Odgađanje početka nastave u cilju poboljšanja obrazovanja, zdravlja i boljitka učenika srednje škole
Abstract
Background
A number of school systems worldwide have proposed and implemented later school start times as a means of avoiding the potentially negative impacts that early morning schedules can have on adolescent students. Even mild sleep deprivation has been associated with significant health and educational concerns: increased risk for accidents and injuries, impaired learning, aggression, memory loss, poor self‐esteem, and changes in metabolism. Although researchers have begun to explore the effects of delayed school start time, no one has conducted a rigorous review of evidence to determine whether later school start times support adolescent health, education, and well‐being.
Objectives
We aimed to assess the effects of a later school start time for supporting health, education, and well‐being in high school students.
Secondary objectives were to explore possible differential effects of later school start times in student subgroups and in different types of schools; to identify implementation practices, contextual factors, and delivery modes associated with positive and negative effects of later start times; and to assess the effects of later school start times on the broader community (high school faculty and staff, neighborhood, and families).
Search methods
We conducted the main search for this review on 28 October 2014 and updated it on 8 February 2016. We searched CENTRAL as well as 17 key electronic databases (including MEDLINE, Embase, ERIC, PsycINFO, and Sociological Abstracts), current editions of relevant journals and organizational websites, trial registries, and Google Scholar.
Selection criteria
We included any randomized controlled trials, controlled before‐and‐after studies, and interrupted time series studies with sufficient data points that pertained to students aged 13 to 19 years and that compared different school start times. Studies that reported either primary outcomes of interest (academic outcomes, amount or quality of sleep, mental health indicators, attendance, or alertness) or secondary outcomes (health behaviors, health and safety indicators, social outcomes, family outcomes, school outcomes, or community outcomes) were eligible.
Data collection and analysis
At least two review authors independently determined inclusion and exclusion decisions through screening titles, abstracts, and full‐text reports. Two review authors independently extracted data for all eligible studies. We presented findings through a narrative synthesis across all studies. When two or more study samples provided sufficient information to permit effect size calculations, we conducted random‐effects meta‐analyses to synthesize effects across studies.
Main results
Our search located 17 eligible records reporting on 11 unique studies with 297,994 participants; the studies examined academic outcomes, amount and quality of sleep, mental health indicators, attendance, and student alertness. Overall, the quality of the body of evidence was very low, as we rated most studies as being at high or unclear risk of bias with respect to allocation, attrition, absence of randomization, and the collection of baseline data. Therefore, we cannot be confident about the effects of later school start times.
Preliminary evidence from the included studies indicated a potential association between later school start times and academic and psychosocial outcomes, but quality and comparability of these data were low and often precluded quantitative synthesis. Four studies examined the association between later school start times and academic outcomes, reporting mixed results. Six studies examined effects on total amount of sleep and reported significant, positive relationships between later school start times and amount of sleep. One study provided information concerning mental health outcomes, reporting an association between decreased depressive symptoms and later school start times. There were mixed results for the association between later school start times and absenteeism. Three studies reported mixed results concerning the association between later school start times and student alertness. There was limited indication of potential adverse effects on logistics, as the qualitative portions of one study reported less interaction between parents and children, and another reported staffing and scheduling difficulties. Because of the insufficient evidence, we cannot draw firm conclusions concerning adverse effects at this time.
It is important to note the limitations of this evidence, especially as randomized controlled trials and high‐quality primary studies are difficult to conduct; school systems are often unwilling or unable to allow researchers the necessary control over scheduling and data collection. Moreover, this evidence does not speak to the process of implementing later school starts, as the included studies focused on reporting the effects rather than exploring the process.
Authors' conclusions
This systematic review on later school start times suggests several potential benefits for this intervention and points to the need for higher quality primary studies. However, as a result of the limited evidence base, we could not determine the effects of later school start times with any confidence.
PICO
Laički sažetak
Kasniji početak nastave u cilju poboljšanja obrazovanja, zdravlja i boljitka učenika srednje škole
Cilj pregleda
Cilj ovog Cochraneovog sustavnog pregleda literature bio je istražiti utjecaj kasnijeg početka nastave na rezultate u školi, količinu i kvalitetu sna, pokazatelje duševnog zdravlja, te nazočnost i pozornost učenika u srednjim školama.
Dosadašnje spoznaje
Učenici srednjih škola su izloženi većem riziku od manjka sna u usporedbi s ostalim skupinama, što je u podjednakoj mjeri posljedica biokemijskih promjena u njihovom središnjem živčanom sustavu, kao i velikog broja vremenski određenih obaveza, uključujući i početak nastave. Zbog toga smo željeli odrediti postoji li veza između odgode početka nastave i školskog uspjeha, dužeg sna, boljeg duševnog zdravlja, veće nazočnosti ili pozornosti učenika, odnosno sekundarnih rezultata, poput ishrane i tjelovježbe, nesreća, socijalnih aspekata u školi, promjena obiteljske dinamike, upisa u školu ili promjena u zajednici.
Obilježja uključenih istraživanja
Podaci iz ovog preglednog članka uključuju istraživanja dostupna do veljače 2016. godine. Temelje se na 17 radova koji opisuju rezultate 11 studija provedenih na 297.994 školska učenika. U studijama je istraženo više obrazaca promjena vremena nastave (npr. pomicanje početka za petnaest minuta ili za jedan sat). Također se trajanje intervencije razlikovalo u tim istraživanjima, od dva tjedna do godine dana. No, sve studije su uključivale normalne uvjete, odnosno obuhvatile su učenike koji su već u školama. Iako je 5 od 11 studija bilo financirano, to financiranje je primljeno od strane akademskih i istraživačkih institucija, a ne agencija koje imaju komercijalne interese od rezultata.
Ključni rezultati
Budući su dokazi bili ograničeni i vrlo niske kvalitete, nismo mogli pouzdano odrediti učinke kasnijeg početka nastave. Pokazali smo da je moguće da kasniji početak nastave ima povoljan učinak na školski uspjeh. Međutim, ezultata četiriju studija daju različite zaključke. U dvjema studijama je pronađena povezanost između kasnijeg početka nastave i duljeg spavanja po noći tijekom radnih dana, dok dokazi iz drugih šest studija također podržavaju povezanost između kasnijeg početka nastave i dužeg trajanja sna. U jednoj studiji se tvrdi da je kod učenika koji kasnije polaze na nastavu zabilježeno manje simptoma depresije u odnosu na učenike koji ranije polaze na nastavu. Različite studije donijele su različite zaključke o povezanosti između kasnijeg početka nastave i povećane nazočnosti i pozornosti učenika. Moguće je da ovakve intervencije imaju i potencijalne štetne učinke na logistiku, pošto su kvalitativni dijelovi jedne studije opisali podatke o manjem stupnju interakcije između roditelja i djece, dok je u okviru druge studije opisan podataka o poteškoćama u organizaciji školskog kadra i rasporeda nastave. No, pošto su dokazi bili ograničeni i niske kvalitete, ne možemo izvući jasne zaključke o štetnim učincima kasnijeg polaska u školu.
Kvaliteta dokaza
Kvaliteta dokaza je bila vrlo niska, zbog čega ne možemo procijeniti prikazuju li rezultati studije pouzdano korisne i štetne efekte kasnijeg početka nastave.
Authors' conclusions
Summary of findings
| Early versus delayed school starts | |||
| Patient or population: students aged 13‐19 | |||
| Outcomes | Impacts | № of Participants (studies) | Quality of the evidence |
| Student academic outcomes | There is no clear association between later school start times and student academic outcomes, as two studies reported significant positive associations (b = 1.78, b = 0.98; effect sizes could not be calculated from one study), one study reported a non‐significant negative association (b = −0.02), and one study reported a significant negative association (MD −0.32 GPA points on a scale of 0 to 4, with higher GPAs indicating better grades). | 254,743 (4) | ⊕⊝⊝⊝ |
| Amount or quality of sleep | All studies that evaluated the association between later school start times and amount or quality of sleep reported significant positive associations, providing evidence that later school start times are associated with increased sleep (effect sizes ranged from MD 0.49 to 1.95 hours) and lower risk of losing sleep (RR 0.41). | 52,340 (8) | ⊕⊝⊝⊝ |
| Mental health outcomes | There is limited evidence concerning the association between later school start times and mental health outcomes: one study reported significant differences in self‐reported depression symptoms for students in later starting schools (07:25 and 08:30) than earlier starting schools (07:15), but no significant difference between students starting school at 08:30 vs 07:25. | 1200 (1) | ⊕⊝⊝⊝ |
| Truancy or attendance outcomes | There is mixed evidence concerning the association between later school starts and attendance outcomes: one study reported a significant increase in attendance, one study reported a non‐significant increase in attendance, and one study reported a significant increase in attendance for 2 of 6 schools and non‐significant effects (no further information provided) for the other 4 schools. | 255,122 (4) | ⊕⊝⊝⊝ |
| Alertness | There is mixed evidence concerning the association between later school starts and student reports of alertness or sleepiness. Two studies found an association between later school start times and decreased daytime sleepiness, while one study found no difference between student reports at later and earlier starting schools. One study reported a significant increase in attention levels but a non‐significant increase in concentration levels. | 2735 (4) | ⊕⊝⊝⊝ |
| Adverse events/unintended consequences | Authors provided limited information concerning adverse events and unintended consequences but did offer that later school start times may be associated with decreased morning interactions between parents and children, decreased alertness in mid‐afternoon, and increased logistical challenges, including missing extracurricular activities, transportation troubles, and safety concerns (as students may have to walk home in the dark). | 207,576 (4) | ⊕⊝⊝⊝ |
| b: regression coefficient; CI: confidence interval; GPA: grade point average; MD: mean difference; RR: risk ratio | |||
| GRADE Working Group grades of evidence | |||
| aDowngraded one level (from starting point of 'low' for observational study designs). The GRADE rating of 'very low' for all findings reflects study designs (absence of RCTs), high risk of bias within the studies, and inconsistency within the estimates. | |||
Background
Students, parents, and administrators are increasingly examining the implications of school start times for adolescents. Within the past decade, school officials have begun intentionally varying start times as a means of improving students' productivity, achievement, health, and well‐being. The current and growing interest in secondary schools' adoption of later start times has been preceded by approximately 20 years of research concerning the issues of adolescent sleep needs, sleep deprivation, adolescents' peak periods of alertness, and the best times of day for learning. However, although anecdotal or even experiential understanding of potential links exists, the often informal experimentation with school start times has proceeded in the absence of clear, detailed, and well‐substantiated guidelines. The purpose of this review is to synthesize existing evidence about school start times and to ultimately support sound policy and decision‐making. School time scheduling has global implications, so we also aim to explore whether this type of intervention works better in certain geographic areas, in certain kinds of schools, or with certain students.
It is our hope that this review will also contribute to the development of systematic review methodologies, particularly the approaches required for conducting reviews in public and population health and education, as well as reviews that have a specific focus on the equity of these kinds of interventions.
We did not identify any existing systematic reviews on the effectiveness of later school start times. We have, however, identified non‐systematic reviews and summaries as well as systematic reviews on related topics. For instance, the Evidence for Policy and Practice Information and Coordinating Centre (EPPI‐Centre) at the Social Science Research Unit, Institute of Education, University of London recently completed a review on the effects of block scheduling (one form of class scheduling) on students. As part of this review, researchers constructed a map of all interventions relating to school time use. The map included, for example, interventions related to the length of the school day, the length of the school year, the length of classes, and the use of Saturdays for schooling. Later school start time was identified as a type of intervention related to school time use. The EPPI‐Centre reviewers did not subsequently consider this topic for synthesis or in‐depth review, however. An undergraduate thesis project was completed on the effectiveness of later school start times in the USA (Kuhfeld 2009), which included a literature review. Researchers in Kentucky, USA have conducted other non‐systematic literature reviews related to later school start times as part of a Blue Valley School District evaluation (Yan 2006; Yan 2007), as have researchers (including a co‐author of this review) for the Toronto District School Board in Canada (Newton 2010). A more recent non‐systematic review of 38 reports also explored the results of delaying school start time and found that later school start times were associated with increased sleep duration among adolescents. They also reported mixed but overall positive findings on its association with improved academic outcomes, fewer depression symptoms, and fewer motor vehicle crashes (Wheaton 2016). None of these previous studies or reviews has provided a comprehensive, systematic picture of the effectiveness of later school start times for improving the education, health, or well‐being of high school students because:
-
the scope of the reviews was limited, and evidence presented in these reviews may be only a partial representation of relevant studies;
-
they did not use systematic inclusion or exclusion criteria; and
-
they did not systematically or critically appraise included studies, so we know little about the quality of the evidence.
Although the topic has global significance, most primary studies to date have been undertaken in North American school settings, with school times being adjusted from early starts (between 07:00 and 08:00) to times after 08:15. There appears to be a preliminary indication from these previous non‐systematic reviews and summaries that later school start times have positively impacted student learning by way of students being more alert, focusing on tasks, attending more first period classes, and falling asleep less often in class. There has been some indication (especially in Wahlstrom 2002) that students in later starting schools eat breakfast more often, get more sleep, and are less tense at home, and school nurses have reported fewer stress‐related complaints and illnesses. Common disadvantages appear to be a longer school day for teachers; later times for sports and after‐school activities resulting in students getting home later; and a decline in work hours for students with after‐school jobs.
Description of the condition
There is ample research available on the biology of sleep, specifically pertaining to adolescents. This body of research details adolescents' unique circadian rhythms, patterns of later melatonin release, bio‐regulatory processes (delayed phase preference) associated with later evening sleepiness, adequate sleep needs (9.25 hours per night), and the growing prevalence of sleep deprivation. The average total hours of adolescent sleep in the USA, for example, is 6.5 to 7.5 hours per night (Carskadon 1990; Dahl 1996). If given a choice, as children progress into adolescence, they tend to both go to sleep and wake up later (Acebo 1991). Sleep research studies commonly find that teenagers have biologically different sleep and wake patterns than the preadolescent or adult populations (Wahlstrom 2002), with adolescents tending towards both going to bed and waking later.
Preliminary research indicates that a number of conditions or behaviors may be remedied by a later school start time. Students with a later school start time of 09:30 averaged 7.5 hours of sleep on weeknights, whereas those with an earlier start time of 07:20 reported only 6.9 hours (Kowalski 1995). Even a moderate increase in sleep (30 minutes to one hour) over a period of time has shown to be associated with increased scores on various performance tasks (e.g. reaction times and memory tests) for youth; in one study, students who slept longer improved their performance on several measures of neurobehavioral functioning (e.g. digit forward memory test and reaction time) and avoided the deterioration of neurobehavioral functioning that students who maintained or decreased sleep times experienced (Sadeh 2003). Further, increased sleep duration has been associated with improved performance on auditory and visual working memory tasks (Steenari 2003). In a three‐year longitudinal study, researchers found that students' increased sleepiness was associated with limited growth over time in verbal comprehension, resulting in an educational deficit at the end of the study (Bub 2011).
