抗氧化剂用于预防与缓解运动后肌肉酸痛
Referencias
References to studies included in this review
References to studies excluded from this review
References to ongoing studies
Additional references
References to other published versions of this review
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | Randomised controlled trial (cross‐over design) Separated by a 5‐day washout | |
| Participants | Setting: laboratory; USA n = 24 college‐aged males with at least 1 year of weightlifting experience; mean age 21.3 (SE 0.4) years 18 participants completed the study; 1 participant dropped out due to training conflicts with his sport and the other 5 participants withdrew of their own volition due to the inability to tolerate the physical demands of the testing protocol. Inclusion/exclusion criteria This study was limited to males in order to control for fluctuations in cortisol that occur during the menstrual cycle. At initial enrolment, all participants self‐reported to be free from current injuries limiting their ability to train and complete physiological testing. | |
| Interventions | Intervention Black tea extract: each 2‐capsule serving contained 880 mg black tea extract and was standardised for 350 mg theaflavin Placebo Not specified Duration Supplements were taken 9 days before and 2 days after exercise (11 days) | |
| Outcomes | PRIMARY Muscle soreness was assessed using a 10 cm visual analogue scale (VAS). The anchor at 0 corresponds to "no soreness" and at 10 to "too sore to move muscles". Participants were asked to perform one squat with hands on hips and then draw a line on the scale corresponding to their level of soreness. SECONDARY Wingate 30‐second sprint was performed on a Monark 894E Anaerobic Test Ergometer (Monark Exercise AB, Sweden). The load was set according to each participant's mass. The test was 30 seconds of all out cycling followed by 5 minutes of rest and then 8 x 10‐second intervals of all out cycling. Each interval was separated by 2 minutes of rest. The resistance for the Wingate and intervals was set at 0.10 kP/kg body mass. | |
| Exercise type | 30‐second Wingate with 5 minutes rest followed by 8 x 10‐second maximal sprints with 2 minutes recovery | |
| Sources of funding | The study was funded by WellGen, Inc USA through an unrestricted research | |
| Notes | Author was contacted via email on 27 May 2016 to request data for delayed onset muscle soreness but did not respond | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details specified in manuscript Author was contacted via email on 27 May 2016 but did not respond |
| Allocation concealment (selection bias) | Unclear risk | No details specified in manuscript Author was contacted via email on 27 May 2016 but did not respond |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | High risk | 6 participants withdrew from the study Attrition rate = 25% |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory medication and other supplements for the duration of the study Participants were also asked to keep food records |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 18 healthy men who were active in endurance sports but not resistance trained (9 in each group) Mean age vitamin group: 22.7 ± 4.1 years Mean age placebo group: 22.3 ± 3.6 years Inclusion/exclusion criteria Participants were normally actively participating in endurance and sports activities but not resistance training to ensure the whole‐body resistance exercise protocol resulted in detectable muscle soreness and muscle disruption. The participants had not lost or gained weight in the previous year, were not adhering to special diets and were not regular consumers of nutritional supplements including vitamin E. All participants were non‐smokers and not currently taking any medication known to affect any of the dependant variables in the study. | |
| Interventions | Intervention Vitamin E supplementation 992 mg per day (1200 IU) Number of capsules per day not specified Placebo Microcrystalline cellulose 31 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness of the shoulders, chest, quadriceps and hamstrings was evaluated using a visual analogue scale (0 to 10 cm) where 0 is "no pain" and 10 is "extreme pain" after performing shoulder abduction, shoulder horizontal adduction and hip flexion (unloaded squat). | |
| Exercise type | Whole body resistance exercise training protocol; 3 sets of 10 repetitions of 30% to 60% 1 RM | |
| Sources of funding | None | |
| Notes | Authors were contacted on 25 May 2016 to request data for delayed onset muscle soreness with no reply. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were matched according to physical characteristics and training history and then randomly assigned using a computer program |
| Allocation concealment (selection bias) | Unclear risk | No details in the manuscript Authors were contacted on 25 May 2016 with no reply |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplement were not reported |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory medication and other supplements for the duration of the study as well as any form of therapeutic intervention such as massage and ice Participants who were exposed to any form of resistance training were also excluded |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: field and laboratory; UK n = 38 healthy young men (18 in the antioxidant group and 20 in the placebo group); mean age 22 (SD 1) years Inclusion/exclusion criteria All participants were non‐smokers and habitually active in a variety of sports but were unfamiliar with the specific exercise protocol involved in the study | |
| Interventions | Intervention Mixed antioxidant supplement. 400 mg vitamin C, 268 mg vitamin E, 2 mg vitamin B6, 200 µg vitamin B9, 5 µg zinc sulphate, 1 µg vitamin B12 capsules 1 capsule daily Placebo Lactose capsules 6 weeks | |
| Outcomes | PRIMARY Delayed onset muscle soreness using a visual analogue scale 1 to 10 with anchor terms ranging from 1 being "not sore" to 10 being "very very sore" SECONDARY Peak isometric torque of knee flexors Range of motion at the knee | |
| Exercise type | 90‐minute intermittent shuttle running | |
| Sources of funding | The study received financial support from Unilever R&D | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised using a computer generator |
| Allocation concealment (selection bias) | Low risk | Identical capsules ingested twice daily with meals |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | No details on whether participants were asked to refrain from using other supplements or anti‐inflammatory medication |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 18 healthy men, mean age 20.3 (SD 1.70) years Inclusion/exclusion criteria Non‐smokers, not taking vitamin E supplements(or any other antioxidant or related supplements) and had not participated in resistance training, or any other form of structured exercise for at least 6 months | |
| Interventions | Intervention 1200 IU vitamin E supplementation Placebo Safflower oil Duration 30 days | |
| Outcomes | PRIMARY Muscle soreness was assessed using the Descriptor Differential Scale (DDS) at the quadriceps where 0 is "no pain" and 10 is "extreme pain" SECONDARY Peak isometric torque of knee flexors performed on the Biodex. Participants performed 3 maximal voluntary contraction repetitions each being of 5 seconds duration with 60 seconds rest in between | |
| Exercise type | 24 sets of 10 repetitions of eccentric knee flexion and extension contractions | |
| Sources of funding | The authors acknowledged Quest vitamins (Vancouver, BC) for the gracious donation of the vitamin E used in the study. "This work was supported by NSERC (SMP). SMP is the recipient of a PREA and gratefully acknowledges that source of support in aiding in the completion of this research." | |
| Notes | Supplements were given in the form of a capsule Authors were contacted on numerous occasions to request data for delayed onset muscle soreness, maximal voluntary isometric contraction and range of motion with the final email sent 25 May 2016 with no reply | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details in the manuscript Authors were contacted on numerous occasions with final email sent 25 May 2016 with no reply |
| Allocation concealment (selection bias) | Unclear risk | No details in the manuscript Authors were contacted on numerous occasions with final email sent 25 May 2016 with no reply |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were non‐resistance trained and were asked to refrain from using other supplements or anti‐inflammatory medication |
| Methods | Double‐blind randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; England n = 16 healthy men (8 in the experimental group; 8 in the placebo group) Mean age 30 (SD 8) years Inclusion/exclusion criteria Exclusion criteria for the study included > 45 years of age, female, allergy to specific fruit products, currently taking any nutritional supplements or medication, and history of gastrointestinal, renal or cardiovascular disease | |
| Interventions | Intervention Participants were instructed to consume 30 mL of the supplement twice per day (0800 and 1800 hours) for 8 consecutive days (4 days pretrial, on the day of, and 3 days post‐trial). Manuscript states "manufacturer's specification (Cherry Active Ltd, Hanworth, UK), each 30 mL dose of MC contained ˜90–110 Montmorency tart cherries; independent laboratory analysis shows the juice to provide 9.2 mg·mL−1 of anthocyanins and 669.4 mg·mL−1 of carbohydrate (Atlas Biosciences, Tuscon, Ariz., USA)" Placebo A commercially available mixed berry cordial (less than 5% fruit in concentrate form), mixed with 100 mL water and maltodextrin (MyProtein Ltd., Northwich, UK) until matched for carbohydrate content Duration 8 days | |
| Outcomes | PRIMARY Muscle soreness was assessed using a 0 to 200 mm visual analogue scale where 0 is "no pain" and 200 is "pain/soreness as bad as it could be". Participants rated their soreness after completing a squat to approximately a 90° knee flexion before standing and immediately marked upon the scale to indicate their level of soreness SECONDARY Maximum voluntary isometric contraction of the dominant knee extensors was determined using a strain gauge (MIE Medical Research Ltd., Leeds, UK). Participants were seated on a platform and the strain gauge was attached to the dominant ankle at an internal joint angle of 80° (verified by a goniometer). Participants were given standardised verbal encouragement for the duration of each of the 3 maximum 3‐second contraction. Each contraction was separated by 1 minute. Power: 6‐second peak cycle power Cycling efficiency | |
| Exercise type | A 109‐minute cycling trial designed to replicate road race demands on an electromagnetically braked, cycle ergometer (Velotron Racer‐Mate, Seattle, Wash., USA) | |
| Sources of funding | Manuscript states: "The Cherry Marketing Institute (a not for profit organisation) provided financial support for the analysis of inflammatory indices" | |
| Notes | Authors were contacted on 3 February 2017 to request raw data for delayed onset muscle soreness and maximal voluntary isometric contraction and responded on 3 February 2017 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | No details in manuscript Authors confirmed via email on 3 February 2017 that stratified randomisation based on aerobic fitness and coin toss was employed |
| Allocation concealment (selection bias) | Low risk | No details in manuscript Author confirmed via email on 3 February 2017 that opaque vessels used for all drinking bottles and this was prepared by an independent member of the department |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | High risk | Delayed onset muscle soreness data immediately post‐exercise not recorded or reported Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants did not complete any other exercise or take supplements/medication over the course of the study |
| Methods | Double‐blind randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; England n = 16 semi professional male soccer players (8 in the experimental group; 8 in the placebo group) Mean age 25 (SD 4) years Inclusion/exclusion criteria Inclusion criteria required participants to have trained in soccer consistently across the preceding 3 years and be free of any lower limb injury for the preceding 6 months | |
| Interventions | Intervention Participants were instructed to consume 30 mL of the supplement twice per day (0800 and 1800 hours) for 7 consecutive days (4 days pretrial and on each trial day). The supplement was a commercially available Montmorency cherry concentrate (CherryActive, Sunbury, UK); containing a total anthocyanin content of 73.5 mg·L−1 of cyanidin‐3‐glucoside, a total phenolic content of 178.8 gallic acid equivalent·L−1 and an antioxidant capacity (TEAC) of 0.58 trolox equivalents·L−1 Placebo A commercially available, less than 5% fruit, cordial, mixed with water and maltodextrin (MyProtein Ltd, Northwich, UK) until matched for energy content of the intervention (102 kcal) Duration 7 days | |
| Outcomes | PRIMARY Muscle soreness was assessed using a 0 to 200 mm visual analogue scale where 0 is "no pain" and 200 is "unbearably painful". Participants rated their soreness after completing a squat to approximately a 90° knee flexion before standing and immediately marked upon the scale to indicate their level of soreness SECONDARY Maximum voluntary isometric contraction of the dominant knee extensors was determined using a strain gauge (MIE Medical Research Ltd., Leeds, UK). Participants were given standardised verbal encouragement for the duration of each of the 3 maximum 3‐second contractions. Each contraction was separated by 1 minute Sprint performance (20 m ‐ infrared timing gates) Agility: 5‐0‐5 agility test (infrared timing gates) Power: counter movement jump (jump mat) | |
| Exercise type | 12 × 20 m run sprints, departing every 60 seconds followed by an adapted version of the Loughborough Intermittent Shuttle Test (LIST) (6 x 15‐minute sections) | |
| Sources of funding | The Cherry Marketing Institute (a not for profit organisation) provided financial support for the analysis of inflammatory indices | |
| Notes | Authors were contacted on 3 February 2017 to request raw data for delayed onset muscle soreness and maximal voluntary isometric contraction and responded on 3 February 2017 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | No details in manuscript Authors confirmed via email on 3 February 2017 that stratified randomisation based on aerobic fitness and coin toss was employed |
| Allocation concealment (selection bias) | Low risk | Manuscript states: "All supplements were prepared by an independent member of the department prepared in opaque bottles in order to maintain the double blind design" |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | No details in manuscript Authors confirmed via email on 3 February 2017 that all participants completed the study |
| Selective reporting (reporting bias) | High risk | Delayed onset muscle soreness data immediately post‐exercise not recorded or reported Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | Manuscript states that participants "were also provided with a diet record diary and a list of foods to avoid throughout the 4 days prior to and during the trial period" No information on NSAIDs or medication |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 18 healthy women age range 19 to 31 years (9 in each group) Inclusion/exclusion criteria Participants provided a medical history and completed physical activity and diet and supplementation questionnaires to determine eligibility. None had orthopaedic or metabolic conditions that could have affected the variables of measurement. All participants were non‐smokers, did not use oral contraceptives, anti‐inflammatory drugs or dietary supplements (i.e. antioxidants for at least the past 3 months), and all were classified as non‐resistance trained (i.e. had not performed resistance training in the past 12 months). | |
| Interventions | Intervention 268 mg vitamin E, 1 g vitamin C, 90 µg selenium Placebo Lactose placebo pill 3 capsules per day Duration 18 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness in both arms using a visual analogue scale (0 to 10 cm) where 0 is "no pain" and 10 is "unbearable pain" Soreness was measured following active movement of elbow flexion or extension, as well as following light palpitation by the investigators SECONDARY Maximum isometric force was performed on the Biodex isokinetic dynamometer (Biodex Medical Systems, Ronkonkoma, NY). Participants were secured in the Biodex chair by shoulder and lap belts. Participants were asked to perform 3 maximal isometric unilateral contractions with their elbow flexors each lasting 3 seconds with 60 seconds rest in between each effort. Range of motion was measured both relaxed and flexed at the elbow. Range of motion was calculated as relaxed minus flexed. | |
| Exercise type | 4 sets of 12 repetitions of non‐dominant elbow flexors at an angular velocity of 20°/second | |
| Sources of funding | None | |
| Notes | Authors were contacted on 3 October 2013 to request raw data for delayed onset muscle soreness and maximal voluntary isometric contraction and responded on 1 November 2013 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | No details in manuscript Authors were contacted on 24 May 2016; response: "Likely via coin flip or random number selection" |
| Allocation concealment (selection bias) | Low risk | Response: "Blinding code retained by person not associated with research and/or provided in sealed envelope" |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study with 100% compliance |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were non‐resistance trained and relatively inactive Participants were asked to refrain from using other supplements or anti‐inflammatory medication and oral contraceptives |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 20 weight‐trained men (10 in the experimental group; 10 in the placebo group) Antioxidant group: mean age 24 (SEM 1.1) years Placebo group: mean age 26.2 (SEM 2.0) years Inclusion/exclusion criteria All participants had been weight training their lower body for a minimum of 12 months prior to testing and demonstrated a minimum strength of 1.5 times their body weight in the barbell back squat exercise. All participants were free of the orthopaedic and metabolic conditions that would have affected the variables of measurement. | |
| Interventions | Intervention Astaxanthin ‐ BioAstin; 1732 mg safflower oil; haematococcus algae extract (contains 4 mg astaxanthin and 480 mg lutein) Placebo 1732 mg safflower oil 2 capsules per day Duration 3 weeks before and 96 hours after | |
| Outcomes | PRIMARY Delayed onset muscle soreness in the dominant leg during knee extension using a 10 cm visual analogue scale where 0 is "no pain" and 10 is "unbearable pain" SECONDARY Muscle performance 1 RM concentric strength in the knee extension Isometric knee extensor action was performed using the modified York barbell (York, P.A. knee extension/flexion machine. The cable length was adjusted so that the knee was at 90 degrees flexion. Mean dynamic force was determined in the knee extension exercise using a Body‐Solid knee extension machine interfaced with a Fitrodyne dynamometer (Fitronic, Bratislava, Slovakia). | |
| Exercise type | York knee extension machine 10 sets of 10 repetitions at 85% of 1 RM | |
| Sources of funding | The study was supported by Cyanotech Corp. Kailua‐Kona, HI, and IMAGINNutrition, Inc. Laguna Niguel, CA | |
| Notes | Authors were contacted on 3 October 2013 to request raw data for delayed onset muscle soreness and maximal voluntary isometric contraction and responded on 1 November 2013 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | No details in manuscript Authors were contacted on 24 May 2016; response: "Likely via coin flip or random number selection" |
| Allocation concealment (selection bias) | Low risk | No details in manuscript Authors were contacted on 24 May 2016; response: "Blinding code retained by person not associated with research and/or provided in sealed envelope" |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants successfully completed testing with 100% compliance |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | No details on whether participants were asked to refrain from using other supplements or anti‐inflammatory medication |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 36 men mean age 25 (SD 5) years 18 participants had prior exercise and 18 had no prior exercise; only the results for the second group were included in this review "6 participants did not complete the study due to personal reasons (e.g. lack of time, problems with blood donation, injury resulting from accident not to the study" Participants withdrew from the following groups: 1 participant from no prior exercise placebo; 2 participants from no prior exercise antioxidant group; 2 participants from prior exercise placebo group; 1 participant from prior exercise antioxidant group Inclusion/exclusion criteria No participant was vegetarian or a smoker, nor did they use tobacco products, anti‐inflammatory drugs, or antioxidant supplements before (for a minimum of 6 months) or during the study period. Eligible participants were those capable of concentrically bench pressing a load greater or equal to their body mass, who performed resistance training using dynamic (concentric/eccentric) muscle actions for a minimum of 1 year before study participation (with no layoffs during this time period), and who performed upper‐body resistance exercises at least once per week the previous year. | |
| Interventions | Intervention Mixed antioxidant 1000 mg of vitamin C + 378 mg mixed tocopherols – 41 mg alpha, 3 mg beta, 84 mg delta, 250 mg gamma; and 39.5 mg mixed tocotrienols – 11 mg Placebo Soft gel (soybean oil) and powder (cellulose) placebos were identical in appearance to the antioxidants 2 capsules per day Duration 14 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness, visual analogue scale (0 to 10 cm) following performance of 2 (concentric‐eccentric) repetitions of the barbell bench press exercise using a standard 20 kg barbell. 0 represents "no pain" and 10 represents "intense pain" SECONDARY Maximal isometric force in a bench press position measured using a customised force plate and power rack design. The upper arm was fixed parallel to the floor with a 90 degree angle about the elbow joint and the bar was in line with the mid‐sternum | |
| Exercise type | Barbell bench press 10 sets, 10 reps of 70% 1 RM | |
| Sources of funding | Supported in part by Jarrow Formulas and The National Strength and Conditioning Association Graduate Student Research Grant | |
| Notes | Authors were contacted on 3 October 2013 to request raw data for delayed onset muscle soreness and maximal voluntary isometric contraction and responded on 1 November 2013 In our review, only the data from the no prior exercise group were used | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | No details in manuscript Authors were contacted on 24 May 2016; response: "Likely via coin flip or random number selection" |
| Allocation concealment (selection bias) | Low risk | No details in manuscript Authors were contacted on 24 May 2016; response: "Blinding code retained by person not associated with research and/or provided in sealed envelope" |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | High risk | 6 participants did not complete all aspects of the study for personal reasons Attrition rate: 17% |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory medication and other supplements for the duration of the study |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory, USA n = 18 young, untrained males who did not weight train for 6 months, mean age 24.4 (SEM 1.7) years Inclusion/exclusion criteria All participants were prescreened, in good health, abstained from vitamin or herbal supplements for at least 6 months and were free of any muscular injuries | |
| Interventions | Intervention Vitamin C supplementation (3 g per day) Placebo Starch pills 3 capsules per day and participants were asked to keep food records Duration Supplementation given 2 weeks prior and 4 days after exercise | |
| Outcomes | PRIMARY Delayed onset muscle soreness was assessed by means of a linear scale from 1 to 10 in a rested position and in response to palpation on the arms of the muscle where 1 is "no pain" and 10 is "extreme pain" SECONDARY Isometric force was conducted on an isokinetic dynamometer (Biodex System 3 Isokinetic Dynamometer, Biodex Medical Systems, Shirely, NY). Participants performed 3 concentric maximum voluntary contractions (MVC) and the forces were recorded for both the dominant and non‐dominant arms through a full range of motion at a speed of 1.75 rad/second. The highest force obtained with no movement of the lever arm was accepted as the maximum isometric force. Range of motion was assessed on both arms using a goniometer placed on markings from the medial aspect of th elbow of the humerus. | |
| Exercise type | 70 eccentric actions using the elbow flexors | |
| Sources of funding | None | |
| Notes | Authors were contacted via email on 25 November 2013 to request data for delayed onset muscle soreness, maximal voluntary isometric contraction and range of motion, but did not respond | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details in manuscript Authors were contacted via email on 25 November 2013 but no information was provided |
| Allocation concealment (selection bias) | Unclear risk | Participants were given numbered containers for the 3 capsules per day Authors were contacted via email on 25 November 2013 but no information was provided |
| Blinding of participants and personnel (performance bias) | Unclear risk | No details provided in the manuscript Authors were contacted via email on 25 November 2013 but no information was provided |
| Blinding of outcome assessment (detection bias) | Unclear risk | No details provided |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study with no adverse outcomes |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using any supplements; medication and diet was controlled in both groups |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; UK n = 20 physically active males naive to downhill running Placebo group mean age 22.1 (SEM 0.4) years (n = 10) Vitamin C group mean age 24.2 (SEM 1.5) years (n = 10) Inclusion/exclusion criteria All participants were non‐smokers and free from any known illness as ascertained by questionnaire Participants taking any form of vitamin supplementation were excluded | |
| Interventions | Intervention 1 g of vitamin C supplementation Placebo Lactose placebo Duration 14 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness was measured at the gastrocnemius, anterior tibialis, hamstrings, quadriceps, gluteals (both sides) and lower back muscles using a 10‐point visual analogue scale where 0 is "no pain" and 10 is "extreme pain" SECONDARY Muscle function was performed an isokinetic dynamometer. The test involved concentric quadriceps muscle torque assessment at 1.06 and 5.20 rad/second as well as eccentric quadriceps assessment at 2.6 rad/second Muscle tenderness was measurement using pressure algometry at the gastrocnemius, anterior tibialis, hamstrings, quadriceps, gluteals (both sides) and lower back muscles | |
| Exercise type | 30 minutes of downhill running on a treadmill at a grade of ‐15% at 60% VO2max | |
| Sources of funding | None | |
| Notes | No details on whether supplement was administered as a drink or a capsule or a powder Authors were contacted to request raw data for PPT, delayed onset muscle soreness and maximal voluntary isometric contraction on 3 October 2013 and responded on 3 December 2013 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | No details in manuscript Authors were contacted via email 17 May 2016 Author response: "A random number generator to allocate into groups and from memory they were block randomised according to their VO2max" |
| Allocation concealment (selection bias) | Low risk | No details in manuscript Authors were contacted via email 17 May 2016 Author response: "All supplements were given in visually identical capsules double blind" |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study with no adverse effects |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory medication and other supplements for the duration of the study as well as any form of therapeutic intervention such as massage and ice |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: Laboratory and Field; UK n = 14 recreationally trained males mean age 24.7 (SD 4.2) years (6 in each group) 2 participants dropped out for personal reasons Inclusion/exclusion criteria Recreationally trained was defined as participating in physical activity of an intermittent nature at least 3 times per week for at least 12 months. Prospective participants were excluded if they smoked or engaged in any course of supplementation or medication (e.g. antioxidant supplementation) that may have interfered with the study's results. | |
| Interventions | Intervention N‐acetylcysteine supplementation 50 mg/kg Placebo Water and cordial Duration 6 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness was assessed by a 12‐point visual analogue scale where 0 is "no pain" and 12 is "intolerable pain". Participants were required to mark a point on the VAS that corresponded to their perception of total muscle soreness after performing a 90 degree squat. SECONDARY Absolute muscle torque was determined in the dominant limb concentric quadriceps using a Isokinetic Dynamomter (Biodex Medical Systems, Shirely, NY). Concentric quadriceps torque was determined at 60, 180 and 300 rad/second. 3 maximal repetitions were performed at each speed with the greatest value attained being recorded. Yo‐Yo Intermittent Recovery Test Level 1. Involves the performance of consecutive 2 x 20 m shuttles separated by 10 seconds recovery intervals. Running velocity is dictated by audio beeps and increased by 0.5 km/hour throughout the test until volitional exhaustion ensues. Loughborough intermittent Shuttle Test was completed in a well‐ventilated indoor runway. This consists of successive cycles of cruising at 95% VO2max (60 m), jogging at 55% VO2max (60 m), walking (60 m) and maximally sprinting (20 m) between 2 pairs of timing lights placed 20 m apart in time with audio beeps for 15 minutes Side effects on a scale of 0 to 10 | |
| Exercise type | Loughborough intermittent Shuttle Test and Yo‐Yo Intermittent Recovery Test Level 1 | |
| Sources of funding | None | |
| Notes | N‐acetylcysteine and placebo supplementation mixed in water Authors were contacted to request raw data for delayed onset muscle soreness, maximal voluntary isometric contraction and performance data on 3 December 2013 and responded on 5 December 2013 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Pair‐matched based on performance on the baseline test |
