Program Penglibatan Keluarga dan Sekolah (FAST) untuk meningkatkan hasil pembelajaran pada kanak‐kanak dan keluarga mereka
Abstract
Background
Parents and carers have a major influence on children's learning and development from birth, through the school years, and into adulthood. Parental contributions to education include providing a secure environment in which to learn, providing intellectual stimulation, transmitting social norms and values, shaping the child’s resilience through fostering literacy and problem‐solving, and encouraging personal and social aspiration. Increasingly, providers of formalised education are recognising the primary role of parents, carers, and the wider family, as well as peers and the environment, in shaping children's education, health, and life experiences.
Objectives
To assess the effectiveness of the Families and Schools Together (FAST) programme in improving outcomes among children and their families.
Search methods
Between October 2018 and December 2018, we searched CENTRAL, MEDLINE, Embase, PsycINFO, 11 additional databases, and three trial registers. We handsearched the reference lists of included studies and relevant reports and reviews, contacted the programme developer and independent researchers, and searched relevant websites to identify other eligible studies.
Selection criteria
We included randomised controlled trials (RCTs) and quasi‐RCTs examining the effects of FAST, relative to waiting list, usual or alternative services, or no intervention, on outcomes for children (aged from birth to completion of compulsory education) and their families.
Data collection and analysis
At least two review authors independently evaluated the records retrieved from the search for relevance. One review author (JV) extracted data from eligible studies with a second independent review author (AF, DK, or SL). Review authors consulted with one another to resolve disagreements. We used a fixed‐effect model for meta‐analysis. We presented results as standardised mean differences (SMDs) because all outcomes were continuously scaled, and we accompanied these with 95% confidence intervals (CIs). We used the GRADE approach to assess the certainty of evidence for each outcome.
Main results
We identified 10 completed RCTs, most of which were relatively recent (2007 or later) and were conducted with at least some involvement from the intervention developer or the FAST organisation. Nine of the 10 trials were from the USA; the other was from the UK. Children were young (five to nine years old; mean age approximately six years), and therefore, whilst not so named in the reports, evaluations consisted of what is sometimes referred to as 'Kids FAST' and sometimes 'Elementary Level FAST'). Among the USA‐based studies, at least 62% of participants were members of a racial/ethnic minority group (most commonly, African American or Latino). FAST was usually delivered in schools after the school day. Trials lasted about eight weeks and usually examined the effects of FAST relative to no additional intervention. Most studies were funded by agencies in the US federal government. We judged the certainty of evidence in the included studies to be moderate or low for the main review outcomes. Failure to include all families in outcome analyses (attrition) and possible bias in recruitment of families into the trials were the main limitations in the evidence.
We included over 9000 children and their families in at least one meta‐analysis. The follow results relate to meta‐analyses of data at long‐term follow‐up.
Primary outcomes
Four studies (approximately 6276 children) assessed child school performance at long‐term follow‐up. The effect size was very small, and the CI did not include effects that, if real, suggest possibly important positive or negative effects if viewed from an individual perspective (SMD ‐0.02, 95% CI ‐0.11 to 0.08). We assessed the certainty of evidence for this outcome as moderate. No studies assessed child adverse events, parental substance use, or parental stress.
Secondary outcomes
Parent reports of child internalising behaviour (SMD ‐0.03, 95% CI ‐0.11 to 0.17; 4 RCTs, approximately 908 children; low‐certainty evidence) and family relationships (SMD 0.08, 95% CI ‐0.03 to 0.19; 4 RCTs, approximately 2569 children; moderate‐certainty evidence) also yielded CIs that did not include effects that, if real, suggest possibly important positive or negative effects.
The CI for parent reports of child externalising behaviour, however, did include effects that, if real, were possibly large enough to be important (SMD ‐0.19, 95% CI ‐0.32 to ‐0.05; 4 RCTs, approximately 754 children; low‐certainty evidence).
Authors' conclusions
Given these results, it is hard to support the assertion that assignment to FAST is associated with important positive outcomes for children and their parents.
PICOs
Ringkasan bahasa mudah
Keluarga dan sekolah seiringan
Latar belakang
Kanak‐kanak yang berprestasi baik di sekolah mempunyai penjaga yang berminat dalam pembelajaran mereka dan menggalakkan mereka untuk membaca dan menyelesaikan masalah pembelajaran dan juga membantu mereka sebaik mungkin. Penjaga yang tinggal di komuniti yang menyokong pembelajaran seperti ini mendapati lebih mudah untuk melaksanakan tanggungjawab keibu‐bapaan seperti yang dikehendaki berbanding dengan mereka yang terasing daripada komuniti yang membantu. Program Penglibatan Keluarga dan Sekolah yang dikenali sebagai FAST‐ adalah satu program yang direka untuk menolong ibu bapa membantu anak mereka untuk belajar dan mendapat keputusan yang baik di sekolah. Ia bertujuan untuk menangani masalah yang menghalang ibu bapa daripada memberi sokongan yang anak mereka perlukan, dengan menambah baik hubungan antara keluarga dan sekolah, meningkatkan sokongan untuk keluarga, dan menangani masalah seperti kemiskinan, penyakit mental, dan penyalahgunaan bahan terlarang. Lima versi FAST yang berbeza telah direka untuk keluarga yang mempunyai anak pada umur yang berbeza.
Soalan ulasan
Adakah Program Penglibatan Keluarga dan Sekolah (FAST) meningkatkan keputusan pembelajaran untuk kanak‐kanak dan membawa kebaikan kepada keluarga mereka?
Ciri‐ciri kajian
Kami mendapati terdapat 10 kajian rawak terkawal (kajian‐kajian yang mana sekolah‐sekolah ditentukan untuk menerima FAST atau untuk meneruskan sistem pembelajaran seperti biasa, dengan kaedah rawak), melibatkan lebih daripada 9000 kanak‐kanak dan keluarga mereka.
Sembilan daripada kajian ini dilakukan di Amerika Syarikat dan dibiayai oleh agensi‐agensi di bawah Kerajaan Persekutuan Amerika Syarikat. Satu kajian dilakukan di UK. Kanak‐kanak berusia daripada lima hingga sembilan tahun, dan sebahagian besar kanak‐kanak berasal dari Amerika Syarikat adalah daripada ahli kumpulan etnik atau kaum minoriti. Penglibatan kanak‐kanak lelaki dan perempuan di dalam kajian ini lebih kurang dengan kadar yang sama. Dalam kebanyakan kajian, FAST dilakukan di sekolah kanak‐kanak yang terlibat selepas tamat waktu persekolahan, walaupun begitu terdapat beberapa kajian yang dilakukan di luar sekolah (contohnya di pusat komuniti). Kajian‐kajian berlangsung selama lapan minggu dan pada akhir tempoh ini kesan program FAST diukur dan dibandingkan dengan tiada intervensi tambahan. Bukti ini adalah terkini sehingga Disember 2018.
Keputusan‐keputusan
Meta‐analisis adalah kaedah statistik yang menggabungkan data daripada beberapa kajian untuk mencapai satu, kesimpulan yang lebih kukuh. Kami dapat menggunakan data dari sembilan kajian dalam meta‐analisis ini bagi mengukur kesan FAST pada kanak‐kanak yang berumur antara lima hingga lapan tahun. Walaupun terdapat kajian‐kajian individu yang melaporkan penemuan positif, terdapat sedikit sahaja bukti yang mencadangkan bahawa penglibatan dalam program FAST dapat meningkatkan prestasi sekolah kanak‐kanak, mengurangkan penyalahgunaan bahan terlarang oleh ibu bapa, atau mengurangkan kadar stres ibu bapa. Tiada kajian mengukur kesan sampingan pada kanak‐kanak. Tambahan pula, hanya terdapat bukti yang sedikit yang mencadangkan bahawa FAST mendorong kepada perubahan penting pada sikap kanak‐kanak atau hubungan kekeluargaan.
Kualiti kajian
Kami menilai kepastian bukti bagi keputusan utama kajian‐kajian ini sebagai sederhana atau rendah. Kegagalan melibatkan kesemua keluarga di dalam hasil analisis (merendahkan atau menurunkan kekuatan hasil kajian) dan kemungkinan terdapat bias dalam pengambilan keluarga ke dalam kajian adalah limitasi (pembatasan) utama pada bukti kajian.
Kesimpulan pengarang
Bukti mengenai keberkesanan pelaksanaan FAST adalah berkepastian sederhana hingga rendah dan tidak dapat mencadangkan bahawa pelaksanaan FAST memberi manfaat penting kepada para pelajar dan keluarga mereka.
Authors' conclusions
Summary of findings
| Families and Schools Together (FAST) compared to no intervention (or care as usual) for children and their families | ||||||
| Patient or population: children and their families | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
| Risk with no intervention (or care as usual) | Risk with FAST | |||||
| Child school performance: long‐term follow up | ‐ | Mean score in the intervention group was0.02 standard deviations lower | ‐ | 6276 children (approximately) (4 RCTs) | ⊕⊕⊕⊝ | Positive effect sizes indicate improvement. Evidence suggests that FAST probably does not have an important positive effect on child school performance at long‐term follow‐up |
| Child adverse events ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Parental substance abuse ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Parental stress ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Child internalising behaviours | ‐ | Mean score in the intervention group was 0.03 standard deviations lower (0.11 lower to 0.17 higher) | ‐ | 908 (approximately) (4 RCTs) | ⊕⊕⊝⊝ | Negative effect sizes indicate improvement. Evidence suggests that FAST probably does not result in an important reduction in child internalising behaviours |
| Child externalising behaviours | ‐ | Mean score in the intervention group was 0.19 standard deviations lower | ‐ | 754 (approximately) (4 RCTs) | ⊕⊕⊝⊝ | Negative effect sizes indicate improvement. FAST may result in a small and possibly important positive effect on parent reports of child externalising behaviour at follow‐up. However, teacher reports for this outcome suggest small and probably unimportant effect sizes, as did parent reports of child externalising behaviours immediately after completion of the intervention |
| Family relationships | ‐ | Mean score in the intervention group was 0.08 standard deviations higher | ‐ | 2569 (approximately) (4 RCTs) | ⊕⊕⊕⊝ | Positive effect sizes indicate improvement. FAST may result in a small and probably unimportant positive effect on parent reports of family relations |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; FAST: Families and Schools Together; RCT: randomised controlled trial. | ||||||
| GRADE Working Group grades of evidence. | ||||||
| aCertainty of evidence downgraded because two studies were at high risk for recruitment bias and two studies were at high risk for incomplete outcome data (attrition bias). | ||||||
Background
Description of the condition
TheMelbourne Declaration on Education Goals for Young Australians is not unusual in recognising the important role played by schools in nurturing the "intellectual, physical, social, emotional, moral, spiritual, and aesthetic development and well‐being" of young people (MCEETYA 2008). In the UK, the Education Act 2002 and the Academies Act 2010 require schools to provide a curriculum that promotes "the spiritual, moral, cultural and physical development of pupils at [...] school and of society, and prepare pupils ... for the opportunities, expendabilities and experiences of later life". Schools are not, therefore, just about educational attainment, they are also about how well children engage with school; in turn, how children do at school is predictive of a range of outcomes in later life, including future employment, income, and physical and mental health (see, for example, Heckmann 2014; Nores 2010).
Investment in education and training is essential for creating sustainable economic growth, competitiveness, and increased productivity (European Commission 2012b). One of the five flagship initiatives of Europe's Growth Strategy is to reduce school dropout rates to below 10% in member nations, where, on average, 73 million adults have low levels of education and 20% of 15‐year‐olds lack basic reading skills (European Commission 2013). The Education and Training Monitor supports efforts to combat early school leaving, to increase participation in education, to improve early education experiences, to reduce inequalities in achievements, and to promote skills‐based learning and participation in education (European Commission 2012a). As part of the global drive to increase the uptake of education (ACARA 2013; Eurydice 2012; National Committee on Inuit Education 2011; USDoE 2002), many education systems have introduced some form of objective‐based educational standards designed to record levels of achievement or 'outcomes' in basic skills such as literacy, numeracy, science, languages, and social skills (The World Bank 2009).
Children whose families live in poverty, particularly persistent poverty, are at increased risk of low educational achievement. The reasons for this are complex, reflecting the interaction of individual, family, school, and community level factors. Beyond the direct negative impacts of poverty (examples of which can include poor housing and nutrition), individual factors that have been indirectly implicated in children's educational attainment include a child's working memory (Alloway 2010); information‐processing efficiency in infancy, general cognitive development in toddlerhood, and behaviour difficulties in early childhood (Bornstein 2013); and children's health (Basch 2011); family factors include mother's educational attainment (Bornstein 2013); school absences and mobility (Ou 2008); and parental aspirations (Goodman 2011). The quality of the school environment also influences outcomes for children (Sylva 2011), as do community factors such as the level of social disorganisation (Nieuwenhuis 2016).
