Akupunktura i medicinski potpomognuta oplodnja
Referencias
References to studies included in this review
References to studies excluded from this review
References to ongoing studies
Additional references
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | Randomised controlled trial of fertility patients in Denmark | |
| Participants | Patients (n = 635) scheduled for embryo transfer were randomised into acupuncture according to the principles of Traditional Chinese Medicine (n = 314) or placebo acupuncture (n = 321). The average age of the two groups of women was 31 years and the average body mass index (BMI) was 22.5 for both groups. There were similar numbers of previous IVF/ICSI cycles and similar proportions of causes of infertility between both groups. | |
| Interventions | Needle acupuncture or placebo acupuncture using Strietberger placebo needle for 25 minutes before and after embryo transfer; performed by nurses who were professional acupuncturists or by nurses who had received instruction and training by the acupuncturists prior to the trial | |
| Outcomes | Ongoing pregnancy rate, implantation and pregnancy rates, live birth rates | |
| Assisted conception protocols | Standard, long protocol GnRH down‐regulation and the follicle stimulating hormone (FSH) or human menopausal gonadotrophin (hMG) | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random sequence generation – LOW RISK ‐ ‘the sequence of cluster randomization was based on a computer‐generated list’ |
| Allocation concealment (selection bias) | Unclear risk | ‘nurses did the randomization with the sealed envelope technique’ |
| Blinding (performance bias and detection bias) | Low risk | Sequence allocation was performed by nurses and the procedure was performed blinded to patients and the clinician performing ET |
| Incomplete outcome data (attrition bias) | Low risk | No patients lost to follow up |
| Selective reporting (reporting bias) | Low risk | None known |
| Other bias | Low risk | None known |
| Methods | Randomised controlled trial of fertility patients in US; abstract only | |
| Participants | Patients (n = 258) who had been scheduled for ET were randomised into needle acupuncture (n = 53), laser acupuncture (n = 53), sham laser acupuncture (n = 52), relaxation treatment (n = 50) and no treatment (n = 50). For the purpose of this meta‐analysis, only the results from the needle acupuncture and no treatment groups were used. There were no details on the demographics as abstract only available | |
| Interventions | Needle acupuncture performed for 25 minutes before and after embryo transfer versus no intervention control group. There were no details on the qualifications of the acupuncturists as abstract only available | |
| Outcomes | Clinical pregnancy rate | |
| Assisted conception protocols | Protocol breakdown not provided | |
| Notes | Emailed authors for LBR but no reply | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Abstract only; sequence generation not stated. |
| Allocation concealment (selection bias) | Unclear risk | Abstract only; allocation concealment not stated. |
| Blinding (performance bias and detection bias) | High risk | No sham needle group used, therefore blinding not possible |
| Incomplete outcome data (attrition bias) | Unclear risk | 258 participants randomized but authors did not state the number of participants that completed the study. |
| Selective reporting (reporting bias) | Unclear risk | Did not report live birth |
| Other bias | Low risk | None known |
| Methods | Multicentre randomised control trial undertaken in the US; abstract only | |
| Participants | 107 patients undergoing IVF randomised women into two groups: one with acupuncture treatment (n = 48) and one without (n = 46). There were no details on demographics as this report was presented as an abstract | |
| Interventions | Acupuncture performed for 25 minutes before and after embryo transfer, against no intervention control group.There were no details on the qualifications of the acupuncturists as abstract only available. | |
| Outcomes | Ongoing and clinical pregnancy rate | |
| Assisted conception protocols | Protocol breakdown not provided | |
| Notes | No information provided by authors | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Abstract only; sequence generation not stated |
| Allocation concealment (selection bias) | Unclear risk | Abstract only; allocation concealment not stated. |
| Blinding (performance bias and detection bias) | High risk | No sham acupuncture control used |
| Incomplete outcome data (attrition bias) | Low risk | 107 participants randomized, 94 completed the study. 10 IVF cycles cancelled, 3 patients withdrew. |
| Selective reporting (reporting bias) | Unclear risk | Did not report live birth |
| Other bias | Low risk | None known |
| Methods | Randomised controlled trial, fertility patients in clinic in Germany | |
| Participants | 225 patients randomised: 116 to treatment and 109 to placebo. Treatment included placing Chinese herbs in patients' ears. No losses to follow up. Placebo treatment at sites that will not affect fertility, but physicians who were performing ET were blinded. The average age (± SD) of the study group (n = 116) was 35.1 years (± 3.8) compared to 34.7 years (± 4) for the placebo group (n = 109). There were no statistical differences in the body mass index (BMI), causes of subfertility, and number of previous cycles between the study and control groups. | |
| Interventions | Treatment included acupuncture + Chinese herbs in ears versus control group of acupuncture at sites that are not believed to affect fertility. The intervention was performed for 30 minutes after embryo transfer and again 3 days later. All acupuncture was performed by the same practitioner | |
| Outcomes | Live birth rate, clinical pregnancy rates and ongoing clinical pregnancy rates | |
| Assisted conception protocols | Standard, long protocol GnRH down‐regulation and the follicle stimulating hormone (FSH) or human menopausal gonadotrophin (hMG) | |
| Notes | Placebo group did not have drugs placed in ears | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated in the manuscript |
| Allocation concealment (selection bias) | Unclear risk | ‘randomised with sealed randomization envelopes’ but not stated if these envelopes where opaque or sequentially numbered. |
| Blinding (performance bias and detection bias) | Low risk | Use of placebo treatment in control group |
| Incomplete outcome data (attrition bias) | Low risk | 225 participants randomized; none lost to follow up. |
| Selective reporting (reporting bias) | Unclear risk | Not known whether LBR a prestated outcome |
| Other bias | Low risk | None known |
| Methods | Randomised controlled trial of fertility patients in the US | |
| Participants | 150 patients recruited and randomised to either needle acupuncture (n = 78) and no treatment (n=68). The average age of the two groups of women was 36 years, with similar numbers of previous IVF cycles in the two groups. | |
| Interventions | Acupuncture performed by an acupuncturist 25 minutes before and after embryo transfer versus no treatment control | |
| Outcomes | Clinical pregnancy rate | |
