流感嗜血杆菌口服接种疫苗预防慢性支气管炎和慢性阻塞性肺病的急性恶化
摘要
研究背景
慢性支气管炎和慢性阻塞性肺病(chronic obstructive pulmonary disease,COPD)是严重的疾病,患者容易感染病毒和细菌从而导致潜在的致命性急性加重。慢性阻塞性肺病被定义为因肺部气流受限而正常呼吸困难的肺部疾病。抗生素疗法在根治如非可分型流感嗜血杆菌(non‐typeable Haemophilus influenzae,NTHi)等细菌方面并不是特别有效,因为它们是许多人上呼吸道中天然存在的菌群。但是,它们会引起机会性感染。已经开发出一种口服NTHi疫苗来预防复发性感染性慢性支气管炎的急性加重。
研究目的
本系统综述旨在评价口服全细胞NTHi疫苗在预防成人慢性支气管炎和COPD急性恶化的反复发作方面的有效性。评价NTHi疫苗在COPD急性恶化的反复发作期间抑制NTHi在呼吸道定植的有效性。
检索策略
我们检索了以下数据库:Cochrane对照试验中心注册库(Cochrane Central Register of Controlled Trials,CENTRAL)(2017年第1期)、MEDLINE(1946年至2017年1月)、Embase(1974年至2017年1月)、CINAHL(1981年至2017年1月)、LILACS(1985年至2017年1月)和Web of Science(1955年至2017年1月)。我们还检索了试验注册库并联系了试验作者以获取未发表的资料。
纳入排除标准
纳入随机对照试验,在疫苗组和安慰剂组在临床上明显匹配时,比较口服单细菌NTHi疫苗对慢性支气管炎或COPD复发性急性恶化成人患者的效果。选取标准考虑了65岁以下和65岁以上的人群。
资料收集与分析
两名综述作者独立评价了试验质量,并从原始记录和出版物中提取了关于支气管炎发作的发病率和严重程度、上呼吸道测量的NTHi携带率以及与其他主要和次要结局相关的资料。
主要结果
我们获得了六项安慰剂对照随机对照试验,共有557名受试者。这些试验研究了流感嗜血杆菌的肠溶灭活制剂在易复发慢性支气管炎或COPD急性恶化的人群中的疗效。所有试验中的疫苗制备和免疫方案包括至少三个疗程的福尔马林灭活的流感嗜血杆菌肠溶片,间隔服用(例如第0、28和56天)。每个疗程通常包括连续三天早餐后服用两片药。在所有情况下,安慰剂组都服用含有葡萄糖的肠溶片。整个研究的偏倚风险为中等,因为有关方法的信息缺失和结果报告不充分。
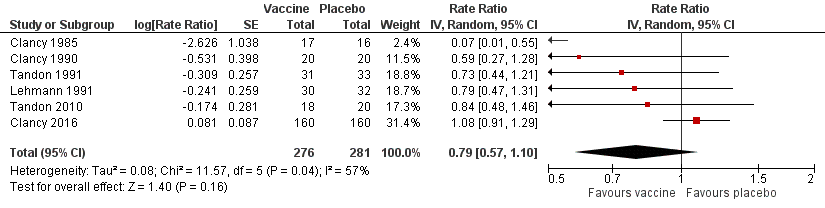
口服NTHi疫苗的meta分析显示,慢性支气管炎或COPD急性加重的发病率有小幅、非统计学意义的降低(风险比(risk ratio,RR)=0.79,95% 置信区间(confidence interval,CI)[0.57,1.10];P=0.16 )。疫苗组和安慰剂组之间的死亡率没有显著差异(比值比(odds ratio,OR)=1.62,95% CI [0.63,4.12];P=0.31)。
我们无法对受试者中NTHi的携带水平进行meta分析,因为每个试验报告这一结果时使用了不同的测量单位和工具。四项试验的携带水平没有显著差异,而两项试验显示与安慰剂组相比,接种疫苗组的携带水平显著降低。
四项试验通过对抗生素的需求来评价恶化的严重程度。其中三项试验具有可比性,meta分析显示安慰剂组中每人疗程中的抗生素有统计学意义上80%的增加(RR=1.81,95% CI [1.35,2.44];P<0.001)。两组间的住院率无显著差异(OR=0.96,95% CI [0.13,7.04];P=0.97)。五项试验报告了不良事件,但不一定与疫苗有关;一项点估计表明不良事件在疫苗组中发生的频率更高,但这一结果没有统计学意义(RR=1.43,95% CI [0.70,2.92];P=0.87)。两项试验中进行报告了生活质量,但未对其进行meta分析。六个月后的结果显示接种疫苗组的生活质量有所改善(得分至少比安慰剂高两分)。
作者结论
分析表明,慢性支气管炎或COPD反复恶化的患者口服NTHi疫苗不会显著减少恶化的次数和严重程度。证据参差不齐,显示疫苗有显著获益的个别试验规模太小,不足以支持提倡对COPD患者进行广泛的口服疫苗接种。
PICO
简语概要
流感嗜血杆菌口服接种疫苗预防慢性支气管炎和慢性阻塞性肺病的急性恶化
系统综述问题
我们评价了关于非可分型流感嗜血杆菌(non‐typeable Haemophilus influenzae,NTHi)疫苗预防慢性阻塞性肺病(chronic obstructive pulmonary disease,COPD)或慢性支气管炎患者反复感染流感嗜血杆菌效果的证据。
系统综述背景
慢性阻塞性肺病患者可能会经常感染,从而加重肺部疾病的症状,即呼吸困难加重、脓性分泌物增多和血氧饱和度失代偿,称为“急性加重”。最常见的病因细菌是流感嗜血杆菌。感染流感嗜血杆菌会导致住院,在某些情况下甚至会导致死亡。与目前在感染发生时进行的治疗做法相比,用疫苗预防这些感染可能会改善慢性阻塞性肺病患者的结局。
研究特征
目前,证据检索截至到2017年1月。我们获得了六项研究,共涉及557名受试者。这些研究是施盲、安慰剂对照的随机试验,测试了NTHi疫苗在预防18岁以上慢性阻塞性肺病或慢性支气管炎患者感染的有效性。在所有六项试验中,疫苗组和安慰剂组均在3至12个月的时间内定期服用至少三个疗程的药。通常情况下,纳入研究中受试者的基线人口统计数据与其他高收入国家具有相似的特征(如饮食、生活方式和生活条件)。年龄介于40至80岁之间。这些研究计算了受试者经历的感染次数、呼吸道细菌水平、死亡、副作用、住院或抗生素治疗。
主要结果
NTHi疫苗对减少COPD患者急性加重的次数没有显著影响。疫苗组和安慰剂组之间的死亡率没有显著差异,疫苗接种组报告的死亡与疫苗无关。
受试者呼吸道中的流感嗜血杆菌水平在疫苗组和安慰剂组间没有差异。由于试验之间的测量标准不一致,我们无法将这些研究相互比较。
抗生素可以成为严重感染的一个指标,在安慰剂组中明显更常见。住院证据表明,疫苗组和安慰剂组入院的可能性没有差异。两项研究生活质量的试验发现,接种疫苗的受试者通常生活质量更好,但这些结果的测量方式不同,因此无法进行比较。
五项试验报告了不良反应,但与疫苗组或安慰剂组没有特别关联。需要进一步研究将不良反应定义为结局指标,以便对疫苗副作用进行更明确的分析。
证据质量
研究进展良好,存在中度偏倚风险。本系统综述的主要局限性在于各个研究之间的定义和结局指标缺乏一致性,这影响了结果的整体综合和阐释。受试者的数量较少可能意味着结果更有可能受到机遇的影响。一项试验的受试者人数超过其他五项试验的总和,并且它对最终分析的贡献更大。当这项研究被纳入分析时,出现了中等的异质性(研究显示出截然不同的结果),尤其是在感染次数方面。然而,当从分析中删除该研究时,结果一致并且没有变化。
系统综述结论
在评价相关研究后,我们得出结论口服流感嗜血杆菌疫苗并不能显著降低慢性支气管炎和COPD患者急性加重的次数和严重程度。
Authors' conclusions
Summary of findings
| Haemophilus influenzae oral vaccination for prevention of acute exacerbations of chronic bronchitis and COPD | ||||||
| Patient or population: adults (> 18 years of age) with either COPD or recurrent acute exacerbations of chronic bronchitis Settings: community and outpatients Intervention: oral monobacterial vaccination with killed NTHi Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No. of participants | Quality of the evidence | Comments | |
| Assumed risk Not vaccinated | Corresponding risk NTHi oral vaccinated | |||||
| Acute exacerbations (number of exacerbations/person/year) | 2.111 exacerbations per person/year | 1.668 exacerbations | RR 0.79 (0.57 to 1.10) | 557 | ⊕⊕⊝⊝ | Despite an absolute estimated decrease in the rate of exacerbations in the vaccinated group, the result is negligible (95% CI crosses 1.00) and not statistically significant (P = 0.16) |
| Mortality (deaths during trial period) | 23 per 1000 | 37 per 1000 | OR 1.62 (0.63 to 4.12) | 518 | ⊕⊝⊝⊝ | Despite more absolute deaths occurring in the vaccinated group, the result is negligible (95% CI crosses 1.00) and not statistically significant (P = 0.31). Deaths were not necessarily attributed to the use of the vaccine |
| Carriage of NTHi Not meta‐analysed | N/A | N/A | N/A | N/A | ⊕⊝⊝⊝ | We were unable to meta‐analyse the carriage levels of NTHi in participants as each trial reported this result using different units and tools of measurement. 4 trials showed no significant difference in carriage levels, while 2 trials showed a significant decrease in carriage levels in the vaccinated group compared with the placebo group |
| Antibiotic prescriptions (number of courses/person/year) **Corticosteroids not meta‐analysed | 5.723 | 3.162 | RR 1.81 (1.35 to 2.44) | 142 | ⊕⊕⊝⊝ | Courses of antibiotics were found to be prescribed in the placebo group at a rate approximately 80% greater than in the vaccinated group (P < 0.001) (Note that a RR > 1.0 here indicates more antibiotics being prescribed to participants in the placebo group, i.e. RR 1.81 corresponds to an approximately 80% increased rate of antibiotic prescriptions when not receiving the vaccine. The placebo group is being compared to the vaccine group in this instance to attempt to demonstrate how many more antibiotics are required in those not vaccinated) **2studies reported corticosteroid use, however due to differences in units of measurement, these results could not be meta‐analysed |
| Hospital admissions (number of participants hospitalised during trial period) | N/A | N/A | N/A | N/A | ⊕⊕⊕⊝ | Hospital admissions was not meta‐analysed due to differing units of measurement by the 2 trials that reported this finding. Notwithstanding that pooling the data for the 2 trials would have yielded high heterogeneity. Hospital admissions were not necessarily attributable to the vaccine |
| Adverse events (number of adverse events/person/year) | 0.319 | 0.456 | RR 1.43 (0.70 to 2.92) | 484 | ⊕⊕⊝⊝ | Despite an estimated absolute increased rate of adverse events in the vaccinated group, the result is negligible (95% CI crosses 1.00) and not statistically significant (P = 0.61). Adverse events were not necessarily attributable to the vaccine |
| Quality of life Not meta‐analysed | N/A | N/A | N/A | N/A | ⊕⊝⊝⊝ | Quality of life was not meta‐analysed due to differing units of measurement, but was reported in 2 trials, which showed an improvement at 6 months in the vaccine group (scoring at least 2 points better than the placebo group; significance unknown) |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in the footnotes. The corresponding risk (and its 95% confidence interval (CI)) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; N/A: not applicable; NTHi: non‐typeable Haemophilus influenzae; OR: odds ratio; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1One study had marked heterogeneity; most studies had a low number of participants; one study had significant attrition. | ||||||
Background
Description of the condition
Chronic obstructive pulmonary disease (COPD) is characterised by persistent airflow limitation that is progressive and associated with an enhanced chronic inflammatory response. The chronic airflow limitation characteristic of COPD is caused by a mixture of small airways disease (obstructive bronchiolitis) and gas‐exchange impediment through parenchymal destruction (emphysema). The changes associated with an inflammatory response include cellular infiltrate, mucus secretion, and structural remodelling, which diminish the overall ability of the airways to remain patent during expiration. This limitation in airflow, as a measurement of disease severity, is best measured and assessed by spirometry (COPD is defined as the forced expiratory volume in one second (FEV1) being lower than 80% of the predicted normal) (GOLD 2011; Otczyk 2011).
