Manipulación y movilización para el dolor de cuello comparadas con un control inactivo u otro tratamiento activo
Appendices
Appendix 1. Search strategy
MEDLINE (Ovid)
Last Update November 2014; research librarian: Maurine Rice, McMaster University
1. neck/ or neck muscles/ or exp cervical plexus/ or exp cervical vertebrae/ or Atlanto‐Axial Joint/ or atlanto‐occipital joint/ or axis/ or atlas/ or spinal nerve roots/ or exp brachial plexus/
2. (odontoid or cervical or occip: or atlant:).tw.
3. 1 or 2
4. exp arthritis/ or exp myofascial pain syndromes/ or fibromyalgia/ or spondylitis/ or exp spinal osteophytosis/ or spondylolisthesis/
5. exp headache/ and cervic:.tw.
6. whiplash injuries/ or cervical rib syndrome/ or torticollis/ or cervico‐brachial neuralgia.ti,ab,sh. or exp radiculitis/ or polyradiculitis/ or polyradiculoneuritis/ or thoracic outlet syndrome/
7. (monoradicul: or monoradicl:).tw.
8. 4 or 5 or 6 or 7
9. random:.ti,ab,sh.
10. randomised controlled trial.pt.
11. double‐blind method/
12. single blind method/
13. placebos/
14. clinical trial.pt.
15. exp clinical trials/
16. controlled clinical trial.pt.
17. (clin$ adj25 trial$).ti,ab.
18. ((singl$ or doubl$ or trebl$) adj25 (blind$ or mask$)).ti,ab.
19. placebo$.ti,ab.
20. or/9‐19
21. exp arthritis/rh,th or exp myofascial pain syndromes/rh,th or fibromyalgia/rh,th or spondylitis/rh,th or exp spinal osteophytosis/rh,th or spondylosis/rh,th or spondylolisthesis/rh,th
22. exp headache/rh,th and cervic:.tw.
23. whiplash injuries/rh,th or cervical rib syndrome/rh,th or thoracic outlet syndrome/rh,th or torticollis/rh,th or cervico‐brachial neuralgia/rh,th or exp radiculitis/rh,th or polyradiculitis/rh,th or polyradiculoneuritis/rh,th
24. or/21‐23
25. exp alternative medicine/ or chiropractic/
26. (acupuncture or biofeedback or chiropract: or electric stimulation therapy or kinesiology or massage or traditional medicine or relaxation or therapeutic touch).tw.
27. or/25‐26
28. 3 and 24
29. 3 and 8 and 27
30. 28 or 29
31. 20 and 30
EMBASE (Ovid)
Last Updated November 2014; research librarian: Maurine Rice, McMaster Univesity
1. neck pain/
2. brachial plexus neuropathy/
3. neck injury/ or whiplash injury/
4. cervical pain.mp.
5. neckache.mp.
6. whiplash.mp.
7. cervicodynia.mp.
8. cervicalgia.mp.
9. brachialgia/
10. brachialgia.mp.
11. brachial neuritis.mp.
12. brachial neuralgia.mp.
13. neck pain.mp.
14. neck injur*.mp.
15. brachial plexus neuropath*.mp.
16. brachial plexus neuritis.mp.
17. thorax outlet syndrome/
18. torticollis/
19. cervico brachial neuralgia.ti,ab.
20. cervicobrachial neuralgia.ti,ab.
21. (monoradicul* or monoradicl*).tw.
22. or/1‐21
23. exp headache/ and cervic*.tw.
24. exp gynecologic disease/
25. genital disease*.mp.
26. exp *uterine cervix/
27. or/24‐26
28. 23 not 27
29. 22 or 28
30. neck/ or neck muscle/
31. cervical plexus/
32. cervical spine/
33. atlantoaxial joint/
34. atlantooccipital joint/
35. atlas/
36. "spinal root"/
37. brachial plexus/
38. (odontoid* or cervical or occip* or atlant*).tw.
39. odontoid process/
40. cervical vertebra.mp.
41. cervical vertebrae.mp.
42. cervical plexus.mp.
43. cervical spine.mp.
44. (neck adj3 muscles).mp.
45. (brachial adj3 plexus).mp.
46. (thoracic adj3 vertebra?).mp.
47. neck.mp.
48. (thoracic adj3 spine).mp.
49. (thoracic adj3 outlet).mp.
50. trapezius.mp.
51. cervical.mp.
52. cervico*.mp.
53. 51 or 52
54. exp gynecologic disease/
55. genital disease*.mp.
56. exp *uterine cervix/
57. 54 or 55 or 56
58. 53 not 57
59. 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 or 58
60. exp pain/
61. exp injury/
62. pain.mp.
63. ache.mp.
64. sore.mp.
65. stiff.mp.
66. discomfort.mp.
67. injur*.mp.
68. neuropath*.mp.
69. or/60‐68
70. radiculopathy/
71. temporomandibular joint disorder/
72. myofascial pain/
73. spondylosis/ or cervical spondylosis/
74. neuritis/
75. exp arthritis/
76. fibromyalgia/
77. exp spondylitis/
78. diskitis/
79. spondylolisthesis/
80. radiculopathy.mp.
81. radiculitis.mp.
82. temporomandibular.mp.
83. myofascial pain syndrome*.mp.
84. spinal osteophytosis.mp.
85. neuritis.mp.
86. spondylosis.mp.
87. spondylitis.mp.
88. spondylolisthesis.mp.
89. or/70‐88
90. 59 and 89
91. neck/
92. cervical spine/
93. neck.mp.
94. (thoracic adj3 vertebra?).mp.
95. cervical.mp.
96. cervico*.mp.
97. exp gynecologic disease/
98. genital disease*.mp.
99. exp *uterine cervix/
100. or/97‐99
101. 95 or 96
102. 101 not 100
103. (thoracic adj3 spine).mp.
104. cervical spine.mp.
105. 91 or 92 or 93 or 94 or 102 or 103 or 104
106. intervertebral disk/
107. (disc or discs).mp.
108. (disk or disks).mp.
109. 106 or 107 or 108
110. 105 and 109
111. herniat*.mp.
112. slipped.mp.
113. prolapse*.mp.
114. displace*.mp.
115. degenerat*.mp.
116. (bulge or bulged or bulging).mp.
117. 110 or 111 or 112 or 113 or 114 or 115 or 116
118. 110 and 117
119. intervertebral disk hernia/
120. intervertebral disk degeneration/
121. intervertebral disc degeneration.mp.
122. intervertebral disk degeneration.mp.
123. intervertebral disc displacement.mp.
124. intervertebral disk displacement.mp.
125. 119 or 120 or 121 or 122 or 123 or 124
126. 105 and 125
127. 59 and 69
128. 29 or 90 or 118 or 126 or 127
129. exp *neoplasm/
130. exp *penetrating trauma/
131. 129 or 130
132. 128 not 131
133. neck pain/rh, th
134. brachial plexus neuropathy/rh, th
135. neck injury/ or whiplash injury/rh, th
136. brachialgia/rh, th
137. thorax outlet syndrome/rh, th
138. Torticollis/rh, th
139. Radiculopathy/rh, th
140. temporomandibular joint disorder/rh, th
141. myofascial pain/rh, th
142. spondylosis/rh, th or cervical spondylosis/rh, th
143. neuritis/rh, th
144. exp arthritis/rh, th
145. Fibromyalgia/rh, th
146. exp spondylitis/rh, th
147. diskitis/rh, th
148. spondylolisthesis/rh, th
149. acupuncture/ or acupressure/ or acupuncture analgesia/
150. exp manipulative medicine/
151. massage.tw.
152. mobili?ation.tw.
153. (acupuncture or acu‐puncture or needling or acupressure or mox?bustion).tw.
154. ((neck or spine or spinal or cervical or chiropractic* or musculoskeletal* or musculo‐skeletal*) adj3 (adjust* or manipulat* or mobiliz* or mobilis*)).tw.
155. (manual adj therap*).tw.
156. (manipulati* adj (therap* or medicine)).tw.
157. (massag* or reflexolog* or rolfing or zone therap*).tw.
158. Nimmo.tw.
159. (vibration adj5 (therap* or treatment*)).tw.
160. (Chih Ya or Shiatsu or Shiatzu or Zhi Ya).tw.
161. (flexion adj2 distraction*).tw.
162. (myofascial adj3 (release or therap*)).tw.
163. muscle energy technique*.tw.
164. trigger point.tw.
165. proprioceptive Neuromuscular Facilitation*.tw.
166. cyriax friction.tw.
167. (lomilomi or lomi‐lomi or trager).tw.
168. aston patterning.tw.
169. (strain adj counterstrain).tw.
170. (craniosacral therap* or cranio‐sacral therap*).tw.
171. (amma or ammo or effleuurage or petrissage or hacking or tapotment).tw.
172. alternative medicine/
173. ((complement* or alternat* or osteopthic*) adj (therap* or medicine)).tw.
174. (Tui Na or Tuina).tw.
175. (swedish massage or rolfing).tw.
176. therapeutic touch.mp.
177. massotherapy.tw.
178. effleurage.mp.
179. or/149‐178
180. 132 and 179
181. 133 or 134 or 135 or 136 or 137 or 138
182. or/139‐148
183. 59 and 182
184. 180 or 181 or 183
185. randomized controlled trial/
186. controlled clinical trial/
187. (random* or sham or placebo*).tw.
188. placebo/
189. randomization/
190. single blind procedure/
191. double blind procedure/
192. ((singl* or doubl* or trebl* or tripl*) adj5 (blind* or dumm*or mask*)).ti,ab.
193. (rct or rcts).tw.
194. (control* adj2 (study or studies or tiral*)).tw.
195. or/185‐194
196. human/
197. nonhuman/
198. animal/
199. animal experiment/
200. or/197‐199
201. 200 not (200 and 196)
202. 195 not 201
203. 184 and 202
204. limit 203 to yr="2006 ‐Current"
205. limit 203 to yr="1928 ‐ 2005"
206. guidelines as topic/
207. practice guidelines as topic/
208. (guideline? or guidance or recommendations).ti.
209. consensus.ti.
210. or/206‐209
211. 184 and 210
212. limit 211 to yr="2006 ‐Current"
213. limit 211 to yr="1928 ‐ 2005"
214. meta analysis/
215. systematic review/
216. (meta analy* or metaanaly* or met analy* or metanaly*).tw.
217. (collaborative research or collaborative review* or collaborative overview*).tw.
218. (integrative research or integrative review* or intergrative overview*).tw.
219. (quantitative adj3 (research or review* or overview*)).tw.
220. (research integration or research overview*).tw.
221. (systematic* adj3 (review* or overview*)).tw.
222. (methodologic* adj3 (review* or overview*)).tw.
223. biomedical technology assessment/
224. (hta or thas or technology assessment*).tw.
225. ((hand adj2 search*) or (manual* adj search*)).tw.
226. ((electronic adj database*) or (bibliographic* adj database*)).tw.
227. ((data adj2 abstract*) or (data adj2 extract*)).tw.
228. (data adj3 (pooled or pool or pooling)).tw.
229. (analys* adj3 (pool or pooled or pooling)).tw.
230. mantel haenszel.tw.
231. (cochrane or Pubmed or pub med or medline or embase or psycinfo or psyclit or psychinfo or psychlit or cinahl or science citation index).ab.
232. or/214‐231
233. 184 and 232
234. limit 233 to yr="2006 ‐Current"
235. limit 233 to yr="1928 ‐ 2005"
236. (ae or co or si or to).fs.
237. (safe or safety or unsafe).tw.
238. (side effect* or side event*).tw.
239. ((adverse or undesirable or harm* or injurious or serious or toxic) adj3 (effect* or event* or reaction* or incident* or outcome*)).tw.
240. (abnormalit* or toxicit* or complication* or consequence* or noxious or tolerabilit*).tw.
241. or/236‐240
242. 184 and 241
243. limit 242 to yr="2006 ‐Current"
244. limit 242 to yr="1928 ‐ 2005"
245. limit 203 to em=201027‐201216
246. limit 211 to em=201027‐201216
247. limit 233 to em=201027‐201216
248. limit 242 to em=201027‐201216
CENTRAL (Ovid)
Last Update November 2014; research librarian: Maurine Rice, McMaster University
1 Neck Pain/
2 exp Brachial Plexus Neuropathies/
3 exp neck injuries/ or exp whiplash injuries/
4 cervical pain.mp.
5 neckache.mp.
6 whiplash.mp.
7 cervicodynia.mp.
8 cervicalgia.mp.
9 brachialgia.mp.
10 brachial neuritis.mp.
11 brachial neuralgia.mp.
12 neck pain.mp.
13 neck injur*.mp.
14 brachial plexus neuropath*.mp.
15 brachial plexus neuritis.mp.
16 thoracic outlet syndrome/ or cervical rib syndrome/
17 Torticollis/
18 exp brachial plexus neuropathies/ or exp brachial plexus neuritis/
19 cervico brachial neuralgia.ti,ab.
20 cervicobrachial neuralgia.ti,ab.
21 (monoradicul* or monoradicl*).tw.
22 or/1‐21
23 exp headache/ and cervic*.tw.
24 exp genital diseases, female/
25 genital disease*.mp.
26 or/24‐25
27 23 not 26
28 22 or 27
29 neck/
30 neck muscles/
31 exp cervical plexus/
32 exp cervical vertebrae/
33 atlanto‐axial joint/
34 atlanto‐occipital joint/
35 Cervical Atlas/
36 spinal nerve roots/
37 exp brachial plexus/
38 (odontoid* or cervical or occip* or atlant*).tw.
39 axis/ or odontoid process/
40 Thoracic Vertebrae/
41 cervical vertebrae.mp.
42 cervical plexus.mp.
43 cervical spine.mp.
44 (neck adj3 muscles).mp.
45 (brachial adj3 plexus).mp.
46 (thoracic adj3 vertebrae).mp.
47 neck.mp.
48 (thoracic adj3 spine).mp.
49 (thoracic adj3 outlet).mp.
50 trapezius.mp.
51 cervical.mp.
52 cervico*.mp.
53 51 or 52
54 exp genital diseases, female/
55 genital disease*.mp.
56 exp *Uterus/
57 54 or 55 or 56
58 53 not 57
59 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 or 58
60 exp pain/
61 exp injuries/
62 pain.mp.
63 ache.mp.
64 sore.mp.
65 stiff.mp.
66 discomfort.mp.
67 injur*.mp.
68 neuropath*.mp.
69 or/60‐68
70 59 and 69
71 Radiculopathy/
72 exp temporomandibular joint disorders/ or exp temporomandibular joint dysfunction syndrome/
73 myofascial pain syndromes/
74 exp "Sprains and Strains"/
75 exp Spinal Osteophytosis/
76 exp Neuritis/
77 Polyradiculopathy/
78 exp Arthritis/
79 Fibromyalgia/
80 spondylitis/ or discitis/
81 spondylosis/ or spondylolysis/ or spondylolisthesis/
82 radiculopathy.mp.
83 radiculitis.mp.
84 temporomandibular.mp.
85 myofascial pain syndrome*.mp.
86 thoracic outlet syndrome*.mp.
87 spinal osteophytosis.mp.
88 neuritis.mp.
89 spondylosis.mp.
90 spondylitis.mp.
91 spondylolisthesis.mp.
92 or/71‐91
93 59 and 92
94 exp neck/
95 exp cervical vertebrae/
96 Thoracic Vertebrae/
97 neck.mp.
98 (thoracic adj3 vertebrae).mp.
99 cervical.mp.
100 cervico*.mp.
101 99 or 100
102 exp genital diseases, female/
103 genital disease*.mp.
104 exp *Uterus/
105 or/102‐104
