Pemberian cecair dan makanan lebih awal berbanding dengan lewat untuk mengurangkan komplikasi selepas pembedahan abdominal ginekologikal major
Abstract
Background
This is an updated version of the original Cochrane review published in 2007. Traditionally, after major abdominal gynaecologic surgery postoperative oral intake is withheld until the return of bowel function. There has been concern that early oral intake would result in vomiting and severe paralytic ileus with subsequent aspiration pneumonia, wound dehiscence, and anastomotic leakage. However, evidence‐based clinical studies suggest that there may be benefits from early postoperative oral intake.
Objectives
To assess the effects of early versus delayed (traditional) initiation of oral intake of food and fluids after major abdominal gynaecologic surgery.
Search methods
We searched the Menstrual Disorders and Subfertility Group's Specialised Register, the Cochrane Central Register of Controlled Trials (CENTRAL), electronic databases (MEDLINE, EMBASE, CINAHL), and the citation lists of relevant publications. The most recent search was conducted 1 April 2014. We also searched a registry for ongoing trials (www.clinicaltrials.gov) on 13 May 2014.
Selection criteria
Randomised controlled trials (RCTs) were eligible that compared the effect of early versus delayed initiation of oral intake of food and fluids after major abdominal gynaecologic surgery. Early feeding was defined as oral intake of fluids or food within 24 hours post‐surgery regardless of the return of bowel function. Delayed feeding was defined as oral intake after 24 hours post‐surgery and only after signs of postoperative ileus resolution.
Data collection and analysis
Two review authors selected studies, assessed study quality and extracted the data. For dichotomous data, we calculated the risk ratio (RR) with a 95% confidence interval (CI). We examined continuous data using the mean difference (MD) and a 95% CI. We tested for heterogeneity between the results of different studies using a forest plot of the meta‐analysis, the statistical tests of homogeneity of 2 x 2 tables and the I² value. We assessed the quality of the evidence using GRADE methods.
Main results
Rates of developing postoperative ileus were comparable between study groups (RR 0.47, 95% CI 0.17 to 1.29, P = 0.14, 3 RCTs, 279 women, I² = 0%, moderate‐quality evidence). When we considered the rates of nausea or vomiting or both, there was no evidence of a difference between the study groups (RR 1.03, 95% CI 0.64 to 1.67, P = 0.90, 4 RCTs, 484 women, I² = 73%, moderate‐quality evidence). There was no evidence of a difference between the study groups in abdominal distension (RR 1.07, 95% CI 0.77 to 1.47, 2 RCTs, 301 women, I² = 0%) or a need for postoperative nasogastric tube placement (RR 0.48, 95% CI 0.13 to 1.80, 1 RCT, 195 women).
Early feeding was associated with shorter time to the presence of bowel sound (MD ‐0.32 days, 95% CI ‐0.61 to ‐0.03, P = 0.03, 2 RCTs, 338 women, I² = 52%, moderate‐quality evidence) and faster onset of flatus (MD ‐0.21 days, 95% CI ‐0.40 to ‐0.01, P = 0.04, 3 RCTs, 444 women, I² = 23%, moderate‐quality evidence). In addition, women in the early feeding group resumed a solid diet sooner (MD ‐1.47 days, 95% CI ‐2.26 to ‐0.68, P = 0.0003, 2 RCTs, 301 women, I² = 92%, moderate‐quality evidence). There was no evidence of a difference in time to the first passage of stool between the two study groups (MD ‐0.25 days, 95% CI ‐0.58 to 0.09, P = 0.15, 2 RCTs, 249 women, I² = 0%, moderate‐quality evidence). Hospital stay was shorter in the early feeding group (MD ‐0.92 days, 95% CI ‐1.53 to ‐0.31, P = 0.003, 4 RCTs, 484 women, I² = 68%, moderate‐quality evidence). Infectious complications were less common in the early feeding group (RR 0.20, 95% CI 0.05 to 0.73, P = 0.02, 2 RCTs, 183 women, I² = 0%, high‐quality evidence). In one study, the satisfaction score was significantly higher in the early feeding group (MD 11.10, 95% CI 6.68 to 15.52, P < 0.00001, 143 women, moderate‐quality evidence).
Authors' conclusions
Early postoperative feeding after major abdominal gynaecologic surgery for either benign or malignant conditions appeared to be safe without increased gastrointestinal morbidities or other postoperative complications. The benefits of this approach include faster recovery of bowel function, lower rates of infectious complications, shorter hospital stay, and higher satisfaction.
PICO
Ringkasan bahasa mudah
Pemberian makanan lebih awal berbanding dengan lewat untuk mengurangkan komplikasi setelah pembedahan ginekologikal
Soalan ulasan
Apakah risiko dan manfaat pemakanan lebih awal berbanding dengan lewat untuk sekurang‐kurangnya 24 jam selepas pembedahan ginekologikal abdominal?
Latar belakang
Doktor kerap melewatkan pemberian makanan dan minuman kepada pesakit wanita selepas pembedahan ginekologikal abdominal (fibroid rahim, endometriosis, sista ovari, kanser rahim dan ovari) setelah fungsi usus bersambung semula (biasanya 24 jam selepas pembedahan). Ini adalah untuk mengurangkan risiko komplikasi seperti pemuntahan, gangguan gastro‐usus dan kepecahan luka atau kebocoran. Namun, ia telah dicadangkan bahawa sesetengah wanita dapat pulih lebih cepat jika makanan diberikan lebih awal. Kami mengulas bukti daripada percubaan terkawal rawak untuk pemberian makanan awal dan lewat setelah pembedahan abdominal ginekologikal.
Ciri‐ciri Kajian
Kami menilai bukti mengenai hasil‐hasil berikut:
1. Loya, muntah, sakit perut, perut kembung, distin abdomen, komplikasi luka, thrombosis vena dalam, jangkitan saluran kencing, pneumonia.
2. Masa pertama untuk: bunyi usus, gas, najis, permulaan pemakanan diet biasa.
3. Tempoh penginapan hospital
Pemberian makanan awal ditakrifkan sebagai pengambilan cecair atau makanan dalam masa 24 jam selepas pembedahan.
Pemberian makanan lewat ditakrifkan sebagai pengambilan cecair atau makanan 24 jam selepas pembedahan, dan hanya jika terdapat bunyi usus, laluan gas atau najis, dan perasaan lapar.
Bukti ini adalah terkini sehingga April 2014
Keputusan utama
Kami memasukkan lima kajian yang diterbitkan yang melibatkan 631 wanita, kebanyakannya dengan kanser ginekologikal.
