اعمال مداخلات هدفمند از طریق رسانههای ارتباط جمعی در جهت ارتقای رفتارهای سالم به منظور کاهش خطر ابتلا به بیماریهای غیر‐واگیردار در بزرگسالان، اقلیتهای قومی
Referencias
منابع مطالعات واردشده در این مرور
منابع مطالعات خارجشده از این مرور
منابع اضافی
منابع دیگر نسخههای منتشرشده این مرور
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Ir a:
| Methods | Study design: cluster‐randomised trial. 14 communities (from 35,600 to 630,000 inhabitants), matched in pairs before randomisation Year of study: 1994‐1995 Intervention period: baseline data collected the year preceding the intervention. Continuous data collection for 15 months. 2 waves of paid advertisements running 6 weeks and 4 weeks in the intervention communities, with some activities (public service announcements (PSAs) and community outreach) throughout the whole period Follow‐up period (postintervention): data collection ended 2 months after last wave of paid advertisement | |
| Participants | Country: USA (communities in 4 US regions) Language: English Target population: adult African American smokers Exposure population: broad population exposure in the intervention communities through mass media exposure. Proportion of African American residents ranged from 17% to 42% in the study communities. Estimated number of African American smokers in intervention communities was N = 310,471 and in control communities, N = 331,360. Socioeconomic profile of the communities not reported | |
| Interventions | Study objective/aim: to evaluate whether a targeted communications campaign would lead more adult African Americans to call the CIS for smoking cessation resources Control: no intervention Intervention: 10 weeks of paid advisements aired in 2 waves of 6 and 4 weeks (in total 3364 radio and 208 television advertisements) in the intervention communities. Attempts were made to use the advertisements as PSAs (media advertisements in the public interest aired free of charge) particularly during times when interest in smoking cessation was expected (i.e. New Year holiday). Outreach packets containing a 12 min video, posters, and flyers (all mass media components) distributed to the target population (1449 packets distributed). Content of the mass media message: encourage smokers to call the CIS for help to quit smoking; emphasis that the CIS service is free of charge Media channel(s) of dissemination: radio, television, video, posters, and flyers Theoretical basis: no theories specifically mentioned Targeting approach: 6 radio and 1 television advertisements developed using programming formats, language and music adapted to the target population. Messages and advertisements were developed through 3 steps: review of past research on unique quitting motives and barriers in target group; focus groups with target population and 40 individual interviews to identify barriers and facilitators for calling the CIS for help to quit smoking; and pre‐test of intervention material in (new) focus groups with target population and feedback from health communication specialists. Radio and television stations with high African American listenership/viewership identified for placement of advertisements. Outreach packets distributed to leaders and contact persons in community organisations, churches, and social groups in African American communities. | |
| Outcomes | Use of health promotion services: calls to the CIS for smoking cessation information and materials by African American adults residing in the intervention and control communities Intervention costs: partial description Adverse outcomes: none reported | |
| Notes | Intervention fidelity: the delivery of the intervention assessed through media "target rating points". Range of estimated reach among African Americans in the seven intervention communities 88.0%‐95.5%; with the target audience hearing or seeing an advertisement at estimated frequency of 7.02‐12.60 times in the study communities. Sources of funding: the National Cancer Institute (USA), the Robert Wood Johnson Foundation | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation sequence adequately generated | Unclear risk | Allocation method not presented |
| Allocation adequately concealed | Low risk | All clusters randomised at once |
| Baseline outcome measurements similar | Unclear risk | Not presented |
| Baseline characteristics similar | Unclear risk | Not presented. Communities matched in pairs based on number and proportion of population that was African American, income, sex, age, education, population proportion below the poverty line, and proportion of dwellings with telephones |
| Incomplete outcome data adequately addressed | Low risk | This was a population study using routinely collected call data |
| Knowledge of allocated interventions prevented | Unclear risk | Neither participants nor outcome assessors blinded to allocation |
| Adequately protected against contamination | Low risk | Geographically spread communities and non‐overlapping media markets |
| Free of selective outcome reporting | Low risk | Selctive reporting not likely; only few relevant outcomes |
| Other bias | Low risk | Judged low risk, but noted that both the study and the quit line services were funded by the National Cancer Institute. |
| Methods | Study design: RCT Year of study: not stated Intervention period: 12 weeks Follow‐up period (postintervention): immediately postintervention (relevant data at 6 and 12 month follow‐up not published) | |
| Participants | Country: USA (San Diego, CA) Language: Spanish Target population: Spanish‐speaking Latino immigrants or Latino American Inclusion criteria: women aged 18‐65 years living in a Spanish‐language dominant household Exclusion criteria: pregnant, on special diet for medical reasons, or planning to leave the area during the study period Participants: intervention 1, N = 119; intervention 2, N = 118; intervention 3, N = 120 Sex: women Socioeconomic characteristics: 95% born in Mexico, 27% with little or no formal education, 27% with some college education, > 50% homemakers, 25% working full‐time. Wide range of family income, 13% with USD 500–USD 1000 per month, 25% with > USD 2501 per month. Low acculturation score. Described by authors as women with low levels of acculturation, income, and education. Other: mean BMI 29.6 kg/m2 ± 5.6 | |