106 101 not 105
107 (thoracic adj3 spine).mp.
108 cervical spine.mp.
109 94 or 95 or 96 or 97 or 98 or 106 or 107 or 108
110 Intervertebral Disk/
111 (disc or discs).mp.
112 (disk or disks).mp.
113 110 or 111 or 112
114 109 and 113
115 herniat*.mp.
116 slipped.mp.
117 prolapse*.mp.
118 displace*.mp.
119 degenerat*.mp.
120 (bulge or bulged or bulging).mp.
121 115 or 116 or 117 or 118 or 119 or 120
122 114 and 121
123 intervertebral disk degeneration/ or intervertebral disk displacement/
124 intervertebral disk displacement.mp.
125 intervertebral disc displacement.mp.
126 intervertebral disk degeneration.mp.
127 intervertebral disc degeneration.mp.
128 123 or 124 or 125 or 126 or 127
129 109 and 128
130 28 or 70 or 93 or 122 or 129
131 animals/ not (animals/ and humans/)
132 130 not 131
133 exp *neoplasms/
134 exp *wounds, penetrating/
135 133 or 134
136 132 not 135
137 Neck Pain/rh, th [Rehabilitation, Therapy]
138 exp Brachial Plexus Neuropathies/rh, th
139 exp neck injuries/rh, th or exp whiplash injuries/rh, th
140 thoracic outlet syndrome/rh, th or cervical rib syndrome/rh, th
141 Torticollis/rh, th
142 exp brachial plexus neuropathies/rh, th or exp brachial plexus neuritis/rh, th
143 or/137‐142
144 Radiculopathy/rh, th
145 exp temporomandibular joint disorders/rh, th or exp temporomandibular joint dysfunction syndrome/rh, th
146 myofascial pain syndromes/rh, th
147 exp "Sprains and Strains"/rh, th
148 exp Spinal Osteophytosis/rh, th
149 exp Neuritis/rh, th
150 Polyradiculopathy/rh, th
151 exp Arthritis/rh, th
152 Fibromyalgia/rh, th
153 spondylitis/rh, th or discitis/rh, th
154 spondylosis/rh, th or spondylolysis/rh, th or spondylolisthesis/rh, th
155 or/144‐154
156 59 and 155
157 acupuncture/ or chiropractic/
158 exp Musculoskeletal Manipulations/
159 massage.tw.
160 mobili?ation.tw.
161 Acupuncture Therapy/
162 (acupuncture or acu‐puncture or needling or acupressure or mox?bustion).tw.
163 ((neck or spine or spinal or cervical or chiropractic* or musculoskeletal* or musculo‐skeletal*) adj3 (adjust* or manipulat* or mobiliz* or mobilis*)).tw.
164 (manual adj therap*).tw.
165 (manipulati* adj (therap* or medicine)).tw.
166 (massag* or reflexolog* or rolfing or zone therap*).tw.
167 Nimmo.mp.
168 exp Vibration/tu [Therapeutic Use]
169 (vibration adj5 (therap* or treatment*)).tw.
170 (Chih Ya or Shiatsu or Shiatzu or Zhi Ya).tw.
171 (flexion adj2 distraction*).tw.
172 (myofascial adj3 (release or therap*)).tw.
173 muscle energy technique*.tw.
174 trigger point.tw.
175 proprioceptive Neuromuscular Facilitation*.tw.
176 cyriax friction.tw.
177 (lomilomi or lomi‐lomi or trager).tw.
178 aston patterning.tw.
179 (strain adj counterstrain).tw.
180 (craniosacral therap* or cranio‐sacral therap*).tw.
181 (amma or ammo or effleuurage or petrissage or hacking or tapotment).tw.
182 Complementary Therapies/
183 ((complement* or alternat* or osteopthic*) adj (therap* or medicine)).tw.
184 (Tui Na or Tuina).tw.
185 or/157‐184
186 136 and 185
187 143 or 156 or 186
188 animals/ not (animals/ and humans/)
189 187 not 188
190 limit 189 to yr="2010 ‐ 2012"
CINAHL (EBSCO)
Last Update November 2014; research librarian: Maurine Rice, McMaster University
S139 S115 and S131 Limiters ‐ Published Date: 20121231‐20140330
S138 S115 and S131
S137 S109 and S131 Limiters ‐ Published Date: 20121231‐20140330
S136 S109 and S131
S135 S94 and S131 Limiters ‐ Published Date: 20121231‐20140330
S134 S94 and S131
S133 S91 and S131 Limiters ‐ Published Date: 20121231‐20140330
S132 S91 and S131
S131 S82 and S130
S130 S116 or S117 or S118 or S119 or S120 or S121 or S122 or S123 or S124 or S125 or S126 or S127 or S128 or S129
S129 TX ( ((complement* or alternat* or osteopthic*) N1 (therap* or medicine)) ) OR TX ( (Tui Na or Tuina) )
S128 TX (strain N1 counterstrain) OR TX ( (craniosacral therap* or cranio‐sacral therap*) ) OR TX ( (amma or ammo or effleuurage or petrissage or hacking or tapotment) )
S127 TX cyriax friction OR TX ( (lomilomi or lomi‐lomi or trager) ) OR TX aston patterning
S126 TX muscle energy technique* OR TX trigger point OR TX proprioceptive Neuromuscular Facilitation*
S125 TX ( (Chih Ya or Shiatsu or Shiatzu or Zhi Ya) ) OR TX (flexion N2 distraction*) OR TX ( (myofascial N3 (release or therap*)) )
S124 (MH "Vibration/TU")
S123 TX ( (massag* or reflexolog* or rolfing or zone therap*) ) OR TX Nimmo OR TX ( (vibration N5 (therap* or treatment*)) )
S122 TX (manipulati* N1 (therap* or medicine))
S121 TX ((neck or spine or spinal or cervical or chiropractic* or musculoskeletal* or musculo‐skeletal*) N3 (adjust* or manipulat* or mobiliz* or mobilis*))
S120 TX mobili?ation OR TX ( (acupuncture or acu‐puncture or needling or acupressure or mox?bustion) ) OR TX manual therapy
S119 (MH "Massage+") OR (MH "Deep Tissue Massage") OR (MH "Neuromuscular Massage") OR (MH "Sports Massage") OR (MH "Massage Therapists") OR (MH "Swedish Massage")
S118 (MH "Manipulation, Chiropractic") OR (MH "Manual Therapy+")
S117 (MH "Chiropractic+") OR (MH "Manipulation, Chiropractic") OR (MH "Chiropractic Practice") OR (MH "Chiropractors")
S116 (MH "Acupuncture+") OR (MH "Acupuncture Points") OR (MH "Acupuncturists")
S115 S110 or S111 or S112 or S113 or S114
S114 TX toxic reaction OR TX allergic reaction OR TX complications Limiters ‐ Published Date: 20100101‐20121231
S113 TX adverse outcome* OR TX adverse incident* Limiters ‐ Published Date: 20100101‐20121231
S112 TX adverse event* OR TX adverse effect* OR TX adverse reaction* Limiters ‐ Published Date: 20100101‐20121231
S111 TX ( (safe or safety or unsafe) ) OR TX ( (side effect* or side event*) ) Limiters ‐ Published Date: 20100101‐20121231
S110 (MH "Adverse Drug Event") Limiters ‐ Published Date: 20100101‐20121231
S109 S95 or S96 or S97 or S98 or S99 or S100 or S101 or S102 or S103 or S104 or S105 or S106 or S107 or S108
S108 TX PsycINFO or TX psycLIT or TX PsychINFO or TX psychLIT or TX CINAHL
S107 TX cochrane or TX pubmed or TX pub med or TX medline or TX embase
S106 TX mantel haenszel
S105 TX data N2 pool* or TX analys* N2 pool*
S104 TX data N2 abstract* or TX data N2 extract*
S103 TX electronic N2 database* or TX bibliographic database*
S102 TX hand N2 search* or TX manual N2 search
S101 TX hta or TX htas or TX technology assessment*
S100 TX methodologic* N3 review* or TX methodologic* N3 overview*
S99 TX systematic* N3 review* or TX systematic* N3 overview*
S98 TX quantitative research or TX quantitative review* or TX quantitative overview*
S97 TX meta analy* or TX metaanaly* or TX met analy* or TX metanaly*
S96 (MH "Meta Analysis")
S95 PT systematic review
S94 S92 or S93
S93 TI guideline* or TI guidance or TI recommendations or TI consensus
S92 (MH "Practice Guidelines")
S91 S83 or S84 or S85 or S86 or S87 or S88 or S89 or S90
S90 TX control* N2 study or TX control* N2 studies or TX control N2 trial*
S89 TX RCT or TX RCTs
S88 TX (singl* N1 (blind* OR dumm* OR mask*))
S87 (MH "Random Sample+")
S86 (MH "Placebos")
S85 TX random* or TX sham or TX placebo*
S84 PT clinical trial or PT randomized controlled trial
S83 (MH "Clinical Trials+")
S82 S78 NOT S81
S81 S79 or S80
S80 (MM "Pregnancy+")
S79 (MM "Abortion, Induced+")
S78 S74 NOT S77
S77 S75 or S76
S76 (MM "Wounds, Penetrating+")
S75 (MM "Neoplasms+")
S74 S16 or S41 or S56 or S69 or S73
S73 S63 and S72
S72 S70 or S71
S71 TX intervertebral disk displacement or TX intervertebral disc displacement or TX intervertebral disk degeneration or TX intervertebral disc degeneration
S70 (MH "Intervertebral Disk Displacement")
S69 S67 and S68
S68 TX herniat* or TX slipped or TX prolapse* or TX displace* or TX degenerat* or TX ( bulged OR bulge OR bulging )
S67 S63 and S66
S66 S64 or S65
S65 TX disc or TX discs or TX disk or TX disks
S64 (MH "Intervertebral Disk")
S63 S61 NOT S62
S62 (MM "Genital Diseases, Female+") or ( (MM "Cervix") or (MM "Cervix Diseases") )
S61 S57 or S58 or S59 or S60
S60 TX thoracic N3 spine or TX cervical spine or TX cervico*
S59 TX neck or TX thoracic N3 vertebr*
S58 (MH "Thoracic Vertebrae")
S57 (MH "Neck")
S56 S34 and S55
S55 S42 or S43 or S44 or S45 or S46 or S47 or S48 or S49 or S50 or S51 or S52 or S53 or S54
S54 TX neuritis or TX spondylosis or TX spondylitis or TX spondylolisthesis
S53 TX myofascial pain syndome* or TX thoracic outlet syndrome* or TX spinalosteophytosis
S52 TX radiculopathy or TX radiculitis or TX temporomandibular
S51 (MH "Spondylolysis") or (MH "Spondylolisthesis+")
S50 (MH "Fibromyalgia")
S49 (MH "Arthritis+")
S48 (MH "Polyradiculopathy")
S47 (MH "Neuritis+")
S46 (MH "Spinal Osteophytosis")
S45 (MH "Sprains and Strains+")
S44 (MH "Myofascial Pain Syndromes+")
S43 (MH "Temporomandibular Joint Diseases+") or (MH "Temporomandibular Joint Syndrome")
S42 (MH "Radiculopathy")
S41 S34 and S40
S40 S35 or S36 or S37 or S38 or S39
S39 (MH "Neuralgia")
S38 TX stiff or TX discomfort or TX injur* or TX neuropath*
S37 TX pain or TX ache* or TX sore
S36 (MH "Wounds and Injuries+")
S35 (MH "Pain+")
S34 S33 NOT S32
S33 S17 or S18 or S19 or S20 or S21 or S22 or S23 or S24 or S25 or S26 or S27 or S28 or S29 or S30 or S31
S32 (MM "Genital Diseases, Female+") or ( (MM "Cervix") or (MM "Cervix Diseases") )
S31 TX trapezius or TX cervico*
S30 TX thoracic N3 spine or TX thoracic N3 outlet
S29 TX neck
S28 TX thoracic N3 verteb*
S27 TX brachial N3 plexus
S26 TX neck n3 muscles
S25 (MH "Thoracic Vertebrae")
S24 TX ondontoid* or TX cervical or TX occip* or TX atlant*
S23 (MH "Brachial Plexus+")
S22 (MH "Spinal Nerve Roots+")
S21 (MH "Atlanto‐Axial Joint") or (MH "Atlanto‐Occipital Joint")
S20 (MH "Cervical Vertebrae+") or (MH "Cervical Atlas")
S19 (MH "Cervical Plexus+")
S18 (MH "Neck")
S17 (MH "Neck Muscles+")
S16 S10 or S15
S15 S11 NOT S14
S14 S12 or S13
S13 (MM "Cervix") or (MM "Cervix Diseases")
S12 (MM "Genital Diseases, Female+")
S11(MH "Headache+") and TX cervic*
S10 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9
S9 (MH "Brachial Plexus Neuritis")
S8 TX cervical brachial neuralgia
S7 TX cervical rib sydrome* or TX cervico brachial neuralgia or TX cervicobrachial neuralgia or TX monoradicul* or TX monoradicl*
S6 (MH "Thoracic Outlet Syndrome") or (MH "Torticollis")
S5 TX brachial neuralgia or TX neck pain or TX neck injur* or TX brachial plexus neuropath* or TX brachial plexus neuralgia or TX brachial plexus neuritis
S4 TX cervicalgia or TX brachialgia or TX brachial neuritis
S3 TX cervical pain or TX neckache or TX neck ache or TX whiplash or TX cervicodynia
S2 (MH "Neck Injuries+")
S1 (MH "Neck Pain") or (MH "Brachial Plexus Neuropathies") or (MH "Brachial Plexus Neuritis")
MANTIS (Ovid)
Last update May 2014; librarian: Dela Shupe, Northwestern Health Science University
1 neck pain.mp. [mp=title, abstract, descriptors]
2 brachial plexus neuropathies.mp. [mp=title, abstract, descriptors]
3 neck injuries.mp. [mp=title, abstract, descriptors]
4 cervical pain.mp. [mp=title, abstract, descriptors]
5 neckache.mp. [mp=title, abstract, descriptors]
6 whiplash.mp. [mp=title, abstract, descriptors]
7 cervicodynia.mp. [mp=title, abstract, descriptors]
8 cervicalgia.mp. [mp=title, abstract, descriptors]
9 brachialgia.mp. [mp=title, abstract, descriptors]
10 brachial neuritis.mp. [mp=title, abstract, descriptors]
11 brachial neuralgia.mp. [mp=title, abstract, descriptors]
12 brachial plexus neuropath*.mp. [mp=title, abstract, descriptors]
13 brachial plexus neuritis.mp. [mp=title, abstract, descriptors]
14 (thoracic outlet syndrome or cervical rib syndrome).mp. [mp=title, abstract, descriptors]
15 torticollis.mp. [mp=title, abstract, descriptors]
16 cervico brachial neuralgia.mp. [mp=title, abstract, descriptors]
17 (monoradicul* or monoradicl*).tw.
18 or/1‐17
19 headache.mp. and cervic*.tw. [mp=title, abstract, descriptors]
20 genital diseases, female.mp. [mp=title, abstract, descriptors]
21 genital disease*.mp. [mp=title, abstract, descriptors]
22 or/20‐21
23 19 not 22
24 18 or 23
25 neck.mp. [mp=title, abstract, descriptors]
26 neck muscles.mp. [mp=title, abstract, descriptors]
27 cervical plexus.mp. [mp=title, abstract, descriptors]
28 cervical vertebrae.mp. [mp=title, abstract, descriptors]
29 atlanto‐axial joint.mp. [mp=title, abstract, descriptors]
30 atlanto‐occipital joint.mp. [mp=title, abstract, descriptors]
31 cervical atlas.mp. [mp=title, abstract, descriptors]
32 spinal nerve roots.mp. [mp=title, abstract, descriptors]
33 brachial plexus.mp. [mp=title, abstract, descriptors]
