استفاده از پلاگ (plug) در مهار بیاختیاری مدفوع
چکیده
پیشینه
بیاختیاری مدفوع (faecal incontinence)، یک اختلال ناراحتکننده با انگ اجتماعی زیاد است. همه افراد مبتلا به بیاختیاری مدفوع را نمیتوان با درمان محافظهکارانه یا جراحی درمان کرد و آنها ممکن است نیاز به استفاده از محصولات مهارکننده، مانند پلاگهای آنال (anal plug) داشته باشند.
اهداف
ارزیابی عملکرد انواع مختلف پلاگهای آنال در مهار بیاختیاری مدفوع.
روشهای جستوجو
پایگاه ثبت تخصصی گروه بیاختیاری در کاکرین را جستوجو کردیم، که حاوی کارآزماییهای شناسایی شده از پایگاه مرکزی ثبت کارآزماییهای کنترل شده کاکرین (CENTRAL)؛ MEاDLINE؛ MEDLINE In‐Process؛ ClinicalTrials.gov؛ ICTRP سازمان جهانی بهداشت (WHO) بوده و جستوجوی دستی را نشریات و خلاصه مقالات کنفرانسها (جستوجو شده تا 26 می 2015) انجام دادیم. فهرست منابع کارآزماییهای شناساییشده جستوجو شدند و برای کارآزماییها، با تولیدکنندگان پلاگها تماس گرفته شد. هیچ محدودیتی در زبان مقاله یا محدودیتهای دیگر اعمال نشدند.
معیارهای انتخاب
انواع مطالعات: این مرور محدود شد به کارآزماییهای تصادفیسازی و شبه‐تصادفیسازی و کنترل شده (شامل کارآزماییهای متقاطع) از کاربرد پلاگهای آنال برای مدیریت بالینی بیاختیاری مدفوع.
انواع شرکتکنندگان: کودکان و بزرگسالان مبتلا به بیاختیاری مدفوع.
انواع مداخلات: هر نوعی از پلاگ آنال. مداخلات مقایسهای شامل عدم‐درمان، درمانهای محافظهکارانه (فیزیکی)، مداخلات تغذیهای، جراحی، استفاده از پد (pad) و دیگر انواع یا اندازههای پلاگ بودند.
گردآوری و تجزیهوتحلیل دادهها
دو نویسنده بهطور مستقل از هم کیفیت روششناسی کارآزماییهای وارد شده را ارزیابی و دادهها را استخراج کردند. برای شفافسازی در مورد مباحث روششناختی، با نویسندگان همه کارآزماییهای وارد شده تماس گرفته شد.
نتایج اصلی
چهار مطالعه با مجموع 136 شرکتکننده وارد شدند. دو مطالعه، استفاده از پلاگها را در برابر عدم استفاده از آنها، یک مطالعه دو اندازه را از یک برند پلاگ، و یک مطالعه دو برند پلاگ را مقایسه کردند. در همه مطالعات وارد شده، تعداد قابلتوجهی از بیماران مطالعه را ترک کردند (در مجموع 48 نفر (35%) پیش از پایان مطالعه، به دلایل مختلف خارج شدند). بنابراین، دادههای ارائه شده در معرض سوگیری (bias) بالقوه هستند. با این حال، «شبه‐اختیار در دفع مدفوع (pseudo‐continence)»، در برخی از افرادی که به استفاده از پلاگها ادامه دادند، حداقل در کوتاه‐مدت، حاصل شد. در یک مقایسه میان دو نوع مختلف از پلاگ، خارج شدن پلاگ کمتر گزارش شد و رضایت کلی از پلاگهای پلیاورتان (polyurethane) نسبت به پلاگهای پلیوینیل‐الکل (polyvinyl‐alcohol) بیشتر بود.
