采取针对性的大众媒体干预措施,促进健康行为,以降低少数民族成人患非传染性疾病的风险
摘要
研究背景
体育锻炼、均衡饮食、避免烟草接触和限制饮酒可降低非传染性疾病(non‐communicable diseases, NCDs)的发病率和死亡率。大众媒体干预通常用于鼓励人口群体采取更健康的行为。目前还不清楚针对少数民族群体的大众传媒干预在改变行为方面的效果是否比针对普通人群的干预更有效。
研究目的
确定针对少数民族成年人的大众媒体干预措施的效果,这些干预措施将提供有关体育锻炼、饮食模式、吸烟或饮酒的信息,以降低非传染性疾病的风险。
检索策略
截至2016年8月,我们检索了Cochrane对照试验中心注册库(Cochrane Central Register of Controlled Trials, CENTRAL)、MEDLINE、Embase、PsycINFO、CINAHL、ERIC、SweMed+和ISI Web of Science。截至2016年10月,我们还检索了OpenGrey、Grey Literature Report、Eldis和两个相关网站中的文献。检索不受语言限制。
纳入排除标准
我们检索了个别和分组随机对照试验、前后对照研究(controlled before‐and‐after studies, CBA)和间断时间序列研究(interrupted time series studies, ITS)。相关干预措施提倡与体育锻炼、饮食模式、吸烟或饮酒相关的健康行为,通过大众媒体渠道传播,并针对少数民族群体。干预对象包括重点国家少数民族群体中的成年人(≥18岁)。主要结局包括行为改变指标、自我报告的行为改变以及对改变的认识和态度。次要结局是健康促进服务的使用情况和与项目有关的费用。
资料收集与分析
两位作者独立审阅了参考文献,以确定纳入的研究。我们提取了所有纳入研究的资料并评估了偏倚风险。由于进行的比较、结局和研究设计存在异质性,我们没有将结果合并。我们对结果进行了叙述性描述,并在"研究结果摘要"表中进行了介绍。我们采用建议评估、发展与评价分级方法((Grading of Recommendations Assessment, Development, and Evaluation, GRADE)对证据质量进行了评估。
主要结果
有六项研究符合纳入标准,其中包括三项随机对照试验(RCT)、两项整群随机对照试验(cluster‐RCT)和一项间断时间序列研究(ITS)。所有研究均在美国进行,包括针对非洲裔(四项研究)、以西班牙语为主的拉丁裔移民(一项研究)和中国移民(一项研究)的大众媒体干预。后两项研究用受试者的母语(西班牙语、粤语或普通话)进行干预。三项干预只针对女性,其中一项专门针对孕妇。我们判断所有研究至少在一个领域存在不明确的偏倚风险,三项研究至少在一个领域存在较高的偏倚风险。
我们将研究结果分为三类比较。第一类比较评价了针对少数民族的大众媒体干预与针对普通人群的同等大众媒体干预。这一类中的一项研究(255名非洲裔受试者)发现,在自我报告的吸烟行为改变方面,两者的效果几乎没有差异,而在改变态度方面,向受试者发放具有文化特色的戒烟手册与向普通人群发放戒烟手册之间的差异很小。根据GRADE方法(效果证据质量极低)的评估,我们无法确定效果估计值。没有研究提供行为改变指标或不良反应的数据。
第二项比较评价了有针对性的大众媒体干预与无干预的对比。一项研究(154名非洲裔受试者)报告了我们的主要结局。干预组的受试者可以在三个月内收看12个小时的有线电视直播节目,并收到有关营养和体育活动的印刷材料,以改善健康和控制体重。干预组与无干预组在基线12个月后的体重指数(BMI)变化相当(低质量证据)。干预组在饮食习惯(脂肪行为)和休闲活动总分方面的变化较好(极低质量证据)。另外两项研究将整个地理区域的人口暴露在针对非裔美国人社区的广播广告中。作者介绍了对我们的两个次要结局(健康促进服务的使用和项目成本)的影响。活动信息是拨打戒烟热线。结局是收到的电话数量。一年后,一项研究报告称,在干预社区(估计目标人群为31.05万人),估计在每1万名目标吸烟者中接到18个电话,而在对照社区(估计目标人群为33.14万人),估计在每1万名目标吸烟者中接到0.2个电话(中等质量证据)。ITS研究还报告称,在活动期间,目标人群的来电数量有所增加(低质量证据)。在这两项研究中,非裔美国人的来电比例都有所上升(低至极低质量证据)。没有任何研究提供了有关改变的知识和态度以及不良影响的数据。有关成本的信息很少。
第三项比较评估了有针对性的大众媒体干预与大众媒体干预加个性化内容。研究结果基于三项研究(1361名受试者)。这些比较组的受试者都收到了个人反馈。其中两项研究记录了体重随时间的变化。这两项研究均未发现组间存在明显差异(低质量证据)。关于行为变化、知识和态度的证据通常发现,接受个性化内容的组别有一些效果,或组别间无明显差异(极低质量证据)。没有任何研究提供有关不良影响的数据。有关成本的信息很少。
作者结论
现有证据不足以让人了解到,针对少数民族人群的大众媒体干预措施在改变健康行为方面是否比针对广大人群的大众媒介干预措施更有效。与不干预相比,有针对性的大众媒体干预可能会增加戒烟热线的数量,但对健康行为的影响尚不清楚。这些研究无法区分不同组成部分的影响,例如听到关于行为变化的信息的影响、对少数民族群体的文化适应,或通过更适当的大众媒体渠道增加对目标群体的影响。新的研究应该探索针对居住国母语,而不是主要语言的少数民族的有针对性的干预措施,并直接比较有针对性和普通人群的大众媒体干预措施。
PICO
简语概要
采取有针对性的大众媒体干预措施,鼓励少数民族成人的健康行为
研究背景和综述问题
卫生当局和非政府组织经常使用大众媒体干预措施(例如传单、广播和电视广告、海报和社交媒体)来鼓励与身体活动、饮食模式、吸烟或饮酒等相关的更健康的行为。在本综述中,我们考虑了针对少数民族的大众媒体干预措施的影响。有针对性的干预措施是为特定群体设计并考虑其特点的,理想情况下为少数民族群体提供平等的机会和资源,以获得信息、生活技能和做出更健康选择的机会。然而,我们不知道有针对性的大众媒体策略是否比为普通民众制定的大众媒体策略更有效地接触和影响少数民族。
研究特征
我们发现了六项研究,全部来自美国,其中四项针对非裔美国人,两项针对拉丁裔或中国移民。在这些研究中,四项是实验性的(1693名志愿者),两项研究报告了在整个社区和城市开展的大型、有针对性的活动的结果。证据检索时间截至2016年8月。
主要研究结果
现有证据不足以得出结论,针对少数族裔群体的有针对性的大众媒体干预措施在改变健康行为方面是否比一般大众媒体干预措施更有效、更无效或同等有效。只有一项研究比较了受试者在收到适应文化的吸烟建议小册子或为普通人群开发的小册子后的吸烟习惯和戒烟意图。他们发现各组之间的吸烟行为几乎没有差异。
与不干预相比,有针对性的大众媒体干预可能会增加戒烟热线的数量,但对健康行为的影响尚不清楚。这一结论基于三项研究的结果。一项研究让受试者观看了一系列12个有线电视直播节目,了解如何通过饮食和体育活动保持健康体重。与没有观看节目的女性相比,受试者表示身体活动略有增加,饮食模式也发生了一些积极的变化;然而,随着时间的推移,他们的体重没有变化。另外两项研究是大规模的有针对性的活动,鼓励吸烟者拨打戒烟热线以获得戒烟建议。活动期间,来自目标人群的电话数量大幅增加。
该综述还比较了有针对性的大众媒体干预与增加个人互动的大众媒体干预。这些基于三项研究的发现尚无结论。
没有一项研究报告干预措施是否会产生任何不利影响,例如感到羞耻的可能或更加抗拒相关信息。
直接比较有针对性的大众媒体干预措施与一般大众媒体干预措施的进一步研究将是有用的。很少有研究调查有针对性的大众媒体干预对主要讲非主流语言的少数民族群体的影响。
证据质量
我们认为,对于影响所有主要结局的证据,证据质量从低到极低。这意味着真实效果可能与本综述呈现的结果有本质的不同。我们对戒烟热线电话数量的估计增加有一定的信心。
Authors' conclusions
Summary of findings
| Comparison 1: targeted mass media intervention versus general population mass media intervention for promoting healthy behaviours | ||||||
| Patient or population: adult, ethnic minority: self‐described Americans of African heritage | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | N of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| General population mass media intervention | Targeted mass media intervention | |||||
| Indicators of behavioural change | ||||||
| Any outcome considered an indicator of change | No study provided data for this outcome. | |||||
| Self‐reported behavioural change | ||||||
| Proportion smoking reduction, 3 months follow‐up | 94% | 95% | — | 255 | ⊕⊝⊝⊝ | No effect measures reported by authors. Not significantly different between groups |
| Quit‐attempts, 3 months follow‐up | — | — | Adjusted OR 1.97 (1.09 to 3.55) in favour of general population mass media intervention | 255 | ⊕⊝⊝⊝ | 24‐hour and 7‐day point prevalence abstinence not significantly different between groups |
| Knowledge and attitudes to change | ||||||
| Contemplation ladder to quit smoking (1‐10), 3 months follow‐up | Mean score: 8.2 (SD 2.4) | Mean score: 7.3 (SD 2.6) | — | 255 (1 RCT) | ⊕⊝⊝⊝ | Difference between group reported at P = 0.01 |
| Adverse effects | ||||||
| Any outcome considered an adverse effect | No study provided data for this outcome. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) | ||||||
| GRADE Working Group grades of evidence | ||||||
| aIn the GRADE assessments for the domain 'directness', we considered the studies directly relevant to the inclusion criteria. Thus, we have not downgraded on this domain. However, the population of interest will be dissimilar in different contexts, relating to characteristics of the ethnic minority group, the country and setting overall. The transferability of results must be considered for each context specifically. | ||||||
| Comparison 2: targeted mass media intervention for promoting healthy behaviours versus no intervention | ||||||
| Patient or population: adult, ethnic minority group: self‐described Americans of African heritage | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | N of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| No intervention | Targeted mass media intervention | |||||
| Indicators of behavioural change | ||||||
| BMI (kg/m2), 12 months from baseline | 34.4 (SD 8.5)b | Mean difference in change 0.1 (−0.4 to 0.6) | — | 154 | ⊕⊕⊝⊝ | Corresponding risk at 3 months: mean difference in change −0.4 (−0.7 to −0.02) |
| Self‐reported behavioural change | ||||||
| Changes in dietary composition, 12 months from baseline | Food habits questionnaire, score on fat behaviours (no scoring scale provided by study authors): 1.0 (SD 0.4) | Mean difference in change −0.2 (−0.3 to ‐0.1) | — | 154 (1 RCT) | ⊕⊝⊝⊝ | Corresponding risk at 3 months: mean difference in change −0.1 (−0.2 to −0.02) |
| Leisure time physical activity, 12 months from baseline | Physical activity score (no scoring scale provided by study authors): 60.0 (SD 47.0)e | Mean difference in change 12.0 (1.0 to 23.0) | — | 154 (1 RCT) | ⊕⊝⊝⊝ | Corresponding risk at 3 months: mean difference in change 10.0 (−1.7 to 21.8) |
| Knowledge and attitudes to change | ||||||
| Any measure of knowledge and attitude | No study provided data for this outcome. | |||||
| Adverse effects | ||||||
| Any outcome considered an adverse effect | No study provided data for this outcome. | |||||
| Use of health promotion services (secondary outcome) | ||||||
| Calls to smoking quit lines, during campaign | 18 calls per estimated 10,000 African American smokers in the intervention group versus 0.2 calls in the control communitiesf. | Estimated target population 641,800 (1 RCT) | ⊕⊕⊕⊝ | — | ||
| Calls to smoking quit lines, during and after campaign | Change from pre‐campaign, calls per month (95% CI) from new pregnant smokers: 8 (1 to 14) first month of campaign, 8 (1 to 14) last month of campaign, 6 (−1 to 12) first month after campaign, 3 (−4 to 10) 4 months after campaign | Population in target city ˜300,000 (1 ITS) | ⊕⊕⊝⊝ | — | ||
| Proportion of calls from target population during campaign | Proportion of calls from African Americans during trial: 82% in intervention and 26% in control communities | Estimated target population 641,800 (1 RCT) | ⊕⊕⊝⊝ | — | ||
| Proportion of calls from target population during and after campaign | Proportion African Americans among pregnant callers: 41% before campaign, 86% during the campaign, 28% after campaign | Population in target city ˜300,000 (1 ITS) | ⊕⊝⊝⊝ | — | ||
| Costs of the project (secondary outcome) | ||||||
| Programme costs | USD 106,821 for radio advertisements and USD 6744 for television advertisements. No overall costs reported | Estimated target population 641,800 (1 RCT) | ⊕⊕⊝⊝ | — | ||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aIn the GRADE assessments for the domain 'directness', we considered the studies directly relevant to the inclusion criteria. Thus, we have not downgraded on this domain. However, the population of interest will be dissimilar in different contexts, relating to characteristics of the ethnic minority group, the country and setting overall. The transferability of results must be considered for each context specifically. | ||||||
| Comparison 3: targeted mass media intervention versus targeted mass media intervention plus personalised content | ||||||
| Patient or population: adult, ethnic minority groups: Latino immigrants, elderly Chinese immigrants, self‐described Americans of African heritage | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | N of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Media intervention with personalised content (comparison) | Targeted mass media intervention | |||||