34 (odontoid* or cervical or occip* or atlant*).tw.
35 (axis or odontoid process).mp. [mp=title, abstract, descriptors]
36 thoracic vertebrae.mp. [mp=title, abstract, descriptors]
37 cervical vertebrae.mp. [mp=title, abstract, descriptors]
38 cervical plexus.mp. [mp=title, abstract, descriptors]
39 cervical spine.mp. [mp=title, abstract, descriptors]
40 (neck adj3 muscles).mp. [mp=title, abstract, descriptors]
41 (brachial adj3 plexus).mp. [mp=title, abstract, descriptors]
42 (thoracic adj3 vertebrae).mp. [mp=title, abstract, descriptors]
43 (thoracic adj3 spine).mp. [mp=title, abstract, descriptors]
44 (thoracic adj3 outlet).mp. [mp=title, abstract, descriptors]
45 trapezius.mp. [mp=title, abstract, descriptors]
46 cervical.mp. [mp=title, abstract, descriptors]
47 cervico*.mp. [mp=title, abstract, descriptors]
48 46 or 47
49 genital diseases, female.mp. [mp=title, abstract, descriptors]
50 genital disease*.mp. [mp=title, abstract, descriptors]
51 uterus.mp. [mp=title, abstract, descriptors]
52 49 or 50 or 51
53 48 not 52
54 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 53
55 pain.mp. [mp=title, abstract, descriptors]
56 injuries.mp. [mp=title, abstract, descriptors]
57 ache.mp. [mp=title, abstract, descriptors]
58 sore.mp. [mp=title, abstract, descriptors]
59 stiff.mp. [mp=title, abstract, descriptors]
60 discomfort.mp. [mp=title, abstract, descriptors]
61 injur*.mp. [mp=title, abstract, descriptors]
62 neuropath*.mp. [mp=title, abstract, descriptors]
63 or/55‐62
64 54 and 63
65 radiculopathy.mp. [mp=title, abstract, descriptors]
66 (temporomandibular joint disorders or temporomandibular joint dysfunction syndrome).mp. [mp=title, abstract, descriptors]
67 myofascial pain syndromes.mp. [mp=title, abstract, descriptors]
68 "sprains and strains".mp. [mp=title, abstract, descriptors]
69 spinal osteophytosis.mp. [mp=title, abstract, descriptors]
70 neuritis.mp. [mp=title, abstract, descriptors]
71 polyradiculopathy.mp. [mp=title, abstract, descriptors]
72 arthritis.mp. [mp=title, abstract, descriptors]
73 fibromyalgia.mp. [mp=title, abstract, descriptors]
74 (spondylitis or discitis).mp. [mp=title, abstract, descriptors]
75 (spondylosis or spondylolysis or spondylolisthesis).mp.,[mp=title, abstract, descriptors]
76 radiculitis.mp. [mp=title, abstract, descriptors]
77 tempomandibular.mp. [mp=title, abstract, descriptors]
78 myofascial pain syndrome*.mp. [mp=title, abstract, descriptors]
79 thoracic outlet syndrome*.mp. [mp=title, abstract, descriptors]
80 spinal osteophytosis.mp. [mp=title, abstract, descriptors]
81 neuritis.mp. [mp=title, abstract, descriptors]
82 spondylosis.mp. [mp=title, abstract, descriptors]
83 spondylitis.mp. [mp=title, abstract, descriptors]
84 spondylolisthesis.mp. [mp=title, abstract, descriptors]
85 or/65‐84
86 54 and 85
87 neck.mp. [mp=title, abstract, descriptors]
88 cervical vertebrae.mp. [mp=title, abstract, descriptors]
89 thoracic vertebrae.mp. [mp=title, abstract, descriptors]
90 (thoracic adj3 vertebrae).mp. [mp=title, abstract, descriptors]
91 cervical.mp. [mp=title, abstract, descriptors]
92 cervico*.mp. [mp=title, abstract, descriptors]
93 91 or 92
94 genital diseases, female.mp. [mp=title, abstract, descriptors]
95 genital disease*.mp. [mp=title, abstract, descriptors]
96 uterus.mp. [mp=title, abstract, descriptors]
97 or/94‐96
98 93 not 97
99 (thoracic adj3 spine).mp. [mp=title, abstract, descriptors]
100 cervical spine.mp. [mp=title, abstract, descriptors]
101 87 or 88 or 89 or 90 or 98 or 99 or 100
102 intervertebral disk.mp. [mp=title, abstract, descriptors]
103 (disc or discs).mp. [mp=title, abstract, descriptors]
104 (disk or disks).mp. [mp=title, abstract, descriptors]
105 102 or 103 or 104
106 101 and 105
107 herniat*.mp. [mp=title, abstract, descriptors]
108 slipped.mp. [mp=title, abstract, descriptors]
109 prolapse*.mp. [mp=title, abstract, descriptors]
110 displace*.mp. [mp=title, abstract, descriptors]
111 degenerat*.mp. [mp=title, abstract, descriptors]
112 (bulge or bulged or bulging).mp. [mp=title, abstract, descriptors]
113 107 or 108 or 109 or 110 or 111 or 112
114 106 and 113
115 intervertebral disk displacement.mp. [mp=title, abstract, descriptors]
116 intervertebral disc displacement.mp. [mp=title, abstract, descriptors]
117 intervertebral disk degeneration.mp. [mp=title, abstract, descriptors]
118 intervertebral disc degeneration.mp. [mp=title, abstract, descriptors]
119 115 or 116 or 117 or 118
120 101 and 119
121 24 or 64 or 86 or 106 or 114 or 120
122 (animals not (animals and humans)).mp. [mp=title, abstract, descriptors]
123 121 not 122
124 neoplasms.mp. [mp=title, abstract, descriptors]
125 wounds, penetrating.mp. [mp=title, abstract, descriptors]
126 124 or 125
127 123 not 126
128 rehabilitation.mp. [mp=title, abstract, descriptors]
129 therapy.mp. [mp=title, abstract, descriptors]
130 128 or 129
131 (neck pain or brachial plexus neuropathies or neck injuries or whiplash or thoracic outlet syndrome or cervical rib syndrome or torticollis
or brachial plexus neuritis).mp. [mp=title, abstract, descriptors]
132 (temporomandibular joint disorder or temporomandibular joint dysfunction syndrome).mp. [mp=title, abstract, descriptors]
133 (myofascial pain syndromes or "sprains and strains").mp. [mp=title, abstract, descriptors]
134 (radiculopathy or osteophytosis or neuritis or polyradiculopathy or arthritis or fibromyalgia or spondylitis or spondylosis or spondylolysis or spondylolisthesis).mp.
135 131 or 132 or 133 or 134
136 130 and 135
137 54 and 136
138 (acupuncture or chiropractic).mp. [mp=title, abstract, descriptors]
139 musculoskeletal manipulation*.mp. [mp=title, abstract, descriptors]
140 massage.mp. [mp=title, abstract, descriptors]
141 mobili?ation.mp. [mp=title, abstract, descriptors]
142 acupuncture therapy.mp. [mp=title, abstract, descriptors]
143 (acupuncture or acu‐puncture or needling or acupressure or mox?bustion).mp. [mp=title, abstract, descriptors]
144 ((neck or spine or spinal or cervical or chiropractic* or musculoskeletal*) adj3 (adjust* or manipulat* or mobiliz* or mobilis*)).mp. [mp=title, abstract, descriptors]
145 (manual adj therap*).mp. [mp=title, abstract, descriptors]
146 (manipulati* adj (therap* or medicine)).mp. [mp=title, abstract, descriptors]
147 (massag* or reflexolog* or rolfing or zone therap*).mp. [mp=title, abstract, descriptors]
148 Nimmo.mp. [mp=title, abstract, descriptors]
149 vibration therapy.mp. [mp=title, abstract, descriptors]
150 (vibration adj5 (therap* or treatment*)).mp. [mp=title, abstract, descriptors]
151 (ChihYa or Shiatsu or Shiatzu or ZhiYa).mp. [mp=title, abstract, descriptors]
152 (flexion adj2 distraction*).mp. [mp=title, abstract,descriptors]
153 (myofascial adj3 (release or therap*)).mp. [mp=title, abstract, descriptors]
154 muscle energy technique*.mp. [mp=title, abstract, descriptors]
155 trigger point.mp. [mp=title, abstract, descriptors]
156 proprioceptive neuromuscular facilitation*.mp. [mp=title, abstract, descriptors]
157 cyriax friction.mp. [mp=title, abstract, descriptors]
158 (lomilomi or lomi‐lomi or trager).mp. [mp=title, abstract, descriptors]
159 aston patterning.mp. [mp=title, abstract, descriptors]
160 (strain adj counterstrain).mp. [mp=title, abstract, descriptors]
161 (craniosacraltherap* or cranio‐sacral therap* or craniosacral therap*).mp. [mp=title, abstract, descriptors]
162 (amma or ammo or effleuurage or effleurage or petrissage or hacking or tapotment).mp. [mp=title, abstract, descriptors]
163 complementary therapies.mp. [mp=title, abstract, descriptors]
164 ((complement* or alternat* or osteopathic*) adj (therap* or medicine)).mp. [mp=title, abstract, descriptors]
165 (Tui Na or Tuina).mp. [mp=title, abstract, descriptors]
166 or/138‐165
167 127 and 166
168 136 or 137 or 167
169 (animals not (animals and humans)).mp. [mp=title, abstract, descriptors]
170 168 not 169
171 randomized controlled trial*.mp. [mp=title, abstract, descriptors]
172 controlled clinical trial*.mp. [mp=title, abstract, descriptors]
173 (random* or sham or placebo*).mp. [mp=title, abstract, descriptors]
174 placebos.mp. [mp=title, abstract, descriptors]
175 random allocation.mp. [mp=title, abstract, descriptors]
176 single blind method.mp. [mp=title, abstract, descriptors]
177 double blind method.mp. [mp=title, abstract, descriptors]
178 ((singl* or doubl* or trebl* or tripl*) adj25 (blind* or dumm* or mask*)).mp. [mp=title, abstract, descriptors]
179 (rct or rcts).mp. [mp=title, abstract, descriptors]
180 (control* adj2 (study or studies or trial*)).mp. [mp=title, abstract, descriptors]
181 or/171‐180
182 170 and 181
183 (guideline* or practice guideline*).mp. [mp=title, abstract, descriptors]
184 (guideline* or guidance* or recommendation*).ti.
185 consensus.ti.
186 183 or 184 or 185
187 170 and 186
188 meta‐analysis.mp. [mp=title, abstract, descriptors]
189 (metaanaly* or meta analy* or met analy* or metanaly*).mp. [mp=title, abstract, descriptors]
190 (collaborative research or collaborative review* or collaborative overview*).mp. [mp=title, abstract, descriptors]
191 (integrative research or integrative review* or integrative overview*).mp. [mp=title, abstract, descriptors]
192 (quantitative adj3 (research or review* or overview*)).mp. [mp=title, abstract, descriptors]
193 (research integration or research overview*).mp. [mp=title, abstract, descriptors]
194 (systematic* adj3 (review* or overview*)).mp. [mp=title, abstract, descriptors]
195 (methodologic* adj3 (review* or overview*)).mp. [mp=title, abstract, descriptors]
196 technology assessment biomedical.mp. [mp=title, abstract, descriptors]
197 (hta or thas or technology assessment*).mp. [mp=title, abstract, descriptors]
198 ((hand adj2 search*) or (manual* adj search*)).mp. [mp=title, abstract, descriptors]
199 ((electronic adj database*) or (bibliographic* adj database*)).mp. [mp=title, abstract, descriptors]
200 ((data adj2 abstract*) or (data adj2 extract*)).mp. [mp=title, abstract, descriptors]
201 (analys* adj3 (pool or pooled or pooling)).mp. [mp=title, abstract, descriptors]
202 mantel haenszel.mp. [mp=title, abstract, descriptors]
203 (cochrane or pubmed or pub med or medline or embase or psycinfo or psyclit or psychinfo or psychlit or cinahl or science citation index).ab.
204 or/188‐203
205 170 and 204
206 182 or 187 or 205 (
207 limit 206 to yr="2009 ‐Current"
Index to chiropractic literature
Jan 10 2014; Librarian: Dela Shupe, Northwestern Health Science University
S1 Subject: "BACK PAIN" OR "BACK INJURIES" OR "NECK INJURIES" OR "NECK PAIN" OR "SPINAL DISEASES" OR "SPINAL INJURIES" OR "SCIATICA" OR All Fields:backpain* or backache* OR "back pain" OR "back ache" OR "back pains" OR "back aches" OR neckpain* OR neckache* OR "neck pain" OR neck ache" OR "neck pains" OR "neck aches" OR All Fields:Spondylolys* or spondylolisthes* or Spondylisthes* or Discitis or diskitis or Spondylod* OR Sciatica OR ischialgia* OR cervicalgia OR Cervicodynia
S2 All Fields:whiplash* or "whip lash" OR "whip lashes" or radiculomyelopath* or "radiculo‐myelopathy" OR "radiculo‐myelopathies" OR All Fields:"failed back" or "back surgery syndrome" or "back surgery syndromes" or FBSS OR All Fields:lumbago or dorsalgia or "myofascial pain" OR "myofascial ache"
S3 All Fields:"cervical pain" OR "cervical ache" OR "vertebrogenic pain syndrome" OR "vertebrogenic pain syndromes" OR All Fields:"degenerated disk" OR "degenerative disk" OR "degenerated disks" OR "degenerative disks" OR All Fields:"degenerated disc" OR "degenerative disc OR "degenerated discs" OR "degenerative discs"
S4 All Fields:"prolapsed disk" OR "prolapsed disks" OR "prolapsed disc" OR "prolapsed discs" OR "disk prolapse" OR "disc prolapse" "herniated disk" OR "herniated disks" OR "herniated disc" OR "herniated discs" OR All Fields:"displaced disk" OR "displaced disks" OR "displaced disc" OR "displaced discs" OR "osteoporotic compression fracture" OR "osteoporotic compression fractures" OR All Fields::"lumbar stenosis" OR "lumbar stenoses" OR "spinal stenosis" OR "spinal stenoses" OR "cervicogenic headache" OR "cervicogenic headaches" OR "cervico‐genic headache" OR "cervico‐genic headaches"
S5 All Fields:radiculomyelopathy OR radiculomyelopathies OR "radiculo‐myelopathy" OR "radiculo‐myelopathies" OR All Fields:"Zygapophyseal joint syndrome" OR "Zygapophyseal joint syndromes" OR "Z‐joint syndrome" OR "Z‐joint syndromes" OR "facet joint syndrome" OR "facet joint syndromes" OR All Fields:"thoracic pain" OR "thoracic ache" OR "spinal pain" OR "spinal ache" OR "lumbar pain" OR "lumbar ache"