| Assisted conception protocols | Protocol breakdown not provided | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | ‘randomisation was accomplished by using a computer‐generated random numbers table’ |
| Allocation concealment (selection bias) | Unclear risk | Not stated in the manuscript |
| Blinding (performance bias and detection bias) | High risk | Not possible to blind as control group had no intervention |
| Incomplete outcome data (attrition bias) | Unclear risk | 146 participants randomized but number completed not reported. |
| Selective reporting (reporting bias) | Unclear risk | No LBR outcomes reported. |
| Other bias | Low risk | None known |
| Methods | Randomised controlled trial of fertility patients in the US; abstract only | |
| Participants | 1000 patients randomised to five arms: needle acupuncture (n = 200), laser acupuncture (n = 202), sham laser acupuncture (n = 198), relaxation (n = 203) and non‐treatment group (n = 197). No demographics breakdown given but stated no difference between groups | |
| Interventions | Two treatment arms (laser and needle acupuncture) and three control arms (sham laser acupuncture, relaxation and non‐treatment). For the purpose of this meta‐analysis, only the results from the needle acupuncture and no treatment groups were used | |
| Outcomes | Chemical and clinical pregnancy rate | |
| Assisted conception protocols | Protocol breakdown not provided | |
| Notes | Only needle acupuncture versus control are relevant to this review | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Abstract only, no randomisation details given |
| Allocation concealment (selection bias) | Unclear risk | Abstract only, no details given |
| Blinding (performance bias and detection bias) | High risk | Control group received no treatment |
| Incomplete outcome data (attrition bias) | Unclear risk | not stated if all participants randomized completed the study |
| Selective reporting (reporting bias) | Unclear risk | No LBR outcomes reported. |
| Other bias | Low risk | None known |
| Methods | Open, randomised single‐centre trial performed at the IVF unit of Reproductive Medicine at Sahlgrenska University Hospital in Goteborg | |
| Participants | There were 160 women randomised in the study: 80 to the EA (electro‐acupuncture) group and 80 to the CA (conventional acupuncture) group. The average age of the women (± SD) in the control group (n = 80) was 33.9 years (± 3.7) compared to 33.2 years (± 3.6) in the intervention group; the average number of IVF cycles performed was 1.56 (± 0.93) compared to 1.48 (± 0.93). The majority of women had male factor or unexplained subfertility. | |
| Interventions | The study compared electro‐acupuncture at the time of oocyte retrieval (EA group) with conventional analgesia (intravenous alfentanil). Both groups also had a paracervical block performed. Electro‐acupuncture was performed by midwives who had been trained in the IVF unit. | |
| Outcomes | Wellbeing was evaluated with the State Trait Anxiety Inventory (STAI). Pain and subjective expectations and experiences were recorded on a visual analogue scale (VAS). Time and drug consumption were recorded Pregnancy rate was recorded as secondary outcome | |
| Assisted conception protocols | Standard, long protocol GnRH down‐regulation and the follicle stimulating hormone (FSH) or human menopausal gonadotrophin (hMG) | |
| Notes | Study designed to assess effectiveness of acupuncture as an analgesic | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | ‘randomisation was performed by the study coordinator according to a computerized list’ |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding (performance bias and detection bias) | High risk | Conventional analgesia of I.V. alfentanil used as control analgesia. Therefore both participants and personnel not blinded. Not stated if assessor was blinded. |
| Incomplete outcome data (attrition bias) | Low risk | 160 women randomized; 2 lost to follow up. |
| Selective reporting (reporting bias) | Unclear risk | No LBR outcome reported. |
| Other bias | Low risk | None |
| Methods | Randomised study performed at the IVF centre of China Medical University Hospital in Taiwan | |
| Participants | A total of 44 women were enrolled in the study: 30 were randomised to acupuncture group and 14 to the control (no‐acupuncture group). The two groups were described as comparable for demographics including age and cause of infertility | |
| Interventions | The study compared electro‐acupuncture (twice a week for two weeks, from cycle day 2 to the day prior to oocyte retrieval) with no acupuncture around the time of oocyte retrieval | |
| Outcomes | Outcome measures studied were clinical pregnancy and the pulsatility index (PI) of left and right uterine arteries | |
| Assisted conception protocols | Protocol breakdown not provided | |
| Notes | The study was designed to assess the impact of acupuncture on uterine artery blood flow and clinical pregnancy rate | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated |
| Allocation concealment (selection bias) | Unclear risk | ‘randomly assigned to one of the two groups by selection of a sealed envelope.’ |
| Blinding (performance bias and detection bias) | High risk | Control group received no treatment |
| Incomplete outcome data (attrition bias) | High risk | 30 randomised to acupuncture group, and 26 to control group (but 12 in the control group dropped out), leaving 30 in the acupuncture group and only 14 in the control group. |
| Selective reporting (reporting bias) | Unclear risk | No LBR outcome data reported. |
| Other bias | Low risk | None known |
| Methods | Randomised trial of fertility patients in Denmark | |
| Participants | 200 patients randomised to either electro‐acupuncture (n = 100) or conventional analgesia (n = 100) at the time of oocyte retrieval. Both groups also received a para‐cervical block. | |
| Interventions | Electro‐acupuncture at the time of oocyte retrieval, given by specially trained nurses, versus conventional analgesia control (benzodiazepine, alfentanil) | |
| Outcomes | VAS scale | |
| Assisted conception protocols | Protocol breakdown not provided | |
| Notes | Study designed to assess effectiveness of acupuncture as an analgesic | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Details not stated |
| Allocation concealment (selection bias) | Low risk | Adequate: randomisation using sealed unlabelled envelopes containing a study number |
| Blinding (performance bias and detection bias) | Low risk | ‘doctors and patients are blinded to the arm of treatment’. |
| Incomplete outcome data (attrition bias) | Low risk | 160 participants randomized; 8 in total withdrew from the study. |
| Selective reporting (reporting bias) | Unclear risk | LBR not a prestated outcome |
| Other bias | Low risk | None known |
| Methods | Randomised controlled trial of fertility patients in Brazil | |
| Participants | 416 patients stratified according to age and then randomised to either acupuncture group (n = 208) or control with no acupuncture (n = 208) | |
