Terapias biológicas anti‐factor de necrosis tumoral en el tratamiento del edema macular uveítico (EMU) para la uveítis no infecciosa
Resumen
Antecedentes
La uveítis no infecciosa describe a un grupo heterogéneo de trastornos oculares caracterizados por inflamación intraocular sin presencia de infección. La uveítis es una causa principal de pérdida de la visión, en su mayoría debido al edema macular uveítico (EMU). El tratamiento tiene como finalidad reducir la actividad de la enfermedad mediante la supresión de la respuesta inflamatoria intraocular. En el caso del edema macular, el objetivo es restaurar la arquitectura de la mácula lo más rápido posible, para prevenir el daño irreversible de los fotorreceptores en esta área. Las exacerbaciones agudas se tratan con frecuencia con corticosteroides, que pueden ser administrados de manera tópica, local o sistémica. Aunque estos suelen ser rápidamente efectivos para lograr el control de la enfermedad, el uso a largo plazo se asocia con efectos secundarios significativos, locales y sistémicos, y con frecuencia se usan fármacos ahorradores de corticosteroides para lograr un control prolongado en la enfermedad severa o recalcitrante. Los fármacos anti‐factor de necrosis tumoral (FNT) bloquean una citocina fundamental para el proceso de señalización inflamatoria y han devenido fármacos inmunorreguladores efectivos que ahorran corticosteroides en un grupo amplio de enfermedades no oculares. Existen datos mecanicistas que sugieren que pueden constituir un enfoque más orientado al control de la enfermedad en el EMU que otros fármacos, pero hasta la fecha, estos agentes se han usado predominantemente sin aprobación debido a que la mayoría no está autorizado para el uso ocular. Esta revisión tiene como objetivo resumir el informe de la bibliografía disponible sobre el uso del tratamiento anti‐FNT en el EMU, mediante el desarrollo de la base de la evidencia sobre la cual tomar decisiones de tratamiento en el futuro y la creación de guías clínicas en esta área.
Objetivos
Evaluar la eficacia del tratamiento anti‐FNT para el EMU.
Métodos de búsqueda
Se realizaron búsquedas en el Registro Cochrane Central de Ensayos Controlados (Cochrane Central Register of Controlled Trials) (CENTRAL; 2018, número 2) que contiene el registro de ensayos del Grupo Cochrane de Trastornos de los Ojos y la Visión [Cochrane Eyes and Vision Group]); Ovid MEDLINE; Ovid EMBASE; LILACS; Web of Science Conference Proceedings Citation Index‐ Science (CPCI‐S); System for Information on Grey Literature in Europe (Sistema para la información sobre literatura gris en Europa) (OpenGrey); el ISRCTN registry; ClinicalTrials.gov y el WHO ICTRP. La fecha de la búsqueda fue el 29 de marzo de 2018.
Criterios de selección
Se propuso incluir todos los ensayos controlados aleatorios relevantes que evalúen la administración de los fármacos anti‐FNT en el tratamiento del EMU. No se aplicaron límites a la edad, el género ni la etnia del participante. Las comparaciones primarias de esta revisión fueron: anti‐FNT versus ningún tratamiento o placebo; anti‐FNT versus otro agente farmacológico; comparación de diferentes fármacos anti‐FNT; comparación de diferentes dosis y vías de administración del mismo fármaco anti‐FNT. La medida de resultado primaria evaluada para esta revisión fue la agudeza visual mejor corregida (AVMC) en el ojo tratado. Las medidas de resultado secundarias fueron: el cambio macular anatómico, la estimación clínica de la neblina vítrea y la calidad de vida relacionada con la salud.
Obtención y análisis de los datos
Los autores de la revisión realizaron de forma independiente la selección de los títulos y resúmenes obtenidos con las búsquedas en bases de datos. Se recuperaron los informes de texto completo de los estudios categorizados como “no seguros” o “incluir” después que se examinaron los resúmenes. Dos autores de la revisión revisaron de forma independiente cada informe de texto completo para determinar su elegibilidad. Las discrepancias se resolvieron mediante discusión.
Resultados principales
No se identificó ningún ensayo completo o en curso que fuera elegible para esta revisión Cochrane.