Chronic bronchitis is clinically defined by the presence of cough and sputum production for at least three months in each of two consecutive years. It is an independent disease entity that may precede or follow the development of airflow limitation and may be associated with the development or acceleration of fixed airflow limitation, or both, that is COPD. Chronic bronchitis may exist in patients with normal spirometry (GOLD 2011). While patients can remain undiagnosed and have no clinical evidence of a lung disease until they present with advanced COPD, many have a history of symptomatic disease, evidenced as chronic cough and sputum (chronic bronchitis) and/or recurrent episodes of acute wheezy bronchitis and/or late‐onset reversible airways disease (intrinsic asthma). Currently, the diagnosis of an acute exacerbation is based entirely on clinical presentation. There is no consensus regarding an objective measurement of an exacerbation (GOLD 2011). The relationship between these entities is complex and not well understood, with no obligatory linkage with COPD, but has the capacity to progress to COPD (Otczyk 2011).
An acute exacerbation is defined as an acute event characterised by worsening of the patient's respiratory symptoms beyond normal daily variations, and can lead to a change in medication (GOLD 2011). The best predictors of exacerbations are a history of previously treated exacerbations and worsening airflow limitation (GOLD 2011). Exacerbations may be triggered by bacterial or viral infection (or both simultaneously), environmental pollutants, or as yet undetermined factors. The characteristic response is increased inflammation resulting in increased purulent sputum production, hyperinflation, and gas trapping, with reduced expiratory flow, thus accounting for the dyspnoea associated with these episodes (GOLD 2011). Whilst participants with an atopic constitution (hypersensitive to allergens) may be predisposed to developing COPD, it should be recognised that bacterial colonisation of damaged airways plays an important pathogenic role. In participants with established obstructive lung disease, acute attacks of infection are a major cause of morbidity and mortality.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines estimate the prevalence of COPD to range from 7.8% to 19.7% of the population worldwide (GOLD 2011). Chronic obstructive pulmonary disease is very prominent in populations of smokers and ex‐smokers. However, estimates of prevalence in people who have never smoked range from 3% to 11% (GOLD 2011). The World Health Organization (WHO) estimates that 5% of all deaths globally can be attributed to COPD, with the disease becoming the third leading cause of death by 2030 (WHO 2013). Whilst epidemiological information regarding COPD comes from high‐income countries, 90% of COPD deaths occur in low‐ and middle‐income countries (WHO 2013).
The management of acute exacerbations focuses on treating triggers (including infections) and relieving symptoms with bronchodilators, glucocorticoids, and antibiotics. Prevention of further exacerbations focuses on vaccination of influenza and pneumococcus strains (WHO 2013). A recent Cochrane review on the use of prophylactic antibiotics for COPD exacerbations concluded that there was a reduction in the number of participants experiencing exacerbations with continuous macrolide antibiotic use. The number needed to treat to prevent one exacerbation was eight. These promising findings need to be weighed against the risks from long‐term antibiotic use, such as side effects of medications and bacterial resistance (Herath 2013).
Bacterial and viral causative agents have been identified and may coexist in a benign or pathogenic capacity; because of this, the specific microbiological aetiology of acute exacerbations in chronic bronchitis and COPD patients remains a matter of debate. The pathogens responsible for these acute exacerbations are often found in the person's upper respiratory tract, and (opportunistic) infections are caused by an upset in the balance of the host‐parasite relationship. Bacterial colonisation is most common and more severe compared to viral infections. The upper respiratory tract is commonly home to Staphylococcus epidermidis,Staphylococcus aureus,Streptococcus pneumoniae,Streptococcus pyogenes,H influenzae, andNeisseria meningitides. The lower respiratory tract is normally virtually free of micro‐organisms, due to physiological clearance mechanisms (e.g. mucociliary clearance). However, should these systems become damaged (as is the case in COPD or bronchitis patients), pathogens such as non‐typeable H influenzae (NTHi) or Pseudomonas aeruginosa are usually the ones to colonise these sites (Butt 1990). Non‐typeable H influenzae is of particular importance in this scenario because of its frequent and predominant pattern of mucosal colonisation of the respiratory tract. Higher levels of immunoglobulin E (IgE) have been detected in the serum of people with COPD, and it has been observed that NTHi triggers histamine release. This process occurs through both IgE‐ and non‐IgE‐dependent mechanisms from cells contained within the respiratory mucosal sensitised to the bacterium. These findings demonstrate that NTHi may also play a role in the development of the reversible component of airways obstruction in COPD. Immediate hypersensitivity via IgE antibacterial antibodies to colonising bacteria may contribute to bronchial disease progression and severity (Otczyk 2011). As these conditions have been associated with high numbers of NTHi, the vaccine was considered to be relevant in the prevention of exacerbation frequency and severity.
Description of the intervention
Various treatment strategies have been attempted including immuno‐stimulatory agents made from bacterial extracts, such as OM‐85 BV, and antibiotics. While OM‐85 BV appears not to affect the occurrence of acute exacerbations of bronchitis, it reduces the severity of the exacerbation (55% fewer total days of hospitalisation compared to placebo) (Collet 1997). Conventional antibiotic therapy has not been particularly helpful, possibly due to the inability to effectively clear respiratory flora such as NTHi, which leads to further growth and sepsis (Foxwell 1998a; Murphy 1992; Van Alphen 1995). Recent studies have identified a role for antibiotics in the treatment of COPD (Albert 2011; Macfarlane 2001). Although significant differences in the incidence of exacerbation were noted between groups, the long‐term effect on microbial resistance was not reported. This underscores the importance of exploring vaccination as a prophylactic treatment of COPD.
An alternative strategy is mucosal immunisation. Successful vaccines for H influenzae depend on immunity stimulation against the type‐specific polysaccharide capsule of Haemophilus influenzae B (Hib). Following the development of successful vaccines for infections caused by Hib, attention is now focused on developing a vaccine for NTHi. Accordingly, an oral, whole‐cell NTHi vaccine has been developed to prevent NTHi infections, which is the focus of this review.
Oral immunisation reduced bacterial loads in participants who were chronically colonised, and NTHi‐specific cellular responses were detected in white blood cells (lymphocytes) in the serum (Otczyk 2010). This suggests that a NTHi vaccine may be useful, as it demonstrates that mucosal immunisation can be used therapeutically to enhance or modify an immune response to improve the outcomes of an established chronic mucosal infection (Otczyk 2010).
How the intervention might work
The vaccine is believed to be most effectively absorbed through the gastrointestinal tract in order to trigger an immune response. The killed NTHi cells of the vaccine are coated with formalin to protect it from gastric degradation, thus enabling it to access the M‐cells of the gut mucosal immune system through pattern‐recognition receptors that are designed to identify pathogen‐associated molecular patterns (i.e. PRR‐PAMP interactions). Human and animal studies support the hypothesis that oral NTHi immunisation stimulates T‐cells in the Peyer's patches of the gastrointestinal tract (Foxwell 1998a). The T‐cells, upon stimulation from the vaccine, migrate to the respiratory system via afferent lymphatics and blood, where they are further stimulated by bacteria in the bronchial mucosa. Cytokines are secreted from the stimulated T‐cells to further increase immune activity. This results in increased recruitment and up‐regulation of neutrophil white blood cells into the bronchial space, which in turn assists in clearing bacteria through phagocytosis and thus reducing the bacterial load (Clancy 2011).
However, it must be noted that this form of immunisation does not trigger classical mucosal immunoglobulin A responses, but rather by the means outlined above. Nonetheless, an oral vaccine of inactivated NTHi makes use of a 'physiological protective loop' to improve airway immune function. The vaccine is consumed orally and digested within the gastrointestinal tract, which triggers an innate immune response in the respiratory tract. Through a specific activation of immune cells (in the gastrointestinal tract) this initiates non‐specific protection (in the airways). Pathways that stimulate T‐helper 17 immune cells responsible for airway protection then generate an increased white blood cell responsiveness to all pathogens in the respiratory tract (Clancy 2011).
