Tratamiento de mantenimiento con fármacos antipsicóticos para la esquizofrenia
References
References to studies included in this review
References to studies excluded from this review
References to ongoing studies
Additional references
References to other published versions of this review
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Jump to:
| Methods | Randomisation: randomised, no further details. | |
| Participants | Diagnosis: schizophrenia (clinical diagnosis), continuously in hospital for at least 6 years (mean 28 years). | |
| Interventions | 1. Drug: Chlorpromazine ‐ mean dose: 216mg/day. N=15. Allowed dose range: the participants were kept on their initial dose. 2. Placebo: Duration of taper 0 days. N=17. Rescue medication: benzodiazepines, anticholinergics. | |
| Outcomes | Examined: Relapse (need of antipsychotic medication). Leaving the study early. Unable to use / Not included: Behaviour: Ward Behaviour Rating Scale of Wing (no SD / no prespecified outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, no further details. |
| Allocation concealment (selection bias) | Low risk | Pharmacists held the key. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules. |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the trial. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No obvious other bias. |
| Methods | Randomisation: random, computer‐generated randomisation code. | |
| Participants | Diagnosis: chronic, stable schizophrenia (DSM‐III‐R), less than markedly ill on Clinical Global Impression Scale. N=278. | |
| Interventions | 1. Drug: ziprasidone ‐ Fixed doses of 40, 80 or 160 mg/day.** N=207. 2. Placebo: Duration of taper <3 days. N=71. Rescue medication: anticholinergics, lorazepam, temazepam, no additional antipsychotic medication. | |
| Outcomes | Examined: Relapse: (Clinical Global Impressionof much worse or more, PANSS items hostility or uncooperativeness > 6, or in need for additional treatment for exacerbation of symptoms). Leaving the study early. Adverse events: binary outcome for generel, specific (movement disorders) ‐ interviews. Unable to use / Not included: Mental state: PANSS total score and subscores (no predefined outcome of interest). Global state: much worse or more ‐ Clinical Global Impression Severity Scale (no prespecified outcome of interest). Functioning: Global Assessment of Functioning Scale (no prespecified outcome of interest). Adverse effects: extrapyramidal symptoms (Simpson Angus Scale, Barnes Akathisia Scale, Abnormal Involuntary Movements Scale ‐ all no SD / continous side‐effect results were not among the prespecified outcomes of interest). Physiological measures: ECG, vital signs, weight, ophthalmological assessment, lab tests (all no SD, no data / not prespecified outcomes of interest). | |
| Notes | ** The results of the three dose groups were pooled. 16 participants from one centre were excluded due to protocol violations. Intention‐to‐treat were only those participants who had received at least one dose. How many did not receive one dose is unclear. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised, computer‐generated randomised code. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | High risk | 64% of the participants left the study early, most due to relapse. The rate was higher in the placebo group (86%) than in the medication group (˜57%). This was probably not a problem for the primary outcome relapse, but for secondary outcomes for which the last‐observation‐carried‐forward method was used. Appropriate survival curve analysis was used for the primary outcome relapse. |
| Selective reporting (reporting bias) | Low risk | No selective reporting. |
| Other bias | Low risk | No obvious other bias. |
| Methods | Randomisation: matched pairs were formed and then randomised, no further details. | |
| Participants | Diagnosis: chronic psychotic hospitalised patients mainly with schizophrenic and paranoid behaviour patterns, suspected of relapsing after withdrawal of medication (clinical diagnosis). | |
| Interventions | 1. Drug: penfluridol once weekly ‐ Fixed dose, mean dose: n.i., range 10‐40mg/weekly. N=13. 2. Placebo: Duration of taper: 0 days. N=13. Rescue medication: sedative neuroleptics allowed for 2 weeks, dexbenzitide. | |
| Outcomes | Examined: Relapse: need of medication as decided by two psychiatrists. Unable to use / Not included: Mental state: Psychiatric Evaluation Scale (no predefined outcome of interest). Adverse effects: movement disorders (Factor Construct Outcome Scale, no data for randomised phase / continous side‐effect results were not among the prespecified outcomes of interest), neurologic effects (graphometric and tapping test, no data for randomised phase / no prespecified outcomes of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Matched pairs were formed and then randomised, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, indistinguishable placebo. |
| Blinding (performance bias and detection bias) | Low risk | Double, indistinguishable placebo. |
| Incomplete outcome data (attrition bias) | Low risk | Apart from those participants who relapsed no participant left the study early and relapse was the only outcome. |
| Selective reporting (reporting bias) | High risk | Adverse events were not reported for the double‐blind phase. |
| Other bias | Low risk | No obvious other bias. |
| Methods | Randomisation: randomised, 2:1 ratio, by an interactive voice response system. | |
| Participants | Diagnosis: schizophrenia (n=266) or schizoaffective disorder (n=60, DSM‐IV). BPRS total score <36, positive symptoms at most mild, Global Assessment of Functioning at least 40, currently on maintenance antipsychotic medication. N=326. | |
| Interventions | Participants were first converted to olanzapine and then stabilized for 8 weeks before randomisation. 1. Drug: olanzapine ‐ Fixed dose of either 10, 15 or 20 mg/day. Mean dose 13.4 mg/day. N=224. 2. Placebo: Duration of taper: 0 days. N=102. Rescue medication: a one time increase of the same medication (olanzapine or placebo) was allowed. Furthermore, antiparkinson medication and benzodiazepines were allowed. | |
| Outcomes | Examined: Relapse: any BPRS positive item > 4, absolute increase of a positive item or of the positive subscore, hospitalisation due to positive symptoms, suicide or suicide attempt. Leaving the study early. Adverse effects: binary outcomes for general, specific (movement disorders) ‐ open interviews. Quality of life: Heinrich Carpenter Quality of Life Scale. Unable to use / Not included: Mental state: PANSS (no prespecified outcome of interest). Adverse effects: adverse effects with an incidence < 10% (no data), laboratory, EPS‐scales (in part no data / no prespecified outcome of interest), EPS‐scales (no SD / continous side‐effect results were not among the prespecified outcomes). Physiological measures: vital signs (no prespecified outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised, 2:1 ratio, by an interactive voice response system. |
| Allocation concealment (selection bias) | Low risk | Interactive voice response system. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | High risk | The overall attrition of 26% was acceptable, but many more participants in the placebo group than in the olanzapine group left the study early. Kaplan‐Meier survival analysis was used for the analysis of relapse, ANOVA based on last‐observation‐carried‐forward was used for continuous outcomes. |
| Selective reporting (reporting bias) | High risk | Only those adverse events with a frequency of at least 10% were reported. Use of antiparkinson medication has not been reported. |
| Other bias | High risk | The study was terminated early when there was a sufficient difference, but this was preplanned. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (clinical diagnosis). N=45. | |
| Interventions | 1. Drug: prochlorpromazine, perphenazine, chlorpromazine, promazine or trifluoperazine. Fixed doses continued with the same drug and dose taken before the study. Mean dose: n.i. N=30. 2. Placebo: Duration of taper: 0 days. N=15*. Rescue medication: not allowed. | |
| Outcomes | Examined: Relapse (need of medication or deterioriation of state or transfer to closed ward) Unable to use / Not included: Behaviour: Patient Adjustment Report (no prespecified outcome of interest). Mental state: Taylor Manifest Anxiety Scale (no prespecified outcome of interest). | |
| Notes | * Another 15 participants were treated only for 8 weeks with placebo and then switched back to their initial antipsychotic drug. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | High risk | Double, thiamine chloride used as placebo, participants and nurses were told that a new medication was given, but nurses soon new that this was a placebo. |
| Blinding (performance bias and detection bias) | Low risk | Double, thiamine chloride used as placebo, participants and nurses were told that a new medication was given, but nurses soon new that this was a placebo. |
| Incomplete outcome data (attrition bias) | Low risk | Only completers were included in the statistical analysis, but because the drop‐out rate was only 13% we did not consider this a source of bias. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear other risk of bias. |
| Methods | Randomisation: An independent rater created randomisation lists stratified for gender with randomly permuted blocks of 4 allocation groups. Allocation: procedure not described. | |
| Participants | Diagnosis: first episode schizophrenia (DSM‐IV). N=20. | |
| Interventions | 1. Drug: olanzapine, risperidone, quetiapine, zuclopenthixol. Flexible doses. Mean dose: n.i. N=9. 2. No treatment: Duration of taper: 6‐12 weeks. N=11. Rescue medication: not indicated. | |
| Outcomes | Examined: Relapse: clinicial judgement. Leaving the study early. Rehospitalisation. | |
| Notes | Sponsor: The Netherlands Organisation for Health Research and Development and EliLilly. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | An independent rater created randomisation lists stratified for gender with randomly permuted blocks of 4 allocation groups. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | High risk | Open study. |
| Blinding (performance bias and detection bias) | Low risk | Open study. |
| Incomplete outcome data (attrition bias) | Low risk | 5 out of 20 participants left the study early (25%). Probably an acceptable rate, there was no big difference between drug and placebo group. Kaplan‐Meier survival curves were used for the primary outcome relapse. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | High risk | Premature termination after interim analysis. |
| Methods | Randomisation: randomised, no further details. | |
| Participants | Diagnosis: schizophrenia (clinical diagnosis), one third paranoid subtype, without central nervous system disease, without lobotomy. N=259. | |
| Interventions | 1. Drug: chlorpromazine or thioridazine.* Fixed dose, continuation of the dose given in the stabilization phase. Mean dose: chlorpromazine mean 400mg/day, thioridazine mean 350mg/day. N=88. 2. Placebo: Duration of taper: 1 ‐ 8 days. N=171. Rescue medication: not indicated. | |
| Outcomes | Examined: Relapse: definitive worsening of the condition and medication again necessary, usually joint decision of treatment team. Unable to use / Not included: Mental state: Inpatient Multidimensional Psychiatric Scale (no prespecified outcome of interest). Behaviour: Psychotic Reaction Profile Scale (no prespecified outcome of interest). | |
| Notes | * There was another group which received half the original dose. It was not considered in this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | High risk | Double, identical tablets. However, placebo dose reduction group received medication only every other day. Therefore, blinding was not fully maintained. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical tablets. However, placebo dose reduction group received medication only every other day. Therefore, blinding was not fully maintained. |
| Incomplete outcome data (attrition bias) | Unclear risk | It is unclear whether there were dropouts or whether the authors analysed only study completers. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Unclear risk | 22 participants who had relapsed in the first 8 weeks were entered in the study again. As the number is small, it is unclear whether they affected the results. |
| Methods | Randomisation: n.i., but double‐blind study. | |
| Participants | Diagnosis: chronic schizophrenia (DSM‐III), all on maintenance medication for control of continuous symptoms, all stable for at least 6 months. N=30. | |
| Interventions | 1. Drug: penfluridol. Fixed dose of 55mg/week. N=15. 2. Placebo: Duration of taper: 0 days. N=15. Rescue medication: antiparkinson medication and haloperidol, but this was considered to be a relapse. | |
| Outcomes | Examined: Relapse (need of additional haloperidol medication). Unable to use / Not included: Mental state (Scale for the Assessment of Positive Symptoms and Negative Symptoms ‐ no data /no predefined outcome of interest). Adverse effects: extrapyramidal side‐effects (Simpson Angus Scale ‐ no data / continuous side‐effect results were not among the prespecified outcomes). Physiological measures: mean body weight, pulse rate, blood pressure, laboratory (all no data / no prespecified outcomes of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | N.i., but double‐blind study. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules. |
| Incomplete outcome data (attrition bias) | Low risk | Only study completers were used in the final analysis, but as there were only two dropouts (one in each group) this was not necessarily a problem. |
| Selective reporting (reporting bias) | Low risk | Rating scale results were not reported, but these were not of interest for the review. |
| Other bias | Low risk | No clear evidence for other bias. |
| Methods | Randomisation: sequence by computer, fixed block size of four without stratification. | |
| Participants | Diagnosis: schizophrenia and related psychoses (DSM‐IV), all first episode, all well remitted, all had remained well on maintenance medication for 1 year. N=178. | |
| Interventions | 1. Drug: quetiapine. Fixed dose of 400mg/day. N=89. 2. Placebo: Duration of taper (days): 35. N=89. Rescue medication: antipsychotics not allowed. | |
| Outcomes | Examined: Relapse: (i) an increase in at least one of the following Positive and Negative Syndrome Scale psychotic symptom items to a threshold score (delusion, hallucinatory behaviour, conceptual disorganisation, unusual thought content, suspiciousness; (ii) Clinical Global Impression Severity of Illness 3 or above and (iii) CGI change 5 or above). Leaving the study early. Rehospitalisation. Suicide attempts. Adverse effects: akathisia, tardive dyskinesia, tremor, sedation, weight gain. Open employment status. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Sequence by computer, fixed block size of four without stratification. |
| Allocation concealment (selection bias) | Low risk | AstraZeneca prepared individually numbered sets of study drugs, packed them according to the randomisation sequence and then shipped them to the study team in numbered but apparently identical capsules. |
| Blinding (performance bias and detection bias) | Unclear risk | Identical capsules, "investigators, patients and all research staff were blind to the study drugs and the block size". |
| Blinding (performance bias and detection bias) | Low risk | Identical capsules, "investigators, patients and all research staff were blind to the study drugs and the block size". |
| Incomplete outcome data (attrition bias) | High risk | 72% of the participants left the study early. As most participants dropped out after relapse this outcome was not affected, but it is a source of bias for other outcomes. Survival analysis for the primary outcome relapse. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear other bias. |
| Methods | Randomisation: randomly in group of 15 each, no further details. | |
| Participants | Diagnosis: schizophrenia (mainly Schneiderian first‐rank symptoms), last relapse 30‐60 months ago, fully remitted since and maintained on antipsychotic drugs. N=30. | |
| Interventions | 1. Drug: switched to various antipsychotic drugs with similar profile as the previous one. Fixed/flexible dose: probably flexible. Allowed dose range: n.i.. Mean dose: n.i.. N=15. 2. Placebo: benzodiazepine (‘active placebo’). Duration of taper 0 days. N=15. Rescue medication: n.i.. | |
| Outcomes | Examined: Relapse: recurrence of symptoms definitely of schizophrenic type, or symptoms not diagnostic of schizophrenia (e.g. sleep problems) which could not be controlled with other measures than antipsychotic drugs or ECT. Leaving the study early. Quality of life: subjective distress (Symptom Questionnaire of Kellner and Sheffield). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomly in group of 15 each, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | High risk | 12 participants left the study early (40%), among those 10 from the placebo group and 8 for relapse. Outcomes other than relapse and leaving early are clearly prone to bias due to this difference in leaving the study early. |
| Selective reporting (reporting bias) | Low risk | Use of benzodiazepines was not indicated, but this was not an outcome of interest in our review. |
| Other bias | Low risk | No evidence for other bias. |
| Methods | Randomisation: random, in blocks of eight, stratified for age, duration ill and time since last admission. | |
| Participants | Diagnosis: chronic schizophrenia (clinical diagnosis), 22 undifferentiated, 7 paranoid, 1 schizoaffective, no severe other psychiatric or somatic illnesses, no severely ill participants. N=40. | |
| Interventions | 1. Drug: pimozide.* Flexible dose. Allowed dose range: 2‐20mg/day. Mean dose: 5.3 mg/day. N=15. 2. Drug: thioridazine.* Flexible dose. Allowed dose range: 75‐750mg/day. Mean dose: 189mg/day. N=15. 3. Placebo: Duration of taper: 0 days. N=10. Rescue medication: antiparkinson medication, bedside sedation. | |
| Outcomes | Examined: Relapse (worsening of global state). Leaving early. Global state: number of participants improved according to Clinical Global Impressions Scale. Adverse effects: binary outcomes ‐ open interview. Unable to use / Not included: Mental state: BPRS (no SD / no prespecified outcome of interest). Functioning: Katz Lyerly Scale of Social Adjustment, Patient Rating Form, Family Rating Form (all no SD / no prespecified outcomes of interest). Physiological measures: biological parameters (temperature, mean weight, pulse, blood pressure, all no data / all no prespecified outcomes of interest), laboratory (blood count, urine analysis, liver enzymes, blood sugar, protein bound iodine, all no prespecified outcomes of interest). | |
| Notes | * The results of pimozide and thioridazine were combined in the analysis. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random, in blocks of eight, stratified for age, duration ill and time since last admission. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules, each participant had an individual stock bottle. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules, each participant had an individual stock bottle. |
| Incomplete outcome data (attrition bias) | High risk | Overall 36% left the study early. The specific reasons why the participants dropped out were not indicated by group. |
| Selective reporting (reporting bias) | Low risk | No clear source for selective reporting. |
| Other bias | Low risk | No clear other sources of bias. |
| Methods | Randomisation: computer‐generated randomisation list. | |
| Participants | Diagnosis: chronic schizophrenia (DSM‐III‐R), at least mildly ill according to CGI, had a history of recurrence in last 18 months, currently maintained on antipsychotic medication. N=121. | |
| Interventions | 1. Drug: zotepine. Fixed dose of 300mg/day which could be reduced once to 150mg/day. Mean dose: n.i.. N =63. 2. Placebo: Duration of taper: 0 days. N =58. Rescue medication: antipsychotic drugs not allowed, but benzodiazepines. | |
