Intervenciones con música para la ansiedad preoperatoria
Referencias
References to studies included in this review
References to studies excluded from this review
References to studies awaiting assessment
Additional references
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | Randomized controlled trial (RCT) 2‐arm parallel group design | |
| Participants | Adult ambulatory surgical patients scheduled for ophthalmic surgery Diagnosis: 2 patients with glaucoma; all others: cataract removal Total N randomized: 40 N randomized to music group: 20 N randomized to control group: 20 N analysed in music group: 20 N analysed in control group: 20 Mean age: 75.5 years Sex: 30 (75%) females, 10 (25%) males Ethnicity: Not reported Setting: outpatient Country: USA | |
| Interventions | Two study groups: 1. Music group: listening to pre‐recorded music through headphones 2. Control group: resting quietly, no music Music provided: participants selected from 22 types of music including soft hits, classical guitar, chamber music, folk music or popular singers from the 1940s and 1950s Number of sessions: 1 Length of sessions: Not reported Categorized as music medicine | |
| Outcomes | Systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR): post‐test scores in preoperative period Stress: not included in this review since this outcome was measured only at baseline and postoperatively Coping: not included in this review since this outcome was measured only at baseline and postoperatively | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Patients were sequentially selected from the patient rosters of two ophthalmic surgeons. Office assistants unaware of the study prepared patient rosters. On each day of data collection surgeons were randomly assigned to have their patients in the experimental or control group." |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | Low risk | This study used two subjective outcomes but these could not be included in this review because they did not pertain to preoperative anxiety. Therefore, a low risk of bias rating is given here. |
| Blinding of outcome assessment (detection bias) | Unclear risk | SBP, DBP and HR measurement were obtained by a Propaq Monitor and digitally recorded. It is unclear if the outcome assessor collecting the physiological responses was blinded. |
| Incomplete outcome data (attrition bias) | Low risk | No subject loss |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | This research was supported in part by a grant from the Food and Drug Administration (FD‐T‐ 000889). No conflicts of interest identified. |
| Methods | Controlled clinical trial (CCT) 2‐arm parallel group design | |
| Participants | Adult patients undergoing urogenital surgery Diagnosis: urinary tract problems (n = 48, 75%); genital tract problems (n = 16, 25%) Total N randomized: 64 N randomized to music group: 32 N randomized to control group: 32 N analysed in music group: 32 N analysed in control group: 32 Mean age: 43.29 years Sex: 0 (0%) females, 64 (100%) males Ethnicity: Turkish (no detailed ethnicity information is reported) Setting: inpatient Country: Turkey | |
| Interventions | Two study groups: 1. Music group: listening to preferred music through headphones plugged into a portable cassette player 2. Control group: standard care Music provided: participants selected from Turkish classical music, folk music, Turkish art music, or pop music Number of sessions: 1 Length of sessions: 30 minutes Categorized as music medicine | |
| Outcomes | State anxiety (Spielberger State‐Trait Anxiety Inventory ‐ State Anxiety form, STAI‐S): post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quote: "Random assignment was achieved based on the day that patients underwent surgery. Patients who underwent surgery on Monday or Wednesday were assigned to the control group while patients who had their surgery on Tuesday or Thursday were assigned to the experimental group." |
| Allocation concealment (selection bias) | High risk | Alternate assignment prohibited allocation concealment |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measures were used for subjective outcomes |
| Blinding of outcome assessment (detection bias) | Low risk | This study did not address objective outcomes |
| Incomplete outcome data (attrition bias) | Low risk | There was no subject loss |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | CCT 2‐arm parallel group design | |
| Participants | Adult patients scheduled for ambulatory surgery Type of surgery: arthroscopy (n = 12, 26%), herniorrhaphy (n = 8, 17%), orthopedic procedure (n = 6, 13%), urologic procedures (n = 5, 11%), nerve repairs (n = 4, 9%), endoscopic procedure (n = 3, 6%), laparoscopic procedures (n = 2, 4%), and breast biopsies (n = 2, 4%) Total N randomized: 42 N randomized to music group: 21 N randomized to control group: 21 N analysed in music group: 21 N analysed in control group: 21 Mean age: 47 Sex: 17 (40%) females, 25 (60%) males Ethnicity: 100% Caucasian Setting: inpatient Country: USA | |
| Interventions | Two study groups: 1. Music group: preoperative instruction coupled with music listening 2. Control group: routine preoperative instruction Music provided: participants selected from classical, environmental, new age, western country, or general easy‐listening music Number of sessions: 1 Length of sessions: 15‐30 minutes Categorized as music medicine | |
| Outcomes | Anxiety (STAI‐S): change score HR, respiratory rate (RR), SBP, DBP: post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quote: "When patients agreed to participate, we obtained their written informed consents and alternately assigned them to either the experimental or control group." |
| Allocation concealment (selection bias) | High risk | Alternate assignment prohibited allocation concealment |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded (personal communication with chief investigator) |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measures were used for subjective outcomes |
| Blinding of outcome assessment (detection bias) | High risk | The outcome assessors were not blinded (personal communication with chief investigator) |
| Incomplete outcome data (attrition bias) | Low risk | There was no subject loss (personal communication with chief investigator) |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Adults patients scheduled for an elective day or short‐stay surgery Type of surgery: laparotomy, hip replacement, laparoscopy, ventral hernia repair, inguinal hernia repair, arthroscopy, varicose vein, scrotal or vaginal surgery (number of participants per diagnosis not reported) Total N randomized: 372 N randomized to music group: 190 N randomized to control group: 182 N analysed in music group: 177 N analysed in control group: 150 Mean age: 50 years Sex: 198 (53%) females, 138 (47%) males Ethnicity: not reported Setting: inpatient Country: Sweden | |
| Interventions | Two study groups: 1. Music group: listening to pre‐recorded music. Patients in the music group did not receive pre‐medication midazolam solution. 2. Control group: standard pre‐medication midazolam solution orally Music provided: participants selected from classical, soft pop/film, soft jazz, nature sound, or instrumental music. CDs were compiled by a professional music therapist. Number of sessions: 1 Length of sessions: 17‐42 minutes Categorized as music medicine | |
| Outcomes | Anxiety (STAI‐S): post‐test score HR, SBP, DBP, arterial pressure (AP): post‐test scores | |