S6 S1 OR S2 OR S3 OR S4 OR S5
S7 Subject:"ACUPUNCTURE" OR "ACUPRESSURE" OR "ACUPUNCTURE THERAPY" OR "ELECTROACUPUNCTURE" OR "MANIPULATION, LUMBAR" OR "MANIPULATION, CERVICAL" OR "MANIPULATION, CHIROPRACTIC" OR "MANIPULATION, SPINAL" OR "MANIPULATION, THORACIC" OR Subject:"MASSAGE" OR "CHIROPRACTIC" OR All Fields:acupuncture or "acu‐puncture" or electroacupuncture or "electro‐acupuncture" or "electric acupuncture" or "electric acu‐puncture" or needling or acupressure or "acu‐pressure" or moxibustion or moxabustion
S8 All Fields:"manual therapy" OR "manual therapies" OR massag* or reflexolog* or rolfing or "zone therapy" or "zone therapies" OR All Fields:"Chih Ya" or Shiatsu or Shiatzu or "Zhi Ya" or "Flexion distraction" OR "Trigger point" OR "Trigger points" OR "Proprioceptive Neuromuscular Facilitation" OR "Proprioceptive Neuromuscular Facilitations" OR All Fields:"myofascial release" or "myofascial therapy" OR "myofascial therapies" OR "Muscle energy technique" OR "Muscle energy techniques" OR "Cyriax Friction"
S9 All Fields:: Lomilomi or "lomi‐lomi" or trager or "Aston patterning" or "Strain counterstrain" or "Alexander technique" or "Alexander techniques" or "Tui Na" or Tuina OR All Fields:Craniosacral Therapy" or "Craniosacral Therapies" or "Cranio‐sacral Therapy"or "Cranio‐sacral Therapies" or amma or ammo or Effleurage or Petrissage or hacking or Tapotment OR All Fields:manipulat* or mobiliz* or mobilis*
S10 All Fields:"complementary therapy" OR "complementary therapies" OR "complementary medicine" OR All Fields:"alternative therapy" OR "alternative therapies" OR "alternative medicine" OR All Fields:"osteopathic therapy" OR "osteopathic therapies" OR "osteopathic medicine"
S11 S7 OR S8 OR S9 OR S10
S12 S6 AND S11
S13 , Publication Type:Randomized Controlled Trial
S14 Subject:"RANDOMIZED CONTROLLED TRIALS AS TOPIC" OR "CONTROLLED CLINICAL TRIALS" OR "PLACEBOS" OR All Fields:random* or sham or placebo* or RCT or RCTs or CCT or CCTs OR All Fields:"controlled clinical trial" or "controlled clinical trials" or "controlled study" or "controlled studies" or "control study" or "controlled studies"
S15 S12 AND S14
S16 S13 OR S15
Appendix 2. Criteria for a judgement of yes for sources of risk of bias
1. Was the method of randomisation adequate?
Was a random (unpredictable) assignment sequence used? Examples of adequate methods are coin toss (for studies with two groups), rolling a dice (for studies with two or more groups), drawing of balls of different colours, drawing of ballots with study group labels from a dark bag, computer‐generated random sequence, pre‐ordered sealed envelopes, sequentially ordered vials, telephone call to a central office and pre‐ordered list of treatment assignments.
Examples of inadequate methods include alternation, birth date, social insurance/security number, date on which individuals are invited to participate in the study and hospital registration number.
2. Was treatment allocation concealed?
Was assignment generated by an independent person not responsible for determining the eligibility of individuals. This person has no information about persons included in the trial and has no influence on the assignment sequence nor on the decision about eligibility of patients for participation.
Was knowledge of the allocated interventions adequately prevented during the study?
3. Was the participant blinded to the intervention?
This item should be scored “yes” if index and control groups are indistinguishable for participants, or if blinding was tested among participants and was found to be successful.
4. Was the care provider blinded to the intervention?
This item should be scored “yes” if index and control groups are indistinguishable for care providers, or if blinding was tested among care providers and was found to be successful
5. Was the outcome assessor blinded to the intervention?
Adequacy of blinding should be assessed for primary outcomes. This item should be scored “yes” if blinding was tested among outcome assessors and was found to be successful or:
-
for patient‐reported outcomes for which the participant is the outcome assessor (e.g. pain, disability): The blinding procedure is adequate for outcome assessors if participant blinding is scored “yes”;
-
for outcome criteria assessed during scheduled visits that suppose a contact between participants and outcome assessors (e.g. clinical examination): The blinding procedure is adequate if participants are blinded, and if treatment or adverse effects of treatment cannot be noticed during clinical examination;
-
for outcome criteria that do not suppose a contact with participants (e.g. radiography, magnetic resonance imaging): The blinding procedure is adequate if treatment or adverse effects of treatment cannot be noticed when the main outcome is assessed;
-
for outcome criteria that are clinical or therapeutic events that will be determined by the interaction between participants and care providers (e.g. co‐interventions, hospitalization length, treatment failure), in which the care provider is the outcome assessor: The blinding procedure is adequate for outcome assessors if the item for care providers is scored “yes”; and
-
for outcome criteria that are assessed from data of the medical forms: The blinding procedure is adequate if treatment or adverse effects of treatment cannot be noticed in extracted data.
Were incomplete outcome data adequately addressed?
6. Was the dropout rate described and acceptable?
The number of participants who were included in the study but did not complete the observation period or were not included in the analysis must be described and reasons given. If the percentage of withdrawals and dropouts does not exceed 20% for short‐term follow‐up, and 30% for long‐term follow‐up, and does not lead to substantial bias, a 'yes' is scored. (N.B. These percentages are arbitrary and are not supported by the literature.)
7. Were all randomly assigned participants analysed in the group to which they were allocated?
All randomly assigned participants are reported/analysed in the group to which they were allocated by randomisation for the most important moments of effect measurement (minus missing values), irrespective of non‐compliance and co‐interventions.
8. Are reports of the study free of the suggestion of selective outcome reporting?
To assign a ‘yes’, the review author determines if all results from all pre‐specified outcomes have been adequately reported in the published report of the trial. This information can be obtained by comparing the protocol versus the report or, in the absence of the protocol, by assessing whether the published report includes enough information to permit this judgement.
Other sources of potential bias
9. Were the groups similar at baseline regarding the most important prognostic indicators?
To receive a “yes”, groups have to be similar at baseline regarding demographic factors, duration and severity of complaints, percentage of participants with neurological symptoms and value of main outcome measure(s).
10. Were co‐interventions avoided or similar?
This item should be scored “yes” if no co‐interventions were provided, or if they were similar between index and control groups.
11. Was compliance acceptable in all groups?
The review author determines whether compliance with the interventions is acceptable, based on reported intensity, duration, number and frequency of sessions for both index interventions and control interventions. For example, physiotherapy treatment is usually administered over several sessions; therefore it is necessary to assess how many sessions each participant attended. For single‐session interventions (e.g. surgery), this item is irrelevant.
12. Was timing of the outcome assessment similar in all groups?
Timing of outcome assessment should be identical for all intervention groups and for all important outcome assessments.
Note: These instructions are adapted from van Tulder 2003 and from the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Appendix 3. Data imputation rules
The preliminary assumption made for imputation of missing values is that data were missing completely at random (Little 1987). In other words, it was assumed that data were not missing as the result of factors confounded by the treatment effect.
As information was available only on change scores:
-
change score treatment (T) is the difference between follow‐up treatment pain score (mFT) and baseline treatment pain score (mBT); and
-
change score control (C) is the difference between follow‐up control pain score (mFC) and pre‐baseline control pain score (mBC).
|
| Baseline | Follow‐up | Difference |
| Treatment | mBT | mFT | T = mFT ‐ mBT |
| Control | mBC | mFC | C = mFC ‐ mBC |
|
| EB = mBT ‐ mBC | EF = mFT ‐ mFC | E = T ‐ C |
If EB = 0, then EF is equal to E.
The mean difference was calculated with the assumption that no baseline differences in scores were present (EB = 00). For the conversion, the mean postscore difference was assumed to be due to differences in postscore values (EF), and then equals the post‐follow‐up difference (E).
Appendix 4. Grading the quality of evidence ‐ definition of domains
Study design refers to type of study (i.e. randomised, observational study).
Limitations in design (quality) refers to the 12 risk of bias criteria noted in Appendix 2.
Consistency refers to similarity of results across studies. When all studies are included in the meta‐analysis, ‘consistency’ is defined as absence of statistical heterogeneity. In the case that not all studies are combined in a meta‐analysis, ‘consistency’ is defined when all studies for the specific outcome lead to the same decision or recommendation, and ‘inconsistency’ is present if the results of two or more studies lead to clinically different decisions or recommendations. Review authors use their judgement to decide whether inconsistency is present when only one study leads to clinically different decisions or recommendations.
Directness (generalisability) refers to the extent to which the people, interventions and outcome measures are similar to those of interest.
Precision of the evidence relates to the numbers of studies, participants and events considered for each outcome. Imprecise data are defined as:
-
only one study for an outcome, regardless of the sample size or the confidence interval;
-
multiple studies combined in a meta‐analysis: The confidence interval is sufficiently wide that the estimate is consistent with conflicting recommendations. For rare events, one should consider the confidence interval around the risk difference rather than the confidence interval around the relative risk; and
-
multiple studies not combined in a meta‐analysis: The total sample size is underpowered to detect a clinically important difference between those who received the index intervention compared with those who received the control intervention. In this case, a post hoc sample size calculation should be performed to determine adequate sample size for each outcome.
Reporting (publication) bias should be considered present only if actual evidence of reporting bias rather than only speculation about reporting bias is found. The Cochrane Reporting Bias Methods Group describes the following types of reporting bias and definitions.
-
Publication bias: publication or non‐publication of research findings, depending on the nature and direction of results.
-
Time lag bias: rapid or delayed publication of research findings, depending on the nature and direction of results.
-
Language bias: publication of research findings in a particular language, depending on the nature and direction of results.
-
Funding bias: reporting of research findings, depending on how results align with the aspirations of the funding body.
-
Outcome variable selection bias: selective reporting of some outcomes but not others, depending on the nature and direction of research findings.
-
Developed country biases: non‐publication or non‐indication of findings, depending on whether study authors were based in developed or developing countries.
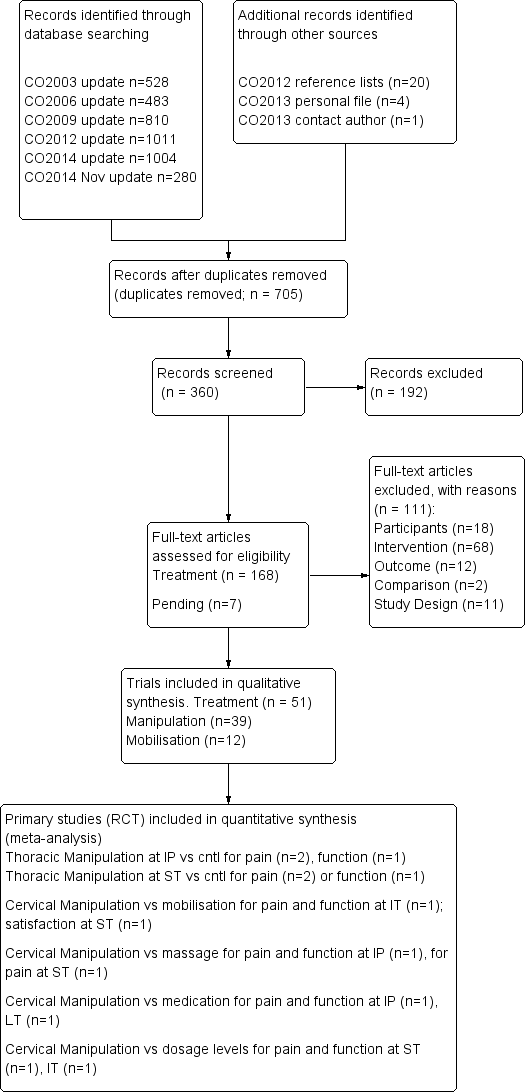
PRISMA diagram for manipulation and mobilisation.

Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
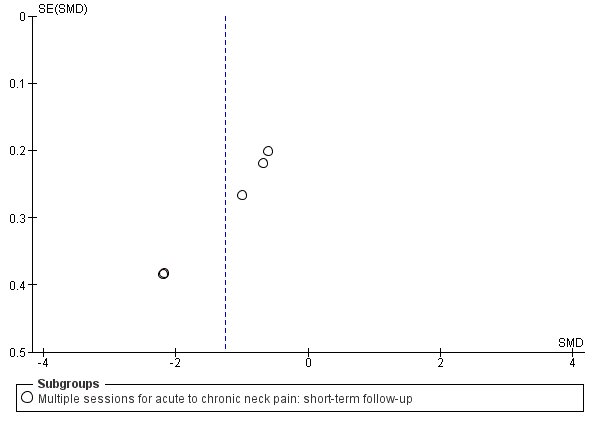
Funnel plot of comparison: manipulation vs control, outcome: FUNNEL PLOT for PAIN: thoracic manipulation vs same treatment in both arms.

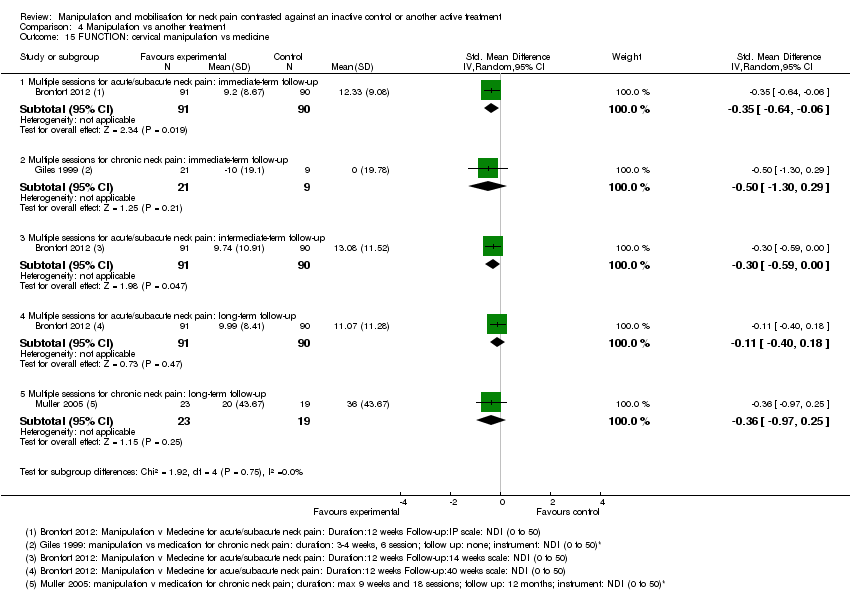
Forest plot of comparison: manipulation vs another treatment, outcome: PAIN: cervical manipulation vs medicine.