| Outcomes | Examined: Relapse: (i) a moderate clinical deterioration from baseline (an increase in CGI severity score of at least 2 points plus an increase of 2 points in at least two positive symptom items on the BPRS persisting for two assessments over 3 days, but not requiring hospitalisation; (ii) deterioration requiring hospitalisation accompanied, on one assessment, by an increase in CGI severity score of at least 2 points plus an increase of 2 points in at least two positive symptom items on the BPRS; and (iii) severe clinical deterioration (an increase in CGI severity score to ‘severely ill’ for 24 hours, or, if in hospital, requiring special observation for suicidal or aggressive behaviour). Global state: number of participants improved according to CGI. Adverse effects: binary outcomes ‐ open interview. Unable to use / Not included: Mental state: BPRS, SANS (no prespecified outcomes of interest). Adverse effects: extrapyramidal side‐effects (SAS, AIMS, no SD / continous side‐effect results were not among the prespecified outcomes). Physiological measures: laboratory, vital signs, ECG (all no data / no prespecified outcomes of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation list. |
| Allocation concealment (selection bias) | Low risk | Allocation to treatment was on a double‐blind basis, codes were not broken until the time of analysis. |
| Blinding (performance bias and detection bias) | Unclear risk | Double‐blind, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double‐blind, no further details. |
| Incomplete outcome data (attrition bias) | High risk | The overall rate of participants leaving the study early was very high (76%) and many more participants in the placebo group than in the drug group dropped out due to relapse. Kaplan‐Meier survival analysis was used for primary outcome relapse. No full ITT analysis, only those participants with at least one post‐baseline assessment were included, but only two participants were excluded on this basis. |
| Selective reporting (reporting bias) | High risk | Only those adverse events that were reported on at least four occasions and serious adverse events were reported. |
| Other bias | Low risk | No clear other bias. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: first episode of schizophrenia (Present State Examination). N=120. | |
| Interventions | 1. Drug: flupenthixol i.m., chlorpromazine, haloperidol, pimozide, trifluoperazine Flexible dose. Allowed dose range: no upper limit, but lower limit was flupenthixol i.m. 40mg/month, chlorpromazine 200mg/day, haloperidol 3mg/day, pimozide 4mg/day, trifluoperazine 5mg/day. Mean dose: flupenthixol 84mg/month (n=31), chlorpromazine 366mg/day (n=3), haloperidol 11.8mg/day (n=3), pimozide 7.8mg/day (n=5), trifluoperazine 11.5mg/day (n=12). N=54. 2. Placebo: Duration of taper (days): 30 days on drug, then received half dose for 30 days before they were put on placebo. N=66. Rescue medication: antiparkinson medication, antidepressants, anxiolyties. | |
| Outcomes | Examined: Relapse: rehospitalisation or rehospitalisation thought necessary although not possible or need of medication. Unable to use / Not included: Hallucinations, delusions (no data / no predefined outcomes of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Allocation lists prepared by pharmacy for five antipsychotic drugs mentioned below, concealment is unclear. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | Low risk | No clear bias. overall rate of leaving early of 11% is acceptable. Survival curve analysis was used for the primary outcome relapse. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | High risk | Blind was broken when a participant relapsed. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: residual schizophrenia (DSM‐II), chronic, currently treated with antipsychotic drugs. N=40. | |
| Interventions | 1. Drug: pimozide. Flexible dose. Allowed dose range: n.i.. Mean dose: n.i.. N=20. 2. Placebo: Duration of taper: 0 days. N=20. Rescue medication: not allowed, only dose increase of pimozide or placebo‐pimozide was possible. Additional use of haloperidol meant relapse. | |
| Outcomes | Examined: Relapse: need of additional haloperido) Adverse effects: number of participants with at least one movement disorder, rigor and tremor. Unable to use / Not included: Mental state: Overall Factor Construct Scale (no mean, no SD / no prespecified outcome of interest) Behaviour: ‘Psychiatric Evaluation Scale’ (no mean, no SD / no prespecified outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules. |
| Incomplete outcome data (attrition bias) | Low risk | 2 (5%) of the participants left the study early which is an acceptable rate. Both participants were included in the endpoint analysis. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear evidence for other bias. |
| Methods | Randomisation: no details (just reported as a "randomised study”). | |
| Participants | Diagnosis: chronic schizophrenia with an acute episode within 6 to 12 months before study entry (no details about diagnostic criteria). N=20. | |
| Interventions | 1. Drug: fluphenazine depot. Fixed dose: 25 or 50 mg/month (long‐acting formulation). Mean dose: n.i.. N=10 randomised (but data available only for 9 patients who completed the study). 2. Placebo: Duration of taper (days): n.i.. N=10 randomised (but data available only for 7 patients who completed the study). Rescue medication: antiparkinson medication at study entry (and then progressively tapered off, without a prespecified schedule). | |
| Outcomes | Examined: Relapse: defined as worsening of clinical status needing an adjunctive new antipsychotic treatment. Unable to use / Not included: Mental state: BPRS (no prespecified outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details (just reported as a "randomised study”). |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double‐blind ("patients and authors were not aware of the allocated treatment”). |
| Blinding (performance bias and detection bias) | Low risk | Double‐blind ("patients and authors were not aware of the allocated treatment”). |
| Incomplete outcome data (attrition bias) | Unclear risk | 25% of the participants dropped out, all due to relapse. This may still be acceptable. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear other bias. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (Research Diagnostic Criteria), requiring neuroleptic maintenance treatment to prevent relapse. N=43. | |
| Interventions | 1. Drug: haloperidol decanoate 60mg/4 weeks. Fixed dose. N=20. 2. Placebo: Duration of taper: 0 days, but all on depot medication before study. N=23. Rescue medication: anticholinergics and sedation. | |
| Outcomes | Examined: Relapse: clinical judgement. Leaving the study early. Unable to use / Not included: Mental state: Comprehensive Psychopathological Rating Scale (no mean, no SD / no prespecified outcome of interest). Adverse effects: extrapyramidal side‐effects, tardive dyskinesia (no mean, no SD / continuous side‐effect results were not among the prespecified outcomes). Physiological measures: laboratory (prolactin and haloperidol levels, no mean/SD / no prespecified outcomes of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, placebo injections, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, placebo injections, no further details. |
| Incomplete outcome data (attrition bias) | High risk | A considerable number of participants (42%) left the study early. The number was clearly higher in the placebo group and the reasons differed. Data were analysed on an intent‐to‐treat basis. |
| Selective reporting (reporting bias) | Low risk | No selective reporting. |
| Other bias | Low risk | No clear other bias. |
| Methods | Randomisation: random number table. | |
| Participants | Diagnosis: chronic schizophrenia (clinical diagnosis). N=14. | |
| Interventions | 1. Drug: chlorpromazine ‐ Fixed dose. Allowed dose range n.i.. Mean dose n.i.. N=7. 2. Placebo: Duration of taper: 0 days. N=7. Rescue medication: benztropine. | |
| Outcomes | Examined: Relapse: worsening of psychotic symptoms. Leaving the study early. Unable to use / Not included: Behaviour: NOSIE (no data / no prespecified outcome of interest). Neurophysiological tests (no SDs / no prespecified outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number table. |
| Allocation concealment (selection bias) | Low risk | All personnel except for the treating psychiatrist remained unaware of the code until the end of the study. |
| Blinding (performance bias and detection bias) | Unclear risk | Double (patients, scientists, nurses, only the treating psychiatrist knew the treatment). |
| Blinding (performance bias and detection bias) | Low risk | Double (patients, scientists, nurses, only the treating psychiatrist knew the treatment). |
| Incomplete outcome data (attrition bias) | Low risk | One participant in the placebo group left the study prematurely which is an acceptable rate. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear other bias. |
| Methods | Randomisation: participants were ranked for morbidity, then matched, then randomised. | |
| Participants | Diagnosis: chronic, long term hospitalised male psychotics (clinical diagnosis), 86 schizophrenia, 6 chronic brain syndrome, 2 personality disorders, 2 n.i.. N=96. | |
| Interventions | 1. Drug: chlorpromazine ‐ Flexible dose. Allowed dose range: n.i.. Mean dose: n.i.. N=48. 2. Placebo: Duration of taper: 0 days. N=48. Rescue medication: occasional use of sedatives, antipsychotics were not allowed. | |
| Outcomes | Examined: Relapse: condition worsened to such a point that ordinarily a complete change in treatment would be considered. Leaving early due to inefficacy. Unable to use / Not included: Behaviour: Lyon’s Behaviour Scale (no SD / no prespecified outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Participants were ranked for morbidity, then matched, then randomised. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules, each participant was provided medication in individual container. Staff guessed on which medication the participants were but could not guess adequately. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules, each participant was provided medication in individual container. Staff guessed on which medication the participants were but could not guess adequately. |
| Incomplete outcome data (attrition bias) | Unclear risk | It can be that there were participants leaving the study early but this was not clearly reported. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | High risk | Blind was broken once a participant relapsed. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: severely ill, chronically hospitalized people with schizophrenia (clinical diagnosis). N=50. | |
| Interventions | 1. Drug: penfluridol once weekly. Fixed dose. Allowed dose range: 40‐160 mg/week. Mean dose: n.i.. N=25. 2. Placebo: Duration of taper: 0 days. N=25. Rescue medication: antiparkinson medication. | |
| Outcomes | Examined: Relapse: worsening of global state. Leaving the study early. Global state: number of participants according to the Clinical Global Impression Scale. Adverse effects: extrapyramidal side‐effects. Unable to use / Not included: Mental state: Brief Psychiatric Rating Scale (no mean, no SD / no prespecified outcome of interest). Behaviour: Nurses´ Observation Scale for Inpatient Evaluation (no mean, no SD / no prespecified outcome of interest). Physiological measures: laboratory, ECG, photosensitivity tests, ophthalmologic examinations, vital signs (no clear data / no prespecified outcomes of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | High risk | It is not entirely clear, whether there were dropouts in addition to 18 participants (7 drug, 11 placebo, 36%) who left the study early due to relapse. However, the 36% drop out rate can be a problem for other outcomes. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No evidence for other bias. |
| Methods | Randomisation: randomised, 3:1 ratio. | |
| Participants | Diagnosis: chronic psychotic outpatients (DSM‐III), schizophrenia (n=26), mental retardation with psychosis (n=9), organic brain syndrome (n=1). N=36. | |
| Interventions | 1. Drug: various antipsychotic drugs. Fixed dose: keeping the dose of the antipsychotic the participant was on at the beginning of the study. Mean dose: 365mg/day chlorpromazine equivalents. N=9. 2. Placebo: Duration of taper: 28 days. N=27. Rescue medication: n.i.. | |
| Outcomes | Examined: Relapse: major clinical deterioration. Leaving the study early. Unable to use / Not included: Global state: Clinical Global Impression (no data for each group separately/no prespecified outcome of interest). Mental state: Brief Psychiatric Rating Scale, Profile of Mood Symptoms (no data for each group separately/no prespecified outcome of interest). Adverse effects: extrapyramidal side‐effects (Abnormal Involuntary Movement Scale, Dyskinesia Rating Scale, no data for each group separately / continuous side‐effect results were not among the prespecified outcomes), other adverse effects (Treatment Emergent Symptoms Scale, no data for each group separately / continuous side‐effect results were not among the prespecified outcomes). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, 3:1 ratio (information obtained from author). |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, ‘matching placebos’ and sesame oil for fluphenazine decanoate treated participants. |
| Blinding (performance bias and detection bias) | Low risk | Double, ‘matching placebos’ and sesame oil for fluphenazine decanoate treated participants. |
| Incomplete outcome data (attrition bias) | Low risk | The differential dropout rate (placebo group 8/27, 0/9 maintenance group, all due to relapse) can have biased other outcomes than relapse and leaving the study early. But data on such other outcomes were not available anyways. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No evidence for other bias. |
| Methods | Randomisation: matched in three groups according to age and hospitalisation, then randomised using a table of random numbers. | |
| Participants | Diagnosis: schizophrenia (clinical diagnosis), undifferentiated type (n=10), hebephrenic (n=6), catatonic (5), paranoid (5), acute undifferentiated (n=1). N=27. | |
| Interventions | 1. Drug: remained on previous antipsychotic medication (chlorpromazine, thioridazine, trifluoperazine, perphenazine, prochlorperazine). Fixed/flexible dose: not clear, but probably fixed. Allowed dose range: n.i.. Mean dose: n.i., because it is unclear which patients were allocated to which group. N=9. 2. Placebo: Duration of taper: 7 days. N=9**. Rescue medication: tranquilizer (=benzodiazepine). | |
| Outcomes | Examined: Relapse: worsening by three points on the factor scores of the IMPS or withdrawn due to being worse. Leaving the study early. Global state: improvement by three points on the factor scores of the IMPS or withdrawn due to being ready for discharge. Unable to use / Not included: Mental state: Inpatient Multidimensional Psychiatric Scale (no data / no prespecified outcome of interest). Behaviour: Psychotic Reaction Profile (no data / no prespecified outcome of interest). | |
| Notes | ** a second placebo group that was referred to a specialised ward was not used in our calculations (n=9). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Matched in three groups according to age and hospitalisation, then randomised using a table of random numbers. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | High risk | There was a considerable number of participants leaving the study early (28%). The approach how missing data were handled is not specified. |
| Selective reporting (reporting bias) | Low risk | Only two factors of the IMPS were presented, but this was no outcome of interest. |
| Other bias | Low risk | No clear other bias. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (n=10), schizoaffective disorder (n=2) according to Research Diagnostic Criteria, first episode no more than 2 years ago. N=12. | |
| Interventions | 1. Drug: fluphenazine i.m. Fixed dose 12.5mg/two weeks fluphenazine i.m.. Mean dose: 12.5mg/two weeks fluphenazine i.m.. N=n.i.. 2. Placebo: Duration of taper 0 days, but depot study. N=n.i.. Rescue medication: n.i.. | |
| Outcomes | Unable to use / Not included: Relapse: no data for first cross‐over phase. Prolactin levels (no data for first cross‐over phase / no prespecified outcome of interest). | |
| Notes | Depot study, at six weeks the full plasma level could still be measured, even at the end of 12 weeks 33% still had substantial fluphenazine plasma levels. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | Unclear risk | Unclear, because not indicated. |
| Selective reporting (reporting bias) | High risk | Data not presented for both groups separately. |
| Other bias | Unclear risk | Unclear ‐ baseline imbalance can not be addressed. |
| Methods | Randomisation: randomly assigned. | |
| Participants | Diagnosis: chronic schizophrenic outpatients (DSM‐III). N=31. | |
| Interventions | 1. Drug: fluphenazine decanoate‐ Fixed doses. Allowed dose range: n.i. ‐ same dose as before. Mean dose: n.i.. N=14. | |
| Outcomes | Examined: Relapse: clinical judgement. Leaving the study early. Adverse effects: tardive dyskinesia (AIMS). Unable to use / Not included: Social Adjustment Scale. Depression: SADS (no mean, no SD / no prespecified outcome of interest). Functioning: GAS (no mean, no SD / no prespecified outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further deatils. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, placebo injection. |
| Blinding (performance bias and detection bias) | Low risk | Double, placebo injection. |
| Incomplete outcome data (attrition bias) | Low risk | 3 out of 30 participants (10%) left the study early which is an acceptable rate, irrespective of the statistical analysis (completer analysis). |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No evidence for other bias. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: chronic psychotic patients (mainly schizophrenia, clinical diagnosis). N=144. | |
| Interventions | 1. Drug: continuation of antipsychotic taken before the study ‐ Fixed/flexible dose: unclear. Allowed dose range: unclear. Mean dose: n.i.. N=46. 2. Placebo: Duration of taper: "4 weeks to five months, usually 2 months”. N=98. Rescue medication: n.i.. | |
| Outcomes | Examined: Relapse: clinical diagnosis. Unable to use / Not included: Social adjustment: (not reported for the randomised participants / no predefined outcome of interest). Rehospitalisation (unclear numbers). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, unidentifiable capsules. |
| Blinding (performance bias and detection bias) | Low risk | Double, unidentifiable capsules. |
| Incomplete outcome data (attrition bias) | Unclear risk | Whether participants left the study early is unclear. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | High risk | In case of relapse the blind was broken. |
| Methods | Randomisation: randomised, no further details. | |
| Participants | Diagnosis: chronic schizophrenia (clinical diagnosis) with positive or negative symptoms, responsive to treatment with antipsychotic drugs, all so ill that they required continuous treatment with antipsychotic medication for at least 3 months. N=61. | |
| Interventions | 1. Drug: pimozide ‐ Flexible dose. Allowed dose range: 2‐12 mg/day. Mean dose: 6.3 mg/day. N=21. 2. Drug: trifluoperazine. Flexible dose. Allowed dose range: 5‐30 mg/day. Mean dose: 17.5 mg/day. N=20. 3. Placebo: Duration of taper: 21 days. N=20. Rescue medication: chloralhydrate, antiparkinson medication. | |
| Outcomes | Examined: Relapse: at least minimally worse on CGI. Leaving the study early. Unable to use / Not included: Mental state: BPRS (no predefined outcome of interest). Global state: CGI (no predefined outcome of interest). Social activity: Family Rating Form (no SD / no predefined outcome of interest). Social adjustment: Harbor View House Residents Rating Report (no SD / no predefined outcome of interest). Adverse effects: open interview (no data). Physiological measures: vital signs, laboratory (both no data / no predefined outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules. |
| Incomplete outcome data (attrition bias) | High risk | The overall number of participants leaving the study early (41%) was considerable, with a higher drop‐out rate in the placebo group. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear evidence for other bias. |
| Methods | Randomisation: randomised, no further details. | |
| Participants | Diagnosis: chronic schizophrenia (clinical diagnosis), >70% of them with extrapyramidal side effects after long treatment with phenothiazines. N=63. | |
| Interventions | 1. Drug: trifluoperazine ‐ Fixed dose (maintaining the initial dose, necessity of dose increase was considered to be a relapse). Mean dose: 17 mg/day. N=31. 2. Placebo: Duration of taper: 0 days. N=32. Rescue medication: n.i.. | |
