Intervenciones terapéuticas con música para los pacientes con demencia
Appendices
Appendix 1. Sources searched and search strategies used (2010 to 2017)
| Source searched | Search strategy | Hits |
| MEDLINE In‐process and other non‐indexed citations and MEDLINE 1950 to present [Most recent search performed: 19 June 2017] | 1. exp Dementia/ 2. Delirium/ 3. Wernicke Encephalopathy/ 4. Delirium, Dementia, Amnestic, Cognitive Disorders/ 5. dement*.mp. 6. alzheimer*.mp. 7. (lewy* adj2 bod*).mp. 8. deliri*.mp. 9. (chronic adj2 cerebrovascular).mp. 10. ("organic brain disease" or "organic brain syndrome").mp. 11. ("normal pressure hydrocephalus" and "shunt*").mp. 12. "benign senescent forgetfulness".mp. 13. (cerebr* adj2 deteriorat*).mp. 14. (cerebral* adj2 insufficient*).mp. 15. (pick* adj2 disease).mp. 16. (creutzfeldt or jcd or cjd).mp. 17. huntington*.mp. 18. binswanger*.mp. 19. korsako*.mp. 20. or/1‐19 21. music*.mp. 22. exp Music Therapy/ 23. singing.mp. 24. sing.mp. 25. "auditory stimul*".mp. 26. piano.mp. 27. or/21‐26 28. 27 and 20 29. randomized controlled trial.pt. 30. controlled clinical trial.pt. 31. random*.ab. 32. placebo.ab. 33. trial.ab. 34. groups.ab. 35. or/29‐34 36. (animals not (humans and animals)).sh. 37. 35 not 36 38. 28 and 37 39. (2008* or 2009* or 2010*).ed. 40. 38 and 39 | Apr 2010: 15 Oct 2014: 59 Jul 2015: 15 Apr 2016: 36 Jun 2017: 47 |
| Embase 1980 to 2010 week 14 [Most recent search performed: 19 June 2017] | 1. exp dementia/ 2. Lewy body/ 3. delirium/ 4. Wernicke encephalopathy/ 5. cognitive defect/ 6. dement*.mp. 7. alzheimer*.mp. 8. (lewy* adj2 bod*).mp. 9. deliri*.mp. 10. (chronic adj2 cerebrovascular).mp. 11. ("organic brain disease" or "organic brain syndrome").mp. 12. "supranuclear palsy".mp. 13. ("normal pressure hydrocephalus" and "shunt*").mp. 14. "benign senescent forgetfulness".mp. 15. (cerebr* adj2 deteriorat*).mp. 16. (cerebral* adj2 insufficient*).mp. 17. (pick* adj2 disease).mp. 18. (creutzfeldt or jcd or cjd).mp. 19. huntington*.mp. 20. binswanger*.mp. 21. korsako*.mp. 22. CADASIL.mp. 23. or/1‐22 24. music*.mp. 25. exp music therapy/ 26. singing.mp. 27. sing.mp. 28. exp singing/ 29. "auditory stimul*".mp. 30. exp auditory stimulation/ 31. piano.mp. 32. or/24‐31 33. 23 and 32 34. randomized controlled trial/ 35. exp controlled clinical trial/ 36. random*.ab. 37. placebo.ab. 38. trial.ab. 39. groups.ab. 40. or/34‐39 41. 33 and 40 42. (2008* or 2009* or 2010*).em. 43. 41 and 42 | Apr 2010: 28 Oct 2014: 230 Jul 2015: 42 Apr 2016: 106 Jun 2017: 101 |
| PsycINFO 1806 to April week 1 2010 [Most recent search performed: 19 June 2017] | 1. exp Dementia/ 2. exp Delirium/ 3. exp Huntingtons Disease/ 4. exp Kluver Bucy Syndrome/ 5. exp Wernickes Syndrome/ 6. exp Cognitive Impairment/ 7. dement*.mp. 8. alzheimer*.mp. 9. (lewy* adj2 bod*).mp. 10. deliri*.mp. 11. (chronic adj2 cerebrovascular).mp. 12. ("organic brain disease" or "organic brain syndrome").mp. 13. "supranuclear palsy".mp. 14. ("normal pressure hydrocephalus" and "shunt*").mp. 15. "benign senescent forgetfulness".mp. 16. (cerebr* adj2 deteriorat*).mp. 17. (cerebral* adj2 insufficient*).mp. 18. (pick* adj2 disease).mp. 19. (creutzfeldt or jcd or cjd).mp. 20. huntington*.mp. 21. binswanger*.mp. 22. korsako*.mp. 23. ("parkinson* disease dementia" or PDD or "parkinson* dementia").mp. 24. or/1‐23 25. music*.mp. 26. exp Music Therapy/ 27. sing.mp. 28. singing.mp. 29. exp Singing/ 30. "auditory stimul*".mp. 31. *Auditory Stimulation/ 32. piano.mp. 33. or/25‐32 34. 24 and 33 35. exp Clinical Trials/ 36. random*.ti,ab. 37. trial.ti,ab. 38. group.ab. 39. placebo.ab. 40. or/35‐39 41. 34 and 40 42. (2008* or 2009* or 2010*).up. 43. 41 and 42 | Apr 2010: 26 Oct 2014: 100 Jul 2015: 14 Apr 2016: 34 Jun 2017: 35 |
| CINAHL [Most recent search performed: 19 June 2017] | S1 (MH "Dementia+") S2 (MH "Delirium") or (MH "Delirium, Dementia, Amnestic, Cognitive Disorders") S3 (MH "Wernicke's Encephalopathy") S4 TX dement* S5 TX alzheimer* S6 TX lewy* N2 bod* S7 TX deliri* S8 TX chronic N2 cerebrovascular S9 TX "organic brain disease" or "organic brain syndrome" S10 TX "normal pressure hydrocephalus" and "shunt*" S11 TX "benign senescent forgetfulness" S12 TX cerebr* N2 deteriorat* S13 TX cerebral* N2 insufficient* S14 TX pick* N2 disease S15 TX creutzfeldt or jcd or cjd S16 TX huntington* S17 TX binswanger* S18 TX korsako* S19 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10 or S11 or S12 or S13 or S14 or S15 or S16 or S17 or S18 S20 TX music* S21 (MH "Music Therapy") or (MH "Music Therapy (Iowa NIC)") S22 TX sing S23 TX singing S24 (MM "Singing") S25 TX "auditory stimul*" S26 (MM "Acoustic Stimulation") S27 S20 or S21 or S22 or S23 or S24 or S25 or S26 S28 S19 and S27 S29 (MH "Clinical Trials+") S30 AB random* S31 AB trial S32 AB placebo S33 AB group* S34 S29 or S30 or S31 or S32 or S33 S35 S28 and S34 S36 EM 2008 S37 EM 2009 S38 EM 2010 S39 S36 or S37 or S38 S40 S35 and S39 | Apr 2010: 18 Oct 2014: 53 Jul 2015: 8 Apr 2016: 12 Jun 2017: 20 |
| Web of Science with Conference Proceedings (1945 to present) [Most recent search performed: 19 June 2017] | Topic=(music* OR singing OR sing OR "auditory stimul*") AND Topic=(dement* OR alzheimer* OR "lew* bod*" OR huntington*) AND Topic=(random* OR trial OR placebo OR "double blind*" OR "single blind*" OR groups) Timespan=2008‐2010. Databases=SCI‐EXPANDED, A&HCI, SSCI, CPCI‐S | Apr 2010: 33 Oct 2014: 205 Jul 2015: 20 Apr 2016: 76 Jun 2017: 45 |
| LILACS [Most recent search performed: 19 June 2017] | demen$ [Words] and music OR singing [Words] | Apr 2010: 7 Oct 2014: 12 Jul 2015: 0 Apr 2016: 0 Jun 2017: 0 |
| ALOIS [Most recent search performed: 19 June 2017] | Advanced search: [study aim: Treatment Dementia] AND [study design: RCT OR CCT] AND [intervention (contains any): music OR singing OR auditory) | Apr 2010: 29 Oct 2014: 18 Jul 2015: 0 Apr 2016: 6 Jun 2017: 0 |
| UMIN (Clinical Trial Register of Japan) [Most recent search performed: 19 June 2017] | Free Keyword: music OR singing OR auditory | Apr 2010: 0 Oct 2014: 0 Jul 2015: 0 Apr 2016: 0 Jun 2017: 0 |
| CENTRAL [Most recent search performed: 19 June 2017] | #1 MeSH descriptor Dementia explode all trees #2 MeSH descriptor Delirium, this term only #3 MeSH descriptor Wernicke Encephalopathy, this term only #4 MeSH descriptor Delirium, Dementia, Amnestic, Cognitive Disorders, this term only #5 dement* #6 alzheimer* #7 "lewy* bod*" #8 deliri* #9 "chronic cerebrovascular" #10 "organic brain disease" or "organic brain syndrome" #11 "normal pressure hydrocephalus" and "shunt*" #12 "benign senescent forgetfulness" #13 "cerebr* deteriorat*" #14 "cerebral* insufficient*" #15 "pick* disease" #16 creutzfeldt or jcd or cjd #17 huntington* #18 binswanger* #19 korsako* #20 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19) #21 MeSH descriptor Music Therapy explode all trees #22 music* #23 singing #24 sing #25 "auditory stimul*" #26 (#21 OR #22 OR #23 OR #24 OR #25) #27 (#20 AND #26), from 2008 to 2010 | Apr 2010: 10 Oct 2014: 53 Jul 2015: 11 Apr 2016: 9 Jun 2017: 38 |
| ClincalTrials.gov [Most recent search performed: 19 June 2017] | dementia OR alzheimer OR alzheimers OR alzheimer's | music OR sing OR singing OR auditory | received from 01/01/2008 to 04/14/2010 | Apr 2010: 2 Oct 2014: 14 Jul 2015: 0 Apr 2016: 0 Jun 2017: 0 |
| ICTRP Search Portal (WHO portal) [Most recent search performed: 19 June 2017] | Advanced search: [condition: Dementia OR alzheimer OR alzheimers] AND [Intervention: music OR singing OR sing OR auditory] AND [date registration: 01/01/08 to 14/04/10] | Apr 2010: 20 Oct 2014: 18 Jul 2015: 0 Apr 2016: 3 Jun 2017: 0 |
