Shouldice technique versus other open techniques for inguinal hernia repair
Referencias
References to studies included in this review
References to studies excluded from this review
References to studies awaiting assessment
Additional references
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | Multicenter, two arms RCT of Shouldice vs Lichtenstein. | |
| Participants | Country: USA. | |
| Interventions | Shouldice standard (n=51) performing 4 layers. Polypropylene 2/0. | |
| Outcomes | Lenght of postoperative stay. | |
| Notes | Conflict of interest: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
| Methods | Single centre, four arms RCT ‐ comparisons: Shouldice vs Bassini (considered in this review); Bassini vs Ring Narrowing (the two arms are not considered in this review). | |
| Participants | Country: Netherlands. | |
| Interventions | Bassini modified by Stetten (n=160). Non Mesh. Nylon 2/0. | |
| Outcomes | Recurrence (lump in groin not necessarily re‐operated). | |
| Notes | Recurrence at 13.7 follow up years assessed by an independent surgeon in 179/194 hernias (four arms); 15/194 by telephone interview. 89 patients (100 hernias) died during the study. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
| Methods | Single centre, three arms RCT ‐ Conparisons: Shouldice vs Lichtenstein vs TAPP (not considered). Randomization: generation of sequence not stated, Allocation concealment using sealed envelopes. Maximum follow up: 52 months. Exclusion after randomization: no. Losses to follow up: Shouldice 19, Lichtenstein 17 (9 deaths, 5 moved to other places and 22 refused to continue). Analyses by protocol | |
| Participants | Country: Germany. Setting: centre specialized in hernia repair. Total enrolled patients: 186 (93 Shouldice vs 93 Lichtenstein). Mean age: Shouldice: 53; Lichtenstein 56. Gender: 186 M. Inclusion criteria: age >18, primary inguinal hernia, elective repair. Exclusion criteria: no known. Demographic and baseline data reported: comparability for age, type of hernia. | |
| Interventions | Shouldice (n=93). Technical notes not specified. Lictenstein standard (n=93). | |
| Outcomes | Recurrence (definition of recurrence not reported). Chronic pain (data from Koninger 2004). Postoperative satisfaction level Testicular atrophy | |
| Notes | 52 months follow up assessed by a resident surgeon by physical examination in 150 patients (80.6%) Conflict of interest: not reported. Sources of funding: not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
| Methods | Single centre, two arms RCT of Shouldice vs Lichtenstein. | |
| Participants | Country: Sweden. | |
| Interventions | Shouldice standard (n=89) performing 4 layers. Non‐absorbable monofilament. | |
| Outcomes | Recurrence (symptomatic lump in groin and re operated). | |
| Notes | Recurrence at 1 year follow up assessed by surgeon or patient himself in 170 patients (84 Shouldice; 86 Lichtenstein). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
| Methods | Multicenter, four arms RCT ‐ comparisons: Shouldice steel and Shouldice polypropylene (pooled together) vs Bassini vs Mc Vay. | |
| Participants | Country: France. | |
| Interventions | Shouldice steel (n=401). 4 layers. Steel wire and polypropylene. | |
| Outcomes | Recurrences (lump in groin not necessarily re operated) ‐ data not extractable | |
| Notes | Recurrence at 8,5 years follow up assessed by an independent surgeon or patient himself or physician. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
| Methods | Multicenter, two arms RCT of Shouldice vs Lichtenstein. | |
| Participants | Country: Switzerland. | |
| Interventions | Shouldice Standard (n=171). 4 layers. PDS 2/0. | |
| Outcomes | Lenght of postoperative stay. | |
| Notes | Conflict of interest: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
| Methods | Single centre, two arms RCT of Shouldice vs Plication Darn (Bassini modified). | |
| Participants | Country: UK. | |
| Interventions | Shouldice (n=151). Technical notes not specified. | |
| Outcomes | Recurrence (definition of recurrence not reported). | |
| Notes | Recurrence at 2 years follow up assessed by a consultant or a surgical registrar or pro forma in 224 patients. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
| Methods | Single centre, two arms RCT of Shouldice vs Bassini‐Kirschner. | |
| Participants | Country: Hungary. | |
