Intervenciones terapéuticas con música para los pacientes con demencia
Resumen
Antecedentes
La demencia es un síndrome clínico con algunas causas diferentes que se caracteriza por el deterioro en las funciones cognitivas, conductuales, sociales y emocionales. Se dispone de intervenciones farmacológicas, pero su capacidad es limitada para el tratamiento de muchas de las características del síndrome. Ha habido menos investigación dirigida a los tratamientos no farmacológicos. En esta revisión, se examinó la evidencia sobre los efectos de las intervenciones con música.
Objetivos
Evaluar los efectos de las intervenciones terapéuticas con música para los pacientes con demencia sobre el bienestar emocional incluida la calidad de vida, el trastorno del estado de ánimo o el afecto negativo, los problemas conductuales, el comportamiento social y la cognición al final del tratamiento y cuatro semanas o más después del final del tratamiento.
Métodos de búsqueda
Se hicieron búsquedas en ALOIS, el registro especializado del Grupo Cochrane de Demencia y Trastornos Cognitivos (Specialized Register of the Cochrane Dementia and Cognitive Improvement Group, CDCIG) el 19 junio 2017, utilizando los términos: music therapy, music, singing, sing, auditory stimulation. También se hicieron búsquedas adicionales el 19 julio 2017 en las principales bases de datos de atención sanitaria MEDLINE, Embase, PsycINFO, CINAHL y LILACS; y en registros de ensayos y fuentes de literatura gris.
Criterios de selección
Se incluyeron ensayos controlados aleatorios de las intervenciones terapéuticas con música (al menos cinco sesiones) para los pacientes con demencia que medían cualquiera de los resultados de interés. Los grupos control recibieron atención habitual u otras actividades con o sin música.
Obtención y análisis de los datos
Dos autores de la revisión trabajaron, de forma independiente, para seleccionar los estudios recuperados en cuanto a los criterios de inclusión y luego para extraer los datos y evaluar la calidad metodológica de los estudios incluidos. Cuando fue necesario, se estableció contacto con los autores de los ensayos para obtener datos adicionales, incluidas las subescalas relevantes o para obtener otra información faltante. Se agruparon los datos con el modelo de efectos aleatorios.
Resultados principales
Se incluyeron 22 estudios con 1097 participantes asignados al azar. Veintiún estudios con 890 participantes aportaron datos a los metanálisis. Los participantes de los estudios presentaban demencia en grados variables de gravedad y todos residían en instituciones. Siete estudios administraron una intervención con música individual; los otros estudios administraron la intervención a grupos de participantes. La mayoría de las intervenciones incluyó elementos musicales tanto activos como receptivos. La calidad metodológica de los estudios varió. Todos estuvieron en alto riesgo de sesgo de realización y algunos estuvieron en alto riesgo de sesgo de detección u otros sesgos.
Al final del tratamiento, se encontró evidencia de baja calidad de que las intervenciones pueden mejorar el bienestar emocional y la calidad de vida (diferencia de medias estandarizada [DME] 0,32; intervalo de confianza [IC] del 95%: 0,02 a 0,62; nueve estudios, 348 participantes) y reducir la ansiedad (DME ‐0,43; IC del 95%: ‐0,72 a ‐0,14; 13 estudios, 478 participantes). Se encontró evidencia de baja calidad de que las intervenciones terapéuticas con música pueden tener poco o ningún efecto sobre la cognición (DME 0,15; IC de 95%: ‐0,06 a 0,36; siete estudios, 350 participantes). Hubo evidencia de calidad moderada de que las intervenciones reducen los síntomas depresivos (DME ‐0,27; IC del 95%: ‐0,45 a ‐0,09; 11 estudios, 503 participantes) y los problemas de conducta generales (DME ‐0,23; IC del 95%: ‐0,46 a ‐0,01; 10 estudios, 442 participantes), pero no disminuyen la agitación ni la agresividad (DME ‐0,07; IC del 95%: ‐0,24 a 0,10; 14 estudios, 626 participantes). La calidad de la evidencia sobre el comportamiento social fue muy baja, de manera que los efectos fueron muy inciertos.
La evidencia en cuanto a los resultados a largo plazo medidos a las cuatro semanas o más después del final del tratamiento fue de muy baja calidad para la ansiedad y el comportamiento social, y para los otros resultados, fue de baja calidad para poco o ningún efecto (con DME pequeñas, entre 0,03 y 0,34).
Conclusiones de los autores
La administración a los pacientes con demencia que reciben asistencia institucional de al menos cinco sesiones de una intervención terapéutica con música probablemente reduce los síntomas depresivos y mejora los problemas conductuales en general al final del tratamiento. También puede mejorar el bienestar emocional y la calidad de vida y reducir la ansiedad, pero puede tener poco o ningún efecto sobre la agitación o la agresión o en la cognición. No existe seguridad acerca de los efectos sobre el comportamiento social ni los efectos a largo plazo. Los estudios futuros deben examinar la duración de los efectos con relación a la duración general del tratamiento y el número de sesiones.
PICOs
Resumen en términos sencillos
Intervenciones terapéuticas con música para los pacientes con demencia
Antecedentes
Los pacientes con demencia desarrollan gradualmente dificultades con la memoria, el pensamiento, el lenguaje y las actividades diarias. La demencia a menudo se asocia con problemas emocionales y conductuales y puede disminuir la calidad de vida del paciente. En los estadios posteriores de la demencia puede ser difícil para los pacientes comunicarse con palabras, pero incluso cuando ya no puedan hablar todavía podrían ser capaces de tararear o jugar con música. Por lo tanto, el tratamiento con música puede ser especialmente apropiado para los pacientes con demencia. Los musicoterapeutas están especialmente calificados para trabajar con individuos o grupos de pacientes, y utilizan la música para tratar de ayudar a satisfacer sus necesidades físicas, psicológicas y sociales. Otros profesionales también pueden ser entrenados para proporcionar tratamientos similares.
Propósito de esta revisión
Se deseaba observar si era posible encontrar evidencia de que los tratamientos basados en música mejoran el bienestar emocional y la calidad de vida de los pacientes con demencia. También había interés en la evidencia acerca de los efectos sobre los problemas emocionales, conductuales, sociales y cognitivos (p.ej. pensamiento y recuerdo) en pacientes con demencia.
Lo realizado
Se realizaron búsquedas de ensayos clínicos que midieron estos efectos y en los cuales los pacientes con demencia se asignaron al azar a una terapia con música o a un grupo de comparación. Los grupos de comparación podrían no haber recibido tratamiento especial o podrían haber ofrecido una actividad diferente. Se requirieron al menos cinco sesiones de tratamiento debido a que se creyó que era poco probable que menos de cinco sesiones tuvieran mucho efecto. Se combinaron los resultados de los ensayos para calcular el efecto del tratamiento con la mayor exactitud posible. La evidencia está actualizada hasta el 19 de junio de 2017.
Datos encontrados
Se encontraron 22 ensayos para incluir en la revisión y fue posible combinar los resultados de al menos 890 pacientes. Todos los pacientes de los ensayos se encontraban en hogares para convalecientes u hospitales. Algunos ensayos compararon terapias con música versus atención habitual, y algunos las compararon con otras actividades, como cocinar o pintar. Se observó variación en cuanto a la calidad de los ensayos y si el informe era adecuado, lo cual afectó la confianza en los resultados. Primero, se consideraron los resultados inmediatamente luego de un ciclo terapéutico concluido. A partir de los resultados, podría existir una seguridad moderada en cuanto a que las terapias con música mejoran los síntomas de depresión y los problemas conductuales en general, pero no específicamente el comportamiento agitado o agresivo. También pueden mejorar la ansiedad y el bienestar emocional incluida la calidad de vida, aunque hubo menos confianza en cuanto a estos resultados. Puede haber poco o ningún efecto sobre la cognición. Hubo muy poca confianza en los resultados de la interacción social. Algunos estudios también consideraron si había efectos duraderos cuatro semanas o más después del tratamiento. Sin embargo, hubo pocos datos y poca o ninguna seguridad acerca de los resultados. Es probable que los ensayos adicionales tengan una repercusión significativa sobre lo que se conoce acerca de los efectos de las terapias con música para los pacientes con demencia, por lo cual es importante continuar la investigación.
Conclusiones de los autores
Summary of findings
| Music‐based therapeutic interventions compared to usual care or other activities for people with dementia: end‐of‐treatment effects | |||
| Patient or population: people with dementia (all resided in institutional settings) | |||
| Outcomes (end of treatment) measured with a variety of scales except for social behaviour | Anticipated absolute effects, SMD* (95% CI) | № of participants | Quality of the evidence |
| Score with music therapy compared with usual care or other activities | |||
| Emotional well‐being including quality of life | The score in the intervention group was 0.32 SDs higher | 348 | ⊕⊕⊝⊝ |
| Mood disturbance or negative affect: depression | The score in the intervention group was 0.27 SDs lower | 503 | ⊕⊕⊕⊝ |
| Mood disturbance or negative affect: anxiety | The score in the intervention group was 0.43 SDs lower | 478 | ⊕⊕⊝⊝ |
| Behavioural problems: agitation or aggression | The score in the intervention group was 0.07 SDs lower | 626 | ⊕⊕⊕⊝ |
| Behavioural problems: overall | The score in the intervention group was 0.23 SDs lower | 442 | ⊕⊕⊕⊝ |
| Social behaviour: music vs other activities | The score in the intervention group was 0.54 SDs higher | 70 | ⊕⊝⊝⊝ |
| Cognition | The score in the intervention group was 0.15 SDs higher | 350 | ⊕⊕⊝⊝ |
| *Interpretation of SMD: a difference of < 0.40 SDs can be regarded as a small effect, 0.40–0.70 a moderate effect, and > 0.70 a large effect. CI: confidence interval; SMD: standardised mean difference; SD: standard deviation. | |||
| GRADE Working Group grades of evidence (GradePro) | |||
| aRisk of bias: no blinding of therapists and participants (not possible), and often no or unclear blinding of outcome assessment. bImprecision: small number of participants and broad CI. cRisk of bias: no blinding of therapists and participants (not possible), and sometimes no or unclear blinding of outcome assessment. dInconsistency: more non‐overlapping CIs. eImprecision: very small number of participants and broad CIs. fImprecision: small number of participants. | |||
| Music‐based therapeutic interventions compared to usual care or other activities for people with dementia: long‐term effects (scores 4 weeks or more after treatment ended) | |||
| Patient or population: people with dementia (all resided in institutional settings) | |||
| Outcomes (long‐term) measured with a variety of scales except for social behaviour | Anticipated absolute effects, SMD* (95% CI) | № of participants | Quality of the evidence |
| Score with music therapy compared with usual care or other activities | |||
| Emotional well‐being including quality of life | The score in the intervention group was 0.34 SDs higher | 180 | ⊕⊕⊝⊝ |
| Mood disturbance or negative affect: depression | The score in the intervention group was 0.03 SDs lower | 354 | ⊕⊕⊝⊝ |
| Mood disturbance or negative affect: anxiety | The score in the intervention group was 0.28 SDs lower | 265 | ⊕⊝⊝⊝ |
| Behavioural problems: agitation or aggression | The score in the intervention group was 0.10 SDs lower | 330 | ⊕⊕⊝⊝ |
| Behavioural problems: overall | The score in the intervention group was 0.19 SDs lower | 351 | ⊕⊕⊝⊝ |
| Social behaviour: music vs other activities | The score in the intervention group was 0.53 SDs higher | 48 | ⊕⊝⊝⊝ |
| Cognition | The score in the intervention group was 0.07 SDs higher | 193 | ⊕⊕⊝⊝ |
| *Interpretation of SMD: a difference of < 0.40 SDs can be regarded as a small effect, 0.40–0.70 a moderate effect, and > 0.70 a large effect. CI: confidence interval; SMD: standardised mean difference; SD: standard deviation. | |||
| GRADE Working Group grades of evidence (GradePro) | |||
| aRisk of bias: no blinding of therapists and participants (not possible), and sometimes no or unclear blinding of outcome assessment. bImprecision: small number of participants and broad CIs includes both benefit and harm. cImprecision: small number of participants. dRisk of bias: no blinding of therapists and participants (not possible). eInconsistency: non‐overlapping CIs. fImprecision: small number of participants and broad CIs includes both benefit and harm. gImprecision: very small number of participants and very broad CIs includes both benefit and harm. hRisk of bias: no blinding of therapists and participants (not possible), and unclear blinding of outcome assessment. | |||
Antecedentes
Descripción de la afección
La demencia es un síndrome clínico caracterizado por la disminución progresiva en las funciones cognitivas. La demencia del tipo del Alzheimer es la forma más común de demencia, seguida de la demencia vascular, la demencia de cuerpos de Lewy y la demencia frontotemporal (Alzheimer's Disease International 2015).
Demencia es un nombre colectivo para los síndromes cerebrales degenerativos progresivos que afectan la memoria, el pensamiento, el comportamiento y la emoción (Alzheimer's Disease International 2015). Los síntomas pueden incluir:
-
pérdida de memoria;
-
dificultad para encontrar las palabras correctas o comprender lo que las personas están diciendo;
-
dificultad para cumplir tareas previamente habituales;
-
cambios de personalidad y del estado de ánimo.
El informe Alzheimer's Disease International's 2015 calculó que 46 800 000 personas presentan demencia en todo el mundo; y que esta cifra aumentará a 74 700 000 para 2030 y a 131 500 000 personas para 2050 (Alzheimer's Disease International 2015).
La investigación sigue diversos resultados alentadores relacionados con la descripción de las causas de la demencia y el tratamiento de la demencia. Debido a que la demencia se debe a un daño en el cerebro, un enfoque es limitar el grado y la tasa de progresión de los procesos patológicos que producen dicho daño. Se dispone de intervenciones farmacológicas, pero su capacidad es limitada para el tratamiento de muchas de las características del síndrome. Sin embargo, hay una amplia investigación que indica que los abordajes terapéuticos no farmacológicos pueden mejorar de forma efectiva los resultados relevantes. Es importante ayudar a los pacientes con demencia y a sus cuidadores a enfrentar las manifestaciones sociales y psicológicas del síndrome. Además de intentar desacelerar el deterioro cognitivo, la atención debe procurar estimular las capacidades, mejorar la calidad de vida y reducir los comportamientos problemáticos asociados con la demencia. El uso terapéutico de la música podría lograr estos objetivos.
