Dosis única oral de etoricoxib para el dolor posoperatorio agudo en pacientes adultos
Resumen
Antecedentes
Ésta es una versión actualizada de la revisión original Cochrane publicada por primera vez en el número 2, 2009 y actualizada anteriormente en el número 4, 2012.
El etoricoxib es un inhibidor selectivo de la ciclooxigenasa 2 (COX‐2) que se indica para el alivio del dolor crónico en la osteoartritis, la artritis reumatoide y el dolor agudo en algunas jurisdicciones. Se cree que este fármaco se asocia con menos efectos adversos digestivos altos que los fármacos antiinflamatorios no esteroideos (AINE) convencionales.
Objetivos
Evaluar la eficacia y los efectos adversos de una dosis única de etoricoxib para el dolor posoperatorio agudo mediante métodos que permitan una comparación precisa con otros analgésicos evaluados de la misma manera, utilizando los criterios de eficacia recomendados por estudios en profundidad a nivel de paciente individual.
Métodos de búsqueda
Se hicieron búsquedas en el Registro Cochrane Central de Ensayos Controlados (Cochrane Central Register of Controlled Trials) (CENTRAL), MEDLINE, EMBASE, la Oxford Pain Database, ClinicalTrials.gov y en listas de referencias de artículos. La fecha de la búsqueda más reciente fue el 31 de enero de 2014.
Criterios de selección
Ensayos clínicos aleatorizados, doble ciego, controlados con placebo de una dosis única oral de etoricoxib para el dolor posoperatorio agudo en pacientes adultos.
Obtención y análisis de los datos
Dos autores de la revisión, de forma independiente, analizaron los ensayos para inclusión en la revisión, evaluaron su calidad y extrajeron los datos. Se utilizó el área bajo la curva alivio del dolor versus tiempo para obtener la proporción de participantes a los que se les prescribió etoricoxib o placebo con al menos un alivio del dolor del 50% durante seis horas, con el uso de ecuaciones validadas. Se calculó el riesgo relativo (RR) y el número necesario a tratar para beneficiar (NNT). La información sobre el uso de la medicación de rescate se utilizó para calcular la proporción de participantes que la necesitaron y la media ponderada del tiempo mediano transcurrido hasta su utilización. También se recopiló información sobre los eventos adversos.
Resultados principales
No se identificaron nuevos estudios para esta revisión actualizada, que incluye seis estudios con 1214 participantes en las comparaciones de etoricoxib con placebo. Los seis estudios informaron sobre la dosis de 120 mg (798 participantes en comparación con placebo). El 66% de los participantes con etoricoxib 120 mg y el 12% con placebo informaron al menos un alivio del dolor del 50% (NNT 1,8 [1,7 a 2,0]; evidencia de calidad alta). Solamente en los estudios dentales el NNT fue 1,6 (1,5 a 1,8). Una dosis única de 90 mg produjo resultados similares en un ensayo grande. Otras dosis (60, 180 y 240 mg) solo se estudiaron en un brazo de tratamiento.
De manera significativa menos participantes utilizaron medicación de rescate durante 24 horas cuando tomaron etoricoxib 120 mg en comparación con placebo (NNT para prevenir la necesidad de nueva medicación 2,2 [1,9 a 2,8]) y el tiempo mediano transcurrido hasta el uso de la medicación de rescate fue 20 horas para etoricoxib y dos para placebo. Los eventos adversos se informaron en una tasa similar a la de placebo (evidencia de calidad moderada), sin eventos graves.
Conclusiones de los autores
Una dosis oral única de etoricoxib produce niveles elevados de alivio del dolor de buena calidad después de una cirugía y los eventos adversos no fueron diferentes de los de placebo. La dosis de 120 mg es tan efectiva o mejor que la de otros analgésicos utilizados habitualmente.
PICOs
Resumen en términos sencillos
Dosis única oral de etoricoxib para el dolor posoperatorio agudo en pacientes adultos
A menudo poco tiempo después de una lesión se percibe dolor agudo. La mayoría de los pacientes a los que se les realiza cirugía presentan dolor moderado o intenso después del procedimiento. Los analgésicos se prueban en pacientes con dolor. Con frecuencia, a dichos pacientes se les extrajeron muelas de juicio. Habitualmente el dolor se trata con analgésicos administrados por vía oral. Los resultados se pueden aplicar a otras formas de dolor agudo.
Una serie de revisiones han examinado la efectividad de los analgésicos. Esta revisión evaluó un fármaco llamado etoricoxib. Este es uno de los tipos de analgésicos llamados AINE (fármaco antiinflamatorio no esteroideo). La cantidad de alivio del dolor experimentado depende de la dosis tomada.
Se encontraron seis ensayos clínicos con 1214 pacientes. Una dosis única de 120 mg de etoricoxib produjo un alivio útil del dolor en siete de diez (66%) pacientes con dolor moderado o intenso, en comparación con poco más de uno de diez (12%) con placebo. Una dosis única de 90 mg produjo resultados similares en un ensayo grande. El alivio del dolor duró 20 horas en la mitad de los pacientes tratados.
En estos estudios de dosis única los eventos adversos ocurrieron en tasas similares con etoricoxib y placebo. No se observaron efectos adversos graves ni retiros debido a efectos adversos con etoricoxib.