| Indicators of behavioural change | ||||||
| BMI (kg/m2), 12 months from baseline | 34.9 (SD 7.7)b | Mean difference in change 0.4 (−0.1 to 0.8) | — | 286 | ⊕⊕⊝⊝ | Two RCTs (643 participants) reported BMI at 3 months. None found significant differences in weight change between study groups |
| Self‐reported behavioural change | ||||||
| Intake meeting target from dietary guidelines, 3 months from baseline | Vegetables: adjusted OR 5.53d (1.96 to 15.58) Fruit: adjusted OR 1.77d (0.99 to 3.15) | 718 (1 RCT) | ⊕⊝⊝⊝ | — | ||
| Changes in dietary composition, 12 months from baseline | Food habits questionnaire, score on fat behaviours (no scoring scale provided by study authors): 1.0 (SD 0.4)f | Mean difference in change −0.1 (−0.2 to −0.02) | — | 286 | ⊕⊝⊝⊝ | Two RCTs (643 participants) reported changes in dietary composition at 3 months. None found significant differences/mean difference in change for energy or dietary fibre intake (study 1) or food habits questionnaire (fat behaviours) (study 2) |
| Weekly physical activity meeting target from guidelines, 3 months from baseline | Adjusted OR 1.27d (0.89 to 1.80) | 718 (1 RCT) | ⊕⊝⊝⊝ | — | ||
| Leisure time physical activity, 12 months from baseline | Physical activity score (no scoring scale provided by study authors): 68.0 (47.6)f | Mean difference in change 12.9 (3.5 to 22.3) | — | 286 | ⊕⊝⊝⊝ | Corresponding risk at 3 months: mean difference in change −2.2 (−12.9 to 8.5) |
| Knowledge and attitudes to change | ||||||
| Knowledge of nutrition and physical activity guidelines | Daily vegetable intake: adjusted OR 12.6d (6.50 to 24.5) Daily fruit intake: adjusted OR 16.2d (5.61 to 46.5) Weekly physical activity: adjusted OR 2.70d (0.31 to 23.2) | ⊕⊝⊝⊝ | — | |||
| Adverse effects | ||||||
| Any outcome considered an adverse effect | No study provided data for this outcome. | |||||
| Costs of the project (secondary outcome) | ||||||
| Costs per person in each treatment arm | USD 9.00 for targeted newsletters, USD 45.00 individually tailored newsletters, and USD 135 for individually tailored newsletters followed by home visits | 357 | ⊕⊝⊝⊝ | — | ||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; RCT: randomised controlled trial;RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence | ||||||
| aIn the GRADE assessments for the domain 'directness', we considered the studies directly relevant to the inclusion criteria. Thus, we have not downgraded on this domain. However, the population of interest will be dissimilar in different contexts, relating to characteristics of the ethnic minority group, the country and setting overall. The transferability of results must be considered for each context specifically. | ||||||
Background
Description of the condition
This Cochrane Review explores the effectiveness of targeted mass media interventions in advising ethnic minority groups on preventing non‐communicable diseases (NCDs) through healthier behaviours. Specifically, this review addresses the question of whether or not ethnic minorities will benefit from targeted approaches, which means that interventions are designed to consider characteristics of particular groups (Kreuter 2003).
The most prevalent NCDs (cardiovascular diseases, cancers, chronic respiratory disease, and diabetes) are also the world's leading causes of morbidity and mortality. According to the World Health Organization (WHO), NCDs cause 63% of global deaths, about 40% of which occur in people between 30 and 70 years of age (WHO 2010). The burden of NCDs is a growing public health crisis worldwide, and WHO has called for more actions to prevent disease. Many NCDs share four modifiable, behavioural risk factors: lack of physical activity, poor diet, tobacco use, and excessive consumption of alcohol. Improvements in these behaviours can prevent or delay the onset of disease (Lim 2012). One of the objectives in the WHO Global Action Plan for the Prevention of Noncommunicable Diseases deals with the need to address these four risk factors throughout populations, and mass media campaigns and social marketing initiatives are among the proposed policy options (WHO 2013a).
The WHO Commission on Social Determinants of Health highlighted how "the conditions in which people are born, grow, live, work and age" strongly determine health status and disease patterns within and between populations (CSDH 2008). This picture includes inequities in the morbidity and mortality patterns of NCDs (WHO 2010). In most countries, life expectancy and health status are correlated with social status, as measured by education, occupation, income, or wealth. The underlying forces behind this link include a wide array of unevenly distributed environmental, structural, economic, social, and cultural factors (CSDH 2008). Health inequities are not simply differences between groups, but differences that are considered both avoidable and unjust (Whitehead 1992). The Rio Political Declaration on Social Determinants of Health reaffirmed a global political commitment to reducing health inequities (WHO 2011).
Inequities in health status and disease risk are also associated with ethnic minority status. In many countries, ethnic minority groups tend to have poorer health outcomes than the majority population (Alderete 1999; Nielsen 2010; AHRQ 2013). Genetic variations only partially contribute to differences between ethnic groups in terms of disease patterns (Bhopal 2007). Differences in cultural factors (e.g. beliefs and practices) may influence health status, but social, economic and structural determinants of health during people's lifespans appear to be associated with health inequities between ethnic groups as well (Nazroo 2003; Mulia 2008; Viruell‐Fuentes 2012). Therefore, cultural influences should not be overemphasised as discrete explanatory factors for health inequities (Nazroo 2003; Acevedo‐Garcia 2012). Ethnic minority groups are heterogeneous, having wide‐ranging living conditions within and between countries, with consequently different health statuses and disease risks. The disease patterns of ethnic minorities may converge over time towards those of the majority population. However, health inequities between groups are sufficiently pronounced in many countries to warrant specific public health considerations.
Physical activity levels, dietary habits, tobacco use and alcohol consumption vary between population groups (WHO 2010). In many countries, unhealthy behaviours tend to be more prevalent in disadvantaged groups (Mackenbach 2008), and disparities in health behaviours have recently been shown to increase over time, as more privileged socioeconomic groups adopt healthier behaviours while disadvantaged groups lag behind (Buck 2012). Thus, although behaviours have an element of personal choice, behavioural patterns reveal the influence of the wider determinants of health.
Concern has been raised that public health interventions that have benefited the population overall might have increased inequities. This effect has been observed in public health interventions aimed at voluntary behavioural change in particular (Lorenc 2013). Public health campaigns delivered through mass media or by other means appear to be less effective in socioeconomically disadvantaged groups, whether for smoking cessation (Niederdeppe 2008a; Thomas 2008), physical activity (De Bourdeaudhuij 2011), or dietary factors (Oldroyd 2008; Stockley 2008). On the contrary, structural interventions, such as taxation of tobacco products and alcoholic beverages, appear more likely to reduce differences in health parameters (Lorenc 2013). It is therefore important to identify effective public health strategies that bridge the health gap rather than amplify it.
There are reasons to believe that mass media interventions can be less effective in reaching many ethnic minority groups as well, although few studies have systematically assessed the effects of these campaigns on ethnic minority groups (Niederdeppe 2008b; Durkin 2012; Bala 2013). The health behaviours of ethnic minority groups in different countries could be both more and less healthy than those of the majority population (e.g. the higher prevalence of smokers in some indigenous populations or lower alcohol consumption among Muslim immigrants). However, by describing ethnic minority health in relative terms only, we may fail to consider the absolute magnitude of a health problem or a health need that should guide public health priorities (Bhopal 2007). The Ottawa Charter for Health Promotion declares that equal opportunities and resources to secure "access to information, life skills and opportunities for making healthy choices" are some of the prerequisites for health improvements (WHO 1986). Targeted mass media interventions are possible strategies to better disseminate health promotion messages among ethnic minorities (Webb 2010b; Gould 2013; Nierkens 2013), but their effectiveness has not been established.