The adverse impact of poverty makes itself felt in children's earliest years, with children from economically disadvantaged backgrounds performing well behind their non‐disadvantaged peers in terms of literacy and communication skills, and school readiness by three years of age (Hirsh 2007). These differences persist and the gap between those in poverty and their more affluent peers increases over time. Good quality parenting can play an important role in mitigating the effects of poverty, and can help to ensure that children reach their educational potential (Kiernan 2011). Sensitive, positive parenting can help ensure that children are ready for school, and can support their learning once there (e.g. Jeynes 2005). However, the stresses of poverty may adversely impact parents' ability to parent their children effectively, and this can be exacerbated by an absence of support networks (Gutman 2010).
Since publication of the Coleman Report (Coleman 1966), which asserted that schools have less influence upon student outcomes than family background and other environmental factors (Emerson 2012), policy makers have adopted increasingly broad‐based approaches to improving educational outcomes, with increasing emphasis upon family involvement within a supported learning environment. Multi‐systemic approaches, which involve staff, students, parents, and the wider community, are thought to have a greater chance of success in improving child outcomes.
Parents and carers have an important role in the socialisation of young people (Foxcroft 2011). They exert a major influence on children's learning and development from birth, through the school years, and long into adulthood (DEEWR 2011). Parental contributions to education include providing a secure environment in which to learn, providing intellectual stimulation, transmitting social norms and values, shaping the child’s resilience through fostering literacy and problem‐solving, and encouraging personal and social aspiration (Kim 2012). Increasingly, providers of formalised education are recognising the primary role of parents, carers, and the wider family, as well as peers and the environment, in shaping children's education, health, and life experiences (Desforges 2003; Sisco 2012). Research suggests that high levels of parental and community involvement in education are related to improved student performance, learning outcomes, attendance, and behaviour, regardless of cultural and social background (DEEWR 2011; Weiss 2010).
Description of the intervention
FAST (Families and Schools Together) was developed in the USA in 1988 at Family Service Incorporated, in Madison, Wisconsin, by Dr Lynn McDonald, in collaboration with the Prevention ‐ Intervention Centre for Alcohol and Other Drug Abuse. It was originally designed as a targeted intervention for children at risk of failure at school (Layzer 2001). Since that time, FAST has evolved into a multi‐family, after‐school programme, which is primarily implemented in schools with populations experiencing multiple risk factors of deprivation (Layzer 2001; McDonald 2009a; WSIPP 2012). The programme has incorporated cultural adaptations to suit White, Hispanic/Latino, American Indian, African American, Southeast Asian American, Alaskan Native, and Australian Indigenous people, and it has been translated into French, German, Japanese, Russian, and Spanish, and has been delivered to multi‐lingual and English groups as a 'second language' (CBCAP 2009; Mupotsa 2010). FAST is in use in over 2000 schools across 11 countries, including the USA, Canada, Australia, Europe and Russia, Brazil, and the UK (McDonald 2010).
McDonald describes FAST as a programme based on family systems theory, and on evidence‐based, published, and funded research on best practices. Overall, FAST is designed to prevent children from experiencing school failure by empowering parents in their role as educators, by fostering closer relationships between families and schools, and by encouraging improvements in children's behaviour and educational outcomes. FAST works with health professionals to prevent substance abuse through increasing knowledge and awareness of effects of substance abuse on child development and by generating links between the programme, local substance abuse, and mental health services. FAST also aims to reduce family stress by developing ongoing supports for parents and children, by facilitating parents' access to local supports and agencies, and by fostering personal achievement and self‐esteem in participants. This element of the programme is referred to as FASTWORKS.
FAST is delivered in a number of age‐specific versions, which have been categorised in various ways. The table below provides an overview of the core programmes, details of which can be found at www.familiesandschools.org. Details of Baby FAST can be found in Fletcher 2013.
| FAST versions across age groups | |
| FAST version | Age group |
| Baby FAST | For young parents and their infants from birth to 3 years of age |
| Elementary school level | For families and their children aged 3 to 10 years |
| Middle school level | For parents and students from 11 to 14 years of age |
| High school level | For families and students aged 13 to 18 years |
The FAST curriculum
The curriculum comprises a set of core elements, 40% of which must be implemented 'precisely' in each of the age‐specific versions. The remaining 60% can be adapted as required to best meet the needs of participating families.
For each FAST version, there are two levels of implementation: 'standard' for a single site, and 'multi‐hub' for multiple, "simultaneous cycles at the same location" (www.familiesandschools.org/programs). Furthermore, each version can be delivered in one of three editions, as listed below.
-
Parent Involvement FAST, with an emphasis on drug and alcohol misuse.
-
Healthy FAST, concentrating on physical and mental health.
-
Achieve FAST, for families of children with special needs.
In all its versions, participation is voluntary, with families invited to attend FAST sessions (usually held after school and, with the exception of Baby FAST, on school premises).
The core programme comprises 8 to 12 weekly sessions of 2.5 hours' duration, usually delivered to between 5 and 10 families by a school site team comprising a professional from the host school (teacher), a mental health professional from FAST, an Alcohol or Drugs Professional, and a parent liaison who has graduated from the FAST programme. In each session, parents are helped to lead their family in "sharing a meal, singing, doing family crafts and playing fun communication games for one hour" (McDonald 2012a, p 79). In the following hour, families separate into parent‐only and children‐only play time. The parents first talk in pairs for 15 minutes ('buddy time'), then participate in a 45‐minute shared session with other parents. This session has no set agenda and is designed to foster bonding and to help parents to 'find their voice'. In the last half hour, parents are coached in how to play responsively for 15 minutes with one child; this is followed by a whole family session organised around routine closing activities. This last session includes a lottery in which every family wins once. The focus is on experiential learning rather than didactic teaching. This core programme encompasses families with children aged 3 to 13/14 years (eight grade), with activities tailored to the age groups being served.
A typical session consists of a family meal, family communication games, a parental self‐help group session, supervised children's play, one‐to‐one mediated parental play therapy, opening and closing routines, and family rituals. Whilst 40% of the programme must be implemented precisely, the remaining 60% can be adapted to meet the needs of the target population.
At the end of the eight‐week programme, families are encouraged to meet monthly over a two‐year period under the acronym FASTWORKS (Families and Schools Together, Working, Organising, Relaxing, Knowing, Sharing). FASTWORKS is organised by a Parent Advisory Council that is made up of elected FAST 'graduates', each of whom is given a budget and responsibility to plan and implement the two‐year programme.
Baby FAST
Baby FAST is specifically designed for young mothers and their infants aged from birth to three years. It is designed to "engage young parents, particularly teenagers, in a socially inclusive experience, thereby counteracting the social disapproval and stigma they have encountered from professionals to date" (Fletcher 2013, p 154). It also seeks to reduce the risks associated with social isolation, improve relationships between parents and grandparents, and reinforce protective factors. In Baby FAST, grandparents (or other support persons) are also involved. The programme structure is broadly similar, but the content is amended to foster developmentally appropriate parent‐baby activities and includes "a structured group discussion using created scenarios, a shared meal, [and] a grandmothers' mini therapy group" (Fletcher 2013, p 155). In Baby FAST, at least 50% of the delivery team consists of service users, with as many drawn from those who have themselves experienced teenage parenting. The team, which must be racially and culturally representative of the community served, includes a young mother, a young father, a grandmother, a social worker, a health professional, and someone who specialises in infant massage. (ibid). Although supported by school and preschool systems, Baby FAST is geared towards supporting parents to help prepare their children for learning. It is often used as an adjunct to home visiting programmes and ‐ unlike other versions of FAST ‐ is normally provided in community settings other than schools. When directed specifically at teenage mothers, it is referred to as Teen FAST.
The aims of each version of FAST for both the child and the family are shown below in their respective tables.
| Child ‐ Explicit FAST core outcomes for the child across FAST versions | ||||||
| FAST aims | FAST version | |||||
| Baby | Pre‐K | Kids | Middle | Teen | ||
| Improve interaction with education and scholastic outputs | X | X | X | X | ‐ | |
| Reduce unhealthy behaviours | X | X | X | X | X | |
| Reduce stress, aggression, and violence | ‐ | ‐ | X | X | X | |
| Improve self‐esteem and coping skills | ‐ | ‐ | X | X | X | |
| Family ‐ Explicit FAST core outcomes in the family realm across FAST versions | ||||||
| FAST aims | FAST version | |||||
| Baby | Pre‐K | Kids | Middle | Teen | ||
| Reduce compulsive/impulsive behaviours (aggression, anxiety, depression) | X | X | X | X | X | |
| Reduce conflict and stress | X | X | ‐ | ‐ | ‐ | |
| Reduce substance abuse | ‐ | ‐ | X | X | X | |
| Improve parenting skills | X | X | ‐ | ‐ | ‐ | |
| Improve family cohesion | X | ‐ | X | X | X | |
| Improve communications | X | X | X | X | ||
| Increase child development and learning environment | X | X | X | X | X | |
| Improve parental self‐esteem and coping skills | X | X | ‐ | ‐ | ‐ | |
| Improve community/social capital | ‐ | X | X | X | X | |
Recruitment
In each school where FAST is offered, when a teacher identifies a child at risk, he or she informs the parent of these concerns and the availability of the FAST programme. This 'targeted recruitment' is followed by a 30‐minute home visit from a member of the FAST staff, accompanied by a parent graduate. Layzer 2001 argued that, due to the highly structured nature of the FAST home visit, the recruitment process itself could be considered to be part of the intervention. In Baby FAST, parents are enrolled by means of outreach programmes in the community, as well as by open enrolment.
Training and delivery
The programme requires that the implementation site must have one certified trainer for each FAST team. Training consists of four days' training over four months, including two days' attendance at workshops, three site visits, and one review day. Family size varies across studies from between two and ‘nine or more’ children (McDonald 2009a): for example, in McDonald 2010, the average number of children per family was 4.9, and in Crozier 2010, it was 2.4.
With the exception of Baby FAST, the programme is delivered on school premises. Baby FAST sessions take place in community locations such as churches and clinical and children's centres.
How the intervention might work
FAST was developed to address the limitations of unidimensional (school or home) and unidirectional (school to home) interventions. With children spending, on average, 30 hours a week at school and 138 hours within their family and community, an intervention that recognised the relatively limited influence that schools can maintain and aimed to capture the influence of wider family and social networks was considered to have greater potential to sustain positive outcomes (see above). Coote 2000 describes the main working characteristics of FAST as an early intervention, ideally reaching at‐risk children early on in their life course, but also providing strategic support at key transition points such as adolescence. As detailed in the programme's logic model (Figure 1), FAST is designed to promote prosocial development in children and families by creating a collaborative support system of family, school, peers, community, and professionals, to develop protective behaviours that promote family resilience and prevent maladaptive behaviours from becoming entrenched.