| Interventions | Study objective/aim: to assess the effect of person‐tailored nutrition education materials, with or without personal delivery and counselling from lay health advisor(promotora), compared to off‐the‐shelf materials targeted to a Latino population Intervention 1 (study control): targeted mass media intervention The women received 12 weekly Spanish‐language newsletters mailed to the participant's home. These were based on brochures containing information on food purchasing, food preparation, and food consumption from the American Heart Association, American Dietetic Association and the American Cancer Society (off‐the‐shelf materials targeted to a Latino population). Intervention 2: individually‐tailored newsletters The women received 12 weekly individually tailored newsletters and activity inserts mailed to the participant's home. The newsletters were tailored by using the participants' baseline data. They provided feedback on the assessment process, opportunity for personalised goal setting and for dealing with identified barriers. Intervention 3: individually‐tailored newsletters + home visits The women received individually tailored newsletters as for intervention 2 and in addition weekly home visits or telephone calls from promotoras over the 12‐week period. Content of the mass media message: behavioural strategies to reduce dietary fat and to increase fibre, fruit and vegetable intake Media channel(s) of dissemination: newsletters Theoretical basis: none stated for the targeted mass media intervention Targeting approach: material presented in participants' first language (Spanish). Some cultural adaptation of targeted print condition may be assumed (off‐the‐shelf materials targeted to a Latino population by national health organisations), but is not described by authors. Recruitment of Spanish‐speaking Latino participants only | |
| Outcomes | Self‐reported behavioural change: energy % calories from fat, dietary fibre intake (g) Intervention costs: partial description Adverse outcomes: none reported | |
| Notes | Intervention fidelity: not reported Sources of funding: the National Cancer institute (USA) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation sequence adequately generated | Unclear risk | Block randomisation. Allocation method otherwise not presented |
| Allocation adequately concealed | Low risk | Participants agreed to participate before randomisation. |
| Baseline outcome measurements similar | Low risk | Analyses adjusted for baseline values |
| Baseline characteristics similar | Low risk | Analyses adjusted for baseline values |
| Incomplete outcome data adequately addressed | Low risk | Missing data imputed with baseline values |
| Knowledge of allocated interventions prevented | High risk | Unclear risk for the BMI measurements. High risk for self‐reported behaviours in non‐blinded study |
| Adequately protected against contamination | Low risk | Primary intervention material delivered by mail |
| Free of selective outcome reporting | Low risk | Width of data presented in 3 papers |
| Other bias | Low risk | None considered |
| Methods | Study design: cluster‐RCT. ˜15 participants recruited by each of 58 lay health workers (LHW). LHW‐groups randomised Year of study: August 2010‐September 2013. Intervention period: 2 months Follow‐up period (postintervention): assessment at 6 months (4 months postintervention) | |
| Participants | Country: USA (San Francisco, CA) Language: Chinese Target population: Chinese American immigrants Inclusion criteria: self‐identifying as Chinese immigrants (foreign born) or Chinese American; aged 50‐75 years; Cantonese, Mandarin or English speaker; intending to stay in area > 6 months Exclusion criteria: other participants in household, personal history of colorectal cancer (focus of parallel RCT) Participants: intervention 1, N = 360; intervention 2, N = 365 Sex: both, 83% women in intervention group 1, 79% women in intervention group 2 Socioeconomic characteristics: mean 17 years in the US, ˜70% with less education than high school diploma, ˜96% self‐reported spoken English proficiency as 'so‐so', 'poor', or 'not at all'. Wide range of family income Other: mean BMI 24.2 kg/m2 ± 3.4 in intervention group 1; 23.3 kg/m2± 4.0 in intervention group 2 | |
| Interventions | Study objective/aim: to evaluate the efficacy of an in‐language intervention of 2 lectures plus printed materials versus printed materials alone on knowledge and adherence to nutrition and physical activity guidelines among older Chinese Americans Intervention 1 (study control): targeted mass media intervention Participants received the printed lecture handouts made for intervention group 2 that focused on culturally appropriate examples of food and physical activity and a Chinese nutrition brochure. Lay health workers (LHW) delivered 2 small group education sessions with follow‐up calls on colorectal cancer (control component). Intervention 2: lectures and targeted mass media intervention Participants received two 60‐90 min lectures, printed lecture handouts and a nutrition brochure about 2 months apart, delivered by an instructor. LHW called about 1 month after each lecture to ask them recall the lecture and remind to attend the next lecture or final assessment. Content of the mass media message: basic nutrition and physical activity education, with focus on recommended daily 5 servings of vegetables and 4 servings of fruit, and ≥ 150 min moderate intensity physical activity weekly Media channel(s) of dissemination: printed information material Theoretical basis: none stated Targeting approach: the lectures were presented in the participants' preferred language (Cantonese, Mandarin, or English). Lectures and material were developed with culturally appropriate examples of common foods, relevant physical activities and familiar portion size models for target group. A community advisory board reviewed the material for cultural and linguistic appropriateness, with subsequent testing in focus groups. | |
| Outcomes | Self‐reported behavioural change: self‐reported behaviour meeting guidelines for ≥ 5 servings of vegetables/day, ≥ 5 servings of fruit/day, ≥ 150 minutes moderate physical activity/week Knowledge or attitudes to change: self‐reported knowledge of recommended ≥ 5 servings of vegetables/day, ≥ 5 servings of fruit/day, ≥ 150 minutes moderate physical activity/week Adverse outcomes: none reported | |
