La thérapie familiale pour le traitement des troubles du spectre autistique
Appendices
Appendix 1. Search strategies
Cochrane Central Register of Controlled Trials (CENTRAL) in the Cochrane Library
#1[mh "child development disorders, pervasive"]
#2[mh ^"Developmental Disabilities"]
#3pervasive development* disorder*
#4(pervasive near/3 child*)
#5(PDD or PDDs or PDD‐NOS or ASD or ASDs)
#6autis*
#7asperger*
#8kanner*
#9childhood near/1 schizophreni*
#10{or #1‐#9}
#11[mh "family therapy"]
#12[mh "group therapy"]
#13[mh "psychotherapy, group"]
#14[mh "couples therapy"]
#15[mh "marital therapy"]
#16(systemic* near/3 psychotherap*)
#17(systemic* near/3 psycho‐therap*)
#18(systemic* near/3 famil*)
#19(famil* near/3 (intervention* or therap* or treat* or program*)) 4
#20(famil* near/3 (psychotherap* or psychoeducation* or psycho next education* or psycho next therap*)) 3
#21((marriage or marital or couple*) near/3 therap*)
#22(famil* near/1 (involv* or integrat* or participat* or focus*))
#23(psychodynamic or psycho next dynamic)
#24(group* near/3 psychotherap*)
#25(group* near/3 psycho next therap*)
#26(systemic next therap*)
#27(solution next focus*)
#28(narrative near/3 therap*)
#29{or #11‐#28}
#30#10 and #29 in Trials
MEDLINE Ovid
1 exp child development disorders, pervasive/
2 Developmental Disabilities/
3 pervasive development$ disorder$.tw.
4 (pervasive adj3 child$).tw.
5 (PDD or PDDs or PDD‐NOS or ASD or ASDs).tw.
6 autis$.tw.
7 asperger$.tw.
8 kanner$.tw.
9 childhood schizophreni$.tw.
10 or/1‐9
11 family therapy/
12 group therapy/
13 psychotherapy, group/
14 couples therapy/
15 marital therapy/
16 (systemic$ adj3 psychotherap$).tw.
17 (systemic$ adj3 psycho‐therap$).tw.
18 (systemic$ adj3 famil$).tw.
19 (famil$ adj3 (intervention$ or therap$ or treat$ or program$)).tw.
20 (famil$ adj3 (psychotherap$ or psychoeducation$ or psycho‐education$ or psycho‐therap$)).tw.
21 ((marriage or marital or couple$) adj3 therap$).tw.
22 (famil$ adj1 (involv$ or integrat$ or participat$ or focus$)).tw.
23 (psychodynamic or psycho‐dynamic).tw.
24 (group$ adj3 psychotherap$).tw.
25 (group$ adj3 psycho‐therap$).tw.
26 systemic therap$.tw.
27 solution focus$.tw.
28 (narrative adj1 therap$).tw.
29 or/11‐28
30 10 and 29
MEDLINE Ovid Epub Ahead of Print
1 pervasive development$ disorder$.tw.
2 (pervasive adj3 child$).tw.
3 (PDD or PDDs or PDD‐NOS or ASD or ASDs).tw.
4 autis$.tw.
5 asperger$.tw.
6 kanner$.tw.
7 childhood schizophrenia.tw.
8 or/1‐7
9 (systemic$ adj3 psychotherap$).tw.
10 (systemic$ adj3 psycho‐therap$).tw.
11 (systemic$ adj3 famil$).tw.
12 (famil$ adj3 (intervention$ or therap$ or treat$ or program$)).tw.
13 (famil$ adj3 (psychotherap$ or psychoeducation$ or psycho‐education$ or psycho‐therap$)).tw.
14 (famil$ adj1 (involv$ or integrat$ or participat$ or focus$)).tw.
15 ((marriage or marital or couple$) adj3 therap$).tw.
16 (psychodynamic or psycho‐dynamic).tw.
17 (group$ adj3 psychotherap$).tw.
18 (group$ adj3 psycho therap$).tw.
19 systemic therap$.tw.
20 solution focus$.tw.
21 (narrative adj1 therap$).tw.
22 or/9‐21
23 8 and 22
MEDLINE Ovid In‐Process and Other Non‐Indexed Citations
1 pervasive development$ disorder$.tw.
2 (pervasive adj3 child$).tw.