Authors' conclusions
Summary of findings
| Etoricoxib compared with placebo for acute postoperative pain | ||||||
| Patient or population: adults with moderate or severe acute postoperative pain Settings: community or hospital Intervention: etoricoxib 120 mg Comparison: placebo | ||||||
| Outcomes | Probable outcome with | Relative effect and NNT or NNH (95% CI) | No of studies, events | Quality of the evidence | Comments | |
| comparator | intervention | |||||
| At least 50% of maximum pain relief over 4 to 6 hours | 120 in 1000 | 660 in 1000 | RR 5.6 (4.0 to 7.8) NNT 1.9 (1.7 to 2.1) | 6 studies 789 participants 366 events | High | Adequate numbers of studies, participants and events. Consistency across studies |
| Participants with at least 1 adverse event | 360 in 1000 | 330 in 1000 | RR 0.93 (0.74 to 1.2) NNH not calculated | 5 studies 643 participants 219 events | Moderate | Moderate numbers of studies, participants and events. Consistency across studies. Single dose studies may not reflect clinical practice |
| Participants with a serious adverse event | No serious adverse events | Low | Studies underpowered to detect rare events | |||
| Deaths | No deaths | Low | Studies underpowered to detect rare events | |||
| CI: Confidence interval; NNH: number needed to treat for harm; NNT: number needed to treat for benefit; RR: Risk Ratio | ||||||
| GRADE Working Group grades of evidence | ||||||
Background
This is an updated version of the original Cochrane review, 'Single dose oral etoricoxib for acute postoperative pain in adults', first published in Issue 2, 2009 (Clarke 2009), and updated in Issue 4, 2012 (Clarke 2012).
Description of the condition
Acute pain occurs as a result of tissue damage either accidentally due to an injury or as a result of surgery. Acute postoperative pain is a manifestation of inflammation due to tissue injury. The management of postoperative pain and inflammation is a critical component of patient care. The aim of this series of reviews is to present evidence for relative analgesic efficacy through indirect comparisons with placebo, in very similar trials performed in a standard manner, with very similar outcomes, and over the same duration. Such relative analgesic efficacy does not in itself determine choice of drug for any situation or patient, but guides policy‐making at the local level. The series includes well‐established analgesics such as paracetamol (Toms 2008), naproxen (Derry 2009a), diclofenac (Derry 2009b), and ibuprofen (Derry 2009c), and newer cyclo‐oxygenase‐2 selective analgesics, such as celecoxib (Derry 2013) and lumiracoxib (Roy 2010). An overview brings together the results from all the individual drug reviews (Moore 2011a).
Single dose trials in acute pain are commonly short in duration, rarely lasting longer than 12 hours. The numbers of participants are small, allowing no reliable conclusions to be drawn about safety. To show that the analgesic is working it is necessary to use placebo (McQuay 2005). There are clear ethical considerations in doing this. These ethical considerations are answered by using acute pain situations where the pain is expected to go away, and by providing additional analgesia, commonly called rescue analgesia, if the pain has not diminished after about an hour. This is reasonable, because not all participants given an analgesic will have significant pain relief. Approximately 18% of participants given placebo will have significant pain relief (Moore 2006), and up to 50% may have inadequate analgesia with active medicines. The use of additional or rescue analgesia is hence important for all participants in trials.
Clinical trials measuring the efficacy of analgesics in acute pain have been standardised over many years. Trials have to be randomised and double‐blind. Typically, in the first few hours or days after an operation, patients develop pain that is moderate to severe in intensity, and will then be given the test analgesic or placebo. Pain is measured using standard pain intensity scales immediately before the intervention, and then using pain intensity and pain relief scales over the following four to six hours for shorter‐acting drugs, and up to 12 or 24 hours for longer‐acting drugs. Pain relief of half the maximum possible pain relief or better (at least 50% pain relief) is typically regarded as a clinically useful outcome. For patients given rescue medication it is usual for no additional pain measurements to be made, and for all subsequent measures to be recorded as initial pain intensity or baseline (zero) pain relief (baseline observation carried forward). This process ensures that analgesia from the rescue medication is not wrongly ascribed to the test intervention. In some trials the last observation is carried forward, which gives an inflated response for the test intervention compared to placebo, but the effect has been shown to be negligible over four to six hours (Moore 2005a). Patients usually remain in the hospital or clinic for at least the first six hours following the intervention, with measurements supervised, although they may then be allowed home to make their own measurements in trials of longer duration.
Knowing the relative efficacy of different analgesic drugs at various doses can be helpful. Results from completed reviews of many different analgesics have been brought together to facilitate (indirect) comparisons in an overview (Moore 2011a), and analgesics relevant for dentistry are discussed in Barden 2004a and Derry 2011.
Description of the intervention
Selective cyclo‐oxygenase‐2 inhibitors (COX‐2 inhibitors or 'coxibs') were developed to address the problem of upper gastrointestinal bleeding associated with traditional non‐steroidal anti‐inflammatory drugs (NSAIDs) (Hawkey 2001). Etoricoxib (sold worldwide under the brand name of Arcoxia, and in Italy as Algix and Tauxib) is one of the second generation of coxibs and is used to treat pain in chronic conditions, such as rheumatoid arthritis and osteoarthritis, ankylosing spondylitis, and low back pain, and also in acute pain and gout. It is available by prescription only as 30 mg, 60 mg, 90 mg, and 120 mg tablets in many parts of the world, but is not licensed for use in the US, due to concerns about safety. In chronic conditions the daily dose is usually 30 mg to 90 mg once daily, and in acute conditions 90 or 120 mg once daily (for up to a week). In primary care in England in 2012, there were almost 50,000 prescriptions for the 120 mg dose, and about 150,000 each for the 60 mg and 90 mg doses (PACT 2013).