Fast logic model. Copyright © 2016 Families and Schools Together, Inc.: reproduced with permission.
FAST aims to nurture high levels of participation and completion of the intervention by encouraging voluntary participation and supportive networks, combined with incentives and structured, enjoyable, interactive group programmes. Family support may include transport to FAST meetings, a meal, child care, prize winning, and access to social supports. Engagement is encouraged through interactive tasks with clear learning goals, and learning takes place in an atmosphere of mutual support rather than passive parental education or training. Conflict and criticism are actively discouraged, whilst positive and supportive behaviours, including the establishment of parental roles, are reinforced through repetition and task completion. Family members are encouraged to act out and discuss their emotions through a positive 'Feelings Charades' activity, designed to break down barriers and facilitate talking openly in family groups about each individual's feelings. A short time is set aside during each session for one‐to‐one play sessions ('Special Play Time'), where adults must let the child lead the play activity and refrain from bossing, teaching, or directing the child, instead learning to let the child direct their time together.
Parents are encouraged to strengthen their relationships with each other by communicating during 'Buddy Time' ‐ a session that allows adults to talk about their day in a controlled, child‐free environment, supported by the following 45‐minute, parental self‐help group exercise. Family cohesion is fostered through family group tasks such as developing a family flag, cooking a family meal, singing, and participating in structured, family communication games. At the end of the FAST session, community is reinforced through announcements (birthdays or other notable events) and a closing ritual. Once families have completed the eight‐week programme, a graduation ceremony is held within the school, and family and friends are encouraged to attend and support the graduating families. Once completed, the further two years of support provided through the FASTWORKS programme is designed to help maintain and further develop progress.
Why it is important to do this review
Several randomised controlled trials (RCTs) have evaluated the effectiveness of FAST, but, to date, no systematic review of FAST has been conducted to summarise and critically appraise this evidence. This review aims to fill this gap.
Objectives
To assess the effectiveness of the Families and Schools Together (FAST) programme in improving outcomes among children and their families.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) and quasi‐RCTs (in which methods of allocation to groups are not truly random, e.g. day of week, case number).
Types of participants
Families with children from birth to age of completion of compulsory education from all ethnic backgrounds and family sizes, however defined by the triallists.
Types of interventions
FAST programmes compared with waiting list, usual services, alternate service, or no treatment.
Types of outcome measures
We assessed outcome measures (1) immediately after completion of the intervention (zero to two months), (2) at short‐term follow‐up (three to nine months), and (3) at long‐term follow‐up (10+ months after completion of the intervention).
We recorded the timing of outcome assessment as presented in studies.
Primary outcomes
Child outcomes
-
Improved school performance*, as measured by grades or marks that students earn, standardised educational tests, performance tests, or other objective measure of educational attainment. Grades/marks that describe academic performance in at least two classes in the same time frame are eligible (e.g. grade in a math course is not eligible, average grade in academic courses is eligible, average grade across all classes is eligible). Grades/marks in a single course are not eligible.
-
Adverse outcomes. Any reported increase in targeted negative child behaviours or conversely reported decrease in promoted positive behaviours, including school performance (which may be indicative of group contagion effect).
Parent outcomes
-
Reduced parental substance use*, as measured by any standardised self‐report or objective measure of substance use, not including indirect attitude, perception, or awareness measures (Foxcroft 2011).
-
Reduced parental stress*, as measured by any standardised measure of parental stress such as the Parenting Stress Index (Loyd 1985).
Secondary outcomes
Child outcomes
-
Improved internalising behaviours or symptoms at school or at home*, as recorded on a standardised measure such as the internalising subscale of the Child Behaviour Checklist (Achenbach 1991), or on a similar standardised measure.
-
Improved externalising behaviours or symptoms at school or at home*, as recorded on a standardised measure such as the externalising subscale of the Child Behaviour Checklist (Achenbach 1991), or on a similar standardised measure.
-
Reduced substance use*, as measured for example by any self‐report or objective measure of alcohol consumption, including quantity, frequency, or incidence of drunkenness (Foxcroft 2011).
-
Increased school attendance, as measured by any objective record of school attendance such as a school or class register.
-
Reduced youth delinquency, as measured by self‐reports or official records of contacts with the juvenile justice system or another similar law enforcement agency.
Parent outcomes
-
Increased parental self‐efficacy*, as measured by improved scores on a standardised measure of parental self‐efficacy such as the Self‐Efficacy for Parenting Tasks Index (SEPTI; Coleman 2000), or on a similar standardised instrument.
-
Improved parent‐child relationship*, as measured by improved scores on a standardised measure of the parent‐child relationship such as the Parent‐Child Relationship Inventory (PCRI; Gerard 1994), or on a similar standardised measure.
-
Increased parental engagement with education*, as measured by both teachers' and parents' reports of parental involvement with education, including attendance at school‐based events, correspondence between parent and teacher, parental engagement with homework, learning activities, and educational materials, as well as extracurricular activities, objective measures of parental values and attitudes towards education, and the aspirations they have for their child's development.
-
Increased parental uptake of services (mental health, drug and alcohol), as measured through reported referrals to, or attendance at, mental health, drug, and/or alcohol services.
-
Increased parental involvement in community‐based activities.
Family outcomes
-
Improved family relationships*, as measured by improved scores on a standardised measure of family relationships such as the Family Environment Scale (FES; Moos 1994), or on a similar standardised instrument.
-
Reduction in child abuse and neglect, as measured by reduced incidence of child maltreatment on a standardised measure of child abuse and neglect such as the Juvenile Victimisation Questionnaire (JVQ; Finkelhor 2005), or on a similar standardised measure, or by official records from law enforcement or social welfare agencies.
We will use those outcomes marked with an asterisk to populate the 'Summary of findings' table for this review.
Search methods for identification of studies
We conducted electronic searches of bibliographic databases, government policy databanks, and professional websites using the search strategies in Appendix 1. We did not apply any geographical, language, or publication restrictions, and we planned to seek translations for reports published in languages other than English. We confined our searches to information post 1988 ‐ the year that FAST was developed.
Electronic searches
We searched the following electronic resources in February 2017, and we updated the searches between 19 October and 14 December 2018.
-
Cochrane Central Register of Controlled Trials (CENTRAL; 2018 Issue 12), in the Cochrane Library, which includes the Cochrane Developmental, Psychosocial, and Learning Problems Specialised Register (searched 14 December 2018).
-
MEDLINE Ovid (1946 to 19 October 2018).
-
Embase Elsevier (1980 to 24 October 2018).
-
PsycINFO EBSCO (1806 to 19 October 2018).
-
Education Resources Information Center (ERIC) EBSCOhost (1966 to 19 October 2018).
-
British Education Index (BEI) EBSCOhost (1950 to 13 November 2018).
-
ProQuest Education Database (1988 to 13 November 2018).
-
Education Abstracts (HW Wilson) EBSCOhost (1983 to 13 November 2018).
-
Social Science Citation Index Web of Science (1970 to 24 October 2018).
-
Conference Proceedings Citation Index Social Science and Humanities Web of Science (1990 to 13 November 2018).
-
Evidence for Policy and Practice Information (EPPI) Centre Database of Education Research (eppi.ioe.ac.uk/webdatabases/Intro.aspx?ID=6) (searched 5 November 2018).
-
Campbell Library of Systematic Reviews (www.campbellcollaboration.org/library.html) (searched 14 December 2018).
-
Cochrane Database of Systematic Reviews (CDSR; 2018 Issue 12), part of the Cochrane Library (searched 14 December 2018).
-
Database of Abstracts of Reviews of Effectiveness (DARE; www.crd.york.ac.uk/CRDWeb/) (searched 5 November 2018).
-
Epistemonikos (www.epistemonikos.org) (searched 13 December 2018).
-
UK Clinical Trials Gateway (www.ukctg.nihr.ac.uk/clinical‐trials) (searched 13 December 2018).
-
ClinicalTrials.gov (clinicaltrials.gov) (searched 13 December 2018).
-
World Health Organization International Clinical Trials Registry Platform (WHO ICTRP; www.who.int/ictrp/en) (searched 14 December 2018).
Searching other resources
We examined the reference lists of reports, reviews, and primary studies, and we contacted the FAST programme developer and independent researchers to identify studies not retrieved by electronic searches. In addition, we searched the Families and Schools Together website (familiesandschoolstogether.com), the US Department of Education's What Works Clearinghouse (ies.ed.gov/ncee/wwc/FWW), the US Department of Education's grant awards (www.ed.gov/category/subject/grants), and the UK's Education Endowment Foundation's projects and evaluation page (educationendowmentfoundation.org.uk/projects‐and‐evaluation).
Data collection and analysis
We used Review Manager 5 (RevMan 5) to organise and analyse our data (Review Manager 2014). We used EndNote to manage our bibliographical data (EndNote 2013).
Selection of studies
At least two review authors independently reviewed all titles and abstracts to determine potentially relevant studies. We retrieved the full text of any citation that was identified by at least two review authors as potentially relevant (the two review authors worked independently, and a third review author (usually JV) reconciled disagreements). At least two review authors independently read all retrieved papers of potentially relevant studies to determine whether they satisfied the inclusion criteria (Criteria for considering studies for this review). Review authors resolved disagreements by discussion with JV and GM, as needed. When we excluded a retrieved study, we documented the reasons for its exclusion (see Figure 2 and Characteristics of excluded studies).