| TOTAL | Apr 2010: 188 Oct 2014: 761 Jul 2015: 110 Apr 2016: 282 Jun 2017: 286 TOTAL: 1627 | |
Appendix 2. Description of the interventions
Ceccato 2012
Music‐based therapeutic intervention: sound training for attention and memory in dementia (STAM‐Dem) (versus a control group of usual care)
Experimental group
A 45‐minute mixed (active and receptive) group intervention delivered by "professionally trained music therapists trained to administer the STAM‐Dem protocol." Highly structured, progressive series music sessions, with a minimum of four and a maximum of five participants per group. The music therapists were instructed to "pay attention to the relational atmosphere" and "maintain the level of motivation as high as possible."
The intervention included "step‐by‐step exercises aimed at stimulating and checking both attention and memory." Participants were asked to perform specific movements, count, clap hands, alternate clapping hands and tapping the table, repeat sequences of previously recorded sounds (not stated how) after listening to recorded and live played music. It was a mixed intervention because the active component was combined with listening to music.
The STAM‐Dem protocol comprises four phases, one for each specific cognitive function that is trained (selective attention, sustained attention, alternate attention and working memory). The phases involve: 1. stimulus‐movement association, 2. reaction to acoustic stimuli, 3. shifting attention with two exercises, and 4. orderly and inverted repetition. It is not clear from the text if the phases each last four sessions, and are progressive, but as described in other sources (not cited in the article) they are (STAM protocol). Each phase then lasts four sessions and is followed by the next. However, the intervention phase lasted 12 weeks, in which 24 sessions were held.
Control group
Usual care.
Cho 2016
Music‐based therapeutic intervention: active group singing (versus two control groups, music listening and television)
Experimental group
A 40‐minute active group music therapy which consisted of singing songs that reflected participants' preferences with regard to music genres, songs and musicians. Eight lists of songs for the music therapy‐singing group were developed centred around a different theme for each session (country, rat pack, the moon, world war II, Broadway, 1950s and 1960s, autumn and patriotic). A board‐certified music therapist with 15 years of experience in dementia care delivered the intervention in a separate room. The sessions were delivered twice a week for 4 weeks.
Control group 1
A 40‐minute music listening session in which participants listened to a CD which contained almost the same songs and order of the songs sung in the music therapy singing group (but, the latter sessions, for example, always concluded with "Show me the way to go home" which was not on the CD). The nursing home activity assistants who delivered this intervention were instructed to lead the group in the same manner as other activities and to validate and process the participants' responses.
Control group 2
A 40‐minute session in which participants watched a DVD of a comedy program ("I Love Lucy"). The intervention was facilitated by nursing home activity assistants who validated any spontaneous responses.
Clark 1998
Music‐based therapeutic intervention: preferred, recorded music during bathing episodes with aggressive behaviour (versus a control group with no music during bathing)
Experimental group
A receptive individual intervention with music, listening through speakers, delivered by nursing staff. Duration followed established nursing routines and varied from 11 to 18 minutes.
Preferred music was recorded and selections played via an audiotape recorder during the bathing episode. Background information on participants' music experiences and preferences was obtained by interviews with the family member or responsible agent. "Bathing times were scheduled for either morning or afternoon" "following established nursing routines." Participants received either a partial bath which was given in the participant's room, or a full bath, which was given in the shower on the nursing unit.
Nursing staff delivered the bathing session. It was not clear from the text whether nursing staff were responsible for turning on the music, but it is highly probable that this was done by the observer: "Initially, consideration was given to having nursing staff be responsible for turning on the audiotape recorder...However, during pilot testing of the procedures, this proved too cumbersome for already overburdened nursing staff." The sessions were given 10 times over two weeks.
Control group
No music during bathing.
Cooke 2010
Music‐based therapeutic intervention: active group music sessions with live and recorded music (versus a reading group as the control condition)
Experimental group
An active, structured 40‐minute group music session delivered by two musicians. The session consisted of singing and playing on instruments accompanied by live familiar songs and recorded instrumental music. The group had a maximum of 16 participants.
The session covered 30 minutes of musician‐led familiar song‐singing with guitar accompaniment, and 10 minutes of prerecorded instrumental music. A set repertoire was established for each of three sessions and this was repeated for eight weeks.
"Residents were encouraged to participate actively through singing/humming, playing instruments and… movement." Choice of the instruments was not described. The repertoire selection was based primarily on participants' musical preferences, musicians' repertoire knowledge and the findings from a practice session (conducted in an alternative aged care setting). The 10 minutes of listening to prerecorded music allowed the musicians and participants to have a short rest from performance and singing and to cater for participants who had a preference for more instrumental music. The sessions were delivered three mornings a week (Monday, Wednesday and Friday) for eight weeks, with a total of 24 sessions.
Control group
An interactive reading session included a range of reading and social activities, such as reading local news stories, short stories, telling jokes and undertaking quiz activities. The sessions were led by one trained research assistant. A maximum number of attendees was not clear from the text. The control sessions took 40 minutes, and were delivered three times a week (Monday, Wednesday and Friday) for eight weeks, totalling 24 sessions.
Guétin 2009
Music‐based therapeutic intervention: individual receptive therapy with the 'U' sequence method (versus a reading group as the control condition)
Experimental group
An individual receptive music therapy method, the 'U‐sequence' method involved listening to music sequences, selected from a limited number of musical styles delivered through headphones, in the patient's room. The musical style was chosen based on the participants' personal tastes following an interview or questionnaire. From the suggested different musical styles, a musical sequence was selected. This usual musical sequence, lasting 20 minutes, was broken down into several phases, according to the 'U sequence' method and making use of a computer program especially designed for this method. Musical rhythm, orchestral formation, frequency and volume were reduced. After a phase of sustained reduced musical rhythm, orchestral formation, frequency and volume, a re‐enlivening phase followed in which musical rhythm, orchestral formation, frequency and volume increased again, and ended at a moderate level in comparison to the beginning phase. The style of music varied from one session to another for a given patient.