| Interventions | Shouldice standard (n=63) performing 4 layers. Non‐absorbable monofilament. | |
| Outcomes | Recurrence (lump in groin and re operated). | |
| Notes | Recurrence at 1 year follow up assessed by a hospital staff surgeon in 85 patients (66%). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
| Methods | Single centre, four arms RCT ‐ comparison: Shouldice vs Bassini (Bassini with absorbable sutures and two‐layers Shouldice not considered). | |
| Participants | Country: Austria. | |
| Interventions | Shouldice standard (n=160). 4 layers. Polypropylene. | |
| Outcomes | Recurrence (lump in groin not necessarily re operated). | |
| Notes | Recurrence at 2 years follow up assessed by a hospital staff surgeon in 683 patients(93,6%). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
| Methods | Single centre, two arms RCT of Shouldice vs Lichtenstein. | |
| Participants | Country: USA | |
| Interventions | Shouldice standard (n=337) performing 4 layers. Non‐absorbable monofilament. | |
| Outcomes | Recurrence | |
| Notes | Recurrence at 5 years follow up assessed by the operating surgeon in 99% of patients. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
| Methods | Single centre, three arms RCT of Shouldice vs Lichtenstein vs Mc Vay. | |
| Participants | Country: USA. | |
| Interventions | Shouldice modified (n=41). 4 layers. Polypropylene. | |
| Outcomes | Recurrence (lump in groin not necessarily re‐operated). | |
| Notes | Recurrence at 6‐9 years follow up assessed by clinical examination in 121 patients(29 lost at follow up). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
| Methods | Single centre, two arms RCT of Shouldice vs Lichtenstein. | |
| Participants | Country: Sweden. | |
| Interventions | Shouldice Standard (n=148). 4 layers. Polypropylene 2/0. | |
| Outcomes | Recurrence (lump in groin not necessarily re operated). | |
| Notes | Recurrence at 3‐6 years follow up assessed by an independent surgeon in 284 patients. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
| Methods | Single centre, two arms RCT of Shouldice vs Bassini. | |
| Participants | Country: Germany. | |
| Interventions | Shouldice modified (n=119). 4 layers. unabsorbable suture. | |
| Outcomes | Recurrence (symptomatic lump in groin and re operated). | |
| Notes | Recurrence at 3 years follow up assessed by clinical examination in 91,5%of Shouldice group and 92,6% of Bassini group. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
| Methods | Single centre, two arms RCT of Shouldice vs Moloney's Darn. | |
| Participants | Country: India. | |
| Interventions | Shouldice standard (n=25). 4 layers. unabsorbable suture. | |
| Outcomes | Recurrence (lump in groin not necessarily re operated). | |
| Notes | Conflict of interest: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
| Methods | Single centre, two arms RCT of Shouldice vs Bassini‐Kirschner. | |
| Participants | Country: Germany. | |
| Interventions | Shouldice unclear (n=70). | |
| Outcomes | Recurrence (lump in groin not necessarily re operated). | |
| Notes | Recurrence at 24 months follow up assessed by a general physician or one of the author in 128 patients. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
| Methods | Single centre, three arms RCT ‐ comparisons: Shouldice vs Plug and patch vs TAPP (not considered for the analyses). | |
| Participants | Country: Germany. | |
| Interventions | Shouldice modified (n=80). 4 layers. Unabsorbable monofilament. | |
| Outcomes | Recurrence (method not stated). | |
| Notes | Recurrence at 25 months assessed for 96% of Shouldice group and 94% of Plug and Patch. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
| Comment to Kingsnorth 1992 | |
| Review | |
| Comparison about different suture materials | |
| Comment to Kingsnorth 1992 | |
| No comparisons between surgical techniques | |
| CCT | |
| CCT | |
| Comment on Kingsnorth 1992 | |
| Data considered in Butters 2007 | |
| Comment to Kingsnorth 1992 | |
| Comment to Schrenk 1996 | |
| Data reprised in Paul 1994 | |
| Out of topic | |
| Letter to Paul 1994 | |
| Comment to Kingsnorth 1992 |
Characteristics of studies awaiting assessment [ordered by study ID]
| Methods | RCT |
| Participants | 280 patients |
| Interventions | Shouldice, Lichtenstein, TAPP |
| Outcomes | Recurrence, Duration of Operation, Wound infection, Complications |
| Notes |
| Methods | RCT |
| Participants | 209 patients |