The standard licensed dose of etoricoxib for acute pain is 120 mg in most countries, but a lower dose of 90 mg may be recommended in others.
How the intervention might work
NSAIDs have pain‐relieving, antipyretic, and anti‐inflammatory properties, and are thought to relieve pain by inhibiting cyclo‐oxygenases and thus the production of prostaglandins (Hawkey 1999). Prostaglandins occur throughout body tissues and fluids and act to stimulate pain nerve endings and promote/inhibit the aggregation of blood platelets. Cyclo‐oxygenase has at least two isoforms: COX‐1 and COX‐2. COX‐1 is constitutive while COX‐2 is induced at sites of inflammation and produces the prostaglandins involved in inflammatory responses and pain mediation (Grahame‐Smith 2002). Unlike traditional NSAIDs such as ibuprofen and ketoprofen, the coxibs are selective inhibitors, blocking primarily the action of COX‐2, providing pain relief, and causing fewer gastrointestinal effects (Moore 2005b). In addition, they should not precipitate bleeding events through inhibition of platelet aggregation (Straube 2005). Etoricoxib is more highly selective of COX‐2 over COX‐1 than celecoxib.
In common with other NSAIDS, COX‐2 inhibitors can give rise to fluid retention and renal damage (Garner 2002), so particular caution is needed in the elderly (Hawkey 2001). COX‐2 inhibitors have been implicated in increased cardiovascular problems in long‐term use, but this is complicated by differences in pharmacology and pharmacokinetics (Patrono 2009). Moreover, recent evidence indicates that prior cardiac damage may be a more important trigger than any particular drug or class of drug (Ruff 2011).
Why it is important to do this review
Etoricoxib is one of a small group of COX‐2 selective NSAIDs that provide pain relief with fewer gastrointestinal adverse events than traditional NSAIDs. This update is important because at licensed doses etoricoxib is one of the more effective and longest lasting analgesics in acute pain.
Objectives
To assess the efficacy and adverse effects of single‐dose etoricoxib for acute postoperative pain using methods that permit accurate comparison with other analgesics evaluated in the same way, using criteria of efficacy recommended by in‐depth studies at the individual patient level (Moore 2005a; Moore 2011b).
Methods
Criteria for considering studies for this review
Types of studies
We included studies if they were full publications of double‐blind studies of a single‐dose oral etoricoxib against placebo for the treatment of moderate to severe postoperative pain in adults, with at least 10 participants randomly allocated to each treatment group. We included multiple‐dose studies if appropriate data from the first dose were available, and we included cross‐over studies provided that data from the first arm were presented separately.
We excluded studies if they were:
-
posters or abstracts not followed up by full publication;
-
reports of studies concerned with pain other than postoperative pain (including experimental pain);
-
studies using volunteer participants;
-
studies where pain relief was assessed by clinicians, nurses, or carers (i.e. not patient‐reported); and
-
studies of less than four hours' duration or that failed to present data over four to six hours post dose.
Types of participants
We included studies of adult participants (15 years old or more) with established postoperative pain of moderate to severe intensity following day surgery or in‐patient surgery. For studies using a visual analogue scale (VAS), pain of at least moderate intensity was assumed when the VAS score was greater than 30 mm (Collins 1997). We included studies of participants with postpartum pain provided the pain investigated resulted from episiotomy or Caesarean section (with or without uterine cramp). We excluded studies investigating participants with pain due to uterine cramps alone.
Types of interventions
We included studies in which orally administered etoricoxib or matched placebo was given as a single dose for relief of postoperative pain.
Types of outcome measures
Data collected included the following:
-
characteristics of participants;
-
pain models;
-
patient‐reported pain at baseline (physician, nurse, or carer reported pain was not included in the analysis);
-
patient‐reported pain relief and pain intensity expressed hourly over four to six hours using validated pain scales (pain intensity and pain relief in the form of VAS or categorical scales, or both), or reported total pain relief (TOTPAR) or summed pain intensity difference (SPID) at four to six hours;
-
patient‐reported global assessment of treatment (PGE), using a validated scale;
-
number of participants using rescue medication and the time of assessment;
-
time to use of rescue medication;
-
withdrawals ‐ all causes and adverse events; and
-
adverse events ‐ participants experiencing one or more, and any serious adverse event, and the time of assessment.
Primary outcomes
Participants achieving at least 50% pain relief over four to six hours.
Secondary outcomes
-
Median (or mean) time to use of rescue medication.
-
Participants using rescue medication.
-
Participants with:
-
any adverse event;
-
any serious adverse event (as reported in the study); and
-
withdrawal due to an adverse event.
-
-
Withdrawals for reasons other than lack of efficacy (participants using rescue medication) and adverse events
Search methods for identification of studies
We applied no language restriction.
Electronic searches
We searched the following databases:
-
the Cochrane Central Register of Controlled Trials (CENTRAL) (in The Cochrane Library Issue 1, 2014);
-
MEDLINE (1996 to 31 January 2014);
-
EMBASE (1980 to 31 January 2014);
-
Oxford Pain Database (Jadad 1996a) for original review only; and
-
www.clinicaltrials.gov (on 31 January 2014) for update only.