There is no internationally agreed‐upon definition of ethnicity, but Bhopal 2007 has summarised some key points: "The concept of ethnicity is complex and implies, according to most accounts, one or more of the following: shared origins or social background; shared culture and traditions which are distinctive, maintained between generations, and lead to a sense of identity and group‐ness; a common language or religious tradition" (Bhopal 2007). Oxford Dictionaries defines an ethnic minority as "a group within a community which has different national or cultural traditions from the main population". Ethnic minority groups are sometimes divided into indigenous populations (SPFII 2004), national ethnic minorities (long‐time residents) (FCNM 2012), and immigrants. Through international migration, most countries gradually become more ethnically diverse. It is important to note that these definitions use social and cultural factors rather than biological ones (physical appearance or genetic differences) to define population groups (Bhopal 2007).
Ethnic minority status is associated with lower socioeconomic status in many countries, but ethnic identity and measures of socioeconomic status have different features. Programmes targeted to ethnic minorities should consider factors such as preferred language; food traditions; different norms, values and knowledge systems; patterns of media use; collective history; and position in the society. Arguably, then, it is appropriate to explore the effectiveness of mass media interventions targeted to ethnic minority groups as distinct from interventions directed at socioeconomically disadvantaged groups.
Description of the intervention
Targeted mass media interventions that promote healthier behaviours to reduce the risk of NCDs in adult ethnic minorities are the subject of this Cochrane Review. Public health authorities, health promotion agencies and non‐governmental organisations (NGOs) are the main providers of health promotion interventions. According to Ferri 2013, most mass media campaigns can be characterised as either information campaigns with messages of warning, empowerment or support, or social marketing campaigns that attempt to correct erroneous normative beliefs, clarify social and legal norms, or set positive role models or social norms. Designers of mass media interventions draw on a wide range of commercial marketing tools and principles. Health promotion campaigns partly overlap with social marketing, using concepts and approaches from marketing to influence behaviours to benefit individuals and communities for the social good (French 2010).
Kreuter 2003 describes a targeted health communication strategy as communication "intended to reach some population subgroup based on characteristics presumed to be shared by the group's members". They distinguish targeted from tailored communication, which is communication adapted to the specific characteristics of an individual. A targeted approach coincides with the principle of audience segmentation in social marketing theory, that is, the identification of meaningful differences among population groups that affect their responses to the promoted action. Thorough knowledge of the target audience is important for developing good combinations of strategic elements and approaches to achieve an intervention's goals (French 2010; MvVey 2010). Targeted communication strategies are only meaningful if the population subgroup is sufficiently homogeneous (Kreuter 2003; Castro 2010). Thus, communication targeted to broadly defined population subgroups, for instance the Latino population in the USA, may fail to recognise subcultures with different history, collective experiences, living conditions and health needs.
Interventions targeting ethnic minority groups should include cultural adaptations that consider "language, culture, and context in such a way that is comparable with the client's cultural patterns, meanings, and values" (Bernal 2009). Common strategies for cultural adaptation of health interventions include gathering information, user input, and feedback from the target group (Netto 2010; Barrera 2013). A targeted approach should also carefully consider ethical aspects to avoid stereotyping and stigmatising. Cultural adaptation strategies have been categorised into surface adjustments and deep, structural‐level adjustments. Surface‐level adjustments involve changing factors such as language, graphics, food, and clothing to match the target audience. Deep, structural‐level adjustments are changes that reflect the cultural, social, historical, environmental, and psychological forces behind behaviours in the target population (Resnicow 1999).
This review includes only health promotion interventions delivered via mass media. Brinn 2010 and Bala 2013 describe mass media as "channels of communication that intend to reach a large number of people without direct person‐to‐person contact". Mass media reach audiences through print material, recordings, broadcast, the Internet, and digital technology. Mass media interventions have the potential to cost effectively reach many people and can spread a message to remote geographical areas or groups that otherwise are difficult to access, or to target certain groups through selected media channels. Mass media channels have diversified quickly in the last couple of decades, including the development of digital communication technology, and national borders now pose fewer constraints on the reach of media channels.
Previous systematic reviews on mass media interventions or campaigns concerning public health issues (smoking cessation, HIV testing, health services utilisation, illicit drug use, mental health‐related stigma) have found that their effects on behavioural outcomes are either inconclusive or exhibit only modest short‐term effects (Grilli 2002; Vidanapathirana 2006; Brinn 2010; Bala 2013; Clement 2013; Ferri 2013). Long‐term effects are generally unclear. Modest effects of mass media interventions on an individual level can still have an important public health impact overall. The population strategy approach to disease prevention, as suggested by Rose 1985, aims to shift the distribution of a risk factor across entire populations. This shift includes the large proportion of the population with only a moderate risk of disease but a significant portion of the total disease burden.
How the intervention might work
The evidence linking increased physical activity, balanced diets, avoidance of tobacco, and limited alcohol consumption to reduced morbidity and mortality from NCDs is well established (WHO 2009; WHO 2010; WHO 2013a; WHO 2013b; WHO 2014). The logic model in Figure 1 (adapted based on Bertrand 2006 and Niederdeppe 2008b) illustrates the possible elements and the relationships by which a targeted mass media intervention can influence these four health‐related behaviours. An additional desired outcome could be that individuals will consult health promotion services, such as smoking cessation assistance or health counselling.

Several theories and models seek to explain health behaviours on the individual level and to determine the most efficient way to influence these behaviours. These theories emphasise that increased knowledge is not sufficient to influence behaviour. Perceived barriers and risks are important moderators of behaviour, while attitudes and self‐efficacy contribute to a person's motivation and competence to act (Brewer 2008). In the logic model, changes in people's knowledge of and attitudes about health behaviours, in addition to self‐efficacy, are the measurable intermediate outcomes of mass media interventions. Contemporary thinking in public health and health promotion acknowledges that social norms, interpersonal interaction and the social and cultural environment influence individual behaviour strongly (Viswanath 2008). People's wider environment – physical, economic, political, legal and policy – may either enable or counteract a certain behaviour (McLeroy 1988; Davis 2014). A basic assumption in this Cochrane Review is that these theories and models are relevant to all population groups.
A mass media intervention can only influence health behaviours if the target audience receives, understands and can recall the message. Based on data and conceptual input (Sorensen 2004; Viswanath 2006; Niederdeppe 2008a), Niederdeppe 2008b has hypothesised that there are three possible sources of differences in response to smoking cessation campaigns that can be traced to socioeconomic status. These three domains probably apply to ethnic minorities as well and may be relevant to consider for targeted mass media interventions, as indicated in the logic model: differences in access, exposure, attention to and retention of the media message; differences in the message's persuasiveness and its motivational response; and differences in opportunities to change in response to the message (Niederdeppe 2008b).
Different media channels might be necessary to reach ethnic minorities, either because conventional media channels are less accessible or not preferred. The language and format of the content (language complexity, illustrations used, skills demonstration) can influence message recall and comprehension. Low health literacy levels, understood as low ability to obtain, process, and understand basic health information, have been identified in many ethnic minority groups and can influence response and compliance with health messages (Berkman 2011). Thus, planners must carefully consider media access, exposure, language and format, attention to and retention of the media message, making these relevant to the targeted ethnic minority group in order to extend the intervention reach.
The second domain relates to the persuasiveness of and motivational response to a message, which could strongly depend on its cultural appropriateness for ethnic minorities. Evidence from health promotion interventions via channels other than mass media have indicated better adherence to a promoted behavioural change when ethnic minorities receive culturally adapted health messages or counselling instead of a standard treatment (Nierkens 2013; Attridge 2014). The four health behaviours in this review relate closely to many markers of ethnic identity. The most obvious ones are dietary patterns and alcohol consumption, but physical activity and smoking patterns may also be closely related to cultural context.
Ethnic minorities might have limited opportunities to change health behaviours, either from a cultural, financial, or structural perspective. Previous reviews on the effect of mass media interventions for smoking cessation indicate that these are more likely to be successful as part of multicomponent programmes with upstream policy support and downstream community‐based activities (Brinn 2010; Bala 2013). Examples of relevant co‐interventions for this Cochrane Review include changes in legislation regarding advertising and taxation of food items, tobacco products, and alcoholic beverages, or changes in available spaces and social arenas for physical activity. Mass media interventions could have an indirect, amplifying effect if family, friends and the wider community adjust their attitudes, norms and behaviours according to the health message. Thus, multicomponent interventions can add benefits to efforts directed at individual change by modifying opportunities to change. Figure 1 indicates relevant sectors for co‐interventions in multicomponent programmes. The logic model also indicates possible unwanted effects of an intervention. Examples of adverse effects are increased resistance to the health promotion message or that the target population will experience more feelings of disempowerment when exposed to a goal they find difficult to achieve.
Why it is important to do this review
Mass media campaigns promoting healthy behaviours are one of several recommended policy options to prevent NCDs (WHO 2009; WHO 2013a), and most countries commonly use them to encourage healthier behaviours (WHO 2009; WHO 2013b; WHO 2014), despite the potentially limited effectiveness. The concern that mass media interventions could widen health inequities warrants more focus on the effect of targeted strategies in population subgroups. It is unclear whether targeted mass media interventions are more effective in changing health behaviours in ethnic minorities than a universal population strategy. This is important to explore, as segmentation of interventions to reach different subgroups may increase programme costs.
The Norwegian Directorate of Health and the Norwegian Cancer Society commissioned a systematic review on this issue to inform public health policy on how to deliver health promotion messages to the growing and increasingly diverse immigrant population. This systematic review has been widened to encompass an international perspective, including a wide focus on ethnic minority groups, as the question may be useful for other national authorities and NGOs as well.
The primary focus of this Cochrane Review is the mode of delivery (mass media intervention) and the strategies used to target such interventions to ethnic minority groups and prevention of NCDs, rather than any of the four specific health behaviours separately. The four behaviours have distinct features and require different messages regarding the suggested action (i.e. to increase physical activity, modify diets, decrease alcohol consumption, or refrain from smoking). At the same time, the behaviours are similar in their focus on preventing negative health outcomes in the future. Thus, the target audience may be less motivated to change ingrained habits in favour of longer‐term – and hence more uncertain – benefits. Our objectives intersect with two Cochrane Reviews on mass media interventions for smoking cessation (Brinn 2010; Bala 2013). Two other systematic reviews have examined the effects of smoking cessation interventions in indigenous populations but are not limited to mass media interventions (Carson 2012a; Carson 2012b). Our objectives include interventions focusing on tobacco use to obtain a full picture of mass media strategies as a means of disseminating health‐promoting messages among ethnic minorities. We gathered additional information on features of these interventions, theoretical frameworks and co‐interventions.
