I1: NR | I1: 2.5 (1.04) | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: 40.1 (16.6) | C1: NR | C1: 2.4 (0.85) | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: 38.9 (17.5) | Total: NR | Total: 2.5 (0.94) | Total: NR | Total: NR | Total: NR | Total: NR | |
| (scale not defined) | |||||||
| Lehmann‐Willenbrock 1988 | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| C2: NR | C2: NR | C2: NR | C2: NR | C2: NR | C2: NR | C2: NR | |
| C3: NR | C3: NR | C3: NR | C3: NR | C3: NR | C3: NR | C3: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Nappi 2005 | I1: 10.5 (1.5) | I1: 11.0 (2.7) | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: 11.5 (1.0) | C1: 10.4 (2.3) | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Newton 2006 / Reed 2008 | I1: 32.9 (17.5) | I1: 4.7 (3.0) | I1: NR | I1: 14.0 (8.4) | I1: NR | I1: NR | I1: NR |
| I2: 30.8 (21.0) | I2: 4.4 (3.0) | I2: NR | I2: 12.6 (7.7) | I2: NR | I2: NR | I2: NR | |
| I3: 32.2 (22.4) | I3: 4.6 (3.0) | I3: NR | I3: 13.3 (8.4) | I3: NR | I3: NR | I3: NR | |
| I4: 35.0 (30.8) | I4: 5.2 (4.6) | I4: NR | I4: 12.6 (7.0) | I4: NR | I4: NR | I4: NR | |
| C1: 30.1 (21.0) | C1: 4.3 (3.0) | C1: NR | C1: 13.3 (8.4) | C1: NR | C1: NR | C1: NR | |
| Total: 32.2 (21.7) | Total: NR | Total: NR | Total: 13.3 (8.4) | Total: NR | Total: NR | Total: NR | |
| Oktem 2007 | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Osmers 2005 | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| (median reported but no ranges) | |||||||
| Pockaj 2006 | I1: NR | I1: 6.7 (3.7) | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: 6.2 (3.6) | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Stoll 1987 | I1: 4.9 (‐) | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: 5.2 (‐) | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| C2: 5.1 (‐) | C2: NR | C2: NR | C2: NR | C2: NR | C2: NR | C2: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Wuttke 2003/2006a/2006b | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| C: control; I: intervention; NR: not recorded. | |||||||
| Study | Intensity of urogenital symptoms, mean (SD) (define symptoms and index/scale) | Menopausal symptom score, mean (SD) (define index/scale) | Quality of life, mean (SD) (define index/scale) | Sexuality, mean (SD) (define outcome measure) | Bone health, mean (SD) (define outcome measure) |
| Amsterdam 2009 | I1: NR | I1: NR | I1: 112.4 (19.5) (PGWBI) | I1: NR | I1: NR |
| C1: NR | C1: NR | C1: 115.2 (24.1) (PGWBI) | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Bai 2007 | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: 24.7 (6.1) (KI) | Total: NR | Total: NR | Total: NR | |
| Bebenek 2010 | I1: NR | I1: 11.86 (4.71) (MRS) | I1: NR | I1: NR | I1: 0.97 (0.13) (BMD, lumbar) |
| I1: 0.77 (0.10) (BMD, fem. head) | |||||
| I2: NR | I2: 10.84 (5.35) (MRS) | I2: NR | I2: NR | I2: 0.96 (0.12) (BMD, lumbar) | |
| I2: 0.76 (0.10) (BMD, fem. head) | |||||
