Incisión con bisturí versus incisión sin bisturí para la vasectomía
Resumen
Antecedentes
Actualmente, las dos técnicas quirúrgicas más frecuentes para abordar el conducto deferente durante la vasectomía son el método de incisión y la técnica sin bisturí. Mientras que la técnica de incisión convencional incluye el uso de un bisturí para realizar una o dos incisiones, la técnica sin bisturí utiliza un instrumento de punta filosa similar al fórceps para punzar la piel. La técnica sin bisturí intenta reducir los eventos adversos, especialmente hemorragias, equimosis, hematomas, infección y dolor, y acortar el tiempo de la cirugía.
Objetivos
El objetivo de esta revisión fue comparar la efectividad, seguridad y aceptabilidad del abordaje del conducto deferente para la vasectomía por incisión versus sin bisturí.
Métodos de búsqueda
En febrero 2014 se buscó en las bases de datos electrónicas CENTRAL, MEDLINE, POPLINE y LILACS. Se buscaron ensayos clínicos recientes en ClinicalTrials.gov y en la International Clinical Trials Registry Platform. Las búsquedas anteriores también incluyeron EMBASE. Para la revisión inicial, se buscaron las listas de referencia de los artículos y capítulos de libros pertinentes.
Criterios de selección
En esta revisión se incluyeron ensayos controlados aleatorizados y ensayos clínicos controlados. No se impusieron restricciones de idiomas a los informes de los ensayos.
Obtención y análisis de los datos
Se evaluaron todos los títulos y resúmenes localizados en las búsquedas bibliográficas y dos autores de la revisión de forma independiente extrajeron los datos de los artículos identificados para inclusión. Las medidas de resultado incluyeron la seguridad, la aceptabilidad, el tiempo de la cirugía, la eficacia anticonceptiva y la interrupción. Se calcularon los odds ratios (OR) de Peto con intervalos de confianza (IC) del 95% para las variables dicotómicas.
Resultados principales
Dos ensayos controlados aleatorizados evaluaron la técnica sin bisturí y difirieron en sus resultados. El ensayo más grande demostró, en comparación con el grupo de incisión estándar, menos hemorragias perioperatorias (OR 0,49; IC del 95%: 0,27 a 0,89) y dolor durante la cirugía (OR 0,75; IC del 95%: 0,61 a 0,93), dolor escrotal (OR 0,63; 95%: 0,50 a 0,80) e infección de la incisión (OR 0,21; IC del 95%: 0,06 a 0,78) durante el seguimiento. Ambos estudios encontraron menos hematomas con la técnica sin bisturí (OR 0,23; IC del 95%: 0,15 a 0,36). Las operaciones que utilizaron el abordaje sin bisturí fueron más rápidas y tuvieron una reanudación más rápida de la actividad sexual. El estudio más pequeño no encontró estas diferencias; sin embargo, es posible que no detectara diferencias por el reducido tamaño de la muestra, así como las grandes pérdidas durante el seguimiento. Ningún ensayo encontró diferencias en cuanto a la efectividad de la vasectomía entre los dos abordajes del conducto deferente.
Conclusiones de los autores
El abordaje del conducto deferente sin bisturí dio lugar a menos hemorragia, hematomas, infección y dolor, así como a un tiempo de la cirugía más corto que con la técnica de incisión tradicional. No se encontraron diferencias en cuanto a la efectividad entre los dos enfoques.
PICO
Resumen en términos sencillos
Enfoque con o sin bisturí para la vasectomía
La vasectomía es un método quirúrgico utilizado en los hombres para cortar o ligar el conducto deferente. El conducto deferente es un tubo por el que pasan los espermatozoides de los testículos. La finalidad de la vasectomía es proporcionar un control permanente de la natalidad. Generalmente, la cirugía consiste en el corte de la piel del escroto con un bisturí. En cambio, una técnica más nueva utiliza un instrumento filoso para punzar la piel. El objetivo es tener menos problemas de hemorragia, equimosis e infección. Esta revisión analizó si el enfoque sin bisturí para el conducto deferente funcionó tan bien como el método con bisturí. También estudió cualquier efecto secundario de los métodos y si los hombres prefirieron el método.
En febrero 2014 se hizo una búsqueda electrónica de estudios que compararon el enfoque para el conducto deferente sin bisturí con el método del bisturí. Se incluyeron ensayos controlados aleatorizados en cualquier idioma. Para la revisión inicial, también se examinaron las listas de referencia de los artículos y capítulos de libros.