نتیجهگیریهای نویسندگان
دادههای موجود محدود و ناقص بوده و همه پیامدهای از پیش مشخص شده، قابل ارزیابی نبودند. بنابراین، فقط نتیجهگیریهای آزمایشی امکانپذیر است. دادههای موجود نشان میدهند که تحمل پلاگهای آنال ممکن است دشوار باشد؛ با این حال، اگر تحمل شوند، میتوانند در پیشگیری از بیاختیاری مدفوع مفید باشند. بنابراین، پلاگها میتوانند در یک گروه منتخب از افراد به عنوان جایگزینی برای دیگر اشکال مدیریت بالینی بیاختیاری مدفوع یا به عنوان یک گزینه درمان کمکی مفید باشند. پلاگها در طرحها و اندازههای مختلف وجود دارند؛ این مرور نشان داد که انتخاب نوع پلاگ میتواند بر عملکرد آن تاثیرگذار باشد.
PICO
خلاصه به زبان ساده
استفاده از پلاگها در پیشگیری از دفع ناخواسته مدفوع در بیماران مبتلا به بیاختیاری مدفوع
بیاختیاری مدفوع، به عبور غیر‐ارادی مواد دفعی از کانال مقعدی گفته شده و یک مشکل شایع و خجالتآور به حساب میآید. درمانهای مختلفی، از جمله اقدامات مرتبط با رژیم غذایی، داروها، فیزیوتراپی تخصصی کف لگن، و جراحی برای این منظور وجود دارند. با این حال، همه بیماران قابل درمان نیستند. استفاده از پلاگهای آنال (anal plug) ممکن است به این بیماران کمک کنند. انواع مختلفی از پلاگهای آنال شناخته شدهاند، که هدف همگی آنها، ممانعت از دفع ناخواسته مدفوع، به منظور کنترل بیاختیاری مدفوع است. هدف این مرور، ارزیابی عملکرد انواع مختلف پلاگهای آنال برای مهار بیاختیاری مدفوع بود.
چهار مطالعه با مجموع 136 شرکتکننده وارد شدند. دو مطالعه، استفاده از پلاگ را در برابر عدم استفاده از آن مقایسه کردند. در شش (38%) شرکتکننده که به استفاده از پلاگها، حداقل در کوتاه‐مدت ادامه دادند، از دست رفتن غیر‐ارادی مدفوع بهطور تاثیرگذاری متوقف شد (شبه‐اختیار در دفع مدفوع (pseudo‐continence)). یک مطالعه، دو اندازه را از یک برند پلاگ مقایسه کرد؛ با توجه به زیاد بودن میزان ترک این مطالعه و ناقص بودن دادهها، هیچ نتیجهای در مورد این مقایسه در دسترس قرار ندارد. در یک مطالعه، مقایسه دو برند مختلف پلاگ انجام شد. از دست رفتن پلاگ توسط 7 بیمار (30%) با یک پلاگ پلیاورتان (polyurethane; PU) و توسط 15 بیمار (65%) با پلاگ پلیوینیل‐الکل (polyvinyl‐alcohol; PVA) گزارش شد. رضایت کلی، که به صورت نظر بیماران مبنی بر این که پلاگ خوب تا خیلی خوب است تعریف شد، برای دریچه PU؛ (N=17) نسبت به دریچه PVA؛ (N=8) بیشتر گزارش شد.
در همه مطالعات وارد شده، میزان قابلتوجهی از بیماران مطالعه را ترک کردند؛ در مجموع 48 شرکتکننده (35%) پیش از پایان مطالعه، به دلایل مختلف از مطالعه خارج شدند. بنابراین، دادههای ارائه شده در معرض سوگیری (bias) بالقوه بوده و فقط نتیجهگیریهای آزمایشی امکانپذیر است. دادههای موجود نشان میدهند که تحمل پلاگهای آنال ممکن است دشوار باشد؛ با این حال، اگر تحمل شوند، میتوانند در پیشگیری از بیاختیاری مدفوع مفید باشند. بنابراین، پلاگها میتوانند در یک گروه منتخب از افراد به عنوان جایگزینی برای دیگر اشکال مدیریت بالینی بیاختیاری مدفوع یا به عنوان یک گزینه درمان کمکی مفید باشند. پلاگها در طرحها و اندازههای مختلف وجود دارند؛ این مرور نشان داد که انتخاب نوع پلاگ میتواند بر عملکرد آن تاثیرگذار باشد.