Study flow diagram for the literature search.
Data extraction and management
For each included study, one review author (JV), along with a second independent review author (AF, DK, or SL), extracted and recorded all relevant data on a specifically designed and piloted data collection form. Review authors consulted with one another to resolve disagreements, as needed. We extracted the following data.
-
Study characteristics: study author(s), year of publication, journal or source, contact details, study design, study duration, attrition details, language.
-
Child characteristics: age, gender, ethnicity, special educational needs or disability.
-
Parent characteristics: age, gender, ethnicity, educational attainment or qualifications or both, employment status.
-
Family characteristics: family size, marital status, annual income.
-
School characteristics: population served, size, other interventions, location.
-
Outcomes and measures used: details on all primary and secondary outcome measures, including measures used, length of follow‐up, summary data, means, and standard deviations.
-
Cost incurred by the intervention.
We collected information on study design and implementation in a format suited to completion of the 'Risk of bias' tables (Higgins 2011a). We collected raw (unadjusted) results in preference to adjusted results, for reasons of consistency of interpretation across studies, and because this choice of analysis appears to be less susceptible to selective reporting bias (e.g. it prevents potentially biased selection of covariates for inclusion in the model). This decision may, however, increase the risk of bias that may be attributable to baseline differences, such as those arising from differential dropout.
Assessment of risk of bias in included studies
We assessed the risk of bias of included studies using Cochrane's 'Risk of bias' tool (Higgins 2011b). For each included study, two review author pairs independently assessed the risk of bias within each included study based on the seven domains listed below, with review authors' judgements presented as 'high', 'low', or 'unclear' risk of bias (see Table 1). When disagreements occurred between the judgements of review authors, they first sought to resolve these disagreements themselves. If needed, they consulted a third review author (usually JV, unless he was one of the review authors, in which case GM was consulted).
| Random sequence generation |
|
|
| Allocation concealment |
|
|
| Blinding of participants and personnel |
|
|
| Blinding of outcome assessment |
|
|
| Incomplete outcome data |
|
|
| Selective outcome reporting |
|
|
-
Random sequence generation. We describe the methods used to generate the allocation sequence in detail, to assess whether it was likely to produce comparable groups of participants. The question: was the allocation sequence adequately generated?
-
Allocation concealment. We describe the methods used to conceal the allocation sequence in detail, to determine whether intervention allocation has been concealed before and during the allocation process. The question: was the allocation adequately concealed?
-
Blinding of participants and personnel. Given the nature of the intervention, it is not possible to blind participants or personnel to knowledge of the allocated intervention, and we examine the extent to which this may have introduced high risk of bias. The question: was performance biased due to knowledge of the allocated interventions by participants and personnel during the study?
-
Blinding of outcome assessment. We provide a description of the methods used to blind outcome assessors to knowledge of the allocated intervention to ascertain whether adequate protection of concealment was maintained throughout the study. The question: was knowledge of the allocated intervention adequately prevented during the study?
-
Incomplete outcome data. We describe the completeness of outcome data for each main outcome, noting reported attrition and exclusions in each intervention group, reasons for attrition or exclusion, and any re‐inclusions in analysis employed by the review authors. The question: were incomplete outcome data adequately addressed?
-
Selective outcome reporting. We examine the comprehensiveness of outcome reporting in relation to published reports or available study protocols to ascertain whether selective outcome reporting was employed. The question: are reports of the study free from selective outcome reporting?
-
Other sources of bias not addressed under the preceding domains. We examined study protocols in sufficient detail to ascertain whether other sources of bias are present. The question: are reports of the study free from the sources of bias listed in the table below?
| Other potential sources of bias | |
| Design bias | Description of effects |
| Cluster‐randomised trials | Recruitment bias |
| Baseline imbalance | |
| Loss of clusters | |
| Incorrect analysis | |
| Comparability with RCT | |
| Early stopping of trial | Results showing statistically significant, large effects |
| Occurrence of harm | |
| Stopping of study contrary to protocol | |
| Randomised block design | In certain circumstances, compromised selection bias and blinding caused by the blocking process |
Measures of treatment effect
Where possible, we calculated intervention effects using Cochrane's software, RevMan 5 (Review Manager 2014).
Dichotomous data
With one exception, all outcomes were measured on a continuous scale. The exception was Layzer 2001 (see Analysis 7.3), in which data were presented as a proportion of parents scoring "high" on subscales that assess family environment. We computed an odds ratio for these effects, then performed a Cox transformation to arrive at an approximate standardised mean difference effect size (and its standard error).
Continuous data
We calculated standardised mean differences (SMDs) (because studies used different measures to assess the same outcomes) and 95% confidence intervals (CIs).
Multiple outcomes
When an included study provided multiple, interchangeable measures of the same construct at the same point in time (e.g. multiple measures of the quality of family relationships), we calculated the average SMD across all relevant outcomes and the average of their estimated variances. This strategy is intended to avoid the need to select a single measure, and to avoid inflated precision in any meta‐analyses that might arise from placing more weight on studies that report on more than one outcome measure than on others that rely on a single measure. Studies were too few to support robust variance estimation.
Some studies measured outcomes at multiple points in time. We analysed outcomes separately for the following three time periods: (1) immediately after completion of the intervention (zero to two months), (2) short‐term follow‐up (three to nine months), and (3) long‐term follow‐up (10+ months after completion of the intervention).
Economic issue
We recorded any costs incurred by the FAST programme reported within the studies under review.
Unit of analysis issues
Cluster‐randomised trials
Several of the studies included in this review are cluster‐randomised trials, and sometimes, study authors analysed data from cluster trials as if the participants were randomly assigned to conditions. In these cases, the standard error of the test statistic can be too small because it ignores systematic similarity between participants within the same cluster. One implication of this is that the probability values that arise from the hypothesis tests can be too small. We planned on implementing a correction to account for this (see Macdonald 2017; Table 2); the correction was needed for several studies in this review. However, we did not implement this correction because doing so would not have changed the conclusions of the review in any way. Most of the effect sizes in the included studies already were not statistically significant, and the three that were statistically significant remained so even after the most conservative cluster correction that we proposed in the protocol (i.e. intraclass correlation coefficient (ICC) = 0.10). Implementing the cluster correction would similarly not have affected the results of the meta‐analyses that we conducted (although in some cases, the 95% CIs would have been somewhat wider).
| Issue | Method |
| Measures of treatment effect | Continuous data Where necessary, we will compute effect measures from P values, t statistics, analysis of variance (ANOVA) tables, or other statistics |
| Unit of analysis issues | Cluster‐randomised trials Where clustering has been appropriately accounted for within the analysis of the original study data, clustered data can be used in a meta‐analysis. However, a 'unit of analysis' error occurs when data from cluster‐randomised trials have been analysed as though the unit of allocation has been the individual rather than the cluster. In these circumstances, corrections are required to produce accurate effect size estimates (Section 16.3.4; Higgins 2011c). To calculate the design effect, we need a measure of the relative variation both within and between clusters. This is known as the intraclass correlation coefficient (ICC). Where the ICC from the original trial is not available, we will use external estimates from similar studies to calculate the design effect. If there are no reported estimates in the literature, we will perform a sensitivity analysis using low (0.01), medium (0.05), and high (0.10) values for ICC. However, as the design effect must be rounded up for entry into RevMan 5 (Review Manager 2014), this approach may be unsuitable for small studies, and we may need to employ an alternative approach that multiplies the standard errors (SEs) of the effect size by the square root of the design effect. In either case, where we include cluster‐randomised trials in the meta‐analysis, we will clearly identify them and will explain the method of calculating effect size estimates and their standard errors. In these circumstances, we will employ a sensitivity analysis to test the robustness of any conclusions deduced from these methods (see Sensitivity Analysis below) |
| Multiple treatment arms We do not anticipate finding studies with multiple treatment groups. However, should we identify such studies, we will first combine all eligible intervention arms and compare these with all control arms, making a single, pair‐wise comparison. If such a strategy seems likely to prevent the investigation of important sources of heterogeneity, we will keep intervention arms separate and will compare each with a common control group, dividing the sample size of the latter proportionately across each comparison, thereby preventing double counting of individuals (Section 16.5.5; Higgins 2011c) | |
| Dealing with missing data | Where we are certain that missing data are 'missing at random' and unlikely to be related to the characteristics of the participants or study design, we will analyse the available data while ignoring the missing data (Higgins 2011c). Conversely, where there is no reason to believe that data are missing at random ‐ that is, as a result of publication or selective reporting bias ‐ we will work with a statistician to select replacement values using imputed mean values or multiple imputation methods |