| C1: NR | C1: 9.88 (3.48) (MRS) | C1: NR | C1: NR | C1: 0.99 (0.13) (BMD, lumbar) | |
| C1: 0.75 (0.11) (BMD, fem. head) | |||||
| Total: NR | Total: NR | Total: NR | Total: NR | Totals: NR | |
| Carlisle 2008 | I1: NR | I1: NR | I1: NR | I1: NR | I1: 10.65 (2.78) (serum osteocalcin, ng/mL) |
| I1: 0.48 (0.25) (C‐terminal telopeptide, ng/mL) | |||||
| C1: NR | C1: NR | C1: NR | C1: NR | C1: 11.19 (4.16) (serum osteocalcin, ng/mL) | |
| C1: 0.56 (0.32) (C‐terminal telopeptide, ng/mL) | |||||
| Total: NR | Total: NR | Total: NR | Total: NR | Totals: NR | |
| Frei‐Kleiner 2005 | I1: NR | I1: 19.5 (7.9) (KI) | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: 19.0 (7.2) (KI) | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Geller 2009 | I1: 0.8 (1.0) | I1: 18.2 (5.4) | I1: NR | I1: NR | I1: NR |
| I2: 1.1 (1.0) | I2: 22.5 (8.1) | I2: NR | I2: NR | I2: NR | |
| I3: 0.7 (0.9) | I3: 19.2 (7.8) | I3: NR | I3: NR | I3: NR | |
| C1: 1.1 (0.9) | C1: 20.7 (6.6) | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| (Vaginal dryness, 3‐point scale) | |||||
| Jacobson 2001 | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Kronenberg 2009 | I1: NR | I1: 18.5 (8.8) (GCS) | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: 19.1 (9.6) (GCS) | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: 18.8 (9.2) (GCS) | Total: NR | Total: NR | Total: NR | |
| Lehmann‐Willenbrock 1988 | I1: NR | I1: 48.73 (8.72) (KI) | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: 49.12 (7.76) (KI) | C1: NR | C1: NR | C1: NR | |
| C2: NR | C2: 46.44 (8.18) (KI) | C2: NR | C2: NR | C2: NR | |
| C3: NR | C3: 47.84 (8.52) (KI) | C3: NR | C3: NR | C3: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Nappi 2005 | I1: NR | I1: 7.5 (0.6) (GCS) | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: 8.0 (0.9) (GCS) | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Newton 2006 / Reed 2008 | I1: NR | I1: 2.2 (1.2) | I1: NR | I1: NR | I1: NR |
| I2: NR | I2: 2.2 (1.1) | I2: NR | I2: NR | I2: NR | |
| I3: NR | I3: 2.2 (1.2) | I3: NR | I3: NR | I3: NR | |
| I4: NR | I4: 2.1 (1.0) | I4: NR | I4: NR | I4: NR | |
| C1: NR | C1: 2.5 (1.2) | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: 2.3 (1.2) | Total: NR | Total: NR | Total: NR | |
| Oktem 2007 | I1: NR | I1: 25.1 (6.7) (mKI) | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: 25.2 (6.8) (mKI) | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Osmers 2005 | I1: NR | I1: 0.35 (0.12) (MRS) | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: 0.35 (0.12) (MRS) | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Pockaj 2006 | I1: NR | I1: NR | I1: NR | I1: NR | I1: NR |
| C1: NR | C1: NR | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Stoll 1987 | I1: NR | I1: 34.4 (‐) (KI) | I1: NR | I1: 1.9 (‐) (NSC) | I1: NR |
| C1: NR | C1: 34.0 (‐) (KI) | C1: NR | C1: 1.5 (‐) (NSC) | C1: NR | |
