Entraînement du corps entier sur appareil vibratoire contre la fibromyalgie
Appendices
Appendix 1. Levels of evidence in overviews of antiepileptic drugs (Wiffen 2013)
First tier ‐ at least 50% pain intensity reduction over baseline (or its equivalent), without the use of last observation carried forward (LOCF) for dropouts, an intention‐to‐treat (ITT) analysis, in parallel‐group studies with at least 200 participants lasting eight weeks or longer.
Second tier ‐ evidence related to data from at least 200 participants when one or more of the above conditions were not met.
Third tier ‐ evidence related to data from fewer than 200 participants, or with several important methodological problems that limited interpretation.
Appendix 2. Example of a vibration exercise regimen
-
Equipment: vibrating platform (PowerPlate, North America Inc., Northbrook, IL)
-
Characteristics of the vibration: triplanar vibration, frequency of 30 Hz, peak to peak displacement of 4 mm (71.1 ms‐2 ≈ 7.2 g)
-
Starting position: participants stood on the platform with weight through both feet with trunk upright and both knees in 60° of knee flexion
-
Exercise instructions: attempt to hold starting position (isometric contraction)
-
Progression of the exercise regimen:
Weeks 1‐2
1. 6 × 30 s/45 s rest (bilateral squat)
2. 4 × 30 s/45 s (unilateral squat)
Weeks 3‐4
1. 7 × 30 s/45 s rest (bilateral squat)
2. 5 × 30 s/45 s (unilateral squat)
Weeks 5‐6
1. 8 × 30 s/45 s rest (bilateral squat)
2. 6 × 30 s/45 s (unilateral squat)
Weeks 7‐8
1. 9 × 30 s/45 s rest (bilateral squat)
2. 7 × 30 s/45 s (unilateral squat)
From Sañudo 2013.
Appendix 3. Medline (OVID) search strategy
1. Fibromyalgia/
2. Fibromyalgi$.tw.
3. fibrositis.tw.
4. or/1‐3
5. exp Exercise/
6. Physical Exertion/
7. Physical Fitness/
8. exp Physical Endurance/
9. exp Sports/
10. Pliability/
11. exertion$.tw.
12. exercis$.tw.
13. sport$.tw.
14. ((physical or motion) adj5 (fitness or therapy or therapies)).tw.
15. (physical$ adj2 endur$).tw.
16. manipulat$.tw.
17. (skate$ or skating).tw.
18. jog$.tw.
19. swim$.tw.
20. bicycl$.tw.
21. (cycle$ or cycling).tw.
22. walk$.tw.
23. (row or rows or rowing).tw.
24. weight train$.tw.
25. muscle strength$.tw.
26. exp Yoga/
27. yoga.tw.
28. exp Tai Ji/
29. tai chi.tw.
30. Ai Chi.tw.
31. exp Vibration/
32. vibration.tw.
33. pilates.tw.
34. or/5‐33
35. 4 and 34
Appendix 4. Embase (OVID) search strategy
1 FIBROMYALGIA/
2 fibromyalgi$.tw.
3 fibrositis.tw.
4 or/1‐3
5 exp exercise/
6 fitness/
7 exercise tolerance/
8 exp sport/
9 pliability/
10 exertion$.tw.
11 exercis$.tw.
12 sport$.tw.
13 ((physical or motion) adj5 (fitness or therapy or therapies)).tw.
14 (physical$ adj2 endur$).tw.
15 manipulat$.tw.
16 (skate$ or skating).tw.
17 jog$.tw.
18 swim$.tw.
19 bicycl$.tw.
20 (cycle$ or cycling).tw.
21 walk$.tw.
22 (row or rows or rowing).tw.
23 weight train$.tw.
24 muscle strength$.tw.
25 or/5‐24
26 4 and 25
Appendix 5. Cochrane Library (Wiley) search strategy
#1 MeSH descriptor Fibromyalgia explode all trees
#2 fibromyalgia
#3 fibrositis
#4 (#1 OR #2 OR #3)
#5 MeSH descriptor Exercise explode all trees
#6 MeSH descriptor Physical Exertion explode all trees
#7 MeSH descriptor Physical Fitness explode all trees
#8 MeSH descriptor Exercise Tolerance explode all trees
#9 MeSH descriptor Sports explode all trees
#10 MeSH descriptor Pliability explode all trees
#11 exertion*
#12 exercis*
#13 sport*
#14 (physical or motion) near/5 (fitness or therapy or therapies)
#15 physical* near/2 endur*
#16 manipulat*
#17 skate* or skating
#18 jog*
#19 swim*
#20 bicycl*
#21 cycle*
#22 walk*
#23 row or rows or rowing
#24 weight next train*
#25 muscle next strength*
#26 MeSH descriptor Yoga explode all trees
#27 yoga
#28 tai chi
#29 MeSH descriptor Tai Ji explode all trees
#30 MeSH descriptor Vibration explode all trees
#31 vibration
#32 pilates
#33 (#5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR ( # AND 27 ) OR #28 OR #29 OR #30 OR #31 OR #32)
#34 (#33 AND #4)
A second search was conducted in the Cochrane Library of the HTA database, specifically, using the vibration terms alone to supplement the search above with a more sensitive search for health technology assessments of vibration platforms.
