Les interventions visant à améliorer l'accès au traitement chirurgical de la cataracte et leur impact sur l'équité dans les pays à revenu faible et intermédiaire
Appendices
Appendix 1. CENTRAL search strategy
#1 MeSH descriptor: [Cataract] explode all trees
#2 MeSH descriptor: [Cataract Extraction] this term only
#3 cataract*
#4 MeSH descriptor: [Lens, Crystalline] explode all trees
#5 MeSH descriptor: [Lenses, Intraocular] explode all trees
#6 MeSH descriptor: [Lens Implantation, Intraocular] this term only
#7 (intraocular lens* or intra ocular lens* or IOL*)
#8 MeSH descriptor: [Phacoemulsification] this term only
#9 pha?oemulsif*
#10 (phaco or phako)
#11 ECCE
#12 (MISICS or SICS)
#13 MeSH descriptor: [Capsulorhexis] this term only
#14 capsulor?hexis
#15 #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14
#16 MeSH descriptor: [Resource Allocation] this term only
#17 MeSH descriptor: [Fees and Charges] this term only
#18 MeSH descriptor: [Fee‐for‐Service Plans] this term only
#19 MeSH descriptor: [Health Care Costs] this term only
#20 (pay* or paid or fee or cost*) near/3 surg*
#21 MeSH descriptor: [Delivery of Health Care] this term only
#22 MeSH descriptor: [State Medicine] this term only
#23 MeSH descriptor: [National Health Programs] this term only
#24 MeSH descriptor: [Quality of Health Care] explode all trees
#25 MeSH descriptor: [Quality Assurance, Health Care] explode all trees
#26 MeSH descriptor: [Health Services Accessibility] this term only
#27 MeSH descriptor: [Health Policy] this term only
#28 MeSH descriptor: [Surgical Procedures, Operative] this term only
#29 MeSH descriptor: [Surgical Equipment] explode all trees
#30 MeSH descriptor: [Health Care Rationing] this term only
#31 MeSH descriptor: [Medically Underserved Area] this term only
#32 MeSH descriptor: [Mass Screening] this term only
#33 MeSH descriptor: [Vision Tests] explode all trees
#34 vis* near/3 (screen* or test*)
#35 MeSH descriptor: [Health Personnel] this term only
#36 MeSH descriptor: [Clinical Competence] this term only
#37 MeSH descriptor: [Clinical Competence] this term only
#38 MeSH descriptor: [Professional Autonomy] this term only
#39 MeSH descriptor: [Healthcare Disparities] this term only
#40 MeSH descriptor: [Health Status Disparities] explode all trees
#41 MeSH descriptor: [Attitude to Health] explode all trees
#42 MeSH descriptor: [Patient Acceptance of Health Care] explode all trees
#43 MeSH descriptor: [Health Education] this term only
#44 MeSH descriptor: [Public Opinion] this term only
#45 MeSH descriptor: [Health Behavior] this term only
#46 MeSH descriptor: [Social Behavior] this term only
#47 MeSH descriptor: [Superstitions] this term only
#48 MeSH descriptor: [Socioeconomic Factors] explode all trees
#49 MeSH descriptor: [Communication] explode all trees
#50 MeSH descriptor: [Culture] explode all trees
#51 MeSH descriptor: [Sex Factors] this term only
#52 MeSH descriptor: [Womens Rights] this term only
#53 MeSH descriptor: [Prejudice] this term only
#54 MeSH descriptor: [Vulnerable Populations] this term only
#55 MeSH descriptor: [Rural Health Services] this term only
#56 transport* near/5 (hospital* or clinic* or access* or provi*)
#57 MeSH descriptor: [Rural Population] this term only
#58 health near/20 (barrier* or belie* or inform* or aware* or knowledge or perceive* or consequence* or uptake or seek* or underutili* or fear* or stigma* or inequaliti* or gender or logistic* or distance*)
#59 #16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29 or #30 or #31 or #32 or #33 or #34 or #35 or #36 or #37 or #38 or #39 or #40 or #41 or #42 or #43 or #44 or #45 or #46 or #47 or #48 or #49 or #50 or #51 or #52 or #53 or #54 or #55 or #56 or #57 or #58
#60 MeSH descriptor: [Developing Countries] explode all trees
#61 MeSH descriptor: [Africa] explode all trees
#62 MeSH descriptor: [Caribbean Region] this term only
#63 MeSH descriptor: [Central America] this term only
#64 MeSH descriptor: [Latin America] this term only
#65 MeSH descriptor: [South America] this term only
#66 MeSH descriptor: [Asia] explode all trees
#67 MeSH descriptor: [China] explode all trees
#68 MeSH descriptor: [Pacific Islands] explode all trees
#69 #60 or #61 or #62 or #63 or #64 or #65 or #66 or #67 or #68
#70 #15 and #59 and #69
Appendix 2. MEDLINE Ovid search strategy
1. randomized controlled trial.pt.