Authors' conclusions
Background
Faecal incontinence is defined as the involuntary passage of faecal material through the anal canal (Soffer 2000). The reported prevalence values range from 1.4% in the general population (defined as soiling of underwear, outer clothing, furnishing, or bedding several times a month or more often) (Perry 2002); to 46% in institutionalised elderly people (defined as at least one incontinent episode per week) (Borrie 1992). It is possible that the real prevalence is even higher than reported as faecal incontinence is associated with high social stigma and people are reluctant to seek help for this disorder because of embarrassment (Jorge 1993; Mavrantonis 1998).
The causes for faecal incontinence are diverse. In most cases a combination of factors leads to incontinence. Frequently cited causes are injuries during childbirth and prior anorectal surgery (Kamm 1998; Toglia 1998). But many other causes have been described, including loose stool, intestinal hurry, and neurological disease or injury.
Treatments available range from conservative therapy, such as dietary recommendations and anti‐diarrhoeal medication, to surgical treatment by either sphincter repair, dynamic graciloplasty, artificial anal sphincter implantation, or sacral nerve stimulation (Jorge 1993; Matzel 2003). Nowadays, the most common treatments are pelvic floor muscle training ‐ with or without biofeedback ‐ and anterior anal sphincter repair (Kamm 1998). The reported success rates with these forms of treatment vary, but it is recognized that none of the treatments will resolve the incontinence problems in all patients. Cochrane reviews are available that cover some of these treatments: these include drug treatment (Omar 2013); electrical stimulation, sphincter exercises and biofeedback (Hosker 2007; Norton 2012); sacral nerve stimulation (Mowatt 2007); surgery (Brown 2013); and management of faecal incontinence and constipation in adults with central neurological diseases (Coggrave 2014).
Where incontinence persists despite active treatment there may be no option other than containment. Brazzelli 2002 have reviewed the use of pads for the containment of anal and urinary incontinence. There is also a Cochrane review covering this topic (Fader 2008). Problems when using pads for faecal incontinence are that the odour from the anal leakage is difficult to control and extensive use of pads can result in skin condition problems. A possible way to avoid these problems is the use of an anal plug (sometimes called 'tampon'): a device specially developed for containing faecal incontinence.
Different types of anal plugs are known, all aiming to block the loss of stool. They were first used in patients suffering from faecal incontinence due to major neurological problems, such as caused by spina bifida (Norton 2001a). Nowadays, plugs are also sometimes used by patients with faecal incontinence who do not have an underlying neurological condition.
At this point it is unclear how effective anal plugs are in controlling stool loss in patients with faecal incontinence (with or without neurological impairments) and whether some types of anal plugs are more effective than others. This review aims to bring together in a systematic way the best available evidence to address these issues.
Objectives
To assess the performance of different types of anal plugs for containment of faecal incontinence.
The following comparisons were considered:
1. anal plugs versus no plugs;
2. one type of anal plug versus another;
3. anal plugs versus any other treatment.
Methods
Criteria for considering studies for this review
Types of studies
This review was limited to randomised and quasi‐randomised controlled trials (including crossovers) of anal plug use for the management of faecal incontinence.
Types of participants
All patients (children and adults) with faecal incontinence.
Types of interventions
Studies investigating the relative performance of anal plugs. Potential comparison interventions include no treatment, conservative (physical) treatments, nutritional interventions, surgery, pads, and other types or sizes of plugs.
Types of outcome measures
1. Patient symptoms:
-
frequency of incontinence of stool or flatus (diary or self‐report);
-
degree of incontinence (e.g. stool weight);
-
incontinence score;
-
episodes of anal urgency.
2. Physical measures:
-
achievement of pseudo‐continence (continence only while wearing a plug);
-
wearing time and frequency of use;
-
leakage rate;
-
odour control.
3. Patient satisfaction:
-
satisfaction with incontinence‐controlling capacity;
-
tolerability of plug (including persistence in using the plug);
-
comfort of plug in use;
-
comfort of plug removal/ease of removal;
-
feeling of cleanness.
4. Health status measures:
-
impact of incontinence on health status, social life, and quality of life.
5. Costs
6. Other outcomes:
-
non pre‐specified outcomes later judged important when performing the review.
Search methods for identification of studies
Electronic searches
We formulated a comprehensive and exhaustive search strategy in an attempt to identify all relevant studies regardless of language or publication status (published, unpublished, in press, and in progress).