Se encontraron dos ensayos que analizaron el enfoque sin bisturí para la vasectomía. Los ensayos tuvieron resultados algo diferentes. El ensayo más grande demostró que el método sin bisturí produjo menos sangrado, infección y dolor durante y después del procedimiento. La técnica sin bisturí requirió menos tiempo para la operación y hubo un retorno más rápido a la actividad sexual. El estudio más pequeño no mostró estas diferencias. Sin embargo, el estudio puede haber sido demasiado pequeño y muchos hombres abandonaron el estudio. Los dos métodos no difieren en cuanto al número de hombres que se vuelven estériles.
Authors' conclusions
Background
Currently, the two most common surgical techniques for approaching the vas during vasectomy are the incisional method and the no‐scalpel technique (Schwingl 2000). Whereas the conventional incisional technique involves the use of a scalpel to make one or two incisions (each 1 to 2 cm in length), the no‐scalpel technique uses a sharp, pointed, forceps‐like instrument to puncture the scrotum. The no‐scalpel technique, which was developed in China, aims to reduce adverse events, especially hematomas, bleeding, bruising, infection and pain, and to shorten the operating time. This method generally requires more training and skill than the conventional incisional method (RCOG 2004).
While adverse events following vasectomy are relatively uncommon (PIP 1992), men may experience bleeding, bruising, infection, acute and chronic pain after the procedure (RCOG 2004). The method of incision used to approach the vas can affect the occurrence of vasectomy‐related adverse events. The method of vas occlusion, though, is thought to be a stronger determinant of effectiveness than the method used to approach the vas (Goldstein 2002; RCOG 2004).
Evaluation of the relative effectiveness, safety and acceptability of these two approaches to the vas during vasectomy is vital to inform the decision making of both health service providers and clients. Ideally, choice of incision method for vasectomy should be based on the best available evidence from randomized controlled trials.
Objectives
The objective of this review was to compare the effectiveness, safety, acceptability and costs of scalpel versus no‐scalpel incision for vasectomy. The review does not address methods of occluding the vas, as that is the subject of another Cochrane review (Cook 2007).
Methods
Criteria for considering studies for this review
Types of studies
We included only randomized controlled trials in this review. No language restrictions were placed on the reporting of the trials.
Types of participants
Men of reproductive age undergoing vasectomy for sterilization.
Types of interventions
We examined two techniques for the approach to the vas for vasectomy: the no‐scalpel and the incisional method.
Types of outcome measures
We focused on clinically relevant outcome measures. We excluded studies evaluating possible long‐term vasectomy side effects (e.g., cancer, cardiovascular disease) or physiopathological outcomes only.
Primary outcomes
Post‐vasectomy adverse events including, but not limited to, the following: hematoma, scrotal abscess, wound infection, local pain and tenderness, reaction to suture material, bleeding, epididymo‐orchitis, chronic testicular/scrotal pain, congestive epidydymitis and vasovagal episodes.
Secondary outcomes
-
Operating time
-
Pain during surgery
-
Time to resumption of intercourse
-
Rates for azoospermia (no sperm detected) at post‐vasectomy follow‐up visits
-
Time to azoospermia
-
Pregnancy (contraceptive failure)
-
Incidence of recanalization
-
Incidence of repeat vasectomy
-
Cost analysis
-
Consumer acceptability measures
-
Provider acceptability measures.
Search methods for identification of studies
Electronic searches
In February 2014, we conducted computerized searches of the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE using PubMed, POPLINE and LILACS. In addition, we searched for recent clinical trials through ClinicalTrials.gov and the International Clinical Trials Registry Platform (ICTRP). The strategies are given in Appendix 1. The earlier strategies, which also included EMBASE, are shown in Appendix 2.
Searching other resources
For the initial review, we obtained relevant randomized and controlled trials from a search of publications describing vasectomy techniques for male sterilization. We searched the reference lists of all identified studies for additional, previously unidentified trials. Relevant book chapters and review articles were searched for all relevant trials. In addition, we attempted to find unpublished randomized controlled trials through personal communication with experts.