| Notes | Intervention fidelity: not reported Sources of funding: National Institutes of Health, the National Cancer institute (USA) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation sequence adequately generated | Low risk | Computer‐generated randomisation |
| Allocation adequately concealed | Low risk | LHW‐groups randomised in blocks. Allocation concealed until LHW had recruited all his/her participants |
| Baseline outcome measurements similar | Low risk | Baseline outcome measurement presented without statistical tests; appears balanced |
| Baseline characteristics similar | Low risk | Baseline characteristics presented with statistical tests. Balances apart from small difference in baseline BMI between groups; adjusted in final analysis |
| Incomplete outcome data adequately addressed | Low risk | Small attrition overall, < 1% of sample. 6.5% had missing data for 1 or more covariates |
| Knowledge of allocated interventions prevented | High risk | Self‐reported behavioural change and knowledge in non‐blinded study |
| Adequately protected against contamination | Unclear risk | No discussion of possible contact between participants in different groups |
| Free of selective outcome reporting | Low risk | Few relevant outcome measures; all reported |
| Other bias | Low risk | Analyses adjusted for clustering |
| Methods | Study design: interrupted time series study (as re‐analysed for this systematic review) Year of study: 2009‐2011 Intervention period: continuous data collection from March 2009 to June 2011. 2 waves of campaign activities, June‐October 2009 and January‐March 2011 Follow‐up period (postintervention): see intervention period | |
| Participants | Country: USA (Richmond, VA) Language: English Target population: pregnant African American smokers Exposure population: full population exposure through media exposure in a city (approximately 200,000 inhabitants). Total target population not known. Approximately 400 births by African American women per month. Interviews indicated that ˜40% of pregnant African American women had smoked the past 3 months. Socioeconomic profile of area not reported | |
| Interventions | Study objective/aim: to evaluate the effect of a social marketing campaign aiming to encourage pregnant African American smokers to call telephone counselling Control (pre‐campaign): no intervention Intervention: 3.5 months of paid radio advisements, billboards and bus ads, with estimated 17 million of impressions (i.e. opportunities to hear the campaign messages). In addition, the campaign consisted of other small media, social media content, press coverage, and distribution of campaign‐branded items (tins of mint, lip balm). Outreach workers and frontline clinic and social service agency staff distributed campaign material and reinforced message. A second wave of advertisements starting at New Year 1.5 years after baseline were not re‐analysed for this systematic review. Content of the mass media message: 'One tiny reason to quit' – message from the baby. Encourage pregnant women to quit smoking and make use of free telephone smoking cessation counselling Media channel(s) of dissemination: radio, billboards, bus ads, newspaper ads, Facebook page, press coverage, and campaign‐branded items Theoretical basis: no theories specifically mentioned for development of intervention content, message, or framing. Positive framing chosen based on previous experiences Targeting approach: message concepts were tested for appropriateness and appeal with pregnant African American current and recent smokers, with additional audience testing of creative material. Creative material featuring African American baby. Outreach workers from the African American community were trained to approach pregnant workers with campaign messages and distribute campaign material. Radio ads in the contemporary radio station most popular with young African American adults according to ratings. Billboards in relevant neighbourhoods. Newspaper ads in African American weekly papers | |
| Outcomes | Use of health promotion services: all calls to telephone smoking cessation counselling by adults between 18‐45 years in counties in the local broadcast range of the radio station that ran the advertisements Adverse outcomes: none reported | |
| Notes | Intervention fidelity: not reported Sources of funding: National Center on Minority Health Dispartities, National Institues of Health (USA) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Intervention independent (ITS) | Low risk | The second wave of advertisements started at New Year, and thus influenced by the normal increase in calls to quit lines at this time of year. This second wave is not included in the re‐analysed material. |
| Analysed appropriately (ITS) | Low risk | Data re‐analysed for this systematic review according to standards (see Methods section) |
| Shape of effect pre‐specified (ITS) | Low risk | Data re‐analysed for this systematic review according to standards (see Methods section) |
| Unlikely to affect data collection (ITS) | Low risk | Study based on routinely collected call data |
| Blinding of outcome assessment (ITS) | Unclear risk | Unclear if assessors were aware of campaign |
| Incomplete outcome data addressed (ITS) | Low risk | Not relevant |
| Free of selective reporting (ITS) | Low risk | Selctive reporting not likely; only a few relevant outcomes from routinely collected call data |
| Other biases (ITS) | Low risk | No other biases identified |
| Methods | Study design: RCT Year of study: not reported Intervention period: participants had access to 12 weekly cable TV shows and 4 months follow‐up intervention Follow‐up period (postintervention): assessment at 3 months (end of TV shows), 8 months (end of follow‐up intervention) and 12 months (4 months postintervention) | |