This review has drawn on the search strategy developed for the Cochrane Incontinence Group. Relevant trials were identified from the Group's Specialised Register of Trials, which is described under the Group's module in the Cochrane Library. The Register contains trials identified from the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, and MEDLINE In‐Process, ClinicalTrials.gov, WHO ICTRP and handsearching of journals and conference proceedings.
The Incontinence Group Specialised Register was searched using the Group's own keyword system. The search terms used are given in Appendix 1. The date of the most recent search of the register for this review: 26 May 2015.
For the first published version of this review the authors performed additional searches which are detailed in Appendix 2.
Searching other resources
Additionally all reference lists of identified trials were searched. We contacted two manufacturers that marketed plugs to ask for details of unpublished or ongoing trials. We did not impose any language or other limitations on the searches.
Data collection and analysis
Study selection
Two reviewers assessed the title and abstract of references identified by the search strategy. The full reports of all potentially eligible randomised and quasi‐randomised controlled trials were then obtained for further assessment of eligibility. Any disagreements were resolved by discussion. Studies were only included if they were randomised or quasi‐randomised trials.
Methodological quality assessment
The quality of eligible trials was assessed independently by the two reviewers using a pre‐defined quality assessment form (see details under the Incontinence Group in The Cochrane Library). Reviewers were not blind to author, institution or journal. Disagreements between reviewers were resolved by discussion. Studies were not excluded from the review on the basis of methodological quality.
Data abstraction
Relevant data regarding inclusion criteria (study design, participants, interventions and outcomes), quality criteria (randomisation and blinding), and results were extracted independently by the two reviewers using a data abstraction form adapted from the form designed by the Dutch Cochrane Centre. In cases where insufficient data were reported authors were contacted for further information (such as method of randomisation, statistical methods).
Data analysis
Data were analysed using the MetaView statistical software in Review Manager 4.2.5 (RevMan 2003). For dichotomous variables, risk ratios (RR) and 95% confidence intervals (CI) were derived for each outcome. It was not possible to combine data from the included studies as outcomes, and type of comparisons varied. We instead present a qualitative synthesis of the results of the primary studies.
Results
Description of studies
The search strategy identified 13 potentially eligible studies. When full citations were obtained nine studies could not be included: seven were patient series, one was a case study, and one study was excluded as we understood from the author that this paper did not report a randomised trial.
Thus in total, four studies met our inclusion criteria (Bond 2005; Norton 2001b; Pfrommer 2000; Van Winckel 2005). Two of these studies were derived from the Specialised Trials Register of the incontinence group (Bond 2005; Pfrommer 2000). One was derived by the additional searches performed by one of the authors (Norton 2001b). The final trial was obtained by contacting an anal plug manufacturer (Van Winckel 2005).
The reports of Bond 2005 and Van Winckel 2005, two of the included trials, had not been published at the time of finishing the original version of the review (Deutekom 2005) . We received permission from the authors to use their data in our review. For the 2010 update of the review (2010, Issue 1 search updated but no new citation) one of the trials had been published but did not add any extra data to that provided by the author for the original version of this review (Van Winckel 2005). For the 2012 update the published journal article for Bond 2005 was available but again this did not add any extra data to that provided by the author for the original version of this review. The flow of literature through the assessment process is shown in Figure 1.
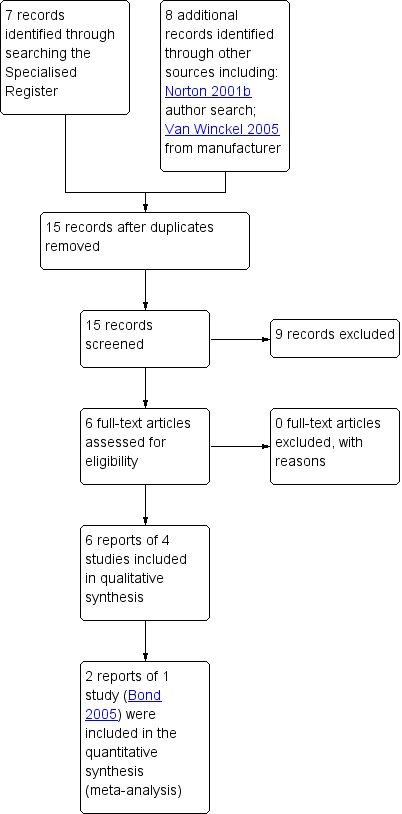
PRISMA study flow diagram.