| Interventions | Needle acupuncture 25 minutes before and after embryo transfer versus no acupuncture control. Intervention performed by the same practitioner in all cases There was no statistically significant difference between the two groups for demographic characteristics. The average age (± SD) in the acupuncture group was 35.3 (± 4.7) compared to 34.6 (± 4.6) in the control group (p = 0.103). The average BMI in the acupuncture group was 22.4 (± 3.8) compared to 22.4 (± 2.9) in the control group (P = 0.951) The main causes of subfertility were ovarian disorders and male factor with no statistical significance between both groups for any cause of subfertility | |
| Outcomes | Pregnancy rate, implantation rate, abortion rate and live birth rate | |
| Assisted conception protocols | Standard, long protocol GnRH down‐regulation and the follicle stimulating hormone (FSH) or human menopausal gonadotrophin (hMG) | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | ‘patients were randomized before the beginning of the ovarian stimulation according to computer generated randomized numbers ‘ |
| Allocation concealment (selection bias) | Unclear risk | method of allocation concealment not reported |
| Blinding (performance bias and detection bias) | High risk | Control group had no treatment. It was not stated if the clinicians or the assessors of the study were blinded. |
| Incomplete outcome data (attrition bias) | Low risk | 416 participants were randomized; no drop out noted. |
| Selective reporting (reporting bias) | Unclear risk | LBR not a prestated outcome. |
| Other bias | Low risk | None |
| Methods | Randomized controlled trial of fertility patients in US | |
| Participants | 160 patients undergoing IVF ± ICSI were randomised to either true acupuncture (n = 87) or sham acupuncture (n = 74) The average age (± SD) in the true acupuncture group was 33.3 (± 0.307) years compared to 33.16 (± 0.334) years in the sham acupuncture group. There was no statistically significant difference in BMI or infertility diagnosis between the two groups, with the leading causes of infertility being male factor, ovarian dysfunction and unexplained. | |
| Interventions | True (needle) acupuncture performed by hospital employed licensed acupuncturists versus sham placebo acupuncture. Both interventions performed for 25 minutes before and after embryo transfer | |
| Outcomes | Clinical pregnancy rate and clinical symptoms during embryo transfer | |
| Assisted conception protocols | Protocol breakdown not provided | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | patients were randomized using a ‘random number generator’ |
| Allocation concealment (selection bias) | Low risk | Use of 'sealed, sequentially numbered, opaque envelopes’. |
| Blinding (performance bias and detection bias) | Low risk | Control group was allocated to Sham acupuncture. The physicians and patients were blinded to the randomization until the conclusion of the study. |
| Incomplete outcome data (attrition bias) | Low risk | 160 participants were randomized; 1 lost to follow up |
| Selective reporting (reporting bias) | Unclear risk | LBR outcome data not reported. |
| Other bias | Low risk | None |
| Methods | Randomised controlled trial in fertility clinic in Germany | |
| Participants | 160 patients randomised: 80 to treatment and 80 to no intervention control. The age of the women (± SD) in the control group (n = 80) was 32.1 years (± 3.9) compared to 32.8 years (± 4.1) in the acupuncture group (n = 80). In the control group the average number of previous cycles was 2.0 (± 2.0) versus 2.1 (± 2.1) in the treatment group. Most women had tubal disease, followed by male factor infertility then polycystic ovarian disease. These were in equal portions in both the study and control groups. | |
| Interventions | Acupuncture performed by "well‐trained examiners" 25 min before and after embryo transfer for treatment group; auricular acupuncture also performed on the treatment group | |
| Outcomes | Clinical pregnancy rates | |
| Assisted conception protocols | Protocol breakdown not given | |
| Notes | Same authors as Paulus 2003 but different group of patients | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated randomisation |
| Allocation concealment (selection bias) | Unclear risk | Not stated how the allocation was carried out. |
| Blinding (performance bias and detection bias) | High risk | Control group had no treatment. Not stated if clinicians or assessors were blinded. |
| Incomplete outcome data (attrition bias) | Low risk | 160 randomised; no drop out. |
| Selective reporting (reporting bias) | Unclear risk | Not known whether LBR a prestated outcome |
| Other bias | Low risk | None |
| Methods | Randomised placebo‐controlled trial; abstract only | |
| Participants | Patients were divided into two groups by random selection: embryo transfer with verum acupuncture (n = 100) and embryo transfer with placebo needling (n = 100). No demographic details presented | |
| Interventions | Acupuncture or sham acupuncture performed for 25 minutes before and after embryo transfer. In the control group (n=100) a placebo needle set was used without penetrating the skin, but at the same acupoints and after the same scheme | |
| Outcomes | Clinical pregnancy rates | |
| Assisted conception protocols | Protocol breakdown not given | |
| Notes | Only included women with good embryos | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | computer generated randomisation |
| Allocation concealment (selection bias) | Unclear risk | Abstract only, not stated |
| Blinding (performance bias and detection bias) | Low risk | Control group had placebo needling. |
| Incomplete outcome data (attrition bias) | Low risk | 100 participants were randomized. No drop out reported. |
| Selective reporting (reporting bias) | Unclear risk | Not known whether LBR a prestated outcome |
| Other bias | Low risk | None |
| Methods | Randomised controlled trial in fertility clinic in Austria | |
| Participants | Patients were randomised in proportions of 1:1:1 to treatment with electro‐acupuncture (n = 32), auricular acupuncture without electrical stimulation (n = 32) or a control group without needles or electrical stimulation (n = 30). The mean ages (± SD) of the women undergoing IVF treatment in the group receiving electro‐acupuncture with remifentanil (EA), acupuncture with remifentanil (A), and remifentanil with placebo (CO) were 33.3 years (± 1.7), 34.2 years (± 1.1) and 33.9 years (± 1.9), respectively. There were no differences in the number of failed cycles or causes of subfertility. | |
| Interventions | EA, or EA with electrical stimulation or control of conventional analgesia (remifentanil) at the time of oocyte retrieval | |
| Outcomes | Pain intensity and subjective well being were assessed using a visual analogue scale Nausea and tiredness were also assessed using a visual rating scale | |
| Assisted conception protocols | Protocol breakdown not provided | |
| Notes | Study designed to assess effectiveness of acupuncture as an analgesic Each P‐Stim™ was programmed by an independent technician for electrical stimulation or no stimulation before the study. To ensure blinding of the investigator, each P‐Stim™ was packed in a non‐transparent case in which the respective permanent needles or adhesive tapes were also included. The packages were numbered consecutively, according to the randomisation list. Patients and investigators were blinded to the randomisation | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | computer generated sequence randomisaton |