Research has also demonstrated that sleep deprivation is also associated with poorer emotional health, as students with decreased sleep duration have shown less positive affective response and poorer emotional regulation compared to their peers who slept longer (Vriend 2013). Further, sleep has been shown to be an important factor in emotional regulation, and decreased sleep is associated with lowered emotional intelligence, increased irritability, increased depressive symptoms, and worsened mood (see Deliens 2014 for a review).
In a noteworthy appraisal of prominent sleep research studies, researchers found that specifically shortened sleep times (later bed times paired with earlier wake times) were associated with lower academic performance, grade point averages (GPAs) and motivation levels (Wolfson 2003). These authors also reported that more sleep and later weekday rise times were associated with better grades and a higher motivation to do well in school. In a further critical review of the literature relating sleep loss to learning capacity and academic performance, researchers found evidence that sleep loss was associated with poorer memory, computational speed, problem solving, verbal creativity, abstract thinking, executive functioning, and other higher level cognitive functioning (Curcio 2006), all aspects that are related to school performance and educational outcomes.
The review of research that focused on laboratory testing for the impacts of sleep disturbances, sleep deprivation and adolescents' bio‐regulatory processes uncovered the following concerns associated with limited sleep deprivation.
-
Aggressive behavior (Gibson 2006).
-
Memory loss (Poirel 1987).
-
Conflict with teachers, increased irritability, and aggressive behavior (Maas 1995).
-
Tardiness (Gibson 2006; Wahlstrom 2002).
-
Falling asleep in class (Maas 1995).
-
Poor self‐esteem (Fredriksen 2004).
-
Greater risk of accidents (Dahl 1996).
-
Anxiety and depression (Chorney 2007).
-
Pre‐frontal cortex dysfunction (inappropriate behavioral responses, negative impact on creative thinking, decreased goal‐oriented behavior) (Drummond 1999; Harrison 1996).
-
Slow performance or lapses of performance, slower reaction times, difficulty concentrating (Sadeh 2003).
-
Low achievement and achievement motivation (Epstein 1998; Meijer 2000).
It appears, therefore, that later school start times, if associated with sleep time increases, could have positive impacts on education, health, and well‐being for adolescent students and their families. This review aims to examine the evidence base for these potential relationships.
Description of the intervention
We specifically conducted this review to examine the effects and implementation of later start times for adolescents. The intervention was an adjustment in the time school starts. We were interested in comparisons of schools that start at different times during the day, as well as comparisons between morning and afternoon or evening 'shifts' at a single school where double or multiple groups or split shifts of students exist.
How the intervention might work
There are two main theories about why a later school start time might improve the education, health, or well‐being of adolescent students. The first relates to the amount of sleep an adolescent gets depending on when they have to wake up to get to school and the various impacts of different amounts of sleep. The second theory relates to there being an optimal time of day for adolescent alertness and learning, which is associated through several mechanisms with health and educational outcomes.
Previous studies indicate that adolescents may not be behaviorally and physiologically ready to fall asleep until approximately 23:00, and some show physiological signs of becoming more energetic and internally stimulated in the late evening (Carskadon 1981; Wolfson 2005). If given a choice, adolescents prefer to go to bed later and wake later. There is general consensus throughout most biomedical and sleep literature that a mismatch exists between school schedules and demands, on the one hand, and the adolescent delayed sleep cycle, on the other. Students who have to rise early in the morning to attend school may not be getting enough sleep. Delaying school start times may allow students to sleep longer and obtain subsequent health and educational benefits.
The second theory about why later school start time interventions might work to support adolescents' education, health, and well‐being is that these schedules may better align the school day with peak times for adolescent alertness and potential for learning, factors that in turn have direct implications for health and educational outcomes. Evidence for this theory relates to investigations of adolescent neuropsychological performance, alertness, and the time of day ideal for learning and short‐ and long‐term memory tasks. Hansen 2005 found that students' performance was better later in the day than in the early morning. Adolescent short‐term memory has also been shown to be better in the morning, but long‐term memory improved in the late afternoon and early evening (Harrison 1996; Monk 1987).
Why it is important to do this review
There is a growing awareness amongst parents, teachers, schools, and community groups that later school start times could potentially support better health and education outcomes for adolescents. For example, the US guidelines for disease prevention and health promotion include a goal to increase the "proportion of students in grades 9 through 12 who get sufficient sleep" (US DHHS 2013). As such, there is a burgeoning body of literature on the effects of even mild sleep deprivation on young people, with research pointing to associations between insufficient sleep and depression (Short 2013), substance use (McKnight‐Eily 2011), and poor academic performance (Ming 2011). Additionally, governmental groups have offered guidance for possible adjustments to school start times in the hopes of increasing sleep duration (ASWG 2014). At the request of parents, teachers, school council members and others, school administrators and educational policymakers in many jurisdictions have recently delayed, or are currently considering delaying, school start times. A number of schools and school districts have also changed times over the past 10 to 15 years, particularly in North America. There have been a number of single studies of these kinds of interventions, but it is unclear whether there is sufficient evidence about the effectiveness of these kinds of approaches overall to support the adoption of them for students, their families or the school's wider community (Taras 2005). The results of this review can be used by school officials to make decisions about whether or not to adopt a later school start time within their own schools or school districts. Moreover, as some research demonstrates the difficulty that stakeholders have in mobilizing the resources necessary to alter school times (Wahlstrom 2014), the results of this review may allow a community to better ready itself for a change in school start times. Considerable research demonstrates the difficulty of the community change process and of conducting research in those spaces (Stoeker 2012), and this review may make those processes easier.
Objectives
To assess the effects of a later school start time for supporting health, education, and well‐being in high school students.
Secondary objectives were to explore possible differential effects of later school start times in student subgroups and in different types of schools; to identify implementation practices, contextual factors, and delivery modes associated with positive and negative effects of later start times; and to assess the effects of later school start times on the broader community (high school faculty and staff, neighborhood, and families).
Methods
Criteria for considering studies for this review
Types of studies
All stages of this review followed the published protocol (Davison 2011), with any deviations specified in the Differences between protocol and review section.
The following study designs were eligible for inclusion in this review.
-
Randomized controlled trials (RCTs) (including cluster‐randomized controlled trials or randomized cross‐over trials).
-
Non‐randomized designs, including:
-
non‐randomized, quasi‐experimental controlled trials of an intervention (including potentially cluster and/or cross‐over trials);
-
controlled before‐and‐after studies (CBAs);
-
interrupted time series studies (ITSs) with at least three pre‐ and postintervention measurements.
-
For the purpose of this review, the term 'intervention' also included changes that were deemed 'natural' or 'natural experiments' (changes that occurred and could be studied but were not under the design or immediate control of the research group). These could include, for example, comparisons of different 'shifts' of students when a high school enters a split‐shift configuration, or studies in groups of students who left a school with an earlier start time and entered a new school with a later one. We conducted separate quantitative syntheses across the different types of study designs.
We placed no limitations on publication date, language, or status.
We used qualitative data only in cases where they were associated with an intervention study included in this review, using qualitative findings to help contextualize and provide explanations for the major findings.
As outlined below, the literature search located a variety of ineligible types of studies on late start interventions (for example, case‐control studies, case studies and other types of observational studies). While we did not include these studies in the review, we used them in the Discussion section to offer advice on designing ideal intervention studies for evaluators of these kinds of schedule changes.
Types of participants
We included studies that pertained to the student age group of 13 to 19 years, for whom this type of intervention is most pertinent. Participants were high school or secondary school (or in some cases middle school or junior high school) students and their families, schools and communities, worldwide. We did not exclude students with special needs, students at alternative schools, or students enrolled in boarding schools. We noted any of these differing circumstances in the narrative summary.
Types of interventions
This review included studies of interventions that involved a comparison between two or more different school start times. These included 'late start' interventions that purposely moved school start times later and then compared outcomes obtained under the previous or another earlier start time. We also included studies that compared outcomes associated with start times at different, but matched, schools; between different 'shifts' of students within the same school (the morning, afternoon or evening shift); and between day versus night school attendance. We did not exclude studies based on type of school (e.g. public, private, boarding etc.).
Types of outcome measures
Based on our study protocol, we divided the many possible outcomes of interest into two categories: primary and secondary outcomes. We included findings related to primary and secondary outcomes in the narrative summary. We also report results associated with differential effects, adverse or unforeseen effects, implementation details, and effects on the broader school community in the narrative summary when available.
Primary outcomes
Primary outcomes included the following.
-
Student academic outcomes, measured, for example, by locally relevant standardized test scores and course grades, midterm and final exam results, and graduation records.
-
Outcomes related to amount or quality of sleep for students, often referred to as total sleep time (TST) for students.
-
Student sleepiness or fatigue.
-
Mental health indicators including, for example, measures of stress, anxiety, feelings of isolation or exclusion, depression or suicidal ideation.
-
Student truancy or attendance.
-
Teacher or self‐reported student alertness.
We also noted any additional adverse outcomes or possible harms. These could have included the following.
-
Increased transportation costs for students, families, or schools.
-
Decreased student supervision outside school time.
-
Decreased time spent with family.
-
Issues with child care and before‐ and after‐school care for younger siblings.
-
Decreases in enrollment in extracurricular and athletic activities.
-
Polarizing or increased conflicts within the school community through this issue.
-
Difficulties for school staff (making medical appointments, attending professional development workshops, etc.).
-
Increased costs and difficulties obtaining substitute teachers.
Secondary outcomes
Secondary outcomes included the following.
-
Outcomes related to health behaviors (e.g. diet, exercise, tobacco use, alcohol or drug use, unsafe sexual practices).
-
Health and safety indicators (e.g. vehicular accidents, falls or other accidents, abductions, transportation issues).
-
Social outcomes (e.g. changes in social supports, peer relations, participation in extracurricular activities, student employment, discipline referrals at school).
-
Family outcomes (e.g. changes in the supervision of children/adolescents and child care, family communication and dynamics, routines, roles).
-
School outcomes (e.g. changes in registration numbers, school climate or discipline referrals).
-
Community outcomes (e.g. reactions from local businesses, feelings of safety on neighborhood streets).
Where possible, we included descriptions of the school and community setting to provide context for study results. We identified qualitative companion studies to help in this regard. Of particular interest were social, political, climatic, and geographic factors that might impact on the delivery of, access to, and experience of schooling, as well as any other school or community‐based interventions that have impacts on students, such as nutritional or other health and development interventions. We also noted, where possible, the season or time of year in which the included studies were undertaken.
Search methods for identification of studies
We undertook electronic searches in scientific databases and handsearched citation lists, recent relevant journal index lists, websites, and publications from relevant conferences and scientific meetings. We contacted key expert informants, including previous authors and researchers in this area. Based on the feedback of reviewers, we also searched clinical trial registries (clinicaltrials.gov and the WHO International Clinical Trials Registry Platform (ICTRP)) for studies of delayed school start times.
Electronic searches
As the literature describes this topic in a very heterogeneous manner, the search process (initially conducted by CMD, LU, and RB) was iterative to ensure that we achieved a balance between recall and precision. We gained input from three reference librarians to develop the MEDLINE search strategy (Appendix 1). The search concepts were divided into 3 groups: population (lines 1‐8 in the sample search), setting (lines 9‐16), and intervention (lines 17‐39). We did not exclude documents on the basis of language, country or publication date.
We modified this search strategy for other databases as required given the inherent differences of the various platforms and quality of the indexing (Appendix 2). A librarian conducted the MEDLINE search on the Ovid MEDLINE(R) In‐Process & Other Non‐Indexed Citations and OvidMEDLINE(R) on 28 October 2014, and we updated that search and included other databases for the comprehensive search periods described below.
-
Cochrane Central Register of Controlled Trials (CENTRAL; 2016, Issue no. 1) in the Cochrane Library (searched 8 February 2016).
-
The Cochrane Database of Systematic Reviews (2016, Issue no. 1) in the Cochrane Library (searched 8 February 2016).
-
MEDLINE Ovid(1946 to 8 February 2016).
-
Embase Ovid (1974 to 8 February 2016).
-
PsycINFO Ovid‐ (1806 to 8 February 2016).
-
Academic Search Complete EBSCO (1887 to 8 February 2016).
-
CINAHL EBSCO (Cumulative Index to Nursing and Allied Health Literature; 1982 to 8 February 2016).
-
Education Full Text Wilson EBSCO (1983 to 8 February 2016).
-
Educator's Reference Complete (1932 to 8 February 2016).
-
ERIC ProQuest (1966 to 8 February 2016).
-
Global Health CAB Health (1973 to 8 February 2016).
-
Sociological Abstracts ProQuest (1963 to 8 February 2016).
-
JSTOR (1870 to 8 February 2016).
-
British Education Index (1986 to 28 October 2014 ‐ no longer available).
-
Australian Education Index (1977 to 8 February 2016).
-
Dissertations and Theses ProQuest (1637 to 8 February 2016).
-
Evidence for Policy and Practice Information and Coordinating Centre Review Databases (including Bibliomap, DoPHER, TRoPHI, Database of Education Research, and CERUK) (8 February 2016, except for CERUK; last searched April 2011).
Thanks to helpful input from reviewers, we additionally used the same search strategy for the following databases.
-
The International Bibliography of the Social Sciences (IBSS)(1951 to 5 May 2017).
-
ClinicalTrials.gov registry (clinicaltrials.gov; last searched 5 May 2017).
-
WHO International Clinical Trials Registry Platform (ICTRP) (last searched 5 May 2017).
Searching other resources
We handsearched the bibliographies of all included studies (as well as excluded but closely related studies). We contacted many of the authors of included studies and the authors of the other related non‐systematic reviews by email, as well as other prominent school‐health researchers and members of our advisory group to request further relevant information on unpublished or ongoing studies.
In addition, we handsearched the most recent issues of the following journals for publications that would not yet be included in the electronic databases.
-
Sleep (2014 to 2016, Volume 39, Issue 1).
-
Behavioural Sleep Medicine (2014 to 2016, Volume 14, Issue 1).
-
Journal of Adolescent Health (2014 to 2016, Volume 58, Issue 1).
-
International Journal of Child and Adolescent Health (2014 to 2016, Volume 9, Number 1).
-
Journal of School Health (2014 to 2016, Volume 86, Issue 1).
-
American Educational Research Journal (2014 to 2015, Volume 52, Issue 6).
-
British Educational Research Journal (2014 to 2015, Volume 41, Issue 6).
-
Canadian Journal of Education (2013 to 2015, Volume 38, Number 4).
-
Review of Educational Research (2014 to 2015, Volume 85, Issue 4).
-
Educational Researcher (2014 to 2016, Volume 45, Issue 1).
-
British Journal of Educational Studies (2014 to 2016, Volume 64, Issue 1).
-
Educational Evaluation and Policy Analysis (2014 to 2015, Volume 37, Issue 4).
-
The High School Journal (2014 to 2015, Volume 99, Number 1).
-
Journal of Sleep Research (2013 to 2015, Volume 24, Issue 6).
We searched the following websites, conference listings, popular media sources and portals for relevant grey literature (such as evaluation reports and policy papers).
-
System for Information on Grey Literature in Europe (SIGLE 1985‐2005).