| C2: NR | C2: 31.0 (‐) (KI) | C2: NR | C2: 1.6 (‐) (NSC) | C2: NR | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| Wuttke 2003/2006a/2006b | I1: NR | I1: 2.73 (0.52) (MRS) | I1: NR | I1: NR | I1: 0.25 (0.2) (CrossLaps, ng/mL) |
| C1: NR | C1: 2.83 (0.51) (MRS) | C1: NR | C1: NR | C1: 0.24 (0.12) (CrossLaps, ng/mL) | |
| C2: NR | C2: 3.23 (1.0) (MRS) | C2: NR | C2: NR | C2: 0.25 (1.6) (CrossLaps, ng/mL) | |
| Total: NR | Total: NR | Total: NR | Total: NR | Total: NR | |
| BMD: bone mineral density; C: control; GCS: Greene Climacteric Scale; I: intervention; KI: Kupperman Index; MDP: medroxyprogesterone; mKI: Modified Kupperman index; MRS: Menopause Rating Scale; NR: not recorded; NSC: number of sexual complaints; PGWBI: Psychological General Wellbeing Index; WMSS: = Wiklund Menopause Symptom Score. | |||||
| Study | Interventions | Participants who died (n) | Adverse events (n, %) | Serious adverse events (n, %) |
| Amsterdam 2009 | I1: black cohosh | I1: NR | I1: 14 (93%) | I1: 1 (7%) |
| C1: placebo | C1: NR | C1: 8 (62%) | C1: 0 (0%) | |
| Total: NR | Total: 22 (78%) | Total: 1 (4%) | ||
| Bai 2007 | I1: black cohosh | I1: 0 | I1: 139 (‐) | I1: 0 (0%) |
| C1: tibolone | C1: 0 | C1: 253 (‐) | C1: 1 (0.8%) | |
| Total: 0 | Total: 392 (‐) | Total: 1 (0.4%) | ||
| Bebenek 2010 | I1: exercise + black cohosh | I1: NR | I1: 0 (0%) | I1: NR |
| I2: exercise only | I2: NR | I2: 0 (0%) | I2: NR | |
| C1: wellness control | C1: NR | C1: 0 (0%) | C1: NR | |
| Total: NR | Total: 1 (1%) | Total: NR | ||
| Carlisle 2008 | I1: black cohosh + calcium and vitamin D supplement | I1: NR | I1: NR | I1: NR |
| C1: placebo + calcium and vitamin D supplement | C1: NR | C1: NR | C1: NR | |
| Frei‐Kleiner 2005 | I1: black cohosh | I1: NR | I1: 17 (20%) | I1: NR |
| C1: placebo | C1: NR | C1: 10 (23%) | C1: NR | |
| Total: NR | Total: 27 (21%) | Total: NR | ||
| Geller 2009 | I1: black cohosh | I1: NR | I1: NR | I1: NR |
| I2: red clover | I2: NR | I2: NR | I2: NR | |
| I3: conjugated oestrogen + MDP | I3: NR | I3: NR | I3: NR | |
| C1: placebo | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | ||
| Jacobson 2001 | I1: black cohosh | I1: NR | I1: 10 (24%) | I1: 2 (5%) |
| C1: placebo | C1: NR | C1: 3 (7%) | C1: 1 (2%) | |
| Total: NR | Total: 13 (15%) | Total: 3 (4%) | ||
| Kronenberg 2009 | I1: black cohosh | I1: NR | I1: 19 (31%) | I1: 0 (0%) |
| C1: placebo | C1: NR | C1: 34 (50%) | C1: 0 (0%) | |
| Total: NR | Total: 53 (41%) | Total: 0 (0%) | ||
| Lehmann‐Willenbrock 1988 | I1: black cohosh | I1: NR | I1: NR | I1: NR |
| C1: oestriol | C1: NR | C1: NR | C1: NR | |
| C2: conjugated oestrogen | C2: NR | C2: NR | C2: NR | |
| C3: oestradiol/ norethisterone acetate | C3: NR | C3: NR | C3: NR | |
| Total: NR | Total: NR | Total: NR | ||
| Nappi 2005 | I1: black cohosh | I1: NR | I1: 0 (0%) | I1: NR |
| C1: oestradiol + dihydrogesterone | C1: NR | C1: 2 (6%) | C1: NR | |
| Total: NR | Total: 2 (3%) | Total: NR | ||