2. (randomized or randomised).ab,ti.
3. placebo.ab,ti.
4. dt.fs.
5. randomly.ab,ti.
6. trial.ab,ti.
7. groups.ab,ti.
8. or/1‐7
9. exp animals/
10. exp humans/
11. 9 not (9 and 10)
12. 8 not 11
13. controlled clinical trial/
14. (control adj3 (area or cohort? or compare? or condition or design or group? or intervention? or participant? or study)).ab. not (controlled clinical trial or randomized controlled trial).pt.
15. ((evaluation or prospective or retrospective) adj1 study).tw.
16. ("quasi‐experiment$" or quasiexperiment$ or "quasi random$" or quasirandom$ or "quasi control$" or quasicontrol$ or ((quasi$ or experimental) adj3 (method$ or study or trial or design$))).tw.
17. ("time series" adj2 interrupt$).tw.
18. (intervention$ or impact or effectiveness or efficacy or service$ or outcome$ or output or treatment$ or management or program$ or project$).tw.
19. or/13‐18
20. 12 or 19
21. exp cataract/
22. cataract extraction/
23. cataract$.tw.
24. exp lens crystalline/
25. exp lenses intraocular/
26. lens implantation intraocular/
27. (intraocular lens$ or intra ocular lens$ or IOL$).tw.
28. phacoemulsification/
29. pha?oemulsif$.tw.
30. (phaco or phako).tw.
31. ECCE.tw.
32. (MISICS or SICS).tw.
33. capsulorhexis/
34. capsulor?hexis.tw.
35. or/21‐34
36. Resource Allocation/
37. "Fees and Charges"/
38. Fee‐for‐Service Plans/
39. Health Care Costs/
40. ((pay$ or paid or fee or cost$) adj3 surg$).tw.
41. Delivery of Health Care/
42. State Medicine/
43. National Health Programs/
44. exp "Quality of Health Care"/
45. exp Quality Assurance, Health Care/
46. Health Services Accessibility/
47. Health Policy/
48. Surgical Procedures, Operative/
49. exp Surgical Equipment/
50. Health Care Rationing/
51. Medically Underserved Area/
52. Mass Screening/
53. exp Vision Tests/
54. (vis$ adj3 (screen$ or test$)).tw.
55. Health Personnel/
56. Clinical Competence/
57. Professional Competence/
58. Professional Autonomy/
59. Healthcare Disparities/
60. Health Status Disparities/
61. exp Attitude to Health/
62. "Patient Acceptance of Health Care"/
63. Health Education/
64. Public Opinion/
65. Health Behavior/
66. Social Behavior/
67. Superstitions/
68. exp Socioeconomic Factors/
69. exp Communication/
70. exp Culture/
71. Sex Factors/
72. Women's Rights/
73. Prejudice/
74. Vulnerable Populations/
75. Rural Health Services/
76. (transport$ adj5 (hospital$ or clinic$ or access$ or provi$)).tw.