Descripción de la intervención
Muchos tratamientos de la demencia dependen de la capacidad del paciente de comunicarse verbalmente. Cuando se ha perdido la capacidad de hablar o de comprender el lenguaje, la música podría ofrecer oportunidades alternativas para la comunicación. Los pacientes que no pueden hablar más todavía podrían tararear o jugar con música.
La World Federation of Music Therapy (WFMT) define a la musicoterapia como "el uso profesional de la música y sus elementos como intervención en el ambiente médico, educativo y cotidiano con individuos, grupos, familias o comunidades, que procuran optimizar su calidad de vida y mejorar su salud y bienestar físico, social, comunicativo, emocional, intelectual y espiritual." La investigación, la práctica, la formación y el entrenamiento clínico en musicoterapia se basan en estándares profesionales según los contextos culturales, sociales y políticos (WFMT 2011). La American Music Therapy Association (AMTA) define la musicoterapia como "el uso clínico y basado en evidencia de intervenciones con música para alcanzar metas individualizadas dentro de una relación terapéutica por parte de un profesional licenciado que ha completado un programa de musicoterapia aprobado" (AMTA). Describe la evaluación del paciente, las intervenciones ("que incluyen crear, cantar, moverse, o escuchar música"), los beneficios y la investigación, y explica que la musicoterapia se usa "dentro de una relación terapéutica para tratar las necesidades físicas, emocionales, cognitivas y sociales de los individuos." Se examinaron las intervenciones con música, que pueden compartir estas metas terapéuticas y el establecimiento de una relación terapéutica, incluso si no son proporcionadas por un musicoterapeuta acreditado.
Pueden distinguirse dos tipos principales de intervenciones terapéuticas con música – musicoterapia receptiva (o pasiva) y activa – que a menudo se combinan (Guetin 2013). Las intervenciones terapéuticas receptivas constan de escuchar música administrada por el terapeuta que canta, interpreta o selecciona la música grabada para los receptores. En la musicoterapia activa, los receptores están involucrados activamente en la realización de la música, por ejemplo, tocando instrumentos pequeños. Se puede alentar a los participantes a participar en la improvisación musical con instrumentos o la voz, con baile, actividades de movimiento o cantando.
La música también puede usarse en formas que son terapéuticas de una manera menos obvia, p.ej. tocar música durante otras actividades como durante las comidas o el baño, o durante la fisioterapia o el movimiento, o como parte de un programa de artes u otras intervenciones psicosociales. La “música como tratamiento” incluye la musicoterapia definida de modo más estricto proporcionada por "un profesional en música formalmente calificado con un énfasis terapéutico" (Ing‐Randolph 2015). Para beneficiar a los pacientes con demencia, los que proporcionan las intervenciones con música con una meta terapéutica pueden necesitar extraer las aptitudes tanto de los músicos como de los terapeutas para seleccionar y aplicar los parámetros musicales de forma adecuada, adaptados a las necesidades individuales y las metas de los receptores. Sin embargo, el entrenamiento de los terapeutas y los requisitos de los programas de entrenamiento, y la práctica de certificación para administrar intervenciones terapéuticas con música varía entre los países, lo cual implica que no sólo los musicoterapeutas acreditados pueden administrar las intervenciones terapéuticas con música.
De qué manera podría funcionar la intervención
Las intervenciones terapéuticas con música, incluidas las intervenciones proporcionadas por un musicoterapeuta certificado, constan principalmente de cantar, escuchar, improvisar o tocar instrumentos musicales. La música y el canto pueden estimular la especialización hemisférica. Las observaciones clínicas indican que cantar depende críticamente de las estructuras del hemisferio derecho. Por el contrario, los pacientes con afasia debido a las lesiones del hemisferio izquierdo a menudo muestran capacidades musicales vocales sorprendentemente preservadas. El canto puede explotarse para facilitar la reconstrucción del habla en los pacientes con afasia (Riecker 2000). Cantar puede ayudar de forma adicional en el desarrollo de la articulación, el ritmo y el control de la respiración. Cantar en un contexto grupal puede mejorar las aptitudes sociales y favorecer una mayor conciencia sobre otros. Para los pacientes con demencia, cantar puede promover la reminiscencia y las discusiones del pasado, mientras se reduce la ansiedad y el temor. Para los pacientes con compromiso de la respiración, cantar puede mejorar las tasas de saturación de oxígeno. Para los pacientes que tienen dificultad con el habla luego de un accidente cerebrovascular, la música puede estimular los centros del lenguaje en el cerebro y promover la capacidad de cantar. En resumen, cantar puede mejorar un rango de parámetros físicos y psicosociales (Clift 2016). Tocar instrumentos puede mejorar la coordinación motora gruesa y fina en los pacientes con deterioro motor o traumatismo neurológico relacionado con un accidente cerebrovascular, traumatismo craneoencefálico o un proceso de enfermedad (Magee 2017; WFMT 2010).
Aunque que las funciones cognitivas disminuyen durante la progresión de la enfermedad, la receptividad a la música puede permanecer hasta las fases tardías de la demencia(Aldridge 1996; Baird 2009; Cowles 2003). Incluso en el último estadio de la enfermedad, los pacientes pueden seguir siendo receptivos a la música cuando otros estímulos ya no pueden evocar una reacción (Norberg 1986). Lo anterior puede estar relacionado con las regiones de memoria musical en el cerebro que están relativamente preservadas en la enfermedad de Alzheimer (Jacobsen 2015). Posiblemente, los fundamentos del lenguaje son musicales y preceden las funciones léxicas en el desarrollo del lenguaje (Aldridge 1996). Escuchar música en sí puede disminuir las hormonas del estrés como el cortisol, y ayuda a los pacientes a enfrentar, p.ej., el estrés preoperatorio(Spintge 2000). La musicoterapia puede traer relajación y tiene un efecto positivo sobre la mejoría de la comunicación y el bienestar emocional (Brotons 2000). La musicoterapia permite el recuerdo de las experiencias de vida y la experiencia de las emociones. Muchos eventos vitales importantes van acompañados de música; casi siempre estos “recuerdos musicales” se almacenan por un tiempo más largo que los recuerdos del mismo período que no estaban acompañados por música (Baird 2009; Broersen 1995). Si ya no se reconocen las palabras, la música familiar puede proporcionar un sentido de seguridad y bienestar, que a su vez puede disminuir la ansiedad. El ritmo musical puede ayudar a los pacientes con enfermedad de Alzheimer a organizar el tiempo y el espacio. Los pacientes pueden tener contacto grupal mediante la comunicación musical con otros participantes, sin tener que hablar. Debido a sus cualidades no verbales, las intervenciones con música podrían ayudar a los pacientes con demencia de todos los niveles de gravedad a enfrentar los efectos de la enfermedad.
Por qué es importante realizar esta revisión
En esta revisión, se examinó la bibliografía proveniente de la investigación actual para evaluar si las intervenciones terapéuticas con música, incluida la musicoterapia, son un enfoque eficaz al tratamiento de los problemas emocionales, conductuales, sociales y cognitivos en los pacientes con demencia. También se investigó si, a falta de problemas específicos, estas intervenciones tienen un efecto sobre el bienestar emocional, incluida la calidad de vida, o el comportamiento social en los pacientes con demencia. La calidad de vida es a menudo una meta apropiada de la atención de los pacientes con demencia (Alzheimer's Disease International 2016), y es importante evaluar a la evidencia sobre si la intervención terapéutica basada en música puede contribuir con la calidad de vida o los resultados relacionados.
Hay pocos datos acerca de con qué frecuencia se están usando las intervenciones terapéuticas con música para los pacientes con demencia. En el Reino Unido, se calcula que 250 de 900 musicoterapeutas trabajan con pacientes con demencia, la cual es una apreciación errónea debido a que algunos cientos de terapeutas no fueron encuestados (Bowell 2018). De los datos informales y más formales, está claro que para los musicoterapeutas, los pacientes con demencia forman una clientela importante. Además, las intervenciones terapéuticas con música, en particular las intervenciones grupales, tienen un costo bastante bajo y también son apropiadas para los pacientes en los estadios más avanzados de la demencia para los que relativamente hay pocas intervenciones disponibles, debido a que jugar o tararear todavía es posible hasta los estadios posteriores de la enfermedad. La administración de intervenciones terapéuticas con música se están afianzando y en consecuencia la necesidad de seguir actualizando la recopilación de evidencia de una manera sistemática.
Objetivos
Evaluar los efectos de las intervenciones terapéuticas con música para los pacientes con demencia sobre el bienestar emocional incluida la calidad de vida, el trastorno del estado de ánimo o el afecto negativo, los problemas conductuales, el comportamiento social y la cognición al final del tratamiento y cuatro semanas o más después del final del tratamiento
Métodos
Criterios de inclusión de estudios para esta revisión
Tipos de estudios
Se incluyeron ensayos controlados aleatorios (ECA) cruzados y paralelos. La unidad de interés es el estudio en lugar del artículo (con artículos que informan sobre más estudios y algunos estudios informados en más artículos).
Tipos de participantes
Se incluyó a pacientes con un diagnóstico formal de cualquier tipo de demencia según el Diagnostic and Statistical Manual of Mental Disorders (DSM)‐IV o la DSM‐5, International Classification of Diseases (ICD)‐10 u otros criterios de diagnóstico aceptados. Para ser relevante a la práctica clínica, también se aceptó el diagnóstico de un médico de demencia si no había datos disponibles sobre los criterios formales como el DSM‐IV, el DSM‐5 o instrumentos equivalentes. Se incluyó a pacientes que vivían en ámbitos diversos incluida la comunidad, los hospitales o los hogares para convalecientes, y todas las gravedades de la demencia. No se usó la edad como un criterio.
Tipos de intervenciones
Se incluyó cualquier intervención basada en música, activa o receptiva, administrada a individuos o grupos. Se requirió un mínimo de cinco sesiones para asegurar que podría haber tenido lugar una intervención terapéutica. Las intervenciones terapéuticas con música se definieron como: el tratamiento proporcionado por un terapeuta calificado en música, o intervenciones basadas en una relación terapéutica y que cumplían con al menos dos de los siguientes criterios/indicadores: 1. objetivo terapéutico que puede incluir comunicación, relaciones, aprendizaje, expresión, movilización y otros objetivos terapéuticos relevantes; 2. música que coincide con las preferencias individuales; 3. participación activa de los pacientes con demencia mediante instrumentos musicales o canto; 4. los participantes tenían una indicación clínica para la intervención o fueron derivados para la intervención por un médico. La mayoría de los artículos informaron sobre estos indicadores que incluían indicadores de la habilidad para motivar a los pacientes individualmente e indicadores de las metas terapéuticas. También se requirió que la música fuese un elemento principal de la intervención (p.ej. no sólo movimiento con uso de música). La simple participación en un coro no reuniría la definición de una intervención terapéutica; ni una intervención individualizada de escucha de música con la música preferida cumpliría con la definición si no había comunicación ni oportunidad de relacionarse con el paciente con demencia durante la sesión.
Las intervenciones con música podrían compararse con cualquier otro tipo de tratamiento o actividad, ningún tratamiento o ninguna actividad. Los grupos control podían recibir actividades en las cuales se usaba música, pero no podían recibir intervención terapéutica con música (incluso si recibían menos sesiones que el grupo de intervención).
Tipos de medida de resultado
-
Bienestar emocional, incluida la calidad de vida y el afecto positivo. Las expresiones faciales (a falta de interacción con el observador) también pueden indicar el bienestar emocional.
-
Trastorno del estado de ánimo o afecto negativo: depresión (síntomas depresivos) y ansiedad.
-
Problemas conductuales: agitación o agresión (o ambos), problemas conductuales en general o síntomas neuropsiquiátricos. (Se combinaron los resultados de la agitación y la agresión conforme a la definición de consenso de la International Psychogeriatric Association de agitación que requiere la presencia de uno de los ítems de "actividad motora excesiva, agresión verbal o agresión física" (Cummings 2015).)
-
Comportamiento social, como la interacción (verbal).
-
Cognición.
-
Además de los siete resultados de interés mencionados anteriormente, se buscó cualquier efecto adverso.
Para estos resultados, se aceptaron todas las herramientas de evaluación usadas en los estudios primarios. Se utilizaron los resultados que se habían evaluado al final del tratamiento (un mínimo de cinco sesiones, para centrarse en metas terapéuticas logradas a más largo plazo en lugar de efectos inmediatos que pueden no perdurar), de forma independiente de la duración y el número de sesiones mayor que cuatro. Cuando hubo evidencia de ningún efecto diferente con el transcurso del tiempo, luego los resultados informados podían haber incluido las evaluaciones anteriores. También se buscaron resultados de un mínimo de cuatro semanas después de que finalizara el tratamiento para evaluar los efectos a largo plazo.
Resultados primarios
-
Bienestar emocional incluida la calidad de vida.
-
Trastorno del estado de ánimo o afecto negativo:
-
depresión;
-
ansiedad.
-
-
Problemas conductuales:
-
agitación o agresividad;
-
general.
-
El protocolo no priorizó los resultados. Se priorizaron los resultados relacionados con las emociones (bienestar emocional incluida la calidad de vida, y el trastorno del estado de ánimo o el afecto negativo) como de importancia fundamental debido a que estos resultados (p.ej. depresión) están estrechamente relacionados con la calidad de vida de los pacientes con demencia (Banerjee 2009; Beerens 2014). La depresión y la ansiedad también son prevalentes y bastante persistentes durante el curso de la demencia (van der Linde 2016; Zhao 2016). Se priorizaron además los problemas conductuales debido a que los mismos afectan las relaciones y la carga para el cuidador(e.g. van der Linde 2012); y algunos también pueden ser indicadores de dificultad.