| Participants | Country: USA (Massachusetts) Language: English Target population: African American women Inclusion criteria: self‐identified as African American or black women, aged 18–70 years, resided in catchment area of the cable TV company, planned to stay in area for ≥ 1 year, access to telephone, television and videocassette recorder (VCR), available to watch the TV programme at its airtime, BMI ≥ 22 kg/m2 Exclusion criteria: pregnant or < 4 months postpartum, physical problems that would prevent mild physical activity, previous history of treatment for eating disorders, unable to speak and read English, participation in other weight‐control research project Participants: control, N = 82; intervention 1, N = 71, Intervention 2, N = 210 (3 intervention arms combined) Sex: women Socioeconomic characteristics: all self‐described African American, black or West Indian/Caribbean ethnicity. 12% foreign‐born. 12% had not completed high school, 40% with college education. 44% in lowest income category. The study paid for cable TV service for participants who could not afford it (19% of participants) Other: 71% obese. Self‐reported hypertension > 25%, diabetes 12%, and on medication for hypertension or heart condition > 25%. | |
| Interventions | Study objective/aim: to evaluate the effectiveness of a culturally tailored weight control cable TV programme for black women Control: wait‐list/attention placebo comparison. Biweekly mailings for 12 weeks with other health‐related information. Received all the TV shows as videos and other intervention material after the 12‐month follow‐up (i.e. after final outcome assessment) Intervention 1: participants were given access to 12 one‐hour live programmes on cable TV and printed material corresponding to the shows biweekly by post. After the shows, participants received 4 monthly mailings with written material and booster videotapes including an exercise video. Intervention 2 (combination of 3 study arms): in addition to all intervention content described under intervention 1, participants received either access to a toll‐free number to call during a live sharing part of show; 12 weekly and 4 monthly telephone support calls from a community outreach educator; or both access to call the 'live' sharing and the 16 telephone support calls Content of the mass media message: educational content regarding nutrition and physical activity to improve health and weight control as defined by each woman. Practical cooking demonstration or physical activity breaks. 20 min of each show devoted to a live 'sharing' between social worker, featured guest, and live callers. Media channel(s) of dissemination: cable TV, print material, video Theoretical basis: intervention based on Social Action Theory. Behavioural change, stress reduction and self‐management principles integrated into nutrition and physical activity sections Targeting approach: designed to be culturally appropriate based on formative research with 500 people from the target population. All African American female cast in the TV shows, including all experts; recruited only target population | |
| Outcomes | Indicators of behavioural change: BMI (kg/m2), weight (kg) Self‐reported behavioural change: food habits questionnaire (fat behaviours), leisure activity score Adverse outcomes: none reported | |
| Notes | Intervention fidelity: random participants were called during shows to monitor who was watching. Calls to live sharing part and support calls logged. At 3 months follow‐up, 69% of participants had watched 7‐12 shows and 57% had read most or all written material. Participants in intervention 2 were more reluctant to call live than expected. < 50% of the planned support calls were completed. Sources of funding: the National Cancer Institute (USA) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation sequence adequately generated | Low risk | After baseline assessment, participants drew an envelope from a container with concealment of allocation. |
| Allocation adequately concealed | Low risk | After baseline assessment, participants drew an envelope from a container with concealment of allocation. |
| Baseline outcome measurements similar | Low risk | Baseline outcome measurements presented and analysed as balanced |
| Baseline characteristics similar | Low risk | Baseline characteristics presented and analysed as balanced |
| Incomplete outcome data adequately addressed | Low risk | ITT analyses conducted |
| Knowledge of allocated interventions prevented | High risk | Unclear risk for the BMI measurements. High risk for self‐reported behaviours in non‐blinded study |
| Adequately protected against contamination | Low risk | Participants reported to be geographically spread |
| Free of selective outcome reporting | Low risk | Results compared with published protocol |
| Other bias | Low risk | None considered |
| Methods | Study design: RCT Year of study: 2006‐2007 Intervention period: 1 mailing of print material Follow‐up period (postintervention): 3 months | |
| Participants | Country: USA (Florida) Language: English Target population: African American smokers Inclusion criteria: 18‐65 years old, smoked ≥ 5 cigarettes/day, had permanent mailing address, could read English, wanted to quit smoking within 1 year Exclusion criteria: currently receiving a quit smoking intervention Participants: intervention 1, N =127; intervention 2, N = 128. (The numbers in the participant flow diagram differs from numbers in text: participants randomised to intervention 1, N = 129; intervention 2, N =132). Sex: 56% women Socioeconomic characteristics: 99% African American (3 Hispanic participants), 61% single, 74% completed high school, 47% household income < USD 10,000. Other: mean age: 43 years; mean cigarettes/day: 23, mean years of smoking: 23 | |