77. Rural Population/
78. (health adj20 (barrier$ or belie$ or inform$ or aware$ or knowledge or perceive$ or consequence$ or uptake or seek$ or underutili$ or fear$ or stigma$ or inequaliti$ or gender or logistic$ or distance$)).tw.
79. or/36‐78
80. exp developing countries/
81. exp africa/
82. caribbean region/ or central america/ or latin america/ or south america/
83. exp asia/
84. exp china/
85. exp pacific islands/
86. or/80‐85
87. 79 and 86
88. 35 and 87
89. 20 and 88
The search filter for trials at the beginning of the MEDLINE strategy is from the published paper by Glanville 2006.
Appendix 3. Embase Ovid search strategy
1. exp randomized controlled trial/
2. exp randomization/
3. exp double blind procedure/
4. exp single blind procedure/
5. random$.tw.
6. or/1‐5
7. (animal or animal experiment).sh.
8. human.sh.
9. 7 and 8
10. 7 not 9
11. 6 not 10
12. exp clinical trial/
13. (clin$ adj3 trial$).tw.
14. ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$)).tw.
15. exp placebo/
16. placebo$.tw.
17. random$.tw.
18. exp experimental design/
19. exp crossover procedure/
20. exp control group/
21. exp latin square design/
22. or/12‐21
23. 22 not 10
24. 23 not 11
25. exp comparative study/
26. exp evaluation/
27. exp prospective study/
28. (control$ or prospectiv$ or volunteer$).tw.
29. or/25‐28
30. 29 not 10
31. 30 not (11 or 23)
32. 11 or 24 or 31
33. controlled clinical trial/
34. (control adj3 (area or cohort? or compare? or condition or design or group? or intervention? or participant? or study)).ab. not (controlled clinical trial or randomized controlled trial).pt.
35. ((evaluation or prospective or retrospective) adj1 study).tw.
36. ("quasi‐experiment$" or quasiexperiment$ or "quasi random$" or quasirandom$ or "quasi control$" or quasicontrol$ or ((quasi$ or experimental) adj3 (method$ or study or trial or design$))).tw.
37. ("time series" adj2 interrupt$).tw.
38. (intervention$ or impact or effectiveness or efficacy or service$ or outcome$ or output or treatment$ or management or program$ or project$).tw.
39. or/33‐38
40. 32 or 39
41. exp cataract/
42. exp cataract extraction/
43. exp lens/
44. exp lens implant/
45. exp lens implantation/
46. (intraocular lens$ or intra ocular lens$ or IOLS).tw.
47. phacoemulsification/
48. pha?oemulsif$.tw.
49. (phaco or phako).tw.
50. ECCE.tw.
51. (MISICS or SICS).tw.
52. capsulorhexis/
53. capsulor?hexis.tw.
54. or/41‐53
55. Resource Allocation/
56. Medical Fee/
57. Health Care Cost/
58. ((pay$ or paid or fee or cost$) adj3 surg$).tw.
59. Health Care Delivery/
60. National Health Service/
61. Public Health/
62. Health Care Quality/
63. Health Care Delivery/
64. Health Care Policy/
65. exp Surgery/
66. exp Surgical Equipment/
67. Health Care Organization/
68. Medically Underserved/
69. Mass Screening/
70. exp Vision Test/
71. (vis$ adj3 (screen$ or test$)).tw.
72. Health Care Personnel/
73. Clinical Competence/
74. Professional Competence/
75. Professional Practice/
76. Health Care Disparity/
77. Health Disparity/
78. exp Attitude to Health/
79. Patient Attitude/
80. Health Education/
81. Public Opinion/
82. Health Behavior/
83. Social Behavior/
84. Superstition/
85. Socioeconomics/
86. exp Interpersonal Communication/
87. exp Cultural Anthropology/
88. Sex Difference/
89. Women's Rights/
90. Social Psychology/
91. Vulnerable Populations/
92. Rural Health Care/
93. (transport$ adj5 (hospital$ or clinic$ or access$ or provi$)).tw.
