Productos con xilitol para la prevención de caries dentales en niños y adultos
Información
- DOI:
- https://doi.org/10.1002/14651858.CD010743.pub2Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 26 marzo 2015see what's new
- Tipo:
-
- Intervention
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Salud oral
- Copyright:
-
- Copyright © 2015 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
Protocol
-
Conceiving the idea: Helen Worthington (HW) and Mohammad O Sharif (MOS).
-
Writing the protocol: MOS, Farooq Ahmed (FA) and HW.
Review
-
Screening the search results and retrieving the papers: Philip Riley (PR), Deborah Moore (DM), HW, MOS and FA.
-
Data extraction and risk of bias assessment: PR, DM and HW.
-
Analysing the data and interpreting the results: PR, DM and HW.
-
Writing the results, discussion, conclusions and abstract: PR, DM and HW.
-
Providing a clinical perspective: DM
Sources of support
Internal sources
-
The University of Manchester, UK.
-
Manchester Academic Health Sciences Centre (MAHSC), UK.
The Cochrane Oral Health Group is supported by MAHSC and the NIHR Manchester Biomedical Research Centre
External sources
-
National Institute for Health Research (NIHR), UK.
The NIHR is the largest single funder of the Cochrane Oral Health Group
Disclaimer:
The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the NIHR, NHS or the Department of Health -
Cochrane Oral Health Group Global Alliance, Other.
The production of all our reviews is assisted by funding from our Global Alliance partners (http://ohg.cochrane.org/): British Association for the Study of Community Dentistry, UK; British Association of Oral Surgeons, UK; British Orthodontic Society, UK; British Society of Paediatric Dentistry, UK; British Society of Periodontology, UK; Canadian Dental Hygienists Association, Canada; Mayo Clinic, USA; National Center for Dental Hygiene Research & Practice, USA; New York University College of Dentistry, USA; and Royal College of Surgeons of Edinburgh, UK
Declarations of interest
There are no financial conflicts of interest and the review authors declare that they do not have any associations with any parties who may have vested interests in the results of this review.
Acknowledgements
We would like to thank Mohammad O Sharif for his help with the protocol and search results screening. We would also like to thank the Cochrane Oral Health Group editorial team and external referees (Professor James D Bader and Mr Derek Richards) for their help in conducting this systematic review.
Version history
| Published | Title | Stage | Authors | Version |
| 2015 Mar 26 | Xylitol‐containing products for preventing dental caries in children and adults | Review | Philip Riley, Deborah Moore, Farooq Ahmed, Mohammad O Sharif, Helen V Worthington | |
| 2013 Sep 11 | Xylitol‐containing products for preventing dental caries in children and adolescents | Protocol | Mohammad O Sharif, Farooq Ahmed, Helen V Worthington | |
Differences between protocol and review
-
We decided to include adults in order to make the review more relevant and usable.
-
In the section 'Data extraction and management' we changed the text 'Data will be collected at all time points' to 'We will report the longest term data available'. We consider longer term data to be more valuable for caries prevention as we feel it will better demonstrate whether or not an effect is sustained.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
Medical Subject Headings Check Words
Adolescent; Adult; Child; Child, Preschool; Female; Humans; Infant; Male;
PICO

Study flow diagram.
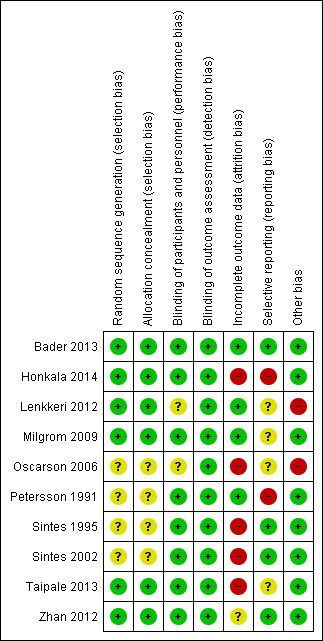
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Comparison 1 Adults: xylitol lozenges versus control lozenges, Outcome 1 Caries increment at 33 months follow‐up (DFS).

Comparison 2 Children: xylitol lozenges versus no treatment, Outcome 1 Caries increment at 4 years follow‐up (DMFS).

Comparison 2 Children: xylitol lozenges versus no treatment, Outcome 2 Number with caries increment at 4 years follow‐up (as opposed to none/no change).

Comparison 3 Children: xylitol topical oral syrup versus control syrup (very low dose xylitol), Outcome 1 Number of decayed primary teeth at 1 year follow‐up.

Comparison 4 Children: xylitol sucking tablets versus no treatment, Outcome 1 Caries increment at 2 years follow‐up (dmfs).

Comparison 4 Children: xylitol sucking tablets versus no treatment, Outcome 2 Number with caries increment at 2 years follow‐up (as opposed to none/no change).

Comparison 5 Children: xylitol plus fluoride toothpaste versus fluoride toothpaste, Outcome 1 Caries increment at 2.5 to 3 years follow‐up (Prevented Fraction).