| Allocation concealment (selection bias) | Unclear risk | ‘Randomisation was concealed until at least 30 patients were randomized.’ ‘Patients and investigators were blinded to the randomisation’. Method of allocation concealment not clearly reported |
| Blinding (performance bias and detection bias) | High risk | Control group had traditional I.V. pain relief. |
| Incomplete outcome data (attrition bias) | Low risk | 94 were randomized. 1 drop out. |
| Selective reporting (reporting bias) | Unclear risk | LBR outcome not reported. |
| Other bias | Low risk | None known |
| Methods | Randomised controlled trial in fertility clinic in Australia | |
| Participants | 228 randomised, 36 excluded: 110 in treatment group and 118 in control group. The average age of the control group (± SD) was 35.9 years (± 4.7) versus 36.1 years (± 4.8) in the study group; there were no differences in the number of previous treatment cycles, BMI, duration of subfertility. | |
| Interventions | All women had 3 sessions: day 9 of stimulation, immediately before ET, and immediately after ET. For the sham acupuncture group a sham needle was used close to but not on the treatment point | |
| Outcomes | Clinical pregnancy rates | |
| Assisted conception protocols | Protocol breakdown not provided | |
| Notes | After 3rd session, 24 in treatment group and 10 in control group guessed their allocation group correctly | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | ‘randomization was in balanced, variable blocks of random size prepared by a researcher not involved in the trial’. |
| Allocation concealment (selection bias) | Unclear risk | Not stated specifically |
| Blinding (performance bias and detection bias) | Unclear risk | Control groups had placebo needles (Streitberger) although after the 3rd session, 24 in the treatment group and 10 in the control group guessed their allocation group correctly. |
| Incomplete outcome data (attrition bias) | High risk | 228 subjects were randomized. 36 women had to be withdrawn (15%). |
| Selective reporting (reporting bias) | Unclear risk | LBR data not reported. |
| Other bias | Low risk | None known |
| Methods | Randomised controlled trial of fertility patients in Hong Kong | |
| Participants | 370 patients undergoing assisted reproductive treatment randomised to either acupuncture (n = 185) or placebo acupuncture arms (n = 185). The median age (interquartile range) in the acupuncture and placebo groups respectively was 36 (33 ‐ 38) and 36 (34 ‐ 38). Mean BMI (± SD) was similar at 21.6 (± 2.1) and 21.7 (± 2.7) kg/m2 for acupuncture and placebo groups respectively. Both groups were comparable in terms of duration of infertility, cause of infertility, previous experience of acupuncture and smoking habit | |
| Interventions | Needle acupuncture or placebo needle acupuncture for 25 minutes before and after embryo transfer. Intervention performed by a certified Chinese acupuncturist with a degree in Chinese Medicine and 3 years experience | |
| Outcomes | Pregnancy rate, clinical pregnancy rate, live birth rate, miscarriage rate | |
| Assisted conception protocols | Standard, long protocol GnRH down‐regulation and the follicle stimulating hormone (FSH) or human menopausal gonadotrophin (hMG) | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were randomized by a computer generated randomization list |
| Allocation concealment (selection bias) | Low risk | Sealed opaque envelopes from the list used. ‘The sequence of randomization was concealed until interventions were assigned.’ |
| Blinding (performance bias and detection bias) | Low risk | ‘patients, clinical staff involved in the care of patients and embryologist were blinded to the treatment group assigned’. The codes were only revealed after the completion of the entire study. Control group also had placebo needles. |
| Incomplete outcome data (attrition bias) | Low risk | 370 participants randomized; all completed the study. |
| Selective reporting (reporting bias) | Low risk | None known. |
| Other bias | Low risk | None known |
| Methods | Randomised controlled trial of fertility patients undergoing frozen embryo transfer in Hong Kong | |
| Participants | 226 patients randomised to either real (n = 113) or placebo acupuncture (n=113). The median age at thawing was 36 (34 ‐ 38) and 36 (34 ‐ 39) years for real and placebo acupuncture respectively. The BMI, duration and cause of infertility and previous experience of acupuncture were also comparable between the two groups. | |
| Interventions | Needle acupuncture according to TCM principles or placebo acupuncture with Streitberger's sham placebo needles. Intervention performed by a certified Chinese acupuncturist with a degree in Chinese Medicine and 3 years experience | |
| Outcomes | Overall pregnancy rate, clinical pregnancy rate, ongoing pregnancy rate, live birth rate | |
| Assisted conception protocols | Standard, long protocol GnRH down‐regulation and the follicle stimulating hormone (FSH) or human menopausal gonadotrophin (hMG) | |
| Notes | More patients in placebo group correctly guessed their randomisation compared to the true acupuncture group | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | participants were randomized by a computer generated randomization list |
| Allocation concealment (selection bias) | Low risk | Sealed opaque envelopes from the list was used. ‘The sequence of randomization was concealed until interventions were assigned.’ |
| Blinding (performance bias and detection bias) | Low risk | ‘patients, clinical staff involved in the care of patients and embryologist were blinded to the treatment group assigned’. The codes were only revealed after the completion of the entire study. Control group also had placebo needles. |
| Incomplete outcome data (attrition bias) | Low risk | 226 participants randomized. All completed the study. |
| Selective reporting (reporting bias) | Low risk | LBR available. |
| Other bias | Low risk | None known |
| Methods | Randomised controlled trial, conducted in Sweden | |
| Participants | 150 women undergoing IVF and ET were randomised to receive either electro‐acupuncture and a paracervical block or alfentanil analgesia and a paracervical block. The mean ages (range) of the study and control groups were 33.3 years (25 to 42) and 34.4 years (25 to 46). There was no difference in the two groups in terms of the cause of subfertility and the number of previous cycles. | |
| Interventions | Acupuncture was performed at least 30 min before oocyte aspiration and PCB was placed at the start of the procedure and terminated directly after oocyte aspiration | |
| Outcomes | VAS, level of stress, implantation and pregnancy rates | |
| Assisted conception protocols | Protocol breakdown not provided | |
| Notes | Study designed to assess effectiveness of acupuncture as an analgesic | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Each centre randomized its patients using sealed, unlabelled envelopes" ‐ no further details |
| Allocation concealment (selection bias) | Unclear risk | ‘sealed unlabelled envelope’ |
| Blinding (performance bias and detection bias) | High risk | Control group had traditional analgesia and t (Alfentanil + para cervical block) therefore blinding nor possible for clinicians or participants. |