94. Rural Population/
95. (health adj20 (barrier$ or belie$ or inform$ or aware$ or knowledge or perceive$ or consequence$ or uptake or seek$ or underutili$ or fear$ or stigma$ or inequaliti$ or gender or logistic$ or distance$)).tw.
96. or/55‐95
97. exp Developing Country/
98. exp africa/
99. South America/
100. Central America/
101. exp asia/
102. exp china/
103. exp pacific islands/
104. or/97‐103
105. 54 and 96 and 104
106. 40 and 105
Appendix 4. LILACS search strategy
cataract and developing country
Appendix 5. ISRCTN search strategy
cataract and developing country
Appendix 6. ClinicalTrials.gov search strategy
Cataract AND Developing Country
Appendix 7. ICTRP search strategy
cataract AND developing country
Appendix 8. Data extraction characteristics
| Mandatory items | Optional items | |
| Methods | ||
| Study design | · Parallel group RCTi.e. people randomised to treatment · Within‐person RCTi.e. eyes randomised to treatment · Cluster‐RCTi.e. communities randomised to treatment · Cross‐over RCT · Other, specify | Exclusions after randomisation Losses to follow‐up Number randomised/analysed Reported power calculation (Y/N), if yes, sample size and power Unusual study design/issues |
| Eyes or Unit of randomisation/ unit of analysis | · One eye included in study, specify how eye selected · Two eyes included in study, both eyes received same treatment, briefly specify how analysed (best/worst/average/both and adjusted for within person correlation/both and not adjusted for within person correlation) and specify if mixture one eye and two eye · Two eyes included in study, eyes received different treatments,specify if correct pair‐matched analysis done | |
| Participants | ||
| Country | Setting Ethnic group Equivalence of baseline characteristics (Y/N) | |
| Total number of participants | This information should be collected for total study population recruited into the study. If these data are reported for the people who were followed up only, please indicate. | |
| Number (%) of men and women | ||
| Average age and age range | ||
| Inclusion criteria | ||
| Exclusion criteria | ||
| Interventions | ||
| Intervention (n = ) Comparator (n = ) See MECIR 65 and 70 | · Number of people randomised to this group · Drug (or intervention) name · Dose · Frequency · Route of administration | |
| Outcomes | ||
| Primary and secondary outcomes as defined in study reports See MECIR R70 | List outcomes Adverse events reported (Y/N) Length of follow‐up and intervals at which outcomes assessed | Planned/actual length of follow‐up |
| Notes | ||
| Date conducted | Specify dates of recruitment of participants mm/yr to mm/yr | Full study name: (if applicable) Reported subgroup analyses (Y/N) Were trial investigators contacted? |
| Sources of funding | ||
| Declaration of interestSee MECIR 69 | ||

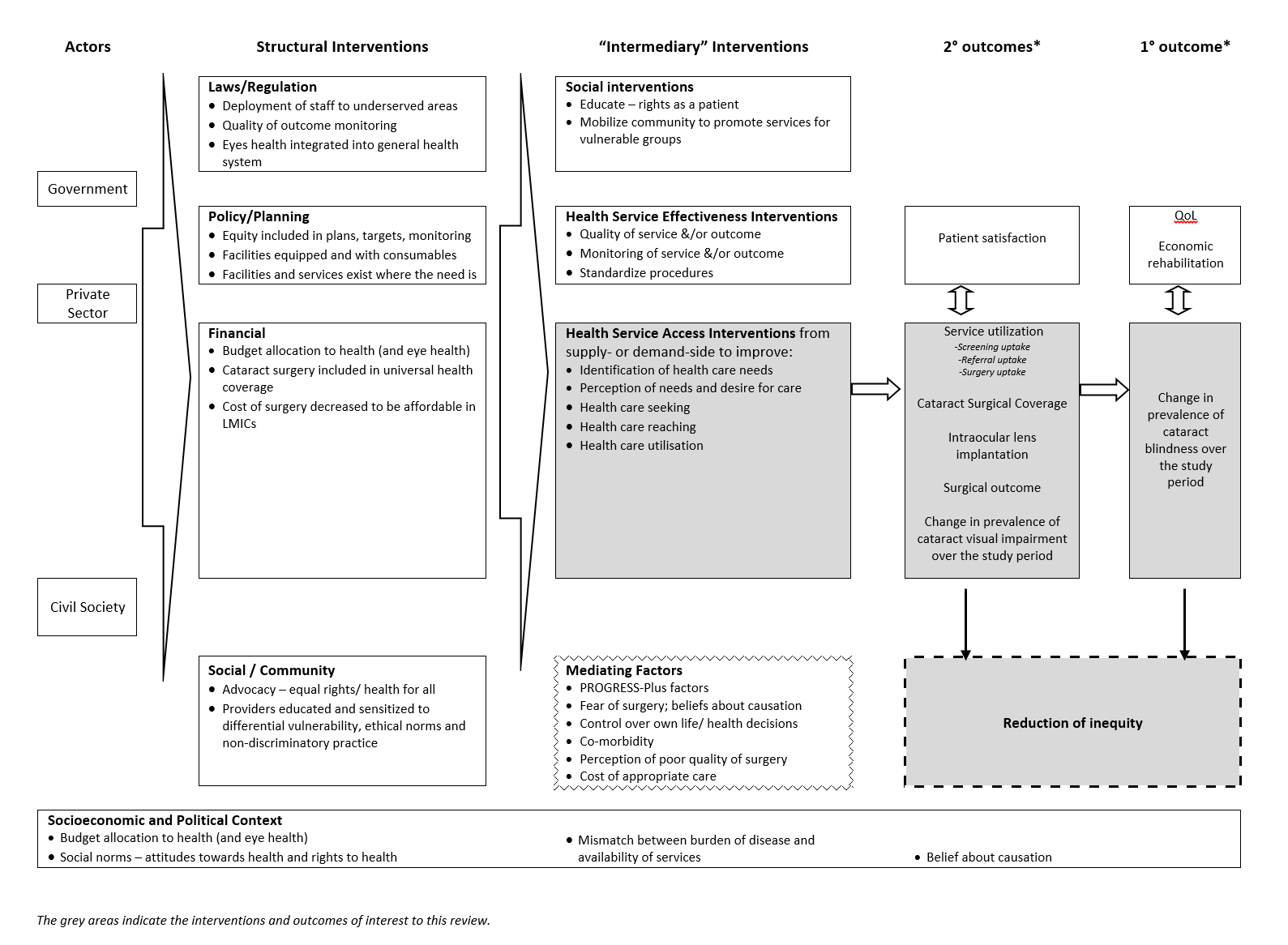
Examples of interventions to improve access to cataract surgical services against Levesque and colleague’s1 conceptual framework of access to health care (Levesque 2013)

Study flow diagram