3 (PDD or PDDs or PDD‐NOS or ASD or ASDs).tw.
4 autis$.tw.
5 asperger$.tw.
6 kanner$.tw.
7 childhood schizophrenia.tw.
8 or/1‐7
9 (systemic$ adj3 psychotherap$).tw.
10 (systemic$ adj3 psycho‐therap$).tw.
11 (systemic$ adj3 famil$).tw.
12 (famil$ adj3 (intervention$ or therap$ or treat$ or program$)).tw.
13 (famil$ adj3 (psychotherap$ or psychoeducation$ or psycho‐education$ or psycho‐therap$)).tw.
14 (famil$ adj1 (involv$ or integrat$ or participat$ or focus$)).tw.
15 ((marriage or marital or couple$) adj3 therap$).tw.
16 (psychodynamic or psycho‐dynamic).tw.
17 (group$ adj3 psychotherap$).tw.
18 (group$ adj3 psycho therap$).tw.
19 systemic therap$.tw.
20 solution focus$.tw.
21 (narrative adj1 therap$).tw.
22 or/9‐21
23 8 and 22
Embase OVID
1 exp autism/
2 pervasive development$ disorder$.tw.
3 (PDD or PDDs or ASD or ASDs).tw.
4 autis$.tw.
5 asperger$.tw.
6 kanner$.tw.
7 childhood schizophreni$.tw.
8 Rett$.tw.
9 (pervasive adj3 child$).tw.
10 or/1‐9
11 family therapy/
12 group therapy/
13 marital therapy/
14 (systemic$ adj3 psychotherap$).tw.
15 (systemic$ adj3 psycho‐therap$).tw.
16 (systemic$ adj3 famil$).tw.
17 (famil$ adj3 (intervention$ or therap$ or treat$ or program$)).tw.
18 (famil$ adj3 (psychotherap$ or psychoeducation$ or psycho‐education$ or psycho‐therap$)).tw.
19 ((marriage or marital or couple$) adj3 therap$).tw.
20 (famil$ adj1 (involv$ or integrat$ or participat$ or focus$)).tw.
21 (psychodynamic or psycho‐dynamic).tw.
22 (group$ adj3 psychotherap$).tw.
23 (group$ adj3 psycho‐therap$).tw.
24 systemic therap$.tw.
25 solution focus$.tw.
26 (narrative adj1 therap$).tw.
27 or/11‐26
28 10 and 27
CINAHLPlus EBSCOhost (Cumulative Index to Nursing and Allied Health Literature)
S27 S9 AND S26
S26 S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25
S25 (narrative N1 therap*)
S24 solution focus*
S23 systemic therap*
S22 (group* N3 (psychotherap* or psycho‐therap*) )
S21 (psychodynamic or psycho‐dynamic)
S20 (famil* N1 (involv* or integrat* or participat* or focus*))
S19 ((marriage or marital or couple*) N3 therap*)
S18 (famil* N3 (psychotherap* or psychoeducation* or psycho‐education*or psycho‐therap*))
S17 (famil* N3 (intervention* or therap* or treat* or program*))
S16 (systemic* N3 famil*)
S15 (systemic* N3 psycho‐therap*)
S14 (systemic* N3 psychotherap*)
S13 (MH "Couples Counseling")
S12 (MH "Psychotherapy, Group")
S11 (MH "Family Therapy")
S10 (MH "Family Systems Theory") OR (MH "Family Services")
S9 S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8
S8 (MH "Developmental Disabilities")
S7 childhood schizophren*
S6 Kanner*
S5 Rett*
S4 Asperger*
S3 (autis* or ASD or ASDs)
S2 (pervasive development* disorder* or PDD or PDDs)
S1 (MH "Child Development Disorders, Pervasive+")
Cochrane Database of Systematic Reviews (CDSR) part of the Cochrane Library
#1[mh "child development disorders, pervasive"]
#2[mh ^"Developmental Disabilities"]
#3"pervasive development* disorder*":ti,ab
#4(pervasive near/3 child*):ti,ab
#5autis* :ti,ab
#6asperger*:ti,ab
#7kanner*:ti,ab
#8{or #1‐#7}
#9[mh "family therapy"]
#10[mh "group therapy"]
#11[mh "psychotherapy, group"]
#12[mh "couples therapy"]
#13[mh "marital therapy"]
#14(systemic* near/3 psychotherap*):ti,ab
#15(systemic* near/3 psycho‐therap*):ti,ab
#16(systemic* near/3 famil*):ti,ab
#17(famil* near/3 (intervention* or therap* or treat* or program*)):ti,ab