| Interventions | Shouldice, Lichtenstein |
| Outcomes | Recurrence, Postoperative pain |
| Notes |
| Methods | RCT |
| Participants | 119 patients |
| Interventions | Shouldice, Bassini, Mc Vay |
| Outcomes | Recurrence |
| Notes |
| Methods | RCT |
| Participants | 269 |
| Interventions | Shouldice, Mc Vay |
| Outcomes | Recurrence |
| Notes |
| Methods | RCT |
| Participants | 54 patients |
| Interventions | Shouldice, Lichtenstein |
| Outcomes | Duration of operation, Lenght of postoperative stay, Costs |
| Notes |
| Methods | No data available |
| Participants | No data available |
| Interventions | No data available |
| Outcomes | No data available |
| Notes |
| Methods | RCT |
| Participants | 64 patients |
| Interventions | Shouldice, Tension‐free |
| Outcomes | Postoperative pain, Complications |
| Notes |
| Methods | No data available |
| Participants | No data available |
| Interventions | No data available |
| Outcomes | No data available |
| Notes |
| Methods | RCT |
| Participants | Shouldice, Bassini, Mc Vay |
| Interventions | 324 |
| Outcomes | Recurrence, Complications |
| Notes |
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Recurrence Show forest plot | 13 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| Analysis 1.1  Comparison 1 Shouldice vs other techniques, Outcome 1 Recurrence. | ||||
| 1.1 Shouldice vs mesh | 6 | 1565 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 3.80 [1.99, 7.26] |
| 1.2 Shouldice vs non‐mesh | 8 | 2865 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.62 [0.45, 0.85] |
| 2 Lenght of postoperative stay (days) Show forest plot | 8 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 1.2  Comparison 1 Shouldice vs other techniques, Outcome 2 Lenght of postoperative stay (days). | ||||
| 2.1 Shouldice vs mesh | 4 | 1045 | Mean Difference (IV, Random, 95% CI) | 0.38 [‐0.41, 1.18] |
| 2.2 Shouldice vs non mesh | 4 | 565 | Mean Difference (IV, Random, 95% CI) | 0.25 [0.01, 0.49] |
| 3 Chronic pain Show forest plot | 7 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| Analysis 1.3  Comparison 1 Shouldice vs other techniques, Outcome 3 Chronic pain. | ||||
| 3.1 Shouldice vs mesh | 5 | 1371 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.87 [0.55, 1.39] |
| 3.2 Shouldice vs non mesh | 3 | 1968 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.70 [0.40, 1.22] |
| 4 Wound Infection Show forest plot | 13 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| Analysis 1.4  Comparison 1 Shouldice vs other techniques, Outcome 4 Wound Infection. | ||||
| 4.1 Shouldice vs mesh | 7 | 1938 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.74 [0.37, 1.49] |
| 4.2 Shouldice vs non mesh | 7 | 2635 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.34 [0.70, 2.54] |
| 5 Seroma Show forest plot | 4 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| Analysis 1.5  Comparison 1 Shouldice vs other techniques, Outcome 5 Seroma. | ||||
| 5.1 Shouldice vs mesh | 3 | 1165 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.96 [0.37, 2.50] |
| 5.2 Shouldice vs non mesh | 1 | 142 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 2.86 [0.39, 20.74] |
| 6 Testicular atrophy Show forest plot | 6 | Odds Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 1.6  Comparison 1 Shouldice vs other techniques, Outcome 6 Testicular atrophy. | ||||
| 6.1 Shouldice vs mesh | 3 | 1155 | Odds Ratio (M‐H, Random, 95% CI) | 1.05 [0.04, 27.38] |
| 6.2 Shouldice vs non mesh | 3 | 1995 | Odds Ratio (M‐H, Random, 95% CI) | 1.09 [0.21, 5.50] |
| 7 Haematoma Show forest plot | 10 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| Analysis 1.7  Comparison 1 Shouldice vs other techniques, Outcome 7 Haematoma. | ||||
| 7.1 Shouldice vs mesh | 3 | 562 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.64 [0.25, 1.64] |
| 7.2 Shouldice vs non mesh | 7 | 2797 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.84 [0.63, 1.13] |
| 8 Duration of the operation (Minutes) Show forest plot | 7 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
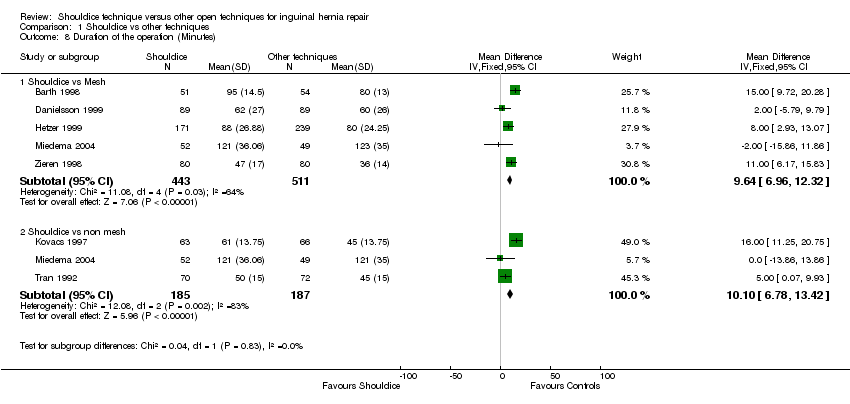
| Analysis 1.8  Comparison 1 Shouldice vs other techniques, Outcome 8 Duration of the operation (Minutes). | ||||
| 8.1 Shouldice vs Mesh | 5 | 954 | Mean Difference (IV, Fixed, 95% CI) | 9.64 [6.96, 12.32] |
| 8.2 Shouldice vs non mesh | 3 | 372 | Mean Difference (IV, Fixed, 95% CI) | 10.10 [6.78, 13.42] |