| Interventions | Study objective/aim: to assess extent to which cultural specificity contributes to the efficacy of written self‐help materials among African American smokers Intervention 1 (control): 1‐2 days after baseline assessment, participants received a non‐culturally specific printed smoking cessation guide Intervention 2: 1‐2 days after baseline assessment, participants received a culturally specific printed smoking cessation guide Content of the mass media message: information about smoking and health, tobacco advertising, secondhand smoke, readiness to quit, quitting strategies, and community efforts Media channel(s) of dissemination: print material Theoretical basis, intervention 1: a non‐culturally specific smoking cessation guide was developed by replacing all culturally specific aspects of the Pathways to freedom smoking cessation guide, while keeping topics and smoking information unchanged. The aim was to create a booklet without attention to any particular ethnic or cultural group. Pictures were changed to cartoons or different ethnicities. Theoretical basis, intervention 2: the Pathways to freedom smoking cessation guide was an established culturally specific guide for African Americans (available from www.cdc.gov/tobacco/quit_smoking/how_to_quit/pathways/pdfs/pathways.pdf). Written at sixth‐grade reading level. Culturally specific elements related to African American values, communication patterns, familial roles, history, statistics specific to African Americans and mobilising the community to fight the tobacco industry. Pictures and testimonials from target group. Stereotypical African American names and colours. | |
| Outcomes | Self‐reported behavioural change: quit attempts, smoking reduction, 24‐hour point prevalence abstinence, 7‐day point prevalence abstinence Knowledge or attitudes to change: readiness to quit Adverse outcomes: none reported Reported outcomes not considered relevant for this review: content evaluation measures | |
| Notes | Intervention fidelity: not reported Sources of funding: Syracuse University (USA) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation sequence adequately generated | Unclear risk | Allocation method not presented |
| Allocation adequately concealed | Unclear risk | Not reported |
| Baseline outcome measurements similar | Low risk | There was no significant differences on demographics and smoking history |
| Baseline characteristics similar | Low risk | There was no significant differences on demographics and smoking history |
| Incomplete outcome data adequately addressed | Unclear risk | Demographics reported as similar in attrition groups, but ITT analyses not mentioned |
| Knowledge of allocated interventions prevented | Unclear risk | Self‐reported smoking behaviours in non‐blinded study, but assumed similar conditions in both groups. Blinding of assessors not presented |
| Adequately protected against contamination | Unclear risk | Not mentioned |
| Free of selective outcome reporting | Low risk | Main outcome (smoking habits) reported using several different measures |
| Other bias | Low risk | None considered |
BMI: body mass index; CIS: Cancer Information Service; ITT: intention‐to‐treat; LHW: lay health worker; PSA: public service announcement; RCT: randomised controlled trial.
Characteristics of excluded studies [ordered by study ID]
Ir a:
| Study | Reason for exclusion |
| Individually tailored text messages. No specific targeting to ethnic minorities | |
| Individual counselling available as part of the intervention. Not targeted to ethnic minority | |
| Not considered a mass media intervention | |
| Not considered a mass media intervention | |
| Before‐after assessment without control group | |
| Participants attended a group event before receiving the mass media component | |
| Individually tailored content. Unclear targeting to ethnic minority | |
| Campaign targeted to a patient group | |
| Individually tailored text messages based on initial counselling | |
| Protocol for a multi‐component store intervention. No relevant outcome measures | |
| Not considered a mass media intervention | |
| Retrospective analyses | |
| Intervention not clearly targeted to ethnic minorities | |
| Intervention focused on risk communication rather than disease prevention. Study not designed to show effect of a targeted approach | |
| Assessment of quit line calls from Latino compared to non‐Latino population before and after Spanish‐language campaign | |
| Individually tailored newsletters | |
| Repeated cross‐sectional surveys. No control group | |
| Experimental study of pictorial versus text‐only tobacco warning labels in different ethnic groups | |
| Personal invitation letters to re‐enrol into counselling. Not considered a mass media intervention | |
| The target population is adolescents, secondarily their parents. Not considered a mass media intervention | |
| Not considered a mass media intervention | |
| As Chang 2010 | |
| Not considered a mass media intervention | |
| Before‐after assessment without control group | |
| Individually tailored text messages | |
| Report on implementation and impact of tobacco quit line counselling services | |
| Results presented as repeated cross‐sectional surveys. Not relevant study design as analysed | |
| Individually tailored automatic telephone coach | |
| Individually tailored intervention components | |
| Individually tailored intervention components. Not targeted to ethnic minorities | |
| Not any of the specified study designs | |
| No impact assessment reported | |
| Multicomponent store intervention. Mass media components only minor part of intervention. No clear targeting to ethnic minorities | |
| Not considered a mass media intervention | |
| Individually tailored intervention components | |
| Multicomponent community intervention. Mass media components only minor part of intervention. No clear targeting to ethnic minorities | |
| Not considered a mass media intervention | |
| Not considered a mass media intervention | |
| Multicomponent store intervention. Mass media components only minor part of complex intervention | |
| Protocol. Not considered a mass media intervention. Before‐after assessment without control group | |
| Description of programme development and click‐through rates for different online advertisements | |
| Protocol. Not considered a mass media intervention | |
| Interrupted time series study with 2 data points before the intervention and 2 after | |
| Not considered a mass media intervention. Before‐after assessment without control group | |
| Description of programme development and user's opinion of campaign | |
| Individually tailored content. Patient education | |
| Protocol. Study does not evaluate the effect of the mass media component | |
| Community intervention with many intervention activities involving several institutions. Mass media component smaller part of complex intervention compared to no intervention | |