Conclusiones de los autores
La revisión no identificó evidencia de los ensayos controlados aleatorios a favor o en contra de la función de los fármacos anti‐FNT en el tratamiento de EMU. Aunque hay varios ensayos controlados aleatorios de calidad alta que demuestran la eficacia de los agentes anti‐FNT en la prevención de la recurrencia de la inflamación en la uveítis, los resultados informados del estudio no incluyen cambios en el EMU. Como resultado, no hubo datos suficientes como para concluir si hubo un efecto del tratamiento significativo y específico para el EMU. Los ensayos futuros deben estar diseñados para incluir medidas cuantitativas de EMU como resultados primarios de estudio, por ejemplo, mediante el informe sobre la presencia o ausencia de EMU o la medición del espesor macular central para los participantes incluidos en el estudio. Además, aunque el EMU es una complicación importante de la uveítis, se sabe que la uveítis se asocia con muchas complicaciones estructurales y funcionales significativas. No es posible determinar la eficacia terapéutica sobre la base de una única medida de resultado. Se recomienda que las revisiones futuras de las intervenciones terapéuticas en la uveítis usen medidas de respuesta al tratamiento compuestas que incluyan una amplia variedad de complicaciones potenciales de la enfermedad.
PICO
Resumen en términos sencillos
Medicación anti‐factor de necrosis tumoral para el tratamiento del edema de la parte posterior del ojo (edema macular) debido a enfermedad ocular inflamatoria (uveítis)
¿Cuál es el objetivo de esta revisión?
El objetivo de esta revisión Cochrane fue determinar si una clase nueva de fármacos (anti‐factor de necrosis tumoral) es efectiva para el tratamiento del edema en la parte posterior del ojo (edema macular) causado por inflamación (uveítis). Los autores de la revisión Cochrane buscaron todos los estudios relevantes para abordar esta pregunta, pero no encontraron estudios adecuados para su inclusión.
Mensajes clave
En la actualidad, no hay evidencia a favor o en contra de la administración de los fármacos anti‐factor de necrosis tumoral en el tratamiento del edema macular en la uveítis.
¿Qué se estudió en esta revisión?
La uveítis es un grupo de afecciones del ojo en que existe inflamación en el interior del ojo. Si hay inflamación en la parte posterior del ojo (mácula) puede causar edema (edema macular). El edema de la mácula puede provocar la pérdida de la visión,
La uveítis se trata con frecuencia con corticosteroides para controlar la inflamación y evitar el daño al ojo. Sin embargo, los corticosteroides tienen efectos secundarios potencialmente graves y los médicos no recomiendan el uso a largo plazo. Los fármacos ahorradores de corticosteroides tienen efectos antiinflamatorios similares a los corticosteroides, pero con menos efectos secundarios. Se prefieren cuando los pacientes con uveítis necesitan tratamiento a largo plazo. Los fármacos anti‐factor de necrosis tumoral son un nuevo tipo de fármaco ahorrador de corticosteroides y se han usado para otras afecciones. Los investigadores Cochrane buscaron determinar si estos fármacos son útiles en el tratamiento del edema macular en la uveítis.
¿Cuáles son los principales resultados de la revisión?
Los autores de la revisión Cochrane realizaron búsquedas de estudios sobre la administración de fármacos anti‐factor de necrosis tumoral en el edema macular por uveítis en múltiples bases de datos electrónicas. No encontraron estudios relevantes. Algunos estudios indican que estos fármacos son efectivos para controlar la inflamación en el ojo, pero ninguno investigó de manera específica el edema macular. Se necesita de investigación adicional para ayudar con la toma de decisiones informada en esta área.
¿Cuál es el grado de actualización de esta revisión?
Los autores de la revisión Cochrane buscaron estudios que se habían publicado hasta el 29 de marzo 2018.
Authors' conclusions
Background
Description of the condition
Uveitis describes a group of disorders characterised by intraocular inflammation. Uveitis is the fifth most common cause of visual loss in high‐income countries, accounting for approximately 10% to 15% of total blindness (Durrani 2004; William 2007). This figure rises to 25% in low‐ and middle‐income countries (Abdulaal 2015; Rao 2013). Although uveitis may affect any age group, it peaks in the working‐age population, with no significant difference between sexes (Acharya 2013). The annual incidence of uveitis is estimated at 17.4 to 52.4 per 100,000 people with a prevalence of around 38 to 114.5 per 100,000 general population (Durrani 2004; Gritz 2004; Suhler 2008; William 2007).
Uveitis often occurs in younger people in the working population compared to other eye diseases such as cataracts and age‐related macular degeneration, so the condition has a huge impact in terms of years of potential blindness and economic cost (Durrani 2004).