Data collection and analysis
Selection of studies
Two authors assessed the titles and abstracts from our literature search and evaluated copies of all possibly relevant articles to determine eligibility. Discrepancies were resolved by discussion.
Data extraction and management
Two authors independently collected the data under unblinded conditions (Berlin 1997). In addition to the outcome measures, we systematically extracted data on the following variables: loss to follow up, study duration, location of health care setting, experience level and number of surgeons, age of the men, total number of men included, inclusion and exclusion criteria, and method of vas occlusion. Discrepancies were resolved by discussion or by consulting a third author. When necessary, we contacted the authors of the trials to seek additional information. Correct entry of the data was verified by one other author.
Assessment of risk of bias in included studies
We assessed the methodological quality of the eligible articles as per Higgins 2005. The assessment of the validity of studies focused on the method of generating the allocation sequence, the use and method of allocation concealment, the use and method of blinding, exclusion of participants after randomization and loss to follow up.
Data synthesis
We calculated Peto odds ratios with 95% confidence intervals for dichotomous variables using the RevMan software. If the data did not permit entry into RevMan, we qualitatively described the findings in the text.
Results
Description of studies
After evaluation of the abstracts from the searches, we excluded articles that clearly were not randomized or controlled trials or did not focus on interventions or outcomes included in this review. We retrieved copies of 55 potentially relevant trials, of which two met the inclusion criteria (Sokal 1999; Christensen 2002). We excluded six reports (Black 1989; Nirapathpongporn 1990; Black 2003; Chen 2004; Chen 2005; Song 2006). No new studies have been found since the review was first published.
The two eligible studies compared similar interventions but differed in their timing and nature of post‐operative evaluations, including the evaluation of sterility. They also differed in operator experience with the no‐scalpel technique. No surgeon in the Christensen 2002 trial had substantial experience with the technique while some (3/8) in the Sokal 1999 trial were experienced with the method.
Christensen 2002 compared vasectomy with bilateral incision versus vasectomy with no‐scalpel approach to the vas. Outcome measures included vasectomy success (defined as azoospermia at three months post‐operation), duration of procedure, pain and discomfort immediately following the procedure using visual analog scales, adverse events, need for second doctor's assistance, and conversion to a different type of procedure. Participants were mailed a survey regarding pain and wound problems after one month, and they were to return after three months for semen analysis for establishing azoospermia. Semen analysis methods were not described.
Sokal 1999 compared vasectomy (small segment of the vas excised and ligated both ends) using a no‐scalpel incision versus vasectomy with a standard incision (i.e., a double vertical incision used in Guatemala and Semarang, Indonesia and a single vertical incisions in the remaining sites). Safety was the primary outcome measure. Other measures were ease of use, duration of procedure and sterility (defined as absence of live spermatozoa). A second measure of vasectomy effectiveness (i.e., failure) was determined at the surgeons' discretion without standardized criteria between centers. Participants were to return between 3 and 15 days for post‐operative evaluation and at 10 weeks for semen analysis. Semen analysis methods were not described. The vas occlusion technique in most cases was ligation (99.8% for the no‐scalpel and 99.6% for the standard incision group). Excision of the vas segment was completed for most participants (99.7% for the no‐scalpel and 99.9% for the incision group) and ligation of both ends of the vas was performed in 99.7% of all vasectomies. Sutures were used for wound closure in 2.2% of no‐scalpel and 28.9% of standard incision procedures.
Risk of bias in included studies