The total number of participants across the trials was 136. For a detailed description of individual studies please refer to the table of Characteristics of included studies.
Design
Three studies used a randomised crossover designs (Norton 2001b; Pfrommer 2000; Van Winckel 2005); and one was a parallel group randomised controlled trial (Bond 2005).
Sample size
Sample sizes were 16 (Van Winckel 2005); 34 (Norton 2001b); 38 (Pfrommer 2000); and 48 (Bond 2005).
Diagnosis
All studies included patients with faecal incontinence.
One study included patients who were partially continent or incontinent following imperforate anus repair (Pfrommer 2000). One study included children who had faecal incontinence due to a high type imperforate anus and children with spina bifida (Van Winckel 2005). One study included children (older than 4 years) and young adults (16 to 45 years) who were incontinent due to congenital or acquired neurogenic disorders (Bond 2005); and one included adult outpatients after failure of previous treatment (Norton 2001b).
Location/setting
One trial was carried out in Scotland and participants were identified primarily by hospital specialists from Paediatric Surgery or Gastroenterology in Aberdeen, Inverness and Glasgow (Bond 2005). One trial was carried out in Germany in a hospital for Paediatric Surgery (Pfrommer 2000); one in Belgium at the departments of Paediatrics and Urology in an academic medical centre (Van Winckel 2005); and one in England in a specialist colorectal hospital where patients received an individual instruction with a nurse specialist (Norton 2001b).
Interventions
The four identified trials made the following comparisons:
1. anal plug versus no plug (Bond 2005; Van Winckel 2005);
2‐I. one type of anal plug versus another: comparison of two sizes of the same type of plug (polyurethane anal plug) (Norton 2001b);
2‐II. one type of anal plug versus another: comparison of two different types of plugs (polyurethane anal plug versus polyvinyl‐alcohol plug) (Pfrommer 2000).
Length of treatment
Three trials lasted between four and six weeks (Norton 2001b; Pfrommer 2000; Van Winckel 2005). One trial lasted one year (Bond 2005).
Outcomes
Common reported outcomes were frequency of incontinent episodes (effectiveness of treatment), satisfaction and tolerance.
Risk of bias in included studies
Potential for selection bias at trial entry
In all crossover trials the order of the intervention was randomised (Norton 2001b; Pfrommer 2000; Van Winckel 2005). In none of these studies were details provided concerning the methods used for randomisation and concealment. In the parallel group randomised controlled trial the participants were randomly allocated to the intervention or control group (Bond 2005). Randomisation was performed using pre‐determined codes.
Potential for bias at time of treatment or outcome assessment
As the studies included in this review investigated anal plugs it is difficult to blind patients and staff to intervention. In two studies the use of plugs was compared to a control intervention in which patients did not receive any treatment (Bond 2005; Van Winckel 2005): blinding was impossible. In the remaining two randomised crossover studies two types or two sizes of plugs were compared (Norton 2001b; Pfrommer 2000). Neither study reported any blinding.
Potential for bias in trial analysis
In three studies the number and reasons for patient dropouts were clearly described (Norton 2001b; Pfrommer 2000; Van Winckel 2005).
-
In one study 23 of the 34 (68%) patients did not start or dropped out (Norton 2001b). Reasons why patients dropped out were: they disliked the idea and did not start the study (n = 4); they failed to attend the clinic (n = 2); they dropped out because of discomfort after trying the first plug (n = 8); and they dropped out after trying one size of plug, refusing to try the second one (n = 9).
-
In one study 15 of the 38 patients (39%) dropped out before the end of the study (Pfrommer 2000). Two patients liked the first tested product and ended participation; six patients found the smallest available size of the products (tested first) to be too big; two patients reported discomfort; one patient constantly lost one of the products; and four patients failed to complete the protocol for non‐plug related reasons.