| Newton 2006 / Reed 2008 | I1: black cohosh | I1: NR | I1: 57 (NR) | I1: 0 (0%) |
| I2: multi‐botanical | I2: NR | I2: 44 (NR) | I2: 1 (1%) | |
| I3: mult‐ibotanical + dietary soy | I3: NR | I3: 57 (NR) | I3: 1 (1%) | |
| I4: conjugated oestrogen + MDP | I4: NR | I4: 41 (NR) | I4: 0 (0%) | |
| C1: placebo | C1: NR | C1: 67 (NR) | C1: 0 (0%) | |
| Total: NR | Total: 266 (NR) | Total: 2 (0.6%) | ||
| Oktem 2007 | I1: black cohosh | I1: NR | I1: 7 (18%) | I1: NR |
| C1: fluoxetine | C1: NR | C1: 13 (33%) | C1: NR | |
| Total: NR | Total: 20 (25%) | Total: NR | ||
| Osmers 2005 | I1: black cohosh | I1: NR | I1: 71 (33%) | I1: 0 (0%) |
| C1: placebo | C1: NR | C1: 67 (31%) | C1: 0 (0%) | |
| Total: NR | Total: 138 (45%) | Total: 0 (0%) | ||
| Pockaj 2006 | I1: black cohosh | I1: NR | I1: NR | I1: NR |
| C1: placebo | C1: NR | C1: NR | C1: NR | |
| Total: NR | Total: NR | Total: NR | ||
| Stoll 1987 | I1: black cohosh | I1: NR | I1: NR | I1: NR |
| C1: oestrogen | C1: NR | C1: NR | C1: NR | |
| C2: placebo | C2: NR | C2: NR | C2: NR | |
| Total: NR | Total: NR | Total: NR | ||
| Wuttke 2003/2006a/2006b | I1: black cohosh | I1: NR | I1: 6 (15%) | I1: 0 (0%) |
| C1: conjugated oestrogens | C1: NR | C1: 8 (18%) | C1: 0 (0%) | |
| C2: placebo | C2: NR | C2: 6 (15%) | C2: 0 (0%) | |
| Total: NR | Total: 20 (32%) | Total: 0 (0%) | ||
| C: control; I: intervention; NR: not recorded. | ||||
| Study | Interventions | Left study because of adverse events (n, %) | Hospitalised (n, %) | Symptoms reported (n, %) | Notes |
| Amsterdam 2009 | I1: black cohosh | I1: 1 (7%) | I1: NR | I1: light headedness (2, 15%), difficulty falling asleep (2, 15%), dry mouth (1, 8%), diaphoresis (1, 8%), pain (1, 8%), oedema, GI bloating (1, 8%), diarrhoea (1, 8%), abdominal cramping (1, 8%), vaginal bleeding (1, 8%), mid‐night wakening (1, 8%), anxiety (1, 8%). | |
| C1: placebo | C1: 0 (0%) | C1: NR | C1: menstrual flow (2, 15.4%), irritability (1, 8%), listlessness (1, 8%), flu symptoms (1, 8%), breast tenderness (1, 8%), constipation (1, 8%), vaginal spotting (1, 8%). | ||
| Total: 1 (4%) | Total: NR | ||||
| Bai 2007 | I1: black cohosh | I1: 5 (6%) | I1: NR | I1: breast pain/enlargement (32, 21%), abdominal pain (12, 10%), vaginal bleeding (6, 5%), vaginal spotting (11, 7%), oedema (7, 5%), leucorrhoea (7, 6%) | |
| C1: tibolone | C1: 9 (7%) | C1: NR | C1: breast pain/enlargement (48, 35%), vaginal bleeding (40, 23%), abdominal pain (30, 24%), leucorrhoea (27, 18%), vaginal spotting (21, 13%), oedema (17, 12%) | ||
| Total: 14 (6%) | Total: NR | ||||
| Bebenek 2010 | I1: exercise + black cohosh | I1: NR | I1: NR | I1: NR | |
| I2: exercise only | I2: NR | I2: NR | I2: NR | ||
| C1: wellness control | C1: NR | C1: NR | C1: NR | ||
| Total: NR | Total: NR | ||||
| Carlisle 2008 | I1: black cohosh + calcium and vitamin D supplement | I1: NR | I1: NR | I1: NR | |