-
The World Federation of Sleep Research & Sleep Medicine Societies (WFSRSMS).
To locate additional unpublished studies not identified through the procedures described above, we carried out an Internet search using key words and prominent author searches. We reviewed five pages of hits for each key word or author search in Google.
Data collection and analysis
Selection of studies
At least two authors (a combination of RM, ETS, CMD, LN, AP, and IC) independently assessed the abstracts and titles of articles retrieved by the electronic and handsearches for eligibility, according to the inclusion or exclusion criteria (i.e. types of studies, participants, and interventions). In instances where it was difficult to make a selection decision on the basis of the title and abstract alone, we retrieved the full article for screening. We obtained full‐text copies of all articles deemed eligible by at least one of the review authors for closer examination. At the full‐text level, at least two authors (a combination of RM, ETS, CMD, LN, and RS) independently assessed each identified study for eligibility, resolving any disagreements about eligibility via consensus.
Data extraction and management
At least two review authors independently extracted data from all eligible studies (a combination of RM, ETS, CMD, AP, and IC). We developed the data extraction form based on the Cochrane checklist (Higgins 2011, p. 157). We discussed and resolved any discrepancies between reviewers in data extraction via consensus. We entered data into Review Manager 5 software (RevMan 5) and recorded study details in the Characteristics of included studies and Characteristics of excluded studies tables (RevMan 2013).
We extracted data on study methods (including study design, description of the intervention or natural change, any process details, total numbers in each group, specific timing data and details about participants). We used the PROGRESS (place, race, occupation, gender, religion, education, socioeconomic status) checklist to provide details about the included sample and to assess whether or not investigators reported outcome data by sociodemographic characteristics known to be important from an equity perspective. We extracted school and community characteristics: geographic location (country, region, rural/urban), school type (grade levels, private versus public, single gender versus mixed gender, boarding school versus day school, alternative school), student transportation options, ethnic distribution, and socioeconomic information. We also extracted any information relevant to the history of intervention where possible (e.g. did the school make other previous changes? What is the norm and what is the difference between that norm and the changed time? How long has the intervention been in place?). We also noted any other interventions affecting the study samples, such as school nutrition programs.
We systematically and comprehensively recorded all timing details for interventions. This included making note of the time of day that school began and the schedule of how the school day unfolded in intervention and comparison schools before and after the intervention. We also recorded time of year or season of intervention, data collection and follow‐up where available. Of particular interest was the exact later start time, as this was key to provide possible evidence for any ideal time of day for schooling 13‐ to 19‐year‐olds.
We attempted to extract the most detailed numerical data possible; when available, we extracted raw data, but when unavailable, we extracted effect estimates and confidence intervals (CIs). For any data that were missing or unclear, we contacted author teams from the primary studies.
Assessment of risk of bias in included studies
Among the included studies is one cluster‐randomized controlled trial. As outlined by Guyatt 2011, for RCTs we were particularly aware of limitations associated with:
-
lack of allocation concealment;
-
lack of blinding;
-
incomplete accounts of student and outcome events;
-
selective outcome reporting;
-
stopping early for benefit;
-
the use of non‐validated outcome measures;
-
incomplete washout period or carry‐over effects in cross‐over trials; and
-
recruitment bias.
We therefore used the 'Risk of bias' tool outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), rating each study as being at high, unclear, or low risk of bias for each of the categories. The remaining included studies were CBAs (3 studies) and non‐randomized, quasi‐experimental designs (7 studies). For these kinds of observational studies, we were particularly aware of limitations associated with:
-
failure to develop and apply appropriate eligibility criteria for study and control populations;
-
under‐ or over‐matching in case‐control studies;
-
selection of exposed or unexposed in cohort studies from different populations;
-
flawed measurement of exposure or outcome;
-
differences in measurement of exposure (e.g. recall bias);
-
differences in the surveillance for outcomes among exposed and unexposed populations in cohort studies;
-
failure to adequately control for confounding;
-
inaccurate measure of prognostic factors;
-
lack of appropriate adjustment in statistical analysis; and
-
incomplete follow‐up.
To assess risk of bias in the included studies, we used the Cochrane Collaboration Handbook for Systematic Reviews of Interventions (Higgins 2011. We used nine standard criteria for the RCT, cluster and/or cross‐over trials, and CBA studies (Yes, No or Unclear).
-
Was the allocation sequence adequately generated?
-
Was the allocation adequately concealed?
-
Were baseline outcome measurements similar?
-
Were baseline characteristics similar?
-
Were incomplete outcome data adequately addressed? (Each primary outcome can be scored separately.)
-
Was knowledge of the allocated interventions adequately prevented during the study?
-
Was the study adequately protected against contamination?
-
Was the study free from selective outcome reporting?
-
Was the study free from other risks of bias?
At least two review authors (of RM, ETS, and JF) independently assessed risk of bias. When possible, we present results of meta‐analyses stratified by summary 'Risk of bias' measures.
For all synthesized effect studies, at least two review authors (a combination RM, ETS, JF, CMD, and RB) independently employed the GRADE method for assessing the quality of the body of evidence, and we have included that information in the summary of findings Table for the main comparison table (Higgins 2011).
Measures of treatment effect
For continuously measured outcomes, we expressed the effect size as the mean difference, measuring differences in postintervention means between the intervention and comparison groups. For outcomes that were not synthesized, we report unstandardized mean differences when possible so that results are easily interpretable. For any outcome variables measured on a dichotomous scale, we used a risk ratio (RR) metric to index differences in the risk of an event between the intervention and comparison groups.
Unit of analysis issues
Studies that allocate by either whole schools or classroom clusters can have unit of analysis issues if authors do not adequately adjust for within‐cluster correlations in their primary analyses. This is often an issue in cluster‐randomized trials, where a school or classroom is the unit of randomization but investigators analyze outcome data at the individual student level (Whiting‐O'Keefe 1984). There are other issues in cross‐over trial designs, especially if meta‐analyses include cross‐over trials and combine measurements from two or more intervention periods as if they used a parallel‐group trial design. In general, there is increased possibility for errors in analysis when there are studies with repeated observations on participants, events that re‐occur, multi‐intervention groups or multiple attempts at an intervention.
Only one included study used a study design with potential unit of analysis errors (Lufi 2011). For this cluster‐randomized trial, we followed the recommendation in Higgins 2011 for adjusting the standard error by multiplying the unadjusted standard error by the design effect (the square root of 1 + (average cluster size − 1) × intra‐class correlation (ICC)). Because the study did not report the ICC, we assumed a value of 0.05, as stipulated in Higgins 2011. The study itself did not account for clustering in any way.
Although we included only one randomized controlled trial in this review, we paid special attention to the unit of randomization, unit of analysis, and underlying design issues. For all studies, we therefore also assessed the appropriateness of analysis and reporting. We used the following questions to guide our assessment.
-
What is the unit of analysis issue?
-
Can the issue be corrected by the review authors (for example, Higgins 2011 contains some guidance to review authors if a study will be included in a meta‐analysis and the original analysis did not adequately adjust for clustering (section 8.11.2.4).
-
Does the unit of analysis issue impact all aspects of the results and analysis or only parts of it?
-
Does the unit of analysis issue represent an error that would warrant exclusion if all other aspects of the study indicated inclusion? Could some aspects of the study be used?
Dealing with missing data
For the included studies, members of the research team (RM and CMD) contacted authors of six articles (Edwards 2012; Hinrichs 2011; Hoehn 2015; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014), receiving responses with additional information from two (Hinrichs 2016; Paksarian 2016).
Assessment of heterogeneity
We assessed statistical heterogeneity by using the Q, I2 and Tau2 statistics. The Q statistic was used to assess whether there was more variability than expected due to chance, and we considered P values less than 0.1 to denote significance. We used the I2 statistic to quantify the percentage of observed variability that could be attributed to true heterogeneity. Finally, we used Tau2 to quantify the average squared deviation around the mean effect size. We planned to conduct subgroup analyses and meta‐regression to address heterogeneity when possible.
Assessment of reporting biases
We recognized that reporting bias can occur via many routes (e.g. biases associated with publication and non‐publication, rapid or delayed publication, multiple publication, the ease of access of publications, publications in certain languages, the citation or non‐citation of research findings depending on their nature and direction, and the selective reporting of outcomes) and can lead to the overly optimistic estimates of intervention effects. Our search strategy was sufficiently comprehensive so as to increase opportunities to identify all studies that met the inclusion criteria and to identify where multiple publications from a single study exist. We included both published and unpublished data in our review. If at least 10 studies were included in a meta‐analysis, we planned to inspect funnel plots for asymmetry and to use Egger's regression test for funnel plot asymmetry. Nonetheless, we recognize the reporting bias inherent in this evidence base, and we discuss it in the limitations section below.
Data synthesis
Meta‐analysis
We used RevMan 5 software to conduct meta‐analysis when feasible and appropriate (i.e. when at least two studies using the same design provided sufficient numerical data on the same outcome construct that permitted estimation of effect sizes) (RevMan 2013). We synthesized results using an inverse‐variance weighted random‐effects model, which we chose because of the presumed variability across interventions, outcomes, and measurement instruments in this literature. We present all pooled effect size estimates along with their 95% CIs and display them in forest plots.
When meta‐analysis was not possible (i.e. no two studies with the same design provided outcome data on the same construct), we still calculated effect sizes where possible and reported those findings from single studies. When the reported data in the primary studies did not permit the calculation of effect sizes, and primary study authors did not provide the requested information needed to calculate those effect sizes, we simply provide a narrative review of study findings.
Summary table
In addition to the outcomes in the 'Summary of findings' table, we include tables that give basic details about included studies (numbers of students, start times, numbers of different types of outcomes measured, types of schools, etc.), the 'Characteristics of study' table that includes the 'Risk of bias' assessments in each study. See Characteristics of included studies for more details. The 'Summary of findings' table includes a narrative synthesis of all primary outcomes and adverse outcomes reported in primary studies.
Narrative summary
Our narrative summary includes the following.
-
A description of the types of interventions in the included studies with any details available about their implementation.
-
A description of the outcomes measured in the included studies and what might be perceived as obvious omissions.
-
Any possibly pertinent contextual details for the included studies that are available.
-
A review of findings for the secondary outcomes.
-
A description of any adverse outcomes or potential harms found.
-
Perceived strengths, weaknesses, and contributions of each included study with specific emphasis on how it supports or detracts from health equity.
-
Any mention of financial costs associated with later start interventions (although not a complete cost‐benefit analysis).
As cautioned in Deeks 2008, we aimed to avoid introducing bias into the narrative synthesis by reporting the results of each study judiciously and making efforts to avoid inappropriate emphasis on the findings of any one particular study.
Report on practical significance
In addition to reporting statistical significance, we also discuss 'clinical' or practical significance. With respect to sleep, for example, average nightly sleep gain of as little as 30 minutes can positively affect education, health, and well‐being outcomes in adolescents where total nightly sleep times are below ideal levels (Sadeh 2003). A study may indicate that a 10‐minute difference in sleep per school night between intervention and control groups leads to a statistically significant difference between groups. This may have very little practical significance, however, as the time difference is very small. For other outcomes, such as indicators of alertness, mental health, or academic success, even small statistically significant differences could have real value for students and schools. We therefore consider these practical implications when interpreting the review findings.
Report on equity
We used the Cochrane Collaboration Equity Field's Equity Checklist for Systematic Review Authors ‐ 2009 to guide us as we aimed to promote and support health equity in the conduct and completion of this review. There was very limited information reported about the differential effects of interventions across population subgroups, however, so we only dedicate a small section of the Discussion and review findings to the potential implications for health equity. Future updates to the review that include more studies might ultimately include more information about the equity of intervention effects across subgroups.
Subgroup analysis and investigation of heterogeneity
As stated in the protocol, we planned subgroup analyses according to participants' gender, age and/or grade, indicators of socioeconomic status and ethnicity, and time of school start, where available. Given the small number of identified studies, however, we were unable to conduct any such subgroup analyses.
Sensitivity analysis
Based on the nature of the meta‐analyses that were possible, we could not conduct sensitivity analyses, as each meta‐analysis combined only two or three effect sizes, though we had planned to conduct comparative analysis (see Davison 2011 for further details).
Results
Description of studies
Results of the search
The electronic databases searches yielded 1890 potentially relevant documents, and we found 61 additional documents via other search methods. Of these 1951 documents, 70 were duplicate hits, which we eliminated from further consideration. We reviewed the titles and abstracts of 1881 documents to determine potential relevance, excluding 1811 due to irrelevance to the review. We obtained and reviewed 70 full‐text documents and formally excluded 59 (31 had no eligible intervention, 24 used an ineligible study design, and 4 featured participants who were either too young or too old). Eleven studies (17 reports) met all eligibility criteria and were included in the review, including two that were pooled in the quantitative synthesis (meta‐analysis). Two studies identified in the search of clinical registries have not yet resulted in published work, and they are therefore awaiting classification (Kwok 2012; Torgerson 2015).
Figure 1 illustrates the flow of studies through the systematic review process.
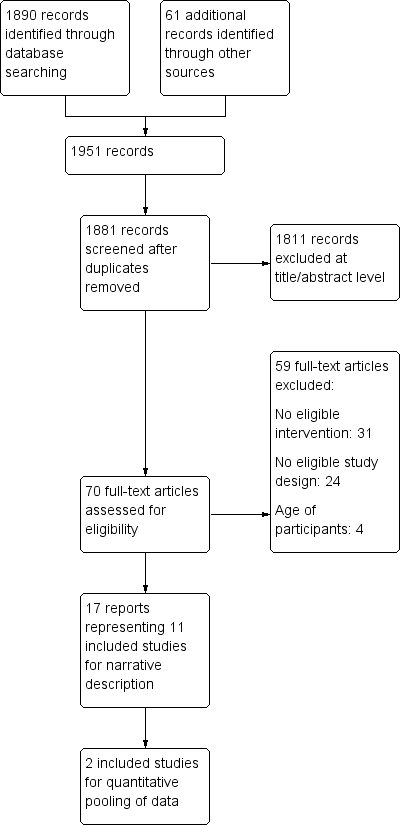
Study flow diagram.
Included studies
An examination of the full texts of 70 potentially relevant reports resulted in eleven studies (17 reports) being included (Borlase 2013; Brandalize 2011; Brown 2011; Edwards 2012; Hinrichs 2011; Hoehn 2015; Lufi 2011; Milic 2014; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014), including a total of 297,994 students. The six additional reports represent a follow‐up to Brown 2011 and five additional reports for Wahlstrom 2002. Although all studies examined the effects of a change in start time on adolescents, there was substantial heterogeneity across studies, as documented in the Characteristics of included studies table.
Study design
Of the 11 included studies, 1 was a cluster‐randomized controlled trial (Lufi 2011), 3 were CBAs (Brandalize 2011; Wahlstrom 2002; Wahlstrom 2014), and 7 were non‐randomized cross‐over trials studies (Borlase 2013; Brown 2011; Edwards 2012; Hinrichs 2011; Hoehn 2015; Milic 2014; Paksarian 2015). Lufi 2011 randomly assigned two classes of eighth grade summer school students in Israel to start class either at the regular time or one hour later for one week of the two‐week class duration. Brandalize 2011 studied two groups of sixth graders in public school in southern Brazil for two years; one group of students had classes only in the afternoons for both years, while the other group had classes in the afternoon in year one and in the morning in year two. Wahlstrom 2002 examined students before and after the Minneapolis Public School district changed their start time from 07:15 to 08:40. Wahlstrom 2014 examined students at eight high schools before and after delays in start times, ranging from a 30‐minute to an 80‐minute delay.