Christensen 2002 was a small (N=100) randomized controlled trial using sealed, sequentially‐numbered envelopes. Blinding was not reported for the outcome assessors or participants. Two randomization envelopes were opened by mistake (both for no‐scalpel arm) and were not replaced. One post‐randomization exclusion was reported (no‐scalpel arm) for a case with high testis due to inability to perform vasectomy under local anesthetic. Two men assigned to the no‐scalpel group were converted to bilateral incision during the procedure but, consistent with intent‐to‐treat principle, they were analyzed according to their randomized group (i.e., not treatment group). The study had a high loss to follow up at the one‐month survey (13%) and at the three‐month assessment for azoospermia (74%), which could have biased the study results greatly.
Sokal 1999 conducted a large randomized controlled trial (N=1429) using randomly‐generated numbers, and opaque, sealed envelopes to conceal the allocation process. Although the outcome assessor was blinded as to the group assignments, the participant blinding was unclear. After randomization, 35 men failed to receive their assigned type of incision due to allocation errors (N=17) or intraoperative obstacles (N=8). The primary analysis included participants with protocol violations, random allocation errors or technical failures (except for the exclusion of one technical failure that used different approaches on each vas). However, the analysis groups were based on the treatment received instead of the randomized assignment (N=705 for the no‐scalpel group and N=723 for the standard incision group). The follow‐up rates were about 77% for short‐term (at 15 days post‐vasectomy) and 91% for long‐term (after 15 days post‐vasectomy).
Both trials were conducted by non‐profit organizations.
Effects of interventions
Although the smaller study did not find any significant difference in perioperative bleeding (Christensen 2002), the no‐scalpel group in the larger trial (Sokal 1999) was half as likely to bleed during surgery as the scalpel group (OR 0.49; 95% CI 0.27 to 0.89). Furthermore, both studies found less hematoma during follow up for the men who received the no‐scalpel technique than those who had the standard incision (OR 0.23; 95% CI 0.15 to 0.36).
Christensen 2002 reported that the median operating times for the no‐scalpel and incisional groups (20 and 24 minutes, respectively) were not significantly different, but provided only the P value without any measure of the precision of the estimates. In contrast, the larger trial of Sokal 1999 showed that the no‐scalpel technique required less surgery time. The no‐scalpel group was more likely to have an operation time of 6 minutes or less (OR 2.37; 95% CI 1.92 to 2.91) and less likely to be 11 minutes or longer in duration (OR 0.56; 95% CI 0.43 to 0.73) than the incisional group (Sokal 1999). The 6 and 11 minute cut points, though, were selected post hoc.Christensen 2002 did not find significant differences between groups in perioperative difficulties (i.e., tight ductus, difficulty in identifying the ductus, hydrocele testis, need for assistance from a second operator). However, Sokal 1999 reported more difficulty isolating the vas (OR 1.80; 95% CI 1.18 to 2.76), short scrotum or thin deferens, and adhesions for this group compared to the scalpel group despite the shorter operation time with the no‐scalpel approach. The no‐scalpel group, though, was less likely to have (unspecified) equipment difficulties than the scalpel group (OR 0.28; 95% CI 0.10 to 0.77) (Sokal 1999). No statistically significant differences were observed for difficulty entering the scrotum, closing the incision, occluding the vas, difficulties due to fatty, adipose or fibrous tissue, chronic infection, pain or patient restlessness (only P value was provided) (Sokal 1999).
The no‐scalpel group was less likely to report perioperative pain than the incisional group (OR 0.75; 95% CI 0.61 to 0.93) in the larger trial (Sokal 1999). In contrast, the smaller study found no differences in visual analog scale scores for perioperative pain or discomfort between the two groups (Christensen 2002). Similarly, no differences in the reporting during follow up of general pain, scrotal pain or pain at ejaculation was found for the smaller study (Christensen 2002). In the larger trial (Sokal 1999), the no‐scalpel group was less likely to report scrotal pain (OR 0.63; 95% CI 0.50 to 0.80) than the standard incision group. The no‐scalpel group in the larger trial (Sokal 1999) also had