| Notes | Even though a professional music therapist helped with the selection of the music for this study, this study is categorized as a music medicine study because the patients listened to pre‐recorded music without the presence of a therapeutic process with the music therapist. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The music therapist randomized the patients through sealed envelopes immediately before the intervention" |
| Allocation concealment (selection bias) | Low risk | Quote: "[the music therapist] drew the first envelope in a row of previously randomly mixed envelopes consisting of an equal number of both allocations." |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measures were used for subjective outcomes |
| Blinding of outcome assessment (detection bias) | High risk | The music therapist recorded the blood pressure and heart rate using a Riester fully automatic digital blood pressure monitor before and after the intervention. The music therapist was not blinded. |
| Incomplete outcome data (attrition bias) | Low risk | Attrition 12%: 13 patients were excluded from experimental group due to logistic reasons (n = 12) and other reason (n = 1), and 23 patients were excluded from the control group due to logistic reasons (n = 19), and not receiving midazolam (n = 4). Quote: "The reasons for exclusion were logistic in the majority of cases, mainly due to a too early call to the operating room, which had the effect that the time between the intervention and the evaluation was too short. Hence, 177 patients in the music group and 159 in the midazolam group went through the study protocol; however, nine patients in the midazolam group were too sedated to be able to complete the second STAI X‐1." |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Adult patients scheduled for elective surgery Type of surgery: no details reported Total N randomized: 32 N randomized to music group: 16 N randomized to control group: 16 N analysed in music group: 16 N analysed in control group: 16 Mean age: 41.5 Sex: 21 (65.6%) females, 11 (34.4%) males Ethnicity: Not reported Setting: Outpatient Country: USA | |
| Interventions | Two study groups: 1. Music group: listening to pre‐recorded music 2. Control group: standard care Music provided: Participants were asked to bring the music of their choice from home Number of sessions: 1 Length of sessions: 15 minutes Categorized as music medicine | |
| Outcomes | Anxiety (STAI‐S): post‐test scores RR, pulse, SBP, DBP: post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quote: "The first patients was assigned to control group or intervention group by a coin toss. Each subsequent subject was assigned alternately to the control group or intervention group" |
| Allocation concealment (selection bias) | High risk | Alternate assignment prohibited allocation concealment |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measures were used for subjective outcomes |
| Blinding of outcome assessment (detection bias) | High risk | The researcher measured the pulse, respiration and blood pressure and was not blinded. |
| Incomplete outcome data (attrition bias) | Low risk | No subject loss |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Adult patients scheduled for surgery Type of surgery: open heart surgery including coronary artery bypass graft surgery (CABG) (n = 17, 27%) , valvular surgery (n = 33, 53%), and other (n = 12, 19%) Total N randomized: 62 N randomized to music group: 32 N randomized to control group: 30 N analysed in music group: 32 N analysed in control group: 30 Mean age: 51.8 Sex: 29 (47%) females, 33 (53%) males Ethnicity: not reported; most participants likely Taiwanese Setting: Inpatient Country: Taiwan | |
| Interventions | Two study groups: 1. Music group: listening to pre‐recorded music 2. Control group: resting Music provided: music with 60‐72 beats per minute with bass tone and soft melody or religious music in a variety of languages including Chinese, Taiwanese, English and Japanese Number of sessions: 1 Length of sessions: 20 minutes Categorized as music medicine | |
| Outcomes | Anxiety (VAS): post‐test scores HR, RR, SBP, DBP, pain, skin temperature: change scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measure was used for this study |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) | Low risk | There was no subject loss |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | RCT 3‐arm parallel group design | |
| Participants | Adult patients scheduled for day surgery Type of surgery: orthopaedic (n = 57, 32%), skin (n = 58,32%), breast (n = 15, 8%), urology (n = 24, 13%), general (n = 15, 8%), other (n = 11, 6%) Total N randomized: 180 (120 included in this review) N randomized to music group: 60 N randomized to control group: 60 N randomized to placebo group: 60 (not included in this review) N analysed in music group: 60 N analysed in control group: 60 N analysed in placebo group: 60 (not included in this review) Mean age: 55.7 years Sex: 90 (50%) females, 90 (50%) males Ethnicity: Not reported Setting: Outpatient Country: USA | |
| Interventions | Three study groups: 1. Music group: listening to pre‐recorded music 2. Control group: standard nursing care 3. Placebo group: Wore headphones for 30 minutes with no sound. Music provided: patient‐selected pre‐recorded CD from one of the following genres, classical, jazz, country and western, new age, or easy‐listening Number of sessions: 1 Length of sessions: 30 minutes Categorized as music medicine | |
| Outcomes | Anxiety (STAI‐S): post‐test scores | |
| Notes | Standard deviations (SDs) are not reported in the research report but we were able to obtain the values from the investigator | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "A computer‐generated list was used for permuted block random assignment to intervention, placebo or control groups by gender. That is, males and females were randomized separately so that equal numbers of each were assured in each group" |
| Allocation concealment (selection bias) | Low risk | Quote: "A biostatistician and research assistant who did not participate in data collection conducted the randomization procedures and prepared sequentially numbered sealed envelopes containing the random assignment for each consenting patient." |
| Blinding of participants and personnel (performance bias) | Low risk | Blinding of participants was not possible. The nurses who provided care were blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measure was used for the subjective outcomes |
| Blinding of outcome assessment (detection bias) | Low risk | The study did not address objective outcomes |
| Incomplete outcome data (attrition bias) | Low risk | There was no subject loss |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases. This research was supported by funding received from the Griffith University New Researcher Grant Scheme |
| Methods | CCT 2‐arm parallel group design | |
| Participants | Adult patients undergoing elective cosmetic surgery Type of surgery: cosmetic surgery (no further details reported) Total N randomized: 38 N randomized to music group: 19 N randomized to control group: 19 N analysed in music group: 14 N analysed in control group:12 Mean age: 46.35 Sex: 24 (96%) females, 2 (4%) males Ethnicity: Not reported Setting: Outpatient Country: USA | |
| Interventions | Two study groups: 1. Music group: listening to prerecorded music via headphones 2. Control group: standard care Music provided: CD selected by a music therapist: "Music for Unwinding". Music was composed by J Nagler, music therapist. The music style was identified as New Age Number of sessions: 1 Length of sessions: 20 minutes Categorized as music medicine | |
| Outcomes | STAI: change scores HR, SBP: change scores | |