| C1: placebo + calcium and vitamin D supplement | C1: NR | C1: NR | C1: NR | ||
| Frei‐Kleiner 2005 | I1: black cohosh | I1: NR | I1: NR | I1: NR | |
| C1: placebo | C1: NR | C1: NR | C1: NR | ||
| Total: NR | Total: NR | ||||
| Geller 2009 | I1: black cohosh | I1: 0 (0%) | I1: NR | I1: NR | |
| I2: red clover | I2: 0 (0%) | I2: NR | I2: NR | ||
| I3: conjugated oestrogen + MDP | I3: 1 (4%) | I3: NR | I3: NR | ||
| C1: placebo | C1: 0 (0%) | C1: NR | C1: NR | ||
| Total: | Total: NR | ||||
| Jacobson 2001 | I1: black cohosh | I1: 3 (7%) | I1: NR | I1: hysterectomy (1, 2%), breast cancer recurrence (1, 2%), constipation (1, 2%), arrhythmia (1, 2%), weight gain (1, 2%), endometrial hyperplasia (1, 2%), dilatation and curettage (1, 2%), cramping (1, 2%), indigestion (1, 2%), vaginal bleeding (1, 2%) | The majority of participants were also taking tamoxifen |
| C1: placebo | C1: 1 (2%) | C1: NR | C1: appendectomy (1, 2%), swollen finger (1, 2%), abdominal rash (1, 2%) | ||
| Total: 4 (5%) | Total: NR | ||||
| Kronenberg 2009 | I1: black cohosh | I1: NR | I1: NR | I1: upper respiratory infection (5, 8%), skin complaints (4, 7%), vaginal bleeding (4, 7%), vaginitis (1, 2%), abnormal ECG (2, 3%), increased endometrial thickness (3, 5%) | |
| C1: placebo | C1: NR | C1: NR | C1: upper respiratory infection (12, 18%), skin complaints (11, 16%), vaginitis (4, 6%), abnormal ECG (3, 4%), elevated liver enzymes (2, 3%), vaginal bleeding (1, 2%), increased endometrial thickness (1, 2%) | ||
| Total: NR | Total: NR | ||||
| Lehmann‐Willenbrock 1988 | I1: black cohosh | I1: NR | I1: NR | ||
| C1: oestriol | C1: NR | C1: NR | C1: NR | ||
| C2: conjugated oestrogen | C2: NR | C2: NR | C2: NR | ||
| C3: oestradiol/ norethisterone acetate | C3: NR | C3: NR | C3: NR | ||
| Total: NR | Total: NR | ||||
| Nappi 2005 | I1: black cohosh | I1: NR | I1: NR | I1: NA | |
| C1: oestradiol + dihydrogesterone | C1: NR | C1: NR | C1: vaginal spotting (2, 6%) | ||
| Total: NR | Total: NR | ||||
| Newton 2006 / Reed 2008 | I1: black cohosh | I1: NR | I1: NR | I1: menstrual disorders (10, NR), GI upset (12, NR), headache (12, NR), fatigue (12, NR), myalgia / arthralgia (11, NR) | |
| I2: multi‐botanical | I2: NR | I2: NR | I2: menstrual disorders (8, NR), breast discomfort (1, NR), GI upset (11, NR), headache (8, NR), fatigue (7, NR), myalgia / arthralgia (9, NR) | ||
| I3: mult‐ibotanical + dietary soy | I3: NR | I3: NR | I3: menstrual disorders (14, NR), breast discomfort (2, NR), GI upset (8, NR), headache (12, NRI4: menstrual disorders (19, NR), breast discomfort (5, NR), GI upset (4, NR), headache (6, NR), fatigue (6, NR), myalgia / arthralgia (1, NR)), fatigue (12, NR), myalgia / arthralgia (9, NR) | ||
| I4: conjugated oestrogen + MDP | I4: NR | I4: NR | I4: menstrual disorders (19, NR), breast discomfort (5, NR), GI upset (4, NR), headache (6, NR), fatigue (6, NR), myalgia / arthralgia (1, NR) | ||
