Ubat antiepileptik untuk sakit kronik bukan kanser dalam kanak‐kanak dan remaja
Appendices
Appendix 1. Meeting for NIHR Programme Grant agenda on pain in children
Date
Monday 1st June 2015
Location
International Association of the Study of Pain (IASP) Conference, Seattle, USA
Delegates
Allen Finlay, Anna Erskine, Boris Zernikow, Chantal Wood, Christopher Eccleston, Elliot Krane, George Chalkaiadis, Gustaf Ljungman, Jacqui Clinch, Jeffrey Gold, Julia Wager, Marie‐Claude Gregoire, Miranda van Tilburg, Navil Sethna, Neil Schechter, Phil Wiffen, Richard Howard, Susie Lord.
Purpose
National Institute for Health Research (NIHR) (UK) Programme Grant ‐ Addressing the unmet need of chronic pain: providing the evidence for treatments of pain.
Proposal
Nine reviews in pharmacological interventions for chronic pain in children and adolescents: Children (5 new, 1 update, 1 overview, and 2 rapid) self‐management of chronic pain is prioritised by the planned NICE guideline. Pain management (young people and adults) with a focus on initial assessment and management of persistent pain in young people and adults.
We propose titles in paracetamol, ibuprofen, diclofenac, other NSAIDs, and codeine, an overview review on pain in the community, 2 rapid reviews on the pharmacotherapy of chronic pain, and cancer pain, and an update of psychological treatments for chronic pain.
Key outcomes
The final titles: (1) opioids for cancer‐related pain (Wiffen 2017), (2) opioids for chronic non‐cancer pain (Cooper 2017a), (3) antiepileptic drugs for chronic non‐cancer pain (Wiffen 2017b ‐ this review), (4) antidepressants for chronic non‐cancer pain (Cooper 2017b), (5) non‐steroidal anti‐inflammatory drugs (NSAIDs) for chronic non‐cancer pain (Eccleston 2017), (6) non‐steroidal anti‐inflammatory drugs (NSAIDs) for cancer‐related pain (Cooper 2017c), (7) paracetamol for chronic non‐cancer pain (Cooper 2017d).
PICO
Patients : children, aged 3 to 12, chronic pain defined as pain persisting for 3 months (NB: now changed to: birth to 17 years to include infants, children and adolescents)
Interventions : by drug class including antiepileptic drugs, antidepressants, opioids, NSAIDs, paracetamol
Comparisons : maintain a separation of cancer and non‐cancer, exclude headache, in comparison with placebo and or active control
Outcomes : we will adopt the IMMPACT criteria
Appendix 2. Methodological considerations for chronic pain
There have been several recent changes in how the efficacy of conventional and unconventional treatments is assessed in chronic painful conditions. The outcomes are now better defined, particularly with new criteria for what constitutes moderate or substantial benefit (Dworkin 2008); older trials may only report participants with 'any improvement'. Newer trials tend to be larger, avoiding problems from the random play of chance. Newer trials also tend to be of longer duration, up to 12 weeks, and longer trials provide a more rigorous and valid assessment of efficacy in chronic conditions. New standards have evolved for assessing efficacy in neuropathic pain, and we are now applying stricter criteria for the inclusion of trials and assessment of outcomes, and are more aware of problems that may affect our overall assessment. We summarise some of the recent insights that must be considered in this new review.
-
Pain results tend to have a U‐shaped distribution rather than a bell‐shaped distribution. This is true in acute pain (Moore 2011a; Moore 2011b), back pain (Moore 2010d), and arthritis (Moore 2010c), as well as in fibromyalgia (Straube 2010); in all cases average results usually describe the experience of almost no one in the trial. Data expressed as averages are potentially misleading, unless they can be proven to be suitable.