Details of the search strategies for MEDLINE are in Appendix 1, EMBASE in Appendix 2, and CENTRAL in Appendix 3.
We did not search online databases from inception because etoricoxib was not in clinical trials until around 2000. We ran searches for the original review up to December 2009, for the first update to 3 January 2012, and for this update to 31 January 2014.
Searching other resources
We searched reference lists of retrieved articles and reviews for additional studies. We did not search short abstracts, conference proceedings, and other grey literature, and we did not contact manufacturers.
Data collection and analysis
Selection of studies
Two review authors independently assessed and agreed the search results for studies that might be included in the review. We resolved disagreements by consensus or referral to a third review author.
Data extraction and management
Two review authors independently extracted and recorded data on a standard data extraction form. One review author entered data suitable for pooling into Review Manager (RevMan) 5.1 (RevMan 2011).
Assessment of risk of bias in included studies
Two review authors independently assessed each study using a three‐item, five‐point scale (Jadad 1996b), and agreed a consensus score. We also completed a 'Risk of bias' table, considering randomisation, allocation concealment, blinding, incomplete outcome data, and size.
Measures of treatment effect
We used relative risk (or 'risk ratio', RR) to establish statistical difference. We used numbers needed to treat (NNT) and pooled percentages as absolute measures of benefit or harm.
We use the following terms to describe adverse outcomes in terms of harm or prevention of harm:
-
When significantly fewer adverse outcomes occur with etoricoxib than with control (placebo or active) we use the term the number needed to treat to prevent one event (NNTp).
-
When significantly more adverse outcomes occur with etoricoxib compared with control (placebo or active) we use the term the number needed to harm or cause one event (NNH).
Unit of analysis issues
We accepted only randomisation to the individual participant.
Dealing with missing data
The only likely issue with missing data in these studies is from imputation using last observation carried forward when a participant requests rescue medication. We have previously shown that this does not affect results for up to six hours after taking study medication (Barden 2004b).
Assessment of heterogeneity
We examined heterogeneity visually using L'Abbé plots (L'Abbé 1987).
Data synthesis
We followed QUOROM (Quality of Reporting of Meta‐analyses) guidelines (Moher 1999). For efficacy analyses we used the number of participants in each treatment group who were randomised, received medication, and provided at least one post‐baseline assessment. For safety analyses we used the number of participants randomised to each treatment group who took the study medication. We planned analyses for different doses.
For each study we converted the mean TOTPAR, SPID, VAS TOTPAR, or VAS SPID (Appendix 4) values for active and placebo to %maxTOTPAR or %maxSPID by division into the calculated maximum value (Cooper 1991), and calculated the proportion of participants in each treatment group who achieved at least 50%maxTOTPAR using verified equations (Moore 1996; Moore 1997a; Moore 1997b). We then converted these proportions into the number of participants achieving at least 50%maxTOTPAR by multiplying by the total number of participants in the treatment group. We used this information on the number of participants with at least 50%maxTOTPAR for active and placebo to calculate relative benefit or relative risk, and number needed to treat to benefit (NNT).
We accepted the following pain measures for the calculation of TOTPAR or SPID:
-
five‐point categorical pain relief (PR) scales with comparable wording to 'none, slight, moderate, good or complete';
-
four‐point categorical pain intensity (PI) scales with comparable wording to 'none, mild, moderate, severe';
-
VAS for pain relief; and
-
VAS for pain intensity.
If none of these measures were available, we used the number of participants reporting 'very good or excellent' on a five‐point categorical global scale with the wording 'poor, fair, good, very good, excellent' for the number of participants achieving at least 50% pain relief (Collins 2001).
For each treatment group we extracted the number of participants reporting treatment‐emergent adverse effects and calculated relative benefit and risk estimates with 95% confidence intervals (CI) using a fixed‐effect model (Morris 1995). We calculated NNT and number needed to treat to harm (NNH) and 95% CI using the pooled number of events using the method devised by Cook and Sackett (Cook 1995). We assumed a statistically significant difference from control when the 95% CI of the relative risk or relative benefit did not include the number one.
A minimum of two studies and 200 participants had to be available for reporting statistical analysis of pooled data.
Subgroup analysis and investigation of heterogeneity
We planned subgroup analyses to determine the effect of dose and presenting condition (pain model).
Sensitivity analysis
We planned sensitivity analyses for trial size (39 participants or fewer versus 40 or more per treatment arm) and quality score (two versus three or more).
A minimum of two studies and 200 participants had to be available in any subgroup or sensitivity analysis (Moore 1998), which were restricted to the primary outcome (50% pain relief over four to six hours) and the dose with the greatest amount of data (120 mg). We determined significant differences between NNT, NNTp, or NNH for different groups in subgroup and sensitivity analyses using the Z test (Tramèr 1997).
Results
Description of studies
Searches for the original review in 2009 (Clarke 2009) identified seven potentially relevant studies. Five of these studies fulfilled the inclusion criteria in 2009 (Chang 2004; Malmstrom 2004a; Malmstrom 2004b; Malmstrom 2005; Rasmussen 2005). We excluded one study after reading the full report, because it had no placebo group (Chalini 2005), and another as it was a press release (Anonymous 2001).
One further study was identified in the original review as ongoing and was subsequently published, and included in the 2012 update (Daniels 2011). One excluded study, previously available only as a summary in a clinical trials registry, has now been published (Viscusi 2012). We identified no new studies for this update (Figure 1).