#1 MeSH descriptor Vibration explode all trees
#2 vibration
#3 (#1 OR #2)
Appendix 6. CINAHL (EBSCOhost) search strategy
S01 (MH "Fibromyalgia")
S02 TI fibromyalgia or AB fibromyalgia
S03 TI fibrositis or AB fibrositis
S04 (MH "Exercise+")
S05 (MH "Exertion+")
S06 (MH "Physical Fitness")
S07 (MH "Exercise Test+")
S08 (MH "Sports+")
S09 (MH "Pliability")
S10 (MH "Physical Endurance+")
S11 TI exertion* or AB exertion*
S12 TI exercis* or AB exercis*
S13 TI sport* or AB sport*
S14 TI physical N5 fitness or TI physical N5 therapy or TI physical N5 therapies or AB physical N5 fitness or AB physical N5 therapy or AB physical N5 therapies
S15 TI motion N5 fitness or TI motion N5 therapy or TI motion N5 therapies or AB motion N5 fitness or AB motion N5 therapy or AB motion N5 therapies
S16 TI physical* N2 endur* or AB physical* N2 endur*
S17 ( skate* or skating ) or AB ( skate* or skating )
S18 jog* or AB jog*
S19 TI swim* or AB swim*
S20 TI bicycl* or AB bicycl*
S21 TI ( (cycle* or cycling) ) or AB ( (cycle* or cycling) )
S22 TI walk* or AB walk*
S23 TI ( row or rows or rowing ) or AB ( row or rows or rowing )
S24 TI weight train* or AB weight train*
S25 TI muscle strength* or AB muscle strength*
S26 TI manipulat* or AB manipulat*
S27 S1 or S2 or S3
S28 S4 or S5 or S6 or S7 or S8 or S9 or S10 or S11 or S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22 or S23 or S24 or S25 or S26
S29 S27 and S28
S30 S27 and S28
S31 (MH "Yoga Pose") OR (MH "Yoga")
S32 TX yoga
S33 TX tai chi
S34 (MM "Tai Chi")
S35 TX tai ji
S36 TX pilates
S37 (MH "Pilates") OR "pilates"
S38 (MH "Vibration")
S39 TX vibration
S40 S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39
S41 (S27 and (S28 or S40)
Appendix 7. PEDro Physiotherapy Evidence Database (http://www.pedro.org.au/) search strategy
Terms searched:
-
fibromyalg* AND fitness training
-
fibromyalg* AND strength training
-
fibrositis
Appendix 8. Dissertation Abstracts (ProQuest) search strategy
Terms searched fibromyalg* or fibrositis (in citation or abstract)
Appendix 9. Current Controlled Trials (http://www.controlled‐trials.com/) and ClinicalTrials.gov search strategy
Terms searched fibromyalg* or fibrositis
Appendix 10. WHO International Clinical Trials Registry Platform (http://www.who.int/ictrp/en/) search strategy
Terms searched fibromyalg* or fibrositis in Condition
Appendix 11. AMED (OVID) Allied and Complementary Medicine search strategy
OVID AMED (Allied and Complementary Medicine)
1 Fibromyalgia/ (1453)
2 Fibromyalgi$.tw. (1626)
3 fibrositis.tw. (20)
4 or/1‐3 (1631)
5 exp Exercise/ (7293)
6 Physical Fitness/ (1655)
7 exp Physical Endurance/ (747)
8 exp Sports/ (3576)
9 Pliability/ (32)
10 exertion$.tw. (1129)
11 exercis$.tw. (18675)
12 sport$.tw. (4952)
13 ((physical or motion) adj5 (fitness or therapy or therapies)).tw. (8773)
14 (physical$ adj2 endur$).tw. (629)
15 manipulat$.tw. (4038)
16 (skate$ or skating).tw. (81)
17 jog$.tw. (158)
18 swim$.tw. (552)
19 bicycl$.tw. (972)
20 (cycle$ or cycling).tw. (3530)
21 walk$.tw. (7139)
22 (row or rows or rowing).tw. (174)
23 weight train$.tw. (149)
24 muscle strength$.tw. (5651)
25 exp pilates/ (22)
26 exp Yoga/ (345)
27 exp Tai chi/ (204)
28 Tai ji.tw. (6)
29 yoga.tw. (448)
30 (hatha or kundalini or ashtunga or bikram).tw. (26)
31 pilates.tw. (62)
32 exp Exercise therapy/ (4945)
33 or/5‐32 (43624)
34 4 and 33 (328)
Appendix 12. Centre for Reviews and Dissemination search strategy
Terms searched in the CRD HTA databas: e(fibromyalg* ) AND (vibrat*).