| Assessment of reporting biases | Where 10 or more studies provide data on a particular outcome, we will draw funnel plots (estimated differences in treatment effects against their standard error). Symmetrical funnel plots are associated with low levels of bias. Asymmetrical funnel plots may reflect publication bias, but they can also reflect real relationships between trial size and effect size, such as when larger trials have lower compliance, and compliance is positively related to effect size. If we have reason to think that this is happening, we will look for a possible explanation in clinical variation across studies To test directly for publication bias, we will conduct a sensitivity analysis (see Sensitivity Analysis below) to compare results from published data vs unpublished data and data from other sources |
| Data synthesis | In future updates of this review, should we encounter serious funnel plot asymmetry, we will assume that neither the fixed‐effect nor the random‐effects models are appropriate and will present the results of both. Where both indicate the presence or absence of an effect, we will assume that we can have some confidence in the results. Where they disagree, we will report this In future, if some included studies report an outcome using dichotomous outcome measures and others use continuous measures, we will convert results from the former, from an OR to an SMD, as long as there is reason to assume that the underlying continuous measure approximates a normal or logistical distribution. Where this is not the case, we will conduct separate analyses |
| Subgroup analysis and investigation of heterogeneity | As the overuse of subgroup analysis is problematic (Deeks 2011), we will use subgroup analyses only to determine a small number of effect modifiers We will conduct the following 4 subgroup analyses.
N.B. Since the protocol was published (Macdonald 2017), the various FAST programmes have been renamed as Baby FAST, Elementary Level, Middle School Level, and High School Level FAST.
As no family size effects are noted in Crozier 2010, McDonald 2009b, and McDonald 2010, despite reports of differing average family sizes, we will not include family size in the subgroup analysis. |
| Sensitivity analysis | We will use sensitivity analyses to explore the impact of studies at high risk of bias on the robustness of review results, restricting the analyses to (1) studies or outcomes with low risk of assessment bias, (2) studies with low risk of attrition bias, and (3) studies with low risk of reporting bias. In addition:
|
FAST: Families and Schools Together.
FASTWORKS: Families and Schools Together, Working, Organising, Relaxing, Knowing, Sharing.
OR: odds ratio.
RCT: randomised controlled trial.
SMD: standardised mean difference.
Studies with multiple treatment groups
We did not find any studies that used multiple treatment groups. See our protocol ‐ Macdonald 2017 ‐ and Table 2 for methods for handling of studies with multiple treatment groups in future updates of this review.
Dealing with missing data
Where necessary, we contacted the corresponding authors of included studies to secure any unreported data (e.g. group means and standard deviations, details of dropouts, reasons for attrition). We also contacted other study authors as necessary. One study reported outcomes only for those participants who were considered to have graduated FAST (McDonald 2012b). We attempted to obtain the additional information necessary to facilitate analyses according to intention‐to‐treat (ITT) principles, but the data were not available. We describe missing data and attrition/dropout rates for each included study in the 'Risk of bias' tables and discuss the extent to which missing data could affect the results of the review or the conclusions drawn.
Assessment of heterogeneity
We assessed and described clinical variation across included studies (variability in participants, the FAST programme) and methodological diversity (randomisation, randomisation concealment, blinding of outcomes assessment, losses to follow‐up, etc.). We described statistical heterogeneity by computing the I² (Deeks 2011; Section 9.5) ‐ a quantity that broadly describes the proportion of variation in point estimates that is due to heterogeneity rather than to sampling error. In addition, we used a Chi² test of homogeneity to determine the strength of evidence that heterogeneity is genuine. Inconsistency between studies may be ambiguous and depends upon several factors; therefore results of the I² test may be roughly interpreted as follows.
-
0% to 40% might not be important.
-
30% to 60% may represent moderate heterogeneity.
-
50% to 90% may represent substantial heterogeneity.
-
75% to 100% represents considerable heterogeneity.
Assessment of reporting biases
We were unable to investigate the potential impact of reporting bias by using funnel plots, as the maximum number of studies contributing to any outcome was five. See our protocol ‐ Macdonald 2017 ‐ and Table 2 to learn how we will manage this if future updates permit.
Data synthesis
We synthesised the data using RevMan 5 (Review Manager 2014). All overall effects were calculated using inverse variance methods. As planned, we used both a fixed‐effect model and a random‐effects model and compared the two to assess the impact of statistical heterogeneity. We present the results from the fixed‐effect model, given that the review is focused on one intervention. See our protocol ‐ Macdonald 2017 ‐ and Table 2 for further details of methods planned but not implemented in this first review of FAST.
'Summary of findings' table
We present the main findings of the review in a 'Summary of findings' table, developed using the GRADEpro Guideline Development Tool (GRADEpro GDT 2017). summary of findings Table for the main comparison briefly describes the population, setting, intervention, and comparison/control for each included study before setting out a summary and assessment of the certainty of the main results, overall completeness and applicability of evidence, certainty of the evidence, and potential sources of bias for each outcome (Schünemann 2011a; Section 11.5.6).
Using the GRADE approach (Schünemann 2011b; Section 12.2), two review authors independently graded the certainty of evidence as high, moderate, low, or very low, according to the presence of the following five factors: limitations in design and implementation of available studies; indirectness of evidence; inconsistency of results; imprecision of results; and high likelihood of publication bias.
As empirical evidence suggests that relative effect measures are both more consistent and more inclined to be understood and used by practitioners, we planned to present odds ratios (ORs) for dichotomous data in the 'Summary of findings' table in terms of a percentage risk ratio reduction; however, all outcomes were measured on a continuous scale.
Subgroup analysis and investigation of heterogeneity
Studies were too few to support any of our planned subgroup analyses in this first systematic review of FAST. Please see our protocol ‐ Macdonald 2017 ‐ and Table 2 for our published strategy on the exploration of potential effect modifiers of FAST.
Sensitivity analysis
We did not conduct any sensitivity analyses in this review because (1) all studies are RCTs, (2) there did not appear to be outliers, (3) all of the meta‐analytical weights are within reason, and (4) studies were too few to support an analysis of cluster RCTs versus individually assigned RCTs. Please see our protocol ‐ Macdonald 2017 ‐ and Table 2 for sensitivity analyses planned but not implemented in this review.
Results
Description of studies
Results of the search
The searches generated 4306 records in total. We excluded 4267 records at title and abstract stage, and we obtained the full texts of 39 papers that merited closer inspection. Assessment of the full texts of each of these led to the inclusion of 16 reports (10 studies; see Included studies). We excluded 23 reports, 18 with reasons (see Excluded studies). The five remaining reports were duplicates of studies that we had already screened. See Figure 2.
Included studies
We included 10 unique RCTs in this review (AIR 2018; Billingham 1993; Knox 2011; Kratochwill 2004; Kratochwill 2009; Layzer 2001; Lord 2018; McDonald 2012b; Moberg 2007; López Turley 2017).
We provide further details about the included studies below and in the Characteristics of included studies tables.
Study design
All 10 studies were RCTs. Five of the 10 studies were cluster‐RCTs (AIR 2018; Knox 2011; López Turley 2017; Lord 2018; Moberg 2007).
Settings and locations
With the exception of one study that took place in the UK (Lord 2018), all studies were conducted in the USA. Of the USA‐based studies, all except Kratochwill 2004 and McDonald 2012b took place in urban environments.
In McDonald 2012b, the intervention took place at a community refugee centre, and in Knox 2011, the intervention took place at a community‐based health centre. Layzer 2001 is unclear about where the intervention took place: "at the school (or other community center)" (quote, p B2‐2). All other studies were implemented in the schools attended by children identified by teachers for inclusion in FAST.
Sample size
Analysis sample sizes varied widely across studies, ranging from two studies with samples of 10 ‐ McDonald 2012b ‐ and 32 ‐ Billingham 1993 ‐ children, to two studies with 2832 ‐ López Turley 2017 and 4221 children ‐ Lord 2018. Over 9000 children and their families contributed to at least one outcome assessed in this review.
Participants
Children were five to nine years old (mean age approximately six years).
The race/ethnicity of participants was not uniformly reported in studies, but at least 62% of children in the USA‐based studies were from an ethnic minority group (largely African American or Latino). About half of children in the samples were girls. Most children were considered to be at risk (vaguely defined), and only one study explicitly recruited children who were believed to be at risk for needing special education services (Kratochwill 2009). The socio‐economic status of the families was not well described, but given the populations served, it is presumably low in most studies (in Lord 2018, to be eligible for the study, schools must have had more than 20% of students eligible for free school meals). When socio‐economic status was described, it was described as low for most of the families in the sample.
Interventions and comparisons
Given the ages of the children, all included studies evaluated what is sometimes referred to as 'Kids FAST' and sometimes 'Elementary Level FAST', although neither name was used in the papers, which simply described the intervention as "FAST".
All studies appear to have had some involvement from either the intervention developer (Dr McDonald is credited with authorship on four of the 10 RCTs) or the FAST organisation (e.g. by providing training to programme implementers). This led to rather more consistency in the FAST programme elements than might be typical for a complex social intervention. In general, FAST was intended to be implemented in eight weekly, multi‐family group sessions lasting two and a half to three hours. All FAST implementations had a similar structure (e.g. had structured time for group family therapy and parent‐child interaction), but the details of these activities differed somewhat across sites.
In general, the experiences of the comparison students and families were not well articulated across studies. Two studies compared FAST to a presumably ineffective intervention (Layzer 2001 and Moberg 2007 provided literature on parenting). Two studies used a wait‐list control condition (AIR 2018; McDonald 2012b). One study described the control condition as "business as usual" (López Turley 2017). The rest of the studies did not describe the control condition.
Primary outcomes
Of the two primary outcomes related to children, five studies provided data on improved school performance. How these were measured in each of the three studies is summarised in the following table.