Uveitis may be classified anatomically as anterior uveitis, intermediate uveitis, posterior uveitis or pan‐uveitis (Bloch‐Michel 1987; Deschenes 2008). It may arise from a range of different infectious and non‐infectious aetiological sources. The focus of this review is non‐infectious uveitis, most of which is thought to be auto‐immune (or at least auto‐inflammatory) and usually requires immunosuppressive treatment (Barry 2014; Van Gelder 1999). Non‐infectious uveitis may be associated with a range of inflammatory syndromes, including ankylosing spondylitis, Behcet's disease, sarcoidosis and multiple sclerosis (Lee 2014a; Lee 2014b; Takeuchi 2013).
The leading cause of sight loss in people with uveitis is macular oedema, known in this context as uveitic macular oedema (UMO) (Durrani 2004; Lardenoye 2006). Macular oedema describes the accumulation of fluid in the retina (the light‐sensitive inner lining of the eye) in the area that provides central vision known as the 'macula' (Davis 2010; De Smet 2010). Macula oedema is more common in forms of uveitis affecting the more posterior structures in the eye, namely intermediate and posterior uveitis and pan‐uveitis; collectively these are sometimes referred to as posterior segment‐involving uveitis. Macular oedema can also occur in association with anterior uveitis (Kaiser 2009).
Macular oedema accounts for 41% of visual impairment and 29% of blindness in uveitis (Levin 2014; Rothova 1996). The impact of UMO on visual acuity is usually assessed using standard distance visual acuity charts, either a Snellen chart or an Early Treatment Diabetic Retinopathy Study (ETDRS) chart. Acuities from Snellen charts are usually reported in metres in the UK and feet in the USA. Acuities from ETDRS charts are usually reported either as 'number of letters read' or converted into a LogMAR fraction. Although certain visual acuities are considered to be equivalent (e.g. 0.0 LogMAR = 6/6 UK Snellen = 20/20 US Snellen), these equivalences are approximate due to intrinsic differences between the charts (Kaiser 2009). Although the Snellen chart is still widely used in clinical practice, most trials use ETDRS charts due to various methodological advantages. Traditionally, macular oedema has been assessed clinically using stereoscopic slit‐lamp fundus bio‐microscopy and fluorescein angiography, an invasive procedure requiring intravenous dye and stereo photography imaging testing (Brown 2004). More recently a non‐invasive imaging technique, optical coherence tomography (OCT), has become a standard clinical practice in monitoring treatment response and follow‐up of UMO (Karim 2013; Reinthal 2004). OCT may be more sensitive than clinical measures in detecting the presence of UMO and provides accurate measures of the structural changes in term of macular thickness (Kempen 2013).
Description of the intervention
There are a wide range of pharmacological treatments for UMO. Corticosteroids are the mainstay of acute treatment (Davis 2010), with alternative routes of administration including: systemic (oral, intravenous and intramuscular); local, which includes periocular injection (sub‐Tenon and orbital floor injection); and intraocular (intravitreal injection or implant) (Kok 2005; Venkatesh 2008). For long‐term treatment it is important to reduce corticosteroid usage, leading to the use of 'second‐line' therapies, which are typically immunomodulatory and include T‐cell inhibitors (e.g. ciclosporin, and tacrolimus) and anti‐metabolites (e.g. azathioprine, methotrexate, mycophenolate mofetil). Alkylating agents (e.g. cyclophosphamide) have traditionally been used as a 'third line' for severe refractory disease (Barry 2014; Deuter 2009; Markomichelakis 2004; Neri 2008; Taylor 2009). Anti‐vascular endothelial growth factor (VEGF) agents and oral carbonic anhydrase inhibitor (acetazolamide) have also occasionally been used to treat UMO (Karim 2013). Anti‐tumour necrosis factor (anti‐TNF) drugs (the subject of this Cochrane Review) have recently been licensed for the treatment of uveitis (NICE 2017); adalimumab has been approved as an option for treating non‐infectious uveitis in the posterior segment of the eye in adults in cases of severe disease that demonstrates an inadequate response or tolerance to immunosuppressant therapy. Historically, anti‐TNF agents have commonly been used off‐licence, after the failure of one or more second‐line agents, but before the use of an alkylating agent (Sharma 2009).
Anti‐TNF drugs are biological agents that selectively block the actions of TNF, a critical cell‐signalling molecule ('cytokine') in the inflammatory process (Deuter 2009; McCluskey 2000). Originally pioneered in the 1990s for use in rheumatoid arthritis (RA), anti‐TNF drugs are now central to the treatment of many inflammatory diseases including RA, juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis (AS), Crohn's disease (Sharma 2009), and Behcet's disease (Hatemi 2008). As noted earlier, most non‐infectious uveitis is immune mediated and is commonly associated with many of these same systemic diseases (Lee 2014a; Lee 2014b; Murphy 2004; Takeuchi 2013).
