Edukacija pacijenata o kroničnoj nespecifičnoj križobolji
Referencias
References to studies included in this review
References to studies excluded from this review
References to studies awaiting assessment
References to ongoing studies
Additional references
References to other published versions of this review
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | RCT | |
| Participants | 57 participants. 1. Back School group n = 29. 2. Waiting‐list group n = 28. Inclusion criteria: non‐specific chronic low back pain for over 3 months, pain present during the study, and cognitive ability to sign the consent form. Exclusion criteria: pregnancy, disc herniation, infectious or inflammatory spondylitis, tumours, fractures, thoracic, shoulder, or neck pain, and fibromyalgia. | |
| Interventions | 1. Back School group: 4 sessions x 60 minutes in 4 weeks. Information on anatomy, causes of LBP, ergonomics, exercises, and advice on physical activity. 2. Waiting‐list group. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Disability: Roland‐Morris Disability Questionnaire. | |
| Notes | Secondary care setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were randomised using a system developed in Visual Basic into 2 groups: experimental (34 participants) and control (36 participants). |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title, abstract, and flowchart indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | Low risk | All participants were evaluated by the same examiner, who was blind to group allocation. |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | No information about intention‐to‐treat analysis |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Table I presents the data at baseline of the experimental and control groups, with no statistically significant difference between groups. |
| Co‐interventions avoided or similar? | Unclear risk | Not mentioned |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the reported intensity/dosage, duration, number, and frequency for both the intervention and control groups. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 224 participants. 1. Back School group n = 72. 2. Usual care group n = 74. 3. Compliance Package n = 76. Inclusion criteria: low back pain, age 21 to 55 years, no serious comorbidity, no prior surgery, at least 2 weeks pain, maximum 6 months pain, no specific illness causing back pain, no prior episode during the previous year. Exclusion criteria: pain characteristically extended below the level of the knee. | |
| Interventions | 1. Back School group: a single 4‐hour instruction session on LBP (psycho‐educational). 2. Usual care group: participants were sent a single short pamphlet on LBP. | |
| Outcomes | Pain: visual analogue scale. | |
| Notes | Primary care setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | The only significant difference that randomisation failed to prevent was on Sickness Impact Profile |
| Co‐interventions avoided or similar? | Low risk | Balanced for both groups |
| Compliance acceptable? | Unclear risk | Not mentioned |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 210 participants. 1. Back School n = 70. 2. Individual physiotherapy n = 70. 3. Spinal manipulation n = 70. Inclusion criteria: non‐specific low back pain, reported "often" to "always" for at least the past 6 months. Exclusion criteria: neurological signs or symptoms, spondylolisthesis 4 second degree, rheumatoid arthritis or spondylitis, previous vertebral fractures, psychiatric disease, cognitive impairment, or pain‐related litigation. | |
| Interventions | 1. Back School: 15 sessions x 1 hour for 3 weeks. The first 5 sessions were devoted to information and group discussions on back physiology and pathology, with reassurance on the benign character of common low back pain and education in ergonomics at home and in different occupational settings by slides and demonstrations. The next 10 sessions included relaxation techniques, postural and respiratory group exercises, and individually tailored back exercises. Each Back School group included 8 participants. *All participants received a booklet with evidence‐based, standardised educational information on basic back anatomy and biomechanics, optimal postures, ergonomics, and advice to stay active. 2. Individual physiotherapy: 15 sessions x 60 minutes for 3 weeks. Included passive and assisted mobilisation, active exercise, massage/treatment of the soft tissues, and proprioceptive neuromuscular facilitation, with emphasis on patient education and active treatment. 3. Spinal manipulation: 4 to 6 sessions (as needed) x 20 minutes for 4 to 6 weeks. Spinal manipulation given according to Manual Medicine. | |
| Outcomes | 1. Pain: Pain Rating Scale. 2. Disability: Roland‐Morris Disability Questionnaire. | |
| Notes | Setting not specified. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Simple (non‐restricted) randomisation led to some imbalances in participants' baseline characteristics. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | Low risk | The examiners were blinded to group assignment. |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | High risk | Analysis was substantially similar to the intention‐to‐treat analysis commonly adopted in reporting randomised trials due to the minimal dropout (5/210, 2.4%). |
| Selective reporting (reporting bias) | Low risk | It was clear that the published report includes all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | No significant difference across the groups was found. |
| Co‐interventions avoided or similar? | Low risk | Balanced for both groups |
| Compliance acceptable? | Unclear risk | There are not enough data. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 54 participants. 1. Back School group n = 27. 2. Hydrotherapy group n = 27. Inclusion criteria: participants aged between 65 and 80 years; diagnosis of chronic non‐specific low back pain. Exclusion criteria: presence of musculoskeletal disorders, severe heart failure, or internal medicine pathologies that could interfere with moderate physical activity; fever or infectious disease; systemic inflammatory or rheumatologic diseases; previous spinal surgery or a history of vertebral traumas/fractures; instrumental physical therapies or physiotherapeutic therapies in the previous 3 months. | |
| Interventions | 1. Back School group: In the first session, individuals were informed about the anatomy of the spinal column, its functioning and ergonomic position and the basis of the pain‐inducing mechanism, psychological aspects and stress management, whereas in the following sessions they performed stretching and muscular strengthening, associated with proper breathing. 2. Hydrotherapy group: Participants at first performed walking exercises to adapt to the pool conditions, and afterwards performed bilateral stretching and selective muscle strengthening exercises. | |
| Outcomes | 1. Disability: Roland‐Morris Disability Questionnaire. | |
| Notes | Setting not specified. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The participants were randomly allocated using computer randomisation software (RANDI2 software version 0.6.1) to the Back School programme (group A) or to the hydrotherapy programme (group B). |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Low risk | All analyses were performed based on the intention‐to‐treat principle. |
| Selective reporting (reporting bias) | Low risk | It was clear that the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | No significant difference across the groups was found. |
| Co‐interventions avoided or similar? | Low risk | Balanced for both groups |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the reported intensity/dosage, duration, number, and frequency for both the intervention and control groups. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 120 participants. 1. Back School group n = 60. 2. Waiting‐list control group n = 60. Inclusion criteria: chronic, recurrent low back pain, age 20 to 40 years, no use of treatment because of acute back pain, no Back School experience, working full time, no expectation of an occupational disease at the time of enrolment. | |
| Interventions | 1. Back School group: 6 sessions (6 to 8 different modules) of 90 minutes in 8 weeks including education (anatomy, pathology, ergonomic, optimal posture during work and other activities) and exercises (isometric and dynamic strength, stretching and relaxation exercises, work simulating). 2. Waiting‐list control group. | |
| Outcomes | Pain: Pain Rating Scale. | |
| Notes | Occupational setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | Not mentioned |
| Similarity of baseline characteristics? | Low risk | Demographic baseline characteristics of the study population are presented in Table 1. |
| Co‐interventions avoided or similar? | Unclear risk | Not mentioned |
| Compliance acceptable? | Unclear risk | Not mentioned |
| Timing outcome assessments similar? | Unclear risk | Not mentioned |
| Methods | RCT | |
| Participants | 28 participants. 1. Back School group n = 14. 2. Mat‐based exercises group n = 14. Inclusion criteria: Candidates with non‐specific low back pain with a pain score < 8 on the verbal numerical pain (VNP) scale, and without significantly impaired spinal mobility, were included in this study. Only candidates who could read and speak English were included. Exclusion criteria: Candidates suffering from numbness, paraesthesia, or radicular symptoms were excluded from this study, as were those with any other musculoskeletal disorders of the lower limbs or upper‐ and mid‐back pain. Candidates with red flags such as cancer, fractures, inflammatory or infective diseases, other neurological disorders, and those having spinal surgery less than 6 months prior to the study were also excluded. | |
| Interventions | 1. Back School group: The participants in the experimental group performed functional back exercises and had back care instruction amounting to 1‐hour duration for each session. The participants received training in specific tasks like lifting, sitting, or mopping in order to correct their body mechanics in their ADL. The first 15 minutes of the session was a PowerPoint presentation on correct postures like upright sitting and standing postures, proper body mechanics of ADL like lifting, mopping and sweeping, walking, going up and down the stairs, information on ergonomic correction and activity pacing. This was followed by a functional task practice of all the above‐mentioned ADL for the next 30 minutes. 2. Mat‐based exercises group: The participants in the control group performed generic mat‐based exercises commonly used to treat people with chronic low back pain. These exercises were not focused on any specific body mechanics or postures. The stretches were performed in reclined position on an exercise mat for the quadriceps, hamstrings, calf, hip external rotators, and spine (such as cat/dog stretches and prayer stretches). Mat exercises (e.g. knee hugs, knee rocking, lumbar rotation, and pelvic tilts in the supine position), mat‐based core stability exercises were also performed. 2 sets of 10 repetitions of each exercise were performed for the 1‐hour duration of each session; this was continued for 4 consecutive sessions once a week. The participants were instructed to follow the exercises as performed by the physiotherapist. The sessions were kept less interactive than they would be in a regular group exercise class. | |