Forest plot of comparison: manipulation vs another treatment, outcome: PAIN: cervical manipulation vs mobilisation at intermediate‐term follow‐up.

Comparison 1 Manipulation versus placebo, Outcome 1 PAIN: cervical manipulation vs placebo.

Comparison 1 Manipulation versus placebo, Outcome 2 PAIN: thoracic manipulation vs placebo.
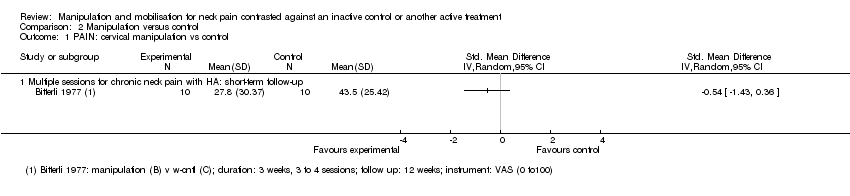
Comparison 2 Manipulation versus control, Outcome 1 PAIN: cervical manipulation vs control.

Comparison 2 Manipulation versus control, Outcome 2 PAIN: cervical manipulation plus treatment vs same treatment in both arms.

Comparison 2 Manipulation versus control, Outcome 3 PAIN: cervical manipulation vs same treatment in both arms.

Comparison 2 Manipulation versus control, Outcome 4 PAIN: thoracic manipulation vs control.

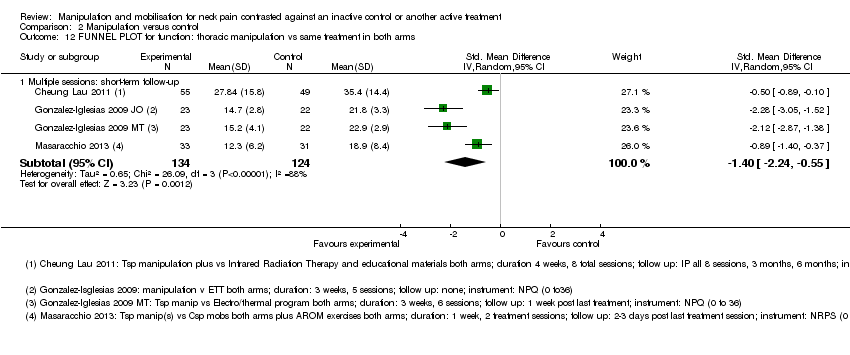
Comparison 2 Manipulation versus control, Outcome 5 PAIN: thoracic manipulation vs same treatment in both arms.
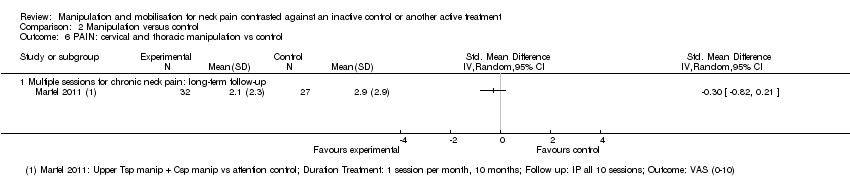
Comparison 2 Manipulation versus control, Outcome 6 PAIN: cervical and thoracic manipulation vs control.

Comparison 2 Manipulation versus control, Outcome 7 FUNCTION: thoracic manipulation vs same treatment in both arms.
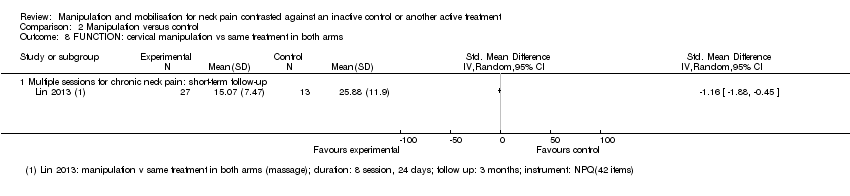
Comparison 2 Manipulation versus control, Outcome 8 FUNCTION: cervical manipulation vs same treatment in both arms.

Comparison 2 Manipulation versus control, Outcome 9 FUNCTION: cervical and thoracic manipulation vs control.

Comparison 2 Manipulation versus control, Outcome 10 QUALITY OF LIFE: thoracic manipulation vs control.

Comparison 2 Manipulation versus control, Outcome 11 FUNNEL PLOT for pain: thoracic manipulation vs same treatment in both arms.
Comparison 2 Manipulation versus control, Outcome 12 FUNNEL PLOT for function: thoracic manipulation vs same treatment in both arms.

Comparison 3 Mobilisation versus control, Outcome 1 PAIN: cervical mobilisation vs control.
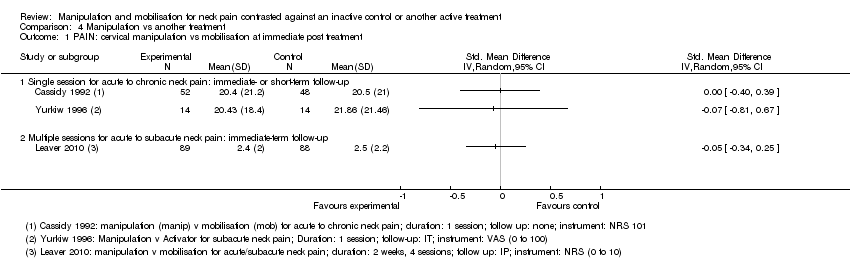
Comparison 4 Manipulation vs another treatment, Outcome 1 PAIN: cervical manipulation vs mobilisation at immediate post treatment.

Comparison 4 Manipulation vs another treatment, Outcome 2 PAIN: cervical manipulation vs mobilisation at intermediate‐term follow‐up.
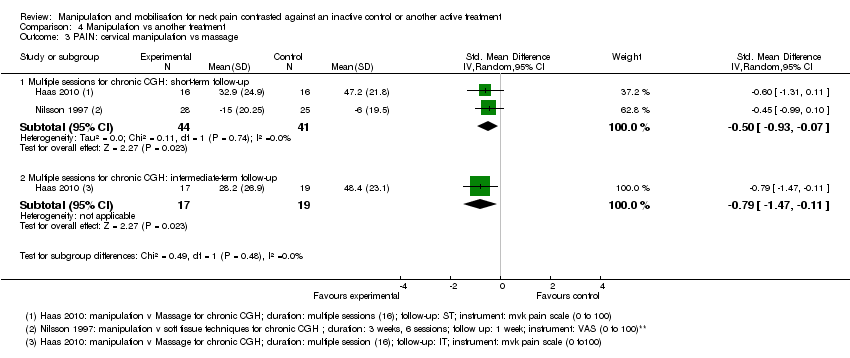
Comparison 4 Manipulation vs another treatment, Outcome 3 PAIN: cervical manipulation vs massage.

Comparison 4 Manipulation vs another treatment, Outcome 4 PAIN: cervical manipulation vs medicine.

Comparison 4 Manipulation vs another treatment, Outcome 5 PAIN: cervical manipulation vs exercise.