| Notes | Even though a music therapist was involved with the music selection, the authors specifically state that this study did not use a music therapy intervention | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | "Patients were randomized based on the day of their surgery using alternating placement in the control and experimental groups" |
| Allocation concealment (selection bias) | High risk | Alternate assignment prohibited allocation concealment |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measure was used for the subjective outcomes |
| Blinding of outcome assessment (detection bias) | High risk | Outcome assessor was not blinded |
| Incomplete outcome data (attrition bias) | High risk | Large subject loss: 32% (n = 12). Subject withdrawals are reported as follows: 38 participants consented and 26 completed all study requirements. Reasons for withdrawal included "patients cancelled the procedures, were taken into surgery early with no adequate time to complete all study requirements" |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No conflict of interest statement was reported |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Patients undergoing surgery under general anaesthesia Type of surgery: endoscopic cholecystectomy (n = 16, 67% ), endoscopic henorrhapsy (n = 7, 29% ), endoscopic appendectomy (n = 1, 4%) Total N randomized: 24 N randomized to music group: 18 N randomized to control group: 6 N analysed in music group: 18 N analysed in control group: 6 Mean age: 48.1 Sex: 14 (58%) females, 10 (42%) males Ethnicity: Not reported Setting: Inpatient Country: USA | |
| Interventions | Two study groups: 1. Music group: listening to pre‐recorded music 2. Control group: receiving verbal reassurance Music provided: Participants selected from a variety of "easy listening" music that the medical staff had recorded. Number of sessions:1 Length of sessions: 20 minutes Categorized as music medicine | |
| Outcomes | Anxiety (STAI, Visual Analogue Anxiety Scale (VAAS)): could not be included in this review (see notes) SBP, DBP, HR: post‐test scores | |
| Notes | State anxiety was measured before the music intervention, but not immediately after the music intervention. The post‐test was administered after the surgery. Therefore, this data could not be included. VAAS was administered before and immediately after the music intervention. However, because of insufficient data reporting, this outcome could not be included in this review | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quotes: "The first 2 patients were assigned to the experimental group, and the third patient to the control group. This pattern was continued until 24 patients were enrolled." |
| Allocation concealment (selection bias) | High risk | Alternate assignment prohibited allocation concealment |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measures were used for the subjective outcomes |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | RCT 3‐arm parallel group design | |
| Participants | Adult patients scheduled for surgical procedures Type of surgery: general, orthopedic, gynaecologic, ophthalmic, otolaryngologic, and dental surgery (number of participants per type of surgery not specified) Total N randomized:46 (31 included in this review) N randomized to music group: 16 N randomized to humorous distraction group: 15 (not included in this review) N randomized to control group: 15 N analysed in music group: 16 N analysed in humorous distraction group:15 (not included in this review) N analysed in control group: 15 Mean age: 47.07 Sex: 27 (59%) females, 19 (41%) males Ethnicity: Not reported Setting: Inpatient Country: USA | |
| Interventions | Three study groups: 1. Music group: listening to pre‐recorded music 2. Humorous distraction group: listening to a humorous tape 3. Control group: received no auditory distraction during the waiting period Music provided: An audiotape of slow, quiet, instrumental music (e.g., Omni Suite by Steven Bergman) Number of sessions: 1 Length of sessions: 20 minutes Categorized as music medicine | |
| Outcomes | Anxiety (VAS): post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Each research assistant randomly assigned subjects by lottery to one of three groups" |
| Allocation concealment (selection bias) | Low risk | Draw by lots ensured allocation concealment |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measure was used for this study |
| Blinding of outcome assessment (detection bias) | Low risk | This study did not address objective outcomes |
| Incomplete outcome data (attrition bias) | Low risk | There was no subject loss |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases. This study was supported by an AORN Nurse Scientist Grant and a Duquesne University, Pittsburgh, Supplemental Faculty Development Grant. |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Adult patients scheduled for surgical procedures Type of surgery: septorhinoplastic surgery Total N randomized:54 N randomized to music group: 28 N randomized to control group: 26 N analysed in music group: 25 N analysed in control group: 25 Mean age: 30 Sex: 21 (42%) females, 29 (58%) males Ethnicity: Not reported Setting: Inpatient Country: Turkey | |
| Interventions | Two study groups: 1. Music group: listening to pre‐recorded music through headphone 2. Control group: listening to a blank cassette or CD through headphone Music provided: Patients brought their own music Number of sessions: 1 Length of sessions: 50 minutes Categorized as music medicine | |
| Outcomes | Anxiety (Observer’s Assessment of Alertness/Sedation Scales, Bispectral Index): post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “they were assigned using a table of random numbers, to receive either music (music group) or no music (control group)" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) | Low risk | Blinding of participants was not possible. Personnel were blinded |
| Blinding of outcome assessment (detection bias) | Low risk | This study did not address any subjective outcomes |
| Blinding of outcome assessment (detection bias) | Low risk | The outcome assessors were blinded |
| Incomplete outcome data (attrition bias) | Low risk | Attrition rate: 7 %(n = 4). Three patients from the music group and one patient from the control group were excluded from the study because of technical problems related to the music player. |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Adults patients scheduled for laparoscopic surgery Type of surgery: laparoscopic surgery Total N randomized: 93 N randomized to music group: 48 N randomized to control group: 45 N analysed in music group: 48 N analysed in control group: 45 Mean age: 40.80 Sex: 54 (58%) females, 39 (42%) males Ethnicity: Not reported Setting: Not reported Country: China | |
| Interventions | Two study groups: 1. Music group: listening to preferred music through headphone 2. Control group: wearing headphone without music Music provided: participants selected from six types of pre‐recorded music (classical music, light music, pop music, folk music, folk songs, and opera). Number of sessions: 1 Length of sessions: 30 minutes Categorized as music medicine | |
| Outcomes | Anxiety (STAI): post‐test score HR, SBP, DBP, skin conductivity response, salivary cortisol: post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated list of numbers |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) | Low risk | Participants could not be blinded. Personnel were blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measures were used for the subjective outcomes |
| Blinding of outcome assessment (detection bias) | Low risk | Outcome assessors were blinded by use of headphones in the control group |