| Outcomes | Examined: Relapse: deterioriation of participant’s condition to such a degree that additional antipsychotic medication was necessary. Unable to use / Not included: Adverse effects: movement disorders (no randomised data). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, no further details. |
| Allocation concealment (selection bias) | Low risk | Capsules dispensed by the hospital pharmacist who was the only person who knew what the capsules were and to whom they were given. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, placebo capsules, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, placebo capsules, no further details. |
| Incomplete outcome data (attrition bias) | Low risk | 16% left the study early, all but one due to relapse. This appears acceptable. relapse and death were the only outcomes. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | High risk | Participants with a relapse were probably removed from the study and the blind broken. Study was probably terminated early. |
| Methods | Randomisation: randomly allocated by research assistant. | |
| Participants | Diagnosis: chronic schizophrenia (Present State Examination), chronicity defined by at least 2 admissions or 1 admission lasting longer than 6 months, 71 schizophrenic psychosis with delusions or auditory hallucinations, six non affective delusional psychoses, three catatonic schizophrenia. N=81. | |
| Interventions | 1. Drug ‐ Fixed/flexible dose: Allowed dose range: 25mg/month ‐ no upper limit. Mean dose: 26.4mg/month. N=41. 2. Placebo: Duration of taper: n.i.. N=40. Rescue medication: antidepressants, antiparkinson medication | |
| Outcomes | Examined: Relapse: deterioration of condition to a degree that participant had to be taken out of the trial to ensure that active medication was prescribed, prescription of oral phenothiazines. Adverse effects: use of antiparkinson medication. Unable to use / Not included: Mental state: Present State Examination (no data / no predefined outcome of interest). Social functioning: Social Performance Schedule, Events Schedule of Bron and Birley (both no predefined outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomly allocated by research assistant. |
| Allocation concealment (selection bias) | Low risk | Apart from the research assistant no one knew who was on drug or placebo until the data were analysed. |
| Blinding (performance bias and detection bias) | Low risk | Double, sesame oil injections, unmarked ampoules. Blinding was tested at the end of the trial and it worked. |
| Blinding (performance bias and detection bias) | Low risk | Double, sesame oil injections, unmarked ampoules. Blinding was tested at the end of the trial and it worked. |
| Incomplete outcome data (attrition bias) | Unclear risk | Overall, 43% of the participants left the study early (no complete ITT for some outcomes). |
| Selective reporting (reporting bias) | Low risk | No evidence for selected reporting. |
| Other bias | Low risk | No evidence of other bias |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (DSM‐III‐R). N=21. | |
| Interventions | 1. Drug: fluphenazine depot. Fixed dose of 25mg/2 weeks. N=11. 2. Placebo: Duration of taper: 0 days. N=10. Rescue medication: | |
| Outcomes | Unable to use / Not included: No data could be used because they have not been presented for the randomised subset. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | Unclear risk | Uncear, whether there were any drop‐outs. |
| Selective reporting (reporting bias) | High risk | No useable data because data of the randomised subsample have not been presented. |
| Other bias | Low risk | No clear evidence for other bias. |
| Methods | Randomisation: randomly assigned, no further details. | |
| Participants | Diagnosis: schizophrenia (DSM‐II, undifferentiated type 46.3%, paranoid 39%, acute differentiated 8%, schizoid affective 2.7%, other 3.8%), currently hospitalised for less than 2 years. N=374. | |
| Interventions | Previous medication was gradually shifted to chlorpromazine for two months. 2. Placebo: Duration of taper: 0 days. N=182. Rescue medication: not indicated, but probably not allowed. | |
| Outcomes | Examined: Relapse: clinical deterioration of such magnitude that hospitalisation appeared imminent. Unable to use / Not included: Leaving the study early (numbers not specified for each group separately). Mental state: Brief Psychiatric Rating Scale, Inpatient Multidimensional Psychiatric Scale, Springfield Symptom Index, Hopkin’s Symptom Distress Check List (all no SDs and data only given for subgroups / no predefined outcome of interest). Social behaviour and adjustment: Katz Adjustment Scale, Major Role Adjustment Inventory (both no SDs and data presented only for subgroups / no predefined outcome of interest). | |
| Notes | Half of the participants randomly received major role therapy in addition to chlorpromazine or placebo. For the purpose of this review the four resulting groups were pooled as described above. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomly assigned, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules, no further details. |
| Incomplete outcome data (attrition bias) | Low risk | Relatively few participants left the study early due to reasons other than relapse which was the only outcome (n=31). Although it is unclear in which group they occurred the small percentage does not represent an important risk of bias. |
| Selective reporting (reporting bias) | Low risk | No clear evidence for selective reporting. |
| Other bias | Low risk | No clear other bias. |
| Methods | Randomisation: patients were randomised in a 1 to 1 ratio (via a sponsor prepared, computer generated randomisation scheme, assigned by an interactive voice system). | |
| Participants | Diagnosis: schizophrenia (DSM‐IV‐TR). N=410. | |
| Interventions | 1. Drug: paliperidone palmitate depot ‐ Fixed dose: originally 25, 50 or 100mg/4 weeks; this dose was maintained. Mean dose: n.i.. N=206. 2. Placebo: Duration of taper: 0 days. N=204. Rescue medication: n.i.. | |
| Outcomes | Examined: Relapse: psychiatric rehospitalisation, deliberate self‐injury or violent behaviour, suicidal or homicidal ideation, certain predefined PANSS score. Leaving the study early. Rehospitalisation. Death natural causes and suicide. Unable to use / Not included: Mental state: Positive and Negative Syndrome Scale (no predefined outcome of interest). Adverse effects: open interviews (only a few adverse events were indicated and these were not of interest for the review). Prolactin levels (no predefined outcome of interest). | |
| Notes | The study was stopped early after a significant interim analysis. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Patients were randomised in a 1 to 1 ratio (via a sponsor prepared, computer generated randomisation scheme, assigned by an interactive voice system). |
| Allocation concealment (selection bias) | Low risk | Interactive voice system. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | High risk | Overall high drop‐out rate (45%). Clearly more participants in the placebo group (95) than in the drug group (31) left the study early due to relapse. This imbalance may have biased the results of other outcomes such as adverse events. Kaplan‐Meier survival curve analysis was used for the primary outcome relapse. |
| Selective reporting (reporting bias) | Low risk | Those adverse events that occurred in at least 2% of the participants and severe adverse events were presented. We feel that's acceptable. |
| Other bias | High risk | Study was stopped early after an interim analysis. |
| Methods | Randomisation: matched then each pair randomised, no further details. | |
| Participants | Diagnosis: probable or definite schizophrenia, any subtype (Research Diagnostic Criteria), in remission for at least 4 weeks or at stable clinical plateau despite vigorous chemotherapy. N=16. | |
| Interventions | 1. Drug: fluphenazine decanoate ‐ Flexible dose. Allowed dose range: 1.25‐5.0mg biweekly. Mean dose: n.i.. N=8. 2. Placebo: Duration of taper: 0 days, but previously treated with depot medication. N=8. Rescue medication: minor tranquilisers, additional antipsychotic drugs were not allowed. | |
| Outcomes | Examined: Relapse: increase in or re‐emergence of significant symptoms suggesting imminent psychotic relapse. Unable to use / Not included: Leaving study early (no data). Adverse effects (no data). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Matched, then each pair randomised, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | Low risk | Two participant in the drug group (1 relapse, 1 unclear) left the study early, and 7/8 participants in the placebo group dropped out due to relapse. As relapse and dropout were the only outcomes, this did not lead to bias. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear evidence for other bias. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: first episode schizophrenia (clinical diagnosis), no evidence of drug abuse or important medical illnesses. When diagnoses were reassessed by Research Diagnostic Criteria, 19 had schizophrenia, 3 had unspecific schizophrenic psychoses, 4 had other psychiatric disorders, one mania with schizotypal features and one depression with schizotypal features. N=28. | |
| Interventions | 1. Drug: oral fluphenazine ‐ Flexible dose. Allowed dose range: 5‐20mg/day. Mean dose: n.i.. N=n.i.. 2. Drug: depot fluphenazine ‐ Flexible dose. Allowed dose range: 12.5‐50/mg biweekly. Mean dose: n.i.. N=n.i.. 2. Placebo: Duration of taper: 0 days. N=17. Rescue medication: not indicated. | |
| Outcomes | Examined: Relapse: a substantial clinical deterioration with a potential for marked social impairment. Patients were considered dropouts only if they showed no signs of clinical deterioration at the time they left the study. Leaving the study early. Unable to use / Not included: Social aspects of premorbid personality: Premorbid Asocial Adjustment Scale (data on placebo group only / no predefined outcome of interest). | |
| Notes | The design was changed during the study in that only non‐compliant patients were randomised to depot fluphenazine or depot placebo, and the randomisation was changed to 2‐1‐1 (placebo, oral fluphenazine, depot fluphenazine). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, all participants received both pills and injections (active or placebo) to maintain double‐blind conditions. |
| Blinding (performance bias and detection bias) | Low risk | Double, all participants received both pills and injections (active or placebo) to maintain double‐blind conditions. |
| Incomplete outcome data (attrition bias) | High risk | 20 out of 28 participants left the study early, 10 for other reasons than relapse, which was the only outcome apart from leaving the study early. This may present a bias. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Unclear risk | The design was changed during the study in that only non‐compliant patients were randomised to depot fluphenazine or depot placebo, and the randomisation was changed to 2‐1‐1 (placebo, oral fluphenazine, depot fluphenazine). It is unclear whether this biased the results. |
| Methods | Randomisation: randomly assigned, no further details. | |
| Participants | Diagnosis: chronic schizophrenia (clinical diagnosis), 12 paranoid, 3 hebephrenic, 2 catatonic, 1 simple, 6 chronic undifferentiated, on antipsychotic medication for a mean duration of 2 years. N=24. | |
| Interventions | 1. Drug: fluphenazine decanoate ‐ Flexible doses. Allowed dose range: 12.5‐75/mg biweekly. Mean dose: n.i.. N=13 2. Placebo: sesame oil injections. Duration of taper: 0 days. N=11. Rescue medication: antiparkinson medication, additional fluphenazine decanoate ‐ but this was considered to be a relapse. | |
| Outcomes | Examined: Relapse: clinical deterioration requiring additional antipsychotic drug treatment. Leaving study early. Unable to use / Not included: Global state: 7 point scale of severity (no data / no predefined outcome of interest). Mental state: scale published by the authors (no SD / no predefined outcome of interest). Adverse effects: scale published by the authors (no numbers). Physiological measures: ECG, EEG, laboratory (all no data / no predefined outcomes of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomly assigned, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, placebo treated participants received injections of sesame oil in a similar amount. |
| Blinding (performance bias and detection bias) | Low risk | Double, placebo treated participants received injections of sesame oil in a similar amount. |
| Incomplete outcome data (attrition bias) | Low risk | No participant left the study early. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | High risk | In case of deterioration the participants received additional antipsychotic drugs. This is a problem for the analysis of side‐effects. |
| Methods | Randomisation: randomised, computerized randomisation and stratification scheme. | |
| Participants | Diagnosis: schizophrenia (DSM‐IV), 80% paranoid subtype, 14% undifferentiated subtype, initially with acute exacerbation, then 8 weeks run in and 6 weeks stabilisation phase. N=207. | |
| Interventions | 1. Drug: paliperidone‐ Flexible doses. Allowed dose range: 3 ‐ 15mg/day Mean dose: 10.8 mg/day. N=105. 2. Placebo: Duration of taper: 0 days. N=102. Rescue medication: benzodiazepines, antiparkinson medication, propanolol, antidepressants when the dose was stable for at least 3 months before the study. | |
| Outcomes | Examined: Relapse: (a) psychiatric hospitalisation (involuntary or voluntary admission); b) increase in Positive and Negative Syndrome Scale (PANSS) total score by 25% for 2 consecutive days for patients who scored more than 40 at randomisation or a 10‐point increase for patients who scored 40 or below at randomisation; c) increase in the Clinical Global Impression‐Severity (CGI‐S) score to at least 4, for patients who scored 3 or below at randomisation, or to at least 5, for patients whose CGI‐S scores were 4 at randomisation, for 2 consecutive days; d) deliberate self‐injury or aggressive behavior, or suicidal or homicidal ideation and aggressive behavior that was clinically significant; e) increase in prespecified individual PANSS item scores to at least 5, for patients whose scores were 3 or below at randomisation, or to at least 6, for patients whose scores were 4 at randomisation, for 2 consecutive days). Quality of life: Schizophrenia Quality‐of‐Life Scale. Unable to use / Not included: Mental state: PANSS (no predefined outcome of interest). Behaviour: suicide, aggression (only mean scores which were no predefined outcomes of interest). Functioning: Personal and Social Performance Scale (no predefined outcome of interest). Global state: CGI‐severity (only mean score which was no predefined outcome of interest). Adverse effects: World Health Organization Adverse Reaction Terminology dictionary (no data / no predefined outcome of interest), movement disorders (Simpson Angus Scale, Barnes Akathisia Rating Scale, and Abnormal Involuntary Movement Scale (all no data / continuous side‐effect results were not among the predefined outcomes of interest). Physiological measures: laboratory (except for metabolic problems no data), vital signs, ECG, prolactin (all no data / no predefined outcomes of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised, computerized randomisation and stratification scheme. |
| Allocation concealment (selection bias) | Low risk | Interactive voice‐response system. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | High risk | Only 28 out of 207 participants left the study prematurely for another reason than relapse. Therefore, missing outcomes may not pose a problem for the primary outcome which was assessed with the Kaplan‐Meier method. Nevertheless, high discontinuations due to relapse (75/207) which were much more frequent in the placebo group than in the drug group pose a major problem for secondary outcomes. No full ITT (participants had to receive at least one dose post‐baseline) but only two participants were excluded on this basis. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | High risk | Study was terminated after an interim analysis showed a clear advantage of paliperidone. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: chronic schizophrenia (clinical diagnosis). N=35. | |
| Interventions | 1. Drug: penfluridol ‐ Flexible dose. Allowed dose range: 20‐120mg/week. Mean dose:n.i.. N=18. 2. Placebo: Duration of taper: 0 days. N=17. Rescue medication: antiparkinson medication, it seems that haloperidol was not allowed in the double‐blind phase. | |
| Outcomes | Examined: Relapse: psychiatric decompensation that could not be controlled by dose increase. Leaving the study early. Unable to use / Not included: Global state: Clinical Global Impression Scale (no numbers / no predefined outcomes of interest). Mental state: Brief Psychiatric Rating Scale (no numbers / no predefined outcomes of interest). Behaviour: Nurses Observation Scale for Inpatient Behaviour (no numbers / no predefined outcomes of interest). Physiological measures: vital signs (weight, pulse, blood pressure, respiratory frequency, temperature ‐ no numbers / no predefined outcomes of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules. |
| Incomplete outcome data (attrition bias) | High risk | 12 of 35 participants left the study early (34%), 11 of them were in the placebo group. As all participants in the placebo group discontinued due to relapse, the primary outcome is not affected. But the results of all other outcomes are biased by this effect. |
| Selective reporting (reporting bias) | Low risk | Results on rating scales have not been reported, but these were not outcomes of interest in our review. |
| Other bias | Low risk | No clear other bias |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (Present State Examination), recently recovered from an acute episode, 32 florid schizophrenia, 3 delusional psychosis. N=35. | |
| Interventions | 1. Drug: trifluoperazine or chlorpromazine (depending on the previous medication so that so far as the patient was concerned there was no apparent change in medication). Flexible dose. Allowed dose range: trifluoperazine 5‐25mg/day, chlorpromazine 100‐500mg/day. Mean dose: chlorpromazine 157.1 mg/day, trifluoperazine 12.3mg/day. N=20. 2. Placebo: Duration of taper: not indicated, probably 0 days. N=15. Rescue medication: antiparkinson medication, antidepressants, no antipsychotics (doctors received a letter asking them not to prescribe other medication). | |
| Outcomes | Examined: Relapse: physician was sufficiently concerned about the patient’s status to want to be certain that he was on active drug. Leaving the study early. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Low risk | Trial medication was held by the unit secretary and dispensed to Julian Leff who gave it to the treating consultant. Only the unit secretary knew which pills were active drug and which were placebo. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. But side‐effects were not troublesome in any patient and therefore doctors concerned probably received no clues about whether a patient was on active drug or not. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. But side‐effects were not troublesome in any patient and therefore doctors concerned probably received no clues about whether a patient was on active drug or not. |
| Incomplete outcome data (attrition bias) | High risk | Overall drop‐out rate was 60%, almost all due to relapse which occured much more frequently in the placebo group. This poses a problem for other outcomes than relapse. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear other bias. |
| Methods | Randomisation: random 2:1, no further details. | |
| Participants | Diagnosis: schizophrenia (DSM‐II). N=67. | |
| Interventions | 1. Drug: oral fluphenazine (n=6) or depot fluphenazine (n=11). Fixed/flexible dose: unclear. Allowed dose range: unclear. Mean dose: unclear. N=17. 2. Placebo: Duration of taper: 0 days. N=50. Rescue medication: n.i., but antipsychotics were probably not allowed. | |
| Outcomes | Examined: Relapse: rehospitalisation or deterioration in clinical condition which could not be managed within protocol limits (e.g., increased psychological support or adjustment of dosage). Adverse effects: tardive dyskinesia (AIMS). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random 2:1, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | Unclear risk | It is unclear whether there were participants who left the study early. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear evidence for other bias. |