-
In one study 4 of the 16 patients dropped out (25%) (Van Winckel 2005). Reported reasons for this were discomfort and pain (n = 2); and losing the plug (n = 2).
-
In one study 6 patients dropped out from the 48 included, but did not report any reasons for this (Bond 2005). All those who dropped out were in the intervention group.
In only one of the studies was an intention‐to‐treat analysis performed (Van Winckel 2005). In none of the trials was there a description whether data analysis was performed blindly.
Effects of interventions
Three randomised crossover trials and one randomised controlled trial were included in this review. As the reported outcome measures varied amongst trials, a quantitative synthesis of the results was not feasible. In the summary tables 'N' denotes the total number of patients and 'n' denotes the number of patients who had the outcome. Unfortunately the data from the randomised crossover studies were not presented in a form suitable for inclusion in the formal analysis.
Comparison 1: anal plugs versus no plugs
Two of the included studies compared the use of anal plugs with standard treatment (Bond 2005; Van Winckel 2005). In both studies patients were allowed to choose their preferred size of plug. In both trials a choice could be made between small or larger Coloplast plugs.
Patient symptoms
Pseudo‐continence was reported in six out of 16 patients in the treatment period in the crossover study, and in none of the 16 during the control period (Analysis 1.7). Patients achieving pseudo‐continence were reported to show greater satisfaction with treatment during plug use (no further data provided by the author) than when not using a plug (Van Winckel 2005). Three of the 16 patients (two with anal atresia and one with spina bifida) continued using the plug after the study. Neither stool frequency nor stool consistency was affected by use of the plug (no further data provided by the author). In the parallel group trial, clinically derived condition‐specific measures (such as protection, rash/skin problems, and unpleasant odour) tended to favour the plugs group for all patients (adults and children) (Analysis 1.4), although no difference was statistically significant, confidence intervals were wide, and dropout rates were considerable (Bond 2005).
Patient satisfaction
In the randomised crossover trial four patients did not complete the treatment period due to discomfort and pain (n = 2; anal atresia) and losing of the plug (n = 2; spina bifida) (Van Winckel 2005). The plug was thus not tolerated in four out of 16 patients. All patients tolerated the control period (Analysis 1.8).
Health status measures
Bond 2005 reported data for adults on changes in general health (3/14 versus 0/5; risk ratio (RR) was 2.63 (95% confidence interval (CI) 0.16 to 43.63) (Analysis 1.1)); bodily pain (6/15 versus 3/5; (RR 0.67, 95% CI 0.26 to 1.72) (Analysis 1.2)); and various measures of well being (derived from SF‐36) (Analysis 1.3). Confidence intervals were all wide, reflecting the small numbers studied.
Costs
Little or no evidence was obtained that the plug led to significant reductions in the overall costs of care (Bond 2005).
No data were available for the other pre‐specified outcomes (see Table of comparisons).
Comparison 2‐I: one type of anal plug versus another (comparison of two sizes)
One study compared two sizes of a plug in a randomised crossover design (Norton 2001b). Due to the high dropout in this study and the incomplete data, no results concerning the comparison are available.
Comparison 2‐II: one type of anal plug versus another (comparison of two types)
One study compared two types of plugs in a randomised crossover design: polyurethane anal plug (Conveen, Coloplast) (PU plug) versus EFF‐EFF polyvinyl‐alcohol plug (Med. SSE‐System) (PVA plug) (Pfrommer 2000).
Patient symptoms
The absence of soiling episodes was reported in 15 (65%) patients when using the PU plug and by 14 (60%) patients when using the PVA plug (Analysis 2.1)
Patient satisfaction
Feelings of security were reported by 16 patients (69%) while using the PU plug and by 10 patients (43%) when using the PVA plug (Analysis 2.2). Loss of plug was reported by 7 patients (30%) with the PU plug and by 15 patient 65% with the PVA plug (Analysis 2.3). Inconvenience was reported by 9 patients (39%) when using the PU plug and by 16 (69%) patients when using the PVA plug (Analysis 2.4). Overall satisfaction, defined as patients' opinion that the plug was good to very good, was reported more often for the PU plug (n = 17) than for the PVA plug (n = 8) (Analysis 2.5). 14 patients preferred the PU plug, 5 patients preferred the PVA plug, and 4 patients reported no preference.