| Written information targeted to problem behaviours or life situations, not to ethnic minority characteristics | |
| Intervention not targeted to ethnic minorities. Not any of the specified study designs | |
| Individually tailored, interactive multimedia programme. Unclear targeting to ethnic minorities | |
| Content of intervention not identical in the 3 intervention sites | |
| Interactive education programme | |
| The whole population exposed to the mass media component (not described as targeted). Study designed to evaluate the effect of extended community outreach to ethnic minority group | |
| Controlled before‐after study with only 1 intervention site and 1 control site | |
| Individually tailored content through interaction and contact with project staff. Mass media component (in control group) not targeted to ethnic minorities | |
| Before‐after assessment with no control group | |
| Not considered a mass media intervention | |
| Text messages sent with a possibility to reply and receive answers | |
| Individually tailored women's magazines based on baseline questionnaire | |
| Individually tailored women's magazines based on baseline questionnaire | |
| Intervention not targeted to ethnic minorities. Individual feedback | |
| Individually tailored content and counselling. Before‐after without control group | |
| Community intervention study with many intervention activities on different levels. Time series data with 5 measurement points and gradual implementation of the intervention | |
| Mass media component (in control group) not targeted to ethnic minorities | |
| Non‐randomised controlled trial with 4 arms. 1 site each for 2 of the arms. Alternating 2 interventions every other week in a third site | |
| Before‐after assessment without control group | |
| Not considered a mass media intervention | |
| Description of programme and campaigns. No impact assessment | |
| Individually tailored content and counselling. Adapted to characteristics of college life, not ethnicity | |
| Individually tailored, interactive computer programme | |
| Interrupted time series study with 2 data points before the intervention and 2 after | |
| Interrupted time series study with 2 data points before the intervention and 1 after | |
| Non‐randomised controlled trial with 2 intervention sites and 1 control site | |
| Study of a culturally adapted self‐help smoking cessation programme delivered either as an interactive web‐programme or as booklets | |
| Community intervention with many intervention activities involving several institutions. Mass media component smaller part of complex intervention compared to no intervention | |
| Pilot study. Description of recruitment and data collection methods | |
| Nutrition education material tailored to individual shopping preferences in addition to cultural targeting | |
| Individually tailored, interactive automatic telephone counselling. Can be considered as patient education | |
| Not considered a mass media intervention | |
| Study of the effect of adding a mood management programme to a culturally adapted smoking cessation self‐help programme | |
| Describes 4 studies, including 2 RCTs. Smoking cessation programme with individual tailoring | |
| Not considered a mass media intervention | |
| Participants randomised to different formats of individual telephone counselling | |
| Not considered a mass media intervention | |
| Description of a research programme. No impact assessment data presented | |
| Individually tailored feedback delivered via Internet or print | |
| Not considered a mass media intervention | |
| Multicomponent community intervention. Mass media components only minor part of intervention. Not any of the specified study designs | |
| Not considered a mass media intervention | |
| Not considered a mass media intervention | |
| Not considered a mass media intervention | |
| Not considered a mass media intervention | |
| Not considered a mass media intervention | |
| Not considered a mass media intervention | |
| Individually tailored newsletters | |
| Mass media component (in control group) not targeted to ethnic minorities | |
| Before‐after assessment without control group | |
| Community intervention study with many intervention activities on different levels. Time series data with 5 measurement points and gradual implementation of the intervention | |
| Individually tailored, interactive computer programme with e‐mail feedback | |
| Not considered a mass media intervention | |
| Community intervention with many components and intervention activities, including social marketing campaigns. Whole population approach, including aboriginal communities. Not specific targeting to and impact assessment in ethnic minority groups. | |
| Description of programme and activities. No impact assessment | |
| Description of programme and activities. No impact assessment | |
| Not considered a mass media intervention | |
| Personal contact with research team through text‐messages and email | |
| Before‐after assessment without control group | |
| The main aim of the study was to reduce secondhand smoke exposure among children with asthma | |
| Individually tailored web‐based smoking cessation programme | |
| Before‐after assessment without control group | |
| Evaluation of intervention without control group | |
| Before‐after assessment without control group | |
| Experimental study of health risk communication with different message content and culturally specific framing | |
| Mass media used to create awareness of Spanish‐language smoking cessation services. Study of different formats of quit line counselling | |
| Individually tailored print material | |
| Study compares the number of calls to quit line services after different campaigns, including 1 designed for Māori audience. Not relevant study design | |
| Cluster‐randomised trial with 3 arms. Only 1 site per arm | |
| Individually tailored, interactive computer programme. Feasibility study without control group | |
| Controlled before‐after study with only 1 intervention site and 1 control site. Not targeted to ethnic minority | |
| Not considered a mass media intervention | |
| Individually tailored automated interactive voice response telephone counselling | |
| Not considered a mass media intervention |


Study flow diagram.