There are currently five anti‐TNF agents licensed for a range of non‐ocular inflammatory diseases; none are licensed for ocular inflammation (Scallon 1995; Scallon 2002). The first anti‐TNF agent to be developed for clinical use was infliximab, a chimeric IgG1 that binds to soluble and membrane TNF‐α, preventing TNF‐α from binding to its receptor in the cell (Wooley 1995). The main route of administration is intravenous (Markomichelakis 2004). The second anti‐TNF agent to reach clinical usage was etanercept. This is a soluble protein linked to the human Fc fragment of IgG1 that prevents TNF‐α and β from interacting with their receptor; its route of administration is subcutaneous (Jabs 2001). The third anti‐TNF drug is adalimumab, which is a humanised IgG monoclonal antibody that binds to human TNF‐α (Kaymakcalan 2009). Adalimumab is administered subcutaneously (Rudwaleit 2009). In addition to direct effects on the TNF‐pathways, downstream effects appear to include an increase of regulatory T cells and modulation of vascular endothelial growth factor (VEGF)‐mediated pathways (Erckens 2011).
Golimumab is a human monoclonal antibody to TNF‐α with the advantage of requiring only monthly subcutaneous injection (Cordero‐Coma 2015; Feaz 2014; Miserocchi 2014). Certolizumab consists only of the pegylated humanised Fab fragment of a monoclonal antibody directed against TNF‐α. It is administered subcutaneously once every two weeks (Sánchez‐Cano 2013; Tlucek 2012). Both agents have shown benefits for ocular inflammatory disease; however, existing data are limited to case reports and case series (Mesquida 2013).
Although people with uveitis have received treatment with other anti‐TNF drugs, the most commonly used anti‐TNF agents are the monoclonal antibodies infliximab and adalimumab; in addition to the standard systemic administration, some authors have reported intravitreal administration (Pascual‐Camps 2014; Schaap‐Fogler 2014). Some people with uveitis have also received other anti‐TNF drugs for uveitis.
How the intervention might work
The pathogenesis of the UMO is related to the underlying ocular inflammatory process (uveitis) causing release of inflammatory mediators including interleukin (IL)‐1, IL‐2, IL‐6, IL‐8, and TNF‐α, transforming growth factor (TGF)‐β and interferon (IFN)‐γ, many of which directly or indirectly contribute to disruption of the blood–retina barrier. As a result, protein and large molecules are trapped within the retina, causing fluid flow out of the vessels via the osmotic gradient (Curnow 2006; Van Kooij 2006).
TNF‐α, a key pro‐inflammatory cytokine in a range of inflammatory conditions, has proven pivotal in animal models of uveitis and is present in intraocular fluids in human uveitis (Foxman 2002; Murphy 2004). It is a pleiotropic cytokine produced by a number of cells and has an important role in a range of leukocyte functions (Feldmann 2005; Sfikakis 2004). Specific roles include: increasing leukocyte recruitment to the eye via induction of chemokines and increased leukocyte adhesion to vascular endothelium; dendritic cell maturation to increase the effectiveness of their antigen presentation and cytokine production; macrophage activation and enhancing T‐cell activation. TNF‐α may also be pro‐apoptotic for both infiltrating and resident cells (Cordero‐Coma 2015). The exact cascade of inflammatory mediators that leads to UMO is not well understood (Curnow 2006; Schaap‐Fogler 2014); however, there is agreement that TNF‐α upregulates VEGF production in choroidal endothelial cells, and TNF‐α blockade is associated with a reduction in serum VEGF levels (Calleja 2012; Giraudo 1998; Hangai 2006).
Why it is important to do this review
UMO is the leading cause of sight loss in uveitis and a major cause of blindness in the working‐age population. There is mechanistic data to support the proposal that anti‐TNF drugs may provide more targeted disease control of uveitis than provided by current non‐biological therapies, and there is evidence demonstrating significant benefit of anti‐TNF drugs in related systemic inflammatory conditions. Off‐licence use of anti‐TNF agents for uveitis has become common in some centres, but there is a lack of national guidelines or consensus statements and considerable variation in practice (Davis 2010; Karim 2013; Sreekantam 2011). This review will assess the effects of the anti‐TNF therapy in the management of UMO. It is timely to review the literature in order to evaluate and summarise the available evidence for anti‐TNF therapy used for the treatment of UMO, which may form the basis of evidence‐based clinical recommendations.
Objectives
To assess the effects of anti‐TNF therapy for UMO.
Methods
Criteria for considering studies for this review
Types of studies
We planned to include all relevant randomised controlled trials (RCTs) assessing anti‐TNF therapy for treating UMO.