Why it is important to do this review
Chronic obstructive pulmonary disease is a major cause of morbidity and mortality. Acute exacerbations of COPD reflect intense intrabronchial inflammation, where recurrent exacerbations are linked to worsening of airflow obstruction and health status of the individual. Acute exacerbations of COPD can be fatal. Recent studies demonstrate that oral immunotherapy with NTHi reduces the level of bacterial colonisation in the airways as well as the incidence and severity of acute exacerbations (Otczyk 2011).
As chronic antibiotic therapy is not particularly feasible, an oral, whole‐cell vaccination for NTHi has been developed to reduce morbidity and mortality in people at risk. Clinical benefit has been reflected in reduced incidence and severity of exacerbations in a number of studies. A review of trials that use oral NTHi whole‐cell vaccinations should evaluate if oral immunotherapy provides a significant therapeutic advance in limiting damage in COPD and may highlight the pathogenic role of bacterial colonisation of damaged airways.
This is an update of a Cochrane review first published in 1998 and last updated in 2006 (Foxwell 2006). The previous authors concluded that participants with recurrent bronchitis vaccinated in the autumn had a decreased incidence and severity of their exacerbations during winter.
Objectives
To assess the effectiveness of an oral, whole‐cell NTHi vaccine in protecting against recurrent episodes of acute exacerbations of chronic bronchitis and COPD in adults. To assess the effectiveness of NTHi vaccine in reducing NTHi colonising the respiratory tract during recurrent episodes of acute exacerbations of COPD.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials investigating the efficacy of an oral monobacterial NTHi vaccine in people predisposed to acute exacerbations of chronic bronchitis and COPD.
Types of participants
Adults (18 years or older) with acute exacerbations of chronic bronchitis or COPD.
Types of interventions
All trials comparing a monobacterial NTHi orally administered vaccine with a placebo. We included trials where bronchodilators, analgesics, and antibiotics were used in both active and placebo groups.
Types of outcome measures
Primary outcomes
-
Incidence of acute exacerbations of chronic bronchitis or COPD.
-
Mortality.
Secondary outcomes
-
Carriage level of NTHi in the respiratory tract (including nasopharyngeal swabs, sputum samples, nasopharyngeal aspirates).
-
Numbers of prescriptions for antibiotics and corticosteroids in the trial and follow‐up periods (including hospital admissions) as an indication of severity of acute exacerbations.
-
Any associated adverse side effects from the NTHi vaccination, measurable from symptomology and participant reports.
-
Quality of life. A validated tool measurement was required for trials to be included in this review.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) (2017, Issue 1), which includes the Cochrane Acute Respiratory Infections Group's Specialised Register, MEDLINE (1946 to January 2017), Embase (1974 to January 2017), CINAHL (Cumulative Index to Nursing and Allied Health Literature) (1981 to January 2017), LILACS (Latin American and Caribbean Health Sciences Literature) (1985 to January 2017), and Web of Science (1955 to January 2017).
We used the search strategy in Appendix 1 to search MEDLINE and CENTRAL. We combined the MEDLINE search with the Cochrane Highly Sensitive Search Strategy for identifying randomised trials in MEDLINE: sensitivity‐maximising version (2008 revision); Ovid format (Lefebvre 2011). We adapted the search strategy to search Embase (see Appendix 2), CINAHL (see Appendix 3), LILACS (see Appendix 4), and Web of Science (see Appendix 5). We used no publication or language restrictions.
Searching other resources
We searched the clinical trials registers World Health Organization International Clinical Trials Registry Platform (WHO ICTRP) (www.who.int/ictrp/en/) and ClinicalTrials.gov (clinicaltrials.gov/) for completed and ongoing trials (last searched January 2017). We also searched reference lists of included trials and review studies; books related to respiratory tract infections, mucosal immunology, or vaccines; abstracts from respiratory conferences, immunology conferences, microbiology conferences, or vaccine conferences; and sent written enquiries to the authors of major relevant studies and experts in the field. We also contacted pharmaceutical companies to obtain access to unpublished trials.
Data collection and analysis
Selection of studies
Two review authors (KL, ET) assessed titles and abstracts retrieved from the search to determine their relevance to the objectives of this review. Any disagreements were resolved through discussion or by consulting a deciding arbiter (MVD). We entered all search results into Review Manager 5 (RevMan 2014).
Data extraction and management
Two review authors (HH, SNP) designed a data extraction sheet for trial reports, which was pilot tested using sample studies and revised by the other review authors. Two review authors (HH, SNP) then independently extracted data from the reports. We extracted data from each report separately and then combined data in the event of multiple reports for the same study. Any disagreements were resolved through discussion or by consulting a deciding arbiter (MVD).
Assessment of risk of bias in included studies
Two review authors (KL, JP) independently analysed each trial using Cochrane's tool for assessing risk of bias (Higgins 2011; RevMan 2014), judging each study on the following domains: sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other potential threats to validity. We rated the risk of bias for each domain as 'high', 'low', or 'unclear' and provided the supporting information that led to that rating. Any disagreements were resolved through discussion or by consulting a deciding arbiter (MVD).
Measures of treatment effect
-
We presented dichotomous (binary) data as a measure of risk and relative risk by using an odds ratio (OR) or risk ratio (RR) with 95% confidence intervals (CIs). We calculated the absolute risk reduction (ARR) for consumer comparison against other treatments or non‐treatment.
-
We presented continuous data as mean differences (MDs) if the same scale was used or as standardised mean differences (SMDs) if different scales were used with a standard deviation (SD) of the estimate.
-
We looked for quality of life outcomes as measured in the included studies. Quality of life measurements had to be measured using a validated tool. We pooled these outcomes where possible, discussing and summarising them where this was not possible.
-
We have pooled data reported as rates by using the inverse variance method as described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Unit of analysis issues
The unit of analysis in our review was the participant.
Dealing with missing data
We contacted the trial authors of the original studies when further information was required. We performed analyses based on intention‐to‐treat (ITT), such that we assumed missing data for randomised participants to be treatment failures in this review. As this ITT analysis may underestimate the effect of the intervention, we performed both ITT and on‐treatment analyses to explore the impact of missing data on the overall outcome. We presented the findings of these analyses in the Discussion section.
Assessment of heterogeneity
We assessed included trials for heterogeneity (which is a variation in study outcomes amongst the studies as further defined in Higgins 2011) through two successive steps to determine if they should be pooled with the rest of the included trials or reported in a systematic review.
-
Two review authors (KL, JP) independently analysed trials for their 'face‐value' similarities, i.e. for clinical diversity (participants, interventions, and outcomes) and methodological diversity (study design and risk of bias).
-
We subsequently assessed trials for statistical heterogeneity using the Chi2 test with a P value of less than 0.10 being statistically significant. We calculated the I2 statistic as instructed in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011; RevMan 2014). If this was greater than 50%, we considered the pooled trials to be significantly heterogeneous.
Assessment of reporting biases
Had a sufficient number of studies had been pooled (i.e. greater than 25), we planned to use a funnel plot to visually inspect the risk of publication bias, where more pronounced asymmetry of the funnel plot may be indicative of a substantial overestimation of the intervention effect (Higgins 2011; RevMan 2014).
Data synthesis
We synthesised the data as follows.
-
We used a fixed‐effect model for binary or continuous data in the absence of statistical heterogeneity (I2 < 50%) according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011; RevMan 2014).
-
We used a random‐effects model for binary or continuous data in the presence of statistical heterogeneity (I2 > 50%) for pooling the trial data using the Mantel‐Haenszel method according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011; RevMan 2014). This model of analysis makes the assumption that the studies are not measuring for the same intervention effect, instead estimating for an overall intervention effect that is trending amongst the studies.
-
We also used the fixed‐effect model to pool study data that reported events as rates according to the Cochrane Handbook for Systematic Reviews of Interventions; only fixed‐effect meta‐analysis methods are available in Review Manager 5 for 'O – E and Variance' outcome (Higgins 2011; RevMan 2014).
GRADE and 'Summary of findings' table
We created a 'Summary of findings' table using the following outcomes: acute exacerbations, mortality, carriage levels, antibiotic prescriptions, hospital admissions, adverse events, and quality of life. We used the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness, and publication bias) to assess the quality of a body of evidence as it relates to the studies which contribute data to the meta‐analyses for the prespecified outcomes (Atkins 2004). We used methods and recommendations described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), using GRADEpro GDT software (GRADEpro GDT 2014). We justified all decisions to down‐ or upgrade the quality of studies using footnotes, and we made comments to aid the reader's understanding of the review where necessary.
Outcomes that presented data as dichotomously, had their assumed risk calculated by taking the proportion of participants in the placebo group that encountered the event, and thus, the corresponding risk calculated by applying the relative effect to the assumed risk.
Outcomes that presented data as rates, had their assumed risk calculated by taking the average rate of events in the placebo group (measured in events per person per year), and thus, the corresponding risk calculated by applying the relative effect to the assumed risk. Refer to the Additional tables for the event rates for each of the studies included in the meta‐analysis.
Subgroup analysis and investigation of heterogeneity
If sufficient data were available, we planned to explore specific subgroups for further analyses of treatment effect.
-
Comparison of continued‐smoking versus ex‐smoking populations.
-
Younger (< 65 years) versus older (65 years and older) participants.
Sensitivity analysis
If sufficient data were available, we planned to perform sensitivity analyses by:
-
examining how the addition of studies at high risk of bias to studies at low risk of bias impacted on the overall outcome to determine the effects of risk of bias; and
-
examining which studies contributed to heterogeneity and how this impacted on the overall outcome.
We used different methods of pooling, for example initially pooling all trials and then excluding one by one specific trials from the meta‐analysis and comparing the results, whilst also comparing the use of a fixed‐effect versus random‐effects model for the pooling analysis. Otherwise, we entered trials one by one into the meta‐analysis to assess the robustness of the pooled estimates.