| Incomplete outcome data (attrition bias) | Low risk | Attrition rate: 7% (n = 7). Seven patients were excluded due to changing surgery, refusing to continue the study and environmental interference. Exact number of subject loss from each group is not reported |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Adult patients undergoing surgery Type of surgery: Not specified Total N randomized: 108 N randomized to music group: 54 N randomized to control group: 54 N analysed in music group: 51 N analysed in control group: 51 Mean age: 40.3 Sex: 108 (100%) females, 0 males Ethnicity: 100% Malaysian Setting: Inpatient Country: Malaysia | |
| Interventions | Two study groups: 1. Music group: listening to pre‐recorded music 2. Control group: standard care Music provided: Participants selected from Western, Malay or Chinese music that the medical staff had recorded. All music has a tempo of 60‐80 bpm Number of sessions: 8 Length of sessions: 30 minutes Categorized as music medicine | |
| Outcomes | Anxiety (STAI, Visual Analogue Scale for Anxiety (VASA)): Only VASA post‐test scores are included in this review (see notes) | |
| Notes | Both VASA and STAI were used to measure anxiety. But STAI post‐test scores were obtained after the surgery. VASA data were obtained at the start and the end of the music intervention prior to surgery. Therefore, only VASA data are used in this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “Subjects were randomly assigned, using the “envelope method,” to either the music therapy group or the control group” |
| Allocation concealment (selection bias) | Low risk | Use of sealed envelopes |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measures were used for the subjective outcomes |
| Blinding of outcome assessment (detection bias) | Low risk | This study did not address objective outcomes |
| Incomplete outcome data (attrition bias) | Low risk | Attrition rate: 6% (n = 6) The reasons for the subject loss were not reported. |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases. This study was supported by Prince of Songkla University, Thailand. |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Adult women undergoing elective cesarean section because of medical reasons Type of surgery: caesarean section Total N randomized: 62 N randomized to music group: 30 N randomized to control group: 32 N analysed in music group: 28 N analysed in control group: 30 Mean age: 32.1 Sex: 60 (100%) females, 0 males Ethnicity: not reported Setting: Inpatient Country: Israel | |
| Interventions | Two study groups: 1. Music group: listening to pre‐recorded music 2. Control group: bedrest with no music Music provided: Participants selected from three options: light popular music, light classical music, Israeli songs Number of sessions: 1 Length of sessions: 40 minutes Categorized as music medicine | |
| Outcomes | Positive mood, negative mood, perceived threat of surgery: not used in this study HR, SBP, DBP: post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "The researchers preprepared sealed envelopes, each containing a card with either "yes" or "no" in equal numbers. Each woman chose a sealed envelope. the women who had the yes card were included in the experimental group, those who had no were included in the control group". |
| Allocation concealment (selection bias) | Low risk | Participants were asked to draw and open a sealed envelope |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measure was used |
| Blinding of outcome assessment (detection bias) | High risk | The outcome assessor was not blinded |
| Incomplete outcome data (attrition bias) | Low risk | Two participants were excluded because of their music selection. Because these two participants were the only ones who selected popular music, the researchers decided to exclude them because analysis per music selection would not be possible with such a small subgroup. |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | CCT 2‐arm parallel group design | |
| Participants | Adults undergoing surgery Type of surgery: cystoscopy, cauterisation or endoscopy Total N randomized: 113 N randomized to music group: 58 N randomized to control group: 55 N analysed in music group: 58 N analysed in control group: 55 Mean age: 51 Sex: 55 (49%) females, 58 (51%) males Ethnicity: 100% Hong Kong Chinese Setting: inpatient Country: China | |
| Interventions | Two study groups: 1. Music group: listening to pre‐recorded music 2. Control group: participating in the usual pre‐procedural relaxing activities (e.g., reading or watching television) in the waiting rooms Music provided: participants selected from eastern and western style easy listening music or Chinese pop music Number of sessions: 1 Length of sessions: 20‐40 minutes Categorized as music medicine | |
| Outcomes | Anxiety (STAI): post‐test scores RR, pulse, SBP, DBP: post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quote: "Patients who had their procedure on Wednesday were assigned to the control group and patients who had their procedure on Thursday were assigned to the music group" |
| Allocation concealment (selection bias) | High risk | Alternate assignment prohibited allocation concealment |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measures were used for the subjective outcomes |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases. The study was supported by the Lee Hysan Foundation and grant from Chinese University of Hong Kong |
| Methods | RCT 3‐arm parallel group design | |
| Participants | Adults undergoing surgery Type of surgery: orthopaedics (n = 23, 14%), general (n = 29, 17%), gynaecology (n = 44, 26%), urology (n = 16, 10%), neurosurgery (n = 20, 12%), other (n = 35, 21%) Total N randomized: 180 N randomized to music (headphone) group: 56 N randomized to music (broadcast) group: 66 N randomized to control group: 58 N analysed in music (headphone) group: 48 N analysed in music (broadcast) group: 66 (not used in this study) N analysed in control group: 53 Mean age: 49.36 Sex: 28 (55%) females, 23 (45%) males Ethnicity: not reported; it is likely that the majority of the participants were Taiwanese Setting: inpatient Country: Taiwan | |
| Interventions | Three study groups: 1. Headphone group: Listening to music through headphone for 10 minutes 2. Broadcast group: Listening to music from an open speaker for 10 minutes 3. Control group: participants were told to rest and relax Music provided: Folk songs or pop music, played at a tempo of 60–80 beats per minute and a volume of 50–55 db Number of sessions: 1 Length of sessions: 10 minutes Categorized as music medicine | |
| Outcomes | Anxiety (Numeric rating scale (NRS): post‐test scores HR and heart rate variability (HRV) (CheckMyHeart handheld HRV device): post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random block sampling. Quote: "We applied random table to divide numbers 1–30 to three groups to determine each day of a month to be ‘headphone day,’ ‘broadcast day’ or ‘control day’" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measure was used to assess the subjective outcome |
| Blinding of outcome assessment (detection bias) | High risk | Outcome assessors were not blinded |