| Incomplete outcome data (attrition bias) | Low risk | 150 women were randomized. 1 drop out. |
| Selective reporting (reporting bias) | Unclear risk | LBR data not reported. |
| Other bias | Unclear risk | "There is a possible bias in the study in that some of the women in the EA group were administered additional alfentanil during oocyte aspiration." |
| Methods | Randomised, controlled multi‐centre trial in Sweden | |
| Participants | Women were randomised to either electro‐acupuncture and a paracervical block or alfentanil and a paracervical block, as analgesia at the time of oocyte retrieval. The mean age (range) in the study group was 32.9 years (22 to 38) and for the control group it was 32.9 years (25 to 38). The causes of infertility and number of IVF attempts did not differ between the two groups. | |
| Interventions | Women were given EA and a PCB of lidocaine hydrochloride during oocyte aspiration. Those women randomised to the alfentanil group were given alfentanil and a PCB during oocyte aspiration. The acupuncture stimulation began at least 30 min before oocyte aspiration | |
| Outcomes | VAS were used for pain assessment Other variables recorded included abdominal pain, pain during placement of PCB, time of discomfort, adequacy of analgesia, stress level, nausea. IVF outcomes were pregnancy rate (number of pregnancies per embryo transfer), implantation rate (number of gestational sacs per number of transferred oocytes) and on‐going pregnancies (number of pregnancies per embryo transfer after the 16th week of gestation) | |
| Assisted conception protocols | Protocol breakdown not provided | |
| Notes | Stopped after interim analysis as results show no difference between two groups. Study designed to assess effectiveness of acupuncture as an analgesic | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | not stated |
| Allocation concealment (selection bias) | Unclear risk | ‘sealed unlabeled envelopes’ |
| Blinding (performance bias and detection bias) | High risk | Control group had paracervical block + Alfentanil and therefore blinding nor possible for clinicians or participants. |
| Incomplete outcome data (attrition bias) | Low risk | 286 randomized; 5 in the acupuncture group and 7 in the control group dropped out. |
| Selective reporting (reporting bias) | Unclear risk | Not known whether LBR a prestated outcome |
| Other bias | Low risk | None |
| Methods | Randomised controlled trial with patients from private clinic in Denmark | |
| Participants | 273 women randomised: 87 allocated to no acupuncture and 95 to acupuncture on ET day only; 91 to acupuncture on ET and ET+2 days; 27 excluded, The average ages of the three groups of women were: 37 years (27 to 45) in the control (n = 87) group, 37 years (24 to 45) in the group who had acupuncture on the day of ET (n = 95), and 37 years (27 to 45) for those with repeated acupuncture (ET + 2) (n = 91). There was no difference in the BMI between the three groups and about 67% of women had one or more attempts of IVF in the three groups. The main causes of subfertility were described as male factor or unexplained | |
| Interventions | Acupuncture was performed by specially trained nurses on patients undergoing ET on the day of ET, ET+2 and not on controls | |
| Outcomes | Clinical pregnancy rate on ultrasound | |
| Assisted conception protocols | Standard, long protocol GnRH down‐regulation and the follicle stimulating hormone (FSH) or human menopausal gonadotrophin (hMG) | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation procedure handled by nurse not involved in study |
| Allocation concealment (selection bias) | Unclear risk | ‘drawing of sealed envelope’ ‐ no further details reported |
| Blinding (performance bias and detection bias) | High risk | Control group had paracervical block, so blinding of the participants and personnel not possible. |
| Incomplete outcome data (attrition bias) | Low risk | 300 participants randomized. 27 dropped out leaving 273 participants for analysis. |
| Selective reporting (reporting bias) | Unclear risk | LBR data not prestated outcome. |
| Other bias | Low risk | none |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
| No reply to written and electronic request; study design, allocation concealment and outcomes unclear | |
| No reply to electronic request; study design, methods and results not known | |
| No outcomes of interest | |
| No reply to electronic request; study design, methods and results not known | |
| Inadequate randomisation process in study design, based on odd and even numbers | |
| Lack details on pregnancy outcome, study design, allocation concealment and type of randomisation; no reply to written or electronic letters | |
| No reply to electronic request; study numbers, randomisation process and outcomes unclear | |
| No reply to electronic request; study design, methods and results not known | |
| No reply to electronic request; study design, allocation concealment and outcomes unclear | |
| Lacks details on allocation concealment and randomisation, no reply to requests for details; crossover design |
Characteristics of ongoing studies [ordered by study ID]
| Trial name or title | Acupuncture compared to sham acupuncture and standard care to improve live birth rates for women undergoing IVF: a randomised controlled trial |
| Methods | Parallel design, randomised controlled trial |
| Participants | Women aged less than 43 years, undergoing a fresh IVF or ICSI cycle, and restricted to women with the potential for a lower live birth rate defined as > 2 previous unsuccessful embryo transfers (fresh or frozen), and unsuccessful clinical pregnancies of quality embryos deemed by the embryologist to have been suitable for freezing by standard criteria |
| Interventions | Needle or sham acupuncture for 1 hr on day 6‐8 of the IVF cycle, plus two treatments on the day of the embryo transfer, 30 minutes before and after embryo transfer. Compared to no treatment control |
| Outcomes | Primary outcome: live birth ‐ defined as the delivery of one or more living infants, greater than 20 weeks gestation or 400 grams or more birth weight. Secondary outcomes: 1. clinical pregnancy defined as demonstration of fetal heart activity on ultrasound scan 2. miscarriage defined as a non viable pregnancy prior to 12 weeks gestation 3. quality of life 4. self efficacy |
| Starting date | Registration: 02/03/2011 |
| Contact information | Caroline Smith Centre for Complementary Medicine Research University of Western Sydney Locked Bag 1797 Penrith South DC NSW 2751, Australia |
| Notes |
| Trial name or title | Effects of acupuncture on outcome of in vitro fertilization and intracytoplasmic sperm injection (IVF/ICSI) in women with polycystic ovarian ‐ |
| Methods | Parallel design, triple blind, randomised controlled trial |
| Participants | Inclusion criteria: women with the diagnosis of PCO (Rotterdam criteria) admitted to the clinic for IVF or ICSI treatments of infertility |
| Interventions | Intervention group 1: acupuncture based on Traditional Chinese Medicine, 5 sessions of thirty minutes. Intervention 2: Control group: (placebo) the same needles are used in 5 sessions of thirty minutes |
| Outcomes | Primary outcomes: Embryo quality. Timepoint: 2 days after embryo transfer. Method of measurement: diagnosed by Embryologist and with embryological criteria. Oocyte fertilisation rate. Timepoint: first day after embryo transfer. Method of measurement: diagnosed by embryologist and with embryological criteria Oocyte metaphase 2. Timepoint: before and after embryo transfer. Method of measurement: diagnosed by embryologist and with embryological criteria Secondary outcomes: Biochemical pregnancy. Timepoint: 2 weeks after embryo transfer. Method of measurement: B‐hCG Clinical pregnancy. Timepoint: 4 weeks after embryo transfer. Method of measurement: sac observed in vaginal sonography Miscarriage. Timepoint: <12 weeks after embryo transfer. Method of measurement: vaginal sonography Take home baby. Timepoint: 9 months after embryo transfer. Method of measurement: Delivery |
| Starting date | Registration 13/04/2011 |
| Contact information | Rashidi Batool Address: Tehran University of Medical Sciences, Valieasr Hospital and Imam Khomeini Hospital Tehran Islamic Republic of Iran |
| Notes |
| Trial name or title | The Effect of Acupuncture on Infertility With In‐Vitro Fertilization (IVF) Patients |
| Methods | Parallel design, single‐blinded randomised controlled trial |
| Participants | Inclusion criteria: ‐ Undergoing in vitro fertilisation protocol (both IVF and intracytoplasmic sperm injection ‐ ICSI) ‐ Acupuncture naive ‐ Basal FSH <10 ‐ Minimum age 21 years |
| Interventions | Acupuncture |
| Outcomes | Primary outcome: Clinical pregnancy rate Secondary outcomes: ‐ B‐endorphin levels ‐ Miscarriage rate ‐ Stress measurement ‐ Take home baby rate |
| Starting date | Registration: 20/06/2006 |
| Contact information | Grant Zhang, Ph.D. Center For Integrative Medicine, University of Maryland |
| Notes |
| Trial name or title | Chinese Traditional Medicine Contribution to Improve In‐vitro Fertilization (IVF) Results: Acupuncture in Embryo Transfer |
| Methods | Parallel design, double‐blinded, randomised controlled trial |
| Participants | Inclusion criteria: ‐ 18 to 35 years old ‐ BMI 20‐25 ‐ Medical indication of intracytoplasmic sperm injection (ICSI) treatment to treat sterility ‐ No previous in vitro fertilisation (IVF) or intracytoplasmic sperm injection (ICSI) treatments ‐ No previous experience of acupuncture treatments ‐ Make cause of sterility ‐ At least one high quality embryo on the day of uterine transfer |
| Interventions | Acupuncture versus bed rest |
| Outcomes | Primary outcome: pregnancy rate Secondary outcomes: ‐ Analysis of the results of assisted reproductive cycle ‐ Determination of serum prolactin and 24h urine cortisol ‐ Endometrial vascularisation study ‐ Rating preconceived ideas about acupuncture |
| Starting date | Registered: 04/10/2011 |
| Contact information | Monica Romeu |
| Notes |
| Trial name or title | Transcutaneous Electrical Acupoint Stimulation to Improve Pregnancy Rates for Women Undergoing in Vitro Fertilization |
| Methods | Single blind RCT |
| Participants | Women undergoing IVF |
| Interventions | Transcutaneous electrical acupoint stimulation vs no acupuncture |
| Outcomes | Live birth, clinical pregnancy |
| Starting date | May 2012 |
| Contact information | Cui Hong Zheng, Doctor ph: 86‐27‐83663275 email: [email protected] |
| Notes |
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Live Birth Rate Show forest plot | 2 | 464 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.59, 1.29] |
| Analysis 1.1  Comparison 1 Acupuncture around the time of oocyte retrieval versus control (sham, placebo, no acupuncture), Outcome 1 Live Birth Rate. | ||||
| 1.1 Acupuncture versus Control | 2 | 464 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.59, 1.29] |
| 2 Ongoing Pregnancy Rate Show forest plot | 2 | 464 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.58, 1.26] |
| Analysis 1.2  Comparison 1 Acupuncture around the time of oocyte retrieval versus control (sham, placebo, no acupuncture), Outcome 2 Ongoing Pregnancy Rate. | ||||
| 2.1 Acupuncture versus Control | 2 | 464 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.58, 1.26] |
| 3 Clinical Pregnancy Rate Show forest plot | 6 | 912 | Odds Ratio (M‐H, Random, 95% CI) | 1.12 [0.78, 1.62] |
| Analysis 1.3  Comparison 1 Acupuncture around the time of oocyte retrieval versus control (sham, placebo, no acupuncture), Outcome 3 Clinical Pregnancy Rate. | ||||
| 3.1 Acupuncture versus Control | 6 | 912 | Odds Ratio (M‐H, Random, 95% CI) | 1.12 [0.78, 1.62] |
| 4 Miscarriage rate Show forest plot | 4 | 262 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.79 [0.42, 1.47] |
| Analysis 1.4  Comparison 1 Acupuncture around the time of oocyte retrieval versus control (sham, placebo, no acupuncture), Outcome 4 Miscarriage rate. | ||||
| 4.1 Acupuncture versus Control | 4 | 262 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.79 [0.42, 1.47] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Live Birth Show forest plot | 8 | 2505 | Odds Ratio (M‐H, Random, 95% CI) | 1.22 [0.87, 1.70] |
| Analysis 2.1  Comparison 2 Acupuncture on and around the day of ET versus control, Outcome 1 Live Birth. | ||||
| 1.1 Acupuncture versus Control (no sham/needling) | 3 | 849 | Odds Ratio (M‐H, Random, 95% CI) | 1.55 [1.14, 2.12] |
| 1.2 Acupuncture versus Control (sham/needling) | 5 | 1656 | Odds Ratio (M‐H, Random, 95% CI) | 1.03 [0.67, 1.58] |
| 2 Ongoing pregnancy Show forest plot | 10 | 2807 | Odds Ratio (M‐H, Random, 95% CI) | 1.10 [0.80, 1.52] |
| Analysis 2.2  Comparison 2 Acupuncture on and around the day of ET versus control, Outcome 2 Ongoing pregnancy. | ||||
| 2.1 Acupuncture versus Control (no sham/needling) | 4 | 924 | Odds Ratio (M‐H, Random, 95% CI) | 1.08 [0.57, 2.07] |
| 2.2 Acupuncture versus Control (sham/needling) | 6 | 1883 | Odds Ratio (M‐H, Random, 95% CI) | 1.10 [0.74, 1.65] |
| 3 Clinical pregnancy Show forest plot | 14 | 3632 | Odds Ratio (M‐H, Random, 95% CI) | 1.11 [0.87, 1.42] |
| Analysis 2.3 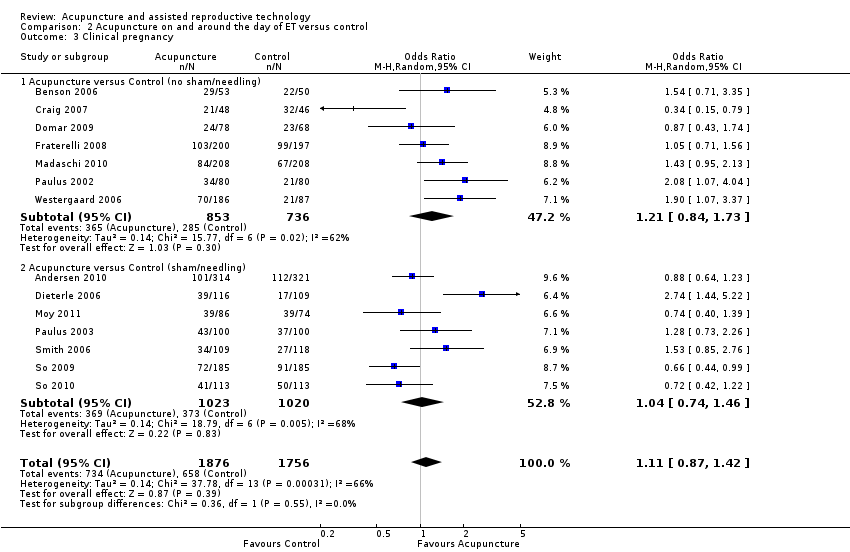 Comparison 2 Acupuncture on and around the day of ET versus control, Outcome 3 Clinical pregnancy. | ||||
| 3.1 Acupuncture versus Control (no sham/needling) | 7 | 1589 | Odds Ratio (M‐H, Random, 95% CI) | 1.21 [0.84, 1.73] |
| 3.2 Acupuncture versus Control (sham/needling) | 7 | 2043 | Odds Ratio (M‐H, Random, 95% CI) | 1.04 [0.74, 1.46] |
| 4 Miscarriage Show forest plot | 6 | 616 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.73, 1.67] |
| Analysis 2.4  Comparison 2 Acupuncture on and around the day of ET versus control, Outcome 4 Miscarriage. | ||||
| 4.1 Acupuncture versus Control (no sham/needling) | 2 | 245 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.20 [0.57, 2.49] |
| 4.2 Acupuncture versus Control (sham/needling) | 4 | 371 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.64, 1.76] |
| 5 Multiple gestation Show forest plot | 2 | 795 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.32 [0.74, 2.35] |
| Analysis 2.5  Comparison 2 Acupuncture on and around the day of ET versus control, Outcome 5 Multiple gestation. | ||||
| 5.1 Acupuncture versus Control (sham/needling) | 2 | 795 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.32 [0.74, 2.35] |