Results
Description of studies
Results of the search
We obtained 199 records from our searches as described in Search methods for identification of studies. From the search result, we identified 10 randomised controlled trials (RCTs) that provided data pertinent to the NTHi oral vaccine in preventing acute exacerbations in chronic bronchitis and COPD (Figure 1).

Inclusion of trials flow diagram.
Included studies
We included six studies in this review (Clancy 1985; Clancy 1990; Clancy 2016; Lehmann 1991; Tandon 1991; Tandon 2010). We have summarised the main features of the included trials in the Characteristics of included studies table. We have summarised the key results of the included trials in the summary of findings Table for the main comparison. We have described the methods here in greater detail, largely using direct excerpts of the original papers, as these demonstrate the strengths and weaknesses of the trials in the words of the original authors.
Overview
All six of the included studies were clinical placebo‐controlled RCTs, five of which were double‐blinded (Clancy 1985; Clancy 2016; Lehmann 1991; Tandon 1991; Tandon 2010), and one of which was single‐blinded (Clancy 1990). They were conducted to test the efficacy of enteric‐coated, killed preparations of H influenzae in populations prone to recurrent acute exacerbations of chronic bronchitis or COPD. The vaccine preparation and immunisation regimen used in all trials consisted of at least three courses of formalin‐killed H influenzae in enteric‐coated tablets taken at intervals (e.g. on days 0, 28, and 56). Each course generally consisted of two tablets taken after breakfast over three consecutive days. In all cases, the placebo groups took enteric‐coated tablets containing glucose.
The trials varied in duration from three to 12 months. Randomisation in the trials was achieved by having a pharmacist independently prepare treatment packages that contained either active or placebo tablets (Clancy 1990; Lehmann 1991; Tandon 1991). These packages were numbered and randomised before being distributed to the clinicians involved in the trials, where the pharmacist was responsible for disclosing the randomised codes at the conclusion of the trial.
The trials varied in population groups, with most trials including chronic bronchitis or COPD patients in Australia with mean ages between 40 and 80 years (Clancy 1985; Clancy 1990; Clancy 2016; Tandon 1991; Tandon 2010). Lehmann 1991 was conducted in chronic bronchitis or COPD patients in Papua New Guinea, with a mean age of 51 years.
Bacterial load was assessed by a standardised method across the six trials. Multiple cultures were performed on each person. In normal circumstances, the first culture following vaccination was taken at three months. Cultures were taken at regular three‐monthly intervals and extra cultures taken during illness. The methods of obtaining samples and transporting material and culture methods generally followed a set protocol for adequate specimen handling and control. However, the lack of consistency and wide variety of measurement styles used amongst the studies to calculate and report carriage levels made analyses between studies difficult.
Measured outcomes in the trials varied but included bacterial load within the respiratory tract, the number and severity of acute exacerbations, and the usage of antibiotics. These outcomes were not always statistically useful.
Corticosteroids were administered at a similar rate in both active and placebo groups. Antibiotics were prescribed in both arms of the trial according to standard respiratory medicine clinical criteria at the time of the respective trials. Such criteria included increase in volume and purulence of sputum, usually with increased breathlessness and sometimes fever.
Clancy 1985 was carried out and published by Clancy in 1985 and 1987 and is the oldest trial relevant to this review. It is a double‐blind, placebo‐controlled RCT conducted in New South Wales (Australia) over a period of three months in the winter of 1983. The mean age was 65.5 years in the treatment group and 64.7 years in the placebo group. The focus of the study was the immunogenicity of the H influenzae oral vaccine and the clinical impact on people with airways damaged by COPD who suffered recurrent episodes of acute bronchitis. Fifty people with COPD (not taking corticosteroids or immunosuppressants) were recruited from the chest clinic of the Royal Newcastle Hospital and were given a three‐day course of tablets (two daily) at 0, 28, and 56 days. Both placebo and NTHi vaccine were enteric‐coated. Clancy 1985 utilised two placebo arms in their trial: the first group was given enteric‐coated glucose tablets, and the second was given sodium tauroglycocholate. We have used the results from the first placebo group as this is a standard, widely used placebo, rather than the sodium tauroglycocholate group, as this placebo may have contributed some therapeutic effect. Participants were assessed by a chest physician, with lung function (spirometry), throat cultures, and saliva samples collected at baseline, 28, 56, and 84 days. The characteristics of participants entered into the trial demonstrated a very representative population: older adults (mean age 65 years), majority male (M:F 4.5:1), majority smokers (86%). H influenzae was isolated from 69% of sputum samples collected during acute bronchitis episodes in this population. Clancy 1985 concluded that the NTHi vaccine resulted in over 90% protection against acute exacerbations compared to the placebo group. This was not the case at follow‐up a year later, at which point there was no significant reduction in incidence of H influenzae carriage, that is no clear correlation between clinical protection from acute exacerbations and either carriage of H influenzae or the level of antibody to H influenzae antigen in saliva was evident. It was also noted that the protection provided by the vaccine did not extend to the subsequent winter, which is consistent with the knowledge that mucosal immunity is less durable than systemic immunity.
Clancy 1990 was a double‐blind RCT conducted in Australia over a six‐month period. There were a total of 37 participants with each group having similar baseline characteristics. The population in this study had a mean age of 65.5 +/‐ 2.9 and was recruited from a chest clinic in Newcastle. Episodes were defined by an increase in purulence and volume of sputum with associated fever, cough, shortness of breath, and antibiotic therapy. Each participant was assessed by a chest physician, completed a respiratory questionnaire (American Thoracic Society Division of Lung Disease questionnaire (ATS‐DLD‐78)), and had sputum and mixed saliva samples taken and lung function via spirometry. Each group received three courses of oral tablets for three consecutive days at 0, 28, and 56 days. One group received the active preparation containing H influenzae vaccine, while the other group received a glucose‐containing placebo preparation. There was a significant reduction in the number of episodes of acute wheezy bronchitis in the treated group with a P value of 0.02. There was a significant reduction (41%) in the total number of acute infections in the treatment group compared to the placebo group but no significant change when acute infections were considered in an individual from either group. This study had other modes of measuring severity, such as the number of participants reporting infections and the number of infections prescribed antibiotics, and all results supported the treatment group. There was no significant difference noted in the side effect profile in either group.
Clancy 2016 was a double‐blind, placebo‐controlled, prospective study conducted for nine months over the Australian winter of 2011. The study included 320 people with moderate‐severe COPD with FEV1 less than 60%, requiring oral systemic corticosteroid therapy or admission into hospital, recruited from 21 sites across Australia; the mean age of participants was 71.2 years in the treatment arm and 67.9 years in the placebo arm. Participants in the intervention group were given two HI‐164 oral vaccine enteric‐coated tablets per day, each of which contained 45 mg of the formalin‐inactivated NTHi (HI‐164) active vaccine; participants in the placebo group received a glucose substitute. Study outcomes assessed the number of exacerbations (according to the St George's Respiratory Questionnaire for COPD), carriage levels (from cultured sputum samples), hospitalisations, and antibiotic/steroid prescriptions (based on medical records). The aim of this study was to extend the database from earlier and smaller studies showing that maximum protection occurred in those with most severe disease, with the most sensitive indicator being a reduction in exacerbations requiring corticosteroid therapy or hospital admission, or both. Clancy 2016 provides evidence that the age‐related vaccine benefits in COPD noted with parenteral vaccines also apply to oral vaccines that enhance mucosal immunity within the bronchus. The results were only minutely significant in circumstances of low exposure to NTHi and only amongst a subgroup of younger participants (aged under 65), given more responsive immune systems and less established airway disease. The results were otherwise not significant for those older than 65 years of age.
Lehmann 1991 was a prospective, double‐blind RCT, conducted through the Pneumonia Research Programme in Papua New Guinea. As a result, the demographic characteristics differed significantly to those found in high‐income communities. Potential participants were identified by nomination from town residents and villagers and were then followed up by a standard questionnaire, which identified people suffering from chronic lung disease. Participants who matched the eligibility criteria were examined with lung function tests and spirometry at time of entry into the trial. Randomisation and blinding of medication and placebo were done by the pharmacy department at the Royal Newcastle Hospital, New South Wales, Australia; the placebo and active vaccine looked identical, and the randomisation code was held by Auspharm International Ltd until the completion of the trial. Both groups were similar at baseline following allocation. Doctors and nurses oversaw the administration of medication to maintain compliance during the 12‐month follow‐up period. Eight participants in the vaccine group and three in the placebo group were lost to follow‐up, with three deaths in the vaccine group and one death in the placebo group. The trial does not mention any ITT analysis for these participants, rather stating "permanent exit from the study were excluded from the calculation", potentially creating attrition bias. The trial concludes that for the population of the highlands of Papua New Guinea, the vaccine protected against episodes of acute bronchitis, but not against more severe forms of acute lower respiratory tract infection. A limitation of the study was the need for a larger population group to ensure greater statistical power to help determine the extent of protection oral H influenzae vaccine could provide.
Tandon 1991 was a double‐blind RCT, conducted in 1988 at the repatriation hospital in Western Australia. This study recruited 64 participants with chronic bronchitis and a history of recurrent respiratory tract infections to learn whether oral NTHi immunisation is effective in this patient population. Participants were divided randomly into placebo (mean age 71.1 years) and vaccine (mean age 73.1 years) groups. All participants followed the same treatment regimen consisting of three courses of the tablets on days 0, 28, and 56. Study outcomes were acute infective episodes, number of antibiotic prescriptions, and colonisation with H influenzae, monitored through the following strategies: primary care physician for diagnosing acute infective episodes, sputum sample, and visual analogue scale. For all of these variables, better outcomes were demonstrated in the vaccine group. Previous studies have demonstrated that H influenzae is the main constituent in bacterial colonisation of the bronchus, and therefore vaccinating against it would reduce the incidence of acute exacerbations, which is consistent with the results of this study.