#18(famil* near/3 (psychotherap* or psychoeducation* or psycho next education* or psycho next therap*)):ti,ab
#19((marriage or marital or couple*) near/3 therap*):ti,ab
#20(famil* near/1 (involv* or integrat* or participat* or focus*)):ti,ab
#21(psychodynamic or psycho next dynamic):ti,ab
#22(group* near/3 psychotherap*):ti,ab
#23(group* near/3 psycho next therap*):ti,ab
#24("systemic therap*"):ti,ab
#25("solution focus*"):ti,ab
#26(narrative near/1 therap*):ti,ab
#27{or #9‐#26}
#28#8 and #27
Database of Abstracts of Reviews of Effects (DARE) part of the Cochrane Library
#1[mh "child development disorders, pervasive"]
#2[mh ^"Developmental Disabilities"]
#3"pervasive development* disorder*"
#4(pervasive near/3 child*)
#5autism or autistic
#6asperger*
#7kanner*:
#8{or #1‐#7}
#9[mh "family therapy"]
#10[mh "group therapy"]
#11[mh "psychotherapy, group"]
#12[mh "couples therapy"]
#13[mh "marital therapy"]
#14(systemic* near/3 psychotherap*)
#15(systemic* near/3 psycho‐therap*)
#16(systemic* near/3 famil*):
#17(famil* near/3 (intervention* or therap* or treat* or program*))
#18(famil* near/3 (psychotherap* or psychoeducation* or psycho next education* or psycho next therap*))
#19((marriage or marital or couple*) near/3 therap*)
#20(famil* near/1 (involv* or integrat* or participat* or focus*))
#21(psychodynamic or psycho next dynamic)
#22(group* near/3 psychotherap*)
#23(group* near/3 psycho next therap*)
#24("systemic therap*")
#25("solution focus*"):
#26(narrative near/1 therap*)
#27{or #9‐#26}
#28#8 and #27
ERIC EBSCOhost (Education Resources Information Center)
S27 S9 AND S26
S26 S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25
S25 (narrative N1 therap*)
S24 "solution focus*"
S23 "systemic therap*"
S22 (group* N3 (psychotherap* or psycho‐therap*))
S21 (psychodynamic or psycho‐dynamic)
S20 TI(famil* N1 (involv* or integrat* or participat* or focus*)) OR AB(famil* N1 (involv* or integrat* or participat* or focus*)
S19 TI ((marriage or marital or couple*) N3 therap*) OR AB((marriage or marital or couple*) N3 therap*) Search modes ‐ Boolean/Phrase
S18 TI(famil* N3 (psychotherap* or psychoeducation* or psycho‐education* or psycho‐therap*))OR AB(famil* N3 (psychotherap* or psychoeducation* or psycho‐education* or psycho‐therap*))
S17 TI(famil* N3 (intervention* or therap* or treat* or program*)) OR AB(famil* N3 (intervention* or therap* or treat* or program*))
S16 (systemic* N3 famil*)
S15 (systemic* N3 psycho‐therap*)
S14 (systemic* N3 psycho‐therap*)
S13 (systemic* N3 psychotherap*)
S12 DE "Marriage Counseling"
S11 DE "Group Counseling" OR DE "Group Therapy"
S10 DE "Family Counseling" OR DE "Family Involvement" OR DE "Family Programs"
S9 S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8
S8 childhood schizophren*
S7 Kanner*
S6 Rett*
S5 Asperger*
S4 (autis* or ASD or ASDs)
S3 (pervasive development* disorder* or PDD or PDDs)
S2 DE "Pervasive Developmental Disorders" OR DE "Asperger Syndrome" OR DE "Autism"
S1 DE "Developmental Disabilities"
PsycINFO (Ovid)
1 exp pervasive developmental disorders/
2 Developmental disabilities/
3 pervasive development$ disorder$.tw.
4 (pervasive adj3 child$).tw.
5 autis$.tw.
6 asperger$.tw.
7 (autis$ or ASD or ASDs).tw.
8 Rett$.tw.
9 Kanner$.tw.
10 (PDD or PDDs or PDD‐NOS).tw.
11 childhood schizophreni$.tw.