Study selection PRISMA flow diagram.

Methodological quality summary: review authors' judgements about each methodological quality item for each included study.

Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.

Forest plot of comparison: 1 Acupuncture around the time of oocyte retrieval versus control (sham, placebo, no acupuncture), outcome: 1.1 Live Birth Rate.

Forest plot of comparison: 1 Acupuncture around the time of oocyte retrieval versus control (sham, placebo, no acupuncture), outcome: 1.4 Miscarriage rate.

Forest plot of comparison: 2 Acupuncture on and around the day of ET versus control, outcome: 2.1 Live Birth.

Forest plot of comparison: 2 Acupuncture on and around the day of ET versus control, outcome: 2.4 Miscarriage.

Comparison 1 Acupuncture around the time of oocyte retrieval versus control (sham, placebo, no acupuncture), Outcome 1 Live Birth Rate.

Comparison 1 Acupuncture around the time of oocyte retrieval versus control (sham, placebo, no acupuncture), Outcome 2 Ongoing Pregnancy Rate.

Comparison 1 Acupuncture around the time of oocyte retrieval versus control (sham, placebo, no acupuncture), Outcome 3 Clinical Pregnancy Rate.

Comparison 1 Acupuncture around the time of oocyte retrieval versus control (sham, placebo, no acupuncture), Outcome 4 Miscarriage rate.

Comparison 2 Acupuncture on and around the day of ET versus control, Outcome 1 Live Birth.

Comparison 2 Acupuncture on and around the day of ET versus control, Outcome 2 Ongoing pregnancy.

Comparison 2 Acupuncture on and around the day of ET versus control, Outcome 3 Clinical pregnancy.

Comparison 2 Acupuncture on and around the day of ET versus control, Outcome 4 Miscarriage.

Comparison 2 Acupuncture on and around the day of ET versus control, Outcome 5 Multiple gestation.
| Acupuncture around the time of oocyte retrieval versus control (sham, placebo, no acupuncture) for women undergoing assisted reproductive technology (ART) | ||||||
| Population: women undergoing ART | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Acupuncture around the time of oocyte retrieval versus control (sham, placebo, no acupuncture) | |||||
| Live birth rate | 357 per 1000 | 326 per 1000 | OR 0.87 | 464 | ⊕⊕⊝⊝ | No significant difference in live birth rate was found between the two groups |
| *The basis for the assumed risk is the median control group risk across studies. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Neither study clearly reported method of random sequence generation, one did not clearly describe method of allocation concealment | ||||||
| Acupuncture on the day of embryo transfer (ET) versus control for women undergoing assisted reproductive technology (ART) | ||||||
| Population: women undergoing ART | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Acupuncture on the day of ET versus control | |||||
| Live birth rate | 281 per 1000 | 323 per 1000 | OR 1.22 | 2505 | ⊕⊕⊝⊝ | No significant difference in live birth rate was found between the two groups |
| *The basis for the assumed risk is the median control group risk across studies. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Two studies did not describe method of random sequence generation; six did not clearly describe method of allocation concealment | ||||||
| Acupuncture points | |||||||||||||||
| Cv6 (Qi Hai) | Y (before ET) | Y | |||||||||||||
| Cx6 (Neiguan) | Y | Y | Y | ||||||||||||
| DU 20 (bai hui) | Y | ||||||||||||||
| GV 20 (Baihui) | Y | Y (around ET and ET + 2) | Y | Y | Y | Y | Y | Y | Y | Y | Y | ||||
| Liv 2 (Xingjian) | |||||||||||||||
| Liv 3 (Taichong) | Y | Y | Y | Y | |||||||||||
| LI 4 (Hegu) | Y | Y ( ET + 2) | Y (ET + 3) | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | |
| LI 10 (Shoushanli) | Y | ||||||||||||||
| LR 3 (Taichong) | Y | Y | Y | Y | |||||||||||
| LU 7 (lieque) | Y | ||||||||||||||
| SP 6 (Sanyinjiao) | Y | Y ( ET + 2) | Y (ET + 3) | Y | Y | Y | Y | Y | Y | Y | Y | Y | |||
| SP 8 (Diji) | Y | Y | Y | Y | Y | Y | Y | Y | |||||||
| SP 10 (Xuehai) | Y | Y | Y | Y | Y | Y | Y | Y | |||||||
| ST28 | Y | ||||||||||||||
| ST29 (Guilai) | Y | Y (ET and ET + 2) | Y | Y | Y | Y | Y | Y | Y | Y | Y | ||||
| ST36 (Zushanli) | Y | Y (ET + 3) | Y | Y | Y | Y | Y | Y | Y | Y | Y | ||||
| PC6 (Neiguan) | Y | Y | Y | Y | |||||||||||
| Ren 3 (Zhongji) | Y (ET + 2) | ||||||||||||||
| RN 4 (Guanyuan) | Y | Y | |||||||||||||
| RN6 (Qihai) | Y | Y | |||||||||||||
| K3 (Tai Xi) | Y (after ET) | ||||||||||||||
| K13 (Taxiu) | Y (ET + 3) | ||||||||||||||
| K1 11(Henggu) | Y | Y | |||||||||||||
| TE 5 (Weiguan) | Y | ||||||||||||||
| EX‐CA 1 (Zigong) | Y |
| Acupuncture points | Intended treatment |
| Cx6 (Neiguan) | Location: 2 cun above the transverse crease of the wrist, between the tendons of muscle palmaris longus and muscle flexor radialis. |
| GV 20 (Baihui) | Location: on the midline of the head, 7 cun directly above the posterior hairline, approximately on the midpoint of the line connecting the apexes of the two auricles. |
| Liv 2 (Xingjian) | Location: on the dorsum of the foot between the 1st and 2nd toes, proximal to the margin of the web at the junction of the red and white skin. |
| Liv 3 (Taichong) | Location: on the dorsum of the foot in a depression distal to the junctions of the 1st and 2nd metatarsal bones. |
| LI 4 (Hegu) | Location: in the middle of the 2nd metacarpal bone on the radial side. |
| LI 10 (Shoushanli) | Location: 2 cm below LI 11 on the LI 5 to LI 11 line. Location: 2 cm below LI 11 on the LI 5 to LI 11 line. |
| SP 6 (Sanyinjiao) | Location: 3 cm directly above the tip of the medial malleolus on the posterior border of the tibia. |
| SP 8 (Diji) | Location: 3 cm below SP 9 on line connecting SP 9 and the tip of the medial malleolus. |
| SP 10 (Xuehai) | Location: with knee flexed, 2 cm above the superior medial border of the patella on the bulge of the medial portion of quadriceps femoris (vastus medialis). |
| ST29 (Guilai) | Location: 2 cm lateral to the AML level with CV 3. |
| ST36 (Zushanli) | Location: 3 cm below ST 35, one finger width lateral from the anterior border of the tibia. |
| PC6 (Neiguan) | Location: 2 cm above the wrist crease between the tendons of palmaris longus and flexor carpi radialis. |
| Ren 3 (Zhongji) | Location (zhongji): 1 cm superior to qugu. Regulates LR, warms KI, irregular menses. |
| RN 4 (Guanyuan) | Location: 1.5 cm lateral to the Du meridian, at the level of the lower border of the spinous process of the 5th lumbar vertebra. |
| RN6 (Qihai) | Location: 1.5 cm lateral to the Du meridian, at the level of the lower border of the spinous process of the third lumbar vertebra. |
| KI 3 (Taixi) | Location: in the depression between the medial malleolus and tendo calcaneus, at the level with the tip of the medial malleolus. |
| KI 11 (Henggu) | Location: 1.5 cm posterior to Wuchu (UB 5), 1.5 cm lateral to the Du meridian. |
| TE 5 (Weiguan) | Location: 1.5 cm lateral to the lower border of the spinous process of the eighth thoracic vertebra. |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Live Birth Rate Show forest plot | 2 | 464 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.59, 1.29] |
| 1.1 Acupuncture versus Control | 2 | 464 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.59, 1.29] |
| 2 Ongoing Pregnancy Rate Show forest plot | 2 | 464 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.58, 1.26] |
| 2.1 Acupuncture versus Control | 2 | 464 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.58, 1.26] |
| 3 Clinical Pregnancy Rate Show forest plot | 6 | 912 | Odds Ratio (M‐H, Random, 95% CI) | 1.12 [0.78, 1.62] |
| 3.1 Acupuncture versus Control | 6 | 912 | Odds Ratio (M‐H, Random, 95% CI) | 1.12 [0.78, 1.62] |
| 4 Miscarriage rate Show forest plot | 4 | 262 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.79 [0.42, 1.47] |
| 4.1 Acupuncture versus Control | 4 | 262 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.79 [0.42, 1.47] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Live Birth Show forest plot | 8 | 2505 | Odds Ratio (M‐H, Random, 95% CI) | 1.22 [0.87, 1.70] |
| 1.1 Acupuncture versus Control (no sham/needling) | 3 | 849 | Odds Ratio (M‐H, Random, 95% CI) | 1.55 [1.14, 2.12] |
| 1.2 Acupuncture versus Control (sham/needling) | 5 | 1656 | Odds Ratio (M‐H, Random, 95% CI) | 1.03 [0.67, 1.58] |
| 2 Ongoing pregnancy Show forest plot | 10 | 2807 | Odds Ratio (M‐H, Random, 95% CI) | 1.10 [0.80, 1.52] |
| 2.1 Acupuncture versus Control (no sham/needling) | 4 | 924 | Odds Ratio (M‐H, Random, 95% CI) | 1.08 [0.57, 2.07] |
| 2.2 Acupuncture versus Control (sham/needling) | 6 | 1883 | Odds Ratio (M‐H, Random, 95% CI) | 1.10 [0.74, 1.65] |
| 3 Clinical pregnancy Show forest plot | 14 | 3632 | Odds Ratio (M‐H, Random, 95% CI) | 1.11 [0.87, 1.42] |
| 3.1 Acupuncture versus Control (no sham/needling) | 7 | 1589 | Odds Ratio (M‐H, Random, 95% CI) | 1.21 [0.84, 1.73] |
| 3.2 Acupuncture versus Control (sham/needling) | 7 | 2043 | Odds Ratio (M‐H, Random, 95% CI) | 1.04 [0.74, 1.46] |
| 4 Miscarriage Show forest plot | 6 | 616 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.73, 1.67] |
| 4.1 Acupuncture versus Control (no sham/needling) | 2 | 245 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.20 [0.57, 2.49] |
| 4.2 Acupuncture versus Control (sham/needling) | 4 | 371 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.64, 1.76] |
| 5 Multiple gestation Show forest plot | 2 | 795 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.32 [0.74, 2.35] |
| 5.1 Acupuncture versus Control (sham/needling) | 2 | 795 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.32 [0.74, 2.35] |