| Measures of primary outcomes from included studies | ||
| Outcome domain | Measure | Study |
| Child school performance* | Peabody Picture Vocabulary Test 4 | |
| Woodcock‐Johnson III Tests of Achievement: Literacy Subscale | ||
| Woodcock‐Johnson III Tests of Achievement: Mathematics Subscale | ||
| Curriculum‐based measure: Reading | ||
| Curriculum‐based measure: Math | ||
| Grades earned (average of all academic subjects) | ||
| Key Stage 1 Test (reading and arithmetic) | ||
| State of Wisconsin Standardised Test: Reading Raw Score | ||
| State of Wisconsin Standardised Test: Reading Scale | ||
| State of Wisconsin Standardised Test: Mathematics Scale | ||
| State of Wisconsin Standardised Test: Science Scale | ||
*Outcomes included in summary of findings Table for the main comparison.
No study reported any adverse outcomes.
No study assessed the impact of FAST on either of the two primary outcomes related to parents, namely, reductions in substance misuse (measured by standardised self‐report or objective measures) or parental stress.
Secondary outcomes
As the following table indicates, four studies provided data on three of the five secondary child outcomes, three of which also provided data on two of the five secondary outcomes related to parents.
| Measures of secondary outcomes from included studies | ||
| Outcome domain | Measure | Study |
| Child internalising symptoms* | Revised Child Behavior Checklist: Parent Form | |
| Revised Child Behavior Checklist: Teacher Form | ||
| Child Behaviour Checklist (CBCL) ‐ Internalising: Parent Form | ||
| Child Behaviour Checklist (CBCL) ‐ Internalising: Teacher Form | ||
| Child externalising symptoms* | Social Competence and Behavior Evaluation Scale (LaFreniere 1996) (note, used 10 items that focused on child aggressive behaviour (see p 69), 5 items adapted from Musher‐Eizenman 2004, and 7 items focusing on self‐reported aggressive behaviour from the Metropolitan Area Child Study (MACS 2002)) | |
| Child Behavior Checklist (CBCL) ‐ Externalising: Parent Form | ||
| Child Behavior Checklist (CBCL) ‐ Externalising: Teacher Form | ||
| Parent engagement with education* | Family Involvement Questionnaire: Home‐Based Involvement Subscale | |
| Family Involvement Questionnaire: School‐Based Involvement Subscale | ||
| Family relationships* | Child‐Parent Relationship Scale: Closeness Subscale | |
| Child‐Parent Relationship Scale: Conflict Subscale | ||
| Family Adaptability and Cohesion Evaluation Scale: Cohesion Subscale | ||
| Family Adaptability and Cohesion Evaluation Scale: Adaptability Subscale | ||
| Family Adaptability and Cohesion Evaluation Scale: Cohesion Subscale | ||
*Outcomes included in summary of findings Table for the main comparison.
No study measured the effects of FAST on children's substance use or delinquency, or on increased parental self‐efficacy, parental uptake of services by parents, or their increased involvement in community‐based activities.
Funding sources
All but two studies (Kratochwill 2009 and McDonald 2012b) explicitly mentioned external funding. The UK trial was funded by the Education Endowment Foundation (Lord 2018). The US studies were largely funded by federal agencies, including the National Institute of Child Health and Human Development (López Turley 2017), the Centers for Disease Control and Prevention (Knox 2011), the Department of Education (AIR 2018; Kratochwill 2004; López Turley 2017), the Department of Health and Human Services (Layzer 2001), and the National Institute on Drug Abuse (Moberg 2007). State sources (Wisconsin Department of Public Instruction) funded Billingham 1993.
Excluded studies
Of the 23 studies that were excluded after full text screening, five were duplicate citations of already identified studies, six were not empirical studies, nine were not RCTs, and three were studies of an intervention other than FAST. See Characteristics of excluded studies tables.
Risk of bias in included studies
We describe and present the risk of bias for each included study (separately by outcome, when necessary) in the Characteristics of included studies tables. Below, we present a summary of our judgements, which we also summarise graphically in Figure 3 and Figure 4.
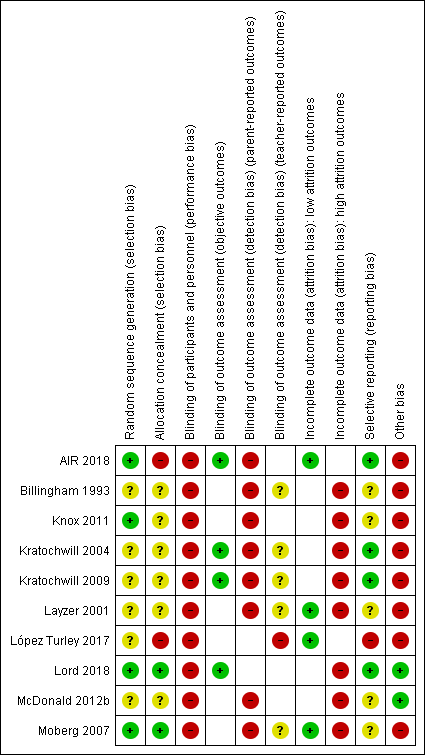
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
Random sequence generation
In terms of random sequence generation, we rated four studies at low risk of bias due to their use of adequate methods of sequence generation (AIR 2018; Knox 2011; Lord 2018; Moberg 2007). We judged the remaining six studies at unclear risk of bias because the method of sequence generation was not described.
Allocation concealment
We judged allocation to be adequately concealed in two studies ‐ Lord 2018; Moberg 2007 ‐ and inadequately concealed in two studies ‐ AIR 2018; López Turley 2017. In AIR 2018, research staff clearly had access to group assignment information during enrolment. In López Turley 2017, it is unclear whether school assignment conditions could have been foreseen in advance of or during enrolment. However, it is clear that participants and programme staff knew the assignment condition before obtaining consent, leaving open the possibility that this knowledge may have influenced the behaviour of the programme staff and/or the participants. We judged the six remaining studies to be at unclear risk of bias in this domain.
Blinding
Performance bias
We judged all studies in this review to be at high risk for performance bias (AIR 2018; Billingham 1993; Knox 2011; Kratochwill 2004; Kratochwill 2009; Layzer 2001; López Turley 2017; Lord 2018; McDonald 2012b; Moberg 2007), as staff were aware of condition assignments, and families in the FAST condition knew that they were participating in an intervention.
Detection bias
Objective outcomes
We judged objective outcomes from four studies to be at low risk of detection bias (AIR 2018; Kratochwill 2004; Kratochwill 2009; Lord 2018). We judged AIR 2018 to be at low risk for detection bias for child school attendance and child academic achievement. Attendance data were taken from school records, and child academic achievement was measured by standardised tests that appear to have been collected from all students. Similarly, child academic outcomes from Kratochwill 2004, Kratochwill 2009, and Lord 2018 were based on standardised tests that appear to have been administered to all students.
Parent‐reported outcomes
We judged all parent‐reported outcomes from eight studies to be at high risk of detection bias because parents knew that they were participating in an intervention (Billingham 1993; Knox 2011; Kratochwill 2004; Kratochwill 2009; Layzer 2001; López Turley 2017; McDonald 2012b; Moberg 2007) .
Teacher‐reported outcomes
We judged teacher‐reported outcomes from five studies to be at unclear risk of detection bias because it is not clear whether teachers were aware of the assignment conditions of the students they were rating (Billingham 1993; Kratochwill 2004; Kratochwill 2009; Layzer 2001; Moberg 2007). We judged one study ‐ López Turley 2017 ‐ to be at high risk of bias because the study authors collected outcome information on students of teachers who, due to school‐level randomisation, appear to have been aware of assignment conditions.
Incomplete outcome data
We judged two studies to be at low risk of attrition bias (AIR 2018; López Turley 2017). Two studies had some outcomes for which we judged attrition bias to be low and others for which we judged attrition bias to be high (Layzer 2001; Moberg 2007). We rated the remaining six studies as having high risk of attrition bias (Billingham 1993; Knox 2011; Kratochwill 2004; Kratochwill 2009; Lord 2018; McDonald 2012b).
We judged two studies to be at low risk of attrition bias (AIR 2018; López Turley 2017). Two studies had some outcomes for which we judged attrition bias to be low and others for which we judged attrition bias to be high (Layzer 2001; Moberg 2007). We rated the six remaining studies as having high risk of attrition bias (Billingham 1993; Knox 2011; Kratochwill 2004; Kratochwill 2009; Lord 2018; McDonald 2012b).
Selective reporting
We rated four studies as having low risk of selecting reporting bias (AIR 2018; Kratochwill 2004; Kratochwill 2009; Lord 2018). AIR 2018 appeared to have an analysis plan that was determined before data collection (p 15). We received statistical output for Kratochwill 2004 and Kratochwill 2009 on all measured outcomes. Lord 2018 was preregistered. We rated López Turley 2017 as having high risk of reporting bias as investigators did not report one measured outcome due to high levels of missing data. For all other studies, we were unable to make a judgement about the risk of reporting bias and thus rated risk as unclear (Billingham 1993; Knox 2011; Layzer 2001; McDonald 2012b; Moberg 2007).
Other potential sources of bias
Participant recruitment presents potential risk of bias in most studies included in this review. In part, this is due to concerns about spillover effects within sites, and in part to the model's explicit theory of change. In most studies, sites were assigned to conditions, and then, within sites, families were recruited into the study. This means that programme staff and families knew their assignment conditions before giving consent to participate ‐ knowledge that in our judgement likely affected participation decisions. We rated Lord 2018, which addressed this potential problem by planning to collect data on all children in the school, and McDonald 2012b, which assigned families to conditions after obtaining their participation consent, to be at low risk of recruitment bias. For all other studies in which recruitment bias was a potential concern, outcomes were collected only for students whose families agreed to participate, and we rated these studies as having high risk of other bias.
Effects of interventions
We conducted both fixed‐effect and random‐effects meta‐analyses when there were at least two studies measuring the same outcome, using the same reporting source (e.g. parent), at the same follow‐up period. We conducted a total of 14 separate meta‐analyses. There were no meta‐analyses in which the between‐studies variance estimate (tau²) was statistically significant. This is not a surprising finding given that the statistical power of this analysis is low when the number of studies is small. More revealing is that in 12 of the 14 meta‐analyses, the estimated between‐studies variance was zero. In these cases, the fixed‐effect and random‐effects models yielded identical results. The two cases in which the between‐studies variance was estimated as larger than zero yielded highly similar results (and the same statistical conclusions). Below, we report the results of the fixed‐effect meta‐analyses.
Primary outcomes
Child school performance
Six studies assessed child school performance ‐ two immediately after the intervention (200 children; Kratochwill 2004; Kratochwill 2009), and four at long‐term follow‐up (approximately 6276 children; AIR 2018; Layzer 2001; Lord 2018; Moberg 2007). In both meta‐analyses, the effect size was small, negative, and not statistically significant.
-
Immediate post‐test: SMD ‐0.06; 95% CI ‐0.34 to 0.22; low‐certainty evidence; Analysis 1.1.
-
Long‐term follow‐up: SMD ‐0.02; 95% CI ‐0.11 to 0.08; moderate‐certainty evidence; Analysis 1.2.
An additional study (120 children) assessed child school performance at follow‐up (Kratochwill 2004). We could not compute an effect size because standard deviations were not reported in the paper. For both measures (reading and math), the effect was negative and was not statistically significant.