12 or/1‐11
13 exp family therapy/
14 family intervention/
15 group psychotherapy/
16 conjoint therapy/
17 couples therapy/
18 marriage counseling/
19 (systemic$ adj3 psychotherap$).tw.
20 (systemic$ adj3 psycho‐therap$).tw.
21 (systemic$ adj3 famil$).tw.
22 (famil$ adj3 (intervention$ or therap$ or treat$ or program$)).tw.
23 (famil$ adj3 (psychotherap$ or psychoeducation$ or psycho‐education$ or psycho‐therap$)).tw.
24 ((marriage or marital or couple$) adj3 therap$).tw.
25 (famil$ adj1 (involv$ or integrat$ or participat$ or focus$)).tw.
26 (psychodynamic or psycho‐dynamic).tw.
27 (group$ adj3 psychotherap$).tw.
28 (group$ adj3 psycho‐therap$).tw.
29 systemic therap$.tw.
30 solution focus$.tw.
31 (narrative adj1 therap$).tw.
32 or/13‐31
33 12 and 32
Sociological Abstracts ProQuest
SU.EXACT("Autism") OR autis* or asperger* or kanner* or Rett* or pervasive N3 disorder* or pervasive N3 child* OR PDD or PDDs or PDD‐NOS or ASD or ASDs) AND ((famil* N/3 (intervention* or therap* or treat* or program*)) or (famil* N/3 (psychotherap* or psychoeducation* or "psycho education*" or "psycho therap*")) or (systemic* N/3 psychotherap*) or (systemic* N/3 "psycho‐ therap*") or (famil* N/1 (involv* or integrat* or participat* or focus*)) OR (group* N/3 psychotherap*) or systemic therap* or (group* N/3 psychotherap*) or (group* N/3 ("psycho‐therap*" or psychoeducation* or "psycho education*" or "psycho therap*")))
Dissertation Abstracts International ProQuest
(ab(child developmental disorders) OR ab((pervasive developmental disorders OR developmental disabilit$)) OR ab((pervasive development$ disorder$ OR pervasive adj3 child$)) OR ab((PDD OR PDDs OR PDD‐NOS OR ASD OR ASDs OR autis$)) OR ab((asperger$ OR kanner$)) OR ab(childhood schizophrenia)) AND (ab(family therapy) OR ab((group therapy OR group psychotherapy)) OR ab((couples therapy OR marital therapy)) OR ab((systemic$ adj3 psychotherap$ OR systemic$ adj3 psycho‐therap$)) OR ab((systemic$ adj3 famil$ OR famil$ adj3 (intervention$ OR therap$ OR treat$ OR program$))) OR ab((famil$ adj3 (psychotherap$ OR psychoeducation$ OR psycho‐education$ OR psycho‐therap$) OR (marriage OR marital OR couple$) adj3 therap$)) OR ab((famil$ adj1 (involv$ OR integrat$ OR participat$ OR focus$) OR psychodynamic OR psycho‐dynamic)) OR ab((group$ adj3 psychotherap$ OR group$ adj3 psycho therap$)) OR ab((systemic therap$ OR solution focus$)) OR ab(narrative adj1 therap))
AutismData
Searched "family therapy" as keyword
Records were compared manually with EN library; 6 unique records added to Endnote
UK Clinical Research Network (UKCRN) Study Portfolio
Searches:
Speciality : Mental health
Subtopic: Autism spectrum disoders
Research summary: family
Speciality : Mental health
Subtopic: Autism spectrum disoders
Research summary: systemic
Speciality : Mental health
Subtopic: Autism spectrum disoders
Research summary: psychotherapy
Speciality : Mental health
Subtopic: Autism spectrum disoders
Research summary: multisystemic
UK Clinical Trials Gateway (UKCTG)
family therapy autis*
systemic autis*
multisystemic autis*