| Incomplete outcome data (attrition bias) | Low risk | Attrition rate 7% (n = 13). Eight patients from the experimental group were excluded due to HRV data incomplete or too much noise (n = 2), being sent to surgery before the end of measurement (n = 3), or refusing to take the measure (n = 3). Five patients from the control group were excluded due to HRV data were incomplete (n = 2) or being sent to surgery before the end of measurement (n = 3). |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Adults undergoing surgery Type of surgery: Gynaecology (n = 41, 25%), orthopaedics (n = 29, 18%), general (n = 14, 8%), urology (n = 12, 7%), neurosurgery (n = 16, 10%), other (n = 25, 16%) Total N randomized: 161 N randomized to music group: 82 N randomized to control group: 79 N analysed in music group: 76 N analysed in control group: 64 Mean age: 49.63 Sex: 70 (50%) females, 70 (50%) males Ethnicity: Not reported Setting: inpatient Country: Taiwan | |
| Interventions | Two study groups: 1. Music group: listening to10‐min session of music through headphones 2. Control group: receiving the VAS and HR measurements by the researcher at a 10‐min interval without a music intervention. Music provided: Patients selected from five kinds of music (folk songs or pop music), played at a tempo of 60–80 beats per minute and a volume of 50–55 db Number of sessions: 1 Length of sessions: 10 minutes Categorized as music medicine | |
| Outcomes | Anxiety (NRS): post‐test scores HR, HRV (CheckMyHeart): post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quote: “We assigned participants to groups using birthdays, placing those with even birth dates in the experimental group and those with odd birth dates in the control group.” |
| Allocation concealment (selection bias) | High risk | Systematic form of group allocation based on date of birth prevented allocation concealment |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measure was used to assess the subjective outcome |
| Blinding of outcome assessment (detection bias) | Unclear risk | HR measurement were obtained by CheckMyHeart HRV device. Unclear if outcome assessor was blinded |
| Incomplete outcome data (attrition bias) | Low risk | Attrition rate: 12% (n = 19). Six patients from the experimental group were excluded due to HRV data incomplete or too much noise (n = 4), or being sent to surgery before the end of measurement (n = 2). Thirteen patients from the control group were excluded due to HRV data incomplete or too much noise (n = 7), being sent to surgery before the end of measurement (n = 4), or refusing to take the measure (n = 2). |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases. There was no external financial support for this research |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Adult patients undergoing surgery Diagnosis: gastric cancer Total N randomized: 60 N randomized to music group: 30 N randomized to control group: 30 N analysed in music group: 30 N analysed in control group: 30 Mean age: Not reported Sex: 23(38%) females, 37 (62%) males Ethnicity: Not reported Setting: Inpatient Country: China | |
| Interventions | Two study groups: 1. Music group: listening to pre‐recorded music 2. Control group: receiving verbal support (explanation, guidance, encouragement and comfort) Music provided: Researcher‐selected Chinese classical music Number of sessions: 8 Length of sessions: 20‐30 minutes Categorized as music medicine | |
| Outcomes | Anxiety (Zung Self‐Rating Anxiety Scale (SAS)): post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) | Unclear risk | Blinding of participants was not possible. Blinding of personnel was not reported |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measure was used to assess the subjective outcome |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) | Low risk | There was no subject loss |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Adults undergoing surgery Type of surgery: Spinal surgery Total N randomized: 60 N randomized to music group: 30 N randomized to control group: 30 N analysed in music group: 30 N analysed in control group: 30 Mean age: 62.18 Sex: 29 (49.3%) females, 31 (51.7%) males Ethnicity: Not reported Setting: Inpatient Country: Taiwan | |
| Interventions | Two study groups: 1. Music group: listening to preferred music through headphones 2. Control group: resting in bed undisturbed while the environment was kept quiet Music provided: Patients selected preferred music from Chinese pop music, classical music, nature sounds and sacred music that researchers provided. All music has a tempo between 6‐ and 72 beats per minute. Number of sessions: 4 sessions with measurements before and after each music session (evening before surgery, one hour before surgery, afternoon of first post‐operative day, and second post‐operative days). We used the one hour pre‐op time point for this review. Length of sessions: 30 minutes Categorized as music medicine | |
| Outcomes | Anxiety (VAS): post‐test score Pulse, DBP, SBP: post‐test score | |
| Notes | Both STAI and VAS were used to measure anxiety but only VAS data are used because the STAI post‐test was administered after the surgery. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quote: "All patients scheduled for surgery on Tuesdays and Thursdays were assigned to the study group, while those scheduled for surgery on Wednesdays and Fridays were assigned to the control group." |
| Allocation concealment (selection bias) | High risk | Systematic form of group allocation prevented allocation concealment |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measure was used for the subjective outcome |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) | Low risk | There was no subject loss |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases. This study was financially sponsored by the Taipei Veterans General Hospital (Grant No.V95B2‐004). |
| Methods | CCT 2‐arm parallel group design | |
| Participants | Adult patients awaiting non‐orthopaedic surgeries Diagnosis: Laryngological surgery (n = 79, 79%), varicectomy (n = 21, 21%) Total N randomized: 100 N randomized to music group: 50 N randomized to control group: 50 N analysed in music group: 50 N analysed in control group: 50 Mean age: range between 20‐60 Sex: 28 (28%) females, 72 (72%) males Ethnicity: Not reported Setting: Inpatient Country: Poland | |
| Interventions | Two study groups: 1. Music group: listening to individually composed music programs from Walkman‐type tape players. 2. Control group: standard care Music provided: Not reported Number of sessions: 1 Length of sessions: 1 hour Categorized as music medicine | |
| Outcomes | SBP, DBP, HR, cardiac output, stroke volume, temperature, and glucose count: only percentage change scores are reported. These cannot be combined with post‐test/change scores in the meta‐analysis and therefore results are only presented in the narrative. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomization method is not reported. Quote: "Subjects were randomly assigned to either group C or Group M" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | Low risk | This study did not address any subjective outcomes |
| Blinding of outcome assessment (detection bias) | Unclear risk | Outcomes were measured with electronic equipment. It is unclear if outcome assessors were blinded |
| Incomplete outcome data (attrition bias) | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | CCT 2‐arm parallel group design | |
| Participants | Patients awaiting for the crural varicectomy or laryngological surgeries Type of surgery: crural varicectomy (n = 19, 21%) or laryngological surgery (n = 70, 79%) Total N randomized: 89 N randomized to music group: 45 N randomized to control group: 44 N analysed in music group: 45 N analysed in control group: 44 Mean age: 40 Sex: 27 (30%) females, 62 (70%) males Ethnicity: Not reported Setting: Inpatient Country: Poland | |
| Interventions | Two study groups: 1. Music group: listening to the music for 60 minutes 2. Control group: standard care Music provided: Not reported Number of sessions: 1 Length of sessions: 60 minutes Categorized as music medicine | |