| Allocation concealment (selection bias) | Low risk | Not specified in manuscript Authors were contacted on 21 February 2017 and replied "treatment allocation was done in sealed opaque containers" |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | 2 participants dropped out for personal reasons Attrition rate: 14.3% |
| Selective reporting (reporting bias) | Low risk | No published protocol available All outcomes reported at all time points |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory medication and other supplements for the duration of the study as well as any form of therapeutic intervention such as massage and ice |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: 2006, USA n = 24 healthy college males and females mean age 22 (SD 4) years Inclusion/exclusion criteria Without upper extremity injury, or previous known history of injury. Potential participants who indicated arm discomfort during any baseline assessments were excluded. Participants who reported habitually participating in a strenuous resistance‐training programme involving elbow flexors, or unusual upper extremity activity were also excluded. | |
| Interventions | Intervention Vitamin C supplementation 1000 mg 3 times per day Placebo 3 x 50 mg per day of glucose Duration Supplements given 3 days before and 5 days after damaging exercise | |
| Outcomes | PRIMARY Delayed onset muscle soreness assessed at the quadriceps by a 0 to 10 visual analogue scale where 0 is "no discomfort whatsoever" and 10 is "indicated extreme pain and discomfort" SECONDARY Maximal isometric strength Muscle tenderness scores were assessed using a standard manual muscle myometer. Measurements were made just proximal to the distal tendon of the biceps. Force was applied via the probe through a 1 cm diameter head until the participant indicated pain or discomfort. | |
| Exercise type | 40 maximal eccentric contractions of the elbow flexors (2 x 20) | |
| Sources of funding | None | |
| Notes | Authors were contacted on 30 October 2013 to request data for delayed onset muscle soreness and maximal voluntary isometric contraction but did not respond | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomly assigned (no details specified in the manuscript) Authors have been contacted with no response (19 May 2016) |
| Allocation concealment (selection bias) | Unclear risk | No details specified in manuscript Authors have been contacted with no response (19 May 2016) |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory medication and other supplements for the duration of the study as well as any form of therapeutic intervention such as massage and ice. Participants who were exposed to any form of resistance training were also excluded |
| Methods | Randomised controlled trial (cross‐over design) Separated by a 14‐day washout | |
| Participants | Setting: laboratory; USA n = 16 men (training status not specified) Mean age vitamin C group 22.3 (SD 3.90) years Mean age placebo group 22.6 (SD 4.6) years Inclusion/exclusion criteria Not specified Authors were contacted via email on 30 October 2013 and again on 26 May 2016 | |
| Interventions | Intervention Freshly prepared tart cherry juice with commercially available apple juice. One 12 oz bottle of juice provided at least 600 mg phenolic compounds and at least 40 mg of anthocyanins. Each bottle contained approximately 50 to 60 cherries. 2 x 12 oz bottles consumed daily Placebo Unsweetened black cherry Kool‐Aid with added sugar Duration 8 days with a 2‐week washout | |
| Outcomes | PRIMARY Pain scores were obtained by asking participants to verbally rate their overall discomfort during active elbow flexion and extension with activities of daily living on a scale of 0 to 10 where 0 is "no discomfort whatsoever" and 10 is "extreme pain and discomfort" SECONDARY Maximal isometric strength was tested on a modified seated arm curl bench (preacher) with the upper arm supported by a padded bench in about 45 degrees shoulder flexion. Isometric strength was tested at 3 different elbow flexion angles: 130, 90 and 30 degrees. Muscle tenderness scores were assessed using a standard manual muscle myometer. Measurements were made just proximal to the distal tendon of the biceps. Force was applied via the probe through a 1 cm diameter head until the participant indicated pain or discomfort. | |
| Exercise type | 40 (2 x 20) maximal eccentric contraction of the elbow flexors using a modified preacher curl | |
| Sources of funding | The study was funded by Cherrypharm Inc (West Hartford, Connecticut, USA) The authors of the study each have 2.5% equity in Cherrypharm Inc. | |
| Notes | Authors were contacted on 30 October 2013 to request data for delayed onset muscle soreness and maximal voluntary isometric contraction but did not respond | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details specified in the manuscript Authors were contacted via email on 30 October 2013 and again on 26 May 2016 |
| Allocation concealment (selection bias) | Unclear risk | No details specified in the manuscript Authors were contacted via email on 30 October 2013 and again on 26 May 2016 |
| Blinding of participants and personnel (performance bias) | Unclear risk | No details specified in the manuscript Authors were contacted via email on 30 October 2013 and again on 26 May 2016 |
| Blinding of outcome assessment (detection bias) | Unclear risk | No details provided |
| Incomplete outcome data (attrition bias) | High risk | 2 participants withdrew before completion; unclear which group they were in Attrition rate: 12.5% |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory medication and other supplements for the duration of the study as well as any form of therapeutic intervention such as massage and ice. Participants who were exposed to any form of resistance training were also excluded |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory, Spain n = 20 male, healthy, moderately exercising (regular aerobic exercise for at least 4 hours per week), non‐smoking with no injury Mean age 38.1 (SD 11.1) years in placebo group (n = 10) Mean age 32.7 (SD 12.3) years in curcumin group (n = 9) | |
| Interventions | Intervention Curcumin given as the Phytosome delivery system (Meriva) 1 g twice daily corresponding to 200 mg curcumin twice daily Placebo Matched capsules Duration 5 days ‐ supplements taken 2 days prior to running | |
| Outcomes | PRIMARY Delayed onset muscle soreness lower limbs when descending and climbing stairs (4‐point visual analogue scale: 0 is "no pain" and 4 is "disabling pain"). Scores were a sum of 8 sites (anterior right thigh, posterior right thigh, anterior right leg, posterior right leg, anterior left thigh, posterior left thigh, anterior left leg, posterior left leg) | |
| Exercise type | Downhill running test on a treadmill at grade ‐10% at a constant speed (anaerobic threshold) for 45 minutes | |
| Sources of funding | Authors Stefano Togni and Fedrico are employees of Indena SpA the manufacturer of Meriva, Giovanni Appendino is a consultant to Indena SpA Statistical analysis assistance was funded by Indena | |
| Notes | Authors were contacted to request raw data for delayed onset muscle soreness on 18 February 2016 and responded on 18 February 2016 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised used computer software |
| Allocation concealment (selection bias) | Unclear risk | No details of safeguards. Although placebo‐controlled, the sports medicine physicians performing the exercise test beforehand were not blinded |
| Blinding of participants and personnel (performance bias) | High risk | "Study subjects and physicians performing the radiologic and laboratory assessments were blinded to treatment, whereas the sports medicine physicians involved in exercise testing were not." It is not explained why the lattermost were not blinded |
| Blinding of outcome assessment (detection bias) | Unclear risk | "Study subjects and physicians performing the radiologic and laboratory assessments were blinded to treatment, whereas the sports medicine physicians involved in exercise testing were not." It is likely that the participants reporting DOMS were blinded but some uncertainty remains |
| Incomplete outcome data (attrition bias) | Low risk | 1 dropout by personal decision; 5% dropout rate |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory medication and other supplements for the duration of the study Participants were familiarised with the protocol and diet was standardised |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 44 healthy college aged men age range 18 to 35 years Mean age in the antioxidant group 23.8 (SEM 3.6) years (n = 21) Mean age in the placebo group 22.8 (SEM 0.7) years (n = 20) Inclusion/exclusion criteria All participants completed a medical history, diet, supplement and fitness questionnaire to determine eligibility. Participants were non‐smokers, were not on anti‐inflammatory drugs or on dietary supplements for at least 3 months and refrained from these substances throughout the study. | |
| Interventions | Intervention Fruit, vegetable and berry juice powder (7.5 mg beta‐carotene, 276 mg vitamin C and 108 IU of vitamin E) (Juice Plus+, NSA, LLC, Collierville, TN) Placebo Microcrystalline cellulose capsules Participants were given a sealed container and were asked to take 6 capsules per day, 3 in the morning and 3 in the afternoon Duration 28 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness was measured at the elbow flexor with the arm rested using a visual linear scale ranging from 1 to 10 where 1 is "no pain" and 10 is "extreme pain" SECONDARY Maximal isometric strength was measured on a Biodex isokinetic dynamometer. Each participant performed 3 maximal isometric force contractions with their non‐dominant and dominant arm elbow flexors each lasting 3 seconds with 60 seconds rest in between each effort. Range of motion was assessed using a goniometer assessing the elbow flexors on both arms by asking participants to flex and extend their arms at the elbows. | |
| Exercise type | 4 sets of 12 repetitions of eccentric actions of the elbow flexors | |
| Sources of funding | The research study was partially supported by the NSA LLC and the University of North Carolina Greensboro | |
| Notes | Authors were contacted on 25 November 2013 to request data for delayed onset muscle soreness, maximal voluntary isometric contraction and range of motion but did not respond | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Participants were randomised but no details provided in the manuscript on how this was done Authors were contacted on 25 November 2013 with no reply |
| Allocation concealment (selection bias) | Unclear risk | No details in the manuscript Authors were contacted on 25 November 2013 via email with no reply |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | 3 participants did not complete the study: 2 participants were from the placebo group and 1 participant was from the supplementation group Attrition rate: 6.8% |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory medication and other supplements for the duration of the study as well as any form of therapeutic intervention such as massage and ice. Participants who were exposed to any form of resistance training were also excluded |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory, USA n = 22 moderately trained males age range 18 to 25 years Mean age supplement group 20.5 (SD 2.3) years n = 11 Mean age placebo group 21.3 (SD 4.0) years n = 11 Inclusion/exclusion criteria Exclusion criteria included people who smoke, take any medication that would alter cardiovascular or metabolic function, have musculoskeletal limitations or use anti‐inflammatory drugs. People who supplemented with vitamin C and vitamin E or other antioxidants within 3 months prior to the study were excluded. | |
| Interventions | Intervention Capsules 100 mg vitamin C and 400 IU vitamin E ingested daily for 2 weeks Placebo Maltodextrin capsules identical to supplement group Duration 17 days to 14 days before and 2 days after the downhill run | |
| Outcomes | PRIMARY Delayed onset muscle soreness of the quadriceps, hamstrings, gluteus, gastrocnemius and tibialis anterior using a visual analogue scale of 0 "no pain" to 6 "unbearable pain" | |
| Exercise type | 40 minutes downhill running ‐10% grade at 65% to 70% VO2max | |
| Sources of funding | Funded by Wastl Human Performance Laboratory, Donald L. Corrigan Professional Development Grant and Purdue Bilsland Strategic Initiative Fellowship | |
| Notes | Compliance with supplementation was 99.4% as assessed by random capsule count Authors were contacted to request raw data for delayed onset muscle soreness on 24 February 2016 and responded on 25 February 2016 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generator |
| Allocation concealment (selection bias) | Low risk | Double‐blind |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory medication and other supplements |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 37 men between the ages of 18 and 35 years who were recreationally active High‐dose (n = 12) mean age 24.33 (SEM 1.54) years Low‐dose (n = 12) mean age 21.67 (SEM 1.12) years Placebo (n = 13) mean age 22.69 (SEM 1) years Inclusion/exclusion criteria Men who were recreationally active in both resistance and cardiovascular training yet not exercising for more that 6 hours per week were included. The training criteria required that participants be actively performing aerobic exercise and partaking in resistance training at least twice per week for a minimum of 3 months. Participants were excluded who were actively engaged in eccentric muscle training, downhill running, running more that 15 miles per week or presented with certain diseases or conditions such as HIV, hepatitis B and C, uncontrolled cardiovascular arrhythmias, chronic obstructive pulmonary disease, emphysema, diabetes, or unresolved orthopaedic concerns. Additional exclusion criteria included a body mass index of < 18 or > 30 kg/m2, use of tobacco products within the previous 12 months, and regular consumption of medications or over‐the‐counter therapies that might affect inflammation such as: green or black tea, green or black tea supplements, cherry juice, vitamin E, vitamin C, aspirin, corticosteroids, anabolic steroids or NSAIDs | |
| Interventions | Intervention A blend of water‐extracted black and green tea (Camellia sinensis) containing a minimum of 40% total polyphenols, 1.3% theaflavins, 5% to 8% epigallocatechin‐3‐gallate, 7% to 13% caffeine, and 600 ppm manganese. There were 3 groups in this study: Group 1: high‐dose (2000 mg per day polyphenolic blend) n = 12 Group 2: low‐dose (1000 mg per day polyphenolic blend) n = 12 Group 3: placebo n = 13 2 capsules twice per day were consumed Placebo 4 capsules per day of 500 mg microcrystalline cellulose excipient as 2 capsules twice per day were consumed Duration 13 weeks | |
| Outcomes | Primary Muscle soreness was assessed using a 7‐point Likert scale questionnaire for a variety of muscle groups including the gastrocnemius, hamstrings, quadriceps, gluteus maximus, lower back, abdominals and the whole body where 1 is "no pain" and 7 is "severe pain" Secondary Muscle strength All muscle strength tests were performed on a Biodex System 3 dynamometer (Biodex Medical Systems, Shirley, NY, USA). Participants performed 3 sets of quadriceps leg extensions on their dominant leg for 12 repetitions at 120 degrees per second. | |
| Exercise type | Downhill running on a treadmill consisted of running at a 10% decline for 40 minutes at a speed associated with 65% of VO2max | |
| Sources of funding | Source of funding for the study was Kemin Foods, L.C. All authors were employed by the sponsor company and manufacturer of the polyphenol blend at the time of the clinical trial. | |
| Notes | The authors of Herrlinger 2015 were contacted on 3 February 2017 and again on 18 February 2017 for missing data (delayed onset muscle soreness and maximal voluntary isometric contraction maximal voluntary isometric contraction) as these were not available in the manuscript and could not be extracted from graphs. No response was received and this study was therefore included in the qualitative analysis but not the quantitative analysis. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Authors indicate random assignment to one of 3 groups (placebo, low‐dose, high‐dose), however methods to achieve randomisation were not indicated in the manuscript Authors contacted 3 February 2017 but no response was received |
| Allocation concealment (selection bias) | Low risk | No details in manuscript Authors contacted 3 February 2017 via email but no response was received |
| Blinding of participants and personnel (performance bias) | Unclear risk | No details in manuscript Authors contacted 3 February 2017 via email but no response was received |
| Blinding of outcome assessment (detection bias) | Unclear risk | No details provided |
| Incomplete outcome data (attrition bias) | Low risk | From 39 participants randomised 37 completed the intervention (12 each for low and high; 13 for placebo); 1 participant was withdrawn due to elevated creatine kinase during follow‐up testing (high‐dose group) and 1 participant was excluded due to < 80% compliance (low‐dose group) |
| Selective reporting (reporting bias) | High risk | All outcomes reported at all time points Manuscripts states that participants were "contacted on a weekly basis by phone or email to ask about any adverse events..." although adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Diet diaries performed prior to and during baseline testing, however diet was not monitored during or post‐intervention. Pre‐test meals not standardised for all participants however advice provided. |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: Field; UK n = 20 moderately trained male (13) and female (7) runners Mean age cherry juice group 37 (SD 13) years Mean age placebo group 38 (SD 5) years Inclusion/exclusion criteria 18 of the participants were accepted for, and completed, the 2008 London Marathon. All participants completed a health screening questionnaire and a written informed consent. | |
| Interventions | Intervention Tart cherry juice blend; 2 x 8 fl oz bottles per day. One bottle of the juice contained the equivalent of 50 to 60 cherries and provided at least 600 mg phenolic compounds, expressed as gallic acid equivalents, 32 g of carbohydrate and at least 40 mg of anthocyanins. One bottle in the morning and one in the afternoon Placebo Fruit flavoured concentrate mixed with 8 fl oz of water Duration 5 days before and 2 days after | |
| Outcomes | PRIMARY Delayed onset muscle soreness was determined using a 200 mm visual analogue scale where 0 is "no soreness" and 200 is "unbearably painful." The participant stood with the hands on hips and feet approximately shoulder width apart. The participant was then asked to squat down to 90 degrees (internal joint angle) rise to the start position and then indicate on the visual analogue scale the soreness felt in the lower limbs. SECONDARY Maximum voluntary isometric contraction of the non‐dominant knee extensors was determined using a strain gauge (MIE Medical Research Ltd, Leeds, UK). Participants were seated on a platform and the non‐dominant ankle was attached to the strain gauge at an internal joint angle of 80 degrees (verified by a goniometer). Participants were given 3 submaximal trials, each separated by 1 minute. Each contraction lasted approximately 3 seconds and all participants were given standardised verbal encouragement throughout. | |
| Exercise type | Participants completed the 2008 London marathon. The environmental conditions on the day were barometric pressure: 758 mmHg; temperature: 7 degrees Celsius; wind speed: 4 km/h; relative humidity: 56%; there were intermittent showers throughout the day. 2 volunteers completed the marathon distance on similar terrain 14 days after the London Marathon | |
| Sources of funding | The authors thanked Dr Marco Cardinale from the British Olympic Association for procuring technical support and St Mary's University College Scholarship and Research Support Fund for financial support of the project | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Pseudo‐randomised based on predicted finishing time. "We also attempted to balance the number of male and female participants in each group to account for possible sex differences" |
| Allocation concealment (selection bias) | Unclear risk | No details in manuscript Authors were contacted via email on 27 May 2016 Author reply: "allocation was based on sex and predicted finish time. So randomised, but stratified. ABBA style and treatments were given in identical containers" |
| Blinding of participants and personnel (performance bias) | High risk | Not specified in manuscript Authors were contacted via email on 27 May 2016 Author reply: "Single blind"; thus the personnel were not blinded |
| Blinding of outcome assessment (detection bias) | Low risk | Blinded for participants |
| Incomplete outcome data (attrition bias) | Low risk | All the participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to keep a food diary and to refrain from taking supplements or taking part in strenuous exercise other than the marathon |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 16 college students (24 were originally recruited) Mean age blackcurrant group (n = 9, 7 female) 19.5 (SEM 0.3) years Mean age placebo group (n = 8, 6 female) 20.9 (SEM 0.9) years Inclusion/exclusion criteria Inclusion criteria included being untrained, moderately active, between the ages of 18 and 40 years. Exclusion criteria included a recent history of ankle, knee, hip or back pain that precluded squatting exercises, and the use of anti‐inflammatory or analgesic drugs that would reduce pain. | |
| Interventions | Intervention Commercially available blackcurrant nectar (CurrantC) was provided by CorpPharms (Staatsburg, NY). Each 16 oz bottle contained approximately 100 g of fruit, malvidin glucosides 193.25 mg, cyanidin glucosides 175.69 mg Placebo The placebo drink was produced by mixing black cherry Kool‐Aid powder (Kraft, Ryrerbrook, NY, USA) with water Duration 8 days | |
| Outcomes | Primary Muscle soreness was assessed during a full range squat with no external weight using a 0 to 10 scale where 0 is "no soreness" and 10 is "extreme discomfort" | |
| Exercise type | Eccentric squatting session consisted of 3 sets of 10 repetitions of eccentric contractions using a bar weighted with 115% of the respective 1 repetition maximum | |
| Sources of funding | None | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Independent 3rd party completed randomisation using random number generation in Excel |
| Allocation concealment (selection bias) | Unclear risk | Not indicated in the manuscript |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind; labels removed from bottles; neither personnel nor participants aware of contents |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | High risk | 24 recruited, 16 completed the study (4 illness; 3 injury; 1 removed due to undertaking resistance training prior to study) |
| Selective reporting (reporting bias) | High risk | All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Diet not standardised during the trial however participants advised to maintain normal diet and avoid anti‐inflammatory foods and drugs |
| Methods | Randomised controlled trial (cross‐over design) | |
| Participants | Setting: laboratory; USA n = 25 healthy college students and college employees. Of the 25 original participants, 2 dropped out of the experiment, 3 were excluded for a variety of reasons (loss of capsule integrity, failure to properly maintain records, non‐compliance with the experimental protocol), and 1 was removed for failure to develop delayed onset muscle soreness in either trial. Left with 19 participants (6 women and 13 men). Age rage 24 to 48 years Inclusion/exclusion criteria Participants were excluded from the study if they were older than 50 years, had a sensitivity to lactose, took analgesic or anti‐inflammatory agents during the trials, participated in rigorous athletic training, had a current musculoskeletal ailment in the legs, or took ascorbic acid or riboflavin supplements within 3 weeks of the study | |
| Interventions | Intervention Vitamin C 1000 mg as 3 capsules per day Placebo Lactose capsules Duration Vitamin C taken 3 days before and 7 days after exercise with a 3‐week washout period | |
| Outcomes | PRIMARY Delayed onset muscle soreness was monitored by self‐reporting using a 10 cm continuous unmarked line as a visual analogue scale anchored with 1 "have no soreness" at one end and 10 "my soreness could not be any worse" at the other | |
| Exercise type | Strenuous eccentric work of the plantar flexors of the calf | |
| Sources of funding | None | |
| Notes | Participants were asked to refrain from using anti‐inflammatory medication and other supplements for the duration of the study Authors were contacted to request raw data for delayed onset muscle soreness on 3 December 2013 and responded on 9 December 2013 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised using a computer program |
| Allocation concealment (selection bias) | Unclear risk | No details provided in manuscript |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | High risk | 6 participants dropped out and were excluded for a variety of reasons Attrition rate: 24% |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory medication and other supplements for the duration of the study |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 30 healthy non‐resistance trained men mean age 20 (SD 1.8) years Inclusion/exclusion criteria Non‐resistance trained men defined as less than 1 workout per month over the last 6 months. All participants were classified as low risk for cardiovascular disease with no contraindications to exercise according to the American College of Sports Medicine. No nutritional supplements (including multivitamins) were consumed at least 3 months prior to the study | |
| Interventions | Interventions 1. 1800 mg N‐acetyl‐cysteine (NAC) Placebo 1000 mg glucomannan Supplements were taken in the morning on an empty stomach and compliance was monitored by making phone calls and participants bringing back empty bottles during next visit Duration 14 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness was assessed at the quadriceps along a 10 cm visual analogue scale where 0 is "no soreness" and 10 is "extreme soreness" SECONDARY Peak isometric torque was assessed using a Biodex System‐3 isokinetic dynamometer 9 Biodex Medical Systems, Inc, NY, USA). Prior to testing participants warmed up on a cycle ergometer for 10 minutes. Changes in dynamic strength of the knee extensors was assessed by having participants complete 10 maximal repetitions in a concentric and eccentric fashion. Peak dynamic torque was measured in the dominant knee extensors, a total of 3 maximal voluntary contractions over 5 seconds duration were completed with 60 seconds rest in between each repetition. Participants were verbally encouraged to produce maximal effort throughout the entire 5‐second period. The peak torque exerted throughout all 3 repetitions was regarded as peak isometric torque. All isometric repetitions were completed at an angle of 90 degrees flexion. | |
| Exercise type | 10 sets of 10 repetitions at an isokinetic dynamometer; 1 minute rest between sets | |
| Sources of funding | Partial funding for the study was provided by the National Strength and Conditioning Association through GNC Nutritional Research Grant, a Baylor University Faculty Research Award for Darryn Willoughby, PhD and HHPR a graduate student research award and indirect costs provided by grants awarded to Richard Kreider, PhD through the Exercise and Sports Nutrition Laboratory while at Baylor university | |
| Notes | Authors were contacted on 2 November 2013 to request raw data for delayed onset muscle soreness and maximal voluntary isometric contraction and responded on 3 December 2013 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Participants were matched in clusters according to age and body weight for assignment |
| Allocation concealment (selection bias) | Low risk | Clear capsules provided |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | A total of 3 participants did not complete the study; 2 participants withdrew from the study and 1 was excluded due to non‐compliance Attrition rate: 10% |
| Selective reporting (reporting bias) | Low risk | No published protocol available All outcomes reported at all time points "No adverse outcomes were reported to the supplementation protocol" |
| Other bias | Low risk | Food records were obtained, participants were instructed to minimise foods high in quercetin and were asked to refrain from taking any other supplements or anti‐inflammatory medication or to engage in any other modality that could enhance recovery |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; Poland n = 50 male volunteers recruited from local paper 36 to the pollen group; mean age pollen extract group 35.1 (SEM 2.62) years 14 to the placebo group; mean age placebo group 35.1 (SEM 2.62) years Inclusion/exclusion criteria Inclusion criteria were absence of hypertension, diabetes, cardiovascular disease, organic brain disease, alcohol or drug dependence and any other deviation from good health, no physical training or permanent or intensive basis and the lack of any ongoing medication | |
| Interventions | Intervention Pollen extract; superoxide dismutase activity of approximately 30,000 units per gram/Polbax (Allegon, Sweden) Placebo Placebo not specified Duration 4 weeks | |
| Outcomes | PRIMARY Delayed onset muscle soreness, visual analogue scale (0 to 10 cm) where 0 is "no pain and discomfort" and 10 is "intense pain and discomfort." | |
| Exercise type | A circuit exercise test which consisted of 10 minutes on the step up test, 30 minutes cycling at 70% VO2max followed by 10 minutes on the step test. 30 minutes of cycling at 60% VO2max followed by 10 minutes on the step test repeated twice. | |
| Sources of funding | The study was supported by the Swedish Sports Council and Askers Foundation | |
| Notes | All the authors were contacted several times via email with no response. Maximal voluntary strength data were not reported in the manuscript either in a graph or a table and delayed onset muscle soreness data were reported as a difference between the starting values therefore data could not be extracted Authors were contacted on 3 November 2016 to request data for delayed onset muscle soreness but did not respond | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details in manuscript 36 participants in experimental group and 14 in the placebo Authors contacted several times but did not respond |