-
As a consequence, we have to depend on dichotomous results (the individual either has or does not have the outcome) usually from pain changes or patient global assessments. The Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) group has helped with their definitions of minimal, moderate, and substantial improvement (Dworkin 2008). In arthritis, trials of less than 12 weeks' duration, and especially those shorter than eight weeks, overestimate the effect of treatment (Moore 2010c); the effect is particularly strong for less effective analgesics, and this may also be relevant in neuropathic‐type pain.
-
The proportion of patients with at least moderate benefit can be small, even with an effective medicine, falling from 60% with an effective medicine in arthritis to 30% in fibromyalgia (Moore 2009; Moore 2010c; Moore 2013b; Moore 2014b; Straube 2008; Sultan 2008). A Cochrane review of pregabalin in neuropathic pain and fibromyalgia demonstrated different response rates for different types of chronic pain (higher in diabetic neuropathy and postherpetic neuralgia and lower in central pain and fibromyalgia) (Moore 2009). This indicates that different neuropathic pain conditions should be treated separately from one another, and that pooling should not be done unless there are good grounds for doing so.
-
Individual patient analyses indicate that patients who get good pain relief (moderate or better) have major benefits in many other outcomes, affecting quality of life in a significant way (Moore 2010b; Moore 2014a).
-
Imputation methods such as last observation carried forward (LOCF), used when participants withdraw from clinical trials, can overstate drug efficacy, especially when adverse event withdrawals with drug are greater than those with placebo (Moore 2012).
Appendix 3. MEDLINE search strategy (via Ovid)
-
exp Child/
-
exp Adolescent/
-
exp Infant/
-
(child* or boy* or girl* or adolescen* or teen* or toddler* or preschooler* or pre‐schooler* or baby or babies or infant*)..tw
-
1 or 2 or 3 or 4
-
exp Anticonvulsants/
-
(carbamazepine or clobazam or clonazepam or ethosuximide or gabapentin or lacosamide or lamotrigine or levetiracetam or oxcarbazepine or phenytoin or pregabalin or rufinamide or topiramate or valproate or vigabatrin or zonisamide).mp.
-
6 or 7
-
exp Pain/
-
pain*.tw
-
9 or 10
-
5 and 8 and 11
-
randomized controlled trial.pt.
-
controlled clinical trial.pt.
-
randomized.ab.
-
placebo.ab.
-
drug therapy.fs.
-
randomly.ab.
-
trial.ab.
-
groups.ab.
-
13 or 14 or 15 or 16 or 17 or 18 or 19 or 20
-
exp animals/ not humans.sh.
-
21 nor 22
-
12 and 23
Appendix 4. Embase search strategy (via Ovid)
-
exp Child/
-
exp Adolescent/
-
exp Infant/
-
(child* or boy* or girl* or adolescen* or teen* or toddler* or preschooler* or pre‐schooler* or baby or babies or infant*).tw.
-
1 or 2 or 3 or 4
-
exp anticonvulsive agent/
-
(carbamazepine or clobazam or clonazepam or ethosuximide or gabapentin or lacosamide or lamotrigine or levetiracetam or oxcarbazepine or phenytoin or pregabalin or rufinamide or topiramate or valproate or vigabatrin or zonisamide).mp.
-
6 or 7
-
exp Pain/
-
pain*.tw
-
5 and 8 and 10
-
random$.tw.
-
factorial$.tw.
-
crossover$.tw.
-
cross over$.tw.
-
cross‐over$.tw.
-
placebo$.tw.
-
(doubl$ adj blind$).tw.
-
(singl$ adj blind$).tw.
-
assign$.tw.
-
allocat$.tw.
-
volunteer$.tw.
-
Crossover Procedure/
-
double‐blind procedure.tw.