Resultados secundarios
-
Comportamiento social.
-
Cognición.
El comportamiento social y la cognición fueron resultados importantes, pero secundarios, en cuanto a estos resultados, el beneficio para los participantes en sí no es tan obvio como para los resultados relacionados más estrechamente con la calidad de vida.
Métodos de búsqueda para la identificación de los estudios
We searched ALOIS, the Cochrane Dementia and Cognitive Improvement Group's (CDCIG's) Specialized Register. The search terms used were: music therapy, music, singing, sing, auditory stimulation.
The Information Specialists for CDCIG maintain ALOIS, which contains studies in the areas of dementia prevention, dementia treatment and cognitive enhancement in healthy people. Details of the search strategies used for the retrieval of reports of trials from the healthcare databases, the Cochrane Central Register of Controlled Trials (CENTRAL) and conference proceedings can be viewed in the ‘Methods used in reviews' section within the editorial information about the Dementia and Cognitive Improvement Group.
We performed additional searches in each of the sources listed above to cover the timeframe from the last searches performed for ALOIS to 19 June 2017. The search strategies for the above described databases are presented in Appendix 1.
In addition, we searched Geronlit/Dimdi, Research Index, Carl Uncover/Ingenta, Musica, and Cairs in January 2006 and June 2010, with the following search terms: music therapy, music, singing, dance, dementia, alzheimer. We also searched on these dates specific music therapy databases, as made available by the University of Witten‐Herdecke on www.musictherapyworld.de, based in Germany. We checked the reference lists of all relevant articles and a clinical librarian conducted a forward search from key articles using SciSearch. In addition, we handsearched conference proceedings of European and World Music Therapy conferences and European music therapy journals, such as the Nordic Journal of Music Therapy (archive), the British Journal of Music Therapy the Musiktherapeutische Umschau and the Dutch Tijdschrift voor Vaktherapie to find RCTs of music therapy for people with dementia up to July 2017. A new database search was performed on 12 April 2016 to identify new studies published after 3 July 2015, and the last new database search was performed on 19 June 2017. Potentially eligible new studies (based on abstract review with two review authors working independently) were included in the Characteristics of studies awaiting classification table.
Obtención y análisis de los datos
Selección de los estudios
Two review authors independently assessed publications for eligibility by checking the title and, if available, the abstract. If any doubt existed as to an article's relevance, they retrieved and assessed the full article.
Extracción y manejo de los datos
Two review authors independently extracted and cross‐checked data to assess eligibility using a brief data collection form, and if eligible, we proceeded to an independent assessment using a longer data collection form to abstract data describing the studies and outcome data. The two authors discussed any discrepancies or difficulties with a third review author. We reviewed articles in English, French, German and Dutch and searched for Cochrane collaborators to assess articles in other languages. We emailed authors for additional information when unclear (e.g. about the type of control group or setting); and for additional data if that would help inclusion of the study data in meta‐analyses (e.g. if estimates from graphical presentation were imprecise, standard deviations (SD) were lacking or item‐level data if items of global tools represented relevant outcomes).
We first extracted data on the design (RCT), population (dementia diagnosis), criteria for music therapy, outcomes and timing of outcome assessment, to evaluate eligibility of the study, Of the eligible studies, we subsequently recorded the following characteristics.
-
Data collection period.
-
Setting: nursing home, residential home, hospital, ambulatory care, other.
-
Participant characteristics: age, sex, severity and type of the dementia.
-
Number of participants included, randomised and lost to follow‐up.
-
Type, frequency and duration of active interventions and control interventions.
-
Description of activities in the control group if not usual care.
-
Outcomes: type of outcome measures about emotional well‐being, emotional problems (mood disturbance or negative affect), problematic or challenging behaviours (in general; and more specifically, agitation or aggression), social behaviours and cognition. Whether outcomes were referred to as primary or secondary outcomes.
-
Timing of outcome measurement including the long term, after treatment ended.
-
Research hypotheses if specified, and a description of the results.
-
Any methodological problems and comments.
-
Funding sources.
-
A 'Risk of bias' assessment (below).
For each study, we extracted relevant outcome data, that is, means, SDs and number of participants in each group for continuous data and numbers with each outcome in each group for dichotomous data. If needed or helpful, we contacted authors for clarification; or for data, such as from relevant subscales.
Evaluación del riesgo de sesgo de los estudios incluidos
Two review authors (neither of whom was an author on any of the studies that they assessed) independently assessed included studies for risk of bias according to the guidelines in the Cochrane Handbook for Systematic Reviews of Interventions, and using the 'Risk of bias' assessment tool (Higgins 2011). They looked at the following elements of study quality: selection bias (random sequence generation, allocation concealment); performance bias (blinding of participants and personnel); detection bias (blinding of outcome assessment); attrition bias (incomplete outcome data); reporting bias (selective reporting) and other potential threats to validity. They assessed performance, detection and attrition bias for each outcome.
Medidas del efecto del tratamiento
We used the risk ratio (RR) to summarise any effects on dichotomous outcome variables and the mean difference (MD) (or if different instruments or scales were used, the standardised mean difference (SMD)) for continuous variables with 95% confidence intervals (CI).
Cuestiones relativas a la unidad de análisis
Only participant‐level outcomes were considered, and all were continuous measures. For cross‐over trials, we extracted data for the first period only because of the likelihood of carry‐over effects.
Manejo de los datos faltantes
We considered if there were missing outcome data, with reasons reported, for example due to participants who moved or died, and how these were dealt with (exclusion of cases for analyses or were dealt with otherwise).
Evaluación de la heterogeneidad
We interpreted the I² statistic according to criteria in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011: Chapter 9.5.2). It offers a rough guide, with no important heterogeneity for I² up to 40%, moderate heterogeneity between 30% and 60%, substantial heterogeneity between 50% and 90%, and considerable heterogeneity for I² 75% and higher. Further, a low P value for the Chi² statistic indicated heterogeneity of intervention effects, which we evaluated against the combined 'usual care' and 'other activities' control groups. Because of small numbers of participants and studies for most outcomes, a non‐significant P value was not decisive in the evaluation of consistency, and we also considered overlap of CIs in the forest plots.
Evaluación de los sesgos de notificación
Selective outcome reporting is one of the elements of the risk of bias assessment, and for this we searched the articles about included studies and related articles for references to study protocols and trial registrations. If available, we compared with outcomes and prioritisation of outcomes in the article. If there was no research protocol available, we set risk of reporting bias to either unclear or high when appropriate. To detect possible publication bias, we examined funnel plots for outcomes with at least 10 studies available.
Síntesis de los datos
We included studies about all eligible interventions in groups of people in different stages of dementia, and we pooled the results of studies that examined effects on the same seven outcomes of interest. We discriminated between effects at the end of treatment and long‐term effects (a minimum of four weeks after treatment ended). In case of clinically homogeneous studies, results would have been combined using a fixed‐effect model. In case of statistical heterogeneity (assessed by visual inspection of the forest plots) and the availability of at least five studies, we used a random‐effects model.
We were interested in both usual care and other activity‐control interventions because usual practice with regard to activities offered is variable, and the question as to whether music‐based therapeutic interventions should be introduced at all and the question as to whether they are superior to other activities are both relevant in practice. We presented data by type of control intervention: usual care or other activities. A control group with other activities may imply that increased social contact and stimulation through an intervention is being controlled for. However, it is unclear whether this increases or decreases contrast with the music‐based intervention group for specific outcomes (e.g. agitation, anxiety). Therefore, we analysed effects against all control groups as planned in the protocol, but for purposes of possible hypothesis generation we presented forest plots by subgroup of control condition.
With probable selective outcome reporting, we ran the analyses for the reported outcomes while omitting the particular studies, to evaluate change and direction of change of the estimate.
Análisis de sensibilidad
Post hoc, we performed a series of sensitivity analyses because there are different possible criteria as to what constitutes music therapy, and because funding related to music therapy potentially involves an intellectual conflict of interest. First, we reran all analyses on end‐of‐treatment effects with studies in which the intervention was probably or definitely (when mentioned explicitly) delivered by a professional music therapist only. Second, we restricted these analyses to studies definitely delivered by a professional music therapist. Third, we restricted the analyses to studies definitely delivered by a professional music therapist and with no potential conflict of interest related to funding parties with a potential interest in promoting music‐based therapeutic interventions or no reported funding source. Finally, because blinding is important but possible only for outcome assessment, we also performed the analyses without studies at high or unclear risk of detection bias, and in view of findings of Tsoi 2018, we explored if effects of individual therapy differed substantially from the effects of the different therapies we included in this review.
Presentation of results and 'Summary of findings' tables
We used GRADE methods to rate the quality of evidence (high, moderate or low) for each effect estimate in the review (Guyatt 2011). This rating refers to our level of confidence that the estimate reflects the true effect, taking account of risk of bias in the included studies, inconsistency between studies, imprecision in the effect estimate, indirectness in addressing our review question and the risk of publication bias. We produced 'Summary of findings' tables for end‐of‐treatment and long‐term outcome comparisons to show the effect estimate and the quantity and quality of the supporting evidence for the outcomes. The 'Summary of findings' tables were generated with Review Manager 5 (Review Manager 2014) data imported into the GradePro Guideline Development Tool (2015); for the last update, the table was revised manually.
Results
Description of studies
Results of the search
The total number of included studies for this update was 22. For the first version of this review (Vink 2003), we identified 354 references related to music‐based interventions and dementia (Figure 1). Of those, on the basis of the abstracts, 254 were discarded as they did not refer to a research study or were identified as anecdotal or reports of case studies. Hard copies were obtained for the initially remaining 100 studies in 2003. We then discarded a further 74 studies as they involved participant series or case studies. As a results, 26 studies remained in 2003, of which five met the criteria for inclusion at that time (Brotons 2000; Clark 1998; Gerdner 2000; Groene 1993; Lord 1993). In 2008, an additional 18 studies were reviewed, of which three studies met the criteria (Svansdottir 2006; Raglio 2008; Sung 2006). For the update of 2010, we retrieved 188 references of possible relevance. After a first assessment, 16 references remained which were further assessed, of which two studies met the criteria of this review (Guétin 2009; Raglio 2010a). In total, 10 studies were included in the previous update. In 2015, due to clarified criteria for eligibility of interventions, randomisation and more stringent application of criteria for analyses of outcomes after a minimum number of sessions, we excluded five of the 10 previously included studies (Brotons 2000; Gerdner 2000; Groene 1993; Raglio 2008; Sung 2006; see Characteristics of excluded studies table). However, we included 12 new studies after evaluating 121 references including 25 full‐text evaluations, which resulted in 17 included studies. A new search on 12 April 2016 identified eight potentially eligible additional studies which warranted review against inclusion criteria (Curto Prieto 2015; Hsiung 2015; Hsu 2015; Raglio 2015; Rouch 2017; Thornley 2016; 신보영, 황은영 2015; 채경숙 2015), in addition to one study for which we were waiting for clarification from the authors about the results (Hong 2011). The latest search was performed 19 June 2017. We identified a new eligible study (Cho 2016), and we included four studies that had been awaiting classification (Hsu 2015; Lyu 2014; Raglio 2015; Thornley 2016; from which we could extract data with the help of collaborators). We excluded 채경숙 2015 (see Characteristics of excluded studies table) and remaining potentially eligible studies are listed in the Characteristics of studies awaiting classification and Characteristics of ongoing studies tables.