| C1: placebo | C1: NR | C1: NR | C1: menstrual disorders (17, NR), headache (16, NR), GI upset (13, NR), myalgia / arthralgia (10, NR), fatigue (8, NR), breast discomfort (3, NR) | ||
| Total: NR | Total: NR | ||||
| Oktem 2007 | I1: black cohosh | I1: NR | I1: NR | I1: dyspepsia (2, 5%), constipation (2, 5%), tiredness (1, 3%), skin allergy (1, 3%), irritability (1, 3%) | |
| C1: fluoxetine | C1: NR | C1: NR | C1: dyspepsia (1, 3%), constipation (1, 3%), sleep disturbance (3, 8%), dry mouth (2, 5%), tiredness (2, 5%), skin allergy (2, 5%), irritability (1, 3%), headache (1, 3%) | ||
| Total: NR | Total: NR | ||||
| Osmers 2005 | I1: black cohosh | I1: 7 (5%) | I1: NR | I1: musculoskeletal disorder (15, 10%) infection (13, 9%), GI disorder (8, 5%), nervous system disorder (4, 3%), reproductive / breast disorder (4, 3%), skin disorder (3, 2%), psychiatric disorder (2, 1%), tachycardia (2, 1%), metabolic / nutrition disorder (2, 1%), blood disorder (1, 1%), renal/urinary disorder (1, 1%), vascular disorder (1, 1%) | |
| C1: placebo | C1: 5 (3%) | C1: NR | C1: infection (19, 13%), musculoskeletal disorder (10, 7%) GI disorder (7, 5%), nervous system disorder (5, 3%), psychiatric disorder (5, 3%), reproductive / breast disorder (4, 3%), skin disorder (3, 2%), blood disorder (1, 1%), ear/labyrinth disorder (1, 1%), vascular disorder (1, 1%), respiratory disorder (1, 1%) | ||
| Total: 12 (4%) | Total: NR | ||||
| Pockaj 2006 | I1: black cohosh | I1: NR | I1: NR | I1: NR | |
| C1: placebo | C1: NR | C1: NR | C1: NR | ||
| Total: NR | Total: NR | ||||
| Stoll 1987 | I1: black cohosh | I1: 1 (3%) | I1: NR | I1: NR | |
| C1: oestrogen | C1: 2 (7%) | C1: NR | C1: NR | ||
| C2: placebo | C2: 2 (10%) | C2: NR | C2: NR | ||
| Total: 5 (6%) | Total: NR | ||||
| Wuttke 2003/2006a/2006b | I1: black cohosh | I1: 0 (0%) | I1: NR | I1: vaginal spotting (3, 15%), vertigo (1, 5%), hypertension (1, 5%), headache (1, 5%), bronchitis (1, 5%), rhinitis (1, 5%), viral infection (1, 5%) | |
| C1: conjugated oestrogens | C1: 0 (0%) | C1: NR | C1: bronchitis (2, 9%), toothache (2, 9%), vaginal spotting (1, 5%), diarrhoea (1, 5%), dermatitis (1, 5%), viral infection (1, 5%), elevated ALT (1, 5%) | ||
| C2: placebo | C2: 0 (0%) | C2: NR | C2: vaginal spotting (2, 10%), hyperglycaemia (1, 5%), arthritis (1, 5%), local skin reaction (1, 5%), rhinitis (1, 5%), back pain (1, 5%), breast pain (1, 5%) | ||
| Total: 0 (0%) | Total: NR | ||||
| C: control; GI: gastrointestinal; I: intervention; MDP: medroxyprogesterone; NR: not recorded. | |||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Vasomotor symptoms: daily hot flush frequency Show forest plot | 3 | 393 | Mean Difference (IV, Fixed, 95% CI) | 0.07 [‐0.43, 0.56] |
| 2 Vasomotor symptoms: weekly hot flush frequency Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 Vasomotor symptoms: hot flush intensity Show forest plot | 3 | 214 | Mean Difference (IV, Fixed, 95% CI) | 0.12 [‐0.06, 0.30] |