| Allocation concealment (selection bias) | Unclear risk | No details in manuscript Authors contacted several times but did not respond |
| Blinding of participants and personnel (performance bias) | Low risk | Manuscript states: "tablets were given in a double blind manner" |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Unclear risk | No details in manuscript It appears as if all participants completed the study Authors contacted several times but did not respond. |
| Selective reporting (reporting bias) | High risk | No protocol available All data reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | Manuscript states: "All participants explicitly asked to follow their habitual style of life, particularly with regards to diet and physical activity", but no details on whether participants were asked to refrain from NSAIDs or any other supplements |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: field; USA n = 54 male (36) and female (18) runners participating in the Hood Coast Relay; mean age 35.8 (SD 9.6) years; 25 participant in the placebo group and 26 participants in the Cherry group Inclusion/exclusion criteria Inclusion criteria included an ability and willingness to abstain from anti‐inflammatory or pain relieving drugs, and willingness to refrain from seeking any other treatment for symptoms of muscle damage until the competition of the study Exclusion criteria included recent use of pain management methods (including acupuncture, transcutaneous electrical nerve stimulation, topical medications/aesthetics, muscle relaxants, injections or systematic steroids). Women capable of becoming pregnant completed a pregnancy test to rule out pregnancy prior to participation. | |
| Interventions | Intervention Cherry juice 10.5 oz: 600 mg phenolic compounds, 40 mg anthocyanins, 40 to 50 cherries Placebo Unsweetened fruit punch with added sugar to match the cherry juice Duration 7 days before the race and 8 days during the race; total 15 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness was assessed using a standard 100 mm visual analogue scale where 0 is "no pain" and 100 is "most severe pain." After finishing the race, participants completed the pain VAS for general soreness. | |
| Exercise type | Hood Coast Relay ‐ 315 km. Each participant completed 3 running segments during the race with individual segments ranging from 5.6 (SD 2.5) km and an average total running distance of 26.3 (SD 2.5) km. | |
| Sources of funding | No external funding was provided for this study. Cherrish Corporation (Seattle. WA) provided the cherry juice in the study | |
| Notes | 2 x 335 bottles daily prior to race | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details in manuscript |
| Allocation concealment (selection bias) | Unclear risk | No details in manuscript |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | 3 participants dropped out (2 from experimental group and 1 from placebo due to NSAID use) Attrition rate: 6% |
| Selective reporting (reporting bias) | Low risk | Study protocol published in ClincalTrials.gov (NCT00733395) All outcomes published in study protocol were reported in the actual study All outcomes reported at all time points Tart cherry juice caused mild gastrointestinal distress in 1 participant |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory medication, any other supplements or seek any modality to reduce muscle soreness |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: field; UK n = 7 (experimental group of 3, placebo group of 4) well trained distance runners, age range 40 to 55 years Originally 8 (all males) were recruited but 1 participant in the experimental group was excluded because of a viral infection during the study Inclusion/exclusion criteria Inclusion criteria were male gender and age 20 to 55 years. The male gender and age were chosen to ensure a homogenous cohort and to optimise the safety of the use of resveratrol Exclusion criteria included a past medical history of chronic inflammatory medical conditions, muscle disorders or heart conditions, and a drug history of immune suppressants or anti‐inflammatories | |
| Interventions | Intervention 600 mg of resveratrol daily for 7 days and immediately before the marathon 2 x 100 mg tablets were taken 3 times daily Placebo Not specified Duration 9 days | |
| Outcomes | PRIMARY General soreness on both legs; delayed onset muscle soreness, 10‐point visual analogue scale: 0 "complete absence of pain" to 10 "indicating extreme soreness with noticeable pain and stiffness at all times" | |
| Exercise type | Running the London marathon race in 2010 | |
| Sources of funding | None declared | |
| Notes | Participants were asked not to alter their diet in any way and were not given any nutrition or hydration advice prior to the race Authors were contacted to request raw data for delayed onset muscle soreness on 18 February 2016 and responded on 18 February 2016 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer block randomisation |
| Allocation concealment (selection bias) | Low risk | Double‐blind Before randomisation 2 different sets of envelopes had been prepared by an independent person not associated with the study |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All outcomes reported at all time points |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points "None of the seven participants reported any adverse effects during the study period or during the marathon itself" |
| Other bias | Low risk | Participants were asked not to alter their diet in any way and were not given any nutrition or hydration advice prior to the race Participants were instructed to avoid anti‐inflammatory medication |
| Methods | Randomised controlled trial (single‐blind, parallel design) | |
| Participants | Setting: field; UK n = 21 (experimental group of 11, placebo group of 10; 2 participants were excluded from the bilberry group as they failed to report to the lab to provide follow‐up data), recreationally trained runners, age range 18 to 55 years Inclusion/exclusion criteria Individuals with cardiovascular disease, diabetes, hypertension, gastrointestinal problems, renal disease, musculoskeletal problems, regular antioxidant or NSAIDs use, and any food allergies were excluded from the study | |
| Interventions | Intervention 2 x 200 mL of bilberry juice daily for 5 days before completing the Sheffield Half Marathon, on race day and for 2 days post‐race Total phenol content per 200 mL serving was 744.14 ± 81.75 mg (n = 3). and 80.04 ± 3.51 mg (n = 3) of total anthocyanins Placebo Energy matched control drink Duration 8 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness, 200 mm visual analogue scale, rated after a squat to a 90 angle and returning to a standing position: 0 "complete absence of pain" to 200 "indicating extreme soreness with noticeable pain and stiffness at all times" | |
| Exercise type | Sheffield half marathon | |
| Sources of funding | The study was funded by Sheffield Hallam University | |
| Notes | 2 x 200 mL of bilberry juice was consumed 5 days before the race, on the day of, and up to 48 hours post race | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | No details in published abstract Authors confirmed via email on 3 February 2017 that a "random numbers generator" was employed |
| Allocation concealment (selection bias) | Unclear risk | No details in published abstract Authors described via email on 3 February 2017 that the "Study was single blind so investigators knew which drink each participant got" and "drinks were given in non‐labelled container" Adequate safeguards not reported |
| Blinding of participants and personnel (performance bias) | High risk | No details in published abstract Authors described via email on 3 February 2017 that the "Study was single blind so investigators knew which drink each participant got" and "drinks were given in non‐labelled container" Not blinded |
| Blinding of outcome assessment (detection bias) | Unclear risk | Participants may have remained blinded but this is not confirmed |
| Incomplete outcome data (attrition bias) | High risk | No details in published abstract Authors confirmed via email on 3 February 2017 that "Of the 21 participants, we missed getting data from 2, one missed the post race sample, and on the last day one other person was missed ‐ both were in the bilberry group" |
| Selective reporting (reporting bias) | Low risk | No published protocol All data available at all time points Personal communication: "None of the participants reported any adverse effects from consuming the Bilberry juice or the placebo" |
| Other bias | Low risk | Participants were asked to complete a food diary and were asked to refrain from using anti‐inflammatory drugs or other supplements that could reduce soreness |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 12 males who were recreationally weight trained for at least 1 year Mean age placebo group 22.0 (SEM) 0.85 (n = 6) Mean age vitamin E group 21.17 (SEM) 0.65 (n = 6) Inclusion/exclusion criteria All participants were required to be recreationally weight trained with resistance training experience of at least 1 year. Participants had no medical problems (e.g. orthopaedic, endocrine, cardiovascular) that would confound the results of this investigation. | |
| Interventions | Intervention 992 mg per day of vitamin E (1200 IU) Placebo Identical looking cellulose capsule ‐ no detail on contents Duration 2 weeks | |
| Outcomes | PRIMARY Delayed onset muscle soreness, visual analogue scale (0 to 10 cm) where 0 is "no soreness" and 10 is "extremely sore" | |
| Exercise type | Heavy resistance exercise protocol | |
| Sources of funding | None | |
| Notes | 1 capsule taken daily | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details in the manuscript Authors were contacted via email on 14 May 2016 but no response |
| Allocation concealment (selection bias) | Unclear risk | No details in the manuscript Authors were contacted via email on 14 May 2016 but no response |
| Blinding of participants and personnel (performance bias) | Unclear risk | No details in the manuscript Authors were contacted via email on 14 May 2016 but no response |
| Blinding of outcome assessment (detection bias) | Unclear risk | No details provided |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | Diet was controlled using food records, however no details on whether participants were asked to refrain from using anti‐inflammatory medication, any other supplements or seeking any modality to reduce muscle soreness |
| Methods | Randomised, double‐blind (cross‐over design) 5‐week washout period | |
| Participants | Setting: field/laboratory; Australia n = 9 highly‐trained (elite) male water polo players from the Western Australian Institute of Sport Mean age 18.6 (SD 1.4) Inclusion/exclusion criteria Not specified ‐ authors contacted on 4 February 2017 and a reply received 8 February 2017: "Participants had to be a part of the West Australian Institute of Sport Men’s High Performance Water polo squad that attend daily training sessions. Participants were not taking any vitamin supplements (as per WAIS supplements policy). Maintained daily contact with the research group to ensure consumption of the prescribed supplement." | |
| Interventions | Intervention 90 mL daily for 6 days of tart Montmorency Cherry Juice (Prunus cerasus) concentrate (Cherry Active, Sunbury, UK) diluted with water, such that each 30 mL serving was made up into a 200 mL beverage. Both the cherry juice and placebo were consumed in 2 doses each day; 200 mL before morning training, and 400 mL in the evening post training. Placebo 3 different 'off the shelf' cordials: lime (Woolworths select lime cordial, Australia), cranberry (Bickford's cranberry juice cordial, Australia) and raspberry (Cottee's raspberry flavoured cordial, Australia). Cordials were mixed with food colouring and 480 mL of water in order to closely imitate the taste, colour and carbohydrate content. Duration 6 days | |
| Outcomes | Primary Delayed onset muscle soreness (delayed onset muscle soreness) was measured on a 0 to 10 scale in the upper body, upper legs, lower legs and overall body encompassing the anchor points of 0 (normal; without pain or stiffness) to 10 (very painful) Total quality of recovery was also recorded on a 6‐ to 20‐point scale for the upper body, upper legs, lower legs and overall body, which encompassed the anchor points 6 (very, very poor recovery) to 20 (very, very good recovery) Secondary Swimming‐based tests comprised of the in‐water vertical jump test, 10 m sprint test, a repeat sprint test and the Water Polo Intermittent Shuttle Test | |
| Exercise type | A fixed training regimen for 6 days. All training (technical skill, weights, and swimming) performed during the 7‐day trials was identical, and took place in the controlled environment of the indoor Water Polo pool or gymnasium. | |
| Sources of funding | Manuscript states: "Funds received from the Australian Institute of Sport and the Australian Sports Commission" | |
| Notes | This study was only included in the qualitative analysis because the exercise paradigm was completely different to all the other studies included in this review. The other studies used an exercise paradigm where mechanical or whole body aerobic exercise was used to cause muscle damage and then a range of outcomes such as muscle soreness, muscle function, range of motion and performance were measured at various time points up to several days after exercise. However, participants in this study had a fixed daily training regimen for 5 continuous days performance, with outcomes being measured at the start and then throughout the trial. Thus the severity of muscle damage caused by the daily training regimen was not controlled | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Manuscript states: "randomised, double‐blind, repeated measures, crossover design". No specific details provided on how randomisation was completed Authors contacted on 4 February 2017 and response was received on 8 February 2017: "Each participant was assigned a participant number and randomised by a number generator into two separate groups." |
| Allocation concealment (selection bias) | Low risk | No specific details provided on how randomisation was completed Authors contacted on 4 February 2017 and a response was received on 8 February 2017: "Fluids were prepared (by an independent researcher) in the absence of the athletes and researchers involved in the performance testing. PLA was made to look and taste the same as the CJ (specific product details within the manuscript). Bottles were then labelled with athlete names to ensure no mix‐up." |
| Blinding of participants and personnel (performance bias) | Low risk | Manuscript states: "randomised, double‐blind, repeated measures, crossover design" |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | No details in the manuscript |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | Manuscript states: "A limitation of this investigation is that the anthocyanin concentration of both the commercial and placebo supplement used was not confirmed" |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 28 participants (40 in all) Mean age curcumin group (n = 16, 11 females) 20 (SD 1) years Mean age placebo group (n = 12, 7 females) 19 (SD 2) years "We experienced a 30% attrition/non‐compliance"; it was not specified which group these participants withdrew from. Inclusion/exclusion criteria Exclusion criteria included regular resistance training in the previous 6 months, leg muscle or orthopaedic condition, arthritis or other chronic inflammatory injury in the lower extremity, regular ingestion of curcumin containing foods, regular anti‐inflammatory use, intake of curcumin supplementation in the pas 6 months and any other condition that would prohibit the completion of the lower body resistance exercise protocol | |
| Interventions | Intervention Curcumin supplementation (Longvida; Verdure Sciences Corp, Noblesville, IN) 400 mg per dose; total study dose 2400 mg Placebo 400 mg rice flour Duration 2 days prior to exercise, the day of and 3 days after exercise, total duration of 6 days | |
| Outcomes | PRIMARY Soreness was measured using a 10 cm visual analogue scale from 0 at one end "no pain" to 10 "severe pain" at the other end. Measures of soreness were made on the thigh (i.e. quadriceps). A gauge was applied using standard fore (20 to 30 N) over the distal, middle and proximal thigh in a seated position with the knee fully extended and relaxed. The 3 ratings for each quadricep were added together | |
| Exercise type | 6 sets of 10 repetition of the leg press exercise with a start load set at 110% of the estimated 1 repetition maximum | |
| Sources of funding | The study was partially funded by a grant from Verdure Sciences Corp (PI: McFarlin) and the National Strength and Conditioning Association to the University of North Texas | |
| Notes | Authors contacted on 4 February 2017 to request data for delayed onset muscle soreness but no reply was received | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Manuscript states: "Stratified randomization (based on gender and initial strength) was used to assign participants to the treatment conditions to ensure similar numbers of men and women and a balance based on initial muscle strength between conditions" |
| Allocation concealment (selection bias) | Unclear risk | No specific details provided on how randomisation was completed Authors contacted on 4 February 2017 but no reply was received |
| Blinding of participants and personnel (performance bias) | Low risk | Manuscript states: "Subjects were provided supplements using a double‐blind approach". However, no specific details were provided. Authors contacted on 4 February 2017 but no reply was received |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | High risk | Manuscript states: "we enrolled 20 subjects per group" and "In the case of the present study, no subjects asked to drop (sic), thus the key source of attrition was associated with lack of adherence to the study protocol or sample collection." This equates to 30% data loss and there was an uneven dropout rate between groups. |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Manuscript states: "Exclusion criteria included: regular resistance training in the previous 6 months, leg muscle or orthopedic condition, arthritis or other chronic inflammatory injury in the lower extremity, regular ingestion (N2 times per week) of curcumin containing foods, regular NSAID use (at least 3 of 7 days), intake of a curcumin supplement (within the past 6 months), and any other condition that would prohibit completion of the lower body resistance exercise protocol" |
| Methods | Randomised controlled trial (balanced randomised cross‐over design) 30 day washout | |
| Participants | Setting: laboratory; New Zealand n = 10 healthy active females mean age 22 (SD 1) years Inclusion/exclusion criteria All participants were physically active and participated in this study. All participants were physically active and participated in recreational level resistance and aerobic‐based exercise at least twice per week. All participants had at least 1 years' experience in training in this manner. Participants completed a Health Screening Questionnaire to exclude those who were at risk physically, culturally or religiously in following the protocol. Those who passed the questionnaire were asked to provide written consent. | |
| Interventions | Intervention Blueberry smoothie 200 g blueberries 50 g banana + 200 mL apple juice. Per 100 mL, total phenolics 168 mg/gallic acid equ.; anthocyanins 96.6 mg; phenolic acid 26 mg, flavonoids 10.2 mg; vitamin C 45 mg; vitamin E 3 mg Placebo Smoothie 25 g dextrose 50 g banana + 200 mL apple juice Duration 4 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness was recorded using a subjective 10‐point scale where 0 is "no soreness" and 10 is "very, very painful." Participants were asked to step up (concentric muscle action) onto a 40 cm box then step down (eccentric muscular contraction) and the soreness was rated. SECONDARY Muscle function was tested using an isokinetic dynamometer (Biodex Medical Systems Inc. 2004). Range of motion of the leg was set at 60 degrees for concentric and eccentric contractions and at 75 degrees for isometric contractions. The participants performed 5 maximal contractions of each type with each set separated by 2 minutes of recovery. Concentric and eccentric torque was measured at an angular velocity of 30 degrees per second. | |
| Exercise type | 3 sets of 100 eccentric repetitions of the quadriceps | |
| Sources of funding | Funded by an Institute of Food, Nutrition and Human Health Postgraduate Research Award, and the New Zealand Ministry of Science and Innovation, contract C06X0807 awarded to Plant and Food research Ltd. | |
| Notes | Drinks consumed on day of exercise the again at 12 hours and 36 hours post‐exercise | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Author response: "A table with vertically numbered cells 1‐10 had either ‘blueberries’ or ‘no blueberries’ (4 of each) next to them. Names were then simply pulled from a hat and typed into these cells in drawn order. A simple method, yet allowed for randomised allocation of treatment." |
| Allocation concealment (selection bias) | High risk | No details in manuscript Authors were contacted on 27 May 2016 via email Author response: "Due to the form the treatment was given as (smoothie), we were unable to blind the study. Both control and blueberry smoothies were isocaloric however. The study was a cross‐over design and both treatment and leg of damage was randomised." Adequate safeguards not reported for the first phase; the second phase was predictable |
| Blinding of participants and personnel (performance bias) | High risk | Not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Probably not blinded |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study with no adverse effects |
| Selective reporting (reporting bias) | Low risk | No published protocol available All outcomes reported at all time points Manuscript states: "there were no reported adverse effects from the dietary intervention" |
| Other bias | Unclear risk | Participants were asked to complete a food diary but no detail on whether participants were asked to refrain from using anti‐inflammatory drugs or other supplements that could reduce soreness |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory, Iran n = 20 male non‐athletic university students mean age 18.2 (SD 0.4) years Inclusion/exclusion criteria Participants were selected based on fitness and health screening tests and recruited in a double‐blind trial. Participants with history of any type of muscle injury, chronic inflammation, coagulation disorders, immune system impairment and cardiovascular problems were excluded. Participants were also excluded if they regularly participated in vigorous exercise in the previous 3 months. | |
| Interventions | Intervention Purslane extract 1200 mg given as 2 x 600 mg capsules per day Placebo Lactose powder placebo capsules Duration 5 days | |
| Outcomes | PRIMARY A general rating of muscle soreness was assessed using a 0‐ to 6‐point scale where 0 corresponded to "no pain" and 6 to "unbearably painful". Participants were requested to rate the discomfort in only the quadriceps and calf regions of the right leg. SECONDARY Knee range of motion ‐ participants laid prone on an examination table with both knees fully extended. The knee joint angle was determined by using a goniometer and universal landmarks to ensure alignment. Knee flexion range was determined when the participant maximally and voluntary flexed the knee. Maximal knee extension isometric force was evaluated using a computerised dynamometer attached to an adjustable steel chain. Participant was seated on a special chair with knee flexed at an angle of 90 degrees then the ankle was fixed by a special belt connected to a force transducer. During a 5‐second test, force‐time data were recorded on a memory card. | |
| Exercise type | 7 sets of 5 minutes of continuous bench stepping exercise with 1 minute rest; 50 cm bench height | |
| Sources of funding | Financial support was received from the university postgraduate grant (no 11‐4‐899). University of Mohaghegh Ardabil, Iran | |
| Notes | 2 capsules daily | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | No details in the manuscript Authors were contacted by email on 25 May 2016 Response: "two groups had selection criteria's and randomly selected by online program from a bigger group of volunteers" |
| Allocation concealment (selection bias) | Low risk | No details in the manuscript Authors were contacted by email on 25 May 2016 Response: "placebo and purslane were capsulated" |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using any supplements and anti‐inflammatory drugs or other treatment that could reduce soreness. Diet not controlled. |
| Methods | Randomised, double‐blind (cross‐over design) 6 weeks washout period | |
| Participants | Setting: laboratory, Greece n = 10 male recreationally active Mean age 23.5 (SD 2.5) years Inclusion/exclusion criteria Participants were recreationally trained, as evidenced by their maximal oxygen consumption (O2max) level (> 45 mL · kg−1 · min−1); had been engaged in systematic exercise ≥ 3 times/week for ≥ 12 months, and were non‐smokers. Participants abstained from any vigorous physical activity and the consumption of caffeine, alcohol or performance‐enhancing or antioxidant supplements and medications before (6 months) and during the exercise trials. Exclusion criteria included a known NAC intolerance or allergy, a recent febrile illness and history of muscle lesion and lower limb trauma. | |
| Interventions | Intervention 20 mg NAC/kg per day was administered orally (Uni‐Pharma) in 3 daily dosages. NAC was dissolved in a 500 mL drink that contained water (375 mL), a sugar‐free cordial (125 mL) and a 2 g low‐calorie glucose/dextrose powder to improve palatability Placebo Placebo solution was formulated to be identical to the NAC solution, except for the NAC content Duration Supplement consumed immediately after muscle‐damaging exercise and for 8 days post‐exercise | |
| Outcomes | PRIMARY Delayed onset of muscle soreness (delayed onset muscle soreness) was determined by palpation of the muscle belly and the distal region of the vastus medialis, vastus lateralis and rectus femoris after a squat. Perceived soreness was rated on a scale ranging from 1 (normal) to 10 (very, very sore). SECONDARY Maximal knee extensor eccentric peak torque at 60°/second on an isokinetic dynamometer (Isoforce) | |
| Exercise type | 300 eccentric unilateral repetitions (20 sets, 15 repetitions/set, 30‐second rest between sets) with the quadriceps muscle group at a speed of 30°/second on an Isoforce (TUR Gmbh) isokinetic dynamometer | |
| Sources of funding | Manuscript states: "Supported by departmental funding, a grant received by Bodosakis Foundation (Greece) for instrument purchase, and grant funding (CE‐80739). APR was supported by a National Health and Medical Research Council Career Development Award, Australia." | |
| Notes | Authors were contacted on 7 February 2017 to request data for delayed onset muscle soreness and maximal voluntary isometric contraction but did not respond | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details in manuscript Authors were contacted on 7 February 2017 but did not respond |
| Allocation concealment (selection bias) | Unclear risk | No details in manuscript Authors were contacted on 7 February 2017 but did not respond |
| Blinding of participants and personnel (performance bias) | Low risk | Manuscript states the design was double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | High risk | Protocol states 20 individuals were enrolled and 12 completed. Manuscript states that 10 males completed the study. |
| Selective reporting (reporting bias) | Low risk | Published protocol available (ClinicalTrials.gov identifier: NCT01778309) All data reported at all time points Manuscript states: "Participants reported no adverse side effects attributed to NAC consumption" |
| Other bias | Unclear risk | 5‐day diet recalls (1 recall/day) were completed before each trial and standardised between trials |
| Methods | Randomised controlled trial (cross‐over design) 14‐day washout | |
| Participants | Setting: laboratory; Australia n = 17 healthy men aged between 18 and 39 years 2 withdrew from the study following acceptance due to the inability to attend testing commitments Inclusion/exclusion criteria Participants were undertaking light to moderate regular physical activity including sports training but not doing lower limb resisted exercise | |
| Interventions | Intervention 2.5 g of curcumin Placebo 2.5 g Avicel 105, an inert plant cellulose 5 capsules taken twice daily Duration 5 capsules were taken twice daily for 2.5 days prior to exercise, then 5 capsules twice daily for 2.5 days after exercise | |
| Outcomes | Primary Muscle soreness using a 0 to 10 cm visual analogue scale where 0 is "no pain" and 10 is "severe pain". Pain was rated for a single leg squat, walking downstairs, passive strength of the gluteals and a single leg vertical jump. Muscle tenderness was assessed using a Somedic pressure algometer (Somedic, Sollentuna, Sweden) at 4 standardised points Secondary Jump performance was measured by a single leg vertical squat jump. The jump and reach method using Vertec (Vertec, Vertec Sports Imports, Hilliard, OH). | |
| Exercise type | Eccentric exercise protocol consisted of 7 sets of 1‐ eccentric single leg press repetitions on a leg press machine | |
| Sources of funding | Manuscript states: "Funding from the Australian Institute of Sport" | |
| Notes | Authors were contacted on 15 March 2016 to request raw data for delayed onset muscle soreness and counter‐movement jump and they responded on 15 March 2016 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Manuscript states that the "randomization sequence was generated using a random numbers table (http://www.ramdomizer.org)". Secondly: "Randomization was applied to both the order of treatment or placebo and to the sequence of right or left leg use within the unilateral crossover". It is known that the repeated bout effects can be observed in the non‐exercised limb. |
| Allocation concealment (selection bias) | Low risk | Manuscript states: "Allocation was concealed using sequentially numbered medication. Investigators and participants were blinded by provision of the medications by AIS nursing staff according to the randomization protocol." |
| Blinding of participants and personnel (performance bias) | Low risk | Manuscript states: "Investigators and participants were blinded by provision of the medications by AIS nursing staff according to the randomization protocol" and that "the participants reported that they could not distinguish between the treatment and placebo" |
