| Lay‐led and peer support interventions compared with usual care for adolescents with asthma |
| Patient or population: adolescents with asthma Settings: school, day camp or primary care Intervention: lay‐led and peer support interventions Comparison: usual care/no intervention |
| Asthma‐related quality of life (PAQLQ) 1 to 7 scale; higher = better 3 to 9 months | Mean change in control groups was 0.05 | Mean change in intervention groups was
0.40 better (0.02 worse to 0.81 better) | 578
(3 RCTs) | ⊕⊕⊝⊝
LOWa,b | |
| Asthma‐related quality of life (MCID) 8 months | 123 per 1000 | 248 per 1000
(145 to 390) | 251
(1 RCT) | ⊕⊕⊝⊝
LOWa,c,d | |
| Asthma control Scale (range, score) ACT (5‐23) and ACQ (4‐16) 4 to 9 months | Not pooled. Two studies reported 2 different measures. Both effects favoured peer support, but neither result was statistically significant | 166
(2 RCTs) | ⊕⊕⊝⊝
LOWa,e | |
| Unscheduled visits 9 months | Somewhat fewer mean visits per person in the intervention group than in the control group, but the data are skewed and are difficult to interpret | 84
(1 RCT) | Not graded | |
| Medication adherence 2.5 months | Skewed data reported non‐parametrically. Low baseline adherence (˜ 26%), which dropped further in both groups after the intervention, although it was less in the intervention group | 68 (1 RCT) | Not graded | Adherence to ICS was measured objectively with a dose counter |
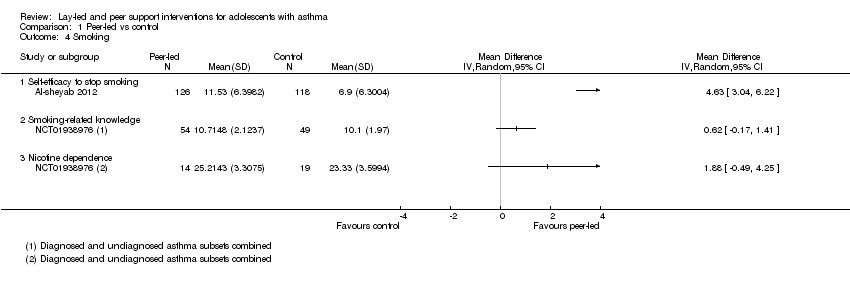
| Smoking 3 to 4 months | Mean self‐efficacy to stop smoking score in control group was 6.9 | Mean score in intervention groups was 4.63 better (3.04 to 6.22 better) | 244
(1 RCT) | ⊕⊕⊝⊝
LOWa,e | SANDS subscale Range 0 to 16 |
| Mean smoking‐related knowledge score in control group was 10.1 | Mean score in intervention groups was 0.62 better (‐0.17 worse to 1.41 better) | 103
(1 RCT) | Modified Tar‐Wars scale Range 0 to 13 |
| Mean nicotine dependence score in control group was 23.3 | Mean score in intervention groups was 1.88 better (‐0.49 worse to 4.25 better) | 33
(1 RCT) | SANDS total Range 0 to 32 |
| Adverse events | No reports of adverse events, although only specifically mentioned in 1 study | ‐ | Not graded | |
| *The basis for the assumed risk (e.g. median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
ACQ: asthma control questionnaire; ACT: asthma control test; CI: confidence interval; ICS: inhaled corticosteroid; MCID: minimal clinically important difference; PAQLQ: Paediatric Asthma Quality of Life Questionnaire; RCT: randomised controlled trial; RR: risk ratio; SANDS: Self‐Administered Nicotine Dependence Scale. |
| GRADE Working Group grades of evidence. High quality: We are very confident that the true effect lies close to the estimate of effect.
Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of effect but may be substantially different.
Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of effect.
Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect. |