Borlase 2013 compared two groups of students in New Zealand: senior students, whose school started at 10:30 versus junior students, whose school started at 09:00. Brown 2011 compared students in a school district that delayed its school start to 10:00 versus students in a matched school who started at 09:00. Edwards 2012 used data on all middle school students in a school district with three different start times (07:30, 08:15, and 09:15). Hinrichs 2011 similarly compared district‐ and state‐level data for students whose start times varied by school and district. Hoehn 2015 used district‐level data, comparing students who had the earliest start time (07:20 to 07:30) to those with early start times (07:40 to 07:55) and later start times (08:00 to 08:10). Milic 2014 compared groups of Croatian high school students; one group started school at 07:00, and one at 08:00. Finally, Paksarian 2015 compared select students at 81 schools using various starting times, comparing the students at earlier starting schools with their peers at later starting schools.
Location of studies
Study locations include Canada (Toronto), the USA (Colorado, Rhode Island, Minnesota, Kentucky, North Carolina, Wyoming), northern Israel, New Zealand (Wellington), Croatia, and southern Brazil. Six studies took place in the USA (Edwards 2012; Hinrichs 2011; Hoehn 2015; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014), and one study each was in Brazil (Brandalize 2011), Canada (Brown 2011), Croatia (Milic 2014), Israel (Lufi 2011), and New Zealand (Borlase 2013).
Participants
All of the included studies involved students aged 13 to 19 years, according to our inclusion criteria. Seven of the 11 studies involved only secondary or high school students (Borlase 2013; Brown 2011; Hinrichs 2011; Milic 2014; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014). Four studies just involved middle school students (Brandalize 2011; Edwards 2012; Hoehn 2015; Lufi 2011). Different types of schools were involved, including a cross‐section of secondary schools in a specific county or district (Brandalize 2011; Edwards 2012; Hinrichs 2011; Hoehn 2015; Milic 2014; Paksarian 2015; Wahlstrom 2002), specifically inner‐city or urban schools (Borlase 2013; Brandalize 2011; Brown 2011), and specialized schools such as those with limited enrollment and specialized curriculum (Edwards 2012). Many of the studies did not provide more specific information about the context of their interventions or did not select schools based on any contextual feature.
Overview of intervention types
No two studies involved identical late start time interventions, although there were some general trends across studies. Namely, all studies compared student outcomes for an earlier and a later school starting time. For most studies, this meant that the start time shifted from an early time (07:15 being the earliest start) to a later time (such as 08:00, 08:45, 09:00, or 10:00). Brandalize 2011 compared students in a morning shift (07:30‐12:00) versus an afternoon shift (13:00‐17:30). Most studies involved time shifts for a whole school year or semester, except Lufi 2011, which explored impacts of a time shift during a brief, two‐week period. Variations in the amount of delay were wide: Borlase 2013 studied the 90‐minute shift from 09:00 to 10:30. Two studies explored the effects of a one‐hour delay: Milic 2014 explored the difference between students starting school at 07:00 and 08:00, and Brown 2011 explored the effects of delaying school start from 09:00 to 10:00. Hoehn 2015 divided students by start time category as earlier (07:20 to 07:30) and later (08:00 to 08:10) start times. Three studies employed statistical methods to compare students across districts to account for the differences that start times had on particular outcomes (Edwards 2012; Hinrichs 2011; Paksarian 2015). Thus, the body of existing literature lacks a standard intervention condition: neither the time in the morning nor the duration of the delay in school start times was consistent across studies.
Overview of outcome measures
Included studies examined a host of variables and associations with a later school start time, including school‐night sleep duration (Borlase 2013; Brandalize 2011; Brown 2011; Lufi 2011; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014), sleepiness (Milic 2014; Wahlstrom 2002), percentage of students receiving adequate sleep (Hoehn 2015; Paksarian 2015; Wahlstrom 2014), academic outcomes (Edwards 2012; Hinrichs 2011; Milic 2014; Wahlstrom 2014), absenteeism (Edwards 2012; Hinrichs 2011; Wahlstrom 2002; Wahlstrom 2014), body mass index (BMI) (Brandalize 2011), body fat percentage (Brandalize 2011), waist circumference (Brandalize 2011), depression (Wahlstrom 2002), social support (Brown 2011), extracurricular activities (Brown 2011), attention (Lufi 2011), and concentration (Lufi 2011). Because of the variety of outcomes across studies, quantitative synthesis proved difficult; not only were the measures themselves different across studies, but the differences in study design made it nearly impossible to meaningfully pool effect sizes. We provide a brief narrative synthesis on the major outcomes as they overlapped among studies. Because of the paucity of evidence that we could quantitatively synthesize, subgroup analysis was not possible.
Primary outcomes
Student academic outcomes
Four studies evaluated the effects of later school start times on students' academic outcomes. Milic 2014 used school‐level administrative data on students' end‐of‐year grade point average (GPA), a five‐point scale, with higher scores indicating better grades. Two studies used standardized test data: Hinrichs 2011 used ACT (from American College Testing) scores, and Edwards 2012 used state standardized measures of reading and math. Wahlstrom 2014 used school‐level administrative data for students in eight schools to examine students' GPA, grades in period 1 classes compared to grades in period 3 classes, ACT/PLAN scores, and state standardized tests of math, reading, writing, and science.
Amount or quality of sleep
Many studies provided measures of school‐night sleep duration, either by time spent in bed or by bedtime and wake time. Seven studies provided school‐night sleep duration as an outcome (Borlase 2013; Brandalize 2011; Brown 2011; Lufi 2011; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014). Studies relied on either self‐reports of students' sleep habits (Borlase 2013; Brandalize 2011; Brown 2011; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014) or an objective measure recorded by an actigraph or similar technology (Lufi 2011).
Three studies reported the percentages of students receiving adequate sleep (Hoehn 2015; Paksarian 2015; Wahlstrom 2014). Hoehn 2015 and Wahlstrom 2014 used student reports of sleep and categorized any student who received eight or more hours of sleep a night on weeknights as receiving adequate sleep. Paksarian 2015 also used student reports of sleep but categorized adequate sleep as 8.5 hours of sleep or more on weeknights.
Mental health indicators
One study employed a student‐reported measure of depression, utilizing a subset of a sleep scale that measures feelings and behaviors associated with depression (Wahlstrom 2002).
Student truancy or attendance
Four studies used measures of student attendance to analyze absenteeism (Edwards 2012; Hinrichs 2011; Wahlstrom 2002; Wahlstrom 2014), employing school‐level administrative data to count numbers of days missed before and after the intervention.
Student alertness
Three studies used the Epsworth Sleepiness Scale to allow students to self‐assess their daytime sleepiness (Borlase 2013; Milic 2014; Wahlstrom 2002). Questions relate to students' experiences of feeling sleepy during various activities, as well as students' reports of various consequences due to sleepiness (i.e. reporting to school late, missing a class). Additionally, one study assessed student attention as measured by the Mathematics Continuous Performance test and the d2 Test of Attention, which can be associated with alertness and concentration (Lufi 2011).
Secondary outcomes
Outcomes related to health behaviors
One study reported outcomes related to diet, exercise, or other health‐related behaviors: Brandalize 2011 used BMI score, waist circumference, and body fat percentage as indicators of health behaviors.
Health and safety indicators
One study explored vehicular accidents; Wahlstrom 2014 collected automobile crash incidence data for the year before and year after the school start time for the districts of interest in four of the five districts where schools had delayed their start times.
Social outcomes
One study explored changes in social support and peer relationships: Brown 2011 explored student‐reported feelings of acceptance by other students and by adults, as well as student reports of participation in sports.
Family outcomes
No eligible study explored changes in the supervision of children or child care.
School outcomes
No eligible study explored changes in registration numbers, school climate, or discipline.
Community outcomes
No eligible study reported outcomes associated with reactions from local businesses or feelings of neighborhood safety.
Excluded studies
There were 59 formally excluded studies with reasons noted (31 had no eligible intervention, 24 used an ineligible study design, and 4 featured participants who were either too young or too old). Among these, single cross‐sectional studies without comparison groups were common. We also excluded many studies because the participants involved were outside of the age range of the current review, or the study did not assess a later start time intervention. Many of the formally excluded studies have useful contextual and intervention‐related information, but do not have study designs that allow unbiased assessment of the intervention effectiveness. Please see Characteristics of excluded studies for more detail.
Risk of bias in included studies
Figure 2 provides the results from the assessment of risk of bias for each of the included studies. Overall, every study had a high risk of bias on at least one risk of bias domain. Indeed, because only one randomized study design was eligible for inclusion (Lufi 2011), almost all studies were at a high risk of bias due to lack of random sequence generation, lack of allocation concealment, or lack of blinding of participants and personnel. Further, most studies made no attempt to ensure baseline equivalence between the groups being compared. It is important to note that because the intervention under study is a delay in school start times, there is almost no risk of contamination between groups; the comparison groups could not receive the intervention, as their school start time was not delayed. Please see Characteristics of included studies for more details.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
All of the studies had either high or unclear risk of allocation bias; only one study used a randomized design (Lufi 2011), and that study also suffered from allocation concerns. Thus, selection bias was a problem throughout the literature. Lufi 2011 did not discuss allocation concealment and thus we rated it as being at high risk overall for selection bias, as the study randomized students by class, rather than at the individual level.
Because CBAs do not randomly allocate participants to a condition, we automatically rated studies of this design type as being at high risk of selection bias due to allocation processes. Thus, we rated the three CBAs as being at high risk of bias for allocation (Brandalize 2011; Wahlstrom 2002; Wahlstrom 2014).
Similarly, we rated non‐randomized, quasi‐experimental trials as being at high risk of bias by definition for allocation, because their participants were not allocated randomly to treatment or comparisons groups. This means that the seven non‐randomized, quasi‐experimental trials all received a score of high risk of bias (Borlase 2013; Brown 2011; Edwards 2012; Hinrichs 2011; Hoehn 2015; Milic 2014; Paksarian 2015)
Blinding
Trials of school start time cannot blind the students to the type of intervention being received—the students know that their school starts earlier or later. For that reason, almost all studies received a high risk rating for blinding (Borlase 2013; Brandalize 2011; Brown 2011; Hoehn 2015; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014). Further, because these studies relied on self‐reported rather than objective data, the potential existed for performance bias as students from schools with later start times may have understood the purpose of their questionnaires, especially as they had undergone informed consent and knew the purpose of the studies in which they were participating. Most of the studies, therefore, had high performance and detection bias, as there was not enough information to determine if participants were affected by the knowledge that their school had shifted start times or that they were being compared to other schools with earlier start times.
Three studies directly addressed blinding and used objective data (i.e. administratively reported absences and grades, standardized test scores), so we coded them as being at low risk of bias (Edwards 2012; Hinrichs 2011; Lufi 2011).
One study used a mix of objective data (i.e. administratively reported grades) and subjective data (i.e. scores on the self‐reported Epsworth Sleepiness Index) and so received an unclear rating for blinding, performance bias, and detection bias (Milic 2014).
Incomplete outcome data
We rated four studies as being at low risk due to attrition (Borlase 2013; Edwards 2012; Hinrichs 2011; Paksarian 2015). Borlase 2013 explicitly reported that there was no student attrition in the study. Three studies statistically controlled for attrition and determined that any missing students' responses did not differ significantly from those included (Edwards 2012; Hinrichs 2011; Paksarian 2015).
We rated four studies as being at high risk of bias due to attrition (Brown 2011; Milic 2014; Wahlstrom 2002; Wahlstrom 2014). Brown 2011 reported that student mobility was high between schools, so more students may have left either the intervention or comparison school, but the researcher did not provide any control for this in the analysis. Milic 2014 noted a 20% attrition rate but did not offer any explanation or account for this attrition in the discussion of results. Similarly, Wahlstrom 2014 reported approximately 16% attrition but also did not account for it in the analysis. Wahlstrom 2002 also declared a high attrition rate but again did not account for the attrition in the analysis or discussion nor specify the exact attrition rate.
We rated three studies as being at unclear risk of attrition bias (Brandalize 2011; Hoehn 2015; Lufi 2011). In these studies, the authors did not explicitly mention attrition, making it difficult to evaluate the associated risk of bias.
Unfortunately, because of reporting issues, we cannot provide a range of attrition, as only three studies explicitly declared attrition or provided necessary data to calculate it: Borlase 2013 reported no attrition, Wahlstrom 2014 reported 16% attrition, and Milic 2014 reported 20% attrition.
Selective reporting
As a whole, the body of evidence was at low risk for reporting bias. Nine studies explicitly mentioned each outcome collected and then reported on those outcomes, regardless of the significance of the findings (Borlase 2013; Brandalize 2011; Brown 2011; Edwards 2012; Hinrichs 2011; Hoehn 2015; Lufi 2011; Milic 2014; Paksarian 2015). One study explicitly stated that the reported outcomes were only a selection of the collected outcomes, meriting a high risk rating for reporting bias (Wahlstrom 2002). Another study explicitly reported outcome data only for significant outcomes, so we also assigned a high risk rating for it (Wahlstrom 2014).
It is important to note the difficulties in evaluating selective reporting bias given the lack of pre‐registered protocols for the included studies; the raters had to make determinations based on only what appeared in the text and figures of the studies. We acknowledge the possibility that some studies rated as a low risk may have neglected to report both the collection and results of a particular outcome; in that case, the raters would have no way of knowing about the selective reporting.
Other potential sources of bias
Because the overall quality of the studies was so low, most clear risks of bias were captured in the other risk of bias domains. Thus, nine of the studies scored a low risk of bias for other potential sources of bias (Brandalize 2011; Brown 2011; Edwards 2012; Hinrichs 2011; Hoehn 2015; Milic 2014; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014).
One potential source of bias in the cluster‐randomized controlled trial was the intervention duration; students in the intervention group were exposed to a change in school start time for only one week (Lufi 2011).
One study had a potential age confounder; Borlase 2013 compared two groups of students with different school start times, but one group was year 11 and the other year 12. Authors made no attempt to account for differences in age.
Effects of interventions
See: Summary of findings for the main comparison Early versus delayed school starts
Meta‐analysis
Sufficient numeric and comparable data were not available in most included studies, which prohibited quantitative synthesis (i.e. meta‐analyses) on most of the primary outcomes of interest. Only two studies provided sufficient and appropriate data amenable to meta‐analysis, for four outcomes (Brandalize 2011; Brown 2011). It is important to note that three of these meta‐analyses are within‐study outcomes from two independent samples (boys and girls) embedded within one study (Brandalize 2011). Given the differences in study designs and outcomes, we conducted four separate meta‐analyses: one synthesizing mean difference effect sizes for postintervention school‐night sleep duration from two non‐randomized cross‐over trials (Brandalize 2011; Brown 2011), one synthesizing mean difference effect sizes for postintervention BMI (Brandalize 2011); one synthesizing mean difference effect sizes for postintervention waist circumference (Brandalize 2011); and one synthesizing mean difference effect sizes for postintervention body fat percentage (Brandalize 2011).
Primary outcomes
Student academic outcomes
Meta‐analysis was not possible for student academic outcomes; we present our narrative synthesis below.
Amount or quality of sleep
For school‐night sleep duration in the three non‐randomized cross‐over trials (Figure 3), there was a moderate and statistically significant difference between students' hours of sleep at earlier and later starting high schools (MD 1.39 h, 95% CI 0.38 to 2.39). This translates to an increase of 83.4 minutes of sleep for students at schools with later start times.