Comparison 5 Children: xylitol plus fluoride toothpaste versus fluoride toothpaste, Outcome 2 Caries increment at 2.5 to 3 years follow‐up (DFS).

Comparison 6 Children: xylitol tablets versus control (sorbitol) tablets, Outcome 1 Number with caries increment at 4 years follow‐up (as opposed to none/no change).

Comparison 7 Children: xylitol wipes versus control wipes, Outcome 1 Number with caries increment at 1 year follow‐up (as opposed to none/no change).
| Xylitol toothpaste compared with control toothpaste for preventing dental caries | ||||||
| Patient or population: children with permanent teeth Settings: schools Intervention: fluoride toothpaste containing 10% xylitol Comparison: fluoride toothpaste | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Xylitol | |||||
| Caries: increment (DFS) prevented fraction (PF) at 2.5 to 3 years follow‐up (higher DFS score indicates worse caries) | The (weighted) mean caries increment for control groups was | The mean caries increment in the xylitol groups was 0.28 lower (0.42 to 0.14 lower) | PF¹ = 0.13 (0.08 to 0.18) | 4216 | ⊕⊕⊝⊝ | The PF of 0.13 means that there was a 13% reduction in caries in the xylitol group There is no compelling evidence, from other comparisons in this systematic review, to support the use of xylitol products. The body of evidence for all other comparisons and caries outcomes is rated as being low to very low quality. This is because they are single studies with imprecision mostly due to very small sample sizes, and most of which have a high risk of bias |
| Adverse effects | Both studies reported that there were no adverse effects in either the xylitol or control group | |||||
| CI: Confidence interval; DFS: decayed filled surfaces; PF: prevented fraction | ||||||
| GRADE Working Group grades of evidence | ||||||
| ¹ The prevented fraction (PF) is calculated as follows: the mean increment in the controls minus the mean increment in the treated group divided by the mean increment in the controls ² Downgraded due to high risk of bias in the included studies (due to high attrition) and both studies were conducted by the same authors in the same population | ||||||
| Comparison (number) | Increment (Study) | PF (95% CI) | Notes |
| Adults | |||
| Xylitol lozenges versus control lozenges (1.1) | 33‐month caries increment (Bader 2013) | 0.08 (–0.03 to 0.20) | 8% reduction in caries in test group |
| Children | |||
| Xylitol lozenges versus no treatment (2.1) | 4 year caries increment (Lenkkeri 2012)
| ‐0.10 (‐0.59 to 0.39) | 10% increase in caries in test group compared to control |
|
| |||
| Xylitol topical oral syrup versus control syrup (3.1) | Caries in primary teeth over 1 year follow‐up (Milgrom 2009) | 0.58 (0.33 to 0.83) | 58% reduction in caries in test group |
|
| |||
| Xylitol sucking tablets versus no treatment (4.1) | 2 year caries increment (Oscarson 2006) | 0.53 (0.001 to 1.04) | 53% reduction in caries in test group |
|
| |||
| Xylitol plus fluoride toothpaste versus fluoride toothpaste (5.1) | 2.5 to 3 year caries increment (Sintes 1995) | 0.12 (0.06 to 0.18) | 12% reduction in caries in test group |
| 2.5 to 3 year caries increment (Sintes 2002) | 0.14 (0.05 to 0.23) | 14% reduction in caries in test group | |
| CI = confidence interval | |||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Caries increment at 33 months follow‐up (DFS) Show forest plot | 1 | 669 | Mean Difference (IV, Fixed, 95% CI) | ‐0.64 [‐1.58, 0.30] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Caries increment at 4 years follow‐up (DMFS) Show forest plot | 1 | 97 | Mean Difference (IV, Fixed, 95% CI) | 0.28 [‐0.99, 1.55] |
| 2 Number with caries increment at 4 years follow‐up (as opposed to none/no change) Show forest plot | 1 | 97 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.83, 1.26] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Number of decayed primary teeth at 1 year follow‐up Show forest plot | 1 | 94 | Mean Difference (IV, Fixed, 95% CI) | ‐1.10 [‐2.03, ‐0.18] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Caries increment at 2 years follow‐up (dmfs) Show forest plot | 1 | 118 | Mean Difference (IV, Fixed, 95% CI) | ‐0.42 [‐1.12, 0.28] |
| 2 Number with caries increment at 2 years follow‐up (as opposed to none/no change) Show forest plot | 1 | 118 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.35, 1.45] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Caries increment at 2.5 to 3 years follow‐up (Prevented Fraction) Show forest plot | 2 | Prevented Fraction (Fixed, 95% CI) | 0.13 [0.08, 0.18] | |
| 2 Caries increment at 2.5 to 3 years follow‐up (DFS) Show forest plot | 2 | 4216 | Mean Difference (IV, Fixed, 95% CI) | ‐0.28 [‐0.42, ‐0.14] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Number with caries increment at 4 years follow‐up (as opposed to none/no change) Show forest plot | 1 | 62 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.08 [0.69, 13.65] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Number with caries increment at 1 year follow‐up (as opposed to none/no change) Show forest plot | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.14 [0.02, 1.07] |