| Blinding of outcome assessment (detection bias) | Low risk | Participants were blinded |
| Incomplete outcome data (attrition bias) | Low risk | Manuscript states" "Two withdrew from the study following acceptance due to the inability to attend testing commitments, and no replacements were added due to resource constraints." This equates to 11% attrition. |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | No information in the manuscript regarding food or using anti‐inflammatory drugs or other supplements during the trial |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; China n = 16 male junior basketball players (8 in each group) Mean age vitamin C group 16.7 (SD 0.3) years Mean age placebo group 16.5 (SD 0.2) years Inclusion/exclusion criteria Participants completed 4 to 5 training sessions a week with an average weekly training of 12.3 (SD 1.3) hours | |
| Interventions | Intervention 800 mg of vitamin C Placebo No details provided other than it was identical in appearance Duration Vitamin C taken 3 hours before exercise and 31 hours after exercise and outcomes measured for up to 2 days post‐exercise | |
| Outcomes | PRIMARY Delayed onset muscle soreness was evaluated in the leg extensors using a 10 cm visual analogue scale where 0 is "complete absence of pain" and 10 is "extremely sore with noticeable pain and stiffness at all times and the muscle and leg are difficult to use". Perceived soreness was done during quadriceps extension. | |
| Exercise type | 10 sets of 15 full‐squat jumps with 10 kg weight imposed at the waist | |
| Sources of funding | None | |
| Notes | No detail on how the supplements were administered or whether it was a drink or capsule | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details in manuscript Authors were contacted via email on 26 May 2016 and responded on 27 May 2016: "distribute subjects by lot" |
| Allocation concealment (selection bias) | Unclear risk | No details in manuscript Authors were contacted via email on 26 May 2016 and responded on 27 May 2016 but did not understand the query |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | No details in manuscript Authors were contacted via email on 26 May 2016 and responded to say that all participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | Diet was controlled 2 days before testing, however no details were provided on whether participants were instructed to avoid other supplements or anti‐inflammatory drugs during the study |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 40 untrained men (20) and women (20); age range 18 to 39 Placebo group (n = 20; 10 women) Antioxidant group (n = 2; 9 women) Inclusion/exclusion criteria Excluded were pregnant women, individuals engaged in vigorous activities on a regular basis (more than once per week on average during the prior month), those with contraindications to exercise, those taking pain or prescription drugs (except for oral contraceptives), and high consumers of 55 fruits, vegetables, drinks or chocolate products known to contain polyphenols (> 1 serving per day during the prior month) | |
| Interventions | Intervention Grape beverage ‐ stilbenes (resveratrol = 1.75 mg/kg), catechins (catechin = 19.7 mg/kg, epicatechin = 12.6 mg/kg), anthocyanins (peonidin = 31.7 mg/kg, cyanidin = 125 mg/kg, malvidin = 145.2 mg/kg) and flavanols (quercetin = 32.6 mg/kg, kaempferol = 5.6 mg/kg, isorhamnetin = 6.8 mg/kg) Placebo A combination of starch, sugars, cellulose, acids, dipotassium phosphate, potassium citrate, grape flavouring and food dyes was used to create a placebo powder that matched the composition and caloric content of the grape powder as closely as possible but without any polyphenolic compounds Duration 45 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness in the arm was rated in response to isometric strength measurement trials using a 100 mm visual analogue scale where 0 is "no pain" and 100 is "extreme pain" SECONDARY Range of motion Isometric strength of the elbow flexors at 90 degrees Maximal oxygen consumption performed on a treadmill | |
| Exercise type | 3 sets of 6 repetitions were performed using the non‐dominant elbow flexors with a weight of 120% of concentric 1 RM | |
| Sources of funding | Financial support for the study was provided by the California table Grape Commission | |
| Notes | One serving of powder daily mixed with 236 mL of water | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | One investigator generated an allocation sequence using an online random number generator that created blocks of 2 with an allocation ratio of 1:1 to the conditions. A different investigator randomly assigned participants in blocks to their groups. |
| Allocation concealment (selection bias) | Low risk | Opaque containers and a clip was placed on the nose |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind: participants as well as researchers administering the intervention, assessing the outcomes and conducting the statistical analyses were blinded |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study with no adverse effects |
| Selective reporting (reporting bias) | Low risk | No published protocol available All outcomes reported at all time points Manuscript states: "No adverse events occurred in response to beverage consumption" |
| Other bias | Low risk | Participants were asked to record food frequency and were asked to refrain from using anti‐inflammatory drugs or other supplements that could reduce soreness |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory, USA n = 30 sedentary adults (15 men and 15 women), age range 18 to 25 years Mean age placebo group men (n = 8) 19.5 (SD 1.1) years, mean age placebo group women (n = 7) 19.6 (SD 1.3) years Mean age supplement group men (n = 7) 20.9 (SD 1.8) years, mean age placebo group women (n = 8) 20.6 (SD 1.1) years Inclusion/exclusion criteria Participants were sedentary to recreationally active, naive to resistance training and resistance‐type activities of the upper extremities for 6 months before participation, negative (by self‐report) for family history of and current musculoskeletal or metabolic impairments, and not taking any dietary supplements | |
| Interventions | Intervention First Strike Nutrition (Natick Soldier Centre, Natick MA) Bars with 1000 mg of Quercitin (Merck, SA Brazil) Placebo Placebo First Strike Nutrition Bar (Natick Soldier Centre, Natick MA) Duration 7 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness was assessed using a 100 mm visual analogue scale where 0 is "no soreness" and 100 is "unbearable pain" Elbow flexor SECONDARY Resting arm angle Upper arm swelling Isometric peak torque | |
| Exercise type | 24 eccentric contractions of the elbow flexors | |
| Sources of funding | Funded by the US Army contract # W911QY‐07‐C‐0001 | |
| Notes | 1 bar twice daily for 7 days Authors were contacted to request raw data for delayed onset muscle soreness, range of motion and maximal voluntary isometric contraction on 3 November 2013 and responded on 3 December 2013 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomly assigned in a permuted block design |
| Allocation concealment (selection bias) | Unclear risk | No details in the manuscript Authors were contacted but no reply received |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study without any adverse effects |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Food records were obtained, participants were instructed to minimise foods high in quercetin and were asked to refrain from taking any other supplements, anti‐inflammatory medication or engage in any other modality that could enhance recovery |
| Methods | Randomised controlled trial (cross‐over design) Separated by a 21‐day washout | |
| Participants | Setting: laboratory, USA n = 8 well‐trained male runners and triathletes age range 18 to 44 years Inclusion/exclusion criteria Inclusion criteria ‐ currently training for at least 6 or more hours per week Exclusion criteria ‐ lower body extremity injury in the past 6 months and/or were currently taking chronic or daily doses of anti‐inflammatory medication or nutritional supplements. Participants who had a history of a recent illness were also excluded from the study. | |
| Interventions | Intervention 240 mL serving of carbohydrate protein beverage plus natural cocoa (350 mg flavanols) Placebo Placebo cocoa‐based (processed with alkali) carbohydrate protein beverage (0 mg of flavanols) Duration Beverage consumed 1 and 2 hours into recovery after downhill running and primary and secondary outcomes measured for up to 2 days after exercise | |
| Outcomes | PRIMARY Delayed onset muscle soreness at the legs (10‐point visual analogue scale: 0 is "no pain at all" and 10 is "unbearable pain") SECONDARY Muscle tenderness using a force algometer (Wagner Pain Test Model FPK Algometer) Muscle function ‐ Quadricep Extension Performance ‐ 5 km running time trial | |
| Exercise type | Downhill running protocol at a ‐10% grade for 30 minutes at a speed equal to 70% of VO2 max | |
| Sources of funding | Chocolate milk was provided by Darigold Co. | |
| Notes | Drinks were 240 mL per serving and consumed 1 hour post‐exercise and 2 hours post‐exercise. Authors were contacted on 18 February 2016 to request data for delayed onset muscle soreness, maximal voluntary isometric contraction and 5 km time trial but did not respond | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised using a computer program |
| Allocation concealment (selection bias) | Low risk | Unmarked bottles |
| Blinding of participants and personnel (performance bias) | High risk | Single‐blind design thus personnel were not blinded |
| Blinding of outcome assessment (detection bias) | Low risk | Participants were blinded |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study without any adverse effects |
| Selective reporting (reporting bias) | High risk | All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were instructed to consume a similar diet during the period of testing and replicate diet during both trials. Participants were instructed to refrain from taking anti‐inflammatory medication. |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; USA n = 40 healthy, untrained, non‐smoking males who were regularly involved with weight training mean; age 22.1 (SEM 3.9) years (16 in the antioxidant group and 19 in the placebo group) Inclusion/exclusion criteria During the screening process an extensive interview to clarify the extent and nature of each individual's exercise habits was conducted, specifically to ascertain whether or not a regular weight‐training programme was a component thereof. Those participants not involved with a regular weight‐training programme and with no prior history of injury to the biceps brachii or elbow region were included in the study. | |
| Interventions | Intervention Mixed antioxidant supplement (300 mg tocopherols, 800 mg docosahexaenoate, 300 mg flavonoids, of which was 100 mg hesperetin and 200 mg quercetin) Placebo Sunflower oil and rice powder capsules Duration 2 weeks of supplementation | |
| Outcomes | PRIMARY Muscle soreness was measured using a visual analogue scale (0 to 10 cm) where 0 is "no pain" and 10 is "extreme pain". Soreness measures were subjectively evaluated through palpitation for oedema at the elbow and were performed by the same researcher throughout the study. SECONDARY Range of motion was measured as active arm flexion from full extension using standard goniometry. Each range of motion value was obtained from an average of 3 measurements. | |
| Exercise type | 3 sets of 10 repetitions at 80% of 1 RM of elbow flexor | |
| Sources of funding | This research was supported with funding from Galileo Laboratories, Inc. | |
| Notes | Supplements were taken in the form of capsules (number of capsules per day not specified) Authors were contacted via email on 2 November 2013 and again on 3 December 2013 to request data for delayed onset muscle soreness and maximal voluntary isometric contraction but they did not respond | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised; however, no details in the manuscript on how this was done Authors were contacted via email on 2 November 2013 and again on 3 December 2013 with no reply |
| Allocation concealment (selection bias) | Unclear risk | No details in the manuscript Authors were contacted via email on 2 November 2013 and again on 3 December 2013 with no reply |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | High risk | 5 participants were excluded from the study due to complications with the blood‐drawing procedures, however it is unclear which group they were from Attrition rate = 12.5% |
| Selective reporting (reporting bias) | Low risk | No published protocol available All outcomes reported at all time points Manuscript states: "During the period of supplementation, there were no reported adverse events by any of the research subjects..." |
| Other bias | Low risk | Participants were asked to refrain from using any other supplements and medication for the duration of the study |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; Ireland n = 12 moderately fit, active, non‐smoking men Mean age vitamin C group 25 (SD 7.5) years Mean age placebo group 20.6 (SD 1.1) years Inclusion/exclusion criteria All volunteers were moderately active non‐smokers who had not participated in any form of resistance training exercise in the previous 6 months. Volunteers who were currently taking supplements in the past 6 months were excluded from the study. | |
| Interventions | Intervention 500 mg vitamin C and 1200 IU vitamin E; 2 x 250 mg tablets of vitamin C + 3 tablets 400 IU each vitamin E Placebo Glucose Duration 37 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness was evaluated using a questionnaire employing a visual analogue scale for a total of 8 sites (6 sites on the anterior muscle of the upper leg and 2 sites on the posterior muscles of the upper leg). The participants were asked to palpate the relaxed muscle and rate soreness on a scale of 1 "normal" to 10 "very very sore". Results were summed for the 8 sites so that no soreness is indicated by a score of 8 and maximal muscle soreness by a score of 80. SECONDARY Maximal voluntary concentric torque for the knee extensors was measured at an angular velocity of 0.5 rad/s 3 minutes to and 3 minutes following the eccentric contraction bout on the Con‐Trex dynamometer. Isometric maximum voluntary contraction force (MVC) and electrically simulated force of the knee extensors were measured using a custom made isometric test rig. Volunteers were seated in the upright position with their leg connected to a pre‐calibrated load cell (Novatech, Hastings, UK). Analogue signals from the strain gauge were converted to digital information using an A:D convertor (Powerlab 1400, ADInstruments, Oxfordshire, UK) and were recorded on a PC. The chair was adjusted to allow attachment of the strain gauge above the ankle with the knee at an angle of 1.57 rad (90 degrees). For MVC, volunteers were instructed to contract maximally for 3 seconds and verbally encouraged during their effort. 3 repetitions were performed, separated by 1 minute. The highest peak force value of the 3 repetitions was recorded as the MVC. | |
| Exercise type | 30 sets of 10 eccentric knee extensions at a velocity of 0.52 rad·s‐1 | |
| Sources of funding | None | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | No details in manuscript Authors were contacted via email on 26 May 2016 and responded on 5 June 2016: "Numbers were drawn out of a hat to determine a set allocation order which was balanced in numbers for treatment and placebo. As participants were recruited to the study, they were allocated to a group according to that random allocation order." |
| Allocation concealment (selection bias) | Unclear risk | No details in manuscript Authors were contacted via email on 26 May 2016 and responded on 5 June 2016: "All volunteers were informed that they were being supplemented. All were supplied with identical labelled dispensers, containing capsules. However, the capsules were not identical in colour or size. We checked, informally, at the end of the testing to see if volunteers thought they were supplemented or controlled and they really had no idea which was which" |
| Blinding of participants and personnel (performance bias) | High risk | Non‐identical capsules; the personnel were not blinded |
| Blinding of outcome assessment (detection bias) | Unclear risk | Non‐identical capsules; some risk of unblinding |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | Participants that took supplements or smoked were excluded No details on whether participants were asked to refrain from using anti‐inflammatory drugs or other treatment modalities that could reduce soreness |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; Brazil n = 29 healthy, male university students mean age 21.3 (SD 4) years Inclusion/exclusion criteria Participants were non‐smokers, did not take NAC or related supplements, had not participated in resistance training or any other form of structured exercise for at least 6 months, did not have a history of muscle lesion, and were not carriers of any disease that might compromise the results or be aggravated by physical exercise | |
| Interventions | Intervention N‐acetylcysteine (NAC) 10 mg/kg of body mass in 3 groups as follows: Group 1: 21 days of N‐acetylcysteine (NAC) 10 mg/kg of body mass n = 8 Group 2: 14 days of N‐acetylcysteine (NAC) 10 mg/kg of body mass + placebo (14 days of NAC + 7 days of placebo) n = 8 Group 3: 21 days of placebo n = 9 Placebo Starch capsules Duration 21 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness at the elbow flexor using a visual analogue scale (0 to 10 cm). Participants marked their subjective rating from 0 "without pain" to 10 "extreme pain" | |
| Exercise type | Elbow flexion and extension on the Scott bench at 80% 1 RM until exhaustion | |
| Sources of funding | The study was supported by grants from UNESC, CNPq and CAPES (Brazil) | |
| Notes | 1 capsule per day for 14 days before the exercise protocol | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | No details in the manuscript Author response: "We selected the individual using a random number table. The participants were selected and they received a number. According with the random number tables all individuals were included in the experimental or control groups." |
| Allocation concealment (selection bias) | Low risk | No details in the manuscript Authors were contacted via email on 24 May 2016 Author response: "Allocation concealment was ensured by the use of sequentially numbered, dark and sealed envelopes. An independent colleague, blinded to the allocated treatment, did the selection and carried out the composition of groups." |
| Blinding of participants and personnel (performance bias) | High risk | Single‐blind; participants were blinded but the researchers were not |
| Blinding of outcome assessment (detection bias) | Low risk | Participants were blinded |
| Incomplete outcome data (attrition bias) | High risk | 4 participants withdrew for personal reasons Attrition rate: 14% |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | Participants were non‐smokers, did not take any other supplements and had not participated in resistance training or any form of structured exercise for 6 months No details on whether the participants used anti‐inflammatory drugs for the duration of the study |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; Brazil n = 27 male university students mean age 25.5 (SD 4) years Inclusion/exclusion criteria All participants were non‐smokers, were not taking vitamin E or any other antioxidant or related supplements, had not participated in resistance training or any other form of structured exercise for at least 6 months, did not have a history of muscular lesions, and were not carriers of any disease that might compromise the results or be aggravated by physical exercise | |
| Interventions | Intervention 800 IU per day of D‐a‐tocopherol acetate (vitamin E); 1 capsule per day Placebo Starch capsules Duration 14 days before and 7 days after (total 21 days) | |
| Outcomes | PRIMARY Muscle soreness of the biceps muscle was assessed using a 10 cm visual analogue scale where 0 is "no muscular soreness" and 10 is "maximum muscular soreness" | |
| Exercise type | Elbow flexion and extension on the Scott bench at an intensity of 80% of 1 RM; 3 sets to exhaustion with 2 minutes recovery | |
| Sources of funding | The research was supported by grants from CNPq/MCT (Brazil), CAPES/MEC (Brazil) and USESC (Brazil) | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | No details in manuscript Authors were contacted on 26 May 2016 via email Author response: "We selected the individual using a random number table. The participants were selected and they received a number. According with the random number tables all individuals were included in the experimental or control groups." |
| Allocation concealment (selection bias) | Low risk | No details in manuscript Authors were contacted on 26 May 2016 via email Author response: "Allocation concealment was ensured by the use of sequentially numbered, dark and sealed envelopes. An independent colleague, blinded to the allocated treatment, did the selection and carried out the composition of groups." |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | High risk | 6 participants withdrew from the study for personal reasons Attrition rate: 22% |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | No data on food records reported Participants were instructed to refrain from taking supplements for the duration of the study but no details on anti‐inflammatory medication |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; China n = 16 athletes aged 18 to 20 years (8 males and 8 females) Mean age 18.9 (SD 0.8) years Inclusion/exclusion criteria A medical exam, including measurement of height, weight, blood pressure and electrocardiogram was performed for each participant before the start of the study. No participants had infectious diseases or were currently taking anti‐inflammatory and anti‐fatigue medicine during the study period. | |
| Interventions | Intervention 80 mg of allicin supplementation Placebo 80 mg maltodextrin Duration 2 weeks before and 2 days after running | |
| Outcomes | PRIMARY Muscle soreness was assessed using the Borg CR‐10 Scale where 0 is "no pain" and 10 is "maximal pain". At the beginning of the exercise test, participants were instructed to give CR‐10 values. | |
| Exercise type | Downhill running on a treadmill at a grade of ‐10% | |
| Sources of funding | No information in the manuscript Authors were contacted on 2 November 2013 and 3 December 2013 via email with no response | |
| Notes | Supplements taken as capsules daily Authors were contacted on 2 November 2013 and 3 December 2013 via email to request data for delayed onset muscle soreness with no response | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Participants were randomly assigned into an allicin or control group by sex and sports participation |
| Allocation concealment (selection bias) | Unclear risk | Not specified in the manuscript Authors were contacted on 2 November 2013 and 3 December 2013 via email with no response |
| Blinding of participants and personnel (performance bias) | Unclear risk | Not specified in the manuscript Authors were contacted on 2 November 2013 and 3 December 2013 via email with no response |
| Blinding of outcome assessment (detection bias) | Unclear risk | No details provided |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to maintain their normal dietary habits and avoid any form of antioxidant supplementation |
| Methods | Randomised controlled trial (cross‐over design) 4‐week washout period | |
| Participants | Setting: laboratory; Japan n = 14 untrained young men mean age 23.5 (SD 2.4) years Inclusion/exclusion criteria Participants had not been involved in any regular resistance exercise training for the past year | |
| Interventions | Intervention 150 mg of curcumin in 6 capsules of 25 mg each Placebo 150 mg of starch in 6 capsules of 25 mg each Duration 1 hour before exercise and 12 hours after exercise separated by a 4‐week washout | |
| Outcomes | Primary Muscle soreness was measured using a 100 mm visual analogue scale where 0 is "no pain" and 100 is "extremely sore." Soreness was measured upon palpitation of the upper arm and passively extending the elbow joint. Secondary Range of motion was measured by actively extending the elbow joint maximally (extended elbow joint) and touching the shoulder of the same side with the hand (flexed elbow joint angle). The range of motion was defined by the difference between the 2 elbow joints. Each angle was measured by a goniometer 3 times and the mean of the 3 measures was used. Maximum voluntary contraction of the exercised elbow flexors was measured using the isokinetic dynamometer in the same positioning as the eccentric exercise and the elbow joint angle was set at 90 degrees. 3 maximal isometric contractions were performed with a 30‐second rest. | |
| Exercise type | 2 bouts of eccentric exercise of the elbow flexors on a Biodex dynamometer (Biodex System 3, USA) using 1 arm for each bout separated by 4 weeks. Each exercise bout consisted of 50 maximal eccentric contractions of the elbow flexors at a velocity of 120 degrees per second. | |
| Sources of funding | The study was supported by Theravalues Corporation, Japan | |
| Notes | Authors were contacted to request raw data for delayed onset muscle soreness, range of motion and maximal voluntary isometric contraction on 8 December 2017 and responded on 9 December 2017 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Manuscript states: "randomised, single‐blinded" design was used; no additional details in the manuscript Authors were contacted via email on 5 February 2017 and responded on 8 February 2017: "One investigator (YT) assigned and managed the order of dominant‐nondominant and active‐placebo to be counterbalanced as described in manuscript." |
| Allocation concealment (selection bias) | Unclear risk | No details in manuscript Authors were contacted via email on 5 February 2017 and responded on 8 February 2017: "The subjects were allocated before the authors got any subject information (e.g., height, weight, day of birth etc)." |
| Blinding of participants and personnel (performance bias) | High risk | The study was a single‐blinded design |
| Blinding of outcome assessment (detection bias) | Unclear risk | No details provided |
| Incomplete outcome data (attrition bias) | Low risk | Authors were contacted via email on 5 February 2017 and responded on 8 February 2017: "all participants completed the study" |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Manuscript states: "Subjects maintained their normal food intake and lifestyle habits, but abstained from strenuous physical activities, and did not take anti‐inflammatory drugs during the study period." |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; Greece n = 28 healthy, recreationally trained men Mean age placebo group 25.6 (SEM 1.2) Mean age vitamin C group 26.2 (SEM 1.5) Inclusion/exclusion criteria Men were recruited after advertising the study in the local media | |
| Interventions | Intervention 1g of vitamin C and 400 IU vitamin E Placebo Lactose Duration 11 weeks | |
| Outcomes | PRIMARY Delayed onset muscle soreness was assessed using a squat using body weight with a 0 to 10 scale where 0 is "normal" and 10 is "very sore" SECONDARY Range of motion Isometric peak torque using an isokinetic dynamometer. Isometric knee extensor peak torque at 90 degrees knee flexion was measured. The average of the 3 best maximal voluntary contractions with the dominant leg was recorded. | |
| Exercise type | Knee extensions on an isokinetic dynamometer | |
| Sources of funding | None: the authors had no personal or financial conflicts of interest | |
| Notes | 1 capsule per day | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Participants were allocated based on age, BMI and maximum isometric torque into equal groups then a computer generator was used for the assignment into groups |
| Allocation concealment (selection bias) | Low risk | No details in manuscript Authors were emailed in 25 May 2016 via email to request this information Author response: "We used an independent person and a sealed opaque envelope for the allocation concealment." |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | Unclear risk | Study protocol published (ClinicalTrials.gov: NCT01290458) All the outcomes published in the study protocol were measured in the actual study All outcomes reported at all time points However, adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | Participants were asked to keep food records for 3 days before testing, however no details on whether participants were asked to refrain from using other supplements and anti‐inflammatory medication |
| Methods | Randomised controlled trial (cross‐over design) Separated by 14‐day washout | |
| Participants | Setting: laboratory, UK n = 9 male, habitually active, male university students Mean age 28.4 (SEM 1.3) years Inclusion/exclusion criteria Participants who smoked or took vitamin supplements were excluded from the study | |
| Interventions | Intervention 1 g of vitamin C 2 hours before exercise Placebo Carbohydrate sports drink Duration Supplement consumed on day of test 2 hours before exercise with a 14‐day washout | |
| Outcomes | PRIMARY Delayed onset muscle soreness at the quadriceps using a 10‐point (1 to 10 cm) visual analogue scale where 0 is "not sore" and 10 is "very very sore" SECONDARY Isometric flexion and extension | |
| Exercise type | Loughborough Intermittent Shuttle Running Test ‐ 90 minutes variable intensity running over 20 m distance | |
| Sources of funding | The authors acknowledged the financial support of SmithKline Beecham | |
| Notes | Supplements were ingested in a drink | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Details not in the manuscript therefore authors were contacted (19 May 2016) "A third party independent from the investigators generated a randomisation plan and held the sequence for allocation" |
| Allocation concealment (selection bias) | Unclear risk | Not reported in manuscript therefore authors were contacted (19 May 2016) No response received |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants complete the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | Vitamin C intake through diet was screened through weighed food records No detail on whether participants were asked to refrain from using supplements or anti‐inflammatory medication |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; UK n = 16 physically active males (8 in the placebo group and 8 in the vitamin C group) Mean age vitamin C group 25 (SEM 2) years Mean age placebo group 23 (SEM 2) years Inclusion/exclusion criteria Participants who had smoked or took vitamin supplements were excluded from the study. All participants regularly took part in a variety of activities but were unfamiliar with the exercise protocol. | |