Tandon 2010 was a multicentre, double‐blind, placebo‐controlled trial conducted at four sites around Australia. The study tested the efficacy of HI‐164OV in reducing the number and severity of acute exacerbations in people with severe COPD. Acute exacerbations were defined by an increase in volume and purulence of sputum. Each participant was administered the same regimen (two tablets daily for three consecutive days) with courses repeated at day 28 and 56. All tablets were identical‐looking, enteric‐coated capsules that contained either vaccine (N = 18) or placebo (N = 20). Participants were followed up every four weeks via a respiratory questionnaire, sputum and nasopharyngeal swabs were collected to monitor bacterial colonisation, and blood samples were collected to monitor antibodies. The primary variables were the number and duration of exacerbations and the number of antibiotic courses prescribed. Baseline demographic characteristics, such as mean age (vaccine 69.5, placebo 67.5) were very similar, demonstrating effective randomisation. However, the exact method of randomisation was not disclosed. Four of the six authors of this study disclosed that they had received funding from Hunter Immunology Ltd. The authors concluded that the vaccine was safe and had a significant efficacy in participants with severe COPD. Benefits were noted with respect to a reduction in the severity of episodes (duration of episodes; 14.3 vaccine group and 22.7 placebo, P < 0.01), which required less antibiotic therapy (event rate; 0.83 vaccine and 1.15 placebo, P < 0.05) and fewer admissions to hospital (three in the vaccine group compared to 12 in the placebo group, P < 0.05). However, a reduction in the incidence of episodes did not reach significance, possibly because the study was significantly underpowered.
Excluded studies
We excluded one study because it did not meet our inclusion criteria (Clancy 2010). As noted in Characteristics of excluded studies, the participant population included smokers who did not have formally diagnosed COPD or chronic bronchitis, and outcome measures were limited to physiological markers that did not include the clinical outcomes defined in this review's protocol.
Two studies are cited only in trial registries and are pending formal publication of the raw trial data by the investigators (ACTRN12606000074594; ACTRN12606000076572). The main features of these unpublished trials can be found in Characteristics of studies awaiting classification. These trials will potentially be incorporated into future updates of this review.
Risk of bias in included studies
A summary of the 'Risk of bias' assessment is detailed in the Characteristics of included studies table.
Allocation
The random sequence generation in the studies was generally determined to be poor, with 50% of the studies graded as either at high or unclear risk of bias because they did not provide any information regarding the random sequence generation and subsequent allocation process (Clancy 1985; Clancy 2016; Tandon 2010). We considered the remaining studies to have a low risk of bias given that it was reported that a third party conducted randomisation and that the allocation codes were kept confidential until the end of the trial (Clancy 1990; Lehmann 1991; Tandon 1991).
The allocation concealment in the selected studies was generally poor, with 67% of the studies categorised as either at unclear or high risk of bias (Clancy 1985; Clancy 1990; Clancy 2016; Tandon 2010). Only two studies demonstrated a low risk of bias, where the handling and distribution of the treatment packages were carried out independently by the pharmacist, who employed an appropriate randomisation chart and safely kept the package trial code associated with the participants (Lehmann 1991; Tandon 1991).
Blinding
All studies performed suitable blinding except for one, which we deemed to be at high risk of bias because it did not blind the commercially available polybacterial tablets (Clancy 1990); for this reason, the study was subsequently conducted as a single‐blind trial (participants blinded). All of the remaining studies reported using double‐blinded identical enteric‐coated tablets for both intervention and placebo arms of the trial.
Incomplete outcome data
Five of the six included studies accounted for and provided sufficient information regarding the follow‐up of participants who had dropped out of the trials (Clancy 1985; Clancy 1990; Clancy 2016; Tandon 1991; Tandon 2010). Lehmann 1991 made no mention of ITT analysis and reported a substantial loss to follow‐up (eight participants from the vaccine group and three from the placebo group), especially considering the small group size.
Selective reporting
We found no selective reporting in any of the studies.
Other potential sources of bias
We identified no other potential sources of bias in any of the studies.
Effects of interventions
Primary outcomes
1. Incidence of acute exacerbations of chronic bronchitis or chronic obstructive pulmonary disease (COPD)
Six trials evaluating 557 participants assessed the effectiveness of non‐typeable Haemophilus influenzae (NTHi) oral vaccination on the frequency of acute exacerbations in people with advanced lung disease (Figure 2; Table 1). The meta‐analysis concluded that there was a small, non‐significant 2.048% decrease in exacerbations in the vaccinated group when compared to the placebo group (RR 0.79, 95% CI 0.57 to 1.10; P = 0.16) (Analysis 1.1).
Forest plot of comparison: 1 Primary outcomes, outcome: 1.1 Exacerbations (number of exacerbations/person/year).
Refer to Table 1 for Overall rate estimates of acute exacerbations across included studies.
| Study | Vaccinated | Placebo | *Absolute rate difference |
| Clancy 1985 | 0.256 | 0.272 | 0.016 (‐) |
| Clancy 1990 | 1.000 | 1.700 | 0.700 (‐) |
| Clancy 2016 | 0.717 | 0.767 | 0.050 (‐) |
| Lehmann 1991 | 0.800 | 1.210 | 0.410 (‐) |
| Tandon 1991 | 3.355 | 4.364 | 1.009 (‐) |
| Tandon 2010 | 3.667 | 4.350 | 0.683 (‐) |
| Overall mean | 1.633 | 2.111 | 0.478 (‐) |
*Estimated rate of exacerbation calculated as number of exacerbations per person per year.
Refer to Analysis 1.1: Forest plot comparison and rate ratios for exacerbations.
Despite all trials having almost identical primary objectives, there were considerable discrepancies in the manner in which the primary outcomes were reported. For example, Clancy 1985 reported overall number of infections, whereas Tandon 2010 reported the number of infections per participant. In order to allow meaningful comparisons between studies, we converted all data into a rate of exacerbations (number of exacerbations per participant per year).
Of the six studies incorporated into the review, only one demonstrated an effect that favoured the vaccination group (Clancy 1985). Clancy 1985 was a small trial that enrolled 33 participants. The data showed a very significant positive effect in favour of the vaccine group, recording only one event compared to 13 in the placebo group, which was statistically significant (RR 0.07, 95% CI 0.01 to 0.55), despite the very large CI. However, subgroup analysis demonstrated that removing this study from the pool had no bearing on the overall meta‐analysis outcome, as its small population meant this study's weighting was very small.
Five studies, with a total of 504 participants, did not show a significant increase in the number of exacerbations (Clancy 1990; Clancy 2016; Lehmann 1991; Tandon 1991; Tandon 2010). As a result, their combined contribution to this meta‐analysis weighting was 99.5%.
Clancy 2016 was the largest trial, comprising 320 participants and receiving over 70% of the meta‐analysis weighting. It showed a non‐significant 8% increase in the number of exacerbations in the placebo group (RR 1.08, 95% CI 0.91 to 1.29). Clancy 2016 reported 249 events in the vaccine group compared with 270 in the placebo group.
There was a moderate degree of heterogeneity in this meta‐analysis (I2 = 57%, P = 0.04), hence a random‐effects model of analysis was used. The study contributing most to this effect was Clancy 1985. Removal of Clancy 1985 dramatically reduces the heterogeneity (I2 = 24%, P = 0.26), but did not change the overall result.
2. Mortality
None of the trials formally assessed mortality as an outcome. However, five trials reported death of trial participants (Figure 3) (Clancy 1985; Clancy 2016; Lehmann 1991; Tandon 1991;Tandon 2010). Of these deaths, none were attributed to the vaccine and most were considered the natural endpoint of the participants' respiratory disease or other unrelated chronic disease. There was a greater incidence of mortality in the placebo group. However, this result was not statistically significant (OR 1.62, 95% CI 0.63 to 4.12; P = 0.31), with a low amount of heterogeneity between results (I2 = 9%, P = 0.36) (Analysis 1.2).

Forest plot of comparison: 1 Primary outcomes, outcome: 1.2 Mortality (deaths during trial period).
Secondary outcomes
1. Carriage level of NTHi in the respiratory tract
All six RCTs attempted analysis of carriage levels of H influenzae in participants. We could not perform a meta‐analysis as a myriad of different techniques were used to measure carriage levels objectively (throat swabs, sputum samples and culture), and carriage rates were measured at different intervals. Three trials failed to find a significant difference between carriage levels (Clancy 1985; Clancy 1990; Tandon 1991). Two studies showed a significant decrease in carriage rates in the vaccine group (Lehmann 1991; Tandon 2010). In one study, carriage levels were measured, but sputum samples could only be obtained at 36% of planned visits, of which 11% grew a respiratory pathogen; these numbers were too small to determine any significant effect following vaccination (Clancy 2016).
Lehmann 1991 showed the mean concentrations of H influenzae carriage levels during acute exacerbations to be higher in the vaccine group (8.91 x 106 colony‐forming units (cfu)) when compared against the placebo (1.55 x 106 cfu). However, this only equated to a 5% difference between the vaccinated and placebo arms when counting individual specimens, whereby 91% of the vaccinated and 86% of the placebo collected specimens successfully grew H influenzae colonisations during the trial period.
Tandon 2010 demonstrated that there was a significant (P < 0.05) two‐fold difference between the placebo and active arms in overall positive cultures (65 positive cultures in the placebo group compared to 33 in the vaccine group). However, the percentage of validated sputum samples was 50% and 48% for placebo and active groups, respectively. H influenzae accounted for only 51% and 33% of positive cultures in the placebo and vaccinated groups, respectively.
There was a trend for studies to report a transient decline in H influenzae carriage levels. However, this had always returned to baseline by the end of the study time frame. Tandon 1991 noted a transient drop in carriage levels to 12% at 14 weeks in the active group, which then reverted back to 25% at 24 weeks. This is a 4% drop over 24 weeks. The placebo group noted a small 2% drop over the 24‐week study period. Furthermore, in Clancy 1985H influenzae was isolated from throat swabs from 70% of the placebo group compared with 53% of the vaccination group at the end of a four‐week period. Carriage rates at 12 weeks declined to 50% in the placebo group and 23% in the vaccine group.
2. Numbers of prescriptions for antibiotics and corticosteroids in the trial and follow‐up periods (including hospital admissions) as an indication of severity of acute exacerbations
Four studies, evaluating 462 participants, assessed the effect of NTHi oral vaccination on the number of antibiotic prescriptions in people with chronic bronchitis (Clancy 1990; Clancy 2016; Tandon 1991; Tandon 2010) (Figure 4; Table 2).