Types of participants
We planned to include trials with participants of any age, sex or ethnicity with a diagnosis of UMO.
Types of interventions
The primary comparisons of this review were:
-
anti‐TNF versus no treatment or placebo;
-
anti‐TNF versus another pharmacological agent;
-
comparison of different anti‐TNF drugs;
-
comparison of different doses and routes of administration of the same anti‐TNF drug.
Types of outcome measures
We planned not to select studies based on outcomes. However, we planned to consider clinical and patient‐reported outcomes to be important for the aims of the review. We planned to classify outcomes as primary and secondary as follows.
Primary outcomes
The primary outcome measure for this review was best corrected visual acuity (BCVA) in the treated eye. This was measured in the following ways.
-
Mean change in LogMAR BCVA between baseline (before treatment) and at the pre‐specified time points.
-
The proportion of participants gaining 5 or more ETDRS letters (equivalent to 1 ETDRS line or 0.1 LogMAR improvement) at the follow‐up visit in the treated eye at the pre‐specified time point.
-
The proportion of participants losing 5 or more ETDRS letters (equivalent to 1 ETDRS line or 0.1 LogMAR worsening) recorded at the follow‐up visit in the treated eye at the pre‐specified time point.
Secondary outcomes
Anatomical macular change
We planned to record anatomical changes in macular structure as studies measured them.
-
Mean change in central macular thickness (CMT) in microns, as assessed by OCT at pre‐specified time points.
-
Proportion with clinical resolution of UMO, as assessed by stereoscopic slit‐lamp fundus biomicroscopy (clinical) at pre‐specified time points.
-
Proportion with angiographic resolution of UMO, as assessed by fundus fluorescein angiography at pre‐specified time points.
Clinical estimation of vitreous haze
-
Changes in vitreous haze, as assessed by stereoscopic fundus indirect biomicroscopy examination at pre‐specified time points.
Health‐related quality of life
-
Mean change in quality‐of‐life score (both vision‐related and non‐vision‐related), as measured by any validated quality‐of‐life questionnaire at the pre‐specified time points
Adverse events
-
We planned to record all adverse events reported in the included studies at the pre‐specified time points.
We expected data to be available at multiple time points within and between studies. We planned to categorise nominal data from each analysis into three groups. We planned to group the postintervention time points for assessment of outcomes into three different time ranges: 3 months or less; more than 3 months and up to 6 months; and more than 6 months.
Search methods for identification of studies
Electronic searches
The Cochrane Eyes and Vision Information Specialist searched the following electronic databases for randomised controlled trials and controlled clinical trials. There were no language or publication year restrictions. The date of the search was 29 March 2018.
-
Cochrane Central Register of Controlled Trials (CENTRAL; 2018, Issue 3), which contains the Cochrane Eyes and Vision Trials Register, in the Cochrane Library (latest issue) (Appendix 1)
-
MEDLINE Ovid (1946 to 29 March 2018) (Appendix 2)
-
Embase Ovid (1947 to 29 March 2018) (Appendix 3)
-
Web of Science Conference Proceedings Citation Index‐ Science (CPCI‐S) (1970 to 29 March 2018) (Appendix 4)
-
System for Information on Grey Literature in Europe (OpenGrey) (www.opengrey.eu/ to 29 March 2018) (Appendix 5)
-
ISRCTN registry (www.isrctn.com/editAdvancedSearch; searched 29 March 2018) 29 March 2018 (Appendix 6).
-
US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.clinicaltrials.gov; searched 29 March 2018) (Appendix 7).
-
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp; searched 29 March 2018) (Appendix 8).
Searching other resources
We planned to search the reference lists of potentially relevant studies to identify any additional trials. We did not handsearch conference proceedings or journals for this review.
Data collection and analysis
Selection of studies
We carried out the study selection process in two stages.
-
First, we screened the title and the abstract of identified articles in order to remove irrelevant records, excluding articles that obviously did not meet the selection criteria.
-
Secondly, we planned to retrieve the full‐text of any potentially relevant articles and assess them against the selection criteria.
At both stages, two review authors (MT and RB) independently assessed articles, resolving any disagreements by discussion and if required by referral to a third review author (DM). Two review authors independently screened the titles and abstracts resulting from the searches using web‐based software Covidence (Covidence). We have illustrated the study selection processes using a PRISMA flow diagram (Moher 2010).
We planned to have non‐English language articles translated in part or in full to aid study selection and analysis.
As we did not identify any published RCTs for inclusion in our review, we were not able to complete the steps for data extraction or analysis. In future updates, if we find any RCTs that meet our inclusion, we will follow the process outlined below.