| Outcomes | 1. Pain: numerical pain scale. 2. Disability: Roland‐Morris Disability Questionnaire. | |
| Notes | Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | Due to the nature of the interventions, it was not possible to blind the participants. |
| Blinding (performance bias and detection bias) | High risk | Due to the nature of the interventions, it was not possible to blind the therapists. |
| Blinding of outcome assessment (detection bias) | Low risk | An independent investigator collected data before and after the exercise classes. |
| Incomplete outcome data (attrition bias) | High risk | Only 15 participants completed the study; 13 participants dropped out of the study due to non‐compliance or inability to obtain time‐off from work, or both. |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | Not mentioned |
| Similarity of baseline characteristics? | Low risk | No significant difference across the groups was found. |
| Co‐interventions avoided or similar? | Low risk | Balanced for both groups |
| Compliance acceptable? | High risk | Only 15 participants completed the study; 13 participants dropped out of the study due to non‐compliance or inability to obtain time‐off from work, or both. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 138 participants. 1. Back School group n = 46. 2. Calisthenics exercises group n = 46. 3. Waiting‐list control group n = 46. Exclusion criteria: not described. | |
| Interventions | 1. Back School group: 4, 90‐minute sessions during a 2‐week period plus a 5th session after 2 months. Each group of 10 to 12 participants was supervised by a physiotherapist (education and exercises for back and abdominal muscles). 2. Calisthenics exercises group: 45‐minute sessions biweekly for 3 months in groups of 10 to 12 participants (flexion and pelvic tilt exercises in order to strengthen the abdominal muscles, expanding spinal forward flexion). 3. Waiting‐list control group. | |
| Outcomes | Disability: Oswestry Low Back Pain Questionnaire. | |
| Notes | Occupational setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | After being examined, the participants were allocated to the 3 groups by a systematic random sampling method. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Demographic and clinical baseline characteristics of the study population are presented in Table 1. Demographic and clinical baseline characteristics were similar for both groups. |
| Co‐interventions avoided or similar? | Unclear risk | There were few reported co‐interventions in the study. |
| Compliance acceptable? | Low risk | Based on the description of both groups, compliance was acceptable. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | quasi‐RCT | |
| Participants | 43 participants. 1. Back School group n = 22. 2. Pilates group n = 21. Inclusion criteria: chronic LBP without peripheral irradiation for at least 3 months; neurological values within the normal range; negative Lasegue’s test and Wassermann test. Exclusion criteria: clinical history of spinal surgery; neurological values outside the normal range; radicular pain with positive Lasegue’s and Wassermann’s signs and straight leg raise test; structural deformities such as spondylolisthesis; stenosis of the vertebral canal; computed tomography or nuclear magnetic resonance documented disc hernia; rheumatoid arthritis or other rheumatologically related pathologies; conditions unrelated to the spinal column that mimic lumbalgic symptoms. | |
| Interventions | 1. Back School group: 10 sessions/60 minutes. During each session, participants performed all the exercises listed in the protocol. The protocol included postural education exercises, respiratory education, muscular extension and strengthening exercises of the paravertebral muscles and lower limbs, mobilising exercises for the spinal column and antalgic postures. During each treatment session, the therapist taught the participants some theoretical notions of the anatomy and pathology of the spinal column and in the principles of postural education. 2. Pilates group: 10 sessions/60 minutes. The protocol comprised a programme of exercise modules that made it easier to adapt the exercise to the requirements of each participant in each group. The protocol comprised postural education, stretching exercises, and breathing education. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Disability: Roland‐Morris Disability Questionnaire. | |
| Notes | Secondary care setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Used a quasi‐random procedure |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Demographic and clinical baseline characteristics were similar for both groups. |
| Co‐interventions avoided or similar? | Unclear risk | There were few reported co‐interventions in the study. |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the descriptions of both groups. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 272 participants. 1. Back School group n = 129. 2. Muscle training exercises group n = 143. Inclusion criteria: low back pain lasting more than 12 weeks with or without pain radiating into the leg(s), and aged 18 to 60 years. Exclusion criteria: symptoms of serious spinal pathology such as malignancy, osteoporosis, vertebral fracture, spinal stenosis, clinical symptoms of an acute herniated disc accompanied by nerve root entrapment, unstable spondylolisthesis, spondylitis, health conditions that prevented them from performing strenuous exercise, and language problems. | |
| Interventions | 1. Back School group: 36 sessions x 2 hours for 12 weeks. Participants received a programme of combined exercise, education, and pain management based on a programme described by Bendix. At the first session, a pre‐programme assessment was performed to familiarise participants with the exercise programme, set treatment goals, and set the initial intensity for each exercise. The bulk of the session consisted of aerobic training and training to strengthen the muscles in the back, gluteus region, and abdominal wall. These exercises were all performed in the supine position using machines and circuit training. A total of 22 hours of exercises was performed. In addition, participants were provided 1.5 hours to play ball games, 1.5 hours of training in hot water, and 2 hours of ball stick training. Bi‐weekly lessons on anatomy, postural techniques, and pain management were provided by a physiotherapist and on back care and lifting techniques by an occupational therapist, for a total of 10 hours. During the second period, 2‐hour exercise sessions were performed twice a week at the study site and once a week at the participant’s home. During the third period, 2‐hour exercise sessions were performed 3 times a week at home. The participants performed a total of 75 hours of moderate muscle training exercise. The treatment‐related cost per participant amounted to 12 hours of therapist assistance. 2. Muscle training exercises group: 24 sessions x 1 hour for 12 weeks. Participants received a programme of specific and intensive muscle training exercises to strengthen and shorten the muscles in the back and gluteus region. The programme did not include stretching or abdominal muscle exercises. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Disability: Roland‐Morris Disability Questionnaire. 3. Adverse events: reported by the physiotherapists on standardised forms. | |
| Notes | Secondary care setting. Funding: The Danish National Board of Health. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were allocated by a separate secretary to a group‐based multidisciplinary biopsychosocial rehabilitation programme (group A) or intensive individually therapist‐assisted back muscle strengthening exercises (group B) according to a random number chart made for each subgroup provided by the Copenhagen Trial Unit, Center for Clinical Intervention Research, Rigshospitalet. |
| Allocation concealment (selection bias) | Low risk | Participants were allocated by a separate secretary to a group‐based multidisciplinary biopsychosocial rehabilitation programme (group A) or intensive individually therapist‐assisted back muscle strengthening exercises (group B) according to a random number chart made for each subgroup provided by the Copenhagen Trial Unit, Center for Clinical Intervention Research, Rigshospitalet. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | Low risk | All physical examinations at trial visits were performed by 1 physician who was blinded to the treatment group and had no access to the treatment area. |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Low risk | Data analysis was performed on the actual data on an intention‐to‐treat basis, with the last value carried forward. |
| Selective reporting (reporting bias) | Low risk | It was clear that the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Demographic and clinical baseline characteristics of the study population are presented in Table 1. There were no significant differences between the groups. |
| Co‐interventions avoided or similar? | Unclear risk | Not mentioned |
| Compliance acceptable? | Unclear risk | There are insufficient data about the control group. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 121 participants. 1. Back School group n = 61. 2. Exercise group n = 60. Inclusion criteria: people with low back pain for at least 3 months. Exclusion criteria: people with acute radicular signs or symptoms, those who had radiographic evidence of inflammatory disease affecting the spine, tumour; serious medical conditions for which exercise is contraindicated; history of spinal surgery; pregnancy. | |
| Interventions | 1. Back School group: 8 sessions within a 4‐week period. Each session entailed approximately half an hour of didactic training and half an hour of practical training. The program was administered by a physiatrist. 2. Exercise group: The participants in both groups were treated with a group‐exercise programme of 60 minutes of exercise 3 times a week. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Disability: Oswestry Disability Index. | |
| Notes | Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was allocated by numbered‐envelopes method. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Demographic and clinical baseline characteristics of the study population are presented in Table 1. There were no significant differences between the groups. |
| Co‐interventions avoided or similar? | Low risk | Balanced for both groups |