Forest plot of comparison: 2 Secondary outcomes, outcome: 2.1 Prescriptions (number of courses/person/year).
Refer to Table 2 for Overall rate estimates of antibiotic prescriptions across included studies.
| Study | Vaccinated | Placebo | *Absolute rate difference |
| Clancy 1990 | 0.500 | 1.200 | 0.700 (‐) |
| Tandon 1991 | 5.806 | 10.194 | 4.388 (‐) |
| Tandon 2010 | 3.180 | 7.200 | 4.020 (‐) |
| Overall mean | 3.162 | 6.198 | 3.036 (‐) |
*Estimated rate of antibiotic prescriptions calculated as number of antibiotic courses per person per year.
Refer to Analysis 2.1: Forest plot comparison and rate ratios for antibiotic prescriptions.
There were considerable discrepancies amongst studies in the way antibiotic prescriptions were objectively measured. We attempted to convert the reported data into a rate (number of courses/person/year) in order to achieve an objective comparison. However, this was not possible with data from the Clancy 2016 trial, which unlike the other studies only reported mean antibiotic use in days. As a result, we could pool only three studies in meta‐analysis. Two studies did not report any information on antibiotic usage in this population (Clancy 1985; Lehmann 1991).
The three studies in the meta‐analysis included 143 participants (Clancy 1990; Tandon 1991; Tandon 2010). Two of these studies produced data that favoured the vaccination group (Tandon 1991; Tandon 2010), whereas the Clancy 1990 data did not reach significance. The overall effect was a statistically non‐significant 81% increase in use of antibiotic courses per person in the placebo group when compared against the vaccinated group (RR 1.81, 95% CI 1.35 to 2.44; P < 0.001; with a RR > 1.0 indicating greater antibiotic usage in the placebo group) (Analysis 2.1). The majority of the weighting could be attributed to Tandon 1991 and Tandon 2010: 64.9% and 31.1%, respectively, and both favoured the vaccination group.
Tandon 1991 showed a significant decrease in antibiotic prescriptions (45 in the active group and 79 in the placebo group). Tandon 2010 showed a significant 56% reduction in the number of prescribed antibiotics following active treatment (P < 0.05). Clancy 1990 reported a reduction in the number of antibiotics in the active group compared to the placebo group, but this failed to reach statistical significance.
The Clancy 2016 trial is by far the largest study in this review (three times the combined size of the other three trials included in this outcome), contributing 320 of the 462 participants. Clancy reported that there was no significant difference between the two groups in terms of antibiotic usage (active group 13.5 days per episode with a range of 0 to 289; placebo group 14 days per episode with a range of 1 to 122). Given the wide and varied protocols for antibiotic administration, it was impossible to translate this into course/person/year as with the other trials.
Corticosteroid prescriptions were not strictly studied as an outcome in the studies, and thus we did not meta‐analyse these; nonetheless, usage was noted in participants in at least two studies (Clancy 2016; Tandon 2010), and we have considered their indications and study findings for their use in the Summary of main results.
Hospitalisation data amongst the studies were limited, with only two studies reporting hospitalisations of their participants (Clancy 2016; Tandon 2010). The two studies presented data different units of measurement therefore not allowing the 2 studies to be meta‐analysed together; Clancy 2016 presented their data has a rate ratio, whereas Tandon 2010 presented data dichotomously. We have considered their indications and study findings for their use in the Summary of main results.
3. Any associated adverse side effects from the NTHi vaccination, measurable from symptomology and participant reports
All studies except Clancy 1985 reported adverse events, although none of the trials studied this as an outcome. In total, 142 adverse events were reported; of these, 72 occurred in the active group and 68 occurred in the placebo group (Analysis 2.2; Figure 5; Table 3). Reported adverse effects were largely gastrointestinal in nature, although increased dyspnoea or general malaise were also commonly reported; none of these were found to be directly attributable to the oral vaccine.

Forest plot of comparison: 2 Secondary outcomes, outcome: 2.3 Adverse events (number of adverse events/person/year).
Refer to Table 3 for Overall rate estimates of adverse events across included studies.
| Study | Vaccinated | Placebo | *Absolute rate difference |
| Clancy 2016 | 0.008 | 0.025 | 0.017 (‐) |
| Lehmann 1991 | 0.067 | 0.031 | 0.036 (+) |
| Tandon 1991 | 1.032 | 1.212 | 0.180 (‐) |
| Tandon 2010 | 0.167 | 0.450 | 0.283 (‐) |
| Overall mean | 0.319 | 0.430 | 0.111 (‐) |
*Estimated rate of adverse events calculated as number of adverse events per person per year.
Refer to Analysis 2.2: Forest plot comparison and rate ratios for adverse events.
Clancy 2016 reported that adverse event rates were similar in both groups (33.5% in the placebo group compared with 38.5% in the vaccinated group), although the actual number of events was not provided in the original publication. Further data provided by the study authors showed that one participant in the active group had an adverse event compared with three participants in the placebo group.
4. Quality of life
Two studies reported quality of life measurements, however as they used different assessment scales they were not comparable and we therefore did not meta‐analyse them (Clancy 2016; Tandon 1991). Tandon 1991 reported a global assessment for general well‐being using a visual analogue scale, which showed at 24 weeks a median score of 5.0 in the vaccine group compared to 2.5 in the placebo group (P = 0.09). Clancy 2016 measured quality of life using the St George's Respiratory Questionnaire for COPD for those under 65 years old, reporting a significant difference in symptom scores in favour of the vaccine group at three months (P = 0.02) and six months (P = 0.01). Data were not provided for older age groups.
Discussion
Summary of main results
Incidence of acute exacerbations of chronic bronchitis or COPD
In this review we evaluated the effectiveness of a NTHi oral vaccination in reducing acute exacerbations in people with chronic bronchitis/COPD. The results indicated that the vaccination has no significant impact in reducing the number of exacerbations. Only one study was able to demonstrate a statistically significant effect, which favoured vaccination (Clancy 1985). This was the smallest study and contributed significant heterogeneity to the meta‐analysis. When we removed Clancy 1985 from the meta‐analysis, we found no significant difference for the primary outcome. All other studies showed no significant treatment effect.
Among the studies included in the review, there were considerable differences in the methodology and intervals at which measurements were recorded. The main outcome (acute exacerbations) was measured differently across the six studies, providing a challenge for comparison. For example, Clancy 1985 records results as a proportion, whereas Lehmann 1991 utilises rates. There were also notable discrepancies in the study time periods, with Clancy 1985 reporting data at three months and Clancy 1990 providing data up to six months. Data recorded at nine to 12 months could only be elicited from two trials. As a result, we converted all data into rates so that studies could be objectively compared, irrespective of their varying follow‐up protocols.
Other differences amongst the trials included variation in population (Lehmann 1991 was conducted in Papua New Guinea), the use of subjective measurements such as respiratory questionnaires to measure exacerbations, and seasonal variations. These may have contributed to the marked heterogeneity (I2 = 57%, P = 0.04) identified in the meta‐analysis.
Only one study was large enough to be able to conduct subgroup analysis stratified by age (Clancy 2016). A subgroup analysis excluding all participants older than 65 years concluded that the mean number of exacerbations was significantly higher in the placebo group (56) when compared to the vaccinated group (34) (P < 0.001). There was also a statistically significant difference in the days to first exacerbation (87 days in the placebo group compared to 111 days in the vaccine group). Although the data at this stage were limited, these results suggest the use of the NTHi vaccination in a younger population, especially considering that there was no difference in mortality or adverse events in the two groups. The apparently greater efficacy of the vaccine seen in those less than 65 years old may be a reflection of a less severe burden of disease; younger patients generally have a shorter smoking history, fewer exacerbations, and fewer comorbidities. Further studies need to be conducted in younger patients and considering the varying severity of COPD to identify whether there is a significant treatment effect in this population.
Mortality
We found mortality rates overall to be higher in the placebo group. However, these results were not statistically significant and are unconvincing. There was no apparent association with treatment effect, and it is unclear whether the administration of the NTHi vaccine contributed to mortality.
Other patient factors were suggested to contribute to mortality in some trials, such as long‐standing cirrhosis or a ruptured aneurysm reported in Tandon 1991 and Lehmann 1991. These comorbidities would have a significant effect on the mortality outcome given the small participant numbers.
Two trials reported the primary cause of death as a terminal respiratory infection (Lehmann 1991; Tandon 1991), with other studies reporting cause of death to be non‐respiratory. Whilst it is understood that the most common cause of death in COPD patients is respiratory failure, it was not clearly demonstrated in this meta‐analysis, which was likely due to inconsistent and insufficient reporting in the studies.
Carriage level of NTHi in the respiratory tract
All six trials measured sputum carriage levels of H influenzae; these were obtained routinely and during acute exacerbations, although the methods of reporting and intervals at which routine samples were taken varied. This limited the extent to which these results could be compared.
A significant difference in the carriage rates was not consistently found between the placebo and vaccine groups in every trial. No significant difference over time in routine carriage rates was found between the groups in Clancy 1985, Lehmann 1991, and Tandon 1991. The largest of the studies obtained samples at only 36% of visits, and of these, a respiratory pathogen was isolated in only 11% (Clancy 2016). The sputum carriage levels were too small to determine any significant effect following vaccination.
In the majority of trials, H influenzae was noted to play a prominent role during infective exacerbations. In Clancy 1985, H influenzae was isolated from 69% of sputum samples collected during acute exacerbations, and from 33% and 44% in the placebo and vaccine groups, respectively in Clancy 1990 (this difference was not significant). Lehmann 1991 and Tandon 2010 did not discuss the bacterial carriage specifically during acute exacerbations. It is notable that Tandon 1991 found that the numbers of acute infective exacerbations were higher (P = 0.011) in participants in the vaccine group from whose sputum H influenzae was isolated either before or during an acute episode.