Pemulihan fungsi usus adalah lebih cepat bagi mereka dengan pemakanan awal. Tiada perbezaan dalam kadar perasaan loya atau pemuntahan, distensi abdominal, keperluan tiub nasogastric selepas pembedahan atau masa untuk pergerakan usus pertama, tetapi pemberian makanan awal dikaitkan dengan masa yang lebih singkat untuk bunyi usus dan permulaan gas. Kumpulan yang diberi makanan awal disambung semula dengan diet makanan pepejal 1½ hari lebih awal daripada kumpulan dengan pemberian makanan lewat, serta tempoh tinggal di hospital adalah sehari lebih pendek. Tambahan pula, kumpulan yang diberi makanan awal berasa lebih puas terhadap jadual waktu pemberian makanan, walaupun hanya satu kajian melaporkan ini.
Pemberian makanan awal nampaknya selamat, tanpa peningkatan komplikasi selepas pembedahan dan juga dengan lebih kurang komplikasi ijangkitan secara keseluruhan.
Kualiti bukti
Kualiti bukti adalah sederhana. Batasan utama adalah kekurangan pembutaan, yang mungkin mempengaruhi penemuan untuk hasil subjektif seperti simtom‐simtom yang dilaporkan sendiri, tempoh tinggal di hospital, kepuasan pesakit serta kualiti hidup.
Kesimpulan
Bukti mencadangkan bahawa memakan dan meminum pada hari pertama selepas pembedahan ginekologikal abdominal adalah selamat dan mungkin dapat mengurangkan tempoh tinggal di hospital.
Authors' conclusions
Summary of findings
| Early oral feeding compared to delayed oral feeding for women who had major abdominal gynaecologic surgery | ||||||
| Patient or population: Women who had major abdominal gynaecologic surgery | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Delayed oral feeding | Early oral feeding | |||||
| Postoperative ileus | 77 per 1000 | 36 per 1000 | RR 0.47 | 279 | ⊕⊕⊕⊝ | |
| Nausea or vomiting or both | 352 per 1000 | 363 per 1000 | RR 1.03 | 484 | ⊕⊕⊕⊝ | Random effects model, deployed because of substantial heterogeneity between studies (I2> 50%) |
| Time to bowel sounds [days] | The mean time to the presence of bowel sound [days] in the intervention groups was | 338 | ⊕⊕⊕⊝ | Random effects model, deployed because of substantial heterogeneity between studies (I2> 50%) | ||
| Time to the passage of flatus [days] | The mean time to the passage of flatus [days] in the intervention groups was | 444 | ⊕⊕⊕⊕ | |||
| Time to the first solid diet [days] | The mean time to the first solid diet [days] in the intervention groups was | 301 | ⊕⊕⊕⊝ | Random effects model, deployed because of substantial heterogeneity between studies (I2> 50%) | ||
| Time to first passage of stool [days] | The mean time to first passage of stool [days] in the intervention groups was | 249 | ⊕⊕⊕⊝ | |||
| Hospital stay [days] | The mean hospital stay [days] in the intervention groups was | 484 | ⊕⊕⊕⊝ | Random effects model, deployed because of substantial heterogeneity between studies (I2> 50%) | ||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 For the three studies contributing data, all were at high risk of performance bias, two were at unclear risk of detection bias, and one was at high risk of selection bias (no allocation concealment). 4 This outcome may be influenced by the high risk of performance bias in all studies that provided data. | ||||||
Background
This review is an update of a previously published review in The Cochrane Library (Issue 4, 2007) on 'Early versus delayed oral fluids and food for reducing complications after major abdominal gynaecologic surgery'
Description of the condition
Abdominal surgery plays a major role in the treatment of various benign and malignant gynaecologic disorders, including uterine fibroids, endometriosis, ovarian cyst, uterine cancer, and ovarian cancer. In this regard, hysterectomy and removal of ovarian cysts or ovarian tumours are commonly performed procedures. Women, especially those with cancer, frequently undergo multiple procedures during surgery.
There is a widespread belief that intestinal stasis (paralytic ileus), a temporary inhibition of bowel motility, follows all abdominal surgery. The exact cause of this clinical phenomenon is unknown, but proposed mechanisms include stimulation of pain fibres, excessive sympathetic tone, and the release of inhibitory neurotransmitters from the gut wall (Kelly 1997). Gynaecologists have traditionally withheld postoperative oral intake until the return of bowel function as evidenced by the presence of bowel sounds, a passing of flatus or stool or both, and a feeling of hunger. There has been concern that early oral intake would result in vomiting and severe paralytic ileus with subsequent aspiration pneumonia, wound dehiscence (break down), and anastomotic leakage (leakage of surgically‐created connections between parts of the intestine) (Fanning 2001). This belief has become surgical dogma, unsupported by scientific evidence.
Description of the intervention
Recently, the practice of delayed postoperative oral intake has been challenged by evidence from several gastrointestinal physiologic studies that examine contractile activity of the intestine. Gastric emptying and small intestinal absorptive capacity resume on the first postoperative day while colonic activity normally returns within 48 hours after surgery (Wells 1964; Wilson 1975; Woods 1978). These data suggest that postoperative ileus may not occur as a paralysis of the entire bowel with complete absence of any functional contractile activity, as is conventionally assumed (Pearl 1998). If postoperative ileus takes place, it is usually transient and not clinically significant. It is also known that typically the stomach and pancreas secrete one to two litres of fluid daily which are readily absorbed in the small intestine (Bufo 1994). Women after surgery without a nasogastric tube are therefore tolerating high volumes of fluid even though nothing is given orally. In addition, there are studies demonstrating that physical signs suggestive of resolution of postoperative ileus are not well correlated with the incidence of nausea and vomiting (Nachlas 1972; Bufo 1994). Based on these findings, withholding oral intake until resolution of postoperative ileus is not an evidence‐based practice, and may also be unnecessary.
How the intervention might work
Several clinical benefits of giving food and fluids soon after surgery have been proposed in the literature. Following surgery, optimal nutritional status and maintenance of bowel function contribute significantly to wound healing (Windsor 1988; Deitch 1991). Early oral intake has also been suggested to be an effective alternative in postoperative stress ulcer prophylaxis as it helps to maintain strength of bowel mucosa. In patients receiving early oral intake, the risk of sepsis is reduced because of decreased bacterial colonisation and reduced migration through defects on the bowel mucosa into blood circulation (Deitch 1991). Furthermore, an improved sense of well‐being was observed in patients who ate sooner (Schilder 1997). This psychological aspect contributes considerably to the entire postoperative recovery process. Cost effectiveness is another potential advantage of early feeding scheme, as those who begin eating sooner tend to have a shorter length of hospital stay.
Regarding the safety of early postoperative oral intake, evidence from general surgical studies (Reissman 1995; Singh 1998) and a systematic review in women undergoing caesarean delivery (Mangesi 2002) have shown that early oral intake is safe and does not result in any significant increase in complications. Another systematic review on feeding after gastrointestinal surgery has confirmed that there is no clear benefit in keeping patients "nil by mouth", and that early feeding might be beneficial (Lewis 2001).