| Compliance acceptable? | Unclear risk | Not mentioned |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 148 participants. 1. Back School group n = 74. 2. McKenzie Method group n = 74. Inclusion criteria: Patients seeking care had to have non‐specific low back pain of at least 3 months’ duration and be between 18 and 80 years of age. Patients with any contraindication to physical exercise based on the recommendations of the guidelines of the American College of Sports Medicine. Exclusion criteria: Serious spinal pathology (e.g. tumours, fractures, inflammatory diseases), previous spinal surgery, nerve root compromise, cardiorespiratory illnesses, or pregnancy. | |
| Interventions | 1. Back School group: 4 sessions x 60 minutes for 4 weeks. Participants received theoretical and practical information during the treatment sessions. The first session was conducted individually, and the 3 remaining sessions were conducted in groups. 2. McKenzie Method: 4 sessions x 60 minutes for 4 weeks. Participants received theoretical information regarding the care of the spine and performed specific exercises according to the direction of preference of movement according to the McKenzie Method. | |
| Outcomes | 1. Pain: numerical pain scale. 2. Disability: Roland‐Morris Disability Questionnaire. 3. Adverse events: reported by the physiotherapists on standardised forms. | |
| Notes | Primary care setting. Funding: Fundação de Amparo a Pesquisa do Estado de São Paulo (FAPESP). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A simple randomisation sequence was computer generated using Microsoft Excel (Microsoft Corporation, Redmond, Washington) by one of the investigators of the study who was not directly involved with the assessment and treatment of participants. |
| Allocation concealment (selection bias) | Low risk | The allocation was concealed by using consecutively numbered, sealed, opaque envelopes. |
| Blinding of participants and personnel (performance bias) | High risk | Given the nature of the interventions, it was not possible to blind the therapist or participants. |
| Blinding (performance bias and detection bias) | High risk | Given the nature of the interventions, it was not possible to blind the therapist or participants. |
| Blinding of outcome assessment (detection bias) | Low risk | This study was a prospectively registered, 2‐arm randomised controlled trial with a blinded assessor. |
| Incomplete outcome data (attrition bias) | Low risk | 146 (98.6%) of participants completed the follow‐up at 1 month for the primary outcome measures of pain and disability and for the secondary outcome measure of quality of life. |
| Intention‐to‐treat Analysis | Low risk | The statistical analysis was conducted on an intention‐to‐treat basis. |
| Selective reporting (reporting bias) | Low risk | It was clear that the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Groups did not differ in the baseline characteristics. |
| Co‐interventions avoided or similar? | Low risk | Balanced for both groups |
| Compliance acceptable? | Low risk | Based on the descriptions of both groups, compliance was acceptable. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 299 participants. 1. Back School (low‐intensity) group n = 98. 2. Back School (high‐intensity) group n = 98. 3. Usual care group n = 103. Inclusion criteria: workers; non‐specific low back pain; being sick‐listed (completely or partially) between 3 and 6 weeks; age 18 to 65 years; and ability to complete written questionnaires in the Dutch language. Exclusion criteria: sick‐listed due to low back pain less than 1 month before the onset of the current episode of sick‐leave; specific pathology; pregnancy. | |
| Interventions | 1. Back School (low‐intensity) group: 4 sessions x 120 minutes for 4 weeks. 2. Back School (high‐intensity) group: 16 sessions x 60 minutes for 8 weeks. 3. Usual care group: Participants allocated to this group received usual care provided by the occupational physician according to the Dutch guidelines for the occupational health management of patients with low back pain. After 12 weeks of continued sick‐leave, the occupational physician was advised to refer the worker to more intensive interventions such as Back Schools or a multidisciplinary rehabilitation programme. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Disability: Roland‐Morris Disability Questionnaire. 3. Return to work: defined as the duration of work absenteeism in calendar days from the first day of sick‐leave until full return to own work or other work with equal earnings for at least 4 weeks without (partial or full) dropout. 4. Adverse events: reported by the physiotherapists on standardised forms. | |
| Notes | Secondary care setting. Funding: The Netherlands Organisation for Health Research and Development (ZonMw), Dutch Ministries of Health, Welfare and Sports and of Social Affairs and Employment. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Using sealed, opaque envelopes, coded according to a computerised random number generator, participants were randomly allocated to either the low‐intensity Back School, high‐intensity Back School, or usual care group. |
| Allocation concealment (selection bias) | Low risk | Using sealed, opaque envelopes, coded according to a computerised random number generator, participants were randomly allocated to either the low‐intensity Back School, high‐intensity Back School, or usual care group. |
| Blinding of participants and personnel (performance bias) | High risk | Occupational and family physicians and physiotherapists were not blinded for the allocated intervention. |
| Blinding (performance bias and detection bias) | High risk | Occupational and family physicians and physiotherapists were not blinded for the allocated intervention. |
| Blinding of outcome assessment (detection bias) | Low risk | An independent research assistant extracted the work absence data. |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Low risk | "Applying the intention‐to‐treat (ITT) principle, we included all patients in the analysis according to the group determined at randomisation." |
| Selective reporting (reporting bias) | Low risk | It was clear that the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Participants did not differ in baseline characteristics. |
| Co‐interventions avoided or similar? | Unclear risk | Not mentioned |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the reported intensity/dosage, duration, number, and frequency for both the intervention and control groups. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 188 participants. 1. Back School group n = 95. 2. Instruction material of the Back School in written form group n = 93. Exclusion criteria: rheumatoid arthritis or other connective tissue disease as well as people with a history of back surgery. | |
| Interventions | 1. Back School group: modified Swedish Back School: 60‐minute education and exercise sessions, 6 times in 3 weeks. Refresher course 2 x 60 minutes after 6 months. Supervised by physiotherapist; 11 participants per group. 2. Instruction material of the Back School in written form group: No actual treatment, but free to use healthcare services. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Disability: Oswestry Disability Index. | |
| Notes | Occupational setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The participants were randomly assigned to one of two groups. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | The 2 groups were comparable for age and duration of low back pain syndrome. |
| Co‐interventions avoided or similar? | Low risk | Balanced for both groups |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the reported intensity/dosage, duration, number, and frequency for both the intervention and control groups. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 111 participants. 1. Back School group n = 56. 2. Passive physiotherapy group n = 55. Inclusion criteria: nurses working in the inpatient department of the university clinics, having LBP syndrome in their medical history, under 60 years of age; more than 3 months of lower back pain with or without referred pain; and having a current active diagnosis of chronic LBP. Exclusion criteria: pregnancy; previous spinal surgery; current nerve root entrapment accompanied by significant neurological deficit; spinal cord compression; tumours; severe structural deformity; severe instability; severe osteoporosis; inflammatory disease of the spine; spinal infection; severe cardiovascular or metabolic disease; depression; and connective tissue disorder. | |
| Interventions | 1. Back School group: 6 sessions for 6 weeks. Sessions of ergonomics training and Back School once a week for a duration of 6 weeks. Each therapy session was divided into a 10‐minute ergonomics training exercise, a 20‐minute muscle strengthening and stretching exercise. 2. Passive physiotherapy group: 1 session for 6 weeks of transcutaneous electrical nerve stimulation (TENS) therapy and heat therapy, which participants were advised to practise at home daily. | |
| Outcomes | 1. Pain: numerical pain scale. | |
| Notes | Occupational setting. Funding: The Netherlands Organisation for Health Research and Development (ZonMw), Dutch Ministries of Health, Welfare and Sports and of Social Affairs and Employment. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Nurses having chronic LBP syndrome were randomised into 2 groups to receive either ergonomics training and Back School (education) or passive therapy. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title, abstract, and flowchart indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | Low risk | The examiner was kept blinded. |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | No information about intention‐to‐treat analysis |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Based on Table 1, participants did not differ in baseline characteristics. |
| Co‐interventions avoided or similar? | Low risk | Balanced for both groups |
| Compliance acceptable? | Unclear risk | There are insufficient data about the control group. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 40 participants. 1. Back School treatment group n = 20. 2. Waiting‐list control group n = 20. Exclusion criteria: medical contraindication list which specified medical disorders and diseases. | |
| Interventions | 1. Back School treatment group: Maastricht Back School: education and skills program in group setting (10 to 12 participants per group), 7 lessons of 2.5 hours and refresher lesson after 8 weeks. Included postural education, exercises, information on psychological factors. 2. Waiting‐list control group. | |
| Outcomes | 1. Pain: visual analogue scale. | |
| Notes | Setting not specified. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | Unclear risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Unclear risk | Not mentioned |
| Co‐interventions avoided or similar? | Unclear risk | There were few reported co‐interventions in the study. |
| Compliance acceptable? | Unclear risk | There are insufficient data about the control group. |
| Timing outcome assessments similar? | Unclear risk | Not mentioned |
| Methods | RCT | |