Data extraction and management
See: Appendix 9
Two review authors (MT and RB) will extract data independently using an online data extraction form in Covidence (Covidence). We will resolve any discrepancies through discussion and referral to a third review author (DM) if needed. We will use a standardised piloted data extraction form. We may contact study authors for further information. We will enter all data into Review Manager 5 (RevMan 5) software (Review Manager 2014). For each study, we will extract at least the following information.
-
Study characteristics
-
Authors, publication year, title and journal
-
Study design
-
Setting
-
Sample size
-
Length of follow‐up
-
Analysis
-
-
Participant characteristics
-
Selection/recruitment criteria
-
Demographic data; number, age, sex, socioeconomic status and ethnicity
-
Type of uveitis (anatomical categorisation, syndrome/aetiological classification)
-
Comorbidity
-
Co‐medication
-
-
Intervention and comparator
-
Pharmacological agents
-
Regimen (dose, frequency of administration, route of administration)
-
Comparator details
-
Any difference in underlying care between treatment groups
-
-
Outcomes and findings
-
Outcomes measured and results for each outcome including precision and statistical test results
-
Completeness of follow‐up for each outcome
-
Assessment of risk of bias in included studies
Two review authors will independently assess the quality of included studies, resolving disagreements through discussion and referral to a third review author (DM) if required. We will employ the methods set out in Chapter 8 of the Cochrane Handbook for Systematic Reviews of Intervention (Higgins 2017).
We will consider the following domains.
-
Selection bias: allocation concealment bias, randomisation sequence generation bias
-
Performance bias: masking (or blinding) of study participants and the researcher
-
Detection bias: masking (or blinding) of outcome assessors
-
Attrition bias: loss to follow‐up and rate of compliance in both groups (withdrawals from the study lead to incomplete outcome data)
-
Reporting bias: selective outcome reporting
We will report the 'Risk of bias' domains as being at low risk, high risk or unclear risk (lack of information or uncertainty of potential bias) (Higgins 2017). We will add data from the included studies on risk of bias into Review Manager 2014.
Measures of treatment effect
Continuous data
We will report continuous variables as mean differences with their corresponding 95% confidence intervals.
Dichotomous data
We will report dichotomous variables as risk ratios (RRs) with their corresponding 95% confidence intervals.
We are likely to present results for some outcomes using a number of different measures/statistics measured within and between studies. For example, studies might report visual acuity in metres or feet (from Snellen charts), a LogMAR score, or number of letters or lines read (from ETDRS charts). Investigators may report the change in acuity as a change in any one of these indices or categorised against a threshold, for example, proportion of participants with change greater than or equal to a specific number of lines/letters read (Kaiser 2009). Thus, different studies may consider visual acuity to be continuous data (e.g. group mean LogMAR score), discrete data (e.g. number of lines read) or dichotomous data (e.g. proportion of participants reading x lines, or proportion with a LogMAR score greater than y). it is likely that continuous and dichotomous data will be most common. We will consider converting data between formats to maximise the data available for each analysis (for example, if authors state the type of chart, we might convert letters into lines; interchange LogMAR score and letters; and approximate Snellen UK, US and ETDRS data). We will undertake any conversion of data with due caution, taking into account known issues (Kaiser 2009). We will explicitly acknowledge the impact of any converted data on findings and explore this aspect through sensitivity analysis.
We will also analyse secondary outcome measures, presenting CMT as mean difference with 95% confidence intervals. We will pool health‐related quality of life from the same scales using mean difference, and when studies use different scales to assess the same underlying concepts/domains, we will use standardised mean difference.
For adverse events reported in the included studies, we will record counts and rates. We may consider these data as continuous if the adverse events are common and occur often (presented as mean difference) or dichotomous data if the adverse events occur rarely (presented as rate ratio).
Unit of analysis issues
Clinical trials in ophthalmology may randomise one or both eyes of participants to the intervention. The unit of randomisation may depend on the intervention.
-
If the intervention is systemic (IV or SC) then the unit of randomisation in the studies will be the participant.
-
If the intervention is intraocular – then the unit of randomisation could be the participant or the eye.
The unit of analysis might also depend on the outcome.
-
For most outcomes related to vision, our primary unit of analysis will be the eye.
-
For outcomes related to things like quality of life, the unit of analysis will be the participant.
-
For adverse events, the unit of analysis will be the participant (and/or the eye in case of intraocular administration).
If studies include only one eye from each participant, the unit of analysis can either be the eye or the person. If two eyes from each participant receive the same intervention, and study authors report them as a single unit (either through only one eye used in analysis, or as the average outcome for the two eyes), then the unit of analysis will be the participant.