Forest plot of comparison: 1 Early school start vs late school start, outcome: 1.1 School‐night sleep duration.
The effect sizes from the three studies ranged from 0.49‐1.95 hours, and there was substantial heterogeneity in effects across the studies, however (Tau2 = 0.76; Chi2 = 56.43, degrees of freedom (df) = 2 (P < 0.001); I2 = 96%), so readers should interpret these results with caution. This meta‐analysis is the synthesis of three independent samples from two included studies (Brandalize 2011; Brown 2011) with 1022 total participants. Both studies used similar measures, as they asked students to self‐report their sleep. It is important to note that Brandalize 2011 reported school‐night sleep duration split by gender; the first study in the forest plot is males, the second, females. Although there was clinically significant heterogeneity, we could not address or explain the heterogeneity through subgroup analysis or meta‐regression due to the small number of studies included in the synthesis.
Mental health indicators
Meta‐analysis was not possible for mental health indicators; narrative synthesis is reported below.
Student truancy or attendance
Meta‐analysis was not possible for student truancy or attendance; narrative synthesis is reported below.
Student alertness
Meta‐analysis was not possible for student alertness; narrative synthesis is reported below.
Secondary outcomes:
Outcomes related to health behaviors
For BMI in the CBAs (Figure 4), there was a small, non‐significant effect indicating that later school start was associated with lower body mass index (MD −0.08 kg/m2, 95% CI −0.30 to 0.13). Again, it is important to note that both independent samples synthesized in this meta‐analysis originated from the same study; Brandalize 2011 reported subgroup scores for males and females (the first study in the forest plot is males; the second, females). This random‐effects meta‐analysis synthesized findings for 379 total participants, and heterogeneity was quite low (Chi2 = 0.05, df = 1 (P = 0.82); I2 = 0%).