Why it is important to do this review
Given the lack of a clear evidence‐based rationale for the traditional practice of delaying oral intake after major abdominal gynaecologic surgery, a systematic review of relevant studies will assess potential benefits and harms from early postoperative oral intake. The scope of this review is focused on a specific group of patients, so that results may be more directly applicable. A larger, heterogeneous group of patients (e.g. gynaecology and general surgery patients combined) could potentially complicate results and delay applicability, due to different courses of diseases and operative characteristics.
Objectives
To assess the effects of early versus delayed (traditional) initiation of oral intake of food and fluids after major abdominal gynaecologic surgery.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) were eligible that compared the effect of early versus delayed initiation of oral intake of food and fluids after major abdominal gynaecologic surgery on clinically meaningful postoperative outcomes. We excluded quasi‐randomised controlled trials. We did not accept studies with significant violations of allocation procedure and exclusions after allocation.
Types of participants
The study participants were women who had had major open abdominal gynaecologic surgery, regardless of the type of the incision (midline or transverse). 'Major open abdominal gynaecologic surgery' excludes any operations performed mainly for tubal sterilisation. We also excluded studies of women who received gynaecologic laparoscopic surgery (major or minor) or vaginal hysterectomy.
Types of interventions
Main intervention
Early postoperative oral intake of fluids and food.
'Early postoperative oral intake' was defined as having oral intake of fluids or food within the first 24 hours after surgery, regardless of the presence or absence of the signs that indicate the return of bowel function.
Comparison intervention
'Delayed postoperative oral intake' was defined as the introduction of oral fluids or food after the first 24 hours following surgery, and only after clinical signs of resolution of postoperative ileus were evident ‐ most commonly a presence of bowel sound, a passing of flatus or stool, and a feeling of hunger.
We considered that having only ice chips or sips of water within the first 24 hours after surgery but nothing else orally until clinical signs of resolution of postoperative ileus counted as part of the 'delayed' group.
Types of outcome measures
We recorded the following outcomes if the information was available.
Primary outcomes
-
Development of symptoms and signs of postoperative ileus: rate of nausea, vomiting, cramping abdominal pain, bloating, abdominal distension [dichotomous data]
-
Time interval: time to the presence of bowel sound, time to the first passage of flatus, time to the first passage of stool, time to the start of regular diet, length of postoperative hospital stay [continuous data]
Secondary outcomes
-
Other major postoperative complications: rate of infectious complication, wound complication, deep venous thrombosis (DVT), urinary tract infection, pneumonia [dichotomous data]
-
Satisfaction and health‐related quality of life [continuous data]
Search methods for identification of studies
We searched for all published and unpublished RCTs, without language restriction and in consultation with the Cochrane Menstrual Disorders and Subfertility Group (CMDSG) Trials Search Co‐ordinator:
Electronic searches
We searched the following electronic databases to find reports of relevant RCTs:
-
Cochrane Menstrual Disorders and Subfertility Group's Specialised Register (searched 1 April 2014);
-
The Cochrane Central Register of Controlled Trials (CENTRAL) (1 April 2014);
-
Ovid MEDLINE (1946 to 1 April 2014);
-
Ovid MEDLINE (In‐Process & Other Non‐Indexed Citations 1 April 2014);
-
Ovid EMBASE (1980 to 2014 Week 13);
-
EBSCO CINAHL (1982 to 1 April 2014)
-
The registry for ongoing trials [www.clinicaltrials.gov; a service of the US National Institutes of Health] (searched 13 May 2014)]
The search strategies for these databases can be found in Appendix 1; Appendix 2; Appendix 3; Appendix 4; Appendix 5.
Searching other resources
We checked the citation lists of relevant publications, systematic reviews, review articles, abstracts of scientific meetings and included studies.
We conducted personal communications with experts, specialists in the field, and the authors of relevant publications in an attempt to identify unpublished studies.
Data collection and analysis
Selection of studies
Two review authors (KC and EM) undertook study selection, screening the titles and abstracts of articles found in the search. We discarded those studies that were clearly ineligible, but the aim was to be overly inclusive rather than risk losing relevant studies. KC obtained copies of the full‐text articles and made copies for EM. Both review authors independently assessed whether the studies met the inclusion criteria, resolving disagreements by discussion. We sought further information from the study authors where papers contained insufficient information to make a decision about eligibility.
Data extraction and management
The review authors independently extracted information using the pro forma designed by the Review Group, resolving discrepancies by discussion. For each included trial, we collected information regarding the study location, study methods (as per quality assessment checklist), participants (age range, eligibility criteria), the nature of the interventions, and data relating to the outcomes specified above. Where possible, we sought missing data from the study authors.
Assessment of risk of bias in included studies
The two review authors independently assessed study quality, with discrepancies resolved by discussion. We explored the risk of bias in the included studies, using the Cochrane 'Risk of bias' assessment tool (Higgins 2011). The domains of bias assessed included selection (random sequence generation and allocation concealment), performance (blinding of participants and personnel), detection (blinding of outcome assessors), attrition (incomplete outcome data), and selective reporting.
We present risk of bias assessments for the included studies in tables within the Characteristics of included studies tables, which provide a context for discussing the reliability of the results.
Measures of treatment effect
For dichotomous data, we express results for each study as a risk ratio (RR) with a 95% confidence interval (CI). For continuous data, we express results from each study as a mean difference (MD) with a 95% confidence interval. Meta‐analytic methods for continuous data assume that the underlying distribution of the measurements was normal. Hence, skewed data were to be reported in the publication separately as the median and range with non‐parametric tests of significance.
Unit of analysis issues
The primary analysis was by the individual woman randomised.
Dealing with missing data
We analysed the data on an intention‐to‐treat basis as far as possible, and sought missing data by contacting investigators from the original trials. If data were still unobtainable, we planned to undertake imputation of individual values for the primary outcomes only.
Assessment of heterogeneity
We examined heterogeneity (variation) between results from different studies by inspecting the forest plot of a meta‐analysis for variation in effects. We also considered formal statistical tests, such as tests of homogeneity of 2 x 2 tables and the I² value (Higgins 2003) in conjunction with graphical approaches, to determine between‐study differences.
When there was substantial unexplained heterogeneity between studies (I2>50%), we used the random‐effects model, and compared pooled results from the fixed‐effect and random‐effects models.
Assessment of reporting biases
For the included studies for which the study protocols were published in www.clinicaltrials.gov, we compared the planned and the reported outcomes to examine their consistency.