| Participants | 90 participants. 1. Back School treatment group n = 45. 2. Waiting‐list control group n = 45. Exclusion criteria: people eligible for surgical treatment were excluded, as were those who were unable to participate in a physical exercise program and relaxation training. | |
| Interventions | 1. Back School group: Maastricht Back School, education and skills program in group setting (10 to 12 participants per group), 7 lessons of 2.5 hours and refresher lesson after 6 months. Included postural education, exercises, information on psychological factors. 2. Waiting‐list control group. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Return to work was expressed in number of days. | |
| Notes | Primary care setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | High risk | Dropouts exceed 20%. |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Unclear risk | Not mentioned |
| Co‐interventions avoided or similar? | Unclear risk | Not mentioned |
| Compliance acceptable? | Unclear risk | Not mentioned |
| Timing outcome assessments similar? | Unclear risk | Not mentioned |
| Methods | RCT | |
| Participants | 78 participants. 1. Back School treatment group n = 40. 2. Exercises group n = 38. Inclusion criteria: chronic (6 months or more) LBP with or without lower limb pain. Exclusion criteria: history of spinal surgery; person concurrently attending physiotherapy treatment; and evidence of underlying disease, such as fracture, ankylosing spondylitis, or multiple myeloma. | |
| Interventions | 1. Back School treatment group: Swedish Back School, 3 sessions containing education on anatomy and body mechanics, semi‐Fowler position, ergonomic counselling, and exercises aimed at strengthening the abdominal muscles. 2. Exercises group. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Disability: Oswestry Low Back Pain Questionnaire. | |
| Notes | Primary care setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The participants were randomly allocated to 2 groups and were assessed by a rheumatologist who was not aware of treatment allocated. |
| Allocation concealment (selection bias) | Low risk | The participants were randomly allocated to 2 groups and were assessed by a rheumatologist who was not aware of treatment allocated. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Based on Table 1, participants did not differ in baseline characteristics. |
| Co‐interventions avoided or similar? | Unclear risk | There were few reported co‐interventions in the study. |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the reported intensity/dosage, duration, number, and frequency for both the intervention and control group. |
| Timing outcome assessments similar? | Unclear risk | Not mentioned |
| Methods | RCT | |
| Participants | 43 participants. 1. Back School treatment group n = 21. 2. Electrotherapy n = 22. Exclusion criteria: inflammatory or other specific disorders of the spine such as ankylosing spondylitis, abnormal reflexes, sensory loss, or muscle weakness. | |
| Interventions | 1. Back School treatment group: Swedish Back School: 4 sessions of 45 minutes each over the course of 2 weeks (anatomy and causes of LBP, function muscles and posture, ergonomics, advice on physical activity). 2. Electrotherapy: 4 sessions with detuned short‐wave diathermy in a period of 2 weeks. | |
| Outcomes | 1. Pain: mean pain score (on 10‐point scale). | |
| Notes | Setting not specified. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Based on Table 1, participants did not differ in baseline characteristics. |
| Co‐interventions avoided or similar? | Unclear risk | Not mentioned |
| Compliance acceptable? | Unclear risk | There are insufficient data about the control group. |
| Timing outcome assessments similar? | Unclear risk | Not mentioned |
| Methods | RCT | |
| Participants | 81 participants. 1. Active Back School group n = 43. 2. No‐treatment group n = 38. Inclusion criteria: individuals of both genders, 18 to 50 years of age, at least 1 episode of low back pain in the last year, and finished treatment and sick leave at the time of enrolment. Exclusion criteria: previous surgical procedures for LBP, pregnancy. specific rheumatologic diseases, spondylolisthesis, spinal tumour, spinal fracture, drug or alcohol abuse, and documented mental illness. | |
| Interventions | 1. Active Back School group: 20 sessions of 1 hour each over 13 weeks, consisting of education (anatomy, biomechanics, pathology, ergonomic principles) and exercise (ergonomic, functional, strength and stretching exercises of upper body, pelvis, and leg muscles and joints, simulation of home and work activities). 2. No‐treatment group. | |
| Outcomes | 1. Pain: overall experienced pain. | |
| Notes | Mixed study setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes |
| Similarity of baseline characteristics? | Low risk | Based on Table 1, participants did not differ in baseline characteristics |
| Co‐interventions avoided or similar? | Low risk | Balanced for both groups |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the reported intensity/dosage, duration, number, and frequency for both the intervention and control groups |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time |
| Methods | RCT | |
| Participants | 360 participants. 1. Back School group n = 187. 2. Usual care group n = 173. Inclusion criteria: people with chronic LBP. | |
| Interventions | 1. Back School group: 7 sessions x 60 minutes. 2. Usual care group: 7 sessions x 60 minutes. | |
| Outcomes | 1. Pain: numerical pain scale. | |
| Notes | Secondary care setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | High risk | Dropouts exceeded 20% |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Unclear risk | Not mentioned |
| Co‐interventions avoided or similar? | Low risk | Balanced for both groups |
| Compliance acceptable? | Unclear risk | There are insufficient data about the control group |
| Timing outcome assessments similar? | Unclear risk | Not mentioned |
| Methods | RCT | |
| Participants | 62 participants. 1. Back School group n = 41. 2. Usual care group n = 21. Inclusion criteria: age between 18 and 80 years, chronic non‐specific low back pain persisting for at least 3 months. Exclusion criteria: acute low back pain; pain due to a specific cause (e.g. fracture, spondylolisthesis, disc herniation, and lumbar stenosis); scheduled back surgery; severe cognitive impairments; pregnancy; and the presence of concomitant rheumatological, neurological, psychiatric, cardiological, respiratory, or oncological diseases that could affect spine function or alter the perception of pain. | |
| Interventions | 1. Back School group: 10 sessions x 60 minutes for 4 weeks. 2. Usual care group: same medical and pharmacological assistance as the other group. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Disability: Oswestry Disability Index. 3. Disability: Waddell Disability Index. | |
| Notes | Mixed study setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title, abstract, and flowchart indicate that it is an RCT |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title, abstract, and flowchart indicate that it is an RCT |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | Unclear risk | The study is described as a single‐blind RCT, but there is not enough information to determine who was blinded |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%) |
| Intention‐to‐treat Analysis | Unclear risk | No information about intention‐to‐treat analysis |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes |
| Similarity of baseline characteristics? | Low risk | Participants did not differ in baseline characteristics |
| Co‐interventions avoided or similar? | Unclear risk | Not mentioned |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the reported intensity/dosage, duration, number, and frequency for both the intervention and control groups |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time |
| Methods | RCT | |
| Participants | 75 participants. 1. Back School group n = 25. 2. Perceptive rehabilitation group n = 25. 3. Control group n = 25. Inclusion criteria: people aged 18 to 75 years with chronic non‐specific low back pain persisting for at least 3 months. Exclusion criteria: acute pain, LBP due to specific cause (fracture, spondylolisthesis, disc herniation, and lumbar stenosis), presence of rheumatological, neurological or oncological concomitant disease, back surgery before study, cognitive impairment (Mini‐Mental State Examination score < 24), and pregnancy. | |
| Interventions | 1. Back School group: 10 sessions for 4 weeks. Information on anatomy, causes of LBP, ergonomics, exercises, and advice on physical activity. 2. Perceptive rehabilitation group: 20 sessions x 45 minutes for 4 weeks 3. Control group: same medical and pharmacological assistance as the other groups. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Pain: McGill Pain Questionnaire. 3. Disability: Oswestry Disability Index. 4. Disability: Waddell Disability index. | |
| Notes | Secondary care setting. Funding: this research received no specific grant from any commercial or public funding agency. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title, abstract, and flowchart indicate that it is an RCT |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title, abstract, and flowchart indicate that it is an RCT |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | The study is described as a single‐blind RCT, but there is not enough information to determine who was blinded |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%) |
| Intention‐to‐treat Analysis | Unclear risk | No information about intention‐to‐treat analysis |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes |
| Similarity of baseline characteristics? | Low risk | Based on Table 1, participants did not differ in baseline characteristics |
| Co‐interventions avoided or similar? | Low risk | Balanced for both groups |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the reported intensity/dosage, duration, number, and frequency for both the intervention and control groups |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time |
| Methods | RCT | |
| Participants | 74 participants. 1. Back School group n = 32. 2. Waiting‐list group n = 42. Inclusion criteria: degenerative LBP (on a waiting list for a Back School). Exclusion criteria: acute pain, LBP due to specific cause (fracture, spondylolisthesis, disc herniation, and lumbar stenosis), presence of rheumatological, neurological, or oncological concomitant disease, back surgery before study, cognitive impairment (Mini‐Mental State Examination score < 24), and pregnancy. | |
| Interventions | 1. Back School group: 4 sessions x 2 hours for 4 weeks. 2. Waiting list. | |
| Outcomes | 1. Pain (own instrument). | |
| Notes | Setting not specified. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Unclear risk | Not mentioned |
| Intention‐to‐treat Analysis | Low risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Unclear risk | Not mentioned |