-
Randomized Controlled Trial/
-
Single Blind Procedure/
-
or/12‐26
-
(animal/ or nonhuman/) not human/
-
27 not 28
-
11 and 29
Appendix 5. CENTRAL search strategy (via Cochrane Register of Studies Online)
-
MESH DESCRIPTOR Child EXPLODE ALL TREES
-
MESH DESCRIPTOR Adolescent EXPLODE ALL TREES
-
MESH DESCRIPTOR Infant EXPLODE ALL TREES
-
(child* or boy* or girl* or adolescen* or teen* or toddler* or preschooler* or pre‐schooler* or baby or babies or infant*):TI,AB,KY
-
#1 OR #2 OR #3 or #4
-
MESH DESCRIPTOR Anticonvulsants EXPLODE ALL TREES
-
(carbamazepine or clobazam or clonazepam or ethosuximide or gabapentin or lacosamide or lamotrigine or levetiracetam or oxcarbazepine or phenytoin or pregabalin or rufinamide or topiramate or valproate or vigabatrin or zonisamide):TI,AB,KY
-
#6 OR #7
-
MESH DESCRIPTOR Pain EXPLODE ALL TREES
-
pain*:TI,AB,KY
-
#9 OR #10
-
#5 AND #8 AND #11
Appendix 6. Summary of efficacy in individual studies
| Study | Treatment | Pain outcome | Other efficacy outcome |
| Intervention group (N = 54): flexible‐dose pregabalin 75 to 450 mg/day Control group (N = 53): flexible‐dose placebo 75 to 450 mg/day Study duration: 15 weeks' duration involving 4 phases: doses were optimised over 3 weeks based on efficacy and tolerability to 75, 150, 300, 450 mg/day. Remaining at that dose for 12 weeks. | Participant‐reported pain relief of 30% or greater: Pregabalin: 18/54 (33.3%) Placebo: 16/51 (31.4%) P = 0.83 Participant‐reported pain relief of 50% or greater: Pregabalin: 9/54 (16.7%) Placebo: 4/51 (7.8%) P = 0.179 PGIC much or very much improved: Pregabalin: 53.1% Placebo: 29.5% | Carer Global Impression of Change: Pregabalin: 51.0% Placebo: 25.0% p = 0.011 Requirement for rescue analgesia: no data Sleep duration and sleep quality: 11‐point numerical rating scale BASELINE Pregabalin: 5.8 (1.6) m (SD). Placebo: 5.6 (2.5) m (SD). WEEK 8: treatment difference: ‐1.01 (95% CI ‐1.73 to ‐0.30); P = 0.006. WEEK 10: treatment difference: P = 0.037. WEEK 15: treatment difference ‐0.17 (95% CI ‐0.95 to 0.61). OVERALL: treatment difference: ‐0.48 (95% CI ‐1.02 to 0.06); P = 0.081. Acceptability of treatment: Pregabalin: no data Placebo: no data Physical functioning: Fibromyalgia Impact Questionnaire for children total score: least squares mean difference: ‐2.46 (95% CI ‐6.87 to 1.95); P = 0.270. Quality of life: Pregabalin: no data Placebo: no data | |
| Intervention group (N = 17): oral gabapentin 900 mg/day (300 x 3) Control group (N = 17): oral amitriptyline 10 mg/day Study duration: 6 weeks | Participant‐reported pain relief of 30% or greater: no data Participant‐reported pain relief of 50% or greater: no data PGIC much or very much improved: no data | Carer Global Impression of Change: no data Requirement for rescue analgesia: no data Sleep duration and sleep quality: Average decrease in sleep score on 5‐point Likert scale Completed participants m (SD) Gabapentin: 0.46 (1.60); n = 14 Amitriptyline: 1.25 (1.86); n = 12 All participants m (SD) Gabapentin: 0.38 (1.45); n = 17 Amitriptyline: 0.88 (1.69); n = 17 Acceptability of treatment: no data Physical functioning: no data Quality of life: no data | |
| CI: confidence interval; m: mean; N: number of participants; PGIC: Patient Global Impression of Change; SD: standard deviation | |||
Appendix 7. Summary of adverse events and withdrawals in individual studies
| Study | Treatment | Adverse events | Withdrawals |