ClinicalTrials.gov
autism | (family OR systemic OR group) AND (therapy) OR autism | (family OR systemic OR group) AND (psychotherapy)
World Health Organisation International Clinical Trials Registry Platform (WHO ICTRP)
(apps.who.int/trialsearch/AdvSearch.aspx)
Basic search: Autism AND group OR autism AND family or autism AND parent OR autism AND systemic
Appendix 2. Record of searches
| Database | Search | Date | Number of |
| Cochrane Central Register of Controlled Trials (CENTRAL) in the Cochrane Library | 23 October 2015 | Issue 9 of 12, September 2015 | 75 |
| 18 January 2017 | Issue 11 of 12, November 2016 | 15 | |
| MEDLINE Ovid | 22 October 2015 | 1946 to October Week 3 2015 | 559 |
| 17 January 2017 | 1946 to December Week 1 2016 | 74 | |
| MEDLINE Ovid Epub Ahead of Print | 17 January 2017 | 16 January 2017 | 15 |
| MEDLINE Ovid In‐Process & Other Non‐Indexed Citations | 17 January 2017 | 16 January 2017 | 39 |
| Embase OVID | 22 October 2015 | 1974 to 2015 Week 42 | 695 |
| 17 January 2017 | 1974 to 2017 Week 3 | 94 | |
| CINAHL Plus EBSCOhost (Cumulative Index to Nursing and Allied Health Literature) | 23 October 2015 | 1937 to current | 402 |
| 17 January 2017 | 1937 to current | 22 | |
| Cochrane Database of Systematic Reviews (CDSR) part of the Cochrane Library | 23 October 2015 | Issue 10 of 12, October 2015 | 15 |
| 18 January 2017 | Issue 1 of 12, January 2015 | 6 | |
| Database of Abstracts of Reviews of Effects (DARE) part of the Cochrane Library | 23 October 2015 | Issue 2 of 4, April 2015 | 4 |
| ERIC EBSCOhost (Education Resources Information Center) | 23 October 2015 | 1966 to current | 564 |
| 17 January 2017 | 1966 to current | 32 | |
| PsycINFO OVID | 22 October 2015 | 1967 to October Week 3 2015 | 1417 |
| 17 January 2017 | 1967 to January Week 2 2017 | 118 | |
| Sociological Abstracts ProQuest | 23 October 2015 | 1952 to current | 52 |
| 18 January 2017 | 1952 to current | 4 | |
| Dissertation Abstracts International ProQuest | 4 November 2015 | 1743 to current | 176 |
| 16 January 2017 | 1743 to current | 215 | |
| AutismData (autism.org.uk/autismdata) | 23 October 2015 | All years | 6 |
| 18 January 2017 | All years | 4 | |
| UK Clinical Research Network Study Portfolio (UKCRN; public.ukcrn.org.uk/search); replaced by UK Clinical Trials Gateway | 23 October 2015 | All years | 1 |
| UK Clinical Trials Gateway (UKCTG; ukctg.nihr.ac.uk); replaces UK Clinical Research Network Study Portfolio | 18 January 2017 | All years | 1 |
| ClinicalTrials.gov (clinicaltrials.gov/ct2/home) | 23 October 2015 | All years | 82 |
| 18 January 2017 | All years | 24 | |
| World Health Organisation International Clinical Trials Registry Platform (WHO ICTRP; apps.who.int/trialsearch/AdvSearch.aspx) | 23 October 2015 | All years | 91 |
| 18 January 2017 | All years | 3 | |
| Total records | 4805 | ||
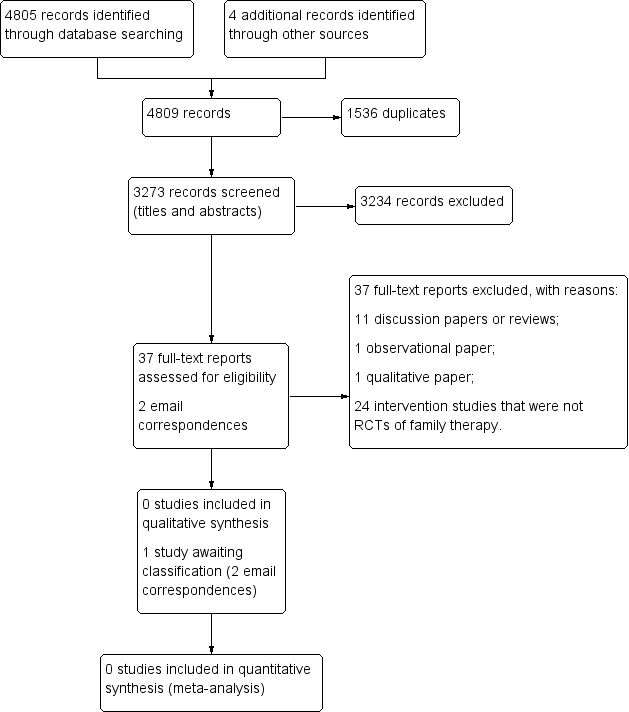
Study flow diagram.
| Unused methods | Description of methods |
| Data extraction and management | The data extraction form will include subheadings relating to the following areas.