Study flow diagram.
Included studies
Details of the included studies are presented in the Characteristics of included studies table. One article (Narme and colleagues 2012: Narme 2012‐study 1 and Narme 2012‐study 1a) reported on two studies with rather similar designs indicated with study 1 and study 2 in the article (note that study 2 is indicated with 1a in our analyses). More articles with additional results or background of the study were available for five studies (Cooke 2010; Lin 2011; Narme 2014; Raglio 2010a; Vink 2013).
Nineteen studies had a parallel‐group designs (Ceccato 2012; Cho 2016; Guétin 2009; Hsu 2015; Liesk 2015; Lin 2011; Lord 1993; Lyu 2014; Narme 2012‐study 1; Narme 2012‐study 1a (also referred to as study 2); Narme 2014; Raglio 2010a; Raglio 2010b; Raglio 2015; Sakamoto 2013; Sung 2012; Svansdottir 2006; Thornley 2016; Vink 2013); and three used a cross‐over design with first‐period data available for all (Clark 1998; Cooke 2010; Ridder 2013).
The 22 studies were performed in 14 countries. Whereas the two oldest studies and one recent study were from the USA (Cho 2016; Clark 1998; Lord 1993), the studies published after 1998 were from a variety of other regions and countries: 13 studies conducted in eight countries in Europe (Italy, France, Germany, the Netherlands, the UK and Iceland, including also one study performed in two countries, Denmark and Norway; Ridder 2013), four studies from three countries in Asia (Taiwan, Japan and China), one study from Australia and one from Canada. The studies were all performed in institutional settings of nursing homes, residential homes and hospital wards for older adults. Dementia severity varied. The total number of randomised participants varied between 14 (Narme 2012‐study 1a) and 120 (Raglio 2015), with a median number of 47 participants across the studies. Nine out of 22 randomised fewer than 40 participants, and only two had more than 100 participants. The total number of participants randomised over all studies was 1097.
The interventions were active (Cho 2016; Cooke 2010; Hsu 2015; Liesk 2015; Lyu 2014; Raglio 2010a; Raglio 2010b; Raglio 2015; Sung 2012; Thornley 2016); receptive (listening interventions while there was communication with the therapist, Clark 1998; Guétin 2009); or a mixture of the two forms (Ceccato 2012; Lin 2011; Lord 1993; Narme 2012‐study 1; Narme 2012‐study 1a; Narme 2014; Ridder 2013; Sakamoto 2013; Svansdottir 2006; Vink 2013). Appendix 2 describes the music‐based therapeutic intervention and other activities of all studies. Music included live or recorded music that met preferences of the group or individual. The active forms often combined playing of instruments and singing activities, and some also combined with movement such as clapping hands and dance. In seven studies, the intervention concerned an individual intervention. Sessions varied in duration between half an hour and two hours. The total number of sessions ranged from six (Narme 2012‐study 1) to 156 (Lord 1993), with a median total number of 14 sessions until the end of treatment assessment. The frequency ranged between one session per week (Guétin 2009; Hsu 2015; Sakamoto 2013) and seven sessions per week (daily, Lyu 2014) with a median and more typical number (mode) of two sessions per week (13 studies employed two per week). These figures probably reflected number of sessions offered, as the number of attended session may be lower. There were few reports about implementation fidelity including adherence and dose received. However, Ridder 2013 reported that a minimum of 12 sessions were offered, but the participants received a mean of 10 sessions, and Thornley 2016, in their study on an acute inpatient psychiatric unit within an academic hospital, mentioned that the participants enrolled in the study were generally hospitalised for two to three weeks, which limited the number of sessions attended.
In 12 of the studies, we could be sure from the report that the interventions had been delivered by an accredited music therapist (Ceccato 2012; Cho 2016; Hsu 2015; Lin 2011; Lyu 2014; Raglio 2010a; Raglio 2010b; Raglio 2015; Ridder 2013; Svansdottir 2006; Thornley 2016; Vink 2013). In four studies, it was unclear whether a music therapist was involved (no profession reported in the older studies, Lord 1993 and Clark 1998; probably delivered by trained music therapists but it was not stated explicitly in Guétin 2009; and delivered by musicians trained in the delivery of sessions and in working with older people with dementia but unclear if these were formally trained music therapists in Cooke 2010). In the other six studies, the intervention was not delivered by a music therapist (psychologist and other supervisor(s) with no training in music therapy: Narme 2012‐study 1; Narme 2012‐study 1a; Narme 2014; trained research assistants: Sung 2012; music facilitator: Sakamoto 2013; music teacher specialised in teaching older people: Liesk 2015). Nine studies selectively included people with agitation, mood or behavioural problems (Clark 1998; Cooke 2010; Guétin 2009; Hsu 2015; Raglio 2010a; Raglio 2015; Ridder 2013; Sung 2012; Vink 2013), while some studies (also) excluded people with major psychiatric conditions such as psychosis or major depression (Ceccato 2012; Cho 2016; Guétin 2009; Raglio 2015), or people with other medical conditions such as hearing impairment or acute illness.
Most studies compared the music intervention with an active control intervention with the same number of sessions and frequency as the music group. Two‐armed studies compared with the following interventions: reading (Cooke 2010; Guétin 2009), a cognitive stimulation intervention (Liesk 2015), painting (Narme 2012‐study 1), cooking (Narme 2012‐study 1a – also referred to as study 2; Narme 2014), or individual active engagement activities (Thornley 2016) or variable recreational activities which included handwork, playing shuffleboard, and cooking and puzzle games (Vink 2013). Five studies had three arms with the active control groups working on jigsaw puzzles (Lord 1993), reading familiar lyrics (Lyu 2014), television watching (Cho 2016), or receiving a passive group music intervention which did not meet our inclusion criteria for a therapeutic music‐based intervention (Cho 2016; Raglio 2015; Sakamoto 2013).
Outcomes that were assessed often were 'emotional well‐being' including quality of life, mood disturbance or negative affect (also as part of behavioural scales), and 'behavioural problems' (agitation or aggression, and behaviour overall) and 'cognition.' Social behaviour was less commonly assessed (Lord 1993; Narme 2012‐study 1; Narme 2012‐study 1a; Narme 2014); and the meta‐analyses of end‐of‐treatment scores included only the three studies from Narme and colleagues. The Cohen‐Mansfield Agitation Inventory (CMAI, for agitation; Cohen‐Mansfield 1986), Mini‐Mental State Examination (MMSE, for cognition; Folstein 1975), and the Neuropsychiatric Inventory (NPI, for behaviour; Cummings 1994) in particular were frequently used. Item‐level NPI outcome data were reported in the article or the author additionally provided data about depression, anxiety and agitation outcomes.
Excluded studies
We screened 769 records and we excluded 678 (Figure 1). Of the remaining 91 records examined in full text, we excluded 70 records (see Characteristics of excluded studies table for a selection of excluded studies which were close but did not qualify upon careful consideration). They were often excluded because the participants did not have dementia, or because of a trial design (i.e. not an RCT). Further, and often less obvious, we critically reviewed whether the intervention met the inclusion criteria for a music‐based therapeutic intervention, and whether the reported outcomes included any assessments after fewer than five sessions. There are a number of studies on group music interventions such as group music in addition to movement interventions (e.g. Sung 2006): these were excluded because music was not the main or only therapeutic element, or was not provided with individual therapeutic intent. Further, some studies assessed outcomes during the treatment sessions only, combining immediate effects, for example, on behaviour during the first session, with effects after multiple sessions (e.g. Gerdner 2000). Studies awaiting classification included conference abstracts and articles about studies in Asia which we could not retrieve or evaluate in time (see Characteristics of studies awaiting classification table).
Risk of bias in included studies
The results of the assessment of risk of bias are presented in the Risk of bias in included studies tables, in Figure 2 and Figure 3, and in funnel plots (Figure 4; Figure 5).