Appendix 13. Agency for Healthcare Research and Quality – Technology Assessments search strategy
Browsed Musculoskeletal Disorders in Research Summaries, Reviews and Reports.
Appendix 14. CADTH Canadian Search Interface HTA Database search strategy
Term searched: “vibration”.
Appendix 15. Selection strategy
Level one screen
Based solely on the title of the report.
-
Does the study deal exclusively with fibromyalgia? No – exclude, Yes or uncertain ‐ go to step two.
-
Does it include exercise? No – exclude, Yes or uncertain – go to step three.
-
Does the study deal exclusively with adults? No – exclude, Yes or uncertain – go to step four.
-
Is it an RCT? No – exclude, Yes or uncertain – include.
Level two screen
Based solely on the abstract of the report.
-
Does the study deal exclusively with fibromyalgia? No – exclude, Yes or uncertain ‐ go to step two.
-
Does it include exercise? No – exclude, Yes or uncertain – go to step three.
-
Does the study deal exclusively with adults? No – exclude, Yes or uncertain – go to step four.
-
Is it an RCT? No – exclude, Yes or uncertain – include.
Level three screen
Based on the full text of the report.
-
Does the study deal exclusively with fibromyalgia? No ‐ exclude, Yes ‐ go to step two, Uncertain ‐ add to list of questions for trial author and proceed to step two.
-
Is the diagnosis of fibromyalgia based on published criteria? No ‐ exclude, Yes ‐ go to step three, Uncertain ‐ add to list of questions for trial author and proceed to step three.
-
Does the study deal exclusively with adults? No ‐ exclude, Yes ‐ go onto step four, Uncertain ‐ add to list of questions for trial author and proceed to step four.
-
Is it an RCT? (study uses terms such as "random," "randomized," "RCT," or "randomization" to describe study design or assignment of participants to groups): No ‐ exclude, Yes ‐ go on to step five, Uncertain ‐ add to list of questions for trial author and proceed to step five.
-
Does the study include exercise (study involves at least one intervention that includes exercise)? No ‐ exclude, Yes ‐ go on to step six, Uncertain ‐ add to list of questions for trial author and proceed to step six.
-
Are between‐group data provided for outcomes? No (study contains only fibromyalgia or results are reported in such a way that effects on fibromyalgia cannot be isolated) ‐ exclude, Yes ‐ include the study, Yes but uncertain about one or more of steps 1 to 5 to reserve judgement until trial authors are contacted.
Level four screen (classification of study using team's intervention listing)
-
Classification of design
-
Number of interventions
-
Type of comparisons:
-
Head‐to‐head comparison?
-
Exercise to control?
-
Composite to control
-
-
-
Control group
-
-
Classify type of control
-
-
Exercise
-
-
Enter types of exercise interventions used in the study
-
Complete the naming of intervention groups
-
Appendix 16. 2011 ACSM position stand: guidance for prescribing exercise
The following recommendations were derived from Garber 2011.
Recommendations for cardiorespiratory fitness
-