| Methods | Randomisation: randomly assigned. | |
| Participants | Diagnosis: chronic psychotic patients, treatment resistive in closed wards. No seizures, no antidepressants, no candidates for discharge. N=88. | |
| Interventions | 1. Drug: trifluoperazine (10‐90 mg/day), chlorprothixene (50‐450 mg/day), same medication (various drugs). Flexible doses. Allowed dose range: n.i.. Mean dose: n.i.. N=54. | |
| Outcomes | Examined: Relapse: clinical judgement. Unable to use / Not included: Ward behaviour: unpublished rating scale (no predefined outcome of interest). Urinary excretion (no predefined outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, different colours. |
| Blinding (performance bias and detection bias) | Low risk | Double, different colours. |
| Incomplete outcome data (attrition bias) | Low risk | Drop‐outs 10 out of 88 is acceptable (11%), although only completers were analysed. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No evidence for other bias. |
| Methods | Randomisation: assumed, because study was double‐blind and because the first study phase was randomised (no further details). | |
| Participants | Diagnosis: first episode schizophrenia (Present State Examination, Feighner criteria and Research Diagnostic Criteria). N=15. | |
| Interventions | 1. Drug: pimozide once weekly or i.m. flupenthixol. Flexible doses. Allowed dose range: n.i.. Mean dose: n.i.. N=8. | |
| Outcomes | Examined: Relapse: re‐admission. Unable to use / Not included: Leaving early (no data). Cognition (no data for withdrawal study / no predefined outcome of interest). Adverse effects: parkinsonism, tardive dyskinesia (no data for withdrawal study). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation assumed. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | Unclear risk | It is unclear whether there were missing data. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Unclear risk | Not entirely clear. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (clinical diagnosis), paranoid schizophrenia (n=19), undifferentiated schizophrenia (n=8), catatonic schizophrenia (n=8), hebephrenic schizophrenia (n=4), acute schizophrenic reaction (n=1). N=40. | |
| Interventions | 1. Drug: chlorpromazine (n=6) or thioridazine (n=14). Flexible dose. Allowed dose range: 100‐600mg/day. Mean dose: n.i.. N=20. 2. Placebo: Duration of taper (days): 0 days. N=20. Rescue medication: n.i.. | |
| Outcomes | Examined: Relapse: symptoms similar to those which had characterized the patient’s illness prior to successful treatment by phenothiazines. Unable to use / Not included: Withdrawal symptoms (no numbers for each group separately / no predefined outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, "the staff, patients and investigators were not aware of which patients were to receive placebo instead of their medication”. |
| Blinding (performance bias and detection bias) | Low risk | Double, "the staff, patients and investigators were not aware of which patients were to receive placebo instead of their medication”. |
| Incomplete outcome data (attrition bias) | Unclear risk | It was not reported whether participants left the study early, but it is well possible that there weren’t any, because it was a relatively short inpatient study. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear evidence for other bias. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: chronic schizophrenia (clinical diagnosis by two psychiatrists). N=40. | |
| Interventions | 1. Drug: chlorpromazine or trifluoperazine. Fixed/flexible dose: n.i.. Allowed dose range: n.i.. Mean dose: n.i.. N=20. 2. Placebo: Duration of taper: 0 days. N=20. Rescue medication: n.i.. | |
| Outcomes | Examined: Relapse: worsening of global state. Unable to use / Not included: Mental state: Wing Scale (no SD / no predefined outcome of interest). Global state: clinical impression of severity (no predefined outcome of interest). Behaviour: Wing Scale (no SD / no predefined outcome of interest). Leaving the study early (no data). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Low risk | The hospital pharmacist was responsible for supplying placebo and active drugs to the ward, no one concerned with the care of patients knew which patients were started on placebo. |
| Blinding (performance bias and detection bias) | High risk | Double, identical tablets, but in most cases nurses made correct forecasts on who was on drug and who was on placebo. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical tablets, but in most cases nurses made correct forecasts on who was on drug and who was on placebo. |
| Incomplete outcome data (attrition bias) | Unclear risk | It is unclear whether there were dropouts. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | High risk | Blind was broken when a participant relapsed. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (clinical diagnosis) in remission. N=30. | |
| Interventions | 1. Drug: chlorpromazine. Fixed dose of 75mg/day. N=10. 2. Drug: haloperidol. Fixed dose of 3mg/day. N=10. 3. Placebo: Duration of taper (days): 0 days. N=10. Rescue medication: only nitrazepam for sleep and biperiden for extrapyramidal side‐effects, no additional antipsychotic drugs. | |
| Outcomes | Examined: Relapse: clinical judgement. Unable to use / Not included: Number of symptom free days (no SD’s / no predefined outcome of interest). | |
| Notes | There were also a diazepam and an imipramine group which were not of interest for the current review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, drug appearance was made identical with respect to taste, colour and volume by adding a kind of "stomatics”. |
| Blinding (performance bias and detection bias) | Low risk | Double, drug appearance was made identical with respect to taste, colour and volume by adding a kind of "stomatics”. |
| Incomplete outcome data (attrition bias) | Low risk | No participant left the study early due to other reasons than relapse in the first phase of the study, the only outcome apart from leaving the study early. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | High risk | The doses used were very low for Western standards. The study was initially planned as a cross‐over trial, but due to high dropout rates after the first phase only the first treatment phase was analysed. Nevertheless, this did not interfere with the aims of our review. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (DSM‐III), in remission or residual state. N=87. | |
| Interventions | 1. Drug: haloperidol combined with biperidine and nitrazepam. Fixed dose: 1, 3 or 6 mg/day.* N=37. 2. Drug: propericiazine combined with biperidine and nitrazepam. Fixed dose: 10, 30 or 60 mg/day.* N=37. 3. Placebo combined with biperidine and nitrazepam. Duration of taper: 0 days. N=13. Rescue medication: not indicated, probably no additional antipsychotic medication allowed. | |
| Outcomes | Examined: Relapse: clinical judgement. Leaving the study early. Unable to use / Not included: Prolactin levels (no predefined outcome of interest). | |
| Notes | * only the highest doses were analysed for the purpose of this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, drug appearance was made identical with respect to powder, color, tast and volume by adding a gastric acid. |
| Blinding (performance bias and detection bias) | Low risk | Double, drug appearance was made identical with respect to powder, color, tast and volume by adding a gastric acid. |
| Incomplete outcome data (attrition bias) | Unclear risk | While in the placebo group and in the haloperidol group the rates of participants leaving early due to other reasons were low, 9 out of 12 participants in the propericiazine group discontinued due to overdose. It is questionable whether relapse rates could be accurately measured, because most participants did not reach the endpoint. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No evidence for other bias. |
| Methods | Randomisation: participants were matched for age, sex, duration of illness, and severity of symptoms in the preceding episode and then assigned based on a randomised schedule. | |
| Participants | Diagnosis: schizophrenia (ICD‐9 and Present State Examination), with two or more episodes and several first rank symptoms in previous episode, free of psychopathology for at least 12 months, on fluphenazine decanoate for at least 2 years. N=70. | |
| Interventions | 1. Drug: fluphenazine decanoate. Fixed dose of 50mg i.m. four/eight weekly. N=35. 2. Placebo: vitamin B complex i.m.. Duration of taper: 0 days. N=35. Rescue medication: nitrazepam for sleep and benzhexol for extrapyramidal side‐effects; additional antipsychotic drugs were not allowed. | |
| Outcomes | Examined: Relapse (re‐emergence of definite schizophrenic psychopathology necessitating hospital admission or other major treatment change). Adverse effects: tardive dyskinesia (Aquired Involuntary Movements Scale). Unable to use / Not included: Mental state: Brief Psychiatric Rating Scale (no mean, no SD / no predefined outcome of interest). Adverse effects: extrapyramidal symptoms ‐ use of antiparkinson medication (combined with nitrazepam), use of additional nitrazepam for sleep (combined with use of antiparkinson medication). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were matched for age, sex, duration of illness, and severity of symptoms in the preceding episode and then assigned based on a randomised schedule. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, evaluating psychiatrist and participants were unaware of the contents of their injections. It seems that treating psychiatrist was aware of the treatment. |
| Blinding (performance bias and detection bias) | Low risk | Double, evaluating psychiatrist and participants were unaware of the contents of their injections. It seems that treating psychiatrist was aware of the treatment. |
| Incomplete outcome data (attrition bias) | High risk | Overall drop‐out rate drug 40%, placebo 66%, most due to relapse. This poses a risk for bias for other outcomes. Completer analysis. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear evidence for other sources of bias. |
| Methods | Randomisation: randomly selected and then assigned. | |
| Participants | Diagnosis: chronically mentally ill, 67%‐83% schizophrenia (clinical diagnosis), in hospital and apparently treated with antipsychotic drugs for the last 18 months. N=60. | |
| Interventions | 1. Drug: chlorpromazine or thioridazine. Fixed/flexible dose: n.i.. Allowed dose range: n.i.. Mean dose: n.i.. N=30. 2. Placebo: Duration of taper: 0 days. N=30. Rescue medication: not indicated. | |
| Outcomes | Examined: Relapse: attrition because of behavioural upset. Unable to use / Not included: Behaviour: various scales (no data reported / no predefined outcome of interest). | |
| Notes | There were several study phases (alternation between drug and placebo). Only the first month was of interest for the review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomly selected and then assigned. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Identical pink capsules. Nurses, raters and patients were blind to the procedure. Treating physician was led to believe that half of the patients were on placebo, the other half on drug. |
| Blinding (performance bias and detection bias) | Low risk | Identical pink capsules. Nurses, raters and patients were blind to the procedure. Treating physician was led to believe that half of the patients were on placebo, the other half on drug. |
| Incomplete outcome data (attrition bias) | Unclear risk | It is unclear how many participants left the study during the first month. |
| Selective reporting (reporting bias) | High risk | Data on behaviour scales were not reported, including aggressive behaviour which was an outcome in our review. |
| Other bias | Low risk | No evidence for other bias. |
| Methods | Randomisation: unclear, randomisation assumed due to double‐blinding. | |
| Participants | Diagnosis: chronic schizophrenia (clinical diagnosis), all had previously responded to haloperidol and were adequately maintained on it. N=49. | |
| Interventions | 1. Drug: haloperidol tablets.* Flexible dose. Allowed dose range: n.i.. Mean dose: mean 8.8mg/day. N=17. 2. Drug: haloperidol liquid.* Flexible dose. Allowed dose range: n.i.. Mean dose: 10.4 mg/day. N=16. 3. Placebo: Duration of taper: 0 days. N=16. Rescue medication: antiparkinson medication was allowed. | |
| Outcomes | Examined: Relapse: deterioration of global state. Unable to use / Not included: Mental state: Brief Psychiatric Rating Scale (no SD / no predefined outcome of interest). Global state: Clinical Global Impression of Severity (no SD / no predefined outcome of interest). Behaviour: Nurses Observation Scale for Inpatient Evalutation (no SD / no predefined outcome of interest). Adverse effects: laboratory (insufficient data / no predefined outcome of interest), vital signs (insufficient data / no predefined outcome of interest). | |
| Notes | *Groups 1 and 2 were pooled for the purpose of this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Unclear, randomisation assumed due to double‐blinding. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, all participants received both (placebo) tablets and (placebo) liquid, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, all participants received both (placebo) tablets and (placebo) liquid, no further details. |
| Incomplete outcome data (attrition bias) | Low risk | Acceptable dropout rate (10%), which should not affect other outcomes (completer analysis). |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear other bias. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (DSM‐IV), duration ill at least 2 years, Positive and Negative Syndrome Scale total score <60 before randomised phase, Clinical Global Impression Severity Scale not more than moderately ill. N=197. | |
| Interventions | 1. Drug: quetiapine XR. Flexible dose 400‐800mg/day. Mean dose: 669mg/day. N=94. 2. Placebo: Duration of taper: 4 days.N=103. Rescue medication: anticholinergic medication, sleep medication, lorazepam, no additional antipsychotic drugs. | |
| Outcomes | Examined: Relapse: increase of Positive and Negative Syndrome Scale by at least 30 percent from baseline, Clinical Global Impression Scale much or very much worse, need for additional antipsychotic medication. Leaving the study early. Adverse events: open interviews. Global state: number of participants improved according to Clinical Global Impression Scale. Extrapyramidal side‐effects: use of antiparkinson medication, Barnes Akathisia Scale, Simpson Angus Scale, Aquired Involuntary Movements Scale. Unable to use / Not included: Mental state: Positive and Negative Syndrome Scale / no predefined outcome of interest. Laboratory: haematology, chemistry, glucose, Hba1c, insulin, lipids, urine analysis, thyroid function), ECG, vital signs, mean weight gain (all no predefined outcomes of interest). Compliance (pill count / no predefined outcome of interest). | |
| Notes | No participant terminated the preplanned study duration of one year. The authors reported that data after 6 months are not reliable because only a few patients were left. Therefore, relapse data after 6 months were not extracted. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Correct randomisation assumed, because recent study from industry. |
| Allocation concealment (selection bias) | Low risk | Correct allocation concealment assumed, because recent study from industry. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules. |
| Incomplete outcome data (attrition bias) | High risk | Overall drop‐out rate was 41%, most of them due to relapse (76%), which occured much more frequently in the placebo group. This difference in attrition may have biased the results of other outcomes than relapse. Kaplan‐Meier survival curve analysis was used for the primary outcome relapse. |
| Selective reporting (reporting bias) | High risk | Only adverse events with a frequency of at least 5% were reported. |
| Other bias | High risk | The study was terminated early after an interim analysis showed a clear superiority of quetiapine; there were certain baseline discrepancies in terms of mean age, duration ill and number of previous episodes. |
| Methods | Randomisation: randomised, computer‐generated randomised code. | |
| Participants | Diagnosis: chronic or subchronic schizophrenia DSM‐III‐R. N=146. | |
| Interventions | 1. Drug: ziprasidone. Fixed dose. Allowed dose range: 160 mg/day. Mean dose: 160mg/day. N=71. 2. Placebo: Duration of taper: 0 days. N=75. Rescue medication: other antipsychotics not allowed, concomitant medication for movement disorders, hypnotics, sedatives, anxiolytics. | |
| Outcomes | Examined: Relapse: as defined by CGI‐Improvement scale of 6 or more and/or score of 6 or more on PANSS items P7,G8 on two successive days. Adverse effects: number of participants with at least one adverse event, akathisia, dyskinesia, dystonia, tremor, use of antiparkinson medication, weight gain. Unable to use / Not included: Global state: mean Clinical Global Impression Severity Scale (no means, no SDs / no predefined outcome of interest). Mental state: Brief Psychiatric Rating Scale, AMDP system, Paranoid Depression Scale (all no means, no SDs / no predefined outcomes of interest). Functioning: Global Assessment Scale (no mean, no SD / no predefined outcome of interest). Subjective well‐being (own scale ‐ no mean, no SD). Adverse effects: extrapyramidal side‐effects (Aquired Involuntary Movement Scale ‐ no SD, Simpson Angus Scale, Dosage Record and Treatment Emergent Symptoms Scale ‐ all no means, no SDs / continuous side‐effect results were not among the prespecified outcome). Concept of illness (concept of illness scale ‐ no mean, no SD / no predefined outcome of interest). Physiological measures: routine laboratory, ECG, EEG physical exams and vital signs (all no data / no predefined outcome of interest). Pharmacokinetics (no predefined outcome of interest). Compliance: doctors’ assessment (no predefined outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomised code. |
| Allocation concealment (selection bias) | Low risk | Treatment cards numbered for each subject entering double‐blind phase, investigator and pharmacist was to allocate numbers to subjects in strict sequence of entry to study. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules. |
| Incomplete outcome data (attrition bias) | High risk | 68% overall dropout, most due to relapse, which occured much more frequently in the placebo group, thus not a problem for this outcome and for drop‐out but for other outcomes. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No evidence for other bias. |
| Methods | Randomisation: centrally randomised by a specialised unit using an "adaptive randomisation method”. | |
| Participants | Diagnosis: schizophrenia or schizoaffective disorder (ICD‐9 and Research Diagnostic Criteria). N=237. | |
| Interventions | 1. Drug: various antipsychotic drugs. Flexible dose, minimum 100mg/day chlorpromazine equivalent. Allowed dose range: 100 ‐ unlimited chlorpromazine equivalents/day. Mean dose: 201 mg/day. N=122. 2. No treatment (=crisis management, medication was only given in case of a full relapse). Duration of taper: 50% every two weeks, thus after 6 weeks only 12.5% of initial dose left, thus 42 days. Note that participants were not withdrawn after they had received crisis intervention. N=115. Rescue medication: in the no treatment group additional antipsychotic medication could only be given in case of relapse. | |
| Outcomes | Examined: Relapse: Brief Psychiatric Rating Scale total score ‐ >10 increase, Global Assessement Scale <20 reduction, deterioration Clinical Global Impression Scale CGI >7. Unable to use / Not included: Global state: Clinical Global Impression (no means, no SDs / no predefined outcome of interest). Mental state: Brief Psychiatric Rating Scale, AMDP system, Paranoid Depression Scale (all no means, no SDs / no predefined outcome of interest). Functioning: Global Assessment Scale (no mean, no SD / no predefined outcome of interest). Subjective well‐being (own scale ‐ no mean, no SD / no predefined outcome of interest). Adverse effects: extrapyramidal side‐effects (Aquired Involuntary Movement Scale ‐ no SD, Simpson Angus Scale, Dosage Record and Treatment Emergent Symptoms Scale ‐ all no means, no SDs / continuous side‐effect results were not among the predefined outcomes of interest). Concept of illness (concept of illness scale ‐ no mean, no SD). Compliance: doctors’ assessment (no predefined outcome of interest). Physiological measures: routine laboratory, ECG, EEG (no data / no predefined outcome of interest). | |