Data synthesis
If the studies were sufficiently similar, we combined the data for meta‐analysis with Review Manager 5 software, using a fixed‐effect model (unless there was substantial unexplained heterogeneity) in the following comparison:
Early versus delayed oral fluids and food after major abdominal gynaecologic surgery
An increase in the risk of a particular outcome, which may be beneficial or detrimental, are displayed graphically in the meta‐analyses to the right of the centre‐line and a decrease in the risk of an outcome to the left of the centre‐line.
Subgroup analysis and investigation of heterogeneity
We did not plan to perform any subgroup analyses.
Sensitivity analysis
We planned to undertake a sensitivity analysis to see whether excluding trials at high risk of bias affected the results; these include trials at high risk of selection bias.
Results
Description of studies
Results of the search
At the time of the original review, we identified 13 trials providing data comparing different feeding schedules or bowel management strategies following gynaecologic surgery (Finan 1995; Griffenberg 1997; Schilder 1997; Pearl 1998; Cutillo 1999; Fanning 1999; Kraus 2000; MacMillan 2000; Amatyakul 2001; Taguchi 2001; Pearl 2002; Steed 2002; Delaney 2005). We reviewed the full‐text reports of these trials. Three randomised controlled studies (RCTs), two published ( Pearl 1998; Steed 2002) and one unpublished study (Amatyakul 2001) met the inclusion criteria and were included in the final analysis. Ten studies failed to meet the inclusion criteria for reasons outlined in the table of Characteristics of excluded studies. We excluded Schilder 1997 because of its quasi‐randomised design. We considered three RCTs to be closely relevant but we excluded them: Cutillo 1999 compared early feeding with nasogastric decompression after major gynaecologic oncology surgery; MacMillan 2000 included women undergoing vaginal gynaecologic surgery (48% of participants); Pearl 2002 compared a regular diet with clear liquid as the first meal after intra‐abdominal gynaecologic oncology surgery. The remaining six studies in the area of postoperative management to reduce intestinal ileus (Finan 1995; Griffenberg 1997; Fanning 1999; Kraus 2000; Taguchi 2001; Delaney 2005) reported comparisons which were clearly not within the scope of this review.
For this updated version of the review, we identified five additional eligible studies (Feng 2008; Minig 2009a; Minig 2009b; Fanning 2011; Terzioglu 2013), and examined the full‐text reports. Two studies (Minig 2009a; Minig 2009b) met the inclusion criteria and are included in the updated analyses. For the three excluded studies: Feng 2008 compared a semiliquid diet with clear feeds, both started at six hours after major abdominal gynaecologic oncology surgery; Fanning 2011 is a non‐comparative study that examined the effects of immediate postoperative feeding and bowel stimulation in 707 women who had major gynaecologic operations over a five‐year period; Terzioglu 2013 compared eight different combinations of postoperative interventions, including gum chewing, early oral hydration, and early mobilisation following abdominal gynaecologic surgery.
See: Study flow diagram (Figure 1), Characteristics of included studies, and Characteristics of excluded studies.
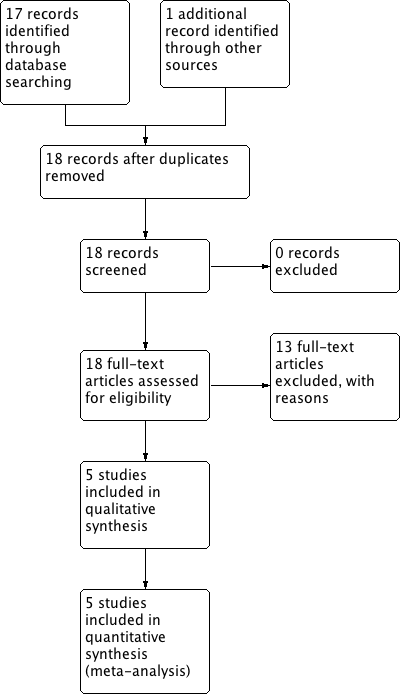
Study flow diagram.
Included studies
Study design and setting
All of the five included studies were parallel‐design randomised controlled trials.
Participants
The updated review includes a total of 631 women, increased from the previous total of 413 women. The size of the included studies was: 200 (Pearl 1998), 106 (Amatyakul 2001), 107 (Steed 2002), 51 (Minig 2009a), and 167 (Minig 2009b). Each study was conducted in a single university‐based hospital. The countries represented were the United States (Pearl 1998), Canada (Steed 2002), Thailand (Amatyakul 2001), and Italy (Minig 2009a; Minig 2009b). Three studies (Pearl 1998; Minig 2009a; Minig 2009b) were conducted essentially in gynaecologic oncology patients. In Steed 2002, the majority of women were gynaecologic oncology patients. Almost all (95%) women in the remaining study (Amatyakul 2001) had benign or pre‐invasive gynaecological diagnoses. The women in Amatyakul 2001 were younger (Mean age: 40.8 years in early group, 41.1 years in delayed group) than those in Pearl 1998 (Mean age: 56.5 years in early group, 57.7 years in delayed group), Steed 2002 (Mean age: 50.0 years in early group, 52.0 years in delayed group), Minig 2009a (Median age: 54 years in early group, 58 years in delayed group), and Minig 2009b (Mean age: 54 years in early group, 57 years in delayed group). Body mass index (BMI) was reported in Steed 2002 (Mean BMI: 28.5 kg/m² in early group, 28.7 kg/m² in delayed group), Minig 2009a (Median BMI: 23.0 kg/m2 in early group, 24.0 kg/m2 in delayed group), and Minig 2009b (Mean BMI: 25.0 kg/m2 in both groups). In three studies (Pearl 1998; Amatyakul 2001; Minig 2009b), baseline characteristics of the women were comparable between the two groups. In Steed 2002, there were significantly more women in the early group who received epidural analgesia for pain treatment. However, there was no effect on the primary outcome of the feeding regimen and length of hospital stay when this potential confounder was factored into the final statistical analysis model. In Minig 2009a, estimated operative blood loss was significantly higher in the delayed feeding group (Median blood loss: 800 ml vs. 300 ml).
Interventions
The definitions of early and delayed feeding schedule varied among included studies in that:
For the early feeding group, the diet schedule applied in Amatyakul 2001, Minig 2009a, and Minig 2009b, appeared to be more aggressive. In Amatyakul 2001, women were started on a soft diet in the morning of the first postoperative day and proceeded to a regular solid diet on the second postoperative day. In Minig 2009a and Minig 2009b, participants were offered liquids, mineral water (still), tea, chamomile infusion, or apple juice during the first 24 hours. If no nausea and vomiting, a regular diet of boiled or grilled beef, chicken, or fish was given starting on day 1 and continued for the entire hospital stay. In the remaining studies the participants began a clear liquid diet on the first postoperative day and then advanced to a regular diet as tolerated.