Study flow diagram.
Details are in the 'Characteristics of included studies' and the 'Characteristics of excluded studies' tables.
In the included studies, a total of 919 participants were treated with different doses of etoricoxib and 295 with placebo; it was common in these studies for placebo group size to be smaller than active group size. In addition, 150 participants were treated with oxycodone/paracetamol (10/650 mg), 162 with codeine/paracetamol (60/600 mg), 240 with ibuprofen (400 or 600 mg), and 73 with controlled‐release naproxen sodium.
Six of the studies (Chang 2004; Daniels 2011; Malmstrom 2004a; Malmstrom 2004b; Malmstrom 2005; Rasmussen 2005), used etoricoxib 120 mg in six treatment arms, etoricoxib 60 mg in one treatment arm (Malmstrom 2004a), etoricoxib 90 mg in one treatment arm (Daniels 2011), etoricoxib 180 mg in one treatment arm (Malmstrom 2004a), and etoricoxib 240 mg in one treatment arm (Malmstrom 2004a).
Five studies (Chang 2004; Daniels 2011; Malmstrom 2004a; Malmstrom 2004b; Malmstrom 2005) enrolled participants with dental pain following extraction of at least one impacted third molar, and one study (Rasmussen 2005) enrolled participants with pain following uncomplicated orthopaedic surgery.
Trial duration was 24 hours in five studies (Chang 2004; Daniels 2011; Malmstrom 2004a; Malmstrom 2004b; Malmstrom 2005), and 24 hours in the single‐dose component of Rasmussen 2005. One study (Rasmussen 2005) included multiple doses, but reported results separately for the first dose (up to 24 hours) for at least some relevant outcomes. Another (Daniels 2011) used four doses over 24 hours, but only the first dose in the etoricoxib arms contained the active ingredient, and efficacy data are reported for the first dose separately.
Risk of bias in included studies
All included studies were both randomised and double‐blind, and were given a quality score of four or five. Full details of the studies can be found in the 'Characteristics of included studies' tables.
We completed a 'Risk of bias' table for each study, with results presented graphically in Figure 2 and summarised in Figure 3. The major threat to reliability was the relatively small size of the studies.

'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
Effects of interventions
See: Summary of findings for the main comparison
All six included studies contributed data for quantitative analysis. Pooled analysis was possible only for the 120 mg dose as only one treatment arm was available for each of the other doses. Details of the results of the individual studies can be seen in Appendix 5 (efficacy) and Appendix 6 (adverse events and withdrawals).
Number of participants with at least 50% pain relief over four to six hours
The 'Summary of results' table below shows all the results available, with relative risk (RR) and number needed to treat to benefit (NNT) calculated. However, data from more than one study were available only for the 120 mg dose, and data with more than 200 participants in the comparison were available only for the 90 mg and 120 mg doses. Etoricoxib 90 mg may be a licensed dose for acute pain in some countries, so we performed calculations despite the limited participant numbers available from a single study.
Etoricoxib 60 mg
Data were available for only 75 participants treated with etoricoxib 60 mg, all with dental pain (Malmstrom 2004a). Of these, the proportion experiencing at least 50% pain relief over six hours was 59% (44/75) compared with 12% (6/49) with placebo.
Etoricoxib 90 mg versus placebo
Data were available for 191 participants treated with etoricoxib 90 mg, all with dental pain (Daniels 2011).
-
The proportion of participants experiencing at least 50% pain relief over four to six hours with etoricoxib 90 mg was 77% (148/191).
-
The proportion of participants experiencing at least 50% pain relief over four to six hours with placebo was 17% (8/46).
-
The relative benefit of treatment compared with placebo was 4.5 (2.4 to 8.4); the NNT was 1.7 (1.4 to 2.1).
Etoricoxib 120 mg versus placebo
Six studies (798 participants) provided data for pain relief over six hours, with pain following dental or orthopaedic surgery (Chang 2004; Daniels 2011; Malmstrom 2004a; Malmstrom 2004b; Malmstrom 2005; Rasmussen 2005).
-
The proportion of participants experiencing at least 50% pain relief over four to six hours with etoricoxib 120 mg was 66% (332/503).
-
The proportion of participants experiencing at least 50% pain relief over four to six hours with placebo was 12% (34/295).
-
The relative benefit of treatment compared with placebo was 5.6 (4.0 to 7.8); the NNT was 1.8 (1.7 to 2.0) (Analysis 1.1; Figure 4).
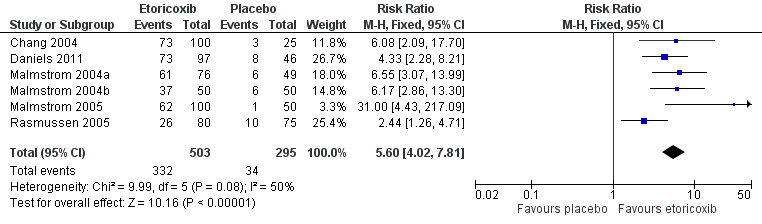
Forest plot of comparison: 1 Etoricoxib 120 mg versus placebo, outcome: 1.1 Participants with at least 50% pain relief over 6 hours
For dental studies only (five studies, 643 participants; Chang 2004; Daniels 2011; Malmstrom 2004a; Malmstrom 2004b; Malmstrom 2005), the relative benefit of treatment compared with placebo was 6.7 (4.6 to 9.8) and the NNT was 1.6 (1.5 to 1.8) (Analysis 1.2; Figure 5).

