Agentes antidiabéticos orales para mujeres con diabetes establecida/tolerancia a la glucosa alterada o diabetes gestacional previa que planifican un embarazo, o embarazadas con diabetes preexistente
Resumen
Antecedentes
Si bien la mayoría de las guías recomiendan la administración de insulina en las mujeres cuyos embarazos se ven afectados por una diabetes preexistente, los agentes antidiabéticos orales pueden ser más aceptables para las mujeres. Es necesario establecer los efectos de estos agentes antidiabéticos orales sobre los resultados de la salud materna e infantil en las embarazadas con diabetes preexistente o tolerancia a la glucosa alterada, así como en las mujeres con diabetes mellitus gestacional previa o durante un embarazo posterior. Esta revisión es una actualización de una revisión que se publicó por primera vez en 2010.
Objetivos
Investigar el efecto sobre la salud materna e infantil de los agentes antidiabéticos orales en mujeres con diabetes mellitus preexistente, tolerancia a la glucosa alterada o diabetes en el embarazo anterior que planifican un embarazo, o en las embarazadas con diabetes mellitus. La administración de los agentes antidiabéticos orales para el tratamiento de la diabetes gestacional en un embarazo actual se evalúa en otra revisión Cochrane.
Métodos de búsqueda
Se hicieron búsquedas en el registro de ensayos del Grupo Cochrane de Embarazo y Parto (Cochrane Pregnancy and Childbirth Group) (31 de octubre 2016) y en las listas de referencias de los estudios recuperados.
Criterios de selección
Ensayos controlados aleatorizados (ECA) y cuasialeatorizados que evaluaron los efectos de los agentes antidiabéticos orales en mujeres con diabetes establecida, tolerancia a la glucosa alterada o diabetes gestacional previa que planificaban un embarazo, o embarazadas con diabetes preexistente. Se consideraron elegibles para inclusión los ECA grupales, aunque no se identificaron ensayos de este tipo.
Obtención y análisis de los datos
Dos autores de la revisión de forma independiente evaluaron la elegibilidad de los estudios, extrajeron los datos y evaluaron el riesgo de sesgo de los ECA incluidos. Los autores de la revisión comprobaron la exactitud de los datos y evaluaron la calidad de la evidencia mediante los criterios GRADE.
Resultados principales
Se identificaron seis ECA (707 mujeres) elegibles para inclusión en esta revisión actualizada; sin embargo, tres ECA tuvieron poblaciones mixtas (es decir, incluyeron embarazadas con diabetes gestacional) y no informaron por separado los datos del subconjunto de mujeres pertinentes para esta revisión. Por lo tanto, solo se incluyeron los datos de resultados de tres ECA; hubo datos disponibles de 241 mujeres y sus hijos. Los tres ECA compararon un agente antidiabético oral (metformina) con la insulina. Las mujeres en los ECA que contribuyeron con datos tenían diabetes tipo 2 diagnosticada antes o durante su embarazo. En general, se consideró que los ECA tuvieron riesgo variable de sesgo. La calidad de la evidencia para determinados resultados importantes se evaluó mediante los criterios GRADE; la evidencia fue de calidad baja o muy baja, y se disminuyó debido a las limitaciones de diseño (riesgo de sesgo) y a las estimaciones imprecisas del efecto (para muchos resultados sólo uno o dos ECA proporcionaron datos).
Para las medidas de resultado primarias no hubo diferencias claras entre los grupos metformina e insulina para la preeclampsia (riesgo relativo [RR] 0,63; intervalo de confianza [IC] del 95%: 0,33 a 1,20; dos ECA; 227 participantes; evidencia de calidad muy baja), aunque en un ECA las mujeres que recibieron metformina tuvieron menos probabilidades de presentar hipertensión inducida por el embarazo (RR 0,58; IC del 95%: 0,37 a 0,91; un ECA; 206 participantes; evidencia de calidad baja). Las mujeres que recibieron metformina tuvieron menos probabilidades de que se les practicara una cesárea en comparación con las que recibieron insulina (RR 0,73; IC del 95%: 0,61 a 0,88; tres ECA; 241 participantes; evidencia de calidad baja). En un ECA no hubo diferencias claras entre los grupos para los recién nacidos grandes para la edad gestacional (RR 1,12; IC del 95%: 0,73 a 1,72; un ECA; 206 participantes; evidencia de calidad muy baja). No hubo muertes perinatales en dos ECA (evidencia de calidad muy baja). No se informó del resultado compuesto de mortalidad o morbilidad neonatal, ni de la discapacidad neurosensorial de la infancia o la adultez.
Para otras medidas de resultado secundarias que se evaluaron mediante los criterios GRADE, no hubo diferencias claras entre los grupos de metformina e insulina en cuanto a la inducción del trabajo de parto (RR 1,42; IC del 95%: 0,62 a 3,28; dos ECA; 35 participantes; evidencia de calidad muy baja), aunque la hipoglucemia infantil se redujo en el grupo de metformina (RR 0,34; IC del 95%: 0,18 a 0,62; tres ECA3; 241 recién nacidos; evidencia de calidad muy baja). No se informó sobre traumas perineales, depresión postnatal materna y retención de peso postnatal, ni de adiposidad y diabetes en la infancia y la adultez.
Conclusiones de los autores
No hay suficientes datos de ECA para evaluar la administración de agentes antidiabéticos orales en mujeres con diabetes establecida, tolerancia a la glucosa alterada o diabetes gestacional previa que planifican un embarazo, o en embarazadas con diabetes preexistente. La evidencia de calidad baja a muy baja indica posibles reducciones de la hipertensión inducida por el embarazo, el parto por cesárea y la hipoglucemia neonatal con la metformina, en comparación con la insulina, para las mujeres con diabetes de tipo 2 diagnosticada antes o durante el embarazo, y no hay diferencias claras en cuanto a la preeclampsia, la inducción del trabajo de parto y los recién nacidos grandes para la edad gestacional. Se necesitan más ECA de alta calidad que comparen cualquier combinación de agente antidiabético oral, insulina y consejos dietéticos y de estilo de vida para estas mujeres. Los ECA futuros podrían tener el poder estadístico suficiente para evaluar los efectos sobre los resultados clínicos a corto y largo plazo, y podrían intentar recopilar e informar sobre los resultados estándar recomendados en esta revisión. Se han identificado cinco estudios en curso y cuatro están en espera de clasificación. Se tomarán en consideración cuando se actualice esta revisión.
PICOs
Resumen en términos sencillos
Agentes antidiabéticos orales para mujeres con diabetes o diabetes previa que planifican un embarazo, o embarazadas con diabetes preexistente
¿Cuál es el problema?
La diabetes preexistente y la diabetes gestacional pueden aumentar los riesgos de varios resultados deficientes para las madres y para los recién nacidos. En el caso de la madre, incluye la hipertensión inducida por el embarazo (preeclampsia) con retención adicional de líquidos y proteínas en la orina, así como el parto por cesárea. En el caso del recién nacido pueden incluir el parto prematuro; así como un mayor riesgo de presencia de defectos físicos al nacer como defectos cardíacos, cerebrales, de la columna vertebral y de la médula espinal, síndrome de Down y aborto espontáneo. Otras complicaciones en el parto incluyen recién nacidos grandes para su edad gestacional, y obstrucción del trabajo de parto (distocia de hombros) causada por el atasco de uno de los hombros en el canal de parto una vez que se ha producido el parto de la cabeza.
¿Por qué es esto importante?
El embarazo puede desencadenar la diabetes (diabetes gestacional) en mujeres con una tolerancia a la glucosa alterada. Las mujeres que presentan diabetes gestacional tienen un mayor riesgo de desarrollar diabetes en etapas posteriores de la vida. Lo anterior significa que el tratamiento es importante para las mujeres con una tolerancia a la glucosa alterada o con diabetes gestacional previa, así como para las mujeres con diabetes establecida. Las mujeres con diabetes establecida necesitan un buen control del azúcar en la sangre antes de quedar embarazadas. La insulina permite un buen control del azúcar en la sangre y no afecta al desarrollo del feto, pero las mujeres pueden encontrar que los agentes antidiabéticos orales son más convenientes y aceptables que las inyecciones de insulina. Sin embargo, se conoce poco sobre los efectos de estos agentes orales.
Esta revisión intentó investigar los efectos sobre la salud materna e infantil de los agentes antidiabéticos orales en las mujeres con diabetes establecida, tolerancia a la glucosa alterada o diabetes gestacional previa que planificaban un embarazo, o en las embarazadas con diabetes preexistente. Esta revisión es una actualización de una revisión que se publicó por primera vez en 2010.
¿Qué evidencia se encontró?
Se buscó evidencia de ensayos controlados aleatorizados (ECA) el 31 de octubre 2016 y se incluyeron seis ECA (707 mujeres). Tres ECA incluyeron mujeres con diabetes gestacional actual y no informaron por separado sobre datos relativos a la población de mujeres pertinentes a esta revisión. Por lo tanto, solo se incluyeron los datos de resultados de tres ECA que incluyen a 241 embarazadas y sus recién nacidos. La calidad de la evidencia se evaluó como baja o muy baja y el riesgo general de sesgo de los ECA fue variado. Los tres ECA compararon un agente antidiabético oral (metformina) con insulina en embarazadas con diabetes preexistente (tipo 2).
No hubo una diferencia clara en cuanto al desarrollo de preeclampsia (hipertensión arterial y proteínas en la orina) en las mujeres que recibieron metformina en comparación con insulina (dos ECA; 227 mujeres; evidencia de calidad muy baja), aunque las mujeres que recibieron metformina tuvieron menos probabilidades de sufrir hipertensión arterial inducida por el embarazo en un ECA (206 mujeres; evidencia de calidad baja). Las mujeres que recibieron metformina tuvieron menos probabilidades de que se les practicara una cesárea (tres ECA; 241 mujeres; evidencia de calidad baja), aunque no se observaron diferencias en la inducción del trabajo de parto (dos ECA; 35 mujeres; evidencia de calidad muy baja). No hubo diferencias claras entre los grupos de recién nacidos de madres que recibieron metformina o insulina en cuanto a grandes para la edad gestacional (un ECA; 206 recién nacidos; evidencia de calidad muy baja), aunque los recién nacidos de madres que recibieron metformina tuvieron menos probabilidades de tener un nivel bajo de azúcar en la sangre (hipoglucemia) (tres ECA; 241 recién nacidos; evidencia de calidad muy baja). No se produjeron muertes infantiles (antes del parto o poco después) (dos ECA; evidencia de calidad muy baja). Los ECA no informaron sobre muchos resultados importantes a corto y largo plazo, como el trauma perineal y el resultado combinado de muerte o morbilidad infantil, depresión postnatal y retención de peso en el caso de las madres, y adiposidad o discapacidad en la infancia o la edad adulta en el caso de los recién nacidos.
¿Qué significa esto?
No hay suficiente evidencia que sirva de guía sobre los efectos de los agentes antidiabéticos orales en las mujeres con diabetes establecida, tolerancia a la glucosa alterada o diabetes gestacional previa que planificaban un embarazo, o en las embarazadas con diabetes preexistente. Se necesitan más ECA de gran tamaño y bien diseñados que puedan evaluar e informar sobre los resultados recomendados en esta revisión, incluidos los resultados a corto y largo plazo para las madres y sus hijos.
Authors' conclusions
Summary of findings
| Maternal outcomes: oral anti‐diabetic agent (metformin) compared with insulin for women with established type 2 diabetes mellitus | ||||||
| Patient or population: women with type 2 diabetes | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | Comments | |
| Risk with insulin | Risk with oral anti‐diabetic (metformin) | |||||
| Hypertensive disorders of pregnancy: pre‐eclampsia | Study population | RR 0.63 | 227 | ⊕⊝⊝⊝ | ||
| 186 per 1000 | 117 per 1000 | |||||
| Hypertensive disorders of pregnancy: pregnancy‐induced hypertension | Study population | RR 0.58 | 206 | ⊕⊕⊝⊝ | ||
| 360 per 1000 | 209 per 1000 | |||||
| Caesarean section | Study population | RR 0.73 | 241 | ⊕⊕⊝⊝ | ||
| 765 per 1000 | 558 per 1000 | |||||
| Induction of labour | Study population | RR 1.42 | 35 | ⊕⊝⊝⊝ | ||
| 316 per 1000 | 448 per 1000 | |||||
| Perineal trauma | Study population | ‐ | (0 RCTs) | ‐ | None of the included RCTs reported this outcome | |
| See comment | See comment | |||||
| Postnatal depression | Study population | ‐ | (0 RCTs) | ‐ | None of the included RCTs reported these outcomes | |
| See comment | See comment | |||||
| Postnatal weight retention | Study population | ‐ | (0 RCTs) | ‐ | None of the included RCTs reported these outcomes | |
| See comment | See comment | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Study limitations (‐2): most of the weight in this analysis was from 1 RCT with very serious design limitations 2 Imprecision (‐2): wide 95% CI crossing the line of no effect and small sample sizes of RCTs 3 Study limitations (‐2): 1 RCT with very serious design limitations contributed data 4 Study limitations (‐1): 2 RCTs with design limitations contributed data | ||||||
| Infant outcomes: oral anti‐diabetic (metformin) compared with insulin for women with established diabetes | ||||||
| Patient or population: women with type 2 diabetes mellitus | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | Comments | |
| Risk with insulin | Risk with oral anti‐diabetic (metformin) | |||||
| Large‐for‐gestational age | Study population | RR 1.12 | 206 | ⊕⊝⊝⊝ | ||
| 270 per 1000 | 302 per 1000 | |||||
| Perinatal mortality | Study population | ‐ | 220 | ⊕⊝⊝⊝ | No perinatal mortality in the 2 RCTs | |
| See comment | See comment | |||||
| Hypoglycaemia | Study population | RR 0.34 | 241 | ⊕⊝⊝⊝ | ||
| 277 per 1000 | 94 per 1000 | |||||
| Neonatal mortality or morbidity composite | Study population | ‐ | (0 studies) | ‐ | None of the included RCTs reported this outcome | |
| See comment | See comment | |||||
| Childhood/adulthood neurosensory disability | Study population | ‐ | (0 studies) | ‐ | None of the included RCTs reported this outcome | |
| See comment | See comment | |||||
| Childhood/adulthood adiposity | Study population | ‐ | (0 studies) | ‐ | None of the included RCTs reported this outcome | |
| See comment | See comment | |||||
| Childhood/adulthood diabetes | Study population | ‐ | (0 studies) | ‐ | None of the included RCTs reported this outcome | |
| See comment | See comment | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Study limitations (‐2): 1 RCT with very serious design limitations contributed data 2 Imprecision (‐2): wide 95% CI crossing the line of no effect and small sample size of RCT 3 Study limitations (‐1): 2 RCTs with design limitations contributed data 4 Imprecision (‐2): no events 5 Study limitations (‐2): most of the weight in this analysis was from 1 RCT with very serious design limitations 6 Imprecision (‐1): small sample sizes of RCTs | ||||||
Background
Description of the condition
Established diabetes prior to pregnancy and pre‐existing diabetes in pregnancy
Pre‐existing (pregestational) diabetes affects pregnant women who have been diagnosed with type 1 or type 2 diabetes ‐ or, in rare cases, other forms of diabetes mellitus ‐ prior to becoming pregnant. While some parts of the world have a significantly higher prevalence of established diabetes than others, in 2015 it was estimated that globally one in 11 (9%) adults aged 20 to 79 years ‐ that is 415 million ‐ had diabetes; this is projected to reach one in 10 (10%) ‐ or 642 million ‐ by 2040 (IDF 2015). An additional 193 million adults are estimated to have undiagnosed diabetes, and a further 318 million, are estimated to have impaired glucose tolerance, which puts them at high risk of developing the disease (IDF 2015). In 2015, it was estimated that 20.9 million, or 16.2% of live births globally were affected by some form of hyperglycaemia in pregnancy ‐ 14.9% (or approximately 3.1 million) of these pregnancies were affected by type 1 or 2 diabetes first detected in pregnancy, or detected prior to pregnancy (established diabetes) (IDF 2015). Prevalence estimates of pre‐existing diabetes in pregnancy have previously been reported as approximately 1% (Bell 2008; Correa 2015; Lawrence 2008), but prevalence is known to be increasing rapidly, with concurrent rises in obesity and type 2 diabetes.
In addition to the impact of diabetes on health, pre‐existing diabetes in pregnancy is commonly associated with a number of adverse health outcomes for mothers and their infants. For pregnant women, pre‐existing diabetes has been associated with caesarean section, pregnancy‐induced hypertension or pre‐eclampsia, and preterm birth (Langer 2000a; Ray 2001; Walkinshaw 2005). Pregnancy in women with pre‐existing diabetes may also exacerbate the effects of diabetes on renal function and retinopathy (Leguizamon 2007; Sheth 2002). Pre‐existing diabetes in pregnancy is associated with an increased risk of fetal congenital anomaly and spontaneous abortion (Kitzmiller 1996). Fetal hyperinsulinaemia associated with pre‐existing diabetes may affect infants by increasing the incidence of: macrosomia (birthweight exceeding 4000 g); large‐for‐gestational age (birthweight greater than 90th centile for age); shoulder dystocia; neonatal hypoglycaemia; preterm birth; hyperbilirubinaemia; hypocalcaemia, and neonatal intensive care admission (Jensen 2004; Macintosh 2006; Ray 2001; Walkinshaw 2005; Weintrob 1996). Furthermore, long‐term follow‐up of infants of diabetic mothers suggests that exposure to maternal diabetes in utero increases the risk of obesity and type 2 diabetes for these children in the future (Dabelea 2000).
Previous gestational diabetes
Gestational diabetes mellitus is defined as "carbohydrate intolerance resulting in hyperglycaemia of variable severity with onset or first recognition during pregnancy" (WHO 1999). The reported incidence of gestational diabetes varies between different populations and the method and criteria by which the diagnosis is made, with studies estimating incidence rates that range between 1% and 28% (Jiwani 2012). Gestational diabetes is associated with an increased risk of a number of adverse perinatal outcomes including macrosomia, shoulder dystocia, perineal trauma, pre‐eclampsia, and neonatal hypoglycaemia (Reece 2010). Although gestational diabetes resolves in 90% of cases, women with a history of gestational diabetes represent a unique group of women who are at significant risk for developing recurrent gestational diabetes and later established diabetes (Kim 2002; Kim 2007). It has been estimated that there is a 2% risk of progression to established diabetes in the subsequent pregnancy for women with gestational diabetes (Khambalia 2013).
Despite the potential need for intervention for these groups of women, there is limited evidence about the use of oral anti‐diabetic agents preconceptionally or during pregnancy.
Description of the intervention
Management of established diabetes before pregnancy, and pre‐existing diabetes during pregnancy
The occurrence of adverse outcomes in women with pre‐existing diabetes and their infants is inversely related to the level of glycaemic control achieved during pregnancy. Therefore, there is a strong focus on the management of maternal glucose concentrations in preconception and antenatal care of women with established diabetes.
Prior to conception, it is recommended that women with established diabetes receive multidisciplinary care including an assessment of diabetes complications, advice on glycaemic control, diet, the importance of family planning, maternal diabetes complications and fetal risks (ADA 2015; ADIPS 2005; CDA 2013; NICE 2015). Oral anti‐diabetic agents are more commonly used by people with type 2 diabetes than people with type 1 diabetes, who commonly will not achieve adequate glycaemic control on oral anti‐diabetics alone. Currently, it is recommended that oral anti‐diabetic agents be substituted for insulin in women planning pregnancy and during pregnancy (ADA 2015; ADIPS 2005; CDA 2013; NICE 2015).
Oral anti‐diabetic agents, also referred to as oral hypoglycaemic agents or oral antihyperglycaemic agents, act in a variety of ways. While widely used in men and women with type 2 diabetes, their use in women with established diabetes who are planning a pregnancy or are pregnant has been controversial, with conflicting reports about their safety. As a result of these concerns, insulin has been the preferred agent for glycaemic management in women with pre‐existing diabetes during pregnancy (ADA 2015; ADIPS 2005; CDA 2013; NICE 2015). Current recommendations suggest that women planning or continuing a pregnancy use insulin, although oral anti‐diabetic agents may be considered on an individual basis, since the harm from uncontrolled diabetes may outweigh any potential harm from the oral agents.
Lack of safety data for the use of oral anti‐diabetic agents in pregnancy has prevented them from being routinely recommended for use during pregnancy. It has also been argued that the use of oral anti‐diabetic agents alone, including glyburide (glibenclamide) and metformin, may be inadequate to manage the post‐prandial glycaemic peaks associated with type 2 diabetes successfully (Jovanovic 2007). However, oral anti‐diabetic agents are convenient, may be preferable to insulin injections, and may not require the intensive education associated with insulin therapy. Where oral agents alone are not sufficient to achieve glycaemic control, they may be used in combination to reduce the frequency or dose of insulin.
A retrospective study of women in South Africa with established diabetes, who remained on oral anti‐diabetic agents, transferred from oral agents to insulin, or transferred from diet alone to insulin, reported no difference in fetal anomaly rates (Ekpebegh 2007). This study, however, did report a significantly higher perinatal mortality rate for women continuing on oral anti‐diabetic agents alone compared with women who received insulin. Meta‐analyses and reviews of observational studies have been unable to provide definitive conclusions about the effects of oral anti‐diabetic agents in pregnancy (Gutzin 2003; Ho 2007).
The Tieu 2017 Cochrane Review found no evidence of benefit for preconception care compared with no preconception care, or any protocol of preconception care over another, for women with established diabetes. Cochrane Reviews have also assessed various management strategies during pregnancy for women with pre‐existing diabetes. The O'Neill 2017 Cochrane Review, which assessed different insulin types and regimens, recently concluded that no firm conclusions could be drawn on the basis of current evidence. The Farrar 2016 Cochrane Review similarly concluded that there is currently no evidence to support the use of one particular form of insulin administration over another. Furthermore, reviews of different intensities of glycaemic control (Middleton 2016), and techniques of monitoring blood glucose for women with pre‐existing diabetes in pregnancy (Moy 2014), have not been able to reach firm conclusions about best practice either.
Management of previous gestational diabetes before and during pregnancy
While the importance of management for women with gestational diabetes has been recognised (Crowther 2005; Landon 2009), the most appropriate form of treatment is uncertain (Alwan 2009). The Cochrane Review 'Treatment for gestational diabetes' concluded that while women with gestational diabetes should be considered for specific treatment in addition to routine antenatal care, the decision about whether to offer dietary advice or more intensive treatment (including insulin or oral agents) was unclear (Alwan 2009), as were the effects on long‐term outcomes for the women and their infants (Alwan 2009). This review assessed a range of management options, including the use of oral anti‐diabetic agents such as metformin and glyburide (glibenclamide). The review found that women who received oral anti‐diabetic agents compared with insulin were less likely to have a caesarean section, and their infants were less likely to develop neonatal hypoglycaemia; there were however, no differences in other important outcomes such as induction of labour and shoulder dystocia (Alwan 2009).
The Alwan 2009 Cochrane Review has now been separated into reviews that address lifestyle interventions (Brown 2017a), dietary supplementation with myo‐inositol (Brown 2016a), different intensities of glycaemic control (Martis 2016), as well as insulin (Brown 2016b), and oral anti‐diabetic agents (Brown 2017b). The recent Brown 2017b review concluded that there are insufficient data from comparisons of oral anti‐diabetic agents versus placebo/standard care (lifestyle advice) in women with gestational diabetes to inform clinical practice, or to draw any meaningful conclusions regarding the benefits or harms of one oral anti‐diabetic agent over another (e.g. metformin versus glibenclamide; and glibenclamide versus acarbose) (Brown 2017b). The Brown 2016b review, which will include comparisons of oral anti‐diabetic agents with insulin is currently being prepared.
The Tieu 2013 Cochrane Review found no evidence to assess the role of interconception care for women with a history of gestational diabetes.
How the intervention might work
Oral anti‐diabetic agents
Common anti‐diabetic agents include sulfonylureas, biguanides, thiazolidinediones, alpha‐glucosidase inhibitors, meglitinides and peptide analogues. Biguanides, including metformin, reduce peripheral insulin resistance, inhibit gluconeogenesis and reduce plasma triglyceride concentrations (DeFronzo 1995; Stumvoll 1995; Yogev 2004). Since metformin does cross the placenta, there have been concerns about its use in pregnancy (Hellmuth 2000; Kovo 2007; Slocum 2002). Since the publication of the Alwan 2009 Cochrane Review, the use of metformin for the treatment of gestational diabetes has been evaluated in a large randomised controlled trial (Rowan 2008a). This trial found that compared with insulin, while metformin was not associated with increased perinatal complications, it was associated with a tendency for less severe neonatal hypoglycaemia, less maternal weight gain and greater maternal acceptability. In this study metformin was commenced in the latter half of pregnancy, between 20 and 34 weeks' gestation.
There is no definitive evidence of the safety of metformin in pregnancies complicated by pre‐existing diabetes (Ho 2007). However, since it has been suggested that metformin increases the incidence of pregnancy and reduces pregnancy loss in women with polycystic ovary syndrome (PCOS), there are data available from babies born to mothers with PCOS who took metformin during pregnancy. Follow‐up at 18 months of age of 126 infants born to 109 mothers with PCOS, who conceived while taking metformin and continued to take it during pregnancy, reported that the metformin‐exposed infants were of similar size and had similar motor‐social development to infants of women not known to have PCOS (Brock 2005; Glueck 2004).
Sulfonylureas, for example glyburide (glibenclamide) and glimepiride, enhance insulin secretion and peripheral tissue sensitivity to insulin while also reducing hepatic clearance of insulin (DeFronzo 1984; Homko 2006; Simonson 1984; Yogev 2004). The main side effect of these agents is hypoglycaemia, and while first generation sulfonylureas cross the placenta, it is unclear whether second generation agents, including glyburide (glibenclamide), do, and what effect this might have on the developing fetus (Jovanovic 2007; Kraemer 2006; Sivan 1995; Slocum 2002). The ability of sulfonylureas to stimulate fetal hyperinsulinaemia is a major concern (Coetzee 2007). However, a randomised controlled trial of treatment of women with gestational diabetes, included in the Alwan 2009 Cochrane Review, which investigated glyburide (glibenclamide; a second generation sulfonylurea), or insulin, found that there were no differences in macrosomic or large‐for‐gestational‐age infants between the two groups (Langer 2000a).
Alpha‐glucosidase inhibitors such as acarbose and miglitol reduce postprandial glucose concentrations by decreasing the breakdown and absorption of carbohydrates in the intestine (Slocum 2002; Yogev 2004). There is little evidence of the use of these agents in pregnancy (Ho 2007). Alpha‐glucosidase inhibitors are typically used in combination with other oral anti‐diabetic agents or insulin (Yogev 2004).
Thiazolidinediones, including rosiglitazone and pioglitazone, result in increased insulin sensitivity and decreased lipid availability (Slocum 2002; Yogev 2004). There is little evidence about the use of thiazolidinediones in pregnancy (Ho 2007), although, placental transfer of thiazolidinediones has been reported (Chan 2005). Furthermore, concerns have been expressed about the use of rosiglitazone in type 2 diabetes due to an increased risk of adverse cardiovascular outcomes (Nissen 2007).
Meglitinides increase pancreatic insulin secretion. There is little evidence of their use in pregnancy (Slocum 2002), and a similar absence of evidence for the use of peptide analogues such as incretin mimetics and dipeptidyl peptidase‐4 inhibitors.
Why it is important to do this review
With the rising prevalence of type 1, type 2 and gestational diabetes, there is an increasing need for evidence‐based management of women with established diabetes or a history of gestational diabetes both preconceptionally and during pregnancy. While most guidelines recommend the use of insulin in place of oral anti‐diabetic agents, oral agents may have benefits, particularly in terms of acceptability and adherence. However, there is little evidence about the effects of these agents on maternal and infant health. It is necessary, therefore, to assess the benefits and harms of anti‐diabetic agents in women with established diabetes, impaired glucose tolerance or previous gestational diabetes who are planning a pregnancy, and pregnant women with pre‐existing diabetes mellitus. The use of oral anti‐diabetic agents for the management of gestational diabetes in a current pregnancy was previously evaluated in the Cochrane Review 'Treatment of gestational diabetes' (Alwan 2009); specific assessments of oral anti‐diabetic agents (Brown 2017b), and comparisons of these agents with insulin for women with gestational diabetes (Brown 2016b), are made in two new Cochrane Reviews.
Objectives
To investigate the effect of oral anti‐diabetic agents in women with established diabetes, impaired glucose tolerance or previous gestational diabetes who are planning a pregnancy, or pregnant women with pre‐existing diabetes, on maternal and infant health. The use of oral anti‐diabetic agents for the management of gestational diabetes in a current pregnancy is evaluated in a separate Cochrane Review.
Methods
Criteria for considering studies for this review
Types of studies
We planned to include randomised and quasi‐randomised controlled trials, and cluster‐randomised trials, and to exclude cross‐over trials. We planned to include trials published in abstract form only where there was sufficient information available to assess study eligibility and risk of bias.
Types of participants
Women with established type 1 or 2 diabetes mellitus, impaired glucose tolerance or previous gestational diabetes mellitus planning a pregnancy or pregnant women with pre‐existing type 1 or 2 diabetes mellitus. Trials involving women with gestational diabetes in a current pregnancy were excluded from this review.
Types of interventions
-
Oral anti‐diabetic agent versus no medication
-
Oral anti‐diabetic agent versus another oral anti‐diabetic agent
-
Oral anti‐diabetic agent versus insulin
-
Oral anti‐diabetic agent versus insulin plus an oral anti‐diabetic agent
-
Oral anti‐diabetic agent plus insulin versus insulin
-
Different regimens of any of the above
Types of outcome measures
For this update, we used the standard outcome set agreed by consensus between review authors of Cochrane Pregnancy and Childbirth systematic reviews for prevention and treatment of gestational diabetes and pre‐existing diabetes.
Primary outcomes
Mother
-
Hypertensive disorders of pregnancy (including pre‐eclampsia, pregnancy‐induced hypertension, eclampsia)
-
Caesarean section
Infant/child/adult
-
Large‐for‐gestational age
-
Perinatal mortality (stillbirth and neonatal mortality)
-
Neonatal mortality or morbidity composite (e.g. perinatal mortality, shoulder dystocia, bone fracture, and admission to the neonatal unit)
-
Childhood/adulthood neurosensory disability
Secondary outcomes
Mother: short‐term
-
Spontaneous abortion/miscarriage
-
Gestational diabetes mellitus
-
Induction of labour
-
Perineal trauma
-
Placental abruption
-
Postpartum haemorrhage
-
Postpartum infection
-
Weight gain during pregnancy
-
Adherence to the intervention
-
Sense of well‐being and quality of life
-
Views of the intervention
-
Adverse effects of the intervention
-
Breastfeeding at discharge, six weeks postpartum, six months or longer
-
Use of additional pharmacotherapy for glycaemic control
-
Glycaemic control during/end of treatment (e.g. blood glucose or haemoglobin A1c (HbA1c))
-
Hypoglycaemia
-
Mortality
-
Complications of diabetes (retinopathy, neuropathy, nephropathy, ischaemic heart disease, cerebrovascular disease, peripheral vascular disease)
Mother: long‐term
-
Postnatal depression
-
Postnatal weight retention or return to prepregnancy weight
-
Body mass index (BMI)
-
Gestational diabetes mellitus in a subsequent pregnancy
-
Type 1 diabetes
-
Type 2 diabetes
-
Impaired glucose tolerance
-
Cardiovascular health (as defined by trialists, including blood pressure, hypertension, cardiovascular disease, metabolic syndrome)
Infant
-
Congenital anomaly
-
Stillbirth
-
Neonatal mortality
-
Gestational age at birth
-
Preterm birth (less than 37 weeks' gestation and less than 32 weeks' gestation)
-
Apgar score (less than seven at five minutes)
-
Macrosomia (birthweight greater than 4000 g and birthweight greater than 4500 g)
-
Small‐for‐gestational age
-
Birthweight and Z score
-
Head circumference and Z score
-
Length and Z score
-
Ponderal index
-
Adiposity
-
Shoulder dystocia
-
Bone fracture
-
Nerve palsy
-
Respiratory distress syndrome
-
Hypoglycaemia
-
Hyperbilirubinaemia
-
Hypocalcaemia
-
Polycythaemia
-
Infection
-
Relevant biomarker changes associated with the intervention (e.g. cord C peptide, cord insulin)
Child/adult
-
Weight and Z scores
-
Height and Z scores
-
Head circumference and Z scores
-
Adiposity (e.g. as measured by BMI, skinfold thickness)
-
Cardiovascular health (as defined by trialists including blood pressure, hypertension, cardiovascular disease, metabolic syndrome)
-
Type 1 diabetes
-
Type 2 diabetes
-
Impaired glucose tolerance
-
Employment, education and social status/achievement
Health service
-
Number of hospital or health professional visits (e.g. midwife, obstetrician, physician, dietitian, diabetic nurse)
-
Number of antenatal visits or admissions
-
Length of antenatal stay
-
Neonatal intensive care unit/nursery admission
-
Duration of stay in neonatal intensive care unit/nursery
-
Length of postnatal stay (mother)
-
Length of postnatal stay (baby)
-
Costs to families associated with the management provided
-
Costs associated with the intervention
-
Cost of maternal care
-
Cost of offspring care
Search methods for identification of studies
The following methods section of this review is based on a standard template used by Cochrane Pregnancy and Childbirth.
Electronic searches
We searched Cochrane Pregnancy and Childbirth’s Trials Register by contacting their Information Specialist (31 October 2016).
The Register is a database containing over 23,000 reports of controlled trials in the field of pregnancy and childbirth. For full search methods used to populate Pregnancy and Childbirth’s Trials Register including the detailed search strategies for CENTRAL, MEDLINE, Embase and CINAHL, the list of handsearched journals and conference proceedings, and the list of journals reviewed via the current awareness service, please follow this link to the editorial information about the Cochrane Pregnancy and Childbirth in the Cochrane Library and select the ‘Specialized Register ’ section from the options on the left side of the screen.
Briefly, Cochrane Pregnancy and Childbirth’s Trials Register is maintained by their Information Specialist and contains trials identified from:
-
monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL);
-
weekly searches of MEDLINE (Ovid);
-
weekly searches of Embase (Ovid);
-
monthly searches of CINAHL (EBSCO);
-
handsearches of 30 journals and the proceedings of major conferences;
-
weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts.
Search results are screened by two people and the full text of all relevant trial reports identified through the searching activities described above is reviewed. Based on the intervention described, each trial report is assigned a number that corresponds to a specific Pregnancy and Childbirth review topic (or topics), and is then added to the Register. The Information Specialist searches the Register for each review using this topic number rather than keywords. This results in a more specific search set that has been fully accounted for in the relevant review sections (Included studies; Excluded studies; Studies awaiting classification; Ongoing studies).
Searching other resources
We searched the reference lists of retrieved studies.
We did not apply any language or date restrictions.
Data collection and analysis
For methods used in the previous version of this review, seeTieu 2010.
For this update, the following methods were used for assessing the 29 new reports that were identified as a result of the updated search, and four reports that were reassessed from the previous version of this review.
The following methods section of this review is based on a standard template used by Cochrane Pregnancy and Childbirth.
Selection of studies
Two review authors independently assessed all the potential studies identified as a result of the search strategy for inclusion. We resolved any disagreement through discussion or, if required, we consulted the third review author.
Data extraction and management
We designed a form to extract data. For eligible studies, two review authors extracted the data using the agreed form. We resolved discrepancies through discussion or, if required, we consulted the third review author. Data were entered into Review Manager 5 software (RevMan 2014), and checked for accuracy.
When information regarding eligibility or data was unclear, we planned to contact authors of the original reports to provide further details.
Assessment of risk of bias in included studies
Two review authors independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Any disagreement was resolved by discussion or by involving a third assessor.
(1) Random sequence generation (checking for possible selection bias)
We described the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups.
For each included study we assessed the method as being at:
-
low risk of bias (any truly random process, e.g. random number table; computer random number generator);
-
high risk of bias (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number);
-
unclear risk of bias.
(2) Allocation concealment (checking for possible selection bias)
For each included study we described the method used to conceal allocation to interventions prior to assignment and assessed whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment.
We assessed the methods as being at:
-
low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
-
high risk of bias (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth);
-
unclear risk of bias.
(3.1) Blinding of participants and personnel (checking for possible performance bias)
For each included study we described the methods used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. We considered that studies were at low risk of bias if they were blinded, or if we judged that the lack of blinding was unlikely to affect results. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed the methods as being at:
-
low, high or unclear risk of bias for participants;
-
low, high or unclear risk of bias for personnel.
(3.2) Blinding of outcome assessment (checking for possible detection bias)
For each included study we described the methods used, if any, to blind outcome assessors from knowledge of which intervention a participant received. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed methods used to blind outcome assessment as being at:
-
low, high or unclear risk of bias.
(4) Incomplete outcome data (checking for possible attrition bias due to the amount, nature and handling of incomplete outcome data)
For each included study, and for each outcome or class of outcomes, we described the completeness of data including attrition and exclusions from the analysis. We stated whether attrition and exclusions were reported and the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. Where sufficient information was reported, or could be supplied by the trial authors, we planned to re‐include missing data in the analyses that we undertook.
We assessed methods as being at:
-
low risk of bias (e.g. no missing outcome data; missing outcome data balanced across groups);
-
high risk of bias (e.g. numbers or reasons for missing data imbalanced across groups; ‘as treated’ analysis done with substantial departure of intervention received from that assigned at randomisation);
-
unclear risk of bias.
(5) Selective reporting (checking for reporting bias)
For each included study we described how we investigated the possibility of selective outcome reporting bias and what we found.
We assessed the methods as being at:
-
low risk of bias (where it was clear that all of the study’s prespecified outcomes and all expected outcomes of interest to the review have been reported);
-
high risk of bias (where not all the study’s prespecified outcomes were reported; one or more reported primary outcomes were not prespecified; outcomes of interest were reported incompletely and so could not be used; study failed to include results of a key outcome that would have been expected to have been reported);
-
unclear risk of bias.
(6) Other bias (checking for bias due to problems not covered by (1) to (5) above)
For each included study we described any important concerns we had about other possible sources of bias.
(7) Overall risk of bias
We made explicit judgements about whether studies were at high risk of bias, according to the criteria given in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). With reference to (1) to (6) above, we planned to assess the likely magnitude and direction of the bias and whether we considered it was likely to have an impact on the findings. In future updates, we will explore the impact of the level of bias through undertaking sensitivity analyses (Sensitivity analysis).
Assessment of the quality of the evidence using the GRADE approach
For this update the quality of the evidence was assessed using the GRADE approach as outlined in the GRADE handbook for the following outcomes.
Mother
-
Hypertensive disorders of pregnancy (including pre‐eclampsia, pregnancy‐induced hypertension, eclampsia)
-
Caesarean section
-
Gestational diabetes mellitus or type 2 diabetes (if applicable)
-
Induction of labour
-
Perineal trauma
-
Postnatal depression
-
Postnatal weight retention or return to prepregnancy weight
Infant/child/adult
-
Large‐for‐gestational age
-
Perinatal mortality (stillbirth and neonatal mortality)
-
Neonatal mortality or morbidity composite (e.g. perinatal mortality, shoulder dystocia, bone fracture, and admission to the neonatal unit)
-
Hypoglycaemia
-
Childhood/adulthood neurosensory disability
-
Childhood/adulthood adiposity
-
Childhood/adulthood diabetes
We used the GRADEpro Guideline Development Tool to import data from Review Manager 5 in order to create ’Summary of findings’ tables. A summary of the intervention effect and a measure of quality for each of the above outcomes was produced using the GRADE approach, which uses five considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the quality of the body of evidence for each outcome. The evidence can be downgraded from 'high quality' by one level for serious (or by two levels for very serious) limitations, depending on assessments for risk of bias, indirectness of evidence, serious inconsistency, imprecision of effect estimates, or potential publication bias.
Measures of treatment effect
Dichotomous data
For dichotomous data, we presented results as summary risk ratio with 95% confidence intervals.
Continuous data
We used the mean difference where outcomes were measured in the same way between trials. We planned to use the standardised mean difference to combine trials that measured the same outcome through different methods.
Unit of analysis issues
Cluster‐randomised trials
We did not identify any cluster‐randomised trials. In future updates of the review, if cluster‐randomised trials are included, we will adjust their sample sizes using the methods described in the Cochrane Handbook for Systematic Reviews of Interventions using an estimate of the intracluster correlation co‐efficient (ICC) derived from the trial (if possible), from a similar trial or from a study of a similar population. If we use ICCs from other sources, we will report this and conduct sensitivity analyses to investigate the effect of variation in the ICC. If we identify both cluster‐randomised trials and individually‐randomised trials, we plan to synthesise the relevant information. We consider it reasonable to combine the results from both if there is little heterogeneity between the study designs, and the interaction between the effect of intervention and the choice of randomisation unit is considered to be unlikely.
We will also acknowledge heterogeneity in the randomisation unit and we will perform a sensitivity analysis to investigate the effects of the randomisation unit.
Cross‐over trials
Cross‐over trials are an inappropriate design for this intervention.
Cross over trials are not a suitable design for trials looking at interventions in labour and have been excluded.
Studies with more than two groups
In Ainuddin 2015, results for the group randomised to metformin were reported separately for those women who remained on metformin alone and those women who subsequently received insulin in addition to metformin. We combined the metformin groups to create a single pair‐wise comparison, as recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Chapter 16, section.5.4), by considering the metformin alone and the metformin plus insulin groups together.
In Notelovitz 1971, we were unable to report any results from this four‐armed RCT (chlorpropamide, tolbutamide, insulin and diet therapy) as women with type 2 diabetes or gestational diabetes mellitus were not reported separately. However, if we had been able to obtain these data separately, we would have created three single pair‐wise comparisons (by combining both oral anti‐diabetic agents compared with insulin, both oral anti‐diabetic agents compared with diet therapy and one oral anti‐diabetic agent compared with the other anti‐diabetic agent).
Dealing with missing data
We noted levels of attrition for included studies. In future updates, if more eligible studies are included, we will explore the impact of including studies with high levels of missing data in the overall assessment of treatment effect by using sensitivity analysis.
For all outcomes, we carried out analyses, as far as possible, on an intention‐to‐treat basis, that is, we attempted to include all participants randomised to each group in the analyses. The denominator for each outcome in each trial was the number randomised minus any participants whose outcomes were known to be missing.
Assessment of heterogeneity
We assessed statistical heterogeneity in each meta‐analysis using the Tau², I² and Chi² statistics. We regarded heterogeneity as substantial if I² was greater than 30% and either Tau² was greater than zero, or there was a low P value (less than 0.10) in the Chi² test for heterogeneity. If we identified substantial heterogeneity (above 30%), we planned to explore it by prespecified subgroup analysis.
Assessment of reporting biases
As there were fewer than 10 trials included in the analyses, we were unable to investigate reporting biases (such as publication bias) using funnel plots. In future updates, as more data become available, we will investigate reporting biases using funnel plots. We will assess funnel plot asymmetry visually. If asymmetry is suggested by visual assessment, we will investigate further.
Data synthesis
We carried out statistical analysis using Review Manager 5 software (RevMan 2014). We used fixed‐effect meta‐analysis for combining data where it was reasonable to assume that studies were estimating the same underlying treatment effect: that is, where trials were examining the same intervention, and the trials’ populations and methods were judged to be sufficiently similar.
In future updates, with more included studies, if there is clinical heterogeneity sufficient to expect that the underlying treatment effects differ between trials, or if substantial statistical heterogeneity is detected, we will use random‐effects meta‐analysis to produce an overall summary, if an average treatment effect across trials is considered clinically meaningful. The random‐effects summary will be treated as the average of the range of possible treatment effects and we will discuss the clinical implications of treatment effects differing between trials. If the average treatment effect is not clinically meaningful, we will not combine trials. Where we use random‐effects analyses, the results will be presented as the average treatment effect with 95% confidence intervals, and the estimates of Tau² and I².
Subgroup analysis and investigation of heterogeneity
We planned to carry out the following subgroup analyses but there were insufficient data to do so.
-
Type of diabetes (e.g. established type 1 diabetes mellitus versus established type 2 diabetes mellitus versus impaired glucose tolerance versus previous gestational diabetes mellitus).
-
Gestational age of women at randomisation (e.g. preconception versus first trimester versus second trimester versus third trimester).
-
Glycaemic control prior to pregnancy/randomisation (e.g. glycaemic targets achieved versus not achieved).
We planned to use only primary outcomes in subgroup analyses. In future updates, we plan to assess differences between subgroups by interaction tests available in RevMan 2014. We will report the results of subgroup analyses quoting the Chi² statistic and P value, and the interaction test I² value.
Sensitivity analysis
We planned to carry out sensitivity analyses to explore the effect of trial quality assessed by concealment of allocation, high attrition rates, or both, with poor‐quality studies (rated at unclear or high risk of bias for these components) being excluded from the analyses in order to assess whether this made any difference to the overall result, however there were insufficient data to do this.
Results
Description of studies
Results of the search
In the previous version on this review we identified no trials eligible for inclusion (Tieu 2010).
An updated search was carried out in October 2016; 29 new reports were identified. We reassessed three studies (four reports) which were either excluded (Notelovitz 1971), ongoing (Hague 2010), or awaiting assessment (Hutchinson 2008) in the previous version. Some studies were published in multiple reports. In total, we have now included six studies and excluded 22. Four studies are awaiting further classification, and three studies are ongoing. See Figure 1.

Study flow diagram
To date, three of the four studies awaiting further classification have been published as abstracts only (Coiner 2014; Hutchinson 2008; Reyes‐Munoz 2014); we have contacted the trial authors regarding availability of full reports in order to assess study eligibility and risk of bias further. The fourth study provided insufficient detail for us to determine study eligibility (specifically regarding whether women with established diabetes were included) (Waheed 2013). For further details see Characteristics of studies awaiting classification.
The three ongoing trials are all assessing metformin in pregnant women with type 2 diabetes (Feig 2011), gestational diabetes or type 2 diabetes (Sheizaf 2006), or at high risk for gestational diabetes (Van der Linden 2014). For further details see Characteristics of ongoing studies.
Included studies
We included six trials in this review (Ainuddin 2015; Beyuo 2015; Hickman 2013; Ibrahim 2014; Notelovitz 1971; Refuerzo 2015). However, as three of the trials had mixed populations (women with gestational diabetes and women with established diabetes) (Beyuo 2015; Ibrahim 2014; Notelovitz 1971), and did not report data separately for the relevant subset of women for this review, we have only included outcome data from three of the included trials (Ainuddin 2015; Hickman 2013; Refuerzo 2015). The Hickman 2013 trial also had a mixed population, but the trial authors provided data for the group of women with established diabetes separately for inclusion in this review. We have contacted the authors of the three trials with mixed populations to ask about the availability of data for women with established diabetes, and await responses. We describe the characteristics of the six included trials below.
Settings
The included trials were conducted in Pakistan (Ainuddin 2015), Ghana (Beyuo 2015), Egypt (Ibrahim 2014), South Africa (Notelovitz 1971) and the USA (Hickman 2013; Refuerzo 2015).
Dates when study conducted
Ainuddin 2015 was conducted from January 2009 to January 2014, Beyuo 2015 from January 2013 to October 2015, Hickman 2013 from July 2008 to December 2009, Ibrahim 2014 from August 2011 to April 2012, and Refuerzo 2015 from September 2009 to August 2011. Notelovitz 1971 did not report when the study was conducted.
Funding
Funding sources were reported by four of the trials; Hickman 2013 and Refuerzo 2015 were funded by non‐commercial organisations; Notelovitz 1971 was funded by a commercial organisation (Pfizer Laboratories Ltd); and Ibrahim 2014 identified the trialists as the source of funding. Ainuddin 2015 did not describe source of funding and Beyuo 2015 reported “no source of funding”.
Declarations of interest
Three of the trials reported that there were no conflicts of interests for any of the authors (Ainuddin 2015; Beyuo 2015; Ibrahim 2014). The remaining three trials did not report any information regarding declarations of interest (Hickman 2013; Notelovitz 1971; Refuerzo 2015).
Participants
Overall, the six trials randomised 707 women and their babies, with sample sizes ranging from 25 women in Refuerzo 2015 to 250 women in Ainuddin 2015.
Two trials included only women with established diabetes; both included women with singleton pregnancies, with type 2 diabetes diagnosed prior to pregnancy, and cases of newly diagnosed overt diabetes in pregnancy beyond the first trimester (Ainuddin 2015), or a self‐reported history of type 2 diabetes for less than 10 years prior to 20 weeks' gestation (Refuerzo 2015).
Four trials included mixed populations of women with gestational diabetes and established type 2 diabetes, prior to 20 weeks' gestation (Hickman 2013), from 20 to 30 weeks' gestation (Beyuo 2015), between 20 and 34 weeks' gestation (Ibrahim 2014), or whose duration of pregnancy would allow at least six consecutive weeks of treatment (Notelovitz 1971).
Interventions
While five of the six included trials compared metformin with insulin (Ainuddin 2015; Beyuo 2015; Hickman 2013; Ibrahim 2014; Refuerzo 2015), their intervention and control regimens varied. Four of the trials assessed 500 mg metformin daily (Ainuddin 2015; Beyuo 2015; Hickman 2013; Refuerzo 2015), which was increased, as required, up to a maximum of 2500 mg daily in the intervention group. In these four trials, if glycaemic control (variously defined) was not achieved with the maximum dose of metformin, insulin was added as supplementary therapy. In the fifth trial (Ibrahim 2014), women commenced on 1500 mg metformin daily, which was raised to 2000 mg daily. In this trial, if glycaemic control was not achieved women were switched to a conventional insulin dose‐raising regimen (Ibrahim 2014). Insulin regimens in the comparison groups were broadly similar; it was commonly given in two doses, with the total daily dose titrated to achieve glycaemic control. Total daily doses were calculated as follows: in Ainuddin 2015 0.6 IU/kg body weight in first trimester, 0.7 IU/kg in second trimester, 0.8 IU/kg from 28 to 32 weeks, 0.9 IU/kg from 32 to 36 weeks, 1 IU/kg from 36 weeks onwards; in Beyuo 2015 0.3 IU/kg body weight at initiation (20 to 30 weeks' gestation); in Hickman 2013 0.7 IU/kg bodyweight at initiation (prior to 20 weeks' gestation); and in Refuerzo 2015: 0.7 IU/kg bodyweight in the first trimester, 0.8 IU/kg in the second trimester, and 0.9 to 1.0 IU/kg/day in the third trimester. Ibrahim 2014 treated women with poor glycaemic control with a daily dose of at least 1.12 IU/kg bodyweight.
The Notelovitz 1971 trial had four groups that compared chlorpropamide, tolbutamide, insulin and diet restriction alone; no further details were provided regarding specific regimens.
For detailed descriptions of the included studies, see Characteristics of included studies.
Excluded studies
We excluded a total of 22 studies. Seventeen of the trials evaluated treatments for gestational diabetes (Anjalakshi 2007; Bertini 2005; Casey 2015; Corrado 2011; George 2015; Golladay 2005; Hague 2003; Langer 2000b; Martinez 2010; Moore 2005; Moore 2007; Mukhopadhyay 2012; Niromanesh 2012; Rowan 2008b; Singh 2011Wali 2012; Zanganeh 2010), and one assessed treatments for women with hyperglycaemia that did not meet the criteria for gestational diabetes (Myers 2013); these trials are, or will be, considered in the other relevant Cochrane Reviews. Three trials evaluated treatment specifically for women with polycystic ovary syndrome (Carlsen 2007; Vanky 2004; Vanky 2005). One potentially relevant trial was planned in women with previous gestational diabetes, but subsequently not conducted (Hague 2010). For further details see Characteristics of excluded studies.
Risk of bias in included studies
Overall we judged the trials to be at varying risks of bias; see Figure 2 and Figure 3.
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies

Risk of bias summary: review authors' judgements about each risk of bias item for each included study
Allocation
We judged that three of the six trials used adequate methods for sequence generation and allocation concealment, and thus were at low risk of selection bias (Beyuo 2015; Hickman 2013; Refuerzo 2015). One trial reported an adequate method for sequence generation, but the method of allocation concealment was unclear (Ibrahim 2014). Another trial did not report the methods for sequence generation or allocation concealment (Notelovitz 1971), and so we judged this trial to be at an unclear risk of selection bias. The final trial used quasi‐randomisation, and we judged it to be at high risk of selection bias (Ainuddin 2015).
Blinding
We judged all of the six included trials to be at high risk of performance bias (blinding of women and study personnel was not possible due to the nature of the differing treatments received by the intervention and comparison groups) (Ainuddin 2015; Beyuo 2015; Hickman 2013; Ibrahim 2014; Notelovitz 1971; Refuerzo 2015). We judged all six trials to be at an unclear risk of detection bias; three trials were reported to be 'open label', but none of these trials specifically reported on whether it was possible to blind outcome assessment (Ainuddin 2015; Beyuo 2015; Refuerzo 2015), and the other three trials provided no details (Hickman 2013; Ibrahim 2014; Notelovitz 1971).
Incomplete outcome data
We judged only one trial to be at low risk of attrition bias (Hickman 2013), as over 90% of the women randomised were included in the analyses, and loss to follow‐up and exclusions occurred in similar numbers, and for similar reasons between groups. We judged two trials to be at an unclear risk of attrition bias; in Beyuo 2015 there appeared to be higher attrition in the insulin group, with 75% of women completing the study, compared with 90% in the metformin group; and in Refuerzo 2015 only 84% of the women randomised were analysed (21/25). We judged three trials to be at a high risk of attrition bias (Ainuddin 2015; Ibrahim 2014; Notelovitz 1971); in Ainuddin 2015 almost 20% of women were excluded from the analyses, and notably, in the analyses, the metformin group was separated into metformin alone, and metformin plus insulin; we combined these groups for the purpose of this review. Ibrahim 2014 reported that 'per‐protocol treatment analyses' were performed (with women who chose to switch from their allocated group excluded from the analyses); and for Notelovitz 1971 it also appeared that analyses were not intention‐to‐treat, as it was reported that, "In the final analysis" women were analysed in the group in which they "completed treatment" or "were treated with for the greater part of their pregnancy".
Selective reporting
We judged only one trial to be at a low risk of reporting bias, as the expected outcomes were reported as they were in the trial registration (Refuerzo 2015). We judged four of the trials to be at an unclear risk of reporting bias, due to the provision of limited detail regarding prespecified outcomes in the trial registrations available, or limited reporting of expected outcomes to date, or both (Ainuddin 2015; Beyuo 2015; Hickman 2013; Ibrahim 2014). We judged one trial to be at a high risk of reporting bias, as it did not prespecify outcomes, and provided incomplete reporting of some outcomes (Notelovitz 1971).
Other potential sources of bias
We judged all six trials to be at unclear risk of other bias. Four of the trials appeared to have imbalances in baseline characteristics despite randomisation (Ainuddin 2015; Beyuo 2015; Hickman 2013; Refuerzo 2015), while the other two provided very limited methodological details and information regarding the comparability of groups at baseline (Ibrahim 2014; Notelovitz 1971).
Effects of interventions
See: Summary of findings for the main comparison Maternal outcomes: oral anti‐diabetic agent (metformin) compared with insulin for women with established type 2 diabetes mellitus; Summary of findings 2 Infant outcomes: oral anti‐diabetic agent (metformin) compared with insulin for women with established type 2 diabetes mellitus
Oral anti‐diabetic agent (metformin) versus insulin
Mother: primary outcomes
Hypertensive disorders of pregnancy
Both Ainuddin 2015 and Refuerzo 2015 reported on pre‐eclampsia and overall, there was no clear difference between the metformin and insulin groups (risk ratio (RR) RR 0.63, 95% confidence interval (CI) 0.33 to 1.20; RCTs = 2; participants = 227; very low‐quality evidence; Analysis 1.1). In Ainuddin 2015, however, women receiving metformin, were less likely to have pregnancy‐induced hypertension (RR 0.58, 95% CI 0.37 to 0.91; RCTs = 1; participants = 206; low‐quality evidence; Analysis 1.2).
Caesarean section
Pooling of data from Ainuddin 2015, Hickman 2013 and Refuerzo 2015 showed that women in the metformin group were less likely to have a caesarean section birth compared with those in the insulin group (RR 0.73, 95% CI 0.61 to 0.88; RCTs = 3; participants = 241; low‐quality evidence; Analysis 1.3).
Infant/child/adult
Large‐for‐gestational age
There was no clear difference between the metformin and insulin groups for large‐for‐gestational age infants in Ainuddin 2015 (RR 1.12, 95% CI 0.73 to 1.72; RCTs = 1; participants = 206; very low‐quality evidence; Analysis 1.4).
Perinatal mortality (stillbirth and neonatal mortality)
There were no perinatal deaths in Ainuddin 2015 or Hickman 2013 (RCTs = 2; participants = 220; very low‐quality evidence; Analysis 1.5).
Neonatal mortality or morbidity composite
Ainuddin 2015, Hickman 2013 and Refuerzo 2015 did not report on this outcome.
Childhood/adulthood neurosensory disability
Ainuddin 2015, Hickman 2013 and Refuerzo 2015 did not report on this outcome.
Mother: short‐term secondary outcomes
In the metformin group in Hickman 2013, one woman experienced a 13‐week intrauterine fetal death attributed to a large subchorionic haematoma noted on ultrasound at 12 weeks (Analysis 1.6).
Meta‐analysis of data from Hickman 2013 and Refuerzo 2015 showed no clear difference between the metformin and insulin groups for induction of labour on (RR 1.42, 95% CI 0.62 to 3.28; RCTs = 2; participants = 35; very low‐quality evidence; Analysis 1.7). In Hickman 2013, no women had postpartum haemorrhage that required treatment (Analysis 1.8). In Ainuddin 2015, on average, women in the metformin group gained less weight in pregnancy than those in the insulin group (mean difference (MD) ‐1.30 kg, 95% CI ‐1.57 to ‐1.03; RCTs = 1; participants = 206; Analysis 1.9). Hickman 2013 additionally reported on weight gain during pregnancy (this was presented as groups medians, with interquartile ranges in Analysis 1.10) with results also favouring the metformin group.
Adherence to the intervention was assessed in the Ainuddin 2015 trial. This showed that women in the metformin group were more likely to report 'never or rarely' forgetting to take their medication (RR 1.37, 95% CI 1.14 to 1.64; RCTs = 1; participants = 206), and were less likely to report forgetting to take their medication two to four times per week (RR 0.45, 95% CI 0.28 to 0.72; RCTs = 1; participants = 206; Analysis 1.11). In Hickman 2013, there was no clear difference between groups for the proportions of women who had missed appointments (RR 2.00, 95% CI 0.59 to 6.79; RCTs = 1; participants = 15), or who completed more than 50% of their log book (RR 1.90, 95% CI 0.89 to 4.04; RCTs = 1; participants = 15; Analysis 1.12).
In Ainuddin 2015, women in the metformin group were more likely to report that they would choose metformin in their next pregnancy (RR 7.70, 95% CI 4.52 to 13.14; RCTs = 1; participants = 206), were less likely to report that they would choose insulin (RR 0.07, 95% CI 0.03 to 0.19; RCTs = 1; participants = 206), and were less likely to report that they were 'not sure' which medication they would choose (RR 0.11, 95% CI 0.04 to 0.29; RCTs = 1; participants = 206) compared with women in the insulin group (Analysis 1.13). In the Ainuddin 2015 trial (Analysis 1.14), when asked what part of the diabetes treatment they found easy, no women in either the metformin or insulin groups reported that doing finger pricks was easy; no women in the metformin group, compared with 25/100 in the insulin group reported that dietary control was easy (RR 0.02, 95% CI 0.00 to 0.30; RCTs = 1; participants = 206), though more women in the metformin group reported that drug treatment was easy (RR 1.33, 95% CI 1.19 to 1.49; RCTs = 1; participants = 206; Analysis 1.14). In the Ainuddin 2015 trial (Analysis 1.15), when asked what part of the diabetes treatment they found difficult, women in the metformin group were more likely to report that doing finger pricks was difficult (RR 3.46, 95% CI 2.42 to 4.95; RCTs = 1; participants = 206), and were less likely to report that drug treatment was difficult (RR 0.14, 95% CI 0.08 to 0.26; RCTs = 1; participants = 206) compared with women in the insulin group; there was no clear difference in the proportion of women finding diet control difficult in the metformin and insulin groups (RR 0.75, 95% CI 0.31 to 1.84; RCTs = 1; participants = 206; Analysis 1.15). In Hickman 2013 women in the metformin group were more likely to report that they would choose the same treatment in the future (RR 11.14, 95% CI 0.78 to 159.58; RCTs = 1; participants = 11; P = 0.08; Analysis 1.16).
Regarding adverse effects of the intervention, in the Ainuddin 2015 trial, six women in the metformin group had gastrointestinal side effects resulting in dose limitation compared with none in the insulin group (RR 12.27, 95% CI 0.70 to 215.04; RCTs = 1; participants = 206). No women in either the metformin or insulin groups had gastrointestinal side effects that resulted in treatment cessation or lactic acidosis (Analysis 1.17).
There was no clear difference between groups in Hickman 2013 for exclusive breastfeeding (time point not clear) (RR 1.59, 95% CI 0.79 to 3.23; RCTs = 1; participants = 11; Analysis 1.18).
With regard to the need for additional pharmacotherapy, Ainuddin 2015 reported that 105/125 women in the metformin group required supplemental insulin to maintain glycaemic control, while Refuerzo 2015 reported that none of the 25 women receiving metformin 'failed' with this therapy and needed insulin. Hickman 2013 reported that 3/9 women in the metformin group required supplemental insulin.
In Ainuddin 2015, with regard to glycaemic control, there was no clear difference in average fasting (MD 0.01 mg/dL, 95% CI ‐0.90 to 0.92; RCTs = 1; participants = 206; Analysis 1.19) or random blood glucose throughout pregnancy (MD ‐0.22 mg/dL, 95% CI ‐1.63 to 1.19; RCTs = 1; participants = 206; Analysis 1.20). Similarly, in Refuerzo 2015, there were no clear differences between groups in the average change in HbA1c from enrolment to the third trimester or birth (MD ‐0.48%, 95% CI ‐1.05 to 0.09; RCTs = 1; participants = 21; Analysis 1.21), or in the proportion of women with HbA1c less than 7% in the third trimester or at birth (RR 1.03, 95% CI 0.76 to 1.39; RCTs = 1; participants = 18; Analysis 1.22). Hickman 2013 reported on glycaemic control (HbA1c in the second and third trimester, delivery glucose, and postpartum fasting glucose), which has been presented as group medians, with interquartile ranges in Analysis 1.23.
Ainuddin 2015, Hickman 2013 and Refuerzo 2015 did not report on: gestational diabetes mellitus*; perinatal trauma; placental abruption; postpartum infection; sense of well‐being and quality of life; hypoglycaemia; mortality; or complications of diabetes.
*Outcome not relevant to trials involving women with established diabetes prior to pregnancy and pre‐existing diabetes in pregnancy
Mother: long‐term secondary outcomes
Ainuddin 2015, Hickman 2013 and Refuerzo 2015 did not report on: postnatal depression; postnatal weight retention or return to prepregnancy weight; body mass index; gestational diabetes in a subsequent pregnancy*; type 1 diabetes*; type 2 diabetes*; impaired glucose tolerance*; and cardiovascular health.
*Outcome not relevant to trials involving women with established diabetes prior to pregnancy and pre‐existing diabetes in pregnancy
Infant: secondary outcomes
There were no congenital anomalies (major malformations) in Hickman 2013 (Analysis 1.24). There were no stillbirths or neonatal deaths in Ainuddin 2015 or Hickman 2013 (Analysis 1.25; Analysis 1.26). Ainuddin 2015 did not show a clear difference in gestational age at birth between the metformin and insulin groups (MD ‐0.30 weeks, 95% CI ‐0.66 to 0.06; RCTs = 1; participants = 206; Analysis 1.27); Hickman 2013 and Refuerzo 2015 also reported on gestational age (presented as group medians, with (interquartile) ranges in Analysis 1.28). There was no clear difference between the metformin and insulin groups for preterm birth in Hickman 2013 and Refuerzo 2015 (RR 0.42, 95% CI 0.08 to 2.30; RCTs = 2; participants = 35; Analysis 1.29). No infants had an Apgar score less than seven at five minutes in Hickman 2013 (Analysis 1.30). There were no clear differences for macrosomia (> 4000 g) (RR 0.37, 95% CI 0.04 to 3.10; RCTs = 2; participants = 35; Analysis 1.31) in Hickman 2013 and Refuerzo 2015.
In Ainuddin 2015 infants born to mothers in the metformin group were more likely to be small‐for‐gestational age compared with those born to mothers in the insulin group (RR 8.49, 95% CI 2.02 to 35.66; RCTs = 1; participants = 206; Analysis 1.32). Meta‐analysis of data from Ainuddin 2015 and Refuerzo 2015 showed no clear difference for birthweight between infants born to mothers in the metformin and insulin groups (MD ‐0.13 kg, 95% CI ‐0.29 to 0.04; RCTs = 2; participants = 227; Analysis 1.33). Hickman 2013 also reported on birthweight, head circumference, length and cord C peptide (these data are presented as group medians, with interquartile ranges in Analysis 1.34; Analysis 1.35; Analysis 1.36; Analysis 1.44).
There were no clear differences between the metformin and insulin groups for shoulder dystocia (RR 4.67, 95% CI 0.21 to 102.47; RCTs = 2; participants = 35; Analysis 1.37) in Hickman 2013 and Refuerzo 2015, or across Ainuddin 2015 and Hickman 2013 in the proportion of infants with clavicle fracture or birth injury (RR 0.94, 95% CI 0.14 to 6.57; RCTs = 2; participants = 220; Analysis 1.38). However, infants in the metformin group were less likely to have hyperbilirubinaemia or jaundice (RR 0.44, 95% CI 0.24 to 0.81; RCTs = 2; participants = 220; Analysis 1.41), or sepsis (RR 0.26, 95% CI 0.08 to 0.81; RCTs = 2; participants = 220; Analysis 1.42).
Meta‐analysis of data from Ainuddin 2015; Hickman 2013 and Refuerzo 2015 showed no clear difference between groups for respiratory distress syndrome (RR 0.52, 95% CI 0.24 to 1.13; RCTs = 3; participants = 241; Analysis 1.39). Infants born to mothers in the metformin group were less likely to have hypoglycaemia (RR 0.34, 95% CI 0.18 to 0.62; RCTs = 3; participants = 241; very low‐quality evidence; Analysis 1.40). However, in Ainuddin 2015, infants born to women in the metformin group had, on average, higher blood glucose at birth (MD 3.57 mg/dL, 95% CI 0.26 to 6.88; RCTs = 1; participants = 206; Analysis 1.43).
Ainuddin 2015, Hickman 2013 and Refuerzo 2015 did not report on: ponderal index; adiposity; nerve palsy; hypocalcaemia; or polycythaemia.
Child/adult: secondary outcomes
Ainuddin 2015, Hickman 2013 and Refuerzo 2015 did not report on: weight; height; head circumference; adiposity; cardiovascular health; type 1 diabetes; type 2 diabetes; impaired glucose tolerance; employment, education and social status/achievement.
Health service: secondary outcomes
In Hickman 2013 there was no clear difference in antenatal hospital admissions between groups (RR 0.22, 95% CI 0.03 to 1.66; RCTs = 1; participants = 15; Analysis 1.45). Meta‐analysis of data from Ainuddin 2015, Hickman 2013 and Refuerzo 2015 showed that infants born to mothers who received metformin compared with insulin were less likely to be admitted to the neonatal intensive care unit (RR 0.37, 95% CI 0.27 to 0.52; RCTs = 3; participants = 241; Analysis 1.46). In Refuerzo 2015 there was no clear difference reported in length of postnatal stay for the infants (reported as median and range) (Analysis 1.47). Hickman 2013 reported that the three neonates who were admitted to the neonatal intensive care unit in the insulin group had lengths of stay of: five days, three to four weeks and 46 days.
In Ainuddin 2015, total costs of treatment throughout pregnancy were, on average, lower for women in the metformin group compared with those in the insulin group (MD ‐65.30 USD, 95% CI ‐77.92 to ‐52.68; RCTs = 1; participants = 206; Analysis 1.48).
Ainuddin 2015, Hickman 2013 and Refuerzo 2015 did not report on: number of hospital or health professional visits; length of antenatal stay; length of postnatal stay (mother); costs to families associated with the management provided; costs associated with the intervention; or cost of offspring care.
Subgroup and sensitivity analyses
We were not able to conduct the planned subgroup analyses or sensitivity analyses due to a paucity of data.
Discussion
Summary of main results
The increasing prevalence and effects of established diabetes on maternal and infant health outcomes highlight the importance of evaluating evidence‐based management for women with established diabetes, impaired glucose tolerance or previous gestational diabetes both preconceptionally and during pregnancy. Additionally, women with impaired glucose tolerance or gestational diabetes in a previous pregnancy represent a group of women with relatively increased insulin resistance, and are at risk of developing type 2 diabetes. Appropriate management of these women is unclear.
Six trials were eligible for inclusion in the review (Ainuddin 2015; Beyuo 2015; Hickman 2013; Ibrahim 2014; Notelovitz 1971; Refuerzo 2015), but only three trials contributed data and are included in the analyses (Ainuddin 2015; Hickman 2013; Refuerzo 2015). These three trials provided data for 241 women who had type 2 diabetes diagnosed before, or during, pregnancy, and their infants.
For our primary outcomes there was no clear difference between the metformin and insulin groups across two trials for pre‐eclampsia (very low‐quality evidence) (Ainuddin 2015; Refuerzo 2015), although in the Ainuddin 2015 trial women receiving metformin were less likely to have pregnancy‐induced hypertension (low‐quality evidence). Women taking metformin were less likely to have a caesarean section birth compared with those taking insulin across the three trials (low‐quality evidence) (Ainuddin 2015; Hickman 2013; Refuerzo 2015). In Ainuddin 2015 there was no clear difference between the metformin groups for large‐for‐gestational‐age infants (very low‐quality evidence). There were no perinatal deaths reported in two trials (very low‐quality evidence) (Ainuddin 2015; Hickman 2013).The trials did not report on neonatal mortality, a morbidity composite outcome, or childhood or adulthood neurosensory disability.
For important secondary outcomes, assessed using the GRADE approach, there were no clear differences between groups in the number of women undergoing induction of labour across two trials (very low‐quality evidence) (Hickman 2013; Refuerzo 2015), though neonatal hypoglycaemia was reduced in the metformin group across the three trials (very low‐quality evidence) (Ainuddin 2015; Hickman 2013; Refuerzo 2015). For mothers, perineal trauma, postnatal depression, and postnatal weight retention were not reported, while for infant outcomes, childhood or adulthood adiposity, and childhood or adulthood diabetes, were not reported.
Few other of this review's secondary outcomes were reported, however additional benefits were observed for metformin, with less weight gain in pregnancy reported in two trials (Ainuddin 2015; Hickman 2013), improved adherence in one trial (Ainuddin 2015), more favourable views of treatment in two trials (Ainuddin 2015; Hickman 2013), less neonatal hyperbilirubinaemia and infection in two trials (Ainuddin 2015; Hickman 2013), less neonatal intensive care unit admission in three trials (Ainuddin 2015; Hickman 2013; Refuerzo 2015), and lower costs of maternal care in one trial (Ainuddin 2015); however there were more small‐for‐gestational‐age infants with metformin in one trial (Ainuddin 2015).
Overall completeness and applicability of evidence
Though we included six trials in this review, we were not able to include outcome data from three of them (Beyuo 2015; Ibrahim 2014; Notelovitz 1971), as they had mixed populations (women with gestational diabetes and established diabetes) and did not report data separately for the subset of women relevant to this review. Two of the three trials that were able to provide data were from the USA (Hickman 2013; Refuerzo 2015), and one was from Pakistan (Ainuddin 2015). These three trials all compared an oral anti‐diabetic agent (metformin) with insulin, therefore, currently no data are available regarding the comparative effects of oral anti‐diabetic agents versus no treatment, or different oral anti‐diabetic agents. Similarly, no data are available regarding the effects of oral anti‐diabetic agents for women with established type 1 or 2 diabetes mellitus, impaired glucose tolerance or previous gestational diabetes mellitus planning a pregnancy, as the three trials that contributed data all recruited pregnant women with type 2 diabetes diagnosed prior to pregnancy (or cases of newly diagnosed overt diabetes in pregnancy, or both).
We selected a number of outcomes for quality assessment using the GRADE approach: while three trials reported on caesarean section, perinatal mortality and neonatal hypoglycaemia, only two reported on pre‐eclampsia and induction of labour, and only one on large‐for‐gestational age infants. There were no data for: perineal trauma, postnatal depression, postnatal weight retention, neonatal mortality or morbidity composite; childhood or adulthood neurosensory disability, or childhood or adulthood diabetes.
Quality of the evidence
Risk of bias in the included studies was mixed. One of the trials contributing data was quasi‐randomised and thus at high risk of selection bias. None of the trials that contributed data were able to blind women or the staff providing care and this may have had an impact on some outcomes. It was not clear in the trials whether there were attempts to blind outcome assessors. In one of the trials that contributed data there was high loss to follow‐up (> 20%) (Ainuddin 2015).
We determined the evidence for outcomes assessed using the GRADE approach to be low quality or very low quality. Evidence was downgraded due to design limitations (risk of bias) and/or imprecision due to small sample sizes, low event rates, and/or uncertain effect estimates.
Potential biases in the review process
We took steps to minimise bias in the review process. Data extraction was carried out by two researchers independently and all data were checked. The GRADE approach assessments were made by two people independently and discrepancies resolved by discussion. We acknowledge that we may have missed relevant trials because we did not formerly search trials registers such as ClinicalTrials.gov or the WHO International Clinical Trials Registry Platform (ICTRP), which became mandatory after October 2016, but we will search these registers in the next update.
Agreements and disagreements with other studies or reviews
There is a dearth of evidence on the use of oral anti‐diabetic agents for women with established diabetes, impaired glucose tolerance or previous gestational diabetes who are planning a pregnancy, or pregnant women with pre‐existing diabetes. Current evidence focuses on women with gestational diabetes, and we refer readers to the Cochrane Reviews Brown 2017b and Brown 2016b for assessments of oral anti‐diabetic agents versus no treatment or alternative oral anti‐diabetic agents, and oral anti‐diabetic agents versus insulin, respectively, in women with gestational diabetes.
One recent systematic review assessed short‐ and long‐term outcomes of metformin compared with insulin in pregnancy, and included trials in women with gestational diabetes or type 2 diabetes (Butalia 2017). The review included data from two of the trials that provided outcome data in our review (Hickman 2013; Refuerzo 2015), one trial included in our review from which we did not include data (Ibrahim 2014), and an additional 13 trials (all in women with gestational diabetes). In agreement with the results of our review, Butalia 2017 reported reductions in pregnancy‐induced hypertension, maternal weight gain in pregnancy, neonatal hypoglycaemia, and neonatal intensive care unit admission with metformin versus insulin, and no clear differences between treatments for pre‐eclampsia, glycaemic control, preterm birth and macrosomia. Conversely, Butalia 2017 reported no clear difference between metformin and insulin for caesarean birth (a reduction with metformin was observed in our review) or small‐for‐gestational age infants (an increase with metformin was observed in our review), and a reduction in large‐for‐gestational age infants (no clear difference was observed in our review).The Butalia 2017 review concluded that while metformin appeared to have short‐term benefits, with no observed harms, information on long‐term benefits and harms is limited, and thus it recommended further follow‐up studies prior to use becoming routine. One of the ongoing trials identified in this review (Feig 2011), the Metformin in Women with Type 2 Diabetes in Pregnancy Trial (MiTy Trial), which compares the effectiveness of the addition of metformin to insulin with standard care (insulin plus placebo) in pregnant women with type 2 diabetes, will provide these longer‐term data from its planned MiTy Kids two‐year follow‐up (NCT01832181).
A systematic review of guidelines for the preconception care of women with type 2 diabetes in pregnancy identified that, while all the included guidelines recommended insulin prior to pregnancy to achieve target concentrations of blood glucose, the more recent ones suggested use of metformin as an adjunct or alternative, for example in situations when insulin is refused or a woman develops resistance (Mahmud 2010). This guideline review noted that while "the safety of currently available oral antidiabetic agents (metformin and glyburide) during pregnancy looks promising, the complete safety and efficacy profile during the full term of pregnancy has not yet been established" (Mahmud 2010).
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
Risk of bias summary: review authors' judgements about each risk of bias item for each included study

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 1 Hypertensive disorders of pregnancy: pre‐eclampsia.
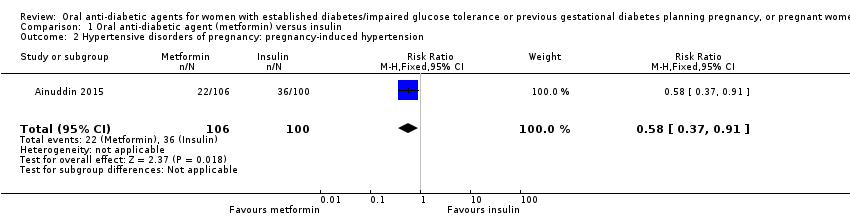
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 2 Hypertensive disorders of pregnancy: pregnancy‐induced hypertension.
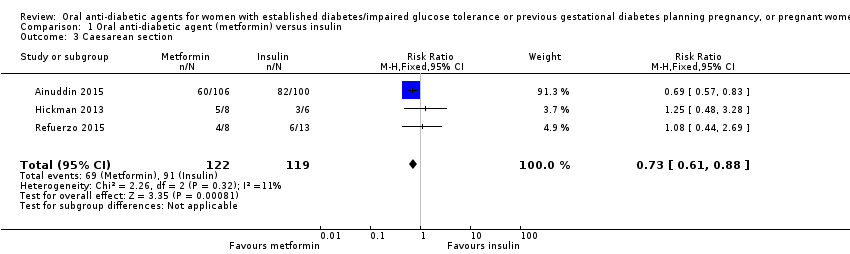
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 3 Caesarean section.
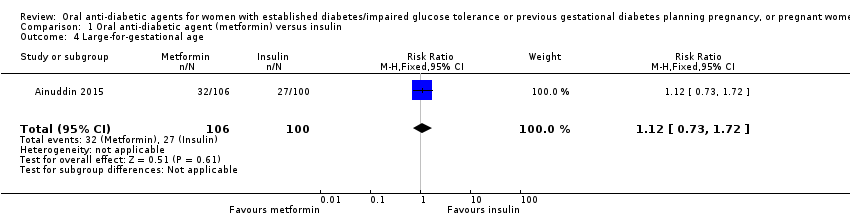
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 4 Large‐for‐gestational age.
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 5 Perinatal mortality.

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 6 Miscarriage.

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 7 Induction of labour.
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 8 Postpartum haemorrhage.

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 9 Weight gain in pregnancy (kg).
| Study | Metformin (N=9) | Insulin (N=6) |
| Hickman 2013 | Median (IQR): 3.16 (2.88, 4.50) | Median (IQR): 10.78 (8.15, 14.42) |
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 10 Weight gain in pregnancy (kg).
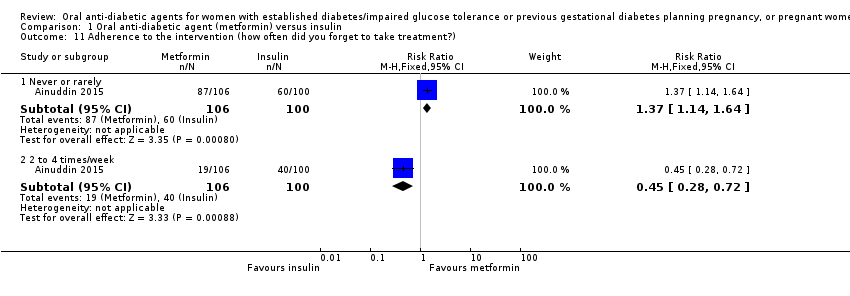
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 11 Adherence to the intervention (how often did you forget to take treatment?).

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 12 Adherence to the intervention.

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 13 Views of the intervention (which medication would you choose in next pregnancy?).
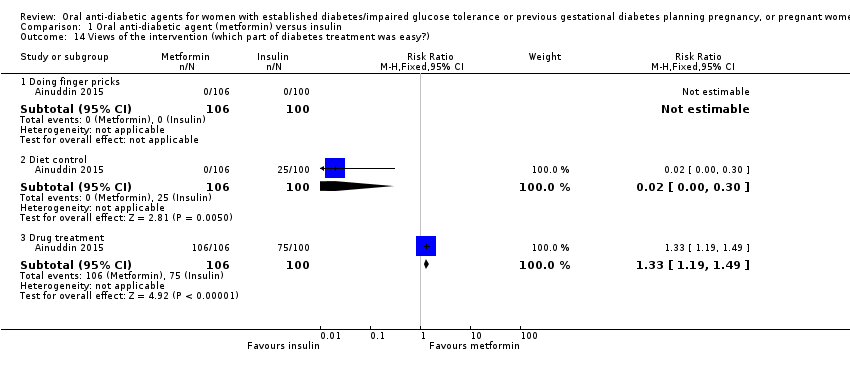
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 14 Views of the intervention (which part of diabetes treatment was easy?).
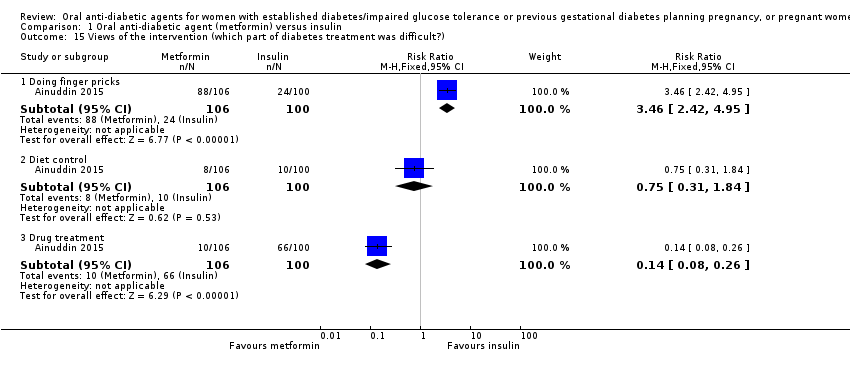
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 15 Views of the intervention (which part of diabetes treatment was difficult?).
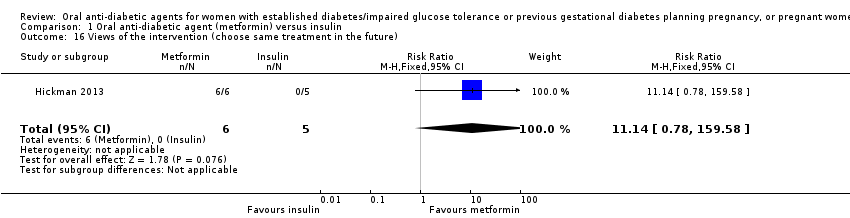
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 16 Views of the intervention (choose same treatment in the future).

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 17 Adverse effects of the intervention (side effects).
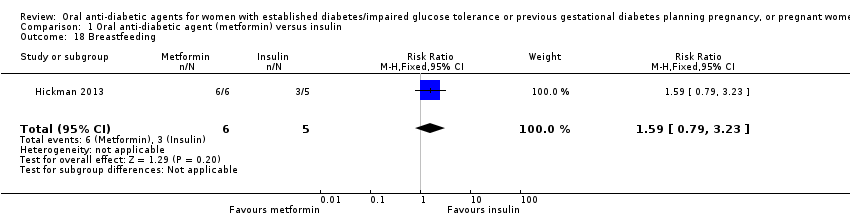
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 18 Breastfeeding.

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 19 Glycaemic control (fasting blood glucose throughout pregnancy (mg/dL)).
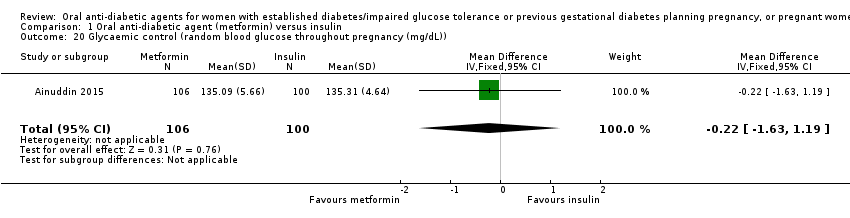
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 20 Glycaemic control (random blood glucose throughout pregnancy (mg/dL)).
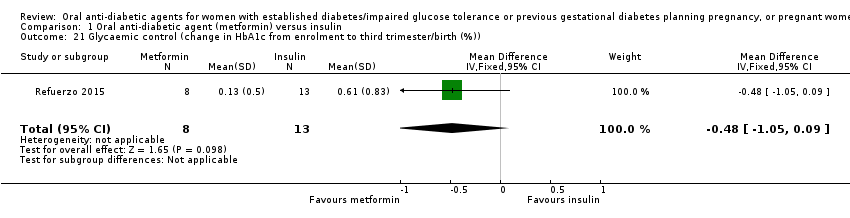
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 21 Glycaemic control (change in HbA1c from enrolment to third trimester/birth (%)).

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 22 Glycaemic control (HbA1c < 7% at third trimester/birth).
| Study | Metformin (N=8) | Insulin (N=6) |
| Hickman 2013 | HbA1c 2nd trimester (%) Median (IQR): 5.55 (5.54, 5.70) | HbA1c 2nd trimester (%) Median (IQR): 5.70 (5.35, 6.28) |
| Hickman 2013 | HbA1c 3rd trimester (%) Median (IQR): 5.85 (5.73, 6.00) | HbA1c 3rd trimester (%) Median (IQR): 5.85 (5.53, 6.55) |
| Hickman 2013 | Delivery glucose (mg/dL) Median (IQR): 96.00 (92.00, 113.00) | Delivery glucose (mg/dL) Median (IQR): 127.50 (109.25, 122.00) |
| Hickman 2013 | Postpartum fasting glucose (mg/dL) Median (IQR): 97.50 (78.50, 108.75) | Postpartum fasting glucose (mg/dL) Median (IQR): 125.50 (109.75, 136.75) |
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 23 Glycaemic control.

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 24 Congenital anomaly (major malformations).

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 25 Stillbirth.

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 26 Neonatal mortality.
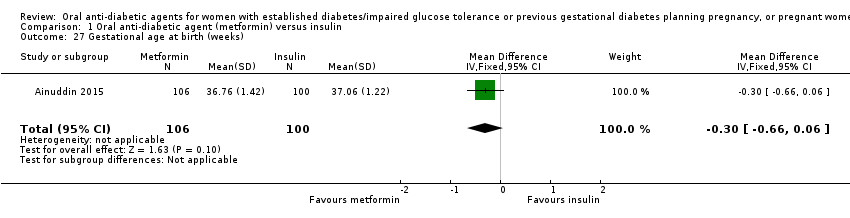
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 27 Gestational age at birth (weeks).
| Study | Metformin | Insulin | P value |
| Hickman 2013 | Median (IQR): 38.40 (37.10, 38.86) N=9 | Median (IQR): 37.50 (35.79, 38.00) N=6 | |
| Refuerzo 2015 | Median (range): 37 (35‐40) N=8 | Median (range): 37 (35‐41) N=13 | 0.977 |
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 28 Gestational age at birth (weeks).

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 29 Preterm birth.
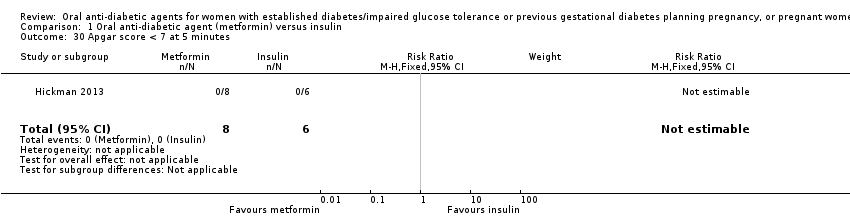
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 30 Apgar score < 7 at 5 minutes.

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 31 Macrosomia (> 4000 g).
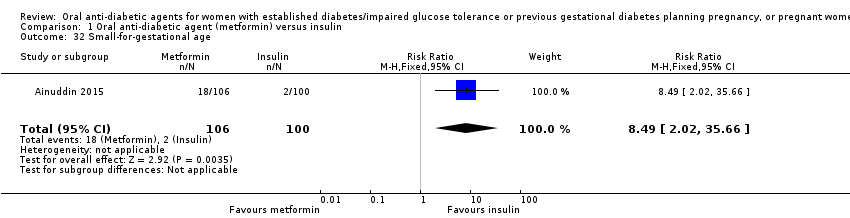
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 32 Small‐for‐gestational age.

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 33 Birthweight (kg).
| Study | Metformin (N=8) | Insulin (N=6) |
| Hickman 2013 | Median (IQR): 3071.50 (2978.75, 3237.75) | Median (IQR): 3295.50 (2964.25, 3566.75) |
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 34 Birthweight (g).
| Study | Metformin (N=8) | Insulin (N=6) |
| Hickman 2013 | Median (IQR): 33.50 (32.48, 34.63) | Median (IQR): 33.50 (32.25, 34.75) |
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 35 Head circumference (cm).
| Study | Metformin (N=8) | Insulin (N=6) |
| Hickman 2013 | Median (IQR): 49.00 (48.07, 50.53) | Median (IQR): 49.50 (48.45, 52.25) |
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 36 Length (cm).
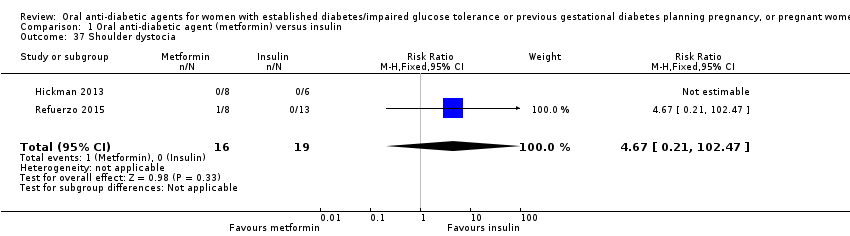
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 37 Shoulder dystocia.

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 38 Bone fracture (birth injury/birth trauma with clavicle fracture).

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 39 Respiratory distress syndrome.
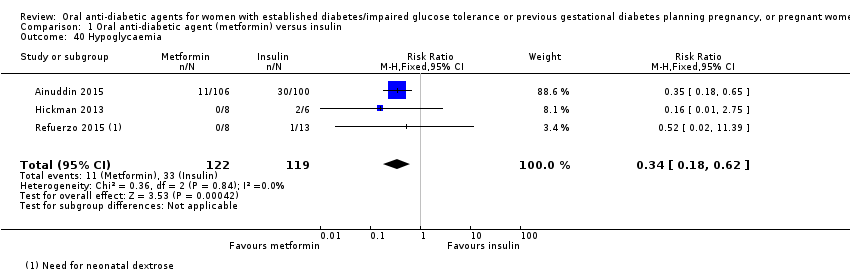
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 40 Hypoglycaemia.
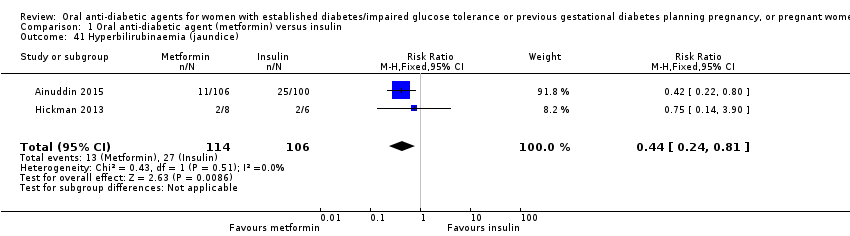
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 41 Hyperbilirubinaemia (jaundice).

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 42 Infection (sepsis).

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 43 Relevant biomarkers (blood glucose level at birth (mg/dL)).
| Study | Metformin (N=6) | Insulin (N=4) |
| Hickman 2013 | Median (IQR): 1.25 (0.92, 1.65) | Median (IQR): 3.95 (2.78, 5.13) |
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 44 Relevant biomarker (cord C peptide).
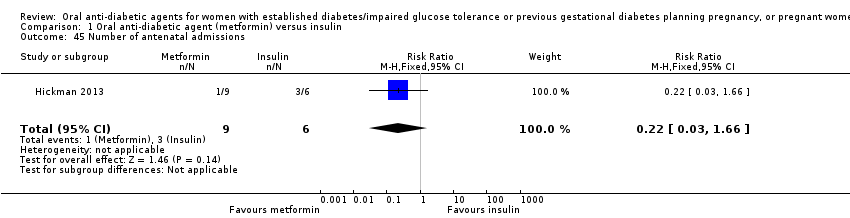
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 45 Number of antenatal admissions.

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 46 Neonatal intensive care unit admission.
| Study | Metformin | Insulin | P value |
| Refuerzo 2015 | Median (range): 3 (1‐8) N=8 | Median (range): 2 (1‐12) N=13 | 0.697 |
Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 47 Length of postnatal stay (baby) (days).

Comparison 1 Oral anti‐diabetic agent (metformin) versus insulin, Outcome 48 Cost of maternal care (total cost of treatment throughout pregnancy (USD)).
| Maternal outcomes: oral anti‐diabetic agent (metformin) compared with insulin for women with established type 2 diabetes mellitus | ||||||
| Patient or population: women with type 2 diabetes | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | Comments | |
| Risk with insulin | Risk with oral anti‐diabetic (metformin) | |||||
| Hypertensive disorders of pregnancy: pre‐eclampsia | Study population | RR 0.63 | 227 | ⊕⊝⊝⊝ | ||
| 186 per 1000 | 117 per 1000 | |||||
| Hypertensive disorders of pregnancy: pregnancy‐induced hypertension | Study population | RR 0.58 | 206 | ⊕⊕⊝⊝ | ||
| 360 per 1000 | 209 per 1000 | |||||
| Caesarean section | Study population | RR 0.73 | 241 | ⊕⊕⊝⊝ | ||
| 765 per 1000 | 558 per 1000 | |||||
| Induction of labour | Study population | RR 1.42 | 35 | ⊕⊝⊝⊝ | ||
| 316 per 1000 | 448 per 1000 | |||||
| Perineal trauma | Study population | ‐ | (0 RCTs) | ‐ | None of the included RCTs reported this outcome | |
| See comment | See comment | |||||
| Postnatal depression | Study population | ‐ | (0 RCTs) | ‐ | None of the included RCTs reported these outcomes | |
| See comment | See comment | |||||
| Postnatal weight retention | Study population | ‐ | (0 RCTs) | ‐ | None of the included RCTs reported these outcomes | |
| See comment | See comment | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Study limitations (‐2): most of the weight in this analysis was from 1 RCT with very serious design limitations 2 Imprecision (‐2): wide 95% CI crossing the line of no effect and small sample sizes of RCTs 3 Study limitations (‐2): 1 RCT with very serious design limitations contributed data 4 Study limitations (‐1): 2 RCTs with design limitations contributed data | ||||||
| Infant outcomes: oral anti‐diabetic (metformin) compared with insulin for women with established diabetes | ||||||
| Patient or population: women with type 2 diabetes mellitus | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | Comments | |
| Risk with insulin | Risk with oral anti‐diabetic (metformin) | |||||
| Large‐for‐gestational age | Study population | RR 1.12 | 206 | ⊕⊝⊝⊝ | ||
| 270 per 1000 | 302 per 1000 | |||||
| Perinatal mortality | Study population | ‐ | 220 | ⊕⊝⊝⊝ | No perinatal mortality in the 2 RCTs | |
| See comment | See comment | |||||
| Hypoglycaemia | Study population | RR 0.34 | 241 | ⊕⊝⊝⊝ | ||
| 277 per 1000 | 94 per 1000 | |||||
| Neonatal mortality or morbidity composite | Study population | ‐ | (0 studies) | ‐ | None of the included RCTs reported this outcome | |
| See comment | See comment | |||||
| Childhood/adulthood neurosensory disability | Study population | ‐ | (0 studies) | ‐ | None of the included RCTs reported this outcome | |
| See comment | See comment | |||||
| Childhood/adulthood adiposity | Study population | ‐ | (0 studies) | ‐ | None of the included RCTs reported this outcome | |
| See comment | See comment | |||||
| Childhood/adulthood diabetes | Study population | ‐ | (0 studies) | ‐ | None of the included RCTs reported this outcome | |
| See comment | See comment | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Study limitations (‐2): 1 RCT with very serious design limitations contributed data 2 Imprecision (‐2): wide 95% CI crossing the line of no effect and small sample size of RCT 3 Study limitations (‐1): 2 RCTs with design limitations contributed data 4 Imprecision (‐2): no events 5 Study limitations (‐2): most of the weight in this analysis was from 1 RCT with very serious design limitations 6 Imprecision (‐1): small sample sizes of RCTs | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Hypertensive disorders of pregnancy: pre‐eclampsia Show forest plot | 2 | 227 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.63 [0.33, 1.20] |
| 2 Hypertensive disorders of pregnancy: pregnancy‐induced hypertension Show forest plot | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.58 [0.37, 0.91] |
| 3 Caesarean section Show forest plot | 3 | 241 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.73 [0.61, 0.88] |
| 4 Large‐for‐gestational age Show forest plot | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.12 [0.73, 1.72] |
| 5 Perinatal mortality Show forest plot | 2 | 220 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Miscarriage Show forest plot | 1 | 15 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.1 [0.10, 44.40] |
| 7 Induction of labour Show forest plot | 2 | 35 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.42 [0.62, 3.28] |
| 8 Postpartum haemorrhage Show forest plot | 1 | 14 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 9 Weight gain in pregnancy (kg) Show forest plot | 1 | 206 | Mean Difference (IV, Fixed, 95% CI) | ‐1.30 [‐1.57, ‐1.03] |
| 10 Weight gain in pregnancy (kg) Show forest plot | Other data | No numeric data | ||
| 11 Adherence to the intervention (how often did you forget to take treatment?) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 11.1 Never or rarely | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.37 [1.14, 1.64] |
| 11.2 2 to 4 times/week | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.45 [0.28, 0.72] |
| 12 Adherence to the intervention Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 12.1 No missed appointments | 1 | 15 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.0 [0.59, 6.79] |
| 12.2 Log book completed > 50% | 1 | 15 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.9 [0.89, 4.04] |
| 13 Views of the intervention (which medication would you choose in next pregnancy?) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 13.1 Metformin | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 7.70 [4.52, 13.14] |
| 13.2 Insulin | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.07 [0.03, 0.19] |
| 13.3 Not sure | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.11 [0.04, 0.29] |
| 14 Views of the intervention (which part of diabetes treatment was easy?) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 14.1 Doing finger pricks | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 14.2 Diet control | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.02 [0.00, 0.30] |
| 14.3 Drug treatment | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.33 [1.19, 1.49] |
| 15 Views of the intervention (which part of diabetes treatment was difficult?) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 15.1 Doing finger pricks | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.46 [2.42, 4.95] |
| 15.2 Diet control | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.31, 1.84] |
| 15.3 Drug treatment | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.14 [0.08, 0.26] |
| 16 Views of the intervention (choose same treatment in the future) Show forest plot | 1 | 11 | Risk Ratio (M‐H, Fixed, 95% CI) | 11.14 [0.78, 159.58] |
| 17 Adverse effects of the intervention (side effects) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 17.1 Gastrointestinal side effects resulting in dose limitation | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 12.27 [0.70, 215.04] |
| 17.2 Gastrointestinal side effects resulting in treatment cessation | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 17.3 Lactic acidosis | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 18 Breastfeeding Show forest plot | 1 | 11 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.59 [0.79, 3.23] |
| 19 Glycaemic control (fasting blood glucose throughout pregnancy (mg/dL)) Show forest plot | 1 | 206 | Mean Difference (IV, Fixed, 95% CI) | 0.01 [‐0.90, 0.92] |
| 20 Glycaemic control (random blood glucose throughout pregnancy (mg/dL)) Show forest plot | 1 | 206 | Mean Difference (IV, Fixed, 95% CI) | ‐0.22 [‐1.63, 1.19] |
| 21 Glycaemic control (change in HbA1c from enrolment to third trimester/birth (%)) Show forest plot | 1 | 21 | Mean Difference (IV, Fixed, 95% CI) | ‐0.48 [‐1.05, 0.09] |
| 22 Glycaemic control (HbA1c < 7% at third trimester/birth) Show forest plot | 1 | 18 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.76, 1.39] |
| 23 Glycaemic control Show forest plot | Other data | No numeric data | ||
| 24 Congenital anomaly (major malformations) Show forest plot | 1 | 15 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 25 Stillbirth Show forest plot | 2 | 220 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 26 Neonatal mortality Show forest plot | 2 | 220 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 27 Gestational age at birth (weeks) Show forest plot | 1 | 206 | Mean Difference (IV, Fixed, 95% CI) | ‐0.30 [‐0.66, 0.06] |
| 28 Gestational age at birth (weeks) Show forest plot | Other data | No numeric data | ||
| 29 Preterm birth Show forest plot | 2 | 35 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.42 [0.08, 2.30] |
| 30 Apgar score < 7 at 5 minutes Show forest plot | 1 | 14 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 31 Macrosomia (> 4000 g) Show forest plot | 2 | 35 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.37 [0.04, 3.10] |
| 32 Small‐for‐gestational age Show forest plot | 1 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 8.49 [2.02, 35.66] |
| 33 Birthweight (kg) Show forest plot | 2 | 227 | Mean Difference (IV, Fixed, 95% CI) | ‐0.13 [‐0.29, 0.04] |
| 34 Birthweight (g) Show forest plot | Other data | No numeric data | ||
| 35 Head circumference (cm) Show forest plot | Other data | No numeric data | ||
| 36 Length (cm) Show forest plot | Other data | No numeric data | ||
| 37 Shoulder dystocia Show forest plot | 2 | 35 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.67 [0.21, 102.47] |
| 38 Bone fracture (birth injury/birth trauma with clavicle fracture) Show forest plot | 2 | 220 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.14, 6.57] |
| 39 Respiratory distress syndrome Show forest plot | 3 | 241 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.52 [0.24, 1.13] |
| 40 Hypoglycaemia Show forest plot | 3 | 241 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.18, 0.62] |
| 41 Hyperbilirubinaemia (jaundice) Show forest plot | 2 | 220 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.44 [0.24, 0.81] |
| 42 Infection (sepsis) Show forest plot | 2 | 220 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.26 [0.08, 0.81] |
| 43 Relevant biomarkers (blood glucose level at birth (mg/dL)) Show forest plot | 1 | 206 | Mean Difference (IV, Fixed, 95% CI) | 3.57 [0.26, 6.88] |
| 44 Relevant biomarker (cord C peptide) Show forest plot | Other data | No numeric data | ||
| 45 Number of antenatal admissions Show forest plot | 1 | 15 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.22 [0.03, 1.66] |
| 46 Neonatal intensive care unit admission Show forest plot | 3 | 241 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.37 [0.27, 0.52] |
| 47 Length of postnatal stay (baby) (days) Show forest plot | Other data | No numeric data | ||
| 48 Cost of maternal care (total cost of treatment throughout pregnancy (USD)) Show forest plot | 1 | 206 | Mean Difference (IV, Fixed, 95% CI) | ‐65.3 [‐77.92, ‐52.68] |