"Patients were either in a supine position or seated in a comfortable armchair and were offered a mask so as to avoid visual stimuli." Details on the 'U sequence' method are retrievable through this external link (not included in the paper): www.music‐care.com/en/page/treatment.
Sessions were extended by a period of time spent listening to the participant. This period of time served "to create a 'psychotherapist'‐type of therapeutic relationship and …reinforced the effect triggered by listening to music." Duration of this 'listening' intervention with a therapist was not reported.
Personnel delivering the music and the listening intervention was not clear from the text. Sessions were delivered once a week, lasted 20 minutes (plus time spent listening to patients' responses – duration of which is not stated), and 16 sessions were delivered.
Control group
"Rest and reading under the same conditions and at the same intervals."
Hsu 2015
Music‐based therapeutic intervention: active individual music therapy for people with dementia and their carers (versus a control group of usual care)
Experimental group
A 30‐minute individual active music therapy which consisted of singing well‐known songs, instrumental improvisation, talking to allow reminiscence and expression of feelings, and use of facial and bodily expressions of the music therapists combined with a weekly 15‐minute video presentation to direct care staff as an ongoing training tool focused on improving staff knowledge of their patients and confidence and skills to interact.
A music therapist delivered the intervention in a separate, quiet room on the unit. The two qualified music therapists had at least two years' experience working in this setting and were registered with the Health and Care Professions Council (HCPC). To provide consistency and to maintain the therapeutic relationship, residents received all sessions from the same music therapist. The sessions were delivered once a week for five months, in addition to standard care.
Control group
Received standard care for five months. This consisted of medical and personal care, provision of basic needs and activities carried out as usual within the home such as chaplaincy services, entertainment and leisure activities).
Liesk 2015
Music‐based therapeutic intervention: a 'Musikgeragogik' group music programme (versus a cognitive stimulation intervention as the control condition)
Experimental group
A 90‐minute structured active group music intervention based on the principles of 'Musikgeragogik' by T Hartogh (2005) which was designated as "music education for elders." Sessions consisted of singing folk songs, rounds and playing on instruments (woodblocks, bells, tambourine and maracas). Participants were stimulated to improvise in a structured way according to cues in the song lyrics, alternated with spontaneous expression of individual impressions provoked by the songs that were played or sung. It is probable that the music used was live as the music intervention was "created as an active therapy form," but this was not explicitly mentioned in the text.
A music recreational therapist ('Musikgeragogin') delivered the intervention. Duration of sessions was 90 minutes and frequency was twice a week, during six weeks, totalling 12 sessions.
Control group
A cognitive stimulation programme in which cognitive function is trained through quiz questions of differing complexity and theme‐focused conversations, a Cognitive training programme of NEUROvitalis from a group in Cologne, adapted for people with dementia. A gerontologist delivered the intervention. The sessions lasted 90 minutes, twice a week over six weeks, totalling 12 sessions.
Lin 2011
Music‐based therapeutic intervention: group music therapy (versus a control group of usual care that "continued to perform their usual daily activities")
Experimental group
This was a 30‐minute structured mixed group music therapy intervention, based on the protocol developed by Clair 1990. The size of the group is not clear from the text.
The intervention consisted of rhythmic music and slow‐tempo instrumental activities (choice of instruments not specified), therapeutic singing, listening to specially selected music, glockenspiel playing and musical activities and traditional holiday and 'music creator' activities. "…before the therapy sessions a subject's fondness for music was evaluated through an interview, and the musical activities in the group sessions were arranged according to the interview findings."
The person delivering the intervention was a researcher schooled in two university music therapy courses. The sessions lasted 30 minutes and were conducted twice a week for six consecutive weeks. The total number of sessions was 12.
Control group
Participants received usual care and "continued to perform their usual daily activities."
Lord 1993
Music‐based therapeutic intervention: mixed music programme (versus two control groups, jigsaw puzzle activities and a control group of usual care)
Experimental group
A 30‐minute mixed group music intervention, during which music of the "Big Bands" of the 1920s and 1930s were played. It is not clear if the music used was repeated every session or varied from session to session. The group had a size of 20 participants. Active music making (on triangles and tambourines) and singing was possible. It is not clear to what degree active music‐making was stimulated by personnel or depended on participants' initiative only.
Personnel delivering the session was an "activities specialist" and two nurses. Sessions were delivered six times per week and continued for six months, therefore totalling 156 sessions.
Control group 1
Participants were given several puzzle‐play activities (cardboard jigsaw cutouts and pegboard puzzles), new puzzles were introduced periodically.
Control group 2
Participants received the usual recreational activities of drawing, painting and watching television.
Lyu 2014
Music‐based therapeutic intervention: active group music therapy (versus a reading control condition and a control group of usual care)
Experimental group
A 30‐minute group active music intervention consisting of the singing of familiar songs. The participants learnt to sing the songs, or sang after the therapists. Classical and soothing old songs familiar to most participants were selected. A qualified music therapist delivered the intervention daily for three months.
Control group 1
The reading of familiar lyrics without music, supervised by a music therapist.
Control group 2
Participants received care as usual.
Narme 2012
Music‐based therapeutic interventions: group music programme (versus the control condition of art therapy in study 1, and versus cooking in study 2)
Study 1: experimental group
A two‐hour structured mixed group intervention, with a maximum of 12 participants. Music selections were chosen independent of participants' preference and were played through a loudspeaker. The selections varied from classical music to songs from the 1950s and included instrumental and vocal music, and varied from 'calming' to 'dynamic' music. Calming music was used at the start and end of each session. The order of the musical selections was the same for every session, and pieces were played twice if participants expressed the wish to hear a song again. Participants were encouraged to play along (on percussion instruments, maracas or bell chains), sing and improvise. Participants were stimulated to express their feeling and memories evoked by the activity.