Moderate‐intensity cardiorespiratory exercise training for ≥ 30 minutes/d on ≥ 5 days per week for a total of ≥ 150 minutes per week, vigorous‐intensity cardiorespiratory exercise training for ≥ 20 minutes/d on ≥ 3 days per week (≥ 75 minutes/wk), or a combination of moderate‐ and vigorous‐intensity exercise to achieve total energy expenditure ≥ 500 to 1000 MET min/wk
Recommendations for muscular fitness
-
On 2 to 3 days per week, adults should also perform resistance exercises for each of the major muscle groups, as well as neuromotor exercise involving balance, agility, and coordination
-
Two to four sets of resistance exercise per muscle group is recommended, but even a single set of exercise may significantly improve muscle strength and size
-
Rest interval between sets if more than one set is performed: 2 to 3 minutes
-
Resistance equivalent of 60% to 80% of one repetition max (1RM) effort. For novices, 60% to 70% of 1RM is recommended; for experienced, exercises ≥ 80% may be appropriate
-
Selected resistance should permit completion of 8 to 12 repetitions per set or number needed to induce muscle fatigue but not exhaustion
-
For people who wish to focus on improving muscular endurance, lower intensity (< 50% of 1RM) can be used with 15 to 25 repetitions in no more than 2 sets
Recommendations for flexibility
-
Series of flexibility exercises for each of the major muscle–tendon groups with a total of 60 seconds per exercise on ≥ 2 days per week is recommended. Series of exercises targeting major muscle‐tendon units of the shoulder girdle, chest, neck, trunk, lower back, hops, posterior and anterior legs, and ankles is recommended. For most individuals, this routine can be completed within 10 minutes
-
Stretches should be held for 1 to 30 seconds at the point of tightness or slight discomfort. Older persons may realize greater improvements in range of motion with longer durations (30 to 60 seconds) os stretching. A 20% to 75% maximum contraction held for 3 to 6 seconds followed by a 10 to 30 second assisted stretch is recommended for PNF (proprioceptive neuromuscular facilitation) techniques
-
Repeating each flexibility exercise 2 to 4 times is effective
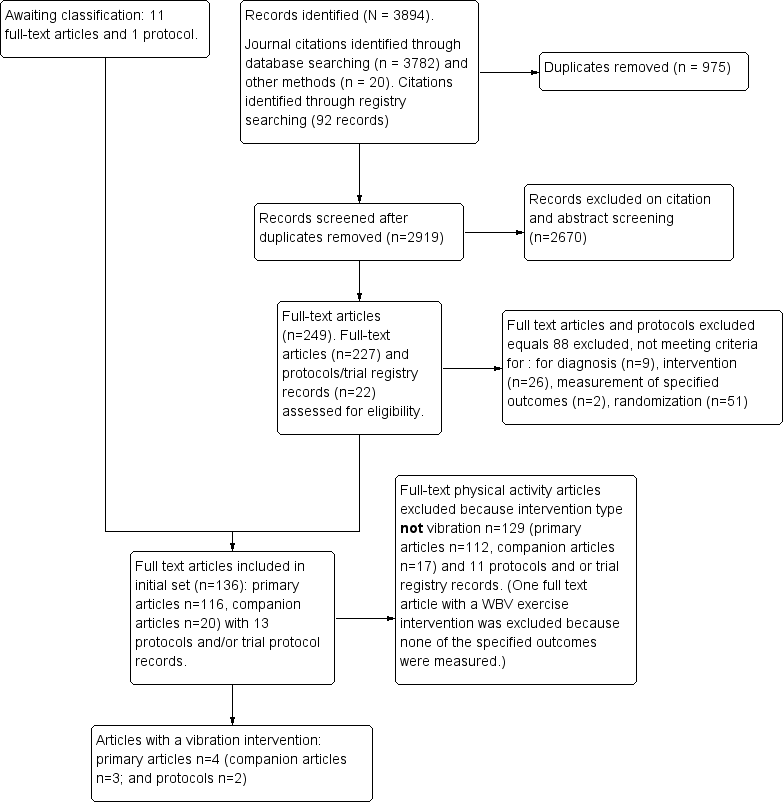
Study flow diagram for vibration training interventions.

Galileo Fitness Platform (Copyright © 2008‐2015 Novotec Medical GmbH; reproduced with permission)

Copyright © 2012 Wellsports GmbH Krefeld ‐ PowerPlate International B.V., The Netherlands ‐ awaiting response.Sept15

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
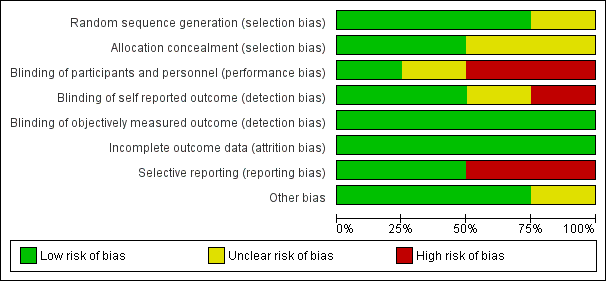
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Comparison 1 WBV vs C, Outcome 1 HRQL, 1‐100 scale, lower means better HRQL.

Comparison 1 WBV vs C, Outcome 2 Balance, degrees of displacement, lower is best.

Comparison 1 WBV vs C, Outcome 3 Withdrawal.

Comparison 2 WBV + MX vs C, Outcome 1 WBV + MX vs C: HRQL, 0‐100 scale, lower is best.
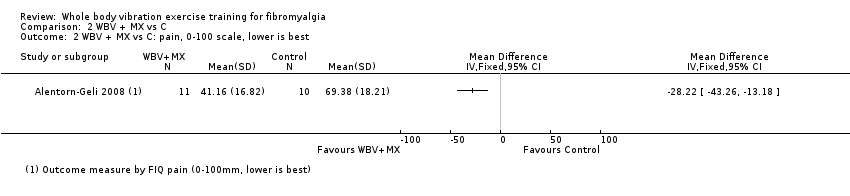
Comparison 2 WBV + MX vs C, Outcome 2 WBV + MX vs C: pain, 0‐100 scale, lower is best.
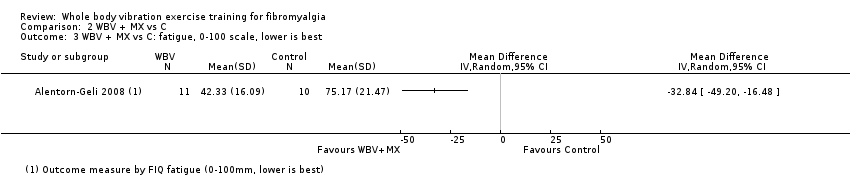
Comparison 2 WBV + MX vs C, Outcome 3 WBV + MX vs C: fatigue, 0‐100 scale, lower is best.