Comparison 1 Shouldice vs other techniques, Outcome 1 Recurrence.

Comparison 1 Shouldice vs other techniques, Outcome 2 Lenght of postoperative stay (days).

Comparison 1 Shouldice vs other techniques, Outcome 3 Chronic pain.

Comparison 1 Shouldice vs other techniques, Outcome 4 Wound Infection.

Comparison 1 Shouldice vs other techniques, Outcome 5 Seroma.

Comparison 1 Shouldice vs other techniques, Outcome 6 Testicular atrophy.

Comparison 1 Shouldice vs other techniques, Outcome 7 Haematoma.
Comparison 1 Shouldice vs other techniques, Outcome 8 Duration of the operation (Minutes).
| Study | Randomization | Double‐blinding | Dropout/Withdrawls | TotalScore |
| Barth | 1 | 0 | 0 | 1 |
| Beets | 2 | 2 | 0 | 4 |
| Butters | 2 | 1 | 1 | 3 |
| Danielsson | 1 | 0 | 1 | 2 |
| Hay | 2 | 1 | 0 | 3 |
| Hetzer | 0 | 0 | 1 | 1 |
| Kingsnorth | 2 | 1 | 0 | 3 |
| Kovacs | 0 | 1 | 1 | 2 |
| Kux | 0 | 1 | 1 | 2 |
| McGillicuddy | 0 | 0 | 1 | 1 |
| Miedema | 2 | 1 | 1 | 4 |
| Nordin | 1 | 2 | 0 | 3 |
| Paul | 1 | 1 | 0 | 2 |
| Thapar | 1 | 0 | 1 | 2 |
| Tran | 1 | 0 | 0 | 1 |
| Zieren | 1 | 1 | 1 | 3 |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Recurrence Show forest plot | 13 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| 1.1 Shouldice vs mesh | 6 | 1565 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 3.80 [1.99, 7.26] |
| 1.2 Shouldice vs non‐mesh | 8 | 2865 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.62 [0.45, 0.85] |
| 2 Lenght of postoperative stay (days) Show forest plot | 8 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 Shouldice vs mesh | 4 | 1045 | Mean Difference (IV, Random, 95% CI) | 0.38 [‐0.41, 1.18] |
| 2.2 Shouldice vs non mesh | 4 | 565 | Mean Difference (IV, Random, 95% CI) | 0.25 [0.01, 0.49] |
| 3 Chronic pain Show forest plot | 7 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| 3.1 Shouldice vs mesh | 5 | 1371 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.87 [0.55, 1.39] |
| 3.2 Shouldice vs non mesh | 3 | 1968 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.70 [0.40, 1.22] |
| 4 Wound Infection Show forest plot | 13 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| 4.1 Shouldice vs mesh | 7 | 1938 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.74 [0.37, 1.49] |
| 4.2 Shouldice vs non mesh | 7 | 2635 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.34 [0.70, 2.54] |
| 5 Seroma Show forest plot | 4 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| 5.1 Shouldice vs mesh | 3 | 1165 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.96 [0.37, 2.50] |
| 5.2 Shouldice vs non mesh | 1 | 142 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 2.86 [0.39, 20.74] |
| 6 Testicular atrophy Show forest plot | 6 | Odds Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 6.1 Shouldice vs mesh | 3 | 1155 | Odds Ratio (M‐H, Random, 95% CI) | 1.05 [0.04, 27.38] |
| 6.2 Shouldice vs non mesh | 3 | 1995 | Odds Ratio (M‐H, Random, 95% CI) | 1.09 [0.21, 5.50] |
| 7 Haematoma Show forest plot | 10 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| 7.1 Shouldice vs mesh | 3 | 562 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.64 [0.25, 1.64] |
| 7.2 Shouldice vs non mesh | 7 | 2797 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.84 [0.63, 1.13] |
| 8 Duration of the operation (Minutes) Show forest plot | 7 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 8.1 Shouldice vs Mesh | 5 | 954 | Mean Difference (IV, Fixed, 95% CI) | 9.64 [6.96, 12.32] |
| 8.2 Shouldice vs non mesh | 3 | 372 | Mean Difference (IV, Fixed, 95% CI) | 10.10 [6.78, 13.42] |