Forest plot of comparison: 1 Early school start vs Late school start, outcome: 1.2 BMI Score ‐ Cross‐over trial.
For waist circumference in the CBAs (Figure 5), there was a moderate but non‐significant result showing that later school start was associated with a decrease in waist circumference (MD −1.14 cm, 95% CI −3.34 to 1.06). Again, it is important to note that the two independent samples synthesized in this meta‐analysis originated from the same study; Brandalize 2011 reported subgroup scores for males and females (the first study in the forest plot is males, the second, females). The random‐effects meta‐analysis synthesized findings from 379 total participants, and heterogeneity was low (Tau2 = 1.28; Chi2 = 2.02, df = 1 (P = 0.15); I2 = 51%).

Forest plot of comparison: 1 Early school start vs Late school start, outcome: 1.3 Waist Circumference ‐ Cross‐over trial.
For body fat percentage in the CBAs (Figure 6), there was a moderate and significant effect showing that later school start was associated with a decrease (MD −1.45%, 95% CI −2.63 to −0.27). Again, it is important to note that the two independent samples synthesized in this meta‐analysis originated from the same study; Brandalize 2011 reported subgroup scores for males and females (the first study in the forest plot is males, the second, females). The random‐effects meta‐analysis synthesized findings from 379 total participants, and heterogeneity was low (Chi2 = 0.43, df = 1 (P = 0.51); I2 = 0%).