L'Abbé plot of etoricoxib 120 mg versus placebo for at least 50% pain relief. Size of circle is proportional to size of study (inset scale). Cream circles ‐ dental studies; pink circle ‐ orthopaedic study.
Etoricoxib 180 mg versus placebo
Data were available for 75 participants treated with etoricoxib 180 mg (Malmstrom 2004a). Of these, the proportion experiencing at least 50% pain relief over six hours was 85% (64/74) compared with 12% (6/49) with placebo.
Etoricoxib 240 mg versus placebo
Data were available for 76 participants treated with etoricoxib 240 mg (Malmstrom 2004a). Of these, the proportion experiencing at least 50% pain relief over six hours was 72% (55/76) compared with 12% (6/49) with placebo.
There was insufficient information to demonstrate a definitive dose response.
| Summary of results: number of participants with ≥ 50% pain relief over 4 to 6 hours | ||||||
| Dose (mg) | Studies | Participants | Etoricoxib (%) | Placebo (%) | RR (95% CI) | NNT (95%CI) |
| 60 | 1 | 124 (dental) | 59 | 12 | not calculated | not calculated |
| 90 | 1 | 237 (dental) | 77 | 17 | 4.5 (2.4 to 8.4) | 1.7 (1.4 to 2.1) |
| 120 | 6 | 798 | 66 | 12 | 5.6 (4.0 to 7.8) | 1.8 (1.7 to 2.0) |
| 120 | 5 | 643 (dental only) | 72 | 11 | 6.7 (4.6 to 9.8) | 1.6 (1.5 to 1.8) |
| 180 | 1 | 123 (dental) | 86 | 12 | not calculated | not calculated |
| 240 | 1 | 125(dental) | 72 | 12 | not calculated | not calculated |
Sensitivity analyses of the primary outcome
Pain model
Only one study (Rasmussen 2005) included participants who had undergone orthopaedic rather than dental surgery. There were insufficient data to compare results for dental and other surgery.
Quality score
All studies scored five for quality, so we did not carry out sensitivity analysis.
Trial size
All studies enrolled more than 40 participants per treatment arm, so we did not carry out sensitivity analysis.
Proportion of participants using rescue medication
All studies reported the proportion of participants using rescue medication for both etoricoxib and placebo, apart from Malmstrom 2005, in which omitted the placebo data (Appendix 5). We therefore excluded this study from this section of our analysis.
Use of rescue medication over six hours
Two studies (Chang 2004; Daniels 2011) reported use of rescue medication over six hours.
-
For etoricoxib 90 mg 8.4% (16/191) required rescue medication, compared with 65% (30/46) with placebo.
-
For etoricoxib 120 mg 17% (34/197) required rescue medication, compared with 68% (48/71) with placebo. The relative benefit of treatment compared with placebo was 0.24 (0.17 to 0.34); the number needed to treat to prevent one event (NNTp) was 2.0 (1.6 to 2.6) (Analysis 1.3).
Use of rescue medication over 24 hours
Four studies (Chang 2004; Malmstrom 2004a; Malmstrom 2004b; Rasmussen 2005) reported use of rescue medication over 24 hours.
-
For etoricoxib 60 mg 52% (39/75) required rescue medication, compared with 82% (40/49) with placebo.
-
For etoricoxib 120 mg 50% (154/306) required rescue medication, compared with 89% (178/199) with placebo. The relative benefit of treatment compared with placebo was 0.60 (0.53 to 0.67); the NNTp was 2.6 (2.2 to 3.1) (Analysis 1.4; Figure 6). For dental studies only, the proportions were 39% (88/226) for etoricoxib and 84% (104/124) for placebo, giving a relative benefit of treatment compared with placebo of 0.46 (0.38 to 0.56), and NNTp of 2.2 (1.9 to 2.8).
-
For etoricoxib 180 mg 26% (19/74) required rescue medication, compared with 82% (40/49) with placebo.
-
For etoricoxib 240 mg 33% (25/76) required rescue medication, compared with 82% (40/49) with placebo.

Forest plot of comparison: 1 Etoricoxib 120 mg vs placebo, outcome: 1.4 Participants using rescue medication within 24 hours
Time to use of rescue medication
For etoricoxib 120 mg the median time to use of rescue medication exceeded 24 hours in all the dental studies, whereas for the orthopaedic study (Rasmussen 2005), it was 3.6 hours (Appendix 5). Daniels 2011 reported this outcome only at six hours, with all active treatment arms having less than 50% remedication, while the median time to use of rescue medication was 2.1 hours with placebo. For the remaining dental and orthopaedic studies combined, the weighted mean of the median time to use of rescue medication was 20.0 hours for etoricoxib 120 mg and 2.0 hours for placebo. For dental studies only, the weighted mean of the median time to use of rescue medication exceeded 24 hours.
Adverse events
All the dental studies (Chang 2004; Daniels 2011; Malmstrom 2004a; Malmstrom 2004b; Malmstrom 2005) reported the number of participants with one or more adverse event for each treatment arm, although the time over which the information was collected varied between trials, from six hours to 14 days. It was unclear in one study (Chang 2004) whether the adverse event reports covered the duration of the trial (24 hours), or whether they included any adverse events occurring between the end of the trial and a follow‐up visit some days later. Rasmussen 2005, the orthopaedic study, did not provide any single dose data for adverse events (Appendix 6).