Study 1: control group
The control intervention in study 1 was another pleasant art therapy intervention. Painting session offered participants the use of wax crayons, colouring pencils, felt pens and gouache painting. They were stimulated to create simple drawings, to make circular movements with different materials and to make drawings based on their imagination. Participants were also encouraged to express their feeling and memories evoked by the activity.
Personnel delivering the two interventions were two psychologists. All sessions lasted two hours and were delivered twice a week during three weeks, totalling 12 hours during six sessions.
Study 2: experimental group
The same two‐hour structured mixed group intervention was delivered by two psychologists, and the sessions were delivered twice a week, but during four weeks, and therefore totalling 16 hours during eight sessions.
Study 2: control group
The control intervention in study 2 was cooking, because it was a pleasant activity that stimulates a number of senses. There was more interaction compared to the painting control condition. Further, more similar with the music therapy intervention, the cooking intervention also involved alternating productive (prepare a recipe) and receptive phases (taste a dessert). The sessions included preparing a different recipe collectively, with roles distributed according to the participants' abilities. Participants were encouraged to taste ingredients, and verbalise remembrances.
Narme 2014
Music‐based therapeutic intervention: a group music programme (versus cooking as the control condition)
Experimental group
A 60‐minute structured mixed group intervention, with a maximum of eight participants. Music selections were chosen independent of the participants' preferences, and were played on a CD player (loudspeaker). The selections varied from classical music to songs from the 1950s to 1980s, included minor and major keys) and were 'calming' with slow to moderate tempo and 'arousing' music with a higher tempo. Calming music was used at the start and end of the session. The same playlist was used in the same order for each music session, but pieces were played twice if participants expressed the wish to hear a song again. Participants were asked to listen or to play along (on percussion instruments: clapping or playing hand drums) and sing along. Receptive and active phases were alternated. Participants were encouraged to express their feelings and autobiographical memories evoked by the activity.
The sessions were delivered twice a week, for a period of four weeks, totalling eight one‐hour sessions. Personnel delivering the intervention were "two supervisors," including one psychologist, with no prior education in music therapy.
Control group
A cooking intervention, in which participants were asked to make a different recipe for each session (e.g. chocolate cake; French pancakes). Each session commenced with a game about ingredients where participants were asked to collectively prepare a given recipe. Roles were distributed according to participants' abilities (e.g. cutting, peeling, measuring quantities, mixing or cooking). Receptive (tasting) and productive phases were alternated. Participants were encouraged to express their feelings and autobiographical memories evoked by the activity.
The sessions had a duration of one hour and were delivered twice a week, for a period of four weeks, totalling eight one‐hour sessions. Personnel delivering the intervention were "two supervisors," including one psychologist, with no prior education in music therapy.
Raglio 2010a
Music‐based therapeutic intervention: active individual music therapy based on relationship (versus a control group of usual care)
Experimental group
A 30‐minute active non‐verbal individual music therapy intervention, in which free musical improvisation is used to build a relationship between participant and music therapist. During the session, the participant and the music therapist had a non‐verbal dialogue and expressed their feelings and emotions through non‐verbal behaviours (possibly by using voice and tapping, not specified in the text) and by playing musical instruments. Choice of instruments included rhythmic‐melodic instruments, percussions, glockenspiels, xylophones, etc. Sharing emotions, raising awareness and the possibility of introducing new ways of expression and communication were a focus of the session and may have led to empathetic processes and mutual calibration.
A music therapist delivered the sessions, which were twice a week for 15 weeks, with a total of 30 sessions.
Control group
Usual care.
Raglio2010b
Music‐based therapeutic intervention: active group music therapy based on relationship (versus a control group of usual care)
Experimental group
A 30‐minute active non‐verbal group music therapy intervention, in which free musical improvisation was used to build a relationship between participant and music therapist. Groups had three participants. The intervention focused on favouring the moments of attunement that help organise and regulate the participants' behaviours and emotions. Participants and music therapist interacted and expressed their feelings and emotions through non‐verbal behaviours and using musical instruments. Note that this approach is inspired by the intersubjective psychology (references provided in the article).
A music therapist delivered the sessions. The sessions were delivered in three non‐continuous treatment cycles consisting of four weeks of three sessions per week followed by one month of no treatment (washout; however, not in the context of a cross‐over design). The total number of sessions was 36, within six months.
Control group
Usual care.
Raglio 2015
Music‐based therapeutic intervention: active music therapy (versus music listening and a control group of usual care)
Experimental group
A 30‐minute individual active music therapy which consisted of playing and improvising on instruments, focused on promoting 'affect attunement' moments. The music therapist followed the participants' rhythm and music production (also introducing variations) to create nonverbal communication. During the session, the music therapist built a relationship with the participant by singing and using melodic and rhythmic instruments (improvisation), facilitating the expression and modulation of the participant's emotions.
The intervention was delivered by a certified specifically trained music therapist, twice a week for 10 weeks in a separate, medium‐sized room.
Control group 1
Individualised 30‐minute music listening sessions, delivered through speakers in the room of the participant or in a quiet private place.
Control group 2
Participants received standard care which included daily educational, occupational and physical activities performed under supervision of specialised professionals. Standard care did not include music exposure.
Ridder 2013
Music‐based therapeutic intervention: individual mixed music therapy (versus a control group of usual care)
Experimental group
An individual mixed music therapy intervention, not prestructured, delivered by music therapists with a mean duration of 33.8 (standard deviation 9.91) minutes. The aim of the music therapy was phrased in a more positive way than a goal of reducing (e.g. challenging behaviour ("to facilitate initiative, engagement, self‐expression and mutual understanding")). The authors refer to Tom Kitwood for the theoretical basis of a relation‐based and person‐centred approach in music therapy.