Comparison 4 Manipulation vs another treatment, Outcome 6 PAIN: cervical manipulation vs electrotherapy.
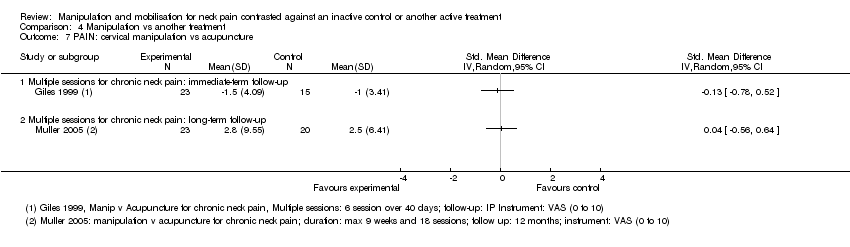
Comparison 4 Manipulation vs another treatment, Outcome 7 PAIN: cervical manipulation vs acupuncture.
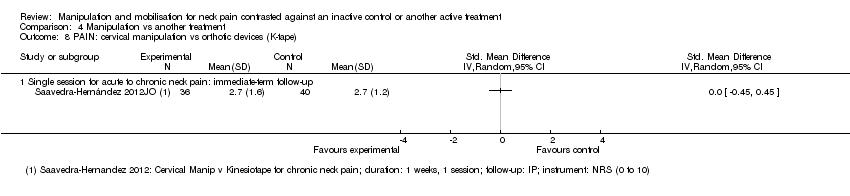
Comparison 4 Manipulation vs another treatment, Outcome 8 PAIN: cervical manipulation vs orthotic devices (K‐tape).
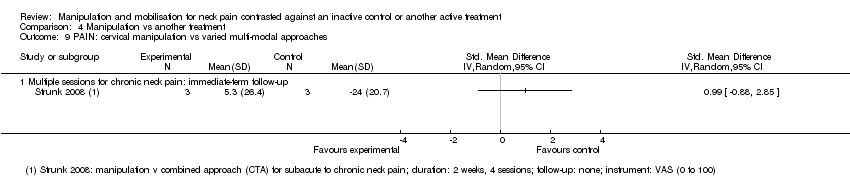
Comparison 4 Manipulation vs another treatment, Outcome 9 PAIN: cervical manipulation vs varied multi‐modal approaches.
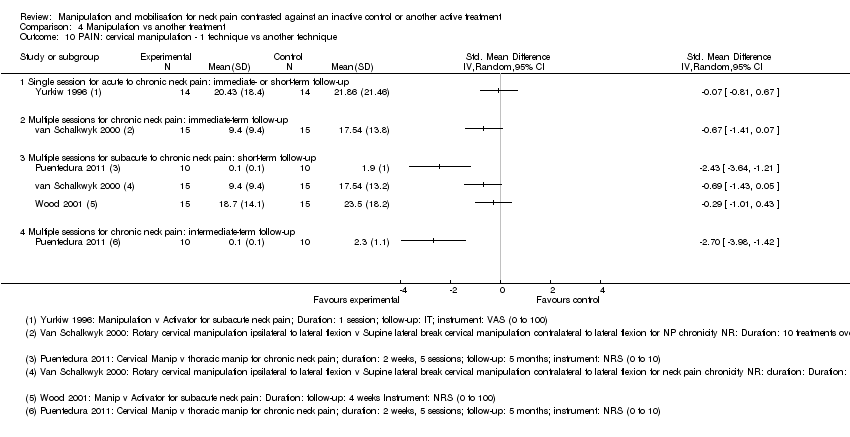
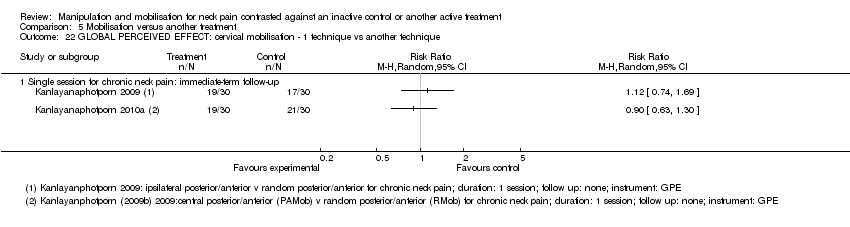
Comparison 4 Manipulation vs another treatment, Outcome 10 PAIN: cervical manipulation ‐ 1 technique vs another technique.
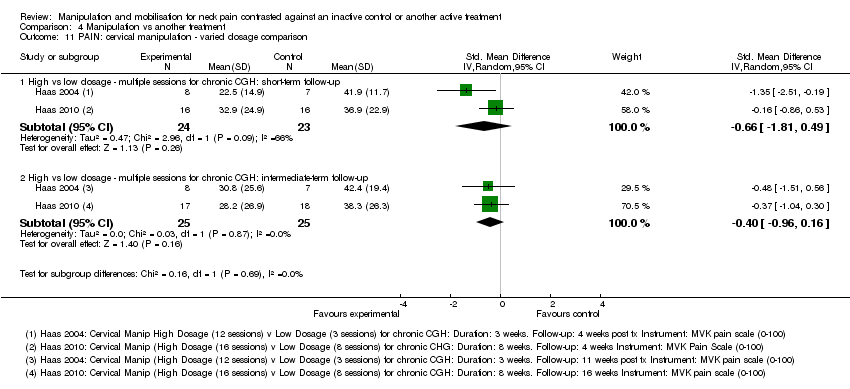
Comparison 4 Manipulation vs another treatment, Outcome 11 PAIN: cervical manipulation ‐ varied dosage comparison.

Comparison 4 Manipulation vs another treatment, Outcome 12 PAIN: thoracic manipulation vs exercise.

Comparison 4 Manipulation vs another treatment, Outcome 13 FUNCTION: cervical manipulation vs mobilisation.
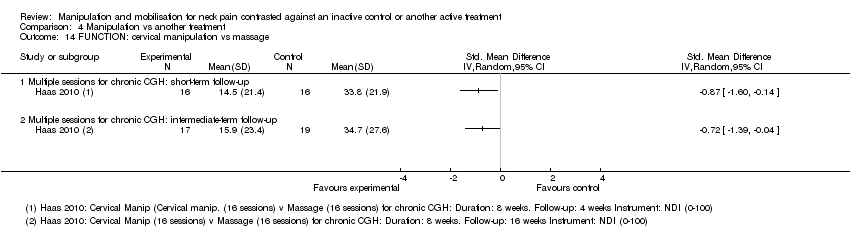
Comparison 4 Manipulation vs another treatment, Outcome 14 FUNCTION: cervical manipulation vs massage.
Comparison 4 Manipulation vs another treatment, Outcome 15 FUNCTION: cervical manipulation vs medicine.

Comparison 4 Manipulation vs another treatment, Outcome 16 FUNCTION: cervical manipulation vs exercise.

Comparison 4 Manipulation vs another treatment, Outcome 17 FUNCTION: cervical manipulation vs orthotic devices (K‐taping).

Comparison 4 Manipulation vs another treatment, Outcome 18 FUNCTION: cervical manipulation vs acupuncture.

Comparison 4 Manipulation vs another treatment, Outcome 19 FUNCTION: cervical manipulation vs varied multi‐modal approaches.

Comparison 4 Manipulation vs another treatment, Outcome 20 FUNCTION: cervical manipulation ‐ 1 technique vs another technique.

Comparison 4 Manipulation vs another treatment, Outcome 21 FUNCTION: cervical manipulation ‐ varied dosage comparison.
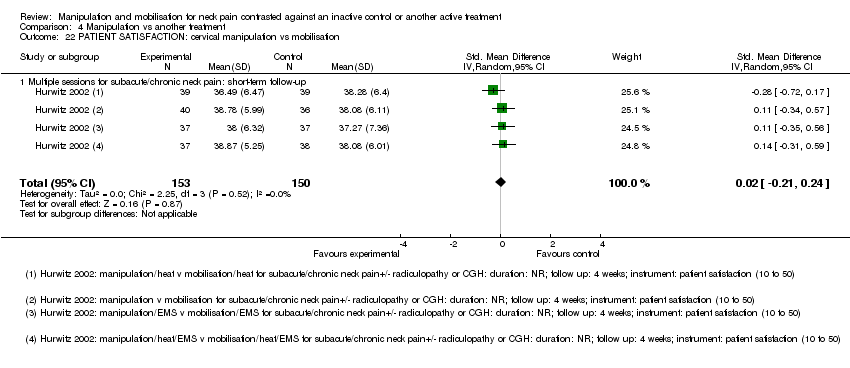
Comparison 4 Manipulation vs another treatment, Outcome 22 PATIENT SATISFACTION: cervical manipulation vs mobilisation.

Comparison 4 Manipulation vs another treatment, Outcome 23 PATIENT SATISFACTION: cervical manipulation vs varied multi‐modal approaches.
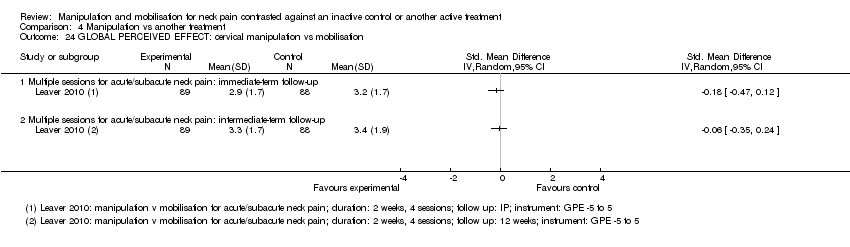
Comparison 4 Manipulation vs another treatment, Outcome 24 GLOBAL PERCEIVED EFFECT: cervical manipulation vs mobilisation.
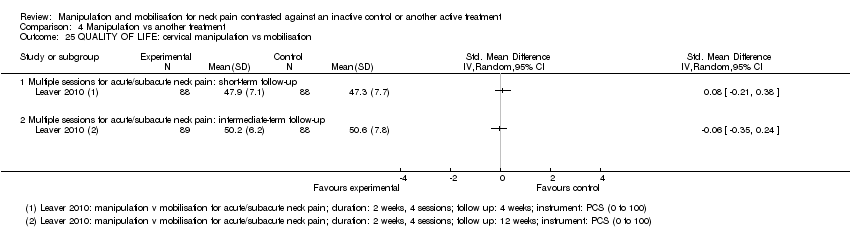
Comparison 4 Manipulation vs another treatment, Outcome 25 QUALITY OF LIFE: cervical manipulation vs mobilisation.

Comparison 4 Manipulation vs another treatment, Outcome 26 QUALITY OF LIFE: cervical manipulation vs medicine.

Comparison 4 Manipulation vs another treatment, Outcome 27 QUALITY OF LIFE: cervical manipulation vs exercise.
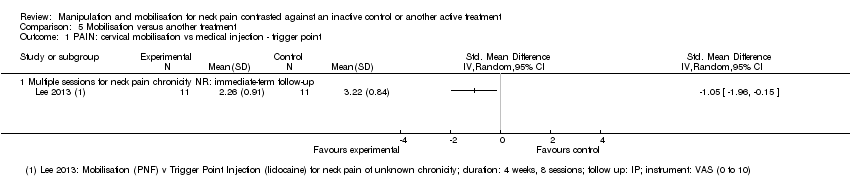
Comparison 5 Mobilisation versus another treatment, Outcome 1 PAIN: cervical mobilisation vs medical injection ‐ trigger point.
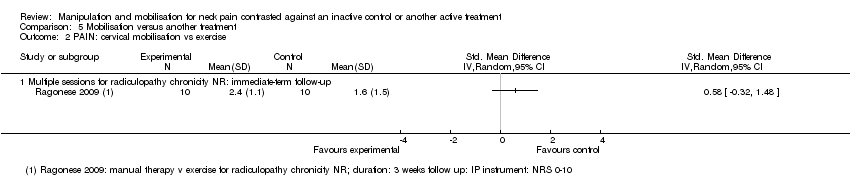
Comparison 5 Mobilisation versus another treatment, Outcome 2 PAIN: cervical mobilisation vs exercise.
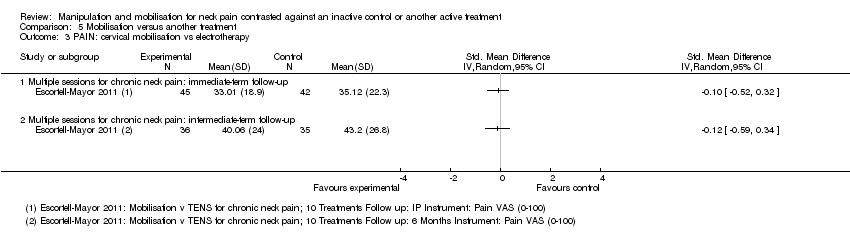
Comparison 5 Mobilisation versus another treatment, Outcome 3 PAIN: cervical mobilisation vs electrotherapy.

Comparison 5 Mobilisation versus another treatment, Outcome 4 PAIN: cervical mobilisation vs sonic devices ‐ ultrasound, shock wave therapy.

Comparison 5 Mobilisation versus another treatment, Outcome 5 PAIN: cervical mobilisation vs mechanical traction.

Comparison 5 Mobilisation versus another treatment, Outcome 6 PAIN: cervical mobilisation vs acupuncture.

Comparison 5 Mobilisation versus another treatment, Outcome 7 PAIN: cervical mobilisation vs varied multi‐modal approaches.

Comparison 5 Mobilisation versus another treatment, Outcome 8 PAIN: cervical mobilisation ‐ 1 technique vs another technique.

Comparison 5 Mobilisation versus another treatment, Outcome 9 PAIN: cervical mobilisation ‐ 1 technique vs another technique.

Comparison 5 Mobilisation versus another treatment, Outcome 10 PAIN: cervical mobilisation vs massage.

Comparison 5 Mobilisation versus another treatment, Outcome 11 FUNCTION: cervical mobilisation vs medical injection ‐ trigger point.

Comparison 5 Mobilisation versus another treatment, Outcome 12 FUNCTION: cervical mobilisation vs exercise.
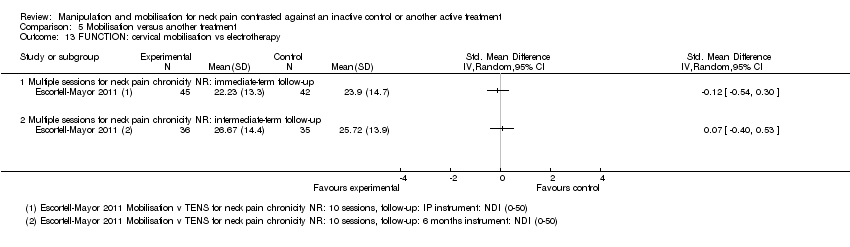
Comparison 5 Mobilisation versus another treatment, Outcome 13 FUNCTION: cervical mobilisation vs electrotherapy.

Comparison 5 Mobilisation versus another treatment, Outcome 14 FUNCTION: cervical mobilisation vs sonic devices ‐ shock wave therapy.

Comparison 5 Mobilisation versus another treatment, Outcome 15 FUNCTION: cervical mobilisation vs acupuncture.

Comparison 5 Mobilisation versus another treatment, Outcome 16 FUNCTION: cervical mobilisation vs varied multi‐modal approaches.