For the delayed feeding group, the schedule used in Amatyakul 2001 was slightly more conservative than others. After signs of the return of bowel function, women were allowed to have only sips of water before advancing to a liquid diet in the evening of the same day, while in the other studies women were readily started on a liquid diet after the presence of those signs. We note that the criteria for a return of bowel function were similar in all studies.
Outcomes
Steed 2002 reported the incidence of postoperative ileus, which was defined as more than two episodes of vomiting of at least 100 ml each within a 24‐hour time period, with associated abdominal distension and no bowel sounds. The other studies indirectly assessed the occurrence of postoperative ileus through the incidence of related postoperative gastrointestinal morbidity. Pearl 1998 reported the incidence of nausea, vomiting, abdominal distension, and nasogastric tube use. Amatyakul 2001 reported the incidence of vomiting and abdominal distension. Minig 2009a and Minig 2009b reported intensity of abdominal pain and presence of nausea and emesis. Regarding data on postoperative time intervals to the return of bowel function, time to the presence of bowel sound was reported in Pearl 1998, Minig 2009a and Minig 2009b. Time to the first passage of flatus and time to the start or tolerance of solid food were reported in Pearl 1998, Amatyakul 2001, Minig 2009a, and Minig 2009b. Amatyakul 2001, Minig 2009a, and Minig 2009b reported time to the first passage of stool.
Length of postoperative hospital stay was reported as means in Pearl 1998, Amatyakul 2001, Minig 2009a, and Minig 2009b. However, these data were reported as medians in Steed 2002, because of the skewed distribution.
For the two studies that assessed wound complications, the reported outcomes vary; Pearl 1998 reported as overall wound complications while Steed 2002, Minig 2009a, and Minig 2009b as wound infection. Meta‐analysis results for these dissimilar wound complication outcomes should therefore be interpreted with caution.
Risk of bias in included studies
See: 'Risk of bias' graph (Figure 2) and 'Risk of bias' summary (Figure 3).
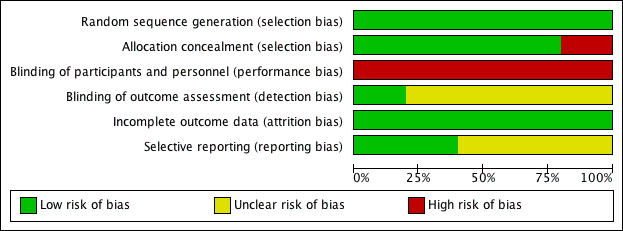
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
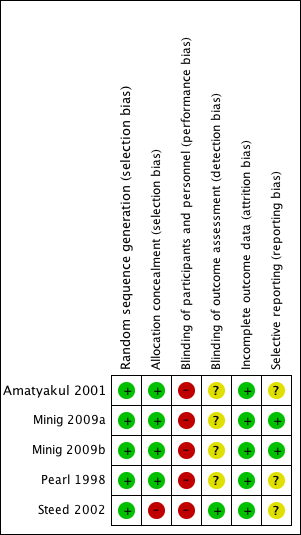
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
The methods of random sequence generation were appropriate in all five included studies. Computer‐generated sequences were employed in four studies (Pearl 1998; Steed 2002; Minig 2009a; Minig 2009b). Amatyakul 2001 used a random number table.
Allocation concealment appeared clearly adequate in four studies (Pearl 1998; Amatyakul 2001; Minig 2009a; Minig 2009b), in which randomisation was performed by using sequentially numbered, sealed, opaque assignment envelopes according to the random number list generated by computer (Pearl 1998), by a random number table (Amatyakul 2001), or by a web‐based Tenalea randomisation system (Minig 2009a; Minig 2009b). In Steed 2002, there appeared to be no concealment of allocation, given the fact that randomisation was performed by the clinic nurses according to an open random number list generated by computer. In Pearl 1998 and Steed 2002, randomisation was performed before the start of the operation. In three studies (Amatyakul 2001; Minig 2009a; Minig 2009b), women were randomised at the end of the operation.
Blinding
Because of the nature of this research question, women and attending physicians were not blinded to the intervention received in any of the studies, and were therefore all at high risk of performance bias.
The outcome assessors in Steed 2002 were blinded, so the risk of detection bias was low. In Amatyakul 2001, Pearl 1998, Minig 2009a, and Minig 2009b, the outcome assessors were aware of participants' study allocation (information from the study authors). However, the influence of the lack of blinding on study outcomes was unclear.
Incomplete outcome data
The follow‐up rate of women in the included studies was: 100% in Amatyakul 2001, 97.5% in Pearl 1998, 90% in Steed 2002, 86% in Minig 2009b, and 78% in Minig 2009a. In Amatyakul 2001, a full intention‐to‐treat analysis was applied. The studies with participant withdrawals used available case analyses.
Selective reporting
In Minig 2009a and Minig 2009b, the study protocols were published in www.clinicaltrials.gov, and the reported outcomes corresponded with those listed in the registered protocols. We therefore judged that these studies were at low risk of reporting bias. In other studies, the study protocols were not published in a protocol registry. However, the report included the expected outcomes. We deemed the risk of reporting bias in these studies to be unclear.
Other potential sources of bias
A power analysis was performed in all trials. With the numbers of women recruited, there was a reasonable probability of detecting a significant effect (should one exist) in Amatyakul 2001, Steed 2002, Minig 2009a, and Minig 2009b, but not in Pearl 1998.
Effects of interventions
For outcomes with data available, the number of studies contributing usable data ranged from one to four (summary of findings Table for the main comparison).
Early versus delayed oral fluids and food after major abdominal gynaecologic surgery
Primary outcomes
1.1 Postoperative ileus
Rates of developing postoperative ileus were comparable between the study groups (risk ratio (RR) 0.47, 95% confidence interval (CI) 0.17 to 1.29, P = 0.14, 3 RCTs, 279 women, I² = 0%, moderate‐quality evidence) (Analysis 1.1.1). This suggests that in women with an 8% chance of developing postoperative ileus with delayed oral feeding, the chance of developing postoperative ileus with early feeding will be between 1% and 10%. When we specifically considered the rates of nausea or vomiting or both, there was no evidence of a difference between the study groups (RR 1.03, 95% CI 0.64 to 1.67, P = 0.90, random‐effects model, 4 RCTs, 484 women, I² = 73%, moderate‐quality evidence) (Analysis 1.1.2; Analysis 1.5). Considering each symptom separately, early commencement of oral fluids and food was associated with increased nausea (RR 1.79, 95% CI 1.19 to 2.71, P = 0.006, 1 RCT, 195 women, moderate‐quality evidence) (Analysis 1.1.3). However, there was no increase in vomiting (RR 0.86, 95% CI 0.37 to 2.00, P = 0.73, 2 RCTs, 301 women, I² = 2%, moderate‐quality evidence) (Analysis 1.1.4).