less incisional infection during follow up than the scalpel group (OR 0.21; 95% CI 0.06 to 0.78). The smaller trial found no statistically significant difference in infection or wound problems (Christensen 2002). Pain or tenderness was the most common long‐term (i.e., at least 15 days post‐operation) side effect reported in Sokal 1999, but the outcome did not differ significantly between groups. Three men in each group in this trial required hospitalization during the follow‐up period, of which three complications appeared to be vasectomy‐related. Sokal 1999 also found a quicker resumption of sexual intercourse among the no‐scalpel than the incision group (P < 0.05 from Kaplan‐Meier survival estimate in article). In addition, nearly 90% of the participants in both groups reported that they were 'satisfied' or 'very satisfied' with the procedure.
In the smaller trial (Christensen 2002), microscopic analysis of resected tissue showed sufficient bilateral vasectomy from 98/99 surgeries. The exception was one case of vasectomy with bilateral incision, in which the operators had difficulty identifying the right‐sided ductus deferens during the surgery, and the microscopic analysis afterwards showed missing material. Only 26 of 99 patients (13 in each group) adhered to the study protocol of returning to provide semen samples at three months post‐operation. Two cases in the scalpel group and three cases in the no‐scalpel group were determined to be insufficient vasectomy. The larger trial (Sokal 1999) found similar rates of vasectomy success for the two groups whether measured as sterility (i.e., azoospermia) (OR 0.94; 95% CI 0.50 to 1.76) or the center‐specific evaluation of vasectomy failure (OR 0.87; 95% CI 0.37 to 2.07). The authors did not find evidence of interaction by clinical sites, and they also found almost identical results when they repeated the analysis using a per‐protocol population (i.e., excluding the 108 men with protocol violations, random allocation errors or technical failures).
Discussion
Men who received the no‐scalpel method in the Sokal 1999 trial had less bleeding, hematoma, infection and pain during surgery and follow up, but they had more surgical difficulties than those who had the incisional method. Despite having more surgical difficulties (i.e., short scrotum or thin deferens, adhesions and difficulties isolating the vas), the no‐scalpel group required a shorter operation time. Men who had the no‐scalpel technique also had a quicker resumption of sexual activity. These findings are consistent with results from large, non‐randomized studies that have documented fewer hematomas and infection, as well as a shorter operation time, with the no‐scalpel than with the scalpel approach (Nirapathpongporn 1990; Li 1991). The results are also consistent with the Labrecque 2004 review of this topic. The favorable results with the no‐scalpel technique are predicated upon good training, which should be standard for all surgical services.
In contrast, the Christensen 2002 trial reported few differences between the two approaches to the vas. The authors hypothesized that the lack of demonstrable benefits with the no‐scalpel technique in their study could have been due to operator inexperience with the method. Methodological differences between the two studies also could account for the inconsistencies. The Christensen 2002 trial was small (N=100) and could have been underpowered to detect differences. Furthermore, the trial had a high loss to follow up, which could have biased the results.
Neither trial found a difference between groups in vasectomy success. The rates in the Christensen 2002 trial are unreliable, though, because most participants (74%) failed to return at the three‐month post‐vasectomy visit to give a semen sample. The authors calculated an inaccurate azoospermia estimate by using the total number of randomized men as the denominator. The tacit assumption that the men who did not return for the three‐month follow‐up visit were azoospermic is untenable. Given the low follow‐up rate, we did not calculate an estimate of the relative effectiveness of the two methods for this trial. Furthermore, the authors did not report the vas occlusion techniques used despite their potential effect on the effectiveness of the procedure. Sokal 1999 had higher follow‐up rates for the 10‐week semen analysis (87%), and did not find a difference in the measures of sterility and vasectomy failure for the two groups.