| Intervention group (N = 54): flexible‐dose pregabalin 75 to 450 mg/day Control group (N = 53): flexible‐dose placebo 75 to 450 mg/day Study duration: 15 weeks' duration involving 4 phases: doses were optimised over 3 weeks based on efficacy and tolerability to 75, 150, 300, 450 mg/day. Remaining at that dose for 12 weeks. | Total adverse events: Pregabalin: 167 Placebo: 132 No. participants with any adverse event: Pregabalin: 38/54 Placebo: 34/53 No. participants with serious adverse events: Pregabalin: 1/54 Placebo: 0/53 | Total all‐cause withdrawals: Pregabalin: 10/54 Placebo: 17/53 Withdrawals due to adverse events: Pregabalin: 4/54 Placebo: 4/53 | |
| Intervention group (N = 17): oral gabapentin 900 mg/day (300 x 3) Control group (N = 17): oral amitriptyline 10 mg/day Study duration: 6 weeks | Total adverse events: Gabapentin: 2/17 Amitriptyline: 1/17 No. participants with any adverse event: Gabapentin: 2/17 Amitriptyline: 1/17 No. participants with serious adverse events: Gabapentin: 0/17 Amitriptyline: 0/17 | Total all‐cause withdrawals: Gabapentin: 2/17 Amitriptyline: 3/17 Withdrawals due to adverse events: Gabapentin: 2/17 Amitriptyline: 1/17 | |
| CI: confidence interval; m: mean; N: number of participants; SD: standard deviation | |||
Appendix 8. GRADE guidelines
Some advantages of utilising the GRADE process are (Guyatt 2008):
-
transparent process of moving from evidence to recommendations;
-
clear separation between quality of evidence and strength of recommendations;
-
explicit, comprehensive criteria for downgrading and upgrading quality of evidence ratings; and
-
clear, pragmatic interpretation of strong versus weak recommendations for clinicians, patients, and policymakers.
The GRADE system uses the following criteria for assigning grades of evidence:
-
high: we are very confident that the true effect lies close to that of the estimate of the effect;
-
moderate: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of effect, but there is a possibility that it is substantially different;
-
low: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect; and
-
very low: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect.
We will decrease the grade if there is:
-
serious (‐1) or very serious (‐2) limitation to study quality;
-
important inconsistency (‐1);
-
some (‐1) or major (‐2) uncertainty about directness;
-
imprecise or sparse data (‐1); or
-
high probability of reporting bias (‐1).
We will increase the grade if there is:
-
strong evidence of association ‐ significant risk ratio of > 2 (< 0.5) based on consistent evidence from two or more observational studies, with no plausible confounders (+1);
-
very strong evidence of association ‐ significant risk ratio of > 5 (< 0.2) based on direct evidence with no major threats to validity (+2);
-
evidence of a dose response gradient (+1); or
-
all plausible confounders would have reduced the effect (+1).
"In addition, there may be circumstances where the overall rating for a particular outcome would need to be adjusted per GRADE guidelines (Guyatt 2013a). For example, if there were so few data that the results were highly susceptible to the random play of chance, or if studies used LOCF imputation in circumstances where there were substantial differences in adverse event withdrawals, one would have no confidence in the result, and would need to downgrade the quality of the evidence by three levels, to very low quality. In circumstances where no data were reported for an outcome, we planned to report the level of evidence as 'no evidence to support or refute' (Guyatt 2013b)."
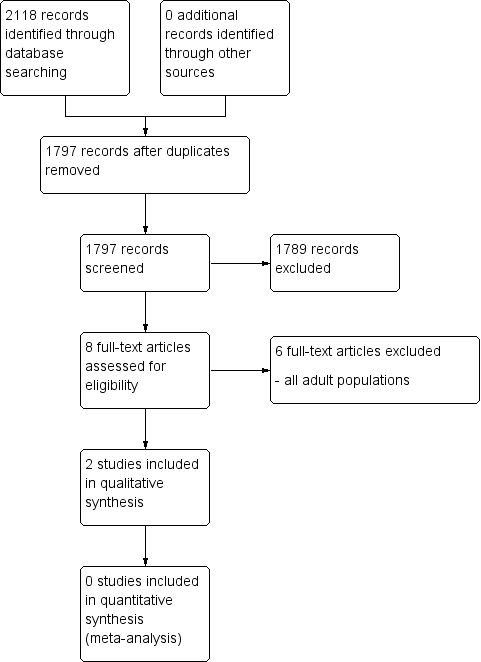
Study flow diagram.