There was no evidence of a difference in abdominal distension (RR 1.07, 95% CI 0.77 to 1.47, 2 RCTs, 301 women, I² = 0%, moderate‐quality evidence) or in the need for postoperative nasogastric tube placement (RR 0.48, 95% CI 0.13 to 1.80, 1 RCT, 195 women, moderate‐quality evidence) between the study groups (Analysis 1.1.5, Analysis 1.1.6).
1.2 Time to recovery of bowel function
Early feeding was associated with shorter time to the presence of bowel sounds (MD ‐0.32 days, 95% CI ‐0.61 to ‐0.03, P = 0.03, random‐effects model, 2 RCTs, 338 women, I² = 52%, moderate‐quality evidence) (Analysis 1.2.1; Analysis 1.6) and faster onset of flatus (MD ‐0.21 days, 95% CI ‐0.40 to ‐0.01, P = 0.04, 3 RCTs, 444 women, I² = 23%, moderate‐quality evidence) (Analysis 1.2.2). In addition, women in the early feeding group resumed a solid diet sooner (MD ‐1.47 days, 95% CI ‐2.26 to ‐0.68, P = 0.0003, random‐effects model, 2 RCTs, 301 women, I² = 92%, moderate‐quality evidence) (Analysis 1.2.3; Analysis 1.7). In Minig 2009b, the proportions of women in the early feeding and delayed feeding groups who tolerated a solid diet were 89% versus 0% on day 1, 10% versus 6% on day 2, and 1% versus 94% on day 3, respectively. However, there was no evidence of a difference in time to the first passage of stool between the two study groups (MD ‐0.25 days, 95% CI ‐0.58 to 0.09, P = 0.15, 2 RCTs, 249 women, I² = 0%, moderate‐quality evidence) (Analysis 1.2.4). The time to the first passage of stool was reported in median in Minig 2009a. They were also comparable between the study groups (5.0 days in the early feeding group and 5.5 days in the delayed feeding group).
Hospital stay was shorter in the early feeding group (MD ‐0.92 days, 95% CI ‐1.53 to ‐0.31, P = 0.003, random‐effects model, 4 RCTs, 484 women, I² = 68%, moderate‐quality evidence) (Analysis 1.2.5; Analysis 1.8). The shorter hospital stay associated with early postoperative feeding was further evident in the only study (Steed 2002) that reported length of hospital stay in median days (‐2 days, 4.0 days in the early feeding group and 6.0 days in the delayed feeding group).
Sensitivity analyses
Some outcomes had substantial heterogeneity: nausea or vomiting or both, time to the presence of bowel sounds, time to the first solid diet, and hospital stay. In those cases, we also produced a random‐effects model and compared the pooled results from the fixed‐ and random‐effects models. Generally, the two models provided similar results.
Exclusion from analyses of the study at high risk of selection bias (Steed 2002) did not substantially influence any of the findings.
Secondary outcomes
1.3 Other postoperative complications
While the rates of febrile morbidity were similar between the group (RR 0.98, 95% CI 0.76 to 1.27, P = 0.89) in Pearl 1998 (Analysis 1.3.1), infectious complications were less common in the early feeding group (RR 0.20, 95% CI 0.05 to 0.73, P = 0.02, 2 RCTs, 183 women, I² = 0%, high‐quality evidence). (Analysis 1.3.2). The rates of wound complications and pneumonia were comparable between the groups. (Analysis 1.3.3, Analysis 1.3.4)
1.4 Satisfaction and health‐related quality of life
Participant satisfaction and quality of life outcomes related to different postoperative feeding schedules were addressed for the first time in the two newly included studies (Minig 2009a; Minig 2009b).
Satisfaction was assessed before hospital discharge by using a visual analogue scale (VAS). In Minig 2009b, the satisfaction score was higher in the early feeding group (MD 11.10, 95% CI 6.68 to 15.52, P < 0.00001, 143 women, moderate‐quality evidence) (Analysis 1.4). In Minig 2009a, the satisfaction score was reported as a median (Q₁ ‐ Q₃). The scores were 80 (80 ‐ 90) in the early feeding group and 75 (60 ‐ 90) in the delayed feeding group (P = 0.07). For women who had delayed feeding, 65% and 58% wished to eat sooner in Minig 2009a and Minig 2009b, respectively.
Quality of life was assessed at 30 days after surgery by using validated questionnaires designed by the European Organization for Research and Treatment of Cancer (EORTC) to measure overall health status in people with cancer in general (EORTC QLQ‐C30), and in those with ovarian cancer (EORTC QLQ‐OV28). The questionnaires focus on global function, physical function, cognitive function, social function, cancer‐related symptoms, and financial impact. There were no statistically significant difference in any of the health‐related quality of life domains between the two study groups.
Discussion
Summary of main results
Early postoperative feeding after major abdominal gynaecologic surgery appeared to be safe without increased gastrointestinal morbidities and other postoperative complications. From the pooled analysis of ileus‐related outcomes, the rates of postoperative ileus (three trials, 279 women), nausea or vomiting or both (four trials, 484 women), and abdominal distention (two trials, 301 women) were comparable between the early and delayed feeding groups. In addition, the rates of overall infectious complications were significantly lower in the participants who had early feeding (two trials, 183 women).
Furthermore, the recovery of bowel function was faster in those with early feeding. These include shorter time to the presence of bowel sounds (two trials, 338 women), shorter time to the passage of flatus (three trials, 444 women), and shorter time to starting a solid diet (two trials, 301 women). Importantly, early feeding was associated with reduced length of hospital stay by one day (four trials, 484 women). It also appeared that women with early feeding were more satisfied with the feeding schedule (one trial, 143 women).
Overall completeness and applicability of evidence
The two newly included studies (Minig 2009a and Minig 2009b, 183 women) have contributed data to most important outcomes of the review, including postoperative ileus, symptoms of nausea or vomiting or both, time to the presence of bowel sounds, time to the passage of flatus, time to the passage of stool, hospital stay, infectious complications, wound complications, pneumonia, and satisfaction. These studies considerably improved the power of the meta‐analysis in detecting the difference between study groups for some outcomes. From this updated version of the review, we can be more confident to suggest the safety of early feeding with its benefits for faster recovery of bowel function, shorter hospital stay, and higher satisfaction. This information would be readily applicable to women undergoing major abdominal gynaecologic surgery for benign or malignant conditions, and to healthcare professionals taking care of them.
It should be noted that the difference between study groups on rare complications might not be detected, given the total number of participants in all of the included studies. Also, there were no data on other outcomes that may also be of interest, such as costs and other physiological benefits of early feeding, e.g. the effects on fluid, electrolyte balance, and wound healing. These data would be useful additional information for patients and physicians deciding on individualised postoperative feeding approaches.