Vocal or instrumental improvisation, singing, dancing/moving, listening and talking/going for a walk could be part of the session. The music accompanying the activities was prerecorded or live music, and consisted of 'free' improvisation or based on songs/melodies. The overall aim of the music therapy was to facilitate initiative, engagement, self‐expression and mutual understanding. Clinicians were instructed to be aware of at least three different ways of applying music in therapy: catching attention and creating a safe setting, regulating arousal level to a point where self‐regulation is possible and engaging in social communication to fulfil psychosocial needs. The session was not especially focused on decreasing agitation.
Music therapists with university‐level training delivered the intervention which were twice a week for a period of six weeks, with 12 sessions offered in total. The mean number of sessions received was 10 (standard deviation 2.82, range 0 to 13).
Control group
Usual care.
Sakamoto 2013
Music‐based therapeutic intervention: an individual mixed music (therapy) intervention (versus 2 control groups)
Experimental group
A 30‐minute individual mixed music therapy intervention. The selection of music was based on determination of a period of the participant's life that was recalled most frequently, interviews with participants and their family, and links to special memories. Music was selected for probable evoking of positive emotions such as pleasure or joy.
The selected music was played via a CD player (loudspeaker). The participants also participated in activities guided by a music facilitator, including clapping, singing and dancing. The sessions took place in a familiar room.
During the session, participants were monitored to confirm that "the music was suitable in terms of engaging the participants and eliciting a joyful emotional state." Participants' attention was directed to the music, and "an interactive approach that responded to the participants' emotional reactions to the music" was used.
The sessions were delivered by music therapists, occupational therapists and nurses, each trained for 10 days in delivering the intervention. The sessions took place weekly for a period of 10 weeks (10 sessions in total), and were scheduled between 10 a.m. and 11 a.m.
Control group 1: passive individual music intervention (the music intervention did not meet our criteria for music‐based therapeutic interventions)
A 30‐minute individual music intervention. The selection of music was made based on determination of a period of participants' life that was recalled most frequently, interviews with participants and their family, and links to special memories. Music was selected for probable evoking of positive emotions such as pleasure or joy.
The selected music was played via a CD player (loudspeaker). Personnel delivering the intervention was a carer and a music provider, but no interaction took place between personnel and participants during the intervention. The session took place in a familiar room weekly for a period of 10 weeks (10 sessions in total), and were scheduled between 10 a.m. and 11 a.m.
Control group 2: observation
Spending 30 minutes in their own room as usual in a silent environment, with a carer observing from a distance and no interaction between carer and participant. The sessions took place weekly for a period of 10 weeks (10 sessions in total), and were scheduled between 10 a.m. and 11 a.m.
Sung 2012
Music‐based therapeutic intervention: active group music intervention (versus a control group of usual care)
Experimental group
A 30‐minute active group music therapy intervention with movement. The sessions included five minutes of warm‐up and five minutes of cooling down (stretching major muscle groups and breathing exercise with music). During the main part of the session, participants were guided in the use of percussion instruments (hand bell, tambourine, maracas, guiro tone block, flapper and loop bell) while listening to music and songs familiar to the participants. Participants' music preferences were assessed through interviewing the participants, carers, families or nursing staff. The preferred music was Taiwanese and Chinese songs from the 1950s to 1970s with moderate rhythm and tempo.
Sessions were delivered by a nursing researcher and two research assistants trained in providing the music intervention, twice a week for six weeks, with a total of 12 sessions.
Control group
Usual care
Svansdottir 2006
Music‐based therapeutic intervention: mixed group music therapy (versus a control group of usual care)
Experimental group
A 30‐minute mixed music therapy intervention, with three or four participants per group. The sessions were accompanied by guitar playing and consisted of (listening to) singing with the help of songbooks, playing along on various kind of instruments (choice of instruments not specified), instrumental improvisation and moving/dancing, if "patients had an urge to move and dance." The music therapist selected a collection of songs that were familiar to the residents.
A music therapist delivered the sessions three times a week for six weeks, totalling 18 sessions.
Control group
Usual care.
Thornley 2016
Music‐based therapeutic intervention: active individual music therapy (versus a control condition with individual active engagement)
Experimental group
A 60‐minute individual active music therapy which consisted of singing and playing simple instruments to music adapted to the participants' preferences.
An accredited music therapist delivered the intervention twice a week for four weeks. The participants were encouraged to actively engage in the musical process and to follow the music therapist's lead. Participants were provided with specific instructions on how to participate by singing or playing simple instruments (or both), including maracas and small drums. The music was selected in accordance with participant preferences and was of a calming nature.
Control group
A 60‐minute individual active engagement and attention (active engagement Intervention) delivered by a social worker, including supportive interviewing, and encouragement of expression through simple occupational activities such as folding towels and browsing magazines. The control intervention was also delivered twice a week for four weeks.
Vink 2013
Music‐based therapeutic intervention: mixed group music therapy (versus a control condition with general recreational activities)
Experimental group
A 40‐minute mixed group music therapy intervention which consisted of a welcome song; listening to selected music, sung or played by the therapist (Dutch familiar songs, classical and folk music); and singing, dancing or playing along (on simple rhythm instruments). Within the group session the therapist adjusted the level of each intervention to individual capacities. The music accompanying the session was played live on, for example, piano or guitar and was selected with the goal of inciting pleasant memories and reducing agitation. For this, musical parameters were used "such as slow tempo and little instrumentation."
Music therapists delivered the intervention, in rooms away from the nursing home ward. The sessions were delivered twice a week for four months, with a total of up to 34 sessions.
Control group
General recreational activities, such as handwork, playing shuffleboard, making flower bouquets and playing games. The sessions also lasted 40 minutes, were delivered twice a week for four months and were also held in rooms away from the nursing home ward.