| Co‐interventions avoided or similar? | Unclear risk | Not mentioned |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the reported intensity/dosage, duration, number, and frequency for both the intervention and control groups. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 50 participants. 1. Back School group n = 29. 2. Medical‐assistance group n = 21. Inclusion criteria: age between 18 and 80 years and a diagnosis of chronic non‐specific low back pain. | |
| Interventions | 1. Back School group: 10 sessions over 4 weeks. First theoretical lesson and then treated 3 times per week for 3 weeks. All sessions lasted 1 hour. Each group included 4 or 5 participants. 2. Medical assistance. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Dsability: Oswestry Disability Index. | |
| Notes | Secondary care setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The concealed randomisation was performed by means of sealed envelopes |
| Allocation concealment (selection bias) | Low risk | The concealed randomisation was performed by means of sealed envelopes |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%) |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes |
| Similarity of baseline characteristics? | Low risk | Based on Table 1, participants did not differ in baseline characteristics |
| Co‐interventions avoided or similar? | Unclear risk | Not mentioned |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the descriptions of both groups |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time |
| Methods | RCT | |
| Participants | 30 participants. 1. Back School group n = 15. 2. Perceptive rehabilitation group n = 15. Inclusion criteria: a diagnosis of chronic non‐specific low back pain and age between 18 and 75 years. | |
| Interventions | 1. Back School group: 10 sessions x 45 minutes for 4 weeks. Comprised an initial lesson on theory and 3 practical sessions per week for 3 weeks. 2. Perceptive rehabilitation group: Utilised a specific tool called "surface for perceptive rehabilitation" composed of about 100 deformable latex cones with a small top, fixed to a rigid surface. Perceptive rehabilitation is a therapeutic system based on the interaction between the patient’s body trunk and a support surface. | |
| Outcomes | 1. Pain: McGill Pain Questionnaire. | |
| Notes | Secondary care setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title, abstract, and flowchart indicate that it is an RCT. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title, abstract, and flowchart indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Unclear risk | Not mentioned |
| Intention‐to‐treat Analysis | Unclear risk | No mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Unclear risk | Not mentioned |
| Co‐interventions avoided or similar? | Unclear risk | Not mentioned |
| Compliance acceptable? | Unclear risk | There are insufficient data about the control group. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 93 participants. 1. Back School group n = 47. 2. Fitness training n = 46. Exclusion criteria: not described. | |
| Interventions | 1. Back School group: 21 sessions (8 supervised and 13 voluntary group meetings) of 85 minutes each over 10 weeks. Swedish type of Back School including fitness training (muscle force, endurance, and stretching exercises for upper and lower back, trunk flexors, upper arm and leg muscles, and ergonomic work techniques), group discussions (structure, functioning and strain of the back, lifting, principles of physical exercises during leisure time and at work), and extra meetings consisting of physical training and social intercourse. 2. Fitness training: 10 sessions of 1 hour each over 5 weeks. | |
| Outcomes | 1. Disability: Oswestry Disability Questionnaire. | |
| Notes | Occupational setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | High risk | Dropouts exceeded 20%. |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Based on Table 1, participants did not differ in baseline characteristics. |
| Co‐interventions avoided or similar? | Unclear risk | There were few reported co‐interventions in the study. |
| Compliance acceptable? | Unclear risk | There are insufficient data about the control group. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 240 participants. 1. Back School treatment group n = 50. 2. Spinal manipulation by chiropractor group n = 52. 3. Usual care n = 47. 4. Physiotherapy group n = 91. Exclusion criteria: LBP related to neoplastic diseases of the spine; pregnant or nursing women; people with serious general diseases. | |
| Interventions | 1. Back School treatment group: based on Canadian Back Education Unit: 4, 1‐hour sessions in a 1‐week period (including muscle exercises). 2. Spinal manipulation by chiropractor: daily for the first week and then twice a week for 6 weeks. 3. Usual care: drug therapy, non‐steroidal anti‐inflammatory drugs (15 to 20 days). 4. Physiotherapy: physiotherapy, light massage, analgesic currents and diathermy daily for 3 weeks. | |
| Outcomes | 1. Pain: visual analogue scale. | |
| Notes | Secondary care setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Allocation concealment (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title and abstract indicate that it is an RCT. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Unclear risk | Not mentioned |
| Co‐interventions avoided or similar? | Unclear risk | Not mentioned |
| Compliance acceptable? | Unclear risk | There are insufficient data about the control group. |
| Timing outcome assessments similar? | Unclear risk | Not mentioned |
| Methods | RCT | |
| Participants | 55 participants. 1. Back School group n = 26. 2. Medical assistance n = 29. Inclusion criteria: aged 18 to 65 years diagnosed with chronic non‐specific low back pain with mechanical characteristics lasting more than 3 months. Exclusion criteria: previous back surgery, spinal tumour, spinal fracture, pregnancy, fibromyalgia, inflammatory or infectious spinal diseases, and litigant patients. | |
| Interventions | 1. Back School group: 3 sessions during 2 months. Orientation was given regarding the anatomy and physiology of the spine, causes and treatment of low back pain, and ergonomic guidelines relevant to back problems. Abdominal and back strengthening exercises were also performed. 2. Medical assistance. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Disability: Roland‐Morris Disability Questionnaire. | |
| Notes | Secondary care setting. Funding: 2 authors (DCR and DA) received support from the University of Otago (University of Otago Doctoral Scholarship). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Folded pieces of paper indicating 1 of the groups were placed in sealed envelopes which were placed in a container. Another investigator selected the envelopes to determine to which group individual participants would belong. |
| Allocation concealment (selection bias) | Low risk | Folded pieces of paper indicating 1 of the groups were placed in sealed envelopes which were placed in a container. Another investigator selected the envelopes to determine to which group individual participants would belong. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | Low risk | Participants were assessed by an investigator (physiotherapist) blinded to treatment groups. |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | High risk | Participants who failed to complete all 4 assessments were also considered dropouts and were excluded from the statistical analysis. |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Based on Table 1, participants did not differ in baseline characteristics. |
| Co‐interventions avoided or similar? | Unclear risk | Not mentioned |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the reported intensity/dosage, duration, number, and frequency for both the intervention and control groups. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 146 participants. 1. Back School group n = 73. 2. Exercise group n = 73. Inclusion criteria: non‐specific low back pain for longer than 12 weeks without neurological deficits. Exclusion criteria: people who had continuous pain, age ≤ 18 years, those who had already attended the Back School programme, those who had previously undergone surgery, who had structural anomalies, spinal cord compressions, severe instabilities, severe osteoporosis, acute infections, severe cardiovascular or metabolic diseases, who were pregnant, and those with a body mass index above 30 kg/m2. | |
| Interventions | 1. Back School group: 4 sessions x 60 minutes for 2 weeks, participants received exercise, physical treatment modalities, and a Back School programme. 2. Exercise group: received exercise and physical treatment modalities. | |
| Outcomes | 1. Pain: visual analogue scale. 2. Disability: Oswestry Disability Index. | |
| Notes | Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Concealed randomisation was conducted using sealed, opaque envelopes coded according to a computerised random number generator. |
| Allocation concealment (selection bias) | Low risk | Concealed randomisation was conducted using sealed, opaque envelopes coded according to a computerised random number generator. |
| Blinding of participants and personnel (performance bias) | High risk | No mention of any attempts to blind the participants |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | Low risk | All participants were examined by the same physician, who was blind to the type of therapy. |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Unclear risk | Not mentioned |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Based on Table 1, participants did not differ in baseline characteristics. |
| Co‐interventions avoided or similar? | Low risk | Balanced for both groups |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the reported intensity/dosage, duration, number, and frequency for both the intervention and control groups. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
| Methods | RCT | |
| Participants | 102 participants. 1. Back School group n = 50. 2. Medical assistance n = 52. Inclusion criteria: age 18 years and over, suffering from chronic back pain (persisting for 90 days or more), and having a telephone number for regular contact with a responsible caregiver. Exclusion criteria: back surgery within the 2 years prior to the initial observation, or if the complaint was restricted to the sacroiliac joint or the cervical or thoracic regions, or if there was congenital spine disease. People with a low back complaint that had persisted less than 90 days were also excluded. | |
| Interventions | 1. Back School group: 5 sessions for 4 days. Multidimensional and interdisciplinary educational regimen designed to assess each patient's physical condition, personal characteristics, lifestyle, and subsequent ability to cope. The program utilises an empowerment approach, providing a combination of knowledge, skills, and heightened self awareness regarding values and needs, so that patients can define and achieve their own goals. 2. Medical assistance: only medication. | |
| Outcomes | 1. Pain: subscale of 36‐Item Short Form Health Survey (SF‐36). | |