Quality of the evidence
The five included studies were randomised controlled trials with study groups directly relevant to the review question, and provided consistent outcome data. The allocation methods were generally appropriate. The follow‐up was acceptable. There were insufficient studies to assess the risk of publication bias. However, the main methodological concern was with lack of blinding. Because of the context and nature of the studies, it was not possible to blind study participants and difficult or impractical to blind attending physicians. Performance bias may therefore have affected all these studies. It is possible that some outcomes (subjective intestinal morbidities, hospital stay, participants' satisfaction and quality of life) were influenced by the lack of blinding. In addition, outcome assessors were blinded in only one of the five included studies. This raises a concern about detection bias. However, the influence of the lack of blinding of the outcome assessors on study outcomes is unclear. This leads to our rating of the evidence as of moderate quality for subjective outcomes and of high quality for more objective outcomes.
Potential biases in the review process
This review addressed an important clinical question with a clearly defined population, intervention, and outcomes. We were able to include directly relevant studies with randomised controlled designs. For this updated version of the review, we searched a registry for ongoing trials (www.clinicaltrials.gov) in addition to the electronic databases. We also contacted study authors directly for information on relevant studies and on individual study methodology. We explored the risk of bias in the included studies by using the updated Cochrane 'Risk of bias' assessment tool, with each domain of bias explicitly considered. We have clearly tabulated the results of the included studies. The results of the studies which contributed to the pooled analyses appeared similar for most outcomes. In the presence of statistically significant heterogeneity, we deployed appropriate statistical analytic tools, i.e. random‐effects model for the meta‐analyses .
Agreements and disagreements with other studies or reviews
In a randomised study comparing early oral feeding and nasogastric decompression followed by feeding at the first passage of flatus in women undergoing major surgery for gynaecologic malignancies (Cutillo 1999), early oral feeding was associated with a faster resolution of postoperative ileus, a faster return to a regular diet, an earlier passage of stool, and a shorter postoperative hospital stay. The rates of nausea and vomiting were comparable in both groups. Nearly 90% of women who had a nasogastric tube inserted reported discomfort related to difficulty in swallowing and nasal soreness.
The safety and benefits of early feeding for bowel recovery following major abdominal gynaecologic surgery was also generally supported by findings from studies that were closely relevant but excluded from this review (Schilder 1997; MacMillan 2000). In Schilder 1997, which was a quasi‐randomised study comparing early commencement of a clear liquid diet on postoperative day one to delayed feeding until the return of bowel function in gynaecologic oncology patients, those with early feeding tolerated the solid diet earlier (1.88 days versus 2.72 days, P < 0.0001) and had shorter hospital stay (3.12 days versus 4.02 days, P = 0.008). However, the incidence of emesis was higher in the early feeding group, but did not translate to significant adverse outcomes. In MacMillan 2000, early feeding (a low‐residue diet started six hours after surgery) was compared to delayed feeding (a clear liquid diet with the presence of normal bowel sound) in women who had major abdominal or vaginal surgery for benign gynaecologic conditions. While the incidence of postoperative ileus was comparable between the study groups (3% in the early group and 5.8% in the delayed feeding group), the incidence of nausea was higher in the delayed feeding group (23% versus 13%, P = 0.04). There were no differences in perioperative complications, gastrointestinal function, pain scores, pain medication requirement, and fluid and calorie intake between the two study groups.
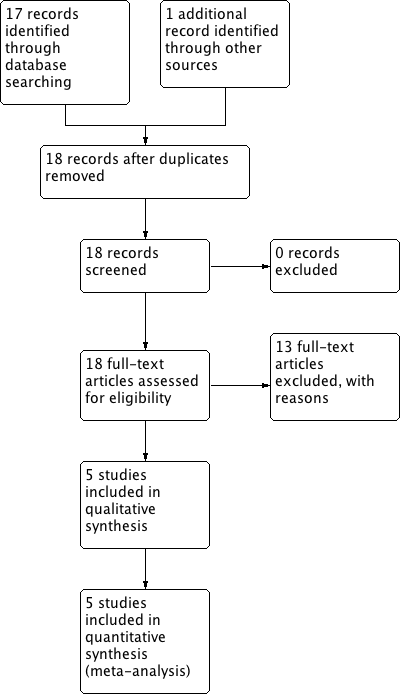
Study flow diagram.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
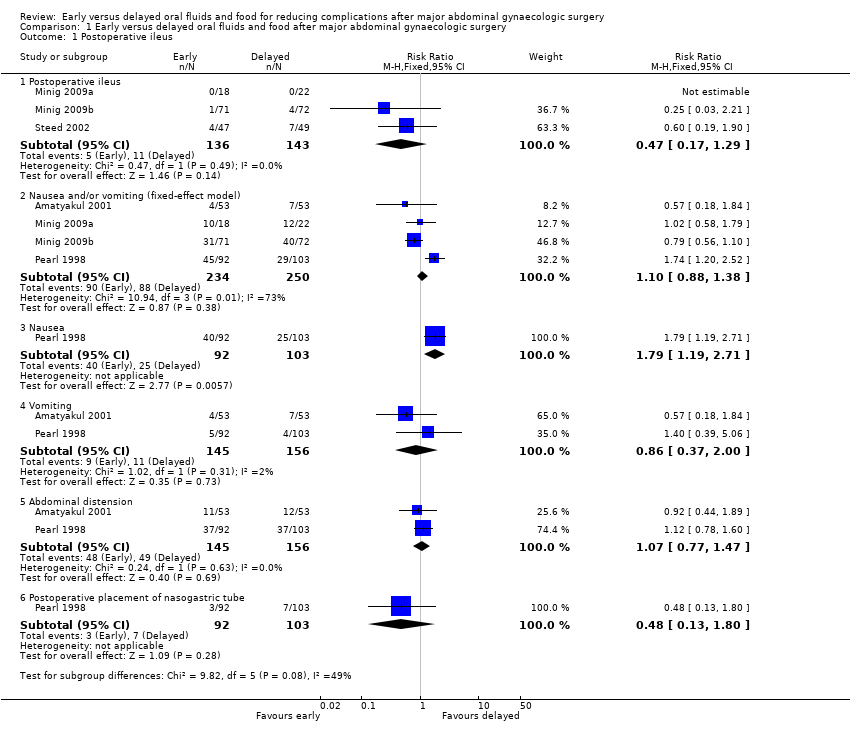
Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 1 Postoperative ileus.
![Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 2 Time intervals (fixed‐effect model) [days].](/es/cdsr/doi/10.1002/14651858.CD004508.pub4/media/CDSR/CD004508/image_n/nCD004508-CMP-001-02.png)
Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 2 Time intervals (fixed‐effect model) [days].

Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 3 Other major postoperative complications.
![Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 4 Satisfaction visual analog scale [mm].](/es/cdsr/doi/10.1002/14651858.CD004508.pub4/media/CDSR/CD004508/image_n/nCD004508-CMP-001-04.png)
Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 4 Satisfaction visual analog scale [mm].
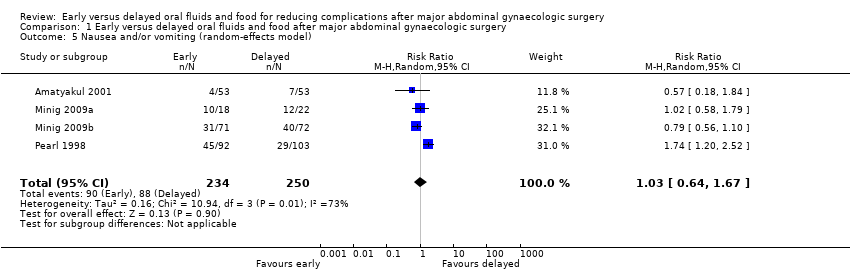
Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 5 Nausea and/or vomiting (random‐effects model).
![Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 6 Time to the presence of bowel sound (random‐effects model) [days].](/es/cdsr/doi/10.1002/14651858.CD004508.pub4/media/CDSR/CD004508/image_n/nCD004508-CMP-001-06.png)
Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 6 Time to the presence of bowel sound (random‐effects model) [days].
![Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 7 Time to the first solid diet (random‐effects model) [days].](/es/cdsr/doi/10.1002/14651858.CD004508.pub4/media/CDSR/CD004508/image_n/nCD004508-CMP-001-07.png)
Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 7 Time to the first solid diet (random‐effects model) [days].
![Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 8 Hospital stay (random‐effects model) [days].](/es/cdsr/doi/10.1002/14651858.CD004508.pub4/media/CDSR/CD004508/image_n/nCD004508-CMP-001-08.png)
Comparison 1 Early versus delayed oral fluids and food after major abdominal gynaecologic surgery, Outcome 8 Hospital stay (random‐effects model) [days].
| Early oral feeding compared to delayed oral feeding for women who had major abdominal gynaecologic surgery | ||||||
| Patient or population: Women who had major abdominal gynaecologic surgery | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Delayed oral feeding | Early oral feeding | |||||
| Postoperative ileus | 77 per 1000 | 36 per 1000 | RR 0.47 | 279 | ⊕⊕⊕⊝ | |
| Nausea or vomiting or both | 352 per 1000 | 363 per 1000 | RR 1.03 | 484 | ⊕⊕⊕⊝ | Random effects model, deployed because of substantial heterogeneity between studies (I2> 50%) |
| Time to bowel sounds [days] | The mean time to the presence of bowel sound [days] in the intervention groups was | 338 | ⊕⊕⊕⊝ | Random effects model, deployed because of substantial heterogeneity between studies (I2> 50%) | ||
| Time to the passage of flatus [days] | The mean time to the passage of flatus [days] in the intervention groups was | 444 | ⊕⊕⊕⊕ | |||
| Time to the first solid diet [days] | The mean time to the first solid diet [days] in the intervention groups was | 301 | ⊕⊕⊕⊝ | Random effects model, deployed because of substantial heterogeneity between studies (I2> 50%) | ||
| Time to first passage of stool [days] | The mean time to first passage of stool [days] in the intervention groups was | 249 | ⊕⊕⊕⊝ | |||
| Hospital stay [days] | The mean hospital stay [days] in the intervention groups was | 484 | ⊕⊕⊕⊝ | Random effects model, deployed because of substantial heterogeneity between studies (I2> 50%) | ||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 For the three studies contributing data, all were at high risk of performance bias, two were at unclear risk of detection bias, and one was at high risk of selection bias (no allocation concealment). 4 This outcome may be influenced by the high risk of performance bias in all studies that provided data. | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Postoperative ileus Show forest plot | 5 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 Postoperative ileus | 3 | 279 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.47 [0.17, 1.29] |
| 1.2 Nausea and/or vomiting (fixed‐effect model) | 4 | 484 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.88, 1.38] |
| 1.3 Nausea | 1 | 195 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.79 [1.19, 2.71] |
| 1.4 Vomiting | 2 | 301 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.37, 2.00] |
| 1.5 Abdominal distension | 2 | 301 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [0.77, 1.47] |
| 1.6 Postoperative placement of nasogastric tube | 1 | 195 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.48 [0.13, 1.80] |
| 2 Time intervals (fixed‐effect model) [days] Show forest plot | 4 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1 Time to the presence of bowel sound (fixed‐effect model) [days] | 2 | 338 | Mean Difference (IV, Fixed, 95% CI) | ‐0.29 [‐0.48, ‐0.11] |
| 2.2 Time to the passage of flatus [days] | 3 | 444 | Mean Difference (IV, Fixed, 95% CI) | ‐0.21 [‐0.40, ‐0.01] |
| 2.3 Time to the first solid diet (fixed‐effect model) [days] | 2 | 301 | Mean Difference (IV, Fixed, 95% CI) | ‐1.19 [‐1.34, ‐1.05] |
| 2.4 Time to the first passage of stool [days] | 2 | 249 | Mean Difference (IV, Fixed, 95% CI) | ‐0.25 [‐0.58, 0.09] |
| 2.5 Hospital stay (fixed‐effect model) [days] | 4 | 484 | Mean Difference (IV, Fixed, 95% CI) | ‐0.59 [‐0.83, ‐0.35] |
| 3 Other major postoperative complications Show forest plot | 4 | 1286 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.63, 1.01] |
| 3.1 Febrile morbidity | 1 | 195 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.76, 1.27] |
| 3.2 Infectious complications | 2 | 183 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.20 [0.05, 0.73] |
| 3.3 Wound complications | 4 | 474 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.50, 1.35] |
| 3.4 Pneumonia | 3 | 434 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.35 [0.07, 1.73] |
| 4 Satisfaction visual analog scale [mm] Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 5 Nausea and/or vomiting (random‐effects model) Show forest plot | 4 | 484 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.64, 1.67] |
| 6 Time to the presence of bowel sound (random‐effects model) [days] Show forest plot | 2 | 338 | Mean Difference (IV, Random, 95% CI) | ‐0.32 [‐0.61, ‐0.03] |
| 7 Time to the first solid diet (random‐effects model) [days] Show forest plot | 2 | 301 | Mean Difference (IV, Random, 95% CI) | ‐1.47 [‐2.26, ‐0.68] |
| 8 Hospital stay (random‐effects model) [days] Show forest plot | 4 | 484 | Mean Difference (IV, Random, 95% CI) | ‐0.92 [‐1.53, ‐0.31] |