Forest plot of comparison: 1 Early school start vs Late school start, outcome: 1.4 Body Fat ‐ Cross‐over trial.
Health and safety indicators
Meta‐analysis was not possible for vehicular accidents, falls, or other accidents; narrative synthesis is reported below.
Social outcomes
Meta‐analysis was not possible for social outcomes; narrative synthesis is reported below.
Family outcomes
No eligible study explored changes in the supervision of children or child care.
School outcomes
No eligible study explored changes in registration numbers, school climate, or discipline.
Community outcomes
No eligible study reported outcomes associated with reactions from local businesses or feelings of neighborhood safety.
Narrative synthesis
Primary outcomes
Student academic outcomes
Four studies measured students' academic outcomes. Milic 2014 used school‐level administrative data on students' end‐of‐year grade point average (GPA) and reported a significant decrease in grades for students in the later school start group (MD −0.32 points (on a five‐point scale, with higher GPA denoting better grades), 95% CI −0.48 to −0.16). Two studies used standardized test data, either ACT scores or state standardized measures of reading and math (Edwards 2012; Hinrichs 2011). Edwards 2012 documented significant positive associations between later start times and student math scores (b = 1.78, 95% CI 1.19 to 2.34) and reading scores (b = 0.98, 95% CI 0.28 to 1.68), and Hinrichs 2011 reported a non‐significant association between school start times and ACT scores (b = −0.02, 95% CI −0.28 to 0.18). Both studies utilized standardized test scores as a measure of academic outcomes and measured school start time as a continuous measure of start time (rather than distinguishing between early versus later start times). Wahlstrom 2014 obtained administrative data for GPA and standardized test performance for students before and after the delay in school start time, but because of selective and limited reporting, we could not calculate or report effect sizes (we requested data from the author).
Amount or quality of sleep
In addition to the two studies that contributed effect sizes to the meta‐analysis reported above (Brandalize 2011; Brown 2011), six studies reported outcomes related to amount or quality of sleep for students (Borlase 2013; Hoehn 2015; Lufi 2011; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014). Four studies employed self‐report measures of sleep (Borlase 2013; Hoehn 2015; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014), and one used an actigraph to objectively measure sleep (Lufi 2011). Although we could not synthesize these findings due to differences in research design and reporting conventions, taken together, the studies indicated that later school start times were associated with increased sleep.
Borlase 2013 used a non‐randomized cross‐over trial to compare outcomes for a sample of New Zealand's year 11 students, whose start time is 09:00, to year 12 students, whose start time was 10:30. The results indicated that students with later school start times were at a significantly lower risk of losing sleep (risk ratio (RR) 0.41, 95% CI 0.28 to 0.62).
Similarly, Hoehn 2015 used a non‐randomized cross‐over trial to examine the effect of early and late school start times on middle school students' school‐night sleep duration, using data from three years of the Youth Risk Behavior survey. Because of the limited data reported in the study, we could not calculate effect sizes, but the primary study reports significant findings that at schools starting between 08:00 and 08:10, a larger percentage of students reported sleeping at least 8 hours (58.7%) than at schools starting between 07:20 and 07:30 (49.7%).
Paksarian 2015 also used a non‐randomized cross‐over trial with a nationally representative sample of US students. The authors used regression modeling techniques to examine the association between actual start time (measured on a continuous scale) and students' school‐night sleep duration. We were unable to extract the correlation coefficient or other standardized effect sizes from the information reported in the study; however, the study reported a non‐standardized regression coefficient indicating a significant positive correlation between school‐night sleep duration and delayed school start times (b = 11.36, 95% CI 3.52 to 19.21). The authors also reported that each half hour delay in school start time was associated with 1.52 times the odds of students sleeping at least eight hours on school nights (OR 1.52, 95% CI 1.16 to 1.98) for schools starting at 08:00 or earlier. The authors find that after 08:00, both the non‐standardized regression coefficient and the adjusted OR were no longer significant (b = 1.55, 95% CI −5.96 to 9.06; OR 0.91, 95% CI 0.74 to 1.11).
Research utilizing other methods also provides preliminary evidence of an association between later school starts and increased sleep duration. Lufi 2011 conducted a cluster‐randomized controlled trial of public school students in Israel, shifting the intervention group to a one‐hour delayed start time over a short two‐week duration. The results indicated a significant increase in school‐night sleep duration (MD 57.00 minutes, cluster corrected 95% CI 47.00 to 67.00).
Wahlstrom 2002 used a CBA to examine the effects of the delay in school start time for three Minnesota school districts, comparing students whose schools started at 08:30 to those whose started at 07:25 and 07:15. Due to limited reporting, we could not calculate effect sizes from the many outcomes reported in the comprehensive study; however, researchers reported statistically significant increases in sleep duration (F(2,411) = 15.06, P < 0.001), such that students in schools with start times at 08:30 reported significantly more sleep than students whose schools started at 07:25 and 07:15. Wahlstrom 2014 used a CBA to examine the effects of a delay in school start time for one high school from 07:35 to 08:55.The authors reported an average increase of 42 minutes in weeknight sleep following the delayed school start time and a decrease of 18 minutes in weekend sleep (due to incomplete reporting of sample sizes, we could not calculate confidence intervals). Further, the authors reported that students at a single school that delayed its start time by 80 minutes reported getting adequate sleep at more than twice the rate of their peers at a school that had not been delayed (OR 2.48, 95% CI 1.89 to 3.24).
Because of the low quality of included studies, readers should interpret these findings with extreme caution.
Mental health indicators
One study reported outcomes associated with mental health indicators: Wahlstrom 2002 used a CBA to examine the effects of the delay in school on students in Minnesota, reporting that when comparing depression and overall sleepiness, the only significant differences were between the two later start times and the earliest start time groups (F(2,412) = 11.49, P < 0.001); that is, although students in the later two start times (07:25 and 08:30) reported less depression that students in the earliest start time (07:15), there was no significant difference between students starting at 08:30 and 07:25 for measures of depression.
Student truancy or attendance
Three studies measured student absences or absenteeism (Edwards 2012; Hinrichs 2011; Wahlstrom 2014), employing school‐level administrative data to count numbers of days missed before and after the intervention. Effect sizes were not estimable from these studies; nonetheless, Edwards 2012 reported a significant decrease in absenteeism associated with each unit increase in school start times (b = −1.33, 95% CI −2.11 to −0.55);in Hinrichs 2011, this correlation was not significant (b = 0.46, 95% CI −1.50 to 1.59). Both studies operationalized school start time as a continuous variable, so we could not use the regression coefficients as a measure of difference between study arms. Wahlstrom 2014 reported significant increases in attendance rates for two of the six schools examined (an increase from 95.0% to 95.8% and from 94.5% to 94.7%; we could not estimate effect sizes due to incomplete reporting of sample sizes) but did not report numeric data for the four schools that had non‐significant changes in attendance rates.
Additionally, Wahlstrom 2002 used a CBA to examine the effects of the delay in school on students in Minnesota, finding that students in the latest start time (08:25) reported significantly decreased likelihood of arriving late to class because of oversleeping (F(2,428) = 8.39, P <0.01), compared to their peers in earlier starting schools (starting at 07:15 and 07:25). Wahlstrom 2014 used a CBA to examine the effects of the delay in school start times on student tardiness at six schools and reported significant decreases in mean number of times tardy per student per year in four of the six schools (from 2.4 to 2.2, 3.7 to 3.2, 2.5 to 1.5, and 6.7 to 3.3); however, the authors reported that two of the schools had non‐significant changes but did not report sufficient data needed to calculate effect sizes for any of the observed differences. Readers should thus interpret these results with caution.
Student alertness
Four studies provided measures of student alertness: three studies used the Epsworth Sleepiness Scale (Borlase 2013; Milic 2014; Wahlstrom 2002) to measure students' self‐reported daytime sleepiness, and one used the Mathematics Continuous Performance Test and the d2 Test of Attention (Lufi 2011). Study design differences precluded synthesizing effect sizes from the four studies into a meta‐analysis. Wahlstrom 2002 found students whose schools started 65 to 75 minutes later experienced less daytime sleepiness (F(2,434) = 31.91, P < 0.001) and decreased likelihood of falling asleep in a morning class (F(2,424) = 6.0, P < 0.005) compared to students in schools starting at 07:15 and 07:25. Milic 2014 found no difference between groups of students starting school 60 minutes later than their peers on scores for the Epworth Sleepiness Scale, a scale from 0‐24 with 24 indicating greatest sleepiness, (MD 0.00, 95% CI −0.56 to 0.56). Borlase 2013 found that for a sample of New Zealand's year 11 students, whose start time was 09:00, and year 12 students, whose start time was 10:30, students with later school start times had significantly lower odds of reporting being overly sleepy (scoring over the median on the Epworth sleepiness scale) (OR 0.48, 95% CI 0.30 to 0.75).
Lufi 2011 conducted a cluster‐randomized controlled trial (RCT) of public school students in Israel, shifting the intervention group to a one‐hour delayed start time over a short two‐week duration. The results indicated a significant increase in attention levels measured by the Mathematics Continuous Performance Test, a test of 450 simple mathematical problems that combined accuracy, response time, and anticipatory‐impulsive responses to generate an overall attention level (MD 0.96, cluster corrected 95% CI 0.22 to 1.70) and a non‐significant increase in concentration levels measured by the d2 Test of Attention, a test of attention based on participants' selecting specific letters from a block of characters that provided an overall attention score based on accuracy, consistency, and speed of selection of designated letters (MD 13.00, cluster corrected 95% CI −3.38 to 29.38). Because this was the only RCT eligible for inclusion in the review, we could not synthesize its findings with those from the other included studies, which used either non‐randomized cross‐over trials or CBA designs.
Because of the low quality of studies and the impossibility of synthesizing outcomes, readers should interpret results with extreme caution.
Secondary outcomes:
Outcomes related to health behaviors
See above meta‐analytic results for Brandalize 2011.
Health and safety indicators
Wahlstrom 2014 collected data on automobile crashes involving 16‐ to 18‐year‐old drivers during the school year before and after delays in school start times in districts in Minnesota and Wyoming. In two of the districts, researchers reported that the incidence rate of accidents decreased by 65% to 70%. In the other two districts, researchers reported a slight decrease of 6% and a slight increase of 9%. Because of the way these data are reported (as incidence rather than prevalence rates), we could not calculate effect sizes. Readers should interpret results with extreme caution.
Social outcomes
One study explored the association between later school starts and students' social outcomes. Brown 2011 used a non‐randomized cross‐over trial to examine the effects of a one‐hour delay on students in a public school in Toronto, Canada, comparing students at a school that started at 09:00 with a matched school that started at 10:00. The results indicated no significant differences in the risk of students reporting feeling accepted by other students (RR 0.84, 95% CI 0.59to 1.18) or feeling accepted by adults (RR 0.71, 95% CI 0.50 to 1.00); however, students at schools with later start times were significantly more likely to participate in sports (RR 1.33, 95% CI 1.09 to 1.63). Because of the low quality of studies and the mixed findings, it is not possible to draw definitive conclusions concerning delaying school start times.
Family outcomes
No eligible study explored changes in the supervision of children or child care.
School outcomes
No eligible study explored changes in registration numbers, school climate, or discipline.
Community outcomes
No eligible study reported outcomes associated with reactions from local businesses or feelings of neighborhood safety.
Missing outcome data
Due to the reporting of primary studies, we could not calculate effect sizes for several studies (Edwards 2012; Hinrichs 2011; Hoehn 2015; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014). We have contacted all authors and hope that updates to this review will include effect sizes from their studies.
Adverse effects or unintended consequences
Although the included studies provided limited information about adverse effects or unintended consequences, study authors did discuss some features outside the main study outcomes. In the narrative discussion of later school start times, Hinrichs 2011 suggested that later school start times may be associated with decreased morning interactions between parents and children and may place students in academic classes, as their homeostatic sleep process causes a mid‐afternoon dip in alertness, potentially limiting the academic gains students in later starting schools might make. Wahlstrom 2002 identified some potential adverse logistical effects, in the form of structural and administrative challenges faced by school systems implementing later start times. According to Wahlstrom 2002, adjusting school start time requires consideration of a myriad of aspects such as the influence the time change will have on staffing and staff training, transportation, extracurricular activities, influences on students' ability to take part‐time jobs, daycare considerations, safety concerns (e.g. walking home in the dark), commuting challenges, and the influence the adapted schedule may have on student co‐op placements or intramural activities. Wahlstrom 2014 echoed these concerns and drew on qualitative data from school policymakers, who discussed the extreme difficulty they had in pushing for and implementing delays in school start time. Brown 2011 also noted specifically that due to the later school start time, students had to miss more class for sports involvement. Students were also more often late for class directly following lunch, likely due to a shortened lunch period. These authors also mentioned additional challenges with respect to teachers. The later start prevented some teachers from supervising extracurricular activities or providing extra help after school hours, and others found it difficult for some to attend school board level professional development activities. When teachers did attend these kinds of events, the school was required to hire substitute teachers more frequently than previous and for later times in the day, which had budgetary implications. In sum, though, given the low quality of the included studies and the mixed results, it is not advisable to draw conclusions about the adverse effects of later school start times.
Differential effects
Few studies reported specific effects by subgroup. Borlase 2013 and Brown 2011 both noted a differential impact of late start time by student age, and Borlase 2013 stated that positive outcomes were observed for the older (grade 12) students with no change for those in grade 9. Similarly, Brown 2011 observed academic improvement for the 14‐, 16‐ and 17‐year‐old students only and not for those 18 and over. Brandalize 2011 split outcomes reporting by gender, so we treated these two independent samples separately and synthesized them in the relevant meta‐analyses. Other studies did not disaggregate data on outcomes of interest, precluding our ability to explore differential effects of the intervention.
Subgroup analysis and investigation of heterogeneity
We were committed to reporting findings from original studies by gender, age and/or grade, indicators of socioeconomic status and ethnicity, and time of school start, where available. We reported results narratively because quantitative pooling of data across studies was limited and data were not generally available at a subgroup level.
Sensitivity analysis
We did not conduct sensitivity analyses given the small number of included studies for any given meta‐analysis.
Discussion
Summary of main results
Eleven studies met the inclusion criteria for this review, and only two of them reported outcomes and used study designs that were sufficiently similar to allow for meta‐analysis. For this reason, interpreting results from this review warrants caution. There were sufficient data to perform four meta‐analyses, synthesizing mean difference effect sizes for school‐night sleep duration (Brandalize 2011; Brown 2011), BMI score (Brandalize 2011), waist circumference (Brandalize 2011), and body fat percentage (Brandalize 2011). The findings for school‐night sleep duration and body fat percentage were statistically significant. The indication that later school start times were associated with greater school sleep night duration (MD 1.39 hours, 95% CI 0.38 to 2.39) was based on the synthesis of only two studies with substantial heterogeneity (Tau2 = 0.54; Chi2 = 62.59, df = 2 (P < 0.001); I2 = 97%) and low‐quality evidence. Further, readers should also use caution when interpreting the finding that later school starts were associated with decreased body fat percentage (MD −1.45%, 95% CI −2.63 to −0.27), as it represents the synthesis of two arms of the same study that had a high risk of bias overall. These findings, along with the null findings for the two meta‐analyses examining effect on BMI (MD −0.08 kg/m2, 95% CI −0.30 to 0.13) and waist circumference (MD −1.14 cm, 95% CI −3.34 to 1.06), thus provide no consistent findings regarding the effects of delayed school start times on students' sleep and well‐being outcomes.
Several individual studies provided promising results, but because of methodological and reporting quality, we could not pool them in meta‐analysis. Research presented a mixed case for the association between later school start times and academic outcomes: one study found a positive association (Edwards 2012); one found no association (Hinrichs 2011); one found a negative association (Milic 2014); and one reported positive, negative, and no associations across different school sites (Wahlstrom 2014). Several studies suggested there was an association between later school start time and increased sleep duration (Borlase 2013; Hoehn 2015; Lufi 2011; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014). One study found limited support for the association between later school start times and lower reports of depressive symptoms (Wahlstrom 2002). There was similarly limited support for the association between later school starts and decreased absenteeism; one study found a significant relationship between later school start times and decreased absences (Edwards 2012), one study found no relationship (Hinrichs 2011), one study found mixed results depending on the district and grade (Wahlstrom 2014), and one study found a significant relationship only for absences due to sleepiness (Wahlstrom 2002). There was greater support for student alertness, as three studies demonstrated positive associations between later school start times and decreased sleepiness or increased attention (Borlase 2013; Lufi 2011; Wahlstrom 2002), while one study found no association (Milic 2014). However, because of the methodological differences and weaknesses that precluded much meta‐analytic synthesis, we can draw no strong conclusions concerning the potential benefits or harms of later school start times. Due to the limitations of the evidence at hand, we cannot be certain of the effects of later school start times.
Overall completeness and applicability of evidence
Owing both to the variety of outcomes and the poor study designs available, the evidence is neither complete nor applicable. Many studies reported outcomes that could not be synthesized, and reporting was such that we could rarely calculate effect sizes or synthesize findings across studies. For that reason, it is difficult to draw conclusions from the current evidence base. Further, the applicability of the research is greatly limited by the study designs available; without rigorous RCTs, it is difficult to assess the impact of later school start times, especially as there are numerous potential confounders. Without random assignment, we cannot be certain if characteristics about a school or school district make it more likely to delay school start times; for example, a school with more resources may be more likely to delay its start time than a school with limited resources, and therefore any outcomes observed may be due to differences in resources, not the delay in school start time. In the same way, schools that are more or less urban, better or worse performing, more or less academically rigorous, or with more or fewer teachers, after school programs, or special education students, may all be more or less likely to alter their school start time, which would present potential confounders to any findings. Random assignment would account for these differences, and without it, one cannot be certain that demographic, performance, or other factors within a school or district were driving the observed changes. Moreover, because the included studies all manipulated school start times in different ways, either because the number of minutes of delay or because the school start times themselves were different, it is difficult to apply this evidence to future decisions. Policymakers must determine not only if they wish to delay their start time, but also by how many minutes, and the evidence presented in this review does not provide sufficient information to answer these questions. Moreover, the studies themselves often observed delayed school starts for only one year; it is possible that changes do not manifest quickly enough to be reflected in such studies.
Strengths, weaknesses, contributions and gaps of included studies
Of the eleven included studies, seven used non‐randomized, quasi‐experimental designs (Borlase 2013; Brown 2011; Edwards 2012; Hinrichs 2011; Hoehn 2015; Milic 2014; Paksarian 2015), which entail potential threats to internal validity related to maturation, history, and selection bias. Three additional studies used CBA (Brandalize 2011; Wahlstrom 2002; Wahlstrom 2014), which have similar threats to internal validity but at least attempt to measure and adjust for baseline differences between groups. We reviewed 61 other potentially relevant studies and excluded many for methodological reasons. Primarily these were study designs that did not have a comparison group and had insufficient pre‐ and post‐data points to be eligible as an ITS. Other studies had no pre‐intervention data. Many of the excluded studies reported provocative findings and contained potentially useful contextual information, but we could not formally include them. In addition, many studies did not provide comparable outcomes, precluding synthesis. While our intention was to include a detailed analysis of differential effects, we were not able to do this due to limitations in the amount of detail that was reported in studies or the lack of differential analyses.
The included studies also did not permit the answering of many questions that might be of potential interest to readers of the review: for example, they did not explain if students were informed of the rationale for delaying start time, which might affect self‐reported answers, and they did not provide comparative information concerning youth's sleep hygiene habits. Further, most studies did not examine dosage or timing effects that would allow readers to better understand if delaying school by 20 minutes was associated with fewer benefits than delaying by 45 minutes, or if there is a time of day past which delays no longer bring benefits. Because of the low quality of the included studies and the limitations of their reporting, we could not answer these questions.
Most importantly, the quality of the body of evidence makes synthesizing effect sizes and drawing conclusions quite difficult; because of the low methodological standards, the variety of particular interventions, and the variation of outcomes measured, meta‐analysis was not possible for most of the recorded outcomes. Further, many studies did not report sufficient data needed to calculate effect sizes, meaning that beyond a synthesis of the data, for several studies we could not provide comparable effect sizes for even narrative synthesis. The presence of only one cluster RCT—albeit a weakly designed RCT that featured a one‐week intervention‐means that the weak internal validity in this body of literature precludes strong causal inferences about the effects of later school start times on high school students' outcomes.
Report on practical significance
The findings from the quantitative synthesis indicated that later school start times might increase students’ sleep by an average of 83.4 minutes per night— an effect with potential practical and clinical significance. Nonetheless, because of the very low quality of the evidence and the difficulty in extracting sufficient data needed to calculate effect sizes, the practical significance of findings from the quantitative synthesis is rather limited. Even where individual effect sizes were calculated and statistically significant, the low quality of studies was such that we would advise against drawing practical conclusions, especially from any given single study.
Report on equity
We used the Cochrane Collaboration Equity Field's Equity Checklist for Systematic Review Authors ‐ 2009 to guide us as we aimed to promote and support health equity in the conduct and completion of this review. We were disappointed with the limited amount of information that was available about the differential effects of interventions across population sub‐groups; however, we dedicate a small section of the discussion and review findings to the potential implications for health equity as well as whether there are research needs that have become evident in the conduct of the review that are specific to promoting health equity.
Quality of the evidence
The quality of the evidence was fairly uniform in that it suffered from poor design and vague reporting that made drawing conclusions difficult. Because school start times are set at the school level by policies made by the district, school start time cannot spread, and the studies therefore have no risk of treatment contamination. Nonetheless, all studies were marked by at least two areas of high risk, and most by far more. The GRADE assessment of the evidence for all primary outcomes was very low.
Potential biases in the review process
The rigorous search, screening, and extraction process, conducted by at least two review authors independently at all stages, allowed us to identify all applicable studies as defined by our inclusion criteria. Our most up to date search (February 2016) ensures that we have captured the evidence base as it currently exists across a wide variety of academic journals and sources of grey literature.
Due to the reporting of primary studies, we could not calculate effect sizes for several studies (Edwards 2012; Hinrichs 2011; Hoehn 2015; Paksarian 2015; Wahlstrom 2002; Wahlstrom 2014). We contacted all authors and hoped to update this review with effect sizes from their studies, but the lack of response from authors could be considered a limitation that contributes to reporting bias. Further, although we explored many sources of grey literature, we did not locate any eligible studies in the grey literature, which may also indicate reporting bias.
Agreements and disagreements with other studies or reviews
Public support and initial scientific research seems to show that later school starts may be an important tool for combating adolescent sleep loss and the negative outcomes associated with sleep deprivation. Because of this, many have argued for later school start times as a means of increasing adolescents' school‐night sleep duration. Even a moderate sleep increase (30 minutes to one hour) over a period of time has shown to be associated with increased scores on various performance tasks (e.g. reaction times and memory tests) in an RCT study (Sadeh 2003). Shortened sleep times (later bed times paired with earlier wake times), have also been reported to correlate with lower academic performance, grade point averages, and motivation levels in prior cluster and/or cross‐over trials (as reported by Wolfson 2003). Further, more sleep and later weekday rise times may be associated with better grades and a higher motivation to do well in school (Wolfson 2003). However, this review was unable to support or transcend the evidence found by other studies to provide reliable, generalizable evidence for the effectiveness of later school starts for increased adolescent sleep duration. It is our hope that updates to this review, which will include more and higher quality studies, will be able to provide stronger conclusions regarding the potential effects of later school start times on students' outcomes.