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies

Risk of bias summary: review authors' judgements about each risk of bias item for each included study
| Information video and counselling to improve access to cataract surgical services compared with standard care for cataract | ||||||
| Patient or population: people with vision impairment caused by cataract Settings: low‐ and middle‐income settings Intervention: information video and counselling* Comparison: standard care | ||||||
| Outcomes | Illustrative comparative risks** (95% CI) | Relative effect | No of participants | Certainty of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Standard care | Intervention to improve access to cataract surgical services | |||||
| Change in the prevalence of cataract blindness | Not reported | |||||
| Prevalence of visual impairment due to cataract | Not reported | |||||
| Service utilisation: uptake of referral | 400 per 1000 | 407 per 1000 (296 to 527) | OR 1.03 (0.63 to 1.67 | 434 (1) | ⊕⊕⊝⊝ Low1 | |
| Service utilisation: uptake of surgery | 340 per 1000 | 364 per 1000 (257 to 487) | OR 1.11 (0.67 to 1.84 | 434 (1) | ⊕⊕⊝⊝ Low1 | |
| Cataract Surgical Coverage | Not reported | |||||
| Surgical outcome (visual acuity in the operated eye) | Not reported | |||||
| Adverse events | Not reported | |||||
| *In this study, the intervention group (n = 212) watched a five‐minute informational video on cataract and cataract surgery then received a five‐minute counselling session (based on a script) from a trained nurse in groups of two to three, with family members. The control group (n = 222) were given standard care: they were advised they had decreased vision due to cataract and it could be treated, without being shown the video or receiving counselling. **The assumed risk was the risk observed in the control group of this study. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1We downgraded by one level for imprecision (wide confidence intervals) and one level for indirectness (study was conducted in rural China and may not be applicable to other settings). | ||||||
| Surgery fee waiver with/without transport provision or reimbursement to improve access to cataract surgical services compared with standard care for cataract | ||||||
| Patient or population: people with vision impairment caused by cataract Settings: low‐ and middle‐income settings Intervention: financial incentives and/or reimbursement* Comparison: standard care | ||||||
| Outcomes | Illustrative comparative risks** (95% CI) | Relative effect | No of participants | Certainty of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Standard care | Intervention to improve access to cataract surgical services | |||||
| Change in the prevalence of cataract blindness | Not reported | |||||
| Prevalence of visual impairment due to cataract | Not reported | |||||
| Service utilisation: uptake of referral | Not reported | |||||
| Service utilisation: uptake of surgery | 150 per 1000 | 291 per 1000 (171 to 497) | RR 1.94 (1.14 to 3.31) | 355 (1) | ⊕⊕⊝⊝ Low1 | |