| Interventions | Intervention Vitamin C supplementation; 1 g of vitamin C on day 1 followed by 400 mg/day divided into 2 doses for 12 days Placebo Lactose capsules Duration 13 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness at the quadriceps using a 10‐point (0 to 10 cm) visual analogue scale where 0 is "not sore" and 10 is "very very sore" SECONDARY Isometric quadriceps muscle contraction. Muscle function was assessed in the flexors and extensors of both legs on an isokinetic dynamometer (CYBEX model 770, LUMEX, USA). | |
| Exercise type | Loughborough Intermittent Shuttle Running Test ‐ 90 minutes variable intensity running over 20 m distance | |
| Sources of funding | The study was financially supported by SmithKline Beecham UK | |
| Notes | 1 g given in a solution followed by 400 mg/day doses in capsule form | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Details not in the manuscript therefore authors were contacted (19 May 2016) "A third party independent from the investigators generated a randomisation plan and held the sequence for allocation" |
| Allocation concealment (selection bias) | Unclear risk | Not reported in the manuscript therefore authors were contacted (19 May 2016) No response received |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All the participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants who smoked or took vitamin supplements were excluded. No detail on whether participants kept food records or were instructed to refrain from taking supplements for the duration of the study and no details on avoiding anti‐inflammatory medication |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; UK n = 16 male university students (8 participants in each group) Mean age vitamin C group 23.6 (± SEM 1.4) years Mean age placebo group 24.3 (± SEM 1.7) years Inclusion/exclusion criteria Participants who smoked or took vitamin supplements were excluded from the investigation. All participants were habitually active in a variety of sports, although none were familiar with the exercise protocol used in the present study. | |
| Interventions | Intervention 200 mg vitamin C Placebo Carbohydrate sports drink Duration 3 days | |
| Outcomes | PRIMARY Delayed onset muscle soreness was rated on a 10‐point scale ranging from 1 "not sore" to 10 "very very sore." Soreness was assessed whilst the participants actively contracted the quadriceps SECONDARY Isometric quadriceps muscle contraction. Muscle function was assessed in the flexors and extensors of both legs on an isokinetic dynamometer (CYBEX model 770, LUMEX, USA). | |
| Exercise type | Loughborough Intermittent Shuttle Running Test ‐ 90 minutes variable intensity running over 20 m distance | |
| Sources of funding | The authors acknowledged the financial support of SmithKline Beecham, UK | |
| Notes | Supplements were ingested in a drink daily | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Details not in the manuscript therefore authors were contacted (19 May 2016) "A third party independent from the investigators generated a randomisation plan and held the sequence for allocation" |
| Allocation concealment (selection bias) | Unclear risk | Not reported in the manuscript therefore authors were contacted (19 May 2016). No response received |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All the participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol Data not reported for all outcomes Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to record food frequency and to refrain from using anti‐inflammatory drugs or other supplements that could reduce soreness |
| Methods | Randomised controlled trial (parallel design) | |
| Participants | Setting: laboratory; UK n = 14 male university students Mean age vitamin C group 25.3 (SEM 1.4) years Mean age placebo group 22.6 (SEM 1.7) years Inclusion/exclusion criteria Participants who smoked or took vitamin supplements were excluded from the study. All participants regularly took part in a variety of activities but were unfamiliar with the exercise protocol used in the study. | |
| Interventions | Intervention 200 mg vitamin C Placebo 200 mg lactose Duration 14 days | |
| Outcomes | PRIMARY Muscle soreness was assessed in the quadriceps using a 0 to 100 mm scale where 0 is "normal" and 100 is "very very sore". In order to activate the sensation of soreness, participants assessed soreness whilst actively contracting the leg extensors against resistance equivalent to 75% of each individual's one repetition maximum. | |
| Exercise type | 30 minutes downhill running at ‐18% gradient | |
| Sources of funding | None | |
| Notes | No details on how many capsules were consumed per day Authors were contacted to request raw data for delayed onset muscle soreness on 3 November 2013 and responded on 4 November 2013 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Details not in the manuscript therefore authors were contacted (19 May 2016) "A third party independent from the investigators generated a randomisation plan and held the sequence for allocation" |
| Allocation concealment (selection bias) | Unclear risk | Not reported in manuscript therefore authors were contacted (19 May 2016) No response received |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All the participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Unclear risk | Vitamin C intake through diet was screened through weighed food records No detail on whether participants were asked to refrain from using supplements or anti‐inflammatory medication |
| Methods | Randomised controlled trial (cross‐over design) Separated by a 14‐day washout | |
| Participants | Setting: laboratory; USA n = 16 healthy, non‐smoking, recreationally active males, mean age 24 (SD 1.4) years Inclusion/exclusion criteria Participants were disqualified if they had participated in resistance exercise training of any kind in the previous 3 months, were currently participating in a formalised endurance training programme or had previous history of upper body injury. Other exclusion criteria included a recent weight change of more than 5 kg, history of hypertension, use of anti‐inflammatory drugs, angiotensin converting enzyme inhibitors lipid‐lowering medications or selective serotonin reuptake inhibitors. | |
| Interventions | Intervention Pomegranate juice POM Wonderful 500 mL twice daily, 650 mg polyphenols, consisting of 95.5% ellagitannins, 3.5% ellagic acid and 1% anthocyanins Placebo 35 g carbohydrate + colouring and flavouring to match the pomegranate juice Duration 2 doses per day separated by 12 hours; 2 x 9‐day treatment periods separated by a 14‐day washout | |
| Outcomes | PRIMARY Delayed onset muscle soreness of the elbow flexor muscles was determined before each isometric strength test using a 0 to 10 visual analogue scale where 0 is "no soreness" and 10 is "unbearable soreness". The rating was obtained before the measurement of strength while performing unloaded elbow flexion of the tested arm. SECONDARY Maximal isometric strength in elbow extensors was performed on a modified preacher curl bench. Force was recorded using a load cell (LC101‐500; Omega Engineering, Stamford, CT) secured to the ground using a galvanised steel cable and a strap secured to the waist of the participant. The participant performed 4 trials, 2 at both 150 degrees and 135 degrees of complete elbow extension, with a 180‐second rest in between each trial. Strength was reported as the average of the peak values at angles 150 and 135 degrees of elbow flexion. | |
| Exercise type | 2 sets of 20 maximal eccentric elbow flexion exercises | |
| Sources of funding | The study was supported by a grant from POM Wonderful, L.L.C. | |
| Notes | 2 doses of 480 mL of the drink consumed daily separated by 12 hours. Participants were reminded to take the products verbally and via email communication to consume the experimental supplements at the required times Authors were contacted to request raw data for delayed onset muscle soreness and maximal voluntary isometric contraction on 2 November 2013 and responded on 5 December 2013 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details in manuscript Authors were contacted on 26 May 2016 via email with no response |
| Allocation concealment (selection bias) | Unclear risk | No details in manuscript Authors were contacted on 26 May 2016 via email with no response |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory drugs or other supplements that could reduce soreness |
| Methods | Randomised controlled trial (cross‐over design) Separated by a 14‐day washout | |
| Participants | Setting: laboratory; USA n = 17 healthy, non‐smoking, resistance‐trained males; mean age 21.9 (SD 2.4) years Inclusion/exclusion criteria The participants were required to have been weight training for at least the last 3 months, exercising both their upper and lower body, at least twice per week. Criteria for exclusion were a recent weight change of > 5 kg; history of hypertension; the prescience of major orthopaedic injury; use of anti‐inflammatory drugs; over‐the‐counter pain medicine, vitamin or mineral supplements, angiotensin‐converting enzyme inhibitors | |
| Interventions | Intervention Pomegranate juice 250 mL POM Wonderful (LA, USA). Each bottle contained approximately 1979 mg/L of tannins, 384 mg/L anthocyanins and 121 mg/L of ellagic derivatives. Placebo 35 g carbohydrate + colouring and flavouring to match the pomegranate juice Duration 44 days; 15 days of supplementation with a 14‐day washout | |
| Outcomes | PRIMARY Delayed onset muscle soreness of the elbow flexor and knee extensor muscles was determined before each isometric strength test using a 0‐ to 10‐point visual analogue scale where 0 is "no soreness" and 10 is "unbearable soreness". The rating was obtained before the measurement of strength while performing unloaded elbow flexion and knee extension on the tested arm and leg. SECONDARY Maximal isometric strength in elbows and knee extensors was performed on a modified preacher curl bench and modified knee extension machine respectively. The participant performed 4 trials at both 30 and 45 degrees above elbow extension and 45 and 90 degree below knee extension with 180‐second rest in between each trial. Strength for both tests was reported as the average peak value of each joint angle. | |
| Exercise type | 3 sets of 20 maximal eccentric elbow extensions on an isokinetic dynamometer | |
| Sources of funding | The study was funded by POM Wonderful, L.L.C. | |
| Notes | Supplement taken as 250 mL bottle twice daily separated by 12 hours. Participants were reminded to take the products verbally and via email communication to consume the experimental supplements at the required times Authors were contacted to request raw data for delayed onset muscle soreness and maximal voluntary isometric contraction on 2 November 2013 and responded on 5 December 2013 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details in manuscript Authors were contacted on 26 May 2016 via email with no response |
| Allocation concealment (selection bias) | Unclear risk | No details in manuscript Authors were contacted on 26 May 2016 via email with no response |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | High risk | No published protocol available All outcomes reported at all time points Adverse effects of antioxidant supplementation were not reported |
| Other bias | Low risk | Participants were asked to refrain from using anti‐inflammatory drugs or other supplements that could reduce soreness |
BMI: body mass index
EGCG: epigallocatechin gallate
IU: international units
NAC: N‐acetyl‐cysteine
NSAID: non‐steroidal anti‐inflammatory drug
PPT: pressure pain threshold
RM: repetition maximum
SD: standard deviation
SE: standard error
SEM: standard error of the mean
VAS: visual analogue scale
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
| Although delayed onset muscle soreness is in the title, it was not measured Authors were contacted on 4 February 2017 to confirm | |
| Examined antioxidants, ibuprofen, cold water immersion and whey protein at the same time compared to a placebo | |
| Non‐randomised study design | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured Tenderness was measured using a handheld algometer | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured. | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Tart cherry juice with whey protein No tart cherry juice only group | |
| Delayed onset muscle soreness not measured. | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Supplementation used was not classed as an antioxidant | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Antioxidant supplement was mixed with fish oils and antioxidant supplement alone not investigated | |
| Delayed onset muscle soreness not measured Tenderness was measured using a handheld algometer | |
| Delayed onset muscle soreness not measured Tenderness was measured using a handheld algometer | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Antioxidant supplement compared to another dietary supplement (protein‐carbohydrate supplement) | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured Tenderness was measured using a handheld algometer | |
| Delayed onset muscle soreness not measured Tenderness was measured using a handheld algometer | |
| Intervention was antioxidants and protein versus carbohydrate only Protein can reduce muscle soreness | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured. | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured | |
| Delayed onset muscle soreness not measured |
Characteristics of ongoing studies [ordered by study ID]
| Trial name or title | The effects of repeated bouts of downhill running and curcumin supplementation on arterial stiffness during recovery |
| Methods | Randomised controlled trial (double‐blind) |
| Participants | Setting: laboratory; USA n = 17 healthy, non‐smoking, resistance‐trained males; mean age 21.9 (SD 2.4) years Inclusion/exclusion criteria The participants were required to have been weight training for at least the last 3 months, exercising both their upper and lower body, at least twice per week. Criteria for exclusion were a recent weight change of > 5 kg; history of hypertension; the prescience of major orthopaedic injury; use of anti‐inflammatory drugs; over‐the‐counter pain medicine, vitamin or mineral supplements, angiotensin‐converting enzyme inhibitors. |
| Interventions | Experimental Curcumin supplement 200 mg, curcuminoids, 7 days of supplementation in capsular form Placebo Sucrose, capsular |
| Outcomes | PRIMARY Delayed onset muscle soreness (every 24 hours up to 72 hours post baseline); subjective analogue scale SECONDARY N/A |
| Starting date | November 2014 |
| Contact information | Dr Jamie Burr, Assistant Professor, University of Prince Edward Island |
| Notes | ClinicalTrials.gov identifier: NCT02281981 |
N/A: not applicable
SD: standard deviation
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Muscle soreness up to 6 hours; random‐effects model Show forest plot | 21 | 525 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.30 [‐0.56, ‐0.04] |
| Analysis 1.1  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 1 Muscle soreness up to 6 hours; random‐effects model. | ||||
| 2 Muscle soreness at 24 hours; random‐effects model Show forest plot | 41 | 936 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.27, 0.00] |
| Analysis 1.2  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 2 Muscle soreness at 24 hours; random‐effects model. | ||||
| 3 Muscle soreness at 48 hours; random‐effects model Show forest plot | 45 | 1047 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.24 [‐0.42, ‐0.07] |
| Analysis 1.3  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 3 Muscle soreness at 48 hours; random‐effects model. | ||||
| 4 Muscle soreness at 72 hours; random‐effects model Show forest plot | 28 | 657 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.19 [‐0.38, ‐0.00] |
| Analysis 1.4  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 4 Muscle soreness at 72 hours; random‐effects model. | ||||
| 5 Muscle soreness at 96 hours; random‐effects model Show forest plot | 17 | 436 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.05 [‐0.29, 0.19] |
| Analysis 1.5  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 5 Muscle soreness at 96 hours; random‐effects model. | ||||
| 6 Muscle soreness (follow‐ups: 120, 144 and 168 hours); random‐effects model Show forest plot | 7 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 1.6  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 6 Muscle soreness (follow‐ups: 120, 144 and 168 hours); random‐effects model. | ||||
| 6.1 at 120 hours | 4 | 128 | Std. Mean Difference (IV, Random, 95% CI) | 0.21 [‐0.26, 0.69] |
| 6.2 at 144 hours | 1 | 20 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.23 [‐1.11, 0.65] |
| 6.3 at 168 hours | 4 | 80 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.04 [‐0.48, 0.41] |
| 7 Muscle soreness up to 6 hours ‐ all at same scale (0 to 10; worst pain) Show forest plot | 21 | 525 | Mean Difference (IV, Random, 95% CI) | ‐0.52 [‐0.95, ‐0.08] |
| Analysis 1.7  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 7 Muscle soreness up to 6 hours ‐ all at same scale (0 to 10; worst pain). | ||||
| 8 Muscle soreness at 24 hours ‐ all at same scale (0 to 10; worst pain) Show forest plot | 41 | 936 | Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.42, 0.07] |
| Analysis 1.8 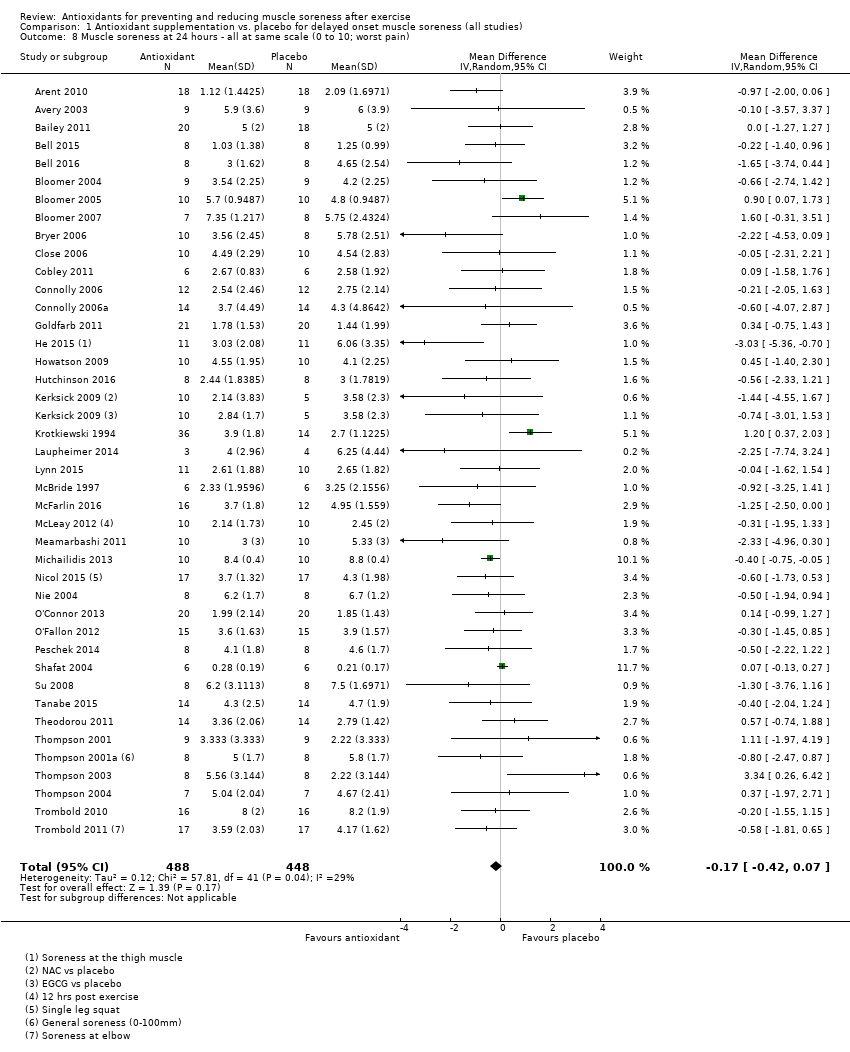 Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 8 Muscle soreness at 24 hours ‐ all at same scale (0 to 10; worst pain). | ||||
| 9 Muscle soreness at 48 hours ‐ all at same scale (0 to 10; worst pain) Show forest plot | 45 | 1047 | Mean Difference (IV, Random, 95% CI) | ‐0.41 [‐0.69, ‐0.12] |
| Analysis 1.9  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 9 Muscle soreness at 48 hours ‐ all at same scale (0 to 10; worst pain). | ||||
| 10 Muscle soreness at 72 hours ‐ all at same scale (0 to 10; worst pain) Show forest plot | 28 | 657 | Mean Difference (IV, Random, 95% CI) | ‐0.29 [‐0.59, 0.02] |
| Analysis 1.10  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 10 Muscle soreness at 72 hours ‐ all at same scale (0 to 10; worst pain). | ||||
| 11 Muscle soreness at 96 hours ‐ all at same scale (0 to 10; worst pain) Show forest plot | 17 | 436 | Mean Difference (IV, Random, 95% CI) | ‐0.03 [‐0.43, 0.37] |
| Analysis 1.11  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 11 Muscle soreness at 96 hours ‐ all at same scale (0 to 10; worst pain). | ||||
| 12 Muscle soreness at 24 hours. Subgroup analysis by type of exercise (whole body aerobic vs. mechanically induced) Show forest plot | 41 | 936 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.27, 0.00] |
| Analysis 1.12  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 12 Muscle soreness at 24 hours. Subgroup analysis by type of exercise (whole body aerobic vs. mechanically induced). | ||||
| 12.1 Whole body aerobic exercise | 17 | 338 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐0.33, 0.18] |
| 12.2 Mechanically induced | 24 | 598 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.18 [‐0.34, ‐0.01] |
| 13 Muscle soreness at 48 hours. Subgroup analysis by type of exercise (whole body aerobic vs. mechanically induced) Show forest plot | 45 | 1047 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.24 [‐0.42, ‐0.07] |
| Analysis 1.13  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 13 Muscle soreness at 48 hours. Subgroup analysis by type of exercise (whole body aerobic vs. mechanically induced). | ||||
| 13.1 Whole body aerobic exercise | 17 | 349 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.12 [‐0.47, 0.23] |
| 13.2 Mechanically induced | 28 | 698 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.31 [‐0.50, ‐0.12] |
| 14 Muscle soreness at 24 hours. Subgroup analysis by funding sources (funded by food company or provider of antioxidant supplements vs. not funded by food company or provider of antioxidant supplements) Show forest plot | 40 | 920 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.13 [‐0.26, 0.01] |
| Analysis 1.14  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 14 Muscle soreness at 24 hours. Subgroup analysis by funding sources (funded by food company or provider of antioxidant supplements vs. not funded by food company or provider of antioxidant supplements). | ||||
| 14.1 Company funding | 17 | 427 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.11 [‐0.31, 0.08] |
| 14.2 Other funding | 23 | 493 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.14 [‐0.32, 0.05] |
| 15 Muscle soreness at 48 hours. Subgroup analysis by funding sources (funded by food company or provider of antioxidant supplements vs. not funded by food company or provider of antioxidant supplements) Show forest plot | 44 | 1031 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.21 [‐0.34, ‐0.09] |
| Analysis 1.15  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 15 Muscle soreness at 48 hours. Subgroup analysis by funding sources (funded by food company or provider of antioxidant supplements vs. not funded by food company or provider of antioxidant supplements). | ||||
| 15.1 Company funding | 18 | 443 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.19 [‐0.38, 0.00] |
| 15.2 Other funding | 26 | 588 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.23 [‐0.40, ‐0.06] |
| 16 Muscle tenderness measured in Newtons (all follow‐up times) Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| Analysis 1.16  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 16 Muscle tenderness measured in Newtons (all follow‐up times). | ||||
| 16.1 at 24 hours | 2 | 52 | Mean Difference (IV, Fixed, 95% CI) | ‐1.60 [‐7.64, 4.45] |
| 16.2 at 48 hours | 2 | 52 | Mean Difference (IV, Fixed, 95% CI) | ‐2.14 [‐9.48, 5.19] |
| 16.3 at 72 hours | 2 | 52 | Mean Difference (IV, Fixed, 95% CI) | ‐0.34 [‐6.55, 5.86] |
| 16.4 at 96 hours | 2 | 52 | Mean Difference (IV, Fixed, 95% CI) | ‐2.32 [‐9.62, 4.99] |
| 17 Muscle tenderness measured in kg (all follow‐up times) Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| Analysis 1.17  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 17 Muscle tenderness measured in kg (all follow‐up times). | ||||
| 17.1 Up to 6 hours | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | ‐0.61 [‐14.10, 12.88] |
| 17.2 at 24 hours | 2 | 36 | Mean Difference (IV, Fixed, 95% CI) | 0.53 [‐0.95, 2.01] |
| 17.3 at 48 hours | 2 | 36 | Mean Difference (IV, Fixed, 95% CI) | 0.52 [‐1.08, 2.13] |
| 17.4 at 72 hours | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | ‐1.03 [‐13.01, 10.95] |
| 17.5 at 96 hours | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | ‐1.39 [‐15.12, 12.33] |
| 18 30‐second Wingate average peak power output (W/kg) (post 7 days of intervention) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Analysis 1.18  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 18 30‐second Wingate average peak power output (W/kg) (post 7 days of intervention). | ||||
| 19 20 m Sprint time (s) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Analysis 1.19  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 19 20 m Sprint time (s). | ||||
| 19.1 at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.2 at 48 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.3 at 120 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 20 Maximal oxygen consumption (mL/kg/min) (post 42 days of supplementation) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Analysis 1.20  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 20 Maximal oxygen consumption (mL/kg/min) (post 42 days of supplementation). | ||||
| 21 Agility (seconds) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Analysis 1.21  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 21 Agility (seconds). | ||||
| 21.1 at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.2 at 48 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.3 at 72 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 22 6 second sprint maximal power (Watts) (all follow‐up times) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Analysis 1.22  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 22 6 second sprint maximal power (Watts) (all follow‐up times). | ||||
| 22.1 at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.2 at 48 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.3 at 72 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23 Maximal voluntary isometric contraction measured as percentage change from baseline Show forest plot | 15 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| Analysis 1.23  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 23 Maximal voluntary isometric contraction measured as percentage change from baseline. | ||||
| 23.1 Up to 6 hours | 11 | 255 | Mean Difference (IV, Fixed, 95% CI) | 5.86 [3.29, 8.42] |
| 23.2 at 24 hours | 15 | 375 | Mean Difference (IV, Fixed, 95% CI) | 2.51 [0.99, 4.04] |
| 23.3 at 48 hours | 15 | 375 | Mean Difference (IV, Fixed, 95% CI) | 4.46 [2.94, 5.98] |
| 23.4 at 72 hours | 11 | 277 | Mean Difference (IV, Fixed, 95% CI) | 3.92 [0.88, 6.96] |
| 23.5 at 96 hours | 9 | 252 | Mean Difference (IV, Fixed, 95% CI) | 5.29 [3.65, 6.92] |
| 23.6 at 168 hours | 2 | 36 | Mean Difference (IV, Fixed, 95% CI) | ‐7.96 [‐15.96, 0.05] |
| 24 Maximal voluntary isometric contraction measured in Newton metres Show forest plot | 6 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| Analysis 1.24  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 24 Maximal voluntary isometric contraction measured in Newton metres. | ||||
| 24.1 Up to 6 hours | 3 | 84 | Mean Difference (IV, Fixed, 95% CI) | ‐1.50 [‐4.77, 1.76] |
| 24.2 at 24 hours | 6 | 148 | Mean Difference (IV, Fixed, 95% CI) | ‐0.63 [‐6.27, 5.01] |
| 24.3 at 48 hours | 6 | 148 | Mean Difference (IV, Fixed, 95% CI) | 0.80 [‐5.46, 7.06] |
| 24.4 at 72 hours | 4 | 94 | Mean Difference (IV, Fixed, 95% CI) | ‐3.62 [‐11.91, 4.67] |
| 24.5 at 96 hours | 3 | 96 | Mean Difference (IV, Fixed, 95% CI) | ‐4.65 [‐16.21, 6.92] |
| 24.6 at 120 hours | 2 | 58 | Mean Difference (IV, Fixed, 95% CI) | ‐5.89 [‐19.14, 7.36] |
| 24.7 at 168 hours | 1 | 38 | Mean Difference (IV, Fixed, 95% CI) | 58.0 [13.57, 102.43] |
| 25 Maximal voluntary isometric contraction measured in Newtons Show forest plot | 6 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| Analysis 1.25  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 25 Maximal voluntary isometric contraction measured in Newtons. | ||||
| 25.1 Up to 6 hours | 4 | 73 | Mean Difference (IV, Fixed, 95% CI) | 6.50 [‐55.11, 68.10] |
| 25.2 at 24 hours | 5 | 87 | Mean Difference (IV, Fixed, 95% CI) | 23.03 [‐23.18, 69.24] |
| 25.3 at 48 hours | 5 | 87 | Mean Difference (IV, Fixed, 95% CI) | 34.87 [‐17.80, 87.55] |
| 25.4 at 72 hours | 4 | 70 | Mean Difference (IV, Fixed, 95% CI) | ‐5.11 [‐73.42, 63.19] |
| 25.5 at 96 hours | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | ‐112.0 [‐265.08, 41.08] |
| 25.6 at 168 hours | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | ‐225.0 [‐534.90, 84.90] |
| 26 Maximal voluntary isometric contraction measured in Newton metres per kg of body mass Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Analysis 1.26  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 26 Maximal voluntary isometric contraction measured in Newton metres per kg of body mass. | ||||
| 26.1 Up to 6 hours | 2 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.2 at 24 hours | 2 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.3 at 48 hours | 2 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.4 at 72 hours | 2 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.5 at 96 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.6 at 120 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.7 at 144 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.8 at 168 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 27 Maximal voluntary isometric contraction measured in kg Show forest plot | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| Analysis 1.27  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 27 Maximal voluntary isometric contraction measured in kg. | ||||
| 27.1 at 24 hours | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 27.2 at 48 hours | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 28 Range of motion (all follow‐up times) Show forest plot | 10 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| Analysis 1.28  Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 28 Range of motion (all follow‐up times). | ||||
| 28.1 Up to 6 hours | 6 | 163 | Mean Difference (IV, Fixed, 95% CI) | ‐0.25 [‐3.31, 2.81] |
| 28.2 at 24 hours | 9 | 259 | Mean Difference (IV, Fixed, 95% CI) | 1.03 [‐0.91, 2.96] |
| 28.3 at 48 hours | 9 | 259 | Mean Difference (IV, Fixed, 95% CI) | 2.71 [0.39, 5.04] |
| 28.4 at 72 hours | 7 | 196 | Mean Difference (IV, Fixed, 95% CI) | 2.93 [‐0.02, 5.87] |
| 28.5 at 96 hours | 6 | 158 | Mean Difference (IV, Fixed, 95% CI) | 0.79 [‐1.26, 2.84] |
| 28.6 at 120 hours | 2 | 63 | Mean Difference (IV, Fixed, 95% CI) | ‐0.34 [‐2.43, 1.76] |
| 28.7 at 168 hours | 1 | 38 | Mean Difference (IV, Fixed, 95% CI) | 5.0 [2.77, 7.23] |
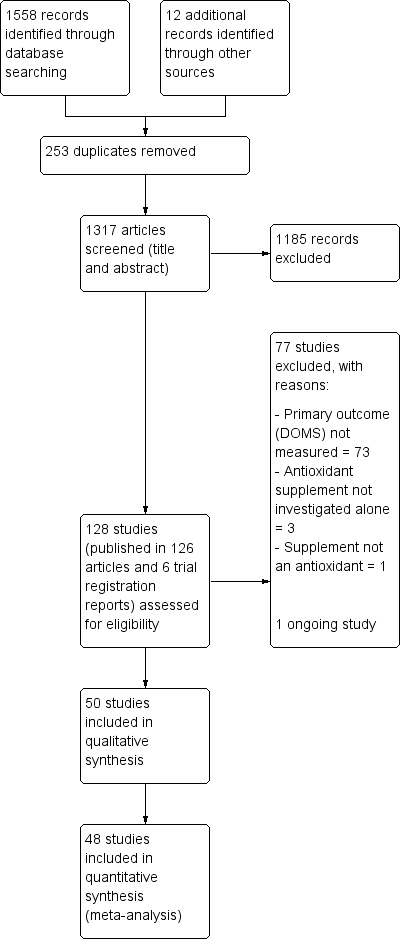
Study flow diagram

'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
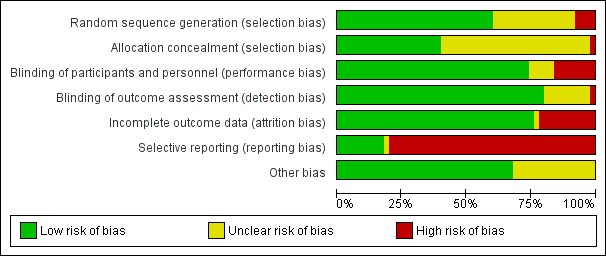
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
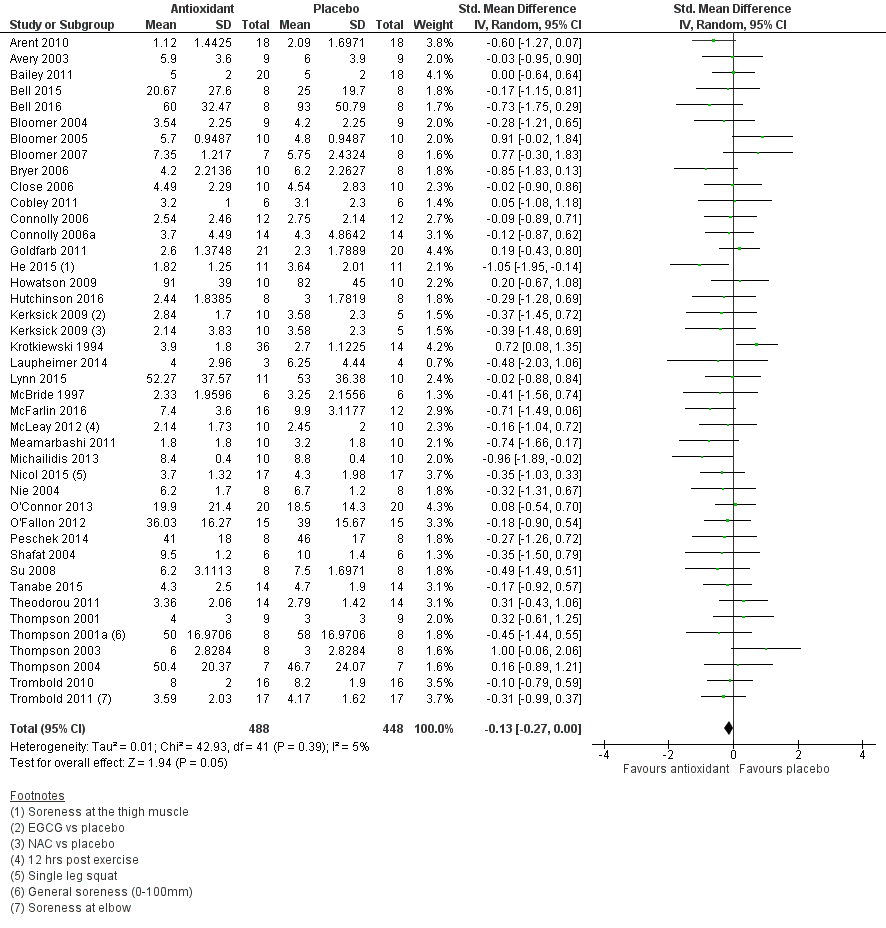
Forest plot of comparison: 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), outcome: 1.2 Muscle soreness at 24 hours; random‐effects model.
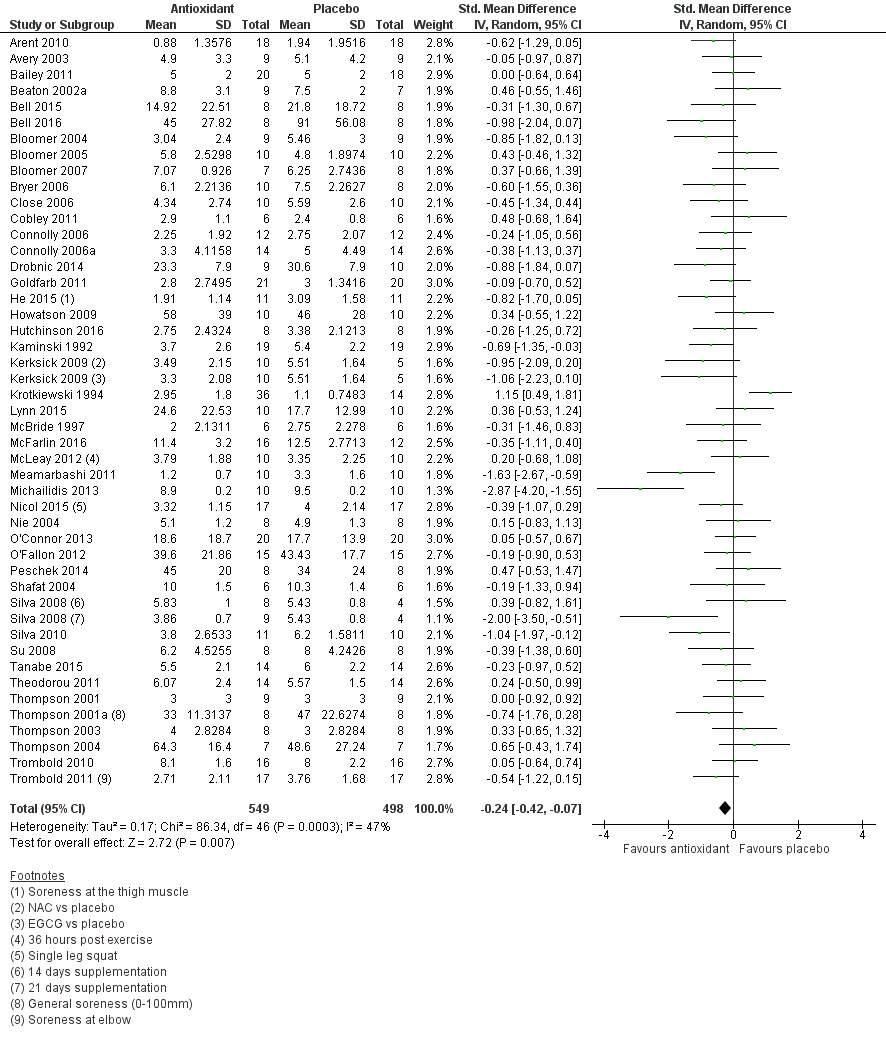
Forest plot of comparison: 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), outcome: 1.3 Muscle soreness at 48 hours; random‐effects model.
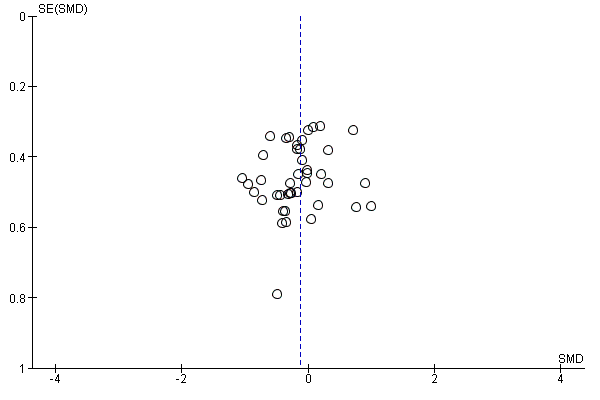
Funnel plot of comparison: 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), outcome: 1.2 Muscle soreness at 24 hours; random‐effects model.
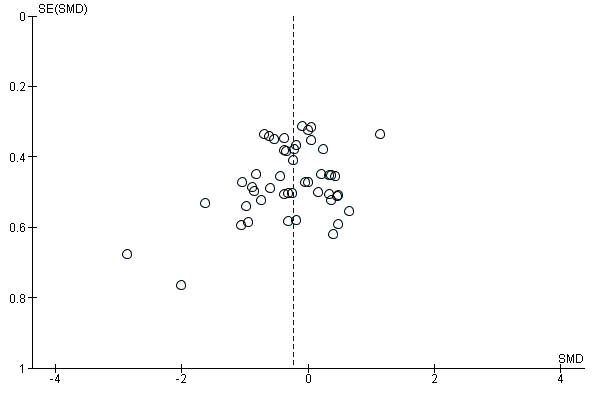
Funnel plot of comparison: 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), outcome: 1.3 Muscle soreness at 48 hours; random‐effects model.
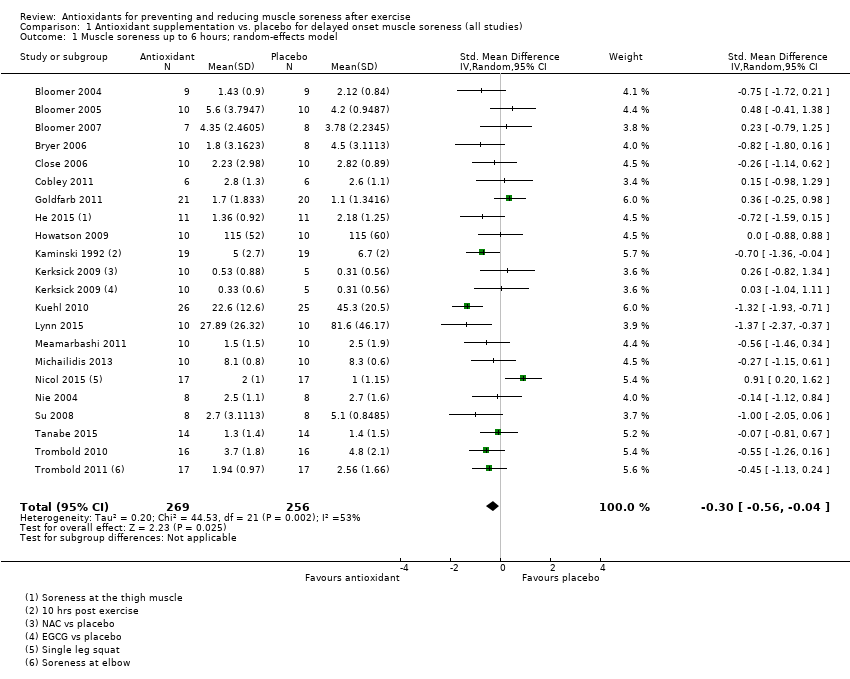
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 1 Muscle soreness up to 6 hours; random‐effects model.
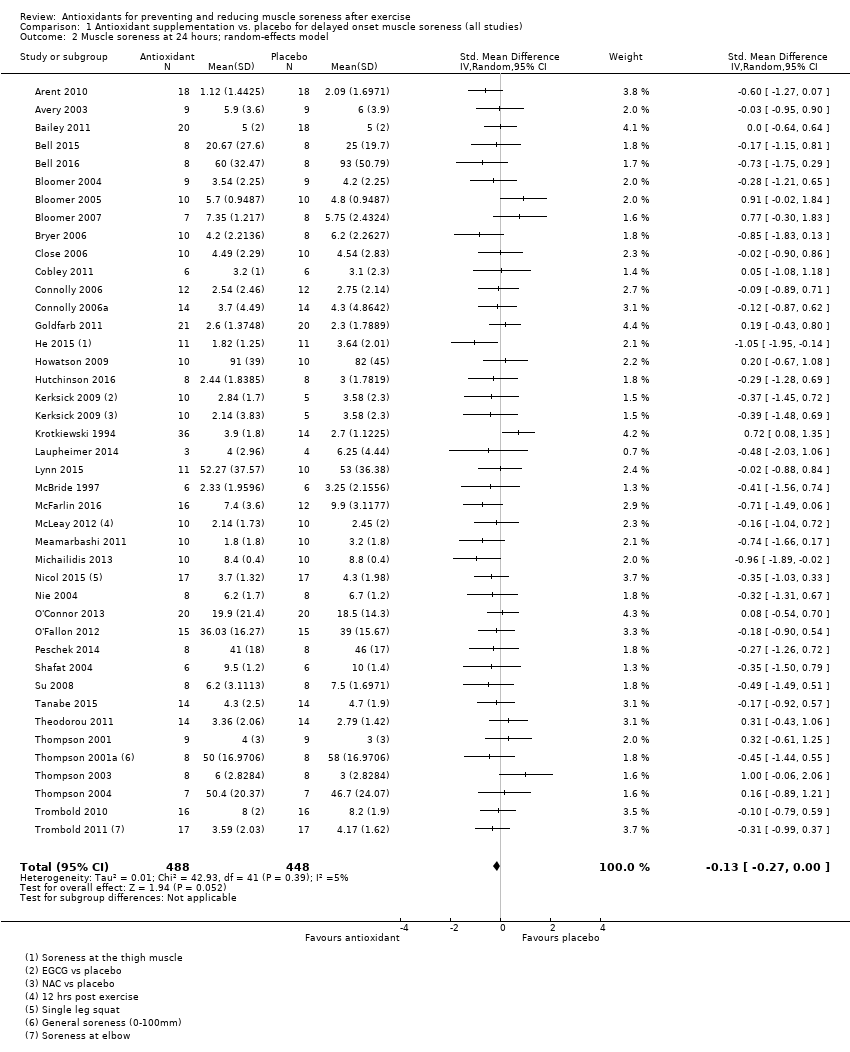
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 2 Muscle soreness at 24 hours; random‐effects model.
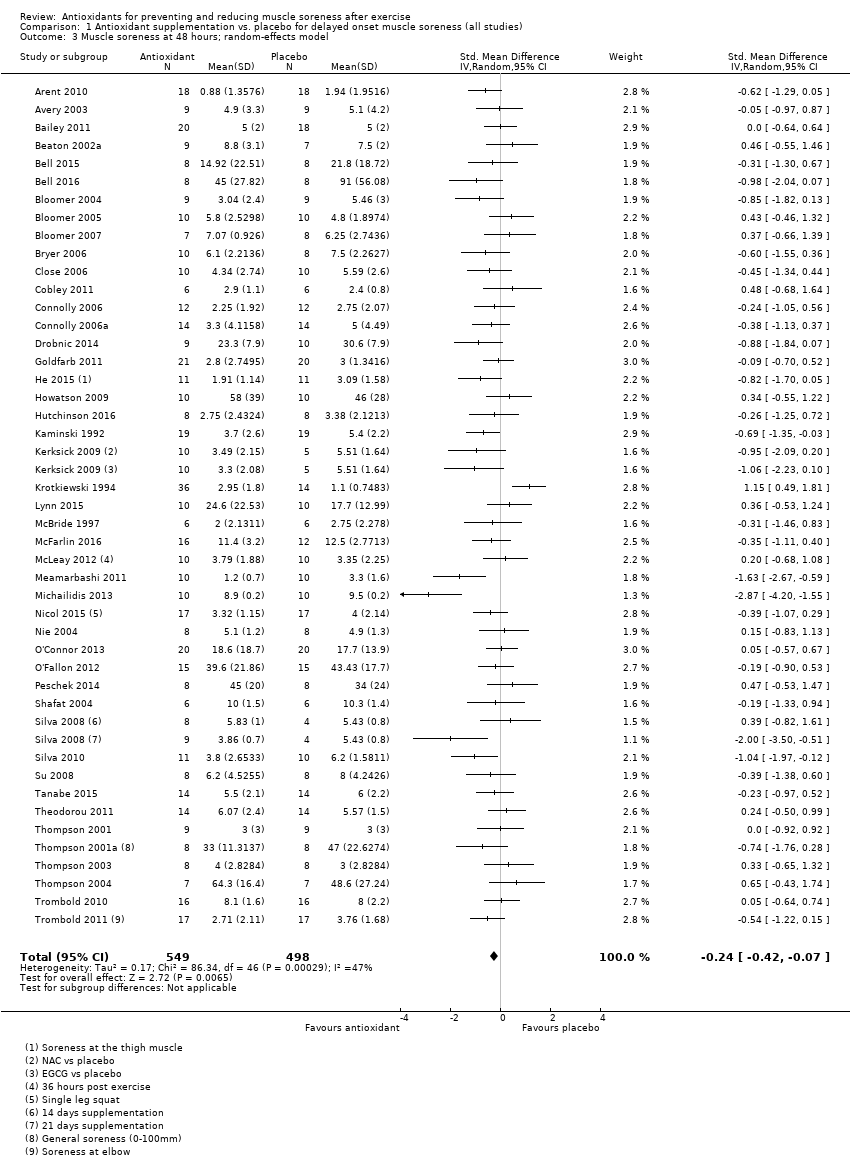
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 3 Muscle soreness at 48 hours; random‐effects model.
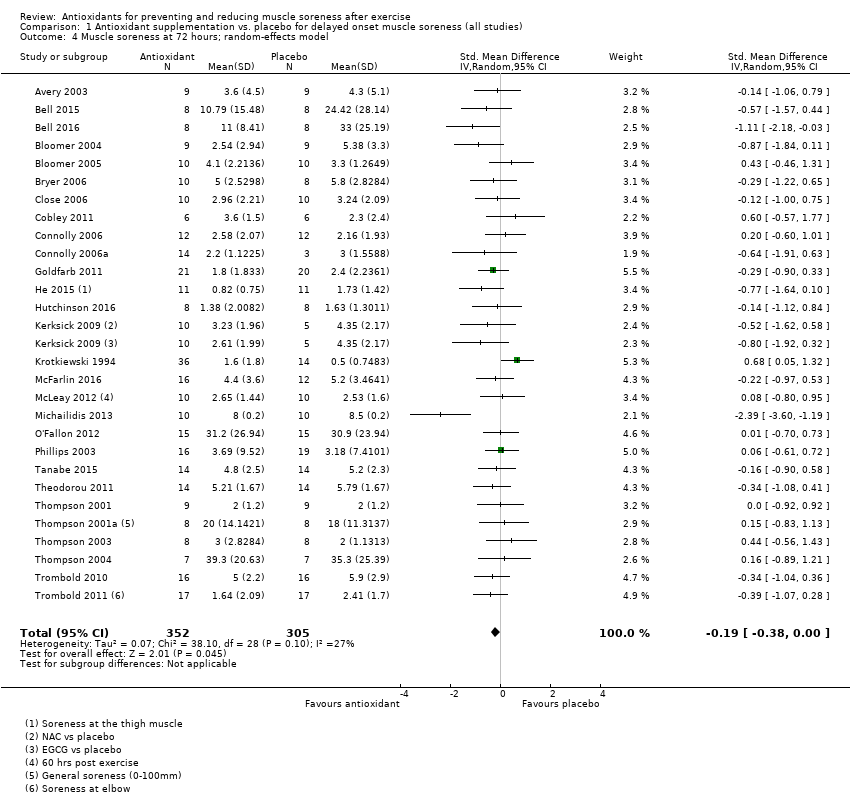
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 4 Muscle soreness at 72 hours; random‐effects model.