Comparison 2 WBV + MX vs C, Outcome 4 WBV + MX vs C: stiffness, 0‐100 scale, lower is best.

Comparison 2 WBV + MX vs C, Outcome 5 WBV + MX vs C: balance, overall stability index ‐ eyes closed (degrees of displacement 0 to 20 scale, lower is best).

Comparison 2 WBV + MX vs C, Outcome 6 Withdrawal.

Comparison 3 WBV + MX vs Other, Outcome 1 WBV + MX vs Other: HRQL, 0‐100 scale, lower is best.

Comparison 3 WBV + MX vs Other, Outcome 2 WBV + MX vs Other: pain, 0‐100 scale, lower is best.

Comparison 3 WBV + MX vs Other, Outcome 3 WBV + MX vs Other: fatigue, 0‐100 scale, lower is best.

Comparison 3 WBV + MX vs Other, Outcome 4 WBV + MX vs Other: stiffness, 0‐100 scale, lower is best.

Comparison 3 WBV + MX vs Other, Outcome 5 WBV + MX vs Other: strength, measured in newtons and number of reps, higher values are best.
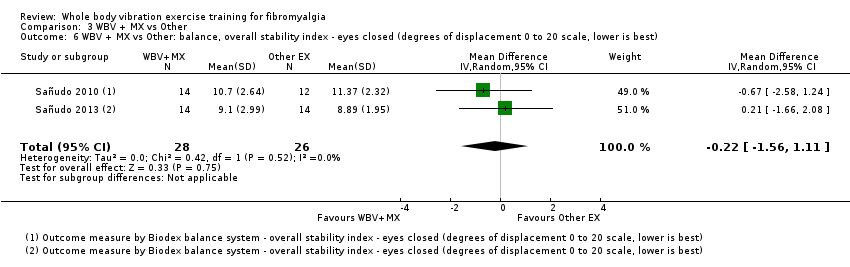
Comparison 3 WBV + MX vs Other, Outcome 6 WBV + MX vs Other: balance, overall stability index ‐ eyes closed (degrees of displacement 0 to 20 scale, lower is best).
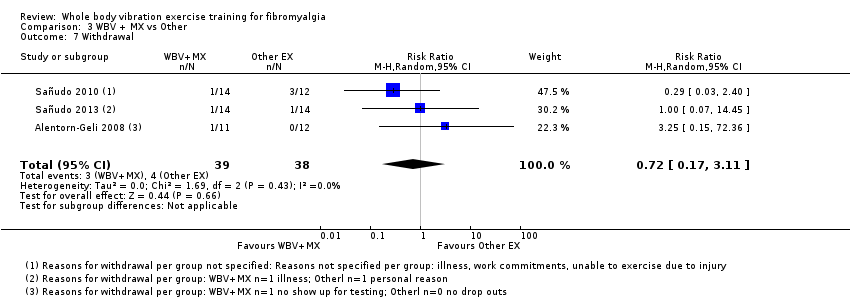
Comparison 3 WBV + MX vs Other, Outcome 7 Withdrawal.
| Whole body vibration versus control | ||||||
| Patient or population: individuals with fibromyalgia | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No. of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with WBV | |||||
| Health‐related quality of life Follow‐up: 12 weeks | Mean health‐related quality of life was 59 points | Mean health‐related quality of life in intervention group was 3.73 points lower (10.81 lower to 3.35 higher) at post‐test than in control group | ‐ | 41 | ♁◯◯◯ | Absolute improvement: 4% (95% CI 11% better to 3% worse) Relative change: 6.7% improvement (95% CI 19.6% improvement to 6.1% worse) NNTB: n/ac |
| Pain intensity | Not measured | Not measured | ‐ | Not measured | Not measured | Not measured |
| Fatigue | Not measured | Not measured | ‐ | Not measured | Not measured | Not measured |
| Stiffness | Not measured | Not measured | ‐ | Not measured | Not measured | Not measured |
| Physical function | Not measured | Not measured | ‐ | Not measured | Not measured | Not measured |
| Adverse events | Gusi 2010: "The program was reasonably safe: only 5% of the participants (n = 1) dropped out of the program because of acute pain in the legs. The program was completed by 85% of the participants, without secondary adverse effects" (page 1076; 1 study) | |||||
| All‐cause withdrawal | Study population | RR 1.43 (0.27 to 7.67) | 41 | ♁◯◯◯ | Absolute risk difference: 4% more events (95% CI 16% fewer to 24% more) Relative change: 43% more (73% fewer to 667% more) NNTH: n/ac | |
| 10 per 100 (2 of 20) | 14 per 100 (3 of 21) | |||||
| *Risk in the intervention group (and its 95% confidence interval) is based on assumed risk in the comparison group and relative effect of the intervention (and its 95% CI) | ||||||
| GRADE Working Group grades of evidence | ||||||
| aImpresicion: number of participants lower than 400 rule of thumb; wide confidence interval (downgraded twice) bHigh risk of biases including detection, performance, and reporting biases cNumber needed to treat for an additional beneficial outcome (NNTB) or number needed to treat for an additional harmful outcome (NNTH) not applicable (n/a) when result is not statistically significant. NNT for dichotomous outcomes calculated with Cates NNT calculator (http://www.nntonline.net/visualrx/). NNT for continuous outcomes calculated with Wells calculator (CMSG Editorial Office) | ||||||
| Whole body vibration plus mixed exercise versus control | ||||||
| Patient or population: individuals with fibromyalgia | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No. of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with WBV + MX | |||||
| Health‐related quality of life | Mean health‐related quality of life was 59.64 points at the end of the study | Mean health‐related quality of life in the intervention group was 16.02 points lower (31.57 lower to 0.47 lower) at post‐test than in the control group | ‐ | 21 | ♁◯◯◯ | Absolute difference: 16% improvement (95% CI 32% to 0.5% improvement). Relative change: 24% (47% to 0.7%)c NNTBd: 3 (2 to 237) |
| Pain Intensity | Mean pain intensity was 69.38 mm in the control group at the end of the study | Mean pain Intensity in the intervention group was 28.22 mm lower (43.26 lower to 13.18 lower) at post‐test than in the control group | ‐ | 21 | ♁◯◯◯ | Absolute difference: 28% (95% CI 43% to 13%). Relative difference: 39% (95% CI 18% to 60%) NNTBd: 2 (1 to 4) |