Clancy 2016 noted that of the sputum samples that grew a respiratory pathogen, H influenzae played a role, but not a prominent one, accounting for only 6%; 6.2% grew S pneumoniae, 7.5% Moraxella catarrhalis, and 6.0% P aeruginosa. Clancy 1990 noted that during the six‐month trial, the proportion of H parainfluenzae infections was between 57% and 89% greater than the proportion of H influenzae infections during the same time period across both groups. This poses the question of the clinical impact of treating H influenzae as prophylaxis, as the background carriage rates may reflect the rates in acute exacerbation. The remaining four studies of this meta‐analysis did not report whether other pathogens were cultured alongside H influenzae; it is worthwhile to consider that acute (infective) exacerbations of COPD may be in part due to a host of multiple organisms rather than a single isolate.
The population studied in the Papua New Guinea study raises concerns about the potential applicability of the results to the COPD patient in high‐income countries (Lehmann 1991). Asymptomatic background carriage rates were high: 57% of routine sputum samples isolated H influenzae (37% isolated S pneumoniae and 11% demonstrated H parainfluenzae). There were also some significant methodological problems in this study, with 53 out of 362 samples needing to be excluded due to betel nut consumption or epithelial contamination.
Numbers of prescriptions for antibiotics and corticosteroids in the trial
Antibiotics were prescribed in four out of the six clinical trials (Clancy 1990; Clancy 2016; Tandon 1991; Tandon 2010), but this was not necessarily an effective outcome measure that correlated with disease progression or severity. Given the high variability and lack of consistency concerning antibiotic course administration and measurements, we could not perform a truly uniform assessment and comparison amongst the trials. Whilst the three studies pooled for quantitative analysis appeared to indicate slightly more prescriptions having been issued to participants in the placebo group (RR 1.81; 95% CI 1.35 to 2.44; P < 0.001) (Clancy 1990; Tandon 1991; Tandon 2010), this conclusion remains unconvincing. There was also no reported follow‐up regarding what effect antibiotics had on participants (e.g. if there was resolution of symptoms or reduction in carriage levels).
The application of current therapeutic guidelines in the trials was similarly questionable, with the intentions and protocols for prescribing antibiotics largely unclear and not reported in their methods. It is understood that at least half of patients with chronic bronchitis and COPD are persistently colonised with H influenzae, S pneumonia, or M catarrhalis (Lehmann 1991), hence a positive sputum culture that is not necessarily indicative of an acute infection and subsequent antibiotic prescription (in Tandon 2010, 48% in the vaccinated group and 50% in the placebo group had a validated positive sputum culture). Normally in exacerbations of COPD, sputum cultures would only be done if there was a failure of response to treatment or if the patient had repeated bacterial exacerbations within several months. Nonetheless, these organisms may be responsible for more severe exacerbations, for which antibiotics have been shown to be of benefit. The aim of treatment with antibiotics in acute exacerbations should be to alleviate symptoms and reduce the volume of sputum rather than total elimination of colonising organisms.
None of the trials specified the class of antibiotic therapy used or explore sensitivities. This is important given that currently only amoxicillin and doxycycline regimens have been shown to be superior over other antibiotic classes such as macrolides, which fail to suppress H influenzae (Longo 2011).
Two trials measured the addition of corticosteroid use as an outcome (Clancy 2016; Tandon 2010). Clancy 2016 reported a median duration of five treatment days (minimum 0, maximum 313) in the vaccine group and 10 days (minimum 0, maximum 306) in the placebo group. Tandon 2010 reported a total 56% reduction in the proportion with acute exacerbations with corticosteroid treatment across both vaccine and placebo arms of their trial; further analysis by the authors to see if it reduced subsequent recurrent exacerbations showed that there was a 33% reduction in the vaccine group compared to a 55% reduction in the placebo group, with an average of about 40% reduction for recurrent exacerbations.
Even though two studies reported the use of corticosteroids for the treatment of acute exacerbations, this does not preclude participants from receiving corticosteroids prior to and during the studies. Many of the participants were admitted to hospital during the study period and were likely to have received a short course of systemic corticosteroids (in Clancy 2016 and Tandon 2010, a total of 83 participants in the vaccinated groups and 56 in the placebo groups). Short (not extended) courses of oral prednis(ol)one or intravenous hydrocortisone have been shown to shorten the duration of hospital admission and hasten return to previous lung function and stable symptom control and are routinely used for severe exacerbations of COPD (Longo 2011).
Hospitalisations
Two studies reported hospitalisations (Clancy 2016; Tandon 2010). Information in the studies regarding participant hospitalisations was limited and in different units of measurement therefore not allowing the 2 studies to be meta‐analysed together; Clancy 2016 presented their data has a rate ratio, whereas Tandon 2010 presented data dichotomously. Further consistent data parameters, such as length of hospital stay and intensive care versus general ward admission, would have been necessary for a more complete analysis.
In the Tandon 2010 study, admissions to hospital were high in the placebo group, with 11 admissions compared to one admission in the vaccination group. This demonstrates that the chance of hospital admission for those receiving the NTHi vaccine was reduced by 90% (P = 0.05). Clancy 2016 noted a similar outcome, showing a 50% acute exacerbation event reduction in hospital admissions following an acute exacerbation in the vaccine group (P = 0.047).
Any associated adverse side effects from the NTHi vaccination, measurable from symptomology and participant reports
There was no clear definition of what constituted an adverse effect and therefore no consistency between the studies' reporting of adverse events. For example, Tandon 1991 included increase of dyspnoea and cough as an adverse event, while Clancy 2016 reported mortality as a severe adverse event. None of the trials reported methods used for monitoring adverse events. There is thus potentially an under‐reporting of less severe side effects. We could reach no clear comparisons or conclusions regarding any association between adverse effects and therapeutic effect. The adverse effects presented in the trials may well have been attributable to the significant comorbidity of the participant rather than to the vaccine. To discern whether these symptoms or adverse effects were true side effects of the vaccine or whether they were sequelae of the participant's disease process was not possible in this review due to the lack of primary study data.
Quality of life
Only two studies reported quality of life (QoL) measures (Clancy 2016; Tandon 1991), and these trials used different measurement tools, limiting the comparisons that could be made between the results. It is also notable that, by nature, the measurement of quality of life is subjective and difficult to quantify; neither study provided further data and information regarding which aspect of QoL was most improved. Nonetheless, both trials reported at least a two‐point improvement in participant QoL in the vaccinated group versus the placebo group. Improvement in QoL was based on overall clinical condition assessed at the start of the trial and at set points during the trial. These intervals differed slightly between the two trials, with Tandon 1991 measuring at six months and Clancy 2016 measuring at three and six months. Clancy 2016 did not provide data on QoL for participants over 65 years of age.
Overall completeness and applicability of evidence
Although the numbers and sizes of the studies were low, all of the trials included participants with established COPD or chronic bronchitis. Clancy 2016 was the only study with sufficient sample size to conduct subgroup analyses assessing the effects of the vaccine in people less than 65 years of age. The majority of studies (with the exception of Lehmann 1991, which was conducted in Papua New Guinea) were conducted in an Australian population. However, trial length and follow‐up periods varied from three to 12 months among the trials. The majority of the studies administered the HI‐164 oral vaccine enteric‐coated tablets (two per day), each of which contained 45 mg active substance of formalin‐inactivated NTHi, which was compared with enteric‐coated placebo tablets (with the exception of Clancy 1985, which used a sodium tauroglycocholate substitute for the placebo). All studies had comparable objectives assessing the effect of the vaccine on acute COPD exacerbations.
We consider the results of this review to be applicable to people with established COPD.
Quality of the evidence
Overall, the methodological quality of the trials was acceptable, with most trials reporting methods of random sequence generation and allocation concealment sufficiently to assess them as adequate. The greatest limitation of the included studies was that of the six trials, one was by far the largest in terms of included population. The smaller studies were underpowered, and even when pooling the five smaller studies, their weighting was inferior to that of the one larger trial (Clancy 2016).
The assessment of primary outcomes of acute exacerbations was carried out through respiratory questionnaires, which are subjective, instead of using objective measures such as spirometry. Secondary outcomes such as H influenzae colonisation and antibiotic use are more objective but may be difficult to measure. Studies had low rates of loss to follow‐up, and attrition rates were low and equal in both arms of the trials.
We found a moderate degree of heterogeneity in this meta‐analysis, specifically in the outcome measuring the number of acute exacerbations of COPD (I2 = 57%, P = 0.04). Clancy 1985 appears to contribute most to the heterogeneity; its exclusion from the analysis dramatically reduces heterogeneity (I2 = 24%, P = 0.26) and can likely be attributed to the study's reported result of only one exacerbation in the vaccinated group. Nonetheless, the exclusion of Clancy 1985 from the meta‐analysis did not appear to have a significant impact on the overall result, given the small study size of approximately 30 participants and the robustness of the data sourced from the remaining studies.
Potential biases in the review process
Two review authors independently conducted all data selection and extraction, with a third review author acting as an arbiter, in order to minimise the risk of error and bias. One of the review authors (AC) was involved as an investigator in four of the six included trials (Clancy 1985; Clancy 1990; Clancy 2016; Lehmann 1991), but not involved in the data extraction and analysis in the review in order to reduce interpretation bias.
It is possible that despite extensive searching we may have missed a trial. However, this is very unlikely as one of the review authors is a world‐renowned expert in the field and has consulted his extensive network to search for additional unpublished data. We are therefore confident that we have captured all available evidence in this review.
Agreements and disagreements with other studies or reviews
This is an update of a previously withdrawn Cochrane review of the same title (Foxwell 2006). The authors of the previous review concluded that the vaccine was efficacious in reducing 20% to 30% of acute exacerbations in COPD patients and supported its use clinically. They also concluded that there was a need for larger clinical trials to assess longer‐term prognosis. Since publication of the previous review a new trial with a substantially larger population has been published (Clancy 2016), and we have been able to include this in our updated meta‐analysis. As a result of the inclusion of this large trial, the validity of the review has increased and the conclusions have changed substantially.