If studies include two eyes per participant, with no differences in treatment between eyes, and they analyse them as two eyes, the outcome in each eye is likely to be more similar to the outcome in the companion eye than the eye of a different participant; therefore the study design could/should be considered as comparable to a cluster‐randomised study.
If the intervention is intraocular administration, and participants receive different treatments in each eye (e.g. paired‐eye/within‐person design), we can compare outcomes between the two eyes and assess within‐person differences if data are available. However, if the study includes more than one eye from some participants but not all participants, and the unit of analysis is the eye, then we should record this, as there are issues with unit of analysis that may not be resolvable. There are inadequate data available to know whether the intravitreal injection of anti‐TNF agents may result in therapeutically significant systemic levels. On this basis, we will include any within‐person (paired‐eye) studies for intravitreal anti‐TNF but report them separately.
Dealing with missing data
We will assess all the included studies for number of participants excluded or lost to follow‐up. For unclear or missing required information in study reports (e.g. on features such as study methods, outcome data, and measures of data variation), we will contact study authors. However, if the study authors do not respond within four weeks or are not able to provide the additional data, we will conduct analyses based on the best available information. We will identify the distribution of missing data between the two arms and discuss the potential impact of missing data on the findings of the review.
Assessment of heterogeneity
We will assess clinical and methodological heterogeneity to determine whether studies are sufficiently similar for each comparison/outcome to ensure that data pooling by meta‐analysis is appropriate (Higgins 2002; Huedo‐Medina 2006). If we combine studies in a meta‐analysis, where appropriate we will report the I2 statistic (Higgins 2003), which gives the percentage of the total variability in the data due to between‐study heterogeneity, and the Tau2 statistic, which gives an estimate of the between‐study variance (Higgins 2017).
Assessment of reporting biases
We will examine selective outcome reporting by comparing outcomes reported in included studies and the outcomes recorded in study protocols. If the protocols are not publicly available, we will contact study authors to supply them. For each meta‐analysis containing 10 or more studies, we will construct a funnel plot and assess asymmetry in the plotted data (Peters 2008). Any asymmetry may imply possible publication bias, poor reporting of small studies, true heterogeneity or chance.
Data synthesis
We will assess the consistency of clinical and methodological study characteristics, and if there is no substantial heterogeneity between the trials, we will combine results in a meta‐analysis using a random‐effects model. If there is substantial clinical or statistical heterogeneity, we will not combine study results in meta‐analysis but will present data in a narrative summary.
Subgroup analysis and investigation of heterogeneity
We will consider subgroup analysis for clinical and anatomical classification of uveitis (anterior, intermediate, posterior and pan‐uveitis) where deemed appropriate.
Sensitivity analysis
We will perform sensitivity analysis to assess the robustness of the results and the effect of excluding trials judged to have a high risk of bias in one or more domains.
'Summary of findings' table and GRADE
If sufficient data are available, we will produce a 'Summary of findings' table for outcomes at six months' follow‐up to provide key information concerning the quality of evidence, the magnitude of effect of the interventions examined, and the sum of available data on all of the primary and secondary outcomes for a given comparison. Two review authors will independently use the GRADE tool to assess the certainty of the evidence in the included studies (GRADEpro GDT). The GRADE system entails an assessment of the quality of a body of evidence for each individual outcome. We will resolve any discrepancies by discussion and refer to a third review author if needed. The table of results will include the primary outcome for the review, which will be the BCVA, using either the mean change in LogMAR BCVA from baseline at the pre‐specified time point or the proportion of participants gaining 5 or more ETDRS letters from baseline BCVA. In addition, the tables will include results for the following outcomes.
-
Mean change in CMT from the baseline at the pre‐specified time point
-
Proportion of eyes with absence of dye leakage on fluorescein angiography
-
Mean change in vitreous haze from the baseline
-
Mean change in quality‐of‐life score
-
Proportion of participants with adverse events
Results
Description of studies
Results of the search
The electronic searches yielded 423 records (Figure 1). The Cochrane Information Specialist removed 81 duplicate records and we screened the remaining 342 reports for potential inclusion in the review. We obtained two full‐text reports for further assessment, however these did not meet the inclusion criteria, see Characteristics of excluded studies for details. We did not identify any ongoing studies from searches of the trials registers.

Study flow diagram
Included studies
We found no studies that met the inclusion criteria for this review.
Excluded studies
We excluded two studies on patients with uveitis because they did not report relevant outcomes separately for any participants with UMO (Jaffe 2016; Nguyen 2016).
Risk of bias in included studies
We found no studies that met the inclusion criteria for this review.