| Cataract Surgical Coverage | Not reported | |||||
| Surgical outcome (visual acuity in the operated eye) | Not reported | |||||
| Adverse events | ||||||
| * In this study, there were three intervention arms and a comparator arm: we have combined the intervention arms to display the results as there were no differences between them.
**The assumed risk was the risk observed in the control group of this study. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1We downgraded by one level for imprecision (wide confidence intervals and statistical analysis not adjusted for cluster randomised design) and one level for indirectness (study was conducted in rural China and may not be applicable to other settings). | ||||||
| Category | Presenting distance visual acuity | |
| Worse than: | Equal to or better than: | |
| 0 Mild or no visual impairment | 6/18 | |
| 1 Moderate visual impairment | 6/18 | 6/60 |
| 2 Severe visual impairment | 6/60 | 3/60 |
| 3 Blindness | 3/60 | 1/60* |
| 4 Blindness | 1/60* | light perception |
| 5 Blindness | No light perception | |
| 9 | Undetermined or unspecified | |
| *or counts fingers (CF) at 1 metre | ||
| The term visual impairment comprises categories 1 to 5; blindness comprises categories 3 to 5 (Pascolini 2012). | ||
| Explanatory factors | In which subgroup is the effect hypothesised to be larger |
| Type of intervention | |
| Uni‐faceted versus multi‐faceted | It is hypothesised that multi‐faceted interventions will have a larger effect than uni‐faceted intentions (Chang 2008). |
| Targeted versus universal | It is hypothesised that targeted interventions will produce a larger effect for socially disadvantaged groups than universal interventions; universal interventions may benefit socially advantaged groups more than socially disadvantaged groups, and thereby increase inequity (Lorenc 2013). |
| Supply‐side versus demand‐side | Demand‐side interventions are unlikely to be effective if surgery is not accessible and affordable. Supply‐side interventions might not be effective if there are unaddressed problems with demand. |
| Population characteristics | |
| Gender/sex: | Women have more barriers and less access to cataract surgical services than men (Lewallen 2009). Lack of social support to seek care is a major barrier for women. It is hypothesised that interventions that aim to modify women’s ability to perceive, to seek or to reach care (Figure 1) will produce larger effects for women than men, while universal interventions may produce larger effects for men. |
| SES/education/occupation: | People with low SES/education have more barriers and less access to cataract surgical services than people with higher SES/education (Abubakar 2012; Jadoon 2007; Kuper 2008). It is hypothesised that interventions targeted to low‐SES people (especially in relation to ability to pay in Figure 1) would produce larger effects than for high‐SES people, while universal interventions may produce larger effects for high‐SES. |