| Notes | There was a third group using intermittent treatment which was not of interest for this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Centrally randomised by a specialised unit using an "adaptive randomisation method”. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Open, only key rating scales were additionally rated by a second blind assessor. |
| Blinding (performance bias and detection bias) | Low risk | Open, only key rating scales were additionally rated by a second blind assessor. |
| Incomplete outcome data (attrition bias) | High risk | High two year discontinuation rate of 43.7%. Analysis was intention‐to‐treat based on Kaplan‐Meier survival curve analysis, completer analyses were presented in addition if different. A risk of bias can not be excluded given the high discontinuation rate. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear evidence for other bias. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: chronic schizophrenia (DSM‐IV), at least two years of continuous antipsychotic medication. N=310. | |
| Interventions | 1. Drug: aripiprazole. Fixed dose of 15mg/day. N=155. 2. Placebo: Duration of taper (days): n.i. (pre‐trial medication was tapered, when appropriate, before stopping treatment). N=155. Rescue medication: additional antipsychotic drugs were not allowed. | |
| Outcomes | Examined: Relapse: CGI at least minimally worse, a PANSS score of ‐ 5 (moderately severe) on the subscore items of hostility or uncooperativeness on 2 successive days; or a ‐ 20% increase in PANSS total score. Leaving the study early. Body weight (mean change and number of participants with increase of body weight). Unable to use / Not included: Global state: CGI (no SD; no dichotomous data / no predefined outcome of interest). Mental state: PANSS, BPRS (no SD / no predefined outcome of interest). Adverse effects: extrapyramidal side‐effects ‐ Simpson‐Angus Scale, Abnormal Involuntary Movement Scale, Barnes Akathisia Scale (all no SD / No predefined outcome of interest). Physiological measures: vital signs (pulse rate, systolic and diastolic blood pressure, no data / no predefined outcome of interest), laboratory (haematology, no data; serum chemistries, no data a apart from creatinine phosphate / no predefined outcome of interest) urine tests, ECG (both no data / no predefined outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Correct randomisation assumed, because recent study from industry.. |
| Allocation concealment (selection bias) | Low risk | Correct allocation concealment assumed, because recent study from industry. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, no further details. |
| Incomplete outcome data (attrition bias) | High risk | A high number of participants (62.2%) left the study early, mostly because of relapse (61%), which was more frequent in the placebo group. For other outcomes this could be a problem. For the primary outcome survival analysis was used which was not a full ITT (one post‐baseline/dose) but only few participants were excluded. |
| Selective reporting (reporting bias) | High risk | Only those adverse events that occurred in at least 5% of the participants in either group were reported. |
| Other bias | Low risk | No clear other bias. |
| Methods | Randomisation: "randomly assigned”, no further details. | |
| Participants | Diagnosis: schizophrenia (clinical diagnosis), continuously hospitalized for at least two years. N=420. | |
| Interventions | 1. Drug: chlorpromazine. Fixed dose of 300mg/day. N=208. *2. Drug: chlorpromazine. Fixed dose of 2000mg/day (titrated within 45 days, dose reduction to 1500mg/day was possible). N=208. 3. Placebo: Duration of taper: 0 days. N=212. *4. Routine treatment (any antipsychotic medication, any dose). N=210. Rescue medication: n.i., but probably not allowed. | |
| Outcomes | Examined: Relapse: apatient was considered relapsed if he regressed and had to be returned to known medication before the end of the 24 week period. Adverse effects: based on clinical interview. Unable to use / Not included: Mental state: Inpatient Multidimensional Psychiatric Scale, Brief Psychiatric Rating Scale (both only p‐values / no predefined outcome of interest). Global state: CGI severity (no predefined outcome of interest). Behaviour: Nurses’ Observation Scale for Inpatient Evaluation (only p‐values / no predefined outcome of interest). Readiness for discharge: Discharge‐Readiness Inventory (only p‐values / no predefined outcome of interest). Ophthalmologic examination (no predefined outcome of interest). | |
| Notes | *We only analysed the low dose group, because the high dose was excessively high (2000mg chlorpromazine per day) and because the conventional treatment group was not double‐blind. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomly assigned, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, liquid formulation. |
| Blinding (performance bias and detection bias) | Low risk | Double, liquid formulation. |
| Incomplete outcome data (attrition bias) | High risk | Overall 26% dropped out (of which 87% due to relapse). 15% of the participants in the drug group compared to 38% of the participants in the placebo group left the study early. This difference in attrition is a problem for the analysis of other outcomes than relapse. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear other bias. |
| Methods | Randomisation: randomised, no further details. | |
| Participants | Diagnosis: chronic schizophrenia (clinical diagnosis), hospitalised for at least 2 years. Gender: n.i.. | |
| Interventions | 1. Drug: high dose trifluoperazine. Fixed dose of 80mg/day (reached within 35 days). N=117. 2. Drug: low dose trifluoperazine. Fixed dose of 15mg/day. N=113. 3. Placebo: Duration of taper: 0 days. N=111. Rescue medication: not indicated, but probably not allowed. | |
| Outcomes | Examined: Relapse: worsening of global state. Adverse effects: clinical interview based on 40 items checklist. Unable to use / Not included: Mental state: Inpatient Multidimensional Psychiatric Scale, Brief Psychiatric Rating Scale (both only p‐values / no predefined outcome of interest). Global state: CGI (no predefined outcome of interest). Behaviour: Nurses’ Observation Scale for Inpatient Evaluation (only p‐values / no predefined outcome of interest). Readiness for discharge: Discharge‐Readiness Inventory (only p‐values / no predefined outcome of interest). Ophthalmologic examination (no predefined outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules. Whether blinding was successful was not assessed, although in one group high doses associated with a lot of side‐effects were administered. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules. Whether blinding was successful was not assessed, although in one group high doses associated with a lot of side‐effects were administered. |
| Incomplete outcome data (attrition bias) | High risk | The overall attrition was considerable (33%) and clearly more participants discontinued the study early in the placebo group (53%) than in the two drug groups (23%), mainly due to inefficacy, which can be a problem for other outcomes than relapse. Not all participants were included in the final analysis. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | High risk | The high‐dose group used too high doses (80mg/day) for current standards, even the low‐dose would nowadays be considered to be quite high /15mg/day). |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (hospital diagnosis, there was an additional evaluation based on research criteria (Kraepelinian), but the results of all participants are presented here), in remission (no positive symptoms, but other symptoms could be present). Patients who were uncooperative in the stabilisation phase were not included in the study. N=73. | |
| Interventions | 1. Drug: fluphenazine decanoate combined with procyclidine Flexible dose of 0.5‐2.0ml biweekly. Mean dose: n.i.. N=23. 2. Drug: oral fluphenazine combined with procyclidine. Flexible dose of 5‐20mg/day. Mean dose: n.i.. N=28. 3. Placebo: Duration of taper: 0 days. N=22. Rescue medication: not clearly indicated, but probably not allowed. | |
| Outcomes | Examined: Relapse: substantial deterioration with a potential of marked social impairment. Leaving the study early. Adverse effects: dropout due to specific adverse events. Unable to use / Not included: Global state (CGI ‐ no SD, data for relapsed subgroup only). mental state (Brief Psychiatric Rating Scale ‐ no SD, data for relapsed subgroup only). Social adjustment: Katz Adjustment Scale ‐ no SD, only data for relapsed subgroup and a matched but not randomised subsample. Akinesia: Periodic Evaluation Record (no SD, data for relapsed subgroup only). Death. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Low risk | Double‐dummy technique, procyclidine was added to fluphenazine to avoid unmasking by extrapyramidal side‐effects. |
| Blinding (performance bias and detection bias) | Low risk | Double‐dummy technique, procyclidine was added to fluphenazine to avoid unmasking by extrapyramidal side‐effects. |
| Incomplete outcome data (attrition bias) | High risk | 67% of the participants discontinued the study due to relapse (41%) or other reasons. More participants in the drug group discontinued due to adverse events, while more participants in the placebo group discontinued due to relapse. This differential attrition can cause bias. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No evidence for other bias. |
| Methods | Randomisation: divided into two comparable groups by an unbiased statistician. | |
| Participants | Diagnosis: chronic psychotic inpatients (clinical diagnosis), 13 schizophrenia, 1 dementia, 1 paranoia. N=15. | |
| Interventions | 1. Drug: penfluridol. Fixed/flexible dose: unclear, but different doses according to pretrial medication. Allowed dose range: unclear, but all participants received 40mg/week. Mean dose: 40mg/week. N=7. 2. Placebo: Duration of taper: 0 days. N=8. Rescue medication: | |
| Outcomes | Examined: Relapse: need of additional antipsychotic medication. Leaving the study early. Unable to use / Not included: Mental state: Zwanikken Scale (no mean, no SD / no predefined outcome of interest). Behaviour: Zwanikken Scale (no mean, no SD / no predefined outcome of interest). Adverse effects: interview (no data). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Divided into two comparable groups by an unbiased statistician. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not explained. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules. |
| Incomplete outcome data (attrition bias) | Low risk | No participant left the study early. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear other bias. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (DSM‐III), not dangerous to themselves, no hospitalisation in the last year. N=23. | |
| Interventions | Before randomisation all participants were put on haloperidol for one month or until they were considered stable. 1. Drug: haloperidol. Fixed dose (dose before randomisation was maintained). Mean dose: n.i.. N=11. 2. Placebo: Duration of taper: 14 days. N=12. Rescue medication: n.i., but probably not allowed. | |
| Outcomes | Examined: Relapse: significant clinical design defined by either reoccurrence of symptoms or worsening of existing symptoms or prodromals signs such as sleep problems or anxiety. Unable to use / Not included: Mental state: BPRS (no data for each group / no predefined outcome of interest). Quality of life: Heinrich Scale (no data for each group). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, "participants and investigators were blind to treatment”, no further details. |
| Blinding (performance bias and detection bias) | Low risk | Double, "participants and investigators were blind to treatment”, no further details. |
| Incomplete outcome data (attrition bias) | Unclear risk | 47% of the participants left the study early, most of them due to a relapse (55%). This attrition can be a source of bias for other outcomes than relapse. |
| Selective reporting (reporting bias) | High risk | Data on quality of life were not reported. |
| Other bias | Low risk | No clear evidence for other bias. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: chronic schizophrenia (Research Diagnostic Criteria), stable for at least 5 years (absence of clinical deterioration and/or an increase of neuroleptic medication, retrospectively and in addition prospectively for at least 12 months), all on fluphenazine decanoate. N=24. | |
| Interventions | 1. Drug: fluphenazine decanoate.Fixed dose: mean 50.4mg/4 weeks. N=12. 2. Placebo: Duration of taper: 0 days, but all participants were on depot medication before the study. N=12. Rescue medication: n.i., but probably not allowed. | |
| Outcomes | Examined: Relapse: at least 25% increase of Brief Psychiatric Rating Scale total score and judgement of by nurse according to Psychotic Inpatient Profile. Unable to use / Not included: Mental state: Brief Psychiatric Rating Scale total, Psychotic Inpatient Profile (for both scales means for subgroups only / no predefined outcome of interest). Physiological measures: prolactin levels (no SD’s / no predefined outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, placebo was sesame oil of identical volume and identical in physical appearance. |
| Blinding (performance bias and detection bias) | Low risk | Double, placebo was sesame oil of identical volume and identical in physical appearance. |
| Incomplete outcome data (attrition bias) | Unclear risk | There is no statement on participants leaving the study early. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | High risk | There was a baseline imbalance in terms of gender and in terms of baseline fluphenazine dose. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (DSM‐IV). N=386. | |
| Interventions | 1. Drug: asenapine. Fixed dose (same dose as at end of stabilisation phase): mean 17.6 mg/day. N=194. 2. Placebo: Duration of taper: 0 days. N=192. Rescue medication: benzodiazepines, anticholinergics, antidepressants. | |
| Outcomes | Examined: Relapse: CGI‐severity >=4, moderately ill for one week was accompanied by: PANSS total score increase >=20% (a 10 point increase if PANSS was lower than 50), a PANSS item score >=5 on hostility of uncooperativeness or a PANSS item score >=5 and two items of unusual thought content, conceptual disorganisation or hallucinatory behaviour. Relapse was also judged to appear if in the investigator's opinion schizophrenia, risk of violence to self or others, or suicide risk increased so >=1 of the following was required: an additional >=2mg/day lorazepam, compared with the highest open label dose for 1 week, addition of antipsychotic, addition or dosage increase of an antidepressant or mood‐stabiliser, increased psychiatric care, arrest or imprisonment, electroconvulsive therapy, or other relevant measures. Death: suicidal ideation, suicide attempts. Adverse effects: at least one adverse event, at least one movement disorder, akathisia, sedation, weight gain. Unable to use / Not included: Mental state: PANSS (no predefined outcome of interest). Global state: CGI (no predefined outcome of interest). Leaving the study early (data are unclear). Hospitalisation (no data). Electrocardiogram (no predefined outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules in taste. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules in taste. |
| Incomplete outcome data (attrition bias) | High risk | High dropout rate, but exact number of drop‐outs could not be calculated. Drop‐outs were not clearly enough reported. Survival curve analysis was used for the primary outcome relapse. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No evidence for selective reporting. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (clinical diagnosis), all withdrawn of subject to periodic disturbances, all needed supervision or management. N=80. | |
| Interventions | 1. Drug: chlorpromazine; flexible dose; allowed dose range 200 to 1000 mg/day; mean dose: 894 mg/day (here mean maximum dose); N=20 2. Drug: trifluoperazine; flexible dose; allowed dose range 10 to 50 mg/day; mean dose: 29 mg/day (here mean maximum dose); N=20 3. Drug: thioridazine; flexible dose; allowed dose range 200 to 1000 mg/day; mean dose: 958 mg/day (here mean maximum dose); N=20 4. Placebo: duration of taper: 0 days; N=20 Rescue medication: phenobarbital and bentropine methansulfonate, no additional antipsychotic drugs | |
| Outcomes | Examined: Relapse: worsening of global state Adverse effects: clinical interview, number of participants receiving antiparkinson medication Unable to use / Not included: Global state: CGI‐Severity Scale (no predefined outcome of interest) Behaviour: Manifest Behaviour Scale (no SD / no predefined outcome of interest) Personality: Minnesota Multiphasic Personality Inventory (no SD / no predefined outcome of interest) | |
| Notes | The results of all drug groups were pooled | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details |
| Allocation concealment (selection bias) | Low risk | Only the hospital pharmacist had the code on what medication the patient was on |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules, each participant had his own container. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules, each participant had his own container. |
| Incomplete outcome data (attrition bias) | Low risk | Only 3 out of 80 participants left the study early and the reasons were well described. |
| Selective reporting (reporting bias) | Low risk | No selective reporting. |
| Other bias | Low risk | No evidence for other bias. |
| Methods | Randomisation: matched and then randomised by a research assistant. | |
| Participants | Diagnosis: chronic schizophrenia (clinical diagnosis), less than 50 years, on chlorpromazine for at least six months, had reached a stable improved state. N=80. | |
| Interventions | 1. Drug: chlorpromazine. Fixed dose of 200mg/day. N=40. 2. Drug: reserpine*. Fixed dose of 2 mg/day. N=40. 3. Placebo: Duration of taper 0 days. N=40. Rescue medication: not indicated, probably not allowed. | |
| Outcomes | Examined: Leaving the study early. Unable to use / Not included: Mental state: Lorr Multidimensional Scale for Rating Psychiatric Patients (no SD / no predefined outcome of interest). Behaviour: Psychiatric Behaviour Rating Scales (no SD / no predefined outcome of interest). | |
| Notes | *this group was not used in the analysis. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Matched and then randomised by a research assistant. |
| Allocation concealment (selection bias) | Low risk | By a research assistant who carefully guarded the identity of patients and the assigned treatment regimen. Furthermore, medication was assigned by the director of professional services who kept the names for use in case a patient had to be withdrawn from the study. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules. |
| Incomplete outcome data (attrition bias) | Low risk | Overall 11% dropped out, most of them due to relapse (88%) in the placebo group. As relapse, drop‐out and suicide were the only outcomes, this did not produce a risk of bias. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear evidence of other bias. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (Schedule for Affective Disorder and Schizophrenia, and Research Diagnostic Criteria), all had previously responded to antipsychotic drugs. N=100. | |
| Interventions | 1. Drug: various antipsychotic drugs. Fixed/flexible dose: probably flexible. Allowed dose range: n.i.. Mean dose: n.i.. N=36. 2. Placebo: Duration of taper 0 days. N=64. Rescue medication: n.i.. | |
| Outcomes | Examined: Relapse: first signs of symptoms according to ward staff and project nurse, full deterioration was not waited for. Unable to use / Not included: Performance tests: Rohrschach test, Wechsler Adult Intelligence Scale (all no clear mean’s, n´s, no SD’s / no predefined outcomes of interest). Mental state: Brief Psychiatric Rating Scale (no clear mean, no number of participatns, no SD / no predefined outcome of interest). Thought disorder: Thought Disorder Index, Psychological Rating Scale (all no clear mean’s, no SD’s / no predefined outcomes of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not explained. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, placebo matching in kind and dose the previous medication. |