| Outcomes | Anxiety (STAI): post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomization method was not reported. Quote: "Patients were allotted to groups at random" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measures were used for the subjective outcomes |
| Blinding of outcome assessment (detection bias) | Low risk | This study does not address objective outcomes |
| Incomplete outcome data (attrition bias) | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Adult patients admitted to outpatient surgery Type of surgery: neurosurgery (n = 29, 17%), obstetrics and gynaecology (n = 32, 7%), general clinic (n = 19, 11.1%), ear ‐ nose ‐ throat (n = 13, 7.6%), urology (n = 14, 8.2%), plastic surgery (n = 61, 35.7%), cardiovascular (n = 3, 1.8%) Total N randomized: 174 N randomized to music group: 87 N randomized to control group: 87 N analysed in music group: 86 N analysed in control group: 86 Mean age: 40.9 (11.8) Sex: 112 (65%) females, 60 (35%) males Ethnicity: Not reported Setting: Outpatient Country: Taiwan | |
| Interventions | Two study groups: 1. Music group: listening to the music for 20 minutes via headphones 2. Control group: standard care Music provided: Investigator‐selected mini library of soothing popular Chinese and Taiwanese pop songs (low‐tone, slow rhythm ballads only). Participants selected music from this library Number of sessions: 1 Length of sessions: 20 minutes Categorized as music medicine | |
| Outcomes | STAI: change scores HR, SBP, DBP: change scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "computer‐generated permuted block randomization was used to assign participants to either experimental or control group" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measures were used for the subjective outcomes |
| Blinding of outcome assessment (detection bias) | High risk | Outcome assessor was not blinded |
| Incomplete outcome data (attrition bias) | Low risk | Authors reported two withdrawals |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | CCT 2‐arm parallel group design | |
| Participants | Adult patients awaiting elective inpatient surgery Diagnosis: Not reported Total N randomized:12 N randomized to music group: 6 N randomized to control group: 6 N analysed in music group: 6 N analysed in control group: 3 Mean age: 58 Sex: Not reported Ethnicity: Not reported Setting: Inpatient Country: Hong Kong | |
| Interventions | Two study groups: 1. Music group: listening to self‐selected music for 20 minutes 2. Control group: standard care Music provided: participants selected from slow rhythmical songs: Chinese or Western music. This music was determined to have sedative qualities by a panel of experts Number of sessions: 1 Length of sessions: 20 minutes Categorized as music medicine | |
| Outcomes | Anxiety (Chinese version STAI): change scores Tension (Subjective Unit of Tension Scale): change scores SBP, DBP: change scores | |
| Notes | JB computed change scores because of large pre‐test differences | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measures were used for subjective outcomes |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) | High risk | Attrition rate: 33% (n = 3). Three patients from the control group could not complete the procedure, as they had to be sent to surgery |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | RCT 2‐arm parallel group design | |
| Participants | Women undergoing elective gynaecological procedures Types of surgery: exploratory laparoscopies, laparoscopic tubal ligation, ovarian cysts excision, and intrauterine device removal Total N randomized: 50 N randomized to music group: 31 N randomized to control group: 19 N analysed in music group: 31 N analysed in control group: 19 Mean age: 37 Sex: 50 (100%) females, 0 (0%) males Ethnicity: Not reported Setting: Outpatient Country: USA | |
| Interventions | Two study groups: 1. Music group: listening to music through headphones 2. Control group: standard care Music provided: Participants were asked to select from Schumann: Quartet for Piano and Strings in E‐Flat Major, Tchaikovsky: Symphony No. 6 in B minor (“Pathetique”), Beethoven: Symphony No. 2 in D Major (op. 36), Johnny Cash’s Greatest Hits, Willie Nelson’s Greatest Hits, The Beatles Part I, The Beatles Part II, Benny Goodman: Small Group 1941‐1945, Johnny Mathis: Better Together, Madonna: True Blue. The Temptations: 26th Anniversary, or The Mamas & The Papas: If You Can Believe Your Eyes Number of sessions: 1 Length of sessions: 50 minutes Categorized as music medicine | |
| Outcomes | Anxiety (STAI‐S): change scores HR, SBP, DBP: change scores | |
| Notes | JB computed change scores and SD | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated list of random numbers |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measures were used for subjective outcomes |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) | Low risk | There was no subject loss. |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | CCT 2‐arm parallel group design | |
| Participants | Chinese male surgical patients in an acute general hospital waiting to undergo inpatient surgery for transurethral resection of the prostate (TURP) Total N randomized: 30 (20 included in this review) N randomized to music group: 10 N randomized to nurse present group: 10 (not included in review) N randomized to control group: 10 N analysed in music group: 10 N analysed in nurse present group: 10 (not included in review) N analysed in control group: 10 Mean age: 67.67 Sex: 0 (0%) females, 30 (100%) males Ethnicity: 100% Chinese Setting: Inpatient Country: Hong Kong | |
| Interventions | Three study groups: 1. Music group: listening to slow rhythm soft music via headphones 2. Nurse present group: A nurse stood with the patients while they were waiting in the holding area. The nurse was present, but there was minimal verbal interaction 3. Control group: No music intervention or nurse present Music provided: participants selected from slow rhythm songs, Chinese slow rhythm songs or Western slow rhythm songs Number of sessions: 1 Length of sessions: 20 minutes Categorized as music medicine | |
| Outcomes | Anxiety (Chinese version STAI): change scores HR, SBP, DBP: change scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "The subjects were randomly allocated to different conditions." |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) | High risk | Blinding of participants was not possible. Personnel were not blinded |
| Blinding of outcome assessment (detection bias) | High risk | Self‐report measure was used for subjective outcome. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) | Low risk | There was no subject loss |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
| Methods | CCT 2‐arm parallel group design | |
| Participants | Patient awaiting urological surgery Type of surgery: TURP; Transurethral resection of the bladder (TURB); Cystolithotripsy; Herniorrhaphy; Laparoscopic cholecystectomy Total N randomized: 66 N randomized to music group: 33 N randomized to control group: 33 N analysed in music group: 33 N analysed in control group: 33 Mean age: 64.68 Sex: 0 (0%) females, 60 (100%) males Ethnicity: 100% Chinese Setting: Inpatient Country: Hong Kong | |
| Interventions | Two study groups: 1. Music group: listening to music through headphones 2. Control group: standard care Music provided: Participants were given choice of 3 tapes approved by panel of 3 music instructors at the university level. The panel agreed that the music was sedative in that it possessed minimal rhythmic characteristics. Choices included: Chinese instrumental music, Western instrumental music, or Western and Chinese slow songs Number of sessions: 1 Length of sessions: 20 minutes Categorized as music medicine | |