| Fatigue | Mean fatigue was 75.17 mm at the end of the study | Mean fatigue in the intervention group was 32.84 mm lower (49.2 lower to 16.48 lower) at post‐test than in the control group | ‐ | 21 | ♁◯◯◯ | Absolute difference: 33% (95% CI 49% to 16%). Relative difference: 47% (95% CI 23% to 70%) NNTBd: 2 (1 to 4) |
| Stiffness | Mean stiffness was 68.71 mm at the end of the study | Mean stiffness in the intervention group was 26.27 mm lower (42.96 lower to 9.58 lower) at post‐test than in the control group | ‐ | 21 | ♁◯◯◯ | Absolute difference 26% (95% CI 43% to 10%). Relative difference: 36.5% (95% CI 60% to 23%) NNTBd: 2 (1 to 6) |
| Physical function | Not measured | Not measured | ‐ | Not measured | Not measured | Not measured |
| Adverse events (narrative) | Alentorn‐Geli 2008: "This program neither exacerbated FM‐related symptoms nor resulted in musculoskeletal injuries; however, 1 patient exhibited a mild anxiety attack on the first session of WBV" (page 978) Sañudo 2013: "This study, however, demonstrated that WBV training is safe (no adverse events)..." (page 683) | |||||
| All‐cause withdrawal | 33 per 100 (7 of 21) | 8 per 100 | RR 0.25, 95% CI 0.06 to 1.12 | 46 | ♁◯◯◯ | Absolute risk difference: 24% (95% CI 3 to 51) NNTHd: n/a |
| *Risk in the intervention group (and its 95% confidence interval) is based on assumed risk in the comparison group and relative effect of the intervention (and its 95% CI) | ||||||
| GRADE Working Group grades of evidence | ||||||
| aImprecision: Number of participants lower than 400 rule of thumb; wide confidence interval. Need for more studies with more participants to reach optimal information size (downgraded twice) bHigh risk of biases including reporting and selection biases. Need for methodologically better designed and executed studies cBaseline control group mean (SD) = 67 (15.81), n = 10 dNumber needed to treat for an additional beneficial outcome (NNTB) or number needed to treat for an additional harmful outcome (NNTH) not applicable (n/a) when result is not statistically significant. NNT for dichotomous outcomes calculated with Cates NNT calculator (http://www.nntonline.net/visualrx/). NNT for continuous outcomes calculated with Wells calculator (CMSG Editorial Office) | ||||||
| Term | Definition |
| Allodynia | Pain resulting from a stimulus that would not normally provoke pain |
| Amplitude | Absolute value of maximum displacement from a zero value during 1 period of an oscillation |
| Damping | Energy dissipation properties of a material or system under cyclic stress |
| Endurance | Two forms of endurance that refer to health‐related physical fitness include cardiorespiratory endurance (also known as cardiovascular endurance, aerobic fitness, aerobic endurance, exercise tolerance), which "relates to the ability of the circulatory and respiratory systems to supply fuel during sustained physical activity and to eliminate waste products after supplying fuel," and muscle endurance, which "relates to the ability of muscle groups to exert external force for many repetitions" (Caspersen 1985) |
| Frequency | Number of cycles or completed alternations per unit time of a wave or oscillation |
| Hertz | One hertz is 1 cycle per second; therefore, when an individual is exposed to a vibration of 30 Hz, targeted muscles receive 30 cycles of vibration per second, which makes muscles contract and relax 30 times in the same period |
| Hyperalgesia | Increased pain from a stimulus that normally provokes pain |
| Natural frequency | Frequency at which a system oscillates when not subjected to continuous or repeated external forces |
| Paresthesia | Abnormal sensation that is spontaneous or is evoked by a stimulus (eg, numbness) |
| Phase angle | Particular stage or point of advancement in a cycle; fractional part of the period through which time has advanced, measured from some arbitrary origin often expressed as an angle (phase angle); the entire period being taken is 360° |
| Abbreviation | Description |
| A | amplitude |
| ACR | American College of Rheumatology |
| ACSM | American College of Sports Medicine |
| AE | aerobic exercise |
| EMG | electromyography |
| f | frequency |
| FIQ | Fibromyalgia Impact Questionnaire |
| FX | flexibility |
| g | gravitational load (G‐force) = 1 cm/s2 |
| HR | heart rate |