| Blinding (performance bias and detection bias) | Low risk | Double, placebo matching in kind and dose the previous medication. |
| Incomplete outcome data (attrition bias) | Unclear risk | Unclear, because these have not been indicated. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Unclear risk | Unclear, baseline data have not been presented for both groups separately. |
| Methods | Randomisation: randomised, no further details. | |
| Participants | Diagnosis: schizophrenia without positive symptoms (clinical diagnosis). N=43. | |
| Interventions | 1. Drug: various phenothiazines, mainly chlorpromazine. Fixed/flexible dose: flexible. Allowed dose range: not limited, but complete discontinuation was not allowed. Mean dose: 150‐200mg/day chlorpromazine. N=24. 2. Placebo: Duration of taper: 0 days. N=19. Rescue medication: not allowed. | |
| Outcomes | Examined: Relapse: clinical judgement. Service use: number of participants rehospitalised. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, no further details. |
| Allocation concealment (selection bias) | Low risk | Psychiatrist without contact to the participants held the key and filled the medication containers. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, exact placebo replicas. |
| Blinding (performance bias and detection bias) | Low risk | Double, exact placebo replicas. |
| Incomplete outcome data (attrition bias) | Unclear risk | Unclear ‐ whether participants discontinued the study prematurely was not reported. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | High risk | Some placebo participants continued to take medication, study terminated early. |
| Methods | Randomisation: randomised, no further details. | |
| Participants | Diagnosis: chronic schizophrenia (DSM‐II), catatonic type (n=2), residual type (n=15), hebephrenic type (n=1), simple type (n=2), paranoid type (n=1). N=21. | |
| Interventions | 1. Drug: penfluridol. Fixed dose, mean 43mg/week. N=10. 2. Placebo: Duration of taper: 0 days. N=11. Rescue medication: antiparkinson medication, haloperidol, but this was considered to be a sign of relapse. | |
| Outcomes | Examined: Relapse: use of additional haloperidol. Leaving the study early. Unable to use / Not included: Mental state: Zwanikken scale (no data / no predefined outcome of interest). Adverse effects: Zwanikken scale (no data / continuous side‐effect results were not among the predefined outcomes of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, identical capsules. |
| Blinding (performance bias and detection bias) | Low risk | Double, identical capsules. |
| Incomplete outcome data (attrition bias) | Low risk | No participant left the study prematurely. |
| Selective reporting (reporting bias) | High risk | Data on side‐effects and the mental state were not reported. |
| Other bias | Low risk | No evidence for other bias. |
| Methods | Randomisation: arbitrarily allocated. | |
| Participants | Diagnosis: chronic schizophrenia (clinical diagnosis by at least two psychiatrists), all with paranoid condition, two additionally catatonic tendencies and one hebephrenic features, six were leucotomised. N=26. | |
| Interventions | 1. Drug: perphenazine liquid. Fixed dose (same dose as before the start of the study) two 12mg tid, one 20mg tid, all other 8mg tid and most less. Mean dose: see above. N=13. 2. Placebo. Duration of taper: 0 days. N=13. 3. No medication*. Duration of taper: 0 days. N=13. Rescue medication: not allowed apart from antiparkinson medication. | |
| Outcomes | Examined: Relapse: "major relapse" = replaced on active medication. Unable to use / Not included: Mental state: self‐developed psychiatric rating scale ‐ unpublished scale (no predefined outcome of interest). Behaviour: Fergus Falls Behaviour Rating Scale (no mean, no SD / no predefined outcome of interest). | |
| Notes | *This group was not used for the review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Arbitrarily allocated. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Low risk | Double ‐ only the pharmacist knew which bottles were active. Participants were asked whether they were aware of the medication, but only one realised a change in taste. Nurses were also asked, but did not guess the correct medication better than by chance alone. |
| Blinding (performance bias and detection bias) | Low risk | Double ‐ only the pharmacist knew which bottles were active. Participants were asked whether they were aware of the medication, but only one realised a change in taste. Nurses were also asked, but did not guess the correct medication better than by chance alone. |
| Incomplete outcome data (attrition bias) | Unclear risk | Dropouts were not reported. It is not clear, whether there really no dropouts. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No clear evidence for other bias. |
| Methods | Randomisation: random, no further details. | |
| Participants | Diagnosis: schizophrenia (according to Bleuler’s concept, with three primary symptoms), duration ill at least 2 years. N=41. | |
| Interventions | 1. Drug: fluphenazine depot (most around 12.5 ‐ 25 mg/3 weeks, mean 21.42mg/3 weeks) or flupenthixol depot (most around 20‐40mg/3 weeks, mean 27.5/3 weeks) ‐ Fixed dose. N=24. 2. Placebo: Duration of taper: 0 days. N=17. Rescue medication: chloral hydrate, antiparkinson medication, additional antipsychotic drugs were not allowed. | |
| Outcomes | Examined: Relapse: psychotic behaviour or increase in six subscales of the Comprehensive Psychopathological Rating Scale. Unable to use / Not included: Mental state: Comprehensive Psychopathological Rating Scale (no SD / no predefined outcome of interest). Behaviour: Nurses Observation Scale of Inpatient Evaluation (no SD / no predefined outcome of interest). Adverse effects: extrapyramidal side‐effects (Simpson Angus Scale, Acquired Involuntary Movements Scale, Akathisia Rating Scale (all no SD, akathisia scale was not published / continuous side‐effect results were not among the predefined outcomes of interest). Physiological measures: various laboratory tests (no data / no predefined outcome of interest). Life events (Life Event Scale / no predefined outcome of interest). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random, no further details. |
| Allocation concealment (selection bias) | Unclear risk | Procedure not described. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, placebo sesame oil. |
| Blinding (performance bias and detection bias) | Low risk | Double, placebo sesame oil. |
| Incomplete outcome data (attrition bias) | Low risk | Overall 3 (7%) out of 41 participants left the study early. Although only completers were analysed, due to the low rate this is not a problem. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No obvious risk for other bias. |
| Methods | Randomisation: randomly assigned according to pre‐established randomisation code. | |
| Participants | Diagnosis: chronic schizophrenia (Feighner’s criteria), treated with antipsychotic drugs for at least 2 years and currently under control. N=32. | |
| Interventions | 1. Drug: haloperidol decanoate. Flexible dose. Allowed dose range: starting dose 1.5 ml (=150mg) four‐weekly, maximum 3ml (=300mg) four‐weekly. Median dose 1.5 ml four‐weekly. N=16. 2. Placebo: Duration of taper: 0 days. N=16. Rescue medication: antiparkinson medication, oral haloperidol, but this was considered to be a relapse. | |
| Outcomes | Examined: Relapse: addition of oral haloperidol. Leaving the study early. Adverse effects: open interviews. Unable to use / Not included: Mental state: Brief Psychiatric Rating Scale (no SD / no predefined outcome of interest). Global state: Clinical Global Impression Severity Scale (no predefined outcome of interest). Behaviour: Nurses Observation Scale for Inpatient Evaluation (no SD / no predefined outcome of interest). Adverse effects: use of antiparkinson medication (only indicated for haloperidol group), at least one movement disorder and sedation (patients received haloperidol). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomly assigned according to pre‐established randomisation code. |
| Allocation concealment (selection bias) | Low risk | Randomisation code was unknown to the evaluating investigators. |
| Blinding (performance bias and detection bias) | Unclear risk | Double, administered by a particular nurse. |
| Blinding (performance bias and detection bias) | Low risk | Double, administered by a particular nurse. |
| Incomplete outcome data (attrition bias) | Low risk | 12 out of 16 participants in the placebo group compared to 0 out of 16 in the haloperidol group were withdrawn from the trial due to inefficacy of treatment. As the only outcomes were relapse, number of participants improved and leaving the study early this should not have been a problem. |
| Selective reporting (reporting bias) | Low risk | No evidence for selective reporting. |
| Other bias | Low risk | No other bias. |
General abbreviations
CNS: central nervous system
CPZ: chlorpromazine
DSM: Diagnostic and Statistical Manual of Mental Disorders
ECG: electrocardiography
ECT: electroconvulsive therapy
EASY: Early Assessment Service for Young People with Psychosis
EEG: electroencephalography
EPS: extrapyramidal symptoms
HbA1c: glycated haemoglobin
ICD: International Statistical Classification of Diseases and Related Health Problems
IM: intramuscular injection
ITT: intention to treat
LOCF: last observation carried forward
NI: not indicated
SD: standard deviation
tid: ter in die (3 times a day)
Rating scales
AIMS: Abnormal Involuntary Movement Scale
AMDP: Arbeitsgemeinschaft für Methodik und Dokumentation in der Psychiatrie
BAS: Barnes Akathisia Scale
CGI: Clinical Global Impression
BPRS: Brief Psychiatric Rating Scale
GAS: Global Assessment Scale
IMPS: Inpatient Multidimensional Psychiatric Rating Scale
MMPI: Minnesota Multiphasic Personality Inventory
NOSIE: Nurses Observation Scale for Inpatient Evaluation
PANSS: Positive And Negative Syndrome Scale
PRP: Psychotic Reaction Profile
PRS: Psychiatric Rating Scale
PSE: Present State Examination
RDC: Research Diagnostic Criteria
SADS: Schedule for Affective Disorders
SANS: Scale for the Assessment of Negative Symptoms
SAS: Simpson‐Angus Scale
Characteristics of excluded studies [ordered by study ID]
Jump to:
| Study | Reason for exclusion |
| Allocation: controlled clinical trial, not randomised. | |
| Allocation: randomised. Participants: not stabilised on antipsychotic drugs. | |
| Allocation: not randomised, matched groups. | |
| Allocation: not randomised. | |
| Allocation: not randomised. | |
| Allocation: randomised. Participants: schizophrenia. Intervention: thiothixene alone versus thiothixene plus group therapy versus chlorpromazine alone versus chlorpromazine plus group therapy. | |
| Allocation: not randomised. | |
| Allocation: not randomised. | |
| Allocation: not randomised. | |
| Allocation: not randomised. | |
| Allocation: not randomised. | |
| Allocation: randomised. Participants: schizophrenia. Intervention: all participants were on neuroleptics and antiparkinson medication at baseline. They were then randomised to neuroleptics plus continuation of antiparkinson medication versus neuroleptics alone. | |
| Allocation: randomised. Participants: chronic schizophrenic outpatients, not truly stabilised on antipsychotic drugs. | |
| Allocation: randomised. Participants: first‐episode psychosis. Intervention: treatment as usual (including antipsychotics) versus multimodal relapse prevention therapy (including antipsychotics and cognitive behavioral therapy/family intervention). | |
| Allocation: not randomised. | |
| Allocation: randomised. Participants: schizophrenia. Interventions: chlorpromazine versus placebo. Outcomes: no usable outcome. | |
| Allocation: randomised. Participants: chronic schizophrenic patients. Intervention: abrupt versus gradual withdrawal of chlorpromazine, but chlorpromazine was withdrawn from both groups. Thus not appropriate control group. | |
| Allocation: not randomised. | |
| Allocation: not randomised. | |
| Allocation: not randomised. | |
| Allocation: randomised. Participants: 50% not diagnosed as with schizophrenia. | |
| Allocation: not randomised. | |
| Allocation: not randomised. | |
| Allocation: randomised. Participants: participants were acutely ill, not stable. | |
| Allocation: randomised. Participants: not stable, not all on antipsychotics before the study. | |
| Allocation: randomised. Participants: participants were not stable, most not on antipsychotics before the study. | |
| Allocation: randomised. Participants: men with schizophrenia. Intervention: chlorpromazine versus placebo. Outcome: no usable outcome. | |
| Allocation: not randomised. | |
| Allocation: part of the participants was matched, not randomised. | |
| Allocation: not randomised. | |
| Allocation: randomised. Participants: schizophrenia. Intervention: chlorpromazine versus chlorpromazine plus propranolol. | |
| Allocation: not randomised. | |
| Allocation: not randomised. | |
| Allocation: randomised. Participants: chronic schizophrenia. Intervention: chlorpromazine, placebo, orphenadrine. Outcome: no relevant outcome, only auditory attention task. | |
| Allocation: not randomised. | |
| Allocation: randomised. Participants: chronic schizophrenia. Intervention: fluphenazine elixir plus placebo injection versus fluphenazine enanthate injection plus oral placebo. | |
| Allocation: randomised. Participants: not stable. | |
| Allocation: not randomised. | |
| Allocation: not randomised. | |
| Allocation: randomised. Participants: schizophrenia, not stabilised on antipsychotic drugs, because all had been withdrawn from antipsychotic drugs for 8‐20 months before study start. | |
| Allocation: randomised, but switch study with very short duration (3‐5 days). | |
| Allocation: randomised. Participants: schizophrenia. Intervention: depot antipsychotics (fluphenazine depot, flupenthixol depot or clopenthixol depot) plus oral dihomo gammalinolenic acid (DHLA) versus oral DHLA plus placebo injections versus DHLA placebo capsules and placebo injections. What is lacking is a depot antipsychotic only group. | |
| Allocation: not randomised. | |
| Allocation: randomised. Participants: psychotic participants. Intervention: fluphenazine enanthate versus fluphenazine decanoate. | |
| Allocation: randomised. Participants: schizophrenia. Intervention: continuation of current antipsychotic versus gradual withdrawal. However, antipsychotic was given again when early warning signs appeared, i.e. intermittent treatment, a design that was excluded a prior by our protocol. | |
| Allocation: not randomised. | |
| Allocation: randomised. Participants: schizophrenia and related psychotic disorder. Intervention: continuation of current antipsychotic versus gradual withdrawal. However, antipsychotic was given again when early warning signs appeared, i.e. intermittent treatment, a design that was excluded by the protocol. Approximately 50% of participants were never withdrawn. | |
| Allocation: all participants were in hospital. 95 were allocated to placebo (not randomly). Then 81 participants were "selected at random to match” the intervention group. We feel that this is no appropriate randomisation method. | |
| Allocation: randomised. Participants: more than 50% had mental retardation, not schizophrenia. |
Characteristics of ongoing studies [ordered by study ID]
Jump to:
| Trial name or title | A randomised double‐blind placebo‐controlled parallel group study evaluating paliperidone palmitate in the prevention of recurrence in patients with schizophrenia. |
| Methods | Allocation: randomised, no further details. Blinding: double‐blind, no further details. Location: multicentre study. Duration: the study consists of 5 periods: an up to 7‐day screening/washout/tolerability period, a 9‐week open‐label transition period, a 24‐week open‐label maintenance period, a randomised, variable‐length double‐blind, placebo‐controlled recurrence prevention period, and an up to 52‐week open‐label extension period. |
| Participants | Diagnosis: stable and symptomatic schizophrenia according to DSM‐IV‐TM. |
| Interventions | 1. Paliperidone palmitate. 2. Placebo. |
| Outcomes | The primary outcome is the time from randomisation to the first recurrence. Mental state: PANSS. Global state: CGI‐S. Personal and Social Performance Scale, adverse events, labs and ECG‐tests. |
| Starting date | March 2005. |
| Contact information | ClinicalTrials.gov identifier: NCT00111189. |
| Notes |
CGI: Clinical Global Impression
DSM: Diagnostic and Statistical Manual of Mental Disorders
ECG: electrocardiography
PANSS: Positive And Negative Syndrome Scale
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Relapse: up to 3 months Show forest plot | 34 | 3942 | Risk Ratio (M‐H, Random, 95% CI) | 0.30 [0.24, 0.38] |
| Analysis 1.1  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 1 Relapse: up to 3 months. | ||||
| 2 Relapse: 4 to 6 months Show forest plot | 40 | 5285 | Risk Ratio (M‐H, Random, 95% CI) | 0.35 [0.30, 0.42] |
| Analysis 1.2 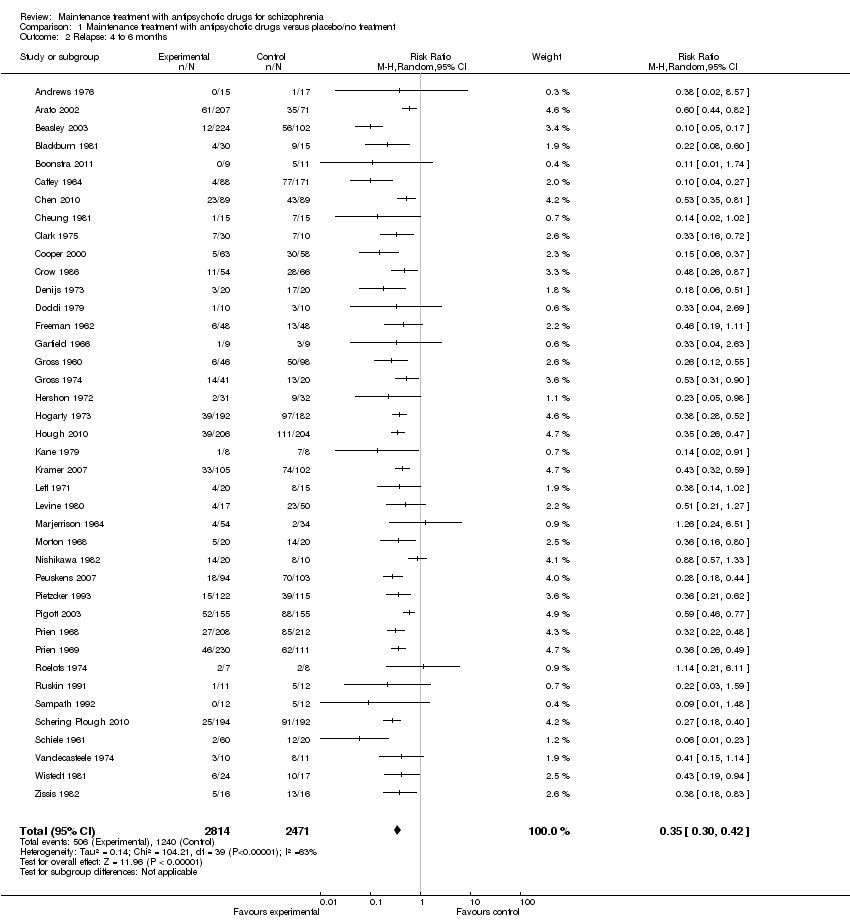 Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 2 Relapse: 4 to 6 months. | ||||
| 3 Relapse: 7 to 12 months Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| Analysis 1.3 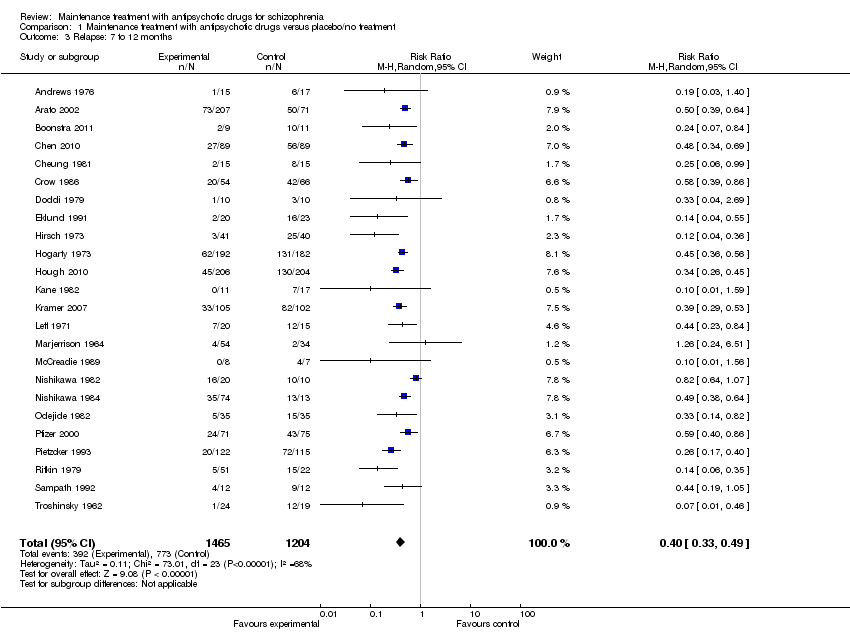 Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 3 Relapse: 7 to 12 months. | ||||
| 4 Relapse: > 12 months Show forest plot | 6 | 811 | Risk Ratio (M‐H, Random, 95% CI) | 0.59 [0.42, 0.82] |
| Analysis 1.4  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 4 Relapse: > 12 months. | ||||
| 5 Relapse: independent of duration Show forest plot | 62 | 6392 | Risk Ratio (M‐H, Random, 95% CI) | 0.35 [0.29, 0.41] |
| Analysis 1.5  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 5 Relapse: independent of duration. | ||||
| 6 Leaving the study early: due to any reason Show forest plot | 47 | 4718 | Risk Ratio (M‐H, Random, 95% CI) | 0.53 [0.46, 0.61] |
| Analysis 1.6  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 6 Leaving the study early: due to any reason. | ||||
| 6.1 up to 3 months | 8 | 245 | Risk Ratio (M‐H, Random, 95% CI) | 0.23 [0.07, 0.72] |
| 6.2 4 to 6 months | 17 | 1646 | Risk Ratio (M‐H, Random, 95% CI) | 0.48 [0.35, 0.66] |
| 6.3 7 to 12 months | 18 | 2420 | Risk Ratio (M‐H, Random, 95% CI) | 0.55 [0.46, 0.66] |
| 6.4 > 12 months | 4 | 407 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.36, 1.26] |
| 7 Leaving the study early: due to adverse events Show forest plot | 43 | 4333 | Risk Ratio (M‐H, Random, 95% CI) | 1.16 [0.70, 1.91] |
| Analysis 1.7  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 7 Leaving the study early: due to adverse events. | ||||
| 7.1 up to 3 months | 8 | 245 | Risk Ratio (M‐H, Random, 95% CI) | 2.84 [0.12, 65.34] |
| 7.2 4 to 6 months | 14 | 1549 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.57, 1.74] |
| 7.3 7 to 12 months | 17 | 2339 | Risk Ratio (M‐H, Random, 95% CI) | 1.24 [0.59, 2.60] |
| 7.4 > 12 months | 4 | 200 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 8 Leaving the study early: due to inefficacy Show forest plot | 46 | 4546 | Risk Ratio (M‐H, Random, 95% CI) | 0.37 [0.31, 0.44] |
| Analysis 1.8  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 8 Leaving the study early: due to inefficacy. | ||||
| 8.1 up to 3 months | 9 | 295 | Risk Ratio (M‐H, Random, 95% CI) | 0.23 [0.07, 0.79] |
| 8.2 4 to 6 months | 16 | 1661 | Risk Ratio (M‐H, Random, 95% CI) | 0.41 [0.31, 0.54] |
| 8.3 7 to 12 months | 18 | 2420 | Risk Ratio (M‐H, Random, 95% CI) | 0.36 [0.28, 0.45] |
| 8.4 > 12 months | 3 | 170 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.08, 0.95] |
| 9 Global state: number of participants improved Show forest plot | 14 | 1524 | Risk Ratio (M‐H, Random, 95% CI) | 2.34 [1.68, 3.26] |
| Analysis 1.9  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 9 Global state: number of participants improved. | ||||
| 9.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 4.61 [1.22, 17.40] |
| 9.2 4 to 6 months | 8 | 1037 | Risk Ratio (M‐H, Random, 95% CI) | 2.33 [1.69, 3.21] |
| 9.3 7 to 12 months | 5 | 438 | Risk Ratio (M‐H, Random, 95% CI) | 1.95 [0.91, 4.18] |
| 10 Service use: number of participants hospitalised Show forest plot | 16 | 2090 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.27, 0.55] |