Methodological quality summary: review authors' judgements about each methodological quality item for each included study.

Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.

Funnel plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.3 Negative affect or mood disturbances: anxiety (13 studies, 15 dots because 2 studies used 2 control groups, 1 with usual care and 1 with other activities).

Funnel plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.4 Problematic behaviour: agitation or aggression (14 studies, 16 dots because 2 studies used 2 control groups, 1 with usual care and 1 with other activities).

Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.1 Emotional well‐being and quality of life. CI: confidence interval; SD: standard deviation.

Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.2 Negative affect or mood disturbances: depression. BEHAVE‐AD: Behavioural Pathology in Alzheimer's Disease; NPI: Neuropsychiatric Inventory; SD: standard deviation.

Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.3 Negative affect or mood disturbances: anxiety. BEHAVE‐AD: Behavioural Pathology in Alzheimer's Disease; NPI: Neuropsychiatric Inventory; SD: standard deviation; STAI‐A: State‐Trait Anxiety Inventory for Adults.

Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.4 Problematic behaviour: agitation or aggression. BEHAVE‐AD: Behavioural Pathology in Alzheimer's Disease; CI: confidence interval; CMAI: Cohen‐Mansfield Agitation Inventory; NPI: Neuropsychiatric Inventory; SD: standard deviation.

Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.5 Problematic behaviour overall. NPI: Neuropsychiatric Inventory; SD: standard deviation.

Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.6 Social behaviour: music vs other activities. SD: standard deviation.
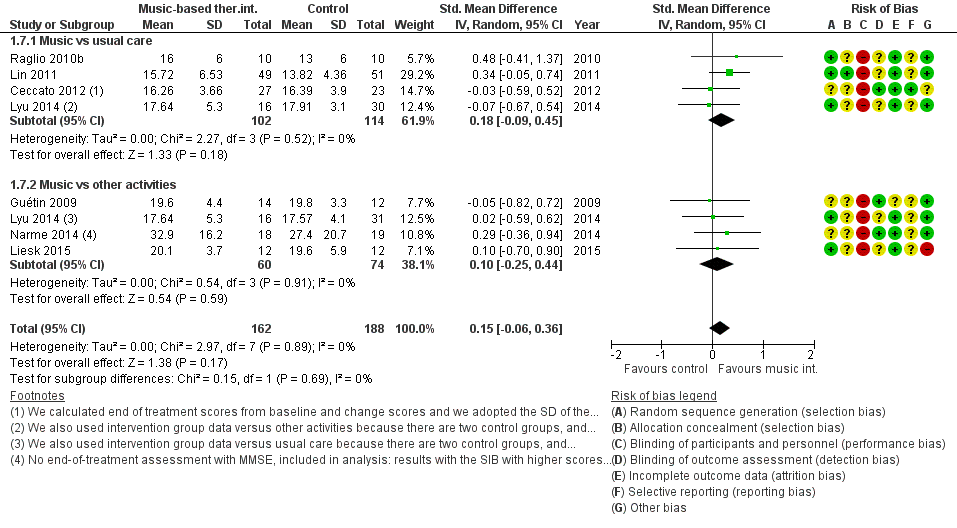
Forest plot of comparison: 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, outcome: 1.7 Cognition. MMSE: Mini‐Mental State Examination; SD: standard deviation; SIB: Severe Impairment Battery.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 1 Emotional well‐being including quality of life.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 2 Mood disturbance or negative affect: depression.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 3 Mood disturbance or negative affect: anxiety.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 4 Behaviour problems: agitation or aggression.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 5 Behaviour problems: overall.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 6 Social behaviour: music vs other activities.