Objectives
Primary
• To determine the effect of mass media interventions targeting adult, ethnic minorities with messages about physical activity, dietary patterns, tobacco use or alcohol consumption to reduce risk of NCDs.
Secondary
• To examine the effect of targeted mass media interventions alone compared to targeted mass media interventions given as part of multi‐component interventions.
Methods
Criteria for considering studies for this review
Types of studies
By definition, mass media communication strategies target large groups of people. Individually randomised controlled trials (RCTs) may be neither the most appropriate nor most feasible study design. Therefore, we included the following study designs and specified features, guided by recommendations from the Effective Practice and Organisation of Care Group (EPOC) review group (EPOC 2016).
-
RCTs.
-
Cluster‐RCTs with at least two intervention groups and two control groups.
-
Non‐RCTs (NRCTs) with at least two intervention sites and two control sites.
-
Controlled before‐and‐after (CBA) studies with at least two intervention sites and two control sites.
-
Interrupted‐time‐series (ITS) or repeated measures studies (RMSs) with a clearly defined point in time when the intervention occurred and at least three data points before and three after the intervention.
Types of participants
The population of interest was adults (≥ 18 years) described as being from an ethnic minority group in their country of residence. We use the terms ethnicity and ethnic minorities as described in the Background but did not limit the eligibility of participants to studies using these terms. Different countries and research traditions have dissimilar terminology relating to aspects of ethnicity (Bhopal 2007). Not all use the terms ethnicity and ethnic minorities. We based inclusion on any direct or implicit description by the study authors that the study participants were selected based on ethnic minority characteristics and that the intervention was targeted to such a population group. Examples of applicable terms are indigenous populations, native, aboriginal, racial groups, immigrants, ancestral origin (countries or continents), countries of birth, or specified first language/mother tongue/language preference.
Types of interventions
To be eligible for inclusion, the intervention had to meet all of the following three criteria.
-
The purpose of the intervention was to promote healthier behaviours related to physical activity, dietary patterns, tobacco use, or alcohol consumption.
-
The intervention was disseminated via a mass media channel.
-
The intervention was targeted to an ethnic minority group.
We used the same definition of mass media as in two related Cochrane Reviews (Brinn 2010; Bala 2013): "Mass media is defined here as channels of communication such as television, radio, newspapers, billboards, posters, leaflets or booklets intended to reach large numbers of people and which are not dependent on person‐to‐person contact". In addition, we aimed to include other contemporary mass media channels, such as campaigns delivered through the Internet, social media, and mass distribution through mobile phones. We used the definition by Kreuter 2003 for targeted interventions but did not limit the inclusion to studies using the same terminology.
We included studies that compared the intervention with a general population mass media intervention, no intervention or any other intervention. We included studies that compared targeted mass media interventions alone with targeted mass media interventions delivered as part of multicomponent interventions to explore the secondary research objective.
There were no set requirements on minimum length of intervention.
We excluded the following interventions.
-
Courses, teaching activities and programmes, interactive self‐help programmes or self‐monitoring services, as these are not considered mass media interventions even though they can be delivered through the Internet, digital applications, or similar media.
-
Interventions with mass distributed print, audio, or visual material where the content has been tailored/personalised to each individual (i.e. based on answers from questionnaires or similar information sources).
-
Interventions for patient groups/patient education (including treatment of alcohol dependency and eating disorders), or interventions aimed specifically at relatives of patients.
Types of outcome measures
We did not expect to find any studies of targeted mass media interventions using morbidity or mortality of NCDs as outcome measures, nor clinical risk factors of disease. We intended to examine a number of surrogate endpoints relating to the four specified health behaviours as primary outcomes as relevant, including both objectively measured and self‐reported outcomes.
There was no requirement for a minimum duration of follow‐up for the outcome measures. We intended to present outcomes separately for short‐term (< six months) and long‐term ( ≥ six months) follow‐up.
Primary outcomes
-
Physiological or clinical parameters that indicate changes in physical activity, dietary intake, use of tobacco, or alcohol consumption
-
Objective or self‐reported measurements of physical activity, dietary intake, use of tobacco, or alcohol consumption
-
Measures of knowledge and attitudes concerning physical activity, dietary intake, use of tobacco, or alcohol consumption
Secondary outcomes
-
Use of health promotion services (for instance smoking quit lines and counselling) or other relevant services
-
Costs related to the project
Adverse outcomes
-
Any reported outcome considered an adverse effect, such as measures of participants' resistance to the health promotion message or measures of perceived disempowerment in participants.
Search methods for identification of studies
A research librarian conducted the electronic literature searches.
Electronic searches
We performed a scoping search to identify any systematic reviews in the last five years with a similar primary research objective. We based the search terms on the strategy described in Appendix 1 but with a filter for systematic reviews. We searched the following electronic databases from the beginning of 2009 until September 2014.
-
Cochrane Database of Systematic Reviews, part of the Cochrane Library (www.thecochranelibrary.com).
-
Database of Abstracts of Reviews of Effects (DARE), part of the Cochrane Library (www.thecochranelibrary.com).
-
Health Technology Assessment Database (HTA), part of the Cochrane Library (www.thecochranelibrary.com).
-
Centre for Reviews and Dissemination (DARE, HTA).
We did not identify any systematic reviews with a similar research objective. As previously described, we are aware of that four Cochrane systematic reviews intersect with the objectives of this Cochrane Review (Brinn 2010; Carson 2012a; Carson 2012b; Bala 2013).
We searched for primary studies without any time limitations or language restrictions on 22 May 2015 and later updated the search to 23 August 2016. We present the search strategies in Appendix 1. We modified the search strategy, subject headings, and syntax to each database and searched the following databases.
-
Cochrane Central Register of Controlled Trials (CENTRAL; 2016; Issue 7), part of the Cochrane Library.
-
MEDLINE Ovid (from 1946).
-
PubMed (from 1946).
-
Embase Ovid (from 1974).
-
PsycINFO Ovid (from 1806).
-
CINAHL EBSCO (Cumulative Index to Nursing and Allied Health Literature; from 1981).
-
ERIC EBSCO (from 1966).
-
SweMed+ (from 1977).
-
ISI Web of Science (from 1987).
After merging the databases from each search into the reference management software Endnote 2015, the librarian removed studies retrieved in duplicate.
Searching other resources
We screened related systematic reviews, as found in the scoping search, for relevant primary studies. We also conducted cited reference searches for all included studies using ISI Web of Knowledge and screened their reference lists.
Trial registries
We searched the following websites to 19 October 2016.
-
WHO International Clinical Trials Search Portal (http://apps.who.int/trialsearch).
-
ClinicalTrials.gov (http://clinicaltrials.gov).
Grey literature
We searched the following websites to 19 October 2016.
-
OpenGrey (www.opengrey.eu).
-
Grey Literature Report (www.greylit.org).
-
Eldis (www.eldis.org).
Data collection and analysis
Selection of studies
Two review authors screened titles and abstracts independently (AM with either IBL or GEV). We retrieved the full text of all potentially relevant studies. Two review authors (AM with either IBL or GEV) independently assessed these for eligibility using a checklist. At each stage, we resolved any disagreement by discussion or consensus with a third review author. The project group read articles in English, Scandinavian languages and German. Staff members at the Norwegian Institute of Public Health read other languages or considered them for translation. We list the studies excluded based on full‐text assessment in the Characteristics of excluded studies table.
Data extraction and management
We extracted data using a form based on the Data Extraction and Assessment Template from the Cochrane Public Health Group (CPHG). This data extraction form embeds items relating to the PROGRESS‐Plus criteria and the PRISMA‐Equity 2012 Extension (Tugwell 2010; Welch 2012). We revised the form before data extraction. One review author retrieved the specified information and data from the included studies, and another review author checked data extraction. We resolved any disagreements by discussion or consensus with a third review author. We contacted the study authors if key information was missing. We entered the extracted data into RevMan 2014 as appropriate.
When more than one publication referred to the same study, we used the relevant paper with the most comprehensive and clear description of methods and outcome reports from a peer‐reviewed journal as the primary reference. If necessary, we used all papers from one study to extract the relevant information. We contacted investigators in cases of contradiction or incomplete reporting.
In addition to the items from the Data Extraction and Assessment Template, which included descriptions of study details (reference, design), participants, setting, intervention, outcomes, and adverse outcomes, we also extracted the following information when available.
-
Context of the intervention (sociodemographic, organisational, political, media structure).
-
Content of the message (health behaviour targeted).
-
Theoretical basis of the intervention, including message development and framing.
-
Theoretical basis for how the intervention and message were adapted to the target population.
-
Media channel(s) used for delivery and frequency of exposure.
-
Intervention fidelity (whether the intervention was delivered as planned).
-
Information on the nature and extent of any additional actions given as part of the intervention (co‐interventions).
-
Intervention costs.
-
Source of funding.
We present these data in the Characteristics of included studies section.
Assessment of risk of bias in included studies
Two review authors independently assessed the included studies with respect to risk of bias (AM, GEV). We assessed all study designs using the suggested 'Risk of bias' criteria for EPOC reviews (EPOC 2015). There are nine standard criteria for RCTs, cluster‐RCTs, NRCTs, and CBAs: adequate generation of allocation sequence; adequate allocation concealment; similar baseline outcome measurements; similar baseline characteristics; adequate handling of incomplete outcome data; adequate prevention of knowledge of the allocated interventions during the study; adequate protection against contamination; freedom from selective outcome reporting; and other risks of bias. For ITS studies we considered the following criteria: intervention independent of other changes, shape of the intervention effect pre‐specified, intervention unlikely to affect data collection, knowledge of the allocated intervention adequately prevented during the study, incomplete outcome data adequately addressed, study free from selective outcome reporting, and any other risks of bias. We resolved any disagreement in the assessment between the two review authors by discussion. We assessed the likely magnitude and direction of the bias on the findings.
Measures of treatment effect
If possible, we presented continuous outcomes with mean difference and standard deviations. When studies had measured the same outcome using different instruments or scales, we considered combining the outcomes using the standardised mean difference. We did not consider any of the outcomes to be appropriate for such a combination. For dichotomous outcomes, where available from RCTs, cluster‐RCTs, NRCTs, and CBA studies, we intended to present the number of events and number of people in groups as proportions and if appropriate, express effect as relative risk ratio (RR) or odds ratio (OR) with 95% confidence intervals (CIs).
For ITS studies, we present the effect as the difference between the expected value at a given point in time based on the pre‐intervention trend and the expected value at the same point in time based on the postintervention trend. We contacted authors of Kennedy 2013, who provided the original data set for re‐analysis as an ITS for this review as described in EPOC 2013.
We present results from randomised studies, non‐randomised studies and ITS separately, as recommended (Higgins 2011). We present the follow‐up according to our predefined categories: short‐term (< six months) and long‐term ( ≥ six months) follow‐up. Where study authors report several follow‐up times from the same study, we present the longest follow‐up.