Comparison 1 No‐scalpel versus standard incision, Outcome 1 Perioperative bleeding.

Comparison 1 No‐scalpel versus standard incision, Outcome 2 Hematoma during follow up.

Comparison 1 No‐scalpel versus standard incision, Outcome 3 Operating time <=6 minutes.

Comparison 1 No‐scalpel versus standard incision, Outcome 4 Operating time >=11 min.

Comparison 1 No‐scalpel versus standard incision, Outcome 5 Perioperative difficulty in identifying ductus.

Comparison 1 No‐scalpel versus standard incision, Outcome 6 Perioperative difficulty in isolating the vas.

Comparison 1 No‐scalpel versus standard incision, Outcome 7 Perioperative equipment difficulties (unspecified).

Comparison 1 No‐scalpel versus standard incision, Outcome 8 Perioperative need for assistance from second operator.

Comparison 1 No‐scalpel versus standard incision, Outcome 9 Perioperative pain.

Comparison 1 No‐scalpel versus standard incision, Outcome 10 Pain during follow up.

Comparison 1 No‐scalpel versus standard incision, Outcome 11 Pain or tenderness during long‐term follow up.

Comparison 1 No‐scalpel versus standard incision, Outcome 12 Scrotal pain during follow up.

Comparison 1 No‐scalpel versus standard incision, Outcome 13 Pain at ejaculation during follow up.
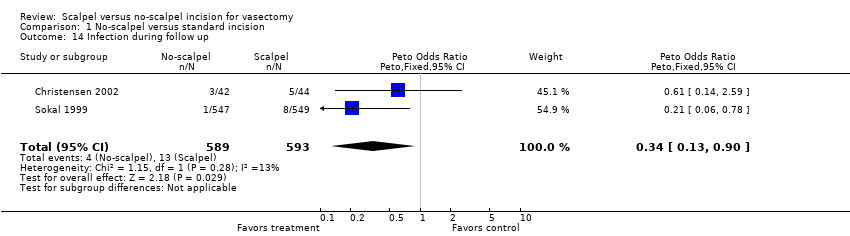
Comparison 1 No‐scalpel versus standard incision, Outcome 14 Infection during follow up.

Comparison 1 No‐scalpel versus standard incision, Outcome 15 Wound problems during follow up.
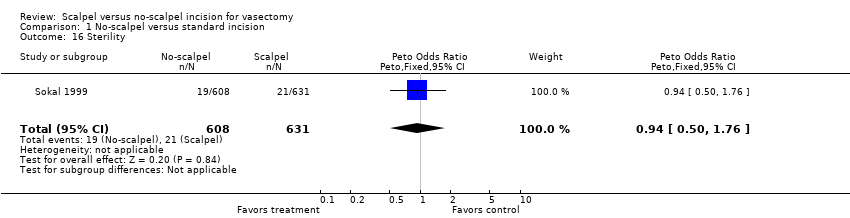
Comparison 1 No‐scalpel versus standard incision, Outcome 16 Sterility.
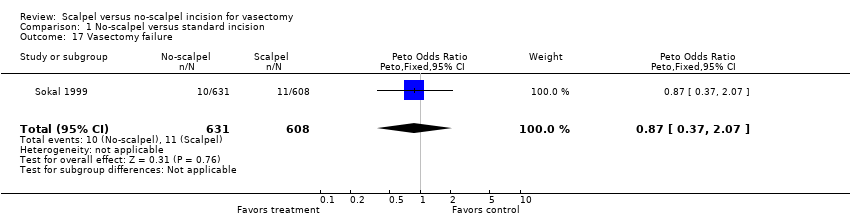
Comparison 1 No‐scalpel versus standard incision, Outcome 17 Vasectomy failure.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Perioperative bleeding Show forest plot | 2 | 1534 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.59 [0.33, 1.04] |
| 2 Hematoma during follow up Show forest plot | 2 | 1182 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.23 [0.15, 0.36] |
| 3 Operating time <=6 minutes Show forest plot | 1 | 1428 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 2.37 [1.92, 2.91] |
| 4 Operating time >=11 min Show forest plot | 1 | 1428 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.56 [0.43, 0.73] |
| 5 Perioperative difficulty in identifying ductus Show forest plot | 1 | 99 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.54 [0.05, 5.30] |
| 6 Perioperative difficulty in isolating the vas Show forest plot | 1 | 1421 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.80 [1.18, 2.76] |
| 7 Perioperative equipment difficulties (unspecified) Show forest plot | 1 | 1456 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.28 [0.10, 0.77] |
| 8 Perioperative need for assistance from second operator Show forest plot | 1 | 99 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.77 [0.67, 4.70] |
| 9 Perioperative pain Show forest plot | 1 | 1428 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.75 [0.61, 0.93] |
| 10 Pain during follow up Show forest plot | 1 | 86 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.03 [0.43, 2.52] |
| 11 Pain or tenderness during long‐term follow up Show forest plot | 1 | 1272 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.78 [0.46, 1.32] |
| 12 Scrotal pain during follow up Show forest plot | 2 | 1179 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.66 [0.52, 0.83] |
| 13 Pain at ejaculation during follow up Show forest plot | 1 | 86 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 7.94 [0.49, 129.15] |
| 14 Infection during follow up Show forest plot | 2 | 1182 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.34 [0.13, 0.90] |
| 15 Wound problems during follow up Show forest plot | 1 | 86 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.51 [0.18, 1.47] |
| 16 Sterility Show forest plot | 1 | 1239 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.94 [0.50, 1.76] |
| 17 Vasectomy failure Show forest plot | 1 | 1239 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.87 [0.37, 2.07] |