We will attempt to separate the outcomes and results between sites for any multi‐centre studies. In the event that data described appear ambiguous for any of the reports, we will contact the authors for clarification. If we are unable to liaise with report authors, we will document this within the review, and the review team will discuss the discrepancies. For any non‐English language studies, we will endeavour to arrange for report translation. |
| Assessment of risk of bias in included studies | DS and JS will independently assess the risk of bias of all included studies across seven domains: random sequence generation; allocation concealment; blinding of participants and trial staff; blinding of outcome assessments; incomplete outcome data; selective outcome reporting; and any other potential sources of bias. For each included study, we will assign each of these domains one of three ratings: high risk of bias, low risk of bias, or unclear risk of bias. We have detailed criteria for rating various domains of bias below, with examples drawn from Chapter 8.5 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011a). Random sequence generation
Allocation concealment
Blinding of participants and research personnel
Blinding of outcome assessment
Incomplete outcome data
Selective reporting
Other sources of bias
We will obtain a third opinion from EP, MF or FH should there be disagreement about the 'Risk of bias' assessment or a lack of consensus about any of the individual domains per study or in terms of the overall appraisal of the trial. We will also attempt to contact report authors to provide clarification about aspects of the trial, as needed. |
| 'Summary of findings' tables | We will import data from Review Manager (Review Manager 2014), into GRADEprofiler (GRADEpro GDT), and use this software to create 'Summary of findings' tables. These tables will provide outcome‐specific information concerning the overall quality of the body of evidence from the studies included in the comparison, the magnitude of effect of the interventions examined, and the sum of available data on outcomes rated as relevant to patient care and decision making. We will include the following outcomes in the 'Summary of findings' tables.
|
| Measures of treatment effect | Dichotomous data For dichotomous outcomes, such as the presence or absence of challenging behaviour(s), we will use the Mantel‐Haenszel method for computing the pooled risk ratio (RR) (Mantel 1959). We will use the RR in meta‐analyses, rather than the odds ratio (OR), because the OR can be susceptible to misinterpretation, which can lead to overestimation of the benefits and harms of the intervention (Deeks 2011, Section 9.4.4.4). We will report the RR with 95% CIs. Continuous data When different measures are used, we will calculate the standardised mean difference and 95% CI. We will calculate the mean difference and 95% CI when all outcomes are measured using the same scale in the same way. |
| Unit of analysis issues | Cluster trials In cluster trials, the independence of individuals cannot be assumed (Higgins 2011b). As we are examining the effectiveness of an intervention for both individuals and family members, we may identify cluster‐randomised trials. If clustering has been incorporated into the analyses of primary studies, we plan to present these data as if from a non‐cluster‐randomised study, but adjust for the clustering effect. We will contact study authors for more information if needed. If we identify cluster trials that have been analysed using incorrect statistical methods (i.e. not taking the clustering into account), we will contact study authors to request individual participant data so that we may calculate an estimate of the intracluster correlation coefficient (ICC). If we are unable to obtain this information, we will adjust sample sizes using an estimate of the ICC from the trial or from a trial of a similar population, with advice from a statistician, and use this to re‐analyse the data. In the event that we are unable to adjust for incorrect statistical methods used by the cluster trials, and therefore cannot estimate the ICC with any a degree of confidence, we will exclude the trial (Higgins 2011b). We will investigate the robustness of our results by conducting sensitivity analyses, for example, to explore the impact of different types of cluster‐randomisation units (such as families, health practitioners) (Higgins 2011b). We will also compare the results with and without cluster trials that have not been analysed correctly by the trialists (where the ICC is estimated from other trials for the adjustment of cluster effect) (see Sensitivity analysis). Cross‐over trials Due to the issue of carry‐over, that is, whereby the effectiveness of a second intervention may be mediated by the first intervention, we will exclude cross‐over trials. Multiple comparisons Where a trial involves more than two treatment (or comparator) arms, we will first assess which intervention (or comparator) groups are relevant to our review. We will use data from the arms of the trial that are relevant to the review objectives, but present all intervention groups in the 'Characteristics of included studies' tables, providing a detailed description of why we have selected particular groups and excluded others. In the event that studies have more than two intervention groups and a control group that are relevant to the review, we will split the control group data proportionately to the other two groups. Repeated measures When a trial reports outcome data obtained at more than one time point, we will conduct analyses separately for each time point (e.g. postintervention and at follow‐up, if follow‐up is specified by the trialist). |