Unit of analysis issues
Unit of analysis error can occur if trials based on group allocation to treatment condition (cluster‐RCTs, NRCTs, and CBA studies) have not accounted for the effect of clustering in the statistical analyses. The included cluster‐RCT by Boyd 1998 did not adjust the results for the effect of clustering, while Jih 2016 did. We did not have sufficient information to re‐analyse the data by Boyd 1998. See Appendix 2 for the methods we intended to use.
Dealing with missing data
We consider that incomplete or missing data was not a problem in any of the included studies and thus did not contact any of the authors for such information. See Appendix 2 for the methods we intended to use.
Assessment of heterogeneity
We did not combine data in meta‐analysis and hence did not assess heterogeneity in the results. See Appendix 2 for the methods we intended to use.
Assessment of reporting biases
We planned to generate funnel plots if 10 or more studies reported the same outcome. See Appendix 2 for the methods we intended to use.
Data synthesis
We categorised the included studies according to the intervention, measures and comparisons made. We assessed results for each comparison and collated them separately. If population, study design, intervention, and outcome measures had been similar enough across studies, we could have conducted meta‐analyses using Review Manager 5 (RevMan) software (RevMan 2014). One comparison had only one included study. Otherwise, the interventions, outcome measurements, or study designs differed in ways that did not support meta‐analyses. We based our judgements on the recommendations in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We considered that one outcome had sufficiently homogeneous populations, interventions, and comparisons to consider a pooled risk ratio, but only one of these two studies reported a measurement of dispersion in the published paper. See Appendix 2 for the methods we intended to use for meta‐analyses. Since meta‐analysis was not appropriate, we present descriptive data in text and tables. Authors of Kennedy 2013 provided data so we could re‐analyse these results as an ITS through segmented time series regression (Ramsay 2003).
Subgroup analysis and investigation of heterogeneity
The included studies did not provide sufficient data for subgroup analyses or investigation of heterogeneity. See Appendix 2 for the methods we intended to use and planned subgroups.
Sensitivity analysis
We intended to perform a sensitivity analysis excluding studies at high risk of bias if there had been a sufficient number of included studies; see Appendix 2.
Summary of findings table
We present the main outcome measures in a 'Summary of findings' table, along with our assessment of the certainty of effect for each outcome using the GRADE methodology (Guyatt 2011). Using GRADE, we reflect on the extent to which we have confidence that the estimates of effect are correct. Our confidence is presented as either high, moderate, low or very low quality evidence. We assess the results for each outcome measure against eight criteria. We consider the first five criteria for possible downgrading of the quality of documentation: study quality (risk of bias), consistency (consistency between studies), directness (the same study participants, intervention, comparator and outcome measures in included studies for the population, measures and outcomes we wanted to study), precision of results, and reporting biases. Results can be upgraded by three criteria: strong or very strong associations between intervention and outcome; large or very large dose‐response effect; and situations where all plausible confounders would have reduced the effect.
Results
Description of studies
See: Characteristics of included studies; Characteristics of excluded studies.
Results of the search
Searches in the electronic databases identified 12,762 unique records (see Figure 2: Study flow diagram). We discovered six additional records through other sources. Based on screening of titles and abstracts, we excluded 12,636 records and retrieved the full text of 132 articles, excluding 124. Six studies (8 articles) were eligible for this review. We did not identify any ongoing studies.

Study flow diagram.
Included studies
Of the included studies, three were individual RCTs (Elder 2005; Webb 2009; Risica 2013), and two were cluster‐RCTs (Boyd 1998; Jih 2016). We obtained the original data from the authors of Kennedy 2013 and were able to re‐analyse this study as an ITS. All of the studies took place in the USA and were published between 1998 and 2016. In four studies, the interventions targeted groups self‐described as Americans of African heritage (Boyd 1998; Webb 2009; Kennedy 2013; Risica 2013), while Elder 2005 targeted Spanish‐language‐dominant Latino immigrants (95% born in Mexico), and Jih 2016, elderly people of Chinese ethnicity (predominantly foreign‐born). Three studies targeted women only (Elder 2005; Kennedy 2013; Risica 2013). In Boyd 1998 and Kennedy 2013, the entire populations of geographically defined areas were potentially exposed to the targeted mass media intervention. The objectives of the interventions were to promote smoking cessation (Boyd 1998; Webb 2009; Kennedy 2013); to encourage dietary changes (particularly regarding fibre and fat intake) (Elder 2005); to promote weight management through modifications to diet and physical activity (Risica 2013); or to increase vegetable intake, fruit intake, and physical activity levels to meet guidelines (Jih 2016). None of the studies examined alcohol intake.
Webb 2009 recruited 261 African American adults who were randomised to receive either a culturally specific smoking cessation booklet or a booklet intended for the general population. The booklet in the intervention arm was culturally adapted using values, communication patterns, statistics, pictures, and other elements considered relevant for the targeted population, and it contained information about smoking and quitting strategies. The booklet used for the control group was identical in format and content and was developed by removing any references to a specific population group and using more general information and graphics.
In Boyd 1998 and Kennedy 2013, the intervention consisted of paid radio advisements, and in Boyd 1998, also some television advertisements, aired repeatedly in two waves that varied from three to six weeks in length. Both studies also included substantial distributions of posters, flyers, and other types of small media. The investigators targeted African American communities by adapting their message, language, and format to the assumed preferences of the group and by user‐testing the intervention with the target population. Advertisements were aired through media channels popular with the target audience or placed in relevant residential areas. The comparator in both studies was no intervention. The main message was to quit smoking and to make use of free telephone smoking cessation information or counselling (quit lines). Calls to this service were also the studies' outcome measurement. Since these studies exposed whole populations to the intervention, the study populations were not fixed. Boyd 1998's targeted mass media intervention was run in seven communities (estimated 310,471 African American smokers), compared to no intervention in seven communities (estimated 331,360 African American smokers). The size of Kennedy 2013's target population was indicated by the 400 births per month among African American women in the catchment area and survey results showing that approximately 40% of pregnant women in this population group were recent smokers.
The study by Risica 2013 gave study participants access to 12, one‐hour live programmes on cable TV over three months, biweekly mailings with printed material corresponding to the shows and, afterwards, four monthly mailings with written material and booster videotapes. The material was culturally adapted based on formative research on the target population. The TV shows had African American female casts, including all experts used. The shows and material contained educational content regarding nutrition and physical activity to improve health and control weight. In total, 71 women received this targeted intervention compared to 82 women on a wait‐list control until the study ended. Another 214 women received both this targeted intervention and the opportunity to engage in personal contact with study staff, either access to a toll‐free number they could use to ask questions during the live‐sharing segments of the shows, and/or weekly telephone support calls with outreach educators. Thus, this study compared the targeted mass media intervention with both a no‐intervention control group and a group receiving the mass media intervention with additional personalised content.
The target mass media intervention in Elder 2005 comprised newsletters in Spanish, mailed to the participants' home (119 women). The targeted newsletters and activity inserts were based on off‐the‐shelf information material developed for the Latino population and contained suggested strategies to change food purchasing, food preparation, and food consumption to reduce the risk of NCDs. This targeted intervention was compared to personalised newsletters and activity inserts in Spanish that were based on baseline questionnaires and specified personal goals. The personalised newsletters (118 women) otherwise focused on the same dietary messages as the targeted materials. A third intervention group (120 women) received both the personalised newsletters and 12 weekly visits by a Spanish‐speeking lay health worker (LHW, called promotora) who reinforced the dietary messages. Similarly, Jih 2016 compared targeted lecture handouts and brochures in 357 participants to the same material delivered through two small‐group, LHW‐facilitated lectures in 361 participants. The main aim was to increase fruit and vegetable intake and physical activity levels to meet guidelines. The researchers developed the lectures and materials using culturally appropriate examples of common foods, relevant physical activities and familiar portion size models for the target group. The lectures were presented in the participants' preferred language (Cantonese, Mandarin, or English).
Figure 3 presents an overview of the strategies that the included studies used to adapt their interventions to the target populations. The strategies are categorised according to the logic model (Figure 1). All of the studies made adaptations to modify message appropriateness, including adapting the message to be culturally appropriate, using selected images or cultural expressions, user‐testing the intervention in the target group, or attempting to address unique barriers and facilitating factors for group change. Two campaigns were implemented in a real context and made adaptations to modify reach by using selected media channels, placing small media in residential areas, distributing outreach packets through community networks, and using people from the target group to convey the media content (Boyd 1998; Kennedy 2013). Two studies presented the mass media interventions in languages that differed from the dominant language of the country (Elder 2005, Jih 2016).

Approaches used in the included studies to target the intervention to the study population, by categories according to logic model.
Three of the included studies received support from the National Cancer Institute (USA) (Boyd 1998; Elder 2005; Risica 2013), and one received funding from both the National Institutes of Health and the National Cancer Institute (Jih 2016). The National Center on Minority Health Disparities, part of the National Institutes of Health (USA), supported Kennedy 2013, and Syracuse University (USA) funded Webb 2009.
Excluded studies
After screening the full texts, we excluded 124 articles (see Characteristics of excluded studies). The main reasons for exclusion were: no mass media intervention or combining the media various forms of personal interaction with the participants; not targeting the intervention to ethnic minorities; or not meeting the inclusion criteria with respect to study design.
Risk of bias in included studies
The Characteristics of included studies table assesses the risk of bias and provides comments for each of the included studies. We used the study‐appropriate risk of bias domains as developed by EPOC 2015, which proposes different domains for assessing ITS studies and the other study designs included in this review. The risk of bias assessment for the ITS study is discussed under the section Other potential sources of bias. Figure 4 and Figure 5 summarise the 'Risk of bias' assessments. These figures present all domains used for both the ITS study and the other study designs but are only filled in for the appropriate categories for each study.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
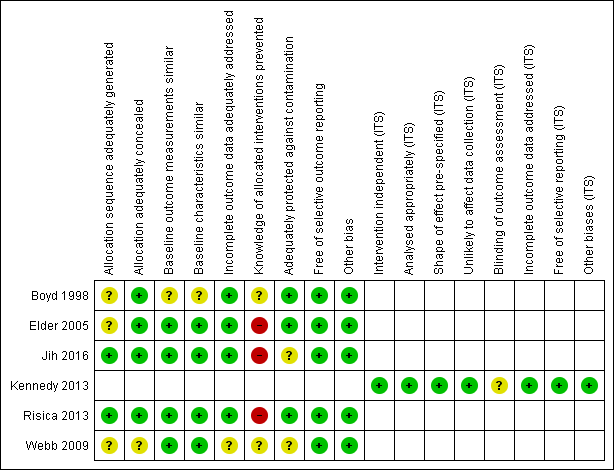
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Two studies reported adequate methods for random sequence allocation (Risica 2013; Jih 2016). Otherwise, the allocation method described in the papers was unclear. We also considered that the method used for allocation concealment in Webb 2009 was at unclear risk of bias. Four studies presented data showing that the groups were similar at baseline with regard to the outcome variables and the participant characteristics (Elder 2005; Webb 2009; Risica 2013; Jih 2016). In Boyd 1998, the communities were matched on selected characteristics before randomisation, but based on the published descriptions we found the distribution of the baseline characteristics to be unclear.