| Outcomes | Anxiety (Chinese version STAI): post‐test scores HR, RR, AP: post‐test scores | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were matched by type of operation into a music treatment group or a test control group." |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) | Unclear risk | The participants were not blinded. It is unknown whether the personnel were blinded |
| Blinding of outcome assessment (detection bias) | High risk | A self‐report measure was used to measure the subjective outcome |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) | Low risk | There was no subject loss |
| Selective reporting (reporting bias) | Low risk | No indication of selective reporting |
| Other bias | Low risk | No indication of other biases |
Key to abbreviations:
AP ‐ Arterial pressure; BPM – beats per minute; CABG ‐ Coronary artery bypass graft surgery; CD – Compact disc; CCT ‐ Controlled clinical trial; DBP ‐ Diastolic blood pressure; HR ‐ Heart rate; HRV ‐ Heart rate variability; N ‐ Numbers; RCT – Randomized controlled trial; RR ‐ Respiratory rate; SAS ‐ Self‐Rating Anxiety Scale; SBP ‐ Systolic blood pressure; SD ‐ Standard deviations; TURB ‐ Transurethral resection of the bladder; TURP ‐ Transurethral resection of the prostate; VAS ‐ Visual analogue scale; VAAS ‐ Visual analogue anxiety scale; STAI ‐ State‐Trait Anxiety Inventory for adults
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
| Not RCT or CCT | |
| Does not address preoperative anxiety; post‐test administered after the surgery | |
| No numerical data reported | |
| Does not address preoperative anxiety; music intervention provided during surgery | |
| Insufficient data reporting | |
| Insufficient data reporting | |
| Not RCT or CCT | |
| Insufficient data reporting | |
| Insufficient data reporting | |
| Not RCT or CCT | |
| Not RCT or CCT | |
| Not RCT or CCT | |
| Unable to obtain Master's thesis from University | |
| Use of binaural beat instead of music | |
| Standard deviations not reported. Unable to obtain contact information for authors | |
| Insufficient data reporting | |
| Not RCT or CCT | |
| Unclear if the study only included surgical biopsy patients. We contacted the authors but no response was received. As procedural patients (e.g., needle aspiration) are not included in this review, we decided to exclude this study | |
| Not population of interest. Participants were family members of surgical patients | |
| Did not address preoperative anxiety; post‐test administered after the surgery | |
| Insufficient data reporting | |
| Insufficient data reporting | |
| Insufficient data reporting | |
| Insufficient data reporting | |
| Does not address preoperative anxiety; music intervention provided during surgery | |
| Does not address preoperative anxiety; music intervention provided during surgery | |
| Did not use standardized measures (personal communication) | |
| Does not address preoperative anxiety; music intervention provided after surgery | |
| Insufficient data reporting | |
| Does not address preoperative anxiety; music intervention provided during surgery | |
| Does not address preoperative anxiety; music intervention provided during surgery | |
| Not RCT or CCT | |
| Does not address preoperative anxiety; music intervention provided during surgery | |
| Not RCT or CCT | |
| Insufficient data reporting | |
| Use of binaural beat instead of music | |
| Not RCT or CCT | |
| Not RCT or CCT | |
| Unable to obtain master's thesis | |
| Insufficient data reporting | |
| No standard deviations reported. Chief investigator could not provide us with this information | |
| Not RCT or CCT | |
| Did not use standardized measures (personal communication) | |
| Insufficient data reporting | |
| Insufficient data reporting | |
| Unacceptable allocation method: participants were assigned to the music intervention group based on availability of a CD player | |
| Not RCT or CCT | |
| Insufficient data reporting | |
| Unclear post‐test data reporting. Post‐test values are expressed as percentages of pretest values but it is unclear how the standard deviations were computed | |
| Did not address preoperative anxiety; only reported data on postoperative anxiety |
Characteristics of studies awaiting assessment [ordered by study ID]
| Methods | Unknown |
| Participants | Patients awaiting surgery |
| Interventions | Music versus midazolam |
| Outcomes | Preoperative anxiety |
| Notes | Unable to obtain article |
| Methods | RCT |
| Participants | Patients awaiting surgery |
| Interventions | Music |
| Outcomes | Preoperative anxiety |
| Notes | Unable to obtain article |
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 State anxiety STAI) Show forest plot | 13 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 1.1  Comparison 1 Music versus standard care, Outcome 1 State anxiety STAI). | ||||
| 1.1 All studies | 13 | 896 | Mean Difference (IV, Random, 95% CI) | ‐5.72 [‐7.27, ‐4.17] |
| 1.2 Adequate randomization | 4 | 435 | Mean Difference (IV, Random, 95% CI) | ‐5.76 [‐7.94, ‐3.57] |
| 2 Anxiety (non‐STAI) Show forest plot | 7 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 1.2 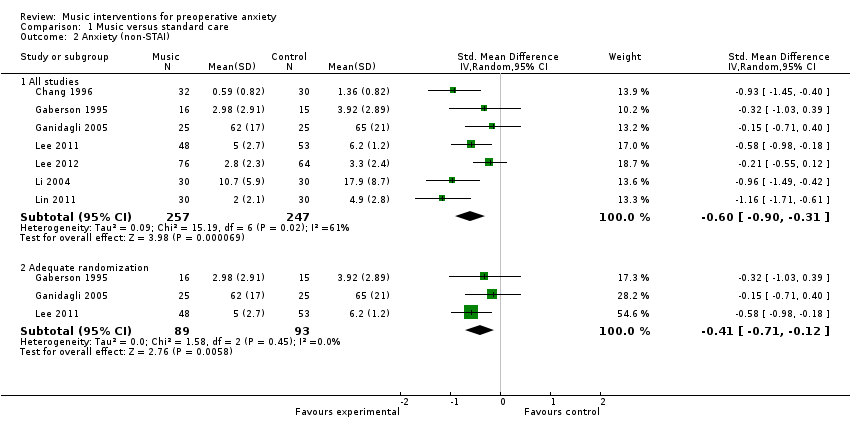 Comparison 1 Music versus standard care, Outcome 2 Anxiety (non‐STAI). | ||||
| 2.1 All studies | 7 | 504 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.60 [‐0.90, ‐0.31] |
| 2.2 Adequate randomization | 3 | 182 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.41 [‐0.71, ‐0.12] |
| 3 Heart rate Show forest plot | 16 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 1.3  Comparison 1 Music versus standard care, Outcome 3 Heart rate. | ||||
| 3.1 All studies | 16 | 1109 | Mean Difference (IV, Random, 95% CI) | ‐2.77 [‐4.76, ‐0.78] |
| 3.2 Adequate randomization | 6 | 525 | Mean Difference (IV, Random, 95% CI) | ‐2.44 [‐5.95, 1.07] |
| 4 Heart rate variability ‐ LF/HF ratio Show forest plot | 2 | 241 | Mean Difference (IV, Random, 95% CI) | ‐0.37 [‐1.16, 0.42] |
| Analysis 1.4  Comparison 1 Music versus standard care, Outcome 4 Heart rate variability ‐ LF/HF ratio. | ||||
| 5 Systolic blood pressure Show forest plot | 14 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 1.5 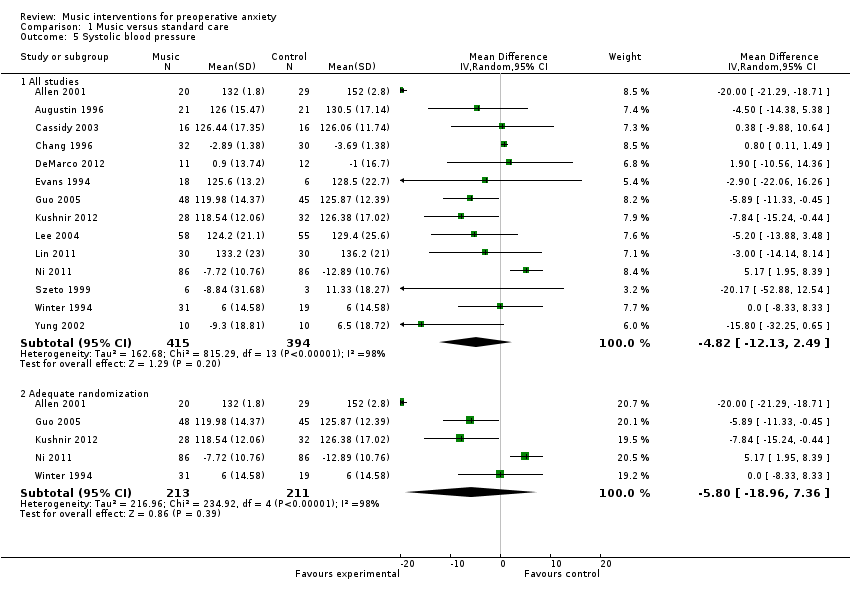 Comparison 1 Music versus standard care, Outcome 5 Systolic blood pressure. | ||||
| 5.1 All studies | 14 | 809 | Mean Difference (IV, Random, 95% CI) | ‐4.82 [‐12.13, 2.49] |
| 5.2 Adequate randomization | 5 | 424 | Mean Difference (IV, Random, 95% CI) | ‐5.80 [‐18.96, 7.36] |
| 6 Diastolic blood pressure Show forest plot | 13 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 1.6  Comparison 1 Music versus standard care, Outcome 6 Diastolic blood pressure. | ||||
| 6.1 All studies | 13 | 786 | Mean Difference (IV, Random, 95% CI) | ‐2.37 [‐4.03, ‐0.71] |
| 6.2 Adequate randomization | 5 | 424 | Mean Difference (IV, Random, 95% CI) | ‐2.74 [‐5.65, 0.17] |
| 7 Respiratory rate Show forest plot | 6 | 375 | Mean Difference (IV, Fixed, 95% CI) | 0.97 [0.82, 1.11] |
| Analysis 1.7 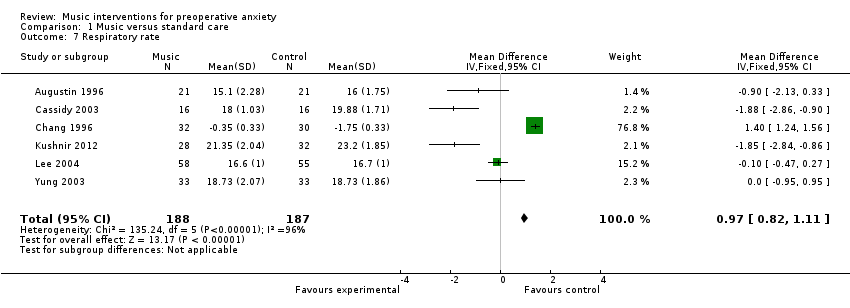 Comparison 1 Music versus standard care, Outcome 7 Respiratory rate. | ||||
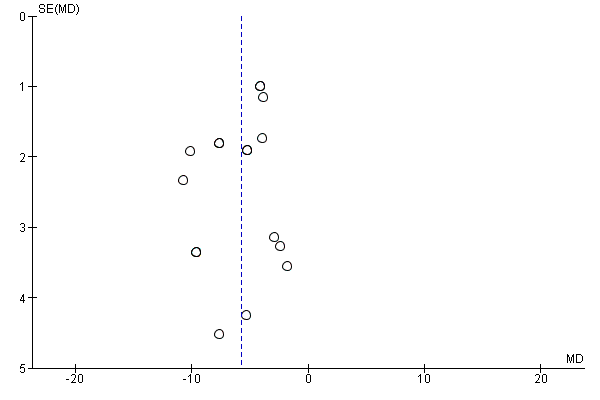
Funnel plot of comparison: 1 Music versus standard care, outcome: 1.1 State Anxiety STAI.

Excluded Study flow diagram.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Comparison 1 Music versus standard care, Outcome 1 State anxiety STAI).

Comparison 1 Music versus standard care, Outcome 2 Anxiety (non‐STAI).