For all doses combined there was no significant difference in the proportion of participants experiencing at least one adverse event with etoricoxib (32%, 272/839) and placebo (36%, 79/220), giving a relative risk of 0.91 (0.74 to 1.1) (Analysis 2.1; Figure 7). There was again no significant difference for the 120 mg dose alone, with 33% (140/423) experiencing adverse events with etoricoxib, and 36% (79/220) with placebo, giving a relative risk of 0.93 (0.74 to 1.2) (Analysis 1.5).

Forest plot of comparison: 2 Etoricoxib (all doses) versus placebo, outcome: 2.1 Participants with any adverse event
Adverse events were generally described as mild to moderate in severity. There were no serious adverse events reported for etoricoxib. One study (Malmstrom 2004b) reported one serious adverse event in the sodium naproxen 550 mg treatment arm. This event, multiple fractures after a car accident, was reported 12 days after the study drug was taken and judged to be unrelated to the study medication.
Withdrawals
We classified participants who took rescue medication as withdrawals due to lack of efficacy, which we reported under 'Use of rescue medication' above. Withdrawals for reasons other than lack of efficacy were uncommon and usually due to protocol violations. No withdrawals due to adverse events were reported (Appendix 6).
Discussion
Summary of main results
Six studies satisfied the inclusion criteria for this updated review, providing information for both efficacy and harm for doses of etoricoxib ranging from 60 mg to 240 mg, although only the 120 mg dose provided sufficient data for a pooled analysis of any outcome. Sixty‐six per cent of those taking a single 120 mg dose of etoricoxib experienced the clinically useful primary outcome of at least 50% pain relief, compared with about 12% of those taking placebo. The number needed to treat to benefit (NNT) for at least 50% pain relief was 1.8 (1.7 to 2.0), meaning that almost one in two participants treated with etoricoxib 120 mg experienced this level of pain relief who would not have done so if treated with placebo. Limited data from one study in orthopaedic pain following initial patient‐controlled analgesia and appropriate washout, suggest that it is also effective in this situation, but less so. There were insufficient data to demonstrate a dose response.
Indirect comparisons of NNTs for at least 50% pain relief over four to six hours in reviews of other analgesics using identical methods (Moore 2011a) indicate that etoricoxib 120 mg has:
-
equivalent efficacy to soluble ibuprofen 400 mg (NNT 1.8 (1.7 to 2.0), naproxen 500/550 mg (NNT 1.8 (1.6 to 2.1)), and diclofenac potassium 100 mg (NNT 1.9 (1.7 to 2.2));
-
slightly better efficacy than standard ibuprofen 400 mg (NNT 2.3 (2.2 to 2.5)) and celecoxib 400 mg (NNT 2.5 (2.2 to 2.9)); and
-
much better efficacy than aspirin 1000 mg (NNT 4.2 (3.2 to 6.0)), diclofenac sodium 100 mg (NNT 4.5 (3.2 to 7.6)), and paracetamol 1000 mg (NNT 3.2 (2.9 to 3.6)).
It has been suggested that data on the use of rescue medication, whether as a proportion of participants requiring it or the median time to its use, might be helpful in assessing the usefulness of an analgesic, and possibly distinguishing between different doses (Moore 2005a). In this review only about half of participants treated with etoricoxib 120 mg following dental surgery required rescue medication within 24 hours, compared to nearly all those treated with placebo. Indirect comparisons with other analgesics for duration of action (Moore 2011a) indicate that etoricoxib 120 mg has a longer duration of action than celecoxib 400 mg (8.4 hours) and commonly used traditional NSAIDs, such as ibuprofen 400 mg (5.4 hours), diclofenac 100 mg (4.9 hours), and naproxen 500 mg (8.9 hours). Longer duration of action may be advantageous in some circumstances. In a postoperative setting, where patients may feel nauseated, a longer time before remedication is needed may be of benefit to the patient, and it may also reduce demands on time for nursing staff. There were insufficient data to examine the effect of dose on duration of action.
Reporting of data for adverse events, withdrawals (other than lack of efficacy), or exclusions, and handling of missing data was better in these recent studies than in many older reports of single‐dose analgesics. Poor reporting of adverse events in acute pain trials has been noted before (Edwards 1999). The method of reporting adverse events (usually specified as 'spontaneous') was not explicit (e.g. patient diary, recall at follow‐up visit) and they were collected over different periods of time. This almost certainly included periods after the use of rescue medication, which may cause its own adverse events. The usefulness of single dose studies for assessing adverse events is questionable, but it is nonetheless reassuring that in these studies there was no difference between etoricoxib (at any dose) and placebo for occurrence of any adverse event, and there were no serious adverse events or adverse event withdrawals. Long‐term, multiple‐dose studies should be used for meaningful analysis of adverse events since, even in acute pain settings, analgesics are likely to be used in multiple doses.