Blinding
It can be difficult to achieve blinding in studies intending to change behaviours. Since most or all the outcomes in Elder 2005, Risica 2013, and Jih 2016 were self‐reported outcomes from non‐blinded studies, we considered these results to be at high risk of bias. In Webb 2009, participants in both study arms received a non‐blinded smoking cessation intervention; we could not tell whether the trial misreported any of the study outcomes with unequal distribution between the groups. Kennedy 2013 reported on a whole‐population mass media campaign, and we considered it to be unclear whether knowledge of the allocated intervention was adequately prevented during the study and in what way this may have biased the findings.
Incomplete outcome data
Loss to follow‐up was unaccounted for in Webb 2009, so we consider the risk of bias to be unclear.
Selective reporting
We found no published study protocols for any of the studies but considered the risk for selective reporting of outcomes to be low in all the studies. This conclusion is based on descriptions in the Methods, expected outcomes reported, and corresponding presentations of results.
Other potential sources of bias
We considered the included studies to be at low risk of other biases.
We re‐analysed Kennedy 2013 as an ITS for this systematic review using the methodology described above. We noted that the second wave of advertisements coincided with a known seasonal increase in call volume and therefore excluded these data from the re‐analysis. We considered the remaining results, as re‐analysed according to the EPOC methods for ITS studies, to be at low risk of bias in all domains except one. As with the study by Boyd 1998, it was unclear whether knowledge of the allocated intervention in Kennedy 2013 (whole population mass media campaign) was adequately prevented during the study and in what way this may have biased the findings.
Effects of interventions
See: Summary of findings for the main comparison Targeted mass media intervention versus general population mass media intervention for promoting healthy behaviours; Summary of findings 2 Targeted mass media intervention for promoting healthy behaviours versus no intervention; Summary of findings 3 Targeted mass media intervention versus targeted mass media intervention plus personalised content
Comparison 1: targeted mass media intervention versus general population mass media intervention
See: summary of findings Table for the main comparison.
Only one study assessed the effect of a targeted mass media intervention versus a mass media intervention intended for the general population (Webb 2009).
Primary outcomes
Webb 2009 did not assess any outcomes using indicators of behavioural change but reported several self‐reported measures, including smoking reduction, attempts to quit, 24‐hour point prevalence abstinence and 7‐day point prevalence abstinence. The authors report that they found no significant difference in smoking reduction between the two conditions at the three‐month follow‐up (94% and 95% reported smoking reduction; adjusted OR for quit attempts was 1.97 (95% CI 1.09 to 3.55) in favour of the general population mass media intervention). Knowledge and attitudes toward change were reported as readiness to quit, measured by a 10‐point contemplation ladder (1: no thoughts of quitting; 10: taking action to quit). The mean score was higher in participants who received the mass media intervention intended for the general population compared to the targeted mass media intervention (8.2 points, SD 2.4 versus 7.3 points, SD 2.6, P = 0.01). We considered all effect estimates of these self‐reported behavioural outcome measures to be very low quality evidence as assessed by the GRADE methodology.
Secondary outcomes
The included study did not assess any outcomes on the use of health promotion services or costs of the project.
Adverse outcomes
The included study did not assess any variables measuring adverse outcomes.
Comparison 2: targeted mass media intervention versus no intervention
See: summary of findings Table 2.
Three studies compared targeted mass media interventions versus no intervention (Boyd 1998; Kennedy 2013; Risica 2013). We could not pool the findings due to differences in outcome measurements and study designs.
Primary outcome
Only one of the included studies reported any of our primary outcomes (Risica 2013). These were: BMI (kg/m2) as an indicator of behavioural change and self‐reported behavioural change using a Food Habits Questionnaire (fat behaviour score) and total leisure activity questionnaire. The included study did not assess knowledge or attitudes toward change.
Changes in BMI were comparable in the two groups 12 months after baseline (longest follow‐up, mean difference in change 0.1 kg/m2, 95% CI −0.4 to 0.6). Fat behaviour scores (no unit described, high scores reflecting high fat intake) were lower in participants who received the targeted mass media intervention compared to the no intervention control group at 12 months (longest follow‐up, mean difference in change −0.2, 95% CI −0.3 to −0.1), while total leisure activity score (no unit described, high scores reflecting more activity) was higher in the intervention group (longest follow‐up, mean difference in change 12.0, 95% CI 1.0 to 23.0). We considered the effect measures based on the outcome BMI to be low quality evidence and the self‐reported behavioural changes to be very low quality evidence.
Secondary outcomes
Two studies reported our secondary outcome: use of health promotion services – in both cases as the number of calls to smoking quit lines (Boyd 1998; Kennedy 2013). During the year of the campaign by Boyd 1998, the quit lines received 558 calls from African American smokers residing in the intervention communities (18 calls per estimated 10,000 African American smokers) compared to 7 calls in the control communities (0.2 calls per estimated 10,000 African American smokers). The proportion of calls from African Americans was 82% of the total number in the experimental communities compared to 26% in the control communities (no measure of dispersion reported). Calls peaked significantly during waves of intense media coverage. We present the re‐analysis of Kennedy 2013 as an ITS for this systematic review in Table 1. During the first and the last month of the campaign, the number of calls from new pregnant women increased by 8 per month (95% CI 1 to 14) over pre‐campaign call rates. Compared to the pre‐campaign monthly call rate, the number was 6 more calls (95% CI −1 to 12) in the first month after the campaign and 3 more calls (95% CI −4 to 10) four months after. The proportion of calls from African American women was 86% during the campaign, compared to 41% before the campaign and 28% after (no measure of dispersion reported). We considered the overall results measured as changes in call volume overall to be moderate quality evidence based on results from the RCT and low quality evidence from the ITS. The change in the proportion of calls from the target population provided low and very low quality evidence from the two respective studies.
| Outcome | Estimated effect (95% CI)a July 2009 (start of campaign) | Estimated effect October 2009 (last month of campaign) | Estimated effect November 2009 (first month after campaign) | Estimated effect March 2010 (4 months after campaign) |
| Total number of calls | 42 (−115 to 198) | 153 (−8 to 314) | 146 (−13 to 304) | 32 (−148 to 212) |
| Calls from pregnant women | 14 (4 to 25) | 15 (4 to 27) | 8 (−3 to 19) | 7 (−5 to 20) |
| Calls from unique pregnant women | 8 (1 to 14) | 8 (1 to 14) | 6 (−1 to 12) | 3 (−4 to 10) |
| Calls from unique previously unknown pregnant women ('first‐timers') | 6 (1 to 11) | 6 (1 to 10) | 2 (−3 to 6) | 3 (−3 to 8) |
aChange from pre‐campaign call rates.
Kennedy 2013 and Risica 2013 did not report the costs of their projects. Boyd 1998 reported the costs to be USD 106,821 for radio advertisements and USD 6744 for television advertisements but did not mention other costs or required resources overall.
Adverse outcomes
The included studies did not assess any variables measuring adverse outcomes.
Comparison 3: targeted mass media intervention versus targeted media intervention plus personalised content
See: summary of findings Table 3.
Comparison 3 examined targeted mass media interventions versus targeted media interventions plus personalised content and included data from three studies (Elder 2005; Risica 2013; Jih 2016). Elder 2005 compared a targeted mass media intervention (newsletters based on off‐the‐shelf targeted material) with two intervention arms categorised as media intervention plus personalised content: one arm received individually tailored newsletters, and the other arm received individually tailored newsletters followed by home visits. Risica 2013 had three intervention arms that we categorised as media intervention plus personalised content. The authors reported incomplete delivery of the interactive programme sessions and support calls in these intervention arms; therefore, tor the purpose of this systematic review, we combined the results of these three intervention arms into a single comparison group. Jih 2016 compared a targeted mass media intervention (targeted print material) with a mass media intervention plus personalised content (lectures).
Primary outcomes
Elder 2005 and Risica 2013 reported BMI an as indicator of behavioural change at 3 months and Risica 2013 also at 12 months from baseline. Neither reported any difference in BMI change over time. Mean difference in change between the groups 12 months after baseline was 0.4 kg/m2 (95% CI −0.1 to 0.8) between groups. All three included studies assessed self‐reported behavioural changes. At three months, participants in Jih 2016 who received media interventions plus personalised content had higher odds of adhering to guidelines on vegetable intake than participants who received targeted mass media alone (adjusted OR 5.53, 95% CI 1.96 to 15.58), but there was no difference for fruit intake (adjusted OR 1.77, 95% CI 0.99 to 3.15). Risica 2013 assessed self‐reported behavioural changes using a Food Habits Questionnaire (fat behaviour score) and a total leisure activity questionnaire, as above, while Elder 2005 used a 24‐hour dietary recall interview. Their papers present results for several nutrients and groupings, but in this review we present only the authors' main outcomes: percentage of calories from fat and total dietary fibre (g). Elder 2005 reported no significant differences (P > 0.05) at the end of the intervention between the tailored intervention group and the two comparison groups for either percentage of calories from fat (30.0%, 30.4%, and 29.3%; no measure of dispersion reported) or total dietary fibre (15.6 g, 17.2 g, and 16.1 g; no measure of dispersion reported). In Risica 2013, the participants who received only the targeted mass media intervention had somewhat larger reductions in fat behaviours scores (no unit described, high scores reflecting high fat intake, mean difference in change −0.1, 95% CI −0.2 to −0.02) and greater increases in total leisure activity score (no unit described, high scores reflecting more activity, mean difference in change 12.9, 95% CI 3.5 to 22.3) compared to the groups with additional personalised components after 12 months. In Jih 2016, results indicated no difference in weekly physical activity meeting guidelines (adjusted OR 1.27, 95% CI 0.89 to 1.80). The same study indicated that more participants receiving personalised content had increased knowledge of nutrition guidelines than participants receiving the targeted mass media alone (knowledge of guideline for vegetables, adjusted OR 12.6, 95% CI 6.5 to 24.5, and fruit, adjusted OR 16.2, 95% CI 5.6 to 46.5), but this finding did not hold for knowledge of physical activity guidelines (adjusted OR 2.70, 95% CI 0.31 to 23.2).