| Analysis 1.10  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 10 Service use: number of participants hospitalised. | ||||
| 10.1 up to 3 months | 2 | 55 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.04, 4.06] |
| 10.2 4 to 6 months | 3 | 109 | Risk Ratio (M‐H, Random, 95% CI) | 0.08 [0.01, 0.42] |
| 10.3 7 to 12 months | 8 | 1295 | Risk Ratio (M‐H, Random, 95% CI) | 0.32 [0.18, 0.57] |
| 10.4 > 12 months | 3 | 631 | Risk Ratio (M‐H, Random, 95% CI) | 0.56 [0.44, 0.70] |
| 11 Service use: number of participants discharged Show forest plot | 3 | 404 | Risk Ratio (M‐H, Random, 95% CI) | 2.76 [0.69, 11.06] |
| Analysis 1.11 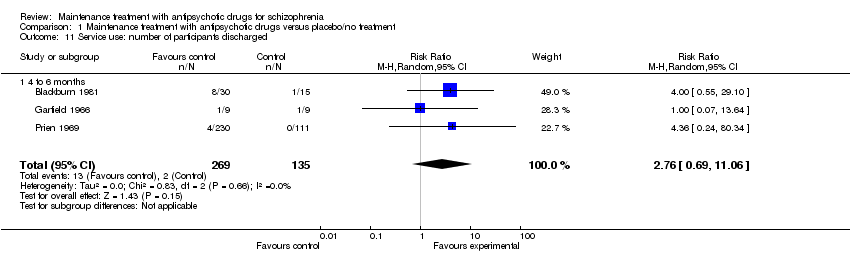 Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 11 Service use: number of participants discharged. | ||||
| 11.1 4 to 6 months | 3 | 404 | Risk Ratio (M‐H, Random, 95% CI) | 2.76 [0.69, 11.06] |
| 12 Death: any Show forest plot | 14 | 2356 | Risk Ratio (M‐H, Random, 95% CI) | 0.77 [0.28, 2.11] |
| Analysis 1.12 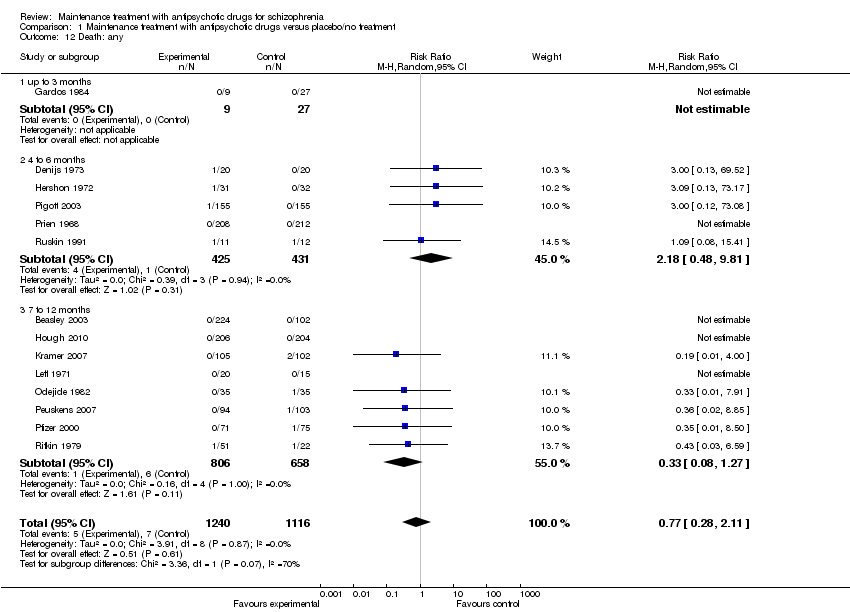 Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 12 Death: any. | ||||
| 12.1 up to 3 months | 1 | 36 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 12.2 4 to 6 months | 5 | 856 | Risk Ratio (M‐H, Random, 95% CI) | 2.18 [0.48, 9.81] |
| 12.3 7 to 12 months | 8 | 1464 | Risk Ratio (M‐H, Random, 95% CI) | 0.33 [0.08, 1.27] |
| 13 Death: due to natural causes Show forest plot | 14 | 2401 | Risk Ratio (M‐H, Random, 95% CI) | 1.24 [0.39, 3.97] |
| Analysis 1.13  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 13 Death: due to natural causes. | ||||
| 13.1 4 to 6 months | 5 | 856 | Risk Ratio (M‐H, Random, 95% CI) | 2.18 [0.48, 9.81] |
| 13.2 7 to 12 months | 9 | 1545 | Risk Ratio (M‐H, Random, 95% CI) | 0.54 [0.09, 3.36] |
| 14 Suicide Show forest plot | 8 | 1941 | Risk Ratio (M‐H, Random, 95% CI) | 0.34 [0.04, 3.28] |
| Analysis 1.14 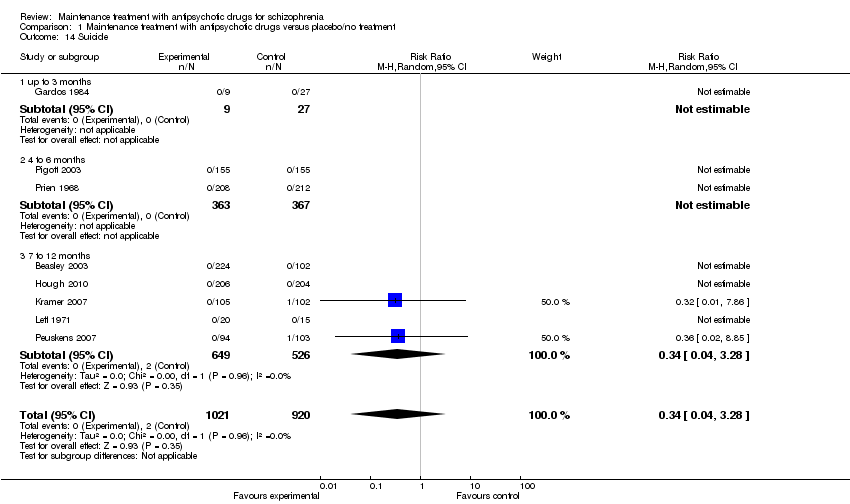 Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 14 Suicide. | ||||
| 14.1 up to 3 months | 1 | 36 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 14.2 4 to 6 months | 2 | 730 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 14.3 7 to 12 months | 5 | 1175 | Risk Ratio (M‐H, Random, 95% CI) | 0.34 [0.04, 3.28] |
| 15 Suicide attempts Show forest plot | 5 | 1177 | Risk Ratio (M‐H, Random, 95% CI) | 0.47 [0.10, 2.33] |
| Analysis 1.15 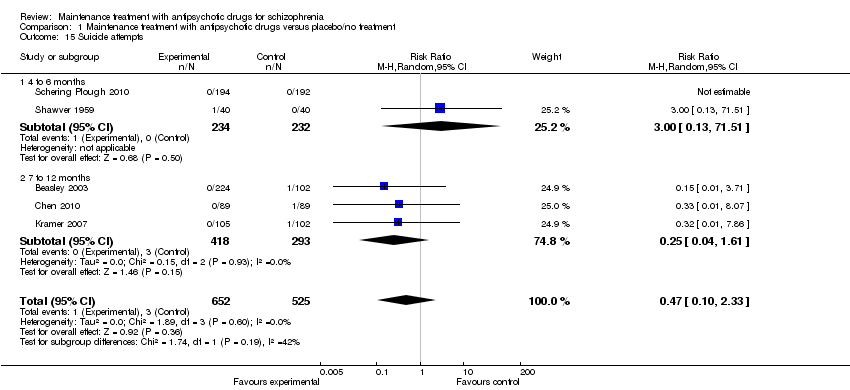 Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 15 Suicide attempts. | ||||
| 15.1 4 to 6 months | 2 | 466 | Risk Ratio (M‐H, Random, 95% CI) | 3.0 [0.13, 71.51] |
| 15.2 7 to 12 months | 3 | 711 | Risk Ratio (M‐H, Random, 95% CI) | 0.25 [0.04, 1.61] |
| 16 Suicide ideation Show forest plot | 3 | 556 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.04, 10.56] |
| Analysis 1.16 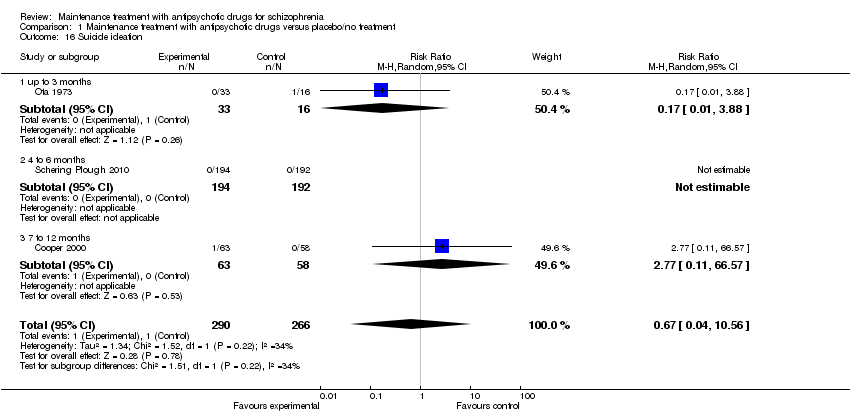 Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 16 Suicide ideation. | ||||
| 16.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.17 [0.01, 3.88] |
| 16.2 4 to 6 months | 1 | 386 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 16.3 7 to 12 months | 1 | 121 | Risk Ratio (M‐H, Random, 95% CI) | 2.77 [0.11, 66.57] |
| 17 Violent/aggressive behaviour Show forest plot | 5 | 680 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.15, 0.52] |
| Analysis 1.17  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 17 Violent/aggressive behaviour. | ||||
| 17.1 up to 3 months | 1 | 26 | Risk Ratio (M‐H, Random, 95% CI) | 0.33 [0.01, 7.50] |
| 17.2 4 to 6 months | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.2 [0.01, 3.92] |
| 17.3 7 to 12 months | 3 | 614 | Risk Ratio (M‐H, Random, 95% CI) | 0.28 [0.14, 0.53] |
| 18 Adverse effects: at least one adverse event Show forest plot | 10 | 2184 | Risk Ratio (M‐H, Random, 95% CI) | 1.01 [0.87, 1.18] |
| Analysis 1.18 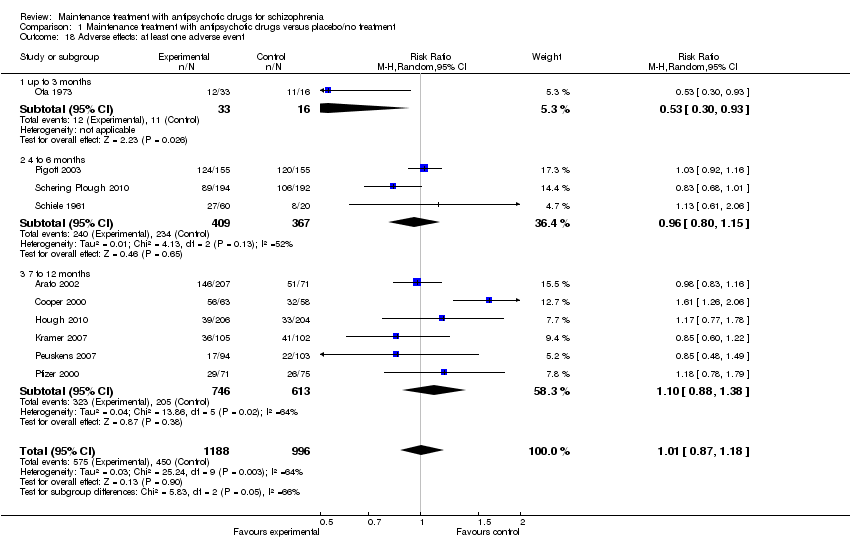 Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 18 Adverse effects: at least one adverse event. | ||||
| 18.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.53 [0.30, 0.93] |
| 18.2 4 to 6 months | 3 | 776 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.80, 1.15] |
| 18.3 7 to 12 months | 6 | 1359 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.88, 1.38] |
| 19 Adverse effects: movement disorders: at least one movement disorder Show forest plot | 22 | 3411 | Risk Ratio (M‐H, Random, 95% CI) | 1.55 [1.25, 1.93] |
| Analysis 1.19  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 19 Adverse effects: movement disorders: at least one movement disorder. | ||||
| 19.1 up to 3 months | 4 | 158 | Risk Ratio (M‐H, Random, 95% CI) | 2.42 [0.70, 8.33] |
| 19.2 4 to 6 months | 8 | 1658 | Risk Ratio (M‐H, Random, 95% CI) | 1.45 [1.06, 1.99] |
| 19.3 7 to 12 months | 10 | 1595 | Risk Ratio (M‐H, Random, 95% CI) | 1.52 [1.11, 2.07] |
| 20 Adverse effects: movement disorders: akathisia Show forest plot | 12 | 2026 | Risk Ratio (M‐H, Random, 95% CI) | 1.75 [0.87, 3.51] |
| Analysis 1.20  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 20 Adverse effects: movement disorders: akathisia. | ||||
| 20.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 1.94 [0.24, 15.97] |
| 20.2 4 to 6 months | 6 | 1009 | Risk Ratio (M‐H, Random, 95% CI) | 1.67 [0.41, 6.80] |
| 20.3 7 to 12 months | 5 | 968 | Risk Ratio (M‐H, Random, 95% CI) | 1.74 [0.88, 3.45] |
| 21 Adverse effects: movement disorders: akinesia Show forest plot | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.09, 9.92] |
| Analysis 1.21 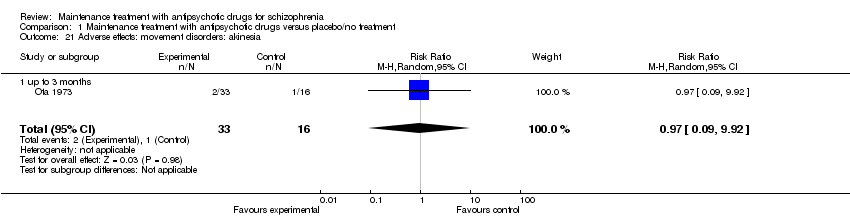 Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 21 Adverse effects: movement disorders: akinesia. | ||||
| 21.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.09, 9.92] |
| 22 Adverse effects: movement disorders: dyskinesia Show forest plot | 13 | 1820 | Risk Ratio (M‐H, Random, 95% CI) | 0.52 [0.28, 0.97] |
| Analysis 1.22  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 22 Adverse effects: movement disorders: dyskinesia. | ||||
| 22.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 1.5 [0.06, 34.91] |
| 22.2 4 to 6 months | 3 | 418 | Risk Ratio (M‐H, Random, 95% CI) | 0.31 [0.11, 0.84] |
| 22.3 7 to 12 months | 9 | 1353 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.30, 1.58] |
| 23 Adverse effects: movement disorders: dystonia Show forest plot | 6 | 824 | Risk Ratio (M‐H, Random, 95% CI) | 1.89 [1.05, 3.41] |
| Analysis 1.23  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 23 Adverse effects: movement disorders: dystonia. | ||||
| 23.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 2.5 [0.13, 49.22] |
| 23.2 4 to 6 months | 2 | 382 | Risk Ratio (M‐H, Random, 95% CI) | 1.75 [0.94, 3.29] |
| 23.3 7 to 12 months | 3 | 393 | Risk Ratio (M‐H, Random, 95% CI) | 3.97 [0.44, 35.54] |
| 24 Adverse effects: movement disorders: rigor Show forest plot | 5 | 249 | Risk Ratio (M‐H, Random, 95% CI) | 1.25 [0.54, 2.88] |
| Analysis 1.24  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 24 Adverse effects: movement disorders: rigor. | ||||
| 24.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.73 [0.24, 2.22] |
| 24.2 4 to 6 months | 3 | 160 | Risk Ratio (M‐H, Random, 95% CI) | 1.98 [0.67, 5.85] |
| 24.3 7 to 12 months | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 25 Adverse effects: movement disorders: tremor Show forest plot | 10 | 1468 | Risk Ratio (M‐H, Random, 95% CI) | 1.25 [0.81, 1.93] |
| Analysis 1.25  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 25 Adverse effects: movement disorders: tremor. | ||||
| 25.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 1.09 [0.40, 3.01] |
| 25.2 4 to 6 months | 3 | 160 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.33, 2.61] |
| 25.3 7 to 12 months | 6 | 1259 | Risk Ratio (M‐H, Random, 95% CI) | 1.41 [0.82, 2.43] |
| 26 Adverse effects: movement disorders: use of antiparkinson medication Show forest plot | 7 | 1317 | Risk Ratio (M‐H, Random, 95% CI) | 1.40 [1.03, 1.89] |
| Analysis 1.26  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 26 Adverse effects: movement disorders: use of antiparkinson medication. | ||||
| 26.1 4 to 6 months | 3 | 841 | Risk Ratio (M‐H, Random, 95% CI) | 1.53 [0.90, 2.61] |
| 26.2 7 to 12 months | 4 | 476 | Risk Ratio (M‐H, Random, 95% CI) | 1.33 [0.86, 2.05] |
| 27 Adverse effects: sedation Show forest plot | 10 | 2146 | Risk Ratio (M‐H, Random, 95% CI) | 1.50 [1.22, 1.84] |
| Analysis 1.27  Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 27 Adverse effects: sedation. | ||||
| 27.1 4 to 6 months | 6 | 1577 | Risk Ratio (M‐H, Random, 95% CI) | 1.33 [0.86, 2.07] |
| 27.2 7 to 12 months | 4 | 569 | Risk Ratio (M‐H, Random, 95% CI) | 1.72 [0.90, 3.31] |
| 28 Adverse effects: weight gain Show forest plot | 10 | 2321 | Risk Ratio (M‐H, Random, 95% CI) | 2.07 [1.31, 3.25] |
| Analysis 1.28 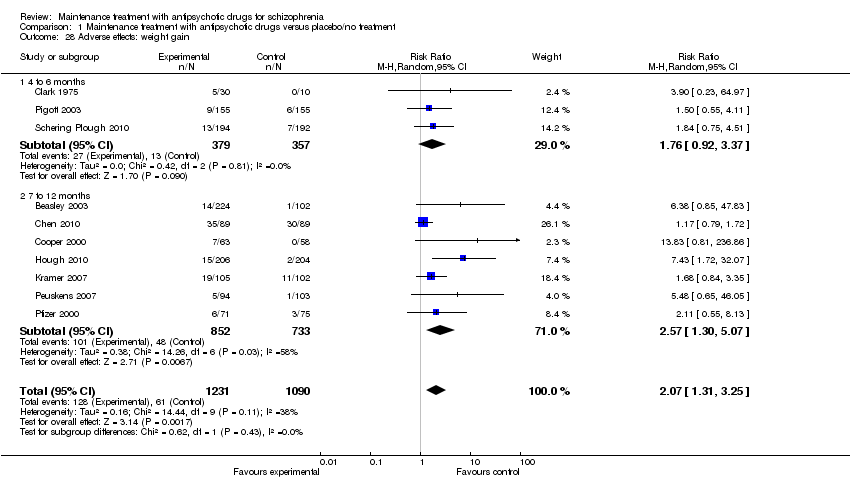 Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 28 Adverse effects: weight gain. | ||||
| 28.1 4 to 6 months | 3 | 736 | Risk Ratio (M‐H, Random, 95% CI) | 1.76 [0.92, 3.37] |
| 28.2 7 to 12 months | 7 | 1585 | Risk Ratio (M‐H, Random, 95% CI) | 2.57 [1.30, 5.07] |
| 29 Quality of life Show forest plot | 3 | 527 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.62 [‐1.15, ‐0.09] |
| Analysis 1.29 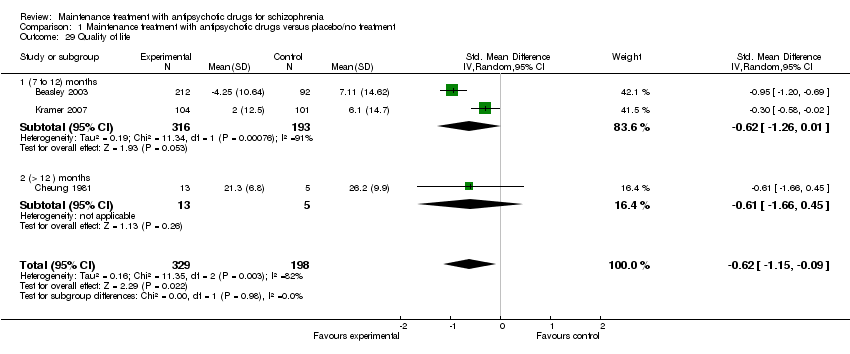 Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 29 Quality of life. | ||||
| 29.1 (7 to 12) months | 2 | 509 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.62 [‐1.26, 0.01] |
| 29.2 (> 12 ) months | 1 | 18 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.61 [‐1.66, 0.45] |
| 30 Number of participants employed: 7 to 12 months Show forest plot | 2 | 259 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.75, 1.23] |
| Analysis 1.30 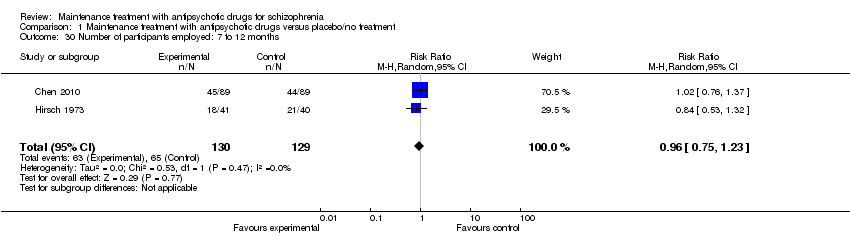 Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 30 Number of participants employed: 7 to 12 months. | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Subgroup analysis: participants with a first episode Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.48] |
| Analysis 2.1 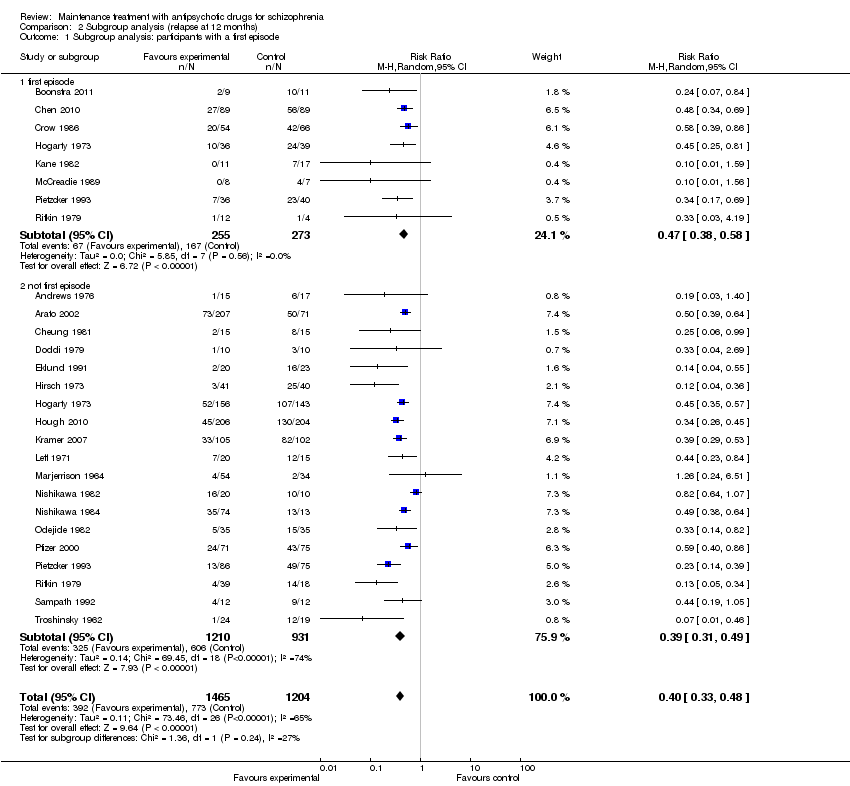 Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 1 Subgroup analysis: participants with a first episode. | ||||
| 1.1 first episode | 8 | 528 | Risk Ratio (M‐H, Random, 95% CI) | 0.47 [0.38, 0.58] |
| 1.2 not first episode | 19 | 2141 | Risk Ratio (M‐H, Random, 95% CI) | 0.39 [0.31, 0.49] |
| 2 Subgroup analysis: participants in remission Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| Analysis 2.2  Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 2 Subgroup analysis: participants in remission. | ||||
| 2.1 in remission | 8 | 516 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.24, 0.61] |
| 2.2 not in remission | 16 | 2153 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| 3 Subgroup analysis: various durations of stability before entering the study Show forest plot | 18 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 2.3 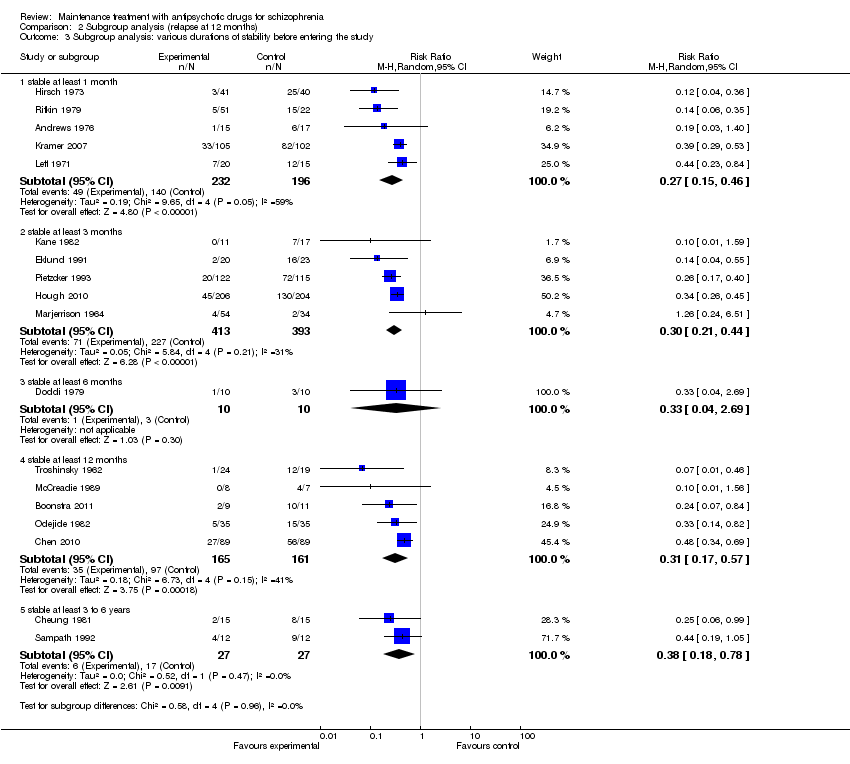 Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 3 Subgroup analysis: various durations of stability before entering the study. | ||||
| 3.1 stable at least 1 month | 5 | 428 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.15, 0.46] |
| 3.2 stable at least 3 months | 5 | 806 | Risk Ratio (M‐H, Random, 95% CI) | 0.30 [0.21, 0.44] |
| 3.3 stable at least 6 months | 1 | 20 | Risk Ratio (M‐H, Random, 95% CI) | 0.33 [0.04, 2.69] |
| 3.4 stable at least 12 months | 5 | 326 | Risk Ratio (M‐H, Random, 95% CI) | 0.31 [0.17, 0.57] |
| 3.5 stable at least 3 to 6 years | 2 | 54 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.18, 0.78] |
| 4 Subgroup analysis: abrupt withdrawal versus tapering Show forest plot | 24 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 2.4  Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 4 Subgroup analysis: abrupt withdrawal versus tapering. | ||||
| 4.1 Abrupt withdrawal | 16 | 1946 | Risk Ratio (M‐H, Random, 95% CI) | 0.43 [0.34, 0.54] |
| 4.2 Taper | 8 | 723 | Risk Ratio (M‐H, Random, 95% CI) | 0.34 [0.23, 0.50] |
| 5 Subgroup analysis: single antipsychotic drugs Show forest plot | 24 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 2.5  Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 5 Subgroup analysis: single antipsychotic drugs. | ||||
| 5.1 Chlorpromazine | 2 | 406 | Risk Ratio (M‐H, Random, 95% CI) | 0.44 [0.36, 0.55] |
| 5.2 Fluphenazine depot | 6 | 296 | Risk Ratio (M‐H, Random, 95% CI) | 0.23 [0.14, 0.39] |
| 5.3 Haloperidol depot | 1 | 43 | Risk Ratio (M‐H, Random, 95% CI) | 0.14 [0.04, 0.55] |
| 5.4 Quetiapine | 1 | 178 | Risk Ratio (M‐H, Random, 95% CI) | 0.48 [0.34, 0.69] |
| 5.5 Paliperidone | 2 | 617 | Risk Ratio (M‐H, Random, 95% CI) | 0.36 [0.30, 0.45] |
| 5.6 Various, mixed groups of antipsychotic drugs | 10 | 705 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.27, 0.65] |
| 5.7 Ziprasidone | 2 | 424 | Risk Ratio (M‐H, Random, 95% CI) | 0.52 [0.43, 0.64] |
| 6 Subgroup analysis: depot versus oral drugs Show forest plot | 21 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 2.6  Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 6 Subgroup analysis: depot versus oral drugs. | ||||
| 6.1 depot | 7 | 663 | Risk Ratio (M‐H, Random, 95% CI) | 0.31 [0.23, 0.41] |
| 6.2 oral | 14 | 1785 | Risk Ratio (M‐H, Random, 95% CI) | 0.46 [0.37, 0.57] |
| 7 Subgroup analysis: first‐ versus second‐generation antipsychotic drugs Show forest plot | 24 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 2.7  Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 7 Subgroup analysis: first‐ versus second‐generation antipsychotic drugs. | ||||
| 7.1 First‐generation antipsychotic drugs | 18 | 1430 | Risk Ratio (M‐H, Random, 95% CI) | 0.35 [0.25, 0.48] |
| 7.2 Second‐generation antipsychotic drugs | 6 | 1239 | Risk Ratio (M‐H, Random, 95% CI) | 0.44 [0.37, 0.53] |
| 8 Subgroup analysis: appropriate versus unclear allocation concealment Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| Analysis 2.8  Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 8 Subgroup analysis: appropriate versus unclear allocation concealment. | ||||
| 8.1 appropriate allocation concealment | 9 | 1410 | Risk Ratio (M‐H, Random, 95% CI) | 0.41 [0.33, 0.52] |
| 8.2 unclear allocation concealment | 15 | 1259 | Risk Ratio (M‐H, Random, 95% CI) | 0.39 [0.28, 0.53] |
| 9 Subgroup analysis: blinded versus open trials Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| Analysis 2.9 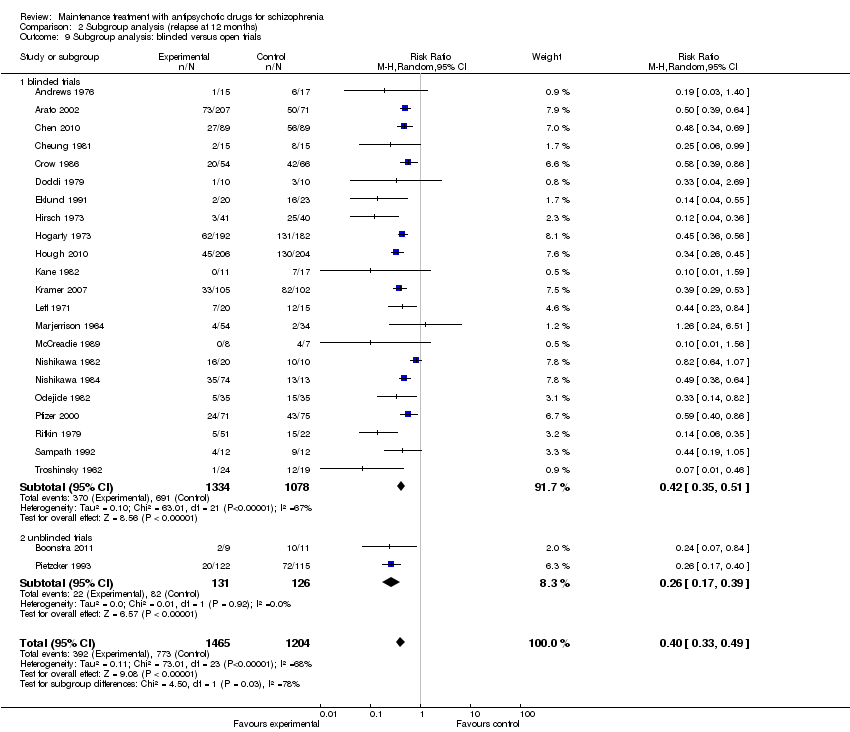 Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 9 Subgroup analysis: blinded versus open trials. | ||||
| 9.1 blinded trials | 22 | 2412 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.35, 0.51] |
| 9.2 unblinded trials | 2 | 257 | Risk Ratio (M‐H, Random, 95% CI) | 0.26 [0.17, 0.39] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Exclusion of studies that were not explicitly described as randomised Show forest plot | 23 | 2654 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| Analysis 3.1  Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 1 Exclusion of studies that were not explicitly described as randomised. | ||||
| 2 Exclusion of non‐double‐blind studies Show forest plot | 22 | 2412 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.35, 0.51] |
| Analysis 3.2  Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 2 Exclusion of non‐double‐blind studies. | ||||
| 3 Fixed‐effects model Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.40 [0.36, 0.44] |
| Analysis 3.3  Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 3 Fixed‐effects model. | ||||
| 4 Original authors' assumptions on dropouts Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| Analysis 3.4  Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 4 Original authors' assumptions on dropouts. | ||||
| 5 Inclusion of only large studies (> 200 participants) Show forest plot | 5 | 1506 | Risk Ratio (M‐H, Random, 95% CI) | 0.39 [0.32, 0.48] |
| Analysis 3.5 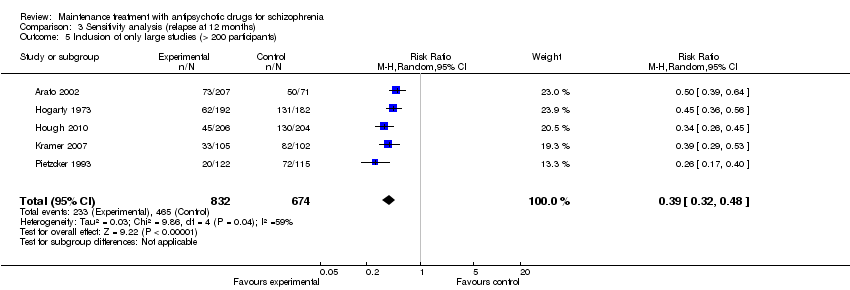 Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 5 Inclusion of only large studies (> 200 participants). | ||||
| 6 Exclusion of studies with clinical diagnosis Show forest plot | 16 | 2325 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.36, 0.49] |
| Analysis 3.6 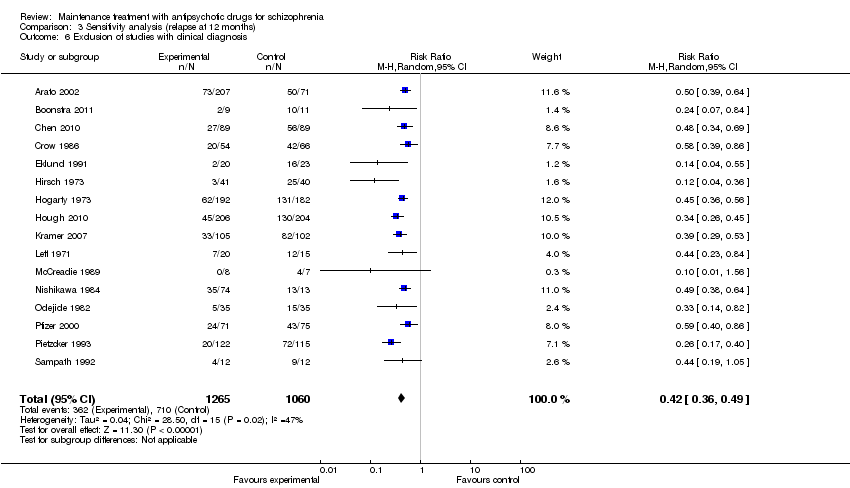 Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 6 Exclusion of studies with clinical diagnosis. | ||||
| 7 Three months stable Show forest plot | 20 | 2942 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.30, 0.55] |
| Analysis 3.7  Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 7 Three months stable. | ||||
| 8 Six months stable Show forest plot | 13 | 1382 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.26, 0.61] |
| Analysis 3.8  Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 8 Six months stable. | ||||
| 9 Nine months stable Show forest plot | 10 | 831 | Risk Ratio (M‐H, Random, 95% CI) | 0.46 [0.29, 0.73] |
| Analysis 3.9 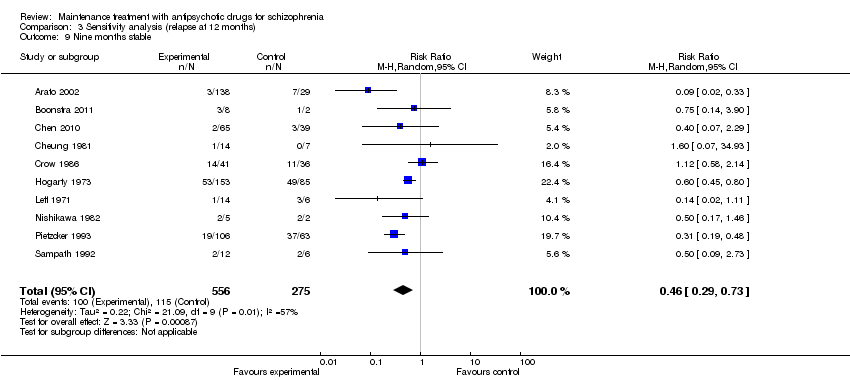 Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 9 Nine months stable. | ||||
| 10 Exclusion of studies with unclear randomisation method Show forest plot | 8 | 1546 | Risk Ratio (IV, Random, 95% CI) | 0.41 [0.34, 0.50] |
| Analysis 3.10  Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 10 Exclusion of studies with unclear randomisation method. | ||||
| 11 Exclusion of studies with unclear allocation concealment method Show forest plot | 9 | 1410 | Risk Ratio (IV, Random, 95% CI) | 0.41 [0.33, 0.52] |
| Analysis 3.11  Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 11 Exclusion of studies with unclear allocation concealment method. | ||||





Funnel plot of comparison: 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, outcome: 1.1 Relapse.

Summary of subgroup analysis

Meta‐regression study duration
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 1 Relapse: up to 3 months.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 2 Relapse: 4 to 6 months.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 3 Relapse: 7 to 12 months.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 4 Relapse: > 12 months.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 5 Relapse: independent of duration.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 6 Leaving the study early: due to any reason.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 7 Leaving the study early: due to adverse events.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 8 Leaving the study early: due to inefficacy.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 9 Global state: number of participants improved.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 10 Service use: number of participants hospitalised.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 11 Service use: number of participants discharged.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 12 Death: any.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 13 Death: due to natural causes.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 14 Suicide.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 15 Suicide attempts.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 16 Suicide ideation.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 17 Violent/aggressive behaviour.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 18 Adverse effects: at least one adverse event.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 19 Adverse effects: movement disorders: at least one movement disorder.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 20 Adverse effects: movement disorders: akathisia.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 21 Adverse effects: movement disorders: akinesia.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 22 Adverse effects: movement disorders: dyskinesia.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 23 Adverse effects: movement disorders: dystonia.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 24 Adverse effects: movement disorders: rigor.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 25 Adverse effects: movement disorders: tremor.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 26 Adverse effects: movement disorders: use of antiparkinson medication.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 27 Adverse effects: sedation.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 28 Adverse effects: weight gain.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 29 Quality of life.