Approaches used in the included studies to target the intervention to the study population, by categories according to logic model.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
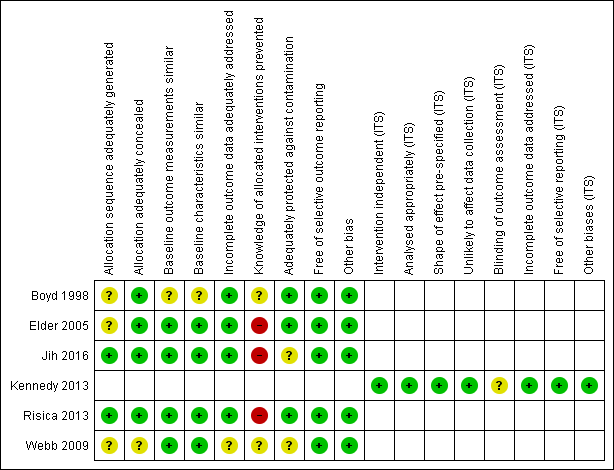
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
| Comparison 1: targeted mass media intervention versus general population mass media intervention for promoting healthy behaviours | ||||||
| Patient or population: adult, ethnic minority: self‐described Americans of African heritage | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | N of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| General population mass media intervention | Targeted mass media intervention | |||||
| Indicators of behavioural change | ||||||
| Any outcome considered an indicator of change | No study provided data for this outcome. | |||||
| Self‐reported behavioural change | ||||||
| Proportion smoking reduction, 3 months follow‐up | 94% | 95% | — | 255 | ⊕⊝⊝⊝ | No effect measures reported by authors. Not significantly different between groups |
| Quit‐attempts, 3 months follow‐up | — | — | Adjusted OR 1.97 (1.09 to 3.55) in favour of general population mass media intervention | 255 | ⊕⊝⊝⊝ | 24‐hour and 7‐day point prevalence abstinence not significantly different between groups |
| Knowledge and attitudes to change | ||||||
| Contemplation ladder to quit smoking (1‐10), 3 months follow‐up | Mean score: 8.2 (SD 2.4) | Mean score: 7.3 (SD 2.6) | — | 255 (1 RCT) | ⊕⊝⊝⊝ | Difference between group reported at P = 0.01 |
| Adverse effects | ||||||
| Any outcome considered an adverse effect | No study provided data for this outcome. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) | ||||||
| GRADE Working Group grades of evidence | ||||||
| aIn the GRADE assessments for the domain 'directness', we considered the studies directly relevant to the inclusion criteria. Thus, we have not downgraded on this domain. However, the population of interest will be dissimilar in different contexts, relating to characteristics of the ethnic minority group, the country and setting overall. The transferability of results must be considered for each context specifically. | ||||||
| Comparison 2: targeted mass media intervention for promoting healthy behaviours versus no intervention | ||||||
| Patient or population: adult, ethnic minority group: self‐described Americans of African heritage | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | N of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| No intervention | Targeted mass media intervention | |||||
| Indicators of behavioural change | ||||||
| BMI (kg/m2), 12 months from baseline | 34.4 (SD 8.5)b | Mean difference in change 0.1 (−0.4 to 0.6) | — | 154 | ⊕⊕⊝⊝ | Corresponding risk at 3 months: mean difference in change −0.4 (−0.7 to −0.02) |
| Self‐reported behavioural change | ||||||
| Changes in dietary composition, 12 months from baseline | Food habits questionnaire, score on fat behaviours (no scoring scale provided by study authors): 1.0 (SD 0.4) | Mean difference in change −0.2 (−0.3 to ‐0.1) | — | 154 (1 RCT) | ⊕⊝⊝⊝ | Corresponding risk at 3 months: mean difference in change −0.1 (−0.2 to −0.02) |
| Leisure time physical activity, 12 months from baseline | Physical activity score (no scoring scale provided by study authors): 60.0 (SD 47.0)e | Mean difference in change 12.0 (1.0 to 23.0) | — | 154 (1 RCT) | ⊕⊝⊝⊝ | Corresponding risk at 3 months: mean difference in change 10.0 (−1.7 to 21.8) |
| Knowledge and attitudes to change | ||||||
| Any measure of knowledge and attitude | No study provided data for this outcome. | |||||
| Adverse effects | ||||||
| Any outcome considered an adverse effect | No study provided data for this outcome. | |||||
| Use of health promotion services (secondary outcome) | ||||||
| Calls to smoking quit lines, during campaign | 18 calls per estimated 10,000 African American smokers in the intervention group versus 0.2 calls in the control communitiesf. | Estimated target population 641,800 (1 RCT) | ⊕⊕⊕⊝ | — | ||
| Calls to smoking quit lines, during and after campaign | Change from pre‐campaign, calls per month (95% CI) from new pregnant smokers: 8 (1 to 14) first month of campaign, 8 (1 to 14) last month of campaign, 6 (−1 to 12) first month after campaign, 3 (−4 to 10) 4 months after campaign | Population in target city ˜300,000 (1 ITS) | ⊕⊕⊝⊝ | — | ||
| Proportion of calls from target population during campaign | Proportion of calls from African Americans during trial: 82% in intervention and 26% in control communities | Estimated target population 641,800 (1 RCT) | ⊕⊕⊝⊝ | — | ||