Effects of interventions
We found no studies that met the inclusion criteria for this review.
Discussion
Summary of main results
We conducted a search of several electronic literature databases to identify randomised or quasi‐randomised trials that evaluated the role of anti‐TNF therapy in the management of UMO. Despite using a sensitive search strategy, we did not identify any such trials. Our search highlighted the lack of rigorous evidence to guide the use of anti‐TNF therapy in the management of UMO, and identifies a need for further work in this area.
Overall completeness and applicability of evidence
Treatment of non‐infectious uveitis necessitates titration of anti‐inflammatory agents in order to achieve suppression of the intra‐ocular inflammatory response. There are no universally accepted guidelines for disease management, and a wide range of immunomodulatory agents have been suggested as having beneficial effects in controlling disease (Barry 2014). Anti‐TNF agents have emerged as a promising treatment modality, with mechanistic data to suggest that they may offer more targeted treatment of intraocular inflammation than existing non‐biologic, steroid‐sparing agents. Off‐licence use of anti‐TNF agents for uveitis has previously been widely reported (Davis 2010; Karim 2013; Sreekantam 2011), and following the recent publication of the National Institute for Health and Care Excellence (NICE) guidelines, the use of adalimumab in resistant disease is now standard practice throughout the UK (NICE 2017).
To date, there have been two large‐scale, placebo‐controlled, randomised controlled trials investigating the effect of adalimumab in non‐infectious intermediate, posterior or pan‐uveitis (Jaffe 2016; Nguyen 2016). In both studies, control of inflammation was first achieved with systemic corticosteroid treatment, before participants were randomised to receive either adalimumab by subcutaneous injection or placebo. The primary outcome was time to treatment failure, defined by a multicomponent endpoint including the occurrence of new inflammatory lesions in the retina, BCVA, anterior chamber cell grade, and vitreous haze grade. Both studies concluded that adalimumab significantly lowered the risk of uveitic flare or loss of visual acuity upon corticosteroid withdrawal in people with inactive, non‐infectious intermediate, posterior, or pan‐uveitic uveitis controlled by systemic corticosteroids.
Since both studies reported time to treatment failure as the primary outcome, neither were suitable for inclusion in this review. Furthermore, neither study reported subgroup analysis of resolution or development of UMO, and we are therefore unable to comment whether adalimumab provides specific treatment benefit in this area.
Quality of the evidence
We did not identify any trials for inclusion in this review.
Potential biases in the review process
We aimed to minimise potential biases in the review process by conducting a highly sensitive search for trials, and following rigorous methods as recommended by Cochrane (Lefebvre 2011).
Agreements and disagreements with other studies or reviews
A few non‐randomised studies supported the use of anti‐TNF agents in the treatment of UMO. However, we did not include such studies in this review, and have not conducted a comprehensive search and critical appraisal of evidence from non‐randomised studies.
In a retrospective review of patients with macular oedema secondary to birdshot chorioretinopathy, Steeples 2017 demonstrated adalimumab to be effective in reducing CMT over a 12‐month period. Calvo‐Rio 2014 demonstrated a similar beneficial effect of adalimumab in a cohort of patients with refractory macular oedema secondary to Behcet's Disease. Schaap‐Fogler 2014 reported outcomes of adalimumab in adults with macular oedema due to non‐infectious uveitis of varying aetiologies, suggesting that maximum improvement in CMT was observed at six months, however the treatment effect had lessened by 12 months' follow‐up, whilst Markomichelakis 2004 demonstrated an improvement in CMT with infliximab therapy, which was maintained to six months' follow‐up.
In summary, whilst these non‐randomised reviews suggest that anti‐TNF therapy is indeed effective in the treatment of UMO, they do not provide definitive evidence of treatment benefit.
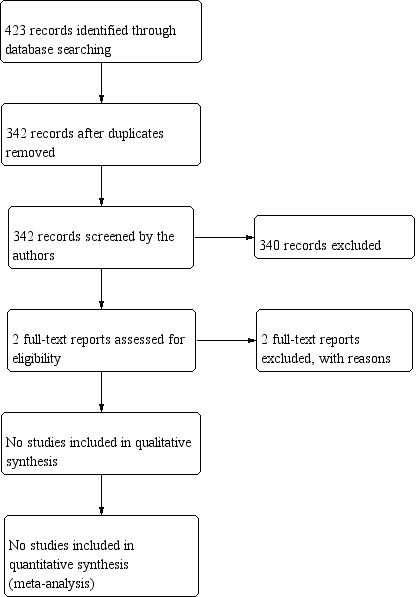
Study flow diagram