No data were available for the other pre‐specified outcomes.
Comparison 3: anal plug versus any other treatment
No eligible trials were found.
Discussion
This review of anal plugs for the containment of faecal incontinence was limited by the small quantity of eligible studies and participants and the fact that combining data was either impossible or inappropriate. Only one parallel group randomised controlled trial that compared the use of plugs with no intervention could be included (Bond 2005). The other three included trials were randomised crossover studies. These also reported dropouts and are further limited by not allowing longer‐term acceptability rates to be assessed. One such trial compared plug use versus no intervention (Van Winckel 2005). The other two studies compared two types of plugs. Two sizes of the same plug were investigated in one study (Norton 2001b); and two brands of plugs were compared in the other study (Pfrommer 2000).
Reported outcome measures varied. Two studies reported patient symptoms (Pfrommer 2000; Van Winckel 2005); one study reported physical measures (Bond 2005); two studies reported patient satisfaction (Pfrommer 2000; Van Winckel 2005); and one study reported the outcome of health status measures and costs (Bond 2005). There are other variables that may influence the successful wearing of anal plugs, such as leakage rate, skin problems, odour, wearing time, frequency of use, age, social environment and patient characteristics. Unfortunately there were insufficient data in the included studies to take these factors into consideration in our review.
Participant groups also varied between the studies. The participants in two studies suffered from faecal incontinence due to congenital diseases (Van Winckel 2005; Pfrommer 2000). These patients are a minority in the total population of patients with faecal incontinence.
Due to the diversity in comparisons, outcome measures, and type of participants, we were not able to perform a quantitative synthesis of the data but described the data per comparison. This does not allow us to state firm and precise conclusions and emphasizes the need for further research.
The methodological quality of the four included trials was generally poor. Inclusion and exclusion criteria were given in two studies (Bond 2005; Van Winckel 2005); and one study described only inclusion criteria (Pfrommer 2000). However, none of the studies provided outcomes related to either severity or frequency of faecal incontinence.
Concealment of allocation was performed in only one study (Bond 2005). Due to the nature of the intervention of the studies it appeared to be impossible to blind the patients or outcome assessors. Only one trial reported that the researcher who was responsible for the inclusion of patients was securely blinded to the randomisation process (Bond 2005).
Incompleteness of follow‐up occurred in most trials, caused by selective withdrawal of patients, to a large extent related to intolerance or dissatisfaction with the intervention. An intention‐to‐treat analysis could be performed in only one trial (Van Winckel 2005). In the study comparing two sizes of anal plugs the high rate of dropout meant that it was not possible to extract data (Norton 2001b). However, it did not appear that there was a difference in dropout rates between studies or patient groups. Most trials studied small patient groups, limiting the power to detect differences between groups.
One trial excluded data from patients who reported that they did not have difficulties with these particular outcomes before or after the intervention (Bond 2005). Thus, Bond 2005 only reported comparisons between the intervention group and control group when the outcome troubled the patient and it was reported as the same, improved or worse. The results presented in this review included data from all the patients. Consequently, our results differ from those published by the author.

PRISMA study flow diagram.

Comparison 1 Anal plugs versus no plugs, Outcome 1 General health improved ‐ adults.

Comparison 1 Anal plugs versus no plugs, Outcome 2 Bodily pain improved ‐ adults.

Comparison 1 Anal plugs versus no plugs, Outcome 3 Well being (adults) improved.