| Proportion of calls from target population during and after campaign | Proportion African Americans among pregnant callers: 41% before campaign, 86% during the campaign, 28% after campaign | Population in target city ˜300,000 (1 ITS) | ⊕⊝⊝⊝ | — | ||
| Costs of the project (secondary outcome) | ||||||
| Programme costs | USD 106,821 for radio advertisements and USD 6744 for television advertisements. No overall costs reported | Estimated target population 641,800 (1 RCT) | ⊕⊕⊝⊝ | — | ||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aIn the GRADE assessments for the domain 'directness', we considered the studies directly relevant to the inclusion criteria. Thus, we have not downgraded on this domain. However, the population of interest will be dissimilar in different contexts, relating to characteristics of the ethnic minority group, the country and setting overall. The transferability of results must be considered for each context specifically. | ||||||
| Comparison 3: targeted mass media intervention versus targeted mass media intervention plus personalised content | ||||||
| Patient or population: adult, ethnic minority groups: Latino immigrants, elderly Chinese immigrants, self‐described Americans of African heritage | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | N of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Media intervention with personalised content (comparison) | Targeted mass media intervention | |||||
| Indicators of behavioural change | ||||||
| BMI (kg/m2), 12 months from baseline | 34.9 (SD 7.7)b | Mean difference in change 0.4 (−0.1 to 0.8) | — | 286 | ⊕⊕⊝⊝ | Two RCTs (643 participants) reported BMI at 3 months. None found significant differences in weight change between study groups |
| Self‐reported behavioural change | ||||||
| Intake meeting target from dietary guidelines, 3 months from baseline | Vegetables: adjusted OR 5.53d (1.96 to 15.58) Fruit: adjusted OR 1.77d (0.99 to 3.15) | 718 (1 RCT) | ⊕⊝⊝⊝ | — | ||
| Changes in dietary composition, 12 months from baseline | Food habits questionnaire, score on fat behaviours (no scoring scale provided by study authors): 1.0 (SD 0.4)f | Mean difference in change −0.1 (−0.2 to −0.02) | — | 286 | ⊕⊝⊝⊝ | Two RCTs (643 participants) reported changes in dietary composition at 3 months. None found significant differences/mean difference in change for energy or dietary fibre intake (study 1) or food habits questionnaire (fat behaviours) (study 2) |
| Weekly physical activity meeting target from guidelines, 3 months from baseline | Adjusted OR 1.27d (0.89 to 1.80) | 718 (1 RCT) | ⊕⊝⊝⊝ | — | ||
| Leisure time physical activity, 12 months from baseline | Physical activity score (no scoring scale provided by study authors): 68.0 (47.6)f | Mean difference in change 12.9 (3.5 to 22.3) | — | 286 | ⊕⊝⊝⊝ | Corresponding risk at 3 months: mean difference in change −2.2 (−12.9 to 8.5) |
| Knowledge and attitudes to change | ||||||
| Knowledge of nutrition and physical activity guidelines | Daily vegetable intake: adjusted OR 12.6d (6.50 to 24.5) Daily fruit intake: adjusted OR 16.2d (5.61 to 46.5) Weekly physical activity: adjusted OR 2.70d (0.31 to 23.2) | ⊕⊝⊝⊝ | — | |||
| Adverse effects | ||||||
| Any outcome considered an adverse effect | No study provided data for this outcome. | |||||
| Costs of the project (secondary outcome) | ||||||
| Costs per person in each treatment arm | USD 9.00 for targeted newsletters, USD 45.00 individually tailored newsletters, and USD 135 for individually tailored newsletters followed by home visits | 357 | ⊕⊝⊝⊝ | — | ||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; RCT: randomised controlled trial;RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence | ||||||
| aIn the GRADE assessments for the domain 'directness', we considered the studies directly relevant to the inclusion criteria. Thus, we have not downgraded on this domain. However, the population of interest will be dissimilar in different contexts, relating to characteristics of the ethnic minority group, the country and setting overall. The transferability of results must be considered for each context specifically. | ||||||
| Outcome | Estimated effect (95% CI)a July 2009 (start of campaign) | Estimated effect October 2009 (last month of campaign) | Estimated effect November 2009 (first month after campaign) | Estimated effect March 2010 (4 months after campaign) |
| Total number of calls | 42 (−115 to 198) | 153 (−8 to 314) | 146 (−13 to 304) | 32 (−148 to 212) |
| Calls from pregnant women | 14 (4 to 25) | 15 (4 to 27) | 8 (−3 to 19) | 7 (−5 to 20) |
| Calls from unique pregnant women | 8 (1 to 14) | 8 (1 to 14) | 6 (−1 to 12) | 3 (−4 to 10) |
| Calls from unique previously unknown pregnant women ('first‐timers') | 6 (1 to 11) | 6 (1 to 10) | 2 (−3 to 6) | 3 (−3 to 8) |
| aChange from pre‐campaign call rates. | ||||