| Notes | Secondary care setting. Funding: N/A. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The sequence generation procedure or the method of allocation were not mentioned. The title, abstract, and flowchart indicate that it is an RCT. |
| Allocation concealment (selection bias) | High risk | The treatment allocation was not concealed. |
| Blinding of participants and personnel (performance bias) | High risk | Participants were not blinded to the intervention. |
| Blinding (performance bias and detection bias) | High risk | No mention of any attempts to blind the care providers |
| Blinding of outcome assessment (detection bias) | High risk | No mention of any attempts to blind the assessors |
| Incomplete outcome data (attrition bias) | Low risk | The percentage of withdrawals and dropouts was within the acceptable rate (less than 20%). |
| Intention‐to‐treat Analysis | Low risk | The study used an intention‐to‐treat analysis. |
| Selective reporting (reporting bias) | Unclear risk | It was unclear if the published report included all expected outcomes. |
| Similarity of baseline characteristics? | Low risk | Participants did not differ in baseline characteristics. |
| Co‐interventions avoided or similar? | Low risk | Co‐interventions were avoided for both groups. |
| Compliance acceptable? | Low risk | Compliance was acceptable based on the descriptions of both groups. |
| Timing outcome assessments similar? | Low risk | All important outcomes assessments for both groups were measured at the same time. |
ADL: activities of daily living
LBP: low back pain
N/A: not applicable
RCT: randomised controlled trial
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
| The average time of symptoms in the inclusion criteria was characterised as acute LBP. | |
| Back School intervention consisted of education only, without exercises. | |
| The intervention was not considered to be Back School. | |
| The average time of symptoms in the inclusion criteria was characterised as acute LBP. | |
| The average time of symptoms in the inclusion criteria was characterised as acute LBP. | |
| Back School intervention consisted of education only, without exercises. | |
| Back School intervention consisted of education only, without exercises. | |
| The average time of symptoms in the inclusion criteria was characterised as acute LBP. | |
| Back School intervention consisted of education only, without exercises. | |
| The average time of symptoms in the inclusion criteria was characterised as acute LBP. | |
| The average time of symptoms in the inclusion criteria was characterised as acute LBP. | |
| The intervention was not considered to be Back School. | |
| Back School intervention consisted of education only, without exercises. | |
| Back School intervention consisted of education only, without exercises. | |
| The Back School intervention was not a clear contrast for the control group. | |
| Each group was assessed once, the control group at the beginning of the programme and the Back School group at the end. | |
| The results are for a single group. | |
| The intervention was not considered to be Back School. | |
| The intervention was not considered to be Back School. |
LBP: low back pain
Characteristics of studies awaiting assessment [ordered by study ID]
| Methods | Randomised controlled trial |
| Participants | 148 people with a diagnosis of chronic low back pain for at least 3 months. |
| Interventions | 1. Back School group: 4 sessions x 60 minutes for 4 weeks. Participants allocated to this group received theoretical and practical information during the treatment sessions. The first session was conducted individually, and the 3 remaining sessions were conducted in groups. 2. McKenzie Method group: 4 sessions x 60 minutes for 4 weeks. Participants allocated to this group received theoretical information regarding the care of the spine and performed specific exercises according to the direction of preference of movement according to the McKenzie Method. |
| Outcomes | 1. Pain: numerical pain scale. 2. Disability: Roland‐Morris Disability Questionnaire. 3. Adverse events: reported by the physiotherapists on standardised forms. |
| Notes |
| Methods | Randomised controlled trial |
| Participants | 53 people with a diagnosis of chronic low back pain for at least 3 months. |
| Interventions | 1. Experimental group: Participants were treated in outpatient with a Back School programme. Each group consisted of 4 or 5 people who underwent the rehabilitation treatment twice a week for 5 consecutive weeks for a total of 10 sessions, each lasting about 1 hour. 2. Control group: Participants were treated in outpatient with the Feldenkrais Method. Each group consisted of 4 or 5 people who underwent the rehabilitation treatment twice a week for 5 consecutive weeks for a total of 10 sessions, each lasting about 1 hour. |
| Outcomes | 1. Pain: visual analogue scale and McGill Pain Questionnaire. 2. Disability: Waddell Disability Index. 3. Quality of life: 36‐Item Short Form Health Survey. 4. Mind‐body interactions: Multidimensional Assessment of Interoceptive Awareness Questionnaire. |
| Notes | No funding was received in support of this work. |
Characteristics of ongoing studies [ordered by study ID]
| Trial name or title | The effect of lumbar care (based on Back School) on nursing staff’s low back pain and functional disability |
| Methods | Clinical trial, 2 arms, randomised controlled, single‐blind |
| Participants | Individuals diagnosed with chronic low back pain. Inclusion criteria: nursing licence, work at hospital in the morning shift during the study, low back pain (based on self report). |
| Interventions | Intervention: a 3‐hour lumbar care workshop based on Back School method. Control: routine care. |
| Outcomes | 1. Functional disability: Roland‐Morris Disability Questionnaire. 2. Pain: visual analogue scale. |
| Starting date | 06 September 2015 |
| Contact information | Name: Mehdi Pakbaz Address: Kodakyar Ave., Daneshjo Blvd., Evin, Post code: 1985713834, Tehran, Iran Email: [email protected]; [email protected] Affiliation: University of Social Welfare and Rehabilitation Sciences |
| Notes |
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain Show forest plot | 7 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 1.1  Comparison 1 Back School versus no treatment, Outcome 1 Pain. | ||||
| 1.1 short‐term follow‐up (<3 months) | 6 | 647 | Mean Difference (IV, Random, 95% CI) | ‐6.10 [‐10.18, ‐2.01] |
| 1.2 intermediate‐term follow up (3‐6 months) | 4 | 257 | Mean Difference (IV, Random, 95% CI) | ‐4.34 [‐14.37, 5.68] |
| 1.3 long‐term follow‐up (>6 months) | 3 | 244 | Mean Difference (IV, Random, 95% CI) | ‐12.16 [‐29.14, 4.83] |
| 2 Disability Show forest plot | 4 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 1.2  Comparison 1 Back School versus no treatment, Outcome 2 Disability. | ||||
| 2.1 short‐term follow‐up (<3 months) | 3 | 426 | Mean Difference (IV, Random, 95% CI) | ‐3.38 [‐6.70, ‐0.05] |
| 2.2 intermediate‐term follow up (3‐6 months) | 3 | 181 | Mean Difference (IV, Random, 95% CI) | ‐5.92 [‐12.08, 0.23] |
| 2.3 long‐term follow‐up (>6 months) | 2 | 124 | Mean Difference (IV, Random, 95% CI) | ‐7.36 [‐22.05, 7.34] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain Show forest plot | 5 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 2.1 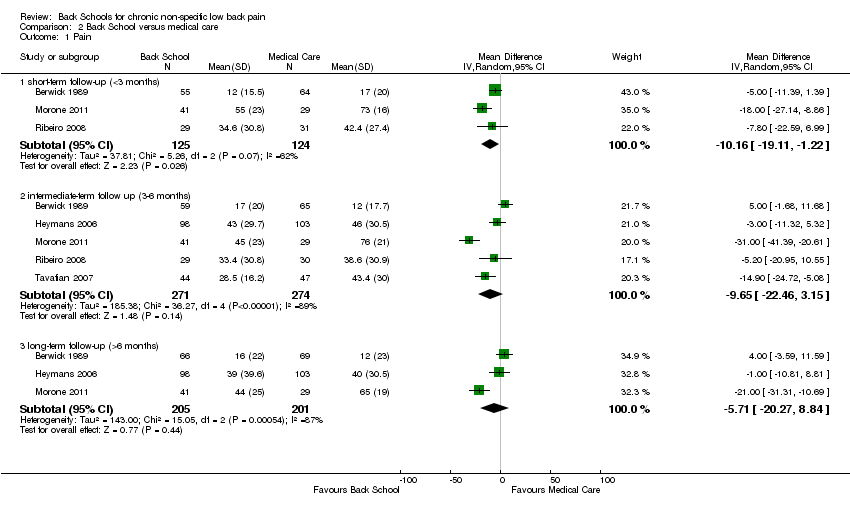 Comparison 2 Back School versus medical care, Outcome 1 Pain. | ||||
| 1.1 short‐term follow‐up (<3 months) | 3 | 249 | Mean Difference (IV, Random, 95% CI) | ‐10.16 [‐19.11, ‐1.22] |
| 1.2 intermediate‐term follow up (3‐6 months) | 5 | 545 | Mean Difference (IV, Random, 95% CI) | ‐9.65 [‐22.46, 3.15] |
| 1.3 long‐term follow‐up (>6 months) | 3 | 406 | Mean Difference (IV, Random, 95% CI) | ‐5.71 [‐20.27, 8.84] |
| 2 Disability Show forest plot | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 2.2 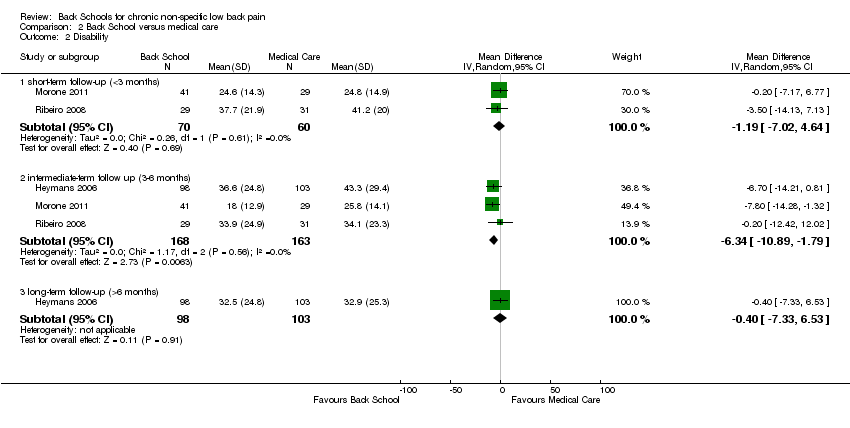 Comparison 2 Back School versus medical care, Outcome 2 Disability. | ||||
| 2.1 short‐term follow‐up (<3 months) | 2 | 130 | Mean Difference (IV, Random, 95% CI) | ‐1.19 [‐7.02, 4.64] |
| 2.2 intermediate‐term follow up (3‐6 months) | 3 | 331 | Mean Difference (IV, Random, 95% CI) | ‐6.34 [‐10.89, ‐1.79] |
| 2.3 long‐term follow‐up (>6 months) | 1 | 201 | Mean Difference (IV, Random, 95% CI) | ‐0.40 [‐7.33, 6.53] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain Show forest plot | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 3.1  Comparison 3 Back School versus passive physiotherapy, Outcome 1 Pain. | ||||
| 1.1 short‐term follow‐up (<3 months) | 3 | 290 | Mean Difference (IV, Random, 95% CI) | 1.96 [‐9.51, 13.43] |
| 1.2 intermediate‐term follow up (3‐6 months) | 3 | 290 | Mean Difference (IV, Random, 95% CI) | ‐16.89 [‐66.56, 32.79] |
| 1.3 long‐term follow‐up (>6 months) | 3 | 291 | Mean Difference (IV, Random, 95% CI) | ‐12.86 [‐61.22, 35.50] |
| 2 Disability Show forest plot | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 3.2  Comparison 3 Back School versus passive physiotherapy, Outcome 2 Disability. | ||||
| 2.1 short‐term follow‐up (<3 months) | 2 | 180 | Mean Difference (IV, Random, 95% CI) | 2.57 [‐15.88, 21.01] |
| 2.2 intermediate‐term follow up (3‐6 months) | 2 | 180 | Mean Difference (IV, Random, 95% CI) | 6.88 [‐4.86, 18.63] |
| 2.3 long‐term follow‐up (>6 months) | 2 | 180 | Mean Difference (IV, Random, 95% CI) | 9.60 [3.65, 15.54] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain Show forest plot | 6 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 4.1  Comparison 4 Back school versus exercise, Outcome 1 Pain. | ||||
| 1.1 short‐term follow‐up (<3 months) | 5 | 416 | Mean Difference (IV, Random, 95% CI) | ‐2.06 [‐14.58, 10.45] |
| 1.2 intermediate‐term follow up (3‐6 months) | 4 | 619 | Mean Difference (IV, Random, 95% CI) | ‐4.46 [‐19.44, 10.52] |
| 1.3 long‐term follow‐up (>6 months) | 3 | 461 | Mean Difference (IV, Random, 95% CI) | 4.58 [‐0.20, 9.36] |
| 2 Disability Show forest plot | 8 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 4.2 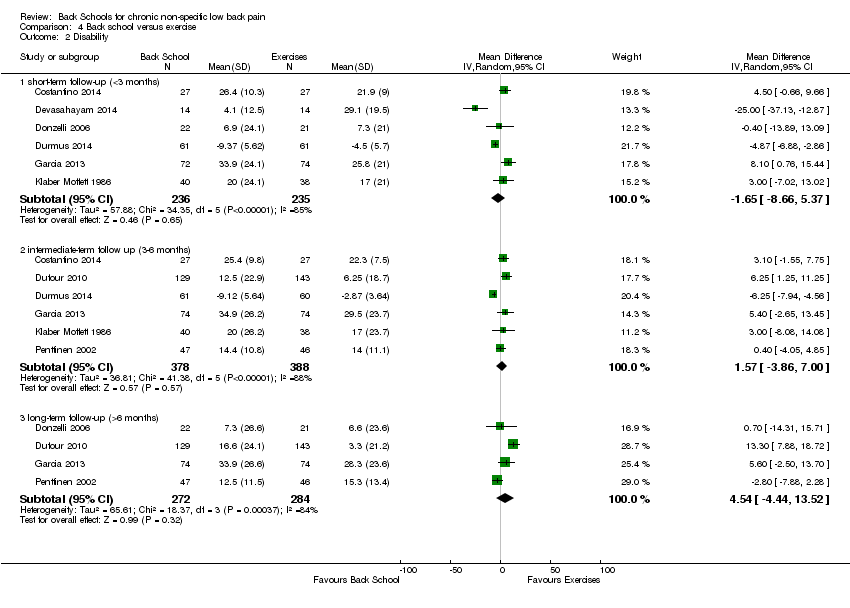 Comparison 4 Back school versus exercise, Outcome 2 Disability. | ||||
| 2.1 short‐term follow‐up (<3 months) | 6 | 471 | Mean Difference (IV, Random, 95% CI) | ‐1.65 [‐8.66, 5.37] |
| 2.2 intermediate‐term follow up (3‐6 months) | 6 | 766 | Mean Difference (IV, Random, 95% CI) | 1.57 [‐3.86, 7.00] |
| 2.3 long‐term follow‐up (>6 months) | 4 | 556 | Mean Difference (IV, Random, 95% CI) | 4.54 [‐4.44, 13.52] |

Study flow diagram.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
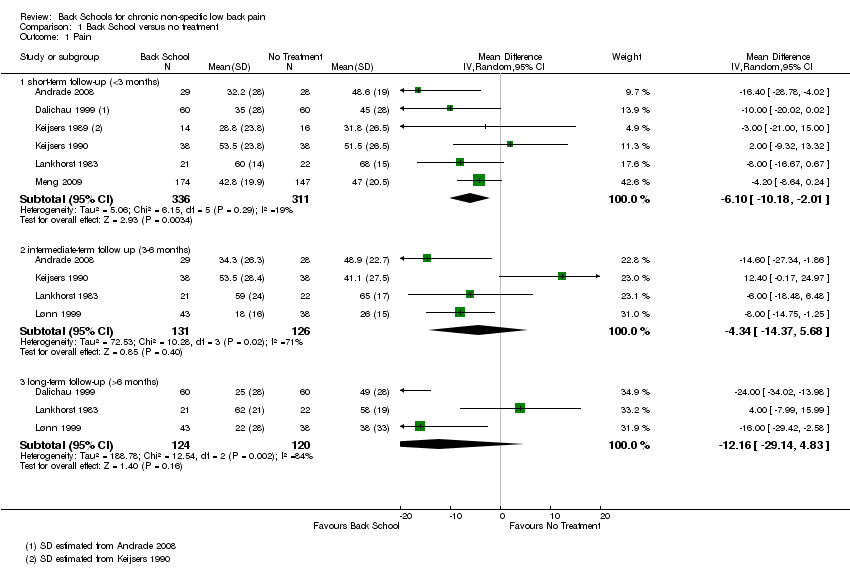
Comparison 1 Back School versus no treatment, Outcome 1 Pain.
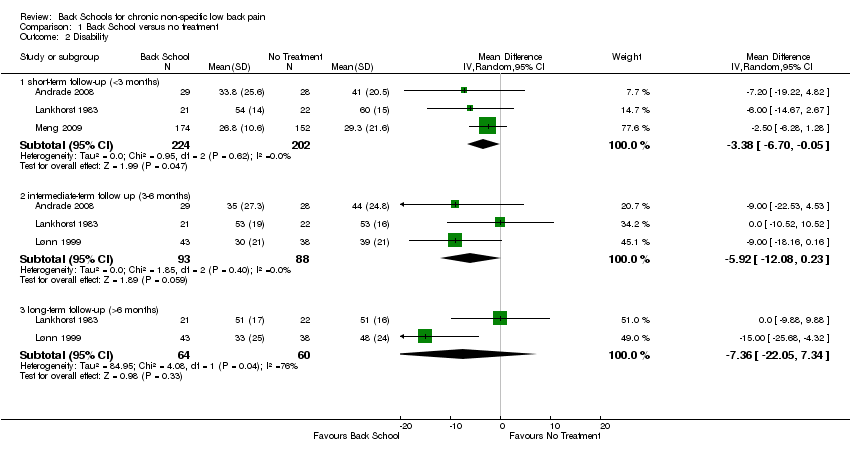
Comparison 1 Back School versus no treatment, Outcome 2 Disability.

Comparison 2 Back School versus medical care, Outcome 1 Pain.

Comparison 2 Back School versus medical care, Outcome 2 Disability.

Comparison 3 Back School versus passive physiotherapy, Outcome 1 Pain.
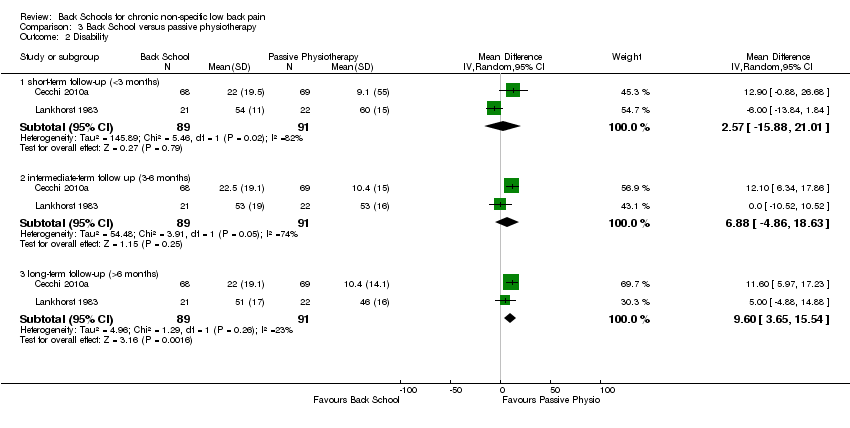
Comparison 3 Back School versus passive physiotherapy, Outcome 2 Disability.

Comparison 4 Back school versus exercise, Outcome 1 Pain.