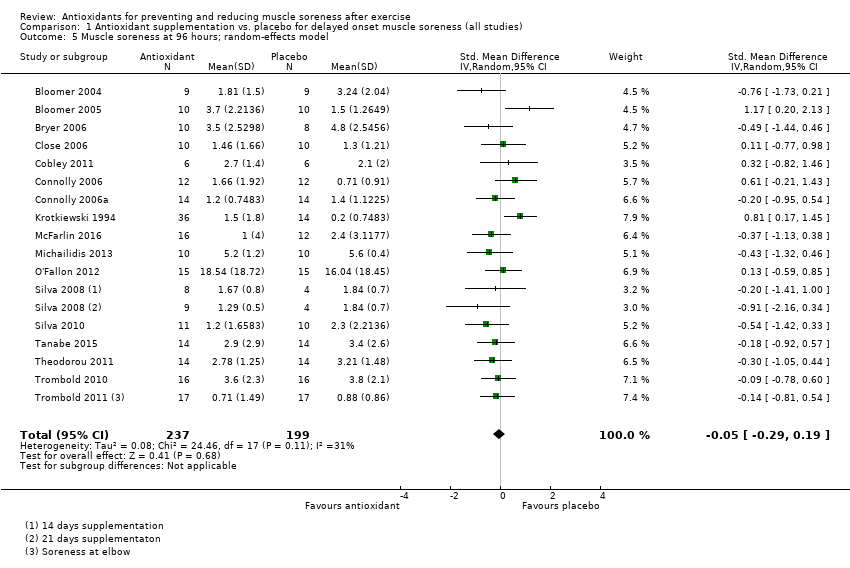
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 5 Muscle soreness at 96 hours; random‐effects model.
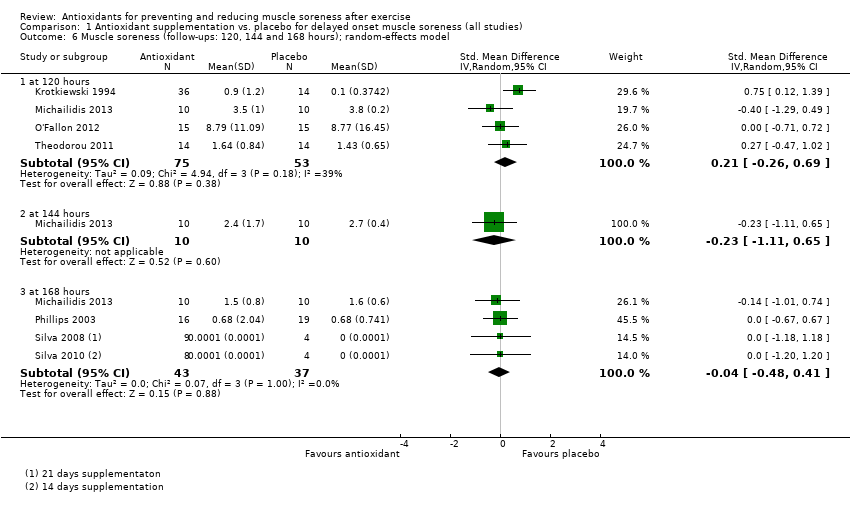
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 6 Muscle soreness (follow‐ups: 120, 144 and 168 hours); random‐effects model.
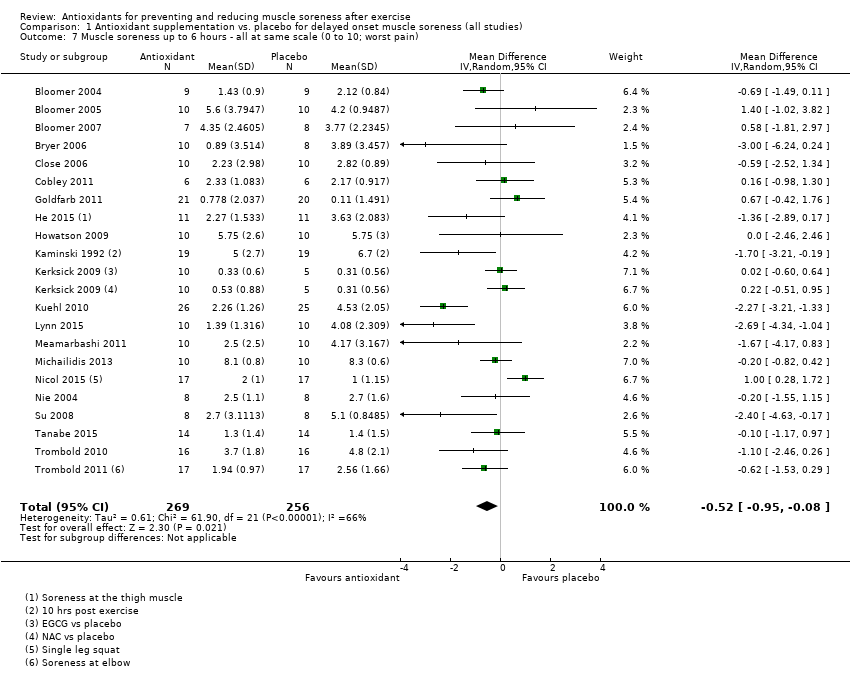
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 7 Muscle soreness up to 6 hours ‐ all at same scale (0 to 10; worst pain).
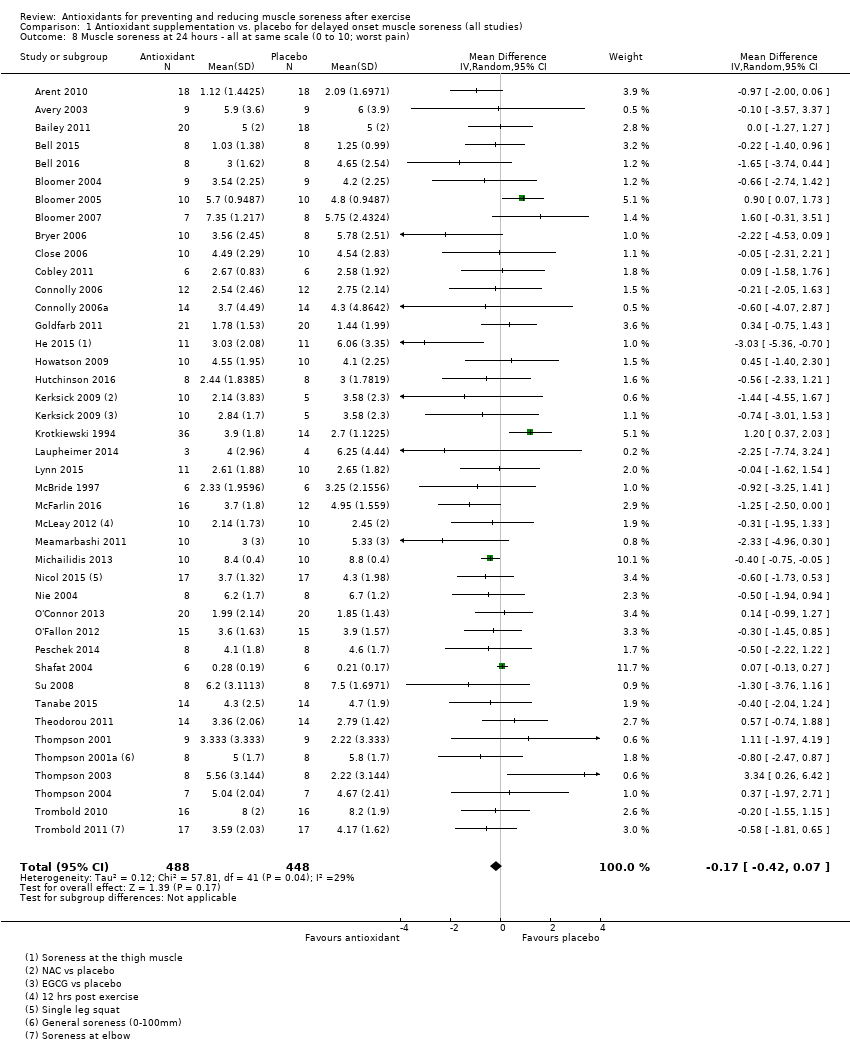
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 8 Muscle soreness at 24 hours ‐ all at same scale (0 to 10; worst pain).
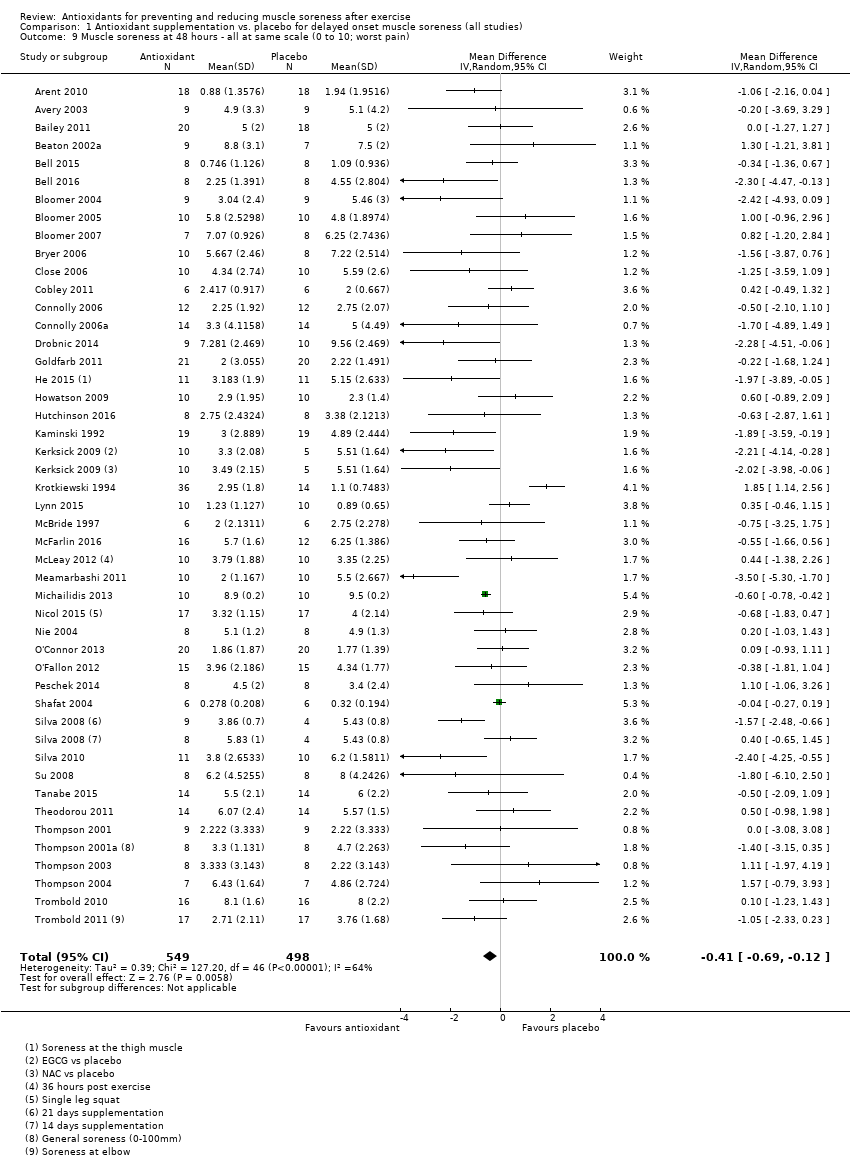
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 9 Muscle soreness at 48 hours ‐ all at same scale (0 to 10; worst pain).
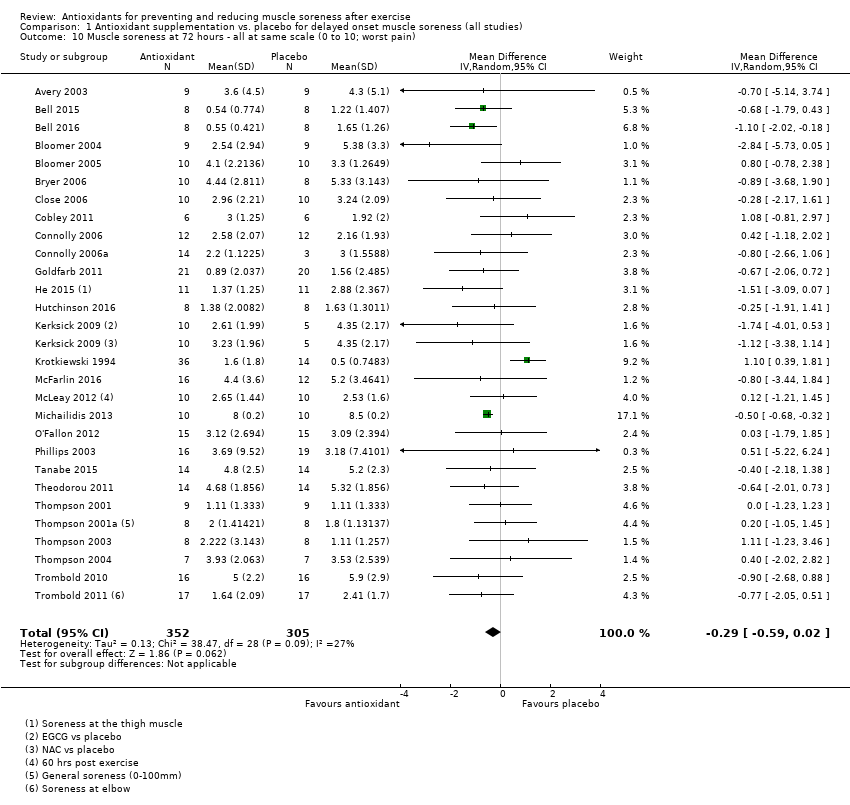
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 10 Muscle soreness at 72 hours ‐ all at same scale (0 to 10; worst pain).
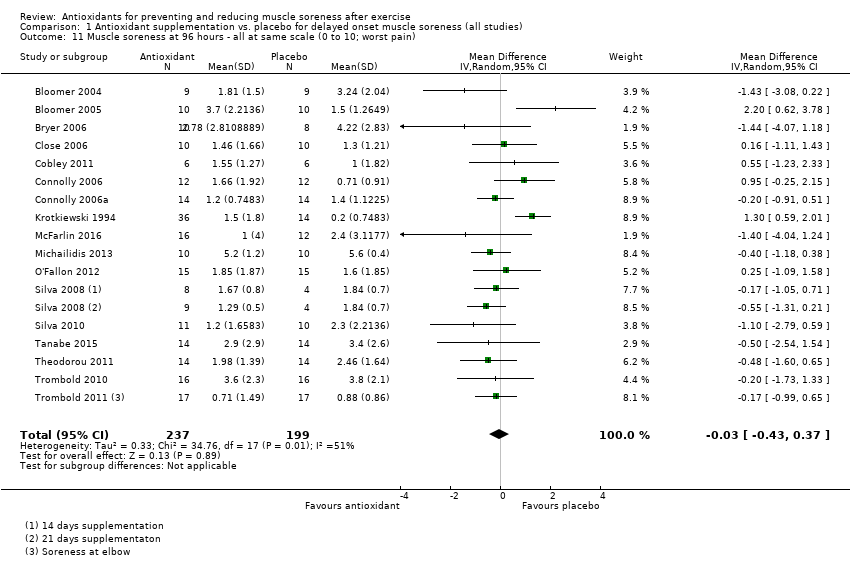
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 11 Muscle soreness at 96 hours ‐ all at same scale (0 to 10; worst pain).
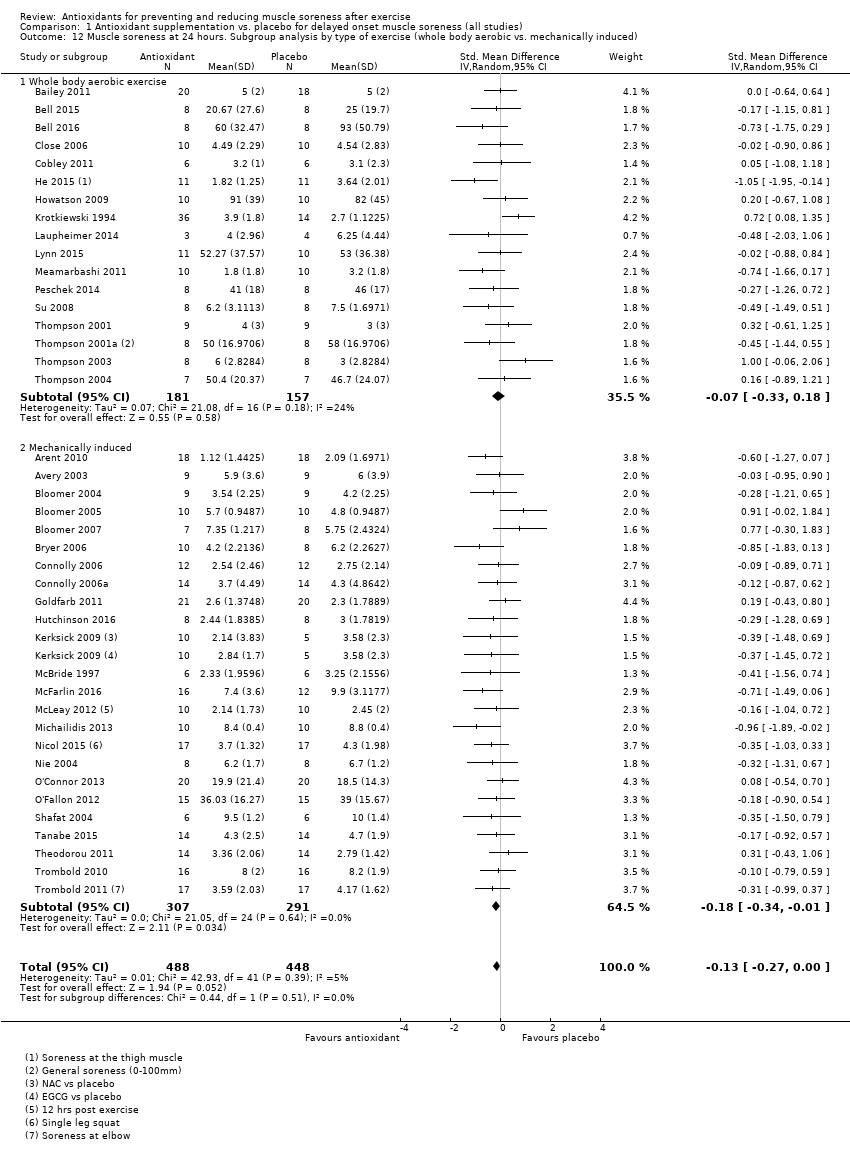
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 12 Muscle soreness at 24 hours. Subgroup analysis by type of exercise (whole body aerobic vs. mechanically induced).
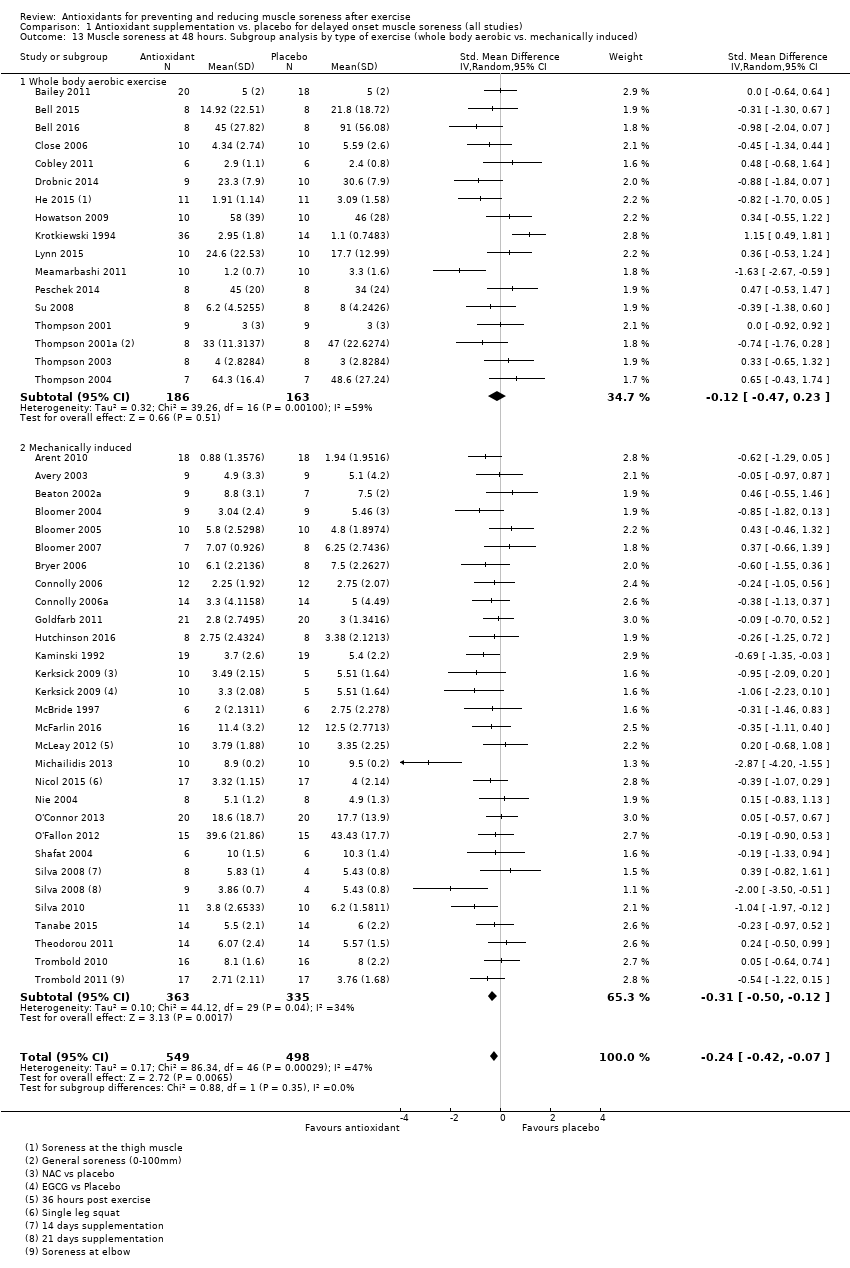
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 13 Muscle soreness at 48 hours. Subgroup analysis by type of exercise (whole body aerobic vs. mechanically induced).
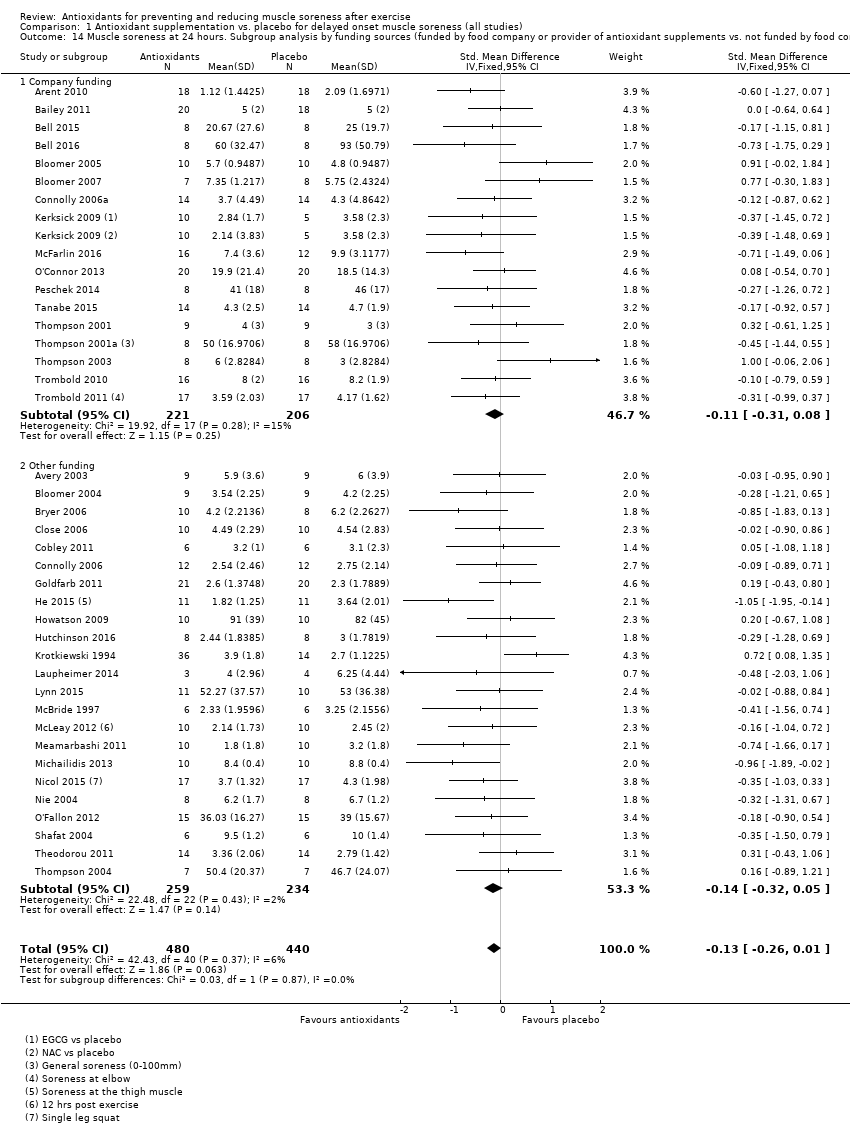
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 14 Muscle soreness at 24 hours. Subgroup analysis by funding sources (funded by food company or provider of antioxidant supplements vs. not funded by food company or provider of antioxidant supplements).
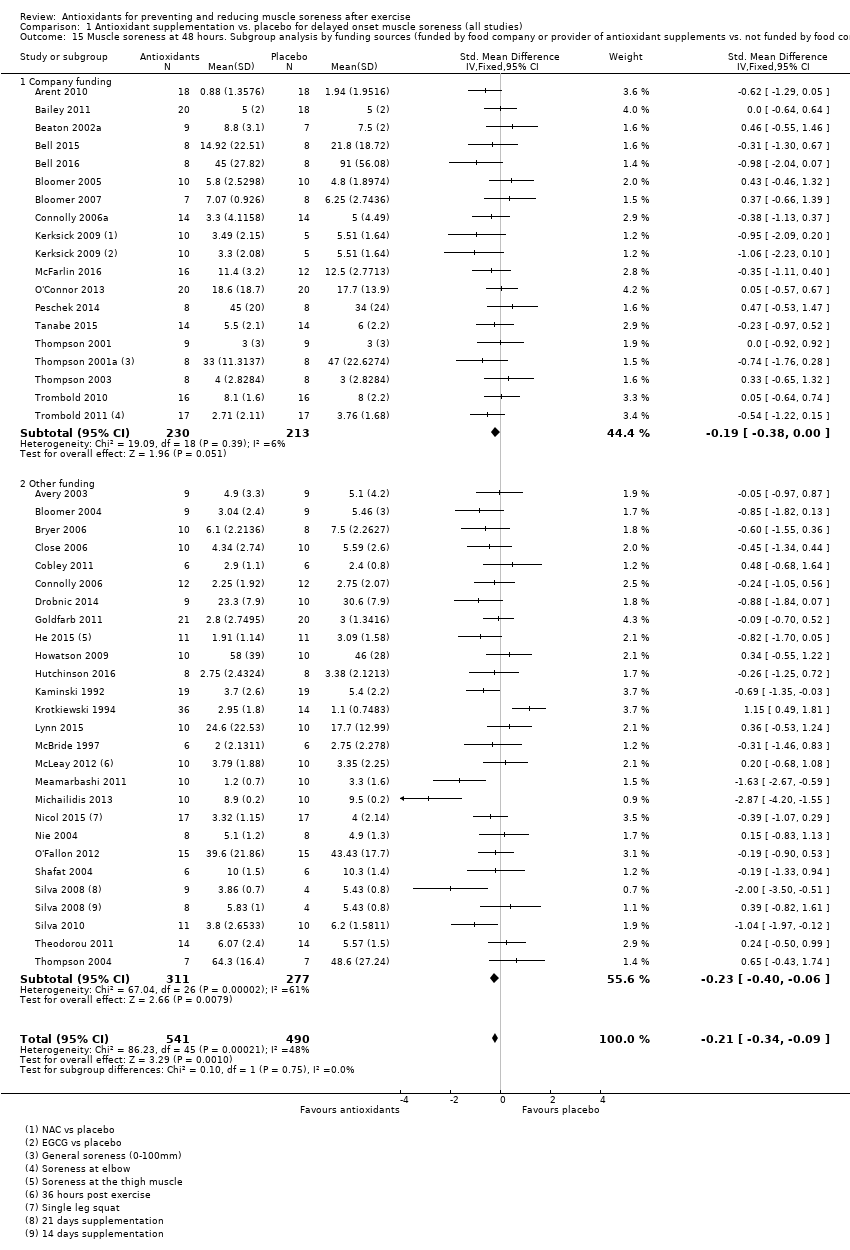
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 15 Muscle soreness at 48 hours. Subgroup analysis by funding sources (funded by food company or provider of antioxidant supplements vs. not funded by food company or provider of antioxidant supplements).