| Place of residence: | As services tend to be located in urban areas, rural dwellers tend to have less access to cataract surgical services than urban dwellers (Abubakar 2012; Jadoon 2007). It is hypothesised that interventions that address barriers faced by rural dwellers (such as those relating to availability and accommodation/ability to reach in Figure 1) would produce larger effects for rural dwellers, while other types of interventions may not produce a difference between urban and rural dwellers. |
| SES: socioeconomic status | |
| Number of people | Odds ratio (95% CI) | Test for interaction (P value) | |
| Outcome: uptake of referral | |||
| Place of residence | |||
| < 1 hour from hospital | 225 | 0.86 (0.50 to 1.48) | 0.49 |
| ≥ 1 hour from hospital | 209 | 1.13 (0.65 to 1.95) | |
| Gender | |||
| Men | 185 | 0.77 (0.42 to 1.38) | 0.35 |
| Women | 249 | 1.11 (0.67 to 1.85) | |
| Education | |||
| Received some formal education | 196 | 1.40 (0.80 to 2.47) | 0.09 |
| Received no formal education | 238 | 0.71 (0.42 to 1.21) | |
| Socioeconomic status | |||
| Patient will self‐pay for surgery | 78 | 1.05 (0.42 to 2.62) | 0.81 |
| Patient will not self‐pay for surgery | 356 | 0.93 (0.61 to 1.42) | |
| Higher anticipated loss of income | 246 | 0.89 (0.54 to 1.48) | 0.63 |
| Lower anticipated loss of income | 167 | 1.10 (0.57 to 2.13) | |
| More floor space/resident | 222 | 0.78 (0.45 to 1.33) | 0.28 |
| Less floor space/resident | 212 | 1.19 (0.69 to 2.05) | |
| Social capital | |||
| Family member can accompany to hospital for surgery | 369 | 0.98 (0.65 to 1.49) | 0.66 |
| Family member can not accompany to hospital for surgery | 65 | 0.77 (0.29 to 2.09) | |
| Family member accompanied patient to screening | 188 | 0.95 (0.53 to 1.70) | 0.77 |
| Family member did not accompany patient to screening | 246 | 1.07 (0.63 to 1.82) | |
| Outcome: uptake of surgery | |||
| Place of residence | |||
| < 1 hour from hospital | 225 | 0.63 (0.36 to 1.13) | 0.10 |
| ≥ 1 hour from hospital | 209 | 1.26 (0.71 to 2.22) | |
| Gender | |||
| Men | 185 | 0.88 (0.48 to 1.64) | 0.94 |
| Women | 249 | 0.85 (0.50 to 1.45) | |
| Education | |||
| Received some formal education | 196 | 1.20 (0.67 to 2.15) | 0.17 |
| Received no formal education | 238 | 0.68 (0.39 to 1.19) | |
| Socioeconomic status | |||
| Patient will self‐pay for surgery | 78 | 0.98 (0.37 to 2.59) | 0.80 |
| Patient will not self‐pay for surgery | 356 | 0.85 (0.55 to 1.33) | |
| Higher anticipated loss of income | 246 | 0.85 (0.51 to 1.43) | 0.58 |
| Lower anticipated loss of income | 167 | 1.09 (0.54 to 2.23) | |
| More floor space/resident | 222 | 0.79 (0.44 to 1.40) | 0.57 |
| Less floor space/resident | 212 | 1.00 (0.57 to 1.75) | |
| Social capital | |||
| Family member can accompany to hospital for surgery | 369 | 0.88 (0.57 to 1.36) | 0.86 |
| Family member can not accompany to hospital for surgery | 65 | 0.80 (0.28 to 2.30) | |
| Family member accompanied patient to screening | 188 | 1.05 (0.58 to 1.88) | 0.64 |
| Family member did not accompany patient to screening | 246 | 0.86 (0.48 to 1.53) | |
| Effect measure: odds ratio; analysis model: fixed effects. | |||