Methodological quality summary: review authors' judgements about each methodological quality item for each included study.

Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.

Funnel plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.3 Negative affect or mood disturbances: anxiety (13 studies, 15 dots because 2 studies used 2 control groups, 1 with usual care and 1 with other activities).

Funnel plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.4 Problematic behaviour: agitation or aggression (14 studies, 16 dots because 2 studies used 2 control groups, 1 with usual care and 1 with other activities).
There were a number of possible biases and often we could not assess the risk of bias due to poor reporting. Risk of performance bias was high for all studies because participants and staff could not be blinded to the intervention. Regarding the other items, in more recent studies risk of bias was lower. An exception was attrition bias, however, it is possible that this was reported more accurately in recent studies. That is, the reporting in terms of interventions, rationale, chosen procedures, design and results was generally better in more recent studies. Still, we are unsure about the methodological quality of a number of studies because several items were rated as unclear.
Allocation
All included studies were RCTs. However, the randomisation procedure was not always described in detail (Figure 2). Moreover, allocation concealment was described and adequate in detail in six studies, all of which were published in 2010 or later (Cho 2016; Cooke 2010; Hsu 2015; Lin 2011; Raglio 2015; Ridder 2013). One older study stated that participants were "non‐systematically separated" into groups without further detail, which we considered posed a high risk of selection bias (Lord 1993). One study used cluster randomisation, but this study contributed only a maximum of 13 participants to the meta‐analyses (Hsu 2015).
Blinding
Blinding of therapists and participants to the intervention is not possible. Therefore, the studies were at high risk of performance bias even though therapists do not generally assess outcomes and participants may not be aware, have no specific expectations or were unable to self‐report. The outcomes were assessed unblinded, by the research team or unblinded nurses, in at least six studies (Figure 2). For example, Narme and colleagues described two studies differing in detection bias (Narme 2012‐study 1; Narme 2012‐study 1a). The first study involved a high risk of detection bias because the outcomes 'anxiety' (measured with the State‐Trait Anxiety Inventory for adults, STAI‐A) and, as assessed from the first two minutes of filmed interviews, 'emotions' (from facial expressions) and 'social behaviour' (discourse content), were assessed by nurses who were not blinded to the interventions (music intervention or painting) (Narme 2012‐study 1). By contrast, in the second study, risk of detection bias was low because five independent observers who were blinded for the type of intervention (music intervention or cooking) assessed the outcomes (Narme 2012‐study 1a). For all outcomes except for cognition, less than half of the number of patients participated in a study that was at high or unclear risk of detection bias (emotional well‐being including quality of life: 134/348 participants; depression: 140/503; anxiety: 117/478; agitation or aggression: 254/626; behavioural problems overall: 147/442; social behaviour: 22/70). For cognition, for 237/350 cases, risk of detection bias was unclear. Risk of performance bias, and for some outcomes also risk of detection bias, in several studies resulted in downgrading of the quality of the evidence for all end‐of‐treatment outcomes (summary of findings Table for the main comparison); and for all long‐term outcomes (summary of findings Table 2).
Incomplete outcome data
Self‐reported outcomes were rarely employed. Occasionally death, hospitalisation, acute illness or no interest in the therapy occurred across the different study arms; and cases with no outcome data were not included in the analyses. Incomplete outcome data were problematic in a few studies (Cho 2016; Hsu 2015; Thornley 2016). In Hsu 2015, three of nine participants in the intervention group died (and one of eight in the control group). In contrast, Cho 2016 lost nine of 17 participants in the television watching control group (and only a few in the other groups) and suggested this was because individual preferences for television programmes were not taken into account. Thornley 2016 did not perform their study in a long‐term care setting but in an inpatient psychiatric unit of a hospital and some participants were discharged after having attended a few sessions. The studies at high risk of attrition bias were three of the five studies added in this update. Newer studies often visualised cases lost to follow‐up and missing outcome assessment in detail using flow diagrams. The two oldest studies, and some newer studies, only reported the number of cases randomised (and analysed) and did not explicitly report reasons for missing outcome data by study arm, or how these were handled. Therefore, it was possible that attrition bias was problematic in more studies, but that the reporting of missing outcome data was better in newer studies.
Selective reporting
Most studies, including the newer studies, did not refer to initial plans, a study protocol or trial registration. Therefore, it was unclear to what extent bias due to selective outcome reporting was pertinent. We found some indication of inconsistent reporting of primary and secondary outcomes (Cooke 2010; Hsu 2015). Without these two studies, the pooled estimate for emotional well‐being and quality of life decreased from 0.32 to 0.23; other SMDs were similar. Only one study clearly referred to a change in initial plans (Ceccato 2012); and two studies referred to a trial registration, and outcome reporting was consistent with the registration for Sakamoto 2013 but not for Hsu 2015. We did not downgrade the quality of the evidence because of unclear risk of selective reporting.
Regarding publication bias, funnel plots for outcomes with sufficient studies (anxiety, 13 studies of which two with both a 'usual care' and 'other activity' control group, Figure 4; and agitation or aggression, 14 studies, also two with two types of control groups, Figure 5) did not clearly suggest possible publication bias.
Other potential sources of bias
We found some other potential sources of bias. Outcome assessment may be either imprecise or biased by the use of non‐validated outcome measures with suboptimal distributions (such as skewed distributions, e.g. number of times yelling was observed; Clark 1998) and different procedures for the baseline and outcome assessment (Sakamoto 2013). Further, we found problems with the reporting of outcomes or we suspected errors (Lord 1993; and for this reason, Hong 2011 is under Studies awaiting classification). Implementation fidelity, including non‐adherence, was infrequently described, but Liesk 2015, one of the few studies with null findings, reported on this in detail. Finally, there may be bias due to a financial or intellectual conflict of interest when funding was provided by a source with a potential interest in the effectiveness of music therapy. This may apply to two studies (Ceccato 2012; Ridder 2013), but it should be noted that no source of funding was reported for more studies (Clark 1998; Liesk 2015; Lin 2011; Lord 1993; Lyu 2014; Raglio 2010a; Raglio 2010b). Only six studies were both definitely delivered by a music therapist and funded by a source unrelated to music or music therapy (no potential financial conflict of interest, but at least for some, the music therapists (co)authored the article; Cho 2016; Hsu 2015; Raglio 2015; Svansdottir 2006; Thornley 2016; Vink 2013).
Effects of interventions
See: Summary of findings for the main comparison Music‐based therapeutic interventions compared to usual care or other activities for people with dementia: end‐of‐treatment effects; Summary of findings 2 Music‐based therapeutic interventions compared to usual care or other activities for people with dementia: long‐term effects (scores 4 weeks or more after treatment ended)
Results at the end of treatment are summarised in summary of findings Table for the main comparison and longer‐term effects in summary of findings Table 2. Long‐term effects were assessed between 4 weeks and 3 months after treatment ended, with a median of 8 weeks after the last session.
Of the 22 included studies, 21 studies with 890 participants contributed to meta‐analyses of effects. One study reported data on emotional well‐being, social behaviour and cognition, but not in enough detail for us to include it in meta‐analyses (Lord 1993). We contacted several authors and they provided the additional data we asked for, in the form of SDs or item‐level outcome data of scales for general behavioural assessments. We pooled data for all end‐of‐treatment and long‐term outcomes. Of the 22 studies, all but three newer studies (Liesk 2015; Raglio 2015; Thornley 2016) reported some significant improvement in outcomes of the music intervention versus control (all outcomes, including physiological outcomes that we did not evaluate). The methodological quality of these three studies varied, but Raglio 2015, with 120 participants, was the largest study with relatively favourable quality ratings (Figure 2). Overall, the quality varied in terms of risk of bias, but also other quality considerations varied substantially across the studies and the particular outcomes.
Emotional well‐being including quality of life
We included nine studies with 348 participants in the analysis of end‐of‐treatment scores for the critically important outcome of emotional well‐being and quality of life. Most studies used a validated quality‐of‐life or well‐being measure for more direct observation; the Dementia Quality of Life (DQOL) (Cooke 2010); a German translation of the Dementia Quality of Life Instrument (DEMQOL) (Liesk 2015); a Danish translation of the Alzheimer's Disease‐Related Quality of Life (ADRQL) (Ridder 2013); the Cornell‐Brown Scale for Quality of Life in Dementia (CBS‐QoL) – although it was unclear if this was a validated translated version (Raglio 2015); a Dementia Care Mapping Wellbeing score (Hsu 2015); and the Quality of Life‐Alzheimer's Disease (QOL‐AD) (Cho 2016). In the three studies conducted by Narme and colleagues, emotional well‐being referred to counts of positive and negative facial expressions as assessed from the first two minutes of filmed interviews (Narme 2012‐study 1; Narme 2012‐study 1a; Narme 2014). We found evidence of an effect at the end of treatment (SMD 0.32, 95% CI 0.02 to 0.62; Analysis 1.1; Figure 6; summary of findings Table for the main comparison). Heterogeneity was low to moderate (I² = 40%; Chi² P = 0.09). There was no blinding of outcome assessment in four of the nine studies. The overall quality for effects of music‐based interventions on emotional well‐being and quality of life at end of treatment was low, downgraded for serious risk of bias and imprecision (wide CI). The quality was also low for long‐term outcomes for which there were only four studies (180 participants; Hsu 2015; Narme 2012‐study 1a; Narme 2014; Raglio 2015). The SMD was similar to the SMD at the end of treatment but the imprecision was greater so we were less certain of the direction of the effect (SMD 0.34, 95% CI –0.12 to 0.80; I² = 46% Chi² P = 0.12; Analysis 2.1; summary of findings Table 2).

Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.1 Emotional well‐being and quality of life. CI: confidence interval; SD: standard deviation.
Mood disturbance or negative affect: depression
Eleven studies contributed 503 participants to the analysis on end‐of‐treatment effect (Figure 7), and six studies contributed 354 participants to the analysis on long‐term effects. Depression or depressive symptoms were measured with (translated versions of) the Geriatric Depression Scale (GDS), the Cornell Scale for Depression in Dementia, or with a subscale of the Behavioural Pathology in Alzheimer's Disease (BEHAVE‐AD) or the NPI. Heterogeneity was not important (I² = 0%) for either end‐of‐treatment or long‐term outcomes. We downgraded both outcomes for risk of bias, due to lack of blinding in many studies. Imprecision was more of an issue for long‐term outcomes. The overall quality of the evidence was moderate for end‐of‐treatment effects and low for long‐term outcomes. We found that music‐based therapeutic interventions probably reduced depressive symptoms at the end of treatment (SMD –0.27, 95% CI –0.45 to –0.09; Analysis 1.2; Figure 7; summary of findings Table for the main comparison). There was no evidence of a reduction in the longer term, with a smaller estimate and a CI including no effect (SMD –0.03, 95% CI –0.24 to 0.19; Analysis 2.2; summary of findings Table 2).

Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.2 Negative affect or mood disturbances: depression. BEHAVE‐AD: Behavioural Pathology in Alzheimer's Disease; NPI: Neuropsychiatric Inventory; SD: standard deviation.
Mood disturbance or negative affect: anxiety
The other mood item we considered was anxiety. For this outcome, at the end of treatment, we included 13 studies with 478 participants. A variety of (translated) outcome measures were used; Rating Anxiety in Dementia Scale (RAID), STAI‐A, Hamilton Anxiety Scale, and subscale scores of the BEHAVE‐AD and NPI. Heterogeneity was substantial for end‐of‐treatment effects (I² = 53%; Chi² P = 0.008) and longer‐term effects (I² = 63%; Chi² P = 0.01). In addition to serious inconsistency, we downgraded the quality for lack of blinding. We did not find clear evidence of publication bias (Figure 4). We judged the quality of the evidence as low at the end of treatment and, for the longer‐term outcome, very low because there was also imprecision. Therefore, we can have little or very little confidence in the results. Anxiety was lower in the music intervention group at the end of treatment (SMD –0.43, 95% CI –0.72 to –0.14; 13 studies, 478 participants; Analysis 1.3; Figure 8; summary of findings Table for the main comparison). In the longer term, we could not be certain of either the size or the direction of effect (SMD –0.28, 95% CI –0.71 to 0.15; 6 studies, 265 participants; Analysis 2.3; summary of findings Table 2).

Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.3 Negative affect or mood disturbances: anxiety. BEHAVE‐AD: Behavioural Pathology in Alzheimer's Disease; NPI: Neuropsychiatric Inventory; SD: standard deviation; STAI‐A: State‐Trait Anxiety Inventory for Adults.
Behavioural problems: agitation or aggression
Fourteen studies with 626 participants contributed to the end‐of‐treatment effect analysis, and five studies with 330 participants contributed to the long‐term effect analysis. Outcome measures used for agitation were (translated versions of) the CMAI and the agitation subscale of the NPI; and for aggression, the aggressiveness subscale of the BEHAVE‐AD and counts of observed aggressive behaviour. Heterogeneity was not important at the end of treatment (I² = 9%, Chi² P = 0.35) and longer term (I² = 6%, Chi² P = 0.38). Inconsistency and imprecision were not serious for effects on agitation or aggression at the end of treatment, but imprecision was serious for effects on the long‐term outcome. There was no evidence of publication bias (regarding end‐of‐treatment effect; Figure 5). We rated the quality of the evidence as moderate for the end‐of‐treatment outcome but low for the long‐term outcome. We found no evidence of an effect on agitation or aggression at the end of treatment (SMD –0.07, 95% CI –0.24 to 0.10; Analysis 1.4; Figure 9; summary of findings Table for the main comparison) or in the long term (SMD –0.10, 95% CI –0.33 to 0.13; Analysis 2.4; summary of findings Table 2).

Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.4 Problematic behaviour: agitation or aggression. BEHAVE‐AD: Behavioural Pathology in Alzheimer's Disease; CI: confidence interval; CMAI: Cohen‐Mansfield Agitation Inventory; NPI: Neuropsychiatric Inventory; SD: standard deviation.
Behavioural problems: overall
Ten studies with 442 participants contributed to the end‐of‐treatment effect analysis, and six studies with 351 participants contributed to the analysis of longer‐term effects. Outcome measures were (translated versions of) the BEHAVE‐AD and NPI. Heterogeneity was low for the end of treatment effect (I² = 19%, Chi² P = 0.25). The quality of the evidence was moderate due to lack of blinding. We found evidence of an effect of music‐based therapeutic interventions on problematic behaviour overall at the end of treatment (SMD –0.23, 95% CI –0.46 to –0.01; Analysis 1.5; Figure 10; summary of findings Table for the main comparison). There was no convincing evidence of a long‐term effect because of imprecision (SMD –0.19, 95% CI –0.51 to 0.14; I² = 51%, Chi² P = 0.05; Analysis 2.5; summary of findings Table 2). Therefore, heterogeneity was moderate, and the quality of the evidence was low due to imprecision in addition to lack of blinding.

Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.5 Problematic behaviour overall. NPI: Neuropsychiatric Inventory; SD: standard deviation.
Social behaviour: music versus other activities
The three studies of Narme and colleagues) contributed 70 participants to the end‐of‐treatment effect analysis (Narme 2012‐study 1; Narme 2012‐study 1a; Narme 2014), and two of them contributed 48 participants to the analyses of longer‐term effects (Narme 2012‐study 1a; Narme 2014). For all, the outcome was the contents of conversation (positive versus negative expressions when interviewed about current feelings and personal history). Lord 1993 reported effects on their self‐made questionnaire on social interaction, mood and recall (combined outcome), but there were no separate figures for social interaction and therefore we could not use the data for the meta‐analysis. We downgraded the evidence at both time points due to serious or very serious risk of bias and very serious imprecision. There was also moderate to substantial heterogeneity in the long‐term analysis (I² = 54%, Chi² P = 0.14). We considered the quality of the evidence to be very low for both outcomes and were therefore very uncertain about the result of more positive expressions in the music‐based interventions group at the end of treatment (SMD 0.54, 95% CI 0.06 to 1.02; 3 studies; I² = 0%, Chi² P = 0.70; Analysis 1.6; Figure 11; summary of findings Table for the main comparison). There was a similar SMD but an even wider CI in the analysis of long‐term effects (SMD 0.53, 95% CI –0.53 to 1.60; Analysis 2.6; summary of findings Table 2).

Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.6 Social behaviour: music vs other activities. SD: standard deviation.
Cognition
Seven studies contributed 350 participants to the end‐of‐treatment effect analysis and two studies with 193 participants assessed long‐term effects. Outcome measures used in the analyses were (translated versions of) the MMSE and the Severe Impairment Battery (SIB). We used the MMSE data if these were available in addition to other cognition measures such as Prose Memory tests, the FAS‐Test (Controlled‐Oral‐Word‐Association Test) or the Alzheimer's Disease Assessment Scale Cognitive subscale (ADAS‐cog). The end‐of‐treatment results were imprecise but not inconsistent. There was no important heterogeneity (I² = 0%; Chi² P = 0.89). There was serious risk of bias. The overall quality of the evidence was low for both time points and suggested that music‐based interventions may have had little or no effect on cognition at the end of treatment (SMD 0.15, 95% CI –0.06 to 0.36; Analysis 1.7; Figure 12; summary of findings Table for the main comparison) or at the long term (SMD 0.07, 95% CI –0.21 to 0.36; I² = 0%; Chi² P = 0.90; Analysis 2.7; summary of findings Table 2).
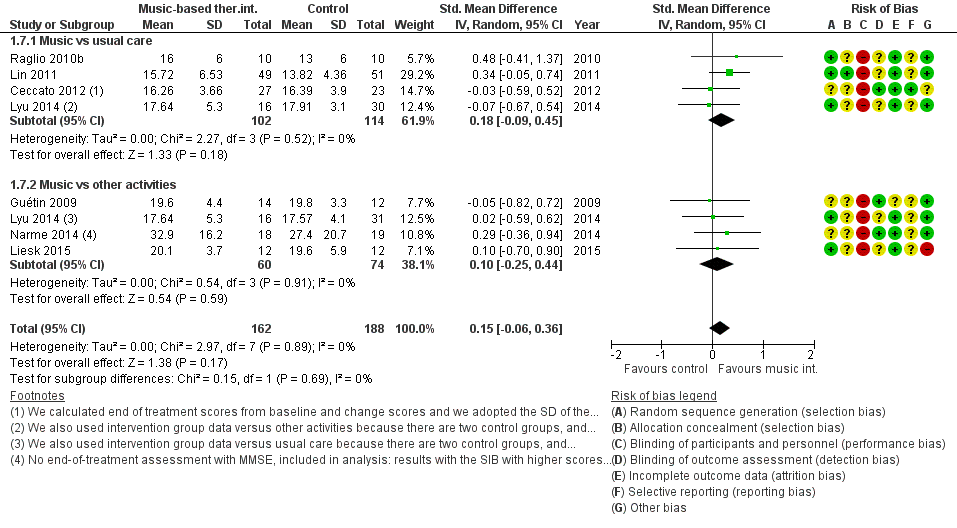
Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.7 Cognition. MMSE: Mini‐Mental State Examination; SD: standard deviation; SIB: Severe Impairment Battery.
Adverse effects
None of the trials reported adverse effects.
Effects of interventions delivered by a music therapist and sensitivity analyses
The sensitivity analyses with analyses restricted to studies where the intervention was definitely or possibly delivered by a qualified music therapist resulted in similar end‐of‐treatment effect estimates (there was no sensitivity analysis for the social behaviour outcome because no study remained). When restricting to studies that were definitely delivered by a music therapist, most effects were similar, but there was a smaller effect on anxiety. In the six of 13 studies in which the intervention was definitely delivered by a music therapist, the estimate for anxiety was –0.19 (SMD –0.19, 95% CI –0.52 to 0.13; with less heterogeneity; I² = 29%, Chi² P = 0.21; 242 participants).
When we restricted analyses further to studies definitely delivered by a music therapist, and having no potential financial conflict of interest or no funding source reported, we removed no studies from the anxiety analysis, and removed one or two studies for the remaining five outcomes. We found somewhat larger SMDs for the end of treatment outcomes. However, when we restricted analyses to studies at low risk of detection bias, the SMDs of six of the seven outcomes were smaller; all except for the SMD of behavioural problems overall, which was slightly larger. SMDs for individual therapy were similar to those for the main analyses (combined individual and group therapy) except for behavioural problems (both agitation or aggression and overall), for which SMDs for individual therapy were clearly larger.
Discusión
Resumen de los resultados principales
El objetivo de esta revisión fue evaluar el efecto de las intervenciones terapéuticas con música sobre un rango de resultados relevantes para los pacientes con demencia. El foco específico fue evaluar si dichas intervenciones podrían mejorar el bienestar emocional incluida la calidad de vida, el trastorno del estado de ánimo o el afecto negativo, los problemas conductuales, el comportamiento social y la cognición.
La revisión incluyó 22 estudios, y fue posible realizar metanálisis sobre los efectos al final del tratamiento y a más largo plazo (principalmente cuatro semanas después de que finalizara el tratamiento). Se encontró evidencia de calidad moderada de que al final del tratamiento las intervenciones terapéuticas con música mejoraron los síntomas depresivos y los problemas conductuales en general, pero no mejoraron la agitación ni la agresión. Hubo evidencia de baja calidad de que mejoró el bienestar emocional incluida la calidad de vida y la ansiedad y no mejoró la cognición. Hubo evidencia de calidad muy baja de un beneficio en el comportamiento social. No hubo evidencia de efectos cuatro semanas o más después del final del tratamiento (a largo plazo), pero la calidad de esta evidencia para todos los resultados fue baja o muy baja. Los análisis de sensibilidad con los resultados del final del tratamiento sugirieron que los efectos no fueron más grandes en los estudios en los que la intervención fue administrada por un musicoterapeuta calificado.
Compleción y aplicabilidad general de las pruebas
Se realizaron búsquedas en los estudios informados en varios idiomas, y también se incluyeron artículos en idiomas distintos del inglés. No se encontraron estudios realizados en el hogar del paciente ni en un contexto comunitario. Sólo tres estudios usaron el comportamiento social como un resultado, y los mismos provinieron de un único grupo de investigadores de Francia(Narme 2012‐study 1; Narme 2012‐study 1a; Narme 2014). La evidencia de esta revisión aplicó a los efectos terapéuticos de las intervenciones terapéuticas con música después de al menos cinco sesiones. Excluyó algunas intervenciones grupales que incluían música, pero en las que la música no era el elemento terapéutico principal o único, o en las que no había interacción durante la sesión. Excluyó los efectos directos durante las sesiones.
Calidad de la evidencia
La calidad de la evidencia fue moderada para la depresión, los problemas conductuales en general y para la agitación o la agresión al final del tratamiento. Para todos los otros resultados, fue baja o muy baja. Se disminuyó la calificación de todos los resultados por el riesgo de sesgo; el bienestar emocional incluida la calidad de vida, el comportamiento social y la cognición al final del tratamiento y todos los resultados a largo plazo se disminuyeron debido a la imprecisión; y la ansiedad, tanto al final del tratamiento como a largo plazo, también se disminuyó debido a la inconsistencia. La evaluación de resultado no cegada puede haber sobrestimado los efectos.
Muchos estudios usaron medidas de resultado validadas para el comportamiento (p.ej. el NPI (Cummings 1994), o BEHAVE‐AD (Reisberg 1987)), dos medidas ampliamente usadas que se recomiendan debido a las propiedades psicométricas favorables(Jeon 2011), y para la cognición (p.ej. la MMSE (Folstein 1975)). Se incluyeron subescalas de las escalas conductuales como medidas de resultado. Sin embargo, hubo menos evidencia en cuanto a la validez de las subescalas en comparación con las puntuaciones totales (Lai 2014). Se combinó la agitación y la agresión en los metanálisis debido a que lo anterior es compatible con la definición proporcionada por la International Psychogeriatric Association (Cummings 2015); y estos ítems también se combinan en el CMAI ampliamente usado(Cohen‐Mansfield 1986). Algunos han planteado temas conceptuales como la superposición de una definición amplia de agitación con la resistencia a la atención (Volicer 2007).
La calidad del informe a veces fue deficiente lo cual dio lugar a incertidumbre acerca de la calidad metodológica exacta de los estudios incluidos y la evidencia sobre los efectos. La mayoría de los estudios tenían tamaños de la muestra pequeños. Pocos estudios informaron la fidelidad de la ejecución de la intervención con música y otras actividades, o sobre otros aspectos de la evaluación del proceso. La fidelidad de la ejecución a menudo se define como el grado al cual se administra una intervención o programa en la forma prevista (Carroll 2007); y en los ensayos de la musicoterapia específicamente, la fidelidad del tratamiento se refiere a las "estrategias metodológicas usadas para vigilar la administración de la intervención de musicoterapia según se describe en el manual de tratamiento" (Bradt 2012). La fidelidad al tratamiento incluye la adherencia a una intervención, la exposición o la dosis, la calidad de la administración, la respuesta del participante y la diferenciación del programa para identificar los componentes esenciales de la intervención (Carroll 2007), y por lo tanto incluye, pero no está limitado a, la adherencia y la respuesta del participante (o del personal). El informe de la intervención puede mejorarse al usar las guías de informe para la descripción y replicación de las intervenciones.
Algunos de los estudios incluidos seleccionaron a los pacientes con comportamiento agitado antes de la intervención, o a los pacientes que presentaban una mayor probabilidad de estar interesados en las intervenciones con música. Por el contrario, hubo estudios en los cuales se excluyó a los pacientes con conocimiento musical (Raglio 2010b), o sin dichos criterios de selección. La deserción se debió principalmente a condiciones relacionadas con la salud como la hospitalización, la enfermedad o la mortalidad. Se informó la deserción debido a la falta de interés para las actividades control en particular (programa de estimulación cognitiva; Liesk 2015, y mirar televisión; Cho 2016 y la deserción debido a los "problemas en el grupo" en un grupo de intervención con música (Liesk 2015), pero ninguno de los otros estudios informó efectos no favorables de las intervenciones con música. No se sabe si hubo efectos adversos sin informar como dolor de garganta después de cantar o casos de dificultad específicamente relacionada con el tratamiento. Tampoco se sabe si, sin incluir de manera selectiva a los pacientes sobre la base del juicio subjetivo de si probablemente aceptarán la intervención, algunos pacientes con demencia podrían presentar desventajas con la intervención. Posiblemente, los efectos en estos estudios dependen de los participantes con problemas al inicio (que son seleccionados sobre la base de la necesidad de tratamiento para problemas específicos) y en consecuencia de que haya posibilidades apreciables de mejoría. Hay subgrupos específicos que podrían beneficiarse con las intervenciones terapéuticas con música más que otros.
Puede haber sesgo de publicación causado por el informe de resultado selectivo en los informes de los estudios publicados. Aunque se registraron pocos protocolos, se encontraron inconsistencias en el informe de las medidas de resultado en dos estudios (Cooke 2010 – inconsistencia entre los informes múltiples; Hsu 2015 – inconsistencia en comparación con el registro del ensayo). Además, aunque la mayoría de los metanálisis realizados no encontraron efectos estadísticamente significativos, 19 de los 22 estudios informaron al menos un efecto significativo (todos, exceptoLiesk 2015; Raglio 2015; Thornley 2016). Para algunos estudios, lo anterior incluyó resultados más allá del alcance de esta revisión, como la frecuencia cardíaca, pero podría indicar el informe selectivo de los resultados significativos o métodos analíticos que dieron lugar a resultados significativos. Sin embargo, los gráficos en embudo de la ansiedad y la agitación o la agresión (final del tratamiento, los dos resultados evaluados en el número más grande de estudios, con 13 [ansiedad] y 14 estudios [agitación o la agresión]) no sugieren claramente un sesgo de publicación. Puede haber un conflicto de intereses económicos si el estudio es financiado por una fuente interesada en los resultados, o un conflicto de intereses intelectuales en caso de que el estudio sea realizado por el musicoterapeuta que escribe el artículo, pero no hubo datos suficientes para examinar los posibles efectos de los conflictos de intereses.
Sesgos potenciales en el proceso de revisión
Aunque se realizó una búsqueda extensiva en la bibliografía en las bases de datos más comúnmente usadas y relevantes y se realizaron búsquedas manuales minuciosas en las revistas de musicoterapia, aún es posible que se haya omitido uno o más ECA realizados.
Acuerdos y desacuerdos con otros estudios o revisiones
En comparación con otras revisiones, los criterios de inclusión para las intervenciones terapéuticas con música fueron más exclusivos. Se excluyeron los estudios de las intervenciones denominadas "musicoterapia" cuando hubo una indicación insuficiente de que la intervención tenía metas terapéuticas y su administración requería habilidades, o cuando la intervención se combinó con otros tipos de intervenciones. Por el contrario, se incluyeron estudios cuando la profesión o el entrenamiento del terapeuta estaban poco claros si se cumplían los criterios para el tratamiento y la habilidad. Los efectos encontrados pueden ser más moderados que en muchas otras revisiones, pero los análisis de sensibilidad indicaron que lo anterior probablemente no es explicado por el hecho de permitir la inclusión de los estudios no proporcionados, o no proporcionados claramente, por un musicoterapeuta profesional.
Una revisión y metanálisis de los efectos de la musicoterapia sobre los síntomas conductuales y psicológicos de la demencia encontró DME más grandes para los problemas conductuales en general (DME ‐0,49; IC del 95%: ‐0,82 a ‐0,17) y para la ansiedad (DME ‐0,64; IC del 95%: ‐1,05 a ‐0,24) en comparación con los resultados(Ueda 2013). Sin embargo, dicha revisión incluyó ensayos no aleatorios y estudios de cohortes y estudios que se excluyeron debido a que no cumplían con los criterios para las intervenciones terapéuticas. Encontraron un efecto aún más grande para los estudios que se prolongaron tres meses o más (DME ‐0,93; IC del 95%: ‐1,72 a ‐0,13), un subgrupo que no se analizó por separado.
La revisión de Chang 2015 incorporó diez estudios, incluido Raglio 2008, que se excluyó después de la inclusión en una versión anterior de la revisión debido a que después de una nueva evaluación, se consideró un estudio cuasialeatorio, Sung 2006, que después de una nueva evaluación no cumplió con los criterios de una intervención terapéutica basada en música (fue música con movimiento); y Janata 2012; que se excluyó debido a que la transmisión de música tampoco cumplió con los criterios de una intervención terapéutica. Chang 2015 incluyó estudios que realizaban comparaciones con atención habitual, con la exclusión de otras actividades excepto las sesiones de lectura como el comparador(Cooke 2010; Guétin 2009; con referencias erróneas de otro estudio de este grupo en pacientes sin demencia en la unidad de cuidados intensivos). La revisión tuvo un período de búsqueda más largo que 2000 a 2014 y se incluyeron artículos en francés y alemán. Tanto esta revisión como Chang 2015 encontraron heterogeneidad apreciable en los análisis de la ansiedad. Los tamaños del efecto para la cognición fueron más pequeños que para el estado de ánimo en ambas revisiones. Chang 2015 encontró un efecto significativo sobre los “comportamientos disruptivos”. No se encontró un efecto sobre la agitación o la agresión, pero se encontró un efecto pequeño sobre los problemas conductuales en general. Las escalas empleadas para evaluar los problemas conductuales, sin embargo, incluyeron ítems del estado de ánimo. Se encontró un efecto sobre la depresión, que Chang 2015 no encontró, a pesar de un tamaño del efecto algo más grande que en esta revisión (Chang 2015: ‐0,39; esta revisión: ‐0,28).
Una revisión de Zhang 2017 incluyó estudios no aleatorios y estudios que aquí se excluyeron debido a las metas terapéuticas insuficientes y sus métodos, y los resultados difirieron de algunas otras maneras. Sus análisis de subgrupos para el efecto en el “comportamiento disruptivo” (escalas conductuales generales y agitación) sugirieron una DME mayor para los estudios no aleatorios (‐1,02 para los estudios no aleatorios versus ‐0,65 [informado en el texto] o ‐0,52 [informado en la tabla] para los ECA paralelos). Encontraron una DME más grande para el comportamiento disruptivo (‐0,42; IC del 95%: ‐0,74 a ‐0,11; en comparación con ‐0,23 para los problemas conductuales en general y ‐0,07 para la agitación o la agresión en este trabajo). En comparación con la revisión (DME ‐0,15), encontraron una DME similar o algo más grande para la cognición (DME 0,20; IC del 95%: ‐0,09 a 0,49), y DME más pequeñas para la ansiedad (DME ‐0,20; IC del 95%: ‐0,37 a ‐0,02), la depresión (DME ‐0,16; IC del 95%: ‐0,41 a 0,08) y la calidad de vida (DME ‐0,12; ‐0,36 a 0,12; sin embargo, las DME negativas favorecieron la musicoterapia). Zhang 2017 realizó análisis diferentes, que probablemente compararon las puntuaciones de antes y después de la intervención para calcular una DME con un control general de si había diferencias iniciales. Lo anterior puede explicar las diferentes DME también para los estudios individuales, y las evaluaciones de la calidad de los mismos estudios incluidos rara vez se correspondieron con la revisión. Por ejemplo, Svansdottir 2006 fue un valor atípico para el efecto sobre el comportamiento en Zhang 2017 (DME ‐3,88), en comparación con una DME de ‐0,06 para las puntuaciones del final del tratamiento en este trabajo. Además, en este caso, Zhang 2017 asignó puntos para la calidad debido al cegamiento del terapeuta mientras que aquí todos los estudios se consideraron en alto riesgo de sesgo de realización (en vista de los métodos estandarizados para permitir la comparación de intervenciones y situaciones muy diferentes) y en este caso, Svansdottir 2006 también reveló que el primer autor "realizó la musicoterapia". Zhang 2017 consideró que todos los estudios fueron de calidad aceptable, incluso los que presentaron una puntuación total de 3 (informada en la tabla suplementaria) o mayor que 4 (informada en el texto) en una escala de 0 a 10 en la que uno de los ítems fue la asignación al azar. Finalmente, los resultados secundarios (depresión, ansiedad y calidad de vida) se priorizaron en esta revisión debido a la importancia evidente para el paciente con demencia.
Múltiples revisiones han resumido los efectos y han establecido la conclusión, a menudo sin metanálisis, de que una intervención terapéutica con música o la musicoterapia puede ser beneficiosa. Algunos se centraron en resultados específicos como los síntomas conductuales y psicológicos de la demencia (p.ej. Raglio 2012); o cubrieron tipos diferentes de resultados como los resultados fisiológicos (p.ej. McDermott 2013, que también observó una falta de evidencia sobre los efectos a largo plazo). Petrovsky 2015 se centró en los efectos sobre la ansiedad y la depresión en los pacientes con demencia leve, pero incluyó estudios con participantes con demencia de gravedad variable mientras que no estuviera limitado a la demencia grave. Concluyeron que, sobre la base de diez estudios, incluidos algunos con un diseño de pre–posprueba, la evidencia no fue concluyente. Fue posible incluir más ECA debido a que los autores proporcionaron datos acerca de la agitación y los ítems del estado de ánimo en las escalas conductuales generales. Ing‐Randolph 2015 examinó los efectos de las intervenciones grupales con música, incluida la musicoterapia, en la ansiedad. Encontraron que las intervenciones con música redujeron la ansiedad en siete de ocho estudios incluidos.
La importancia clínica del efecto de las intervenciones con música sobre la depresión es algo incierta debido a la variedad de escalas usadas, aunque no hubo heterogeneidad en los efectos entre los estudios. La DME para la depresión de ‐0,27 y de la ansiedad de ‐0,43 (pero incierto debido al riesgo grave de sesgo y la inconsistencia) estuvo dentro del rango, o fue más grande, de las estimaciones agrupadas de los efectos de la medicación sobre la depresión en los pacientes con demencia (antidepresivos, seis ensayos, DME a favor de la medicación 0,29; IC del 95%: 0,02 a 0,60; Nelson 2011; inhibidores selectivos de la recaptación de serotonina, 12 ensayos, tamaños del efecto a favor de la medicación 0,06 a 0,10; Sepehry 2012). Puede haber habido menos efectos adversos de las intervenciones terapéuticas con música en comparación con medicación.
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
Funnel plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.3 Negative affect or mood disturbances: anxiety (13 studies, 15 dots because 2 studies used 2 control groups, 1 with usual care and 1 with other activities).
Funnel plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.4 Problematic behaviour: agitation or aggression (14 studies, 16 dots because 2 studies used 2 control groups, 1 with usual care and 1 with other activities).
Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.1 Emotional well‐being and quality of life. CI: confidence interval; SD: standard deviation.
Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.2 Negative affect or mood disturbances: depression. BEHAVE‐AD: Behavioural Pathology in Alzheimer's Disease; NPI: Neuropsychiatric Inventory; SD: standard deviation.
Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.3 Negative affect or mood disturbances: anxiety. BEHAVE‐AD: Behavioural Pathology in Alzheimer's Disease; NPI: Neuropsychiatric Inventory; SD: standard deviation; STAI‐A: State‐Trait Anxiety Inventory for Adults.
Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.4 Problematic behaviour: agitation or aggression. BEHAVE‐AD: Behavioural Pathology in Alzheimer's Disease; CI: confidence interval; CMAI: Cohen‐Mansfield Agitation Inventory; NPI: Neuropsychiatric Inventory; SD: standard deviation.
Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.5 Problematic behaviour overall. NPI: Neuropsychiatric Inventory; SD: standard deviation.
Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.6 Social behaviour: music vs other activities. SD: standard deviation.
Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.7 Cognition. MMSE: Mini‐Mental State Examination; SD: standard deviation; SIB: Severe Impairment Battery.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 1 Emotional well‐being including quality of life.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 2 Mood disturbance or negative affect: depression.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 3 Mood disturbance or negative affect: anxiety.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 4 Behaviour problems: agitation or aggression.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 5 Behaviour problems: overall.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 6 Social behaviour: music vs other activities.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 7 Cognition.

Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 1 Emotional well‐being including quality of life.

Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 2 Mood disturbance or negative affect: depression.

Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 3 Mood disturbance or negative affect: anxiety.

Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 4 Behavioural problems: agitation or aggression.

Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 5 Behavioural problems: overall.

Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 6 Social behaviour: music versus other activities.
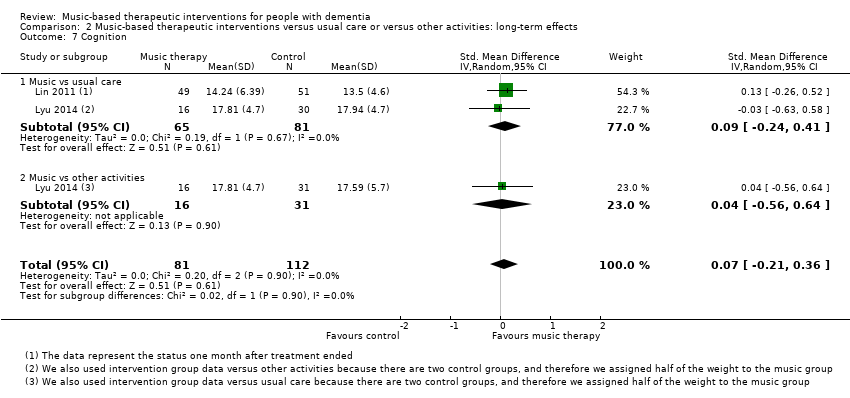
Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 7 Cognition.
| Music‐based therapeutic interventions compared to usual care or other activities for people with dementia: end‐of‐treatment effects | |||
| Patient or population: people with dementia (all resided in institutional settings) | |||
| Outcomes (end of treatment) measured with a variety of scales except for social behaviour | Anticipated absolute effects, SMD* (95% CI) | № of participants | Quality of the evidence |
| Score with music therapy compared with usual care or other activities | |||
| Emotional well‐being including quality of life | The score in the intervention group was 0.32 SDs higher | 348 | ⊕⊕⊝⊝ |
| Mood disturbance or negative affect: depression | The score in the intervention group was 0.27 SDs lower | 503 | ⊕⊕⊕⊝ |
| Mood disturbance or negative affect: anxiety | The score in the intervention group was 0.43 SDs lower | 478 | ⊕⊕⊝⊝ |
| Behavioural problems: agitation or aggression | The score in the intervention group was 0.07 SDs lower | 626 | ⊕⊕⊕⊝ |
| Behavioural problems: overall | The score in the intervention group was 0.23 SDs lower | 442 | ⊕⊕⊕⊝ |
| Social behaviour: music vs other activities | The score in the intervention group was 0.54 SDs higher | 70 | ⊕⊝⊝⊝ |
| Cognition | The score in the intervention group was 0.15 SDs higher | 350 | ⊕⊕⊝⊝ |
| *Interpretation of SMD: a difference of < 0.40 SDs can be regarded as a small effect, 0.40–0.70 a moderate effect, and > 0.70 a large effect. CI: confidence interval; SMD: standardised mean difference; SD: standard deviation. | |||
| GRADE Working Group grades of evidence (GradePro) | |||
| aRisk of bias: no blinding of therapists and participants (not possible), and often no or unclear blinding of outcome assessment. bImprecision: small number of participants and broad CI. cRisk of bias: no blinding of therapists and participants (not possible), and sometimes no or unclear blinding of outcome assessment. dInconsistency: more non‐overlapping CIs. eImprecision: very small number of participants and broad CIs. fImprecision: small number of participants. | |||
| Music‐based therapeutic interventions compared to usual care or other activities for people with dementia: long‐term effects (scores 4 weeks or more after treatment ended) | |||
| Patient or population: people with dementia (all resided in institutional settings) | |||
| Outcomes (long‐term) measured with a variety of scales except for social behaviour | Anticipated absolute effects, SMD* (95% CI) | № of participants | Quality of the evidence |
| Score with music therapy compared with usual care or other activities | |||
| Emotional well‐being including quality of life | The score in the intervention group was 0.34 SDs higher | 180 | ⊕⊕⊝⊝ |
| Mood disturbance or negative affect: depression | The score in the intervention group was 0.03 SDs lower | 354 | ⊕⊕⊝⊝ |
| Mood disturbance or negative affect: anxiety | The score in the intervention group was 0.28 SDs lower | 265 | ⊕⊝⊝⊝ |
| Behavioural problems: agitation or aggression | The score in the intervention group was 0.10 SDs lower | 330 | ⊕⊕⊝⊝ |
| Behavioural problems: overall | The score in the intervention group was 0.19 SDs lower | 351 | ⊕⊕⊝⊝ |
| Social behaviour: music vs other activities | The score in the intervention group was 0.53 SDs higher | 48 | ⊕⊝⊝⊝ |
| Cognition | The score in the intervention group was 0.07 SDs higher | 193 | ⊕⊕⊝⊝ |
| *Interpretation of SMD: a difference of < 0.40 SDs can be regarded as a small effect, 0.40–0.70 a moderate effect, and > 0.70 a large effect. CI: confidence interval; SMD: standardised mean difference; SD: standard deviation. | |||
| GRADE Working Group grades of evidence (GradePro) | |||
| aRisk of bias: no blinding of therapists and participants (not possible), and sometimes no or unclear blinding of outcome assessment. bImprecision: small number of participants and broad CIs includes both benefit and harm. cImprecision: small number of participants. dRisk of bias: no blinding of therapists and participants (not possible). eInconsistency: non‐overlapping CIs. fImprecision: small number of participants and broad CIs includes both benefit and harm. gImprecision: very small number of participants and very broad CIs includes both benefit and harm. hRisk of bias: no blinding of therapists and participants (not possible), and unclear blinding of outcome assessment. | |||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Emotional well‐being including quality of life Show forest plot | 9 | 348 | Std. Mean Difference (IV, Random, 95% CI) | 0.32 [0.02, 0.62] |
| 1.1 Music vs usual care | 3 | 113 | Std. Mean Difference (IV, Random, 95% CI) | 0.47 [‐0.30, 1.25] |
| 1.2 Music vs other activities | 7 | 235 | Std. Mean Difference (IV, Random, 95% CI) | 0.30 [‐0.04, 0.64] |
| 2 Mood disturbance or negative affect: depression Show forest plot | 11 | 503 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.27 [‐0.45, ‐0.09] |
| 2.1 Music vs usual care | 6 | 307 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.28 [‐0.53, ‐0.04] |
| 2.2 Music vs other activities | 6 | 196 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.23 [‐0.52, 0.06] |
| 3 Mood disturbance or negative affect: anxiety Show forest plot | 13 | 478 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.43 [‐0.72, ‐0.14] |
| 3.1 Music vs usual care | 6 | 237 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.22 [‐0.48, 0.04] |
| 3.2 Music vs other activities | 9 | 241 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.63 [‐1.13, ‐0.12] |
| 4 Behaviour problems: agitation or aggression Show forest plot | 14 | 626 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐0.24, 0.10] |
| 4.1 Music vs usual care | 10 | 458 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.10 [‐0.31, 0.11] |
| 4.2 Music vs other activities | 6 | 168 | Std. Mean Difference (IV, Random, 95% CI) | 0.01 [‐0.31, 0.32] |
| 5 Behaviour problems: overall Show forest plot | 10 | 442 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.23 [‐0.46, ‐0.01] |
| 5.1 Music vs usual care | 7 | 251 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.40 [‐0.71, ‐0.10] |
| 5.2 Music vs other activities | 6 | 191 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.02 [‐0.32, 0.28] |
| 6 Social behaviour: music vs other activities Show forest plot | 3 | 70 | Std. Mean Difference (IV, Random, 95% CI) | 0.54 [0.06, 1.02] |
| 7 Cognition Show forest plot | 7 | 350 | Std. Mean Difference (IV, Random, 95% CI) | 0.15 [‐0.06, 0.36] |
| 7.1 Music vs usual care | 4 | 216 | Std. Mean Difference (IV, Random, 95% CI) | 0.18 [‐0.09, 0.45] |
| 7.2 Music vs other activities | 4 | 134 | Std. Mean Difference (IV, Random, 95% CI) | 0.10 [‐0.25, 0.44] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Emotional well‐being including quality of life Show forest plot | 4 | 180 | Std. Mean Difference (IV, Random, 95% CI) | 0.34 [‐0.12, 0.80] |
| 1.1 Music vs usual care | 2 | 72 | Std. Mean Difference (IV, Random, 95% CI) | 0.91 [‐0.85, 2.67] |
| 1.2 Music vs other activities | 3 | 108 | Std. Mean Difference (IV, Random, 95% CI) | 0.18 [‐0.22, 0.58] |
| 2 Mood disturbance or negative affect: depression Show forest plot | 6 | 354 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.03 [‐0.24, 0.19] |
| 2.1 Music vs usual care | 4 | 233 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.02 [‐0.28, 0.24] |
| 2.2 Music vs other activities | 3 | 121 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.04 [‐0.41, 0.33] |
| 3 Mood disturbance or negative affect: anxiety Show forest plot | 6 | 265 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.28 [‐0.71, 0.15] |
| 3.1 Music vs usual care | 3 | 141 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.06 [‐0.48, 0.37] |
| 3.2 Music vs other activities | 4 | 124 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.53 [‐1.31, 0.25] |
| 4 Behavioural problems: agitation or aggression Show forest plot | 5 | 330 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.10 [‐0.33, 0.13] |
| 4.1 Music vs usual care | 4 | 241 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.42, 0.09] |
| 4.2 Music vs other activities | 2 | 89 | Std. Mean Difference (IV, Random, 95% CI) | 0.10 [‐0.66, 0.86] |
| 5 Behavioural problems: overall Show forest plot | 6 | 351 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.19 [‐0.51, 0.14] |
| 5.1 Music vs usual care | 5 | 207 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.32 [‐0.85, 0.21] |
| 5.2 Music vs other activities | 3 | 144 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.44, 0.25] |
| 6 Social behaviour: music versus other activities Show forest plot | 2 | 48 | Std. Mean Difference (IV, Random, 95% CI) | 0.53 [‐0.53, 1.60] |
| 6.1 Music vs usual care | 0 | 0 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 6.2 Music vs other activities | 2 | 48 | Std. Mean Difference (IV, Random, 95% CI) | 0.53 [‐0.53, 1.60] |
| 7 Cognition Show forest plot | 2 | 193 | Std. Mean Difference (IV, Random, 95% CI) | 0.07 [‐0.21, 0.36] |
| 7.1 Music vs usual care | 2 | 146 | Std. Mean Difference (IV, Random, 95% CI) | 0.09 [‐0.24, 0.41] |
| 7.2 Music vs other activities | 1 | 47 | Std. Mean Difference (IV, Random, 95% CI) | 0.04 [‐0.56, 0.64] |