Comparison 1 Music‐based therapeutic interventions versus usual care or versus other activities: end of treatment, Outcome 7 Cognition.

Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 1 Emotional well‐being including quality of life.

Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 2 Mood disturbance or negative affect: depression.

Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 3 Mood disturbance or negative affect: anxiety.

Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 4 Behavioural problems: agitation or aggression.

Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 5 Behavioural problems: overall.

Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 6 Social behaviour: music versus other activities.
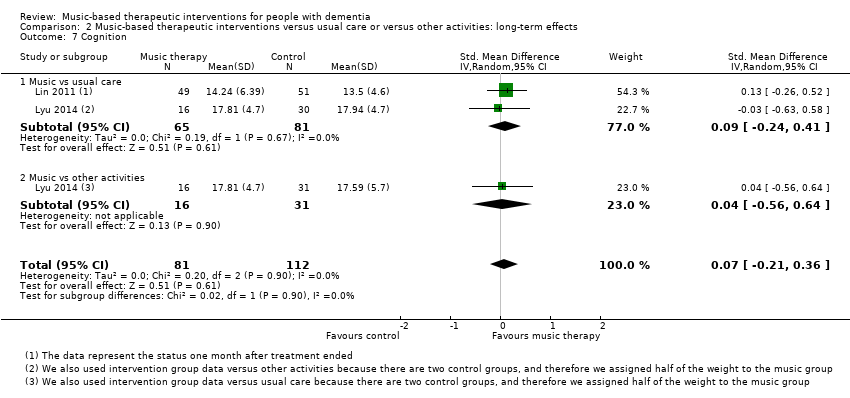
Comparison 2 Music‐based therapeutic interventions versus usual care or versus other activities: long‐term effects, Outcome 7 Cognition.
| Music‐based therapeutic interventions compared to usual care or other activities for people with dementia: end‐of‐treatment effects | |||
| Patient or population: people with dementia (all resided in institutional settings) | |||
| Outcomes (end of treatment) measured with a variety of scales except for social behaviour | Anticipated absolute effects, SMD* (95% CI) | № of participants | Quality of the evidence |
| Score with music therapy compared with usual care or other activities | |||
| Emotional well‐being including quality of life | The score in the intervention group was 0.32 SDs higher | 348 | ⊕⊕⊝⊝ |
| Mood disturbance or negative affect: depression | The score in the intervention group was 0.27 SDs lower | 503 | ⊕⊕⊕⊝ |
| Mood disturbance or negative affect: anxiety | The score in the intervention group was 0.43 SDs lower | 478 | ⊕⊕⊝⊝ |
| Behavioural problems: agitation or aggression | The score in the intervention group was 0.07 SDs lower | 626 | ⊕⊕⊕⊝ |
| Behavioural problems: overall | The score in the intervention group was 0.23 SDs lower | 442 | ⊕⊕⊕⊝ |
| Social behaviour: music vs other activities | The score in the intervention group was 0.54 SDs higher | 70 | ⊕⊝⊝⊝ |
| Cognition | The score in the intervention group was 0.15 SDs higher | 350 | ⊕⊕⊝⊝ |
| *Interpretation of SMD: a difference of < 0.40 SDs can be regarded as a small effect, 0.40–0.70 a moderate effect, and > 0.70 a large effect. CI: confidence interval; SMD: standardised mean difference; SD: standard deviation. | |||
| GRADE Working Group grades of evidence (GradePro) | |||
| aRisk of bias: no blinding of therapists and participants (not possible), and often no or unclear blinding of outcome assessment. bImprecision: small number of participants and broad CI. cRisk of bias: no blinding of therapists and participants (not possible), and sometimes no or unclear blinding of outcome assessment. dInconsistency: more non‐overlapping CIs. eImprecision: very small number of participants and broad CIs. fImprecision: small number of participants. | |||
| Music‐based therapeutic interventions compared to usual care or other activities for people with dementia: long‐term effects (scores 4 weeks or more after treatment ended) | |||
| Patient or population: people with dementia (all resided in institutional settings) | |||
| Outcomes (long‐term) measured with a variety of scales except for social behaviour | Anticipated absolute effects, SMD* (95% CI) | № of participants | Quality of the evidence |
| Score with music therapy compared with usual care or other activities | |||
| Emotional well‐being including quality of life | The score in the intervention group was 0.34 SDs higher | 180 | ⊕⊕⊝⊝ |
| Mood disturbance or negative affect: depression | The score in the intervention group was 0.03 SDs lower | 354 | ⊕⊕⊝⊝ |
| Mood disturbance or negative affect: anxiety | The score in the intervention group was 0.28 SDs lower | 265 | ⊕⊝⊝⊝ |
| Behavioural problems: agitation or aggression | The score in the intervention group was 0.10 SDs lower | 330 | ⊕⊕⊝⊝ |
| Behavioural problems: overall | The score in the intervention group was 0.19 SDs lower | 351 | ⊕⊕⊝⊝ |
| Social behaviour: music vs other activities | The score in the intervention group was 0.53 SDs higher | 48 | ⊕⊝⊝⊝ |
| Cognition | The score in the intervention group was 0.07 SDs higher | 193 | ⊕⊕⊝⊝ |
| *Interpretation of SMD: a difference of < 0.40 SDs can be regarded as a small effect, 0.40–0.70 a moderate effect, and > 0.70 a large effect. CI: confidence interval; SMD: standardised mean difference; SD: standard deviation. | |||
| GRADE Working Group grades of evidence (GradePro) | |||
| aRisk of bias: no blinding of therapists and participants (not possible), and sometimes no or unclear blinding of outcome assessment. bImprecision: small number of participants and broad CIs includes both benefit and harm. cImprecision: small number of participants. dRisk of bias: no blinding of therapists and participants (not possible). eInconsistency: non‐overlapping CIs. fImprecision: small number of participants and broad CIs includes both benefit and harm. gImprecision: very small number of participants and very broad CIs includes both benefit and harm. hRisk of bias: no blinding of therapists and participants (not possible), and unclear blinding of outcome assessment. | |||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Emotional well‐being including quality of life Show forest plot | 9 | 348 | Std. Mean Difference (IV, Random, 95% CI) | 0.32 [0.02, 0.62] |