Comparison 5 Mobilisation versus another treatment, Outcome 17 FUNCTION: cervical mobilisation vs massage.

Comparison 5 Mobilisation versus another treatment, Outcome 18 FUNCTION: cervical mobilisation ‐ 1 technique vs another technique.
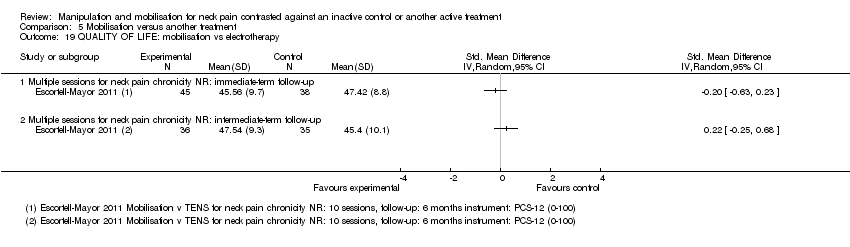
Comparison 5 Mobilisation versus another treatment, Outcome 19 QUALITY OF LIFE: mobilisation vs electrotherapy.

Comparison 5 Mobilisation versus another treatment, Outcome 20 PATIENT SATISFACTION: cervical mobilisation vs varied multi‐modal approaches.
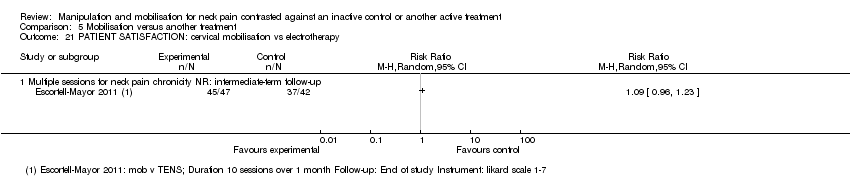
Comparison 5 Mobilisation versus another treatment, Outcome 21 PATIENT SATISFACTION: cervical mobilisation vs electrotherapy.
Comparison 5 Mobilisation versus another treatment, Outcome 22 GLOBAL PERCEIVED EFFECT: cervical mobilisation ‐ 1 technique vs another technique.
| Manipulation (cervical) compared with oral medicine for acute/subacute neck pain | ||||
| Patient or population: patients with acute and subacute neck pain Settings: outpatient clinics, ambulatory care services Intervention: manipulation of cervical region ‐ multiple sessions Comparison: oral medicine ‐ varied combinations of non‐steroidal anti‐inflammatory drugs (NSAIDs), analgesics, opioid analgesics and muscle relaxants | ||||
| Outcomes | Relative effect | Number of participants | Quality of the evidence | Comments |
| PAIN | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD ‐0.21 (‐0.5 to 0.08) | 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Acute and subacute neck pain Long‐term follow‐up | SMD ‐0.32 (‐0.61 to ‐0.02) | 181 | ⊕⊕⊕⊝ Moderatea | Pain reduction favouring manipulation over medication |
| FUNCTION | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD ‐0.30 (‐0.59 to ‐0.00) | 182 | ⊕⊕⊕⊝ Moderatea | Functional improvement favouring manipulation over medication |
| Acute and subacute neck pain Long‐term follow‐up | SMD ‐0.11 (‐0.40 to 0.18)
| 181 | ⊕⊕⊕⊝ Moderatea | No significant difference between groups |
| PARTICIPANT SATISFACTION | ||||
| Acute and subacute neck pain Long‐term follow‐up | Not estimable | 182 | ⊕⊕⊕⊝ Moderatea | Manipulation favoured over medication |
| QUALITY OF LIFE | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD 0.22 (‐0.07 to 0.51) | 181 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Acute and subacute neck pain Long‐term follow‐up | SMD: 0.19 (‐0.10 to 0.49) | 181 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Moderate‐quality evidence suggests that multiple sessions of cervical manipulation are more effective than medication (analgesics and non‐steroidal anti‐inflammatory drugs (NSAIDs)) for improving pain at immediate‐term and long‐term follow‐up (1 trial; 181 participants); function at intermediate term and satisfaction over the long term. Quality of life was similar between groups (1 trial, 182 participants) at intermediate‐ and long‐term follow‐up. | ||||
| GRADE Working Group grades of evidence. | ||||
| aIndirectness: ‐1; a second independent trial is needed to clarify emerging data. | ||||
| Manipulation (thoracic) compared with inactive control for neck pain | ||||
| Patient or population: patients with acute, subacute and chronic neck pain Settings: outpatient clinics, ambulatory care services Intervention: manipulation of thoracic region ‐ multiple sessions Comparison: inactive control | ||||
| Outcomes | Relative effect | Number of participants | Quality of the evidence | Comments |
| PAIN | ||||
| Acute and subacute neck pain Short‐term follow‐up | SMD pooled ‐1.46 (‐2.20 to ‐0.71) | 242 Fernandez 2004 JWRD; Fernandez 2009; Gonzalez‐Iglesias 2009 JO; | ⊕⊕⊕⊝ Moderatea | Favoured treatment; NNTB: 4 to 7; magnitude of effect: medium |
| Chronic neck pain Intermediate‐term follow‐up | SMD ‐0.64 (‐1.04 to ‐0.25) | 111 | ⊕⊕⊝⊝ Lowb,c | Favoured treatment; NNTB 4; magnitude of effect: small |
| FUNCTION | ||||
| Acute and subacute neck pain Short‐term follow‐up | SMD pooled ‐1.73 (‐2.68 to ‐0.78) | 258 | ⊕⊕⊕⊝ Moderatea | Favoured treatment; NNTB 4 to 5; magnitude of effect: medium |
| Chronic neck pain Short‐term follow‐up | SMD ‐0.50 (‐0.89 to ‐0.10) | 111 | ⊕⊕⊝⊝ Lowb,c | Favoured treatment; NNTB 5; magnitude of effect: small |
| Chronic neck pain Intermediate‐term follow‐up | SMD ‐0.38 (‐0.77 to 0.01) | 111 (1 trial; Cheung Lau 2011) | ⊕⊕⊝⊝ Lowb,c | Favoured treatment; NNTB 5; magnitude of effect: small |
| QUALITY OF LIFE (QoL) | ||||
| Chronic neck pain Short‐term follow‐up | SMD ‐0.82 (‐1.23 to ‐0.42) | 111 | ⊕⊕⊝⊝ Lowb,c | Favoured treatment |
| Chronic neck pain Intermediate‐term follow‐up | SMD ‐0.61 (‐1.01 to ‐0.22) | 111 | ⊕⊕⊝⊝ Lowc | Favoured treatment |
| Seven trials (428 participants) using multiple sessions of thoracic manipulation for acute to chronic neck pain were assessed at 3 time intervals. At short‐term follow‐up, moderate‐quality evidence favoured thoracic manipulation for pain reduction among participants with acute/subacute neck pain, and with acute to chronic neck pain, it improved function. These findings were consistent but small at intermediate follow‐up for pain, function and quality of life (low‐quality evidence). | ||||
| GRADE Working Group grades of evidence. | ||||
| bIndirectness: ‐1, immediate post‐treatment data have limited clinical relevance; single trials with only immediate‐ and short‐term follow‐up are downgraded (ceiling effect) because future research is likely to have an important impact on the direction of the reported effect, and a second independent trial is needed to clarify emerging short‐term data. cImprecision: ‐1, small sample size. aInconsistency: P value = 0.002; I² = 84%; sensitivity analysis: Statistical differences led us to explore heterogeneity by the following PICO factors: P: about the same; I: about the same; C: about the same; O: for pain, VAS, NPRS; for disability, NPQ, NDI; RoB: most often low RoB but when the trial of high RoB is removed, pooled SMD increases to ‐2.18 (‐2.71 to ‐1.65) for pain, but these data were derived from trials conducted in the same lab. | ||||
| Manipulation compared with mobilisation for neck pain | ||||
| Patient or population: patients with acute, subacute and chronic neck pain Settings: ambulatory care or outpatient clinic Intervention: manipulation of cervical region ‐ multiple sessions Comparison: mobilisation | ||||
| Outcomes | Relative effect | Number of participants | Quality of the evidence | Comments |
| PAIN | ||||
| Acute, subacute and chronic neck pain Intermediate‐term follow‐up | MD pooled ‐0.07 (‐0.72 to 0.59) | 446 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| FUNCTION AND DISABILITY | ||||
| Acute and subacute neck pain Short‐term follow‐up | SMD: ‐0.06 (‐0.35 to 0.24) | 176 | ⊕⊕⊕⊝ Moderateb | No significant differences between groups |
| Acute, subacute and chronic neck pain Intermediate‐term follow‐up | SMD pooled: 0.10 (‐0.18 to 0.37)
| 446 | ⊕⊕⊕⊕ High | No significant differences between groups |
| PARTICIPANT SATISFACTION | ||||
| Subacute and chronic neck pain Short‐term follow‐up | SMD: ‐0.02 (‐0.21 to 0.24) | 269 | ⊕⊕⊕⊝ Moderateb | No significant differences between groups |
| GLOBAL PERCEIVED EFFECT | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD: ‐0.06 | 177 | ⊕⊕⊕⊝ Moderateb | No significant differences between groups |
| QUALITY OF LIFE | ||||
| Acute and subacute neck pain Short‐term follow‐up | SMD: 0.08 (‐0.21 to 0.38) | 176 | ⊕⊕⊕⊝ Moderateb | No significant differences between groups |
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD: ‐0.06 (‐0.35 to 0.24) | 177 | ⊕⊕⊕⊝ Moderateb | No significant differences between groups |
| Moderate‐ to high‐quality evidence (2 trials, 446 participants) suggests that multiple sessions of cervical manipulation produced similar changes in pain, function, quality of life, global perceived effect and patient satisfaction when compared with multiple sessions of cervical mobilisation at immediate‐, short‐ and intermediate‐term follow‐up. | ||||
| GRADE Working Group grades of evidence. | ||||
| aInconsistency: ‐1. bIndirectness: ‐1. | ||||
| Manipulation compared with exercise for neck pain | ||||
| Patient or population: patients with acute and subacute neck pain Settings: ambulatory care or outpatient clinic setting Intervention: manipulation of cervical region Comparison: exercise | ||||
| Outcomes | Relative effect | Number of participants | Quality of the evidence | Comments |
| PAIN | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD: ‐0.16 (‐0.45 to 0.13) | 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Acute and subacute neck pain Long‐term follow‐up | SMD: 0.06 (‐0.23 to 0.35) | 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| FUNCTION | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD: ‐0.01 (‐0.30 to 0.28)
| 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Acute and subacute neck pain Long‐term follow‐up | SMD: ‐0.02 (‐0.31 to 0.27)
| 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| PARTICIPANT SATISFACTION | ||||
| Acute and subacute neck pain Long‐term follow‐up | Not estimable | 182 | ⊕⊕⊕⊝ Moderatea | Improvement in participant satisfaction for manipulation over exercise |
| GLOBAL PERCEIVED EFFECT | ||||
| Acute and subacute neck pain Immediate post‐treatment follow‐up | Not estimable | 182 (1 trial; Bronfort 2012) | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| QUALITY OF LIFE | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD: ‐0.05 (‐0.35 to 0.24) | 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Acute and subacute neck pain Long‐term follow‐up | SMD: 0.0 (‐0.29 to 0.29) | 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Moderate‐quality evidence suggests no differences in pain, function, global perceived effect and quality of life when multiple sessions of cervical manipulation are compared with exercise at immediate‐, intermediate‐ and long‐term follow‐up. Moderate‐quality evidence indicates that use of cervical manipulation led to greater participant satisfaction when compared with an exercise programme at long‐term follow‐up. | ||||
| GRADE Working Group grades of evidence. | ||||
| aIndirectness: ‐1. | ||||
| High dose of manipulation compared with low dose of manipulation for chronic neck pain | ||||
| Patient or population: patients with chronic neck pain with cervicogenic headache (CGH) Settings: ambulatory care or outpatient clinic setting Intervention: manipulation of cervical region Comparison: high dose vs low dose | ||||
| Outcomes | Relative effect | Number of participants | Quality of the evidence | Comments |
| PAIN | ||||
| Chronic neck pain and CGH Intermediate‐term follow‐up | SMD pooled: ‐0.40 (‐0.96 to 0.16)
| ⊕⊕⊕⊝ Moderatea | Two trials showed no significant differences between groups | |
| FUNCTION | ||||
| Chronic neck pain and CGH Intermediate‐term follow‐up | SMD pooled: ‐0.61 (‐1.38 to 0.17) | ⊕⊕⊕⊝ Moderatea | Two trials showed no significant differences between groups | |
| Moderate‐quality evidence shows that high‐dose (12 to 18 sessions) contrasted against low‐dose (3 to 8 sessions) cervical manipulation produced similar changes in pain and function at intermediate‐term follow‐up for individuals with chronic neck pain with cervicogenic headache. | ||||
| GRADE Working Group grades of evidence. | ||||
| aImprecision: ‐1. | ||||
| Term | Definiton |
| Per cent treatment advantage (%) | Calculation of the clinically important difference or change in a per cent scale was estimated as follows. Karlberg 1996 data are used in this example. % improvement (control) equals the difference between the change in the control group (1) divided by the control baseline (56), which equals 1.8%. Treatment advantage = 42.6% ‐ 1.8% = 40.8% |
| Number needed to treat (NNTB) | For this example, Karlberg 1996 outcomes measured at short‐term follow‐up are used to derive the data. Number needed to treat is the number of patients a clinician needs to treat to achieve a clinically important improvement in 1. If we assume the minimal clinically important difference to be 10% of the baseline mean in the control group, and the control group mean at baseline is 56, then 10% of 56 is 5.6 The effect is baseline ‐ final value; therefore:
Converting these to standard normal values means that:
NNTB = 1 divided by the difference in areas under the normal curve (experimental group ‐ control group):
|
| Author/Comparison | NNTB | Advantage, % |
| PAIN | ||
| Haas 2004: pain | 12 (clinically important pain reduction) at ST | 23 |
| Haas 2010: pain | 4 (clinically important pain reduction) at IT | 29 |
| Cleland 2005 | 5 (clinically important pain reduction) | 29 |
| Cheung Lau 2011: pain | 4 (clinically important pain reduction) | |
| Fernandez 2004a | Unable to calculate because baseline data not reported | |
| Gonzalez‐Iglesias 2009 | 7 (clinically important pain reduction) | 47 |
| Martinez‐Segura 2006, | 2 (clinically important pain reduction) | 54 |
| Massaracchio 2013: pain | 4 (clinically important pain reduction) | |
| von Piekartz 2011: pain | 2 (clinically important pain reduction) at IT | |
| FUNCTION | ||
| Cheung Lau 2011: function | 5 (clinically important functional improvement) at IT | |
| Gonzalez‐Iglesias 2009 | 5 (clinically important functional improvement) | 41 |
| Haas 2010: function | 5 (clinically important functional improvement) at ST and IT | ST: 41 IT: 39 |
| Massaracchio 2013: function | 4 (clinically important functional improvement) | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 PAIN: cervical manipulation vs placebo Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Single session: immediate‐ or short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 PAIN: thoracic manipulation vs placebo Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Single session: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 PAIN: cervical manipulation vs control Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Multiple sessions for chronic neck pain with HA: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 PAIN: cervical manipulation plus treatment vs same treatment in both arms Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Single session for subacute/chronic neck pain: immediate‐ or short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Multiple sessions for subacute/chronic neck pain: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 PAIN: cervical manipulation vs same treatment in both arms Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3.1 Single session for subacute/chronic neck pain with radicular findings and HA: short‐term follow‐up | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 PAIN: thoracic manipulation vs control Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 Single session for neck pain of not reported duration: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 PAIN: thoracic manipulation vs same treatment in both arms Show forest plot | 8 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5.1 Multiple sessions for acute neck pain: immediate‐term follow‐up | 2 | 90 | Std. Mean Difference (IV, Random, 95% CI) | ‐3.46 [‐4.13, ‐2.79] |
| 5.2 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 2 | 141 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.23 [‐1.15, 0.69] |
| 5.3 Single session for chronic neck pain: short‐term follow‐up | 1 | 82 | Std. Mean Difference (IV, Random, 95% CI) | 0.08 [‐0.36, 0.51] |
| 5.4 Multiple sessions for acute/subacute neck pain: short‐term follow‐up | 4 | 242 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.46 [‐2.20, ‐0.71] |
| 5.5 Multiple sessions for chronic neck pain: short‐term follow‐up | 1 | 104 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.60 [‐0.99, ‐0.20] |
| 5.6 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | 103 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.64 [‐1.04, ‐0.25] |
| 6 PAIN: cervical and thoracic manipulation vs control Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Multiple sessions for chronic neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 FUNCTION: thoracic manipulation vs same treatment in both arms Show forest plot | 6 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 7.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 2 | 141 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.52 [‐0.85, ‐0.18] |
| 7.2 Single session for chronic neck pain: short‐term follow‐up | 1 | 81 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.61, 0.27] |
| 7.3 Multiple sessions for acute neck pain: short‐term follow‐up | 3 | 154 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.73 [‐2.68, ‐0.78] |
| 7.4 Multiple sessions for chronic neck pain: short‐term follow‐up | 1 | 104 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.50 [‐0.89, ‐0.10] |
| 7.5 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | 103 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.38 [‐0.77, 0.01] |
| 8 FUNCTION: cervical manipulation vs same treatment in both arms Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 Multiple sessions for chronic neck pain: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 FUNCTION: cervical and thoracic manipulation vs control Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 9.1 Multiple sessions for chronic neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 QUALITY OF LIFE: thoracic manipulation vs control Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 10.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 Multiple sessions for chronic neck pain: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 FUNNEL PLOT for pain: thoracic manipulation vs same treatment in both arms Show forest plot | 5 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 11.1 Multiple sessions for acute to chronic neck pain: short‐term follow‐up | 5 | 346 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.26 [‐1.86, ‐0.66] |
| 12 FUNNEL PLOT for function: thoracic manipulation vs same treatment in both arms Show forest plot | 4 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 12.1 Multiple sessions: short‐term follow‐up | 4 | 258 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.40 [‐2.24, ‐0.55] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 PAIN: cervical mobilisation vs control Show forest plot | 2 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Single session: intermediate post treatment | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Multiple sessions: short‐term follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 PAIN: cervical manipulation vs mobilisation at immediate post treatment Show forest plot | 3 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Single session for acute to chronic neck pain: immediate‐ or short‐term follow‐up | 2 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Multiple sessions for acute to subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 PAIN: cervical manipulation vs mobilisation at intermediate‐term follow‐up Show forest plot | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 Multiple sessions for acute to chronic neck pain: intermediate‐term follow‐up | 2 | 446 | Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐0.72, 0.59] |
| 3 PAIN: cervical manipulation vs massage Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 Multiple sessions for chronic CGH: short‐term follow‐up | 2 | 85 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.50 [‐0.93, ‐0.07] |
| 3.2 Multiple sessions for chronic CGH: intermediate‐term follow‐up | 1 | 36 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.79 [‐1.47, ‐0.11] |
| 4 PAIN: cervical manipulation vs medicine Show forest plot | 3 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 Multiple sessions for acute/subacute neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.4 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.5 Multiple sessions for chronic neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 PAIN: cervical manipulation vs exercise Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.3 Multiple sessions for acute/subacute neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 PAIN: cervical manipulation vs electrotherapy Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Multiple sessions for subacute to chronic CGH: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 Multiple sessions for subacute to chronic neck pain: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 PAIN: cervical manipulation vs acupuncture Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 Multiple sessions for chronic neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 PAIN: cervical manipulation vs orthotic devices (K‐tape) Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 Single session for acute to chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 PAIN: cervical manipulation vs varied multi‐modal approaches Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 9.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 PAIN: cervical manipulation ‐ 1 technique vs another technique Show forest plot | 4 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 10.1 Single session for acute to chronic neck pain: immediate‐ or short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 Multiple sessions for subacute to chronic neck pain: short‐term follow‐up | 3 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.4 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 PAIN: cervical manipulation ‐ varied dosage comparison Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 11.1 High vs low dosage ‐ multiple sessions for chronic CGH: short‐term follow‐up | 2 | 47 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.66 [‐1.81, 0.49] |
| 11.2 High vs low dosage ‐ multiple sessions for chronic CGH: intermediate‐term follow‐up | 2 | 50 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.40 [‐0.96, 0.16] |
| 12 PAIN: thoracic manipulation vs exercise Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 12.1 Multiple sessions for neck pain chronicity NR: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 FUNCTION: cervical manipulation vs mobilisation Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 13.1 Multiple sessions for acute/subacute neck pain: short‐term follow‐up | 1 | 176 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.06 [‐0.35, 0.24] |
| 13.2 Multiple sessions for acute to chronic neck pain: intermediate‐term follow‐up | 2 | 445 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.01 [‐0.21, 0.18] |
| 14 FUNCTION: cervical manipulation vs massage Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 14.1 Multiple sessions for chronic CGH: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.2 Multiple sessions for chronic CGH: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 FUNCTION: cervical manipulation vs medicine Show forest plot | 3 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 15.1 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | 181 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.35 [‐0.64, ‐0.06] |
| 15.2 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | 30 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.50 [‐1.30, 0.29] |
| 15.3 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | 181 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.30 [‐0.59, ‐0.00] |
| 15.4 Multiple sessions for acute/subacute neck pain: long‐term follow‐up | 1 | 181 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.11 [‐0.40, 0.18] |
| 15.5 Multiple sessions for chronic neck pain: long‐term follow‐up | 1 | 42 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.36 [‐0.97, 0.25] |
| 16 FUNCTION: cervical manipulation vs exercise Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 16.1 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.2 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.3 Multiple sessions for acute/subacute neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17 FUNCTION: cervical manipulation vs orthotic devices (K‐taping) Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 17.1 Single session for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18 FUNCTION: cervical manipulation vs acupuncture Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 18.1 Multiple sessions for subacute/chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.2 Multiple sessions for chronic neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19 FUNCTION: cervical manipulation vs varied multi‐modal approaches Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 19.1 Multiple sessions for subacute/chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.2 Multiple sessions for subacute/chronic neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20 FUNCTION: cervical manipulation ‐ 1 technique vs another technique Show forest plot | 3 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 20.1 Multiple sessions for subacute/chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.2 Multiple sessions for acute/subacute neck pain: short‐term follow‐up | 2 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.3 Multiple sessions for neck pain chronicity NR: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.4 Multiple sessions for acute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21 FUNCTION: cervical manipulation ‐ varied dosage comparison Show forest plot | 2 | 97 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.61 [‐1.09, ‐0.14] |
| 21.1 High vs low dosage ‐ multiple sessions for chronic CGH: short‐term follow‐up | 2 | 47 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.75 [‐1.71, 0.22] |
| 21.2 High vs low dosage ‐ multiple sessions for chronic CGH: intermediate‐term follow‐up | 2 | 50 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.61 [‐1.38, 0.17] |
| 22 PATIENT SATISFACTION: cervical manipulation vs mobilisation Show forest plot | 1 | 303 | Std. Mean Difference (IV, Random, 95% CI) | 0.02 [‐0.21, 0.24] |
| 22.1 Multiple sessions for subacute/chronic neck pain: short‐term follow‐up | 1 | 303 | Std. Mean Difference (IV, Random, 95% CI) | 0.02 [‐0.21, 0.24] |
| 23 PATIENT SATISFACTION: cervical manipulation vs varied multi‐modal approaches Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 23.1 Multiple sessions for subacute/chronic neck pain: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 24 GLOBAL PERCEIVED EFFECT: cervical manipulation vs mobilisation Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 24.1 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 24.2 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 25 QUALITY OF LIFE: cervical manipulation vs mobilisation Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 25.1 Multiple sessions for acute/subacute neck pain: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 25.2 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26 QUALITY OF LIFE: cervical manipulation vs medicine Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 26.1 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.2 Multiple sessions for acute/subacute neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27 QUALITY OF LIFE: cervical manipulation vs exercise Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 27.1 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27.2 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27.3 Multiple sessions for acute/subacute neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 PAIN: cervical mobilisation vs medical injection ‐ trigger point Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 PAIN: cervical mobilisation vs exercise Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Multiple sessions for radiculopathy chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 PAIN: cervical mobilisation vs electrotherapy Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 PAIN: cervical mobilisation vs sonic devices ‐ ultrasound, shock wave therapy Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 Single session for subacute/chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 PAIN: cervical mobilisation vs mechanical traction Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 PAIN: cervical mobilisation vs acupuncture Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 PAIN: cervical mobilisation vs varied multi‐modal approaches Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 Multiple sessions for subacute/chronic neck pain ± radiculopathy or CGH: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 PAIN: cervical mobilisation ‐ 1 technique vs another technique Show forest plot | 5 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 Single session for chronic neck pain: immediate‐term follow‐up | 2 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 Single session for chronic neck pain ± radiculopathy: immediate‐term follow‐up | 2 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.3 Multiple sessions for chronic CGH: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.4 Multiple sessions for chronic CGH: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 PAIN: cervical mobilisation ‐ 1 technique vs another technique Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 9.1 PA vs other mobilisation for acute/subacute neck pain: multiple sessions: immediate‐term follow‐up | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.2 AP vs other mobilisation: multiple sessions: immediate‐term follow‐up | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 PAIN: cervical mobilisation vs massage Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 10.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 2 | 58 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.56 [‐4.15, 1.03] |
| 10.2 Multiple sessions for chronic CGH: immediate‐term follow‐up | 1 | 36 | Std. Mean Difference (IV, Random, 95% CI) | ‐2.89 [‐3.85, ‐1.93] |
| 11 FUNCTION: cervical mobilisation vs medical injection ‐ trigger point Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 11.1 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12 FUNCTION: cervical mobilisation vs exercise Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 12.1 Multiple sessions for radiculopathy: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 FUNCTION: cervical mobilisation vs electrotherapy Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 13.1 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.2 Multiple sessions for neck pain chronicity NR: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14 FUNCTION: cervical mobilisation vs sonic devices ‐ shock wave therapy Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 14.1 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.2 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 FUNCTION: cervical mobilisation vs acupuncture Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 15.1 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16 FUNCTION: cervical mobilisation vs varied multi‐modal approaches Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 16.1 Multiple sessions for subacute/chronic neck pain ± radiculopathy or CGH: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17 FUNCTION: cervical mobilisation vs massage Show forest plot | 2 | 59 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.03 [‐0.90, 0.84] |
| 17.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | 23 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.52 [‐1.35, 0.32] |
| 17.2 Multiple sessions for subacute/chronic CGH: immediate‐term follow‐up | 1 | 36 | Std. Mean Difference (IV, Random, 95% CI) | 0.38 [‐0.28, 1.04] |
| 18 FUNCTION: cervical mobilisation ‐ 1 technique vs another technique Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 18.1 Multiple sessions for chronic CGH: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.2 Multiple sessions for chronic CGH: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19 QUALITY OF LIFE: mobilisation vs electrotherapy Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 19.1 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.2 Multiple sessions for neck pain chronicity NR: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20 PATIENT SATISFACTION: cervical mobilisation vs varied multi‐modal approaches Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 20.1 Multiple sessions for subacute/chronic neck pain ± radiculopathy or CGH: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21 PATIENT SATISFACTION: cervical mobilisation vs electrotherapy Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 21.1 Multiple sessions for neck pain chronicity NR: intermediate‐term follow‐up | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22 GLOBAL PERCEIVED EFFECT: cervical mobilisation ‐ 1 technique vs another technique Show forest plot | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 22.1 Single session for chronic neck pain: immediate‐term follow‐up | 2 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |