Magnesium for skeletal muscle cramps
Abstract
Background
Skeletal muscle cramps are common and often occur in association with pregnancy, advanced age, exercise or motor neuron disorders (such as amyotrophic lateral sclerosis). Typically, such cramps have no obvious underlying pathology, and so are termed idiopathic. Magnesium supplements are marketed for the prophylaxis of cramps but the efficacy of magnesium for this purpose remains unclear.
This is an update of a Cochrane Review first published in 2012, and performed to identify and incorporate more recent studies.
Objectives
To assess the effects of magnesium supplementation compared to no treatment, placebo control or other cramp therapies in people with skeletal muscle cramps.
Search methods
On 9 September 2019, we searched the Cochrane Neuromuscular Specialised Register, CENTRAL, MEDLINE, Embase, LILACS, CINAHL Plus, AMED, and SPORTDiscus. We also searched WHO‐ICTRP and ClinicalTrials.gov for registered trials that might be ongoing or unpublished, and ISI Web of Science for studies citing the studies included in this review.
Selection criteria
Randomized controlled trials (RCTs) of magnesium supplementation (in any form) to prevent skeletal muscle cramps in any patient group (i.e. all clinical presentations of cramp). We considered comparisons of magnesium with no treatment, placebo control, or other therapy.
Data collection and analysis
Two review authors independently selected trials for inclusion and extracted data. Two review authors assessed risk of bias. We attempted to contact all study authors when questions arose and obtained participant‐level data for four of the included trials, one of which was unpublished. We collected all data on adverse effects from the included RCTs.
Main results
We identified 11 trials (nine parallel‐group, two cross‐over) enrolling a total of 735 individuals, amongst whom 118 cross‐over participants additionally served as their own controls. Five trials enrolled women with pregnancy‐associated leg cramps (408 participants) and five trials enrolled people with idiopathic cramps (271 participants, with 118 additionally crossed over to control). Another study enrolled 29 people with liver cirrhosis, only some of whom suffered muscle cramps. All trials provided magnesium as an oral supplement, except for one trial which provided magnesium as a series of slow intravenous infusions. Nine trials compared magnesium to placebo, one trial compared magnesium to no treatment, calcium carbonate or vitamin B, and another trial compared magnesium to vitamin E or calcium. We judged the single trial in people with liver cirrhosis and all five trials in participants with pregnancy‐associated leg cramps to be at high risk of bias. In contrast, we rated the risk of bias high in only one of five trials in participants with idiopathic rest cramps.
For idiopathic cramps, largely in older adults (mean age 61.6 to 69.3 years) presumed to have nocturnal leg cramps (the commonest presentation), differences in measures of cramp frequency when comparing magnesium to placebo were small, not statistically significant, and showed minimal heterogeneity (I² = 0% to 12%). This includes the primary endpoint, percentage change from baseline in the number of cramps per week at four weeks (mean difference (MD) −9.59%, 95% confidence interval (CI) −23.14% to 3.97%; 3 studies, 177 participants; moderate‐certainty evidence); and the difference in the number of cramps per week at four weeks (MD −0.18 cramps/week, 95% CI −0.84 to 0.49; 5 studies, 307 participants; moderate‐certainty evidence). The percentage of individuals experiencing a 25% or better reduction in cramp rate from baseline was also no different (RR 1.04, 95% CI 0.84 to 1.29; 3 studies, 177 participants; high‐certainty evidence). Similarly, no statistically significant difference was found at four weeks in measures of cramp intensity or cramp duration. This includes the number of participants rating their cramps as moderate or severe at four weeks (RR 1.33, 95% CI 0.81 to 2.21; 2 studies, 91 participants; moderate‐certainty evidence); and the percentage of participants with the majority of cramp durations of one minute or more at four weeks (RR 1.83, 95% CI 0.74 to 4.53, 1 study, 46 participants; low‐certainty evidence).
We were unable to perform meta‐analysis for trials of pregnancy‐associated leg cramps. The single study comparing magnesium to no treatment failed to find statistically significant benefit on a three‐point ordinal scale of overall treatment efficacy. Of the three trials comparing magnesium to placebo, one found no benefit on frequency or intensity measures, another found benefit for both, and a third reported inconsistent results for frequency that could not be reconciled. The single study in people with liver cirrhosis was small and had limited reporting of cramps, but found no difference in terms of cramp frequency or cramp intensity.
Our analysis of adverse events pooled all studies, regardless of the setting in which cramps occurred. Major adverse events (occurring in 2 out of 72 magnesium recipients and 3 out of 68 placebo recipients), and withdrawals due to adverse events, were not significantly different from placebo. However, in the four studies for which it could be determined, more participants experienced minor adverse events in the magnesium group than in the placebo group (RR 1.51, 95% CI 0.98 to 2.33; 4 studies, 254 participants; low‐certainty evidence). Overall, oral magnesium was associated with mostly gastrointestinal adverse events (e.g. diarrhoea), experienced by 11% (10% in control) to 37% (14% in control) of participants.
Authors' conclusions
It is unlikely that magnesium supplementation provides clinically meaningful cramp prophylaxis to older adults experiencing skeletal muscle cramps. In contrast, for those experiencing pregnancy‐associated rest cramps the literature is conflicting and further research in this population is needed. We found no RCTs evaluating magnesium for exercise‐associated muscle cramps or disease‐state‐associated muscle cramps (for example amyotrophic lateral sclerosis/motor neuron disease) other than a single small (inconclusive) study in people with liver cirrhosis, only some of whom suffered cramps.
PICO
Plain language summary
Magnesium for muscle cramps
Review question
We reviewed the evidence about the effect of magnesium supplements on muscle cramps, and included the widest possible range of studies. This meant including studies on anyone suffering muscle cramps, regardless of why they suffered them. It also meant including studies where magnesium was given in any of the ways available. This includes being swallowed as a pill or liquid, being injected slowly over a number of hours directly into the blood ('intravenous infusion'), and being injected into muscle ('intramuscular injection'). We included studies comparing magnesium to placebo, comparing magnesium to no treatment, and comparing magnesium to other existing cramp treatments. We found a total of 11 studies. To assess benefit, we examined the effect of magnesium on cramp frequency, cramp pain, and cramp duration, and we examined the number of participants whose cramp rate reduced by 25% or more. To assess for potential harm, we examined how often major and minor adverse health events occurred.
Background
Muscle cramps are common and occur in a wide range of settings. Older adults and pregnant women commonly complain of leg cramps while they are resting, athletes can cramp when they are pushing the limits of their endurance, and some people develop muscle cramps as a symptom of other medical conditions. One potential treatment that is already being marketed to prevent muscle cramps is magnesium supplementation. Magnesium is a common mineral in our diets and extra oral supplements of this mineral are available either over the Internet or in health food stores and pharmacies (usually in the form of tablets or powders to be dissolved in water). We wanted to combine studies to get the best estimate of magnesium's effect on cramping. We also wanted to examine the effect of magnesium in different categories of cramp sufferers, in case it might work in one setting, and not another.
Study characteristics
We searched for all high‐quality published studies evaluating the effectiveness of magnesium to prevent muscle cramps and found five studies in older adults, five studies in pregnant women, and one study in people with liver cirrhosis. The studies in older adults included 271 participants (61.6 to 69.3 years of age) and the studies in pregnant women included 408 participants. The single study in people with liver cirrhosis enrolled only 29 people, not all of whom experienced cramping. There were no studies of people who cramp while exercising. Magnesium was compared to placebo in nine of 11 studies, and compared to calcium, vitamin E, vitamins B₁ and B₆, and no treatment, in two studies of pregnant women. The included studies ranged from 14 to 56 days of treatment. Magnesium was given orally in 10 of 11 studies, and by four‐hour intravenous infusion on five consecutive days in one study. Funding for included studies came from a manufacturer of magnesium tablets in two studies, independent sources in three studies, and was not reported in six studies.
Key results and certainty of the evidence
The combined results of five seemingly reliable studies suggest, with moderate‐certainty, that magnesium is unlikely to reduce the frequency or severity of muscle cramps in older adults. In contrast, the five studies in pregnant women had important limitations to their reliability (both in study design and reporting of results), did not consistently show benefit, and could not be combined. As a result we are very uncertain as to whether pregnant women experiencing muscle cramps would benefit from magnesium. The single study in people with liver cirrhosis reported no difference in cramp frequency or intensity but was too small for conclusions to be drawn.
More research on magnesium in pregnant women is needed. The same is true for those who suffer cramps associated with medical conditions, or while exercising. However older adult cramp sufferers appear unlikely to benefit from this therapy. Major side effects were infrequent and participants withdrew from the study at similar rates when given magnesium or placebo. However minor side effects, mostly diarrhoea (as would be expected from magnesium salts) and nausea, were common and affected roughly 11% (10% in control) to 37% (14% in control) of participants.
The review is up to date to September 2019.
Authors' conclusions
Summary of findings
| Magnesium compared with placebo for skeletal muscle cramps | ||||||
| Patient or population: for effects on cramps, people (other than pregnant women) with muscle cramps (largely older adults); for adverse events, all populations Settings: outpatients recruited through primary care clinics or community advertising Intervention: magnesium supplements (oral or intravenous) Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No. of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Assumed risk | Corresponding risk | |||||
| Placebo | Magnesium | |||||
| People (other than pregnant women) with muscle cramps, largely older adults | ||||||
| Cramp frequency (percentage change from baseline at 4 weeks) | The mean percentage change in cramp frequency in the control groups was −28.7% | The mean percentage change in cramp frequency in the magnesium groups was an additional 9.59% lower (23.14% lower to 3.97% higher) | MD −9.59% (−23.14 to 3.97) | 177 | ⊕⊕⊕⊝ due to imprecision | Magnesium probably results in little to no difference in cramp frequency (based on percentage change from baseline at 4 weeks). The 95% CI excludes a 25% reduction beyond placebo |
| Cramp frequency (responder analysis: 25% or better reduction at 4 weeks) | 644 per 1000 | 669 per 1000 (541 to 830) | RR 1.04 (0.84 to 1.29) | 177 | ⊕⊕⊕⊕ | Magnesium results in little to no difference in cramp frequency (based on the proportion of people responding at 4 weeks) |
| Cramp frequency (mean number of cramps per week on treatment at 4 weeks) | The mean number of cramps per week in the placebo groups while on treatment was 4.68 | The mean number of cramps per week in the magnesium groups was 0.18 cramps per week lower (0.84 lower to 0.49 higher) | MD −0.18 cramps per week (−0.84 to 0.49) | 307 | ⊕⊕⊕⊝ due to inconsistency | Magnesium probably results in little to no difference in cramp frequency (based on number of cramps per week at 4 weeks). The 95% CI excludes a 1 cramp per week reduction |
| Cramp intensity (moderate or worse at 4 weeks) | 300 per 1000 | 399 per 1000 (243 to 663) | RR 1.33 (0.81 to 2.21) | 91 (2 studies) | ⊕⊕⊕⊝ due to imprecision | Magnesium is unlikely to reduce the number of people with cramp intensity of moderate or worse at 4 weeks |
| Cramp duration (≥ 1 minute at 4 weeks) | 227 per 1000 | 416 per 1000 (168 to 1000) | RR 1.83 (0.74 to 4.53) | 46 | ⊕⊕⊝⊝ due to very serious imprecision | Magnesium may not reduce the number of people with a cramp duration ≥ 1 minute at 4 weeks |
| Adverse events: all populations | ||||||
| Major adverse events | 33 per 1000 | 23 per 1000 (5 to 110) | RR 0.68 (0.14 to 3.31) | 185 | ⊕⊝⊝⊝ due to very serious imprecision and indirectness | It is uncertain as to whether magnesium differs from placebo in terms of major adverse events |
| Minor adverse events | 198 per 1000 | 305 per 1000 | RR 1.51 (0.98 to 2.33) | 254 (4 studies) | ⊕⊕⊝⊝ due to imprecision and indirectness | Although this difference was borderline for statistical significance, the number of people dropping out of the included studies was no different in the magnesium group than it was in the placebo group. |
| CI: confidence interval; IV: intravenous; MD: mean difference; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence | ||||||
| aDowngraded once for imprecision since our investigator‐defined 25% minimum clinically important difference (MCID) is not derived from feedback from people with cramps. A smaller MD (e.g. 20%) might still be important to some people and is not yet ruled out. An additional consideration was that 1 unpublished study combined in this analysis was rated at high risk of bias for selective (incomplete) reporting. However this study was combined with 2 studies at low risk of bias with which its findings were consistent, and our initial downgrade for imprecision due to investigator‐defined MCID was considered a soft indication for a downgrade. Hence we chose not to add a second downgrade. | ||||||
| Magnesium compared with placebo for skeletal muscle cramps | ||||||
| Patient or population: pregnant women with leg cramps Settings: outpatients recruited through obstetrical care providers Intervention: magnesium supplements (oral) Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No. of participants | Quality of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Assumed risk | Corresponding risk | |||||
| Placebo | Magnesium | |||||
| Cramp frequency (percentage change from baseline at 4 weeks) | None of the 3 relevant studies measured cramp frequency in a way that permitted pooling of data. 1 study found benefit, 1 study was uninterpretable, and 1 study (the only 1 of the 3 that was not rated high risk of bias) trended in favor of placebo. Taken collectively, no conclusions can be drawn. | 204 (3 studies) | ⊕⊝⊝⊝ due to very serious risk of bias, inconsistency, and imprecision | Whether or not magnesium supplementation reduces cramp frequency in pregnant women is uncertain | ||
| Cramp frequency (responder analysis: 25% or better reduction at 4 weeks) | ||||||
| Cramp frequency (mean number of cramps per week on treatment at 4 weeks) | ||||||
| Cramp intensity (moderate or worse at 4 weeks) | None of the studies reported cramp intensity in a way that permitted this to be determined. | No studies | No evidence | |||
| Cramp duration (≥ 1 minute at 4 weeks) | None of the studies reported cramp duration | No studies | No evidence | |||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aDowngraded twice for very serious risk of bias given 2 of the 3 studies were considered at high risk of bias; downgraded once for inconsistency given 1 study reported benefit and another trended towards harm; and downgraded once for imprecision given all studies were relatively small (largest had 86 participants) and none could be pooled. | ||||||
Background
Description of the condition
Skeletal muscle cramps are sudden, involuntary, painful, and palpable muscle contractions lasting seconds to minutes. Skeletal muscle cramps can be disease‐associated but are more commonly idiopathic, that is they occur in the absence of obvious pathology. An understanding of the mechanism behind muscle cramps is lacking but a variety of evidence points either to the lower motor neuron or its distal axonal extensions as the site of origin (Miller 2005). In support of this, neuromuscular diseases associated with cramps are those that involve the lower motor neuron (e.g. amyotrophic lateral sclerosis, which is also known as motor neuron disease (ALS/MND), recovered poliomyelitis, nerve root compression, and polyneuropathies), while diseases of the muscle or central nervous system are not usually associated with cramps. Other conditions associated with cramps include some metabolic diseases (for example liver failure), medications (for example diuretics and inhaled beta‐agonists), and haemodialysis (especially if large volumes of fluid are being removed) (Garrison 2012a; McGee 1990). Cramping is commonly seen in the absence of serious disease, however, and is more frequent in individuals who are either elderly, pregnant, continuing to contract a muscle already at its shortest length, or exercising vigorously.
Exercise‐associated muscle cramps occur either during or immediately following intense exercise, usually in the exercising muscle groups (Schwellnus 2008). In contrast, cramps associated with pregnancy or advanced age occur in the legs or feet during periods of prolonged inactivity, such as while lying in bed at night, when they are termed rest cramps or nocturnal leg cramps. Rest cramps associated with aging are very common in general practice. Within a UK general practice population, roughly one‐third of men and women over the age of 50 reported experiencing a rest cramp during the preceding two months and of those who experienced such cramps, 40% cramped three or more times per week and six per cent cramped nightly (Naylor 1994). Although they can occasionally occur in the same people and share a similar name, rest cramps and restless leg syndrome should not be confused. Restless leg syndrome is not painful and has no palpable muscle tightening, rather it is an unpleasant sensation of 'needing to move' one's legs that prevents relaxation.
Description of the intervention
Magnesium (chemical symbol: Mg) is the fourth most abundant mineral in the human body and a normal component of a typical diet. Foods which are generally high in magnesium include dark green leafy vegetables, legumes, nuts, seeds, and unrefined grains. Oral magnesium supplements are also widely available without prescription and many of these are actively marketed for cramp prophylaxis. Such supplements are salts of magnesium and typically combine magnesium with citrate, lactate, gluconate, malate, orotate, chloride, oxide, carbonate, hydroxide, sulphate, or combinations of these anions. Most are in tablet form but some are available as liquid suspensions or as powders or crystals to be dissolved in water. Magnesium is absorbed largely in the small bowel by both passive diffusion and by a saturable active transport mechanism that results in a smaller percentage of the ingested oral magnesium being absorbed as dosage increases (Graham 1960; Quamme 2008). As a result, higher doses of oral magnesium salts can potentially lead to diarrhoea because of osmotic retention of fluid within the colon. Some magnesium salts, such as magnesium sulphate and magnesium hydroxide, are commonly employed as laxatives for that reason. Other than the diarrhoea occurring with high doses, oral magnesium supplements are generally considered to be safe and relatively free of adverse effects. Injectable magnesium salts (e.g. magnesium sulphate) are also available and are indicated intravenously (IV) in some countries for the acute management of seizures, especially in pregnancy (eclampsia). Excessively rapid IV magnesium infusion can lead to cardiorespiratory suppression and flaccid paralysis of skeletal muscle (AHFS 2010). Although the IV preparation can be given intramuscularly (IM), it is associated with discomfort at the injection site.
How the intervention might work
The demonstrated efficacy of IV magnesium to prevent eclamptic seizures (Eclampsia Trialists 1995; MAGPIE 2002), and the neuromuscular suppression (loss of strength, diminished reflexes) which can manifest when high parenteral doses of magnesium are used (Somjen 1966), both suggest that magnesium could potentially play a role in reducing neuromuscular excitability. Although the mechanism behind skeletal muscle cramps is unclear, if a threshold for depolarization needs to be reached within motor neurons to initiate cramping, anything which conceivably reduces excitability might provide cramp prophylaxis. Hence, if magnesium supplementation were to truly suppress excitable tissue, it might also suppress muscle cramps. This would be consistent with the description of symptoms said to arise from severe magnesium deficiency, which include muscle cramping, though probably as a manifestation of tetany (Bilbey 1996; Hall 1973; Shils 1969).
Why it is important to do this review
The only intervention for cramp prophylaxis whose (modest) efficacy is supported by systematic review is the antimalarial drug quinine. Compared to placebo, over a two‐week interval quinine significantly reduced cramp number by 28%, cramp intensity by 10% and number of cramp days by 20% (El‐Tawil 2015). Cramp duration remained unchanged. Unfortunately, quinine has also been associated with significant haematologic and cardiac toxicity and its use as an off‐label cramp prophylactic has been actively discouraged by multiple drug regulatory agencies such as the US Food and Drug Administration (FDA) and its counterparts in Australia and New Zealand (ADRAC 2002; FDA 2006; Medsafe 2007). The commonest non‐prescription alternative to quinine for the prophylaxis of cramps, widely marketed over the Internet and readily available in both pharmacies and health food stores, is oral magnesium supplementation. We are aware of several studies employing oral magnesium for rest cramp prophylaxis in both pregnant and elderly populations. We are also aware that these data conflict to some degree. Given how common skeletal muscle cramps are, especially in older adults, an effective and safe alternative to quinine is needed. With this review we hope to determine whether, in any setting in which skeletal muscle cramps occur, magnesium supplementation provides effective cramp prophylaxis. The current version of this review is an update, with the original protocol published in 2011 (Garrison 2011b), and the original full review published in 2012 (Garrison 2012b).
Objectives
To assess the effects of magnesium supplementation compared to no treatment, placebo control, or other cramp therapies in people with skeletal muscle cramps.
Methods
Criteria for considering studies for this review
Types of studies
Open‐label, single‐blind, or double‐blind randomized controlled trials (RCTs) (including parallel‐group and cross‐over trials). We did not exclude studies based on language or publication status.
Types of participants
People in any age group with any form of skeletal muscle cramp, whether idiopathic or disease‐associated, and in any body part.
Participants potentially included (but were not limited to) those with nocturnal leg cramps, pregnancy‐associated leg cramps, exercise‐associated cramps, and disease‐state‐associated cramps such as those associated with ALS/MND, haemodialysis or liver failure.
Types of interventions
Magnesium salts and combinations of salts (e.g. magnesium citrate, lactate, gluconate, malate, orotate, chloride, oxide, carbonate, hydroxide, or sulphate) administered orally or parenterally (IM or IV) at any dose. We excluded trials if the intervention combined magnesium salts with other active ingredients unless the same intervention was given to both groups.
Valid comparators included placebo, no treatment, or other cramp therapies (e.g. prophylactic stretching, quinine, calcium channel blockers, sodium channel blockers, electrolyte supplements, or supplemental hydration).
Types of outcome measures
The outcomes gathered for meta‐analysis are listed below, but we used none as criteria for study inclusion.
Primary outcomes
Cramp frequency (percentage change from baseline at 4 weeks), measured as the per cent change from baseline in the number of muscle cramps per week at four weeks
We chose per cent change from baseline in the number of muscle cramps per week as the primary outcome because we believe it to be the most clinically relevant outcome measure and because the effect of cramp treatments in general is more likely to be proportional to baseline cramp rate than to be additive (i.e. a person with 20 cramps per week and a person with two cramps per week who receive benefit from a therapy are more likely to see a similar percentage reduction in cramps than to share a similar absolute reduction in the number of cramps per week).
Secondary outcomes
-
Cramp frequency (percentage change from baseline at 12 weeks)
-
Cramp frequency (responder analysis), measured as the percentage of participants with at least a 25% reduction from baseline in the number of muscle cramps per week at four weeks and 12 weeks
We performed a responder analysis as a secondary outcome since most therapies only work in a subset of individuals. Hence, it is useful to know how many people experience what we believe to be the minimum clinically important difference (a 25% reduction in cramp rate).
-
Cramp frequency (cramps per week on treatment), measured as the number of cramps per week at four weeks and 12 weeks
We chose this as a secondary outcome to improve the ability to pool results if studies did not report baseline cramp rates. We also chose this measure because percentage change in cramp rate (the primary outcome) can have low power when the correlation between baseline and post‐treatment measures is low (i.e. Pearson correlation coefficient less than 0.5) and in this low range of correlation the difference between treatment groups at the end of treatment offers better power than either percentage change or absolute change from baseline (Vickers 2001). In a recent RCT that we conducted (five consecutive days of IV magnesium versus IV placebo infusions in nocturnal leg cramp sufferers with comparison of change in cramp rate from baseline at days 30 and 90), we found the correlation coefficient between baseline and post‐treatment cramps to be approximately 0.5 (Garrison 2011a). We believe the minimum clinically important difference for this measure to be one cramp per week.
-
Cramp intensity (pain scale), as measured on a three‐point scale at four weeks and 12 weeks
We chose to work with a three‐point intensity scale believing that some studies would record intensity as mild, moderate, or severe. If discretely recorded in this way, we would consider that mild equals 1, moderate equals 2, and severe equals 3 on our three‐point scale. We translated the mean of all cramp intensities (if cramps were individually rated) or the global assessment of cramp pain while on treatment into a three‐point scale representing cramp intensity if the study used a scale with a different range. If cramp intensity was rated on a scale from 0 to 10, for instance, we converted to a three‐point scale by multiplying mean and SD by 3/10. We analyzed intensity this way because it allowed us to combine the largest possible number of studies, and have the greatest power to demonstrate a difference between groups. However, our conversion of ordinal data to continuous data impairs the clinical interpretation of the resulting mean difference. Like the common use of standard mean difference to pool disparate scales, this measure sacrifices clinical meaning to have the greatest chance of determining whether a difference exists. To provide clinical meaning for cramp intensity, we have also included the following dichotomous measure.
-
Cramp intensity (moderate or worse), as measured by the number of individuals rating their cramps as moderate or severe (i.e. a score of at least 2 on a 3‐point intensity scale)
Counting the number of people with at least moderately painful cramps allowed us to report any change in cramp intensity in a more relatable way than a pain scale can provide.
-
Cramp duration of 1 minute or more, as measured by the number of individuals with the majority of their cramps lasting one minute or more
Knowing that duration was often being recorded categorically, and with different scales, we chose to analyse it as a dichotomous outcome in order to maximize the chance of being able to combine participant‐level data.
-
Treatment withdrawals due to adverse events
-
Minor adverse events, measured as the number of participants reporting minor adverse events (minor adverse events being symptoms not requiring medical treatment).
-
Major adverse events, measured as the number of participants reporting major adverse events (major adverse events being death, hospitalizations, or symptoms requiring medical treatment)
Search methods for identification of studies
Electronic searches
We searched the following databases.
-
Cochrane Neuromuscular Specialised Register via the Cochrane Register of Studies (CRS Web; searched 9 September 2019; Appendix 1)
-
Cochrane Central Register of Controlled Trials (CENTRAL) via the CRS Web; searched 9 September 2019; Appendix 2)
-
MEDLINE (1946 to 6 September 2019; Appendix 3)
-
Embase (1974 to 6 September 2019; Appendix 4)
-
AMED (1985 to August 2019; Appendix 5)
-
LILACS (1982 to 6 September 2019; Appendix 6)
-
CINAHL (1937 6 September 2019; Appendix 7)
-
SPORTDiscus (1985 to 6 September 2019; Appendix 8)
-
US National Institutes of Health Ongoing Trials Register (www.ClinicalTrials.gov; searched 6 September 2019; Appendix 9)
-
World Health Organization International Clinical Trials Registry Platform (WHO‐ICTRP; apps.who.int/trialsearch; searched 6 September 2019; Appendix 10)
Searching other resources
We searched ISI Web of Science for articles citing the studies included in this review (2 December 2019). To do this, we manually used their "cited reference browser" to separately locate each included study and then reviewed all titles listed as citing that work. We also checked all references in the identified trials and, when needed, contacted the trial authors for clarification and to obtain additional published or unpublished data. In our original review (2012), hoping to capture any trials that predated trial registration, we also contacted the American Food and Drug Administration (FDA), Health Canada, and relevant pharmaceutical manufacturers to request any unpublished trials that might be in their possession.
Data collection and analysis
Selection of studies
Two review authors (from SG, RS, ND) independently examined the titles and abstracts of all articles identified by the searches, obtained the full text of all potentially relevant studies and determined which studies met the inclusion criteria. A third review author (either SG or ND) was available to adjudicate any disagreements regarding study inclusion.
We created a PRISMA flow chart to outline the study selection process.
Data extraction and management
We collected information on study design and setting, participant characteristics (including cramp‐associated conditions and age), study eligibility criteria, details of the intervention(s) given, the outcomes assessed, the source of study funding and any conflicts of interest stated by the investigators. Two review authors (from SG, ND, MK, TK, GMA) independently extracted data onto specially designed forms. SG (original review) and ND (2019 update) entered data into Review Manager 5 (RevMan 5) and a second author (from VM, GMA, RS) independently checked data entry (Review Manager 2014).
Assessment of risk of bias in included studies
Two review authors (from SG, VM, GMA, TK, MK, ND) assessed the risk of bias in the included studies using the Cochrane 'Risk of bias' tool (Higgins 2011). We resolved differences in assessment of bias by consensus with a third author (SG), available in cases of disagreement. We documented the risk of bias within each study according to eight domains: sequence generation; allocation concealment; blinding of participants and personnel; blinding of outcome assessment; incomplete outcome data; selective outcome reporting; use of a cramp diary; and 'other sources of bias'. We rated the included studies at high, low, or unclear risk of bias in each domain. Use of a cramp diary was included as a dimension for bias in this review since participant recollection at the time of an exit interview is open to more bias, especially if blinding is poor. Two review authors, SG and Karim Khan (author of previous version), were also co‐authors of one of the included trials. Neither of these authors participated in the bias rating of their own trial.
Measures of treatment effect
Diary recording of individual cramps, along with their intensity and duration, was the preferred measure of cramps, but we accepted any means of recording cramp data (e.g. participant recollection at the time of reassessment) from which the number of cramps per week could be calculated. In order to combine results, the number of cramps per week needed to be reported and calculable on a continuous scale. We did not use cramp frequency data for meta‐analysis if it was reported in category ranges such as 'less than two cramps per week' or 'more than seven cramps per week'.
For duration and intensity of cramps, either an average of the duration and intensity of each cramp over the treatment period or a global assessment by each participant regarding duration and intensity was acceptable, so long as we could meaningfully convert intensity into our three‐point intensity scale, and so long as we could meaningfully apply our '1 minute or more' duration cut‐off.
We reported the mean difference (MD) and 95% confidence interval (CI) for cramp frequency, cramp intensity and cramp duration. For responder analyses and adverse events we reported the risk ratio (RR) with 95% CI.
Unit of analysis issues
For each included study, the unit of analysis and the unit of randomization (expected to be the participant) needed to match to prevent the introduction of bias. We combined continuous outcomes using the generic inverse variance method (GIV) which allowed paired data from cross‐over trials (in which participants serve as their own controls) to be combined with two‐group parallel studies. We obtained standard error estimates for included studies from intervention and control group means and standard deviations when unpaired t‐tests were applied (parallel‐group trials), and from the MD between groups and P value for the difference when paired t‐tests were used (cross‐over trials).
Dealing with missing data
We requested any missing data from the study authors. Where studies measured cramp rate, intensity, or duration in categories that did not allow us to meaningfully convert cramp rate into a continuous number of cramps per week (or intensity and duration into our three‐point scales), we described and discussed these studies but did not include them in the meta‐analysis.
Assessment of heterogeneity
We assessed heterogeneity by using a Chi² test on n minus 1 degree of freedom and by calculating the I² statistic. If I² exceeded 25% we conducted a sensitivity analysis. We considered heterogeneity to have potential clinical importance when I² exceeded 40% and also the Chi² test was significant at P less than 0.1.
Assessment of reporting biases
We planned to use a funnel plot to assess publication bias but there were too few studies for this to be meaningful. We considered outcome reporting bias in 'Risk of bias' assessments.
Data synthesis
Our inclusion criteria encompassed a wide range of diagnoses (e.g. cramps associated with exercise, pregnancy, aging or disease states such as ALS/MND) for which a variation in treatment effect was certainly possible. However, combining such disparate patient populations using a random‐effects model and producing an overall treatment effect for magnesium across all populations could have been misleading and not properly address the clinical question, which should clearly account for the clinical setting. Accordingly, we undertook a fixed‐effect analysis within each of the clearly defined clinical settings for which data were available (these being pregnancy and idiopathic leg cramps) and did not provide meta‐analysis across all participant groups. The exception to this was adverse events, which we needed to pool across patient groups in order to obtain sufficient data to report, and which we believed would be more similar across populations. Any across‐group comparison was descriptive (qualitative) in nature. For meta‐analysis within each clinical setting we calculated the I² statistic and, if it exceeded 25%, we conducted a sensitivity analysis (see Sensitivity analysis). We combined trial data identified for inclusion in this review using the Cochrane statistical package, RevMan 5 (Review Manager 2014).
Subgroup analysis and investigation of heterogeneity
An insufficient number of studies was available to permit meaningful subgroup analysis at this time.
We planned, if a sufficient number of studies had been found, to use subgroup analysis to search for variation in treatment effect and to explore possible sources of heterogeneity. Subgroups related to clinical presentation were to include gender and cramp frequency with a 'high frequency' versus 'low frequency' subgroup defined as averaging one or more cramps per day at baseline. Subgroups related to method of treatment were to include route of administration (oral versus parenteral), formulation (grouped by the specific magnesium salt used), and duration of therapy (four weeks or less, more than four to eight weeks, more than eight weeks). We intended to view results from these subgroup analyses merely as hypothesis generating. To conduct a predefined subgroup analysis we required two or more subgroups within the analysis to have a minimum of 75 participants in each treatment arm.
Sensitivity analysis
We planned in our protocol to present results both with and without the outlying trial(s), where heterogeneity exists. While 'outlying' trials potentially include trials with extreme results, we also mean it to encompass any trial with a meaningful difference in study design ‒ such as high risk of bias, differing approaches to recruitment or resulting study populations, differing intervention (e.g. dose, formulation, duration of treatment), and differing sources of funding.
Heterogeneity existed only in the trials of magnesium versus placebo for the prophylaxis of pregnancy‐associated leg cramps (three studies). None of these trials reported outcomes in a way that permitted data pooling. We discussed differences in study design that could have led to their discrepant results qualitatively.
Summarizing findings and assessing certainty of the evidence
We included 'Summary of findings' tables for magnesium versus placebo in people with idiopathic cramps and in people with pregnancy‐associated cramps. We included adverse events' data for all causes of cramp. The 'Summary of findings' table presented our assessments of the certainty of the evidence for the following outcomes.
-
Cramp frequency
-
Percentage change from baseline at four weeks
-
Responder analysis
-
Cramps per week on treatment
-
-
Cramp intensity (moderate or worse))
-
Cramp duration ≥ one minute at four weeks
-
Minor adverse events (all causes)
-
Major adverse events (all causes)
We used the GRADE approach to assess the overall certainty of the evidence for each outcome and each comparison, and used GRADEpro GDT to calculate natural frequencies (GRADEpro GDT). Starting from ’high certainty’ (because we only included RCTs), we downgraded the certainty for serious study limitations including high risk of bias, indirectness of evidence, serious inconsistency, imprecision of effect estimates, or potential publication bias. We downgraded once if a consideration was present to a serious degree and twice if very serious. We included footnotes to explain reasons for downgrading (Schünemann 2011a; Schünemann 2011b).
Results
Description of studies
Results of the search
In total (current update and original search) our search returned the following number of citations: Medline 110, Embase 93, CENTRAL 35, CINAHL Plus 21, SPORTDiscus 16, Cochrane Neuromuscular Specialized Register 7, AMED 1, LILACS 1, WHO‐ICTRP 76, ClinicalTrials.gov 3, ISI Web of Science 79.
The authors reviewed full texts of 21 studies. We excluded 10 (see Characteristics of excluded studies), leaving 10 published studies that met our inclusion criteria. Additionally, one completed but unpublished study was identified through the WHO‐ICTRP registry (NCT00963638), bringing the total of included studies to 11.
Searching CinicalTrials.gov and WHO‐ICTRP revealed one ongoing study (NCT03082625). We contacted the author and no preliminary results were available. Examining reference lists of all included studies and relevant reviews revealed two studies whose full papers we obtained but which we excluded. Contacting the FDA, Health Canada, and relevant manufacturers (for our original 2012 review) revealed no additional studies.
See Table 1 for a tabulated summary of the included trials, and Figure 1 and Figure 2 for the study flow diagrams of the original and updated searches. All included trials are in English but we made no exclusions based on language. Of the 11 included studies, seven were available for our original (2012) review and four are newly identified (Cohen‐Hagai 2018; Roguin Maor 2017; Shahraki 2006; Supakatisant 2015). Study design and participant characteristics are summarized in Table 1.
| Study | Number/design/clinical Setting | Mean age (years) | % Female | Magnesium dose and route of administration | Frequency of administration | Treatment and assessment periods | Washout period | Comparator |
|---|---|---|---|---|---|---|---|---|
| N = 29 Parallel Liver cirrhosis | 62.0 | 41.4% | 520 mg magnesium oxide tablets (315 mg elemental Mg) | Once daily | Treatment 56 Assessment 56 | Not applicable | Matched placebo tablet | |
| N = 73 Parallel Pregnancy | Not given (child‐ bearing years) | 100% | 5 mmol combination Mg lactate + Mg citrate (122 mg elemental Mg) taken orally | Once each morning and twice each evening | Treatment 21 Assessment 21 | Not applicable | Matched placebo tablet | |
| N = 45 Cross‐over Idiopathic | 61.6 | 73.3% | Mg citrate 900 mg tablet (100 mg elemental Mg) taken orally | Twice daily | Treatment 28 Assessment 28 | 28 | Matched placebo tablet | |
| N = 46 Parallel Idiopathic | 69.3 | 69.6% | 20 mmol Mg sulphate (486 mg elemental Mg) given intravenously | Once daily over 4 hrs on 5 consecutive days | Treatment 5 Assessment 90 | Not applicable | Matched placebo solution | |
| N = 45 Parallel Pregnancy | 30.9 | 100% | Mg lactate and Mg citrate chewable tablets containing 122 mg elemental Mg taken orally | Once each morning and twice each evening | Treatment 14 Assessment 14 | Not applicable | Matched placebo tablet | |
| N = 73 Cross‐over Idiopathic | 62.9 | 54.3% | 1830 mg of tri‐magnesium dicitrate powder (300 mg elemental Mg) poured from a sachet into a glass of water taken orally | Once each evening | Treatment 42 Assessment during last 28 days of treatment | First 14 days of second treatment period considered as washout | Matched placebo powder | |
| N = 40 Parallel Idiopathic | 66.6 | 57.5% | Slow release tablet of Mg lactate containing 84 mg of elemental Mg taken orally | 2 tablets twice daily | Treatment 30 Assessment 30 | Not applicable | Matched placebo tablet | |
| N = 84 Parallel Pregnancy | Not given (child‐ bearing years) | 100% | 7.5 mmol magnesium aspartate (182 mg elemental Mg) taken orally. Unclear if tablet or powder / solution | Twice daily | Treatment 14 Assessment 28 | Not applicable | 3 different comparators 1) No treatment 2) 500 mg calcium carbonate tablet once daily 3)100 mg of thiamine (vit B₁) plus 40 mg of pyridoxine (vit B₆) once daily | |
| N = 120 Parallel Pregnancy | 29.2 | 100% | 8 cc of an 8% milk of magnesium suspension (267.2 mg of elemental magnesium) | 3 times a day | Treatment 45 Assessment 90 | Not applicable | 2 different comparators 1) 100 mg of vitamin E once daily 2) 500 mg of calcium carbonate once daily | |
| N = 86 Parallel Pregnancy | 28.7 | 100% | Mg bisglycinate tablets containing 100 mg of elemental mg taken orally | 3 times a day | Treatment 28 Assessment 28 | Not applicable | Matched placebo tablets | |
| N = 94 Parallel Idiopathic | 64.9 | 63% | 865 mg magnesium oxide capsules (520 mg elemental Mg) | Once daily at bedtime | Treatment 28 Assessment 28 | Not applicable | Matched placebo capsules |
vit B₁: vitamin B₁

Study flow diagram for the original (2012) systematic review.
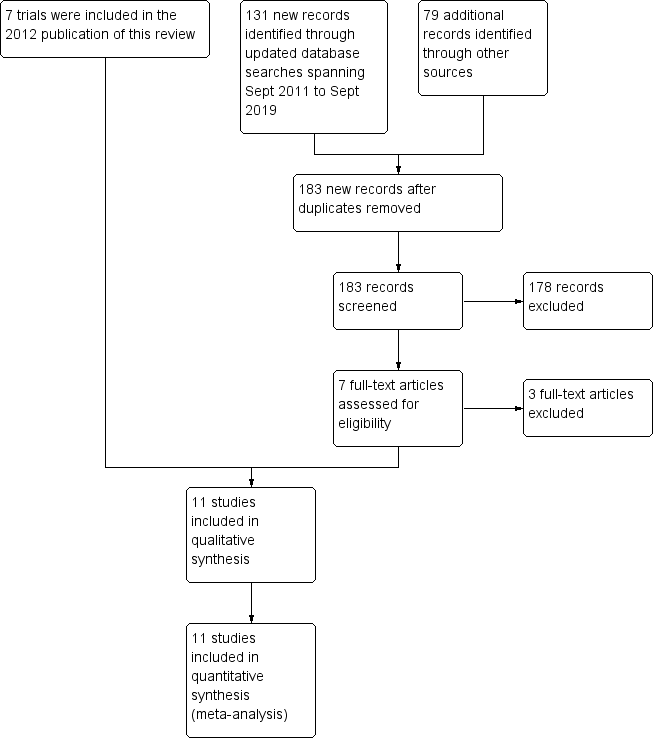
Study flow diagram for the September 2019 update.
Included studies
Study design
Nine of the studies were parallel in design (Cohen‐Hagai 2018; Dahle 1995; Garrison 2011a; NCT00963638; Nygaard 2008; Roguin Maor 2017; Shahraki 2006; Sohrabvand 2006; Supakatisant 2015); and two idiopathic cramp studies were cross‐over (Frusso 1999; Roffe 2002). One of the cross‐over trials included a 28‐day washout period (Frusso 1999). The other did not have a formal washout period but evaluated outcomes only in the last four weeks of each of two sequential six‐week treatment periods (Roffe 2002). This effectively gave a two‐week washout to those who started on magnesium and an extra two weeks of magnesium therapy (while on magnesium) prior to each evaluation period. A total of 735 participants were enrolled in these trials. Of these, 118 were participants in cross‐over trials and additionally formed their own controls. All trials were small, varying from 29 to 120 participants.
Interventions and comparators
Magnesium was generally compared to placebo (eight trials). One trial, however, with four parallel treatment arms compared no treatment to magnesium, calcium carbonate, and a combined supplement of vitamins B₁ and B₆ (Sohrabvand 2006), and one trial compared magnesium to either a calcium or a vitamin E supplement (Shahraki 2006).
Magnesium was given orally in all but one trial, where it was administered as a series of intravenous infusions (Garrison 2011a). Oral magnesium was given either once daily (Cohen‐Hagai 2018; Roffe 2002; Roguin Maor 2017); twice daily (Dahle 1995; Frusso 1999; NCT00963638; Nygaard 2008; Sohrabvand 2006), with larger doses at night in two studies (Dahle 1995; Nygaard 2008); or three times a day (Shahraki 2006; Supakatisant 2015).
The amount of elemental magnesium administered daily through the various oral protocols included 366 mg from "primarily magnesium lactate and magnesium citrate" tablets (Dahle 1995; Nygaard 2008), 200 mg from magnesium citrate tablets (Frusso 1999), 300 mg from tri‐magnesium dicitrate powder dissolved in water (Roffe 2002), 336 mg from magnesium lactate as slow‐release tablets (NCT00963638), 300 mg from magnesium bisglycinate tablets (Supakatisant 2015), 802 mg from 8% milk of magnesium suspension (Shahraki 2006), 520 mg from magnesium oxide tablets (Roguin Maor 2017), 315 mg from magnesium oxide tablets (Cohen‐Hagai 2018), and 364 mg from magnesium aspartate (Sohrabvand 2006) (unclear if tablet or powder).
The durations of treatment for oral magnesium ranged from 14 to 56 days, with total oral doses of elemental magnesium over the entire treatment period ranging from 5096 mg to 36,072 mg. The study providing magnesium intravenously gave 20 mmol of magnesium sulphate (486 mg of elemental magnesium) as an infusion over four hours on five consecutive days (Garrison 2011a). This provided a total treatment dose of 2430 mg of elemental magnesium, although with possibly different (higher) bioavailability. This trial recorded cramps for 90 days post infusions but all other trials recorded cramps over only two to four weeks.
Outcomes
Published and unpublished data were available for the following outcomes.
Cramp frequency
All five idiopathic cramps trials reported the number of cramps per week during the treatment period. Of these, three trials also provided data for per cent change from baseline in the number of cramps per week, and three trials provided data for a responder analysis (≥ 25% reduction from baseline frequency). In contrast, of the five pregnancy‐associated cramp trials, one reported per cent change from baseline, one reported a responder analysis (≥ 50% reduction from baseline frequency), and three reported cramp frequency on treatment but each was reported in a way that prevented results being combined. This included cramp frequency on a five‐point ordinal scale (daily, every other day, twice a week, once a week, never), mean number of days and nights with leg cramps present, and number of days and nights of cramping. The single trial in people with liver cirrhosis collected information on cramp frequency but did not report cramp frequencies in each group, instead reporting only 1) a P value for the difference in cramp frequency between groups and 2) the number of people who were experiencing cramps in each group at baseline and on treatment.
Cramp intensity
Four of the idiopathic cramp trials provided cramp intensity on a pain scale such that results could be scaled and pooled, and two trials provided data that allowed us to determine the number of cramps that were moderate or worse. Three of the pregnancy‐associated cramp trials reported pain intensity, but none in a way that permitted pooling of results. The single trial in people with liver cirrhosis provided only a P value for the difference in cramp intensity between groups.
Cramp duration
Four idiopathic cramp trials reported cramp duration, but only one reported it in a way that allowed us to determine the number of cramps that lasted one minute or more. None of the pregnancy‐associated trials reported cramp duration, nor did the trial in people with liver cirrhosis.
Withdrawals due to adverse effects
Most studies had omissions or inconsistencies which prevented the determination of the number of withdrawals due to adverse effects but the total number of withdrawals was available for three of five idiopathic cramp trials, all five pregnancy‐associated cramp trials, and the single trial in people with liver cirrhosis.
Minor adverse events
Most trials reported minor adverse events, but only one idiopathic cramp trial, two pregnancy‐associated cramp trials, and the single trial in people with liver‐cirrhosis‐associated muscle cramps did so in a way that allowed us to determine the number of people experiencing any minor adverse event.
Major adverse events
Major adverse events were reported in two idiopathic cramp trials and one pregnancy‐associated cramp trial.
Participants
Five studies involved treatment of pregnancy‐associated leg cramps (Dahle 1995; Nygaard 2008; Shahraki 2006; Sohrabvand 2006; Supakatisant 2015), one study involved treatment of people with liver cirrhosis (only some of whom experienced cramps) (Cohen‐Hagai 2018), and the remaining five studies involved the treatment of idiopathic cramps in older adults (most of whom are presumed to have been suffering nocturnal leg cramps) (Frusso 1999; Garrison 2011a; NCT00963638; Roffe 2002; Roguin Maor 2017). We found no studies investigating exercise‐associated cramps. All participants were community dwelling. Most participants were outpatients recruited from primary care or maternity clinics, although some were recruited by newspaper or radio advertisement. In the five trials reporting participants' age and sex, idiopathic cramp trial participants were 64.9 years of age on average and 62.1% were female. In the single study of people with liver cirrhosis, participants were 62.0 years of age and 41.4% were female. Only three of the five pregnancy‐associated cramp trials provided data on mean age (29.3 years).
Unpublished data
One of the trials was unpublished (NCT00963638), but some participant‐level data were made available to us. Three other studies also made participant‐level data available (Garrison 2011a; Roffe 2002; Roguin Maor 2017), although the data from Roffe 2002 did not include noncompleters.
See Characteristics of included studies and Additional tables.
Excluded studies
We excluded 10 studies. Excluded trials were either uncontrolled, not randomized, did not have a magnesium treatment arm, did not measure outcomes relevant to cramping, or had differences in how groups were treated other than receipt of magnesium or control. See Characteristics of excluded studies.
Ongoing studies
We identified one ongoing study (NCT03082625). See Characteristics of ongoing studies.
Risk of bias in included studies
We carried out the 'Risk of bias' assessment as outlined in the methods and summarized our assessments in Figure 3. There was considerable variability in the quality of included trials. There was also an issue with one of the cross‐over studies whose author kindly provided us participant‐level data (Roffe 2002). It is our opinion that this cross‐over trial demonstrated a large difference in treatment effect depending on the sequence of treatments. Of 17 participants receiving the sequence magnesium followed by placebo, eight favoured magnesium, seven favoured placebo, and two were unchanged. In contrast, of 29 participants receiving the sequence placebo followed by magnesium, 21 favoured magnesium, five favoured placebo, and three were unchanged. It is unclear how much of this difference was due to the period effect and how much was due either to the high rate of noncompleters (27 of 73 participants did not complete the trial), the potential for carry‐over, or the potential for unblinding. As a result of this sequence order effect we chose to minimize these potential sources of bias by using only data from the first period of the study.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study. Red (+) = high risk of bias; yellow (?) = unclear risk of bias; green (+) = low risk of bias.
Allocation
The risk of selection bias (randomization or allocation) was unclear (though likely adequate) in six of 11 trials, largely because of inadequate description of methods in the manuscripts and our inability to obtain responses from some authors (Cohen‐Hagai 2018; Dahle 1995; Frusso 1999; NCT00963638; Nygaard 2008; Sohrabvand 2006). In one cross‐over trial, the manufacturer provided randomization in large blocks that were either unbalanced initially or became unbalanced because of noncompleters (17 participants were randomized to placebo followed by magnesium and 29 to magnesium followed by placebo) (Roffe 2002). Since the treatment effect in this trial varied depending on the sequence order of treatment, this imbalance in sequence allocation was an important potential source of bias and thus we pooled data only for the first treatment period, effectively considering this as a parallel‐group study. Once this limitation to the first treatment period was made, we considered Roffe 2002 to be at low risk of allocation bias. We considered one trial at high risk of bias because it was unclear how randomization was done and no information was available regarding allocation concealment (mentioning only that a written prescription was given to each participant) (Shahraki 2006). We considered the three remaining trials at low risk of selection bias (Garrison 2011a; Roguin Maor 2017; Supakatisant 2015).
Blinding
Blinding was at low risk of bias for both performance and detection bias in six of 11 trials (Cohen‐Hagai 2018; Frusso 1999; NCT00963638; Nygaard 2008; Roguin Maor 2017; Supakatisant 2015). In one trial the risk of bias was unclear because of a greater likelihood of magnesium recipients experiencing a burning sensation at the IV site during intravenous infusion (Garrison 2011a). In one cross‐over trial the risk of bias was unclear because no description was given as to whether magnesium and placebo solutions could be distinguished by taste (Roffe 2002). In one trial, the risk of performance bias was low, but the risk of detection bias was unclear because the investigators obtained data through interview of participants, but provided no information regarding the blinding of interviewers (Dahle 1995). The risk of bias was high in two trials because they were unblinded (open label) (Sohrabvand 2006; Shahraki 2006).
Incomplete outcome data
Six of the 11 trials were at low risk of attrition bias (Dahle 1995; Frusso 1999; Garrison 2011a; NCT00963638; Roguin Maor 2017; Sohrabvand 2006). The risk of attrition bias was unclear in one trial with a 15.6% dropout rate (Nygaard 2008); and unclear in one trial that dealt with missing data by treating all participants with missing data as treatment failures ‒ as more data were missing in the control group, this favoured the intervention (Supakatisant 2015). We considered three trials at high risk of bias: the first because of a 37% dropout rate (Roffe 2002); the second because 30 out of 120 participants were not included in the analysis, and the report provided no information concerning at least 10 of them (Shahraki 2006); and the third because of a per‐protocol analysis and a large imbalance in dropout rates, with six of 14 magnesium recipients dropping out (42.8%) compared to only one of 15 (6.7%) placebo recipients (Cohen‐Hagai 2018).
Selective reporting
In six of the 11 trials, we considered the risk of reporting bias to be low (Frusso 1999; Garrison 2011a; Nygaard 2008; Roffe 2002; Roguin Maor 2017; Shahraki 2006). This included two studies whose manuscripts did report selectively (that is, both reported that some secondary outcomes were not statistically significant without providing actual numbers), but whose authors made the participant‐level data available to the authors of this review to allow for the calculation of these outcomes (Garrison 2011a; Roffe 2002). One study had an unclear risk of bias because of inconsistencies in reporting (Sohrabvand 2006). Four studies were at high risk of bias: one study because of inconsistency and possible mislabelling of results (Supakatisant 2015); one unpublished study, whose risk was high because only a subset of outcomes was available (NCT00963638); one study because it was unclear how well the outcomes were predefined (there was no description of outcomes by primary and secondary and the outcomes were incompletely described in the methods) (Dahle 1995); and one study which stated that cramp frequency and intensity were collected, but reported only P values for differences (Cohen‐Hagai 2018).
Other potential sources of bias
Cramp diary (recall bias)
We viewed two of the five trials in pregnant women as having a high risk of bias because they did not use cramp diaries (instead recalling cramp frequency at the time of exit interviews) (Dahle 1995; Sohrabvand 2006); and we considered three at unclear risk of bias because how they recorded cramps was not clear (Cohen‐Hagai 2018; Shahraki 2006; Supakatisant 2015).
Other bias
We identified no other potential sources of bias.
Effects of interventions
See: Summary of findings 1 Magnesium for idiopathic rest cramps (largely older adults); Summary of findings 2 Magnesium for pregnancy‐associated leg cramps
Magnesium versus placebo
Primary outcome: cramp frequency (percentage change from baseline at four weeks)
While all studies attempted to measure the cramp frequency, or change in cramp frequency, three trials in pregnant women used frequency measures that prevented data pooling and only one clearly used a cramp diary (Nygaard 2008). Cramp frequency measures that could not be pooled included cramp frequency on a five‐point ordinal scale (Dahle 1995), change in cramp frequency on a three‐point ordinal scale (Sohrabvand 2006), and number of days and nights in which cramps occurred (Nygaard 2008). In contrast, all five idiopathic rest cramp trials used cramp diaries and recorded the occurrence of each cramp, permitting analysis of cramp frequency as a continuous variable. The resulting pooled estimates of cramp frequency measures include data from two trials rated as having a high risk of bias, either due to a high dropout rate (Roffe 2002), which we mitigated by using only the first cross‐over period, or selective reporting (NCT00963638).
Pregnancy‐associated cramps
Only one pregnancy‐associated cramp trial reported a mean percentage reduction in the number of muscle cramps per week at four weeks (Supakatisant 2015). In this trial, 86 pregnant women received 100 mg of elemental magnesium three times daily or a matching placebo for four weeks. Participants in the magnesium group noted a 79% (95% CI 70.2% to 87.8%) mean reduction at four weeks compared to a 32.4% (95% CI 3.4% to 61.5%) reduction in the placebo group (P = 0.003). However, reporting in this trial appeared inconsistent (possibly due to a language barrier) with the authors stating and confirming by e‐mail that the median cramp rate actually increased during the trial. The other two trials did not appear to determine the baseline cramp rate needed to calculate a percentage change (Dahle 1995; Nygaard 2008).
Idiopathic rest cramps
At four weeks
Three of the five idiopathic rest cramp trials measured the baseline cramp rate over a pre‐treatment period of 30 days (Garrison 2011a), 14 days (Roguin Maor 2017), or seven days (NCT00963638). Pooling these three studies produced a small difference in the percentage change in cramp rate, magnesium versus placebo (MD −9.59%, 95% CI −23.14% to 3.97%; I² = 0%; 3 trials, 177 participants; moderate‐certainty evidence; Figure 4; Analysis 1.1). There was no evidence of heterogeneity and the resulting 95% CI excludes a 25% reduction in cramp rate over placebo.

Forest plot of comparison: 1 Idiopathic rest cramps, magnesium versus placebo, outcome: 1.1 % Change in cramp frequency from baseline at 4 weeks.
Secondary outcome: cramp frequency (percentage change from baseline at 12 weeks)
Pregnancy‐associated cramps
This outcome was not measured in the pregnancy‐associated cramp trials.
Idiopathic rest cramps
Only one study had data to 12 weeks (Garrison 2011a). The trial found a small difference in the percentage reduction in cramps for magnesium versus placebo (MD −12.09%, 95% CI −40.22% to 16.04%: 43 participants; Analysis 1.2).
Secondary outcome: cramp frequency (responder analysis)
Pregnancy‐associated cramps
None of the pregnancy‐associated cramp trials reported percentage of participants with 25% or more reduction in cramp frequency or provided sufficient data to calculate such an effect. One trial did report percentage of participants with 50% or more reduction in cramp frequency (Supakatisant 2015). In this four‐week trial, 86% of women in the magnesium group noted a 50% or more reduction compared to 60.5% of women in the placebo group (P = 0.007).
Idiopathic rest cramps
At four weeks
Pooling results from the three trials with sufficient available data to calculate this outcome showed 64.4% of participants (56 of 87) in the placebo group to have achieved a 25% or better reduction in cramp frequency (Garrison 2011a; NCT00963638; Roguin Maor 2017), compared to 60 of 90 participants (66.6%) in the magnesium group, which is essentially equivalent (RR 1.04, 95% CI 0.84 to 1.29; I² = 12%; 3 studies, 177 participants; high‐certainty evidence; Figure 5; Analysis 1.3). There was only minor heterogeneity for which we did not downgrade the certainty of the evidence.

Forest plot of comparison: 1 Magnesium versus placebo (idiopathic cramps ‐ efficacy), outcome: 1.3 Cramp frequency (responder analysis at four weeks).
At 12 weeks
The single study to 12 weeks found the percentage of participants achieving a 25% or better reduction in the frequency of cramps to be 10 of 20 participants in the placebo group (50%) and 14 of 23 participants (61%) in the magnesium group (Garrison 2011a), which is 22% higher in favour of magnesium (RR 1.22, 95% CI 0.70 to 2.10; 1 study, 43 participants; Analysis 1.4). The result was very imprecise.
Secondary outcome: cramp frequency (number of cramps on treatment)
Pregnancy‐associated cramps
At four weeks
Three trials evaluating the frequency of leg cramps compared magnesium to placebo in pregnant women (Dahle 1995; Nygaard 2008; Supakatisant 2015).
The earliest was the first published RCT of magnesium for cramping in any setting (Dahle 1995). It measured cramp frequency on a five‐point ordinal scale (daily, every other day, twice a week, once a week, never) and also measured participant evaluation of treatment effect on a five‐point ordinal scale (entirely free of symptoms, considerably improved, unchanged, worsened, considerably worsened). This study reported a reduction in the frequency of symptoms "from the initial average of every other day, to every three days in the placebo group and one to two times a week in the magnesium group (P < 0.05)". The way in which this result is reported is problematic in that "every 3 days" and "one to two times a week" do not belong to the five‐point ordinal scale used to measure this outcome. Dahle 1995 also reported benefit in participant evaluation of treatment effect, in that "the magnesium group indicated that they had to a significantly greater extent "improved considerably" or "become asymptomatic" compared with the placebo group (P = 0.0002)" (17/34 magnesium and 11/35 placebo recipients improving considerably, and 10/34 magnesium and 3/35 placebo recipients becoming asymptomatic). In contrast, the subsequent trial measured the mean number of days and nights with leg cramps present and found no significant benefit with 7.7 ± 4.7 (SD) days and nights of cramping over two weeks in the placebo group and 9.5 ± 5.1 in the magnesium group (P = 0.27) (Nygaard 2008). The most recent trial in pregnancy‐associated cramps reported an increase in the median number of cramps per week in both the magnesium (1 cramp per week increase) and placebo groups (3 cramps per week increase) (Supakatisant 2015). These increases, which we confirmed with the trial authors, are hard to reconcile with the substantial mean percentage reduction in cramp rate for both groups that the trial authors simultaneously report.
At 12 weeks
There were no trials of more than four weeks' duration that compared magnesium to placebo in pregnant women.
Idiopathic rest cramps
At four weeks
Cramps per week on treatment was available as an outcome for all five of the idiopathic rest cramp trials. The pooled estimate for the number of cramps per week was MD −0.18 cramps per week for magnesium versus placebo (95% CI −0.84 to 0.49; I² = 0; 5 studies, 307 participants; moderate‐certainty evidence due to inconsistency; Figure 6; Analysis 1.5). There was no evidence of heterogeneity and the CI excluded a 'one cramp per week' reduction. However the overall estimate is pulled towards less benefit by one trial with 70% of the weighting in the analysis. If this heavily weighted trial were removed the (non‐significant) pooled estimate would be for a 'one cramp per week' reduction. Hence there is some inconsistency in the results. As mentioned under Included studies, we used data from only the first period of Roffe 2002 because of an unbalanced randomization and a difference in benefit depending on treatment order.

Forest plot of comparison: 1 Idiopathic rest cramps, magnesium versus placebo, outcome: 1.6 Number of cramps per week at 4 weeks.
At 12 weeks
The single study to 12 weeks found a nonsignificant MD in the number of cramps per week of −0.84 (95% CI −3.23 to 1.55; 1 study, 43 participants; Analysis 1.6) (Garrison 2011a). The result was very imprecise and consistent with a difference of more than a one cramp per week reduction in favour of either magnesium or placebo.
Liver‐cirrhosis‐associated cramps
Although the single trial in people with liver cirrhosis collected data on cramp frequency, the trialists reported only that at eight weeks: "Improvement in the severity and frequency of muscle cramps was not significant (P = 0.438 and 0.483 respectively)" (Cohen‐Hagai 2018). They additionally reported that in the intervention group, the percentage of people experiencing cramps fell from 80% at baseline to 22.2% at eight weeks, compared to the percentage of people in the control group experiencing cramps falling from 84% at baseline to 58.33% at eight weeks (with the P value stated to not be significant, but with no actual numeric P value provided). These numbers are somewhat problematic, in that it is not clear how a percentage of 22.2% could be obtained given there were only eight people analysed in the intervention group (i.e. no integer divided by eight equals 0.222). We were unable to reach the trial authors by e‐mail to obtain more information.
Secondary outcome: cramp intensity (pain scale)
Pregnancy‐associated cramps
Although all three trials comparing magnesium to placebo in pregnant women recorded cramp severity on scales which could potentially have been transformed into our three‐point scale, none reported results in a manner that allowed us to do so. In Dahle 1995, cramp intensity was recorded on a 0 mm to 100 mm visual analogue scale (VAS) but mean scores were reported without SD along with P value thresholds for the difference in change from baseline within and between groups. These results were reported as follows: "Subjectively experienced distress according to the VAS was reduced from 68.2 mm before to 47.8 mm after treatment (P < 0.05) in the placebo group and from 70.4 mm to 30.3 mm (P < 0.05) in the magnesium group. The reduction of distress in the magnesium group was significantly greater (P < 0.05) than in the placebo group." In Nygaard 2008, the intensity of cramping during each nighttime and each daytime were recorded on a 0 to 4 intensity scale (0 = no pain, 1 = light pain, 2 = medium pain, 3 = strong pain, 4 = severe pain) and added together over the two‐week assessment period. The mean of each participant's summed intensity scores was 11.4 ± 8.5 (SD) for placebo and 13.2 ± 6.5 for magnesium, with a nonsignificant P value for the difference (P = 0.46). In Supakatisant 2015, cramp intensity was recorded on a 0 mm to 100 mm VAS and results were reported as median absolute change of pain score at four weeks, being 34 mm and 53 mm with magnesium and placebo, respectively. This is difficult to interpret, as greater change is suggested in the placebo group. By contacting the authors we learned that mean cramp intensity score on the 0 mm to 100 mm VAS at four weeks was 20.3 mm with magnesium versus 32.1 mm with placebo. It seems likely that there is some mislabelling of what the reported numbers in the manuscript represent.
Idiopathic rest cramps
At four weeks
Pooling results from the four trials with available data (Frusso 1999; Garrison 2011a; Roguin Maor 2017; first period of Roffe 2002) shows, on a three‐point intensity scale, no important difference between magnesium and placebo (MD −0.02, 95% CI −0.16 to 0.12; I² = 0; 4 studies, 269 participants; Analysis 1.7).
At 12 weeks
The single study with 12‐week data showed no important difference, on a three‐point intensity scale, between magnesium and placebo (MD −0.18, 95% CI −0.55 to 0.19; 1 study, 43 participants; Analysis 1.8) (Garrison 2011a).
Liver‐cirrhosis‐associated cramps
Although the single trial in people with liver cirrhosis collected data on cramp intensity, the trialists reported only that at eight weeks: "Improvement in the severity and frequency of muscle cramps was not significant (P = 0.438 and 0.483 respectively)" (Cohen‐Hagai 2018). We were unable to reach the authors by e‐mail to obtain more information.
Secondary outcome: cramp intensity (moderate or worse)
Pregnancy‐associated cramps
None of the studies in pregnant women reported results in this way and participant‐level data were unavailable.
Idiopathic rest cramps
At four weeks
Results were not reported in this manner but participant‐level data were available from two studies (Garrison 2011a; first period of Roffe 2002) to allow us to calculate this statistic. Pooled results showed the mean percentage of placebo recipients rating their cramps as moderate or severe (i.e. 2 or 3 on the 3‐point scale) to be 30% (15 of 50 participants), with the mean percentage of magnesium recipients rating their cramps as moderate or severe being somewhat higher than in the placebo group (RR 1.33, 95% CI 0.81 to 2.21; 2 studies, 91 participants; I² = 6%; moderate‐certainty evidence; Analysis 1.9). Study populations were very different on this measure. Only three of 46 participants (6.5%) in Garrison 2011a rated their cramps as moderate to severe, compared to 25 of 45 participants (56%) in Roffe 2002. Differences in recruitment methods might account for the difference in participant populations, since Roffe 2002 recruited 100% of participants from community advertising, while Garrison 2011a recruited half from advertising and half from GP referral. Alternatively, the conversion of different scales to our three‐point scale (one integer, and one ordinal) might explain the difference. The higher dropout rate in Roffe 2002 (37% versus 0%) might also have contributed if participants who would have rated their cramps as less severe were more likely to drop out of the trial.
At 12 weeks
The single study with 12‐week data found that 10% of placebo recipients (2 of 20) and 4% (1 of 23) magnesium recipients rated their cramps as moderate or severe (RR 0.43, 95% CI 0.04 to 4.44; 1 study, 43 participants; Analysis 1.10) (Garrison 2011a).
Secondary outcome: cramp duration
Pregnancy‐associated cramps
None of the studies comparing magnesium to placebo in pregnant women recorded the duration of cramps.
Idiopathic rest cramps
At four weeks
Four idiopathic cramp trials measured cramp duration. Frusso 1999 used a four‐point ordinal scale divided into less than five minutes, 5 to 10 minutes, 10 to 30 minutes and over 30 minutes. Garrison 2011a used a three‐point ordinal scale divided into less than 1 minute, one to five minutes and over five minutes. Roffe 2002 used a three‐point ordinal scale divided into short, medium and long. Roguin Maor 2017 reported mean cramp duration in minutes. All four studies reported no statistically significant difference in duration. The single study that recorded duration using a one‐minute cut‐off found the mean percentage of placebo recipients with a majority of cramp durations of one minute or more to be 22.7% (Garrison 2011a). Five of 22 participants who received placebo and 10 of 24 participants who received magnesium experienced cramps lasting one minute or more. This favoured placebo (RR 1.83, 95% CI 0.74 to 4.53; 1 study, 46 participants; low‐certainty evidence due to imprecision; Analysis 1.11).
At 12 weeks
The single study with 12‐week data found the placebo group to have 25% (5 of 20) of participants reporting the majority of their cramps as lasting one minute or more, compared to 39% (9 of 23 participants) in the magnesium group, which also favoured placebo (RR 1.57, 95% CI 0.63 to 3.91; 1 study, 43 participants; Analysis 1.12) (Garrison 2011a). The data were very imprecise.
Secondary outcome: treatment withdrawals due to adverse events
Most studies had omissions or inconsistencies which made the determination of the number of withdrawals due to adverse effects difficult. Because we believed that the difference in withdrawals due to adverse events and the difference in total withdrawals between groups would be estimating the same parameter, we used total withdrawals for each group whenever it was unclear how many participants withdrew due to adverse effects. Neither of the cross‐over studies could be used to estimate withdrawals due to adverse effects (Frusso 1999; Roffe 2002), since information on participant experience in each period was not available (i.e. would participants withdrawing in one period have also withdrawn in the other?). Although we had participant‐level data for Roffe 2002, we could not use data from the first period to estimate withdrawals, since the data provided to us only included participants completing both study periods. Determined in this way, and using only parallel studies, 13 of 206 magnesium‐treated participants and 11 of 204 placebo group participants withdrew. The percentage difference in withdrawals across all studies (which we presume to be due to adverse events) was slightly higher in the magnesium group compared to the placebo group (RR 1.17, 95% CI 0.56 to 2.47; 7 studies, 410 participants; Analysis 2.1).
Secondary outcome: minor adverse events
Adverse events were reported in most studies but usually not in a way that allowed us to determine the number of participants reporting minor adverse events. Some studies reported any adverse events, others reported only gastrointestinal adverse events.
Pregnancy‐associated cramps
In Nygaard 2008, six of 23 participants (26.1%) in the magnesium arm and six of 22 participants (27.3%) in the placebo arm reported adverse events which were lumped together as gastrointestinal in nature (nausea, flatulence, diarrhoea, intestinal air). Dahle 1995 only noted adverse events as being infrequent (without specifying placebo versus magnesium) and consisting of "primarily slight or initial nausea". In Supakatisant 2015, 16 of 43 participants (37.2%) in the magnesium arm and six of 43 participants (14.0%) in the placebo arm reported diarrhoea, nausea, or both.
Idiopathic rest cramps
Frusso 1999 reported diarrhoea, nausea or vomiting as occurring in 10.7% of magnesium recipients and 10.1% of placebo recipients. Roguin Maor 2017 reported minor adverse events (mostly gastrointestinal) in 14 of 48 participants (29.2%) receiving magnesium and 13 of 46 participants (28.3%) receiving placebo. Roffe 2002 and Garrison 2011a reported the number of participants with different specific side effects but not the number of participants with any side effect (i.e. the same participants may be counted more than once). In Roffe 2002, diarrhoea occurred in 30% on magnesium and 17% on placebo. Constipation occurred in 13% on magnesium and 24% on placebo. Nausea, indigestion or flatulence occurred in two magnesium and four placebo participants. Other side effects included skin peeling (one on magnesium), bruising (one on placebo) and headaches (one on placebo). Garrison 2011a was different, in that it was a study of magnesium given intravenously. Side effects included asymptomatic hypotension (reported by the study nurse) in three of 24 magnesium versus none of 22 placebo participants and facial flushing being noted in nine of 24 magnesium and seven of 22 placebo recipients but not generally complained of by participants. Two magnesium recipients noted transient light‐headedness several hours after the infusions on day three and day four and more magnesium recipients noted burning of the IV site (12 of 24 versus 0 of 22) with five of 24 magnesium participants receiving some piggybacked extra dilution of the IV solution to improve tolerability.
Liver‐cirrhosis‐associated cramps
In Cohen‐Hagai 2018, three of 14 (21.4%) magnesium recipients experienced diarrhoea bad enough to stop treatment, compared to none of 15 placebo recipients. No other specific adverse effects were described.
Pregnancy‐associated, idiopathic, and liver‐cirrhosis‐associated cramps combined
Overall, when we combined data from the four trials of oral magnesium reporting the number of participants with minor adverse events (Cohen‐Hagai 2018; Nygaard 2008; Roguin Maor 2017; Supakatisant 2015), 39 of 128 magnesium‐treated participants and 25 of 126 participants in the placebo group experienced minor adverse events, which was higher in the magnesium group (RR 1.51, 95% CI 0.98 to 2.33; I² = 28.9%; 4 studies, 254 participants; low‐certainty evidence due to imprecision and indirectness; Analysis 2.2).
Secondary outcome: major adverse effects
Pregnancy‐associated cramps
Nygaard 2008 reported no major adverse events during the study. The other studies do not state this outcome explicitly.
Idiopathic rest cramps
Garrison 2011a and Roffe 2002 both reported one stroke that occurred in the placebo arms but reported no other major adverse events. Roguin Maor 2017 reported four major adverse events (hospitalizations) during the treatment phase, two in each group. These data were not available from NCT00963638; and Frusso 1999 did not explicitly state whether major adverse events occurred. When we combined data from Garrison 2011a and Roguin Maor 2017, two of 95 magnesium‐treated participants and three of 90 placebo group participants experienced major adverse events, which was similar in both groups (RR 0.68, 95% CI 0.14 to 3.31; 2 studies, 140 participants; I² = 0%; very low certainty evidence; Analysis 2.3). Being a cross‐over trial without data on all participants for both periods, Roffe 2002 could not be combined in this analysis.
Magnesium versus other treatments
Two trials in pregnant women compared magnesium with other treatments for pregnancy‐associated cramps. Sohrabvand 2006 compared no treatment to magnesium, calcium carbonate and a combined supplement of vitamins B₁ and B₆, and Shahraki 2006 compared magnesium to either a calcium or a vitamin E supplement.
Primary outcome: cramp frequency (percentage change from baseline at 4 weeks)
Pregnancy‐associated cramps
The two trials comparing magnesium to other treatments in pregnant women did not report the percentage reduction in the number of cramps (Shahraki 2006; Sohrabvand 2006).
Secondary outcome: cramp frequency (responder analysis)
Pregnancy‐associated cramps
The two trials comparing magnesium to other treatments in pregnant women did not provide the necessary data to calculate the percentage of participants with a 25% or more reduction in cramp frequency (Shahraki 2006; Sohrabvand 2006).
Secondary outcome: cramp frequency (number of cramps on treatment)
Pregnancy‐associated cramps
At four weeks
One study used four parallel treatment arms to compare no treatment with either 182 mg elemental magnesium twice daily (from magnesium aspartate), 500 mg of calcium carbonate once daily, or 100 mg of thiamine (vitamin B₁) combined with 40 mg of pyridoxine (vitamin B₆) once daily in a group of pregnant Iranian women (Sohrabvand 2006). This trial had an unusual design, with the intervention being given over two weeks but outcomes assessed over four weeks. The outcome for this study was "change in muscle spasms" on a three‐point ordinal scale of "no change", "relative improvement", and "absolute improvement." We clarified with the authors that this meant no improvement, partial resolution and complete resolution of cramping. A multinomial regression test was applied to each of the three possible response categories to see if any of the active treatment arms differed from no treatment. Significantly more women reported absolute improvement in both the B vitamin and calcium arms, but not in the magnesium arm. Neither was there a difference in relative improvement between no treatment and the magnesium arm. Comparisons between the active intervention arms were not made.
One 3‐arm study compared 8 mL of an 8% milk of magnesium suspension three times daily to either 100 mg of vitamin E once daily or 500 mg of calcium carbonate once daily in 120 pregnant women for 45 days (Shahraki 2006). This trial was considered at high risk of bias as a lot of information was unclear and data were not available for 30 of the 120 enrolled participants. Twenty of these participants were described as being excluded due to side effects, while another 10 appear unaccounted for. We sought more information by contacting the author but we got no response. They reported number of cramps per day at 45 days and not number of cramps per week at four or 12 weeks. The mean number of cramps per day in the milk of magnesium group went from 4.7 at baseline to 3.6 at 45 days. It is unclear if the difference was statistically significant. In participants using vitamin E and calcium carbonate, similar reductions in daily cramps were observed, with the mean number of cramps per day falling from 5.5 to 2.8 and from 4.9 to 3.6, respectively.
Secondary outcome: cramp intensity (pain scale)
Pregnancy‐associated cramps
None of the studies comparing magnesium to other treatments in pregnant women reported results that permitted cramp intensity to be determined as a continuous variable.
Secondary outcome: cramp intensity (moderate or worse)
Pregnancy‐associated cramps
In Shahraki 2006, cramp intensity was classified as low pain (1 to 5 on a 1 to 10 VAS) or high pain (6 to 10). The number of magnesium recipients with high pain went from 25 of 30 at baseline to 20 of 30 at day 45, as compared to vitamin E recipients (29 of 30 at baseline, 17 of 30 at day 45), and calcium carbonate recipients (29 of 30 at baseline, 23 of 30 day 45). Again, we considered this trial at high risk of bias and data are missing for 30 of the 120 enrolled participants. Patient‐level data was not available to convert to our three‐point intensity scale. Sohrabvand 2006 did not report cramp intensity.
Secondary outcome: cramp duration
Pregnancy‐associated cramps
Shahraki 2006 reported cramp duration in seconds. At 45 days, participants receiving magnesium recorded a mean reduction in cramp duration of 6.8 seconds. It was not clear if this result was statistically significant but it is likely not clinically important. Sohrabvand 2006 did not report cramp duration.
Secondary outcome: treatment withdrawals due to adverse events
Pregnancy‐associated cramps
Treatment withdrawals due to adverse events could be calculated from the two trials comparing magnesium to different treatments in pregnant women. Of these, one trial did not report any treatment withdrawal or adverse event (Sohrabvand 2006), and the other reported some withdrawals and some adverse events, but there is no information regarding at least 10 participants who were not included in the analysis (Shahraki 2006).
Secondary outcome: minor adverse events
Pregnancy‐associated cramps
Adverse events were not reported in the two trials comparing magnesium to other treatments in pregnant women.
Secondary outcome: major adverse effects
Pregnancy‐associated cramps
Adverse events were not reported in the two trials comparing magnesium to other treatments in pregnant women.
Discussion
Summary of main results
We identified 11 trials (9 parallel‐group, 2 cross‐over) enrolling a total of 735 individuals, amongst whom 118 cross‐over participants additionally served as their own controls. Our main findings are as follows.
Magnesium versus placebo
Idiopathic rest cramps
There is moderate‐certainty evidence that magnesium supplementation does not offer a clinically important benefit over placebo in the prophylaxis of idiopathic cramps in older adults (most of whom are presumed to have been experiencing nocturnal leg cramps). The difference in percentage change in cramps per week from baseline at four weeks was small and the CI excluded a 25% reduction (the difference we predefined as being clinically important). In addition, while medications are often only effective in a subset of participants, the percentage of participants obtaining a 25% or greater reduction from baseline in the number of cramps per week at four weeks was similar in both groups. This makes it less likely that a meaningful subset of participants receiving a greater than 25% benefit is being missed by averaging their results in with non‐responders. Cramp frequency was also measured looking at the number of cramps per week on treatment at four weeks. This measure allowed pooling of the largest number of studies (five studies, 307 participants) and similarly found no evidence of a difference in the change in cramps per week on treatment with a CI that excluded a 'one cramp per week' reduction.
Similarly, there is moderate‐certainty evidence that cramp intensity is no different in magnesium recipients than in placebo participants, whether measured on a three‐point pain scale at four weeks, or by examining the number of participants rating their cramps as moderate or severe. Only one study reported cramp duration in a format that allowed us to determine the number of participants with the majority of cramp durations longer than one minute. In this study, the mean percentage of participants having the majority of their cramp durations lasting one minute or longer was slightly higher in the magnesium group than the placebo group (low‐certainty evidence). Three other studies reported cramp duration in different formats and in none was there a significant difference. We also sought all the above outcomes at 12 weeks but only one study had 12‐week data. The results of this single study at 12 weeks were not materially different from the four‐week results above.
Pregnancy‐associated cramps
According to three discordant studies that we could not pool (very low certainty evidence), it is unclear whether magnesium supplementation can provide an advantage over placebo in the prophylaxis of pregnancy‐associated cramps. Dahle 1995 reported a reduction in cramp frequency on a five‐point ordinal scale, a reduction in cramp intensity on a VAS, and a more favourable global assessment of treatment effect also on a five‐point ordinal scale. In contrast, the subsequent trial measured the mean number of days and nights with leg cramps present and found no benefit (7.7 ± 4.7 (SD) days and nights of cramping over two weeks in the placebo group and 9.5 ± 5.1 in the magnesium group; P = 0.27) (Nygaard 2008). Nor was there evidence of a difference in cramp intensity (on a 5‐point ordinal scale). The most recent study reported benefit, but the results provided appear contradictory (Supakatisant 2015). Specifically, this study reported 1) a higher percentage reduction in the number of cramps per week at four weeks among magnesium recipients compared to placebo (79.0% versus 32.4%; P = 0.003); and 2) a higher proportion of participants reporting at least a 50% reduction in cramp frequency (86.0% versus 60.5%; P = 0.007), but simultaneously reported (confirmed with the trial author) that the median number of cramps per week increased in both the magnesium and placebo groups (which is not compatible with the large reported percentage reductions).
Two of these trials were parallel double‐blind RCTs in women attending Scandinavian maternity clinics and used the same intervention, a chewable tablet containing 122 mg elemental magnesium "primarily as Mg lactate or Mg citrate" taken once each morning and twice each evening (366 mg daily). Despite these similarities, they were discrepant (Dahle 1995; Nygaard 2008). Factors which might have prevented Nygaard 2008 from showing benefit include less power (although there was not even a trend to benefit) due to fewer participants (45 versus 73), a shorter period of therapy (two weeks versus three) and the lack of baseline measures of cramp frequency. The lack of baseline measures is particularly important, since the outcome was the number of cramps during the treatment period and it is not known if the mean baseline cramp rates were equal. Conversely, the trial design of Dahle 1995 might have biased towards benefit in that outcomes were not well defined (in particular no primary outcome was identified), randomization and allocation concealment were not described and no cramp diary was used. Of these, the only trial not judged to be at high risk of bias is Nygaard 2008, which found not even a trend to benefit for magnesium.
Liver‐cirrhosis‐associated cramps
The single study of magnesium in people with liver cirrhosis reported results on only 22 participants, and only about 82% of those participants were experiencing muscle cramps at baseline. Although the trial reported that no statistically significant difference in cramp frequency or cramp intensity was observed, the focus of this study was on other issues (primarily cognitive changes), it was at high risk of bias because of a per protocol analysis and a large imbalance in dropouts (42.8% dropping out of the magnesium group compared to 6.7% dropping out from the placebo group), and it was likely underpowered for this outcome. As a result, we could draw no conclusions regarding the utility of magnesium to reduce the burden of muscle cramps in people with liver cirrhosis.
Adverse events
Adverse events and withdrawals due to adverse events were poorly reported in most trials. When combining data from all trials comparing magnesium to placebo and supplementing the number of withdrawals due to adverse events with total withdrawals, we found no difference for the number of withdrawals due to adverse events. Three major adverse events (strokes or hospitalizations) were reported in the placebo groups (90 participants) and two in the magnesium group (95 participants). However, in the four of eight trials comparing oral magnesium to placebo that had relevant data, minor adverse effects were more common in the magnesium group. Qualitatively it appears that side effects while on oral magnesium are mostly gastrointestinal (e.g. diarrhoea), and common, ranging from 11% (10% in control) to 37% (14% in control) of participants. Intravenous magnesium appeared to cause a burning sensation at the IV site in half of participants (compared to none in the placebo group) and a small subset of participants had either asymptomatic hypotension or light‐headedness.
Magnesium versus other treatments
Pregnancy‐associated cramps
Two trials used a comparator other than placebo. Sohrabvand 2006 used four parallel treatment arms to compare no treatment with either oral magnesium, calcium carbonate or a combined vitamin B₁ and B₆ supplement. The outcome for this study was the participants' reporting of either no improvement, partial resolution or complete resolution of cramping. A multinomial regression test was applied to each of the three possible response categories to see if any of the active treatment arms differed from no treatment. Significantly more women reported absolute improvement in the B vitamin and calcium arms, but not in the magnesium arm. Neither was there a significant difference in relative improvement between the no treatment and the magnesium arm. Comparisons between the active intervention arms were not made. It would not be unusual for placebo to show benefit from baseline in cramp trials. One might speculate that the same 'placebo effect' benefit might be seen for any active intervention over no treatment, which makes the benefit seen for B vitamins and calcium over no treatment in this trial unreliable. Magnesium was certainly no better than calcium or vitamin B supplements, however, and was alone in not reaching significance for benefit against no treatment. Collectively, these results do not support a clinically important benefit for magnesium over no treatment. Shahraki 2006 compared magnesium to vitamin E or calcium carbonate in pregnant women for 45 days. This trial was at high risk of bias because of lack of blinding and what appeared to be a per protocol analysis. An improvement in the number of cramps per day over time was reported for the magnesium group but was not larger than the improvement seen in vitamin E or calcium carbonate recipients. Neither did the magnesium group outperform vitamin E or calcium carbonate at lowering cramp intensity or reducing cramp duration. The results of this study are hard to interpret but they do not suggest a clinically important benefit.
Effect of dose, duration and route of administration
Serum magnesium levels are known to correlate poorly with tissue magnesium, making it difficult to detect participants with magnesium deficiency in the clinic. In theory, if magnesium deficiency played a role in skeletal muscle cramping, either the duration of therapy or the total dose provided over the course of the trial might be an important variable (since a deficit might be better replaced in longer duration, higher total dose trials). The differences in dosing and duration for the oral magnesium trials is modest, with the idiopathic rest cramp trials using 200 mg to 520 mg of elemental magnesium daily over four to six weeks and the pregnancy‐associated cramp trials using 300 to 802 mg per day over 14 to 45 days. Overall, no obvious dose response is present, although the oral trials may be too few and too close in dose and duration to be able to detect any meaningful pattern. However, one trial used a series of slow IV infusions of magnesium to improve delivery and simultaneously measured 24‐hour urinary magnesium excretion to determine the extent to which participants were retaining magnesium (Garrison 2011a). Measuring the percentage retention of the infused magnesium was felt to be important because it had been used as a tool to predict total body magnesium deficiency (retention of magnesium suggesting the presence of deficiency) (al‐Ghamdi 1994; Cohen 1990; Lim 1972; Quamme 1993; Ryzen 1985), and because there is a strong positive correlation between the total amount of IV magnesium retained during replacement therapy and the rise in intracellular magnesium on skeletal muscle biopsy (Lim 1972). In this trial of IV magnesium, no correlation was found between per cent retention of magnesium on day one of infusions and the reduction in the number of cramps per week from baseline. On its own, this finding argues against a therapeutic benefit from magnesium in providing cramp prophylaxis.
Overall completeness and applicability of evidence
Idiopathic cramp sufferers are often older adults with rest cramps ‒ individuals who typically wake from sleep with cramps in the lower limbs. In our experience, this is the commonest presentation of muscle cramping in a primary care population. For this large subgroup of cramp sufferers we can say with moderate certainty that magnesium is unlikely to provide a meaningful clinical benefit. In contrast, the evidence for those with pregnancy‐associated cramps and liver‐cirrhosis‐associated cramps is far from clear, and there is no evidence for the role of magnesium in treating cramps associated with exercise or other medical conditions (e.g. motor neuron disease or renal failure).
Quality of the evidence
Idiopathic rest cramps
We identified five trials of idiopathic rest cramps (313 participants including useable cross‐over controls). The largest amount of poolable data (all five trials) was available to estimate the number of cramps per week at four weeks. In this analysis, the mean difference compared to placebo was clinically unimportant (−0.02 cramps per week), the CI excluded a 'one cramp per week' reduction, and there was no heterogeneity (I² = 0). Risk of bias was low overall for three of the five studies we combined for this analysis, and risk was mitigated for one of the two studies at high risk by using only the first study period. Concordant results were obtained for other measures of cramp frequency, including our primary outcome (per cent change from baseline in the number of cramps per week) whose 95% CI excluded the 25% reduction we had predefined as clinically important. We did not downgrade the responder analysis but did downgrade the number of cramps per week on treatment (due to inconsistency) and the percentage change from baseline (due to imprecision), providing moderate‐certainty evidence for each. We similarly found no difference in cramp intensity when examining the number of participants with moderate or worse cramps (2 studies, 91 participants, downgraded to moderate‐certainty evidence due to imprecision). And we found no difference in cramp duration when measured as cramps lasting one minute or more (1 study, 43 participants, downgraded to low‐certainty evidence due to very serious imprecision).
Pregnancy‐associated cramps
We considered all but one of the five pregnancy‐associated cramp trials to be at high risk of bias; and none measured frequency, intensity, or duration in a way that permitted us to pool data. Trial results were discrepant. Of the three trials comparing magnesium to placebo, two trials reported benefit (Supakatisant 2015; Dahle 1995), but each had inconsistency in how cramp frequency was being reported. The one trial at low overall risk of bias reported not even a trend to benefit for its frequency measure (Nygaard 2008), and the two trials comparing magnesium to other treatments (which included calcium, B vitamins, vitamin E, and no treatment), found magnesium to be no better than any of the other treatment arms (Shahraki 2006; Sohrabvand 2006). Given results were discrepant, and given the studies did not report results in a way that permitted pooling of data, we were unable to produce a meaningful estimate of effect.
Liver‐cirrhosis‐associated cramps
The single study in people with liver cirrhosis was underpowered, at high risk of bias, and did not report results in a way that allowed us to calculate any of our pre‐defined outcomes. Hence we were unable to provide a meaningful estimate of effect.
Adverse events
Only two studies (140 participants) reported major adverse events, for which we downgraded the evidence to low certainty because of very serious imprecision. Four studies (254 participants) reported the number of participants with minor adverse effects but we downgraded the evidence to low because of imprecision and indirectness (due to combining trials with multiple clinical presentations).
Potential biases in the review process
Data were available from all relevant RCTs identified for inclusion in this trial. This includes participant‐level data for three of the five trials of magnesium for idiopathic cramps in older adults, including one cross‐over trial from which we used participant‐level data (by looking at the first period only) to reduce potential bias from an unbalanced randomization and a strong treatment‐order effect (Roffe 2002). Although we were able to identify one relatively recent (2011) unpublished trial using a clinical trial registry (NCT00963638), we could be missing other unpublished RCTs that predate trial registration. However, we would expect such missing trials to be less likely to have demonstrated a significant benefit because of publication bias. All of the included trials were fairly small, ranging from 29 to 120 participants, and all had some degree of methodological limitations (Figure 3). However, heterogeneity was low whenever studies could be pooled.
Agreements and disagreements with other studies or reviews
We have found that magnesium is unlikely to provide meaningful cramp prevention to older adults (the majority of cramp sufferers), but that its role in the prophylaxis of pregnancy‐associated cramps is unclear. These are effectively the same conclusions reached in other systematic reviews, including one systematic review examining magnesium for the prevention of muscle cramps in any clinical setting (Sebo 2014), and one systematic review examining any treatments for pregnancy‐associated cramps (Zhou 2015). Although we did not attempt a systematic review of non‐randomized studies, we also know our results to be consistent with a survey in which cramp sufferers were asked to rate the effectiveness of any treatments they had tried. In that survey quinine, an agent with modest established benefit, was found to be "quite helpful", "very helpful", or "100% effective" by 16 of 18 respondents (89%), and found to be "a little help" or "useless" by 2 of 18 (11%). In comparison, magnesium was found to be "quite helpful", "very helpful", or "100% effective" by only 16 of 44 respondents (36%), and found to be "a little help" or "useless" by 28 of 44 (64%) (Blyton 2012).

Study flow diagram for the original (2012) systematic review.

Study flow diagram for the September 2019 update.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study. Red (+) = high risk of bias; yellow (?) = unclear risk of bias; green (+) = low risk of bias.

Forest plot of comparison: 1 Idiopathic rest cramps, magnesium versus placebo, outcome: 1.1 % Change in cramp frequency from baseline at 4 weeks.

Forest plot of comparison: 1 Magnesium versus placebo (idiopathic cramps ‐ efficacy), outcome: 1.3 Cramp frequency (responder analysis at four weeks).

Forest plot of comparison: 1 Idiopathic rest cramps, magnesium versus placebo, outcome: 1.6 Number of cramps per week at 4 weeks.

Comparison 1: Magnesium versus placebo (idiopathic cramps): efficacy, Outcome 1: Cramp frequency (percentage change from baseline at four weeks)

Comparison 1: Magnesium versus placebo (idiopathic cramps): efficacy, Outcome 2: Cramp frequency (percentage change from baseline at 12 weeks)

Comparison 1: Magnesium versus placebo (idiopathic cramps): efficacy, Outcome 3: Cramp frequency (responder analysis at four weeks)

Comparison 1: Magnesium versus placebo (idiopathic cramps): efficacy, Outcome 4: Cramp frequency (responder analysis at 12 weeks)

Comparison 1: Magnesium versus placebo (idiopathic cramps): efficacy, Outcome 5: Cramp frequency (number of cramps per week at four weeks)

Comparison 1: Magnesium versus placebo (idiopathic cramps): efficacy, Outcome 6: Cramp frequency (number of cramps on treatment at 12 weeks)

Comparison 1: Magnesium versus placebo (idiopathic cramps): efficacy, Outcome 7: Cramp intensity (pain scale) at four weeks

Comparison 1: Magnesium versus placebo (idiopathic cramps): efficacy, Outcome 8: Cramp intensity (pain scale) at 12 weeks

Comparison 1: Magnesium versus placebo (idiopathic cramps): efficacy, Outcome 9: Cramp intensity (moderate or worse) at four weeks

Comparison 1: Magnesium versus placebo (idiopathic cramps): efficacy, Outcome 10: Cramp intensity (moderate or worse) at 12 weeks

Comparison 1: Magnesium versus placebo (idiopathic cramps): efficacy, Outcome 11: Cramp duration ≥ 1 minute at four weeks

Comparison 1: Magnesium versus placebo (idiopathic cramps): efficacy, Outcome 12: Cramp duration ≥ 1 minute at 12 weeks

Comparison 2: Magnesium versus placebo (pregnancy‐associated, idiopathic, and liver‐cirrhosis‐associated cramps): adverse effects, Outcome 1: Treatment withdrawals due to adverse events

Comparison 2: Magnesium versus placebo (pregnancy‐associated, idiopathic, and liver‐cirrhosis‐associated cramps): adverse effects, Outcome 2: Minor adverse events

Comparison 2: Magnesium versus placebo (pregnancy‐associated, idiopathic, and liver‐cirrhosis‐associated cramps): adverse effects, Outcome 3: Major adverse events
| Magnesium compared with placebo for skeletal muscle cramps | ||||||
| Patient or population: for effects on cramps, people (other than pregnant women) with muscle cramps (largely older adults); for adverse events, all populations Settings: outpatients recruited through primary care clinics or community advertising Intervention: magnesium supplements (oral or intravenous) Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No. of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Assumed risk | Corresponding risk | |||||
| Placebo | Magnesium | |||||
| People (other than pregnant women) with muscle cramps, largely older adults | ||||||
| Cramp frequency (percentage change from baseline at 4 weeks) | The mean percentage change in cramp frequency in the control groups was −28.7% | The mean percentage change in cramp frequency in the magnesium groups was an additional 9.59% lower (23.14% lower to 3.97% higher) | MD −9.59% (−23.14 to 3.97) | 177 | ⊕⊕⊕⊝ due to imprecision | Magnesium probably results in little to no difference in cramp frequency (based on percentage change from baseline at 4 weeks). The 95% CI excludes a 25% reduction beyond placebo |
| Cramp frequency (responder analysis: 25% or better reduction at 4 weeks) | 644 per 1000 | 669 per 1000 (541 to 830) | RR 1.04 (0.84 to 1.29) | 177 | ⊕⊕⊕⊕ | Magnesium results in little to no difference in cramp frequency (based on the proportion of people responding at 4 weeks) |
| Cramp frequency (mean number of cramps per week on treatment at 4 weeks) | The mean number of cramps per week in the placebo groups while on treatment was 4.68 | The mean number of cramps per week in the magnesium groups was 0.18 cramps per week lower (0.84 lower to 0.49 higher) | MD −0.18 cramps per week (−0.84 to 0.49) | 307 | ⊕⊕⊕⊝ due to inconsistency | Magnesium probably results in little to no difference in cramp frequency (based on number of cramps per week at 4 weeks). The 95% CI excludes a 1 cramp per week reduction |
| Cramp intensity (moderate or worse at 4 weeks) | 300 per 1000 | 399 per 1000 (243 to 663) | RR 1.33 (0.81 to 2.21) | 91 (2 studies) | ⊕⊕⊕⊝ due to imprecision | Magnesium is unlikely to reduce the number of people with cramp intensity of moderate or worse at 4 weeks |
| Cramp duration (≥ 1 minute at 4 weeks) | 227 per 1000 | 416 per 1000 (168 to 1000) | RR 1.83 (0.74 to 4.53) | 46 | ⊕⊕⊝⊝ due to very serious imprecision | Magnesium may not reduce the number of people with a cramp duration ≥ 1 minute at 4 weeks |
| Adverse events: all populations | ||||||
| Major adverse events | 33 per 1000 | 23 per 1000 (5 to 110) | RR 0.68 (0.14 to 3.31) | 185 | ⊕⊝⊝⊝ due to very serious imprecision and indirectness | It is uncertain as to whether magnesium differs from placebo in terms of major adverse events |
| Minor adverse events | 198 per 1000 | 305 per 1000 | RR 1.51 (0.98 to 2.33) | 254 (4 studies) | ⊕⊕⊝⊝ due to imprecision and indirectness | Although this difference was borderline for statistical significance, the number of people dropping out of the included studies was no different in the magnesium group than it was in the placebo group. |
| CI: confidence interval; IV: intravenous; MD: mean difference; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence | ||||||
| aDowngraded once for imprecision since our investigator‐defined 25% minimum clinically important difference (MCID) is not derived from feedback from people with cramps. A smaller MD (e.g. 20%) might still be important to some people and is not yet ruled out. An additional consideration was that 1 unpublished study combined in this analysis was rated at high risk of bias for selective (incomplete) reporting. However this study was combined with 2 studies at low risk of bias with which its findings were consistent, and our initial downgrade for imprecision due to investigator‐defined MCID was considered a soft indication for a downgrade. Hence we chose not to add a second downgrade. | ||||||
| Magnesium compared with placebo for skeletal muscle cramps | ||||||
| Patient or population: pregnant women with leg cramps Settings: outpatients recruited through obstetrical care providers Intervention: magnesium supplements (oral) Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No. of participants | Quality of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Assumed risk | Corresponding risk | |||||
| Placebo | Magnesium | |||||
| Cramp frequency (percentage change from baseline at 4 weeks) | None of the 3 relevant studies measured cramp frequency in a way that permitted pooling of data. 1 study found benefit, 1 study was uninterpretable, and 1 study (the only 1 of the 3 that was not rated high risk of bias) trended in favor of placebo. Taken collectively, no conclusions can be drawn. | 204 (3 studies) | ⊕⊝⊝⊝ due to very serious risk of bias, inconsistency, and imprecision | Whether or not magnesium supplementation reduces cramp frequency in pregnant women is uncertain | ||
| Cramp frequency (responder analysis: 25% or better reduction at 4 weeks) | ||||||
| Cramp frequency (mean number of cramps per week on treatment at 4 weeks) | ||||||
| Cramp intensity (moderate or worse at 4 weeks) | None of the studies reported cramp intensity in a way that permitted this to be determined. | No studies | No evidence | |||
| Cramp duration (≥ 1 minute at 4 weeks) | None of the studies reported cramp duration | No studies | No evidence | |||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aDowngraded twice for very serious risk of bias given 2 of the 3 studies were considered at high risk of bias; downgraded once for inconsistency given 1 study reported benefit and another trended towards harm; and downgraded once for imprecision given all studies were relatively small (largest had 86 participants) and none could be pooled. | ||||||
| Study | Number/design/clinical Setting | Mean age (years) | % Female | Magnesium dose and route of administration | Frequency of administration | Treatment and assessment periods | Washout period | Comparator |
|---|---|---|---|---|---|---|---|---|
| N = 29 Parallel Liver cirrhosis | 62.0 | 41.4% | 520 mg magnesium oxide tablets (315 mg elemental Mg) | Once daily | Treatment 56 Assessment 56 | Not applicable | Matched placebo tablet | |
| N = 73 Parallel Pregnancy | Not given (child‐ bearing years) | 100% | 5 mmol combination Mg lactate + Mg citrate (122 mg elemental Mg) taken orally | Once each morning and twice each evening | Treatment 21 Assessment 21 | Not applicable | Matched placebo tablet | |
| N = 45 Cross‐over Idiopathic | 61.6 | 73.3% | Mg citrate 900 mg tablet (100 mg elemental Mg) taken orally | Twice daily | Treatment 28 Assessment 28 | 28 | Matched placebo tablet | |
| N = 46 Parallel Idiopathic | 69.3 | 69.6% | 20 mmol Mg sulphate (486 mg elemental Mg) given intravenously | Once daily over 4 hrs on 5 consecutive days | Treatment 5 Assessment 90 | Not applicable | Matched placebo solution | |
| N = 45 Parallel Pregnancy | 30.9 | 100% | Mg lactate and Mg citrate chewable tablets containing 122 mg elemental Mg taken orally | Once each morning and twice each evening | Treatment 14 Assessment 14 | Not applicable | Matched placebo tablet | |
| N = 73 Cross‐over Idiopathic | 62.9 | 54.3% | 1830 mg of tri‐magnesium dicitrate powder (300 mg elemental Mg) poured from a sachet into a glass of water taken orally | Once each evening | Treatment 42 Assessment during last 28 days of treatment | First 14 days of second treatment period considered as washout | Matched placebo powder | |
| N = 40 Parallel Idiopathic | 66.6 | 57.5% | Slow release tablet of Mg lactate containing 84 mg of elemental Mg taken orally | 2 tablets twice daily | Treatment 30 Assessment 30 | Not applicable | Matched placebo tablet | |
| N = 84 Parallel Pregnancy | Not given (child‐ bearing years) | 100% | 7.5 mmol magnesium aspartate (182 mg elemental Mg) taken orally. Unclear if tablet or powder / solution | Twice daily | Treatment 14 Assessment 28 | Not applicable | 3 different comparators 1) No treatment 2) 500 mg calcium carbonate tablet once daily 3)100 mg of thiamine (vit B₁) plus 40 mg of pyridoxine (vit B₆) once daily | |
| N = 120 Parallel Pregnancy | 29.2 | 100% | 8 cc of an 8% milk of magnesium suspension (267.2 mg of elemental magnesium) | 3 times a day | Treatment 45 Assessment 90 | Not applicable | 2 different comparators 1) 100 mg of vitamin E once daily 2) 500 mg of calcium carbonate once daily | |
| N = 86 Parallel Pregnancy | 28.7 | 100% | Mg bisglycinate tablets containing 100 mg of elemental mg taken orally | 3 times a day | Treatment 28 Assessment 28 | Not applicable | Matched placebo tablets | |
| N = 94 Parallel Idiopathic | 64.9 | 63% | 865 mg magnesium oxide capsules (520 mg elemental Mg) | Once daily at bedtime | Treatment 28 Assessment 28 | Not applicable | Matched placebo capsules | |
| vit B₁: vitamin B₁ | ||||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1.1 Cramp frequency (percentage change from baseline at four weeks) Show forest plot | 3 | 177 | Mean Difference (IV, Fixed, 95% CI) | ‐9.59 [‐23.14, 3.97] |
| 1.2 Cramp frequency (percentage change from baseline at 12 weeks) Show forest plot | 1 | 43 | Mean Difference (IV, Fixed, 95% CI) | ‐12.09 [‐40.22, 16.04] |
| 1.3 Cramp frequency (responder analysis at four weeks) Show forest plot | 3 | 177 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.84, 1.29] |
| 1.4 Cramp frequency (responder analysis at 12 weeks) Show forest plot | 1 | 43 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.22 [0.70, 2.10] |
| 1.5 Cramp frequency (number of cramps per week at four weeks) Show forest plot | 5 | 307 | Mean Difference (IV, Fixed, 95% CI) | ‐0.18 [‐0.84, 0.49] |
| 1.6 Cramp frequency (number of cramps on treatment at 12 weeks) Show forest plot | 1 | 43 | Mean Difference (IV, Fixed, 95% CI) | ‐0.84 [‐3.23, 1.55] |
| 1.7 Cramp intensity (pain scale) at four weeks Show forest plot | 4 | 269 | Mean Difference (IV, Fixed, 95% CI) | ‐0.02 [‐0.16, 0.12] |
| 1.8 Cramp intensity (pain scale) at 12 weeks Show forest plot | 1 | 43 | Mean Difference (IV, Fixed, 95% CI) | ‐0.18 [‐0.55, 0.19] |
| 1.9 Cramp intensity (moderate or worse) at four weeks Show forest plot | 2 | 91 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.33 [0.81, 2.21] |
| 1.10 Cramp intensity (moderate or worse) at 12 weeks Show forest plot | 1 | 43 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.43 [0.04, 4.44] |
| 1.11 Cramp duration ≥ 1 minute at four weeks Show forest plot | 1 | 46 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.83 [0.74, 4.53] |
| 1.12 Cramp duration ≥ 1 minute at 12 weeks Show forest plot | 1 | 43 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.57 [0.63, 3.91] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 2.1 Treatment withdrawals due to adverse events Show forest plot | 7 | 410 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.17 [0.56, 2.47] |
| 2.1.1 Idiopathic cramps (largely older adults) | 3 | 180 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.21 [0.34, 4.32] |
| 2.1.2 Pregnancy‐associated leg cramps | 3 | 201 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.38 [0.09, 1.50] |
| 2.1.3 Liver‐cirrhosis‐associated cramps | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 6.43 [0.88, 46.92] |
| 2.2 Minor adverse events Show forest plot | 4 | 254 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.51 [0.98, 2.33] |
| 2.2.1 Idiopathic cramps (largely older adults) | 1 | 94 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.55, 1.95] |
| 2.2.2 Pregnancy‐associated leg cramps | 2 | 131 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.80 [0.97, 3.34] |
| 2.2.3 Liver‐cirrhosis‐associated cramps | 1 | 29 | Risk Ratio (M‐H, Fixed, 95% CI) | 7.47 [0.42, 132.78] |
| 2.3 Major adverse events Show forest plot | 3 | 185 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.14, 3.31] |
| 2.3.1 Idiopathic cramps (largely older adults) | 2 | 140 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.14, 3.31] |
| 2.3.2 Pregnancy‐associated leg cramps | 1 | 45 | Risk Ratio (M‐H, Fixed, 95% CI) | Not estimable |