| Dealing with missing data | We will consider the possible impact of missing data on the results of the review. Data may be missing either because (1) they have been insufficiently or inadequately reported, or (2) due to dropout or attrition. In the event of insufficient or inadequate reporting, we will first try to obtain any missing data from the trial authors, including unreported data (e.g. group means and SDs), details of dropouts, and interventions provided. We will describe the missing data in the 'Risk of bias' table. In either case outlined above, and when we cannot obtain data, we will conduct analyses using ITT principles. For dichotomous outcomes (those not deemed to be missing at random), we will impute the outcomes for the missing participants using both the most optimistic (i.e. assuming participants with missing data improve) and the most pessimistic (i.e. assuming participants with missing data deteriorate) scenarios. When data are missing for continuous outcomes (e.g. data pertaining to means or SD), we will attempt to calculate them based on the standard errors, CIs, and t values, according to the rules described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011c). If this information is missing, and we are unable to obtain it from trial authors, we will report it as missing data in the review. We will also conduct a sensitivity analysis to compare the results from the ITT analysis with the imputation and ‘available case’ analysis (see Sensitivity analysis). If these analyses yield similar results in terms of the effects of treatment, we will present the results of the available case analyses. |
| Assessment of heterogeneity | Within each comparison, we will first assess clinical heterogeneity (e.g. variability in active and comparator interventions, participant characteristics, or outcome measures used) and methodological heterogeneity (e.g. variability in study design, including differences in the nature of the randomisation unit and the size of cluster randomised; and risk of bias, which we will assess according to the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2011)). If there is clinical or methodological heterogeneity, we will extract and document all of these characteristics onto the data extraction form and synthesise the results narratively. We will then assess statistical heterogeneity using the I² and Chi² statistics, and by visually inspecting the forest plots. If we identify a substantial level of heterogeneity in trials (e.g. the I² is more than 30% to 60%, the P value is less than 0.10 in the Chi² test for heterogeneity, or there is a different direction of the effects), we will conduct prespecified subgroup analyses (see Subgroup analysis and investigation of heterogeneity). |
| Assessment of reporting biases | We will assess reporting biases, including (multiple) publication, selective reporting, outcome and language biases (Sterne 2011, Table 10.1.a). First, we will try to locate protocols of included trials. If the protocol is available, we will compare outcomes documented in the protocol and the published report. If the protocol is not available, we will compare outcomes listed in the methods section of the trial report with the reported results. In addition, we will create funnel plots to investigate the possibility of publication bias and other small‐study effects when there is a sufficient number of trials (10 or more). While funnel plots may be useful in investigating reporting biases, there is some concern that tests for funnel plot asymmetry have limited power to detect small‐study effects, particularly when there are fewer than 10 studies, or when all studies are of a similar sample size (Sterne 2011). In the event that funnel plots are possible, we will produce them and seek statistical advice in their interpretation. |
| Data synthesis | We will conduct random‐effects meta‐analyses to produce the average effect size of the intervention across trials. A random‐effects model is considered more appropriate than a fixed‐effect model because the population and setting of trials are likely to be different, and therefore the effects are also likely to be different (Deeks 2011). |
| Subgroup analysis and assessment of heterogeneity | Depending on the sample size and heterogeneity of study populations, we propose to undertake subgroup analyses as follows:
To limit the risk of multiple comparisons, we will conduct subgroup analyses on primary outcomes only. |
| Sensitivity analysis | We will undertake sensitivity analyses to evaluate the impact of excluding trials (or trial data) that are judged to have a high risk of bias (e.g. in terms of the domains of random sequence generation, allocation concealment, blinding, or outcome reporting). We will also undertake sensitivity analyses to assess the potential impact of missing outcome data. |
| ASD: autism spectrum disorder; CI: confidence interval; GRADE: Grades of Recommendation, Assessment, Development and Evaluation; ITT: intention‐to‐treat; IQ: intelligence quotient; RCTs: randomised controlled trials; SD: standard deviation. | |