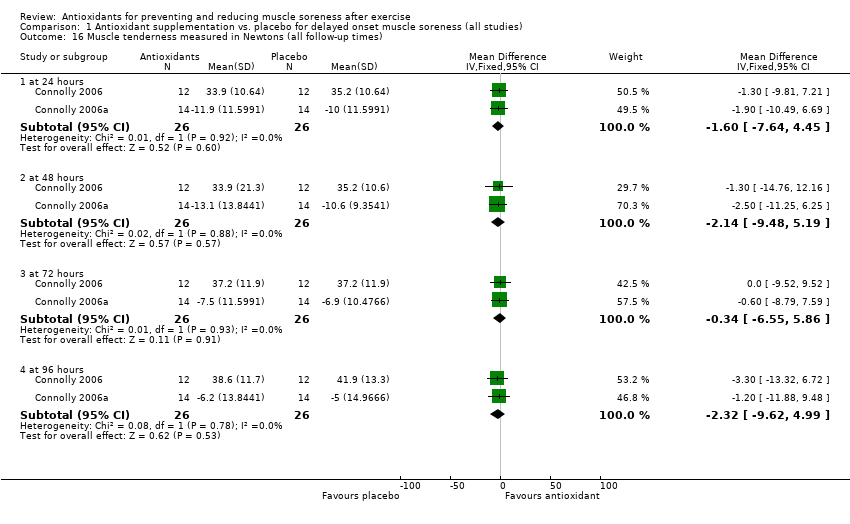
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 16 Muscle tenderness measured in Newtons (all follow‐up times).
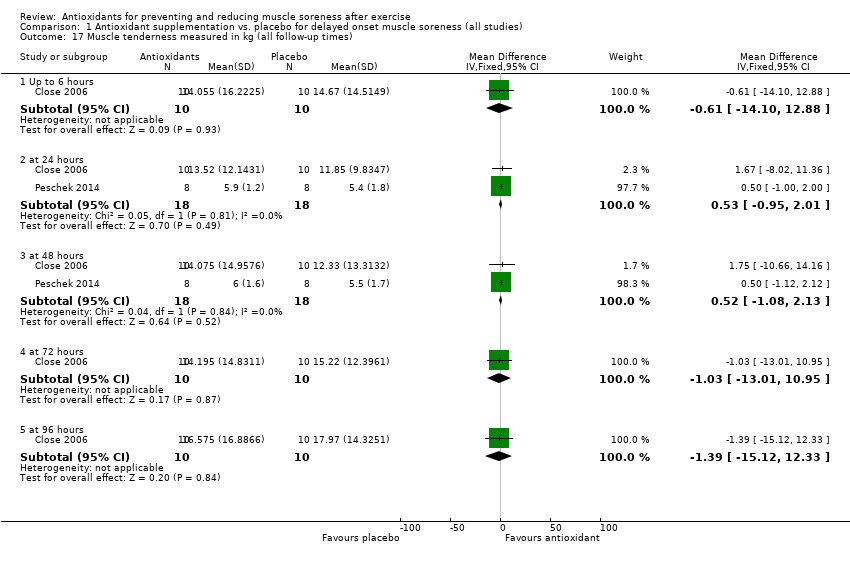
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 17 Muscle tenderness measured in kg (all follow‐up times).
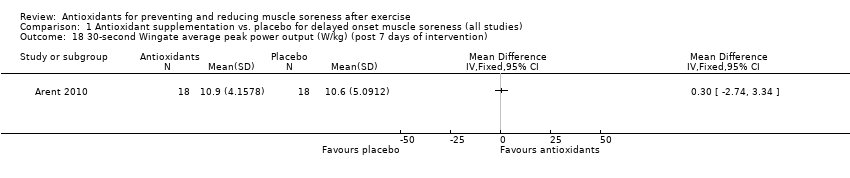
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 18 30‐second Wingate average peak power output (W/kg) (post 7 days of intervention).
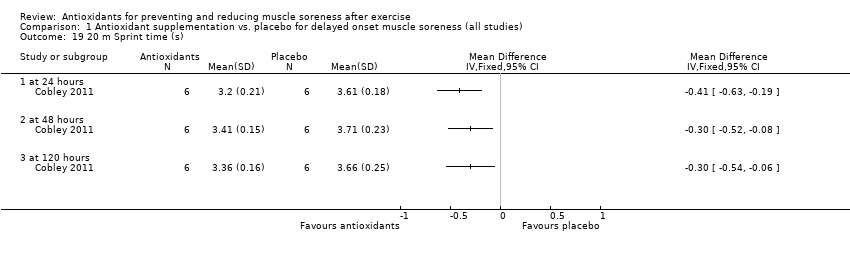
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 19 20 m Sprint time (s).
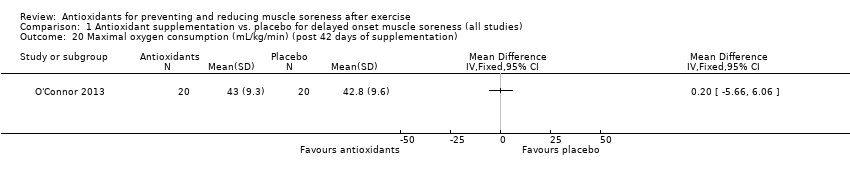
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 20 Maximal oxygen consumption (mL/kg/min) (post 42 days of supplementation).
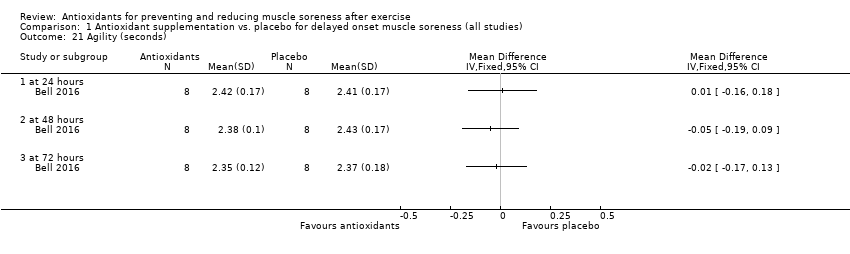
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 21 Agility (seconds).
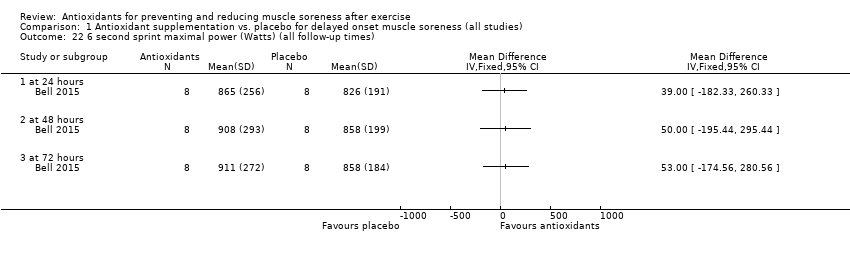
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 22 6 second sprint maximal power (Watts) (all follow‐up times).
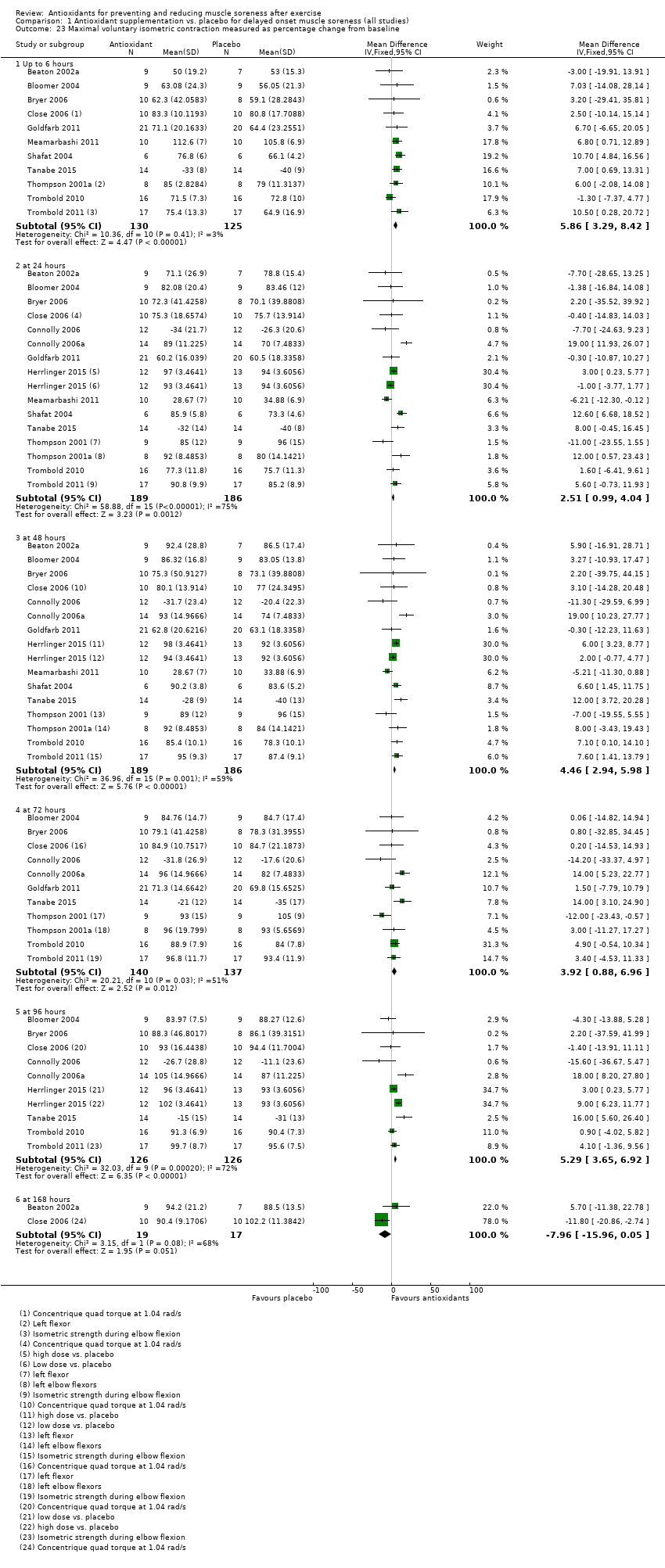
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 23 Maximal voluntary isometric contraction measured as percentage change from baseline.
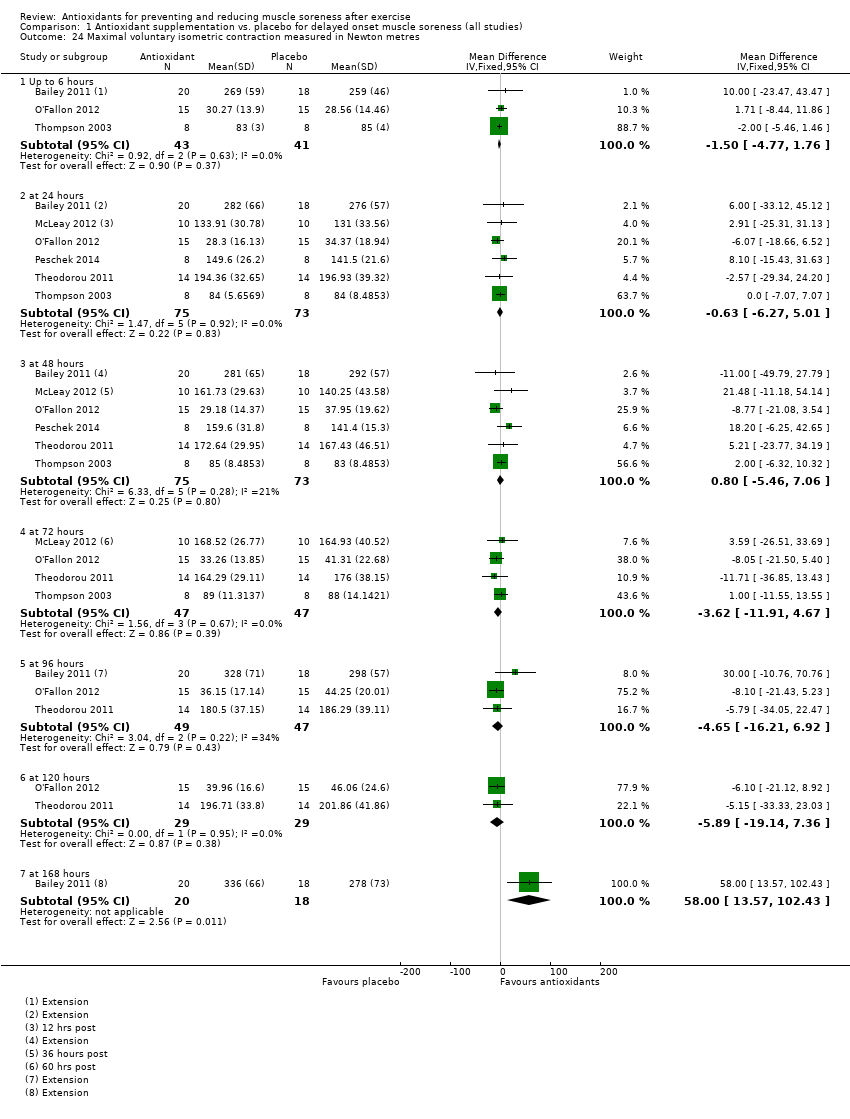
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 24 Maximal voluntary isometric contraction measured in Newton metres.
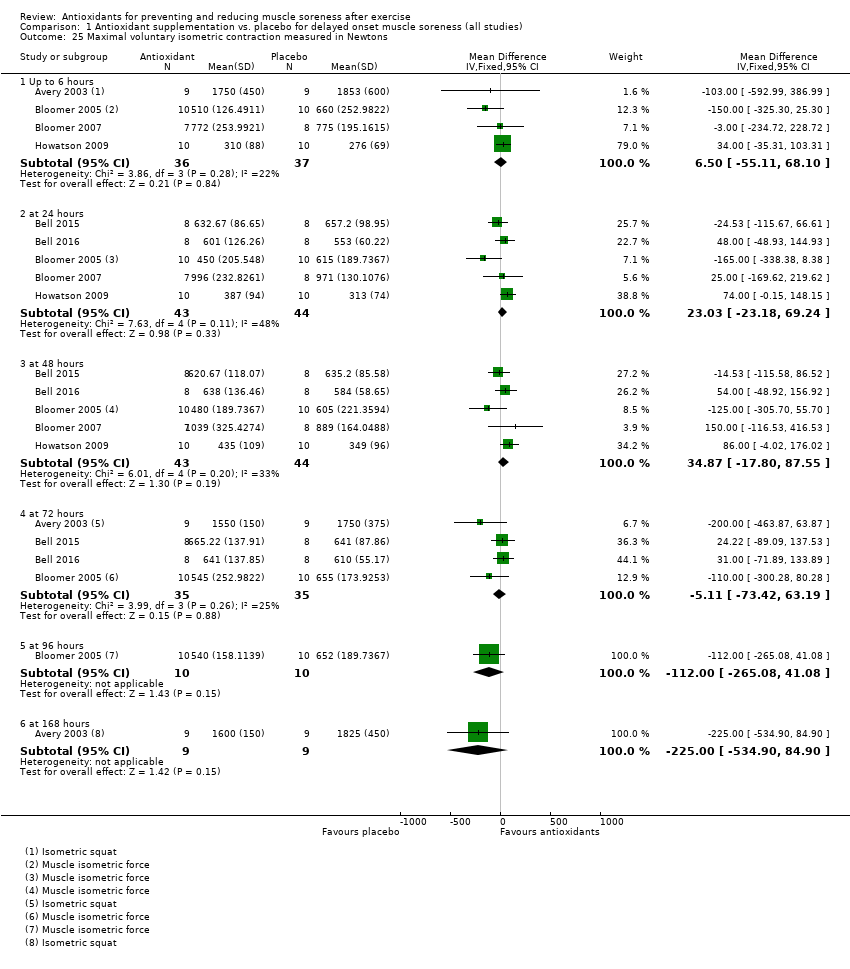
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 25 Maximal voluntary isometric contraction measured in Newtons.
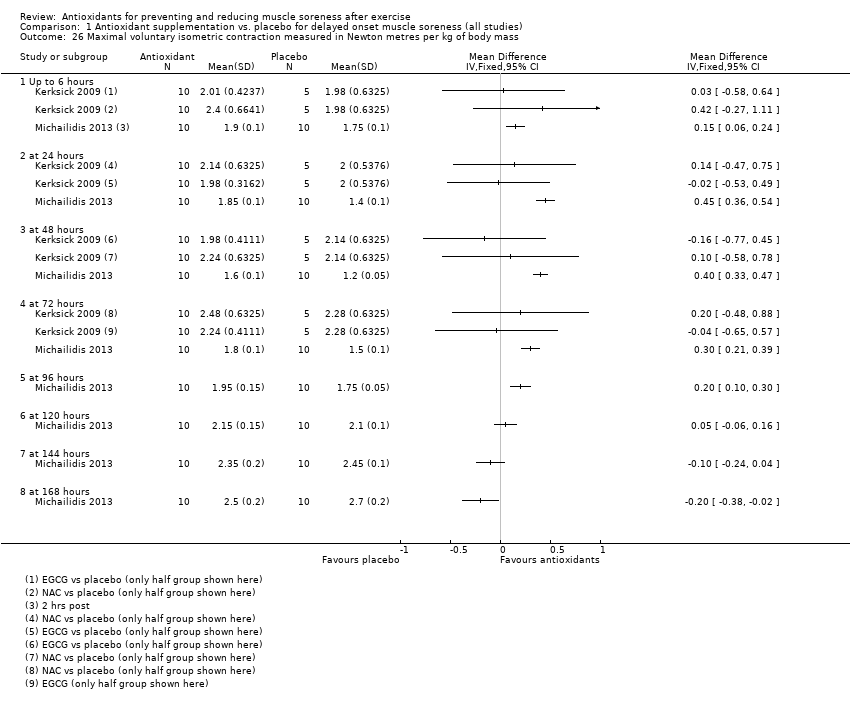
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 26 Maximal voluntary isometric contraction measured in Newton metres per kg of body mass.
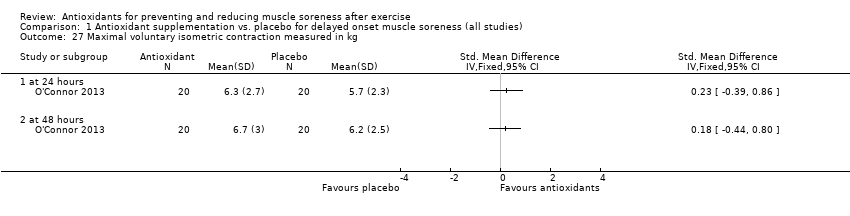
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 27 Maximal voluntary isometric contraction measured in kg.
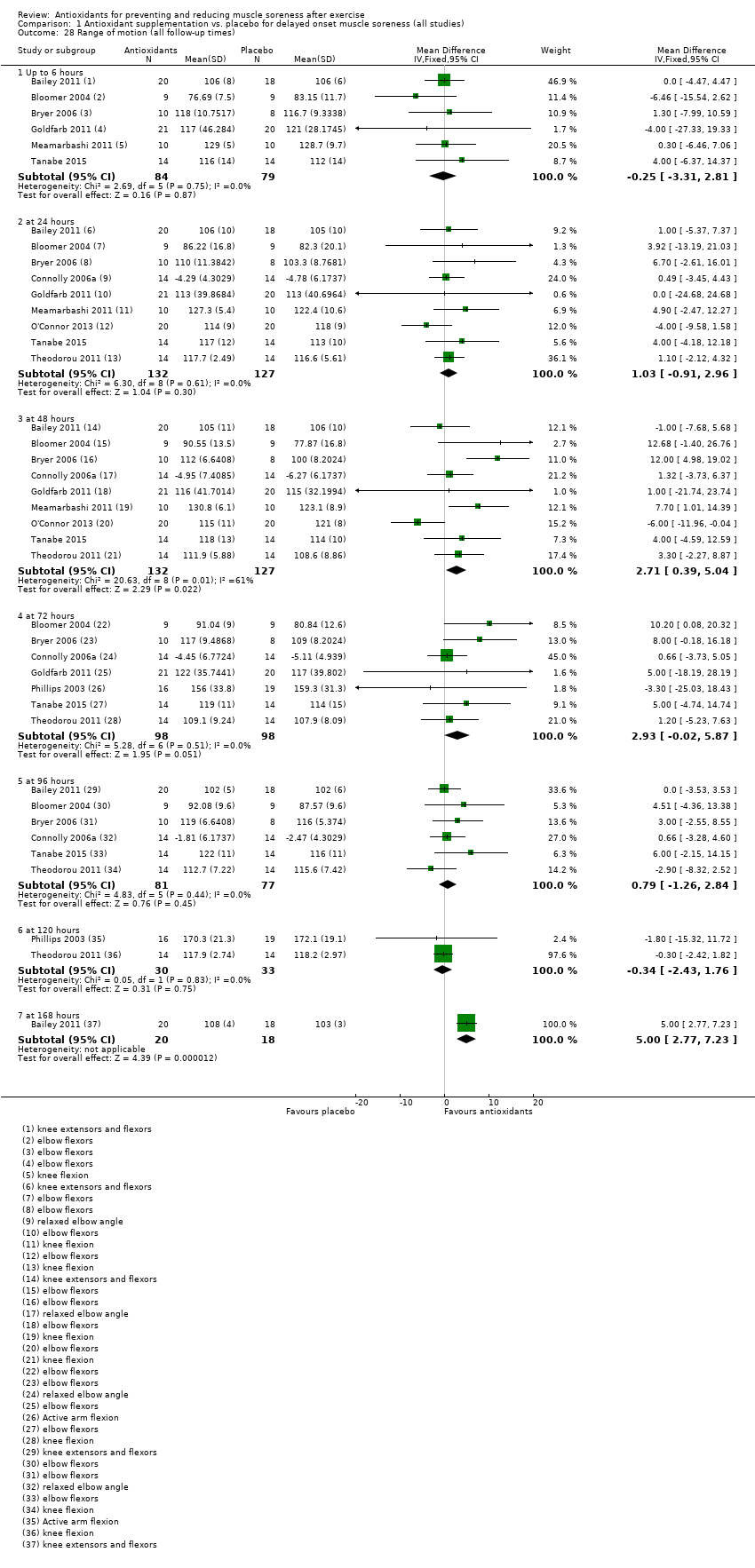
Comparison 1 Antioxidant supplementation vs. placebo for delayed onset muscle soreness (all studies), Outcome 28 Range of motion (all follow‐up times).