No study measured any of the other primary outcomes: child adverse events; parent stress; or parent substance abuse. See above section on 'Outcomes' under Included studies.
Secondary outcomes
Child internalising behaviour
Six studies assessed child internalising behaviour immediately after the intervention, five using parent reports (approximately 646 children; Billingham 1993; Kratochwill 2004; Kratochwill 2009; McDonald 2012b; Moberg 2007), and five using teacher reports (approximately 3557 children; Billingham 1993; Kratochwill 2004; Kratochwill 2009; López Turley 2017; Moberg 2007). Four studies assessed child internalising behaviour at long‐term follow up (Kratochwill 2004; Kratochwill 2009; Layzer 2001; Moberg 2007), using both parent reports (approximately 908 children) and teacher reports (approximately 912 children). In all cases, the effect sizes were negative (which in this case implies better internalising symptoms for FAST children and therefore a positive intervention effect), small, and not statistically significant.
-
Immediate post‐test, parent report: SMD ‐0.05, 95% CI ‐0.21 to 0.10; Analysis 2.1.
-
Immediate post‐test, teacher report: SMD ‐0.09, 95% CI ‐0.18 to 0.00; Analysis 2.2.
-
Long‐term follow‐up, parent report: SMD 0.03, 95% CI ‐0.11 to 0.17; Analysis 2.3.
-
Long‐term follow‐up, teacher report: SMD ‐0.06, 95% CI ‐0.19 to 0.07; Analysis 2.4.
We considered the certainty of the evidence to be low. See summary of findings Table for the main comparison.
Child externalising behaviour
Six studies assessed child externalising behaviour immediately after the intervention, four using parent reports (approximately 627 children; Kratochwill 2004;Kratochwill 2009;McDonald 2012b;Moberg 2007), and four using teacher reports (approximately 3557 children; Kratochwill 2004;Kratochwill 2009;López Turley 2017;Moberg 2007). Four studies assessed child externalising behaviour at long‐term follow‐up (Kratochwill 2004; Kratochwill 2009; Layzer 2001; Moberg 2007), using both parent reports (approximately 754 children) and teacher reports (approximately 912 children). In all cases, the effect sizes were negative (which in this case implies better externalising symptoms for FAST children and therefore a positive intervention effect) and small.
-
Immediate post‐test, parent report: SMD ‐0.04, 95% CI ‐0.20 to 0.12; Analysis 3.1.
-
Immediate post‐test, teacher report: SMD ‐0.02, 95% CI ‐0.11 to 0.07; Analysis 3.2.
-
Long‐term follow‐up, parent report: SMD ‐0.19, 95% CI ‐0.32 to ‐0.05; Analysis 3.3.
-
Long‐term follow‐up, teacher report: SMD ‐0.10, 95% CI ‐0.24 to 0.04; Analysis 3.4.
We considered the certainty of the evidence to be low. See summary of findings Table for the main comparison.
One study assessed child externalising behaviour using three different measures: one parent report and two child reports (282 children; Knox 2011). We were unable to include these data in our meta‐analysis because we lacked sufficient information to compute effect sizes for these outcomes. The study authors reported no statistically significant differences between the FAST and control groups for any of these measures.
Child school attendance
Three studies assessed child school attendance: one at short‐term follow‐up (1361 children; AIR 2018) and two at long‐term follow‐up (1430 children; AIR 2018; Layzer 2001). Both effect sizes were small and were not statistically significant.
-
Short‐term follow‐up: SMD 0.02, 95% CI ‐0.11 to 0.15; Analysis 4.1.
-
Long‐term follow‐up: SMD 0.03, 95% CI ‐0.10 to 0.16; Analysis 4.2.
We considered certainty of the evidence to be moderate.
Parent engagement with education
Three studies assessed parent engagement with education: one immediately after completion of the intervention (approximately 473 children; Moberg 2007), one at short‐term follow‐up (1050 children; AIR 2018), and two at long‐term follow‐up (1232 children; AIR 2018; Layzer 2001). The effect size observed in the one study at immediate post‐test was possibly large enough to be meaningful, and the CI included values that, if real, were likely to be meaningful (SMD 0.34, 95% CI 0.15 to 0.53; Analysis 5.1). The effect size observed in one study at short‐term follow‐up was probably not large enough to be meaningful, but the CI included values that, if real, were possibly large enough to be meaningful (SMD 0.20, 95% CI 0.06 to 0.33; Analysis 5.2). The effect size observed in two studies that assessed parent engagement with education at long‐term follow‐up was very small, and its CI did not include values that are meaningful (SMD 0.03, 95% CI ‐0.07 to 0.12; Analysis 5.3).
Parent involvement in community‐based activities
One study assessed parent involvement in the community at long‐term follow‐up (386 children; Layzer 2001). The effect size was small (SMD 0.11, 95% CI ‐0.15 to 0.38; Analysis 6.1), and the CI contained values that, if real, were possibly meaningful.
Family relationships
Seven studies assessed the quality of the family relationship: four immediately after completion of the intervention (183 children; low‐certainty evidence; Billingham 1993; Kratochwill 2004; Kratochwill 2009; McDonald 2012b), one at short‐term follow‐up (1053 children; low‐certainty evidence; AIR 2018), and four at long‐term follow‐up (approximately 2569 children; low‐certainty evidence; AIR 2018; Kratochwill 2009; Layzer 2001; Moberg 2007). In all cases, effect sizes were small.
-
Immediate post‐test: SMD 0.03, 95% CI ‐0.27 to 0.33; Analysis 7.1.
-
Short‐term follow‐up: SMD 0.00, 95% CI ‐0.12 to 0.13; Analysis 7.2.
-
Long‐term follow‐up: SMD 0.08, 95% CI ‐0.03 to 0.19; Analysis 7.3 (moderate‐certainty evidence).
Of these three results, only the CI for the immediate post‐test contained values that, if real, were possibly large enough to be meaningful.
No included study assessed the following secondary outcomes: child substance abuse; child delinquency; parental self‐efficacy; parental uptake of services (mental health, drug, and alcohol); and child abuse and neglect.
Costs
Two studies provided information on costs (Kratochwill 2009; Lord 2018). Kratochwill 2009 estimated that training FAST providers, implementing the intervention, and evaluating the impact of costs of USD 1200 per child (probably in 2002 or 2003 dollars). Lord 2018 estimated the cost of FAST to schools to be £133 per child (in 2018 pounds). These estimates are quite different from one another, but Lord 2018 may have benefited from economies of scale, and Kratochwill 2009 included evaluation costs in their estimate.
Discussion
Summary of main results
We identified 10 eligible randomised controlled trials (RCTs) examining the relative effects of assignment to Families and Schools Together (FAST) on child and parent outcomes. Nine of these studies (all except Knox 2011, which we discuss separately) contributed to at least one meta‐analysis. Of the primary outcomes, four studies assessed child school performance at long‐term follow‐up, but this analysis did not suggest that FAST might have an important impact. None of the studies assessed child adverse events, parent substance abuse, and parental stress. Of the secondary outcomes, only one (parent report of child externalising behaviour at long‐term follow‐up; Analysis 3.3) suggested that FAST might possibly have effects that are large enough to be meaningful, and had we been able to include the data from Knox 2011, which also measured this outcome, the effect size would likely have been smaller and the resulting confidence interval (CI) might not have suggested values that are possibly meaningful. Results for the outcomes of 'child internalising behaviour' and 'family relationships' suggest that FAST probably does not have an important impact on these outcomes. These conclusions are tempered by two considerations. Whilst both fixed‐effect and random‐effects meta‐analyses produced the same results in this review, these meta‐analyses were based on a small number of studies (two to five), and some of the underlying samples sizes are small. As a result, additional studies might change the point estimates. Whilst this would decrease uncertainty in fixed‐effect models, it might either reduce or increase uncertainty about the estimates from random‐effects models.
Overall completeness and applicability of evidence
All but one of the included studies was conducted in urban environments in the USA and focused on children aged 5 to 11 years who could be considered to be vaguely 'at risk' (most often due to living in poverty). Given the widespread adoption of FAST, which has been implemented in more than 20 countries, the available evidence is limited. We found no trials of Baby FAST or of the versions of FAST targeted at middle or high school level students.
The studies included in this review were relatively well reported. We were able to compute effect sizes for eligible outcomes for all but one study, and the studies generally provided detailed information about FAST as it was implemented and the families receiving it.
Most trials were not large, but three studies were. AIR 2018 implemented FAST in 30 schools in the USA, Lord 2018 implemented FAST in 60 schools in England, and López Turley 2017 implemented FAST in 26 schools in the USA. Overall, over 9000 students were included in at least one analysis in this review. Our conclusions are likely most applicable to low‐income children in the USA, and perhaps in the UK. This review might be less applicable to educational contexts that differ from these, and to minority groups not represented in the review.
Quality of the evidence
Using the GRADE approach, we rated the certainty of evidence as moderate for two outcomes, and as low for two outcomes. Reasons for these judgements are set out in the summary of findings Table for the main comparison. Many of the studies included in this review were at serious risk of bias. The most common problems were recruitment bias, attrition bias, and performance bias. We further downgraded two outcomes due to imprecision because the 95% CI included both potentially meaningful and beneficial, and potentially meaningful and harmful, effects of FAST.
Potential biases in the review process
We followed standard Cochrane procedures when developing the protocol for this review (Macdonald 2017), and, whenever possible, in conducting the review. This means that we employed state‐of‐the‐art literature search procedures in an effort to find all relevant studies examining the effectiveness of FAST.
We used multiple, trained review authors to identify potentially eligible studies and to extract descriptive information from study reports. Some details of this review were not anticipated by the protocol (see Differences between protocol and review), but we attempted to arrive at solutions without considering the analytical consequences of our choices. None of the review authors have any known conflicts of interest.
Agreements and disagreements with other studies or reviews
To our knowledge, this is the first systematic review of FAST. That said, the conclusions of our review are generally consistent with the themes that emerge from the individual studies. No studies included in this review were uniformly positive about the effects of FAST on child and parent outcomes. Instead, studies provided a mix of results, some of which were statistically significant or had CIs that contained values suggesting a potentially meaningful effect, but most of which were not statistically significant and did not have CIs suggesting a potentially meaningful effect.
Fast logic model. Copyright © 2016 Families and Schools Together, Inc.: reproduced with permission.
Study flow diagram for the literature search.
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Comparison 1 Child school performance, Outcome 1 Immediate post‐test.