Study flow diagram.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Forest plot of comparison: 1 Early school start vs late school start, outcome: 1.1 School‐night sleep duration.

Forest plot of comparison: 1 Early school start vs Late school start, outcome: 1.2 BMI Score ‐ Cross‐over trial.

Forest plot of comparison: 1 Early school start vs Late school start, outcome: 1.3 Waist Circumference ‐ Cross‐over trial.

Forest plot of comparison: 1 Early school start vs Late school start, outcome: 1.4 Body Fat ‐ Cross‐over trial.
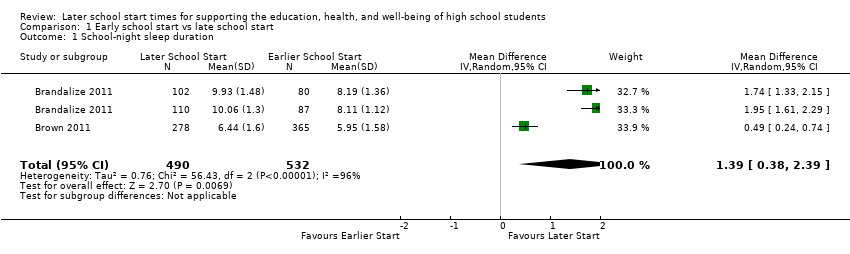
Comparison 1 Early school start vs late school start, Outcome 1 School‐night sleep duration.
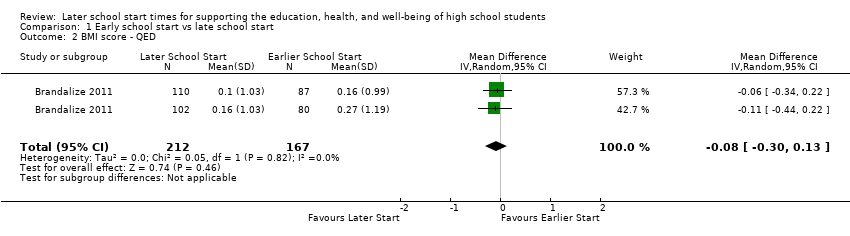
Comparison 1 Early school start vs late school start, Outcome 2 BMI score ‐ QED.

Comparison 1 Early school start vs late school start, Outcome 3 Waist circumference ‐ QED.

Comparison 1 Early school start vs late school start, Outcome 4 Body fat ‐ QED.
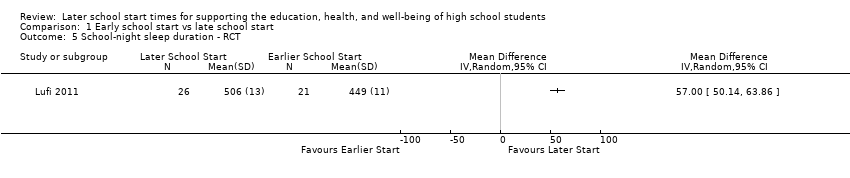
Comparison 1 Early school start vs late school start, Outcome 5 School‐night sleep duration ‐ RCT.

Comparison 1 Early school start vs late school start, Outcome 6 Concentration performance ‐ RCT.

Comparison 1 Early school start vs late school start, Outcome 7 Attention level ‐ RCT.
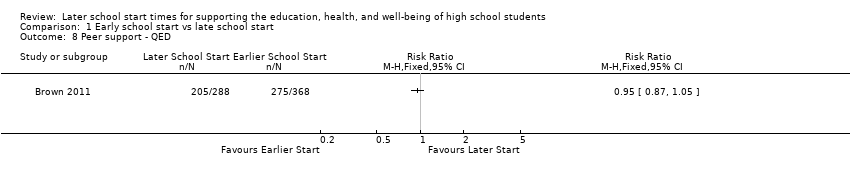
Comparison 1 Early school start vs late school start, Outcome 8 Peer support ‐ QED.

Comparison 1 Early school start vs late school start, Outcome 9 Social support ‐ QED.

Comparison 1 Early school start vs late school start, Outcome 10 Extracurricular activities ‐ QED.
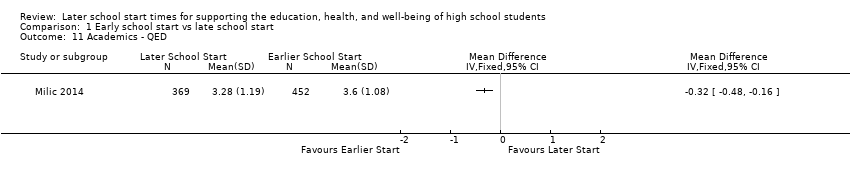
Comparison 1 Early school start vs late school start, Outcome 11 Academics ‐ QED.

Comparison 1 Early school start vs late school start, Outcome 12 Risk of losing sleep ‐ QED.

Comparison 1 Early school start vs late school start, Outcome 13 Overly sleepy ‐ QED.

Comparison 1 Early school start vs late school start, Outcome 14 Sleepiness ‐ QED.

Comparison 1 Early school start vs late school start, Outcome 15 Percentage of students getting adequate sleep.
| Early versus delayed school starts | |||
| Patient or population: students aged 13‐19 | |||
| Outcomes | Impacts | № of Participants (studies) | Quality of the evidence |
| Student academic outcomes | There is no clear association between later school start times and student academic outcomes, as two studies reported significant positive associations (b = 1.78, b = 0.98; effect sizes could not be calculated from one study), one study reported a non‐significant negative association (b = −0.02), and one study reported a significant negative association (MD −0.32 GPA points on a scale of 0 to 4, with higher GPAs indicating better grades). | 254,743 (4) | ⊕⊝⊝⊝ |
| Amount or quality of sleep | All studies that evaluated the association between later school start times and amount or quality of sleep reported significant positive associations, providing evidence that later school start times are associated with increased sleep (effect sizes ranged from MD 0.49 to 1.95 hours) and lower risk of losing sleep (RR 0.41). | 52,340 (8) | ⊕⊝⊝⊝ |
| Mental health outcomes | There is limited evidence concerning the association between later school start times and mental health outcomes: one study reported significant differences in self‐reported depression symptoms for students in later starting schools (07:25 and 08:30) than earlier starting schools (07:15), but no significant difference between students starting school at 08:30 vs 07:25. | 1200 (1) | ⊕⊝⊝⊝ |
| Truancy or attendance outcomes | There is mixed evidence concerning the association between later school starts and attendance outcomes: one study reported a significant increase in attendance, one study reported a non‐significant increase in attendance, and one study reported a significant increase in attendance for 2 of 6 schools and non‐significant effects (no further information provided) for the other 4 schools. | 255,122 (4) | ⊕⊝⊝⊝ |
| Alertness | There is mixed evidence concerning the association between later school starts and student reports of alertness or sleepiness. Two studies found an association between later school start times and decreased daytime sleepiness, while one study found no difference between student reports at later and earlier starting schools. One study reported a significant increase in attention levels but a non‐significant increase in concentration levels. | 2735 (4) | ⊕⊝⊝⊝ |
| Adverse events/unintended consequences | Authors provided limited information concerning adverse events and unintended consequences but did offer that later school start times may be associated with decreased morning interactions between parents and children, decreased alertness in mid‐afternoon, and increased logistical challenges, including missing extracurricular activities, transportation troubles, and safety concerns (as students may have to walk home in the dark). | 207,576 (4) | ⊕⊝⊝⊝ |
| b: regression coefficient; CI: confidence interval; GPA: grade point average; MD: mean difference; RR: risk ratio | |||
| GRADE Working Group grades of evidence | |||
| aDowngraded one level (from starting point of 'low' for observational study designs). The GRADE rating of 'very low' for all findings reflects study designs (absence of RCTs), high risk of bias within the studies, and inconsistency within the estimates. | |||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 School‐night sleep duration Show forest plot | 2 | 1022 | Mean Difference (IV, Random, 95% CI) | 1.39 [0.38, 2.39] |
| 2 BMI score ‐ QED Show forest plot | 1 | 379 | Mean Difference (IV, Random, 95% CI) | ‐0.08 [‐0.30, 0.13] |
| 3 Waist circumference ‐ QED Show forest plot | 1 | 379 | Mean Difference (IV, Random, 95% CI) | ‐1.14 [‐3.34, 1.06] |
| 4 Body fat ‐ QED Show forest plot | 1 | 379 | Mean Difference (IV, Random, 95% CI) | ‐1.45 [‐2.63, ‐0.27] |
| 5 School‐night sleep duration ‐ RCT Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6 Concentration performance ‐ RCT Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7 Attention level ‐ RCT Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8 Peer support ‐ QED Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 9 Social support ‐ QED Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 10 Extracurricular activities ‐ QED Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 11 Academics ‐ QED Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 12 Risk of losing sleep ‐ QED Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 13 Overly sleepy ‐ QED Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 14 Sleepiness ‐ QED Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 15 Percentage of students getting adequate sleep Show forest plot | 1 | 905 | Risk Ratio (M‐H, Random, 95% CI) | 1.50 [1.33, 1.70] |