| 4 Vasomotor symptoms: night sweats Show forest plot | 1 | 164 | Mean Difference (IV, Fixed, 95% CI) | 0.27 [‐0.16, 0.70] |
| 4.1 Night sweat frequency per day | 1 | 164 | Mean Difference (IV, Fixed, 95% CI) | 0.27 [‐0.16, 0.70] |
| 5 Menopausal Symptom Score Show forest plot | 4 | 357 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐0.32, 0.11] |
| 5.1 Kupperman Index | 2 | 165 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.02 [‐0.34, 0.30] |
| 5.2 Greene Climacteric Scale | 1 | 28 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.43 [‐0.32, 1.18] |
| 5.3 Wiklund Menopause Symptom Score | 1 | 164 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.27 [‐0.58, 0.04] |
| 6 Adverse events Show forest plot | 2 | 344 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.82, 1.32] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Vasomotor symptoms: daily hot flush frequency Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Vasomotor symptoms: weekly hot flush frequency Show forest plot | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 26.42 [18.59, 34.25] |
| 3 Vasomotor symptoms: hot flush intensity Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4 Vasomotor symptoms: night sweats Show forest plot | 1 | 112 | Mean Difference (IV, Fixed, 95% CI) | 0.93 [0.47, 1.39] |
| 4.1 Night sweat frequency per day | 1 | 112 | Mean Difference (IV, Fixed, 95% CI) | 0.93 [0.47, 1.39] |
| 5 Menopausal Symptom Score Show forest plot | 5 | 468 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.32 [0.13, 0.51] |
| 5.1 Kupperman Index | 3 | 312 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.20 [‐0.02, 0.43] |
| 5.2 Greene Climacteric Scale | 1 | 44 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.25 [‐0.37, 0.87] |
| 5.3 Wiklund Menopause Symptom Score | 1 | 112 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.77 [0.35, 1.19] |
| 6 Adverse events Show forest plot | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.21, 3.24] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Vasomotor symptoms: hot flush frequency Show forest plot | 1 | 49 | Mean Difference (IV, Fixed, 95% CI) | 9.38 [‐1.04, 19.80] |
| 2 Vasomotor symptoms: hot flush intensity Show forest plot | 1 | 50 | Mean Difference (IV, Fixed, 95% CI) | 0.42 [‐0.08, 0.92] |
| 3 Menopausal score Show forest plot | 1 | 51 | Mean Difference (IV, Fixed, 95% CI) | ‐1.28 [‐5.48, 2.92] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Vasomotor symptoms: night sweats Show forest plot | 1 | 80 | Mean Difference (IV, Fixed, 95% CI) | ‐85.0 [‐132.50, ‐37.50] |
| 1.1 Night sweat score per month | 1 | 80 | Mean Difference (IV, Fixed, 95% CI) | ‐85.0 [‐132.50, ‐37.50] |
| 2 Menopausal score Show forest plot | 1 | 80 | Mean Difference (IV, Fixed, 95% CI) | ‐5.5 [‐8.86, ‐2.14] |
| 2.1 Kupperman Index | 1 | 80 | Mean Difference (IV, Fixed, 95% CI) | ‐5.5 [‐8.86, ‐2.14] |