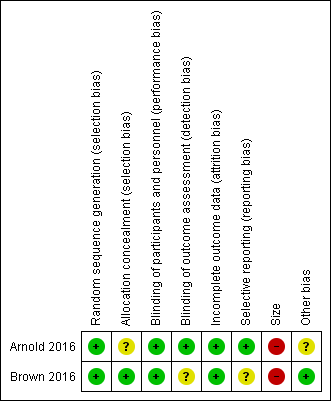
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
| Gabapentin compared with amitriptyline for chronic non‐cancer pain | ||||||
| Patient or population: children and adolescents (birth to 17 years of age) with chronic non‐cancer pain Settings: primary care Intervention: gabapentin Comparison: amitriptyline | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No. of participants | Quality of the evidence | Comments | |
| Amitriptyline | Gabapentin | |||||
| Participant‐reported pain relief of 30% or greater | No data | No data | N/A | N/A | ‐ | No evidence to support or refuteb |
| Participant‐reported pain relief of 50% or greater | No data | No data | N/A | N/A | ‐ | No evidence to support or refuteb |
| Patient Global Impression of Change: much improved or very much improved | No data | No data | N/A | N/A | ‐ | No evidence to support or refuteb |
| Any adverse events | 1/17 | 2/17 | N/A | 34 participants (1 study) | ⊕⊝⊝⊝ | |
| Serious adverse events | 0/17 | 0/17 | N/A | 34 participants (1 study) | ⊕⊝⊝⊝ | |
| Withdrawals due to adverse events | 1/17 | 2/17 | N/A | 34 participants (1 study) | ⊕⊝⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; N/A: not applicable; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: We are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of effect, but there is a possibility that it is substantially different. Low quality: Our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low quality: We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
| aDowngraded three levels due to too few data and number of events were too small to be meaningful. bNo data available for this outcome, and therefore no GRADE rating has been applied and there is no evidence to support or refute. | ||||||
| Pregabalin compared with placebo for chronic non‐cancer pain | ||||||
| Patient or population: children and adolescents (birth to 17 years of age) with chronic non‐cancer pain Settings: multicentre, USA (28 primary care centres), India (5 primary care centres), Taiwan (2 primary care centres), and Czech Republic (1 primary care centre) Intervention: pregabalin Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No. of participants | Quality of the evidence | Comments | |
| Placebo | Pregabalin | |||||
| Participant‐reported pain relief of 30% or greater** | 16/51 | 18/54 | N/A | 107 participants (1 study) | ⊕⊝⊝⊝ | |
| Participant‐reported pain relief of 50% or greater** | 4/51 | 9/54 | N/A | 107 participants (1 study) | ⊕⊝⊝⊝ | |
| Patient Global Impression of Change: much improved or very much improved** | 15/51 | 29/54 | N/A | 107 participants (1 study) | ⊕⊝⊝⊝ | |
| Adverse events | 34/53 | 38/54 | N/A | 107 participants (1 study) | ⊕⊝⊝⊝ | |
| Serious adverse events | 0/53 | 1/54 | N/A | 107 participants (1 study) | ⊕⊝⊝⊝ | |
| Withdrawals due to adverse events | 4/53 | 4/54 | N/A | 107 participants (1 study) | ⊕⊝⊝⊝ | |
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: We are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of effect, but there is a possibility that it is substantially different. Low quality: Our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. Very low quality: We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect. | ||||||
| aDowngraded three levels due to too few data and number of events were too small to be meaningful. bNo data available for this outcome, and therefore no GRADE rating has been applied and there is no evidence to support or refute. | ||||||