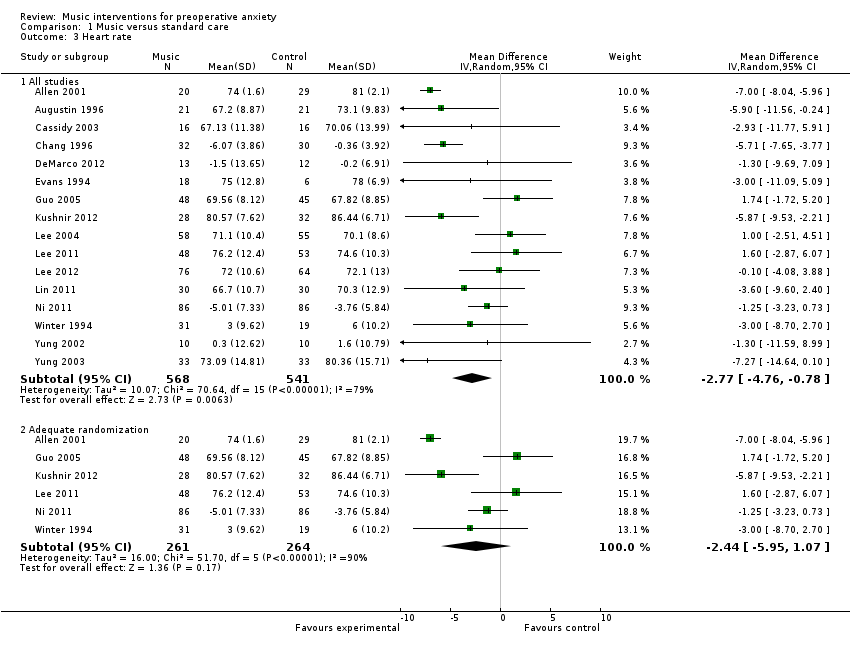
Comparison 1 Music versus standard care, Outcome 3 Heart rate.

Comparison 1 Music versus standard care, Outcome 4 Heart rate variability ‐ LF/HF ratio.

Comparison 1 Music versus standard care, Outcome 5 Systolic blood pressure.
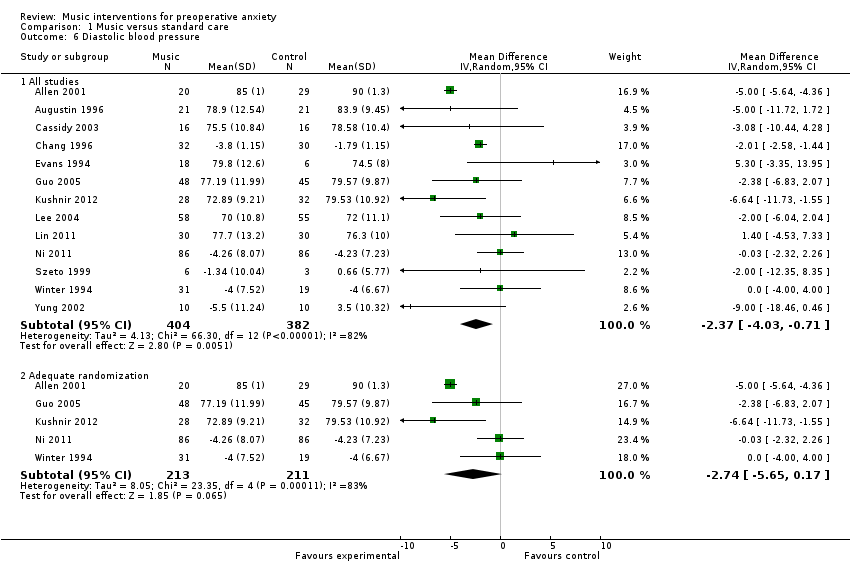
Comparison 1 Music versus standard care, Outcome 6 Diastolic blood pressure.

Comparison 1 Music versus standard care, Outcome 7 Respiratory rate.
| Patient or population: patients with preoperative anxiety | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Standard care | Music | |||||
| Preoperative anxiety (STAI) | The mean preoperative anxiety (stai) ranged across control groups from | The mean preoperative anxiety (stai) in the intervention groups was | 896 | ⊕⊕⊝⊝ | ||
| Preoperative anxiety (non‐STAI) | The mean preoperative anxiety (non‐stai) in the intervention groups was | 504 | ⊕⊕⊝⊝ | |||
| Heart rate | The mean heart rate ranged across control groups from | The mean heart rate in the intervention groups was | 1109 | ⊕⊝⊝⊝ | ||
| Heart rate variability | The mean heart rate variability ranged across control groups from | The mean heart rate variability in the intervention groups was | 241 | ⊕⊝⊝⊝ | ||
| Systolic blood pressure | The mean systolic blood pressure ranged across control groups from | The mean systolic blood pressure in the intervention groups was | 809 | ⊕⊝⊝⊝ | ||
| Diastolic blood pressure | The mean diastolic blood pressure ranged across control groups from | The mean diastolic blood pressure in the intervention groups was | 786 | ⊕⊝⊝⊝ | ||
| Respiratory rate | The mean respiratory rate ranged across control groups from | The mean respiratory rate in the intervention groups was | 375 | ⊕⊝⊝⊝ | ||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 The majority of the trials were assessed as high risk of bias studies | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 State anxiety STAI) Show forest plot | 13 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 All studies | 13 | 896 | Mean Difference (IV, Random, 95% CI) | ‐5.72 [‐7.27, ‐4.17] |
| 1.2 Adequate randomization | 4 | 435 | Mean Difference (IV, Random, 95% CI) | ‐5.76 [‐7.94, ‐3.57] |
| 2 Anxiety (non‐STAI) Show forest plot | 7 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 All studies | 7 | 504 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.60 [‐0.90, ‐0.31] |
| 2.2 Adequate randomization | 3 | 182 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.41 [‐0.71, ‐0.12] |
| 3 Heart rate Show forest plot | 16 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 All studies | 16 | 1109 | Mean Difference (IV, Random, 95% CI) | ‐2.77 [‐4.76, ‐0.78] |
| 3.2 Adequate randomization | 6 | 525 | Mean Difference (IV, Random, 95% CI) | ‐2.44 [‐5.95, 1.07] |
| 4 Heart rate variability ‐ LF/HF ratio Show forest plot | 2 | 241 | Mean Difference (IV, Random, 95% CI) | ‐0.37 [‐1.16, 0.42] |
| 5 Systolic blood pressure Show forest plot | 14 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5.1 All studies | 14 | 809 | Mean Difference (IV, Random, 95% CI) | ‐4.82 [‐12.13, 2.49] |
| 5.2 Adequate randomization | 5 | 424 | Mean Difference (IV, Random, 95% CI) | ‐5.80 [‐18.96, 7.36] |
| 6 Diastolic blood pressure Show forest plot | 13 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 6.1 All studies | 13 | 786 | Mean Difference (IV, Random, 95% CI) | ‐2.37 [‐4.03, ‐0.71] |
| 6.2 Adequate randomization | 5 | 424 | Mean Difference (IV, Random, 95% CI) | ‐2.74 [‐5.65, 0.17] |
| 7 Respiratory rate Show forest plot | 6 | 375 | Mean Difference (IV, Fixed, 95% CI) | 0.97 [0.82, 1.11] |