| Antioxidants compared with placebo or no treatment for preventing and reducing muscle soreness after exercise | ||||||
| Patient or population: mainly physically active individuals1 partaking in exercise2 designed to produce delayed onset muscle soreness Settings: controlled laboratory studies and field‐based studies Intervention: antioxidant supplements3. These fell into 3 main categories: whole natural food source (e.g. bilberry juice, cherry, pomegranate juice); antioxidant extract or mixed antioxidants (e.g. black tea extract, curcumin); and vitamin C or E or both combined. Comparison: all were placebo controls | ||||||
| Outcomes | Illustrative comparative risks (95% CI) | Relative effect (95% CI) | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (placebo or no antioxidants) | Antioxidant supplementation | |||||
| Muscle soreness Follow‐up: immediately up to 6 hours post‐exercise | The mean level of muscle soreness in the control group ranged from 1.0 to 8.3 cm (adjusted to a 0 to 10 cm scale) | The mean level of muscle soreness after antioxidant supplementation was 0.30 standard deviations lower | SMD ‐0.30 (‐0.56 to ‐0.04) | 525 | ⊕⊕⊝⊝ | One 'rule of thumb' is that 0.2 represents a small difference, 0.5 a moderate difference and 0.8 a large difference. Based on this 'rule of thumb', this result equates to a small to moderate difference in favour of antioxidant supplementation. However, when we rescaled the data to a 0 to 10 cm scale, the MD was lower by 0.52 cm (0.95 to 0.08 cm lower). These are all under the typical MID for pain (taken here as 1.4 cm). |
| Muscle soreness Follow‐up: 24 hours | The mean level of muscle soreness in the control group ranged from 0.21 to 8.8 cm (adjusted to a 0 to 10 cm scale) | The mean level of muscle soreness after antioxidant supplementation was 0.13 standard deviations lower | SMD ‐0.13 (‐0.27 to ‐0.00) | 936 | ⊕⊕⊕⊝ | Based on the above 'rule of thumb', this result equates to a small difference in favour of antioxidant supplementation. However, when we rescaled the data to a 0 to 10 cm scale, the MD was lower by 0.17 cm (0.42 lower to 0.07 higher). These are all under the typical MID for pain (taken here as 1.4 cm). |
| Muscle soreness Follow‐up: 48 hours | The mean level of muscle soreness in the control group ranged from 0.32 to 9.56 cm (adjusted to a 0 to 10 cm scale) | The mean level of muscle soreness after antioxidant supplementation was 0.24 standard deviations lower | SMD ‐0.24 (‐0.42 to ‐0.07) | 1047 | ⊕⊕⊝⊝ | Based on the above 'rule of thumb', this result equates to a small difference in favour of antioxidant supplementation. However, when we rescaled the data to a 0 to 10 cm scale, the MD was lower by 0.41 cm (0.69 to 0.12 lower). These are all under the typical MID for pain (taken here as 1.4 cm). |
| Muscle soreness Follow‐up: 72 hours | The mean level of muscle soreness in the control group ranged from 0.5 to 8.5 cm (adjusted to a 0 to 10 cm scale) | The mean level of muscle soreness after antioxidant supplementation was 0.19 standard deviations lower | SMD ‐0.19 (‐0.38 to ‐0.00) | 657 | ⊕⊕⊕⊝ | Based on the above 'rule of thumb', this result equates to a small difference in favour of antioxidant supplementation. When we rescaled the data to a 0 to 10 cm scale, the MD was lower by 0.29 cm (0.59 lower to 0.02 higher). These are all under the typical MID for pain (taken here as 1.4 cm). |
| Muscle soreness Follow‐up: 96 hours | The mean level of muscle soreness in the control group ranged from 0.2 to 5.6 cm (adjusted to a 0 to 10 cm scale) | The mean level of muscle soreness after antioxidant supplementation was 0.05 standard deviations lower | SMD ‐0.05 (‐0.29 to 0.19) | 436 | ⊕⊕⊝⊝ | Based on the above 'rule of thumb', this result equates to a small difference in favour of antioxidant supplementation but also includes a small effect in favour of placebo or no antioxidants. However, when we rescaled the data to a 0 to 10 cm scale, the MD was lower by 0.03 cm (0.43 lower to 0.37 higher). These are all under the typical MID for pain (taken here as 1.4 cm). |
| Subjective recovery | See comment | See comment | — | See comment | — | None of the 50 studies included in this review measured subjective recovery (return to previous activities without signs or symptoms). |
| Adverse events | See comment | See comment | — | See comment 9 studies | ⊕⊝⊝⊝ | Adverse effects were considered in only 9 studies and actual events reported in 2 studies. One study reported that all 6 participants in the antioxidant supplementation group10 had diarrhoea (5 mild, 1 severe); 4 participants also reported mild indigestion. One placebo group participant also had mild indigestion. The second study reported mild gastrointestinal distress in 1 of 26 participants taking the antioxidant supplement. |
| CI: confidence interval; RR: risk ratio; MD: mean difference; MID: minimal important difference; SMD: standardised mean difference | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Although some participants were sedentary, the majority of participants were recreationally active or moderately trained athletes. No data were included from highly trained elite athletes. Most trial participants were male. 2Muscle damage was induced either mechanically (e.g. resistance‐based exercise) or through whole body aerobic exercise (e.g. running, cycling, bench stepping). 3Typically, supplementation was taken before, the day of and after exercise for up to several days. The supplements were all taken orally, either as capsules, powders or drinks. All studies used an antioxidant dosage higher than the recommended daily amount. 4In this analysis, one study tested two antioxidants compared with placebo control. 5We downgraded the quality of evidence one level for serious study limitations (high/unclear risk of bias) and one level for serious inconsistency. 6We downgraded the quality of evidence one level for serious study limitations (high/unclear risk of bias). 7In this analysis, two studies tested two antioxidants compared with placebo control. 8We downgraded the quality of evidence one level for serious study limitations (high/unclear risk of bias) and one level for serious inconsistency. 9We downgraded the quality of evidence three levels for very serious study limitations, in particular reflecting bias relating failure to record or report on adverse events by the majority of trials. 10Notably the antioxidant used was NAC (N‐acetylcysteine), which is a prescription medicine with antioxidant properties. Listed side effects of NAC include nausea, vomiting and diarrhoea or constipation. | ||||||
| Study ID | Antioxidant (type: Ex; Vit; Whole)* | Dose** | Form taken | Regimen | Started: before exercise | Duration |
| Ex: black tea extract; theaflavin | 700 mg/day | Capsule | 4 capsules daily | 9 days | 11 days | |
| Vit: vitamin E | 992 mg (1200 IU)/day | Capsule | Not known (daily) | 21 days | 31 days | |
| Ex: mixed supplement: vitamins C, E, B6, B9, B12 and zinc | 400 mg vitamin C | Capsule | 1 capsule daily | 42 days | 6 weeks | |
| Vit: vitamin E | 1200 IU | Capsule | ? | 30 days | 30 days | |
| Whole: tart cherry | 9.2 mg/mL anthocyanins | Drink | 30 mL twice daily | 3 days | 8 days | |
| Whole: tart cherry | 73.5 mg/L total anthocyanin content | Drink | 30 mL twice daily | 4 days | 7 days | |
| Vit: vitamin C, E and selenium | 268 mg vitamin E 1 g vitamin C 90 µg selenium | Capsule | 3 capsules daily | 14 days | 18 days | |
| Ex: astaxanthin | 4 mg astaxanthin 480 mg lutein | Capsule | 2 capsules daily | 21 days | 25 days | |
| Vit: vitamin C and E | 1000 mg of vitamin C 378 mg vitamin E | Capsule | 2 capsules daily | 14 days | 14 days | |
| Vit: vitamin C | 3 g/day vitamin C | Capsule | 3 capsules daily | 14 days | 18 days | |
| Vit: vitamin C | 1 g/day vitamin C | ? | ? | 0 days (day of exercise) | 14 days | |
| Ex: N‐acetyl‐cysteine | 50 mg/kg/day | Powder dissolved in water | 50 mg/kg/day once daily dissolved in 500 mL water | 1 hour | 6 days | |
| Vit: vitamin C | 1 g/day vitamin C | Capsule | 3 capsules daily | 3 days | 8 days | |
| Whole: cherry | 600 mg phenolic compounds 40 mg anthocyanins | Drink | 2 x 12 oz bottle daily | 4 days | 8 days | |
| Ex: curcumin | 400 mg/day curcumin | Capsule | 2 capsules daily | 2 days | 5 days | |
| Ex: Juice Plus powder | 7.5 mg beta‐carotene 276 mg vitamin C | Capsule | 6 capsules daily | 4 days | 8 days | |
| Vit: vitamin C and vitamin E | 100 mg of vitamin C 268 mg (400 IU) of vitamin E | Capsule | ? | 14 days | 17 days | |
| Ex: black and green tea | High‐dose = 2000 mg per Low‐dose = 1000 mg per day polyphenolic blend | Capsule | 4 capsules daily | 91 days | 91 days | |
| Whole: cherry | 600 mg phenolic compounds expressed as gallic acid equivalents, 32 g of carbohydrate and at least 40 mg of anthocyanins | Drink | 2 x 8 fl oz bottles per day | 5 days | 7 days | |
| Whole: blackcurrant nectar | 193.25 mg/day of malvidin glucosides 175.69 mg/day of cyanidin glucosides | Drink | 16 oz bottle per day | 8 days | 8 days | |
| Vit: vitamin C | 1 g/day vitamin C | Capsule | 3 capsules daily | 3 days | 10 days | |
| Ex: N‐acetyl‐cysteine and epigallocatechin gallate (EGCG) | 1800 mg/day N‐acetyl‐cysteine (NAC) 1800 mg/day epigallocatechin gallate (EGCG) | Drink | ? | 14 days | 14 days | |
| Ex: pollen extract | 30,000 units per gram of Polbax | ? | ? | 28 days | 28 days | |
| Whole: cherry | 600 mg phenolic compounds 40 mg anthocyanins | Drink | 2 x 335 mL bottles daily | 7 days | 15 days | |
| Ex: resveratrol | 600 mg/day of resveratrol | Capsules | 6 capsules daily | 7 days | 9 days | |
| Whole: bilberry juice | Total phenol content per 200 mL serving was 744.14 ± 81.75 mg (n = 3) and 80.04 ± 3.51 mg (n = 3) of total anthocyanins | Drink | 2 x 200 mL daily | 5 days | 8 days | |
| Vit: vitamin E | 992 mg/day of vitamin E (1200 IU) | Capsules | 1 capsule daily | 14 days | 14 days | |
| Whole: cherry | 9.117 mg/mL anthocyanins | Drink | 90 mL daily (2 x 30 mL) | 6 days | 6 days | |
| Ex: curcumin | 400 mg/day curcumin | Capsules | Capsules | 2 days | 6 days | |
| Whole: blueberry smoothie | Per 100 mL: total phenolics 168 mg/gallic acid equ.; anthocyanins 96.6 mg; phenolic acid 26 mg, | Drink | 200 g blueberries, 50 g banana + 200 mL apple juice daily | 0 days (day of exercise) | 4 days | |
| Ex: purslane extract | 1200 mg/day purslane extract | Capsules | 2 capsules daily | 3 days | 5 days | |
| Vit: N‐acetyl‐cysteine | 20 mg/kg/day N‐acetyl‐cysteine | Drink | 3 x 500 mL drink daily | 0 days (day of exercise) | 9 days | |
| Ex: curcumin | 2.5 g/day of curcumin | Capsules | 10 capsules daily (2 x 5 capsules) | 2.5 days | 5 days | |
| Vit: vitamin C | 800 mg/day vitamin C | Capsules | ? | 3 hours | 2 days | |
| Whole: grape juice | 1.75 mg/kg resveratrol 19.7 mg/kg catechin 12.6 mg/kg 31.7 mg/kg peonidin 125 mg/kg cyanidin 145.2 mg/kg 32.6 mg/kg quercetin 5.6 mg/kg kaempferol 6.8 mg/kg isorhamnetin | Drink (dissolved powder) | 1 serving of powder daily mixed with 236 mL of water | 45 days | 50 days | |
| Ex: quercetin | 1000 mg/day quercetin | Bar | 2 bars daily | 7 days | 7 days | |
| Whole: cocoa | 350 mg/day flavanols | Drink | 240 mL daily | 0 days (day of exercise) | 3 days | |
| Ex: mixed antioxidants | 300 mg/day tocopherols 800 mg/day docosahexaenoate 300 mg/day flavonoids of which was 100 mg hesperetin and 200 mg quercetin | Capsules | Vitamin E: 1 capsule; docosahexaenoate: 3 capsules; flavonoids: 3 capsules | 14 days | 14 days | |
| Vit: vitamin C + vitamin E | 500 mg/day vitamin C 992 mg/day (1200 IU/day) vitamin E | Capsules | ? | ? | 37 days | |
| Ex: N‐acetyl‐cysteine | 10 mg/kg/day of body mass N‐acetyl‐cysteine | Capsules | 1 capsule daily | 14 days | 21 days | |
| Vit: vitamin E | 536 mg/day (800 IU/day) vitamin E | Capsules | 1 capsule daily | 14 days | 21 days | |
| Ex: allicin | 80 mg/day allicin | Capsules | Capsules | 14 days | 16 days | |
| Ex: curcumin | 150 mg/day curcumin | Capsules | 6 capsules daily | 0 days (day of exercise; 1 hour before) | 1 day | |
| Vit: vitamin C + vitamin E | 1 g/day vitamin C 268 mg/day (1200 IU/day) vitamin E | Capsules | 1 capsule daily | 28 days | 77 days | |
| Vit: vitamin C | 1 g/day vitamin C | Drink | ? | 0 days (day of exercise; 2 hours before) | 1 day | |
| Vit: vitamin C | 1 g/day of vitamin C on day 1 followed by 400 mg/day divided into 2 doses for 12 days | Drink and capsules | 1 g given in a solution followed by 400 mg/day doses in capsules | 14 days | 14 days | |
| Vit: vitamin C | 200 mg/day vitamin C | Drink | Daily drink | 0 days (day of exercise) | 3 days | |
| Vit: vitamin C | 200 mg/day vitamin C | Drink | Daily drink | 14 days | 14 days | |
| Whole: pomegranate juice | 650 mg/day polyphenols, consisting of 95.5% ellagitannins, 3.5% ellagic acid and 1% anthocyanins | Drink | 960 mL per day (as 2 x 480 mL drinks) | 9 days | 32 days | |
| Whole: pomegranate juice | 3958 mg/L of tannins 768 mg/L anthocyanins 242 mg/L of ellagic derivatives | Drink | 500 mL per day (as 2 x 250 mL drinks) | 15 days | 44 days | |
| * Types: Extract, mixed or other (e.g. amino‐acid derivative) antioxidants; Vitamin; and Whole natural food source. | ||||||
| Study ID | Outcome measure | Score (higher = worse) | Timing post‐exercise | Data extraction |
| Muscle soreness during a squat | VAS (0 to 10 cm) | 24, 48 hours | Text (SDs from SEs) | |
| Muscle soreness during shoulder abduction, shoulder horizontal adduction and hip flexion (unloaded squat) | VAS (0 to 10 cm) | 24, 48, 72 hours | Text | |
| General soreness at the quadriceps | VAS (1 to 10 cm) | 24, 48 hours | Text | |
| General soreness at the quadriceps | VAS (0 to 10 cm) | 48 hours | Text | |
| Muscle soreness during a squat | VAS (0 to 200 mm) | 24, 48, 72 hours | Raw data provided by the authors | |
| Muscle soreness during a squat | VAS (0 to 200 mm) | 24, 48, 72 hours | Raw data provided by the authors | |
| Active movement of elbow flexion or extension, as well as following light palpitation by the investigators | VAS (0 to 10 cm) | 0, 2, 6, 24, 48, 72, 96 hours | Raw data provided by the authors | |
| Dominant leg during knee extension | VAS (0 to 10 cm) | 0, 10, 24, 48, 72, 96 hours | Raw data provided by the authors Immediate pain data used for the up to 6 hours analysis | |
| Performance of 2 (concentric‐eccentric) repetitions of the barbell bench press exercise using a standard 20 kg barbell | VAS (0 to 10 cm) | 0, 24, 48 hours | Raw data provided by the authors | |
| Delayed onset muscle soreness was assessed in a rested position and in response to palpation on the muscle of the arms | VAS (1 to 10 cm) | 0, 4, 24, 48, 72, 96 hours | Text (SDs from SEs) Immediate pain data used for the up to 6 hours analysis | |
| Delayed onset muscle soreness was measured at the gastrocnemius, anterior tibialis, hamstrings, quadriceps, gluteals (both sides) and lower back muscles | VAS (0 to 10 cm) | 0, 24, 48, 72, 96, 168, 336 hours | Raw data provided by the authors Immediate pain data used for the up to 6 hours analysis | |
| Total muscle soreness after performing a 90 degree squat | VAS (0 to 12 cm) | 0, 24, 48, 50, 72, 96, 98 hours | Raw data provided by the authors Immediate pain data used for the up to 6 hours analysis | |
| General delayed onset muscle soreness assessed at the quadriceps | VAS (0 to 10 cm) | 24, 48, 72, 96 hours | Text | |
| Pain scores were obtained by asking participants to verbally rate their overall discomfort during active elbow flexion and extension | VAS (0 to 10 cm) | 24, 48, 72, 96 hours | Text (SDs from SEs) | |
| Muscle soreness during descending and climbing stairs. The following 8 sites were measured: anterior right thigh, posterior right thigh, anterior right leg, posterior right leg, anterior left thigh, posterior left thigh, anterior left leg, posterior left leg and added together for a total score. | VAS (0 to 4) | 48 hours | Raw data provided by the authors | |
| Delayed onset muscle soreness was measured at the elbow flexor with the arm rested | VAS (1 to 10 cm) | 0, 2, 6, 24, 48, 72 hours | Text (SDs from SEs) Immediate pain data used for the up to 6 hours analysis | |
| Delayed onset muscle soreness of the quadriceps, hamstrings, gluteus, gastrocnemius and tibialis anterior | VAS (0 to 6) | 0, 24, 48, 72 hours | Raw data provided by the authors Immediate pain data used for the up to 6 hours analysis | |
| Soreness was assessed in a variety of muscle groups including the gastrocnemius, hamstrings, quadriceps, gluteus maximus, lower back, abdominals and the whole body | Likert (0 to 7) | 24, 48, 72, 96 hours | The authors of Herrlinger 2015 were contacted on 2 February 2017 and again on 18February 2017 for missing data as these were not available in the manuscript and could not be extracted from graphs. No response was received and this study was therefore included in the qualitative analysis but not the quantitative analysis. | |
| Squat down to 90 degrees (internal joint angle) rise to the start position | VAS (0 to 200 mm) | 0, 24, 48 hours | Text Immediate pain data used for the up to 6 hours analysis | |
| Full range squat with no external weight | VAS (0 to 10 cm) | 24, 48, 72 hours | Text (SDs from SEs) | |
| General delayed onset muscle soreness was monitored by self‐reporting | VAS (1 to 10 cm) | 0, 10, 24, 48, 58, 72, 96 hours | Raw data provided by the authors Immediate pain data used for the up to 6 hours analysis | |
| Delayed onset muscle soreness was assessed at the quadriceps | VAS (0 to 10 cm) | 6, 24, 48 hours | Raw data provided by the authors 6 hours post‐exercise data used for the up to 6 hours analysis | |
| General soreness | VAS (0 to 10 cm) | 24, 48, 72, 96, 120 hours | Text (SDs from SEs) | |
| General soreness in the legs | VAS (0 to 100 mm) | 0 hours | Text Immediate pain data used for the up to 6 hours analysis | |
| General soreness in both legs | VAS (0 to 10 cm) | 24 hours | Raw data provided by the authors | |
| Squat to a 90 angle and returning to a standing position | VAS (0 to 200 mm) | 0, 24, 48 hours | Text Immediate pain data used for the up to 6 hours analysis | |
| General soreness | VAS (0 to 10 cm) | 24, 48 hours | Text (SDs from SEs) | |
| Upper body, upper legs, lower legs and overall body | VAS (0 to 10 cm) | 24, 48, 72, 96, 120, 144 hours | This study was only included in the qualitative analysis because the exercise paradigm was completely different to all the other studies included in this review | |
| Muscle soreness measured using a gauge. Pressure was applied using standard force (20 to 30 N) over the distal, middle and proximal thigh in a seated position with the knee fully extended and relaxed. The 3 ratings for each quadricep were added together. | VAS (0 to 10 cm) | 24, 48, 72, 96 hours | Text (SDs from SEs) | |
| Step up (concentric muscle action) onto a 40 cm box then step down (eccentric muscular contraction) and the soreness was rated | VAS (0 to 10 cm) | 24, 48, 72 hours | Text | |
| Participants were requested to rate the general discomfort in only the quadriceps and calf regions of the right leg | VAS (0 to 6) | 0, 24, 48 hours | Text Immediate pain data used for the up to 6 hours analysis | |
| Palpation of the muscle belly and the distal region of the vastus medialis, vastus lateralis and rectus femoris after a squat | VAS (1 to 10 cm) | 0, 2, 24, 48, 72, 96, 120, 144, 168 hours | Text Immediate pain data used for the up to 6 hours analysis | |
| Pain was rated for single leg squat, walking downstairs, passive strength of the gluteals and single leg vertical jump | VAS (0 to 10 cm) | 0, 24, 48 hours | Raw data provided by the authors Immediate pain data used for the up to 6 hours analysis | |
| Perceived soreness was done during quadriceps extension | VAS (0 to 10 cm) | 0, 24, 48 hours | Text Immediate pain data used for the up to 6 hours analysis | |
| Delayed onset muscle soreness in the arm was rated in response to isometric strength measurement | VAS (0 to 100 mm) | 24, 48 hours | Text | |
| Delayed onset muscle soreness at the elbow flexor | VAS (0 to 100 mm) | 24, 48, 72, 96, 120 hours | Raw data provided by the authors | |
| Delayed onset muscle soreness at the legs | VAS (0 to 10 cm) | 24, 48 hours | Text | |
| Soreness measures were subjectively evaluated through palpitation for oedema at he elbow | VAS (0 to 10 cm) | 72, 168 hours | Text (SDs from SEs) | |
| Delayed onset muscle soreness was evaluated using a questionnaire employing a visual analogue scale for a total of 8 sites (6 sites on the anterior muscle of the upper leg and 2 sites on the posterior muscles of the upper leg). The participants were asked to palpate the relaxed muscle and rate soreness. | VAS (1 to 10 cm) (x 8): 8 to 80 score | 24, 48 hours | Text | |
| Delayed onset muscle soreness at the elbow flexor | VAS (0 to 10 cm) | 48, 96, 168 hours | Text | |
| Muscle soreness of the biceps muscle was assessed | VAS (0 to 10 cm) | 48, 96, 168 hours | Text (SDs from SEs) | |
| At the beginning of the exercise test, participants were instructed to give CR‐10 values | Borg CR (0‐10) | 0, 24, 48 hours | Text (SDs from SEs) Immediate pain data used for the up to 6 hours analysis | |
| Palpitation of the upper arm and passively extending the elbow joint | VAS (0 to 100 mm) | 0, 24. 48, 72, 96 hours | Raw data provided by the authors Immediate pain data used for the up to 6 hours analysis | |
| Squat using body weight | VAS (0 to 10 cm) | 24, 48, 72, 96, 120 hours | Text | |
| Actively contracted the quadriceps | VAS (1 to 10 cm) | 24, 48, 72 hours | Text (SDs from SEs); there are no decimal places; where SE = 0, we have put this as 0.4 (SD = 1.2) | |
| Actively contracted the quadriceps | VAS (0 to 100 mm) | 24, 48, 72 hours | Text (SDs from SEs) | |
| Actively contracted the quadriceps | VAS (1 to 10 cm) | 24, 48, 72 hours | Text (SDs from SEs); there are no decimal places; where SE = 0, we have put this as 0.4 (SD = 1.1313) | |
| Actively contracting the leg extensors against resistance equivalent to 75% of each individual's 1 repetition maximum | VAS (0 to 10 cm) | 24, 48, 72 hours | Raw data provided by the authors | |
| Unloaded elbow flexion of the tested arm | VAS (0 to 10 cm) | 2, 24, 48, 72, 96 hours | Raw data provided by the authors 2 hours post‐exercise data used for the up to 6 hours analysis | |
| Unloaded elbow flexion and knee extension on the tested arm and leg | VAS (0 to 10 cm) | 2, 24, 48, 72, 96 hours | Raw data provided by the authors 2 hours post‐exercise data used for the up to 6 hours analysis | |
| SD: standard deviation | ||||
| Follow‐up times | No. studies | No. participants | SMD (95% CI) |
| Up to 6 hours | 21 | 525 | ‐0.31 (‐0.49 to ‐0.13) |
| 24 hours | 41 | 936 | ‐0.13 (‐0.26 to ‐0.00) |
| 48 hours | 45 | 1047 | ‐0.22 (‐0.34 to ‐0.09) |
| 72 hours | 28 | 657 | ‐0.17 (‐0.33 to ‐0.02) |
| 96 hours | 17 | 436 | ‐0.04 (‐0.23 to 0.16) |
| 120 hours | 4 | 128 | 0.25 (‐0.12 to 0.61) |
| 144 hours | 1 | 20 | ‐0.23 (‐1.11 to 0.65) |
| 168 hours | 4 | 80 | ‐0.04 (‐0.48 to 0.41) |
| CI: confidence interval | |||
| Follow‐up times | All studies | Parallel group studies only | ||
| No. studies | SMD (95% CI) | No. studies | SMD (95% CI) | |
| Up to 6 hours | 21 | ‐0.30 (‐0.56 to ‐0.04) | 15 | ‐0.35 (‐0.67 to ‐0.03) |
| 24 hours | 41 | ‐0.13 (‐0.27 to 0.00) | 32 | ‐0.08 (‐0.25 to 0.08) |
| 48 hours | 45 | ‐0.24 (‐0.42 to ‐0.07) | 34 | ‐0.19 (‐0.40 to 0.01) |
| 72 hours | 28 | ‐0.19 (‐0.38 to ‐0.00) | 22 | ‐0.11 (‐0.30 to 0.08) |
| 96 hours | 17 | ‐0.05 (‐0.29 to 0.19) | 12 | 0.01 (‐0.33 to 0.34) |
| Table produced independently of the authors by Newton Opiyo and checked by Helen Handoll | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Muscle soreness up to 6 hours; random‐effects model Show forest plot | 21 | 525 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.30 [‐0.56, ‐0.04] |
| 2 Muscle soreness at 24 hours; random‐effects model Show forest plot | 41 | 936 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.27, 0.00] |
| 3 Muscle soreness at 48 hours; random‐effects model Show forest plot | 45 | 1047 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.24 [‐0.42, ‐0.07] |
| 4 Muscle soreness at 72 hours; random‐effects model Show forest plot | 28 | 657 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.19 [‐0.38, ‐0.00] |
| 5 Muscle soreness at 96 hours; random‐effects model Show forest plot | 17 | 436 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.05 [‐0.29, 0.19] |
| 6 Muscle soreness (follow‐ups: 120, 144 and 168 hours); random‐effects model Show forest plot | 7 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 6.1 at 120 hours | 4 | 128 | Std. Mean Difference (IV, Random, 95% CI) | 0.21 [‐0.26, 0.69] |
| 6.2 at 144 hours | 1 | 20 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.23 [‐1.11, 0.65] |
| 6.3 at 168 hours | 4 | 80 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.04 [‐0.48, 0.41] |
| 7 Muscle soreness up to 6 hours ‐ all at same scale (0 to 10; worst pain) Show forest plot | 21 | 525 | Mean Difference (IV, Random, 95% CI) | ‐0.52 [‐0.95, ‐0.08] |
| 8 Muscle soreness at 24 hours ‐ all at same scale (0 to 10; worst pain) Show forest plot | 41 | 936 | Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.42, 0.07] |
| 9 Muscle soreness at 48 hours ‐ all at same scale (0 to 10; worst pain) Show forest plot | 45 | 1047 | Mean Difference (IV, Random, 95% CI) | ‐0.41 [‐0.69, ‐0.12] |
| 10 Muscle soreness at 72 hours ‐ all at same scale (0 to 10; worst pain) Show forest plot | 28 | 657 | Mean Difference (IV, Random, 95% CI) | ‐0.29 [‐0.59, 0.02] |
| 11 Muscle soreness at 96 hours ‐ all at same scale (0 to 10; worst pain) Show forest plot | 17 | 436 | Mean Difference (IV, Random, 95% CI) | ‐0.03 [‐0.43, 0.37] |
| 12 Muscle soreness at 24 hours. Subgroup analysis by type of exercise (whole body aerobic vs. mechanically induced) Show forest plot | 41 | 936 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.27, 0.00] |
| 12.1 Whole body aerobic exercise | 17 | 338 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐0.33, 0.18] |
| 12.2 Mechanically induced | 24 | 598 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.18 [‐0.34, ‐0.01] |
| 13 Muscle soreness at 48 hours. Subgroup analysis by type of exercise (whole body aerobic vs. mechanically induced) Show forest plot | 45 | 1047 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.24 [‐0.42, ‐0.07] |
| 13.1 Whole body aerobic exercise | 17 | 349 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.12 [‐0.47, 0.23] |
| 13.2 Mechanically induced | 28 | 698 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.31 [‐0.50, ‐0.12] |
| 14 Muscle soreness at 24 hours. Subgroup analysis by funding sources (funded by food company or provider of antioxidant supplements vs. not funded by food company or provider of antioxidant supplements) Show forest plot | 40 | 920 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.13 [‐0.26, 0.01] |
| 14.1 Company funding | 17 | 427 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.11 [‐0.31, 0.08] |
| 14.2 Other funding | 23 | 493 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.14 [‐0.32, 0.05] |
| 15 Muscle soreness at 48 hours. Subgroup analysis by funding sources (funded by food company or provider of antioxidant supplements vs. not funded by food company or provider of antioxidant supplements) Show forest plot | 44 | 1031 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.21 [‐0.34, ‐0.09] |
| 15.1 Company funding | 18 | 443 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.19 [‐0.38, 0.00] |
| 15.2 Other funding | 26 | 588 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.23 [‐0.40, ‐0.06] |
| 16 Muscle tenderness measured in Newtons (all follow‐up times) Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.1 at 24 hours | 2 | 52 | Mean Difference (IV, Fixed, 95% CI) | ‐1.60 [‐7.64, 4.45] |
| 16.2 at 48 hours | 2 | 52 | Mean Difference (IV, Fixed, 95% CI) | ‐2.14 [‐9.48, 5.19] |
| 16.3 at 72 hours | 2 | 52 | Mean Difference (IV, Fixed, 95% CI) | ‐0.34 [‐6.55, 5.86] |
| 16.4 at 96 hours | 2 | 52 | Mean Difference (IV, Fixed, 95% CI) | ‐2.32 [‐9.62, 4.99] |
| 17 Muscle tenderness measured in kg (all follow‐up times) Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 17.1 Up to 6 hours | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | ‐0.61 [‐14.10, 12.88] |
| 17.2 at 24 hours | 2 | 36 | Mean Difference (IV, Fixed, 95% CI) | 0.53 [‐0.95, 2.01] |
| 17.3 at 48 hours | 2 | 36 | Mean Difference (IV, Fixed, 95% CI) | 0.52 [‐1.08, 2.13] |
| 17.4 at 72 hours | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | ‐1.03 [‐13.01, 10.95] |
| 17.5 at 96 hours | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | ‐1.39 [‐15.12, 12.33] |
| 18 30‐second Wingate average peak power output (W/kg) (post 7 days of intervention) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 19 20 m Sprint time (s) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 19.1 at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.2 at 48 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.3 at 120 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 20 Maximal oxygen consumption (mL/kg/min) (post 42 days of supplementation) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 21 Agility (seconds) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 21.1 at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.2 at 48 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.3 at 72 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 22 6 second sprint maximal power (Watts) (all follow‐up times) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 22.1 at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.2 at 48 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 22.3 at 72 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23 Maximal voluntary isometric contraction measured as percentage change from baseline Show forest plot | 15 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 23.1 Up to 6 hours | 11 | 255 | Mean Difference (IV, Fixed, 95% CI) | 5.86 [3.29, 8.42] |
| 23.2 at 24 hours | 15 | 375 | Mean Difference (IV, Fixed, 95% CI) | 2.51 [0.99, 4.04] |
| 23.3 at 48 hours | 15 | 375 | Mean Difference (IV, Fixed, 95% CI) | 4.46 [2.94, 5.98] |
| 23.4 at 72 hours | 11 | 277 | Mean Difference (IV, Fixed, 95% CI) | 3.92 [0.88, 6.96] |
| 23.5 at 96 hours | 9 | 252 | Mean Difference (IV, Fixed, 95% CI) | 5.29 [3.65, 6.92] |
| 23.6 at 168 hours | 2 | 36 | Mean Difference (IV, Fixed, 95% CI) | ‐7.96 [‐15.96, 0.05] |
| 24 Maximal voluntary isometric contraction measured in Newton metres Show forest plot | 6 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 24.1 Up to 6 hours | 3 | 84 | Mean Difference (IV, Fixed, 95% CI) | ‐1.50 [‐4.77, 1.76] |
| 24.2 at 24 hours | 6 | 148 | Mean Difference (IV, Fixed, 95% CI) | ‐0.63 [‐6.27, 5.01] |
| 24.3 at 48 hours | 6 | 148 | Mean Difference (IV, Fixed, 95% CI) | 0.80 [‐5.46, 7.06] |
| 24.4 at 72 hours | 4 | 94 | Mean Difference (IV, Fixed, 95% CI) | ‐3.62 [‐11.91, 4.67] |
| 24.5 at 96 hours | 3 | 96 | Mean Difference (IV, Fixed, 95% CI) | ‐4.65 [‐16.21, 6.92] |
| 24.6 at 120 hours | 2 | 58 | Mean Difference (IV, Fixed, 95% CI) | ‐5.89 [‐19.14, 7.36] |
| 24.7 at 168 hours | 1 | 38 | Mean Difference (IV, Fixed, 95% CI) | 58.0 [13.57, 102.43] |
| 25 Maximal voluntary isometric contraction measured in Newtons Show forest plot | 6 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 25.1 Up to 6 hours | 4 | 73 | Mean Difference (IV, Fixed, 95% CI) | 6.50 [‐55.11, 68.10] |
| 25.2 at 24 hours | 5 | 87 | Mean Difference (IV, Fixed, 95% CI) | 23.03 [‐23.18, 69.24] |
| 25.3 at 48 hours | 5 | 87 | Mean Difference (IV, Fixed, 95% CI) | 34.87 [‐17.80, 87.55] |
| 25.4 at 72 hours | 4 | 70 | Mean Difference (IV, Fixed, 95% CI) | ‐5.11 [‐73.42, 63.19] |
| 25.5 at 96 hours | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | ‐112.0 [‐265.08, 41.08] |
| 25.6 at 168 hours | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | ‐225.0 [‐534.90, 84.90] |
| 26 Maximal voluntary isometric contraction measured in Newton metres per kg of body mass Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 26.1 Up to 6 hours | 2 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.2 at 24 hours | 2 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.3 at 48 hours | 2 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.4 at 72 hours | 2 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.5 at 96 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.6 at 120 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.7 at 144 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.8 at 168 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 27 Maximal voluntary isometric contraction measured in kg Show forest plot | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 27.1 at 24 hours | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 27.2 at 48 hours | 1 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 28 Range of motion (all follow‐up times) Show forest plot | 10 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 28.1 Up to 6 hours | 6 | 163 | Mean Difference (IV, Fixed, 95% CI) | ‐0.25 [‐3.31, 2.81] |
| 28.2 at 24 hours | 9 | 259 | Mean Difference (IV, Fixed, 95% CI) | 1.03 [‐0.91, 2.96] |
| 28.3 at 48 hours | 9 | 259 | Mean Difference (IV, Fixed, 95% CI) | 2.71 [0.39, 5.04] |
| 28.4 at 72 hours | 7 | 196 | Mean Difference (IV, Fixed, 95% CI) | 2.93 [‐0.02, 5.87] |
| 28.5 at 96 hours | 6 | 158 | Mean Difference (IV, Fixed, 95% CI) | 0.79 [‐1.26, 2.84] |
| 28.6 at 120 hours | 2 | 63 | Mean Difference (IV, Fixed, 95% CI) | ‐0.34 [‐2.43, 1.76] |
| 28.7 at 168 hours | 1 | 38 | Mean Difference (IV, Fixed, 95% CI) | 5.0 [2.77, 7.23] |