Comparison 1 Child school performance, Outcome 2 Long‐term follow‐up.

Comparison 2 Child internalising behaviour, Outcome 1 Immediate post‐test, parent report.

Comparison 2 Child internalising behaviour, Outcome 2 Immediate post‐test, teacher report.

Comparison 2 Child internalising behaviour, Outcome 3 Long‐term follow‐up, parent report.

Comparison 2 Child internalising behaviour, Outcome 4 Long‐term follow‐up, teacher report.

Comparison 3 Child externalising behaviour, Outcome 1 Immediate post‐test, parent report.

Comparison 3 Child externalising behaviour, Outcome 2 Immediate post‐test, teacher report.

Comparison 3 Child externalising behaviour, Outcome 3 Long‐term follow‐up, parent report.

Comparison 3 Child externalising behaviour, Outcome 4 Long‐term follow‐up, teacher report.

Comparison 4 Child school attendance, Outcome 1 Short‐term follow‐up.

Comparison 4 Child school attendance, Outcome 2 Long‐term follow‐up.

Comparison 5 Parental engagement with education, Outcome 1 Immediate post‐test.

Comparison 5 Parental engagement with education, Outcome 2 Short‐term follow‐up.

Comparison 5 Parental engagement with education, Outcome 3 Long‐term follow‐up.

Comparison 6 Parental involvement in community‐based activities, Outcome 1 Long‐term follow‐up.

Comparison 7 Family relationships, Outcome 1 Immediate post‐test.

Comparison 7 Family relationships, Outcome 2 Short‐term follow‐up.

Comparison 7 Family relationships, Outcome 3 Long‐term follow up.
| Families and Schools Together (FAST) compared to no intervention (or care as usual) for children and their families | ||||||
| Patient or population: children and their families | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
| Risk with no intervention (or care as usual) | Risk with FAST | |||||
| Child school performance: long‐term follow up | ‐ | Mean score in the intervention group was0.02 standard deviations lower | ‐ | 6276 children (approximately) (4 RCTs) | ⊕⊕⊕⊝ | Positive effect sizes indicate improvement. Evidence suggests that FAST probably does not have an important positive effect on child school performance at long‐term follow‐up |
| Child adverse events ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Parental substance abuse ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Parental stress ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| Child internalising behaviours | ‐ | Mean score in the intervention group was 0.03 standard deviations lower (0.11 lower to 0.17 higher) | ‐ | 908 (approximately) (4 RCTs) | ⊕⊕⊝⊝ | Negative effect sizes indicate improvement. Evidence suggests that FAST probably does not result in an important reduction in child internalising behaviours |
| Child externalising behaviours | ‐ | Mean score in the intervention group was 0.19 standard deviations lower | ‐ | 754 (approximately) (4 RCTs) | ⊕⊕⊝⊝ | Negative effect sizes indicate improvement. FAST may result in a small and possibly important positive effect on parent reports of child externalising behaviour at follow‐up. However, teacher reports for this outcome suggest small and probably unimportant effect sizes, as did parent reports of child externalising behaviours immediately after completion of the intervention |
| Family relationships | ‐ | Mean score in the intervention group was 0.08 standard deviations higher | ‐ | 2569 (approximately) (4 RCTs) | ⊕⊕⊕⊝ | Positive effect sizes indicate improvement. FAST may result in a small and probably unimportant positive effect on parent reports of family relations |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; FAST: Families and Schools Together; RCT: randomised controlled trial. | ||||||
| GRADE Working Group grades of evidence. | ||||||
| aCertainty of evidence downgraded because two studies were at high risk for recruitment bias and two studies were at high risk for incomplete outcome data (attrition bias). | ||||||
| Random sequence generation |
|
|
| Allocation concealment |
|
|
| Blinding of participants and personnel |
|
|
| Blinding of outcome assessment |
|
|
| Incomplete outcome data |
|
|
| Selective outcome reporting |
|
|
| Issue | Method |
| Measures of treatment effect | Continuous data Where necessary, we will compute effect measures from P values, t statistics, analysis of variance (ANOVA) tables, or other statistics |
| Unit of analysis issues | Cluster‐randomised trials Where clustering has been appropriately accounted for within the analysis of the original study data, clustered data can be used in a meta‐analysis. However, a 'unit of analysis' error occurs when data from cluster‐randomised trials have been analysed as though the unit of allocation has been the individual rather than the cluster. In these circumstances, corrections are required to produce accurate effect size estimates (Section 16.3.4; Higgins 2011c). To calculate the design effect, we need a measure of the relative variation both within and between clusters. This is known as the intraclass correlation coefficient (ICC). Where the ICC from the original trial is not available, we will use external estimates from similar studies to calculate the design effect. If there are no reported estimates in the literature, we will perform a sensitivity analysis using low (0.01), medium (0.05), and high (0.10) values for ICC. However, as the design effect must be rounded up for entry into RevMan 5 (Review Manager 2014), this approach may be unsuitable for small studies, and we may need to employ an alternative approach that multiplies the standard errors (SEs) of the effect size by the square root of the design effect. In either case, where we include cluster‐randomised trials in the meta‐analysis, we will clearly identify them and will explain the method of calculating effect size estimates and their standard errors. In these circumstances, we will employ a sensitivity analysis to test the robustness of any conclusions deduced from these methods (see Sensitivity Analysis below) |
| Multiple treatment arms We do not anticipate finding studies with multiple treatment groups. However, should we identify such studies, we will first combine all eligible intervention arms and compare these with all control arms, making a single, pair‐wise comparison. If such a strategy seems likely to prevent the investigation of important sources of heterogeneity, we will keep intervention arms separate and will compare each with a common control group, dividing the sample size of the latter proportionately across each comparison, thereby preventing double counting of individuals (Section 16.5.5; Higgins 2011c) | |
| Dealing with missing data | Where we are certain that missing data are 'missing at random' and unlikely to be related to the characteristics of the participants or study design, we will analyse the available data while ignoring the missing data (Higgins 2011c). Conversely, where there is no reason to believe that data are missing at random ‐ that is, as a result of publication or selective reporting bias ‐ we will work with a statistician to select replacement values using imputed mean values or multiple imputation methods |
| Assessment of reporting biases | Where 10 or more studies provide data on a particular outcome, we will draw funnel plots (estimated differences in treatment effects against their standard error). Symmetrical funnel plots are associated with low levels of bias. Asymmetrical funnel plots may reflect publication bias, but they can also reflect real relationships between trial size and effect size, such as when larger trials have lower compliance, and compliance is positively related to effect size. If we have reason to think that this is happening, we will look for a possible explanation in clinical variation across studies To test directly for publication bias, we will conduct a sensitivity analysis (see Sensitivity Analysis below) to compare results from published data vs unpublished data and data from other sources |
| Data synthesis | In future updates of this review, should we encounter serious funnel plot asymmetry, we will assume that neither the fixed‐effect nor the random‐effects models are appropriate and will present the results of both. Where both indicate the presence or absence of an effect, we will assume that we can have some confidence in the results. Where they disagree, we will report this In future, if some included studies report an outcome using dichotomous outcome measures and others use continuous measures, we will convert results from the former, from an OR to an SMD, as long as there is reason to assume that the underlying continuous measure approximates a normal or logistical distribution. Where this is not the case, we will conduct separate analyses |
| Subgroup analysis and investigation of heterogeneity | As the overuse of subgroup analysis is problematic (Deeks 2011), we will use subgroup analyses only to determine a small number of effect modifiers We will conduct the following 4 subgroup analyses.
N.B. Since the protocol was published (Macdonald 2017), the various FAST programmes have been renamed as Baby FAST, Elementary Level, Middle School Level, and High School Level FAST.
As no family size effects are noted in Crozier 2010, McDonald 2009b, and McDonald 2010, despite reports of differing average family sizes, we will not include family size in the subgroup analysis. |
| Sensitivity analysis | We will use sensitivity analyses to explore the impact of studies at high risk of bias on the robustness of review results, restricting the analyses to (1) studies or outcomes with low risk of assessment bias, (2) studies with low risk of attrition bias, and (3) studies with low risk of reporting bias. In addition:
|
| FAST: Families and Schools Together. | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Immediate post‐test Show forest plot | 2 | Std. Mean Difference (Fixed, 95% CI) | ‐0.06 [‐0.34, 0.22] | |
| 2 Long‐term follow‐up Show forest plot | 4 | Std. Mean Difference (Fixed, 95% CI) | ‐0.02 [‐0.11, 0.08] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Immediate post‐test, parent report Show forest plot | 5 | Std. Mean Difference (Fixed, 95% CI) | ‐0.05 [‐0.21, 0.10] | |
| 2 Immediate post‐test, teacher report Show forest plot | 5 | Std. Mean Difference (Fixed, 95% CI) | ‐0.09 [‐0.18, 0.00] | |
| 3 Long‐term follow‐up, parent report Show forest plot | 4 | Std. Mean Difference (Fixed, 95% CI) | 0.03 [‐0.11, 0.17] | |
| 4 Long‐term follow‐up, teacher report Show forest plot | 4 | Std. Mean Difference (Fixed, 95% CI) | ‐0.06 [‐0.19, 0.07] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Immediate post‐test, parent report Show forest plot | 4 | Std. Mean Difference (Fixed, 95% CI) | ‐0.04 [‐0.20, 0.12] | |
| 2 Immediate post‐test, teacher report Show forest plot | 4 | Std. Mean Difference (Fixed, 95% CI) | ‐0.02 [‐0.11, 0.07] | |
| 3 Long‐term follow‐up, parent report Show forest plot | 4 | Std. Mean Difference (Fixed, 95% CI) | ‐0.19 [‐0.32, ‐0.05] | |
| 4 Long‐term follow‐up, teacher report Show forest plot | 4 | Std. Mean Difference (Fixed, 95% CI) | ‐0.10 [‐0.24, 0.04] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Short‐term follow‐up Show forest plot | 1 | Std. Mean Difference (Fixed, 95% CI) | 0.02 [‐0.11, 0.15] | |
| 2 Long‐term follow‐up Show forest plot | 2 | Std. Mean Difference (Fixed, 95% CI) | 0.03 [‐0.10, 0.16] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Immediate post‐test Show forest plot | 1 | Std. Mean Difference (Fixed, 95% CI) | 0.34 [0.15, 0.53] | |
| 2 Short‐term follow‐up Show forest plot | 1 | Std. Mean Difference (Fixed, 95% CI) | 0.20 [0.06, 0.33] | |
| 3 Long‐term follow‐up Show forest plot | 2 | Std. Mean Difference (Fixed, 95% CI) | 0.03 [‐0.07, 0.12] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Long‐term follow‐up Show forest plot | 1 | Std. Mean Difference (Fixed, 95% CI) | 0.11 [‐0.15, 0.38] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Immediate post‐test Show forest plot | 4 | Std. Mean Difference (Fixed, 95% CI) | 0.03 [‐0.27, 0.33] | |
| 2 Short‐term follow‐up Show forest plot | 1 | Std. Mean Difference (Fixed, 95% CI) | 0.00 [‐0.12, 0.13] | |
| 3 Long‐term follow up Show forest plot | 4 | Std. Mean Difference (Fixed, 95% CI) | 0.08 [‐0.03, 0.19] | |