We considered the effect measures based on the outcome BMI to be low quality evidence and all self‐reported behavioural changes and knowledge of guidelines to be very low quality evidence.
Secondary outcomes
The included studies did not assess any outcomes concerning the use of health promotion services. Elder 2005 reported that the costs per participant in the three intervention arms were USD 9.00 for targeted newsletters, USD 45.00 individually tailored newsletters, and USD 135 for individually tailored newsletters followed by home visits. Jih 2016 and Risica 2013 did not report project costs.
Adverse outcomes
The included studies did not assess any variables considered adverse outcomes.
Discussion
Summary of main results
Six studies met the inclusion criteria: three RCTs, two cluster‐RCTs, and one ITS. All took place in the USA and consisted of mass media interventions targeting either African Americans (4 studies), Spanish‐language‐dominant Latino immigrants (1 study) or Chinese immigrants (1 study). Furthermore, three targeted women only, and one specifically targeted pregnant women. The interventions addressed physical activity, dietary patterns, or tobacco use, but none addressed alcohol consumption. The studies were diverse with respect to the comparisons made, the outcomes and the study designs. We did not pool data for meta‐analyses.
We categorised the comparisons into three groups: a targeted mass media intervention versus a general mass media intervention; a targeted mass media intervention versus no intervention; and a targeted mass media intervention versus a media intervention plus personalised content.
Only one study compared the relative effects of a culturally targeted mass media intervention and a general mass media intervention on smoking behaviours. The results were inconclusive.
Two studies compared the relative effects of a targeted mass media intervention versus no intervention. The findings suggested that, compared to no intervention, the targeted mass media intervention possibly produced small, short‐term shifts in physical activity and dietary patterns and probably increased calls to smoking quit lines.
Three studies compared a targeted mass media intervention versus a media intervention combined with personalised content. Overall, the results of these studies were too uncertain to conclude whether there were differences between groups with respect to weight changes, dietary changes, or physical activity. Most of the outcomes had either small effects or inconclusive confidence intervals, and the evidence of effect was low to very low quality.
Overall completeness and applicability of evidence
Given the widespread interest in mass media interventions targeting ethnic minority populations with health‐promoting messages regarding physical activity, dietary patterns, tobacco use, or alcohol consumption, the number of relevant studies was small. Only one study, Webb 2009, directly compared the effect of a culturally targeted mass media intervention with the effect of a general mass media intervention using the same format (i.e. smoking cessation advice and general content). The targeting did not involve any change in language use. In the included study, the delivery methods and, therefore, the expected reach were the same between groups. Although this comparison focuses on the value and effectiveness of targeting strategies on their own, the included study only assessed the value of targeting through cultural adaptation. The study was inconclusive regarding the differential effects on smoking behaviours and attitudes. We have very little confidence in the effect estimates and believe that any true effect could be substantially different from the authors' reports. Thus, the evidence is insufficient to conclude whether targeted mass media interventions are more effective than mass media interventions intended for the general population in changing health behaviours among ethnic minority groups.
When comparing the effects of targeted mass media interventions versus no interventions, findings from two large campaigns showed that these probably produce a considerable response, as measured by a surrogate outcome: the use of health promotion services in the form of smoking quit lines (Boyd 1998; Kennedy 2013). These studies did not measure changes in actual smoking behaviours. Calling a smoking quit line may not lead to an actual change in smoking habits or to long‐term smoking cessation. Population‐wide campaigns, such as those reported here (Boyd 1998; Kennedy 2013), may, however, contribute to population changes in attitudes toward smoking, intentions to quit, self‐administered attempts to quit, or use of other health services offering smoking cessation support, thereby providing additional effects through the measured outcomes. Self‐reported changes in behaviours are, when sustained, important outcomes in causal pathways (see Figure 1); however, they are not the ultimate aim, which is to improve health status and decrease the mortality and morbidity of NCDs. The one study in this comparison that measured a physiological indicator of change (BMI), using self‐reported changes in dietary patterns and physical activity, found small effects in the expected direction after three months (the end of the main intervention). The longer‐term effects were more uncertain (Risica 2013). It should be noted that this targeted mass media intervention was relatively high‐intensity, comprising 12, one‐hour live cable TV programmes over three months, with additional mailings over an extended period. The measured effect size was relatively small, and we have low to very low confidence in the effect estimates.
All three studies in this comparison targeted population groups with the same native language as the general population. During the campaigns, these studies also registered smaller or larger increases in call rates in non‐targeted population groups (Boyd 1998; Kennedy 2013). However, the relative shifts in the proportions of callers, as well as the increases in total numbers of calls from the target populations, still indicate that these interventions had specific effects on the intended population group. These results cannot distinguish whether higher responses by the target population were due to the targeting of media content and format, better reach through the targeting of media channels, or both.
Overall, the three studies comparing a targeted mass media intervention with a media intervention plus personalised content were inconclusive (Elder 2005; Jih 2016; Risica 2013). It could be expected that person‐tailored or one‐to‐one intervention content would produce a better response than a mass media intervention alone. In two of these studies (Elder 2005; Risica 2013), all study arms had a relatively high exposure to the intervention, with at least 12 deliveries of mass media content over an extended period. Thus, the intervention groups may not have been sufficiently different to constitute a meaningful comparison.
All six studies in this systematic review were conducted in the USA, and four targeted African American population groups. Only two studies examined the effect of a targeted mass media intervention in a population group with a first language that differed from the national language (Spanish‐dominant Latino immigrants and Chinese immigrants). The current evidence is therefore very limited with respect to different ethnic groups and contexts beyond the USA. Additionally, the cultural gap between the populations considered minorities and majorities may be more or less wide. All of the studies adapted their interventions to the target group by culturally customising the content or format (Figure 3). It is unclear to what extent these adaptations also considered other relevant factors that may characterise the target group, such as gender or socioeconomic status related to income, education, health literacy level, living conditions, or other resources available to the target population. The transferability of the results from this review must be considered for each context specifically.
None of the studies reported or discussed possible adverse effects of the intervention. A targeted mass media intervention can be a means to provide ethnic minority groups with equal opportunities and resources to access information, life skills, and opportunities for making healthier choices; however, by treating the target group differently, targeted efforts may also create a stigma. Drawing attention to the need for additional public health efforts directed toward a particular population subgroup may, in some situations, be considered or experienced as discrimination (Nayar 2014). Different population segments may also experience public health efforts to change personal behaviours as more or less intrusive or unacceptable to their rights to personal freedom. None of the included studies reported resistance to the message or other possible adverse effects as outcomes.
Targeted interventions are considered to be more expensive; however, this may not be universally true. Though the production of a targeted intervention or several adapted versions of the same intervention for different population groups may increase programme costs, the budget upside of a targeted intervention may be the need for fewer or potentially less costly media channels to reach the target group. Furthermore, new digital media channels have significantly changed the picture of media costs. This can make it easier to target specific groups at a low cost, but the new diversity in media markets can also create more 'noise' and increase reach dispersion. Overall, research still needs to explore the cost aspects of targeted interventions.
Quality of the evidence
In the GRADE assessments for the domain 'directness' (Guyatt 2011), we considered the studies directly relevant to the inclusion criteria. Thus, we did not downgrade quality for this domain. The population of interest, and therefore also the directness of these findings, will be dissimilar in different contexts, relating to characteristics of the ethnic minority group, the country, and the overall setting.
Based on the GRADE methodology (Guyatt 2011), we have moderate confidence in the estimated short‐term increase in the number of calls to smoking quit lines. The cluster‐RCT reporting this outcome did not provide measures of dispersion or adjust for effects of the cluster‐randomised design (Boyd 1998). Failing to adjust for cluster effects will overestimate the precision of the effect estimate. However, the study reported a large effect, and additional results from the ITS study had similar conclusions (Kennedy 2013). Otherwise, our confidence in the described effect sizes ranged from low to very low. A low to very low confidence in the evidence means that the true effect can be either different or substantially different from the numbers presented in this review.
Potential biases in the review process
In this review, we focused on the effect of targeted mass media interventions on their own. This means that we have excluded targeted mass media interventions that were combined with any form of personal interaction or feedback (including digital feedback), group sessions, or changes in available resources. We also excluded studies in which a mass media component was part of a complex community intervention involving many intervention activities across several institutions. The only exceptions were studies in which this type of complex intervention served as a comparator for a targeted mass media intervention alone (Elder 2005; Risica 2013; Jih 2016). A boundary that we found difficult to operationalise was the distinction between a mass media intervention and a self‐help programme. We included Webb 2009, where the intervention was a smoking cessation booklet, while we excluded more extensive self‐help programmes with teaching modules and worksheets.
Inclusion criteria regarding study design were based on recommendations from the EPOC group (EPOC 2016). These criteria are well reasoned and include several different study designs but are slightly narrower than those used in other Cochrane Reviews on mass media interventions for smoking cessation. We excluded a few studies that Bala 2013 included, as we used different inclusion criteria regarding study designs; however, we believe that the inclusion of their studies would not have altered our conclusions.
Agreements and disagreements with other studies or reviews
We have not found any other systematic reviews regarding the specific effects of mass media interventions targeting adult ethnic minorities with health promotion messages. One mixed‐methods evidence synthesis identified and assessed the effects of adapted health promotion interventions for ethnic minority populations of African, Chinese, and South Asian origin (Liu 2012). They identified only nine studies (among them Webb 2009, included in our review) directly comparing a culturally adapted health promotion intervention with a standard intervention of equal format, intensity and content. The included studies did not indicate any tendency toward increased effectiveness for culturally adapted interventions. The studies were either inconclusive (k = 5) or found increased effectiveness in the opposite direction of the hypothesis on some outcome variables (k = 3). Only one study found increased effectiveness of the culturally adapted intervention over the standard intervention. All nine studies were conducted in the USA, and eight targeted African Americans. The review authors of Liu 2012 considered that most studies considered in the evidence synthesis were inappropriately designed to establish the effectiveness of the cultural adaptations. Another Cochrane Review, focusing on culturally appropriate health education for people in ethnic minority groups with type 2 diabetes mellitus, found that such education likely improves glycaemic control compared to standard diabetes care. Here, the contexts and the targeted ethnic minority groups were more variable, including several studies of programmes targeting immigrants. Many of the diabetes education programmes in that review were more comprehensive than their standard care counterparts in terms of counselling frequency, personal interaction, and other intervention components (Attridge 2014). Another review found that cultural adaptations resulting in higher‐intensity health promotion interventions appeared to be more effective (Nierkens 2013). However, these reviews also failed to scrutinise the specific effect of the cultural adaptations to the ethnic minority group. Reviews and guidelines increasingly acknowledge ethnic health inequalities and the possibility of differential effects of health promotion interventions (Davidson 2013a). Recommended adaptation strategies can be derived based on current strategies in use; however, there is still little evidence regarding which health promotion interventions are effective for ethnic minority populations (Davidson 2013b).