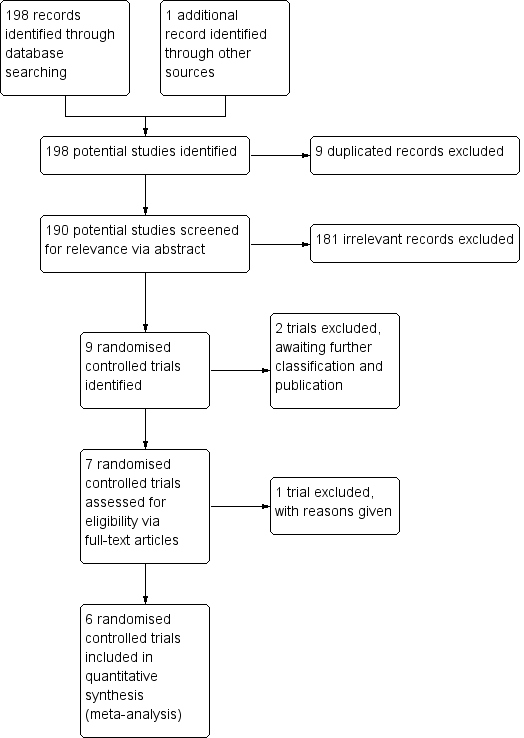
Inclusion of trials flow diagram.

Forest plot of comparison: 1 Primary outcomes, outcome: 1.1 Exacerbations (number of exacerbations/person/year).
Refer to Table 1 for Overall rate estimates of acute exacerbations across included studies.

Forest plot of comparison: 1 Primary outcomes, outcome: 1.2 Mortality (deaths during trial period).

Forest plot of comparison: 2 Secondary outcomes, outcome: 2.1 Prescriptions (number of courses/person/year).
Refer to Table 2 for Overall rate estimates of antibiotic prescriptions across included studies.

Forest plot of comparison: 2 Secondary outcomes, outcome: 2.3 Adverse events (number of adverse events/person/year).
Refer to Table 3 for Overall rate estimates of adverse events across included studies.
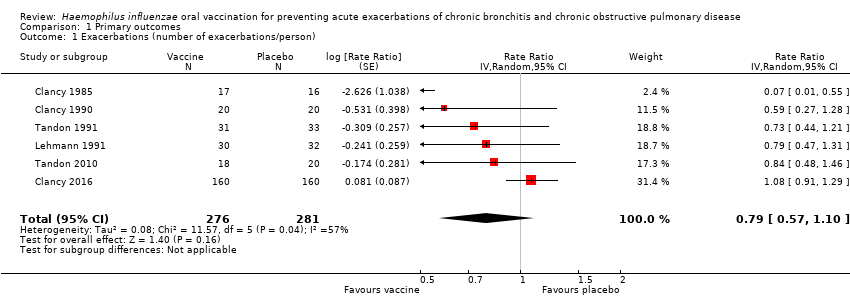
Comparison 1 Primary outcomes, Outcome 1 Exacerbations (number of exacerbations/person).
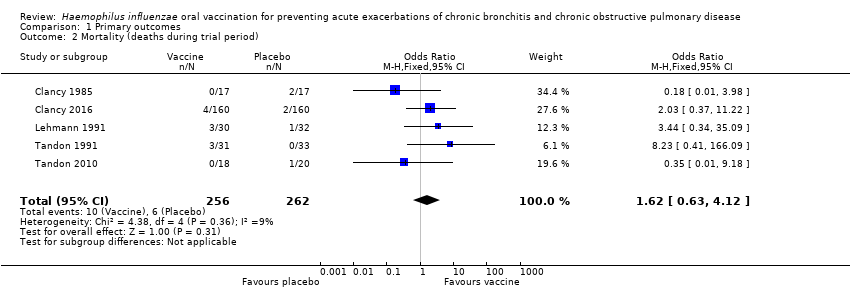
Comparison 1 Primary outcomes, Outcome 2 Mortality (deaths during trial period).

Comparison 2 Secondary outcomes, Outcome 1 Prescriptions (number of courses/person/year).

Comparison 2 Secondary outcomes, Outcome 2 Adverse events (number of adverse events/person).
| Haemophilus influenzae oral vaccination for prevention of acute exacerbations of chronic bronchitis and COPD | ||||||
| Patient or population: adults (> 18 years of age) with either COPD or recurrent acute exacerbations of chronic bronchitis Settings: community and outpatients Intervention: oral monobacterial vaccination with killed NTHi Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No. of participants | Quality of the evidence | Comments | |
| Assumed risk Not vaccinated | Corresponding risk NTHi oral vaccinated | |||||
| Acute exacerbations (number of exacerbations/person/year) | 2.111 exacerbations per person/year | 1.668 exacerbations | RR 0.79 (0.57 to 1.10) | 557 | ⊕⊕⊝⊝ | Despite an absolute estimated decrease in the rate of exacerbations in the vaccinated group, the result is negligible (95% CI crosses 1.00) and not statistically significant (P = 0.16) |
| Mortality (deaths during trial period) | 23 per 1000 | 37 per 1000 | OR 1.62 (0.63 to 4.12) | 518 | ⊕⊝⊝⊝ | Despite more absolute deaths occurring in the vaccinated group, the result is negligible (95% CI crosses 1.00) and not statistically significant (P = 0.31). Deaths were not necessarily attributed to the use of the vaccine |
| Carriage of NTHi Not meta‐analysed | N/A | N/A | N/A | N/A | ⊕⊝⊝⊝ | We were unable to meta‐analyse the carriage levels of NTHi in participants as each trial reported this result using different units and tools of measurement. 4 trials showed no significant difference in carriage levels, while 2 trials showed a significant decrease in carriage levels in the vaccinated group compared with the placebo group |
| Antibiotic prescriptions (number of courses/person/year) **Corticosteroids not meta‐analysed | 5.723 | 3.162 | RR 1.81 (1.35 to 2.44) | 142 | ⊕⊕⊝⊝ | Courses of antibiotics were found to be prescribed in the placebo group at a rate approximately 80% greater than in the vaccinated group (P < 0.001) (Note that a RR > 1.0 here indicates more antibiotics being prescribed to participants in the placebo group, i.e. RR 1.81 corresponds to an approximately 80% increased rate of antibiotic prescriptions when not receiving the vaccine. The placebo group is being compared to the vaccine group in this instance to attempt to demonstrate how many more antibiotics are required in those not vaccinated) **2studies reported corticosteroid use, however due to differences in units of measurement, these results could not be meta‐analysed |
| Hospital admissions (number of participants hospitalised during trial period) | N/A | N/A | N/A | N/A | ⊕⊕⊕⊝ | Hospital admissions was not meta‐analysed due to differing units of measurement by the 2 trials that reported this finding. Notwithstanding that pooling the data for the 2 trials would have yielded high heterogeneity. Hospital admissions were not necessarily attributable to the vaccine |
| Adverse events (number of adverse events/person/year) | 0.319 | 0.456 | RR 1.43 (0.70 to 2.92) | 484 | ⊕⊕⊝⊝ | Despite an estimated absolute increased rate of adverse events in the vaccinated group, the result is negligible (95% CI crosses 1.00) and not statistically significant (P = 0.61). Adverse events were not necessarily attributable to the vaccine |
| Quality of life Not meta‐analysed | N/A | N/A | N/A | N/A | ⊕⊝⊝⊝ | Quality of life was not meta‐analysed due to differing units of measurement, but was reported in 2 trials, which showed an improvement at 6 months in the vaccine group (scoring at least 2 points better than the placebo group; significance unknown) |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in the footnotes. The corresponding risk (and its 95% confidence interval (CI)) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; N/A: not applicable; NTHi: non‐typeable Haemophilus influenzae; OR: odds ratio; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1One study had marked heterogeneity; most studies had a low number of participants; one study had significant attrition. | ||||||
| Study | Vaccinated | Placebo | *Absolute rate difference |
| Clancy 1985 | 0.256 | 0.272 | 0.016 (‐) |
| Clancy 1990 | 1.000 | 1.700 | 0.700 (‐) |
| Clancy 2016 | 0.717 | 0.767 | 0.050 (‐) |
| Lehmann 1991 | 0.800 | 1.210 | 0.410 (‐) |
| Tandon 1991 | 3.355 | 4.364 | 1.009 (‐) |
| Tandon 2010 | 3.667 | 4.350 | 0.683 (‐) |
| Overall mean | 1.633 | 2.111 | 0.478 (‐) |
| *Estimated rate of exacerbation calculated as number of exacerbations per person per year. Refer to Analysis 1.1: Forest plot comparison and rate ratios for exacerbations. | |||
| Study | Vaccinated | Placebo | *Absolute rate difference |
| Clancy 1990 | 0.500 | 1.200 | 0.700 (‐) |
| Tandon 1991 | 5.806 | 10.194 | 4.388 (‐) |
| Tandon 2010 | 3.180 | 7.200 | 4.020 (‐) |
| Overall mean | 3.162 | 6.198 | 3.036 (‐) |
| *Estimated rate of antibiotic prescriptions calculated as number of antibiotic courses per person per year. Refer to Analysis 2.1: Forest plot comparison and rate ratios for antibiotic prescriptions. | |||
| Study | Vaccinated | Placebo | *Absolute rate difference |
| Clancy 2016 | 0.008 | 0.025 | 0.017 (‐) |
| Lehmann 1991 | 0.067 | 0.031 | 0.036 (+) |
| Tandon 1991 | 1.032 | 1.212 | 0.180 (‐) |
| Tandon 2010 | 0.167 | 0.450 | 0.283 (‐) |
| Overall mean | 0.319 | 0.430 | 0.111 (‐) |
| *Estimated rate of adverse events calculated as number of adverse events per person per year. Refer to Analysis 2.2: Forest plot comparison and rate ratios for adverse events. | |||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Exacerbations (number of exacerbations/person) Show forest plot | 6 | 557 | Rate Ratio (Random, 95% CI) | 0.79 [0.57, 1.10] |
| 2 Mortality (deaths during trial period) Show forest plot | 5 | 518 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.62 [0.63, 4.12] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Prescriptions (number of courses/person/year) Show forest plot | 3 | 142 | Rate Ratio (Fixed, 95% CI) | 1.81 [1.35, 2.44] |
| 2 Adverse events (number of adverse events/person) Show forest plot | 4 | 484 | Rate Ratio (Fixed, 95% CI) | 1.43 [0.70, 2.92] |