| HRQL | health‐related quality of life |
| hz | Hertz |
| ITT | intention‐to‐treat |
| kg | kilogram |
| m/s2 | unit of acceleration: 1 Gal = 0.01 m/s2 |
| MCID | minimal clinically important difference |
| MD | mean difference |
| MX | mixed intervention (includes more than 1 mode of physical activity) |
| n | number of studies |
| N | number of individuals |
| RD | risk difference |
| Relax | relaxation |
| RT | resistance training |
| s | seconds |
| SD | standard deviation |
| SE | standard error |
| SMD | standardized mean difference |
| sTNFR1 and sTNFR2 | soluble tumor necrosis factor receptor 1 and 2 |
| VAS | visual analogue scale |
| WBV | whole body vibration |
| wk | week(s) |
| WU | warm‐up |
| Vibration + Mixed vs Mixed + Placebo vs Control | |||||||||
| Author, year | Intervention | Frequency (times per week | length in weeks) | Total duration | Supervised or home program | Aerobic component | Resistance component | Flexibility Component | Other | |
| I (intensity): ACSM classification and physiological measure; M (mode): mode of exercise; T (time): duration of aerobic component in minutes | M (muscle groups, joints or areas of body); I (intensity resistance, repetitions, sets); T (type), T (time) | M (muscle groups, joints or areas of body); T (type of stretch, repetition, set), T (time) | |||||||
| AE + FX + Relax | 2 times/wk | 6 weeks | 90’ | Not specified | I: moderate to vigorous (65%‐85% HR max), T: primarily level ground walking with games and dance, T: 30' | Not applicable | M: 5 whole body stretches involving lower and upper limbs, neck, back; T: dynamic, 5 reps held for 30 s with 30 s rests, T: 25' | Relaxation | |
| Vibration + Mixed vs Mixed | |||||||||
| AE + RT + FX | 2 times/wk | 6 weeks | 60’ | Supervised | I: light to moderate (50%‐69% HR max), M: not specified, T: 4‐6 intervals of 2‐3’, 1‐2’ rest between intervals | M: major muscle groups, I: 8 exercises, 1 × 8‐10 reps with 1‐3 kg, T: not specified | M: not specified, I: 1x 3 reps holding for 30s, T: not specified | ||
| AE + RT + FX | 2 times/wk | 8 weeks | 45‐60’ | Supervised | I: moderate (65%‐70% HR max), M: not specified, T: 10‐15’ | M: deltoids, biceps, neck, hips, back, and chest, I: 1 set of 8‐10 reps for 8 different muscle groups against 1‐3 kg, T: 15‐20’ | M: deltoids, biceps, neck, hips, back, and chest I: 1 set of 3 reps for 8‐9 different ex, maintained for 30 s, T: 10’ | ||
| Study name/year | Name of device | Vibration frequency and amplitude | Position of participant | Stabilizing support | Footwear | Static/Dynamic; unilateral/bilateral |
| PowerPlate (PowerPlate International B.V., Badhoevendorp, The Netherlands) | 30 Hz; 2 mm vertical amplitude | The following 6 exercises were performed for 30 s each during whole body vibration (WBV) and were repeated 6 times with recovery of 3 minutes between repetitions (a) static squat at 100° of knee flexion (b) dynamic squat between 90° and 130° of knee flexion (c) maintained ankle plantar‐flexion with legs in extension (d) flexion‐extension of right leg between 100° and 130° of knee flexion (e) flexion‐extension of left leg between 100° and 130° of knee flexion (f) squat at 100° of knee flexion shifting body weight from 1 leg to the other For adaptation purposes, only tasks (a), (b), and (c) (repeated 3 times) were performed during first 2 sessions | Yes ‐ for all tasks, individuals held onto the supporting bar | Does not state | Static bilateral | |
| Galileo Fitness Platform (Novotec Medical, Pforzheim, Germany) | 12.5 Hz; 3 mm vertical amplitude | Participants alternated between 2 stances for each repetition Stance A: feet perpendicular to midline axis of the platform with right foot placed slightly ahead of left foot. Toes of right foot and heel of left foot lifted 4 mm above surface of the platform. Knees bent to 45° angle. Back and head kept straight Stance B: as per Stance A, except with left foot placed slightly ahead of right foot | Not reported and not pictured in Figure 2 | Balance testing was performed barefoot. Does not specify that exercise was done barefoot, but Figure 2 indicates this | Static and dynamic both unilateral and bilateral | |
| Galileo Fitness Platform (Novotec Medical, Pforzheim, Germany) | 20 Hz; variable amplitude of 2‐3 mm | Three sets of 45 s of bilateral static squat with 120 s recovery between sets (amplitude = 3 mm) followed by 4 sets of 15 s of unilateral static squat on each leg (amplitude = 2 mm). During WBV, participants stood with both knees in 120° isometric knee flexion (half‐squatting position) as measured by a goniometer | Does not state | Does not state | Static unilateral and bilateral | |