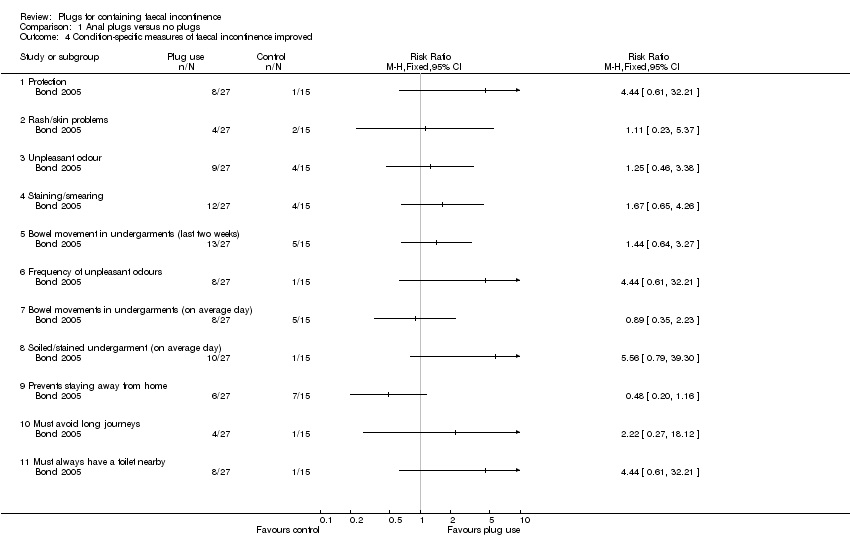
Comparison 1 Anal plugs versus no plugs, Outcome 4 Condition‐specific measures of faecal incontinence improved.
| Study | |
| Bond 2005 | No differences were observed between control and intervention group |
Comparison 1 Anal plugs versus no plugs, Outcome 5 Stool frequency.
| Study | |
| Bond 2005 | Little or no evidence that the plug led to significant reductions in the overall costs of care |
Comparison 1 Anal plugs versus no plugs, Outcome 6 Costs.
| Study | Anal plug period | Control period |
| Van Winckel 2005 | 6/12 | 0/12 |
Comparison 1 Anal plugs versus no plugs, Outcome 7 Achievement of pseudo‐continence.
| Study | Anal plug period | Control period |
| Van Winckel 2005 | 4/16 | 0/16 |
Comparison 1 Anal plugs versus no plugs, Outcome 8 Intolerance of intervention.
| Study | PU plug | PVA plug |
| Pfrommer 2000 | 15/23 | 14/23 |
Comparison 2 One type of anal plug versus another type, Outcome 1 Plug effectiveness: number of people with no soiling.
| Study | PU plug | PVA plug |
| Pfrommer 2000 | 16/23 | 10/23 |
Comparison 2 One type of anal plug versus another type, Outcome 2 Feeling of security.
| Study | PU plug | PVA plug |
| Pfrommer 2000 | 7/23 | 15/23 |
Comparison 2 One type of anal plug versus another type, Outcome 3 Loss of plug.
| Study | PU plug | PVA plug |
| Pfrommer 2000 | 9/23 | 16/23 |
Comparison 2 One type of anal plug versus another type, Outcome 4 Inconvenience.
| Study | PU plug | PVA plug |
| Pfrommer 2000 | 17/23 | 8/23 |
Comparison 2 One type of anal plug versus another type, Outcome 5 Overall satisfaction.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 General health improved ‐ adults Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2 Bodily pain improved ‐ adults Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3 Well being (adults) improved Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.1 Full of life | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Very nervous | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.3 Down in the dumps | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.4 Calm and peaceful | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.5 Lot of energy | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.6 Downhearted and low | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.7 Feel worn out | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.8 Happy | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.9 Tired | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Condition‐specific measures of faecal incontinence improved Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.1 Protection | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Rash/skin problems | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 Unpleasant odour | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.4 Staining/smearing | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.5 Bowel movement in undergarments (last two weeks) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.6 Frequency of unpleasant odours | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.7 Bowel movements in undergarments (on average day) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.8 Soiled/stained undergarment (on average day) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.9 Prevents staying away from home | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.10 Must avoid long journeys | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.11 Must always have a toilet nearby | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Stool frequency Show forest plot | Other data | No numeric data | ||
| 6 Costs Show forest plot | Other data | No numeric data | ||
| 7 Achievement of pseudo‐continence Show forest plot | Other data | No numeric data | ||
| 8 Intolerance of intervention Show forest plot | Other data | No numeric data | ||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Plug effectiveness: number of people with no soiling Show forest plot | Other data | No numeric data | ||
| 2 Feeling of security Show forest plot | Other data | No numeric data | ||
| 3 Loss of plug Show forest plot | Other data | No numeric data | ||
| 4 Inconvenience Show forest plot | Other data | No numeric data | ||
| 5 Overall satisfaction Show forest plot | Other data | No numeric data | ||