| 1.1 Music vs usual care | 3 | 113 | Std. Mean Difference (IV, Random, 95% CI) | 0.47 [‐0.30, 1.25] |
| 1.2 Music vs other activities | 7 | 235 | Std. Mean Difference (IV, Random, 95% CI) | 0.30 [‐0.04, 0.64] |
| 2 Mood disturbance or negative affect: depression Show forest plot | 11 | 503 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.27 [‐0.45, ‐0.09] |
| 2.1 Music vs usual care | 6 | 307 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.28 [‐0.53, ‐0.04] |
| 2.2 Music vs other activities | 6 | 196 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.23 [‐0.52, 0.06] |
| 3 Mood disturbance or negative affect: anxiety Show forest plot | 13 | 478 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.43 [‐0.72, ‐0.14] |
| 3.1 Music vs usual care | 6 | 237 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.22 [‐0.48, 0.04] |
| 3.2 Music vs other activities | 9 | 241 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.63 [‐1.13, ‐0.12] |
| 4 Behaviour problems: agitation or aggression Show forest plot | 14 | 626 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐0.24, 0.10] |
| 4.1 Music vs usual care | 10 | 458 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.10 [‐0.31, 0.11] |
| 4.2 Music vs other activities | 6 | 168 | Std. Mean Difference (IV, Random, 95% CI) | 0.01 [‐0.31, 0.32] |
| 5 Behaviour problems: overall Show forest plot | 10 | 442 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.23 [‐0.46, ‐0.01] |
| 5.1 Music vs usual care | 7 | 251 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.40 [‐0.71, ‐0.10] |
| 5.2 Music vs other activities | 6 | 191 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.02 [‐0.32, 0.28] |
| 6 Social behaviour: music vs other activities Show forest plot | 3 | 70 | Std. Mean Difference (IV, Random, 95% CI) | 0.54 [0.06, 1.02] |
| 7 Cognition Show forest plot | 7 | 350 | Std. Mean Difference (IV, Random, 95% CI) | 0.15 [‐0.06, 0.36] |
| 7.1 Music vs usual care | 4 | 216 | Std. Mean Difference (IV, Random, 95% CI) | 0.18 [‐0.09, 0.45] |
| 7.2 Music vs other activities | 4 | 134 | Std. Mean Difference (IV, Random, 95% CI) | 0.10 [‐0.25, 0.44] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Emotional well‐being including quality of life Show forest plot | 4 | 180 | Std. Mean Difference (IV, Random, 95% CI) | 0.34 [‐0.12, 0.80] |
| 1.1 Music vs usual care | 2 | 72 | Std. Mean Difference (IV, Random, 95% CI) | 0.91 [‐0.85, 2.67] |
| 1.2 Music vs other activities | 3 | 108 | Std. Mean Difference (IV, Random, 95% CI) | 0.18 [‐0.22, 0.58] |
| 2 Mood disturbance or negative affect: depression Show forest plot | 6 | 354 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.03 [‐0.24, 0.19] |
| 2.1 Music vs usual care | 4 | 233 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.02 [‐0.28, 0.24] |
| 2.2 Music vs other activities | 3 | 121 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.04 [‐0.41, 0.33] |
| 3 Mood disturbance or negative affect: anxiety Show forest plot | 6 | 265 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.28 [‐0.71, 0.15] |
| 3.1 Music vs usual care | 3 | 141 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.06 [‐0.48, 0.37] |
| 3.2 Music vs other activities | 4 | 124 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.53 [‐1.31, 0.25] |
| 4 Behavioural problems: agitation or aggression Show forest plot | 5 | 330 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.10 [‐0.33, 0.13] |
| 4.1 Music vs usual care | 4 | 241 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.42, 0.09] |
| 4.2 Music vs other activities | 2 | 89 | Std. Mean Difference (IV, Random, 95% CI) | 0.10 [‐0.66, 0.86] |
| 5 Behavioural problems: overall Show forest plot | 6 | 351 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.19 [‐0.51, 0.14] |
| 5.1 Music vs usual care | 5 | 207 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.32 [‐0.85, 0.21] |
| 5.2 Music vs other activities | 3 | 144 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.44, 0.25] |
| 6 Social behaviour: music versus other activities Show forest plot | 2 | 48 | Std. Mean Difference (IV, Random, 95% CI) | 0.53 [‐0.53, 1.60] |
| 6.1 Music vs usual care | 0 | 0 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 6.2 Music vs other activities | 2 | 48 | Std. Mean Difference (IV, Random, 95% CI) | 0.53 [‐0.53, 1.60] |
| 7 Cognition Show forest plot | 2 | 193 | Std. Mean Difference (IV, Random, 95% CI) | 0.07 [‐0.21, 0.36] |
| 7.1 Music vs usual care | 2 | 146 | Std. Mean Difference (IV, Random, 95% CI) | 0.09 [‐0.24, 0.41] |
| 7.2 Music vs other activities | 1 | 47 | Std. Mean Difference (IV, Random, 95% CI) | 0.04 [‐0.56, 0.64] |