| PowerPlate, North America Inc., Northbrook, IL, United States | 30 Hz; vertical displacement of 4 mm (71.1 m/s‐2 ≈ 7.2 g) | Standing on the platform, with knees in 120º isometric knee flexion (measured by a goniometer) and trunk upright Bilateral static squat: 6 sets of 30 s, with 45‐s recovery between sets Unilateral static squat: 4 sets of 30 s each leg | Does not state | All participants wore sport shoes for vibration exercises | Static unilateral and bilateral |
| Quality assessment | No. of participants | Quality | Importance | |||||||
| No. of studies | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | Aerobic exercise (AE) intervention | AE control | ||
| Health‐related quality of life (HRQL), 0‐100, lower is best | ||||||||||
| 2 | Randomized trial | Very serious1 | Not serious | Not serious | Serious2 | 23 | 26 | ⊕⊝⊝⊝ | CRITICAL | |
| Pain intensity, 0‐100, lower is best | ||||||||||
| 1 | Randomized trial | Serious3 | Not serious | Not serious | Serious2 | One very small study | 11 | 12 | ⊕⊝⊝⊝ | CRITICAL |
| Fatigue, 0‐100, lower is best | ||||||||||
| 1 | Randomized trial | Serious1 | Not serious | Not serious | Serious2 | One very small study | 11 | 12 | ⊕⊝⊝⊝ | IMPORTANT |
| Stiffness, 0‐100, lower is best | ||||||||||
| 1 | Randomized trial | Serious1 | Not serious | Not serious | Serious2 | One very small study | 11 | 12 | ⊕⊝⊝⊝ | IMPORTANT |
| Physical function, not reported | ||||||||||
| Withdrawals | ||||||||||
| 3 | Randomized trial | Very serious4 | Not serious | Not serious | Serious2 | 3/39 (7.69%) | 4/38 (10.52%) | ⊕⊝⊝⊝ | IMPORTANT | |
| Adverse events:Alentorn‐Geli 2008: "This program neither exacerbated FM‐related symptoms nor resulted in musculoskeletal injuries; however, one patient exhibited a mild anxiety attack on the first session of WBV" (page 978); Sañudo 2010: Trial authors clarified that one person in the comparison group ("other exercise group") dropped out owing to an injury that was not an injury related to the program (participant fell down on the street); Sañudo 2013: "This study, however, demonstrated that WBV training is a safe (no adverse effects), suitable (no dropouts due to the intervention), and effective (increased lower limb muscle strength) way to exercise the musculoskeletal system, and potentially a feasible intervention for those patients who cannot participate in conventional strength training" (page 683) | ||||||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 HRQL, 1‐100 scale, lower means better HRQL Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Balance, degrees of displacement, lower is best Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 Withdrawal Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 WBV + MX vs C: HRQL, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2 WBV + MX vs C: pain, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 WBV + MX vs C: fatigue, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4 WBV + MX vs C: stiffness, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5 WBV + MX vs C: balance, overall stability index ‐ eyes closed (degrees of displacement 0 to 20 scale, lower is best) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6 Withdrawal Show forest plot | 2 | 46 | Risk Ratio (M‐H, Random, 95% CI) | 0.25 [0.06, 1.12] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 WBV + MX vs Other: HRQL, 0‐100 scale, lower is best Show forest plot | 2 | 49 | Mean Difference (IV, Random, 95% CI) | ‐6.67 [‐14.65, 1.31] |
| 2 WBV + MX vs Other: pain, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3 WBV + MX vs Other: fatigue, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4 WBV + MX vs Other: stiffness, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5 WBV + MX vs Other: strength, measured in newtons and number of reps, higher values are best Show forest plot | 2 | 54 | Std. Mean Difference (IV, Random, 95% CI) | 0.77 [0.20, 1.35] |
| 6 WBV + MX vs Other: balance, overall stability index ‐ eyes closed (degrees of displacement 0 to 20 scale, lower is best) Show forest plot | 2 | 54 | Mean Difference (IV, Random, 95% CI) | ‐0.22 [‐1.56, 1.11] |
| 7 Withdrawal Show forest plot | 3 | 77 | Risk Ratio (M‐H, Random, 95% CI) | 0.72 [0.17, 3.11] |