Overall completeness and applicability of evidence
Included studies reported useful data for both primary and secondary outcomes, with the exception of placebo results for time to use of rescue medication in Malmstrom 2005. Five studies were carried out in participants with pain following surgical removal of impacted third molars. These individuals were generally in their early 20s and otherwise fit and healthy, so are clearly not representative of the range of individuals who might need analgesia for acute postoperative pain. There is no a priori reason why analgesic response in these individuals should differ in any systematic way from a more generalised population, but it is entirely possible that adverse events (gastrointestinal in particular) may be more frequent, intense, or severe in older patients and those with comorbidities. The remaining study was carried out in patients with pain following orthopaedic surgery, and while response with placebo was the same as in dental pain, response with etoricoxib was lower in this one study. This may be due to chance, greater age of participants (mean 65 years), or a fundamental difference in the painful condition. Differences between different pain models have either not been demonstrable in the past (Barden 2004c) or have been possible to demonstrate only where there is an abundance of data (e.g. for ibuprofen; Derry 2009c).
Data for doses other than 120 mg were limited to one treatment arm each, so we could not make inferences about benefit and harm of lower and higher doses.
Quality of the evidence
All studies were of high methodological quality, scoring 4/5 or 5/5 on the Oxford Quality Scale, and all administered the medication when pain levels were moderate or severe, ensuring that the study was sensitive to detect a 50% reduction.
We judged two studies to be at high risk of bias because the placebo arms were small (< 50 participants), despite moderate numbers (100 to 200) in the active treatment arms (Chang 2004; Daniels 2011). There were no other major concerns about potential bias in individual studies.
Potential biases in the review process
We carried out a comprehensive search for relevant studies and investigated the potential influence of publication bias by examining the number of participants in studies with zero effect (relative risk of 1.0) needed for the point estimate of the NNT to increase beyond a clinically useful level (Moore 2008). In this case, we chose a clinically useful level as eight. For the primary outcome of at least 50% pain relief with etoricoxib 120 mg, more than 5000 participants would have to have been involved in unpublished trials with zero treatment effects for the NNT to increase above this threshold. It is highly unlikely that this amount of missing data exists.
Agreements and disagreements with other studies or reviews
We are not aware of any other reviews of etoricoxib to treat acute postoperative pain.
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
Forest plot of comparison: 1 Etoricoxib 120 mg versus placebo, outcome: 1.1 Participants with at least 50% pain relief over 6 hours
L'Abbé plot of etoricoxib 120 mg versus placebo for at least 50% pain relief. Size of circle is proportional to size of study (inset scale). Cream circles ‐ dental studies; pink circle ‐ orthopaedic study.
Forest plot of comparison: 1 Etoricoxib 120 mg vs placebo, outcome: 1.4 Participants using rescue medication within 24 hours
Forest plot of comparison: 2 Etoricoxib (all doses) versus placebo, outcome: 2.1 Participants with any adverse event

Comparison 1 Etoricoxib 120 mg vs placebo, Outcome 1 Participants with at least 50% pain relief over 6 hours.

Comparison 1 Etoricoxib 120 mg vs placebo, Outcome 2 Participants with at least 50% pain relief over 6 hours, dental.

Comparison 1 Etoricoxib 120 mg vs placebo, Outcome 3 Participants using rescue medication within 6 hours.

Comparison 1 Etoricoxib 120 mg vs placebo, Outcome 4 Participants using rescue medication within 24 hours.

Comparison 1 Etoricoxib 120 mg vs placebo, Outcome 5 Participants with any adverse event.

Comparison 2 Etoricoxib (all doses) versus placebo, Outcome 1 Participants with any adverse event.
| Etoricoxib compared with placebo for acute postoperative pain | ||||||
| Patient or population: adults with moderate or severe acute postoperative pain Settings: community or hospital Intervention: etoricoxib 120 mg Comparison: placebo | ||||||
| Outcomes | Probable outcome with | Relative effect and NNT or NNH (95% CI) | No of studies, events | Quality of the evidence | Comments | |
| comparator | intervention | |||||
| At least 50% of maximum pain relief over 4 to 6 hours | 120 in 1000 | 660 in 1000 | RR 5.6 (4.0 to 7.8) NNT 1.9 (1.7 to 2.1) | 6 studies 789 participants 366 events | High | Adequate numbers of studies, participants and events. Consistency across studies |
| Participants with at least 1 adverse event | 360 in 1000 | 330 in 1000 | RR 0.93 (0.74 to 1.2) NNH not calculated | 5 studies 643 participants 219 events | Moderate | Moderate numbers of studies, participants and events. Consistency across studies. Single dose studies may not reflect clinical practice |
| Participants with a serious adverse event | No serious adverse events | Low | Studies underpowered to detect rare events | |||
| Deaths | No deaths | Low | Studies underpowered to detect rare events | |||
| CI: Confidence interval; NNH: number needed to treat for harm; NNT: number needed to treat for benefit; RR: Risk Ratio | ||||||
| GRADE Working Group grades of evidence | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Participants with at least 50% pain relief over 6 hours Show forest plot | 6 | 798 | Risk Ratio (M‐H, Fixed, 95% CI) | 5.60 [4.02, 7.81] |
| 2 Participants with at least 50% pain relief over 6 hours, dental Show forest plot | 5 | 643 | Risk Ratio (M‐H, Fixed, 95% CI) | 6.68 [4.55, 9.82] |
| 3 Participants using rescue medication within 6 hours Show forest plot | 2 | 268 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.24 [0.17, 0.34] |
| 4 Participants using rescue medication within 24 hours Show forest plot | 4 | 505 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.60 [0.53, 0.67] |
| 5 Participants with any adverse event Show forest plot | 5 | 643 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.74, 1.17] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Participants with any adverse event Show forest plot | 5 | 1059 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.74, 1.12] |