Comparison 1 Maintenance treatment with antipsychotic drugs versus placebo/no treatment, Outcome 30 Number of participants employed: 7 to 12 months.
Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 1 Subgroup analysis: participants with a first episode.
Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 2 Subgroup analysis: participants in remission.
Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 3 Subgroup analysis: various durations of stability before entering the study.
Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 4 Subgroup analysis: abrupt withdrawal versus tapering.
Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 5 Subgroup analysis: single antipsychotic drugs.
Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 6 Subgroup analysis: depot versus oral drugs.
Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 7 Subgroup analysis: first‐ versus second‐generation antipsychotic drugs.
Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 8 Subgroup analysis: appropriate versus unclear allocation concealment.
Comparison 2 Subgroup analysis (relapse at 12 months), Outcome 9 Subgroup analysis: blinded versus open trials.
Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 1 Exclusion of studies that were not explicitly described as randomised.
Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 2 Exclusion of non‐double‐blind studies.
Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 3 Fixed‐effects model.
Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 4 Original authors' assumptions on dropouts.
Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 5 Inclusion of only large studies (> 200 participants).
Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 6 Exclusion of studies with clinical diagnosis.
Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 7 Three months stable.
Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 8 Six months stable.
Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 9 Nine months stable.
Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 10 Exclusion of studies with unclear randomisation method.
Comparison 3 Sensitivity analysis (relapse at 12 months), Outcome 11 Exclusion of studies with unclear allocation concealment method.
| Methods | Allocation: randomised ‐ clearly described generation of sequence and concealment of allocation. |
| Participants | People with schizophrenia or schizophrenia like disorder in remission for at least one month. |
| Interventions | 1. Any antipsychotic drug (flexible dose within appropriate range). 2. Placebo (after gradual withdrawal of the previous antipsychotic drug). |
| Outcomes | Relapse (primary outcome) Rehospitalisation for psychosis Time ill Global state (number of participants improved) Leaving the study early (including specific causes) Death (natural and unnatural causes) Violence Quality of life Satisfaction with care Side‐effects Employment and other measures of functioning |
| Maintenance treatment with antipsychotic drugs versus placebo/no treatment for schizophrenia | ||||||
| Patient or population: patients with schizophrenia | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Maintenance treatment with antipsychotic drugs versus placebo/no treatment | |||||
| Relapse: 7 to 12 months | 642 per 1000 | 263 per 1000 | RR 0.41 | 2669 | ⊕⊕⊕⊕ | |
| Leaving the study early: due to any reason | 544 per 1000 | 288 per 1000 | RR 0.53 | 4718 | ⊕⊕⊕⊕ | |
| Service use: Number of participants hospitalised | 256 per 1000 | 97 per 1000 | RR 0.38 | 2090 | ⊕⊕⊕⊕ | |
| Suicide | 2 per 1000 | 1 per 1000 | RR 0.34 | 1941 | ⊕⊕⊝⊝ | |
| Quality of life | The mean quality of life in the intervention groups was | 527 | ⊕⊕⊝⊝ | SMD ‐0.62 (‐1.15 to ‐0.09) | ||
| Number of participants employed: 7 to 12 months | 504 per 1000 | 484 per 1000 | RR 0.96 | 259 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Risk of bias: rated 'no' ‐ many studies did not report the methods for sequence generation and/or allocation concealment. However, the ones that did, showed a similar effect size in subgroup and sensitivity analyses. | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Relapse: up to 3 months Show forest plot | 34 | 3942 | Risk Ratio (M‐H, Random, 95% CI) | 0.30 [0.24, 0.38] |
| 2 Relapse: 4 to 6 months Show forest plot | 40 | 5285 | Risk Ratio (M‐H, Random, 95% CI) | 0.35 [0.30, 0.42] |
| 3 Relapse: 7 to 12 months Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| 4 Relapse: > 12 months Show forest plot | 6 | 811 | Risk Ratio (M‐H, Random, 95% CI) | 0.59 [0.42, 0.82] |
| 5 Relapse: independent of duration Show forest plot | 62 | 6392 | Risk Ratio (M‐H, Random, 95% CI) | 0.35 [0.29, 0.41] |
| 6 Leaving the study early: due to any reason Show forest plot | 47 | 4718 | Risk Ratio (M‐H, Random, 95% CI) | 0.53 [0.46, 0.61] |
| 6.1 up to 3 months | 8 | 245 | Risk Ratio (M‐H, Random, 95% CI) | 0.23 [0.07, 0.72] |
| 6.2 4 to 6 months | 17 | 1646 | Risk Ratio (M‐H, Random, 95% CI) | 0.48 [0.35, 0.66] |
| 6.3 7 to 12 months | 18 | 2420 | Risk Ratio (M‐H, Random, 95% CI) | 0.55 [0.46, 0.66] |
| 6.4 > 12 months | 4 | 407 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.36, 1.26] |
| 7 Leaving the study early: due to adverse events Show forest plot | 43 | 4333 | Risk Ratio (M‐H, Random, 95% CI) | 1.16 [0.70, 1.91] |
| 7.1 up to 3 months | 8 | 245 | Risk Ratio (M‐H, Random, 95% CI) | 2.84 [0.12, 65.34] |
| 7.2 4 to 6 months | 14 | 1549 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.57, 1.74] |
| 7.3 7 to 12 months | 17 | 2339 | Risk Ratio (M‐H, Random, 95% CI) | 1.24 [0.59, 2.60] |
| 7.4 > 12 months | 4 | 200 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 8 Leaving the study early: due to inefficacy Show forest plot | 46 | 4546 | Risk Ratio (M‐H, Random, 95% CI) | 0.37 [0.31, 0.44] |
| 8.1 up to 3 months | 9 | 295 | Risk Ratio (M‐H, Random, 95% CI) | 0.23 [0.07, 0.79] |
| 8.2 4 to 6 months | 16 | 1661 | Risk Ratio (M‐H, Random, 95% CI) | 0.41 [0.31, 0.54] |
| 8.3 7 to 12 months | 18 | 2420 | Risk Ratio (M‐H, Random, 95% CI) | 0.36 [0.28, 0.45] |
| 8.4 > 12 months | 3 | 170 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.08, 0.95] |
| 9 Global state: number of participants improved Show forest plot | 14 | 1524 | Risk Ratio (M‐H, Random, 95% CI) | 2.34 [1.68, 3.26] |
| 9.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 4.61 [1.22, 17.40] |
| 9.2 4 to 6 months | 8 | 1037 | Risk Ratio (M‐H, Random, 95% CI) | 2.33 [1.69, 3.21] |
| 9.3 7 to 12 months | 5 | 438 | Risk Ratio (M‐H, Random, 95% CI) | 1.95 [0.91, 4.18] |
| 10 Service use: number of participants hospitalised Show forest plot | 16 | 2090 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.27, 0.55] |
| 10.1 up to 3 months | 2 | 55 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.04, 4.06] |
| 10.2 4 to 6 months | 3 | 109 | Risk Ratio (M‐H, Random, 95% CI) | 0.08 [0.01, 0.42] |
| 10.3 7 to 12 months | 8 | 1295 | Risk Ratio (M‐H, Random, 95% CI) | 0.32 [0.18, 0.57] |
| 10.4 > 12 months | 3 | 631 | Risk Ratio (M‐H, Random, 95% CI) | 0.56 [0.44, 0.70] |
| 11 Service use: number of participants discharged Show forest plot | 3 | 404 | Risk Ratio (M‐H, Random, 95% CI) | 2.76 [0.69, 11.06] |
| 11.1 4 to 6 months | 3 | 404 | Risk Ratio (M‐H, Random, 95% CI) | 2.76 [0.69, 11.06] |
| 12 Death: any Show forest plot | 14 | 2356 | Risk Ratio (M‐H, Random, 95% CI) | 0.77 [0.28, 2.11] |
| 12.1 up to 3 months | 1 | 36 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 12.2 4 to 6 months | 5 | 856 | Risk Ratio (M‐H, Random, 95% CI) | 2.18 [0.48, 9.81] |
| 12.3 7 to 12 months | 8 | 1464 | Risk Ratio (M‐H, Random, 95% CI) | 0.33 [0.08, 1.27] |
| 13 Death: due to natural causes Show forest plot | 14 | 2401 | Risk Ratio (M‐H, Random, 95% CI) | 1.24 [0.39, 3.97] |
| 13.1 4 to 6 months | 5 | 856 | Risk Ratio (M‐H, Random, 95% CI) | 2.18 [0.48, 9.81] |
| 13.2 7 to 12 months | 9 | 1545 | Risk Ratio (M‐H, Random, 95% CI) | 0.54 [0.09, 3.36] |
| 14 Suicide Show forest plot | 8 | 1941 | Risk Ratio (M‐H, Random, 95% CI) | 0.34 [0.04, 3.28] |
| 14.1 up to 3 months | 1 | 36 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 14.2 4 to 6 months | 2 | 730 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 14.3 7 to 12 months | 5 | 1175 | Risk Ratio (M‐H, Random, 95% CI) | 0.34 [0.04, 3.28] |
| 15 Suicide attempts Show forest plot | 5 | 1177 | Risk Ratio (M‐H, Random, 95% CI) | 0.47 [0.10, 2.33] |
| 15.1 4 to 6 months | 2 | 466 | Risk Ratio (M‐H, Random, 95% CI) | 3.0 [0.13, 71.51] |
| 15.2 7 to 12 months | 3 | 711 | Risk Ratio (M‐H, Random, 95% CI) | 0.25 [0.04, 1.61] |
| 16 Suicide ideation Show forest plot | 3 | 556 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.04, 10.56] |
| 16.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.17 [0.01, 3.88] |
| 16.2 4 to 6 months | 1 | 386 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 16.3 7 to 12 months | 1 | 121 | Risk Ratio (M‐H, Random, 95% CI) | 2.77 [0.11, 66.57] |
| 17 Violent/aggressive behaviour Show forest plot | 5 | 680 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.15, 0.52] |
| 17.1 up to 3 months | 1 | 26 | Risk Ratio (M‐H, Random, 95% CI) | 0.33 [0.01, 7.50] |
| 17.2 4 to 6 months | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.2 [0.01, 3.92] |
| 17.3 7 to 12 months | 3 | 614 | Risk Ratio (M‐H, Random, 95% CI) | 0.28 [0.14, 0.53] |
| 18 Adverse effects: at least one adverse event Show forest plot | 10 | 2184 | Risk Ratio (M‐H, Random, 95% CI) | 1.01 [0.87, 1.18] |
| 18.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.53 [0.30, 0.93] |
| 18.2 4 to 6 months | 3 | 776 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.80, 1.15] |
| 18.3 7 to 12 months | 6 | 1359 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.88, 1.38] |
| 19 Adverse effects: movement disorders: at least one movement disorder Show forest plot | 22 | 3411 | Risk Ratio (M‐H, Random, 95% CI) | 1.55 [1.25, 1.93] |
| 19.1 up to 3 months | 4 | 158 | Risk Ratio (M‐H, Random, 95% CI) | 2.42 [0.70, 8.33] |
| 19.2 4 to 6 months | 8 | 1658 | Risk Ratio (M‐H, Random, 95% CI) | 1.45 [1.06, 1.99] |
| 19.3 7 to 12 months | 10 | 1595 | Risk Ratio (M‐H, Random, 95% CI) | 1.52 [1.11, 2.07] |
| 20 Adverse effects: movement disorders: akathisia Show forest plot | 12 | 2026 | Risk Ratio (M‐H, Random, 95% CI) | 1.75 [0.87, 3.51] |
| 20.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 1.94 [0.24, 15.97] |
| 20.2 4 to 6 months | 6 | 1009 | Risk Ratio (M‐H, Random, 95% CI) | 1.67 [0.41, 6.80] |
| 20.3 7 to 12 months | 5 | 968 | Risk Ratio (M‐H, Random, 95% CI) | 1.74 [0.88, 3.45] |
| 21 Adverse effects: movement disorders: akinesia Show forest plot | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.09, 9.92] |
| 21.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.09, 9.92] |
| 22 Adverse effects: movement disorders: dyskinesia Show forest plot | 13 | 1820 | Risk Ratio (M‐H, Random, 95% CI) | 0.52 [0.28, 0.97] |
| 22.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 1.5 [0.06, 34.91] |
| 22.2 4 to 6 months | 3 | 418 | Risk Ratio (M‐H, Random, 95% CI) | 0.31 [0.11, 0.84] |
| 22.3 7 to 12 months | 9 | 1353 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.30, 1.58] |
| 23 Adverse effects: movement disorders: dystonia Show forest plot | 6 | 824 | Risk Ratio (M‐H, Random, 95% CI) | 1.89 [1.05, 3.41] |
| 23.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 2.5 [0.13, 49.22] |
| 23.2 4 to 6 months | 2 | 382 | Risk Ratio (M‐H, Random, 95% CI) | 1.75 [0.94, 3.29] |
| 23.3 7 to 12 months | 3 | 393 | Risk Ratio (M‐H, Random, 95% CI) | 3.97 [0.44, 35.54] |
| 24 Adverse effects: movement disorders: rigor Show forest plot | 5 | 249 | Risk Ratio (M‐H, Random, 95% CI) | 1.25 [0.54, 2.88] |
| 24.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.73 [0.24, 2.22] |
| 24.2 4 to 6 months | 3 | 160 | Risk Ratio (M‐H, Random, 95% CI) | 1.98 [0.67, 5.85] |
| 24.3 7 to 12 months | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 25 Adverse effects: movement disorders: tremor Show forest plot | 10 | 1468 | Risk Ratio (M‐H, Random, 95% CI) | 1.25 [0.81, 1.93] |
| 25.1 up to 3 months | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 1.09 [0.40, 3.01] |
| 25.2 4 to 6 months | 3 | 160 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.33, 2.61] |
| 25.3 7 to 12 months | 6 | 1259 | Risk Ratio (M‐H, Random, 95% CI) | 1.41 [0.82, 2.43] |
| 26 Adverse effects: movement disorders: use of antiparkinson medication Show forest plot | 7 | 1317 | Risk Ratio (M‐H, Random, 95% CI) | 1.40 [1.03, 1.89] |
| 26.1 4 to 6 months | 3 | 841 | Risk Ratio (M‐H, Random, 95% CI) | 1.53 [0.90, 2.61] |
| 26.2 7 to 12 months | 4 | 476 | Risk Ratio (M‐H, Random, 95% CI) | 1.33 [0.86, 2.05] |
| 27 Adverse effects: sedation Show forest plot | 10 | 2146 | Risk Ratio (M‐H, Random, 95% CI) | 1.50 [1.22, 1.84] |
| 27.1 4 to 6 months | 6 | 1577 | Risk Ratio (M‐H, Random, 95% CI) | 1.33 [0.86, 2.07] |
| 27.2 7 to 12 months | 4 | 569 | Risk Ratio (M‐H, Random, 95% CI) | 1.72 [0.90, 3.31] |
| 28 Adverse effects: weight gain Show forest plot | 10 | 2321 | Risk Ratio (M‐H, Random, 95% CI) | 2.07 [1.31, 3.25] |
| 28.1 4 to 6 months | 3 | 736 | Risk Ratio (M‐H, Random, 95% CI) | 1.76 [0.92, 3.37] |
| 28.2 7 to 12 months | 7 | 1585 | Risk Ratio (M‐H, Random, 95% CI) | 2.57 [1.30, 5.07] |
| 29 Quality of life Show forest plot | 3 | 527 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.62 [‐1.15, ‐0.09] |
| 29.1 (7 to 12) months | 2 | 509 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.62 [‐1.26, 0.01] |
| 29.2 (> 12 ) months | 1 | 18 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.61 [‐1.66, 0.45] |
| 30 Number of participants employed: 7 to 12 months Show forest plot | 2 | 259 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.75, 1.23] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Subgroup analysis: participants with a first episode Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.48] |
| 1.1 first episode | 8 | 528 | Risk Ratio (M‐H, Random, 95% CI) | 0.47 [0.38, 0.58] |
| 1.2 not first episode | 19 | 2141 | Risk Ratio (M‐H, Random, 95% CI) | 0.39 [0.31, 0.49] |
| 2 Subgroup analysis: participants in remission Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| 2.1 in remission | 8 | 516 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.24, 0.61] |
| 2.2 not in remission | 16 | 2153 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| 3 Subgroup analysis: various durations of stability before entering the study Show forest plot | 18 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 3.1 stable at least 1 month | 5 | 428 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.15, 0.46] |
| 3.2 stable at least 3 months | 5 | 806 | Risk Ratio (M‐H, Random, 95% CI) | 0.30 [0.21, 0.44] |
| 3.3 stable at least 6 months | 1 | 20 | Risk Ratio (M‐H, Random, 95% CI) | 0.33 [0.04, 2.69] |
| 3.4 stable at least 12 months | 5 | 326 | Risk Ratio (M‐H, Random, 95% CI) | 0.31 [0.17, 0.57] |
| 3.5 stable at least 3 to 6 years | 2 | 54 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.18, 0.78] |
| 4 Subgroup analysis: abrupt withdrawal versus tapering Show forest plot | 24 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 4.1 Abrupt withdrawal | 16 | 1946 | Risk Ratio (M‐H, Random, 95% CI) | 0.43 [0.34, 0.54] |
| 4.2 Taper | 8 | 723 | Risk Ratio (M‐H, Random, 95% CI) | 0.34 [0.23, 0.50] |
| 5 Subgroup analysis: single antipsychotic drugs Show forest plot | 24 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 5.1 Chlorpromazine | 2 | 406 | Risk Ratio (M‐H, Random, 95% CI) | 0.44 [0.36, 0.55] |
| 5.2 Fluphenazine depot | 6 | 296 | Risk Ratio (M‐H, Random, 95% CI) | 0.23 [0.14, 0.39] |
| 5.3 Haloperidol depot | 1 | 43 | Risk Ratio (M‐H, Random, 95% CI) | 0.14 [0.04, 0.55] |
| 5.4 Quetiapine | 1 | 178 | Risk Ratio (M‐H, Random, 95% CI) | 0.48 [0.34, 0.69] |
| 5.5 Paliperidone | 2 | 617 | Risk Ratio (M‐H, Random, 95% CI) | 0.36 [0.30, 0.45] |
| 5.6 Various, mixed groups of antipsychotic drugs | 10 | 705 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.27, 0.65] |
| 5.7 Ziprasidone | 2 | 424 | Risk Ratio (M‐H, Random, 95% CI) | 0.52 [0.43, 0.64] |
| 6 Subgroup analysis: depot versus oral drugs Show forest plot | 21 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 6.1 depot | 7 | 663 | Risk Ratio (M‐H, Random, 95% CI) | 0.31 [0.23, 0.41] |
| 6.2 oral | 14 | 1785 | Risk Ratio (M‐H, Random, 95% CI) | 0.46 [0.37, 0.57] |
| 7 Subgroup analysis: first‐ versus second‐generation antipsychotic drugs Show forest plot | 24 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 7.1 First‐generation antipsychotic drugs | 18 | 1430 | Risk Ratio (M‐H, Random, 95% CI) | 0.35 [0.25, 0.48] |
| 7.2 Second‐generation antipsychotic drugs | 6 | 1239 | Risk Ratio (M‐H, Random, 95% CI) | 0.44 [0.37, 0.53] |
| 8 Subgroup analysis: appropriate versus unclear allocation concealment Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| 8.1 appropriate allocation concealment | 9 | 1410 | Risk Ratio (M‐H, Random, 95% CI) | 0.41 [0.33, 0.52] |
| 8.2 unclear allocation concealment | 15 | 1259 | Risk Ratio (M‐H, Random, 95% CI) | 0.39 [0.28, 0.53] |
| 9 Subgroup analysis: blinded versus open trials Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| 9.1 blinded trials | 22 | 2412 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.35, 0.51] |
| 9.2 unblinded trials | 2 | 257 | Risk Ratio (M‐H, Random, 95% CI) | 0.26 [0.17, 0.39] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Exclusion of studies that were not explicitly described as randomised Show forest plot | 23 | 2654 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| 2 Exclusion of non‐double‐blind studies Show forest plot | 22 | 2412 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.35, 0.51] |
| 3 Fixed‐effects model Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.40 [0.36, 0.44] |
| 4 Original authors' assumptions on dropouts Show forest plot | 24 | 2669 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.33, 0.49] |
| 5 Inclusion of only large studies (> 200 participants) Show forest plot | 5 | 1506 | Risk Ratio (M‐H, Random, 95% CI) | 0.39 [0.32, 0.48] |
| 6 Exclusion of studies with clinical diagnosis Show forest plot | 16 | 2325 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.36, 0.49] |
| 7 Three months stable Show forest plot | 20 | 2942 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.30, 0.55] |
| 8 Six months stable Show forest plot | 13 | 1382 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.26, 0.61] |
| 9 Nine months stable Show forest plot | 10 | 831 | Risk Ratio (M‐H, Random, 95% CI) | 0.46 [0.29, 0.73] |
| 10 Exclusion of studies with unclear randomisation method Show forest plot | 8 | 1546 | Risk Ratio (IV, Random, 95% CI) | 0.41 [0.34, 0.50] |
| 11 Exclusion of studies with unclear allocation concealment method Show forest plot | 9 | 1410 | Risk Ratio (IV, Random, 95% CI) | 0.41 [0.33, 0.52] |