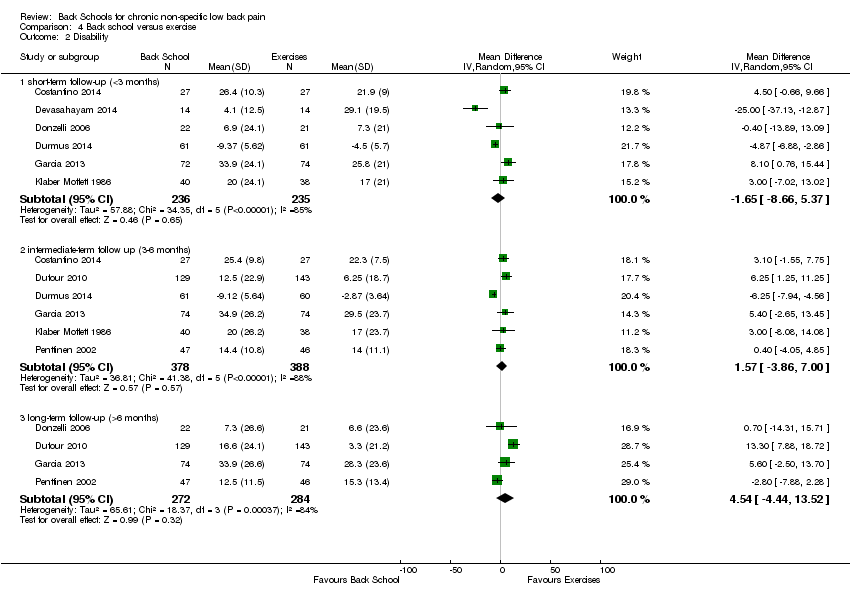
Comparison 4 Back school versus exercise, Outcome 2 Disability.
| Back School compared with no treatment for low back pain | |||||
| Patient or population: people with low back pain Intervention: Back School Comparison: no treatment | |||||
| Outcomes | lIIustrative comparative risks (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk* | ||||
| No treatment | Back School | ||||
| Pain: short‐term follow‐up (< 3 months) Multiple scales: scale from 0 to 100 | The mean pain at short‐term follow‐up ranged across control groups from 31.8 to 68 points. | The mean pain (short term) in the intervention groups was 6.10 lower (10.18 lower to 2.01 lower). | MD ‐6.10 (‐10.18 to ‐2.01) | 647 participants (6 studies) | ⊕⊝⊝⊝ |
| Pain: intermediate‐term follow‐up (3 to 6 months) Multiple scales: scale from 0 to 100 | The mean pain at intermediate‐term follow‐up ranged across control groups from 26 to 65 points. | The mean pain (intermediate term) in the intervention groups was 4.34 lower (14.37 lower to 5.68 higher). | MD ‐4.34 (‐14.37 to 5.68) | 257 participants (4 studies) | ⊕⊝⊝⊝ |
| Pain: long‐term follow‐up (> 6 months) Multiple scales: scale from 0 to 100 | The mean pain at long‐term follow‐up ranged across control groups from 38 to 58 points. | The mean pain (long term) in the intervention groups was 12.16 lower (29.14 lower to 4.83 higher). | MD ‐12.16 (‐29.14 to 4.38) | 244 participants (3 studies) | ⊝⊝⊝⊝ |
| Disability: short‐term follow‐up (< 3 months) Multiple scales: scale from 0 to 100 (worse disability) | The mean disability at short‐term follow‐up ranged across control groups from 29.3 to 60 points. | The mean disability (short term) in the intervention groups was 3.83 lower (6.70 lower to 0.05 lower). | MD ‐3.38 (‐6.70 to ‐0.05) | 426 participants (3 studies) | ⊕⊝⊝⊝ |
| Disability: intermediate‐term follow‐up (3 to 6 months) Multiple scales: scale from 0 to 100 (worse disability) | The mean disability at intermediate‐term follow‐up ranged across control groups from 39 to 53 points. | The mean disability (intermediate term) in the intervention groups was 5.92 lower (12.80 lower to 0.23 higher). | MD ‐5.92 (‐12.08 to 0.23) | 181 participants (3 studies) | ⊕⊝⊝⊝ |
| Disability: long‐term follow‐up (> 6 months) Multiple scales: scale from 0 to 100 (worse disability) | The mean disability long‐term follow‐up ranged across control groups from 48 to 51 points. | The mean disability (long term) in the intervention | MD ‐7.36 (‐22.05 to 7.34) | 124 participants (2 studies) | ⊕⊝⊝⊝ |
| Adverse events Not reported | |||||
| Work status Not reported | |||||
| The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference | |||||
| GRADE Working Group grades of evidence High‐quality evidence: There are consistent findings among at least 75% of randomised controlled trials with low risk of bias; consistent, direct, and precise data; and no known or suspected publication biases. Further research is unlikely to change either the estimate or our confidence in the results. Moderate‐quality evidence: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. | |||||
| 1Downgraded one level due to imprecision (fewer than 400 participants in total). | |||||
| Back School compared with medical care for low back pain | |||||
| Patient or population: people with low back pain Intervention: Back School Comparison: medical care | |||||
| Outcomes | Illustrative comparative risks (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk* | ||||
| Medical care | Back School | ||||
| Pain: short‐term follow‐up (< 3 months) Multiple scales: scale from 0 to 100 | The mean pain at short‐term follow‐up ranged across control groups from 17 to 73 points. | The mean pain (short term) in the intervention groups was 10.16 lower (19.11 lower to 1.22 lower). | MD ‐10.16 (‐19.11 to ‐1.22) | 249 participants (3 studies) | ⊕⊝⊝⊝ |
| Pain: intermediate‐term follow‐up (3 to 6 months) Multiple scales: scale from 0 to 100 | The mean pain at intermediate‐term follow‐up ranged across control groups from 12 to 76 points. | The mean pain (intermediate term) in the intervention groups was 9.65 lower (22.46 lower to 3.15 higher). | MD ‐9.65 (‐22.46 to 3.15) | 545 participants (5 studies) | ⊕⊝⊝⊝ |
| Pain: long‐term follow‐up (> 6 months) Multiple scales: scale from 0 to 100 | The mean pain at long‐term follow‐up ranged across control groups from 12 to 65 points. | The mean pain (long term) in the intervention groups was 5.71 lower (20.27 lower to 8.84 higher). | MD ‐5.71 (‐20.27 to 8.84) | 406 participants (3 studies) | ⊕⊝⊝⊝ |
| Disability: short‐term follow‐up (< 3 months) Multiple scales: scale from 0 to 100 (worse disability) | The mean disability at short‐term follow‐up ranged across control groups from 24.8 to 41.2 points. | The mean disability at short‐term follow‐up in the intervention groups was 1.19 lower (7.02 lower to 4.64 higher). | MD ‐1.19 (‐7.02 to 4.64) | 130 participants (2 studies) | ⊕⊝⊝⊝ |
| Disability: intermediate‐term follow‐up (3 to 6 months) Multiple scales: scale from 0 to 100 (worse disability) | The mean disability at intermediate‐term follow‐up ranged across control groups from 25.8 to 43.3 points. | The mean disability at intermediate‐term follow‐up in the intervention groups was 6.34 lower (10.89 lower to 1.79 lower). | MD ‐6.34 (‐10.89 to ‐1.79) | 331 participants (3 studies) | ⊕⊝⊝⊝ |
| Disability: long‐term follow‐up (> 6 months) Multiple scales: scale from 0 to 100 (worse disability) | The mean disability at long‐term follow‐up was 32.9 points. | The mean disability at long‐term follow‐up in the intervention groups was 0.40 lower (7.33 lower to 6.53 higher). | MD ‐0.40 (‐7.33 to 6.53) | 201 participants (1 study) | ⊕⊝⊝⊝ |
| Adverse events Two workers in the Back School group (n=98) reported a strong increase in low back pain (Heymans 2006). | |||||
| Work status Not reported | |||||
| The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference | |||||
| GRADE Working Group grades of evidence High‐quality evidence: There are consistent findings among at least 75% of randomised controlled trials with low risk of bias; consistent, direct, and precise data; and no known or suspected publication biases. Further research is unlikely to change either the estimate or our confidence in the results. Moderate‐quality evidence: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. | |||||
| 1Downgraded one level due to imprecision (fewer than 400 participants in total). | |||||
| Back School compared with passive physiotherapy for low back pain | |||||
| Patient or population: people with low back pain. Intervention: Back School Comparison: passive physiotherapy | |||||
| Outcomes | Illustrative comparative risks (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk* | ||||
| Passive physiotherapy | Back School | ||||
| pain: short‐term follow‐up (< 3 | The mean pain at short‐term follow‐up ranged across control groups from 7.1 to 88 points. | The mean pain (short‐ term) in the intervention groups was 1.96 higher (9.51 lower to 13.43 higher). | MD 1.96 (‐9.51 to | 290 | ⊝⊝⊝⊝ |
| pain ‐ intermediate‐term follow up (3‐6 months) Multiple scales: scale from 0 to 100 (worse pain) | The mean pain at intermediate‐term follow‐up ranged across control | The mean pain (intermediate‐term) in the intervention groups was 16.89 lower (66.56 lower to 32.79 higher). | MD ‐16.89 (‐66.56 | 290 | ⊝⊝⊝⊝ |
| pain ‐ long‐term follow‐up (>6 months) Multiple scales: scale from 0 to 100 (worse pain) | The mean pain at long‐term follow‐up ranged across control groups from 11.6 to 60.5 points. | The mean pain (long‐ term) in the intervention groups was 12.86 lower (61.22 lower to 35.50 higher). | MD ‐12.86 (‐61.22 | 291 | ⊝⊝⊝⊝ |
| Disability ‐ short‐term follow‐up (<3 months) Multiple scales: | The mean disability at short‐term follow‐up ranged across control groups from 9.1 to 60 points. | The mean disability at short‐term follow‐up in the intervention groups was 2.57 higher (15.88 lower to 21.01 higher). | MD 2.57 | 180 | ⊝⊝⊝⊝ |
| Disability ‐ intermediate‐term follow up (3‐6 months) Multiple scales: | The mean disability at intermediate‐term follow‐up | The mean disability at short‐term follow‐up in the intervention groups was 6.88 higher (‐4.86 lower to 18.63 higher). | MD 6.88 | 180 | ⊕⊝⊝⊝ |
| Disability ‐ long‐term follow‐up (>6 months) Multiple scales: | The mean disability at long‐term follow‐up ranged across | The mean disability at long‐term follow‐up in the intervention groups was 9.60 higher (3.65 higher to 15.54 higher). | MD 9.60 | 180 | ⊕⊝⊝⊝ |
| Adverse events Not reported | |||||
| Work status Not reported | |||||
| The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference | |||||
| GRADE Working Group grades of evidence High‐quality evidence: There are consistent findings among at least 75% of randomised controlled trials with low risk of bias; consistent, direct, and precise data; and no known or suspected publication biases. Further research is unlikely to change either the estimate or our confidence in the results. Moderate‐quality evidence: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. | |||||
| 1 Downgraded one level due to imprecision (fewer than 400 participants, in total). | |||||
| Back School compared with exercise for low back pain | |||||
| Patient or population: people with low back pain Intervention: Back School Comparison: exercise | |||||
| Outcomes | Illustrative comparative risks (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk* | ||||
| Exercise | Back School | ||||
| Pain: short‐term follow‐up (< 3 months) Multiple scales: scale from 0 to 100 | The mean pain at short‐term follow‐up ranged across control groups from 25 to 40 points. | The mean pain (short term) in the intervention groups was 2.06 lower (14.58 lower to 10.45 higher). | MD ‐2.06 (‐14.58 to 10.45) | 416 participants (5 studies) | ⊕⊝⊝⊝ |
| Pain: intermediate‐term follow‐up (3 to 6 months) Multiple scales: scale from 0 to 100 | The mean pain at intermediate‐term follow‐up ranged across control groups from 11.2 to 40 points. | The mean pain (intermediate term) in the intervention groups was 4.46 lower (19.44 lower to 10.52 higher). | MD ‐4.46 (‐19.44 to 10.52) | 619 participants (4 studies) | ⊕⊕⊝⊝ |