Of the studies included in our review, three compared targeted mass media interventions to no intervention. Their findings contribute more to the general evidence regarding the effectiveness of mass media interventions addressing health behaviours to reduce the risk of NCDs. In two of the included studies, the interventions were mass media campaigns for smoking cessation. The effectiveness of mass media interventions for smoking cessation is also addressed in two Cochrane Reviews: Bala 2013 in adults and Brinn 2010 in young people (up to age 25). These conclude that there is evidence of some positive effect of these interventions on smoking behaviours, at least in the short term.


Study flow diagram.

Approaches used in the included studies to target the intervention to the study population, by categories according to logic model.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
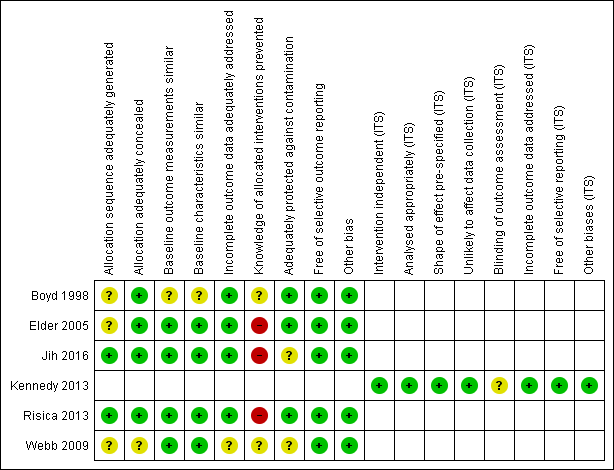
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
| Comparison 1: targeted mass media intervention versus general population mass media intervention for promoting healthy behaviours | ||||||
| Patient or population: adult, ethnic minority: self‐described Americans of African heritage | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | N of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| General population mass media intervention | Targeted mass media intervention | |||||
| Indicators of behavioural change | ||||||
| Any outcome considered an indicator of change | No study provided data for this outcome. | |||||
| Self‐reported behavioural change | ||||||
| Proportion smoking reduction, 3 months follow‐up | 94% | 95% | — | 255 | ⊕⊝⊝⊝ | No effect measures reported by authors. Not significantly different between groups |
| Quit‐attempts, 3 months follow‐up | — | — | Adjusted OR 1.97 (1.09 to 3.55) in favour of general population mass media intervention | 255 | ⊕⊝⊝⊝ | 24‐hour and 7‐day point prevalence abstinence not significantly different between groups |
| Knowledge and attitudes to change | ||||||
| Contemplation ladder to quit smoking (1‐10), 3 months follow‐up | Mean score: 8.2 (SD 2.4) | Mean score: 7.3 (SD 2.6) | — | 255 (1 RCT) | ⊕⊝⊝⊝ | Difference between group reported at P = 0.01 |
| Adverse effects | ||||||
| Any outcome considered an adverse effect | No study provided data for this outcome. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) | ||||||
| GRADE Working Group grades of evidence | ||||||
| aIn the GRADE assessments for the domain 'directness', we considered the studies directly relevant to the inclusion criteria. Thus, we have not downgraded on this domain. However, the population of interest will be dissimilar in different contexts, relating to characteristics of the ethnic minority group, the country and setting overall. The transferability of results must be considered for each context specifically. | ||||||
| Comparison 2: targeted mass media intervention for promoting healthy behaviours versus no intervention | ||||||
| Patient or population: adult, ethnic minority group: self‐described Americans of African heritage | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | N of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| No intervention | Targeted mass media intervention | |||||
| Indicators of behavioural change | ||||||
| BMI (kg/m2), 12 months from baseline | 34.4 (SD 8.5)b | Mean difference in change 0.1 (−0.4 to 0.6) | — | 154 | ⊕⊕⊝⊝ | Corresponding risk at 3 months: mean difference in change −0.4 (−0.7 to −0.02) |
| Self‐reported behavioural change | ||||||
| Changes in dietary composition, 12 months from baseline | Food habits questionnaire, score on fat behaviours (no scoring scale provided by study authors): 1.0 (SD 0.4) | Mean difference in change −0.2 (−0.3 to ‐0.1) | — | 154 (1 RCT) | ⊕⊝⊝⊝ | Corresponding risk at 3 months: mean difference in change −0.1 (−0.2 to −0.02) |
| Leisure time physical activity, 12 months from baseline | Physical activity score (no scoring scale provided by study authors): 60.0 (SD 47.0)e | Mean difference in change 12.0 (1.0 to 23.0) | — | 154 (1 RCT) | ⊕⊝⊝⊝ | Corresponding risk at 3 months: mean difference in change 10.0 (−1.7 to 21.8) |
| Knowledge and attitudes to change | ||||||
| Any measure of knowledge and attitude | No study provided data for this outcome. | |||||
| Adverse effects | ||||||
| Any outcome considered an adverse effect | No study provided data for this outcome. | |||||
| Use of health promotion services (secondary outcome) | ||||||
| Calls to smoking quit lines, during campaign | 18 calls per estimated 10,000 African American smokers in the intervention group versus 0.2 calls in the control communitiesf. | Estimated target population 641,800 (1 RCT) | ⊕⊕⊕⊝ | — | ||
| Calls to smoking quit lines, during and after campaign | Change from pre‐campaign, calls per month (95% CI) from new pregnant smokers: 8 (1 to 14) first month of campaign, 8 (1 to 14) last month of campaign, 6 (−1 to 12) first month after campaign, 3 (−4 to 10) 4 months after campaign | Population in target city ˜300,000 (1 ITS) | ⊕⊕⊝⊝ | — | ||
| Proportion of calls from target population during campaign | Proportion of calls from African Americans during trial: 82% in intervention and 26% in control communities | Estimated target population 641,800 (1 RCT) | ⊕⊕⊝⊝ | — | ||
| Proportion of calls from target population during and after campaign | Proportion African Americans among pregnant callers: 41% before campaign, 86% during the campaign, 28% after campaign | Population in target city ˜300,000 (1 ITS) | ⊕⊝⊝⊝ | — | ||
| Costs of the project (secondary outcome) | ||||||
| Programme costs | USD 106,821 for radio advertisements and USD 6744 for television advertisements. No overall costs reported | Estimated target population 641,800 (1 RCT) | ⊕⊕⊝⊝ | — | ||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aIn the GRADE assessments for the domain 'directness', we considered the studies directly relevant to the inclusion criteria. Thus, we have not downgraded on this domain. However, the population of interest will be dissimilar in different contexts, relating to characteristics of the ethnic minority group, the country and setting overall. The transferability of results must be considered for each context specifically. | ||||||
| Comparison 3: targeted mass media intervention versus targeted mass media intervention plus personalised content | ||||||
| Patient or population: adult, ethnic minority groups: Latino immigrants, elderly Chinese immigrants, self‐described Americans of African heritage | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | N of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Media intervention with personalised content (comparison) | Targeted mass media intervention | |||||
| Indicators of behavioural change | ||||||
| BMI (kg/m2), 12 months from baseline | 34.9 (SD 7.7)b | Mean difference in change 0.4 (−0.1 to 0.8) | — | 286 | ⊕⊕⊝⊝ | Two RCTs (643 participants) reported BMI at 3 months. None found significant differences in weight change between study groups |
| Self‐reported behavioural change | ||||||
| Intake meeting target from dietary guidelines, 3 months from baseline | Vegetables: adjusted OR 5.53d (1.96 to 15.58) Fruit: adjusted OR 1.77d (0.99 to 3.15) | 718 (1 RCT) | ⊕⊝⊝⊝ | — | ||
| Changes in dietary composition, 12 months from baseline | Food habits questionnaire, score on fat behaviours (no scoring scale provided by study authors): 1.0 (SD 0.4)f | Mean difference in change −0.1 (−0.2 to −0.02) | — | 286 | ⊕⊝⊝⊝ | Two RCTs (643 participants) reported changes in dietary composition at 3 months. None found significant differences/mean difference in change for energy or dietary fibre intake (study 1) or food habits questionnaire (fat behaviours) (study 2) |
| Weekly physical activity meeting target from guidelines, 3 months from baseline | Adjusted OR 1.27d (0.89 to 1.80) | 718 (1 RCT) | ⊕⊝⊝⊝ | — | ||
| Leisure time physical activity, 12 months from baseline | Physical activity score (no scoring scale provided by study authors): 68.0 (47.6)f | Mean difference in change 12.9 (3.5 to 22.3) | — | 286 | ⊕⊝⊝⊝ | Corresponding risk at 3 months: mean difference in change −2.2 (−12.9 to 8.5) |
| Knowledge and attitudes to change | ||||||
| Knowledge of nutrition and physical activity guidelines | Daily vegetable intake: adjusted OR 12.6d (6.50 to 24.5) Daily fruit intake: adjusted OR 16.2d (5.61 to 46.5) Weekly physical activity: adjusted OR 2.70d (0.31 to 23.2) | ⊕⊝⊝⊝ | — | |||
| Adverse effects | ||||||
| Any outcome considered an adverse effect | No study provided data for this outcome. | |||||
| Costs of the project (secondary outcome) | ||||||
| Costs per person in each treatment arm | USD 9.00 for targeted newsletters, USD 45.00 individually tailored newsletters, and USD 135 for individually tailored newsletters followed by home visits | 357 | ⊕⊝⊝⊝ | — | ||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; RCT: randomised controlled trial;RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence | ||||||
| aIn the GRADE assessments for the domain 'directness', we considered the studies directly relevant to the inclusion criteria. Thus, we have not downgraded on this domain. However, the population of interest will be dissimilar in different contexts, relating to characteristics of the ethnic minority group, the country and setting overall. The transferability of results must be considered for each context specifically. | ||||||
| Outcome | Estimated effect (95% CI)a July 2009 (start of campaign) | Estimated effect October 2009 (last month of campaign) | Estimated effect November 2009 (first month after campaign) | Estimated effect March 2010 (4 months after campaign) |
| Total number of calls | 42 (−115 to 198) | 153 (−8 to 314) | 146 (−13 to 304) | 32 (−148 to 212) |
| Calls from pregnant women | 14 (4 to 25) | 15 (4 to 27) | 8 (−3 to 19) | 7 (−5 to 20) |
| Calls from unique pregnant women | 8 (1 to 14) | 8 (1 to 14) | 6 (−1 to 12) | 3 (−4 to 10) |
| Calls from unique previously unknown pregnant women ('first‐timers') | 6 (1 to 11) | 6 (1 to 10) | 2 (−3 to 6) | 3 (−3 to 8) |
| aChange from pre‐campaign call rates. | ||||