| Pain: long‐term follow‐up (> 6 months) Multiple scales: scale from 0 to 100 | The mean pain at long‐term follow‐up ranged across control groups from 8.6 to 50.9 points. | The mean pain (long term) in the intervention groups was 4.58 higher (0.20 lower to 9.36 higher). | MD 4.58 (‐0.20 to 9.36) | 461 participants (3 studies) | ⊕⊕⊝⊝ |
| Disability: short‐term follow‐up (< 3 months) Multiple scales: scale from 0 to 100 (worse disability) | The mean disability at short‐term follow‐up ranged across control groups from 4.5 to 29.1 points. | The mean disability at short‐term follow‐up in the intervention groups was 1.65 lower (8.66 lower to 5.37 higher). | MD ‐1.65 (‐8.66 to 5.37) | 471 participants (6 studies) | ⊕⊝⊝⊝ |
| Disability: intermediate‐term follow‐up (3 to 6 months) Multiple scales: scale from 0 to 100 (worse disability) | The mean disability at intermediate‐term follow‐up ranged across control groups from 2.87 to 29.5 points. | The mean disability at intermediate‐term follow‐up in the intervention groups was 1.57 higher (3.86 lower to 7.00 higher). | MD 1.57 (‐3.86 to 7.00) | 766 participants (6 studies) | ⊕⊝⊝⊝ |
| Disability: long‐term follow‐up (> 6 months) Multiple scales: scale from 0 to 100 (worse disability | The mean disability at long‐term follow‐up ranged across control groups from 3.3 to 28.3 points. | The mean disability at long‐term follow‐up in the intervention groups was 4.54 higher (4.44 lower to 13.52 higher). | MD 4.54 (‐4.44 to 13.52) | 556 participants (4 studies) | ⊕⊝⊝⊝ |
| Adverse events One participant in the Back School group reported a temporary exacerbation of pain (Garcia 2013) and 5 patients in exercise group experienced worsening of leg pain (Dufour 2010) | |||||
| Work status Not reported | |||||
| The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference | |||||
| GRADE Working Group grades of evidence High‐quality evidence: There are consistent findings among at least 75% of randomised controlled trials with low risk of bias; consistent, direct, and precise data; and no known or suspected publication biases. Further research is unlikely to change either the estimate or our confidence in the results. Moderate‐quality evidence: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. | |||||
| 1Downgraded one level due to imprecision (fewer than 400 participants in total). | |||||
| Bias domain | Source of bias | Possible answers |
| Selection | (1) Was the method of randomization adequate? | Yes/no/unsure |
| Selection | (2) Was the treatment allocation concealed? | Yes/no/unsure |
| Performance | (3) Was the patient blinded to the intervention? | Yes/no/unsure |
| Performance | (4) Was the care provider blinded to the intervention? | Yes/no/unsure |
| Detection | (5) Was the outcome assessor blinded to the intervention? | Yes/no/unsure |
| Attrition | (6) Was the drop‐out rate described and acceptable? | Yes/no/unsure |
| Attrition | (7) Were all randomized participants analyzed in the group to which they were allocated? | Yes/no/unsure |
| Reporting | (8) Are reports of the study free of suggestion of selective outcome reporting? | Yes/no/unsure |
| Selection | (9) Were the groups similar at baseline regarding the most important prognostic indicators? | Yes/no/unsure |
| Performance | (10) Were co‐interventions avoided or similar? | Yes/no/unsure |
| Performance | (11) Was the compliance acceptable in all groups? | Yes/no/unsure |
| Detection | (12) Was the timing of the outcome assessment similar in all groups? | Yes/no/unsure |
| Other | (13) Are other sources of potential bias unlikely? | Yes/no/unsure |
| 1 | A random (unpredictable) assignment sequence. Examples of adequate methods are coin toss (for studies with 2 groups), rolling a dice (for studies with 2 or more groups), drawing of balls of different colours, drawing of ballots with the study group labels from a dark bag, computer‐generated random sequence, preordered sealed envelopes, sequentially‐ordered vials, telephone call to a central office, and preordered list of treatment assignments. Examples of inadequate methods are: alternation, birth date, social insurance/security number, date in which they are invited to participate in the study, and hospital registration number. |
| 2 | Assignment generated by an independent person not responsible for determining the eligibility of the patients. This person has no information about the persons included in the trial and has no influence on the assignment sequence or on the decision about eligibility of the patient. |
| 3 | Index and control groups are indistinguishable for the patients or if the success of blinding was tested among the patients and it was successful. |
| 4 | Index and control groups are indistinguishable for the care providers or if the success of blinding was tested among the care providers and it was successful. |
| 5 | Adequacy of blinding should be assessed for each primary outcome separately. This item should be scored ‘‘yes’’ if the success of blinding was tested among the outcome assessors and it was successful or:
|
| 6 | The number of participants who were included in the study but did not complete the observation period or were not included in the analysis must be described and reasons given. If the percentage of withdrawals and drop‐outs does not exceed 20% for short‐term follow‐up and 30% for long‐term follow‐up and does not lead to substantial bias a ‘‘yes’’ is scored. (N.B. these percentages are arbitrary, not supported by literature). |
| 7 | All randomized patients are reported/analyzed in the group they were allocated to by randomization for the most important moments of effect measurement (minus missing values) irrespective of noncompliance and co‐interventions. |
| 8 | All the results from all prespecified outcomes have been adequately reported in the published report of the trial. This information is either obtained by comparing the protocol and the report, or in the absence of the protocol, assessing that the published report includes enough information to make this judgment. |
| 9 | Groups have to be similar at baseline regarding demographic factors, duration and severity of complaints, percentage of patients with neurological symptoms, and value of main outcome measure(s). |
| 10 | If there were no co‐interventions or they were similar between the index and control groups. |
| 11 | The reviewer determines if the compliance with the interventions is acceptable, based on the reported intensity, duration, number and frequency of sessions for both the index intervention and control intervention(s). For example, physiotherapy treatment is usually administered for several sessions; therefore it is necessary to assess how many sessions each patient attended. For single‐session interventions (e.g., surgery), this item is irrelevant. |
| 12 | Timing of outcome assessment should be identical for all intervention groups and for all primary outcome measures. |
| 13 | Other types of biases. For example:
|
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain Show forest plot | 7 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 short‐term follow‐up (<3 months) | 6 | 647 | Mean Difference (IV, Random, 95% CI) | ‐6.10 [‐10.18, ‐2.01] |
| 1.2 intermediate‐term follow up (3‐6 months) | 4 | 257 | Mean Difference (IV, Random, 95% CI) | ‐4.34 [‐14.37, 5.68] |
| 1.3 long‐term follow‐up (>6 months) | 3 | 244 | Mean Difference (IV, Random, 95% CI) | ‐12.16 [‐29.14, 4.83] |
| 2 Disability Show forest plot | 4 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 short‐term follow‐up (<3 months) | 3 | 426 | Mean Difference (IV, Random, 95% CI) | ‐3.38 [‐6.70, ‐0.05] |
| 2.2 intermediate‐term follow up (3‐6 months) | 3 | 181 | Mean Difference (IV, Random, 95% CI) | ‐5.92 [‐12.08, 0.23] |
| 2.3 long‐term follow‐up (>6 months) | 2 | 124 | Mean Difference (IV, Random, 95% CI) | ‐7.36 [‐22.05, 7.34] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain Show forest plot | 5 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 short‐term follow‐up (<3 months) | 3 | 249 | Mean Difference (IV, Random, 95% CI) | ‐10.16 [‐19.11, ‐1.22] |
| 1.2 intermediate‐term follow up (3‐6 months) | 5 | 545 | Mean Difference (IV, Random, 95% CI) | ‐9.65 [‐22.46, 3.15] |
| 1.3 long‐term follow‐up (>6 months) | 3 | 406 | Mean Difference (IV, Random, 95% CI) | ‐5.71 [‐20.27, 8.84] |
| 2 Disability Show forest plot | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 short‐term follow‐up (<3 months) | 2 | 130 | Mean Difference (IV, Random, 95% CI) | ‐1.19 [‐7.02, 4.64] |
| 2.2 intermediate‐term follow up (3‐6 months) | 3 | 331 | Mean Difference (IV, Random, 95% CI) | ‐6.34 [‐10.89, ‐1.79] |
| 2.3 long‐term follow‐up (>6 months) | 1 | 201 | Mean Difference (IV, Random, 95% CI) | ‐0.40 [‐7.33, 6.53] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain Show forest plot | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 short‐term follow‐up (<3 months) | 3 | 290 | Mean Difference (IV, Random, 95% CI) | 1.96 [‐9.51, 13.43] |
| 1.2 intermediate‐term follow up (3‐6 months) | 3 | 290 | Mean Difference (IV, Random, 95% CI) | ‐16.89 [‐66.56, 32.79] |
| 1.3 long‐term follow‐up (>6 months) | 3 | 291 | Mean Difference (IV, Random, 95% CI) | ‐12.86 [‐61.22, 35.50] |
| 2 Disability Show forest plot | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 short‐term follow‐up (<3 months) | 2 | 180 | Mean Difference (IV, Random, 95% CI) | 2.57 [‐15.88, 21.01] |
| 2.2 intermediate‐term follow up (3‐6 months) | 2 | 180 | Mean Difference (IV, Random, 95% CI) | 6.88 [‐4.86, 18.63] |
| 2.3 long‐term follow‐up (>6 months) | 2 | 180 | Mean Difference (IV, Random, 95% CI) | 9.60 [3.65, 15.54] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain Show forest plot | 6 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 short‐term follow‐up (<3 months) | 5 | 416 | Mean Difference (IV, Random, 95% CI) | ‐2.06 [‐14.58, 10.45] |
| 1.2 intermediate‐term follow up (3‐6 months) | 4 | 619 | Mean Difference (IV, Random, 95% CI) | ‐4.46 [‐19.44, 10.52] |
| 1.3 long‐term follow‐up (>6 months) | 3 | 461 | Mean Difference (IV, Random, 95% CI) | 4.58 [‐0.20, 9.36] |
| 2 Disability Show forest plot | 8 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 short‐term follow‐up (<3 months) | 6 | 471 | Mean Difference (IV, Random, 95% CI) | ‐1.65 [‐8.66, 5.37] |
| 2.2 intermediate‐term follow up (3‐6 months) | 6 | 766 | Mean Difference (IV, Random, 95% CI) | 1.57 [‐3.86, 7.00] |
| 2.3 long‐term follow‐up (>6 months) | 4 | 556 | Mean Difference (IV, Random, 95% CI) | 4.54 [‐4.44, 13.52] |